Embed Size (px)
Citation preview
SCIENTIFIC ARTICLE
MRI of double-bundle ACL reconstruction: evaluationof graft findings
Tommi Kiekara & Timo Järvelä & Heini Huhtala &
Antti Paakkala
Received: 15 June 2011 /Revised: 25 August 2011 /Accepted: 12 September 2011 /Published online: 30 September 2011# ISS 2011
AbstractObjective To demonstrate the magnetic resonance imaging(MRI) findings of double-bundle (DB) anterior cruciateligament (ACL) reconstruction grafts.Materials and methods Sixty-six patients with DB ACLreconstruction were evaluated with MRI 2 years postoper-atively. Graft thickness was measured separately by twomusculoskeletal radiologists. The MRI findings of graftdisruption, signal intensity (SI) changes, cystic degenera-tion, arthrofibrosis, and impingement were analyzed. Thestatistical significance of the association between MRIfindings was calculated.Results The mean anteromedial (AM) graft thickness wasreduced 9% and the mean posterolateral (PL) graftthickness was reduced 18% from the original graftthickness. Disruption was seen in 3% of AM grafts and6% of PL grafts and a partial tear in 8 and 23%,respectively. Both grafts were disrupted in 3% of patients.Increased SI was seen in 14% of intact AM grafts and in60% of partially torn AM grafts (p=0.032). In PL grafts the
increased SI was seen in 51% of the intact grafts and in 93% ofthe partially torn grafts (p=0.005). Cystic degeneration wasseen in 8% of AM grafts and in 5% of PL grafts. Diffusearthrofibrosis was seen in 5% of patients and a localizedcyclops lesion in 3% of patients. Impingement of the AMgraft was seen in 8% of patients.Conclusion Both grafts were disrupted in 3% of patients.Also, the frequencies of other complications were low. Theuse of orthogonal sequences in the evaluation of the PLgraft SI seems to cause volume-averaging artefacts.
Keywords MRI .Anterior cruciate ligament . Double-bundlereconstruction
Introduction
The anatomy of the anterior cruciate ligament (ACL) consistsof two bundles: anteromedial (AM) and posterolateral (PL).The bundles are named according to their insertion on the tibia.The AM bundle originates more proximally and anteriorly onthe lateral femoral condyle than the PL bundle [1–3]. On thetibial site the AM bundle inserts anteromedially and the PLbundle posterolaterally [1–3]. When the knee is extended, thePL bundle is tight and the AM bundle is relatively loose. Asthe knee is flexed, the AM bundle tightens and the PL bundleloosens. The PL bundle is also tightened during internal andexternal rotation of the tibia [4–6].
Some studies have shown that the DB (double-bundle)ACL reconstruction restores knee kinematics and especiallyrotational stability of the knee more closely than the SB(single-bundle) ACL reconstruction, although anteriorstability of the knee can be restored well with the SBACL reconstruction, too [4, 7–16]. Modern surgicaltechniques for DB ACL reconstruction incorporate two tibial
T. Kiekara (*) :A. PaakkalaMedical Imaging Centre, Tampere University Hospital,FIN-33521 Tampere, Finlande-mail: [email protected]
A. Paakkalae-mail: [email protected]
T. JärveläSports Clinic and Hospital Mehiläinen,FIN-33210 Tampere, Finlande-mail: [email protected]
H. HuhtalaSchool of Health Sciences, University of Tampere,FIN-33014 Tampere, Finlande-mail: [email protected]
Skeletal Radiol (2012) 41:835–842DOI 10.1007/s00256-011-1285-1

and two femoral tunnels and various tendon autografts andfixation devices [4, 7–16]. According to some prospective,randomized clinical studies it seems that DB ACL reconstruc-tion results in better rotational stability and fewer graft failureswhen compared to SB ACL reconstruction [9, 10, 14, 16, 17].
MRI is the preferred imaging modality for the evaluationof ACL graft reconstructions [18, 19]. Prior studies havedescribed the appearance and maturation of an intact SBACL reconstruction graft [20, 21] and also the MRIfindings of postsurgical complications [18, 19, 21–24].The most common complications include graft rupture,cystic degeneration of the graft, graft impingement, andarthrofibrosis [18, 19, 21–24].
According to Casagranda et al. [25] the complications andMRI findings of DB ACL graft reconstruction are similar tothose of SB reconstruction. The normal appearance of DBgrafts in MRI with increased proton density (PD)-weightedSI at 6 months after operation and decreased SI at 12 monthsafter operation is described by Poellinger et al. [26]. Apreliminary study investigating the T2-weighted SI of DBACL grafts 1 year after operation suggests that the PL graftSI is increased at that time compared to the AM graft SI [27].In SB ACL reconstruction the graft SI is increased in bothT1-weighted and T2-weighted images during the ligamenti-zation period 3–24 months after surgery [20, 28].
To date, there is only one prospective study [27] of the DBACL reconstruction graft MRI SI findings. Because theligamentization may cause increased graft SI up to 2 yearsafter operation we aimed to perform the MRI after theligamentization period. In this study we aim to systematicallyreport the MRI findings of both normal graft and complica-tions including disruption, cystic degeneration, arthrofibrosis,and impingement of the DB ACL reconstruction graft.
Materials and methods
Patients
Between 2004 and 2008, 75 patients underwent DB ACLreconstruction carried out by a single experienced ortho-
paedic surgeon. The inclusion criteria were primary ACLreconstruction and closed growth plates. The anatomicalDB technique used in this study and described previouslyby Järvelä [9] uses AM portal and doubled semitendinosusand doubled gracilis autografts with a bioabsorbableinterference screw fixation. Eight patients were lost tofollow-up and one patient underwent revision ACL recon-struction. Finally, 66 patients (49 male and 17 female) wereavailable for 2-year MRI evaluation. Mean patient age was35 years (range 19–59 years). The research was approvedby the medical ethics committee at the study hospital.Written consent was required.
