Embed Size (px)
Citation preview

REVIEW
Mucinous carcinoma of the rectum: a distinctclinicopathological entity
M. Chand • S. Yu • R. I. Swift • G. Brown
Received: 16 June 2013 / Accepted: 18 November 2013 / Published online: 11 December 2013
� Springer-Verlag Italia 2013
Abstract
Purpose The definition of mucinous tumours relies on
quantification of the amount of mucus produced by neo-
plastic cells within the rectum. This has changed over the
years to include varying degrees of mucin production. The
inconsistency of diagnosis has led to conflicting reports in
the literature regarding clinical outcomes and treatment
response. A universally accepted definition and improved
imaging and surgical techniques in the last decade are now
challenging the traditional view of these tumours. The aim
of this review was to present the current evidence on the
clinicopathological characteristics of mucinous tumours of
the rectum.
Methods A systematic review was conducted using Pre-
ferred Reporting for Systematic Reviews and Meta-Anal-
yses guidelines. A literature search was performed using
the Ovid SP to search both EMBASE and MEDLINE
databases, Google Scholar and PubMed to find all studies
relating to mucinous carcinoma of the rectum. The search
dates were between 1 January 1965 and 1 March 2013.
Results Mucinous tumours comprise 5–20 % of all rectal
cancers and commonly present at a more advanced stage
and in younger patients. They are readily identified on
MRI, and the diagnosis is confirmed on histological ana-
lysis, demonstrating more than 50 % of extracellular mucin
within the tumour complex. They carry an overall worse
prognosis compared to adenocarcinoma of the same stage.
The response to oncological treatment remains
controversial.
Conclusion Mucinous tumours of the rectum are less well
understood than non-mucinous adenocarcinoma. This is
due to the inconsistent histopathological definitions of the
past making comparison of clinical outcome data difficult.
They remain challenging to treat and are associated with a
poor prognosis. A universally accepted definition and the
role of imaging techniques such as MRI to accurately
detect mucinous tumours are likely to lead to a better
understanding of these cancers.
Keywords Mucinous carcinoma � Rectum �Magnetic resonance imaging � Histopathology �Neoadjuvant chemoradiotherapy � Rectal cancer
Introduction
Mucinous carcinoma is a specific morphological subtype of
rectal cancer. It is characterised by an abundance of
extracellular mucin secreted by overactive neoplastic aci-
nar cells. Mucin-producing tumours have been described in
other sites such as breast, prostate, ovary and pancreas and
share some generic characteristics [1]. The abundance of
mucin within the tumour complex gives it a unique
appearance both histologically and radiologically. Contrast
this with signet cell carcinomas, which are a specific type
of mucin-producing tumour in which single neoplastic cells
demonstrate large amounts of intracytoplasmic mucin that
results in displacement of the nuclei.
Over the years, there has been debate on the precise
histological definition of mucinous tumours, which has
M. Chand (&) � S. Yu � G. Brown
Royal Marsden Hospital, Downs Road, Sutton SM2 5PT, UK
e-mail: [email protected]; [email protected]
M. Chand � G. Brown
Royal Marsden Hospital, Fulham Road, London, UK
M. Chand � R. I. Swift
Croydon University Hospital, London Road,
Croydon CR7 7YE, UK
123
Tech Coloproctol (2014) 18:335–344
DOI 10.1007/s10151-013-1099-3

made interpretation of studies problematic. The current
accepted definition, initially proposed by Jass, is based on
the presence of a minimum of 50 % of mucin to tumour
volume [2]. Previous studies have used varying propor-
tions of mucin to define these tumours [3, 4]. They rep-
resent 5–20 % of all colorectal cancers [5–8] and are
generally considered to have a worse prognosis than non-
mucinous tumours of the rectum. Furthermore, they are
also suggested to have a limited response to oncological
treatments.
This paper reviews the clincopathological characteristics
of mucinous rectal cancer and presents the evidence on
treatment response to determine whether these tumours
may be considered as a unique entity.
Methods
Identification of studies
An electronic search was carried out using MEDLINE
(1965–2013), EMBASE (1980–2013), CINAHL (1982–
2013) and the Cochrane library databases. The following
medical subject heading (MeSH) terms and keywords were
used as follows: The keywords ‘‘mucinous’’; ‘‘mucoid’’;
‘‘colloid’’; ‘‘colorectal’’; ‘‘rectal’’; ‘‘tumours/tumors’’;
‘‘cancer’’ were used in combination. The ‘‘related articles’’
function was used to broaden the search, and all
abstracts, studies and citations retrieved were scanned for
subject relevance. The latest date of this search was 1
March 2013.
Complete articles of all potentially relevant manuscripts
were retrieved and evaluated for inclusion. To be included
in this review process, additional references from the col-
lective libraries of the senior authors were identified.
Reference lists of all relevant publications were hand-
searched for additional studies missed by the search strat-
egy, and this cross-referencing continued until no further
relevant publications were identified.
Study inclusion criteria and data extraction
Study methodology was carried out in accordance with
the ‘‘Preferred Reporting for Systematic Reviews and
Meta-Analyses’’ (PRISMA) recommendations for
improving the standard of systematic reviews. Where
multiple studies describing the same patient population
were identified, the most recent publication was used
unless additional information was imparted by earlier
work (Fig. 1).
