Embed Size (px)
Citation preview
CIRN_23506_5_Myelodysplastic Syndrome_DT10 7/18/2005 2:18 PM
Disclosures for Ayalew Tefferi
Presentation includes discussion of the following off-label use of a drug or medical device:
Hydroxyurea, Interferon-alpha, Busulfan, Ruxolitinib, Cladribine, ESAs, Prednisone, Danazol, Androgens, Thalidomide, Lenalidomide, Imatinib, Alemtuzumab
PI/co-PICelgene, Novartis, BMS, YM Biosciences, Sanofi-Aventis, Incyte, PharmaMar
Research support None
Employee/Consultant None
Major Stockholder None
Speakers’ Bureau None
Scientific Advisory Board None
Myeloproliferative Neoplasms 2012-2013: Science and Practice
Ayalew TefferiMayo Clinic, Rochester, MN
Myeloid Malignancies
Chronic myeloidmalignancies
Acute myeloid
leukemia
Acquired mutation *
CytopeniaGranulocytosisErythrocytosis
ThrombocytosisMonocytosisEosinophiliaMastocytosis
≥20% BM or PBblasts
Or
t(15;17)t(8;21)Inv(16)
Or
Myeloid sarcoma
Redcells
Platelets Mono-cytes
Neutro-phils
Eosino-phils
Baso-phils
Pluripotentstem cellCFUGEMM
BFUE
CFU-G
CFUEOCFUE
CFUGMCFUMegr
CFU-M
MDS MPNMDS/MPN
Tefferi 2012
Myeloproliferative Neoplasms (MPN)
1. Chronic myelogenous leukemia
2. Polycythemia vera
3. Essential thrombocythemia
4. Primary myelofibrosis
5. Mastocytosis
6. Primary eosinophilia
7. Chronic neutrophilic leukemia
8. MPN-U
Myeloproliferative Neoplasms (MPN)
1. Chronic myelogenous leukemia
2. Polycythemia vera
3. Essential thrombocythemia
4. Primary myelofibrosis
5. Mastocytosis
6. Primary eosinophilia
7. Chronic neutrophilic leukemia
8. MPN-U
BCR-ABL1-negative MPN
*
*
CMML*
Objectives
1. Pathogenetic mechanisms
2. Contemporary diagnosis
3. Prognostication
4. Management
CIRN_23506_5_Myelodysplastic Syndrome_DT10 7/18/2005 2:18 PM
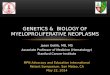
Tefferi A. Leukemia 24:1128-38, 2010
BCR-ABL1negative
MPN
** * ** *
**
*JAK2(+)
AML
JAK2(-)AML
