Embed Size (px)
Citation preview

Review
10.1586/14779072.3.6.1035 © 2005 Future Drugs Ltd ISSN 1477-9072 1035www.future-drugs.com
Myocardial protection in reperfusion with postconditioningJakob Vinten-Johansen†, Zhi-Qing Zhao , Rong Jiang and Amanda J Zatta
†Author for correspondenceCarlyle Fraser Heart Center, Cardiothoracic Research Laboratory,Carlyle Fraser Heart Center of Emory Crawford Long Hospital,550 Peachtree Street NE Atlanta, GA 30308-2225, USATel.: +1 404 686 2511Fax: +1 404 686 [email protected]
KEYWORDS: apoptosis, ischemia, myocardial infarction, postconditioning, reperfusion, reperfusion injury, survival kinases
Reperfusion is the definitive treatment for coronary occlusive disease. However, reperfusion carries the potential to exacerbate lethal injury, termed ‘reperfusion injury’. Studies have suggested that reperfusion injury events are triggered during the early moments of reflow, and determine, in part, the severity of downstream manifestations of postischemic injury, including endothelial dysfunction, infarction and apoptosis. The application of brief iterative episodes of reflow (reoxygenation) and reocclusion (ischemia, hypoxia) at the immediate onset of reperfusion, which has been termed ‘postconditioning’ by the authors, reduces many manifestations of postischemic injury, notably infarct size, apoptosis, coronary vascular endothelial injury and reperfusion arrhythmias. Cardioprotection with postconditioning has been reported to be comparable with that observed using the gold standard maneuver ischemic preconditioning. In contrast to preconditioning, which exerts its effects primarily during the index ischemia, postconditioning appears to exert its effects during reperfusion alone. Postconditioning modifies the early phase of reperfusion in ways that are just beginning to be understood. It appears to first: reduce the oxidant burden and consequent oxidant-induced injury; secondly, attenuate the local inflammatory response to reperfusion; and thirdly, engage end effectors and signaling pathways implicated in other cardioprotective maneuvers, such as ischemic and pharmacologic preconditioning. Postconditioning seems to trigger the upregulation of survival kinases principally known to attenuate the pathogenesis of apoptosis and possibly necrosis. The postconditioning phenomenon has been reproduced by a number of independent laboratories and has been observed in both large and small animal in vivo models, as well as in ex vivo and cell culture models. In contrast to preconditioning, postconditioning may have widespread clinical application because it can be applied during reperfusion at the point of service for angioplasty, stenting, cardiac surgery and organ transplantation.
Expert Rev. Cardiovasc. Ther. 3(6), 1035–1045 (2005)
There were 1,121,000 angioplasties per-formed in the USA alone in 2002. Currently,primary angioplasty and placement of stentsis the therapy of choice to open blocked cor-onary arteries. This reflects the primary strat-egy of initiating reperfusion in as timely amanner as possible, as time to reperfusion isa primary determinant of mortality and effi-cacy. Reperfusion is the definitive treatmentfor coronary occlusive disease leading toacute myocardial infarction. Reperfusionlimits myocardial infarct size by interruptingthe ischemia, which would otherwiseprogress in a wave-front pattern, starting at
the subendocardium and eventually encom-passing the transmural area at risk (AAR) [1].Reperfusion can be achieved in the catheteri-zation laboratory using intravenous deliveryof thrombolytic therapy (tissue plasminogenactivator, urokinase and streptokinase) aloneor in conjunction with catheter-based tech-nology, such as percutaneous transluminalcoronary angioplasty (PTCA), with or with-out stents. Successful reperfusion is achievedin acutely occluded coronary arteries in80–95% of cases. The salvage of myo-cardium by timely reperfusion is associatedwith smaller infarct sizes and less enzyme
CONTENTS
Cardioprotection by postconditioning
Mechanisms of postconditioning
Clinical application of postconditioning
Summary & conclusions
Five-year view
Expert commentary
Key issues
References
Affiliations
For reprint orders, please contact [email protected]

Vinten-Johansen, Zhao, Jiang & Zatta
1036 Expert Rev. Cardiovasc. Ther. 3(6), (2005)
release, better global ventricular function, lower morbidityand mortality and a greater chance of return to an acceptablelifestyle for the patient. In addition, early reperfusion reducesthe consequences of a second ischemic event, which occurs in18% of men and 35% of women suffering a first-time heartattack. These data suggest that the catheterization laboratoryin which reperfusion is achieved is an effective setting inwhich to initiate therapies designed to salvage myocardiumagainst postischemic injury.
Although early reperfusion limits infarct size relative to per-manent occlusion or medical therapy, the process of reper-fusion of coronary arteries is now recognized from manyexperimental studies as contributing to postischemic injury ofthe myocardium, namely, reperfusion injury [2–7]. Reperfusioninjury expresses a broad range of injury pathologies, asdescribed hereafter. Reperfusion injury has been recognized inclinical cardiac surgery for many years. Clinical studies suggestthat reperfusion injury also occurs in the catheter-labsetting [8]. This reperfusion injury begins in the early momentsafter onset of reflow by angioplasty (with or without stents),and has the effect of offsetting the clinical advantage of reduc-ing infarct size by initiating timely reperfusion alone [9,10].New data show that the first few minutes of reperfusion repre-sent an active time of damage, and an absolutely critical win-dow for the effective application of reperfusion therapy [11–14].The discussion on postconditioning that follows will reinforcethe importance of the early stages of reperfusion with regardsto postischemic outcomes.
Reperfusion injury has a complex etiology. The primarymechanisms attributed to triggering reperfusion injury in theearly minutes of reflow are reactive oxygen species (ROS),intracellular calcium overload and a local inflammatoryresponse, in which the interaction between neutrophils andcoronary vascular (arterial and venous) endothelium plays acentral role. The generation of ROS has been observed tooccur within the first minutes [15], and even seconds [16], ofmyocardial reperfusion. These ROS are generated by anumber of sources, including activated neutrophils, cardio-myocytes and activated coronary vascular endothelium. Neu-trophils generate ROS principally through the NADPH oxi-dase system, which converts molecular oxygen to superoxideanions. The generation of ROS also occurs in reperfused tis-sue during sustained reperfusion, even hours and days afterthe onset of reflow. ROS can also be generated by activatedendothelial cells by several enzymes including the endothelialNAD(P)H oxidase, xanthine oxidase and endothelial nitricoxide synthase (eNOS) (under some conditions).
Calcium overload is also an early event during reperfusion.The exquisite control that the cell normally exerts on the steepcalcium gradient is compromized during ischemia, such thatlimited calcium may enter the cell during short-term ischemia.However, with the renewal of interstitial calcium levels duringreperfusion, the gradient overwhelms the cell’s calcium regula-tory system and intracellular calcium increases. Intracellular cal-cium accumulation and dyshomeostasis leads to mitochondrial
dysfunction, activation of calcium-sensitive enzyme systems andhypercontracture of the ischemic reperfused myocardium,marked by a sustained shortening and stiffening of the myo-cardium during the early moments of reperfusion [17–20]. BothROS and calcium overload events have been linked to thepathogenesis of necrosis.
