Embed Size (px)
Citation preview

Myers’ PSYCHOLOGY
(7th Ed)
Chapter 16
Psychological Disorders
James A. McCubbin, PhDClemson University
Worth Publishers

Psychological Disorders
Psychological Disordera “harmful dysfunction” in which behavior is judged to be:atypical--not enough in itselfdisturbing--varies with time and culture
maladaptive--harmfulunjustifiable--sometimes there’s a good reason

Historical Perspective Perceived Causes
movements of sun or moon lunacy--full moon
evil spirits Ancient Treatments
exorcism, caged like animals, beaten, burned, castrated, mutilated, blood replaced with animal’s blood

Psychological Disorders
Medical Model concept that diseases have physical causes can be diagnosed, treated, and in most
cases, cured assumes that these “mental” illnesses can
be diagnosed on the basis of their symptoms and cured through therapy, which may include treatment in a psychiatric hospital

Psychological Disorders
Bio-Psycho-Social Perspectiveassumes that biological, sociocultural, and psychological factors combine and interact to produce psychological disorders

Psychological Disorders

Psychological Disorders--Etiology
DSM-IV American Psychiatric Association’s
Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition)
a widely used system for classifying psychological disorders
presently distributed as DSM-IV-TR (text revision)

Psychological Disorders- Etiology
Neurotic Disorder (term seldom used now) usually distressing but that allows
one to think rationally and function socially
Psychotic Disorder person loses contact with reality experiences irrational ideas and
distorted perceptions

What is abnormal behavior?

Psychologists typically identify abnormal behavior based on a combination of the following criteria:
UnusualnessSocial devianceEmotional DistressMaladaptive BehaviorDangerousnessFaulty perceptions/interpretations of
reality

Unusualness
Behavior that is experienced by only a few people may be abnormal, but not in all cases.
Unusualness, by itself, is not enough to be called abnormal.

Social Deviance
All societies establish social norms that define socially acceptable behaviors.
Deviation from these norms is often used as a criterion for labeling behavior as abnormal.
The same behavior might be considered abnormal in some contexts but acceptable in others.

Emotional DistressStates of emotional distress, such
as anxiety or depression are considered abnormal when: Inappropriate Excessive Prolonged
(relative to the person’s situation)

Maladaptive Behavior
Behavior is maladaptive when: it causes personal distress is self-defeating is associated with significant health or
social problems (alcohol or drug abuse)

Dangerousness
Violent or dangerous behavior needs to be looked at in context

Faulty perceptions or interpretations of reality
Hallucinations: distorted perceptions of reality (seeing or hearing things that are not real)
Delusions: Fixed but unfounded beliefs are also distortions of reality (believing people are plotting against you)

Cultural context must be considered
The cultural context in which behavior occurs must also be evaluated when making judgments about whether behavior is abnormal.

Is this abnormal behavior?

Psychological Disorders
Anxiety Disorders: Generalized Anxiety Disorder Panic Disorder Phobic Disorder Post-traumatic Stress Disorder Obsessive Compulsive Disorder

Generalized Anxiety Disorder:
GAD is characterized by persistent anxiety, unrelated to a specific event.
People suffering from GAD cannot help worrying about anything and everything, even in calm situations.
They have difficulty relaxing, falling asleep, and/or concentrating, and tend to be impatient and irritable.

Physical symptoms accompanying GAD include: sweating; an upset stomach; diarrhea;
frequent urination; cold, clammy hands; a lump in the throat; a dry mouth; shortness of breath; headaches; and dizziness.

Managing the normal demands of a job, relationships, and everyday life can become more and more difficult for people with this disorder.
GAD appears in four percent of the general population.

Panic DisorderPanic attacks are sudden, unexplainable
waves of panic that seem to come out of the blue.
The body responds with the "fight-or-flight" response, anticipating clear and immediate danger.
Often, these attacks subside as mysteriously as they occur.

A person who has experienced one or more panic attacks often develops a fear of having one again.
Some professionals call this a "fear of fear."
The individual may even try to stay away from anything that reminds him or her of the last attack to avoid having another one.

