Embed Size (px)
Citation preview

MusculoskeletalCurriculum
History & Exam of the Injured
Knee

2
Goal
Learn a standardized, evidence-based history and physical examination of patients with knee injuries
WHICH WILL:
Enable family medicine resident physicians to accurately diagnose common knee problems throughout the full age spectrum of patients seen in family medicine

3
Competency-Based Objectives Patient care – focused history and exam
Professionalism – respect, compassion
Interpersonal and communication skills – differential diagnosis
Medical knowledge base – anatomy, injury mechanisms
Systems based practice – accuracy, time-efficiency

4
Assessing a knee injury
Components of the assessment include Focused history Attentive physical examination Thoughtfully ordered tests/studies (for future
discussion)

Focused History

6
Focused History Questions
Onset of Pain Date of injury Character/nature of pain
Location of pain* Anterior Medial Lateral Posterior

7
Focused History Questions2
Mechanism of Injury – helps predict injured structure
Contact or noncontact injury?*
If contact, what part of the knee was contacted? Anterior blow? Valgus force? Varus force?
Was foot of affected knee planted on the ground?**
Valgus alignment = distal segment deviates lateral with respect to proximal segment. Patellas Touch
http://moon.ouhsc.edu/dthompso/namics/varus.gif

8
Focused History Questions3
Injury-Associated Events Pop heard or felt?
Swelling after injury (immediate vs delayed)
Catching / Locking
Buckling / Instability (“giving way”)
9
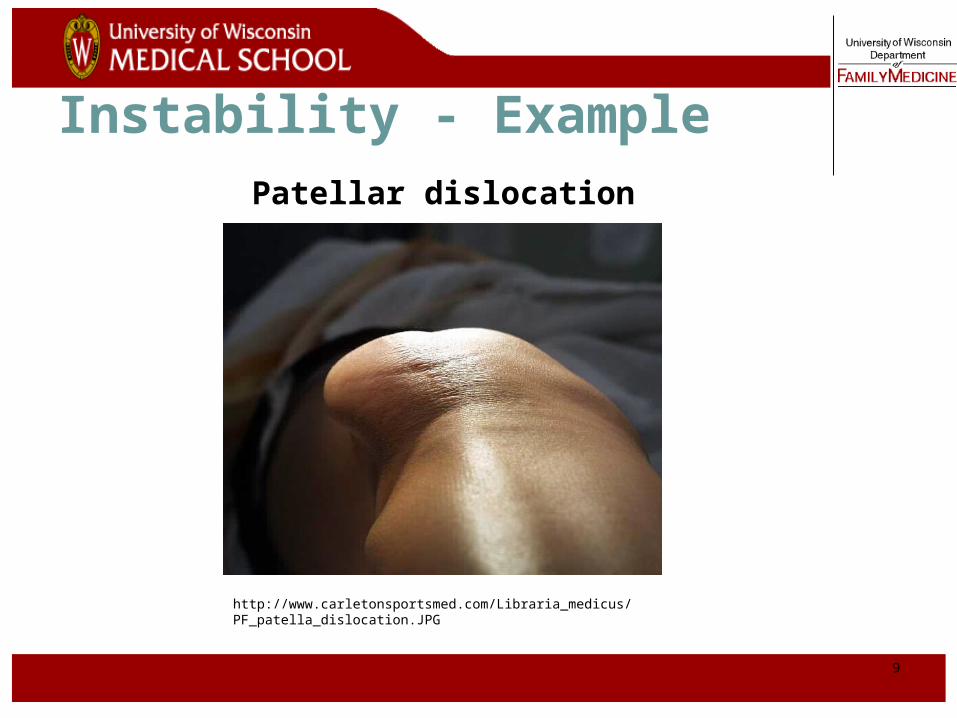
Instability - Example
http://www.carletonsportsmed.com/Libraria_medicus/PF_patella_dislocation.JPG
Patellar dislocation

