Embed Size (px)
Citation preview
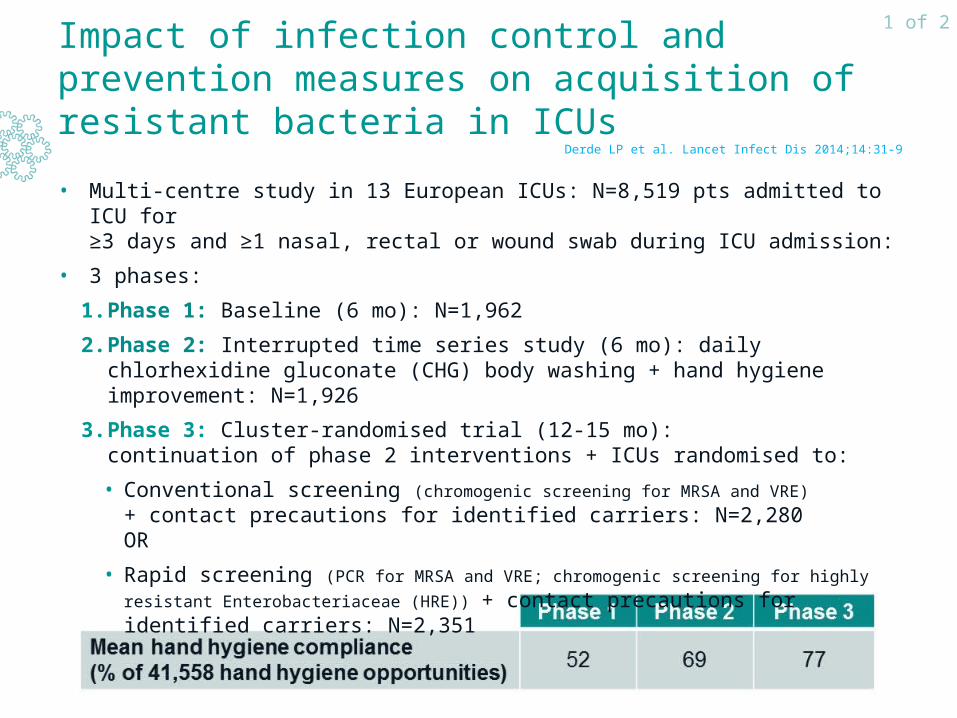
• Multi-centre study in 13 European ICUs: N=8,519 pts admitted to ICU for ≥3 days and ≥1 nasal, rectal or wound swab during ICU admission:
• 3 phases:
1. Phase 1: Baseline (6 mo): N=1,962
2. Phase 2: Interrupted time series study (6 mo): daily chlorhexidine gluconate (CHG) body washing + hand hygiene improvement: N=1,926
3. Phase 3: Cluster-randomised trial (12-15 mo): continuation of phase 2 interventions + ICUs randomised to:
• Conventional screening (chromogenic screening for MRSA and VRE) + contact precautions for identified carriers: N=2,280 OR
• Rapid screening (PCR for MRSA and VRE; chromogenic screening for highly resistant
Enterobacteriaceae (HRE)) + contact precautions for identified carriers: N=2,351
Impact of infection control and prevention measures on acquisition of resistant bacteria in ICUs
Derde LP et al. Lancet Infect Dis 2014;14:31-9
1 of 2
Impact of infection control and prevention measures on acquisition of resistant bacteria in ICUs
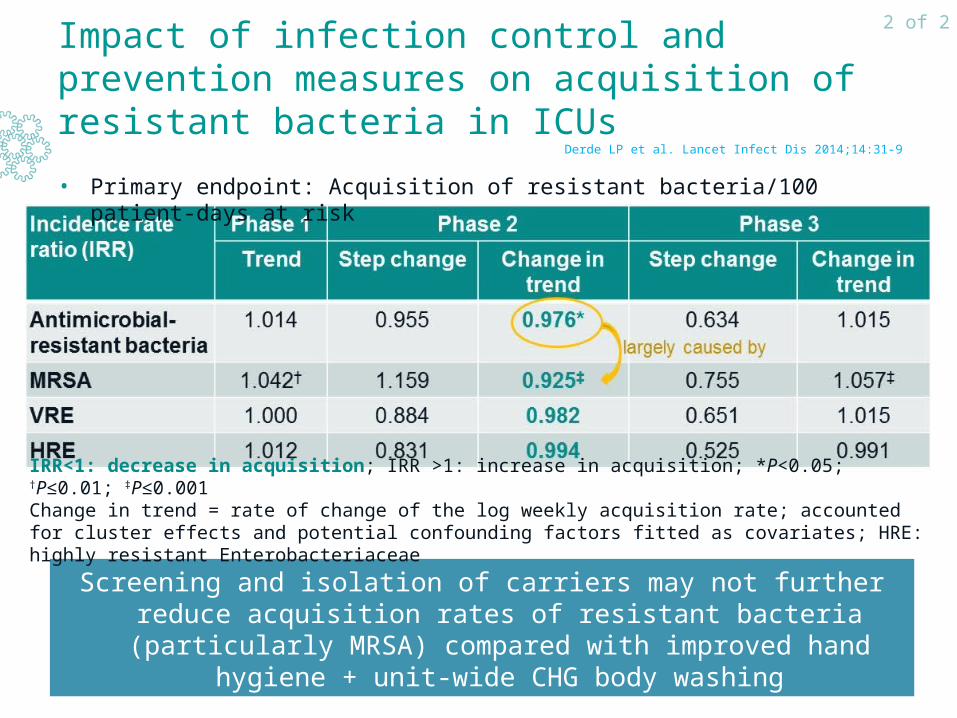
• Primary endpoint: Acquisition of resistant bacteria/100 patient-days at risk
• IRRconventional screening < IRRrapid screening, but no significant ≠ (P=0.06)
Screening and isolation of carriers may not further reduce acquisition rates of resistant bacteria (particularly MRSA) compared with
improved hand hygiene + unit-wide CHG body washing
