Embed Size (px)
Citation preview
MUSCULOSKELETAL DISORDERS (MSDS)-CONSEQUENCES OF PROLONGED
STATIC POSTURES
Introduction
The World Health Organization defines MSD as “a
disorder of the muscles, tendons, joints, intervertebral
discs, peripheral nerves and vascular system, not directly
resulting from an acute or instantaneous event but
installing gradually and chronically”.
There are many types of factors responsible for MSD:
occupational factors, medical factors (physical disorders,
genetic predisposition, and age) and life style factors.
Usually two or more factors trigger MSD. Work in
dentistry is characterized by some body postures with
different degrees of distortion. In this case the
professional factors are represented by: prolonged static
postures, repetitive movements, inadequate lighting, the
excessive exertion of the small muscles, and the
instrument tight grip, raised arms, static exertion of the
muscles on long term, vibrations.
Working tasks in dentistry have an intellectual and a
physical component - the result of the muscular effort.
The muscular effort can be either static – the length of the
167
Journal of Experimental Medical & Surgical Research
Cercetãri Experimentale & Medico-Chirurgicale
Year XIV · Nr.4/2007 · Pag.167-172C e r c e t a r ie x p e r i m e n ta le &
m edico-chirurgicale
)
1 - UMF”Victor Babeº” Timiºoara, University of Dentistry, Department of Oral-Dental Diagnosis.2 - UPTimiºoara, Faculty of Mechanics.
3 - UMF”Victor Babeº” Timiºoara, Department of Medical Informatics
SUMMARY:Musculoskeletal disorders (MSDs) are progressively installed. In dentistry prolonged staticpostures, repetitive movements, excessive contraction of short muscles could causemusculoskeletal disorders. Even when the sitting posture is the one recommended by ISO11226 – Ergonomics-Evaluation of static working postures, there is a high risk of developing musculoskeletal disorders. Each member of the dental team is predisposed to pain or injuryin different areas of the body, depending on their tasks and position in relation to the patient. This presentation shows the causes and the mechanisms that lead to musculoskeletaldisorders and some methods for prevention.
Key Words: dentists, musculoskeletal disorders, static working postures
AFECTIUNI MUSCULO-SCHELETALE – CONSECINTE ALE POSTURII ORTOSTATICEPRELUNGITE
REZUMAT:Afectiunile musculo-scheletale se instaleaza progresiv. In stomatologie cele mai frecventecauze sunt reprezentate de posturi statice prelungite, miscari repetitive, folosirea in exces amuschilor scurti. Chiar daca pozitia sezanda este cea recomandata de ISO 11226 –Evaluarea ergonomica a pozitiilor statice de munca, exista un risc crescut de aparitie aacestor afectiuni. Fiecare membru al echipelor stomatologice este predispus la dureri sileziuni in diferite zone ale corpului in functie de posturile pe care le adopta la locul demunca. Aceasta lucrare prezinta cauzele si mecanismele ce conduc la afectiunilemusculo-scheletale si citeva metode pentru prevenirea lor.
Mirella Anghel1
Veronica Argeºanu2
Cristina Talpoº-Niculescu1
Diana Lungeanu3
Received for publication: 19.07.2007
Revised: 11.09.2007
Correspondence to: Mirella Anghel, e- mail: [email protected]
E x p e r i m e n t a l
M e d i c a l S u r g i c a l
R E S E A R C H
J O U R N A L o f
muscle remains unchanged (isometric contraction) or
dynamic - rhythmic changes of alternations and
shortenings of the muscles (isotonic contraction). The
physical expressions of the muscles are characterized by
gesture - the direct relation between man and working
means by repeated movements and posture – the static
posture.
The posture is the complex term used as reference for
a number of movements and posture concepts. The
posture was defined in various ways: a posture or a body
position, the relative postures of the body parts for a
specific activity.
The static posture implies the followings:
l isometric muscular contractions with acid
lactic accumulation,
l compression of the blood vessels,
l vicious static postures and non physiological
moments: of the spine (resulting in
discopathia) and of the arms (resulting in
tendinitis, epicondylitis).
l repetitive disorders – that have a cumulative
effect, affecting the joints, ligaments and
tendons.