Blast phaseCML
Disease-initiatingmutations
BCR-ABL1
?
Polyclonal stem cellsharboring
disease-susceptibilityalleles such as
JAK2 46/1 haplotype
JAK2, MPL, TET2, ASXL1, CBL, IDH1/2, IKZF4, LNK, EZH2, DNMT3A, SF3B1, TP53
?
?
?
Disease-transformingmutations
?
Phenotype-modifyingmutations
PVET
PMF
**
****
**
**
** *
**
*
CML
?
JAK2, MPL, TET2, ASXL1, CBL, IDH1/2, IKZF4, LNK, EZH2, DNMT3A, SF3B1, SRSF2, TP53The two pathogenetic faces of myelofibrosis
Bone marrowstromal reaction
Ineffective hematopoiesis (anemia)Extramedullary hematopoiesis (splenomegaly)
Hypercatabolic symptoms, pruritus and cachexia
AMLSurvival
LeukocytosisThrombocytosisAbnormal
cytokine milieu
Secondaryinflammatory
state
Mutation-drivenclonal
myeloproliferation
Tefferi et al. JCO 2011Tefferi NEJM 2012
IL-1b
IL-1RA
IL-2R
IL-6
IL-8
IL-10
IL-12
IL-13
IL-15
TNF-α
G-CSF
INF-α
INF-γ
MIP-1a
MIP-1b
HGF
IP-10
MIG
MCP-1
VEGF
Diagnosis
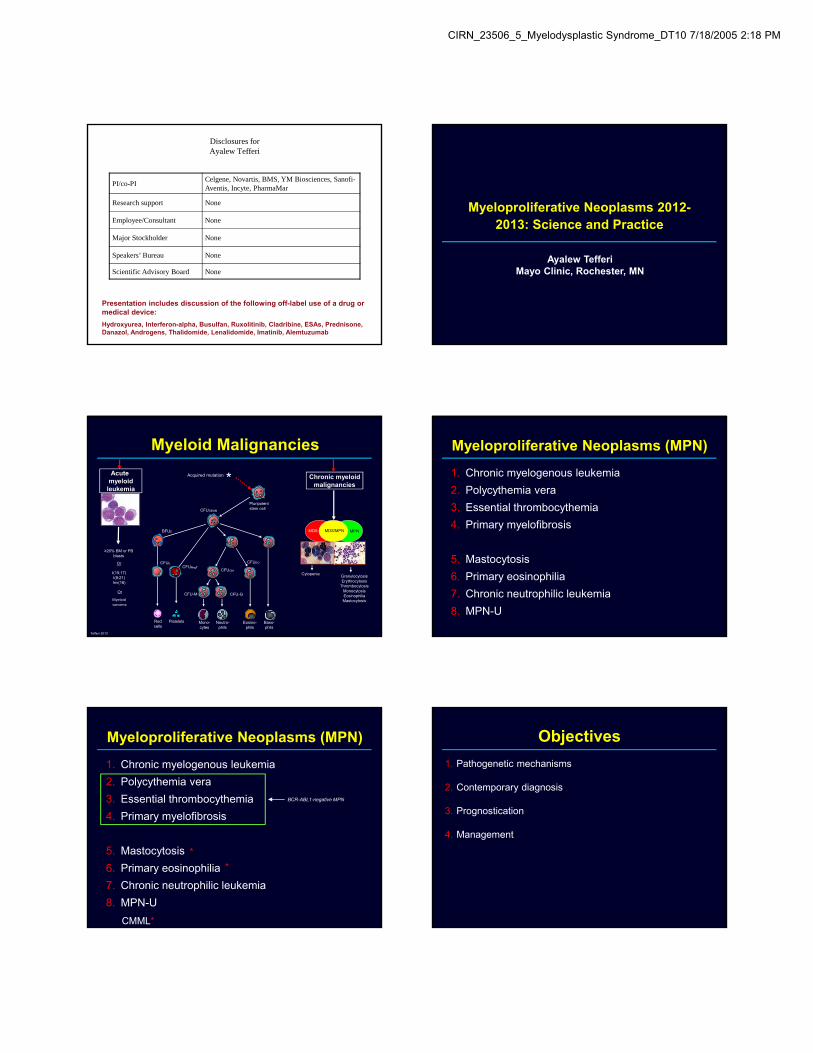
PV 97% V617F and 3% JAK2 exon 12 mutationsET 60% V617F and 4% MPL515 mutationsPMF 60% V617F and 8% MPL 515 mutations
NOT FOUND IN SECONDARY POLYCYTHEMIANOT FOUND IN REACTIVE THROMBOCYTOSISNOT FOUND IN LYMPHOMA OR METASTATIC CANCER
JAK2 mutations
Levine et al. Nat Rev Cancer. 2007;7:673
RasPI3K
P PPStatStat RafAKT
Activation of genes importantin proliferation and survival
PPPStatStat Erk
Src
C
StatStat
A BLigand Binding
JAK2V617For JAK2 Exon 12
MPLW515L/K
JAK2JAK2PP
StatStat
JAK2JAK2PP
StatStat
JAK2JAK2PP
P
PMekFoxOmTOR
ErkX
?
X
SOCS1 SOCS3
BloodJAK2V617F and
Epo screen
(+) V617F
Polycythemia vera
BloodJAK2V617F
screen
Diagnostic algorithm
PV
Not PV
Screen forJAK2 exon 12
mutation
(-) V617F
Eposubnormal
Eponormal orelevated
(+) V617F
BM biopsy
(-) V617F
MPNpresent
MPNpossible
Essential thrombocythemia
Myelofibrosis V617F, +9 or 13q- = PMF
Tefferi AJH 2012
CML
PrefibroticPMF
MDS(e.g. RARS-T)
ET
VS.VS.
VS.