Derde LP et al. Lancet Infect Dis 2014;14:31-9
2 of 2
IRR<1: decrease in acquisition; IRR >1: increase in acquisition; *P<0.05; †P≤0.01; ‡P≤0.001Change in trend = rate of change of the log weekly acquisition rate; accounted for cluster effects and potential confounding factors fitted as covariates; HRE: highly resistant Enterobacteriaceae
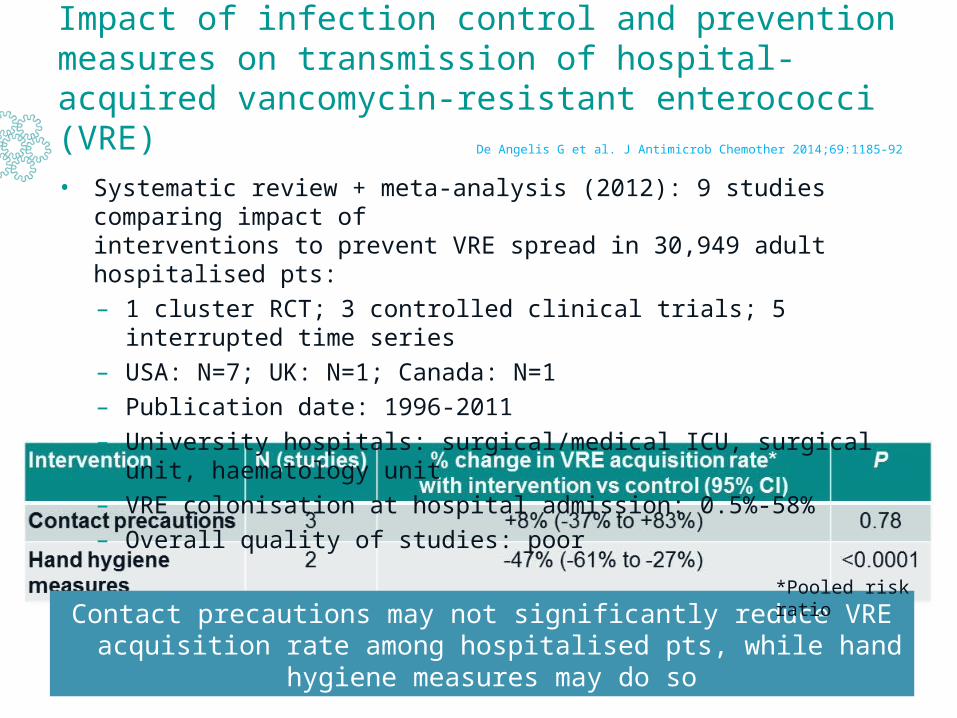
• Systematic review + meta-analysis (2012): 9 studies comparing impact of interventions to prevent VRE spread in 30,949 adult hospitalised pts:
– 1 cluster RCT; 3 controlled clinical trials; 5 interrupted time series
– USA: N=7; UK: N=1; Canada: N=1
– Publication date: 1996-2011
– University hospitals: surgical/medical ICU, surgical unit, haematology unit
– VRE colonisation at hospital admission: 0.5%-58%
– Overall quality of studies: poor
Impact of infection control and prevention measures on transmission of hospital-acquired vancomycin-resistant enterococci (VRE)
Contact precautions may not significantly reduce VRE acquisition rate among hospitalised pts, while hand hygiene measures may do so
De Angelis G et al. J Antimicrob Chemother 2014;69:1185-92
*Pooled risk ratio
Combination Tx vs monotherapy for carbapenemase-producing Enterobacteriaceae
• Systematic review (2013): 20 non-randomised studies: N=692 pts receiving definitive Tx for infections caused by:
– Carbapenemase-producing Enterobacteriaceae: 15 studies OR
