Embed Size (px)
Citation preview
MYCOTIC ENDOPHTHALMITIS IN DRUG ABUSERS
JAMES H. E L L I O T T , M.D., D E N I S M. O ' D A Y , M.D., GARY S. G U T O W , M.D. S T E V E N F. PODGORSKI, M.D., AND PATRICIA AKRABAWI, M.S.
Nashville, Tennesee
Five recent reports have associated mycotic endophthalmitis with intravenous drug abuse. Sugar, Mandell, and Shalev1
reported two cases, one with bilateral involvement. In the first case, definite septate hyphal fragments were identified in the sections of the enucleated eye specimen. Their second patient was an intravenous methylphenidate abuser, who had a chronic progressive bilateral inflammatory process that progressed to retinal detachment in one eye and to phthisis bulbi in both eyes. In this case, a clinical diagnosis was made without any corroborative laboratory studies.
Getnick and Rodriques2 reported a case of unilateral mycotic endophthalmitis in a heroin addict. Smears of a vitreous tap revealed budding yeast forms provisionally identified as a strain of Candida albicans, but all cultures were negative. Treatment of this patient with intravenous amphotericin resulted in vision of finger counting at one foot. Stone, Irvine, and O'Connor3 reported one case with unilateral involvement in a heroin addict who had a positive culture for Candida. Treatment of this patient with intravenous amphotericin and oral flucytosine resulted in vision of light perception only. Snip and Michels4 reported a case diagnosed by pars plana vitrectomy with a culture positive for C. albicans. Treatment with intravenous amphotericin and
From the Department of Ophthalmology, Vander-bilt University School of Medicine, Nashville, Tennessee.
Reprint requests to James H. Elliott, M.D., Professor and Chairman, Department of Ophthalmology, Vanderbilt University School of Medicine, Nashville, TN 37232.
oral flucytosine restored the visual acuity to 6/4.5 (20/15). Vastine and associates5
described four heroin abusers with mycotic endophthalmitis, but did not indicate the treatment used or the visual result.
We describe herein a husband and wife with mycotic endophthalmitis associated with intravenous drug abuse.
C A S E REPORTS
Case 1—A 47-year-old man with no prior history of ocular problems first noted "black spots" in his left eye on Sept. 10, 1975. On previous examination, the visual acuity of the left eye was 6/6 (20/20) with correction. One week later he consulted an ophthalmologist for progressive blurring of vision in the left eye. An exudative lesion was noted in the left retina and vitreous. After two weeks of treatment with topical and systemic corticosteroids without improvement, he was referred here. On ocular examination, the right eye was normal. The vision of the left eye was finger counting at 3 feet. An anterior uveitis with 2+ cells and flare and punctate keratitic precipitates were present. A mild cellular reaction was observed in the vitreous associated with a massive vitreous exudation containing precipitates on the back of a detached posterior hyaloid face. The principal area of involvement was a whitish yellow, 1 x 1-disk diameter preretinal lesion bordering on the optic nerve inferiorly. Streamers of opacities radiated from this lesion in candelabra fashion, dissecting the collagen lamellae of the vitreous (Figs. 1 and 2). A presumptive diagnosis of toxoplas-mic retinochoroiditis was made. Prednisone dosage was increased to 40 mg/day; and 4 g/day of triple sulfa tablets, orally, in divided doses were also given. His clinical course remained essentially unchanged for a two-month period despite continuation of his oral and topical corticosteroids, oral triple sulfa, and the addition of infraorbital corticosteroids, isoniazid, and pyridoxine. At this time the patient admitted that both he and his wife were intravenous abusers of amphetamines.