MRI analysis
MRI was performed at a mean 22 months (range16–29 months) postoperatively with a 1.5-T SignaExcite HD imager (GE Medical Systems, Milwaukee,WI) using an eight-channel receiver/transmitter extrem-ity coil. The knee was placed into the coil in a slightflexion of a mean 8° resulting from the shape of thecoil and imaged at rest. The imaging planes werechosen the same way in all patients. The MRIsequences and parameters are shown in Table 1.
The MR images were evaluated by two experiencedmusculoskeletal radiologists who were unaware of thepatients’ clinical data. Evaluations were done on an ImpaxDS 3000 workstation (Agfa HealthCare, Mortsel, Belgium).Both radiologists measured the thickness of the graftsseparately, and the interobserver agreements were evaluat-ed. The mean values of these measurements were used.Other MRI findings were evaluated together with agree-ment by consensus.
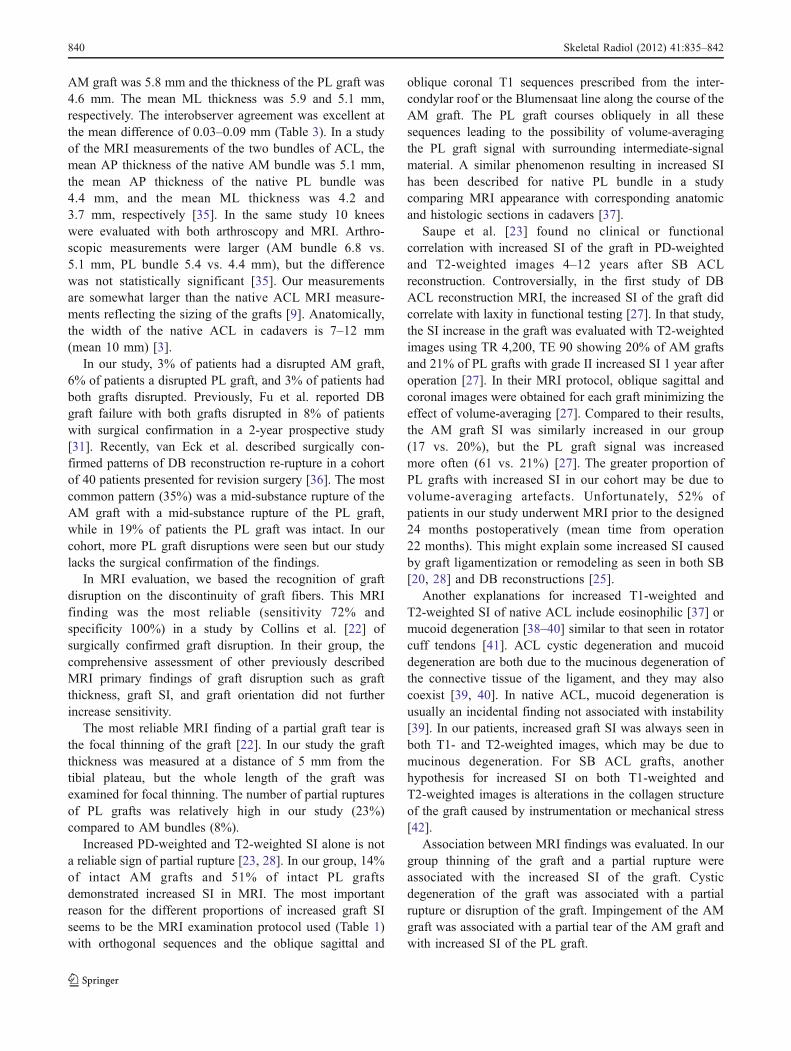
Graft thickness was measured for both grafts anteropos-teriorly (AP) and mediolaterally (ML) at a distance of 5 mmabove the tibial plateau (Fig. 1). Disrupted grafts could notbe reliably measured and were excluded from graftmeasurements. The original thickness of both grafts wasmeasured at the operation by pulling each graft in a tensionthrough the specific metallic tubes made for the measure-ments. The thickness of the graft was the same as the
Table 1 MRI sequences andtheir parameters
Sag Sagittal, Cor coronal, Axaxial, Obl oblique, FSE fast spinecho, FS fat saturation, TR timeto repeat, TE time to echo, NEXnumber of excitations, FOVfield of view, ETL echo trainlength
TR (ms) TE (ms) NEX Slice/gap (mm/mm) Matrix FOV (cm) ETL
Sag T1 FSE 500 16 2 4.0/1.0 512/224 20 2
Sag PD FSE 2,320 24 2 4.0/1.0 512/256 20 8
Sag T2 FSE 3,740 78 2 4.0/1.0 512/224 20 16
Cor T1 FSE 500 16 2 4.0/1.0 512/224 20 2
Cor T2 FSE FS 3,300 74 2 4.0/1.0 256/224 20 16
Ax PD FSE FS 1,940 40 2 4.0/1.0 256/224 18 10
Obl Sag T1 FSE 660 16 2 3.0/0.3 512/224 20 2
Obl Cor T1 FSE 660 16 2 3.0/0.3 512/224 20 2
836 Skeletal Radiol (2012) 41:835–842

diameter of the metallic tube the graft was able to passthrough [9].
Graft disruption was assessed. A graft was considereddisrupted when no intact fibers were seen and fluid signalwas interposed between the ends of graft fibers [18, 19, 22,24]. The graft was considered partially torn when a focalgraft thinning compared with any detected segment ofnormal graft diameter was seen [22].