People can have panic attacks with or without agoraphobia.
These attacks include symptoms such as heart palpitations, shortness of breath, chest pain, feelings of choking or smothering, nausea, dizziness, sweating, and trembling.
An afflicted person might also be overwhelmed by a fear of dying, going crazy, or losing control.

Phobias:
Phobias are attempts to compartmentalize fear into a few situations that can be avoided.
By attaching all the panicky feelings onto a few situations, the person can avoid those situations and go on with life.
Unfortunately, phobias can take on a life of their own and take over more and more of a person's life.

A fear of dogs can, for example, be fairly easy to manage, just don't go near dogs.
But a fear of flying may limit social and business opportunities.
Some of the more common phobias include claustrophobia (fear of closed spaces), agoraphobia (fear of public places, sometimes related to panic attacks), and acrophobia (fear of heights).

Posttraumatic Stress Disorder:
Posttraumatic stress disorder (PTSD) can develop in the wake of a traumatic event that is outside the usual human experience.
A person either experiences direct or threatened injury, or witnesses the serious injury or death of another.
In some cases, learning of the unexpected death or injury of a loved one can also bring on symptoms of PTSD.

For a diagnosis of PTSD to be made, there must be both an identifiable terrifying event and a response of intense fear, helplessness and horror, as well as one or more characteristic symptoms.
These include re-experiencing of the event through: nightmares daytime flashbacks physical sensations that recall the feelings
present during the event.

PTSD Symptoms continuedShutting down feelings and memory. Feeling detached from others. Dissociating from the distressing memories
and feelings.Hyperalertness to danger. The individual
often has difficulty shutting down the fight-or-flight response that was activated during the event. This causes sleeplessness, irritability, difficulty concentrating, restlessness, and sometimes the development of an exaggerated startle.
Hypervigilance and avoidance of any situation associated with the event. These symptoms significantly disrupt an afflicted
person’s daily life.

Obsessive-Compulsive DisorderAlthough classified as an anxiety disorder,
obsessive-compulsive disorder (OCD) differs from these disorders in significant ways.
It is the one anxiety diagnosis that seems to have a clear biological cause. Unlike the other kinds of anxiety disorders, therapy alone isn't much help. Medication is also necessary.
OCD is a disorder in which the mind is flooded with involuntary thoughts, or in which an individual feels compelled to repeat certain acts over and over again (for example, hand washing).

This disorder can interfere significantly with everyday living, and usually leads to concern and/or resentment among friends, family, and co-workers.
A person who suffers from OCD doesn't want the thoughts and doesn't want to do the behaviors. Unfortunately, he or she really can't help it.
About half the people with OCD report that it began in childhood; most others start in adolescence or early adulthood. OCD affects approximately two percent of the general population.

Anxiety Disorders Common and uncommon fears

Anxiety Disorders

Anxiety Disorders
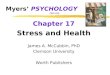
PET Scan of brain of person with Obsessive/ Compulsive disorder
High metabolic activity (red) in frontal lobe areas involved with directing attention

Two Broad Categories of Mood Disorders
Depressive DisordersBipolar Disorders

Depressive Disorders
(1) Major Depressive Disorder (major depression) The most common type of depressive
disorder. Characterized by periods of downcast
mood, feelings of worthlessness, and loss of interest in pleasurable activities.
Is more common in women

Depressive Disorders Continued
(2) Seasonal Affective Disorder (SAD) A type of major depression that
involves a recurring pattern of Winter depressions followed by elevations in mood in the Spring and Summer.
More common in extreme northern climates

Depressive Disorders Continued
(3) Dysthymic Disorder A relatively mild but chronic form of
depression Can last for months or years More common in women

Bipolar Disorders
Characterized by alternating moods that shift between euphoric feelings and depression.
There are two major types: (1) Bipolar disorder (2) Cyclothymic disorder

Bipolar Disorder
Formerly called manic depressionInvolves mood swings that shift between
elevated moods or “euphoria” “manic” episodes and depression.
People with this disorder experience normal moods also. Examples of manic behavior:
Extreme restlessness argumentativenessExcitability lavish spendingTalkativeness reckless drivingTaking on tasks beyond a person’s ability

Bipolar Continued
Mania eventually gives way to depression: Feelings of hopelessness and despair Suicidal feelings
About 1% of the adult population in the U.S. suffers from bipolar disorder.