The local inflammatory component of reperfusion injury issimilar to that engaged during shock and sepsis [21]. Oxidantsand cytokines released during the early moments of reperfusionactivate both neutrophils and endothelium, leading to the adhe-sion and accumulation of neutrophils on the vascular endo-thelial surface. This adhesion, and the subsequent rapid releaseof oxidants and other noxious agents, has not only been associ-ated with endothelial dysfunction, but some studies also suggestthat these early events may ultimately contribute to necrosis andapoptosis. Although ROS have been linked to reversible (stun-ning) and irreversible (necrosis and apoptosis) myocardialinjury, the link between neutrophils and tissue injury afterischemia-reperfusion (I/R) (via ROS, other oxidants, proteasesand cytokines) is not as clear [10,22]. The observation that reper-fusion injury is observed in models not involving neutrophilssuggests that either neutrophils are not a source of injury, or thatthere are neutrophil-dependent and -independent componentsof reperfusion injury.
A number of studies suggest that the ‘end effector’ of reper-fusion injury, namely, the event that deals the final blow to thecardiomyocytes and supporting tissue (i.e., vascular endothelium),is the mitochondrial permeability transition pore (mPTP). ThemPTP is a nonspecific pore localized in the mitochondrial innermembrane. Normally, this pore is closed, which prevents theinflux of water and small molecules into the mitochondrion. Anincrease in oxidants and/or cytosolic calcium, both of which occurduring early reperfusion, stimulates the mPTP to open. Thisopening of the mPTP disrupts the permeability characteristics ofthe mitochondrial membrane, leading to an influx of usuallyimpermeable proteins, with subsequent mitochondrial swelling, abreakdown in the proton gradient and uncoupling of oxidativephosphorylation, and release of the proapoptotic factorscytochrome c and apoptosis-inducing factor. The opening of themPTP during the early minutes of reperfusion has been linked tothe pathogenesis of both necrosis and apoptosis, and may be a keyfactor in the transition from reversible to irreversible celldeath [23,24].
These early reperfusion events cause injury during the acutephase of reperfusion, but can also trigger events, such asincreased capillary permeability, edema, no-reflow, necrosis andapoptosis, which may be either expressed later or undergo pro-gressive exacerbation. In addition, the events described aboveare not mutually exclusive, but rather they form a cooperativeresponse to reperfusion. Hence, the response to reperfusion isvery complex, and such a broad spectrum response to the stressassociated with I/R may require an equally broad spectrumtherapeutic approach [10]. Certainly, the events that first occurin the chronology of reperfusion injury must be targeted first asstated by Piper [9].

Myocardial protection with postconditioning
www.future-drugs.com 1037
One important question is whether there is a need for myocar-dial protection in the setting of acute myocardial infarction. Strat-egies to reduce mortality, morbidity and infarction, and to restoreglobal function in the setting of acute myocardial infarction, havecentered on restoring blood flow in a timely manner. Thrombo-lytic therapy and timely reperfusion achieved by percutaneousintervention has been the standard of care to date. Recentadvances in therapeutic strategies has maintained the focus on tar-get vessel patency with aspirin, low-molecularweight heparin andantiplatelet (glycoprotein IIb/IIIa receptor inhibitors) agents [25].Although these approaches may limit the duration of ischemiaand the no-reflow phenomenon, they do not address the mecha-nisms of reperfusion injury already described. The concept ofmodifying the conditions (hypothermia and gentle reperfusion)and composition (hypocalcemia, metabolic substrates, pH con-trol and drugs) of the initial reperfusate adopted long ago by car-diac surgeons may prove a useful addition to the cardiologists’armamentarium by actively intervening in the mechanisms ofreperfusion injury. However, this concept has yet to take hold inreperfusion in the catheterization laboratory setting. This strategyof reperfusion therapeutics could synergize with current strategiesof maintaining blood flow and coronary artery patency. The car-dioprotective maneuver of postconditioning, described hereafter,is a novel and potentially clinically applicable addition to thereperfusion therapy armamentarium.
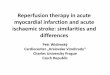
Cardioprotection by postconditioningPostconditioning is defined as a series of brief, iterative interrup-tions in coronary artery reperfusion applied at the immediateonset of reperfusion. The reflow during this postconditioningmaneuver therefore resembles a ‘stuttering pattern’, as depicted inFIGURE 1. The ‘bursts’ of reflow and subsequent occlusive inter-ruptions last for a matter of seconds, ranging from 30-s intervalsin larger animal models [11,14] to 10-s intervals in smaller rodentmodels. This maneuver therefore appears to be a simplistic mod-ification of the hydrodynamics of early reperfusion, but it triggerscomplex, and as yet unknown, biologic and molecular cascadesin the myocardium, as described hereafter.
The moniker of ‘ischemic postconditioning’ was initiallyadopted because the intermittent reocclusion–reperfusion eventswere applied after the index ischemia, and this technique wastherefore positioned conceptually opposite to ‘preconditioning’,in which the I/R sequences are applied before the index ischemia.Since the initial report by Zhao and colleagues, has been droppedfrom the authors’ laboratory, the reference to ischemic postcondi-tioning because it is unclear whether the cardioprotection isdependent on either intermittent ischemia or reperfusion [11].There is also the question of whether a ‘conditioning’ is actuallyimposed physiologically speaking. However, the recognition thatbiochemical events and molecular signaling are taking place dur-ing the early minutes of reperfusion that may attenuate both theearly and later events of reperfusion injury, leads to the idea that aconditioning-like response against early reperfusion events maybe taking place (i.e., the triggering of survival kinases and openingof KATP channels and closing of mitochondrial pores).
The major and more obvious differentiator between pre- andpostconditioning is that preconditioning can exert protectionduring both ischemia and reperfusion, whereas post-conditioning exerts its cardioprotective effects only duringreperfusion. This simple difference implies important varia-tions in the biology and clinical applicability of the two strate-gies. Although variously referred to as ‘stutter reperfusion’ [26],‘old wine in a new bottle’ [27] and the ‘emperor’s newclothes’ [28], the name postconditioning is likely to be debatedfor some time, but it has certainly drawn attention to reper-fusion events and biology and their potential attenuation by‘reperfusion therapies’.
Zhao and coworkers first demonstrated, in a canine modelof 60-min coronary artery occlusion and 3-h reperfusion, thatpostconditioning reduced myocardial infarct size comparedwith a control group with no intervention at reperfusion [11].Postconditioning by three 30-s cycles of alternating left ante-rior descending (LAD) reperfusion and ischemia (reocclusion)applied before full reperfusion-reduced infarct size by approxi-mately 50% relative to the control group; this infarct sizereduction was similar to that achieved by ischemic pre-conditioning of a single 5-min occlusion and 10-min reper-fusion cycle preceding the index coronary occlusion (FIGURE 2).Zhao and colleagues also noted that postconditioning reduced
Figure 1. Mean left anterior descending (LAD )coronary artery blood flow in the acute canine model of 60 min LAD occlusion and 3 h of reperfusion during baseline, LAD occlusion and either abrupt reperfusion (panel A noted as full reperfusion) or reperfusion following a postconditioning (postcon) algorithm of 30 reperfusion (rep), 30 s reocclusion repeated for three cycles (panel B). The representation of the duration of LAD occlusion has been shortened (hatch marks).