All these factors contribute to the occurrence of MSDs
and affect the personnel involved in static activities
(dentists, PC operators, tailors). Pain, fatigue and
disorders of the musculoskeletal system may result from
sustained inadequate working postures and poor
working conditions. Musculoskeletal pain and fatigue
may influence posture control which can increase the
risk of errors and may result in low work efficiency. Good
ergonomic design of the workplace is a basic
requirement for improving musculoskeletal health.
Working posture in the dental surgery
Despite that since 1958 (as the result of the study
“Time and Motion”) the sitting postures have been
recommended as the healthiest and the most correct
ones, the findings of a research done in Timisoara proved
that more than 50% of the dentists that are over 45 work
in dental surgery in orthostatic postures, while those
168
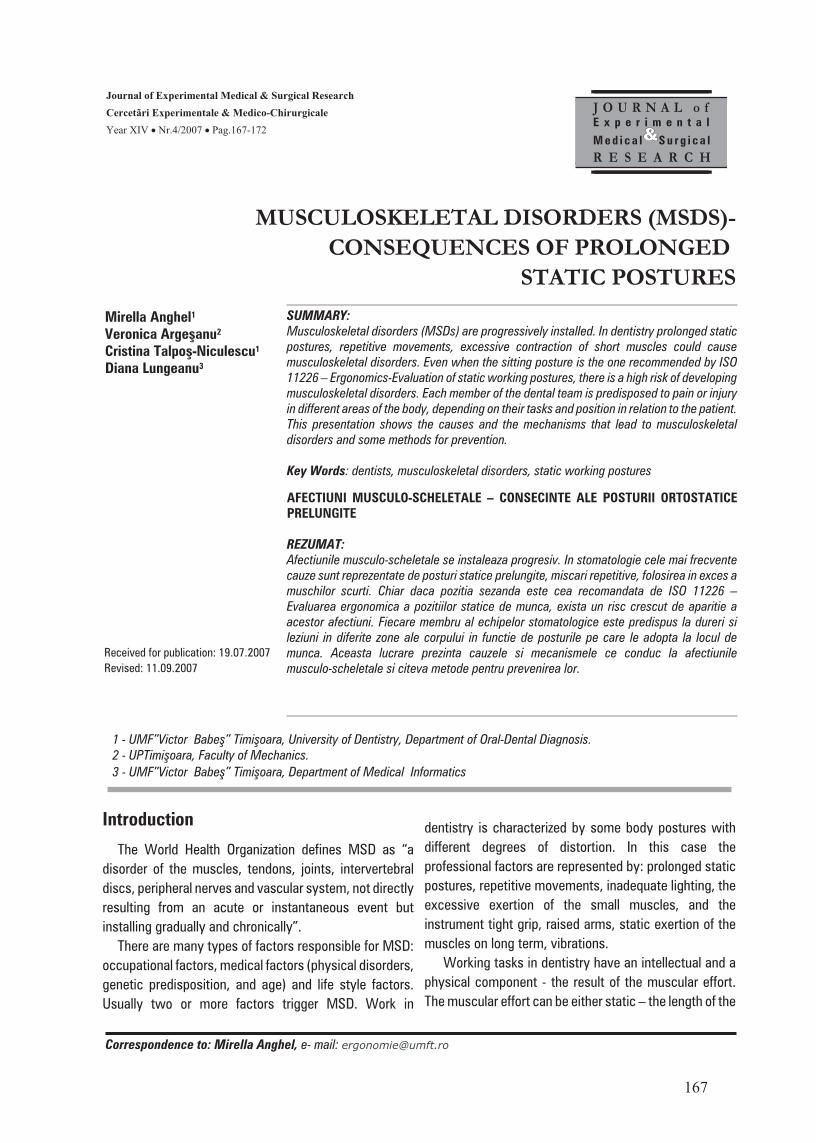
Fig.1 Sample
Fig. 2 Orthostatic posture
aged between 24 and 35 exclusively prefer the sitting
postures. The aim of the survey, performed with the help
of Medical Informatics, is to show to what extent the
dentists’ working manner (posture, habits, schedule etc)
affects their health. 70 dentists were selected (figure1)
out of 850, women and men and all age categories
(between 24 and 75 years old). Most of them had a
upright working posture and those adopting sitting
postures chose wrong, incorrect postures. A
questionnaire with several topics was filled in and the
data analysis used SPSS v. 13. The results proved that
60% of the dentists worked in orthostatic position.
