Embed Size (px)
Citation preview

REVIEW ARTICLES
The State of the Evidence for Whole-System,Multi-Modality Naturopathic Medicine:A Systematic Scoping Review
Stephen P. Myers, PhD, BMed, ND,1–3 and Vanessa Vigar, BNat (Hons)1,2,4
Abstract
Objective: To summarize the current state of the research evidence for whole-system, multi-modality na-turopathic medicine.
Design: A systematic search for research articles from around the world was undertaken using MEDLINE,Embase, CINAHL, AMED, and WHO regional indexes. Naturopathic journals and gray literature were handsearched. No language restrictions were imposed.
Interventions: All human research evaluating the effectiveness of naturopathic medicine, where two or morenaturopathic modalities are delivered by naturopathic clinicians, were included in the review. Case studies offive or more cases were included.
Results: Thirty-three published studies (n = 9859) met inclusion criteria (11 American; 4 Canadian; 6 Ger-man; 7 Indian; 3 Australian; 1 United Kingdom; and 1 Japanese) across a range of mainly chronic clinicalconditions. The studies predominantly showed evidence for the efficacy of naturopathic medicine for the con-ditions and settings in which they were based.
Conclusions: To date, research in whole-system, multi-modality naturopathic medicine shows that it iseffective for treating cardiovascular disease, musculoskeletal pain, type 2 diabetes, polycystic ovary syndrome,depression, anxiety, and a range of complex chronic conditions.
Keywords: naturopathic medicine, naturopathy, global, systematic review, whole-system, pragmatic
Introduction
Naturopathic medicine is an eclectic practice of healthcare united by core underlying philosophy, theory, and
principles. A central tenet of naturopathic philosophy is vismedicatrix naturae (the healing power of nature), an ancientconcept often ascribed to Hippocrates,1,2 that refers to aninherent, self-organizing healing process in living systemswhich establishes, maintains, and restores health.1
The terms ‘‘whole-system’’ & ‘‘multi-modality’’ withinthe context of naturopathic medicine are outlined in Table 1.Broadly these refer to the practice of naturopathic medi-cine as a complex health care intervention, which utilizesa combination of clinical modalities (or therapies) in the
treatment of each individual. This contrasts with a singlemodality approach where only one therapy is used. Mod-alities used in naturopathic practice are determined by astructured system of theory and principles based within itsphilosophy; refer to Table 1 for a list of core modalities.
The World Health Organization (WHO) defines natu-ropathy as part of Traditional and Complementary Medicine(T&CM) and has recommended this sector to build evi-dence to support its safe and effective use.3 The imperativeto increase the evidence base of T&CM results from theemergence of evidence-based medicine (EBM) in the lastquarter of the twentieth century.4 While a substantial body ofevidence for the effectiveness of the ‘‘tools of trade’’ of na-turopathic medicine (i.e., herbal and nutritional supplements;
1National Centre for Naturopathic Medicine, Southern Cross University, Lismore, Australia.2NatMed Research Unit, Division of Research, Southern Cross University, Lismore, Australia.3Foundations of Naturopathic Medicine Institute, Snoqualmie, Washington.4Integria Healthcare, Ballina, Australia.
ª Stephen P. Myers and Vanessa Vigar, 2019; Published by Mary Ann Liebert, Inc. This Open Access article is distributedunder the terms of the Creative Commons License (http://creativecommons.org/licenses/by/4.0), which permits unrestricteduse, distribution, and reproduction in any medium, provided the original work is properly cited.
THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE JACMVolume 25, Number 2, 2019, pp. 141–168Mary Ann Liebert, Inc.DOI: 10.1089/acm.2018.0340
141

and lifestyle interventions [LIs]) is now available, thereexists little quantitative scientific evidence documenting itas an effective medical practice.5
The movement toward developing a scientific evidencebase for naturopathic medicine is not without controversy.Some have argued that EBM is antithetical to naturopathy,out of concern that traditional naturopathic philosophy andpractice will be marginalized or excluded in a process ofcoercing nonorthodox systems of health and healing to fitinto the mainstream scientific paradigm.6 Others argue thatalthough there exist inevitable tensions between T&CM and
EBM epistemologies, these tensions and their resolutionsalso can hold the key to a more productive understandingbetween traditional and scientific knowledge.7
Galvanized by this need to develop a body of quantitativescientific evidence supporting naturopathic medicine, a groupof U.S. naturopathic researchers received a grant from theNational Institutes of Health’s National Center for Com-plementary and Integrative Health (previously the NationalCenter for Complementary and Alternative Medicine) in2006 to develop a Naturopathic Medical Research Agenda(NMRA).8 The project involved research directors from ev-ery North American institution with a naturopathic program,Southern Cross University (an Australian institution with apublicly funded naturopathic medicine program), along with1200 naturopathic academics, practitioners, students, andselected medical researchers. The primary recommendationfrom the NMRA was that research be conducted on the wholepractice of naturopathic medicine, rather than on singleagents (such as individual herbal or nutritional supplements).8
Following the NMRA recommendations, significant re-search occurred, especially in North America. In 2015, asystematic review of this research,9 including 15 clinicalstudies reporting on the outcomes of multi-modality treat-ment delivered by North American naturopathic physicians,was published. They concluded that while many samplesizes were small, results indicated that receiving whole-system naturopathic medicine was associated with improvedhealth outcomes and improved quality of life (QOL) inpatients with or at risk for chronic conditions, includingcardiovascular disease (CVD), type 2 diabetes, chronic pain,anxiety, multiple sclerosis, hepatitis C, and menopausalsymptoms.9 Also in 2015,9 the World Naturopathic Fed-eration (WNF) convened its inaugural meeting. The WNFnow represents more than 50 international naturopathic or-ganizations with a primary goal to promote and advancethe naturopathic profession. Given this international interest,it is timely to undertake a systematic scoping review thatsummarizes the state of the evidence for whole-system,multi-modality naturopathic medicine across the world. Asystematic scoping review differs from a systematic reviewin that it sets out to examine the extent, range, and nature ofresearch activity in a broad area,10 while a systematic reviewgenerally sets out to answer a focused question by synthe-sizing all available research. The main goal of this scopingstudy is to highlight the breadth of the quantitative scientificresearch in naturopathic medicine.
Methods
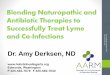
In July 2018, the authors undertook a comprehensive searchof MEDLINE, Embase, CINAHL, AMED, and the WHOregional indexes (AIM, LILACS, IMEMR, IMSEAR, WPRIM).The MEDLINE search strategy is shown in Figure 1; othersearch strings are available upon request.
In addition, the authors conducted additional hand sear-ches of the following journals: British Naturopathic Jour-nal, Townsend Letters, Journal of the Australian TraditionalMedicine Society, The International Journal of Naturo-pathic Medicine, and the Journal of Orthomolecular Medi-cine. Submissions to the Australian Natural Therapy Reviewregarding the effectiveness of naturopathic medicine11 werealso searched for additional references.
Table 1. Definitions for Key Study Components
Naturopathicmedicine
The WNF defines the naturopathicprofession based on two fundamentalphilosophies of medicine (vitalism andholism) and seven principles of practice(healing power of nature; treat thewhole person; treat the cause; first, dono harm; doctor as teacher; healthpromotion and disease prevention; andwellness).10 The philosophy, theory,and principles are translated to clinicalpractice through a range of therapeuticmodalities. The WNF has identifiedseven core modalities: (1) clinicalnutrition and diet modification/counseling; (2) applied nutrition (use ofdietary supplements, traditionalmedicines, and natural health careproducts); (3) herbal medicine; (4)lifestyle counseling; (5) hydrotherapy;(6) homeopathy, including complexhomeopathy; and (7) physicalmodalities (based on the treatmentmodalities taught and allowed in eachjurisdiction, including yoga,naturopathic manipulation, and musclerelease techniques).10 This scopingstudy is limited to naturopathicmedicine as defined and encompassedby the WNF. Other systems oftraditional medicine, such asTraditional Chinese Medicine andAyurveda, are not included in thissystematic scoping review study.
Multi-modality Within the context of this systematicscoping review, ‘‘multi-modalitynaturopathic practice’’ was defined asincluding a minimum of two modalitiesas part of a single clinical approach totreatment of an individual. The practiceof a single modality was considered tobe more indicative of that specificmodality, rather than eclecticnaturopathic general practice.
Whole system Refers to the practice of naturopathicmedicine as a complex health careintervention that addressessimultaneously the multiple dimensions(physical, mental, spiritual, family,community, and environment) of anindividual patient1 as pragmaticallypracticed by naturopathic clinicians.
WNF, World Naturopathic Federation.
142 MYERS AND VIGAR

Studies were included if they met the following criteria:
(1) Controlled clinical trials, longitudinal cohort studies,observational trials, or case series involving five ormore cases presented in any language
(2) Human studies(3) Multi-modality treatment administered by a naturo-
path (naturopathic clinician, naturopathic physician)as an intervention
(4) Non-English language studies in which an Englishtitle and abstract provided sufficient information todetermine effectiveness
(5) Case series in which five or more individual cases werepooled and authors provided a summative discussion ofthe cases in the context of naturopathic medicine
It was decided that case series with less than five caseswere more representative of the individual cases, rather thanan evaluation of whole-system naturopathic treatment in aspecific condition.
Titles and abstracts were screened by both authors, basedon the inclusion criteria, with disagreements settled bydiscussion.
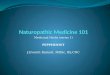
See Figure 2 for a flowchart documenting the studyselection.
Data extraction
The following data from included studies were extracted(V.V.) and summarized using a data extraction sheet: studyreference, origin, condition, number of participants, studydesign, primary outcomes, patient-reported outcomes, andmodalities utilized. Data were divided by conditions treated(Tables 2–8).
Methodological assessment and quality rating
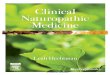
Risk of bias assessment was conducted on all clinical trialreports using the Cochrane Collaboration Risk of Bias tool(Fig. 3).12
Results
Studies meeting inclusion criteria
A total of 2551 titles were located and the titles and ab-stracts screened for eligibility. Full text of 95 primarystudies and 12 gray literature studies were reviewed in detail(totalling 107). Thirty-three articles were accepted for in-clusion, totalling 9859 study participants. The primary rea-sons for exclusion were lack of multi-modality treatment(i.e., only a single modality was practiced) or the studies didnot identify that treatments were conducted by naturopathicclinicians. Notably, studies were excluded because theyprescribed naturopathic-style treatments, but were adminis-tered by integrative doctors or other personnel not identifiedas naturopathic. Two poster presentations were includ-ed,13,14 in which the data were relevant and not reportedelsewhere.
Characteristics of included studies
A majority of the included studies were observationalcohort studies (12 prospective and 8 retrospective), with 11clinical trials and 2 case series (Table 9). Studies were re-ported from seven different locations: United States (US),Canada, Germany, India, Australia, Japan, and the UnitedKingdom. The studies are diverse in nature, representingshort-term inpatient care (primarily in studies from Indiaand Germany) to longer term observational reports of out-patient treatment (primarily in the US and Canada). Thesettings of care included private naturopathic practice, in-tegrative hospitals, inpatient health care clinics, or researchinstitutes.
Research locations
United States. Eleven articles from the US are includedin this review. Of these, nine also are included in the Oberget al. (2015) systematic review of naturopathic wholesystem practice in North America.9 Two additional studies
FIG. 1. Medline SearchStrategy.
WHOLE-SYSTEM MULTI-MODALITY NATUROPATHIC MEDICINE: A SCOPING REVIEW 143

published after the 2015 review also were identified.15,16 Allstudies were of chronic disease conditions: three in chronicpain management of different etiologies17–19; three evalu-ated outcomes in type 2 diabetes management20–22; two inmood disorders15,16; and one on treatment of hypertension.23
The remaining two studies included treatment for hepatitisC24 and menopausal symptoms.25
Seven publications were prospective or retrospectiveobservational studies,15,20–25 three were randomized con-trolled trials (RCTs),17–19 and one was a case series ofdifficult-to-treat patients.16 All the studies were conductedin the community in either public or private naturopathicclinics or in community health centers.
The naturopathic modalities included diet counseling andphysical activity recommendations, stress reduction strate-gies, dietary supplements, hydrotherapy, manual therapy,and botanical medicines.9
Canada. Four articles were conducted in Canada spe-cifically in a population of Canada Post employees. Theseincluded two in chronic pain management,26,27 one in anx-iety,28 and one for primary prevention in CVD.29 All ofthese studies were RCTs, conducted at work-site clinics, andall were included in the Oberg et al. review of 2015. Nat-uropathic modalities included dietary counseling, nutritionalsupplementation, and relaxation techniques. One study usedacupuncture in addition to the other modalities.27
Germany. Six articles from Germany were identified forinclusion.14,30–34 Two were conducted in the treatment ofmusculoskeletal pain,14,33 three in various chronic conditions ofmixed etiology,31,32,34 and one examining QOL measures.35
Five were conducted in integrative hospitals, and one wasconducted in a residential, long-term care setting. The naturo-pathic care reported in these studies is from integrative inpatient
FIG. 2. Flow diagram of study selection.
144 MYERS AND VIGAR