Fig. 1 Flowchart showing the
systematic methodology used to
extract articles for review
336 Tech Coloproctol (2014) 18:335–344
123
Results
Epidemiology and clinical characteristics
Mucinous carcinoma accounts for between 5 and 20 % of
all colorectal cancers [5–8]. It is relatively rare to find such
tumours in the rectum, being most commonly found in the
proximal colon. One of the largest studies examining the
outcomes of mucinous tumours investigated 16,991
patients and found that just over 18 % of all mucinous
tumours were found in the rectum compared with 29 % of
non-mucinous tumours [9]. A recent meta-analysis of
outcomes in mucinous colon cancer, which included some
studies with rectal tumours, reported that mucinous
tumours were more frequently found proximal to the
splenic flexure compared to non-mucinous adenocarcinoma
[10]. Conversely, mucinous tumours are more common
than non-mucinous in the proximal colon. A study using
the National Cancer Database in the USA reported that
60 % of mucinous tumours were right-sided compared to
42 % of non-mucinous tumours [11]. Consorti et al. [12]
conducted a prospective study of mucinous and non-
mucinous tumours and reported 31 % of mucinous tumours
in the rectum compared to 44.3 % non-mucinous.
There is a higher incidence in younger patients [13–15].
A study by Dozois et al. [16], which investigated the
characteristics of colon and rectal cancer in patients below
the age of 50, found that patients with mucinous tumours
had a mean age at presentation of 42.2 years. Furthermore,
rectal cancers were found to be more common below the
age of 50 (49.1 vs. 21.9 %). Other studies have shown
similar results [17, 18]. Wu and colleagues used a cut-off
of 39 years in their comparison of mucinous and non-
mucinous tumours, and although this included patients with
colonic cancer as well, they found mucinous tumours more
commonly in patients \39 years old [19]. A further study
of 2,089 patients (of which 144 had mucinous tumours)
reported a mean age at presentation of 54.2 ± 16.25 years.
This was statistically less than patients with non-mucinous
adenocarcinoma who had a mean age at presentation of
58.73 ± 13.62 years [20].
Morphology and pathological characteristics
Histological diagnosis remains the ‘‘gold standard’’. Mucin
produced by the tumour cells aggregates into ‘‘pools’’ or
‘‘lakes’’, which produce a distinctive pattern on haema-
toxylin and eosin stain (H&E stain). Although histopa-
thological detection of the mucinous component of
tumours is not particularly challenging, sufficient tissue is
required to make a diagnosis. Therefore, there may be
under-reporting using biopsy specimens due to insufficient
tissue [21], and definitive diagnosis is confirmed on ana-
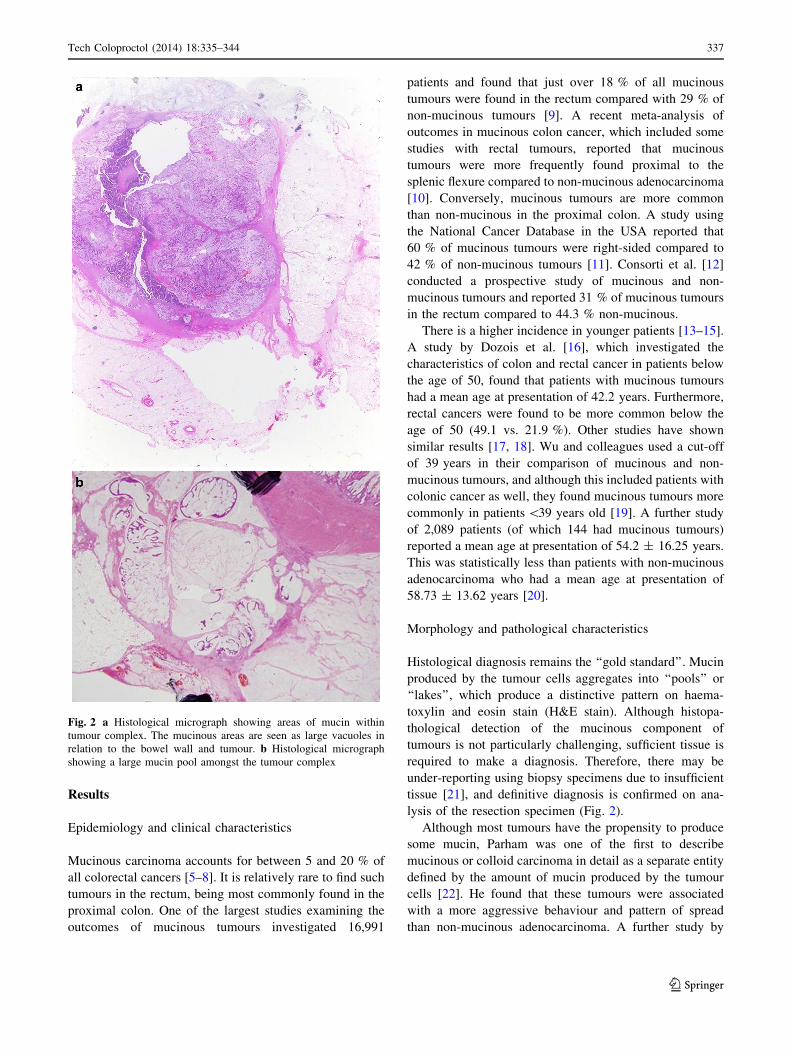
lysis of the resection specimen (Fig. 2).