Orthostatics. Although there is manual work that can
be performed only in orthostatic posture (the
determination of occlusion, some extractions), but still
the inconveniences of this posture should be mentioned
(fig.2):
- it is more tiring due to a heavier blood flow
- the body weight is distributed on a smaller surface,
fact that negatively influences the equilibrium,
- when the pedal is used, the support is only on one
leg,
- movements accuracy is diminished.
The effects of a prolonged orthostatic posture upon
health are the followings:
169
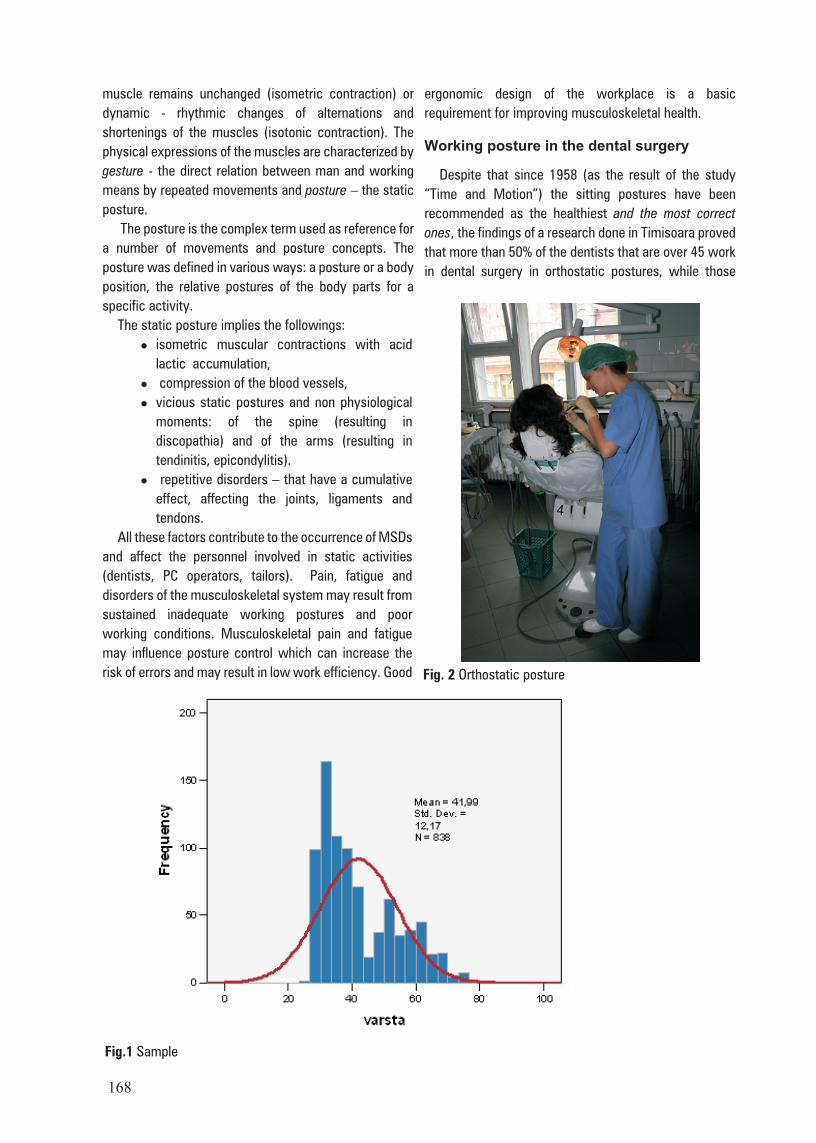
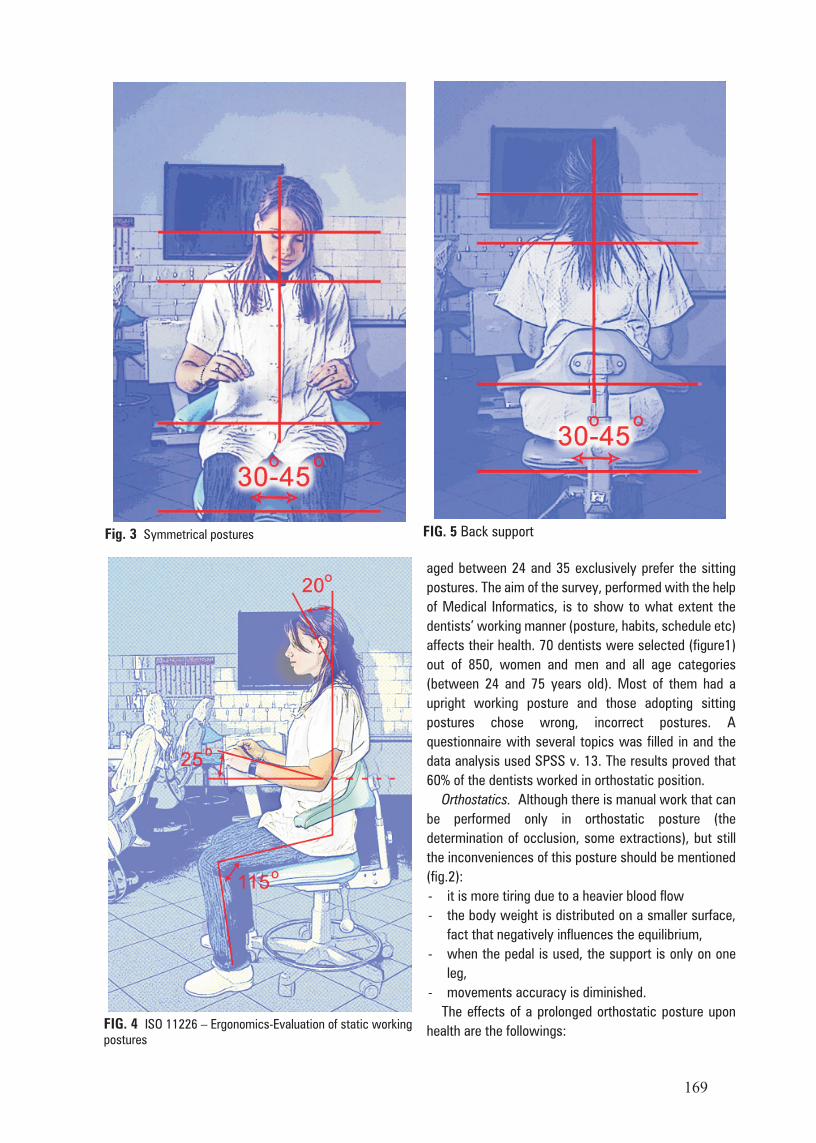
Fig. 3 Symmetrical postures
FIG. 4 ISO 11226 – Ergonomics-Evaluation of static workingpostures
FIG. 5 Back support
- the energy consumption is10% higher than in sitting
postures,
- the heart rate gets higher,
- the static effort is higher than sitting effort,
- the osteoarticular system is affected,
- the peripheral venous circulation is affected
- pains in the lower members occur associated with
the feeling of burden and cramps of the calf.
The sitting postures. The correct working postures in
the dental surgery are the sitting postures that conform to
the following requirements:
- symmetrical postures (fig.3),
- all horizontal axes should be parallel,
- the legs should be slightly apart (a 30º-45º angle),
- the shank should be perpendicular on the floor,
- the upper part of the body should be perpendicular on
the chair – forward movements should be made
without curving the spine,
- the head could bend 20º-25º
- the arms should be close to the body
- the forearms should be nearly horizontal (max. 25%
raised)
- the shank / thigh should be at 115º
- the soles should be on the floor (fig.4)
When working in sitting postures a chair is required to
support the seat and back (fig.5). In this situation one
should alternate active and passive sitting postures.