Ta
ble
2.
Ca
rd
io
va
scu
la
rD
isea
se
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Edla
2016
India
Hyper
tensi
on
104
Pro
spec
tive
cohort
study.
Hyper
tensi
ve
pat
ients
enro
lled
into
ayoga
and
inte
gra
ted
nat
uro
pat
hy
hosp
ital
over
a3-m
onth
per
iod.
All
had
15
day
sin
care
and
3-m
onth
foll
ow
-up.
Blo
od
pre
ssure
,an
thro
pom
etry
,ch
ole
ster
ol,
Tgs,
and
HbA
1C
.P
rim
ary
study
outc
om
e—B
Pco
ntr
ol
plu
s50%
or
gre
ater
reduct
ion
indose
of
anti
hyper
tensi
ve
med
icat
ion
rela
tive
tobas
elin
e.C
om
pli
ance
.
79
(99%
)ac
hie
ved
targ
etB
Pco
ntr
ol
(<140/9
0m
mH
g)
and
66
(83%
)ac
hie
ved
this
wit
h>5
0%
reduct
ion
inan
tihyper
tensi
ve
med
icat
ion
dose
,an
din
8(1
0%
)pat
ients
,al
lm
edic
atio
ns
wer
ew
ithdra
wn.
Red
uct
ion
intr
igly
ceri
des
was
signifi
cant
mea
ndif
fere
nce
of
-19.3
(85.4
)(
p<
0.0
01),
and
HbA
1C
was
signifi
cantl
yre
duce
dam
ong
dia
bet
ics.
Ast
ruct
ure
dre
siden
tial
pac
kag
eof
veg
etar
ian
die
t,yoga-
bas
edex
erci
se,
and
pat
ient
educa
tion
inad
dit
ion
tophar
mac
oth
erap
y.
Bra
un
2014
Aust
rali
aC
ardia
csu
rger
ypat
ients
—post
oper
ativ
eoutc
om
es
337
Pro
spec
tive
cohort
study—
Inte
gra
tive
card
iac
wel
lnes
spro
gra
m(I
CW
P)
(n=
337),
del
iver
edto
pat
ients
under
goin
gca
rdia
csu
rger
y,
com
par
edw
ith
mat
ched
cohort
rece
ivin
g‘u
sual
care
’fr
om
pre
vio
us
yea
rs(n
=585).
Post
surg
ery
outc
om
es:
24
hr
seru
mtr
oponin
I,in
otr
ope
requir
emen
ts,
low
outp
ut
stat
e,at
rial
fibri
llat
ion
(AF
),hosp
ital
length
of
stay
(LO
S),
blo
od
loss
.
ICW
Phad
signifi
cantl
yre
duce
dre
quir
emen
tfo
rpost
surg
ery
inotr
opic
support
(p
<0.0
001),
are
duce
din
ciden
ceof
low
outp
ut
stat
e(
p=
0.0
25)
and
are
duce
dra
teof
atri
alfi
bri
llat
ion
(p
=0.0
29)
inco
mpar
ison
to‘u
sual
care
’gro
up.
Aft
erad
just
ing
for
bas
elin
eim
bal
ance
sby
mult
ivar
iate
anal
ysi
s,th
ere
duct
ion
inin
otr
opic
support
rem
ained
signifi
cant
(p
<0.0
01)
wit
ha
rela
tive
reduct
ion
of
42%
.
Sta
ndar
diz
ednutr
itio
nal
supple
men
tre
gim
ew
ith
short
indiv
idual
ized
nat
uro
pat
hic
consu
ltat
ion
(10–
20
min
)to
dis
cuss
die
tan
dli
fest
yle
chan
ge.
See
ly2013
Can
ada
CV
D246
Ran
dom
ized
contr
oll
edtr
ial—
2ar
ms:
-usu
alca
re(U
C)
-ad
junct
nat
uro
pat
hic
care
(NC
-enhan
ced
usu
alca
re)
Pre
ven
tion
of
CV
Din
cohort
atin
crea
sed
risk
of
CV
D—
1yea
rev
aluat
ion
of
risk
pro
file
Fra
min
gham
risk
score
,pre
val
ent
met
aboli
csy
ndro
me,
SF
-36
Com
par
edw
ith
par
tici
pan
tsin
the
UC
gro
up,
at52
wee
ks
those
inth
eN
Cgro
up
had
are
duce
dad
just
ed10-y
ear
card
iovas
cula
rri
skU
C:
10.8
1%
;N
C:
7.7
4%
;ri
skre
duct
ion–3.0
7%
[95%
confi
den
cein
terv
al(C
I):
-4.3
5%
to- 1
.78%
],p
<0.0
01,
and
alo
wer
adju
sted
freq
uen
cyof
met
aboli
csy
ndro
me
UC
:48.4
8%
;N
C:
31.5
8%
;ri
skre
duct
ion–16.9
0%
[95%
CI:
-29.5
5%
to-4
.25%
],p
=0.0
02.
Indiv
idual
ized
trea
tmen
t,in
cludin
gsp
ecifi
cdie
tan
dli
fest
yle
reco
mm
endat
ions,
and
the
pre
scri
pti
on
of
sele
cted
nat
ura
lhea
lth
pro
duct
s
(conti
nued
)
145

Ta
ble
2.
(Co
ntin
ued
)
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Nan
dak
um
ar2012
India
CV
Dri
skfa
ctors
72
PO
ST
ER
PR
ES
EN
TA
TIO
N.
Pil
ot
study
of
3-w
eek
yoga
and
nat
uro
pat
hy
inte
rven
tion
inpat
ients
wit
hknow
nC
VD
risk
fact
ors
.A
ctiv
egro
up
com
par
edto
wai
t-li
sted
contr
ol.
BP
,B
MI,
lipid
pro
file
,blo
od
glu
cose
,an
dpsy
cholo
gic
mea
sure
ssu
chas
Hosp
ital
Anxie
tyan
dD
epre
ssio
nS
cale
(HA
DS
).S
om
atiz
atio
nco
mponen
tof
SC
L90
and
gen
eral
hea
lth
per
cepti
on
Sig
nifi
cant
reduct
ions
(p
<0.0
5)
insy
stoli
cblo
od
pre
ssure
(140.3
6vs.
124.6
2),
dia
stoli
cblo
od
pre
ssure
(85.2
8vs.
76.9
3),
fast
ing
blo
od
glu
cose
(142.2
9vs.
116.6
1),
post
pra
ndia
lblo
od
glu
cose
(233.2
vs.
172.1
9),
body
mas
sin
dex
(33.0
5vs.
31.8
6),
tota
lch
ole
ster
ol
(181.6
1vs.
161.0
4),
LD
Lch
ole
ster
ol
(107.7
6vs.
85.7
2),
trig
lyce
rides
(152.8
vs.
131.7
4),
anxie
ty(6
.79
vs.
4.9
8),
dep
ress
ion
(6.5
4vs.
4.4
5),
and
som
atiz
atio
nsy
mpto
ms
(7.8
4vs.
3.5
6)
com
par
edto
wai
t-li
sted
contr
ol
at3
wee
ks.
Yoga
pri
mar
ytr
eatm
ent.
Nat
uro
pat
hy
bas
edli
fest
yle
inte
rven
tion.
Murt
hy
2011
India
Hyper
tensi
on
104
Pro
spec
tive
cohort
study.
Inpat
ient
trea
tmen
tw
ith
nat
uro
pat
hy
and
yoga
for
3w
eeks
inpat
ients
wit
hm
ild-t
o-
moder
ate
hyper
tensi
on.
1-y
ear
foll
ow
-up.
Med
icat
ion
was
rem
oved
wher
eposs
ible
.
Blo
od
pre
ssure
,body
wei
ght,
lipid
pro
file
Mea
nsy
stoli
cblo
od
pre
ssure
on
adm
issi
on
was
139.6
–16.2
,w
hic
hre
duce
dto
129.6
–10.4
on
dis
char
ge,
dia
stoli
cre
duce
dfr
om
91.2
–9.8
to86.1
–5.6
,(
p<
0.0
01).
Of
thes
e(9
3%
achie
ved
‘norm
al’
blo
od
pre
ssure
of
whic
h54%
wer
eno
longer
rece
ivin
gan
tihyper
tensi
ve
med
icat
ion).
All
pat
ients
wer
efo
llow
edup
for
aper
iod
of
1yea
rpost
dis
char
ge.
The
num
ber
of
pat
ients
who
report
edfo
rfo
llow
-up
wer
e74
(71.1
%)
at3
month
s,68
(65%
)at
6m
onth
s,62
(57%
)at
9m
onth
s,an
d57
(54%
)at
1yea
r.T
he
per
centa
ge
of
pat
ients
mai
nta
inin
gnorm
alblo
od
pre
ssure
wit
hout
med
icat
ion
dec
reas
edover
the
12-
month
per
iod
to24%
at12
month
s(o
fth
ose
that
retu
rned
for
foll
ow
-up).
Res
iden
tial
yoga
and
nat
uro
pat
hy
bas
edli
fest
yle
inte
rven
tion.
Bra
dle
y2011
Unit
edS
tate
sH
yper
tensi
on
85
Ret
rosp
ecti
ve
cohort
study.
Pat
ients
wit
hst
age
1an
dst
age
2hyper
tensi
on,
wit
hco
ncu
rren
tuse
of
med
icat
ion.
Min
imum
6m
onth
sof
nat
uro
pat
hic
care
Blo
od
pre
ssure
-sy
stoli
c(S
BP
)&
dia
stoli
c(D
BP
)
Pat
ients
wit
hboth
stag
e1
and
stag
e2
hyper
tensi
on
appea
red
toim
pro
ve
duri
ng
care
,w
ith
stag
e2
pat
ients
achie
vin
gm
ean
reduct
ions
of
-26
mm
Hg
(p
<0.0
001)
and
-11
mm
Hg
(p
<0.0
001)
inS
BP
and
DB
P,
resp
ecti
vel
y.
The
pro
port
ion
of
pat
ients
achie
vin
gco
ntr
ol
(<140/
90
mm
Hg)
inboth
SB
Pan
dD
BP
was
incr
ease
dsi
gnifi
cantl
yfr
om
14%
to44%
(p
<0.0
33).
Die
t,ex
erci
se,
and
pre
ven
tive
counse
ling
wer
eco
mm
only
pre
scri
bed
.N
utr
itio
nal
and
bota
nic
alsu
pple
men
tati
on
was
also
com
monly
pre
scri
bed
.
CV
D,
card
iovas
cula
rdis
ease
.
146

Ta
ble
3.
Ty
pe
2D
ia
betes
Mellitu
s
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Bai
ry2016
India
T2D
M101
Pro
spec
tive
cohort
study.
Dia
bet
ics
adm
itte
dto
yoga/
nat
uro
pat
hic
hosp
ital
for
trea
tmen
t(1
5-
or
30-d
ayst
ay).
3m
onth
foll
ow
-up.
Ach
ievem
ent
of
gly
cem
icco
ntr
ol
along
wit
hat
leas
t50%
reduct
ion
indose
of
anti
dia
bet
esm
edic
atio
nat
3m
onth
sre
lati
ve
toli
ne
Gly
cem
icco
ntr
ol
par
amet
ers
mea
sure
dat
bas
elin
ean
dat
3m
onth
s,sh
ow
edsi
gnifi
cant
mea
nre
duct
ions
inle
vel
sof
HbA
1C
,F
BS
,an
dP
PB
S,
resp
ecti
vel
y,
0.9
%,
39
mg/d
L,
and
36
mg/d
L(
p<
0.0
01).
This
effe
ctw
asm
ore
pro
nounce
dam
ong
pat
ients
wit
ha
bas
elin
eH
bA
1c
of
‡7%
,w
ith
mea
nre
duct
ions
of
1.2
%,
53
mg/d
L,
and
53
mg/d
Lfo
rH
bA
1c,
FB
S,
and
PP
BS
,re
spec
tivel
y.
Ther
ew
asa
dose
–re
sponse
rela
tionsh
ipbet
wee
nco
mpli
ance
todie
tary
pra
ctic
esan
dH
bA
1c
at3
month
sw
ith
mea
nre
duct
ions
of
0.4
%,1.1
%,
and
1.7
%am
ong
those
wit
hpoor,
moder
ate,
and
exce
llen
tco
mpli
ance
todie
tary
pra
ctic
es,
resp
ecti
vel
y.
Ast
ruct
ure
dre
siden
tial
pac
kag
eof
veg
etar
ian
die
t,yoga-
bas
edex
erci
se,
and
pat
ient
educa
tion
inad
dit
ion
tophar
mac
oth
erap
y.
Bra
dle
y2012
Unit
edS
tate
sD
iabet
es40
Pro
spec
tive
cohort
study
for
adju
nct
ive
care
wit
hnat
uro
pat
hic
med
icin
e(A
NC
,n
=40)
vs.
contr
ols
(Usu
alca
reU
C,
n=
329),
elec
tronic
ally
mat
ched
from
elec
tronic
hea
lth
reco
rds)
—1
yea
rev
aluat
ion
of
effe
cton
dia
bet
espar
amet
ers
inpat
ients
wit
hin
adeq
uat
ely
contr
oll
eddia
bet
es.
HbA
1C
,D
iabet
esse
lf-c
are
asse
ssm
ent
scal
e(S
DS
CA
),P
HQ
-8dep
ress
ion
scal
e
Impro
vem
ents
wer
enote
din
AN
Cgro
up
inse
lf-m
onit
ori
ng
of
glu
cose
,die
t,se
lf-e
ffica
cy,
moti
vat
ion,
and
mood
inS
DS
CA
(p
=0.0
01).
Mea
nH
bA
1c
dec
reas
edby
-0.9
0%
(p
=0.0
2)
inth
eA
NC
cohort
at6
month
s,a
-0.5
1%
mea
ndif
fere
nce
com
par
edto
usu
alca
re(
p=
0.0
7).
Red
uct
ions
at12
month
sw
ere
not
stat
isti
call
ysi
gnifi
cant
(-0.3
4%
inth
eA
NC
cohort
,p
=0.1
4;
-0.3
7%
dif
fere
nce
com
par
edto
the
usu
alca
reco
hort
,p
=0.1
2).
Med
icat
ion
pre
scri
pti
on
and
uti
liza
tion
for
dia
bet
esal
soin
crea
sed
inth
eA
NC
gro
up,
whic
hm
ayhav
eco
ntr
ibute
dto
bet
ter
man
agem
ent
of
glu
cose
level
s.
ND
sw
ere
inst
ruct
edto
del
iver
thei
rty
pic
alca
reto
par
tici
pan
ts.
Die
tan
dli
fest
yle
advic
epre
scri
bed
innea
rly
all
case
s,nutr
itio
nal
supple
men
tati
on
in74%
of
pat
ients
,an
doth
erin
div
idual
ized
care
pla
ns.
Phar
mac
oth
erap
yw
asad
just
ed(i
ncr
ease
d,
dec
reas
ed,
or
chan
ged
)as
nee
ded
.
(conti
nued
)
147

Ta
ble
3.
(Co
ntin
ued
)
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Bra
dle
y2009
Unit
edS
tate
sD
iabet
es37
Ret
rosp
ecti
ve
cohort
study.
Type
2dia
bet
ic(T
2D
M)
pat
ients
,w
ith
mea
ndura
tion
of
care
27
month
san
dav
erag
eof
11
vis
its.
Car
efo
rT
2D
Mw
aspre
dom
inan
tly
adju
nct
ive
care
(80%
)ver
sus
pri
mar
yca
re(2
0%
)duri
ng
obse
rvat
ion
per
iod.
HbA
1C
,li
pid
s,blo
od
pre
ssure
Sig
nifi
cant
mea
nch
anges
wer
e:-0
.65%
for
HbA
1c
(p
=0.0
46),
-45
mg/d
Lfo
rT
AG
(p
=0.0
37),
-7m
mH
gin
SB
P(
p=
0.0
2),
and
-5m
mH
gin
DB
P(
p=
0.0
03)
from
bas
elin
eto
last
vis
it.
Chole
ster
ol
level
ssh
ow
edno
signifi
cant
dif
fere
nce
.
Die
t,li
fest
yle
,st
ress
man
agem
ent,
and
nutr
itio
nal
and
her
bal
supple
men
tati
on
wer
eco
mm
only
pre
scri
bed
.P
har
mac
oth
erap
yw
asad
just
ed(i
ncr
ease
d,
dec
reas
ed,
or
chan
ged
)as
nee
ded
.
Bra
dle
y2006
Unit
edS
tate
sD
iabet
es16
Ret
rosp
ecti
ve
cohort
study.
T2D
Mpat
ients
wit
hat
leas
t6
month
sof
nat
uro
pat
hic
trea
tmen
tev
aluat
ed.
%H
bA
1C
,%
of
pat
ients
reac
hin
gad
equat
egly
cem
icco
ntr
ol,
or
impro
vem
ent
ingly
cem
icco
ntr
ol.
31%
achie
ved
HbA
1C
<7%
,61%
achie
ved
7–10%
,an
d8%
wer
e>1
0%
.T
her
ew
ere
posi
tive
contr
ols
of
chole
ster
ol
and
trig
lyce
ride
mea
sure
s,as
wel
las
44%
achie
vin
g‘g
ood
contr
ol’
of
blo
od
pre
ssure
.44%
of
the
popula
tion
was
also
takin
gora
lan
tidia
bet
icm
edic
atio
nan
d40%
takin
gin
suli
n.
100%
rece
ived
die
tary
counse
ling,
69%
wer
eta
ught
stre
ssre
duct
ion
tech
niq
ues
,an
d94%
wer
epre
scri
bed
exer
cise
.P
atie
nts
addit
ional
lyre
ceiv
edpre
scri
pti
ons
for
bota
nic
alan
dnutr
itio
nal
supple
men
tati
on,
oft
enin
com
bin
atio
nw
ith
conven
tional
med
icat
ion.
148