Blo
od fl
ow (
ml/m
in)
300
250
200
150
100
50
0
Baseline
Occlusion
Fullrep
A
Blo
od fl
ow (
ml/m
in)
0
50
100
150
200
250
300
Baseline
Occlusion
Postcon
30 s
Fullrep
B

Vinten-Johansen, Zhao, Jiang & Zatta
1038 Expert Rev. Cardiovasc. Ther. 3(6), (2005)
neutrophil accumulation (myeloperoxidase activity) and tissueedema in the area of the myocardium at risk, and attenuatedboth P-selectin expression (a measure of vascular endothelialcell activation) and vasoreactivity (endothelial cell function) inthe ischemic-reperfused LAD [11]. In addition, post-conditioning resulted in the production of attenuated super-oxide radicals (assessed by dihydroethidium staining) in thereperfused myocardium, as well as production of lipid perox-ide product malondialdehyde, suggesting a reduction in oxi-dant burden and oxidant-mediated injury. As with infarct size,these outcomes after postconditioning mirrored the cardio-protection observed with the gold standard ischemic pre-conditioning. These results were recapitulated by a subsequentstudy by Halkos and colleagues, which showed, additionally,that postconditioning reduced reperfusion arrhythmias to asimilar or slightly greater extent than preconditioning [14].
The question that naturally arises is whether the first min-utes during which postconditioning is applied are critical forprotection. Kin and coworkers addressed this question in a ratmodel of myocardial infarction induced by 30 min of left cor-onary artery occlusion followed by 3 h of reperfusion [12]. Inthe rat model, the time course of the postconditioningsequences is reduced to 10 s of reperfusion and 10 s of reocclu-sion, repeated for either three or six cycles; either number ofcycles gives the same degree of infarct-sparing effect in thismodel. Accordingly, postconditioning was applied during thefirst 1 min (three cycles) to 2 min (six cycles) of reperfusion.As shown in FIGURE 3, the infarct-sparing effect of postcondi-tioning was lost when the three-cycle maneuver was delayedfor 1 min of reperfusion. A similar loss of cardioprotectionwhen postconditioning was delayed was later observed by Yangand coworkers in an in situ rabbit coronary artery occlusion-reperfusion model, using a delay of 10 min [29]. The reductionin oxidant generation in reperfused myocardium and the lipidperoxidation products of oxidant-mediated membrane damage
observed with postconditioning by Kin and colleagues was alsolost when the postconditioning algorithm was delayed for1 min [12]. Still, it is not clear whether oxidants are a pedestrianmarker of less damage or a causative player in protection bypostconditioning. Therefore, the biochemical or moleculareffects engaged by postconditioning occur during a very nar-row window of time, and potentially target the early compo-nents of reperfusion injury described previously. Hence, post-conditioning may act as a trigger for early or latecardioprotective responses, which ultimately lead to a reduc-tion of injury to cardiomyocytes (necrosis and apoptosis [30,31])and coronary artery endothelium.
In addition to infarction and endothelial dysfunction, apopto-sis in myocardium has been suggested to be primarily triggeredby reperfusion [32,33]. Apoptosis may be triggered by pro-inflammatory signals, such as tumor necrosis factor (TNF)-α, orby oxidants ostensibly generated during reperfusion. There havebeen no full-length studies on the effects of postconditioning onapoptosis in the ischemic-reperfused heart. However, Zhao andcolleagues reported in abstract form that ‘hypoxic’ post-conditioning of neonatal cardiomyocytes in vitro reduced apop-tosis detected by terminal deoxynucleotidyl-mediated dUTPNick End Labeling (TUNEL) assay, appearance of DNA ‘lad-ders’ and caspase-3 and -8. Relative to hypoxia-reoxygenationcontrols, the antiapoptotic Bcl-2 was not augmented, but theproapoptotic protein Bax was reduced by hypoxic post-conditioning. TNF-α levels in the culture medium were reducedin the postconditioning group. Taken together with the reduc-tion in oxidant generation discussed above, these observationswould suggest that postconditioning attenuates the triggers ofapoptosis, in addition to altering the balance of regulatory pro-teins to favor an anti-apoptotic state. However, these in vitroobservations should be investigated in in vivo models of I/R.
Mechanisms of postconditioningThe studies discussed so far provide some insight into thenature of cardioprotection by postconditioning, in that thisvery brief intervention protected against downstream physio-logic outcomes, such as coronary vascular endothelial dysfunc-tion, apoptosis and necrosis, and that the number of cyclesimposed at the onset of reflow was not as important as theirimmediate application at the onset of reperfusion. However,the trigger of this protection was unknown. Two laboratoriesindependently investigated the involvement of endogenousadenosine; this was not a far-fetched hypothesis, as adenosine islinked with the cardioprotection of preconditioning [35–37] andhas potent anti-inflammatory properties specifically relevant toreperfusion [38–40]. Indeed, endogenous adenosine released dur-ing coronary occlusion-reperfusion is sufficient to conferinfarct-size modulation during reperfusion via activation of theA2A, but not the A1, receptors [41]. Kin and colleagues observedin isolated mouse hearts subjected to 20-min global ischemiaand 30-min of reperfusion with or without postconditioning(six cycles of 10 s of ischemia and reperfusion) that post-conditioning delayed the washout of adenosine in coronary
Figure 2. Area at risk (AAR) as a percentage of left ventricular (LV) mass and infarct size (mass of area of necrosis, [An] within the AAR) are shown for vehicle controls, post conditioning (postcon) and preconditioning (precon) groups from anesthetized canine model of 60 min LAD-occlusion and 3 h of reperfusion. The 30 s reperfusion-reocclusion algorithm of postconditioning was followed.*p < 0.05 versus vehicle control group.Modified from Zhao and colleagues [11].
AAR/LV An/AAR
Per
cent
05
10
1520
25
3035
**
VehiclePost-conPre-con

Myocardial protection with postconditioning
www.future-drugs.com 1039
venous effluent during the intervention (FIGURE 4) without alter-ing the total purine content during reperfusion, thereby sug-gesting that adenosine was retained ostensibly in the intravascu-lar space where it can exert cardioprotection [13,42,43]. Kin andcoworkers then investigated whether there was a functional linkbetween adenosine receptor activation and the infarct-sparingeffect of postconditioning [42]. In rats, the cardioprotection ofpostconditioning was abrogated by 8-p-sulphenyl-theophylline(8-SPT), a general adenosine receptor blocker. In addition, theinfarct-sparing effect of postconditioning was abrogated byZM241385 (selective A2A receptor antagonist) or MRS1523 (aselective A3 receptor antagonist), all given 5 min before reper-fusion (FIGURE 5). However, infarct size reduction by postcondi-tioning was not abrogated by 8-cyclopentyl-1,3-dipropylxan-thine (DPCPX) (a selective A1 receptor antagonist) given 5 minbefore reperfusion. These data indicate that:
• Postconditioning delays the washout of intravascular adenos-ine during early reperfusion, which may potentiate adenosinereceptor activation
• The A2A and/or the A3 receptor is primarily involved
It is noteworthy that these data are consistent with thewell-known cardioprotective effects of adenosine whenadministered at the onset of reperfusion. These data are con-sistent with a report from Yang and colleagues, which sug-gested a functional role for adenosine receptor activation [44].Other conventional (ligand) triggers of cardioprotection,whether associated with preconditioning or not, have yet tobe linked with postconditioning’s cardioprotection at thetime of writing.