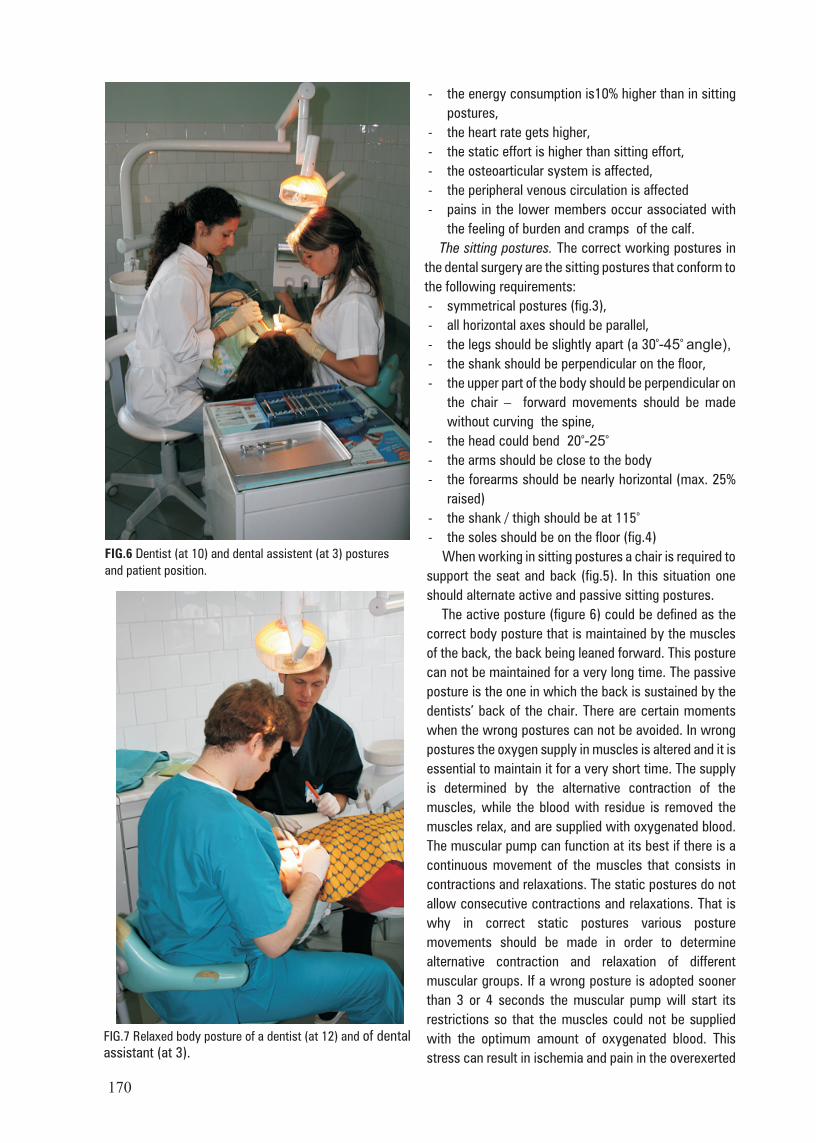
The active posture (figure 6) could be defined as the
correct body posture that is maintained by the muscles
of the back, the back being leaned forward. This posture
can not be maintained for a very long time. The passive
posture is the one in which the back is sustained by the
dentists’ back of the chair. There are certain moments
when the wrong postures can not be avoided. In wrong
postures the oxygen supply in muscles is altered and it is
essential to maintain it for a very short time. The supply
is determined by the alternative contraction of the
muscles, while the blood with residue is removed the
muscles relax, and are supplied with oxygenated blood.
The muscular pump can function at its best if there is a
continuous movement of the muscles that consists in
contractions and relaxations. The static postures do not
allow consecutive contractions and relaxations. That is
why in correct static postures various posture
movements should be made in order to determine
alternative contraction and relaxation of different
muscular groups. If a wrong posture is adopted sooner
than 3 or 4 seconds the muscular pump will start its
restrictions so that the muscles could not be supplied
with the optimum amount of oxygenated blood. This
stress can result in ischemia and pain in the overexerted
170
FIG.6 Dentist (at 10) and dental assistent (at 3) postures
and patient position.
FIG.7 Relaxed body posture of a dentist (at 12) and of dentalassistant (at 3).