– Carbapenem-resistant Enterobacteriaceae (CRE): 5 studies
• Predominant causative pathogen: 19 studies: Klebsiella spp. − 1 study: Enterobacter cloacae
• Predominant type of infections (>50% of included infections): Bacteraemia: 8 studies − Pneumonia/urinary tract infections: 12 studies
• Critically ill pts: 10/20 studies (50%)
• Primary outcome: 30-day mortality / Secondary outcome: Tx failure
• Synthesis of available evidence using statistical analyses, including meta-analysis: not possible due to methodological issues, including clinical heterogeneity → only descriptive analysis
• 3 studies: 194 critically ill pts with bloodstream infections (BSIs) due to carbapenemase-producing Klebsiella spp.: significantly lower mortality with combination Tx than with monotherapy
Falagas ME et al. Antimicrob Agents Chemother 2014;58:654-63
1 of 2
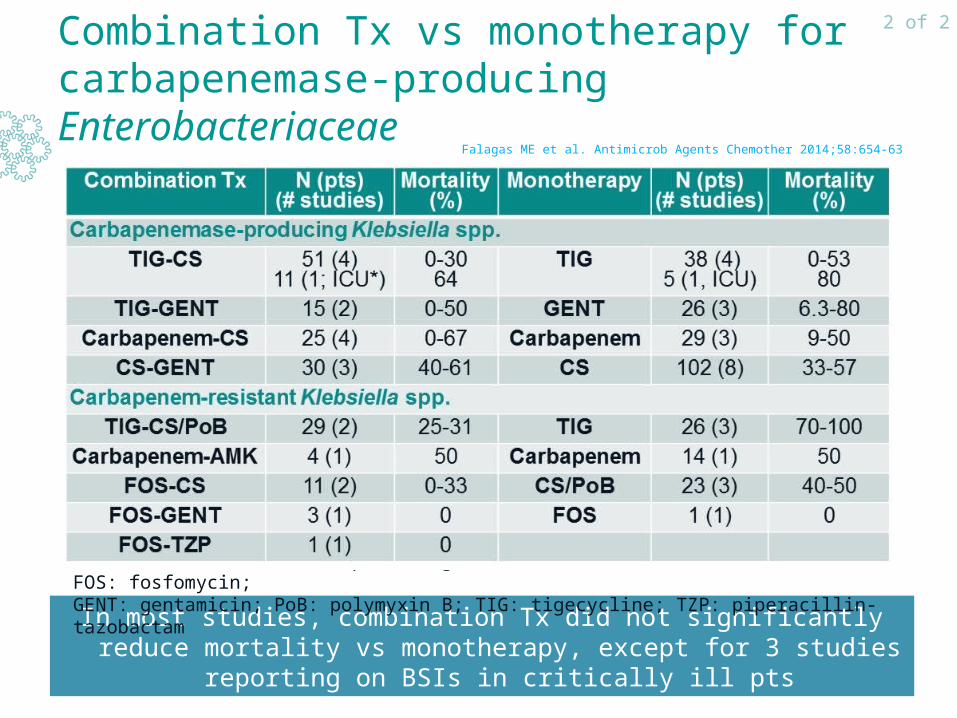
Combination Tx vs monotherapy for carbapenemase-producing Enterobacteriaceae
In most studies, combination Tx did not significantly reduce mortality vs monotherapy, except for 3 studies reporting on BSIs in critically ill pts
Falagas ME et al. Antimicrob Agents Chemother 2014;58:654-63
2 of 2
*Infections due to VIM-1-producing isolates; AMK: amikacin; CS: colistin; FOS: fosfomycin; GENT: gentamicin; PoB: polymyxin B; TIG: tigecycline; TZP: piperacillin-tazobactam