10
Focused History Questions4
Degree of Immediate Dysfunction
|------------------------|Unable to Antalgic Continued
Ambulate Gait* to Participate
History of Prior Knee Injuries or Surgeries

11
Historical Clues to Knee Injury DiagnosisNoncontact injury with “pop” ACL tear
Contact injury with “pop” MCL or LCL tear, meniscus tear, fracture
Acute swelling ACL tear, fracture, knee dislocation
Lateral blow to the knee MCL tear
Medial blow to the knee LCL tear
Knee “gave out” or “buckled” ACL tear, patellar dislocation
Fall onto a flexed knee PCL tear

Physical Exam
13
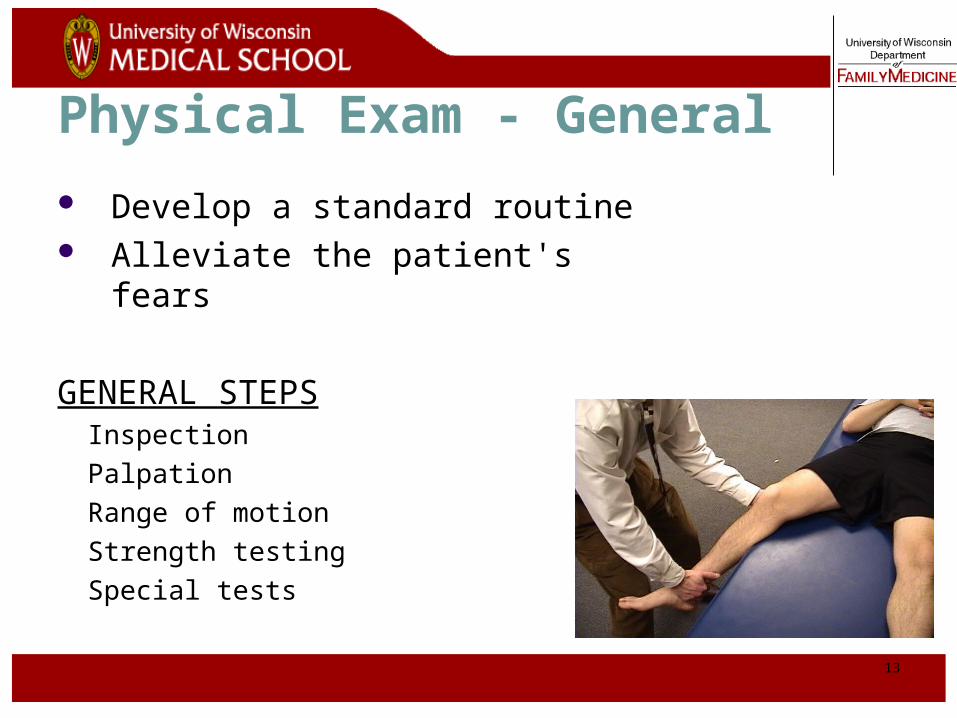
Physical Exam - General
Develop a standard routine Alleviate the patient's fears
GENERAL STEPSInspection
Palpation
Range of motion
Strength testing
Special tests

14
Physical Exam - Exposure
Adequate exposure - groin to toes bilaterally
Examine in supine position Compare knees

15
Observe – Static Alignment Patient stands facing examiner with
feet shoulder width apart Ankles, subtalar joints – pronation, supination Feet – pes planus, pes cavus
(http://www.steenwyk.com/pronsup.htm)
Pes planus Pes cavus
(http://www.arc.org.uk/about_arth/booklets/6012/images/6012_1.gif)

16
Patient then brings medial aspects of knees and ankles in contact Knees – genu valgum
(I), genu varum (II)
Observe – Static Alignment
(http://www.orthoseek.com/articles/img/bowl1.gif)
Genu valgum Genu varum

17
Observe – Dynamic Alignment
Pronation/Supination may be enhanced with ambulation
Antalgic gait indicates significant problem (anti = against, algic = pain)

18
Inspect Knee
Warmth Erythema Effusion*
Evidence of local traumaAbrasionsContusionsLacerations
Patella positionMuscle atrophy