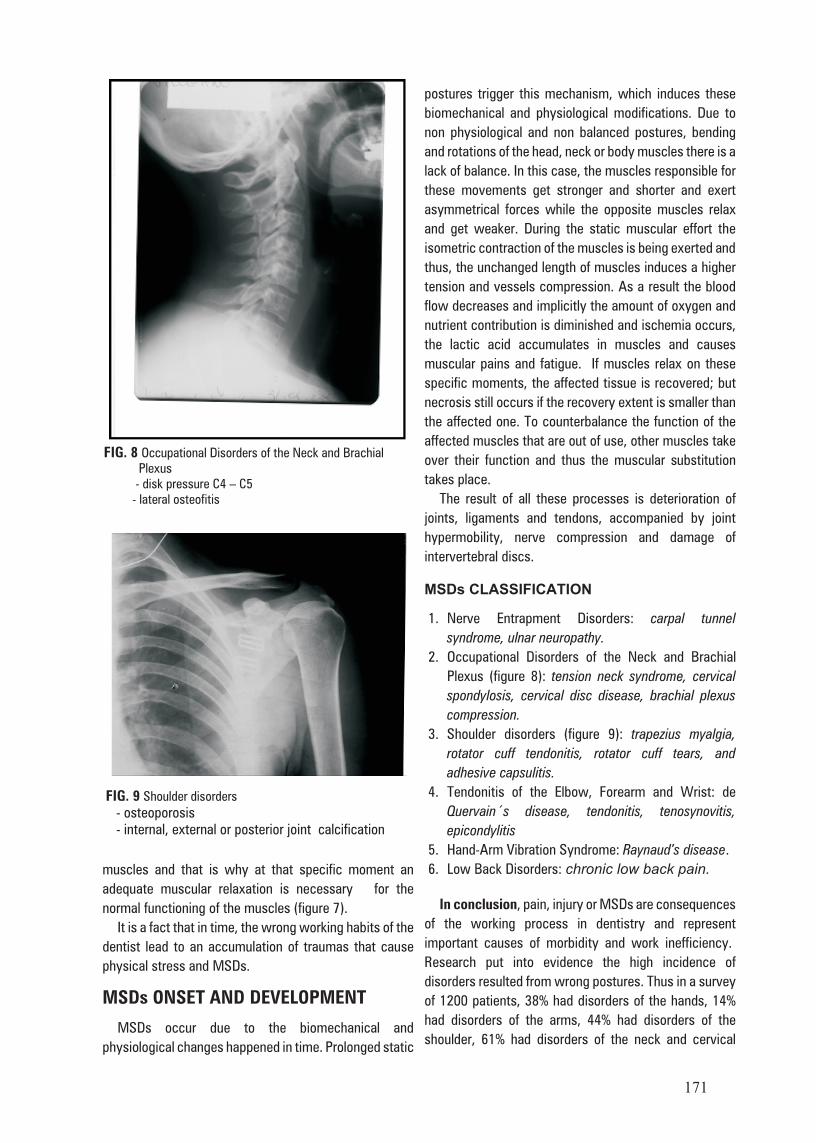
muscles and that is why at that specific moment an
adequate muscular relaxation is necessary for the
normal functioning of the muscles (figure 7).
It is a fact that in time, the wrong working habits of the
dentist lead to an accumulation of traumas that cause
physical stress and MSDs.
MSDs ONSET AND DEVELOPMENT
MSDs occur due to the biomechanical and
physiological changes happened in time. Prolonged static
postures trigger this mechanism, which induces these
biomechanical and physiological modifications. Due to
non physiological and non balanced postures, bending
and rotations of the head, neck or body muscles there is a
lack of balance. In this case, the muscles responsible for
these movements get stronger and shorter and exert
asymmetrical forces while the opposite muscles relax
and get weaker. During the static muscular effort the
isometric contraction of the muscles is being exerted and
thus, the unchanged length of muscles induces a higher
tension and vessels compression. As a result the blood
flow decreases and implicitly the amount of oxygen and
nutrient contribution is diminished and ischemia occurs,
the lactic acid accumulates in muscles and causes
muscular pains and fatigue. If muscles relax on these
specific moments, the affected tissue is recovered; but
necrosis still occurs if the recovery extent is smaller than
the affected one. To counterbalance the function of the
affected muscles that are out of use, other muscles take
over their function and thus the muscular substitution
takes place.