Ta
ble
4.
Mu
scu
lo
sk
eleta
lP
ain
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Sta
nge
2012
Ger
man
yM
usc
ulo
skel
etal
pai
n221
(IT
T)
101
(pp)
PO
ST
ER
PR
ES
EN
TA
TIO
NP
rosp
ecti
ve
cohort
study.
Pat
ients
wit
hch
ronic
musc
ulo
skel
etal
pai
n(d
ura
tion
>2yea
rs),
trea
ted
for
2w
eeks
appro
xim
atel
yas
inpat
ient
inin
tegra
tive
hosp
ital
.O
utc
om
em
easu
red
atad
mit
tance
tohosp
ital
and
1yea
rpost
inpat
ient
trea
tmen
t.T
reat
men
tin
cluded
allo
pat
hic
med
icin
e,w
ith
inte
gra
tive
CA
Mtr
eatm
ent.
Pai
nas
mea
sure
don
avis
ual
anal
og
scal
e(V
AS
).Q
OL
mea
sure
dw
ith
SF
-36
Mea
npai
nV
AS
dec
reas
edby
15.1
from
60.7
–23.0
(adm
issi
on)
to45.6
–26.2
(1yea
rpost
-tr
eatm
ent)
(p
<0.0
001,
two-s
ided
tte
st),
wit
hhig
hes
tim
pro
vem
ent
for
low
bac
kpai
n(d
ecre
ase
of
17.5
)an
dno
dif
fere
nti
atio
nfo
rm
ult
i-m
orb
idit
y(n
=46
wit
h,
n=
55
wit
hout)
.S
F-3
6physi
cal
and
men
tal
com
ponen
tsc
ore
sim
pro
ved
signifi
cantl
yfr
om
40.0
–12.2
to44.3
–12.5
and
from
29.6
–8.2
to32.9
–10.5
,re
spec
tivel
y(p
<0.0
001
for
each
).
Die
tan
dfa
stin
g,
physi
cal
ther
apy,
rela
xat
ion,
her
bs,
acupunct
ure
,an
dneu
ral
ther
apy.
Wie
bel
itz
2011
Ger
man
yC
hro
nic
bac
kpai
n161
Pro
spec
tive
cohort
study.
Nat
uro
pat
hic
(n=
161)
vs.
ort
hoped
ic(n
=187)
care
of
bac
kpai
n.
Outc
om
em
easu
red
atdis
char
ge,
3m
onth
s,an
d6
month
s.
Osw
estr
ysc
ore
and
SF
-36.
Num
ber
of
spec
iali
stco
nsu
ltat
ions,
med
icat
ion,
psy
choth
erap
yco
sts
For
the
mai
nan
dse
condar
yobje
ctiv
es,
ther
ew
asno
signifi
cant
dif
fere
nce
bet
wee
ngro
ups.
Osw
estr
yS
core
atT
0:
43.0
,95%
CI:
39.6
–45.3
;at
T2:
40.7
,95%
CI:
37.4
–44.0
).O
nly
inth
esu
bgro
up
of
wom
en,
who
acco
unt
for
86%
of
the
nat
uro
pat
hic
pat
ients
,a
dif
fere
nce
inth
em
ain
obje
ctiv
e(O
swes
try
Sco
re)
was
found
(p
=0.0
14)
infa
vor
of
nat
uro
pat
hy
(T2:
32.6
,95%
CI:
24.9
–40.2
)co
mpar
edto
ort
hoped
ics
(T2:
45.1
,95%
CI:
41.2
–49.1
).T
reat
men
tre
sult
sof
nat
uro
pat
hic
inpat
ient
trea
tmen
tof
chro
nic
bac
kpai
nar
eco
mpar
able
toco
nven
tional
ort
hoped
ictr
eatm
ent
atal
lpoin
tsof
tim
e.
Die
t,physi
cal
ther
apy,
life
style
advic
e,psy
choth
erap
y,
and
phyto
ther
apy.
(conti
nued
)
149

Ta
ble
4.
(Co
ntin
ued
)
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Szc
zurk
o2009
Can
ada
Rota
tor
cuff
tendin
itis
85
Ran
dom
ized
contr
oll
edtr
ial—
2ar
ms:
-st
andar
diz
edphysi
cal
exer
cise
sw
ith
pla
cebo
supple
men
tati
on
(PC
)-
nat
uro
pat
hic
care
(NC
)C
anad
ian
post
alw
ork
ers
wit
hro
tato
rcu
ffte
ndin
itis
trea
ted
for
12
wee
ks.
Should
erP
ain
and
Dis
abil
ity
Index
(SP
AD
I),
SF
-36
Fin
alto
tal
SP
AD
Isc
ore
sdec
reas
edby
54.5
%(
p<
0.0
001)
inth
eN
Cgro
up
and
by
18%
(p
=0.0
241)
inth
eP
Cgro
up.
The
SF
-36
show
edst
atis
tica
lly
signifi
cant
dif
fere
nce
s(
p<
0.0
1)
bet
wee
nth
eN
Can
dP
Cgro
ups
inal
lsu
bca
tegori
esex
cept
soci
alfu
nct
ionin
g,
whic
hsh
ow
eda
tren
dto
war
dim
pro
vem
ent
(p
=0.0
38).
The
NC
gro
up
show
edth
egre
ates
tim
pro
vem
ent
over
the
PC
gro
up
inro
lephysi
cal
(p
=0.0
015),
bodil
ypai
n(
p=
0.0
004),
and
inro
leem
oti
onal
(p
=0.0
020).
Die
tary
counse
ling,
acupunct
ure
,an
dP
hlo
gen
zym
(2ta
ble
tsth
rice
/day
)—not
an‘i
ndiv
idual
ized
‘nat
uro
pat
hic
’m
odel
of
trea
tmen
t.
Shin
to2008
Unit
edS
tate
sM
ult
iple
scle
rosi
s45
Ran
dom
ized
contr
oll
edtr
ial—
6m
onth
s,3
arm
s:-
nat
uro
pat
hic
med
icin
e(n
m)
-usu
alca
re(U
C)
-U
C+
educa
tion
Modifi
edfa
tigue
impac
tsc
ale,
Bec
kdep
ress
ion
inven
tory
(BD
I),
cognit
ion
test
s,neu
rolo
gic
impai
rmen
t(E
DS
S),
mult
iple
scle
rosi
sfu
nct
ional
ity,
SF
-36
No
signifi
cant
dif
fere
nce
sbet
wee
ngro
ups
on
any
outc
om
em
easu
re.
Atr
end
favori
ng
the
nat
uro
pat
hic
care
gro
up
inth
egen
eral
hea
lth
subsc
ale
of
the
SF
-36
(p
=0.1
1),
tim
edw
alk
(p
=0.1
1),
and
neu
rolo
gic
impai
rmen
t(
p=
0.0
7).
Set
nat
uro
pat
hic
inte
rven
tion:
mult
ivit
amin
/min
eral
wit
hout
iron,
vit
amin
C,
vit
amin
E,
fish
oil
,an
da-
lipoic
acid
and
intr
amusc
ula
rvit
amin
B12
once
aw
eek.
Spec
ific
die
t.
Rit
enbau
gh
2008
Unit
edS
tate
sT
emporo
man
dib
ula
rdis
ord
ers
(TM
Ds)
160
Ran
dom
ized
contr
oll
edtr
ial—
3ar
ms:
-usu
alca
re(U
C)
-T
radit
ional
Chin
ese
Med
icin
e(T
CM
)-
nat
uro
pat
hic
med
icin
e(N
M)
TC
M-2
0tr
eatm
ents
NM
-10
appoin
tmen
ts
Wors
t/av
erag
esc
ore
of
faci
alpai
n,
inte
rfer
ence
wit
hac
tivit
ies,
effe
ctof
pai
non
Act
ivit
ies
of
Dai
lyL
ife
(AD
L)
Over
all,
reduct
ions
inw
ors
tpai
nat
end
of
trea
tmen
tan
d3
month
spost
-tre
atm
ent
wer
e13%
and
22%
for
UC
,29%
and
33%
for
TC
M,
and
28%
and
39%
for
NM
.O
ver
all,
the
aver
age
pai
nre
duct
ions
aten
dof
trea
tmen
tan
d3
month
spost
-tre
atm
ent
wer
e,re
spec
tivel
y,16%
and
27%
inS
C,
35%
and
42%
inT
CM
,an
d28%
and
40%
inN
M.
No
signifi
cant
dif
fere
nce
inan
yof
the
trea
tmen
tar
ms
for
chan
ges
inA
DL
.
TC
M(a
cupunct
ure
,her
bs,
tuin
a,re
laxat
ion).
NM
(her
bs,
nutr
ients
,an
dphysi
cal
med
icin
e).
All
trea
tmen
tsw
ere
indiv
idual
ized
.
(conti
nued
)
150

Ta
ble
4.
(Co
ntin
ued
)
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Szc
zurk
o2007
Can
ada
Chro
nic
low
bac
kpai
n75
Ran
dom
ized
contr
oll
edtr
ial—
2ar
ms:
-st
andar
diz
edphysi
oth
erap
ypro
gra
m(P
C-
educa
tion
and
inst
ruct
ion
on
physi
oth
erap
yex
erci
ses)
-nat
uro
pat
hic
care
(NC
)C
anad
ian
post
alw
ork
ers
wit
hlo
wer
bac
kpai
n>6
wee
ks,
trea
tmen
tfo
r12
wee
ks.
Osw
estr
yL
ow
Bac
kP
ain
Dis
abil
ity
Ques
tionnai
re(O
LB
PD
),S
F-3
6
NC
gro
up
report
edsi
gnifi
cantl
ylo
wer
bac
kpai
n(2
6.8
9,
95%
CI:
29.2
3–23.5
4,
p=
0.0
001)
than
the
physi
oth
erap
ygro
up.
The
dif
fere
nce
inm
ean
chan
ge
score
sin
the
OL
BP
Dfr
om
bas
elin
eto
wee
k12
resu
lted
ina
signifi
cant
reduct
ion
of
dis
abil
ity
inth
enat
uro
pat
hic
care
gro
up
com
par
edto
the
contr
ol
gro
up
(med
ian
chan
ge
=25;
p=
0.0
001).
QO
Lw
asal
sosi
gnifi
cantl
yim
pro
ved
inth
egro
up
rece
ivin
gN
Cin
all
dom
ains
exce
pt
for
vit
alit
y.
Die
tary
counse
ling,
dee
pbre
athin
gre
laxat
ion
tech
niq
ues
,an
dac
upunct
ure
.
Sec
or
2004
Unit
edS
tate
sP
ain
from
any
cause
,as
afe
ature
of
adm
issi
on
94
Pro
spec
tive
cohort
study—
3ar
ms:
-ac
upunct
ure
(AC
)-
chir
opra
ctic
(CC
)-
nat
uro
pat
hic
med
icin
e(N
M)
All
pat
ients
had
‡3tr
eatm
ents
and
ast
arti
ng
vis
ual
anal
og
score
(VA
S)
pai
nle
vel
of
>2.
Pai
nV
AS
,S
F-1
2F
rom
bas
elin
eto
end
of
study,
the
VA
Sav
erag
eac
ross
all
arm
sof
the
study
was
signifi
cantl
yre
duce
dby
49%
from
4.4
to2.3
(p
<0.0
001).
Acu
punct
ure
reduce
dfr
om
5.0
to3.3
(34%
);C
hir
opra
ctic
from
4.2
to2.0
(52%
);nat
uro
pat
hic
60%
pai
nre
duct
ion
(p
<0.0
001).
SF
-12
—si
gnifi
cant
impro
vem
ent
over
all
inphysi
cal
hea
lth
seen
inal
lm
odal
itie
s(
p<
0.0
001)
and
for
the
indiv
idual
modal
itie
sof
acupunct
ure
(p
<0.0
09)
and
chir
opra
ctic
(p
<0.0
05).
Men
tal
hea
lth
had
no
signifi
cant
chan
ge
for
all
trea
tmen
ts.
Acu
punct
ure
,ch
iropra
ctic
,or
nat
uro
pat
hic
trea
tmen
t.N
aturo
pat
hic
trea
tmen
tin
cluded
nutr
itio
nal
supple
men
tati
on,
her
bal
med
icin
e,nutr
itio
n,
exer
cise
,physi
cal
med
icin
em
odal
itie
s,poss
ibly
pre
scri
pti
on
dru
gs.
QO
L,
qual
ity
of
life
.
151

Ta
ble
5.
Mo
od
Diso
rd
ers
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Bre
ed2017
Unit
edS
tate
sD
epre
ssio
nan
dA
nxie
ty60
Pro
spec
tive
cohort
study.
Pat
ients
atte
ndin
gco
mm
unit
yhea
lth
cente
rfo
ran
xie
tyor
dep
ress
ion
trea
tmen
t.T
hose
that
atte
nded
>2vis
its
had
dat
aan
alyze
d,
mea
nnum
ber
of
vis
its
=3.3
.D
uri
ng
the
study
per
iod,
all
60
par
tici
pan
tssa
wa
nat
uro
pat
hic
physi
cian
(25%
saw
only
anat
uro
pat
h),
and
55%
also
saw
aco
nven
tional
pro
vid
er.
Pat
ient
Hea
lth
Ques
tionnai
re(P
HQ
-9)
for
dep
ress
ion.
Gen
eral
ized
Anxie
tyD
isord
er7-i
tem
scal
e(G
AD
-7)
for
anxie
ty.
Res
ponse
rate
mea
sure
dby
those
wit
ha
50%
dec
reas
ein
score
from
anin
itia
lsc
ore
of
‡10
Mea
nbas
elin
eP
HQ
-9w
as16.4
(i.e
.,m
oder
ate-
to-s
ever
edep
ress
ion)
Mea
nbas
elin
eG
AD
-7sc
ore
was
12.4
(i.e
.,m
oder
ate
anxie
ty).
Impro
vem
ent
of
sym
pto
ms
over
tim
e(1
6.4
vs.
8.6
,p
<0.0
001)
for
dep
ress
ion
and
for
anxie
ty(1
2.4
vs.
7.2
,p
<0.0
001).
The
aver
age
chan
ge
over
all
was
48%
dec
reas
efo
rdep
ress
ion
and
42%
dec
reas
efo
ran
xie
ty.
The
pri
mar
youtc
om
eof
>50%
dec
reas
efr
om
init
ial
score
sw
asac
hie
ved
by
58.6
%of
dep
ress
ion
pat
ients
and
50%
of
anxie
typat
ients
.T
he
over
all
impro
vem
ent
insy
mpto
ms
of
dep
ress
ion
and
anxie
tyw
ashig
hly
signifi
cant
(p
<0.0
001).
Modal
itie
sin
cluded
all
types
of
Nth
Am
eric
annat
uro
pat
hic
care
.M
ost
com
monly
use
dw
ere
nutr
aceu
tica
ls(7
5%
),hom
eopat
hy
(30%
),her
bal
s(2
5%
),an
dac
upunct
ure
(20%
).P
har
mac
euti
cm
edic
atio
nw
asal
sopre
scri
bed
.
Gure
vic
h2015
Unit
edS
tate
sB
ipola
rdis
ord
er7
Cas
ese
ries
—7
pat
ients
that
had
poor
resp
onse
or
signifi
cant
side
effe
cts
from
conven
tional
med
icat
ion.
Ret
rosp
ecti
ve
anal
ysi
sof
pat
ients
wit
htr
eatm
ent
>1yea
r.
Wit
hdra
wal
of
med
icat
ion.
Men
tal/
mood
stat
e.C
linic
alG
lobal
Impre
ssio
nS
core
for
Impro
vem
ent
(CG
I-I)
Psy
chotr
opic
med
icat
ions
wer
egra
dual
lyel
imin
ated
wit
hnat
uro
pat
hic
support
.C
GI-
Isc
ore
sim
pro
ved
from
aver
age
of
5dow
nto
1–2
for
all
pat
ients
.N
opat
ients
suff
ered
psy
choti
cep
isodes
or
hosp
ital
izat
ion
duri
ng
trea
tmen
tper
iod.
Long-t
erm
mai
nte
nan
ceof
bip
ola
rdis
ord
er.
Phyto
ther
apy,
vit
amin
/min
eral
supple
men
tati
on,
acupunct
ure
,hom
eopat
hy,
die
tm
odifi
cati
on,
exer
cise
,an
dre
gula
tion
of
slee
pcy
cles
.G
uid
edim
ager
y,
ener
get
ic/
spir
itual
ther
apie
s,an
dpsy
choth
erap
yw
ere
use
das
nee
ded
.
(conti
nued
)
152