Impact of antibiotic stewardship (ASP) and infectious disease (ID) consultation on antibiotic use in the emergency department (ED)
• Single-centre study (USA; Jan-June 2014): collaborative ED, ASP and ID management pilot programme:
– ID specialist formally evaluated pts presenting in ED with infectious conditions and offered recommendations regarding antibiotic selection, dosing, duration and additional testing
– Pts were offered appropriate in- or outpatient FU
• N=331 pts evaluated by ID consultant over 6 mo: ±3 pts/day
• Additional time spent by ID consultant on evaluating pts in ED, coordinating care and communicating with other providers: 4 h/day
• Number of additional FU visits/pt after initial consultation: ≥1
• Most common reasons for ID consultation in ED:Pneumonia (30.5%), sepsis (16.9%), skin and soft tissue infections (11.2%), urinary tract infections and pyelonephritis (11.2%), CNS infections (5.4%), osteomyelitis or joint infections (5.4%), intraabdominal infections (5.1%), other (14.3%)
Madaline T. IDWeek 2014 abs. 228
1 of 2
Data from poster
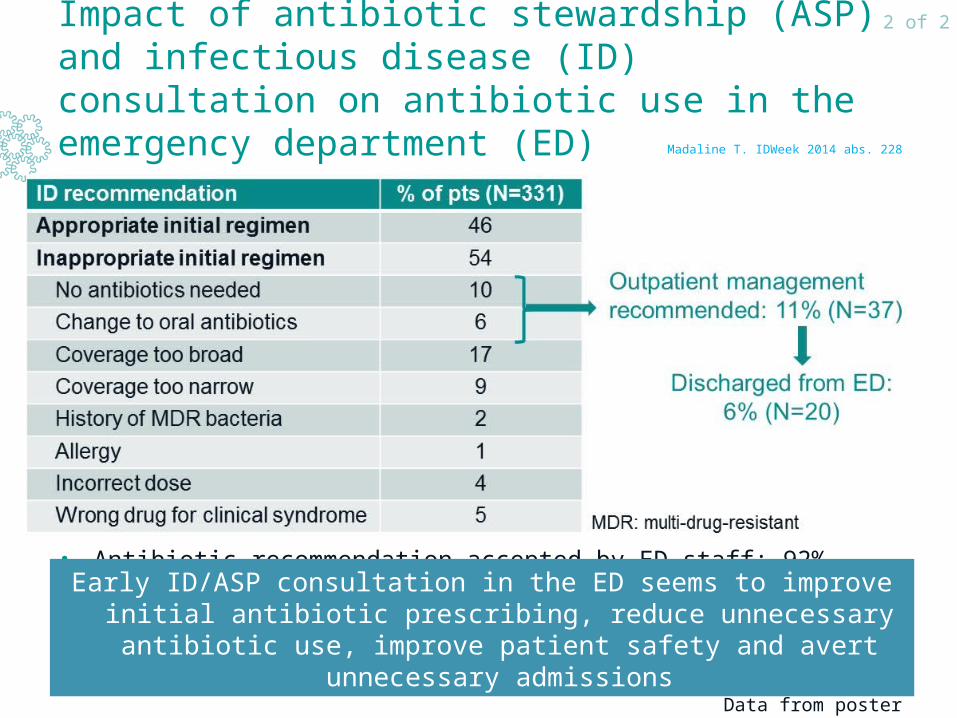
Impact of antibiotic stewardship (ASP) and infectious disease (ID) consultation on antibiotic use in the emergency department (ED)
• Antibiotic recommendation accepted by ED staff: 92%
Early ID/ASP consultation in the ED seems to improve initial antibiotic prescribing, reduce unnecessary antibiotic use, improve patient
safety and avert unnecessary admissions