The SI of the intra-articular portion of both grafts wasanalyzed as described by Howell [28]. The intra-articularportion of the grafts was divided into proximal, middle, anddistal thirds (Fig. 2). The SI was analyzed on PD-weightedand T2-weighted images and graded on a scale with (I) beinga normal SI similar to posterior cruciate ligament (PCL), (II)>50% of the graft having a normal SI, and (III) <50% of thegraft having a normal SI. The grade IV by Howell (100% ofthe graft having an increased SI) was incorporated withgrade III. When increased PD-weighted and T2-weighted SIwas present, T1-weighted SI changes were also analyzed.
Cystic degeneration of the graft was defined as a fluidcollection within the graft [19]. The cyst was located withinthe portion of the graft inside the femoral tunnel, in theintra-articular portion of the graft, or inside the tibial tunnel.
Roof impingement of the graft was defined as contact ofthe impinged graft with the anteroinferior margin of theintercondylar roof and posterior bowing and SI alteration ofthe graft [19, 29]. Osteophytes of the femoral intercondylarnotch were assessed.
In addition, generalized and localized arthrofibrosis wasassessed. Arthrofibrosis was defined as the presence of scar
tissue in the knee joint [19, 24]. Localized anteriorarhtrofibrosis, or cyclops lesion, was defined as a nodularfibrous lesion in the anterior intercondylar notch [24].
Finally, PCL, lateral collateral ligament (LCL), medialcollateral ligament (MCL), quadriceps tendon and patellartendon were analyzed and graded as normal, degenerativeand thickened, partially torn, or torn.
Data analysis
The data analysis was carried out using SPSS 14.0statistical software. Interobserver agreements between theradiologists’ measurements were estimated according to themethod of Bland and Altman [30] using Strata 8.2statistical software. The statistical significance of associa-tion between MRI findings was calculated using Fisher’sExact Test except for the equality of means in which thetwo-tailed t-test was used.
Results
The findings of the graft evaluation are shown in Table 2.
Graft thickness
The mean original graft thickness (femoral drill size) in theoperation for the AM graft was 6.4 mm (range 6.0–7.5 mm)and 5.9 mm (range 4.0–6.0 mm) for the PL graft. In theMRI, the mean AM graft AP thickness was 5.8 mm (range
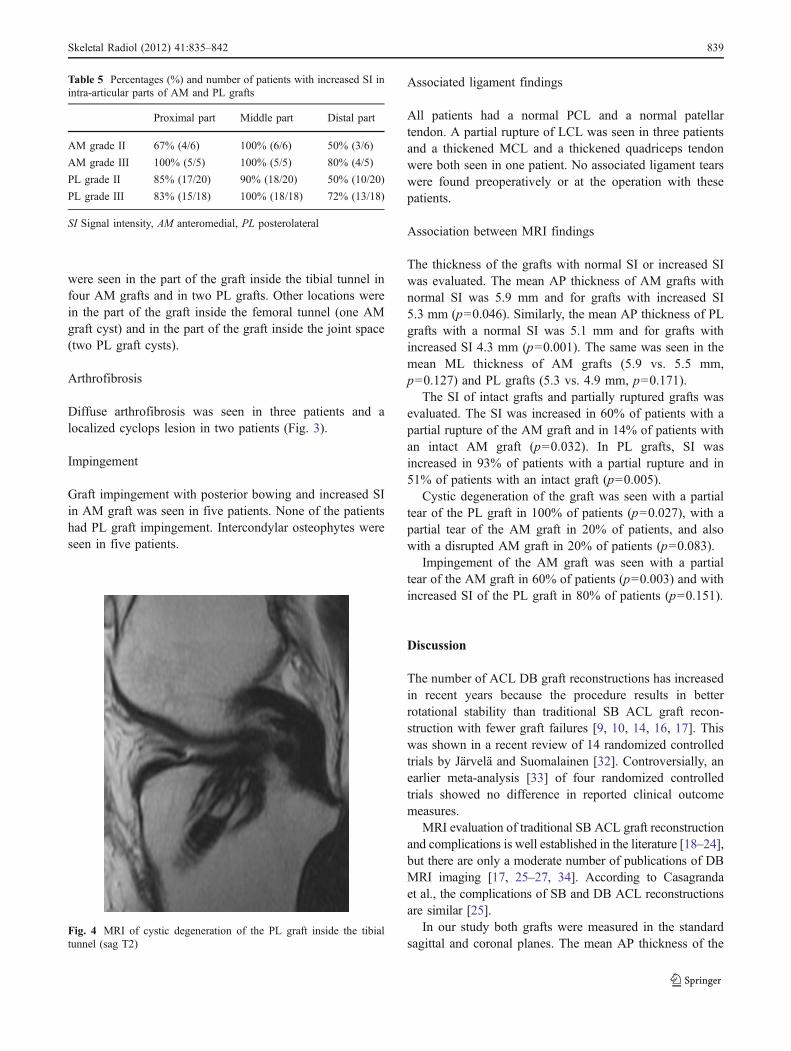
Fig. 2 Evaluation of the AM graft SI (sag PD). The SI of theproximal third is normal. The SI of the middle third is grade III, andthe distal third grade II
Fig. 1 Anteroposterior graft thickness was measured by evaluating asagittal PD-weighted image. The SI of both grafts is normal
Skeletal Radiol (2012) 41:835–842 837
2.0–8.0 mm) and the ML thickness 5.9 mm (range 3.0–9.0 mm). The mean PL graft AP thickness was 4.6 mm(range 2.0–7.0 mm) and the ML thickness was 5.1 mm(range 2.0–8.0 mm). Compared with the mean original graftthickness, the AM graft had reduced 9% and the PL graft18% in diameter. The interobserver agreement on measure-ments of the graft thickness between the two radiologistswas excellent (Table 3).