Ta
ble
5.
(Co
ntin
ued
)
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Sar
ris
2014
Aust
rali
aA
nxie
ty&
mood
15
Pil
ot
obse
rvat
ional
study
of
nat
uro
pat
hic
care
inpri
vat
enat
uro
pat
hic
pra
ctic
e.D
ata
from
15
nat
uro
pat
hs
over
31
consu
ltat
ions
was
poole
dfo
ran
alysi
s,w
ith
only
8re
turn
consu
ltat
ions
bei
ng
report
ed.
DA
SS
-21,
PO
MS
-65,G
ener
alH
ealt
hQ
ues
tionnai
re(G
HQ
-28)
Asi
gnifi
cant
effe
ctocc
urr
edfo
rti
me,
wit
hpat
ients
hav
ing
are
duct
ion
of
pat
ient-
rate
ddep
ress
ion,
anxie
ty,
and
stre
sson
the
DA
SS
-21.
Spec
ifica
lly,
dep
ress
ion
was
reduce
dby
-9.5
0(F
=18.1
3,
p=
0.0
02);
anxie
tyby
-9.2
5poin
ts(F
=13.7
8,
p=
0.0
05),
and
stre
ssby
-12.0
0poin
ts(F
=18.8
0,
p=
0.0
02).
On
the
PO
MS
-65,
tota
lm
ood
dis
turb
ance
was
signifi
cantl
yre
duce
dac
ross
Tim
eby
-33.1
3poin
ts(F
=11.6
6,
p=
0.0
01).
On
the
GH
Q-2
8,
asi
gnifi
cant
reduct
ion
occ
urr
edfo
rpat
ient-
rate
dso
mat
icsy
mpto
ms
-5.7
5(F
=5.4
6,
p=
0.0
18),
anxie
tyan
din
som
nia
sym
pto
ms
-6.2
5(F
=14.7
1,
p<
0.0
01),
and
soci
aldysf
unct
ion
-9.5
0(F
=14.0
2,
p<
0.0
01).
Her
bal
,nutr
itio
nal
,li
fest
yle
advic
e,die
tad
vic
e.In
div
idual
ized
trea
tmen
tpla
ns.
Coole
y2009
Can
ada
Anxie
ty75
Ran
dom
ized
contr
oll
edtr
ial—
2ar
ms:
-st
andar
diz
edpsy
choth
erap
yca
rew
ith
pla
cebo
supple
men
tati
on
(PT
)-
nat
uro
pat
hic
care
(NC
)E
mplo
yee
sw
ith
moder
ate-
to-s
ever
ean
xie
ty(>
6w
eeks)
.T
he
NC
was
ase
tre
gim
enan
dnot
indiv
idual
ized
toea
chper
son.
Bec
kA
nxie
tyIn
ven
tory
(BA
I),
SF
-36,
Mea
sure
Yours
elf
Med
ical
Outc
om
eP
rofi
le(M
YM
OP
)
Bec
kA
nxie
tyIn
ven
tory
(BA
I)dec
reas
edby
56.5
%(p
<0.0
001)
inth
eN
Cgro
up
and
30.5
%(
p<
0.0
001)
inth
eP
Tgro
up
from
bas
elin
eto
study
end,
asw
ell
asin
the
subsc
ales
of
the
BA
I,sh
ow
ing
gre
ater
impro
vem
ent
com
par
edto
PT
.P
atie
nt
cente
red
outc
om
esas
mea
sure
dby
the
MY
MO
Pques
tionnai
resh
ow
edsi
gnifi
cant
reduct
ions
insy
mpto
ms
1(
p<
0.0
001)
and
sym
pto
m2
(p
=0.0
12)
inth
eN
Cgro
up
com
par
edto
the
PT
gro
up.
Die
tary
counse
ling,
dee
pbre
athin
gre
laxat
ion
tech
niq
ues
,a
stan
dar
dm
ult
ivit
amin
,an
dW
ithania
som
nif
era
(600
mg
per
day
of
stan
dar
diz
edro
ot)
.N
ot
an‘i
ndiv
idual
ized
‘nat
uro
pat
hic
’m
odel
.T
he
PT
inte
rven
tion
rece
ived
psy
choth
erap
y,
mat
ched
dee
pbre
athin
gre
laxat
ion
tech
niq
ues
,an
dpla
cebo
table
ts.
153

Ta
ble
6.
Co
mplex
Ch
ro
nic
Disea
se
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
eR
esult
sM
odali
ties
Teu
t2013
Ger
man
yO
lder
adult
sin
nurs
ing
hom
es,
mix
edet
iolo
gy
58
Pra
gm
atic
pil
ot
study,
clust
erra
ndom
ized
.O
lder
adult
sli
vin
gin
nurs
ing
hom
ety
pe
situ
atio
n,
random
ized
tousu
alca
re(U
C)
or
addit
ional
inte
gra
tive
med
icin
e(I
M)
regim
esover
12
month
s.A
ver
age
age
76.0
–12.8
(UC
)an
d82.7
–8.6
(IM
)
Nurs
esO
bse
rvat
ion
Sca
lefo
rG
eria
tric
Pat
ients
(NO
SG
ER
);A
sses
smen
tof
Moto
ran
dP
roce
ssS
kil
ls;
Bar
thel
Index
;Q
ual
idem
;an
dM
ini-
men
tal
Sta
teE
xam
inat
ion.
Pro
file
of
wel
l-bei
ng
Aft
er12
month
s,ef
fect
size
sin
the
IMgro
up
inco
mpar
ison
toU
Cw
ere
incr
ease
din
the
foll
ow
ing
area
s.E
ffec
tsi
ze‡0
.3w
ere
obse
rved
for
acti
vit
ies
of
dai
lyli
vin
gon
the
NO
SG
ER
-Act
ivit
ies
of
Dai
lyL
ivin
gsu
bsc
ale
(0.5
3),
Bar
thel
Index
(0.3
0),
Qual
idem
tota
lsu
msc
ore
(0.3
9),
Pro
file
of
Wel
l-bei
ng
(0.3
6),
NO
SG
ER
-Im
pai
red
Soci
alB
ehav
ior
(0.4
7),
and
NO
SG
ER
-Dep
ress
edM
ood
subsc
ales
(0.4
0).
Sm
alle
ror
no
effe
cts
wer
eobse
rved
for
all
oth
eroutc
om
es.
Mult
ifac
eted
trea
tmen
tpla
n.
Wee
kly
60-m
inex
erci
se;
nat
uro
pat
hic
care
(tea
s,w
raps,
com
pre
sses
,her
bal
mas
sage)
;fr
esh
fruit
/veg
juic
es;
hom
eopat
hy.
Chan
ges
inm
edic
atio
ns
wer
epre
scri
bed
by
the
IMdoct
ors
involv
ed.
Med
ical
doct
ors
and
nurs
esad
min
iste
red
most
of
the
ther
apy,
one
nat
uro
pat
hin
volv
ed.
Wei
den
ham
mer
2007
Ger
man
yR
ehab
ilit
atio
ncl
inic
—var
ious
chro
nic
condit
ions
5278
Pro
spec
tive
cohort
study.
Eval
uat
ion
of
nat
uro
pat
hic
trea
tmen
tef
fect
on
chro
nic
condit
ions
(all
of
the
pat
ients
adm
itte
dto
the
hosp
ital
over
2yea
rs)
Foll
ow
-up
dis
char
ge,
2m
th,
6m
th,
and
12m
th.
Var
ious,
SF
-36
The
inte
nsi
tyof
the
mai
nco
mpla
int
dec
reas
edfr
om
59
–25
by
anav
erag
eof
25
poin
tsat
dis
char
ge
(19
poin
tsat
6-m
onth
foll
ow
-up)
corr
espondin
gto
anef
fect
size
of
0.8
6(0
.62
at6-m
onth
foll
ow
-up).
At
6-m
onth
foll
ow
-up
about
hal
fof
the
pat
ients
show
eda
clin
ical
lyre
levan
tim
pro
vem
ent
of
qual
ity
of
life
(SF
-36
sum
score
sin
crea
sed
by
5or
more
poin
ts).
Inta
ke
of
dru
gs
was
reduce
d,
the
num
ber
of
day
soff
work
had
dec
reas
edaf
ter
rehab
ilit
atio
n.
Pat
ients
’sa
tisf
acti
on
was
‘good’
on
aver
age;
wit
hre
spec
tto
food
sati
sfac
tion
itw
aslo
wer
.
Phyto
ther
apy,
life
style
,an
dhydro
ther
apy—
adap
ted
toth
ein
div
idual
.
Isbel
l2007
UK
Mix
edet
iolo
gy
49
Ret
rosp
ecti
ve
eval
uat
ion
of
pat
ient
asse
ssed
impro
vem
ent
inm
ain
sym
pto
ms
afte
rtr
eatm
ent
ata
mult
idis
cipli
nar
yco
mple
men
tary
ther
apie
scl
inic
.P
rim
aril
ym
usc
ulo
skel
etal
pro
ble
ms
trea
ted.
All
pat
ients
wit
h>2
trea
tmen
tsover
3yea
rsev
aluat
ed.
MY
MO
Pev
aluat
ion
of
all
pat
ients
Bet
wee
nfi
rst
and
last
consu
ltat
ion,
57%
(n=
28)
rate
dan
impro
vem
ent
inth
eir
firs
tsy
mpto
mM
YM
OP
and
35%
rate
dan
impro
vem
ent
inth
eir
over
all
wel
l-bei
ng
score
.B
efore
trea
tmen
t37%
of
the
sam
ple
(n=
46)
rate
dth
eir
sym
pto
ms
as3
or
less
.A
fter
trea
tmen
t78%
of
pat
ients
rate
dth
eir
sym
pto
ms
as3
or
less
.
Nat
uro
pat
hy,
ost
eopat
hy,
and
Cra
nio
Sac
ral
ther
apy
clin
ic—
ther
ew
asno
dif
fere
nti
atio
nbet
wee
nth
edif
fere
nt
trea
tmen
tsre
port
ed.
(conti
nued
)
154

Ta
ble
6.
(Co
ntin
ued
)
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
eR
esult
sM
odali
ties
Ost
erm
ann
2002
Ger
man
yM
ult
iple
-rh
eum
atic
,m
etab
oli
c,&
alle
rgic
-type
dis
ease
1026
Pro
spec
tive
cohort
study.
Bla
nken
stei
nnat
uro
pat
hic
hosp
ital
eval
uat
ing
effe
ctiv
enes
sof
trea
tmen
t.>3
wee
kin
pat
ient
nat
uro
pat
hic
trea
tmen
t.O
utc
om
esev
aluat
edon
adm
issi
on,
dis
char
ge,
and
3m
onth
san
d6
month
saf
ter
dis
char
ge.
QO
L(H
LQ
&S
F-3
6),
mood,
physi
cal
com
pla
ints
(GB
B24),
and
pai
nper
cepti
on
(SE
S)
All
subsc
ales
,as
wel
las
the
tota
lsc
ore
sof
the
psy
chom
etri
cte
stin
stru
men
ts,
show
edhig
hly
signifi
cant
chan
ges
(tte
st,
p<
0.0
1)
bet
wee
nth
eti
me
‘hosp
ital
izat
ion’
and
‘dis
char
ge’
.W
ithin
the
foll
ow
-up
thes
eval
ues
wer
est
abil
ized
on
ale
vel
signifi
cantl
yhig
her
than
the
init
ial
level
.P
ain
dec
reas
edon
aver
age
from
26
on
adm
itta
nce
to15
on
dis
char
ge
wit
ha
level
bet
wee
n20
and
22
at3-
and
6-m
onth
foll
ow
-up.
HL
Qan
dS
F-3
6w
ere
both
hig
her
on
dis
char
ge
than
at3
or
6m
onth
sfo
llow
-up,
but
stil
lsi
gnifi
cantl
yhig
her
than
on
adm
issi
on.
Phyto
ther
apy,
life
style
,an
dhydro
ther
apy—
adap
ted
toth
ein
div
idual
.
Bee
r2001
Ger
man
yA
cute
inpat
ient
nat
uro
pat
hic
care
618
Pro
spec
tive
cohort
study.
Inpat
ient
nat
uro
pat
hic
trea
tmen
t(B
lanken
stei
nhosp
ital
).T
hre
ew
eeks
of
trea
tmen
tw
ith
outc
om
esev
aluat
edon
adm
issi
on,
dis
char
ge,
3m
onth
s,&
6m
onth
s.
Qual
ity
of
life
—m
easu
red
by
short
form
-36
(SF
-36)
and
Her
dec
ke
Ques
tionnai
refo
rQ
ual
ity
of
Lif
e(H
LQ
)
HL
Qim
pro
ved
from
bas
elin
esc
ore
of
50–58
on
dis
char
ge
and
dro
pped
to55
at3
month
san
d54
at6
month
s,in
dic
atin
gth
atth
eim
pro
vem
ent
was
atle
ast
par
tial
lysu
stai
ned
.S
F-3
6sh
ow
edim
pro
vem
ent
inso
me
subdom
ains
afte
rdis
char
ge,
wit
hphysi
cal
pai
n,
gen
eral
hea
lth
per
cepti
on,
and
emoti
onal
/soci
alas
pec
tsim
pro
vin
gfu
rther
bet
wee
n3–6
month
saf
ter
dis
char
ge.
All
subsc
ales
,as
wel
las
the
tota
lsc
ore
sof
life
qual
ity,
show
edhig
hly
signifi
cant
impro
vem
ents
(tte
st,
p<
0.0
1)
bet
wee
nth
eti
mes
of
‘hosp
ital
izat
ion’
and
‘dis
char
ge’
.D
uri
ng
foll
ow
-up
thes
eval
ues
stab
iliz
edon
ale
vel
signifi
cantl
yhig
her
than
the
init
ial
level
.
Phyto
ther
apy,
life
style
,an
dhydro
ther
apy—
adap
ted
toth
ein
div
idual
.
QO
L,
qual
ity
of
life
.
155