Nitric oxide (NO) is a radical species that is derived from thebioconversion of L-arginine by nitric oxide synthase (NOS).NO is tonically released from normal endothelial cells by theendothelial NOS isoforms, eNOS, but is also released bycardiomyocytes [45]. NO has been demonstrated to be cardio-protective when released or supplemented during early reper-fusion [46,47], and deleterious when released in overabundancelater after cardiopulmonary bypass via inducible NOS. In addi-tion, NO quenches superoxide anions in a very rapid biradicalreaction, that in effect removes this oxidant from the intra- orextracellular environment. However, the product of this reac-tion, peroxynitrite, may itself be an oxidant under some condi-tions. NO also acts as an intracellular signal in both classical anddelayed preconditioning [48], in which it may inhibit the open-ing of the mPTP and thereby inhibit necrosis and apoptosis.The tonic release of NO by vascular endothelium is impairedspecifically during early reperfusion, which then reduces inher-ent inhibition of neutrophils. It is thought that this loss of NOis a major mechanism in recruiting neutrophils to postischemicmyocardium, and thereby initiates the local inflammatoryresponse to reperfusion [49]. NO has also recently been impli-cated as a mechanism in the infarct size reduction ofpostconditioning [44]. In isolated perfused rat hearts, eNOS(phosphor-eNOS) is increased by postconditioning [50]. Accord-ingly, inhibition of NOS with Nω-nitro-L-arginine methyl ester
(L-NAME) abrogated the infarct-sparing effects of post-conditioning. NO activates guanylyl cyclase and increases cyclicguanosine 3´,5´-cyclic monophosphate (GMP) formation,which stimulates protein kinase G and mediates many of thephysiologic effects of NO. Commensurate with this NO–guan-ylate cyclase pathway, the infusion of the guanylyl cyclase inhib-itor 1H-[1,2,4]oxadiasole[4,3-a]quinoxalin-1-one (ODQ) alsoabrogated the infarct-reducing effects of postconditioning [44,51].
Figure 3. Area at risk (AAR) as a percentage of left ventricular (LV) mass and infarct size (percentage area of necrosis [AN] relative to the AAR) in the in vivo rat ischemia-reperfusion model of 30 min left coronary artery occlusion and 3 h of reperfusion. Postconditioning was achieved by either three or six cycles of 10 s reperfusion and reocclusion of the left coronary artery. A 1 minute delay of the post conditioning algorithm (delayed group) reversed the infarct-sparing effects of postconditioning.*p < 0.06 versus control, in which reperfusion was begun abruptly.IPC: Ischemic preconditioning of 5 min occlusion and 10 min reperfusion before index ischemia.
AAR/LV AN/AAR
0
10
20
30
40
50
60
Perc
ent 3 cycles
IPC
Control 6 cycles
Delayed
*
* *
Figure 4. Effect of postconditioning on adenosine concentration in coronary venus effluent in isolated perfused mouse hearts during reperfusion following normothermic global ischemia. The postconditioning algorithm was 10 s reperfusion followed by 10 s global ischemia, repeated for either three or six cycles. The concentration pattern may reflect retention of adenosine and potential differeneces in washout during early reperfusion. Note that the appearence of adenosine in coronary venous effluent buffer of control untreated hearts occurs within the first minute of reperfusion collection time, peaks between 2 and 3 min and decreases thereafter. With either three or six cycles of postconditioning during the onset of reperfusion, coronary venous effluent adenosine concentration is significantly decreased during the first 2 min of reperfusion, coincident with postconditioning. All values are means ± standard error of the mea.*p < 0.05 versus control hearts.Ado: Adenosinee; Rep: Reperfusion; Occ: Global ischemia.
Reperfusion (min)0 2 4 6 8 10
0
50
100
150
200
250
Ext
race
llula
r A
do(n
M/m
in/g
)
*
*
**
Control10 Rep/10 Occ x310 Rep/10 Occ x6

Vinten-Johansen, Zhao, Jiang & Zatta
1040 Expert Rev. Cardiovasc. Ther. 3(6), (2005)
Therefore, postconditioning may preserve NO generation byprotecting intracellular sources and/or by protecting the vascularendothelium as a source of NO, although NO levels have notbeen directly measured after postconditioning. Indeed, theobservation that NO concentrations increase during the firstminutes of reperfusion makes this hypothesis feasible [52]. Theprotection of the coronary vascular endothelium [11,14], which isrelated to preserved function of the L-arginine-NO pathway, by
postconditioning is consistent with preser-vation of NO release. However, at thistime, it is not clear whether NO serves anintracellular signaling function, exertsextracellular inhibitory actions on theinflammatory response, or both.
Some evidence suggests that the cardio-protection conferred by postconditioning isrelated to a reduction in the oxidant andproinflammatory responses to reperfusion.As reviewed previously, oxidants andinflammatory mediators may play a causa-tive role in reperfusion-inducedinjury [2,53], although this hypothesis ishighly controversial. Indeed, reperfusion-induced injury has been observed in theabsence of neutrophils, and cardioprotec-tion by postconditioning has been observedin neutrophil-free cell culture [30] and bufferperfused hearts [26,44,51]. These observationsmay suggest that there are neutrophil-dependent as well as -independent mecha-nisms of injury. However, it is currentlyunknown whether oxidants or other nox-ious agents released by neutrophils are theinjurious culprits. There are other cellularsources of these products; certainly the cor-onary vascular endothelium is a rich sourceof both oxidants and proinflammatorycytokines. However, as discussed in moredetail hereafter, some endogenous autacoidsinvolved in postconditioning are alsopotent inhibitors of neutrophil activation.
Regarding the role of oxidants(regardless of cellular source), post-conditioning was reported by Sun andcolleagues to reduce the oxidant burdenin vitro [54], in accordance with theobservations and hypothesis originallyproposed in the in vivo study by Zhaoand coworkers [11]. In neonatal cardio-myocytes, a decrease in cell injurymarker (lactate dehydrogenase leakage)hypoxic postconditioning was associatedwith a reduction in superoxide radicaland hydrogen peroxide generation afterreoxygenation, commensurate with a
significant reduction in oxidant product formation (e.g., thelipid peroxide product malondialdehyde). The recent studyby Serviddio and colleagues, in which a brief hypoxic ‘post-conditioning’ period preceding full reperfusion in isolatedhearts reduced mitochondrial peroxide and carbonyl proteingeneration and glutathione oxidation, lends support to theconcept that postconditioning reduces oxidantgeneration [55]. However, it remains to be determined if the
Figure 5. Effect of adenosine receptor blockers on the infarct-sparing effects of postconditioning. (A) Shows the effects of nonselective adenosine receptor (AR) antagonist, 8-SPT (10 mg/kg) or A1AR inhibitor, DPCPX (0.1 mg/kg), in the absence or presence of postconditioning. (B) Shows the effects of the A2AAR blocker, ZM241385 (0.2 mg/kg) or A3AR blockers, MRS1523 (2 mg/kg) in the absence or presence of postconditioning. All values are means ± standard error ofthe mean.*p < 0.05 versus control group; † p < 0.05 versus postconditioning alone. DPCPX: ; Post: ; 8-SPT: 8-p-sulphenyl-theophylline.