Although most tumours have the propensity to produce
some mucin, Parham was one of the first to describe
mucinous or colloid carcinoma in detail as a separate entity
defined by the amount of mucin produced by the tumour
cells [22]. He found that these tumours were associated
with a more aggressive behaviour and pattern of spread
than non-mucinous adenocarcinoma. A further study by
Fig. 2 a Histological micrograph showing areas of mucin within
tumour complex. The mucinous areas are seen as large vacuoles in
relation to the bowel wall and tumour. b Histological micrograph
showing a large mucin pool amongst the tumour complex
Tech Coloproctol (2014) 18:335–344 337
123

Symonds and Vickery reviewed the pathological charac-
teristics of mucinous tumours and found that the micro-
scopic appearance of these tumours is of particular interest
with regard to their behaviour [5]. They found that mucin
deposits comprise the main bulk of the tumour complex
and are lined by epithelial cells around their perimeter.
They proposed that the spread of mucin separated the
muscle bundles but upon reaching the perirectal fat showed
pooling. This may explain the perceived aggressiveness of
these tumours. One theory is that the tumour cells have the
ability to imbibe water causing swelling of the tumour
complex. As they splay the muscle structure and pass
through the layers of the bowel wall, they disseminate
tumour cells. This is similar to the pressure theory put
forward by Sugarbaker whereby the mucin exerts a pres-
sure effect on the bowel wall structure, thus disseminating
cancer cells into the peritoneal cavity that are taken up into
lymphatics [23].
Clinical outcomes and survival
Survival outcomes between mucinous and non-mucinous
tumours have been much studied. A recent meta-analysis of
mucinous cancers of the colon and rectum showed a worse
prognosis for mucinous cancers compared with non-
mucinous types, even when corrected for stage at presen-
tation [10]. Previously, suggestions had been made that any
difference in clinical outcomes between mucinous and non-
mucinous carcinomas were attributed to a more advanced
stage at presentation. There is a higher incidence of stage III
and IV disease associated with mucinous tumours. They are
more likely to have lymph nodes involvement in addition to
increased tumour penetration [11, 20, 24]. The association
with lymph node involvement has led to suggestions of
more radical dissections for this tumour subtype [25].
A study by Hyngstrom et al. [11] found that mucinous
subtype was only associated with worse survival outcomes
when the tumour was located in the rectum. The hazard
ratio (HR) of death was 1.22 (95 % CI 1.16–1.29), for
rectal cancers but a HR of 1.03 (95 % CI 1.00–1.06), for
colonic cancers. This contrasts with signet cell tumours (a
special type of mucinous tumour) who had an increased
risk of death regardless of tumour location.
In a study of 97 patients with mucinous colorectal
cancer who underwent surgery with curative intent, the
clinically significant predictive factors on multivariate
analysis included stage at diagnosis, mucinous histology,
tumour location, gender and age [26]. Mucinous tumours
were found to have a worse survival independent of other
factors. Curative surgery was defined as obtaining a mar-
gin-free resection; however, details on surgical technique
and whether surgery was based on principles of total
mesorectal excision (TME) were not provided.
One of the largest studies into the outcomes of
mucinous tumours that looked at over 160,000 patients did
show a survival advantage for non-mucinous tumours [9].
Overall, for all locations of colorectal cancer, mucinous
tumours had a significantly worse 5-year survival (58.1 vs.
62.9 %), and this was also apparent for rectal cancers
specifically.
One study found a difference in 5-year survival in stages
II and III but not for stages I and IV. Further, when com-
paring patients of all stages who had undergone supposed
‘‘curative’’ resection, the 5-year survival was 70 % for non-
mucinous tumours and 62 % for mucinous tumours; this
was considered statistically significant [20].
However, there are reports that have showed no survival
differences between mucinous and non-mucinous adeno-
carcinomas of the rectum. A prospective, case–control
study comparing survival outcomes of Dukes C or stage III
tumours showed that there was no significant difference in
overall survival at 5 years. For both groups, this was
approximately 50–55 % [12]. Although the study included
colon and rectal cancers, the survival analysis was pre-
dominantly rectal tumours.
A Canadian study also found no difference in survival
between mucinous and non-mucinous tumours independent
of tumour location [27]. However, a sub-analysis per stage
of presentation found that stage III mucinous tumours did
have a worse overall survival compared with non-mucinous
tumours of the same stage.
Radiological diagnosis and measuring response
Magnetic resonance imaging (MRI) has the ability to dif-
ferentiate mucinous tumours from non-mucinous tumours.
This is advantageous in being able to diagnose mucinous
carcinoma early in the treatment pathway rather than
relying on histological diagnosis following surgery. The
signal characteristics depend on imaging protocol—T1-
weighted images show low signal intensity, whereas on T2-
weighted images, there is a significant hyper-intense signal.
In contrast, non-mucinous tumours demonstrate interme-
diate signal intensity on T2 imaging. The difference in
signal characteristics is due to the abundant mucin com-
position [28, 29].
The signal and enhancement characteristics on MRI may
make it difficult to distinguish mucinous tumours from other
fluid-containing pathologies such as cysts, fluid collections
and even necrotic tumours [30]. Although it is unusual to
confuse these benign conditions with cancer during pre-
liminary imaging of the pelvis, the difficulty arises during
follow-up imaging after treatment. Figure 3 shows the signal
characteristics of mucinous tumour on MRI.
Allen et al. [31] studied the MRI features of rectal can-
cers and the changes following chemoradiotherapy. They
338 Tech Coloproctol (2014) 18:335–344
123

defined mucinous tumours on T2-weighted images as high
signal intensity, similar to that of obturator internus muscle.