Ta
ble
7.
Asth
ma
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Rao
2014
India
Ast
hm
a134
Ret
rosp
ecti
ve
anal
ysi
sof
bro
nch
ial
asth
ma
pat
ients
’in
-pat
ient
nat
uro
pat
hy
and
yoga
pro
gra
mfo
r21
day
s,w
ith
foll
ow
-up
monit
ori
ng
for
up
to3
yea
rs.
Lung
funct
ion
capac
ity
(FV
C,
PE
FR
,V
C,
FE
V1,
FE
V/F
EC
%,
MV
V).
Ther
ew
asa
signifi
cant
incr
ease
inF
VC
,F
EV
1,
and
PE
FR
atal
lti
me
poin
tspost
adm
issi
on
to6
month
s,p
<0.0
035.
Chan
ges
inP
EF
Rw
ere
mai
nta
ined
toth
e36-m
onth
foll
ow
-up.
Ther
ew
asal
sosi
gnifi
cant
incr
ease
inth
eM
VV
mea
nval
ues
;how
ever
only
from
adm
issi
on
till
the
dat
eof
dis
char
ge
(p
<0.0
035).
Yoga
pri
mar
ytr
eatm
ent.
Nat
uro
pat
hic
care
incl
uded
die
t,m
ud
pac
k,
enem
a,st
eam
trea
tmen
ts,
hydro
ther
apy,
and
mas
sage.
Phar
mac
olo
gic
trea
tmen
tsal
sopre
scri
bed
.
Sat
hyap
rabha
2001
India
Bro
nch
ial
asth
ma
37
Nonra
ndom
ized
tria
l.P
atie
nts
wit
has
thm
afo
llow
edfo
r21-d
ayobse
rvat
ional
per
iod
(contr
ol)
bef
ore
inpat
ient
trea
tmen
tfo
r21
day
s(y
oga/
nat
uro
pat
hic
care
).
Lung
funct
ion
capac
ity
(FV
C,
PE
FR
,V
C,
FE
V1,
FE
V/F
EC
%,
MV
V).
ES
R,
eosi
nophil
count.
Med
icat
ion
was
wit
hdra
wn
over
the
firs
tfe
wday
sin
the
trea
tmen
thosp
ital
.L
ung
funct
ion
signifi
cantl
yin
crea
sed
acro
ssal
lm
easu
red
par
amet
ers
(p
<0.0
01).
Eosi
nophil
counts
and
ES
Ral
sore
duce
dsi
gnifi
cantl
yover
3w
eeks
(p
<0.0
1).
Die
tin
cluded
fast
ing
pro
toco
l,nat
ure
cure
—ex
tern
alher
bal
trea
tmen
ts(s
team
bat
hin
g,
hot
pac
ks
etc.
),yoga
>1hour
dai
ly.
156

Ta
ble
8.
Mix
ed
Co
nd
itio
ns
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Cra
mer
2003
Unit
edS
tate
sM
enopau
sesy
mpto
ms
239
Ret
rosp
ecti
ve
cohort
wit
h’u
sual
care
’(U
C)
contr
ols
(UC
—th
ese
wer
eel
ectr
onic
ally
mat
ched
hea
lth
reco
rds)
.P
atie
nt
gro
up
consi
sted
of
79
nat
uro
pat
hic
pat
ients
and
160
conven
tional
pat
ients
.
%of
pat
ients
wit
him
pro
vem
ent
insy
mpto
ms
Inm
ult
ivar
iate
anal
yse
s,pat
ients
trea
ted
wit
hnat
uro
pat
hy
wer
eap
pro
xim
atel
yse
ven
tim
esm
ore
likel
yth
anco
nven
tional
lytr
eate
dpat
ients
tore
port
impro
vem
ent
for
inso
mnia
(odds
rati
o[O
R],
6.7
7;
95%
CI:
1.7
1–26.6
3)
and
dec
reas
eden
ergy
(OR
,6.5
5;
95%
CI:
0.9
6–44.7
4).
Nat
uro
pat
hy
pat
ients
report
edim
pro
vem
ent
for
anxie
ty(O
R,
1.2
7;
95%
CI:
0.6
3–2.5
6),
hot
flas
hes
(OR
,1.4
0;
95%
CI:
0.6
8–2.8
8),
men
stru
alch
anges
(OR
,0.9
8;
95%
CI:
0.4
3–2.2
4),
and
vag
inal
dry
nes
s(O
R,
0.9
1;
95%
CI:
0.2
1–3.9
6)
about
asfr
equen
tly
aspat
ients
who
wer
etr
eate
dco
nven
tional
ly.
ND
physi
cian
sar
epri
mar
yca
repro
vid
ers
wit
ha
scope
of
pra
ctic
eth
atin
cludes
nutr
itio
nal
supple
men
tati
on,
her
bal
med
icin
e,nutr
itio
n,
exer
cise
,physi
cal
med
icin
em
odal
itie
s,m
inor
surg
ery,
and
phar
mac
oth
erap
y.
Mil
lim
an2000
Unit
edS
tate
sH
epat
itis
C41
Ret
rosp
ecti
ve
revie
wof
41
conse
cuti
ve
case
sof
Hep
atit
isC
.O
fth
ese
only
14
did
not
under
go
inte
rfer
on
ther
apy
and
wer
etr
eate
dw
ith
nat
uro
pat
hic
met
hods.
Nat
uro
pat
hic
trea
tmen
tfo
r>1
month
was
requir
edfo
rin
clusi
on.
Ala
nin
eam
inotr
ansf
eras
e(A
LT
)
Bas
elin
eA
LT
level
was
127
U/L
(ran
ge:
47–256).
The
aver
age
AL
Tval
ues
for
pat
ients
on
the
pro
toco
lfo
ra
min
imum
of
1m
onth
was
92
U/L
(ran
ge:
25–
235;
p=
0.0
26,
pai
red
tte
st).
Of
the
14
pat
ients
report
ed,
seven
show
edan
AL
Tre
duct
ion
of
gre
ater
than
25%
.T
he
oth
erse
ven
pat
ients
had
no
chan
ge
or
asl
ight
incr
ease
inA
LT
.
Set
her
bal
/nutr
itio
nal
pro
toco
lw
ith
var
iati
on
avai
lable
dep
endin
gon
indiv
idual
pre
senta
tion
Niw
a2013
Japan
Hep
atoce
llula
rca
rcin
om
a101
Ret
rosp
ecti
ve
anal
ysi
sof
nat
uro
pat
hic
care
giv
ento
pat
ients
wit
hhep
atoce
llula
rca
rcin
om
a.T
reat
men
tsw
ere
indiv
idual
ized
nat
uro
pat
hic
trea
tmen
ts.
Pro
longed
surv
ival
.K
eyfi
ndin
gw
asth
atth
ose
who
wer
etr
eate
dw
ith
4or
more
dif
fere
nt
agen
tshad
agre
atly
incr
ease
dm
edia
nsu
rviv
alti
me
than
those
trea
ted
wit
h<4
.A
lso,
Cord
ycep
ssi
nen
sis
had
anex
clusi
ve
ben
efit
wit
ha
dra
mat
ical
lyim
pro
ved
surv
ival
inth
ose
that
wer
egiv
enth
isas
par
tof
thei
rtr
eatm
ent.
Pre
dom
inan
tly
her
bal
com
bin
atio
ns,
wit
hC
ord
yce
ps
bei
ng
anim
port
ant
one,
but
also
sand
bat
htr
eatm
ent
(infr
a-re
d),
intr
aven
ous
mult
ivit
amin
infu
sions,
and
life
style
counse
ling.
(conti
nued
)
157

Ta
ble
8.
(Co
ntin
ued
)
Auth
or/
Yea
rC
ountr
yC
ondit
ion
ND
esig
n(a
nd
com
para
tor)
Outc
om
esR
esult
sM
odali
ties
Are
ntz
2017
Aust
rali
aP
oly
cyst
icO
var
ian
Syndro
me
inover
wei
ght
wom
en
122
Ran
dom
ized
contr
oll
edtr
ial—
2ar
ms:
-L
ifes
tyle
inte
rven
tion
-L
ifes
tyle
inte
rven
tion
plu
sst
andar
diz
edher
bal
trea
tmen
tpro
toco
l.3-m
onth
trea
tmen
tper
iod.
Pri
mar
youtc
om
ew
asoli
gom
enorr
hea
/am
enorr
hea
Sec
ondar
youtc
om
esin
cluded
horm
one
modula
tion,
anth
ropom
etri
cs,
QO
L,
mood,
pre
gnan
cy,
bir
thoutc
om
es
At
3m
onth
s,w
om
enin
the
com
bin
atio
ngro
up
reco
rded
are
duct
ion
inoli
gom
enorr
hea
of
32.9
%(9
5%
CI:
23.3
–42.6
,p
<0.0
1)
com
par
edw
ith
contr
ols
.M
enst
rual
cycl
ele
ngth
was
43
day
s(9
5%
CI:
21–65,
p<
0.0
01)
low
erfo
rw
om
enin
the
her
bal
med
icin
egro
up
than
for
those
inth
eli
fest
yle
only
gro
up.
The
trea
tmen
tef
fect
size
was
esti
mat
edas
larg
eZ
2/
p=
0:1
1.
Oth
ersi
gnifi
cant
impro
vem
ents
wer
efo
und
for
BM
I(
p<
0.0
1);
insu
lin
(p
=0.0
2)
and
lute
iniz
ing
horm
one
(p
=0.0
4);
blo
od
pre
ssure
(p
=0.0
1);
qual
ity
of
life
(p
<0.0
1);
dep
ress
ion,
anxie
ty,
and
stre
ss(
p<
0.0
1);
and
pre
gnan
cyra
tes
(p
=0.0
1).
Per
sonal
ized
life
style
pla
ns
and
life
-coac
hin
gfo
ral
lpar
tici
pan
ts.
Addit
ional
poly
-her
bal
form
ula
tion
for
the
com
bin
edli
fest
yle
and
her
bal
trea
tmen
tgro
up.
Pra
dee
p2016
India
HIV
posi
tive
pat
ients
under
goin
gan
tire
trovir
al(A
RT
)tr
eatm
ent
40
Par
alle
lnonra
ndom
ized
mat
ched
case
–co
ntr
ol
tria
l—2
arm
s:-
AR
T+
life
style
counse
ling
-A
RT
+nat
uro
pat
hic
care
1-m
onth
trea
tmen
tw
ith
resu
lts
eval
uat
edat
6m
onth
s.P
atie
nts
wer
em
atch
edfo
rag
e,se
x,
CD
4co
unts
,an
dnum
ber
of
yea
rsof
infe
ctio
n.
CD
4co
unts
Res
ult
s:A
fter
the
end
of
6m
onth
s,th
eIG
show
edsi
gnifi
cant
chan
ges
CD
4ce
llco
unt
(p
=3.9
6E
-05).
The
CG
also
show
eda
signifi
cant
impro
vem
ent
inC
D4
cell
counts
(p
=0.0
24)
but
not
of
the
sam
em
agnit
ude
asof
IG.
An
indep
enden
tt
test
bet
wee
nth
egro
ups
has
show
nth
atth
eIG
was
more
signifi
cant
(p
=0.0
47).
Aw
ide
range
of
hydro
ther
apy
trea
tmen
tsw
ere
giv
en,
asw
ell
asyoga,
counse
ling,
die
t,ju
ice
ther
apy,
mudpac
ks,
and
sun
bat
hs.
Pat
ients
wer
egiv
entr
eatm
ents
asin
pat
ients
for
1m
onth
and
then
foll
ow
edth
ese
inte
rven
tions
athom
eunti
l6
month
s.
QO
L,
qual
ity
of
life
.
158

treatment in hospitals where naturopathic methods are usedalong with conventional medical methods. Four of thestudies were observational, while two were RCTs.31,33 Nat-uropathic modalities included dietary interventions (in-cluding fasting), botanical medicine, physical therapy, andhydrotherapy as the main interventions, with additionalhomeopathy,31 acupuncture,14 and psychotherapy33 providedin one study each.
India. Seven studies from India13,36–41 included three inhypertension or CVD risk,13,37,38 two in asthma,39,40 one intype 2 diabetes,36 and one as an adjuvant to antiretroviraltherapy.41 All of the Indian studies were inpatient treatmentsin either naturopathic hospitals or research institutes, with15–30 days of care. These residential treatments could beclassed as highly intensive, with yoga as the primary focusfor all of the studies (being practiced up to four sessionsper day). Naturopathic modalities included in the treat-ments varied, but consisted mainly of a specific vegetariandiet (often including a fasting protocol) and topical or in-
halation applications that may or may not include botanicalmedicine. Pharmaceutic medication is also used as needed,with medication being concurrently reduced or withdrawn,as appropriate.
Australia. Three studies from Australia were identi-fied.42–44 One of these was an observational pilot study ofindividualized naturopathic care for patients with anxietyand mood disorders conducted across private practice clin-ics,42 with most of the practitioners providing botanicaland nutritional medicine along with diet and lifestyle ad-vice. The second study was an open-label prospective cohortstudy of an integrative cardiac wellness program in patientsundergoing cardiac surgery in a hospital setting, which wascompared with a matched cohort of patients receiving‘‘usual care’’,43 and the third was a pragmatic clinical trialin private naturopathic practice.44 These latter two studiesprovided a set naturopathic protocol, including nutritional orbotanical medicine in conjunction with personalized life-style and dietary planning.
FIG. 3. Cochrane riskof bias assessment tables. gray,low risk of bias; light gray, un-clear risk of bias; dark gray, highrisk of bias
WHOLE-SYSTEM MULTI-MODALITY NATUROPATHIC MEDICINE: A SCOPING REVIEW 159