Graft disruption
Of the 66 patients included in this study, 5 patients had apartially torn AM graft and 2 had a disrupted AM graft. ThePL graft was partially torn in 15 and disrupted in 4 patients.Both AM and PL grafts were disrupted in 2 patients(Fig. 3). The frequencies of disruptions and partial rupturesare displayed in Table 4.
Graft SI findings
AM graft SI was graded normal in 53 patients, grade II in 6patients, and grade III in 5 patients. The intra-articular part
of the graft was divided into proximal, middle, and distalparts (Fig. 2). The increased AM graft SI was seen in theproximal part in 9 patients, in the middle part in 11 patients,and in the distal part in 7 patients (Table 5).
PL graft SI was graded normal in 24 patients, grade II in20 patients, and grade III in 18 patients. The increased PLgraft SI was seen in the proximal part in 32 patients, in themiddle part in 36 patients, and in the distal part in 23patients (Table 5).
Altogether, SI was increased in 17% of AM grafts and in61% of PL grafts. All of the grafts with increased PD-weightedand T2-weighted SI also had increased T1-weighted SI.
Cystic degeneration
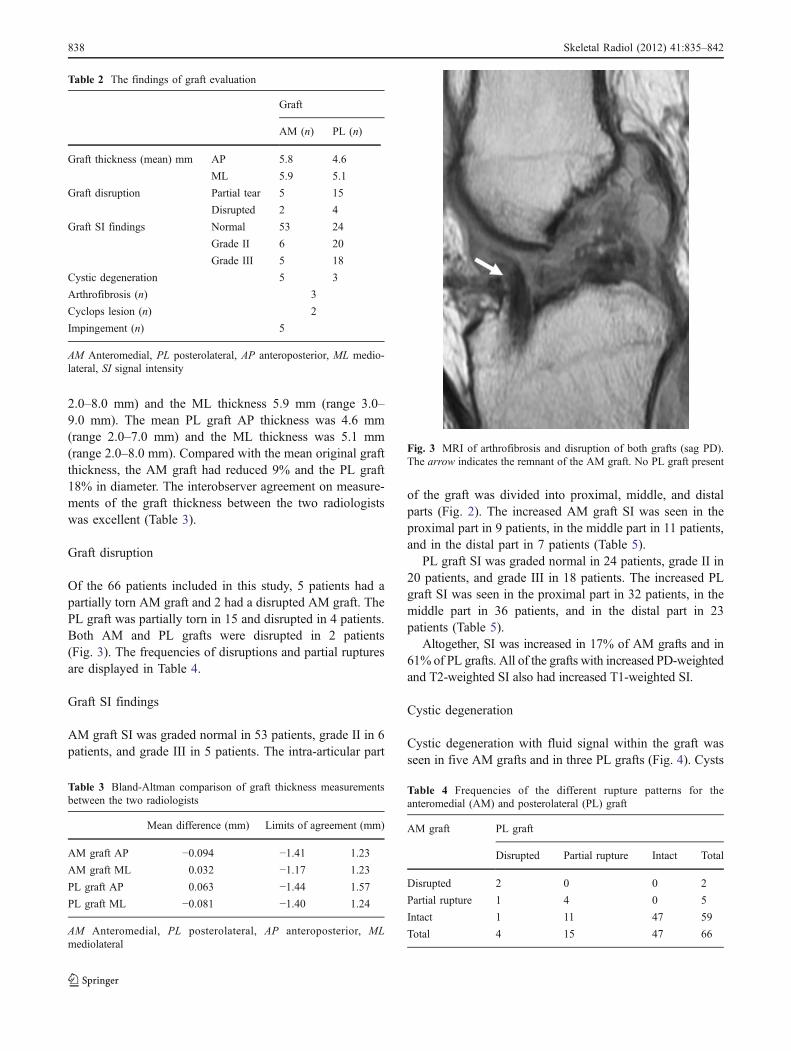
Cystic degeneration with fluid signal within the graft wasseen in five AM grafts and in three PL grafts (Fig. 4). Cysts
Table 2 The findings of graft evaluation
Graft
AM (n) PL (n)
Graft thickness (mean) mm AP 5.8 4.6
ML 5.9 5.1
Graft disruption Partial tear 5 15
Disrupted 2 4
Graft SI findings Normal 53 24
Grade II 6 20
Grade III 5 18
Cystic degeneration 5 3
Arthrofibrosis (n) 3
Cyclops lesion (n) 2
Impingement (n) 5
AM Anteromedial, PL posterolateral, AP anteroposterior, ML medio-lateral, SI signal intensity
Table 3 Bland-Altman comparison of graft thickness measurementsbetween the two radiologists
Mean difference (mm) Limits of agreement (mm)
AM graft AP −0.094 −1.41 1.23
AM graft ML 0.032 −1.17 1.23
PL graft AP 0.063 −1.44 1.57
PL graft ML −0.081 −1.40 1.24
AM Anteromedial, PL posterolateral, AP anteroposterior, MLmediolateral
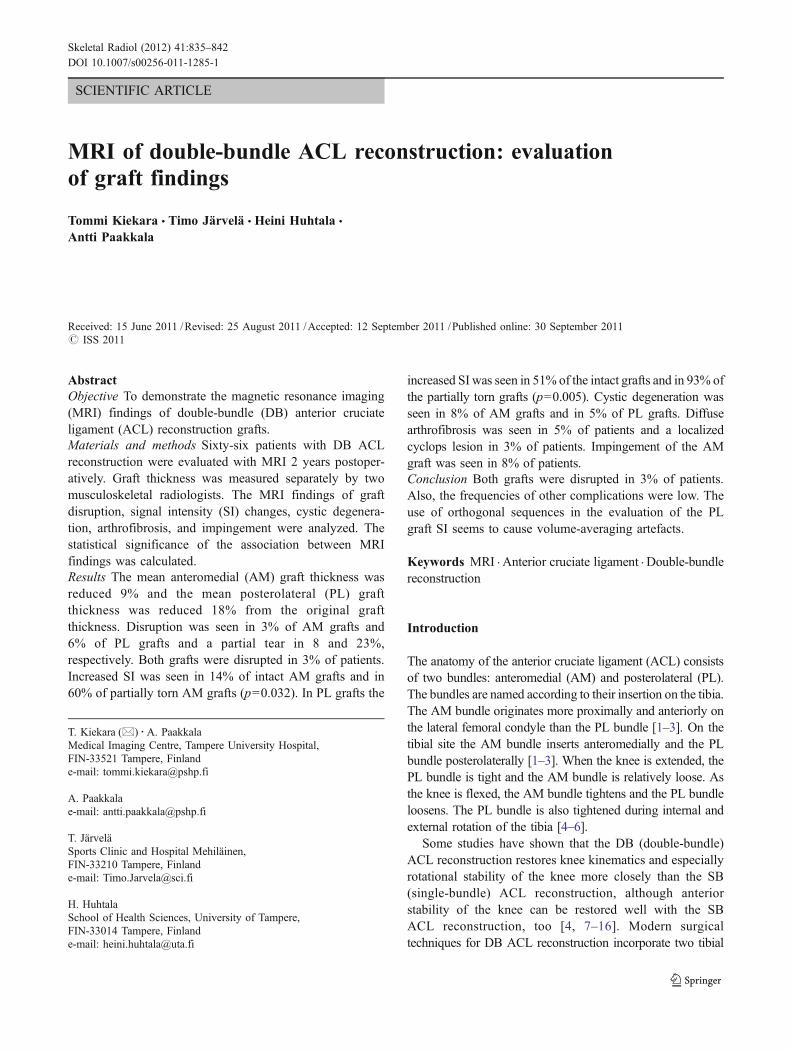
Fig. 3 MRI of arthrofibrosis and disruption of both grafts (sag PD).The arrow indicates the remnant of the AM graft. No PL graft present
Table 4 Frequencies of the different rupture patterns for theanteromedial (AM) and posterolateral (PL) graft
AM graft PL graft
Disrupted Partial rupture Intact Total
Disrupted 2 0 0 2
Partial rupture 1 4 0 5
Intact 1 11 47 59
Total 4 15 47 66
838 Skeletal Radiol (2012) 41:835–842
were seen in the part of the graft inside the tibial tunnel infour AM grafts and in two PL grafts. Other locations werein the part of the graft inside the femoral tunnel (one AMgraft cyst) and in the part of the graft inside the joint space(two PL graft cysts).