The same areas showed a uniform hyper-intensity after
chemoradiation on T2-weighted images. However, there
were no other morphological changes or shrinkage seen
radiologically with persistent areas of high signal intensity.
Oberholzer correlated the radiological changes on MRI
following CRT with pathology in order to describe the
accuracy of MRI in predicting response in mucinous
tumours [32]. They found that more advanced mucinous
tumours (CRM to tumour distance of \5 mm) showed a
worse response to CRT in terms of down-staging than non-
mucinous tumours leading to increased rates of R1
resections. In addition, there was also disease progression
in mucinous tumours only (Fig. 4).
A sub-classification of mucinous tumours
Mucinous tumours may fall into one of three categories.
There are those tumours, which are diagnosed as mucinous
prior to any treatment and remain mucinous throughout
their course. For example, they are identified as mucinous
on biopsy and/or MRI as well as on the surgical resection
specimen. These tumours appear to have the worst prog-
nosis and increased risk of local recurrence [33, 34]. The
documentation of the extent of residual cellular mucin is
Fig. 3 a, b MRI showing a rectal cancer with focal areas of mucin. There is a difference in signal characteristics between the tumour itself and
the areas of mucin which have a higher signal. The heterogeneous nature of the signal is indicative of cellular mucin
Fig. 4 a, b MRI showing areas of mucin which have responded to chemoradiation. The homogeneous signal characteristics as depicted by the
arrow suggest an acellular component to the mucin which is thought to represent tumour response
Tech Coloproctol (2014) 18:335–344 339
123

important since the risk of tumour spillage from such
mucin pools will increase the risk of local recurrence.
A second group of tumours exist, which become
mucinous during treatment. These tumours may have
started out as non-mucinous and subsequently show mor-
phological change as a consequence of either natural dis-
ease progression or chemoradiotherapy. This group is of
particular interest as it may represent a specific type of
tumour, which behaves as non-mucinous adenocarcinoma
despite having the phenotype of mucinous carcinoma.
Nagtegaal et al. [35] studied a number of mucinous
tumours and found that those tumours that had become
mucinous following short-course radiotherapy (SCRT) had
a better prognosis than those tumours that were mucinous
prior to treatment.
Post-therapeutic change leading to mucinous differen-
tiation has previously been well documented; however, the
clinical significance of this is now better understood. For
example, on baseline imaging, such as MRI, this corre-
sponds to a tumour that is of entirely intermediate signal
intensity with no areas of high signal intensity mucin. After
neo-adjuvant chemoradiation or radiotherapy alone,
necrosis of the tumour can result in mucinous degeneration.
In such cases, degeneration of the tumour results in high
signal intensity pools within the previously documented
intermediate signal intensity tumour stroma, and can
therefore be interpreted as evidence of treatment response.
In a further study by Allen et al. [31] in which the MRI
features of rectal carcinoma were studied before and after
chemoradiation, an additional 4 tumours were added to the
original 7 tumours, which were identified as mucinous by
MRI. Tumours were classified as mucinous on signal
intensity of the supposed mucinous area having greater
signal intensity than the obturator internus muscle. Inter-
estingly, although chemoradiation may increase the degree
of mucinous differentiation, these tumours do show a
response to treatment. They show tumour regression and
down-staging, meaning that induced mucinous change does
not appear to be a poor prognostic factor. The European
Organisation for Research and Treatment of Cancer (EO-
RTC) trial investigated the effect of adding chemotherapy
to pre-operative radiotherapy and the role of adjuvant
chemotherapy in stages II and IV rectal cancer. As part of
the analysis, they found that in addition to there being an
increased proportion of mucinous tumours found following
neo-adjuvant treatment, this was further enhanced in the
group with chemo- and radiotherapy than just pre-operative
radiotherapy alone [36]. This phenomenon is not fully
understood; however, one explanation offered by the Col-
lege of American Pathologists is that mucinous change is a
feature of response to pre-operative treatment [33].
The final group of mucinous tumours are those that
demonstrate acellular mucin on histological analysis. The
relevance of acellular mucin remains controversial. A
recent analysis of 108 prospectively collected post-treat-
ment specimens showed acellular mucin pools in 16 cases.
The presence of acellular mucin pools had no impact on
recurrence-free survival [37]. Acellular mucin may be
regarded as a type of treatment response and not as residual
tumour although this is still contentious. Cellular mucin on
T2 imaging is hyper-intense but contains areas of more
intermediate signal corresponding to the histologically
demonstrated malignant cells, cords and vessels. After
treatment, the necrosis of these morphological features
results in the formation of acellular mucin—namely pools
of featureless high signal intensity fluid-like signal on the
T2-weighted images which when compared with pre-
treatment scans contain no or minimal intermediate signal
intensity. The clinical outcomes of these tumours that show
colloid or mucin pools with little or no tumour activity
have been studied by Rullier et al. [38]. They differ in
behaviour and morphology from pre-existing mucinous
tumours and commonly have a much greater component of
mucin in the tumour complex, sometimes as much as 80 %.
The pools of mucin are also less basophilic than pre-
existing mucin. The debate as to whether this variant of
mucin should be considered as complete response—
ypT0N0; or consider these mucin pools to contain residual
tumour continues. Rullier showed some similarities with
tumours that have shown down-staging and some similar-
ities with tumours that have shown no response at all. It
may be prudent not to consider mucin response as complete
response.