United Kingdom. One study was identified from theUnited Kingdom, which was a retrospective evaluation ofpatient-assessed improvement in their primary symptomafter treatment at a multidisciplinary complementary ther-apy clinic.45 The conditions were primarily musculoskeletalcomplaints and were treated with naturopathy, osteopathy,or CranioSacral therapy, with no distinction given betweenthe different treatments in the report.
Japan. One study was identified from Japan, whichwas a retrospective analysis of all patients from a particu-lar treatment center with hepatocellular carcinoma. Patientsreceived individualized naturopathic treatment, including theuse of medicinal mushrooms and other botanical medicinesas the mainstay of treatment, with additional therapies, in-cluding intravenous multivitamin infusions and lifestylecounseling.46
Clinical conditions, study design, settings,and modalities
Included studies are categorized by clinical condition andstudy design (Table 9) and by clinical setting (outpatient andinpatient) and modalities (Table 10).
Cardiovascular disease. Six studies were assessed thatinvestigated outcomes for present CVD or development ofCVD risk factors, including two RCTs and four prospectivecohort studies.
Four of these studies evaluated hypertension as a primaryoutcome.
� In India, results of two observational inpatient studies onpopulations with hypertension demonstrated substantiveblood pressure control (<140/90 mmHg) after naturo-pathic treatment.37,38 In one study (n = 104), 93% ofparticipants achieved control after 21 days ( p < 0.001),38
while a separate study (n = 104) found that 99% ofparticipants achieved control after 15 days ( p < 0.001).37
In both studies, results were achieved in addition tosimultaneous reduction or elimination of antihyper-tensive medication in a substantive number of theparticipants.
� A poster abstract from India reported a randomizedwaitlisted controlled clinical trial (n = 72),13 whichdemonstrated an overall significant reduction ( p < 0.05)in mean systolic blood pressure (-15 mmHg; 140–125 mmHg) and mean diastolic blood pressure (-8 mmHg;85–77 mmHg) after 3 weeks of intensive inpatienttreatment.13
Table 9. Clinical Conditions and Study Design Index
Condition Year Author RCTNoncontrolled
trialProspective
cohortRetrospective
cohortCaseseries
Musculoskeletal pain 2012 Stange X
2010 Wiebelitz X
2009 Szczurko X
2008 Shinto X
2008 Ritenbaugh X
2007 Szczurko X
2004 Secor X
Cardiovascular disease 2016 Edla X
2014 Braun X
2013 Seely X
2012 Nandakumar X
2011 Bradley X
2011 Murthy X
Diabetes 2016 Bairy X
2012 Bradley X
2009 Bradley X
2006 Bradley X
Mood 2017 Breed X
2015 Gurevich X
2014 Sarris X
2009 Cooley X
Asthma 2014 Rao X
2001 Sathyaprabha X
Polycystic ovarian syndrome 2017 Arentz X
Cancer 2013 Niwa X
Menopause 2003 Cramer X
Hepatitis C 2000 Milliman X
Multiple sclerosis 2008 Shinto X
HIV 2016 Pradeep X
Mixed chronic conditions 2013 Teut X
2007 Weidenhammer X
2007 Isbell X
2002 Ostermann X
2001 Beer X
RCT, randomized controlled trial.
160 MYERS AND VIGAR

Ta
ble
10.
Clin
ica
lS
ettin
gs
an
dM
od
alities
Used
Co
un
try
Au
tho
r/Y
ear
Set
tin
gIn
pa
tien
tY
/ND
ura
tio
n(w
eeks
)
Mo
da
liti
esp
resc
rib
ed
Pharm
ace
uti
cD
iet
Phyt
oth
erapy
Nu
trit
ion
al
Agen
tsA
cupunct
ure
Yoga
Hyd
roth
erapy
Hom
eopath
yP
hys
ical
ther
apy
Rel
axa
tio
nex
erci
ses
Oth
er
US
Bre
ed2017
Hea
lthP
oin
t—in
tegra
ted
mult
idis
cipli
nar
yco
mm
unit
yh
ealt
hce
nte
r
NA
v3
vis
its
XX
XX
XX
Gu
rev
ich
20
15
Pri
vat
ep
sych
iatr
icp
ract
ice
N>5
2X
XX
XX
Bra
dle
y2012
Gro
up
hea
lth—
inte
gra
ted
hea
lth
care
N>5
2X
XX
X
Bra
dle
y2
01
1B
asty
rce
nte
rfo
rn
atu
ral
hea
lth
N>2
6X
XX
Bra
dle
y2
00
9B
asty
rce
nte
rfo
rn
atu
ral
hea
lth
N*
11
0X
XX
X
Rit
enb
aug
h2
00
8M
edic
alcl
inic
N1
6X
XX
Sh
into
20
08
Nat
uro
pat
hic
clin
icN
26
XX
XX
Bra
dle
y2
00
6B
asty
rce
nte
rfo
rn
atu
ral
hea
lth
N>2
6X
XX
X
Sec
or
2004
Spec
ial
care
holi
stic
wel
lnes
sco
nnec
tion-h
osp
ital
-affi
liat
edo
utp
atie
nt
CA
Mcl
inic
N1
2X
XX
XX
Cra
mer
20
03
1C
AM
Cli
nic
&6
Co
nv
enti
on
alM
edic
alC
lin
ics
NA
v6
vis
its
XX
XX
Mil
lim
an2
00
0P
riv
ate
nat
uro
pat
hic
pra
ctic
eN
>4X
X
Can
ada
See
ly2
01
3W
ork
site
loca
tio
n—
Can
ada
Po
stem
plo
yee
sN
52
XX
XX
Co
ole
y2
00
9W
ork
site
loca
tio
n—
Can
ada
Po
stem
plo
yee
sN
12
XX
XX
Szc
zurk
o2009
Work
site
loca
tion
—C
anad
aP
ost
emp
loy
ees
N1
2X
XX
X
Szc
zurk
o2007
Work
site
loca
tion
—C
anad
aP
ost
emp
loy
ees
N1
2X
XX
Ger
man
yT
eut
2013
Res
iden
tial
care
pro
gra
mY
52
XX
XX
X
Sta
nge
2012
Cen
tre
of
Inte
gra
tive
Med
icin
eY
52
XX
XX
Wie
bel
itz
20
11
Pri
vat
en
atu
ropat
hic
pra
ctic
eY
2–
3X
XX
X
Wei
den
ham
mer
20
07
CA
Mre
hab
ilit
atio
ncl
inic
YV
arie
sX
XX
Ost
erm
ann
20
02
Bla
nk
enst
ein
ho
spit
alY
3X
XX
Bee
r2
00
1B
lan
ken
stei
nh
osp
ital
Y3
XX
X
Ind
iaE
dla
20
16
Man
then
aS
aty
anar
ayan
aR
aju
Aro
gy
alay
amh
osp
ital
Y2
XX
X
Pra
dee
p2016
HIV
sanat
ori
um
of
Nat
ional
inst
itu
teo
fN
atu
rop
ath
y(N
IN),
Pan
chag
ani,
Mah
aras
htr
a
Y4
XX
XX
X
Bai
ry2
01
6M
anth
ena
Sat
yan
aray
ana
Raj
uA
rogy
alay
amh
osp
ital
Y2
–4
XX
X
Rao
2014
Jindal
Nat
ure
Cure
Inst
itute
,B
ang
alore
Y3
XX
XX
X
Nan
dak
um
ar2
01
2N
atu
rop
ath
iccl
inic
Y3
XX
X
Murt
hy
2011
Jindal
Nat
ure
Cure
Inst
itute
,B
ang
alore
Y3
XX
XX
X
Sat
hy
apra
bh
a2
00
1In
stit
ute
of
Nat
uro
pat
hy
and
Yo
gic
Sci
ence
sY
3X
XX
Au
stra
lia
Are
ntz
20
17
Pri
vat
en
atu
ropat
hic
pra
ctic
eN
12
XX
XX
Sar
ris
20
14
Pri
vat
en
atu
ropat
hic
pra
ctic
eN
4–
6X
XX
Bra
un
20
14
Th
eA
lfre
dH
osp
ital
Y>4
XX
X
Un
ited
Kin
gd
om
Isb
ell
20
07
Mu
ltid
isci
pli
nar
yC
AM
clin
icN
Var
ies
XX
XX
Jap
anN
iwa
20
13
Ho
spit
alre
cord
sN
*5
8X
XX
X
161

� A US retrospective analysis of outpatients (n = 85)treated for hypertension in a naturopathic clinic over 6months showed a mean reduction of 26 mmHg systolicand 11 mmHg diastolic ( p < 0.0001) in those with stage2 hypertension and an overall increase from 14% atbaseline to 44% of patients achieving blood pressurecontrol (<140/90 mmHg) over the 6-month treatmentperiod.23
Three studies examined multicomponent CVD risk astreatment outcomes.13,29,43
� An Australian prospective cohort study of patients un-dergoing cardiac surgery compared usual care (n = 585)against a standardized nutritional supplement treat-ment combined with individualized diet and lifestylechange (n = 337).43 Results showed significant post-surgery improvements in cardiac outcomes in the natu-ropathic care group and a 42% reduction in postsurgeryinotropic support ( p < 0.001).
� A Canadian RCT compared usual care against ad-junctive naturopathic care for reducing CVD risk(n = 246).29 Results showed the 10-year FraminghamCVD risk reduced by -3.07%, p < 0.001 for the natu-ropathic over the ‘‘usual care’’ group after 52 weeks.This study also showed a lower frequency of metabolicsyndrome (-16.9%, p = 0.002) in the naturopathic carecohort compared with usual care.
� In addition to the beneficial effects on blood pressurereported above, the randomized waitlisted controlledclinical trial (n = 72)13 from India showed reductions inblood glucose, LDL cholesterol, and triglycerides after3 weeks of residential naturopathic treatment.
Overall, these studies show naturopathic treatment resultsin a clinically significant benefit for treatment of hyperten-sion, reduction in metabolic syndrome parameters, and im-proved cardiac outcomes postsurgery.
Type 2 diabetes. Four studies on type 2 diabetes mel-litus were assessed, including two retrospective and twoprospective cohort studies.
In the US, two retrospective studies and one prospectivecohort study by the same research group from BastyrUniversity20–22 focused on blood glucose management.
� In the initial retrospective study, all subjects (n = 16)received 6 months or more of naturopathic care. Resultsshowed that 31% of patients achieved blood glucosecontrol (HbA1c <7%) and 61% achieved moderatecontrol (HbA1c 7%–10%).21
� A second retrospective study (n = 37) showed reducedHbA1c of -0.65% ( p = 0.046), with a mean duration ofcare of 27 months.20 Other significant positive changeswere demonstrated for blood pressure (-7 mmHg sys-tolic, p = 0.02; and -5 mmHg diastolic, p = 0.003) andtriglycerides (-45 mg/dL, p = 0.037), with no differencein cholesterol.20
� A prospective study (n = 40) showed reduction inHbA1c of -0.90% ( p = 0.02) at 6 months after theinitial visit.22
� One prospective cohort study in India (n = 101)36 ex-amined inpatient naturopathic treatment for 15–30 days,with patients reviewed again at 3 months. Findings
included significant mean reductions of -0.9% inHbA1c ( p < 0.001) after the initial treatment periodand a reduction of -1.7% at 3 months for those withexcellent adherence to the treatment provided.
Overall, these studies show naturopathic treatment resultsin a significant benefit for treatment of diabetes, with re-ductions in HbA1c that are clinically relevant.
Musculoskeletal pain. Six studies of musculoskeletalpain (five articles and one abstract) were included. Clinicalconditions included chronic back pain, rotator cuff tendini-tis, multiple sclerosis, temporomandibular disorder (TMD),and generalized chronic body pain. Two studies were con-ducted in Germany,14,33 three in the US,17–19 and two inCanada.26,27
� A Canadian RCT compared 12 weeks of naturopathiccare with standard physical therapy (n = 75) in em-ployees of Canada Post who had chronic lower backpain. Participants in the naturopathic care cohort showedsignificant improvement ( p < 0.0001) in back pain com-pared with patients receiving standard physical therapy.26
� A German controlled prospective cohort study com-pared naturopathic care with orthopedic care (n = 348)in adults who had chronic back pain requiring inpatienttreatment. This study showed no differences betweennaturopathic and standard orthopedic treatment in thewhole study population. However, at 3 months, a sig-nificant improvement ( p = < 0.014) was found in asubgroup of women receiving naturopathic medicine(86% of the naturopathic patients), compared with or-thopedic care.33
� Also in Germany, a poster abstract reported a prospec-tive clinical trial in chronic musculoskeletal pain (in-cluding back pain), conducted over 2 weeks of inpatienttreatment (n = 221). Naturopathic care decreased meanpain scores by 15.1 from 60.7 – 23.0 (admission) to45.6 – 26.2 (1 year post-treatment) ( p < 0.0001).14
� In Canada, a RCT conducted in rotator cuff tendinitis(n = 85) compared a set naturopathic treatment protocolto a standardized exercise routine/placebo supplemen-tation over 12 weeks. Naturopathic treatment decreasedthe Shoulder Pain and Disability Index by 54.5%( p < 0.0001) compared to 18% ( p = 0.0241) in thecontrol group.27
� In the US, a multiple sclerosis RCT (n = 45) comparednaturopathic treatment with ‘‘usual care’’ and with‘‘usual care plus education’’. They found no significantdifferences between groups on any outcome measure at6 months.19
� Another US RCT investigated naturopathic treatment incomparison to Traditional Chinese Medicine (TCM) andspecialized dental care (n = 160) for TMD. For worstpain, the improvement in the naturopathic medicinegroup was statistically significant compared to special-ized dental care (-1.02 – 0.45, p = 0.025). Naturopathictreatment provided significantly greater decreases thaneither TCM ( p < 0.034) or specialized dental care( p < 0.012) in TMD-related psychosocial interference.17
� Also in the US, subjects with pain from any cause as afeature of presentation were randomized to acupunc-ture, chiropractic, or naturopathic medicine treatment
162 MYERS AND VIGAR