19
Inspect Knee-Related Muscles
Quadriceps atrophy Long-standing problem
Vastus medialis atrophy
After surgery
http://www.neuro.wustl.edu/neuromuscular/pics/people/patients/Hands/ibmquadatrsm.jpg

20
Normal Knee – Anterior, Extended

21
Surface Anatomy - Anterior, Extended
Patella
Hollow
Indented
22
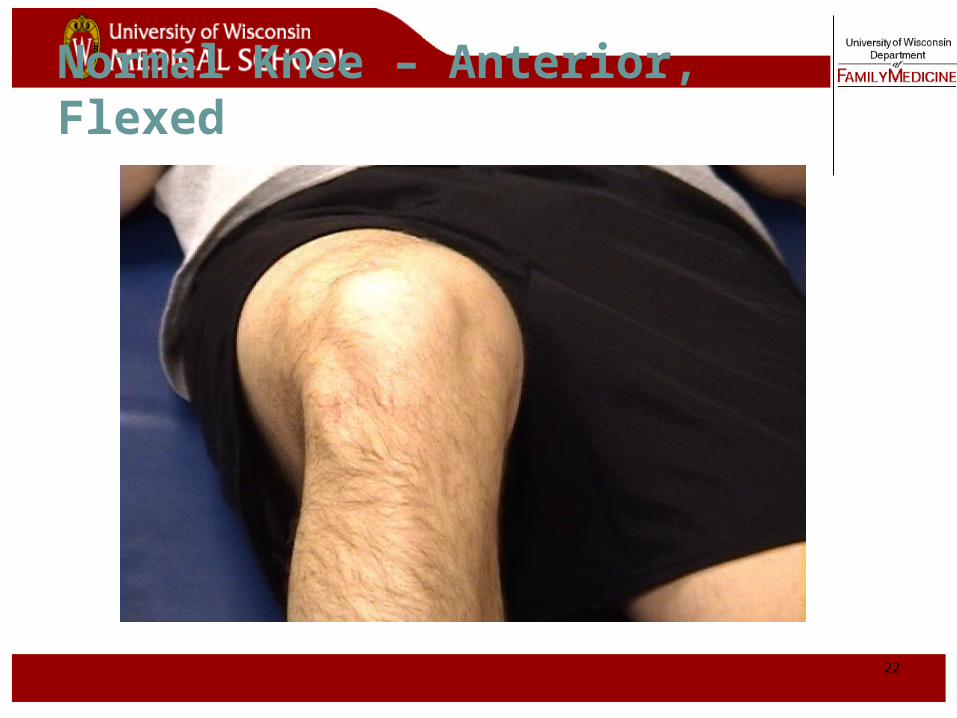
Normal Knee – Anterior, Flexed

23
Surface Anatomy - Anterior, Flexed
Head OfFibula
Patella
TibialTuberosity

24
Palpation – Anterior*Patella:
Lateral and Medial Patellar Facets
Superior AndInferior Patellar Facets
Patellar Tendon**
Lateral Fat PadMedial Fat Pat