Cyclothymic Disorder
A mood disorder characterized by milder mood swings than bipolar disorder.
It is about as common as bipolar disorder.

Causes of Mood Disorders
There are several possible causes which may occur separately or together to cause mood disorders:

Biological Causes
Brain chemicals: Neurotransmitters serotonin and norepinephrine may be too low in depressed people.
Genetic factors: There is a family connection
Faulty brain structure and function: Research is being done in this area to see if the structures responsible for emotions, etc. are different in depressed people.

Psychological Factors
Each approach to psychology has a theory of what causes depression. Psychodynamic Theory (Freud) says
depression is the result of anger turned inward against the self.
Learning Theory (Behaviorist) Depression is the result of changes in reinforcement levels.
Cognitive Theory: Says the way people interpret events, and distorted thinking can cause depression.
Learned Helplessness Theory: Says people become depressed when they feel powerless to control aspects of their lives

Mood Disorders-Depression

Mood Disorders-Depression
Canadian depression rates

Mood Disorders- Suicide

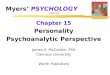
Mood Disorders-Bipolar
PET scans show that brain energy consumption rises and falls with emotional switches
Depressed state Manic state Depressed state

Mood Disorders-Depression
Altering any one component of the chemistry-cognition-mood circuit can alter the others

Mood Disorders-Depression
The vicious cycle of depression can be broken at any point

Somatoform Disorders

Somatoform Disorders
Physical symptoms for which there is no apparent physical cause.

Sick Role
Have you ever “played sick” in order to get out of something? How did that work out (did you get what you wanted)?
Sick attention (friends, family, medical) = secondary gains
Likely link between secondary gains and somatoform disorders
Some medical condition may actually exist

Types of Somatoform Disorders
1. Somatization Disorder Known as “Hysteria,” “hypochondriasis,” and
“melancholia” until 1800’s Term “somatization disorder” was first used in
DSM-III (1980)

Diagnosis
DSM-IV criteria History of many physical complaints beginning before age 30 occurring over several years resulting in treatment being sought or significant impairment in functioning.

Additional info
Primary relationships are with doctors; personal relationships usually have problems
Physical symptoms become part of their identity
This disorder is chronic and rarely goes away completely

Causes of Somatization
Genetic Genetic influence (30-50%) on
somatization symptomsSocial learning Parents may reinforce somatic
complaints in children gain attention (sick role)Societal
More acceptance of medical vs. psychological problems


Types of Somatoform Disorders, cont.
2. Conversion Disorder• Changing emotional difficulties into a loss
of a specific voluntary body function.• Loss of function is real, but no physical
damage is present.• Can be persistent, lasting for years.• Examples: paralysis, loss of sight or
hearing, loss of speech• May free the person from dealing with
difficult emotional situations.

Dissociative Disorders

Dissociative Disorders
Involve disruption in the usually integrated functions of consciousness, memory, identity, or perception of the environment
What are some “normal” dissociative experiences that people have sometimes? You dissociate sometimes when you “space
out” while driving, reading, watching t.v., etc.

Dissociative Identity Disorder (DID)
Formerly known as multiple personality disorder
DSM-IV criteriaA. presence of 2 or more distinct identities or personality statesB. At least 2 identities/personalities recurrently take control of the person’s behavior

DSM-IV criteria (cont.)
C. Inability to recall important personal information (goes beyond ordinary forgetfulness)D. Not due to effects of a substance; in children, symptoms not attributable to imaginary playmates or fantasy play

Additional descriptive info
Alter = identity or personality in DID Many have at least 1 impulsive alter Alters of the opposite gender are
common
Switch = transition to another identity

DID (cont.)
- more common among women
- number of identities varies:- women average about 15- men average about 8
- dissociation can be spurred by stress