(n = 94). Naturopathic treatment significantly reducedpain from baseline to end of treatment ( p < 0.0001), butwas not statistically significantly different from theother groups.18
Overall, this diverse group of studies shows that naturo-pathic treatment decreased pain scores to a degree compa-rable or better than standard care or other active treatmentcontrols.
Mood disorders. Four studies reported on naturopathictreatment for mood disorders: one in anxiety, one in de-pression, one on both anxiety and depression, and anotheron bipolar disorder.
� A Canadian RCT randomized patients to standardizedpsychotherapy with or without naturopathic care formoderate-to-severe anxiety (n = 75).28 Beck AnxietyInventory scores decreased by 56.5% ( p < 0.0001) inthe naturopathic treatment group compared to 30.5%( p < 0.0001) in the psychotherapy-only group.
� A US prospective cohort study (n = 60) showed sig-nificant improvements using naturopathic treatment,with symptomatic improvement in depression (16.4 vs.8.6, p < 0.0001) and anxiety (12.4 vs. 7.2, p < 0.0001)scores in patients who returned for two or more visits.15
� A small Australian observational study42 (n = 8) showedimproved scores on all areas of the Depression AnxietyStress Scale-21 (DASS-21) and significant improvementin clinical outcomes with naturopathic treatment in pa-tients who returned for two or more visits ( p < 0.005).
� In the US, a retrospective case series reported on asmall subset of patients diagnosed with treatment-resistantbipolar disorder (n = 7) receiving >1 year of naturo-pathic treatment.16 Results were varied, but showedmood stabilization along with withdrawal of psycho-tropic medication.
Overall, significant reductions in anxiety and depressionlevels were shown across this group of studies.
Complex chronic disease. A total of five studies wereincluded for complex chronic disease, comprising a broadgroup of mixed chronic conditions within individuals. Theprimary outcomes included changes in QOL and symptomscores.
� In Germany, three prospective cohort studies examinedeffectiveness of naturopathic treatment outcomes over abroad group of mixed chronic conditions, in terms ofQOL outcomes.32,34,35 The studies all used differentoutcome measures to evaluate treatment effectiveness,with all showing positive results for improving QOL. Inone study, the intensity of the main complaint de-creased from 59 – 25 by an average of 25 points atdischarge (reduced to 19 points at 6-month follow-up)corresponding to an effect size of 0.86 (0.62 at 6-monthfollow-up).32 The other two studies report statisticallysignificant increases across the majority of QOL do-mains as measured by two independent QOL scales( p < 0.01).34,35
� Also in Germany, a cluster-randomized trial (n = 58) ofnaturopathic care compared with usual care in aged
residential community living31 showed a small-to-medium effect size on a range of geriatric QOL scales.
� In the United Kingdom (UK), a retrospective evalua-tion of clinic outpatients (n = 49) receiving naturopathiccare over a 3-year period45 showed improvement( p < 0.001) between the first and last consultation inpatients’ symptom scores.
While difficult to group together, this varied group ofstudies shows an overall positive effect on QOL and symp-tomatic improvement with naturopathic care.
Asthma. Two studies of naturopathic treatment forasthma were included.39,40 Both studies were conducted inIndia and both showed that naturopathic inpatient treatmentimproved clinical asthma profiles.
� A nonrandomized crossover trial (n = 37)40 examined21 days of standard drug therapy at home followed by,and compared to, 21 days of intensive naturopathic in-patient treatment. Results showed significant increaseacross all measured lung function parameters ( p < 0.001)and reduced eosinophil counts after naturopathic treat-ment ( p < 0.01).40
� A retrospective evaluation of patients (n = 134)39 alsoinvestigated intensive naturopathic inpatient treatmentfor 21 days and showed a significant increase in someindices of lung function at all time points, from post-admission to 6 months ( p < 0.0035),39 with increasedpeak expiratory flow rate maintained to a 36-monthfollow-up.
Overall, these two Indian studies show significant positiveresults for intensive inpatient naturopathic treatment ofasthma in lung function parameters.
Mixed conditions. This group contains conditions whereonly a single study was found. The areas of these conditionsare as follows: cancer,46 menopause,25 hepatitis C,24 mul-tiple sclerosis,19 polycystic ovary syndrome (PCOS),44 andHIV (as an adjuvant to antiretroviral therapy).41
� In liver cancer, a single retrospective analysis of na-turopathic treatment in Japan (n = 101) showed a dra-matically improved survival rate when Cordycepssinensis was a component of the multi-modality treat-ment administered.46
� In a retrospective cohort study on menopause in the US(n = 79), researchers compared naturopathic treatmentwith usual care (n = 160). The most significant improve-ments resulting from naturopathic treatment occurredfor insomnia and decreased energy, with a sevenfold im-provement over usual care. Improvements in othersymptoms were comparable with improvements in thecontrol group.25
� In a retrospective case series of patients with HepatitisC undertaking naturopathic treatment (n = 14), all par-ticipants showed reductions in serum alanine amino-transferase (ALT) (average 35 U/L). Seven cases showedan ALT reduction of more than 25%.24
� An RCT in multiple sclerosis found no significantdifferences between usual care, usual care plus educa-tion, and usual care plus naturopathic treatment.19
However, statistical trends favoring the naturopathic
WHOLE-SYSTEM MULTI-MODALITY NATUROPATHIC MEDICINE: A SCOPING REVIEW 163

treatment group were found in a single subscale of SF-36 (general health) and in the timed-walk and symp-toms of neurologic impairment (EDSS).
� An RCT in overweight PCOS patients (n = 122) foundhighly significant improvement ( p < 0.001) in the primaryoutcome of oligomenorrhea/amenorrhea after 3 months oftreatment.44 The trial compared effect of a LI alone, withLI plus a botanical medicine protocol. Menstrual cyclelength was 43 days lower for women in the herbal medi-cine group (95% CI: 21–65, p < 0.001) than for those in thelifestyle-only group, with a large effect size. Improve-ments across other areas, including BMI, insulin, hormonelevels, stress, and pregnancy, also were seen.
� A prospective, parallel, matched-control study of na-turopathic and yoga interventions as adjuvant treat-ments to antiretroviral therapy in a group with HIV,conducted over 1 month, showed improved CD4 countin the intervention group over the control group whichreceived only antiretroviral therapy ( p = 0.047).41
Heterogeneity. Clinical heterogeneity (defined as differ-ences in participants, treatments, outcome characteristics, orresearch setting)47 in this scoping review is substantial.While all the interventions are similar in intervention type(whole-system, multi-modality naturopathic medicine), theyvary substantively at the patient level (condition, baselineseverity, age, gender, ethnicity, and comorbidities); inter-vention level (duration and comparator/controls); outcomelevel (outcome measure and definitions); and in researchsetting. The authors did not test for statistical heterogeneity.
Study quality and risk of bias. There is a wide range ofquality in the included studies, given the breadth of the researchreported. Cochrane risk of bias assessments were completed onthe nine RCTs (Fig. 3), showing low risk of bias for all areas,except blinding of participants and personnel, and moderate biasfor allocation concealment. In observational research, selectionbias is considered high for several studies in which retrospectivedata have been reported and where outcomes include only pa-tients who have returned for multiple visits. Reporting bias alsois likely to be high in retrospective studies in which isolatedoutcomes are reported. Several of the prospective cohort studiesare well-conducted, with a low level of bias, particularly those,such as Braun et al.,43 Teut et al.,31 and Bradley et al.,22 thatcompared results with a ‘‘usual care’’ cohort.
Discussion
This systematic scoping review identified a diverse col-lection of quantitative whole-system, multi-modality natu-ropathic medicine research from around the world reported in33 publications. A majority of the research (15 articles) wasconducted in North America, where the modern naturopathicmedical profession has developed48 and where the first schoolof naturopathic medicine was founded by Benedict Lust in1902.1 Other countries contributing research include Ger-many (six studies), where naturopathy is rooted in the de-velopment of hydrotherapy by founders Priessnitz andKneipp,49 and India (six articles) where naturopathy waspopularized and influenced by MK Gandhi, regarded as theFather of the Indian nation, at the turn of the 20th century.50
Clinical outcomes
Although results from these studies are highly diverse, theyalso are predominantly positive, showing improved healthoutcomes and QOL across conditions and across nationalities.These studies demonstrate a broad range of naturopathicmodalities, against a background of different practitionertraining, legislative and regulatory jurisdictions, and differentresearch approaches. Their results concur with Oberg et al.9
who determined the effect sizes of the primary medical out-comes for 13 North American studies, concluding that therewere positive outcomes and improved QOL in individualswith, or at risk for, chronic conditions, including CVD,23,29
type 2 diabetes,20–22 chronic pain,17,18,26,27 anxiety,28 hepa-titis C,24 and menopausal symptoms.25 The authors haveupdated and expanded this review to the global literature,thereby increasing the range of positive outcomes to includedepression and anxiety,15 bipolar disorder,16 asthma,39,40
PCOS,44 and increased cancer survival time.46 It also addsadditional studies to support positive outcomes forCVD,13,37,38,43 type 2 diabetes,36 chronic pain,14,32 and anx-iety and mood disorders.42
Three of the German studies examined mixed chronicconditions and demonstrated positive outcomes for QOL andperceived pain in: older adults (mean age 79.4 years) living innursing homes31 and older adults (mean age 57.3 years) ad-mitted to hospital for allergic complaints and rheumatic,chronic-bronchial, and metabolic diseases.34,35 In addition,one UK study of mixed chronic conditions demonstratedpositive outcome for overall symptom improvement.45
The benefit of naturopathic treatment as an adjunct toantiretroviral treatment in individuals with HIV could not beassessed, because the study41 lacked the data required tomake a clinical assessment of the effect.
The study on multiple sclerosis19 showed no difference inthe primary outcome (the QOL short form 36; SF-36) be-tween the three intervention groups (usual care, usual careplus naturopathic care, or usual care plus education). Shintoet al.19 concluded that positive outcome trends in individualswith multiple sclerosis warranted further evaluation.
Community versus inpatient studies
A main characteristic of the North American research isthat all the studies were undertaken in free-living individualstreated in a community setting. By comparison, all six of theIndian studies, a single UK study, and five of the six Germanstudies were undertaken in inpatients admitted to a treat-ment facility. The three Australian studies were mixed, withtwo in community practice and one in an inpatient setting(Table 9).
In Germany, naturopaths (heilpraktikers) are licensed bythe state and comprise 40,000 of the 60,000 naturopathicprofessionals in Europe.51 Heilpraktikers are nonmedicalpractitioners trained in the philosophy and modalities ofnaturopathic medicine and trace their roots to the origin ofthe profession. To date, no research into whole-system na-turopathic medicine by Heilpraktikers could be located withan English title and abstract. In addition to Heilpraktikers,there is a group of medical doctors (naturheilkunde) whospecialize in naturopathic modalities and self-identify asproviding naturopathic treatment.49 All studies from Ger-many included in this review were undertaken by these
164 MYERS AND VIGAR

naturopathic practitioners in both inpatient and in residentialfacilities.
A meta-analysis52 of eight studies on the effect of Ger-man inpatient integrative medicine research on QOL in-cluded four of the studies included in this scoping review. Arandom effect meta-analysis of the eight studies revealed anoverall effect size of 0.37 (95% CI: 0.28–0.45) in thephysical score and 0.38 (95% CI: 0.30–0.45) in the mentalscore of the SF-36, demonstrating the effectiveness of theinpatient treatment model used in Germany.
Different countries, different designs,similar conclusions
An insight into the diversity of naturopathic treatment,and the outcomes that can be achieved, can be gained bycontrasting two different studies on chronic lower back pain.One study was undertaken in Canada26 in an outpatientsetting in individuals with chronic lower back and the otherin Germany33 in a cohort who required hospitalization forchronic lower back pain.
The Canadian naturopathic treatment consisted of acu-puncture, relaxation techniques, and dietary recommenda-tions (diet high in omega three fatty acids, magnesium, andcalcium). In Germany, classical naturopathic treatment iscodified for use in acute inpatient settings with a minimumrequirement that five of these eight therapies are applied: (1)nutrition therapy; (2) hydrotherapy/thermotherapy; (3) otherphysical modalities; (4) phytotherapy; (5) lifestyle-regulatorytherapy; (6) exercise therapy; (7) detoxification procedures;or (8) an additional procedure (manual therapy, acupuncture/Chinese medicine, homeopathy, neural therapy, or art/musictherapy).53
Both studies used the Oswestry Disability Index as theprimary outcome measure and demonstrated that whole-system multi-modality naturopathic medicine made a sig-nificant difference in comparison to controls. The Canadianstudy demonstrated that naturopathic treatment is more ef-fective than education and exercise for chronic lower backpain. The German study demonstrated that it is comparablewith mainstream orthopedic treatment when back pain is soacute as to warrant inpatient care and that it is potentiallybetter than mainstream orthopedic care for women. Together,these two very different studies demonstrate a stronger casefor the effectiveness of whole-system multi-modality natu-ropathic treatment of chronic lower pain.
Regional differences and generalizability
The WNF has determined that there is a high degree ofglobal consistency in the core concepts that define naturo-pathic medicine and that all countries utilize a commonset of naturopathic modalities.54,55 The consistent positiveoutcomes in similar conditions in different countries arelikely to reflect this commonality.
Regional differences, however, may affect the general-izability of studies, if the scope of practice used in a specificstudy includes treatment modalities that are not accessibleor utilized in other regional areas for historical, legal, oreducational reasons.
Specific regional differences exist in naturopathic practiceconcerning modalities emphasized (e.g., the addition ofacupuncture in Canada or pharmaceutic prescribing rights in
some areas of the US). In some jurisdictions, there are coremodalities underlying naturopathic practice, such as yoga inIndia or the combination of osteopathic techniques withnaturopathic practice in the UK. Thus, the UK study on thetreatment of musculoskeletal conditions using a mixture ofosteopathic and naturopathic techniques45 is consistent withnaturopathic practice in that country.
The diverse practice settings and the extensive range ofmodalities represented in the research provide a sound ar-gument for expanding the scope of practice in jurisdictionswhere generalizability is limited. The extent to which thestudies included in this scoping review are generalizable toother countries must be assessed on a study-by-study basis.
Pragmatic trials versus therapeutic tools
Pragmatic whole-system (whole-practice) research provi-des a ‘‘real life’’ snapshot of how naturopathic medicine ispracticed in the community, reflecting the naturopathic indi-vidualized approach to treatment and ongoing management.In the absence of whole-system data, the only way to effec-tively and objectively evaluate a discipline is to assess itsmajor therapeutic tools. In naturopathic medicine this wouldinclude evidence for dietary and lifestyle interventions andspecific botanical medicines and nutritional supplements.
In 2005, a review was undertaken of naturopathy and ofWestern herbal medicine in Australia.5 The report con-cluded that while evidence for the whole-system practice ofnaturopathic medicine was lacking, a range of nutritionalsupplements and botanical medicines (the ‘‘tools of trade’’)demonstrated benefits at the highest levels of evidence andhave proven efficacy.
In conventional medicine, evidence for the effectivenessof their ‘‘tools of trade’’ (pharmaceutics and surgery) isgenerally considered sufficient to demonstrate the effec-tiveness of its practice. By comparison, a recent govern-mental review of naturopathic medicine in Australia judgedthe practice of naturopathic medicine solely on the scope ofwhole-system research, limited to only systematic reviewscontaining RCTs published since 2008.11 Based on thislimited scope, they concluded that naturopathic medicine’soverall effectiveness could not be proven, and the Govern-ment has proposed exclusion from private health insuranceeffective from April 1st, 2019.
To provide a more comprehensive method for assessingthe effectiveness of naturopathic medicine, there is a realneed for a new type of effectiveness review. Such a reviewwould systematically evaluate evidence for specific thera-peutic agents used by naturopathic clinicians combined withthe results of pragmatic clinical trials on whole-system na-turopathic practice, in a specific condition or population. Itis not sufficient, nor appropriate, to rely on either aspectalone as the sole method of assessment of the effectivenessof naturopathic medicine.
Context of EBM
The EBM movement began in conventional medicine dueto a concern that clinical decision-making was not evidencebased.56 The scope of conventional medicine is so large thatcharting the extent of its total evidence at any given point intime is problematic. In 2007, BMJ Clinical Evidence re-viewed 2500 treatments supported by good evidence. It
WHOLE-SYSTEM MULTI-MODALITY NATUROPATHIC MEDICINE: A SCOPING REVIEW 165