Madaline T. IDWeek 2014 abs. 228
2 of 2
Data from poster
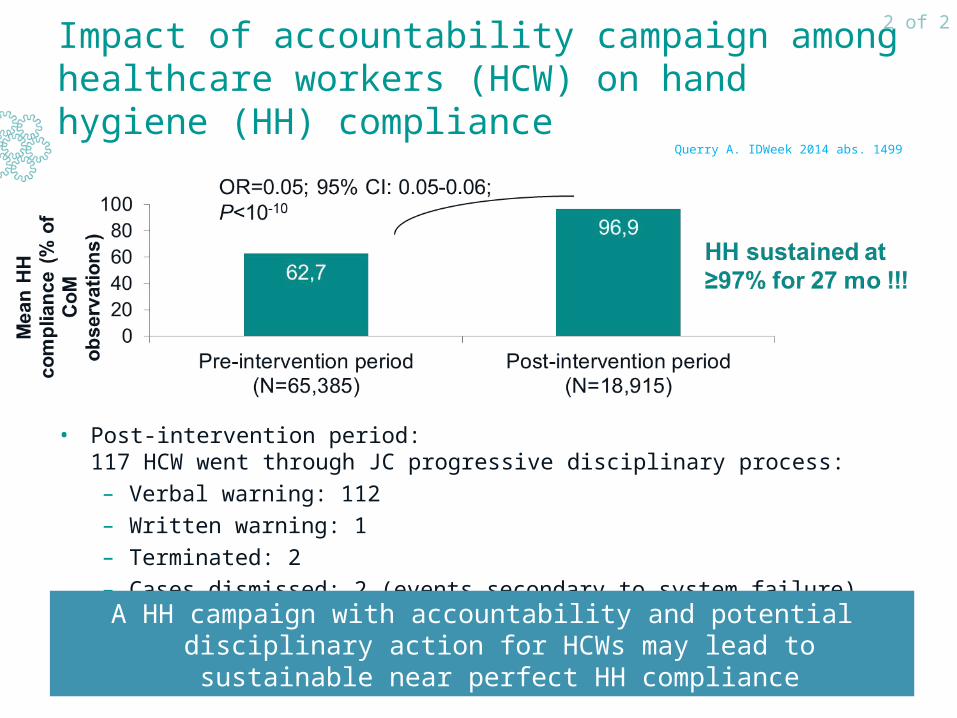
Impact of accountability campaign among healthcare workers (HCW) on hand hygiene (HH) compliance
Single-centre before-after study (35 units, including 8 ICUs; USA): ±800 stan-dardised HH observations collected monthly by 4 trained covert monitors (CoM)
•Pre-intervention period: 03/2008-05/2012
•Post-intervention period: 06/2012-08/2014: ‘Just Culture’ (JC) campaign:HCWs held accountable for conscious disregard for safety, but not for system failures:
– Progressive discipline: if non-compliance with HH (CoM observation): verbal warning → written warning → final written warning → termination
– Education/communication:
• Annual education of >2,000 employees; biannual CoM training
• Online promotional material, electronic communication, screensavers
• Non-compliance observations by anyone other than CoM: considered as teaching moments
– Environment: ongoing inspection of availability of alcohol hand sanitiser and chlorhexidine gluconate soap
– System change to reliably support HH practices: leadership, case reviews
Querry A. IDWeek 2014 abs. 1499
1 of 2
Data from poster
Impact of accountability campaign among healthcare workers (HCW) on hand hygiene (HH) compliance
• Post-intervention period: 117 HCW went through JC progressive disciplinary process:
– Verbal warning: 112
– Written warning: 1