A clinical diagnosis of presumed Candida endophthalmitis was made, and the patient was admitted to the hospital on Dec. 1, 1975. Laboratory studies before and after hospitalization included: automated multiple-analysis system (SMA-12), complete blood cell count and white blood cell differential count, total eosinophil count, urinalysis, chest
66 AMERICAN JOURNAL OF OPHTHALMOLOGY 88:66-72, 1979
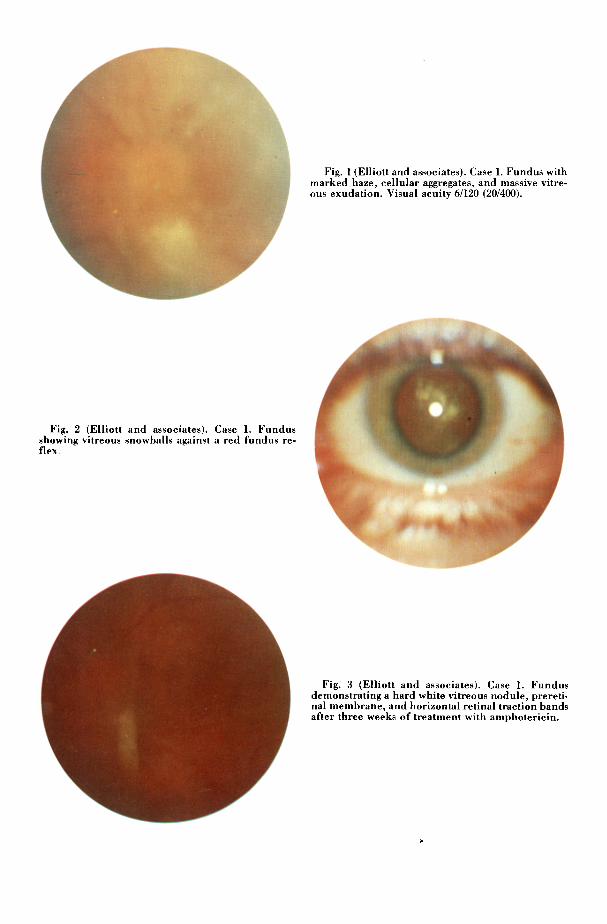
Fig. 1 (Elliott and associates). Case 1. Fundus with marked haze, cellular aggregates, and massive vitreous exudation. Visual acuity 6/120 (20/400).
Fig. 2 (Elliott and associates). Case 1. Fundus showing vitreous snowballs against a red fundus reflex .
Fig. 3 (Elliott and associates). Case 1. Fundus demonstrating a hard white vitreous nodule, prereti-nal membrane, and horizontal retinal traction bands after three weeks of treatment with amphotericin.
VOL. 88 , N O . 1 MYCOTIC E N D O P H T H A L M I T I S 69
x-ray films, VDRL, Sabin-Feldman Dye Test on two occasions, Toxocara hemagglutination and benton-ite flocculation, histoplasmin latex agglutination, repeated blood cultures for bacteria and fungi, and x-ray films for possible retained intraocular foreign body were normal. Positive tests were: histoplasmin skin test in 1:100 dilution, intermediate purified protein derivative and high anti-A and anti-B hemagglutination titers. (On Oct. 31, 1975, titers were for anti-A, 1:1204, anti-B, 1:512; on Nov. 14, 1975, anti-A was 1:4096, anti-B, 1:512; on Nov. 19, 1975, anti-A was unchanged and anti-B was 1:2024). On Dec. 3, 1975, a diagnostic pars plana vitrectomy was performed. Gram and Giemsa stains of the vitreous aspirate revealed no organisms, but four days later a positive culture of C. albicans was obtained. In vitro susceptibilities to the isolate revealed greatest sensitivity to fiucytosine, amphotericin B, and miconazole nitrate. Minimal inhibitory concentrations by the tube dilution method were 0.39, 0.20, and 0.78 u.g/ml, respectively. Therapy with amphotericin with a maximum of 30 mg/day, 150 mg/kg of body weight of oral fiucytosine per day in four divided doses, and 30 mg every other day of oral prednisolone was initiated on Dec. 4,1975, with careful monitoring of renal, hepatic, and hematopo-etic functions. A total dose of 600 mg of amphotericin was given in four weeks before severe renal toxicity necessitated cessation of therapy. Visual acuity steadily improved during therapy. Predni-sone was gradually tapered, and the eye improved rapidly in three weeks (Fig. 3). His vision returned to 6/12 (20/40) by April 20, 1976.