rated 15% of treatments as beneficial, 22% as likely to bebeneficial, 7% as partly beneficial and partly harmful, 5%unlikely to be beneficial, and 4% likely to be ineffective orharmful. For the remaining 47%, the effect of treatment wasrated as currently not demonstrated.57 If this review wasundertaken today, these numbers would differ; however, it isimportant to recognize from these figures that conventionalmedicine, like all fields in health care, has extensive work todo regarding the evidence on which practice is based.
In contrast to classical RCTs which have dominated EBMand which utilize a reductionist approach that fails to rec-ognize the complexities of real-world clinical practice,2 theresearch outlined in this scoping review is pragmatic innature and sets out to determine the effectiveness of awhole-system approach in real-world clinical practice.
Limitations
There are several limitations inherent in grouping such asa broad range of heterogeneous studies. No specific analysisof the effectiveness of naturopathic treatment was con-ducted, due to the breadth of study types, outcomes as-sessed, treatment settings, and modalities used. The mostrobust studies reported results in comparison with usualcare; however, comparative controls were used in only 4 of12 prospective studies18,22,33,43 and in one of eight retro-spective studies.25 In addition, there is a high risk of re-porting and selection bias in many of the observationalstudies (i.e., criteria such as multiple return visits to natu-ropathic centers for patient inclusion in the dataset).
The types of modalities used and the intensity of treatmentsare highly variable across the studies reported here. It is notpossible to compare outcomes for intensive inpatient treatmentwith several visits spaced over 6 months in a community set-ting. As such, the aim of this scoping report was not to com-pare the effectiveness of the research, but to show the breadthof the research into whole-system naturopathic medicine.
There is little distinction between some included studieswhere ‘‘integrative medicine’’ is applied and some of theexcluded studies using integrative medicine. The acceptancecriterion was that treatments were administered by a self-identified naturopath, as opposed to a conventional doctor ornurse; however, the authors recognize that some studies ofintegrated hospital care might not represent naturopathicmedicine as clearly as studies that have naturopathic-onlytreatment. Also some studies of treatment provided by natu-ropaths might have been overlooked if this was not specifiedin the text. In addition, inclusion criteria for non-Englishlanguage articles might have precluded relevant studies.
The decision to limit inclusion of case series to those withfive or more cases was arbitrary and might have excludedsome studies. Although seven was the median number ofcases included in articles with titles specifying ‘‘case series,’’the number of cases included is not a differentiating charac-teristic.58 The decision was taken to ensure that any inferenceabout clinical practice was based on multiple observations.
The majority of studies assessed were positive, whichcarries a specific concern regarding publication bias (thepossibility that negative studies might have been under-taken, but not reported). This is known to be true in phar-maceutic research,59 but currently difficult to assess innaturopathic medicine.
Conclusions and Future Directions
The global naturopathic research landscape contains asmall, but expanding body of practice-based, whole-system,multi-modality research. To date, research with higher meth-odological quality shows that whole-system multi-modalitynaturopathic medicine is effective for treating a range of con-ditions, including cardiovascular disorders, musculoskeletalpain, type 2 diabetes, PCOS, depression, and anxiety. Researchwith lower methodological quality also suggests that naturo-pathic medicine is effective for treating chronic pain, hepatitis C,menopausal symptoms, bipolar disorder, and asthma and in in-creasing cancer survival time. Results were positive across worldregions for similar conditions, which are likely to reflect theglobal consistency in applying the core concepts of naturopathicpractice utilizing the common set of naturopathic modalities.
Although there is a vast array of clinical trial evidencesupporting the tools of trade used in naturopathic medicine(dietary and lifestyle interventions and specific botanicalmedicines and nutritional supplements), there is a distinctlack of well-conducted pragmatic trials evaluating the complexintervention of whole-system, multi-modality naturopathiccare. Until substantively more whole-system research is un-dertaken, evaluating the effectiveness of naturopathic medi-cine requires a combination of both these types of evidence.
There is a need for pragmatic, real-world trials in whichcomplex naturopathic treatment is compared with usual careto build a high-quality evidence base on the effectiveness ofwhole-system, multi-modality naturopathic practice. Thisneed has recently led to development of a research con-sortium of naturopathic academic clinics in four countriesand across multiple world regions to develop robust, inter-national, multicenter collaboration.60 This consortium hasbeen endorsed by the World Naturopathic Federation, withthe goal to significantly increase the amount and quality ofglobal naturopathic whole-system research.
Author Disclosure Statement
No competing financial interests exist.
References
1. Myers SP, Hunter A, Snider P, Zeff J. Naturopathic Med-icine. In: Robson T, ed. Introduction to ComplementaryMedicine. Sydney: Allan and Unwin, 2003.
2. Wardle J, Oberg EB. The intersecting paradigms of natu-ropathic medicine and public health: Opportunities fornaturopathic medicine. J Altern Complement Med 2011;17:1079–1084.
3. World Health Organisation. WHO Traditional MedicineStrategy 2014–2023. World Health Organization, Geneva,Switzerland 2013.
4. Margolis SA, Russell B. Evidence based medicine.Evidence-Based Medicine Editorial 2018;47:6.
5. Lin V, Bensoussan A, Myers S, et al. The Practice andRegulatory Requirements of Naturopathy and WesternHerbal Medicine. Melbourne: School of Public Health,Latrobe University; 2005.
6. Jagtenberg T, Evans S, Grant A, et al. Evidence-basedmedicine and naturopathy. J Altern Complement Med2006;12:323–328.
7. Ooi SL, Rae J, Pak SC. Implementation of evidence-basedpractice: A naturopath perspective. Complement Ther ClinPract 2016;22:24–28.
166 MYERS AND VIGAR

8. Standish LJ, Calabrese C, Snider P. The naturopathicmedical research agenda: The future and foundation ofnaturopathic medical science. J Altern Complement Med2006;12:341–345.
9. Oberg E, Bradley R, Cooley K, et al. Estimated effects ofwhole-system naturopathic medicine in select chronic dis-ease conditions: A systematic review. Altern Integr Med2015;4:192.
10. Levac D, Colquhoun H, O’Brien KK. Scoping studies:Advancing the methodology. Implement Sci 2010;5:69.
11. Baggoley C. Review of the Australian Government Rebateon Natural Therapies for Private Health Insurance. Aus-tralia Government Department of Health, Australia, 2017.
12. Higgins JPT, Altman DG, Gøtzsche PC, et al. The Co-chrane Collaboration’s tool for assessing risk of bias inrandomised trials. BMJ 2011;343:d5928.
13. Nandakumar B, Kadam A, Srikanth H, Rao R. P02.50.Naturopathy and yoga based life style intervention forcardiovascular risk reduction in patients with cardiovascu-lar risk factors: A pilot study. BMC Complement AlternMed 2012;12(Suppl 1):1–1.
14. Stange R, Hackermeier U, Franzen G, et al. P02.172. 1-yearsustaining efficacy of multidimensional therapy for inpa-tients with different conditions of chronic musculoskeletalpain. BMC Complement Altern Med 2012;12(Suppl 1):P228–P228.
15. Breed C, Bereznay C. Treatment of Depression and Anxietyby Naturopathic Physicians: An Observational Study of Nat-uropathic Medicine Within an Integrated MultidisciplinaryCommunity Health Center. J Altern Complement Med 2017;23:348–354.
16. Gurevich MI, Robinson CL. Medication-free Alternativesfor Long-term Maintenance of Bipolar Disorder: A CaseSeries. Glob Adv Health Med 2015;4:53–60.
17. Ritenbaugh C, Hammerschlag R, Calabrese C, et al. A pilotwhole systems clinical trial of traditional Chinese medicine andnaturopathic medicine for the treatment of temporomandibu-lar disorders. J Altern Complement Med 2008;14:475–487.
18. Secor ER, Markow MJ, Mackenzie J, Thrall RS. Im-plementation of outcome measures in a complementary andalternative medicine clinic: Evidence of decreased pain andimproved quality of life. J Altern Complement Med (NewYork, N.Y.) 2004;10:506–513.
19. Shinto L, Calabrese C, Morris C, et al. A randomized pilotstudy of naturopathic medicine in multiple sclerosis. J Al-tern Complement Med 2008;14:489–496.
20. Bradley R, Kozura E, Buckle H, et al. Description ofclinical risk factor changes during naturopathic care fortype 2 diabetes. J Altern Complement Med (New York,N.Y.) 2009;15:633–638.
21. Bradley R, Oberg EB. Naturopathic Medicine and Type 2Diabetes: A Retrospective Analysis from an AcademicClinic. Altern Med Rev 2006;11:30.
22. Bradley R, Sherman KJ, Catz S, et al. Adjunctive naturo-pathic care for type 2 diabetes: Patient-reported and clinicaloutcomes after one year. BMC Complement Altern Med2012;12:44–44.
23. Bradley R, Kozura E, Kaltunas J, et al. Observed Changesin Risk during Naturopathic Treatment of Hypertension.Evid Based Complement Altern Med 2011;2011:826751–826751.
24. Milliman WB, Lamson DW, Brignall MS. Hepatitis C; aretrospective study, literature review, and naturopathicprotocol. Altern Med Rev 2000;5:355–371.
25. Cramer EH, Jones P, Keenan NL, Thompson BL. Is natu-ropathy as effective as conventional therapy for treatmentof menopausal symptoms? J Altern Complement Med(New York, N.Y.) 2003;9:529–538.
26. Szczurko O, Cooley K, Busse JW, et al. Naturopathic carefor chronic low back pain: A randomized trial. PLoS One2007;2:e919–e919.
27. Szczurko O, Cooley K, Mills EJ, et al. Naturopathictreatment of rotator cuff tendinitis among Canadian postalworkers: A randomized controlled trial. Arthritis Rheum2009;61:1037–1045.
28. Cooley K, Szczurko O, Perri D, et al. Naturopathic care foranxiety: A randomized controlled trial ISRCTN78958974.PLoS One 2009;4 (no pagination)(e6628).
29. Seely D, Szczurko O, Cooley K, et al. Naturopathic med-icine for the prevention of cardiovascular disease: A ran-domized clinical trial. CMAJ 2013;185:E409–E416.
30. Beer AM, Ostermann T, Matthiessen PF. Evaluation of in-hospital treatment with naturopathic methods — The‘blankenstein model’. Part I: Patients and therapeutic con-cepts. Forsch Komplementarmed Klass Naturheilkd 2001;8:6–13.
31. Teut M, Schnabel K, Baur R, et al. Effects and feasibility ofan Integrative Medicine program for geriatric patients-Acluster-randomized pilot study. Clin Interv Aging 2013;8:953–961.
32. Weidenhammer W, Wessel A, Melchart D. Quality profileof a CAM rehabilitation clinic — Part 2: Patients andoutcome profile. Forsch Komplementarmed 2007;14:335–345.
33. Wiebelitz KR, Teske W, Henke T, et al. [Naturopathic andorthopaedic in-patient treatment of chronic back pain—acomparison study]. [German]. MMW Fortschr Med 2011;153 Suppl 2:47–55.
34. Ostermann T, Beer AM, Matthiessen PF. Evaluation ofinpatient naturopathic treatment - The Blankenstein model.Part II: Effect size and health status of patients in the courseof time. Forsch Komplementarmed Klass Naturheilkd2002;9:269–276.
35. Beer AM, Ostermann T, Matthiessen PF. Changed qualityof life by in-patient naturopathic treatment results of the‘‘Blankenstein Model’’. [German]. Gesundheitswesen2001;63:242–247.
36. Bairy S, Kumar AMV, Raju M, et al. Is adjunctive natu-ropathy associated with improved glycaemic control and areduction in need for medications among type 2 Diabetespatients? A prospective cohort study from India. BMCComplement Altern Med 2016;16:290–290.
37. Edla SR, Kumar AMV, Srinivas B, et al. ’Integrated Nat-uropathy and Yoga’ reduces blood pressure and the needfor medications among a cohort of hypertensive patients inSouth India: 3-months follow-up study. Adv Integr Med2016;3:90–97.
38. Murthy SN, Rao NSN, Nandkumar B, Kadam A. Roleof naturopathy and yoga treatment in the managementof hypertension. Complement Ther Clin Pract 2011;17:9–12.
39. Rao Y, Kadam A, Jagannathan A, et al. Efficacy of natu-ropathy and yoga in bronchial asthma. Indian J PhysiolPharmacol 2014;58:232–238.
40. Sathyaprabha TN, Murthy H, Murthy BTC. Efficacy ofnaturopathy and yoga in bronchial asthma—A self con-trolled matched scientific study. Indian J Physiol Pharmacol2001;45:80–86.
WHOLE-SYSTEM MULTI-MODALITY NATUROPATHIC MEDICINE: A SCOPING REVIEW 167

41. Pradeep N, Mohanty S, Hyndavi S. Evidence for naturo-pathic and yogic interventions to augment the effects of artcare as an adjuvant therapy—A parallel matched controlstudy. Int J Clin Biomed Res 2016;2:19–23.
42. Sarris J, Gadsden S, Schweitzer I. Naturopathic medicinefor treating self-reported depression and anxiety: An ob-servational pilot study of naturalistic practice. Adv IntegrMed 2014;1:87–92.
43. Braun L, Stanguts C, Spitzer O, et al. A wellness programfor cardiac surgery improves clinical outcomes. Adv IntegrMed 2014;1:32–37.
44. Arentz S, Smith CA, Abbott J, et al. Combined Lifestyleand Herbal Medicine in Overweight Women with Poly-cystic Ovary Syndrome (PCOS): A randomized controlledtrial. Phytother Res 2017;31:1330–1340.
45. Isbell B, Carroll S. Clinical outcome research at the Uni-versity of Westminster Polyclinic. Br Naturopathic J 2007;24:10.
46. Niwa Y, Matsuura H, Murakami M, et al. Evidence thatnaturopathic therapy including Cordyceps sinensis prolongssurvival of patients with hepatocellular carcinoma. IntegrCancer Ther 2013;12:50–68.
47. Gagnier JJ, Moher D, Boon H, et al. Investigating clinicalheterogeneity in systematic reviews: A methodologic re-view of guidance in the literature. BMC Med Res Methodol2012;12:111.
48. World Naturopathic Federation. World Naturopathic Fed-eration: About Naturopathy. 2018. Online document at:http://worldnaturopathicfederation.org/about-naturopathy,accessed July 17, 2018.
49. Beer AM, Uehleke B, Wiebelitz KR. The history of inpa-tient care in German departments focussing on naturalhealing. Evid Based Complement Altern Med 2013;2013:521879.
50. Nair PM, Nanda A. Naturopathic medicine in India. FocusAltern Complement Ther 2014;19:140–147.
51. Hausser T. Update on Naturopathy in Europe: From itsroots to global modern practice. Naturopathic Doctor NewsRev 2018;14:15–16.
52. Ostermann T, Beer AM, Langhorst J. The effect of in-tegrative in-patient treatment on patients’ quality of life:A meta-analysis. J Altern Complement Med 2013;20:A115.
53. Romeyke T, Stummer H. A study of costs and length ofstay of inpatient naturopathy—Evidence from Germany.Complement Ther Clin Pract 2011;17:90–95.
54. Loyd I, Hausser T, Wardle J, et al. World NaturopathicFederation Report: Findings from the 1st World Naturo-pathic Federation survey. Toronto, World NaturopathicFederation, 2015.
55. Hausser T, Loyd I, Yanez J, et al. WNF Naturopathic RootsReport. Toronto, World Naturopathic Federation, 2016.
56. Sur RL, Dahm P. History of evidence-based medicine. In-dian J Urol 2011;27:487.
57. Garrow JS. How much of orthodox medicine is evidencebased? Br Med J 2007;335:951.
58. Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodo-logical quality and synthesis of case series and case reports.BMJ Evid Based Med 2018;23:60–63.
59. Dwan K, Gamble C, Williamson PR, et al. Systematic re-view of the empirical evidence of study publication biasand outcome reporting bias—an updated review. PLoS One2013;8:e66844.
60. Steel A, Goldenberg J, Cooley K. Establishing an interna-tional research collaborative for naturopathy: The Interna-tional Research Consortium of Naturopathic AcademicClinics (IRCNAC). Adv Integr Med 2017;4:93–97.
Address correspondence to:Stephen P. Myers, BNat (Hons)
National Centre for Naturopathic MedicineSouthern Cross University
Lismore 2480Australia
E-mail: [email protected]
168 MYERS AND VIGAR