CIRN_23506_5_Myelodysplastic Syndrome_DT10 7/18/2005 2:18 PM
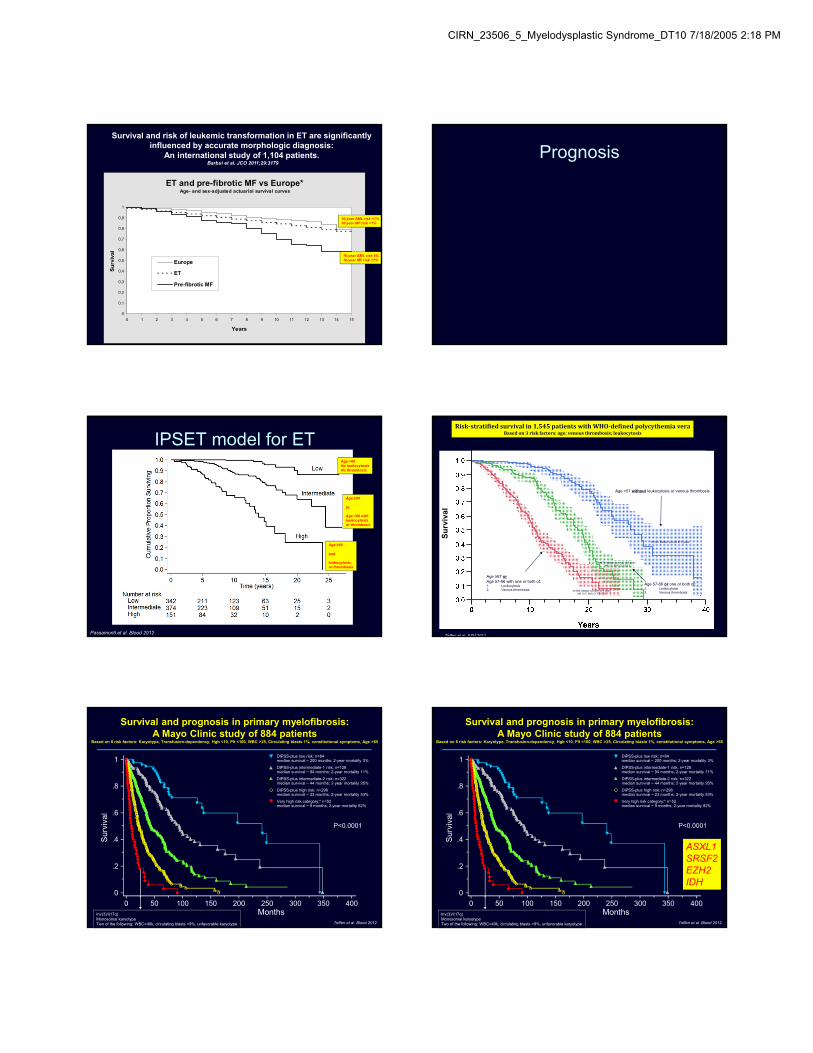
ET and pre-fibrotic MF vs Europe*Age- and sex-adjusted actuarial survival curves
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
Su
rviv
al
Europe
ET
Pre-fibrotic MF
Survival and risk of leukemic transformation in ET are significantly influenced by accurate morphologic diagnosis:
An international study of 1,104 patients. Barbui et al. JCO 2011;29:3179
10-year AML risk <1%10-year MF risk <1%
10-year AML risk 6%10-year MF risk 12%
Prognosis
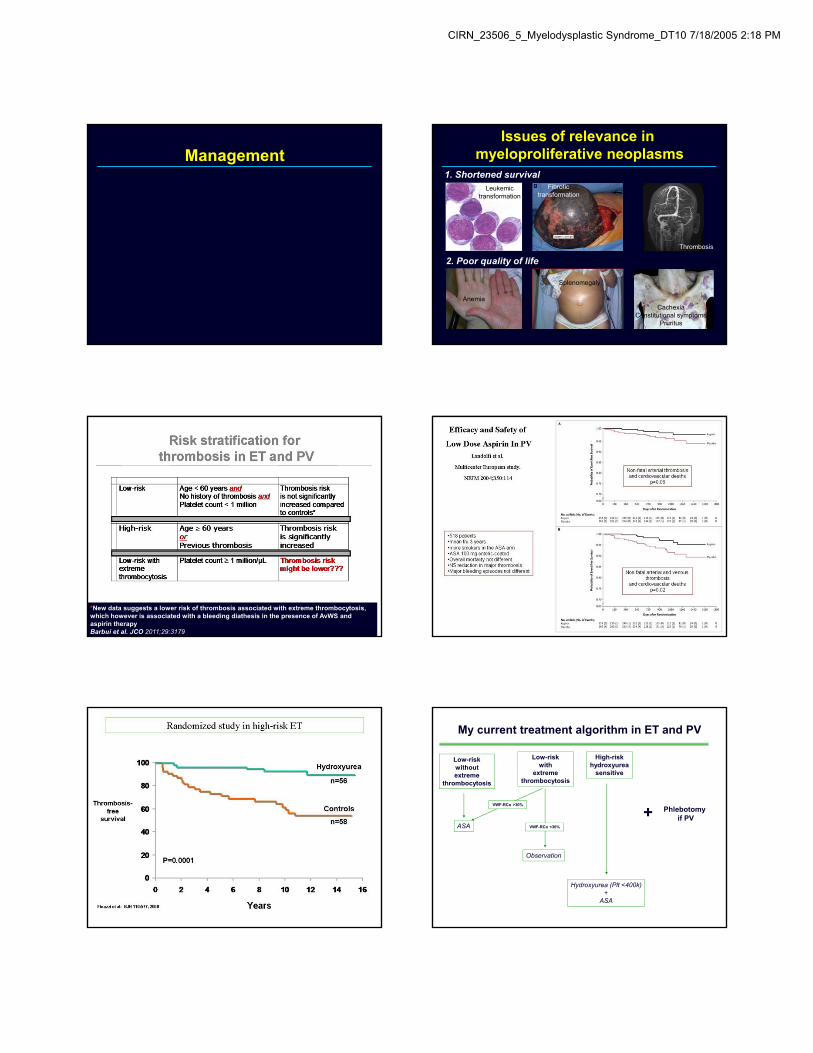
IPSET model for ET
Passamonti et al. Blood 2012
Age <60No leukocytosisNo thrombosis
Age ≥60
or
Age <60 withleukocytosisor thrombosis
Age ≥60
and
leukocytosisor thrombosis
Risk‐stratifiedsurvivalin1,545patientswithWHO‐definedpolycythemiaveraBasedon3riskfactors:age;venousthrombosis;leukocytosis
Su
rviv
al
N=568; Median survival 10.9 yearsHR 10.7; 95% CI 7.7-15.0
N=474; Median survival 18.9 years HR 3.7; 95% CI 2.6-5.2
N=503; Median survival 27.8 years
Age <57 without leukocytosis or venous thrombosis
Age 57-66 or one or both of: 1. Leukocytosis2. Venous thrombosis