The effect of chemo/radiotherapy
Neo-adjuvant chemo/radiotherapy (CRT) is an integral part
of the management of rectal cancer. CRT may be given for a
combination of reasons based on the evidence of poor
prognostic factors. Several studies have shown that patients
with mucinous tumours respond more poorly to radiotherapy
than non-mucinous tumours. One such study of 136 patients
compared the outcome of 25 mucinous tumours with 111
non-mucinous tumours. Although the results showed
decreased down-staging in the mucinous group, this was not
seen to affect overall survival or disease-free survival [39].
Interestingly, there was a benefit for the mucinous tumours
that received neo-adjuvant CRT. None of the mucinous
tumour achieved complete response, but almost half were
down-staged by one stage. Sengul et al. [40] reported a sta-
tistically significant difference in tumour regression grade
(TRG) between the two subtypes and a much smaller
decrease in T and N staging. However, only 16 patients were
studied and the small numbers may account for the results.
The underlying biology of these tumours may explain their
different responses to oncological therapy.
340 Tech Coloproctol (2014) 18:335–344
123

Shin et al. [41] reported on the effectiveness of pre-
operative CRT on 23 patients with mucinous rectal cancer.
Seven patients showed minimal down-staging of one stage,
and one patient showed disease progression. There were no
cases of pathological complete response unlike the non-
mucinous group where this was the case in 16 % of
patients. Recurrence was not statistically significant, but
there was a difference in 5-year survival (64.8 vs. 79.8 %).
This was more apparent in more advanced stages of dis-
ease. They compared the response to CRT of 23 mucinous
tumours with 345 non-mucinous tumours. T-stage down-
staging was much worse in the mucinous group although
there was no difference in nodal down-staging. However,
the numbers of mucinous tumours in this study were again
small. A study by Qiu found that mucinous type along with
T4 stage on multivariate analysis negatively affected
tumour response [42]. These findings may be explained by
underlying gene expression which results in chemo-resis-
tivity. Enzymes that interfere with pyrimidine and plati-
num-based compounds are overexpressed in mucinous
tumours [43].
Mucin or colloid production by a tumour may represent
a measure of response to neo-adjuvant treatment. The
production of mucin without the presence of tumour cells is
a common phenomenon after radiotherapy in particular
[32, 37, 44–46]. Rullier et al. [38] found that 39 patients
out of 200 demonstrated a colloid response to pre-operative
radiotherapy, of which the vast majority (n = 34) showed
no regression in tumour grade. But this is a separate phe-
nomenon to radiation causing mucinous tumours. A sig-
nificant proportion of tumours that arise following pelvic
irradiation for other cancers are seen to be mucinous—
approximately 25 % [47].
Yet the role of adjuvant therapy in the treatment for
mucinous tumours may be changing. Previous studies have
suggested that mucinous tumours do not response well to
5-FU-based chemotherapy after surgery [48, 49]. Negri
et al. [49] studied the effect of 5-FU-based adjuvant
chemotherapy on survival in colorectal cancers. Median
overall survival was 11.8 vs. 17.9 months, which showed
statistical significance on multivariate analysis. The view
had been that mucinous tumours show little response to
adjuvant therapy, but this may have been due to inade-
quate oncological surgery. The acceptance of TME in
rectal cancer has changed outcomes for all stages of dis-
ease. More recent studies have accounted for this factor as
a reason for local, and in the case of nodal disease, distant
recurrence. A recent report by Catalano studying the
outcomes of mucinous colon cancer in stage II and stage
III disease has shown a survival benefit for patients with
mucinous tumours that are offered adjuvant chemotherapy.
This was shown on multivariate analysis with a hazard
ratio of 2.73 [50].
The biology of mucinous rectal cancer
Cancer of the colon and cancer of the rectum demonstrate
many biological and molecular differences. This raises the
possibility of different pathways governing tumorigenesis
in these malignancies. The differences in clinicopatholog-
ical such as location of tumour may be a reflection of the
underlying molecular profiles or different embryological
origin of the different parts of the gut.
Mucin is produced as a protein by a group of specific
mucin-producing genes, which are prefixed by the name—
‘‘MUC’’. There are several genes within this family, and
they are able to produce two distinct types of mucin—a
transmembranous type and a secretory type. These genes
are not part of a gene family in the truest sense of the term as
their gene products vary dramatically in their structure and
function. However, it is the characterisation of specific parts
of the gene products, which have led to them sharing the
name ‘‘MUC’’. The two types of mucins are classified
according to whether they are secreted mucins or trans-
membranous mucins. MUC1 produces a transmembranous
mucin, which is associated with a poor prognosis. MUC1
expression is low in mucinous tumours but in those tumours
that show overexpression, there is an association with worse
prognosis and chemoresistivity to certain chemotherapy
agents [51]. Conversely, the MUC5 gene has been shown to
confer a survival benefit [52] and unusually is overexpres-
sed in some mucinous tumours. However, MUC5 also
shows a greater association with proximal location of the
colorectum, which may explain the poor prognosis of
mucinous rectal cancer; that this may be due to relative
underexpression of MUC5. MUC2 on the other hand is
almost exclusively associated with mucinous tumours. It
may play a role in p53 mutation. There are also reports of
MUC2 and liver metastases [53]. Kim et al. [54] studied the
prevalence and expression of specific mucin core proteins in
a variety of colorectal polyps in addition to mucinous and
non-mucinous tumours. MUC2 and MUC5 were most fre-
quently found in mucinous tumours and villous adenomas.