The result of all these processes is deterioration of
joints, ligaments and tendons, accompanied by joint
hypermobility, nerve compression and damage of
intervertebral discs.
MSDs CLASSIFICATION
1. Nerve Entrapment Disorders: carpal tunnel
syndrome, ulnar neuropathy.
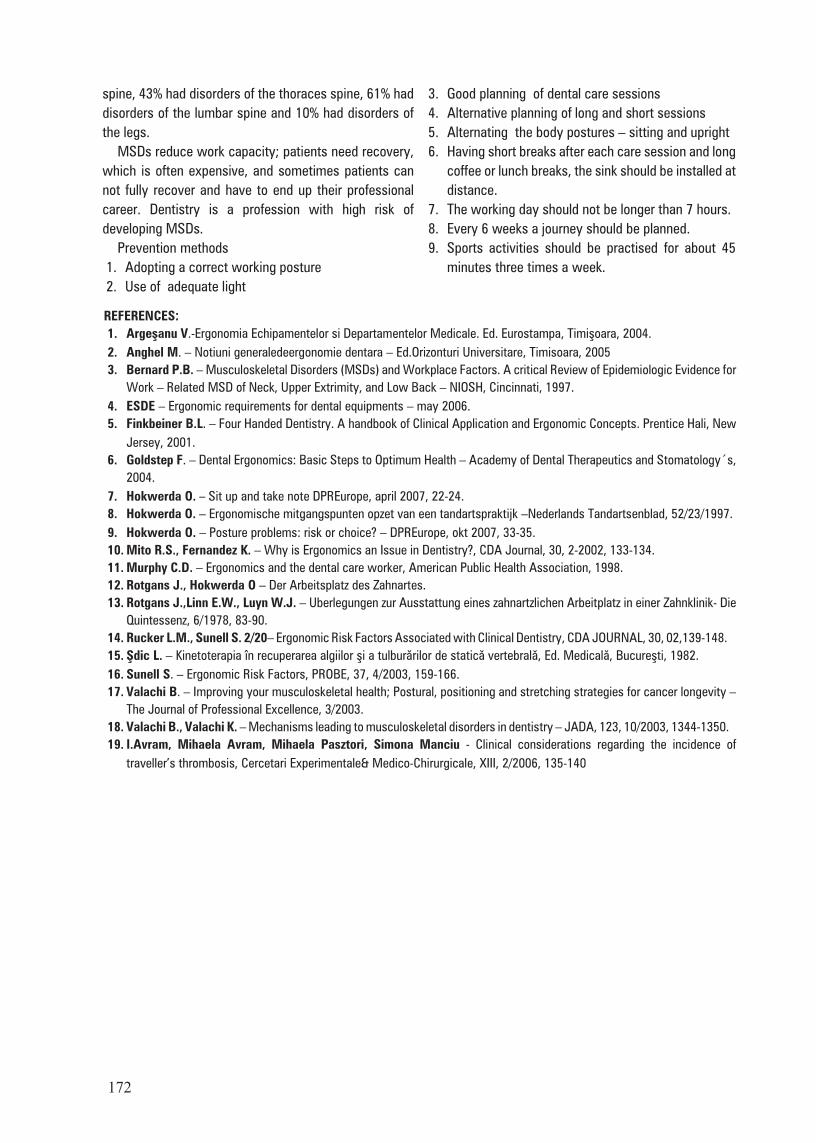
2. Occupational Disorders of the Neck and Brachial
Plexus (figure 8): tension neck syndrome, cervical
spondylosis, cervical disc disease, brachial plexus
compression.
3. Shoulder disorders (figure 9): trapezius myalgia,
rotator cuff tendonitis, rotator cuff tears, and
adhesive capsulitis.
4. Tendonitis of the Elbow, Forearm and Wrist: de
Quervain´s disease, tendonitis, tenosynovitis,
epicondylitis
5. Hand-Arm Vibration Syndrome: Raynaud’s disease.
6. Low Back Disorders: chronic low back pain.
In conclusion, pain, injury or MSDs are consequences
of the working process in dentistry and represent
important causes of morbidity and work inefficiency.