Age ≥67 orAge 57-66 with one or both of: 1. Leukocytosis2. Venous thrombosis
Tefferi et al. ASH 2011
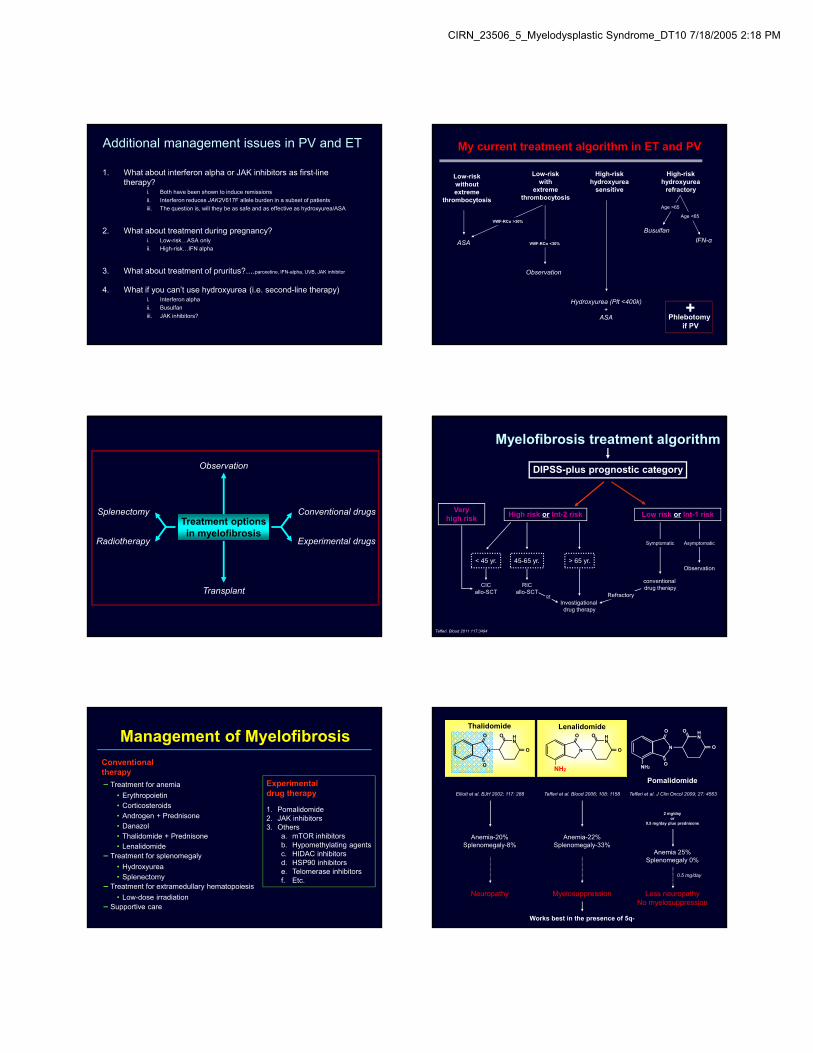
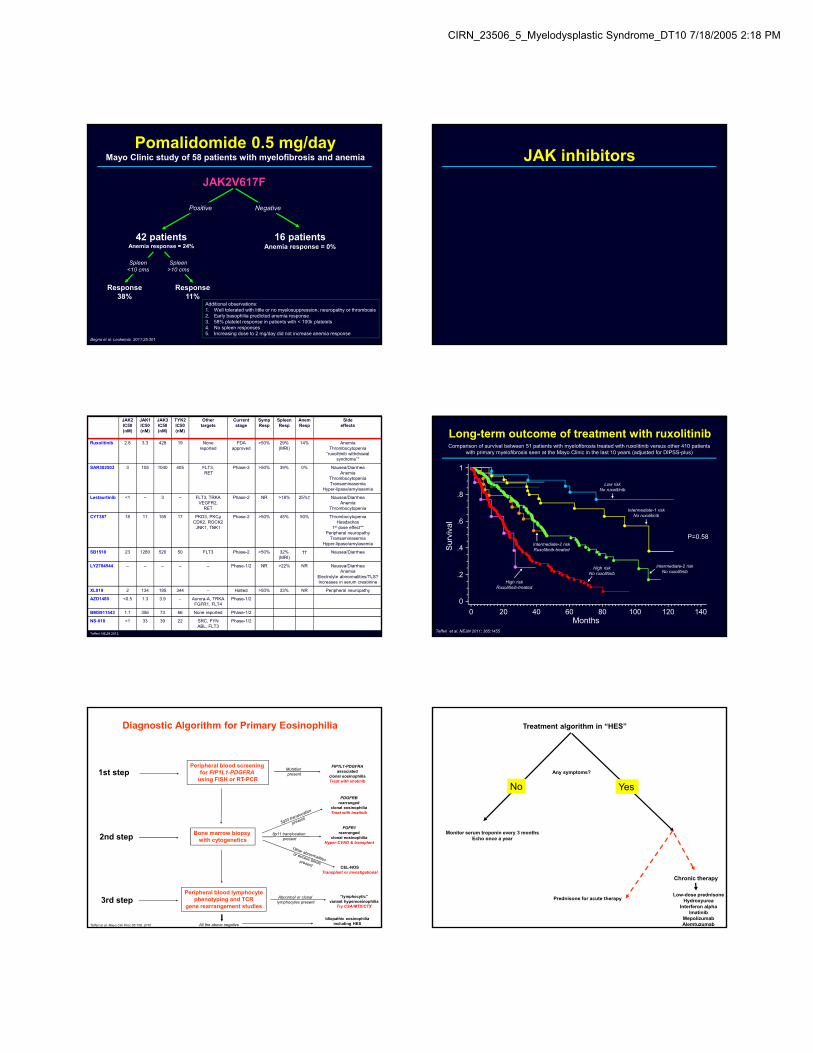
Survival and prognosis in primary myelofibrosis: A Mayo Clinic study of 884 patients
Based on 8 risk factors: Karyotype, Transfusion-dependency, Hgb <10, Plt <100, WBC >25, Circulating blasts 1%, constitutional symptoms, Age >65
DIPSS-plus intermediate-1 risk; n=128median survival ~ 94 months; 2-year mortality 11%
DIPSS-plus low risk; n=84median survival ~ 200 months; 2-year mortality 3%
DIPSS-plus high risk; n=298median survival ~ 23 months; 2-year mortality 53%
DIPSS-plus intermediate-2 risk; n=322median survival ~ 44 months; 2-year mortality 26%
Sur
viva
l
Months
1
.8
.6
.4
.2
0
0 50 100 150 200 250 300 350 400
P<0.0001
Tefferi et al. Blood 2012
Very high risk category;* n=52median survival ~ 9 months; 2-year mortality 82%
Inv(3)/i(17q)Monosomal karyotypeTwo of the following: WBC>40k, circulating blasts >9%, unfavorable karyotype
Survival and prognosis in primary myelofibrosis: A Mayo Clinic study of 884 patients
Based on 8 risk factors: Karyotype, Transfusion-dependency, Hgb <10, Plt <100, WBC >25, Circulating blasts 1%, constitutional symptoms, Age >65