In addition to the pattern of mucin gene expression,
mucinous tumours also express other distinct genetic features.
For example, there is a lower frequency of p53 mutations and
conversely a higher frequency of K-Ras mutations [55]. p53
mutations are interesting as they are associated with rectal
cancers but not common in mucinous subtype [56, 57]. There
may be heterogeneity in p53 mutations that accounts for dif-
ferent phenotypic effects on individual tumours.
Discussion
The results of this study have highlighted specific charac-
teristics of mucinous rectal cancer, which distinguishes it
Tech Coloproctol (2014) 18:335–344 341
123

from non-mucinous disease. These tumours are more
commonly found in the proximal colon; however, when
present in the rectum, they appear to behave more
aggressively. The location of tumours may reflect the
underlying molecular profile although this has not been
definitively proven. It is also unclear as to whether fair
comparisons can be made between the clinical outcomes of
colon and rectal cancer; the survival outcomes, response to
chemotherapy and ability of the tumour to metastasise are
not immediately comparable between non-mucinous
tumours. The more aggressive behaviour of mucinous
rectal, rather than colonic tumours, may simply be due to
anatomical location and that the mechanism of spread
described above has a more immediate effect in the narrow
confines of the pelvis.
The results of the demographic profile of mucinous
tumours consistently showed that they are more common in
younger patients. Different studies used varying cut-offs;
however, the trend was that these tumours manifest earlier in
younger patients. Whilst the explanation to this observation
will most likely lie in the genetic make-up of these tumours,
this may simply reflect their aggressive nature. Whilst non-
mucinous tumours may take longer to progress through
carcinogenesis, mucinous tumours may accelerate through
this pathway and thus present earlier. Another explanation
may be related to the stage at presentation. Early tumours that
are confined to the bowel wall may not present with symp-
toms compared to more locally advanced tumours. Mucin-
ous tumours are more commonly seen at an advanced stage,
which may be due to aggressive spread through the bowel
wall causing symptoms requiring investigation.
The actual response of these cancers to oncological
treatment is becoming clearer. The challenge over the years
in both mucinous and non-mucinous tumours with regard
to survival outcomes following varying types of oncolog-
ical treatment has been interpreting the results in the light
of pathological scrutiny of the surgical technique. Several
of the historical studies did not include operative details or
grade the quality of the specimens. The importance of this
has been highlighted by Quirke [58]. Therefore, attempting
to apply the results of these studies, which do not describe
surgical technique and histopathological audit, may not be
relevant to today’s practice. However, more recent studies,
which include TME surgery and note the importance of a
positive CRM, have challenged the traditional view of
chemoresistance. And whilst the survival benefit of adju-
vant chemotherapy has not been specifically documented in
any high-quality randomised trial for this type of rectal
cancer, it is becoming clear that adjuvant chemotherapy
may indeed have a role to play in mucinous cancer.
Equally, whether pre-operative radiotherapy leads to down-
staging is another issue, which must be resolved with
greater accuracy. If these issues do become clearer, it will
allow clinicians to decide whether and when radio- or
chemotherapy should be given and what the survival ben-
efit will be.
The acceptance of TME as the optimal surgical tech-
nique for rectal cancer has helped standardise practise. A
discussion on the modifications of this technique is beyond
the scope of this review; however, the association of an
increased nodal burden in mucinous disease should not
impact on technique. If the principles of TME are followed
and the mesorectal nodes are removed en-bloc with the
specimen, there should be prognostic relevance to local
recurrence although this may be a stronger indication for
adjuvant chemotherapy.
Conclusion
Mucinous tumours of the rectum remain difficult to treat
and are still associated with worse survival outcomes than
non-mucinous tumours. However, with a universally
accepted definition, better pre-operative detection using
MRI and high-quality oncological surgery, we may see
improvement in outcomes in the future. This will aid fur-
ther study of these subtypes and allow clinicians to risk
stratify patients in terms of oncological treatment.
Acknowledgments Authors received fund from NIHR BRC Pro-
gramme Grant Royal Marsden Hospital.
Conflict of interest None.
References
1. Hanski C, Hofmeier M, Schmitt-Graff A et al (1997) Overex-
pression or ectopic expression of MUC2 is the common property
of mucinous carcinomas of the colon, pancreas, breast, and ovary.
J Pathol 182:385–391
2. Jass JR, Sobin LH, Watanabe H (1990) The world health orga-
nization’s histologic classification of gastrointestinal tumors. A
commentary on the second edition. Cancer 66:2162–2167
3. Pihl E, Nairn RC, Hughes ES, Cuthbertson AM, Rollo AJ (1980)
Mucinous colorectal carcinoma: immunopathology and progno-
sis. Pathology 12:439–447
4. Umpleby HC, Ranson DL, Williamson RC (1985) Peculiarities of
mucinous colorectal carcinoma. Br J Surg 72:715–718
5. Symonds DA, Vickery AL (1976) Mucinous carcinoma of the
colon and rectum. Cancer 37:1891–1900
6. Green JB, Timmcke AE, Mitchell WT, Hicks TC, Gathright JB
Jr, Ray JE (1993) Mucinous carcinoma-just another colon can-
cer? Dis Colon Rectum 36:49–54
7. Nozoe T, Anai H, Nasu S, Sugimachi K (2000) Clinicopatho-
logical characteristics of mucinous carcinoma of the colon and
rectum. J Surg Oncol 75:103–107
8. Du W, Mah JT, Lee J, Sankila R, Sankaranarayanan R, Chia KS
(2004) Incidence and survival of mucinous adenocarcinoma of
the colorectum: a population-based study from an Asian country.