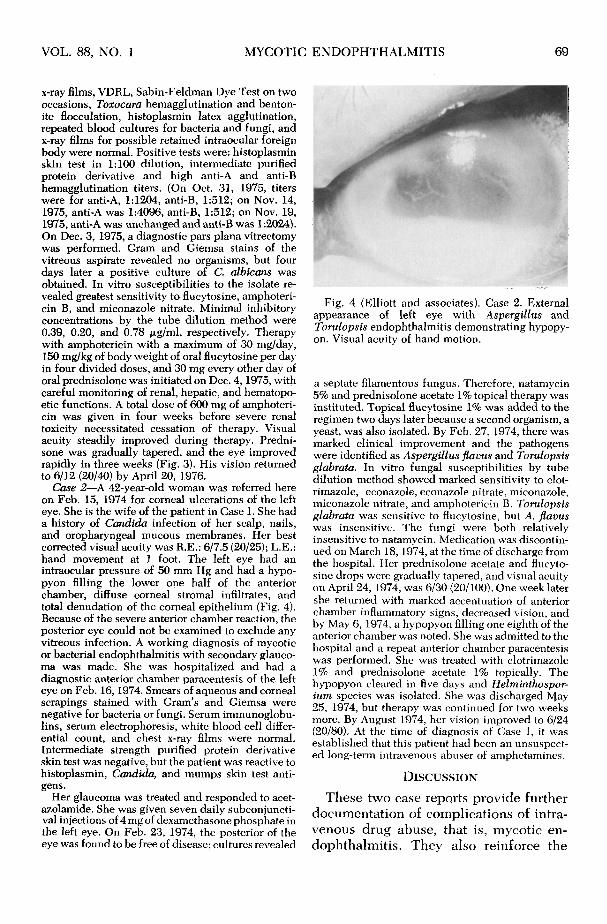
Case 2—A 42-year-old woman was referred here on Feb. 15, 1974 for corneal ulcerations of the left eye. She is the wife of the patient in Case 1. She had a history of Candida infection of her scalp, nails, and oropharyngeal mucous membranes. Her best corrected visual acuity was R.E.: 6/7.5 (20/25); L.E.: hand movement at 1 foot. The left eye had an intraocular pressure of 50 mm Hg and had a hypo-pyon filling the lower one half of the anterior chamber, diffuse corneal stromal infiltrates, and total denudation of the corneal epithelium (Fig. 4). Because of the severe anterior chamber reaction, the posterior eye could not be examined to exclude any vitreous infection. A working diagnosis of mycotic or bacterial endophthalmitis with secondary glaucoma was made. She was hospitalized and had a diagnostic anterior chamber paracentesis of the left eye on Feb. 16,1974. Smears of aqueous and corneal scrapings stained with Gram's and Giemsa were negative for bacteria or fungi. Serum immunoglobu-lins, serum electrophoresis, white blood cell differential count, and chest x-ray films were normal. Intermediate strength purified protein derivative skin test was negative, but the patient was reactive to histoplasmin, Candida, and mumps skin test antigens.
Her glaucoma was treated and responded to acet-azolamide. She was given seven daily subconjuncti-val injections of 4 mg of dexamethasone phosphate in the left eye. On Feb. 23, 1974, the posterior of the eye was found to be free of disease; cultures revealed
Hf$L
Fig. 4 (Elliott and associates). Case 2. External appearance of left eye with Aspergillus and Torulopsis endophthalmitis demonstrating hypopy-on. Visual acuity of hand motion.
a septate filamentous fungus. Therefore, natamycin 5% and prednisolone acetate 1% topical therapy was instituted. Topical fiucytosine 1% was added to the regimen two days later because a second organism, a yeast, was also isolated. By Feb. 27, 1974, there was marked clinical improvement and the pathogens were identified as Aspergillus flavus and Torulopsis glabrata. In vitro fungal susceptibilities by tube dilution method showed marked sensitivity to clot-rimazole, econazole, econazole nitrate, miconazole, miconazole nitrate, and amphotericin B. Torulopsis glabrata was sensitive to fiucytosine, but A. flavus was insensitive. The fungi were both relatively insensitive to natamycin. Medication was discontinued on March 18,1974, at the time of discharge from the hospital. Her prednisolone acetate and fiucytosine drops were gradually tapered, and visual acuity on April 24, 1974, was 6/30 (20/100). One week later she returned with marked accentuation of anterior chamber inflammatory signs, decreased vision, and by May 6, 1974, a hypopyon filling one eighth of the anterior chamber was noted. She was admitted to the hospital and a repeat anterior chamber paracentesis was performed. She was treated with clotrimazole 1% and prednisolone acetate 1% topically. The hypopyon cleared in five days and Helminthospor-ium species was isolated. She was discharged May 25, 1974, but therapy was continued for two weeks more. By August 1974, her vision improved to 6/24 (20/80). At the time of diagnosis of Case 1, it was established that this patient had been an unsuspected long-term intravenous abuser of amphetamines.
DISCUSSION
These two case reports provide further documentation of complications of intravenous drug abuse, that is, mycotic endophthalmitis. They also reinforce the

70 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1979
difficulty and delay in diagnosis of ocular fungal infections. With appropriate management and therapy, the visual prognosis in mycptic endophthalmitis can be improved.