AN
/AA
R (
%)
30
40
50
60
Contro
l
Vehic
lePos
t8-
spt
DPCPXPos
t +
8-SPT
Post +
DPCPX
AN
/AA
R (
%)
30
40
50
60
Contro
l
Vehic
lePos
t
ZM24
1385
MRS15
23
Post +
ZM24
1385
Post +
MRS15
23
*
A
B
†
†
††
†
†
†††
†
†
*
*

Myocardial protection with postconditioning
www.future-drugs.com 1041
reduction of oxidant generation, particularly at early reper-fusion, represents a major cardioprotective mechanism or afootprint of myocardial salvage.
On the other side of this argument, selected cytokines (i.e.,TNF-α), as well as ROS, have been implicated in the signalingpathways that trigger cardioprotection by preconditioning [56].For example, preconditioning transiently increases superoxideanion generation during ischemia, and reduces their genera-tion as a burst during reperfusion (reoxygenation) [57]. As a sig-naling agent, ROS may act by opening the mitochondrial KATPchannel (potentially via activation of PKC), an event associ-ated with cardioprotection. However, ROS may also beinvolved in signaling distal to the opening of the mitochon-drial KATP channel. ROS may be generated by the mitochon-dria at site III of the electron transport chain, which may, inturn, activate survival kinases. These observations suggest thatROS may have a dual role in I/R, that is, the role of mediatorof cellular injury secondary to respiratory bursts of ROS and ofsmaller redox-dependent signals implicated in the induction ofpreconditioning protection before the index ischemia. How-ever, the mechanisms by which ROS are involved in signalingat reperfusion, and whether there is a two-tier effect of ROSspecifically in postconditioning are questions that still remain.
Cohen and Downey [29,44] and others [58] have identifieddownstream mediators of postconditioning, such as KATP chan-nels and the mPTP, the latter of which has been viewed as anearly reperfusion event [59]. Opening of the mitochondrial KATPchannel has been associated to the greatest extent with cardiopro-tection. Studies suggest that phosphorylation and subsequentopening of mitochondrial KATP channels by upstream PKC gen-erates ROS and potentially NO, which can activate downstreamprotective kinases. The open probability of the mPTP can bereduced by intracellular NO and attenuation of oxidants and cal-cium accumulation, as well as by activation of reperfusion injurysurvival kinases (phosphatidylinositol 3 kinase [PI3]-Akt, mitro-gen-induced extracellular kinase [MEK]1/2, extracellular signal-regulated kinase [ERK]1/2). Activation of these pathways seemsto converge on the mPTP to inhibit opening, ostensibly duringreperfusion. Emerging concepts suggest that the mitochondrialKATP channel functions as a modulator of mPTP opening. Theopening of the mitochondrial KATP channel and inhibition ofmPTP opening have both been strongly linked with cardiopro-tection by preconditioning [60–62]. Yang and colleagues reportedthat postconditioning in the rabbit in situ model of coronaryartery occlusion and reperfusion involved the opening of mito-chondrial KATP channels which, when activated (opening ofchannels), protects the heart from I/R injury [29]. Argaud andcoworkers reported in an anesthetized open-chest rabbit modelof coronary artery occlusion and reperfusion that postcondition-ing reduced infarct size and inhibited calcium-induced openingof the mPTP in mitochondria isolated from the area at risk myo-cardium [58]. The attenuation of mPTP opening with post-conditioning was similar to that achieved by preconditioning andby a pharmacologic inhibitor of mPTP opening (NIM811),mPTP opening is triggered by calcium overload or increased
ROS generation. The data reported by Sun and coworkers thatpostconditioning reduced both superoxide generation and cal-cium accumulation in isolated cardiomyocytes [30] lends supportto the inhibition of the mPTP reported by Argaud andcolleagues [58].
Several important molecular signaling mechanisms have beenidentified with myocardial protection from I/R injury. Thep42/p44 ERK1/2 and PI3K-Akt pathways, termed the reper-fusion injury survival kinase (RISK) pathway, are innate cellularsurvival pathways stimulated during I/R. Activation of these pro-survival kinases inhibits proapoptotic pathways, stimulateseNOS and may activate the KATP channel. However, as cell deathby necrosis and apoptosis is still an outcome of I/R injury, theRISK pathway must be overwhelmed by other deleterious mech-anisms, reflecting the complex nature of reperfusion injury.However, recruitment of these pathways and their components atthe time of reperfusion may be an important target in cardiopro-tection through pharmacologic stimulation [63]. The PI3-Aktpathway, for example, stimulates eNOS by phosphorylation,ostensibly increasing NO levels which, as already discussed, caninhibit the mPTP and, in turn, attenuate necrosis or apoptosis.Accordingly, known stimulants of the RISK pathway, such asinsulin (glucose–insulin–potassium), insulin-like growth factor,cardiotropin and the HMG (CoA) reductase inhibitor atorvasta-tin, when given at reperfusion, may reduce infarct size or apopto-sis. Recently, postconditioning has been reported to activatecomponents of the RISK pathway, notably, PI3-Akt. Accord-ingly, inhibitors of PI3K [44,50] and ERK1/2 [29] have been dem-onstrated to abrogate the infarct size reduction of post-conditioning, implicating a functional role for these kinasepathways, although not without some controversy [26]. It is possi-ble that the cardioprotection of postconditioning can beexploited by enhancing the survival kinases.
Clinical application of postconditioningUnlike its predecessor, preconditioning, which is not clinicallyapplicable in the setting of nonsurgical interventions for acutecoronary infarction because it requires a foreknowledge of theischemic event, postconditioning has potential for clinical appli-cation, since it is applied at the onset of reperfusion. In the cathe-terization laboratory setting, one can visualize that the angi-oplasty balloon catheter is introduced into the culprit vessel andthe balloon inflated to open it, but then, instead of initiating fullreperfusion by rapidly deflating and removing the balloon cathe-ter, the interventionist would follow a prescribed algorithm ofinflation–deflation before removing the balloon catheter. Thiswould add only 3–5 min to the overall angioplasty or stentdeployment procedure, which is less than preconditioning algo-rithms. Conceptually, the multiple inflations of angioplasty bal-loons may be implemented as early as in the catheter lab [64].However, as is apparent from the previous discussion, the cardio-protection exerted by this algorithm is sensitive to the infla-tion–deflation duration, and is very sensitive to the immediateimplementation of the algorithm upon reperfusion. Cardiopro-tection can be lost if implementation of the postconditioning

Vinten-Johansen, Zhao, Jiang & Zatta
1042 Expert Rev. Cardiovasc. Ther. 3(6), (2005)
algorithm is delayed. An advantage of the postconditioningmaneuver is that it can be performed with the current ballooncatheters, and requires no additional accessories or expensiveequipment. This is not to say that equipment facilitating thedelivery of the algorithm would not be helpful.