Arthrofibrosis
Diffuse arthrofibrosis was seen in three patients and alocalized cyclops lesion in two patients (Fig. 3).
Impingement
Graft impingement with posterior bowing and increased SIin AM graft was seen in five patients. None of the patientshad PL graft impingement. Intercondylar osteophytes wereseen in five patients.
Associated ligament findings
All patients had a normal PCL and a normal patellartendon. A partial rupture of LCL was seen in three patientsand a thickened MCL and a thickened quadriceps tendonwere both seen in one patient. No associated ligament tearswere found preoperatively or at the operation with thesepatients.
Association between MRI findings
The thickness of the grafts with normal SI or increased SIwas evaluated. The mean AP thickness of AM grafts withnormal SI was 5.9 mm and for grafts with increased SI5.3 mm (p=0.046). Similarly, the mean AP thickness of PLgrafts with a normal SI was 5.1 mm and for grafts withincreased SI 4.3 mm (p=0.001). The same was seen in themean ML thickness of AM grafts (5.9 vs. 5.5 mm,p=0.127) and PL grafts (5.3 vs. 4.9 mm, p=0.171).
The SI of intact grafts and partially ruptured grafts wasevaluated. The SI was increased in 60% of patients with apartial rupture of the AM graft and in 14% of patients withan intact AM graft (p=0.032). In PL grafts, SI wasincreased in 93% of patients with a partial rupture and in51% of patients with an intact graft (p=0.005).
Cystic degeneration of the graft was seen with a partialtear of the PL graft in 100% of patients (p=0.027), with apartial tear of the AM graft in 20% of patients, and alsowith a disrupted AM graft in 20% of patients (p=0.083).
Impingement of the AM graft was seen with a partialtear of the AM graft in 60% of patients (p=0.003) and withincreased SI of the PL graft in 80% of patients (p=0.151).
Discussion
The number of ACL DB graft reconstructions has increasedin recent years because the procedure results in betterrotational stability than traditional SB ACL graft recon-struction with fewer graft failures [9, 10, 14, 16, 17]. Thiswas shown in a recent review of 14 randomized controlledtrials by Järvelä and Suomalainen [32]. Controversially, anearlier meta-analysis [33] of four randomized controlledtrials showed no difference in reported clinical outcomemeasures.
MRI evaluation of traditional SB ACL graft reconstructionand complications is well established in the literature [18–24],but there are only a moderate number of publications of DBMRI imaging [17, 25–27, 34]. According to Casagrandaet al., the complications of SB and DB ACL reconstructionsare similar [25].