DID (cont.)
Causes- almost every DID case has history of severe sexual or physical abuse dissociation seems to be a defense
- may be extreme form of PTSD- biological influences not clear
- very few twin studies suggest environment is more influential
than genes

Causes (cont.)
Most are highly suggestible; easily hypnotized

DID (cont.)
Treatment- similar to treatment of PTSD
- exposure to traumatic memories; goal is desensitization and prevention of response (dissociation)

Other Dissociative Disorders
Dissociative Amnesia: the inability to recall important personal events or information; is usually associated with stressful events
Dissociative Fugue: a person suddenly travels away from home or work and is unable to recall the past

Summary
Somatoform disorders involve a focus on physical symptoms that are either not real or are exaggerated
Dissociative disorders involve a disturbance in normally integrated functions (memory, identity, etc.)
Course is usually chronicCauses for most are unknown

Dissociative Disorders
Dissociative Disorders conscious awareness becomes separated
(dissociated) from previous memories, thoughts, and feelings
Dissociative Identity Disorder rare dissociative disorder in which a
person exhibits two or more distinct and alternating personalities
formerly called multiple personality disorder

Schizophrenia
Schizophrenia literal translation “split mind” a group of severe disorders
characterized by: disorganized and delusional thinking disturbed perceptions inappropriate emotions and actions

Schizophrenia
Delusions false beliefs, often of persecution
or grandeur, that may accompany psychotic disorders
Hallucinations sensory experiences without
sensory stimulation

Schizophrenia
A thought Disorder

Schizophrenia
It is a disease that affects 1% of the world’s population
It has more impact on urban people than rural people
It is a disease that affects men and women equally
It is a disease of the brain

Schizophrenia is not caused by:
Inadequate parenting Overzealous mothers Poor family relations It is not split personality

Schizophrenia and Genetics
70% of persons who develop schizophrenia have a genetic basis for it. Usually, there is a relative who has the disease.
The closer in relation to the ill person, the more likely one is to get the disease.

Schizophrenia and Genetics
If you have an identical twin who has schizophrenia, you have a 50% chance of developing schizophrenia.

Schizophrenia: Three Types
Paranoid typeCatatonic typeDisorganized type

Paranoid Schizophrenia: the affected person may:
Talk to himself Gesture to himself Become preoccupied with idea that he/she is
being followed or watchedHear voices (possibly from “the devil” or “God”)Develop elaborate delusions and believe
outrageous things (such as aliens from another planet have invaded his/her body).

Paranoid Schizophrenia: the affected person may:
See things like dark figures, bugs or spotsFeel people are out to get them Believe in all sorts of conspiracies Have ideas that no amount of evidence to
the contrary can dislodge

Catatonic Schizophrenia: the affected person may:
Seem almost frozen and unable to move at times
Stop talking or greatly reduce conversation Appear lazy, unmotivated and uninterested
“out of it”Become completely detached from reality
and have no sense of anything going on around them.

Disorganized Schizophrenia: the affected person may:
Talk in jumbled sentencesBe essentially incoherent in their
speechSuffer from an inability to keep track
of his/her thought processes and will jump from subject to subject
Become detached from what is happening around them

Schizophrenia is often described in terms of positive (not meaning good) and negative (not meaning bad) symptoms
Positive symptoms include delusions and hallucinations
Negative symptoms are the loss or absence of normal traits or abilities, and include flat affect and emotion, and lack of motivation.
A third symptom grouping, the disorganization syndrome, includes chaotic speech, thought, and behavior.

Schizophrenia treatment
BiologicalPsychologicalSocial

Schizophrenia Treatment: Biological
Medications called antipsychotic (not “antischizophrenic”) they deal with some of the symptoms
delusions, hallucinations, disorganized behaviorThese drugs work by blocking dopamine receptors
in the brain.