25
Surface Anatomy - Medial
Medial FemoralCondyle
Patella
JointLine
MedialTibial Condyle
TibialTuberosity
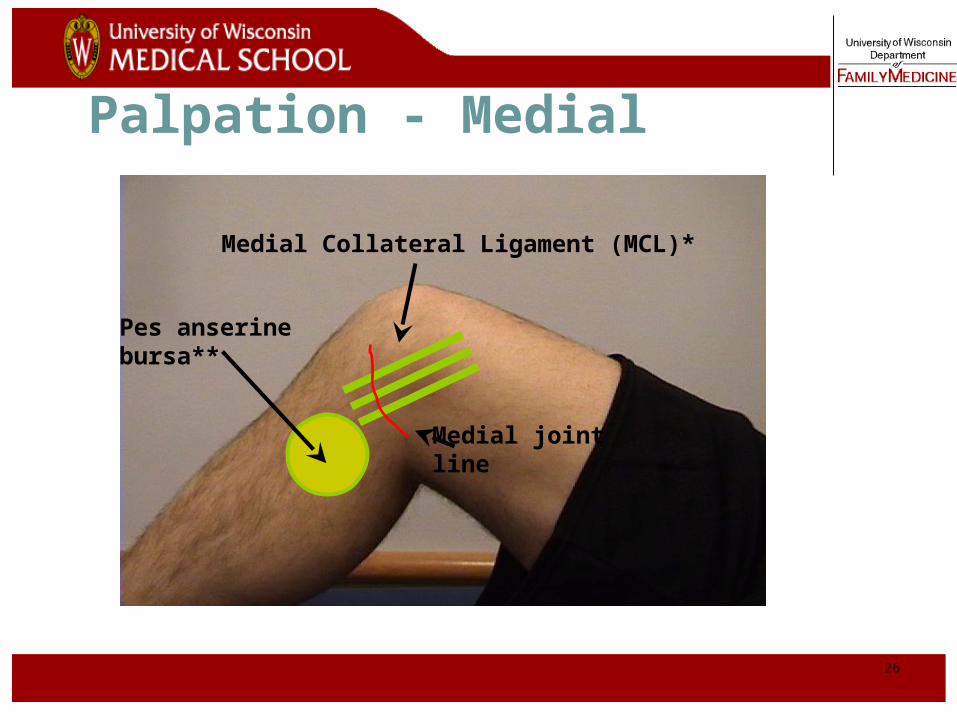
26
Palpation - Medial
Medial Collateral Ligament (MCL)*
Pes anserine bursa**
Medial joint line

27
Surface Anatomy – Lateral
Patella
Head OfFibula
TibialTuberosity
Quadriceps

28
Palpation – Lateral*
Lateral joint line
Lateral Collateral Ligament (LCL)**

29
Palpation - Posterior
Popliteal fossa
Abnormal bulges Popliteal artery aneurysm Popliteal thrombophlebitis Baker’s cyst
30
Range Of Motion Testing Extension Flexion
0º 135º
Describe loss of degrees of extension Example: “lacks 5 degrees of
extension,” or “extension = minus 5 degrees”
Locking* = patient unable to fully extend or flex knee
due to a mechanical blockage in the knee (i.e., loose body, bucket-handle meniscus tear)

31
Special Tests – Anterior Knee Pain
Patellar apprehension test*
Patellofemoral grind test**

32
Special Tests - Ligaments
Assess stability of 4 knee ligaments via applied stresses*
Anterior CruciatePosteriorCruciate
Lateral Collateral
Medial Collateral

33
Stress Testing of Ligaments2
Use a standard exam routine Direct, gentle pressure No sudden forces
Abnormal test 1. Excessive motion = laxity
What is NORMAL motion?*
2. Soft/mushy end point**

34
Collateral Ligament Assessment
Patient and Examiner Position*

35
Valgus Stress Test for MCL*
Note Direction Of Forces

36
Video of Valgus Stress Test
Click on image for video

37
Varus Stress Test for LCL*
Note direction of forces

38
Video of Varus Stress Test
Click on image for video

39
Lachman’s Test* Patient Position Physician hand placement

40
Lachman’s Test2
View from lateral aspect*
Note direction of forces

41
Video of Lachman’s Test
Click on image for video

42
Alternate Lachman’s Test
Click on image for video

43
Anterior Drawer Test for ACL
Physician Position & Movements* Patient Position
Note direction of forces

44
Posterior Drawer Testing- PCL*
Note direction of forces

45
Assess Meniscus – Knee Flexion
Most sensitive test is full flexion* Examiner passively flexes the knee or has patient
perform a full two-legged squat to test for meniscal injury
Joint line tenderness** Flexion of the knee enhances palpation of the
anterior half of each meniscus

46
No Evidence to Support
Pivot-Shift* - for ACL tear
McMurray Testing**- for meniscus tears