The known predisposing factors for the development of mycotic endophthalmitis are: intraocular surgery, penetrating intraocular trauma, prolonged intravenous therapy, hyperalimentation, gastrointestinal surgery, or general debilitating diseases (such as terminal malignancy, and immunosuppressed or immunoin-competent patients with widely disseminated mycotic involvement, with or without fungemia). More recently it has been recognized that mycotic endophthalmitis can occur in intravenous drug abusers and in recipients of intraocular lens implants6,7 even in the absence of systemic diseases, immune deficiencies, or both. The diseases that should be considered in the differential diagnosis of mycotic endophthalmitis are bacterial and nema-tode endophthalmitis, toxoplasmic retino-choroiditis, herpes simplex Type 2 necrotizing retinopathy, sarcoidosis, his-toplasmosis, cytomegalic inclusion disease, and reticulum cell sarcoma (immu-noblastoma).
Mycotic endophthalmitis is a difficult clinical diagnostic problem.8 At present it is often necessary to perform both a diagnostic paracentesis and vitrectomy. The treatment of ocular fungal infections is hampered not only by the difficulty in culturing fastidious fungal organisms, but also by a lack of effective nontoxic antifungal agents that readily penetrate the eye.9 '10 Existing agents must be administered for prolonged periods, which produce serious toxic side effects.
Fungi in intravenous drug abusers who develop systemic infections may result from contamination of the drug, syringes, needles, or the cotton used to filter the drug before intravenous injection. We ob
tained some of the cotton balls used by the patient in Case 1 and the plastic vials that served as the receptacle for the cotton balls used by the patient in Case 2. Cultures revealed both Cryptococcus laurent-ii and Rhodotorula from each fomite. Although we failed to culture the same fungi as were isolated from the eyes, this shows that unsterile cotton balls may be contaminated with fungi and serve as a source of infection.
In intravenous drug abusers, the mycotic organisms, once injected, spread hematogenously to the eye. The route of ocular invasion, pathogenesis, and histo-pathology have been reported by other researchers.11 '12
Some interesting features in our cases deserve special mention. First, in Case 2, the fungal infections (Aspergillus and Torulopsis in the initial episode and Hel-minthosporium in the second) were exclusively confined to the anterior chamber. This is most unusual in blood-borne mycotic endophthalmitis, and, indeed, we have been unable to find any other documented case. It has been reported, however, after penetrating intraocular trauma or surgery. The fungi in Case 2 probably gained access to the anterior chamber via the ciliary body, the iris vessels, or both. Another unique feature of Case 2 is the reinfection with a different fungus species, which can best be explained by continued amphetamine abuse during treatment.
It has been emphasized that anti-A and anti-B isohemmaglutinin titers above 1:512 are presumptive and corroborative laboratory evidence of nematode endophthalmitis (Toxocara).13 Whether C. albic-ans or other fungi may also share antigen-ic cross-reactivity with human A and B blood group antigens and thus serve as an antigenic stimulus to boost the anti-A and anti-B isohemagglutinins is unknown. This possibility deserves further study.
V O L . 8 8 , N O . 1 M Y C O T I C E N D O P H T H A L M I T I S 7 1
In Case 1, we decided to use both intravenous amphotericin and oral flucy-tosine because of their known synergistic action in some Candida infections.10,14
The route and dosage for amphotericin as used in this case was established by the infectious disease group at Vanderbilt University Hospital.15,16 Some isolates of Candida species are known to be resistant to flucytosine.10,17,18 However, this only emphasizes the general principle that in the therapy of fungal diseases, in vitro susceptibilities are only a relative, not an absolute guide to the selection of the appropriate antifungal agent.
We are aware of the dangers of using topical and periocular corticosteroids in fungal infections of the eye. They must be used judiciously. Nevertheless, to achieve a good visual result, they may be mandatory in certain clinical situations, such as mycotic corneal disease or mycotic endophthalmitis.19 Our objective in therapy of ocular infections always has been to sterilize the eye with appropriate antibiotic or antifungal agents and to preserve visual function. To achieve the latter goal, we have been forced many times to administer adjunctive corticosteroid therapy. No rules can be written for the appropriate time to initiate corticosteroids, the dose and route to be used, or the length of time they should be given. Certainly, the clinical severity of the disease and the availability of an effective antifungal agent are crucial considerations in the use of corticosteroids. Also, the status of the host immune response should be evaluated. In a patient with a compromised host response, caused by either immune deficiency or severe debilitating disease, one should err on the side of conservatism and withhold corticosteroid therapy until the pathogen has been eradicated. Systemic corticosteroids are never indicated in the treatment of ocular mycoses. In our two cases, the results achieved with com
bined use of antifungals and corticosteroids were excellent.