Summary & conclusionsPostconditioning is a maneuver applied immediately follow-ing the onset of reperfusion after myocardial ischemia. Thismaneuver essentially interrupts the reflow process with inter-mittent episodes of ischemia (reocclusion), but under a veryprecise algorithm and without delay during reperfusion.Although this maneuver is seemingly brief and its mecha-nisms not immediately intuitive, postconditioning has beenreported to preserve coronary vascular endothelial function,reduce superoxide radical generation of oxidant-inducedmembrane damage, attenuate reperfusion arrhythmias, andreduce edema, infarct size and apoptosis in the area at risk.The infarct size reduction has now been reported bothacutely, as well as long term (72 h [58]), by several independ-ent laboratories, using several different animal models andin vivo as well as in vitro models. In addition, postcondition-ing has been demonstrated to reduce infarct size in hyperc-holesterolemic models. Mechanisms of cardioprotection maybe related to increasing the exposure of vascular endotheliumin the area at risk to adenosine, increasing the release of NOin intra- or extracellular compartments, or stimulating spe-cific survival kinase pathways. Whatever the mechanism, theprotective mechanisms engaged by postconditioning, such asactivation of KATP channels and inhibiting mPTP opening,are similar to those stimulated by other cardioprotectivemodalities, including preconditioning. The similaritybetween pre- and postconditioning, with regards to the phys-iologic outcomes of protection and the pathways and endeffectors affected, is remarkable. These data collectively addto mounting evidence that imply that pre- and postcondi-tioning have similar effects, but are exerted at very differenttimes. Positive results with postconditioning have beenreproduced in multiple laboratories in different countriesusing different models, both in vivo and in vitro. In the cur-rent environment, in which the field of cardioprotection is ata crossroads [65] and the very discipline is threatened, post-conditioning may offer a unique therapy that may require avery different course of investigation and regulatory approvalto pharmacologic therapies. However, postconditioning,which is really only in its infancy, has not been attempted inhumans undergoing percutaneous treatments, cardiac sur-gery or transplantation surgery in which ischemia and reper-fusion are encountered. Postconditioning is a remarkableexample of innate defenses the heart can raise against I/R.
Five-year view The next few years will hopefully see much research activityin postconditioning physiology and biology. The conceptmust still be confirmed by other laboratories using a wide
variety of models in which I/R or hypoxia-reoxygenation areinduced. The very basic question of whether the interrupt-ing ischemia, intermittent reperfusion sequences, or a com-bination of the two triggers cardioprotection will undoubt-edly be investigated. In addition, the involvement ofproximal triggers, such as adenosine, opioids and angiogenicfactors, as well as the various molecular ‘survival’ pathways,will be areas of fruitful and necessary research. The connec-tion between these molecular pathways and their translationto physiologic outcomes should be carefully monitored, par-ticularly the role of postconditioning on apoptosis andnecrosis, and which of these events most influences infarctsize and the degree of endothelial protection and so on.Much of the current basic research is conducted in modelswithout superimposed comorbidities simply due to the factthat interpretation of data are more complex in the comor-bid models. However, patients can present with comorbidi-ties that increase the vulnerability of myocardium to infarc-tion, and endothelium to injury. There is controversywhether the cardioprotection achieved by preconditioning islost or attenuated in models with pre-existing hyperlipi-demia, and similar questions and controversies will likelyarise with postconditioning. Models of disease states, such ashyperlipidemia, hypertension and diabetes should be avidlypursued, as these are comorbidities that are part of thepatient disease matrix, and that also decrease the tolerance toI/R. The role of a local inflammatory response mediated byoxidants and neutrophils, which is a controversial topic inthe biology of reperfusion injury [10,22], needs to be investi-gated, specifically answering whether this response is anactive participant or a pedestrian epiphenomenon in thepostconditioning phenotype. It is also anticipated that someform of postconditioning will be tried in human patientsundergoing percutaneous interventions or cardiac surgery.Postconditioning may, in particular, have application in off-pump cardiac surgery, in which the target vessels are ligatedduring the procedure, thereby creating iatrogenic ischemia,but also posing the opportunity to postcondition the newlyrevascularized segment.
Expert commentaryThe current clinical strategies of reperfusion therapies, such asangioplasty and stenting, with concomitant adjunctive admin-istration of statins, glycoprotein IIb/IIIa inhibitors, aspirin orunfractionated heparin, are effective in salvaging myocardium,relative to no treatment at the time of percutaneous interven-tion. However, these strategies do not directly target the perpe-trators of reperfusion injury, as already summarized. Post-conditioning in its simplest mechanical form of rapidly anditeratively interrupting early reflow is but one strategy by whichearly reperfusion injury can be attenuated. Postconditioningmay be mimicked by pharmacologic means that capture theprotective actions of the proximal mediators, such as adenosineand opioids. Hence, a pharmacologic postconditioning, whichis, in reality, reperfusion therapeutics, can be applied during the

Myocardial protection with postconditioning
www.future-drugs.com 1043
early moments of reflow. In addition, facilitating devices willlikely be developed in the next few years that will simplify theapplication of reperfusion therapeutics, whether this is postcon-ditioning of one form or another, or some other form of modi-fied reperfusion. Hence, an industry of reperfusion therapeuticsthat differs radically from its present form will likely develop.
AcknowledgementsThe authors thank Laurie Berley for assistance with wordprocessing of the manuscript. Supported in part by grants fromthe National Institutes of Health (JV-J: HL069487; Z-QZ:HL64886), the American Heart Association (AJZ), and theCarlyle Fraser Heart Center of Emory Crawford Long Hospital.
Key Issues
• Reperfusion contributes to the pathology of myocardial postischemic injury.
• Postconditioning is induced by applying an alogorithm consisting of alternating reperfusion and reocclusion sequences immediately at the onset of reperfusion. This algorithm lasts only a few minutes.
• Postconditioning protects the previously ischemic myocardium by reducing infarct size, the extent of apoptosis, endothelial dysfunction, edema, local inflammatory responses, oxidant burden, oxidant-mediated damage to membranes, calcium accumulation in the cytoplasmic and mitochondrial compartments and, finally, opening of the mitochondrial permeability transition pore. The degree and phenotype of cardioprotection is comparable to that of ischemic preconditioning, but the two interventions may not be additive.
• The cardioprotection of postconditioning has been observed in numerous independent laboratories in several countries, in several animal and cell culture models.
• Protection by postconditioning involves activation of adenosine receptors, potentially by delaying the washout of intravascular adenosine from the area at risk.
• Protection by postconditioning involves molecular signaling pathways, such as phosphatidylinositol 3 kinase-Akt and extracellular signal-regulated kinase. Blockade of these pathways abrogates the cardioprotection of postconditioning, suggesting a functional link. The targets distal to these survival pathways have not been identified.
• The end effectors targeted by postconditioning appear to be KATP (mitochondrial) channels and the mitochondrial permeability transition pore.
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Reimer KA, Jennings RB. The ‘wavefront phenomenon’ of myocardial ischemic cell death. II. Transmural progression of necrosis within the framework of ischemic bed size (myocardial at risk) and collateral flow. Lab. Invest. 40(6), 633–644 (1979).
2 Jordan JE, Zhao ZQ, Vinten-Johansen J. The role of neutrophils in myocardial ischemia-reperfusion injury. Cardiovasc. Res. 43(4), 860–878 (1999).
3 Vinten-Johansen J, Edgerton TA, Howe HR et al. Immediate functional recovery and avoidance of reperfusion injury with surgical revascularization of short-term coronary occlusion. Circulation 72, 431–439 (1985).
4 Vinten-Johansen J. Reperfusion injury: idle curiosity or therapeutic vector? J. Thrombosis Thrombolysis 4, 59–61 (1997).
5 Ambrosio G, Chiariello M. Myocardial reperfusion injury: mechanisms and management-a review. Review. Am. J. Med. 91, S86–S88 (1991).