In our study both grafts were measured in the standardsagittal and coronal planes. The mean AP thickness of the
Table 5 Percentages (%) and number of patients with increased SI inintra-articular parts of AM and PL grafts
Proximal part Middle part Distal part
AM grade II 67% (4/6) 100% (6/6) 50% (3/6)
AM grade III 100% (5/5) 100% (5/5) 80% (4/5)
PL grade II 85% (17/20) 90% (18/20) 50% (10/20)
PL grade III 83% (15/18) 100% (18/18) 72% (13/18)
SI Signal intensity, AM anteromedial, PL posterolateral
Fig. 4 MRI of cystic degeneration of the PL graft inside the tibialtunnel (sag T2)
Skeletal Radiol (2012) 41:835–842 839
AM graft was 5.8 mm and the thickness of the PL graft was4.6 mm. The mean ML thickness was 5.9 and 5.1 mm,respectively. The interobserver agreement was excellent atthe mean difference of 0.03–0.09 mm (Table 3). In a studyof the MRI measurements of the two bundles of ACL, themean AP thickness of the native AM bundle was 5.1 mm,the mean AP thickness of the native PL bundle was4.4 mm, and the mean ML thickness was 4.2 and3.7 mm, respectively [35]. In the same study 10 kneeswere evaluated with both arthroscopy and MRI. Arthro-scopic measurements were larger (AM bundle 6.8 vs.5.1 mm, PL bundle 5.4 vs. 4.4 mm), but the differencewas not statistically significant [35]. Our measurementsare somewhat larger than the native ACL MRI measure-ments reflecting the sizing of the grafts [9]. Anatomically,the width of the native ACL in cadavers is 7–12 mm(mean 10 mm) [3].
In our study, 3% of patients had a disrupted AM graft,6% of patients a disrupted PL graft, and 3% of patients hadboth grafts disrupted. Previously, Fu et al. reported DBgraft failure with both grafts disrupted in 8% of patientswith surgical confirmation in a 2-year prospective study[31]. Recently, van Eck et al. described surgically con-firmed patterns of DB reconstruction re-rupture in a cohortof 40 patients presented for revision surgery [36]. The mostcommon pattern (35%) was a mid-substance rupture of theAM graft with a mid-substance rupture of the PL graft,while in 19% of patients the PL graft was intact. In ourcohort, more PL graft disruptions were seen but our studylacks the surgical confirmation of the findings.
In MRI evaluation, we based the recognition of graftdisruption on the discontinuity of graft fibers. This MRIfinding was the most reliable (sensitivity 72% andspecificity 100%) in a study by Collins et al. [22] ofsurgically confirmed graft disruption. In their group, thecomprehensive assessment of other previously describedMRI primary findings of graft disruption such as graftthickness, graft SI, and graft orientation did not furtherincrease sensitivity.
The most reliable MRI finding of a partial graft tear isthe focal thinning of the graft [22]. In our study the graftthickness was measured at a distance of 5 mm from thetibial plateau, but the whole length of the graft wasexamined for focal thinning. The number of partial rupturesof PL grafts was relatively high in our study (23%)compared to AM bundles (8%).
Increased PD-weighted and T2-weighted SI alone is nota reliable sign of partial rupture [23, 28]. In our group, 14%of intact AM grafts and 51% of intact PL graftsdemonstrated increased SI in MRI. The most importantreason for the different proportions of increased graft SIseems to be the MRI examination protocol used (Table 1)with orthogonal sequences and the oblique sagittal and
oblique coronal T1 sequences prescribed from the inter-condylar roof or the Blumensaat line along the course of theAM graft. The PL graft courses obliquely in all thesesequences leading to the possibility of volume-averagingthe PL graft signal with surrounding intermediate-signalmaterial. A similar phenomenon resulting in increased SIhas been described for native PL bundle in a studycomparing MRI appearance with corresponding anatomicand histologic sections in cadavers [37].
Saupe et al. [23] found no clinical or functionalcorrelation with increased SI of the graft in PD-weightedand T2-weighted images 4–12 years after SB ACLreconstruction. Controversially, in the first study of DBACL reconstruction MRI, the increased SI of the graft didcorrelate with laxity in functional testing [27]. In that study,the SI increase in the graft was evaluated with T2-weightedimages using TR 4,200, TE 90 showing 20% of AM graftsand 21% of PL grafts with grade II increased SI 1 year afteroperation [27]. In their MRI protocol, oblique sagittal andcoronal images were obtained for each graft minimizing theeffect of volume-averaging [27]. Compared to their results,the AM graft SI was similarly increased in our group(17 vs. 20%), but the PL graft signal was increasedmore often (61 vs. 21%) [27]. The greater proportion ofPL grafts with increased SI in our cohort may be due tovolume-averaging artefacts. Unfortunately, 52% ofpatients in our study underwent MRI prior to the designed24 months postoperatively (mean time from operation22 months). This might explain some increased SI causedby graft ligamentization or remodeling as seen in both SB[20, 28] and DB reconstructions [25].
Another explanations for increased T1-weighted andT2-weighted SI of native ACL include eosinophilic [37] ormucoid degeneration [38–40] similar to that seen in rotatorcuff tendons [41]. ACL cystic degeneration and mucoiddegeneration are both due to the mucinous degeneration ofthe connective tissue of the ligament, and they may alsocoexist [39, 40]. In native ACL, mucoid degeneration isusually an incidental finding not associated with instability[39]. In our patients, increased graft SI was always seen inboth T1- and T2-weighted images, which may be due tomucinous degeneration. For SB ACL grafts, anotherhypothesis for increased SI on both T1-weighted andT2-weighted images is alterations in the collagen structureof the graft caused by instrumentation or mechanical stress[42].
Association between MRI findings was evaluated. In ourgroup thinning of the graft and a partial rupture wereassociated with the increased SI of the graft. Cysticdegeneration of the graft was associated with a partialrupture or disruption of the graft. Impingement of the AMgraft was associated with a partial tear of the AM graft andwith increased SI of the PL graft.