DIPSS-plus intermediate-1 risk; n=128median survival ~ 94 months; 2-year mortality 11%
DIPSS-plus low risk; n=84median survival ~ 200 months; 2-year mortality 3%
DIPSS-plus high risk; n=298median survival ~ 23 months; 2-year mortality 53%
DIPSS-plus intermediate-2 risk; n=322median survival ~ 44 months; 2-year mortality 26%
Sur
viva
l
Months
1
.8
.6
.4
.2
0
0 50 100 150 200 250 300 350 400
P<0.0001
Tefferi et al. Blood 2012
Very high risk category;* n=52median survival ~ 9 months; 2-year mortality 82%
Inv(3)/i(17q)Monosomal karyotypeTwo of the following: WBC>40k, circulating blasts >9%, unfavorable karyotype
ASXL1SRSF2EZH2IDH
CIRN_23506_5_Myelodysplastic Syndrome_DT10 7/18/2005 2:18 PM
ManagementIssues of relevance in
myeloproliferative neoplasms1. Shortened survival
2. Poor quality of life
Thrombosis
CachexiaConstitutional symptoms
Pruritus
Anemia
Splenomegaly
Leukemictransformation
Fibrotictransformation
*New data suggests a lower risk of thrombosis associated with extreme thrombocytosis, which however is associated with a bleeding diathesis in the presence of AvWS and aspirin therapyBarbui et al. JCO 2011;29:3179