SUMMARY
We diagnosed mycotic endophthalmitis by positive cultures in a 47-year-old man and a 42-year-old woman, both intravenous amphetamine users. Reinfection with a different fungal species was documented in one case. Rapid identification of the isolate, in vitro susceptibilities, selection of appropriate routes and dosages of antifungals, and the role of adjunctive corticosteroids are crucial factors in the management of these difficult cases. We prescribed antifungals and adjunctive corticosteroids, and our patients' vision improved.
REFERENCES 1. Sugar, H. S., Mandell, G. H., and Shalev, J. S.:
Metastatic endophthalmitis associated with injection of addictive drugs. Am. J. Ophthalmol. 71:1055, 1971.
2. Getnick, R. A., and Rodriques, M. M.: Endogenous fungal endophthalmitis in a drug addict. Am. J. Ophthalmol. 77:680, 1974.
3. Stone, R. D., Irvine, A. R., and O'Connor, G. R.: Candida endophthalmitis. Report of an unusual case with isolation of the etiologic agent by vitreous biopsy. Ann. Ophthalmol. 7:757, 1975.
4. Snip, R. C , and Michels, R. G.: Pars plana vitrectomy in the management of endogenous Candida endophthalmitis. Am. J. Ophthalmol. 82:699, 1976.
5. Vastine, D. W., Horsley, W., Guth, S. B., and Goldberg, M. F.: Endogenous Candida endophthalmitis associated with heroin use. Arch. Ophthalmol. 94:1805, 1976.
6. O'Day, D. M.: Fungal endophthalmitis caused by Paecilomyces lilacinus after intraocular lens implantation. Am. J. Ophthalmol. 83:130, 1977.
7. Mosier, M. A., Lusk, B., Pettit, T. H., Howard, D. H., and Rhodes, J.: Fungal endophthalmitis following intraocular lens implantation. Am. J. Ophthalmol. 83:1, 1977.
8. Michelson, P. E., Stark, W., Reeser, F., and Green, W. R.: Endogenous Candida endophthalmitis. Int. Ophthalmol. Clin. 2:125, 1971.
9. Green, W. R., Bennett, J. E., and Goos, R. D.: Ocular penetration of amphotericin B. Arch. Ophthalmol. 73:769, 1965.
10. Jones, B. R.: Principles in the management of oculomycosis. Am. J. Ophthalmol. 79:719, 1975.
11. Griffin, J. R., Pettit, T. H., Fishman, L. S., and
72 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1979
Foos, R. Y.: Blood-borne Candida endophthalmitis. Arch. Ophthalmol. 89:450, 1973.
12. McLean, J. M.: Oculomycosis. Am. J. Ophthalmol. 56:537, 1963.
13. Huntley, C. C , Lyerly, A. D., and Patterson, M. V.: Isohemagglutinins in parasitic infection. J.A.M.A. 208:1145, 1969.
14. Rabinovich, S., Shaw, B. D., Bryant, T., and Donta, S. T.: The effect of 5-fluorocytosine and amphotericin B on Candida albicans infection in mice. J. Infect. Dis. 130:28, 1974.
15. Drutz, D. J., Spickard, A., and Koenig, M. G.: New approach to therapy with amphotericin B. Antimicrob. Agents Chemother.: 202, 1966.
16. Drutz, D. J., Spickard A., Rogers, D. E., and Koenig, M. G.: Treatment of disseminated mycotic infections. A new approach to amphotericin B therapy. Am. J. Med. 45:45, 1968.
17. Robertson, D. M., Riley, F. C., and Hermans, P. E.: Endogenous Candida oculomycosis. Arch. Ophthalmol. 91:33, 1974.
18. Fishman, L. S., Griffin, J. R., Sapico, F. L., and Hecht, R.: Hematogenous Candida endophthalmitis. A complication of candidemia. N. Engl. J. Med. 286:675, 1972.
19. O'Day, D. M., Moore, T. E., Jr., and Aronson, S. B.: Deep fungal corneal abscess. Arch. Ophthalmol. 86:414, 1971.