6 Forman MB, Virmani R, Puett DW. Mechanisms and therapy of myocardial reperfusion injury. Circulation 81(Suppl. IV), IV69–IV78 (1990).
7 Hearse DJ. Reperfusion-induced injury: a possible role for oxidant stress and its manipulation. Cardiovasc. Drugs Ther. 5, 225–235 (1991).
8 Cobbaert C, Hermens WT, Kint PP et al. Thrombolysis-induced coronary reperfusion causes acute and massive interstitial release of cardiac muscle cell proteins. Cardiovasc. Res. 33(1), 147–155 (1997).
9 Piper HM, Schafer AC. The first minutes of reperfusion: a window of opportunity for cardioprotection. Cardiovasc. Res. 61, 365–371 (2004).
•• Reviews some of the authors’ work on myocardial contracture induced after the onset of reperfusion, and considers how this phenomenon correlates with necrosis. Most importantly, this article concludes that the first minutes of reperfusion are associated with rapidly developing events that are ultimately deleterious to the cardiomyocyte, and that early treatment is required to address
these early events. This conclusion is entirely supported by the concept of postconditioning and the observations of Kin and colleagues [12].
10 Vinten-Johansen J. Involvement of neutrophils in the pathogenesis of lethal myocardial reperfusion injury. Cardiovasc. Res. 61, 481–497 (2004).
11 Zhao Z-Q, Corvera JS, Halkos ME et al. Inhibition of myocardial injury by ischemic postconditioning during reperfusion: comparison with ischemic preconditioning. Am. J. Physiol. (Heart Circ. Physiol.) 285, 579–588 (2003).
•• Original report introducing the concept of postconditioning. A canine model of 60 min coronary artery occlusion and 3 h of reperfusion was used, in which a 30 s reperfusion and 30 s reocclusion postconditioning algorithm preceded full left anterior descending (LAD) reflow. This study found that postconditioning reduced infarct size (relative to control) by approximately 50%, which was comparable with the infarct reduction achieved with a single preconditioning cycle. The authors also noted that postconditioning reduced LAD coronary artery endothelial cell activation

Vinten-Johansen, Zhao, Jiang & Zatta
1044 Expert Rev. Cardiovasc. Ther. 3(6), (2005)
(P-selectin surface expression) dysfunction, neutrophil accumulation and superoxide anion generation in area at risk myocardium, as well as presumptive markers of oxidant-mediated cell membrane damage.
12 Kin H, Zhao Z-Q, Sun H-Y et al. Postconditioning attenuates myocardial ischemia-reperfusion injury by inhibiting events in the early minutes of reperfusion. Cardiovasc. Res. 62, 74–85 (2004).
• First report of postconditioning in a rat model of coronary artery occlusion-reperfusion. This study recapitulated the infarct size and neutrophil accumulation data reported in [11], but was also the first report to show that delaying the application of postconditioning abrogated its cardioprotection. This observation suggested that the postconditioning algorithm triggers cardioprotective mechanisms, and that the inhibitory effect was exerted on the reperfusion injury events occurring within the first minutes of reperfusion.
13 Kin H, Lofye MT, Amerson BS et al. Cardioprotection by ‘postconditioning’ is mediated by increased retention of endogenous intravascular adenosine and activation of A2a receptors during reperfusion. Circulation 110(17), III–168 (2004).
14 Halkos ME, Kerendi F, Corvera JS et al. Myocardial protection with postconditioning is not enhanced by ischemic preconditioning. Ann. Thorac. Surg. 78(3), 961–969 (2004).
15 Kevin LG, Camara AKS, Riess ML, Novalija E, Stowe DF. Ischemic preconditioning alters real-time measure of O2 radicals in intact hearts with ischemia and reperfusion. Am. J. Physiol. (Heart Circ. Physiol.) 284, H566–H574 (2003).
16 Ambrosio G, Zweier JL, Flaherty JT. The relationship between oxygen radical generation and impairment of myocardial energy metabolism following postischemic reperfusion. J. Mol. Cell Cardiol. 23(12), 1359–1374 (1991).
17 Piper HM, Garcia-Dorado D, Ovize M. A fresh look at reperfusion injury. Cardiovasc. Res. 38, 291–300 (1998).
18 Piper HM. Energy deficiency, calcium overload or oxidative stress: possible causes of irreversible ischemic myocardial injury. Klin. Wochenschr. 67(9), 465–476 (1989).
19 Garcia-Dorado D, Gonzalez MA, Barrabes JA et al. Prevention of ischemic rigor contracture during coronary occlusion by inhibition of Na+-H+ exchange. Cardiovas. Res. 35, 80–89 (1997).
20 Piper HM, Garcia-Dorado D. Prime cause of rapid cardiomyocyte death during reperfusion. Ann. Thorac. Surg. 68, 1913–1919 (1999).
21 Lefer AM, Lefer DJ. Pharmacology of the endothelium in ischemia-reperfusion and circulatory shock. Ann. Rev. Pharmacol. Toxicol. 33, 71–90 (1993).
22 Baxter GF. The neutrophil as a mediator of myocardial ischemia-reperfusion injury: time to move on. Basic Res. Cardiol. 97(4), 268–275 (2002).
23 Crompton M. The mitochondrial permeability transition pore and its role in cell death. Biochem. J. 341, 233–249 (1999).
24 Halestrap AP, Kerr PM, Javadov S, Woodfield KY. Elucidating the molecular mechanism of the permeability transition pore and its role in reperfusion injury of the heart. Biochim. Biophys. Acta 1366(1–2), 79–94 (1998).
25 Kloner RA, Rezkalla SH. Cardiac protection during acute myocardial infarction: where do we stand in 2004? J. Am. Coll. Cardiol. 44(2), 276–286 (2004).
26 Darling C, Maynard M, Przyklenk K. Post-conditioning via stuttering reperfusion limits myocardial infarct size in rabbit heart. Acad. Emerg. Med. 11, 536-a (2004).
27 Heusch G. Postconditioning old wine in a new bottle. J. Am. Coll. Cardiol. 44(5), 1111–1112 (2004).
28 Valen G, Vaage J. Pre-and postconditioning during cardiac surgery. Bas. Res. Cardiol. 100, 1–8 (2005).
29 Yang XM, Proctor JB, Cui L et al. Multiple, brief coronary occlusions during early reperfusion protect rabbit hearts by targeting cell signaling pathways. J. Am. Coll. Cardiol. 44(5), 1103–1110 (2004).
• Recapitulated the original observations in a rabbit model of coronary artery occlusion-reperfusion, using infarct size as the primary end point. However, importantly, this study also introduced the involvement of signaling kinases (ERK1/2), nitric oxide and KATP channels in the cardioprotection of postconditioning.
30 Sun H-Y, Wang N-P, Kerendi F et al. Hypoxic postconditioning reduces cardiomyocyte loss by inhibiting the generation of reactive oxygen species and intracellular calcium overload. Am. J. Physiol.288(4), 1900–1908 (2004).
31 Zhao Z-Q, Sun H-Y, Wang N-P et al. Hypoxic post-conditioning reduces cardiomyocyte loss by inhibiting reactive oxygen species-triggered mitochondrial calcium overload. Circulation (Suppl.) 108(17), IV-174 (2003).