My current treatment algorithm in ET and PV
Low-riskwithoutextreme
thrombocytosis
Low-riskwith
extremethrombocytosis
High-riskhydroxyurea
sensitive
ASA
VWF-RCo >30%
VWF-RCo <30%
Observation
Hydroxyurea (Plt <400k)+
ASA
Phlebotomy if PV+
CIRN_23506_5_Myelodysplastic Syndrome_DT10 7/18/2005 2:18 PM
Additional management issues in PV and ET
1. What about interferon alpha or JAK inhibitors as first-line therapy?
i. Both have been shown to induce remissions
ii. Interferon reduces JAK2V617F allele burden in a subset of patients
iii. The question is, will they be as safe and as effective as hydroxyurea/ASA
2. What about treatment during pregnancy?i. Low-risk…ASA only
ii. High-risk…IFN alpha
3. What about treatment of pruritus?....paroxetine, IFN-alpha, UVB, JAK inhibitor
4. What if you can’t use hydroxyurea (i.e. second-line therapy)i. Interferon alpha
ii. Busulfan
iii. JAK inhibitors?
My current treatment algorithm in ET and PV
Low-riskwithoutextreme
thrombocytosis
Low-riskwith
extremethrombocytosis
High-riskhydroxyurea
sensitive
High-riskhydroxyurea
refractory
ASA
VWF-RCo >30%
VWF-RCo <30%
Observation
Hydroxyurea (Plt <400k)+
ASA
Busulfan
Age >65
Age <65
IFN-α
+Phlebotomy
if PV
Observation
Transplant
Conventional drugsSplenectomy
Radiotherapy Experimental drugs
Treatment optionsin myelofibrosis
Tefferi. Blood 2011 117:3494
DIPSS-plus prognostic category
Myelofibrosis treatment algorithm
High risk or Int-2 risk Low risk or Int-1 riskVery
high risk
< 45 yr. > 65 yr.
Symptomatic
45-65 yr.
Asymptomatic
Investigational drug therapy
or Refractory
Observation
CICallo-SCT
conventional drug therapyRIC
allo-SCT
Management of Myelofibrosis
Experimental drug therapy
1. Pomalidomide2. JAK inhibitors3. Others
a. mTOR inhibitorsb. Hypomethylating agentsc. HIDAC inhibitorsd. HSP90 inhibitorse. Telomerase inhibitorsf. Etc.
Conventional therapy
-Treatment for anemia
• Erythropoietin• Corticosteroids• Androgen + Prednisone• Danazol• Thalidomide + Prednisone• Lenalidomide
-Treatment for splenomegaly
• Hydroxyurea• Splenectomy
-Treatment for extramedullary hematopoiesis
• Low-dose irradiation-Supportive care
Anemia 25%Splenomegaly 0%
Works best in the presence of 5q-
Tefferi et al. Blood 2006; 108: 1158
Anemia-22%Splenomegaly-33%
Elliott et al. BJH 2002; 117: 288
Anemia-20%Splenomegaly-8%
Lenalidomide
Pomalidomide
Tefferi et al. J Clin Oncol 2009; 27: 4563
2 mg/dayor
0.5 mg/day plus prednisone
0.5 mg/day
Less neuropathyNo myelosuppression
MyelosuppressionNeuropathy
NH2O
N
O O HN
O
NH2
N
O O HN
O
O
N
O O HN
O
Thalidomide
CIRN_23506_5_Myelodysplastic Syndrome_DT10 7/18/2005 2:18 PM
Pomalidomide 0.5 mg/dayMayo Clinic study of 58 patients with myelofibrosis and anemia
Begna et al. Leukemia. 2011;25:301