Research put into evidence the high incidence of
disorders resulted from wrong postures. Thus in a survey
of 1200 patients, 38% had disorders of the hands, 14%
had disorders of the arms, 44% had disorders of the
shoulder, 61% had disorders of the neck and cervical
171
FIG. 8 Occupational Disorders of the Neck and Brachial Plexus - disk pressure C4 – C5 - lateral osteofitis
FIG. 9 Shoulder disorders
- osteoporosis - internal, external or posterior joint calcification
spine, 43% had disorders of the thoraces spine, 61% had
disorders of the lumbar spine and 10% had disorders of
the legs.
MSDs reduce work capacity; patients need recovery,
which is often expensive, and sometimes patients can
not fully recover and have to end up their professional
career. Dentistry is a profession with high risk of
developing MSDs.
Prevention methods
1. Adopting a correct working posture
2. Use of adequate light
3. Good planning of dental care sessions
4. Alternative planning of long and short sessions
5. Alternating the body postures – sitting and upright
6. Having short breaks after each care session and long
coffee or lunch breaks, the sink should be installed at
distance.
7. The working day should not be longer than 7 hours.
8. Every 6 weeks a journey should be planned.
9. Sports activities should be practised for about 45
minutes three times a week.
172
REFERENCES:1. Argeºanu V.-Ergonomia Echipamentelor si Departamentelor Medicale. Ed. Eurostampa, Timiºoara, 2004.
2. Anghel M. – Notiuni generaledeergonomie dentara – Ed.Orizonturi Universitare, Timisoara, 2005
3. Bernard P.B. – Musculoskeletal Disorders (MSDs) and Workplace Factors. A critical Review of Epidemiologic Evidence for
Work – Related MSD of Neck, Upper Extrimity, and Low Back – NIOSH, Cincinnati, 1997.
4. ESDE – Ergonomic requirements for dental equipments – may 2006.
5. Finkbeiner B.L. – Four Handed Dentistry. A handbook of Clinical Application and Ergonomic Concepts. Prentice Hali, New
Jersey, 2001.
6. Goldstep F. – Dental Ergonomics: Basic Steps to Optimum Health – Academy of Dental Therapeutics and Stomatology´s,
2004.
7. Hokwerda O. – Sit up and take note DPREurope, april 2007, 22-24.
8. Hokwerda O. – Ergonomische mitgangspunten opzet van een tandartspraktijk –Nederlands Tandartsenblad, 52/23/1997.
9. Hokwerda O. – Posture problems: risk or choice? – DPREurope, okt 2007, 33-35.
10. Mito R.S., Fernandez K. – Why is Ergonomics an Issue in Dentistry?, CDA Journal, 30, 2-2002, 133-134.
11. Murphy C.D. – Ergonomics and the dental care worker, American Public Health Association, 1998.
12. Rotgans J., Hokwerda O – Der Arbeitsplatz des Zahnartes.
13. Rotgans J.,Linn E.W., Luyn W.J. – Uberlegungen zur Ausstattung eines zahnartzlichen Arbeitplatz in einer Zahnklinik- Die
Quintessenz, 6/1978, 83-90.
14. Rucker L.M., Sunell S. 2/20– Ergonomic Risk Factors Associated with Clinical Dentistry, CDA JOURNAL, 30, 02,139-148.
15. ªdic L. – Kinetoterapia în recuperarea algiilor ºi a tulburãrilor de staticã vertebralã, Ed. Medicalã, Bucureºti, 1982.
16. Sunell S. – Ergonomic Risk Factors, PROBE, 37, 4/2003, 159-166.
17. Valachi B. – Improving your musculoskeletal health; Postural, positioning and stretching strategies for cancer longevity –
The Journal of Professional Excellence, 3/2003.
18. Valachi B., Valachi K. – Mechanisms leading to musculoskeletal disorders in dentistry – JADA, 123, 10/2003, 1344-1350.
19. I.Avram, Mihaela Avram, Mihaela Pasztori, Simona Manciu - Clinical considerations regarding the incidence of
traveller’s thrombosis, Cercetari Experimentale& Medico-Chirurgicale, XIII, 2/2006, 135-140