– Terminated: 2
– Cases dismissed: 2 (events secondary to system failure)
A HH campaign with accountability and potential disciplinary action for HCWs may lead to sustainable near perfect HH compliance
Querry A. IDWeek 2014 abs. 1499
2 of 2
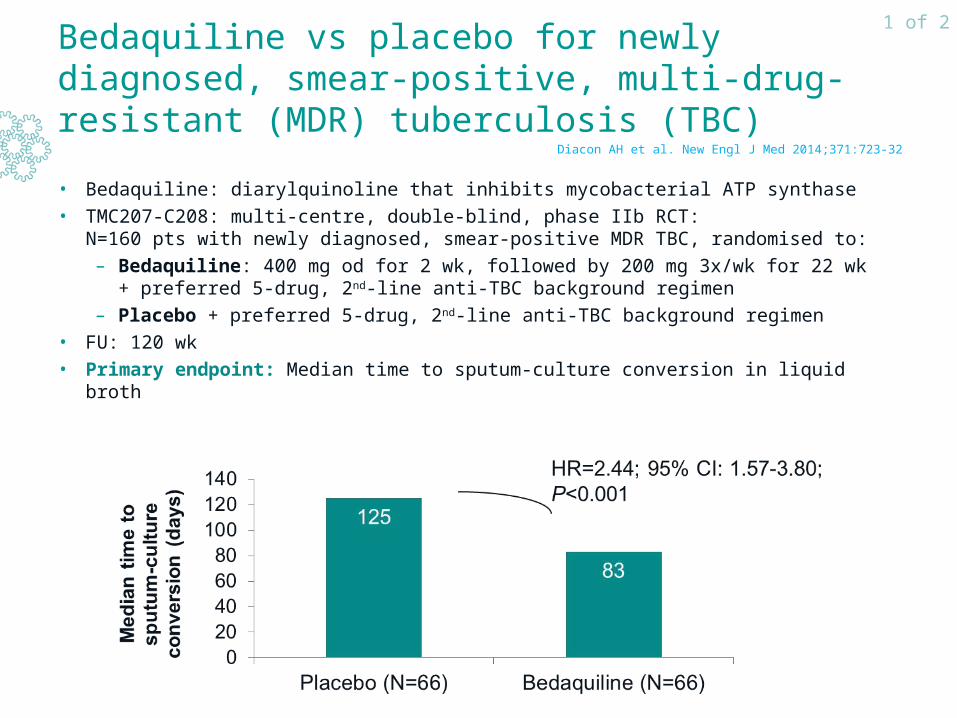
Bedaquiline vs placebo for newly diagnosed, smear-positive, multi-drug-resistant (MDR) tuberculosis (TBC)
• Bedaquiline: diarylquinoline that inhibits mycobacterial ATP synthase
• TMC207-C208: multi-centre, double-blind, phase IIb RCT: N=160 pts with newly diagnosed, smear-positive MDR TBC, randomised to:
– Bedaquiline: 400 mg od for 2 wk, followed by 200 mg 3x/wk for 22 wk+ preferred 5-drug, 2nd-line anti-TBC background regimen
– Placebo + preferred 5-drug, 2nd-line anti-TBC background regimen
• FU: 120 wk
• Primary endpoint: Median time to sputum-culture conversion in liquid broth
Diacon AH et al. New Engl J Med 2014;371:723-32
1 of 2
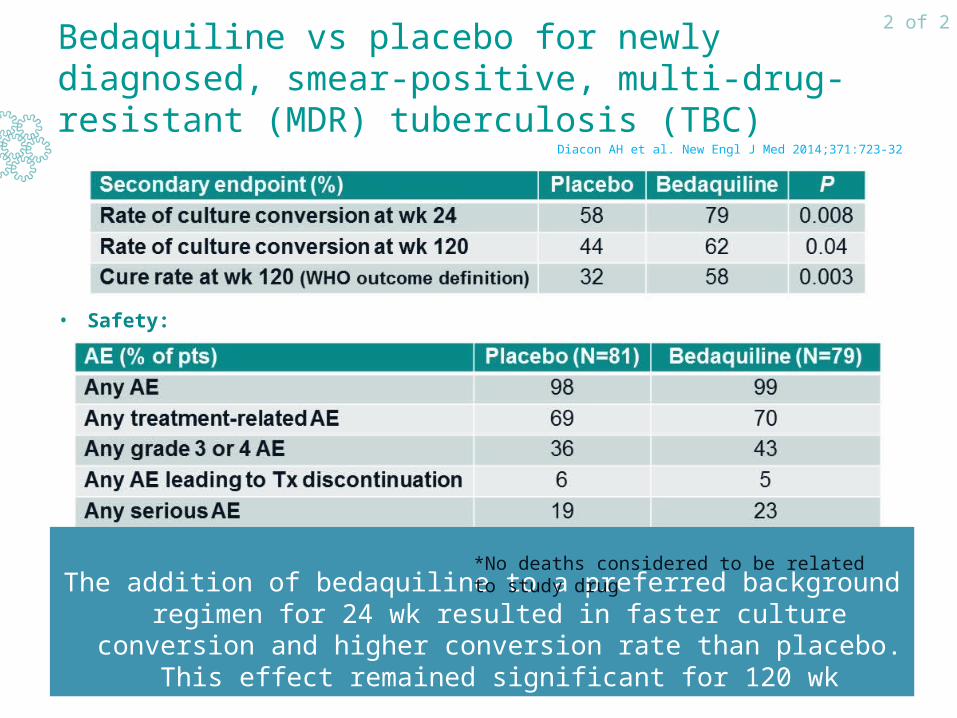
Bedaquiline vs placebo for newly diagnosed, smear-positive, multi-drug-resistant (MDR) tuberculosis (TBC)
• Safety:
The addition of bedaquiline to a preferred background regimen for 24 wk resulted in faster culture conversion and higher conversion rate
than placebo. This effect remained significant for 120 wk
Diacon AH et al. New Engl J Med 2014;371:723-32
2 of 2
*No deaths considered to be related to study drug





