Dis Colon Rectum 47:78–85
342 Tech Coloproctol (2014) 18:335–344
123
9. Kang H, O’Connell JB, Maggard MA, Sack J, Ko CY (2005) A
10-year outcomes evaluation of mucinous and signet-ring cell
carcinoma of the colon and rectum. Dis Colon Rectum
48:1161–1168
10. Verhulst J, Ferdinande L, Demetter P, Ceelen W (2012) Mucin-
ous subtype as prognostic factor in colorectal cancer: a systematic
review and meta-analysis. J Clin Pathol 65:381–388
11. Hyngstrom JR, Hu CY, Xing Y et al (2012) Clinicopathology and
outcomes for mucinous and signet ring colorectal adenocarci-
noma: analysis from the national cancer data base. Ann Surg
Oncol 19:2814–2821
12. Consorti F, Lorenzotti A, Midiri G, Di Paola M (2000) Prognostic
significance of mucinous carcinoma of colon and rectum: a
prospective case-control study. J Surg Oncol 73:70–74
13. Heys SD, Sherif A, Bagley JS, Brittenden J, Smart C, Eremin O
(1994) Prognostic factors and survival of patients aged less than
45 years with colorectal cancer. Br J Surg 81:685–688
14. Adloff M, Arnaud JP, Schloegel M, Thibaud D, Bergamaschi R
(1986) Colorectal cancer in patients under 40 years of age. Dis
Colon Rectum 29:322–325
15. Umpleby HC, Williamson RC (1984) Carcinoma of the large
bowel in the first four decades. Br J Surg 71:272–277
16. Dozois EJ, Boardman LA, Suwanthanma W et al (2008) Young-
onset colorectal cancer in patients with no known genetic pre-
disposition: can we increase early recognition and improve out-
come? Medicine (Baltimore) 87:259–263
17. You YN, Dozois EJ, Boardman LA, Aakre J, Huebner M, Larson
DW (2011) Young-onset rectal cancer: presentation, pattern of
care and long-term oncologic outcomes compared to a matched
older-onset cohort. Ann Surg Oncol 18:2469–7246
18. Chou CL, Chang SC, Lin TC et al (2011) Differences in clini-
copathological characteristics of colorectal cancer between
younger and elderly patients: an analysis of 322 patients from a
single institution. Am J Surg 202:574–582
19. Wu CS, Tung SY, Chen PC, Kuo YC (1996) Clinicopathological
study of colorectal mucinous carcinoma in Taiwan: a multivariate
analysis. J Gastroenterol Hepatol 11:77–81
20. Song W, Wu SJ, He YL et al (2009) Clinicopathologic features
and survival of patients with colorectal mucinous, signet-ring cell
or non-mucinous adenocarcinoma: experience at an institution in
southern China. Chin Med J (Engl) 122:1486–1491
21. Younes M, Katikaneni PR, Lechago J (1993) The value of the
preoperative mucosal biopsy in the diagnosis of colorectal
mucinous adenocarcinoma. Cancer 72:3588–3592
22. Parham D (1923) Colloid carcinoma. Ann Surg 77:90–105
23. Sugarbaker PH (2001) Mucinous colorectal carcinoma. J Surg
Oncol 77:282–283
24. Sasaki O, Atkin WS, Jass JR (1987) Mucinous carcinoma of the
rectum. Histopathology 11:259–272
25. Okuno M, Ikehara T, Nagayama M, Kato Y, Yui S, Umeyama K
(1988) Mucinous colorectal carcinoma: clinical pathology and
prognosis. Am Surg 54:681–685
26. Kanemitsu Y, Kato T, Hirai T et al (2003) Survival after curative
resection for mucinous adenocarcinoma of the colorectum. Dis
Colon Rectum 46:160–167
27. Xie L, Villeneuve PJ, Shaw A (2009) Survival of patients diag-
nosed with either colorectal mucinous or non-mucinous adeno-
carcinoma: a population-based study in Canada. Int J Oncol
34:1109–1115
28. Hussain SM, Outwater EK, Siegelman ES (1999) Mucinous
versus nonmucinous rectal carcinomas: differentiation with MR
imaging. Radiology 213:79–85
29. Kim MJ, Huh YM, Park YN et al (1999) Colorectal mucinous
carcinoma: findings on MRI. J Comput Assist Tomogr
23:291–296
30. Hussain SM, Outwater EK, Siegelman ES (2000) MR imaging
features of pelvic mucinous carcinomas. Eur Radiol 10:885–891
31. Allen SD, Padhani AR, Dzik-Jurasz AS, Glynne-Jones R (2007)
Rectal carcinoma: MRI with histologic correlation before and
after chemoradiation therapy. AJR Am J Roentgenol 188:
442–451
32. Oberholzer K, Menig M, Kreft A et al (2012) Rectal cancer:
mucinous carcinoma on magnetic resonance imaging indicates
poor response to neoadjuvant chemoradiation. Int J Radiat Oncol
Biol Phys 82:842–848
33. Bouzourene H, Bosman FT, Matter M, Coucke P (2003) Pre-
dictive factors in locally advanced rectal cancer treated with
preoperative hyperfractionated and accelerated radiotherapy.