Additional observations:1. Well tolerated with little or no myelosuppression, neuropathy or thrombosis2. Early basophilia predicted anemia response3. 58% platelet response in patients with < 100k platelets4. No spleen responses5. Increasing dose to 2 mg/day did not increase anemia response
JAK2V617F
Positive Negative
42 patientsAnemia response = 24%
16 patientsAnemia response = 0%
Response38%
Response11%
Spleen>10 cms
Spleen<10 cms
JAK inhibitors
JAK2IC50(nM)
JAK1IC50(nM)
JAK3IC50(nM)
TYK2IC50(nM)
Other targets
Currentstage
SympResp
Spleen Resp
AnemResp
Side effects
Ruxolitinib 2.8 3.3 428 19 None reported
FDAapproved
>50% 29%(MRI)
14% Anemia Thrombocytopenia
“ruxolitinib withdrawal syndrome”*
SAR302503 3 105 1040 405 FLT3,RET
Phase-3 >50% 39% 0% Nausea/DiarrheaAnemia
ThrombocytopeniaTransaminasemia
Hyper-lipase/amylasemia
Lestaurtinib <1 – 3 – FLT3, TRKAVEGFR2,
RET
Phase-2 NR >18% 25%† Nausea/DiarrheaAnemia
Thrombocytopenia
CYT387 18 11 155 17 PKD3, PKCμCDK2, ROCK2
JNK1, TBK1
Phase-2 >50% 45% 50% ThrombocytopeniaHeadaches
1st dose effect**Peripheral neuropathy
TransaminasemiaHyper-lipase/amylasemia
SB1518 23 1280 520 50 FLT3 Phase-2 >50% 32%(MRI)
†† Nausea/Diarrhea
LY2784544 – – – – – Phase-1/2 NR >22% NR Nausea/DiarrheaAnemia
Electrolyte abnormalities/TLS?Increases in serum creatinine
XL019 2 134 195 344 – Halted >50% 33% NR Peripheral neuropathy
AZD1480 <0.5 1.3 3.9 – Aurora-A, TRKAFGFR1, FLT4
Phase-1/2
BMS911543 1.1 356 73 66 None reported Phase-1/2
NS-018 <1 33 39 22 SRC, FYNABL, FLT3
Phase-1/2
Tefferi. NEJM 2012
Long-term outcome of treatment with ruxolitinibComparison of survival between 51 patients with myelofibrosis treated with ruxolitinib versus other 410 patients
with primary myelofibrosis seen at the Mayo Clinic in the last 10 years (adjusted for DIPSS-plus)S
urvi
val
Months
1
.8
.6
.4
.2
0
1000 20 40 60 80 120
P=0.58
Tefferi et al. NEJM 2011; 365:1455
Intermediate-2 riskNo ruxolitinib
140
High riskRuxolitinib-treated
High riskNo ruxolitinib
Intermediate-2 riskRuxolitinib-treated
Intermediate-1 riskNo ruxolitinib
Low riskNo ruxolitinib
Diagnostic Algorithm for Primary Eosinophilia
1st step
2nd step
3rd step
Peripheral blood screening for FIP1L1-PDGFRA
using FISH or RT-PCR
Bone marrow biopsy with cytogenetics
Peripheral blood lymphocytephenotyping and TCR
gene rearrangement studies
Mutation present
FIP1L1-PDGFRAassociated
clonal eosinophiliaTreat with imatinib
PDGFRBrearranged
clonal eosinophiliaTreat with imatinib
8p11 translocation present
FGFR1rearranged
clonal eosinophiliaHyper-CVAD & transplant
CEL-NOSTransplant or investigational
Abnormal or clonal lymphocytes present
“lymphocytic”variant hypereosinophilia
Try CSA/MTX/CTX
All the above negative
Idiopathic eosinophiliaincluding HESTefferi et al. Mayo Clin Proc 85:158, 2010
Treatment algorithm in “HES”
Any symptoms?