840 Skeletal Radiol (2012) 41:835–842

Limitations of our study include the lack of obliquesagittal and coronal sequences along the course of the PLgraft resulting in volume-averaging of PL graft SI inorthogonal sequences. Another limitation is the lack ofsurgical confirmation of the findings of this study. Becauseof the prospective nature of the study, the follow-up MRIwas performed 2 years after operation and for most patientsthere was no indication for re-arthroscopy.
In summary, this study describes the 2-year postopera-tive MRI findings and the frequencies of complications ofDB ACL grafts. AM and PL graft thicknesses were nearoriginal graft thickness after operation. The AM graft waspartially torn in 8% and disrupted in 3% of patients. The PLgraft was partially torn in 23% and disrupted in 6% ofpatients. Both grafts were disrupted in 3% of patients. Forthe clinical point of view, the disruption of both grafts is animportant finding because it can lead to revision ACLsurgery if the patient complains of symptoms of instabilityin the operated knee as well. Luckily, only 3% of thepatients had both grafts disrupted. However, only thefollowing years will reveal if the partial tears of the graftsseen in MRI will lead to total disruption of the grafts andinstability symptoms of the operated knees with a need fora revision ACL surgery. We will continue the study follow-up to find out the long-term MRI findings, and the revisionrate of the patients needing revision ACL surgery becauseof graft failure and instability symptoms.
Conflict of interest The authors declare that they have no conflict ofinterest.
References
1. Colombet P, Robinson J, Christel P, et al. Morphology of anteriorcruciate ligament attachments for anatomic reconstruction: acadaveric dissection and radiographic study. Arthroscopy.2006;22:984–92.
2. Petersen W, Zantop T. Anatomy of the anterior cruciate ligamentwith regard to its two bundles. Clin Orthoped Relat Res.2007;454:35–47.
3. Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, MenetreyJ. Anatomy of the anterior cruciate ligament. Knee Surg SportsTraumatol Arthrosc. 2006;14:204–13.
4. Ishibashi Y, Tsuda E, Fukuda A, Tsukada H, Toh S. Stabilityevaluation of single-bundle and double-bundle reconstructionduring navigated ACL reconstruction. Sports Med Arthrosc.2008;16:77–83.
5. Ishibashi Y, Tsuda E, Yamamoto Y, Tsukada H, Toh S. Navigationevaluation of the pivot-shift phenomenon during double-bundleanterior cruciate ligament reconstruction: is the posterolateralbundle more important? Arthroscopy. 2009;25:488–95.
6. Wu JL, Seon JK, Gadikota HR, et al. In situ forces in theanteromedial and posterolateral bundles of the anterior cruciateligament under simulated functional loading conditions. Am JSports Med. 2010;38:558–63.
7. Aglietti P, Giron F, Losco M, Cuomo P, Ciardullo A, MondanelliN. Comparison between single- and double-bundle anteriorcruciate ligament reconstruction: a prospective, randomized,single-blinded clinical trial. Am J Sports Med. 2010;38:25–34.
8. Hofbauer M, Valentin P, Kdolsky R, et al. Rotational andtranslational laxity after computer-navigated single- and double-bundle anterior cruciate ligament reconstruction. Knee SurgSports Traumatol Arthrosc. 2010;18:1201–7.
9. Järvelä T. Double-bundle versus single-bundle anterior cruciateligament reconstruction: a prospective, randomize clinical study.Knee Surg Sports Traumatol Arthrosc. 2007;15:500–7.
10. Järvelä T, Moisala AS, Sihvonen R, Järvelä S, Kannus P, JärvinenM. Double-bundle anterior cruciate ligament reconstruction usinghamstring autografts and bioabsorbable interference screw fixa-tion: prospective, randomized, clinical study with 2-year results.Am J Sports Med. 2008;36:290–7.
11. Kim SJ, Jo SB, Kumar P, Oh K. Comparison of single- anddouble-bundle anterior cruciate ligament reconstruction usingquadriceps tendon-bone autografts. Arthroscopy. 2009;25:70–7.
12. Kondo E, Merican AM, Yasuda K, Amis AA. Biomechanicalcomparisons of knee stability after anterior cruciate ligamentreconstruction between 2 clinically available transtibial proce-dures: anatomic double bundle versus single bundle. Am J SportsMed. 2010;38:1349–58.
13. Kondo E, Yasuda K, Azuma H, Tanabe Y, Yagi T. Prospectiveclinical comparisons of anatomic double-bundle versus single-bundle anterior cruciate ligament reconstruction procedures in 328consecutive patients. Am J Sports Med. 2008;36:1675–87.
14. Muneta T, Koga H, Mochizuki T, et al. A prospective randomizedstudy of 4-strand semitendinosus tendon anterior cruciate ligamentreconstruction comparing single-bundle and double-bundle techni-ques. Arthroscopy. 2007;23:618–28.
15. Seon JK, Park SJ, Lee KB, Yoon TR, Seo HY, Song EK. Stabilitycomparison of anterior cruciate ligament between double- andsingle-bundle reconstructions. Int Orthop. 2009;33:425–9.
16. Siebold R, Dehler C, Ellert T. Prospective randomized comparisonof double-bundle versus single-bundle anterior cruciate ligamentreconstruction. Arthroscopy. 2008;24:137–45.
17. Suomalainen P, Moisala AS, Paakkala A, Kannus P, Järvelä T.Double-bundle versus single-bundle anterior cruciate ligamentreconstruction: randomized clinical and magnetic resonanceimaging study with 2-year follow-up. Am J Sports Med.2011;39:1615–22.