Hum Pathol 34:541–548
34. Compton CC, Fielding LP, Burgart LJ et al (2000) Prognostic
factors in colorectal cancer. College of American pathologists
consensus statement 1999. Arch Pathol Lab Med 124:979–994
35. Nagtegaal I, Gaspar C, Marijnen C, Van De Velde C, Fodde R,
Van Krieken H (2004) Morphological changes in tumour type
after radiotherapy are accompanied by changes in gene expres-
sion profile but not in clinical behaviour. J Pathol 204:183–192
36. Bosset JF, Calais G, Mineur L et al (2005) Enhanced tumorocidal
effect of chemotherapy with preoperative radiotherapy for rectal
cancer: preliminary results-EORTC 22921. J Clin Oncol
23:5620–5627
37. Shia J, McManus M, Guillem JG et al (2011) Significance of
acellular mucin pools in rectal carcinoma after neoadjuvant
chemoradiotherapy. Am J Surg Pathol 35:127–134
38. Rullier A, Laurent C, Vendrely V, Le Bail B, Bioulac-Sage P,
Rullier E (2005) Impact of colloid response on survival after
preoperative radiotherapy in locally advanced rectal carcinoma.
Am J Surg Pathol 29:602–606
39. Grillo-Ruggieri F, Mantello G, Berardi R et al (2007) Mucinous
rectal adenocarcinoma can be associated to tumor downstaging
after preoperative chemoradiotherapy. Dis Colon Rectum
50:1594–1603
40. Sengul N, Wexner SD, Woodhouse S et al (2006) Effects of
radiotherapy on different histopathological types of rectal carci-
noma. Colorectal Dis 8:283–288
41. Shin US, Yu CS, Kim JH et al (2011) Mucinous rectal cancer:
effectiveness of preoperative chemoradiotherapy and prognosis.
Ann Surg Oncol 18:2232–2239
42. Qiu HZ, Wu B, Xiao Y, Lin GL (2011) Combination of differ-
entiation and T stage can predict unresponsiveness to neoadjuvant
therapy for rectal cancer. Colorectal Dis 13:1353–1360
43. Glasgow SC, Yu J, Carvalho LP, Shannon WD, Fleshman JW,
McLeod HL (2005) Unfavourable expression of pharmacologic
markers in mucinous colorectal cancer. Br J Cancer 92:259–264
44. Bozzetti F, Baratti D, Andreola S et al (1999) Preoperative
radiation therapy for patients with T2-T3 carcinoma of the mid-
dle-to-lower rectum. Cancer 86:398–404
45. Dworak O, Keilholz L, Hoffmann A (1997) Pathological features
of rectal cancer after preoperative radiochemotherapy. Int J
Colorectal Dis 12:19–23
46. Wheeler JM, Warren BF, Jones AC, Mortensen NJ (1999) Pre-
operative radiotherapy for rectal cancer: implications for sur-
geons, pathologists and radiologists. Br J Surg 86:1108–1120
47. Jao SW, Beart RW Jr, Reiman HM, Gunderson LL, Ilstrup DM
(1987) Colon and anorectal cancer after pelvic irradiation. Dis
Colon Rectum 30:953–958
48. Catalano V, Loupakis F, Graziano F et al (2009) Mucinous his-
tology predicts for poor response rate and overall survival of
patients with colorectal cancer and treated with first-line oxa-
liplatin- and/or irinotecan-based chemotherapy. Br J Cancer
100:881–887
Tech Coloproctol (2014) 18:335–344 343
123

49. Negri FV, Wotherspoon A, Cunningham D, Norman AR, Chong
G, Ross PJ (2005) Mucinous histology predicts for reduced flu-
orouracil responsiveness and survival in advanced colorectal
cancer. Ann Oncol 16:1305–1310
50. Catalano V, Loupakis F, Graziano F et al (2012) Prognosis of
mucinous histology for patients with radically resected stage II
and III colon cancer. Ann Oncol 23:135–141
51. Byrd JC, Bresalier RS (2004) Mucins and mucin binding proteins
in colorectal cancer. Cancer Metastasis Rev 23:77–99
52. Kocer B, Soran A, Erdogan S et al (2002) Expression of
MUC5AC in colorectal carcinoma and relationship with prog-
nosis. Pathol Int 52:470–477
53. Bresalier RS, Niv Y, Byrd JC et al (1991) Mucin production by
human colonic carcinoma cells correlates with their metastatic
potential in animal models of colon cancer metastasis. J Clin
Invest 87:1037–1045
54. Kim DH, Kim JW, Cho JH et al (2005) Expression of mucin core
proteins, trefoil factors, APC and p21 in subsets of colorectal
polyps and cancers suggests a distinct pathway of pathogenesis of
mucinous carcinoma of the colorectum. Int J Oncol 27:957–964
55. Hanski C (1995) Is mucinous carcinoma of the colorectum a
distinct genetic entity? Br J Cancer 72:1350–1356
56. Iacopetta B (2003) TP53 mutation in colorectal cancer. Hum
Mutat 21:271–276
57. Russo G, Anzivino E, Fioriti D et al (2008) p53 gene mutational
rate, Gleason score, and BK virus infection in prostate adeno-
carcinoma: is there a correlation? J Med Virol 80:2100–2107
58. Quirke P, Steele R, Monson J et al (2009) Effect of the plane of
surgery achieved on local recurrence in patients with operable
rectal cancer: a prospective study using data from the MRC CR07
and NCIC-CTG CO16 randomised clinical trial. Lancet
373:821–828
344 Tech Coloproctol (2014) 18:335–344
123