Prednisone for acute therapy
Chronic therapy
Low-dose prednisoneHydroxyurea
Interferon alphaImatinib
MepolizumabAlemtuzumab
YesNo
Monitor serum troponin every 3 monthsEcho once a year
CIRN_23506_5_Myelodysplastic Syndrome_DT10 7/18/2005 2:18 PM
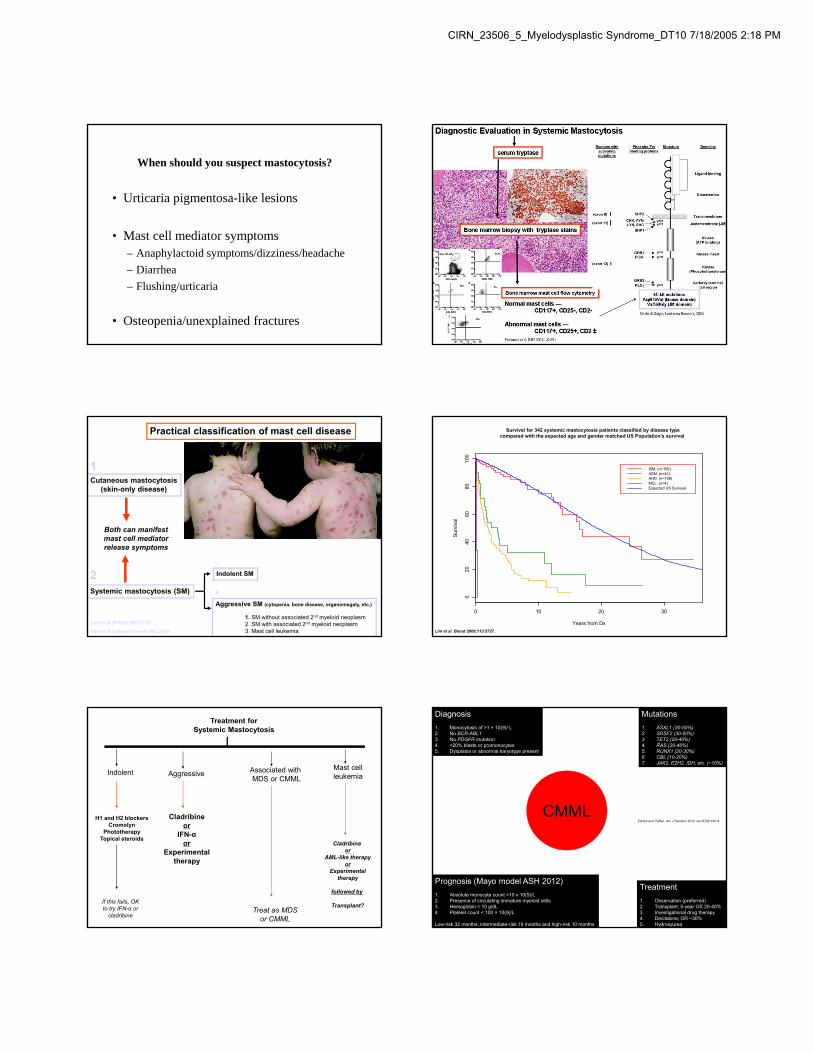
When should you suspect mastocytosis?
• Urticaria pigmentosa-like lesions
• Mast cell mediator symptoms– Anaphylactoid symptoms/dizziness/headache
– Diarrhea
– Flushing/urticaria
• Osteopenia/unexplained fractures
Practical classification of mast cell disease
Cutaneous mastocytosis(skin-only disease)
Systemic mastocytosis (SM)
Aggressive SM (cytopenia, bone disease, organomegaly, etc.)
1. SM without associated 2nd myeloid neoplasm2. SM with associated 2nd myeloid neoplasm3. Mast cell leukemia
Indolent SM
Hartmann. & Henz, Br J Derm 2001;144:682
Travis et al. Medicine 1988;67:345
Valent et al. Leukemia Research 2001;25:603
Both can manifestmast cell mediatorrelease symptoms
1
2i
ii
Years from Dx
Sur
viva
l
0 10 20 30
020
4060
8010
0
01Oct08
ISM, (n=159)ASM, (n=41)AHD, (n=138)MCL, (n=4)Expected US Survival
Survival for 342 systemic mastocytosis patients classified by disease type compared with the expected age and gender matched US Population’s survival
Lim et al. Blood 2009;113:5727.
Treatment forSystemic Mastocytosis
Indolent Associated with MDS or CMML
AggressiveMast cellleukemia
Treat as MDSor CMML
Cladribine or
AML-like therapyor
Experimentaltherapy
followed by
Transplant?
Cladribineor
IFN-αor
Experimentaltherapy
If this fails, OKto try IFN-α or
cladribine
H1 and H2 blockersCromolyn
PhototherapyTopical steroids
CMMLParikh and Tefferi, Am J Hematol 2012 Jun;87(6):610-9
Diagnosis
1. Monocytosis of >1 × 10(9)/ L2. No BCR-ABL13. No PDGFR mutation4. <20% blasts or promonocytes5. Dysplasia or abnormal karyotype present
Prognosis (Mayo model ASH 2012)
1. Absolute monocyte count >10 x 10(9)/L2. Presence of circulating immature myeloid cells3. Hemoglobin < 10 g/dL 4. Platelet count < 100 × 10(9)/L
Low-risk 32 months, intermediate-risk 19 months and high-risk 10 months
Treatment
1. Observation (preferred)2. Transplant; 5-year OS 20-40%3. Investigational drug therapy4. Decitabine; OR ~30%5. Hydroxyurea
Mutations
1. ASXL1 (30-50%)2. SRSF2 (30-50%)3. TET2 (20-40%)4. RAS (20-40%)5. RUNX1 (20-30%)6. CBL (10-20%)7. JAK2, EZH2, IDH, etc. (~10%)