Schizophrenia Treatment: Psychological
Patients will need therapy supportive “digging deep” can help some, but that is the
exception, not the rule

Schizophrenia Treatment: Psychological
Those who have family benefit most from families who: are informed about the illness have support Have skills to deal with the ill family member

Schizophrenia Treatment: Psychological
Family member skills: low key low demand use simple sentences able to ignore the inconsequential features of the
illness are able to respond to dangerous behavior can accept that their ill family member may never
be like he once was

Schizophrenia Treatment: Social
Rehabilitation Social skills training Vocational assistanceEnvironmental modification
reduce stimuli

Schizophrenia

Schizophrenia

PERSONALITY DISORDERS
A class of psychological disorders characterized by rigid personality traits that impair people’s ability to adjust to the demands they face in the environment and that interfere with their relationships with others.

Cluster A (odd, eccentric) personality disorders

PARANOID PERSONALITY DISORDER
High levels of suspiciousness of the motives and intentions of others
No paranoid delusions as in schizophreniaBelief that others are lying, cheating,
exploiting or trying to harm youPerception of hidden, malicious meaning
in benign comments

SCHIZOID PERSONALITY DISORDER
Shallow or blunted emotionsFantasizingExtreme introversionEmotional distance, even from family
membersFixation on your own thoughts and
feelings

SCHIZOTYPAL PERSONALITY DISORDER
Holding beliefs or showing behaviors that are odd or peculiar but not clearly psychotic
"Magical thinking" — the idea that you can influence people and events with your thoughts
Odd, elaborate style of dressing, speaking and interacting with others

Signs and symptoms of cluster B (dramatic, emotional) personality disorders

ANTISOCIAL PERSONALITY DISORDER
Callous treatment of othersLack of remorse for wrongdoingChronic irresponsibility and unreliabilityLack of regard for the law and for others'
rightsPersistent lying and stealingAggressive, often violent behaviorLack of remorse for hurting othersLack of concern for the safety of yourself
and others

BORDERLINE PERSONALITY DISORDER
A failure to develop a stable self- imageDifficulty controlling emotions or
impulsesFrequent, dramatic changes in mood,
opinions and plansStormy relationships involving frequent,
intense anger and possibly physical fights
Feeling of emptiness insideSuicide attempts or self-mutilation

HISTRIONIC PERSONALITY DISORDER
Dramatic and emotional behaviorExcessive demands to be the center of
attentionExcessive needs for reassurance, praise
and approvalAttention-grabbing, often sexually
provocative clothing and behaviorExcessive concern with your physical
appearanceFalse sense of intimacy with others

NARCISSISTIC PERSONALITY DISORDER
Excessive need for admirationInflated sense of — and preoccupation with —
your importance, achievements and talentsConstant attention-grabbing and admiration-
seeking behaviorInability to empathize with othersExcessive anger or shame in response to
criticismManipulation of others to further your own
desires

Signs and symptoms of cluster C (anxious, fearful) personality disorders

AVOIDANT PERSONALITY DISORDER
Pattern of avoiding social relationships out of fear of rejection
Hypersensitivity to criticism or rejection
Self-imposed social isolationExtreme shyness in social situations,
though you strongly desire close relationships

DEPENDENT PERSONALITY DISORDER
Excessive dependence on others to meet your physical and emotional needs
Tolerance of poor, even abusive treatment in order to stay in relationships
Unwillingness to independently voice opinions, make decisions or initiate activities
Intense fear of being aloneUrgent need to start a new relationship when one
has ended

OBSESSIVE-COMPULSIVE PERSONALITY DISORDER
Rigid ways of relating to others Excessive concern with order, rules, schedules and lists Perfectionism, often so pronounced that you can't complete
tasks because your standards are impossible to meet Inability to throw out even broken, worthless objects Inability to share responsibility with others Inflexibility about the "right" ethics, ideas and methods Compulsive devotion to work at the expense of recreation and
relationships Financial stinginess Discomfort with emotions and aspects of personal relationships
that you can't control
Obsessive-compulsive personality disorder is not the same as obsessive-compulsive disorder, an anxiety disorder that shares some symptoms but is more extreme and disabling.

Mood Disorders-Depression
Boys who were later convicted of a crime showed relatively low arousal

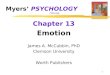
Personality Disorders PET scans illustrate reduced activation in a
murderer’s frontal cortexNormal Murderer

Rates of Psychological Disorders