18. Recht MP, Kramer J. MR imaging of the postoperative knee: apictorial essay. Radiographics. 2002;22:765–74.
19. Papakonstantinou O, Chung CB, Chanchairujira K, Resnick DL.Complications of anterior cruciate ligament reconstruction: MRimaging. Eur Radiol. 2003;13:1106–17.
20. Vogl TJ, Schmitt J, Lumbrich J, et al. Reconstructed anteriorcruciate ligaments using patellar tendon ligament grafts. Diagnos-tic value of contrast-enhanced MRI in a 2-year follow-up regimen.Eur Radiol. 2001;11:1450–6.
21. White LM, Kramer J, Recht MP. MR imaging evaluation of thepostoperative knee: ligaments, menisci, and articular cartilage.Skeletal Radiol. 2005;34:431–52.
22. Collins MS, Unruh KP, Bond JR, Mandrekar JN. Magneticresonance imaging of surgically confirmed anterior cruciateligament graft disruption. Skeletal Radiol. 2008;37:233–43.
23. Saupe N et al. Anterior cruciate ligament reconstruction grafts:MR imaging features at long-term follow-up—correlation withfunctional and clinical evaluation. Radiology. 2008;249:581–90.
24. Bencardino JT, Beltran J, Feldman MI, Rose DJ. MR imaging ofcomplications of anterior cruciate ligament graft reconstruction.Radiographics. 2009;29:2115–26.
25. Casagranda BC, Maxwell NJ, Kavanagh EC, Towers JD, Shen W,Fu FF. Normal appearance and complications of double-bundle
Skeletal Radiol (2012) 41:835–842 841

and selective-bundle anterior ligament reconstructions using optimalMRI techniques. AJR Am J Roentgenol. 2009;192:1407–15.
26. Poellinger A, Scheffler S, Hamm B, Asbach P. Magneticresonance imaging of double-bundle anterior cruciate ligamentreconstruction. Skeletal Radiol. 2009;38:308–15.
27. Sonoda M, Morikawa T, Tsuchiya K, Moriya H. Correlationbetween knee laxity and graft appearance on magneticreconance imaging after double-bundle hamstring graftanterior cruciate ligament reconstruction. Am J Sports Med.2007;35:936–42.
28. Howell SM, Clark JA, Blasier RD. Serial magnetic resonanceimaging of hamstring anterior cruciate ligament autograftsduring the first year of implantation. Am J Sports Med.1991;19:42–7.
29. Howell SM. Principles for placing the tibial tunnel and avoidingroof impingement during reconstruction of a torn anterior cruciateligament. Knee Surg Sports Traumatol Arthrosc. 1998;6 suppl 1:S49–55.
30. Bland JM, Altman DG. Statistical methods for assessingagreement between two methods of clinical measurements.Lancet. 1986;8:307–10.
31. Fu FH, Shen W, Starman JS, Okeke N, Irrgang JJ. Primaryanatomic double-bundle anterior cruciate ligament reconstruction:a preliminary 2-year prospective study. Am J Sports Med.2008;36:1263–74.
32. Järvelä T, Suomalainen P. ACL reconstruction with double-bundletechnique: a review on clinical results. Phys Sportsmed.2011;39:85–92.
33. Meredick RB, Vance KJ, Appleby D, Lubowitz JH. Outcome ofsingle-bundle versus double-bundle reconstruction of the anteriorcruciate ligament: a meta-analysis. Am J Sports Med.2008;36:1414–21.
34. Giaconi JC, Allen CR, Steinbach LS. Anterior cruciate ligamentgraft reconstruction: clinical, technical, and imaging overview.Top Magn Reson Imaging. 2009;20:129–50.
35. Cohen SB, VanBeek C, Starman JS, Armfield D, Irrgang JJ, FuFH. MRI measurement of the 2 bundles of the normal anteriorcruciate ligament. Orthopedics 2009;32:687. doi:10.3928/01477447-20090728-35.
36. van Eck CF, Kropf EJ, Romanowski JR, Lesniak BP, TranovichMJ, van Dijk CN, et al. ACL graft re-rupture after double-bundlereconstruction: factors that influence the intra-articular pattern ofinjury. Knee Surg Sports Traumatol Arthrosc. 2011;19:340–6.
37. Hodler J, Haghighi P, Trudell D, Resnick D. The cruciateligaments of the knee: correlation between MR appearance andgross and histologic findings in cadaveric specimens. AJR Am JRoentgenol. 1992;159:357–60.
38. McIntyre J, Moelleken S, Tirman P. Mucoid degeneration of theanterior cruciate ligament mistaken for ligamentous tears. SkeletalRadiol. 2001;30:312–5.
39. Bergin D, Morrison WB, Carrino JA, Nallamshetty SN,Bartolozzi AR. Anterior cruciate ligament ganglia and mucoiddegeneration: coexistence and clinical correlation. AJR Am JRoentgenol. 2004;182:1283–7.
40. Bining J, Andrews G, Forster BB. The ABCs of the anteriorcruciate ligament: a primer for magnetic resonance imagingassessment of the normal, injured and surgically repaired anteriorcruciate ligament. Br J Sports Med. 2009;43:856–62.
41. Buck FM, Grehn H, Hilbe M, Pfirrmann CWA, Manzanell S,Hodler J. Magnetic resonance histologic correlation in rotator cufftendons. J Magn Res Im. 2010;32:165–72.
42. Jansson KA et al. MRI of the anterior cruciate ligament repairwith patellar and hamstring autografts. Skeletal Radiol.2001;30:8–14.
842 Skeletal Radiol (2012) 41:835–842





