32 Gottlieb RA, Burleson KO, Kloner RA, Babior BM, Engler RL. Reperfusion injury induces apoptosis in rabbit cardiomyocytes. J. Clin. Invest. 94, 1621–1628 (1994).
33 Zhao Z-Q, Velez DA, Wang N-P et al. Progressively developed myocardial apoptotic cell death during late phase of reperfusion. Apoptosis 6(4), 279–290 (2001).
34 Zhao Z-Q, Sun H-Y, Wang N-P et al. Hypoxic postconditioning attenuates cardiomyocyte apoptosis via inhibition of jnk and p38 kinases pathway. J. Mol. Cell Cardiol. 38, 870 (2005).
35 Headrick JP. Ischemic preconditioning: bioenergetic and metabolic changes and the role of endogenous adenosine. J. Mol. Cell Cardiol. 28, 1227–1240 (1996).
36 Liu GS, Thornton J, Vanwinkle DM et al. Preconditionings protection is mediated by A1 adenosine receptors in the rabbit heart. FASEB J. 5(5), A1050 (1991).
37 Thornton JD, Vanwinkle DM, Downey JM. Preconditioning protection is mediated through adenosine receptors. Circulation 82(4), 464 (1990).
38 Olafsson B, Forman MB, Puett DW et al. Reduction of reperfusion injury in the canine preparation by intracoronary adenosine: importance of the endothelium and the no-reflow phenomenon. Circulation 76(5), 1135–1145 (1987).
39 Zhao ZQ, Nakamura M, Wang NP et al. Administration of adenosine during reperfusion reduces injury of vascular endothelium and death of myocytes. Coron. Artery Dis. 10(8), 617–628 (1999).
40 Zhao Z-Q, McGee DS, Nakanishi K et al. Receptor-mediated cardioprotective effects of endogenous adenosine are exerted primarily during reperfusion after coronary occlusion in the rabbit. Circulation 88(2), 709–719 (1993).
41 Zhao Z-Q, Nakanishi K, McGee DS, Tan P, Vinten-Johansen J. A1-receptor mediated myocardial infarct size reduction by endogenous adenosine is exerted primarily during ischaemia. Cardiovasc. Res. 28(2), 270–279 (1994).
42 Kin H, Zatta AJ, Lofye MT et al. Postconditioning reduces infarct size via adenosine receptor activation by endogenous adenosine. Cardiovasc. Res. 67, 124–133 (2005).
43 Todd JC, Zhao Z-Q, Williams MW et al. Intravascular adenosine at reperfusion reduces infarct size and neutrophil adherence. Ann. Thorac. Surg. 62, 1364–1372 (1996).

Myocardial protection with postconditioning
www.future-drugs.com 1045
44 Yang X-M, Philipp S, Downey JM, Cohen MV. Postconditioning’s protection is not dependent on circulating blood factors or cells but involves adenosine receptors and requires PI3-kinase and guanylyl cyclase activation. Bas. Res. Cardiol. 100, 57–63 (2005).
45 Balligand J-L, Ungureanu D, Kelly RA et al. Abnormal contractile function due to induction of nitric oxide synthase in rat cardiac myocytes follows exposure to activated macrophage-conditioned medium. J. Clin. Invest. 91, 2314–2319 (1993).
46 Johnson G, III, Tsao PS, Mulloy D, Lefer AM. Cardioprotective effects of acidified sodium nitrite in myocardial ischemia with reperfusion. J. Pharmacol. Exp. Ther. 252, 35–41 (1990).
47 Lefer DJ, Nakanishi K, Johnston WE, Vinten-Johansen J. Anti-neutrophil and myocardial protecting action of SPM-5185, a novel nitric oxide (NO) donor, following acute myocardial ischemia and reperfusion in dogs. Circulation 88, 2337–2350 (1993).
48 Bolli R, Dawn B, Tang X-L et al. The nitric oxide hypothesis of late preconditioning. Basic Res. Cardio. 93, 325–338 (1998).
49 Ma X-L, Weyrich AS, Lefer DJ, Lefer AM. Diminished basal nitric oxide release after myocardial ischemia and reperfusion promotes neutrophil adherence to coronary endothelium. Circ. Res. 72, 403–412 (1993).
50 Tsang A, Hausenloy DJ, Mocanu MM, Yellon DM. Postconditioning: a form of ‘modified reperfusion’ protects the myocardium by activating the phosphatidylinositol 3-kinase-Akt pathway. Circ. Res. 95(3), 230–232 (2004).
• This study in isolated perfused rat hearts showed that the postconditioning response could be recapitulated in ex vivo models, as also demonstrated by Zhao and coworkers [31]. Importantly, this study suggested the involvement of the phosphatidylinositol 3 kinase survival pathway and downstream targets endothelial nitric oxide synthase and p70S6K. These pathways influence the pathogenesis of apoptosis, but the data also show effects on infarct size; the correlation between apoptosis and necrosis (infarction)was not determined.
51 Pagliaro PR, Rastaldo R, Penna C et al. Nitric oxide (NO)-cylic guanosine monophosphate (cGMP) pathway is involved in ischemic postconditioning in the isolated rat heart. Circulation 110(17), 111–136 (2004).
52 Wang P, Zweier JL. Measurement of nitric oxide and peroxynitrite generation in the postischemic heart. Evidence for peroxynitrite-mediated reperfusion injury. J. Biol. Chem. 271(46), 29223–29230 (1996).
53 Lefer DJ, Nakanishi K, Vinten-Johansen J. Endothelial and myocardial cell protection by a cysteine- containing nitric oxide donor after myocardial ischemia and reperfusion. J. Cardiovasc. Pharmacol. 22(Suppl. 7), S34–S43 (1993).
54 Sun H-Y, Wang N-P, Kerendi F et al. Hypoxic postconditioning reduces cardiomyocyte loss by inhibiting ROS generation and intracellular Ca2+ overload. Am. J. Physiol. 288, H1900–H1908 (2005).
55 Serviddio G, Di Venosa N, Federici A et al. Brief hypoxia before normoxic reperfusion (postconditioning) protects the heart against ischemia-reperfusion injury by preventing mitochondria peroxyde production and glutathione depletion. FASEB J. 19, 354–361 (2005).
56 Ambrosio G, Tritto I, Chiariello M. The role of oxygen free radicals in preconditioning (Copenhagen symposia special review). J. Mol. Cell Cardiol. 27, 1035–1039 (1995).
57 Vanden Hoek TL, Becker LB, Shao ZH, Li CQ, Schumacker PT. Preconditioning in cardiomyocytes protects by attenuating oxidant stress at reperfusion. Circ. Res. 86(5), 541–548 (2000).
58 Argaud L, Gateau-Roesch O, Raisky O et al. Post-conditioning inhibits mitochondrial permeability transition. Circulation 111, 194–197 (2005).
59 Di Lisa F, Menabo R, Canton M, Barile M, Bernardi P. Opening of the mitochondrial permeability transition pore causes depletion of mitochondrial and cytosolic NAD(+) and is a causative event in the death of myocytes in postischemic reperfusion of the heart. J. Biol. Chem. 276(4), 2571–2575 (2001).
60 Gross GJ, Fryer RM. Mitochondrial KATP channels: Triggers or distal effectors of ischemic or pharmacological preconditioning? Circ. Res. 87(6), 431–433 (2000).
61 Hausenloy D, Wynne A, Duchen M, Yellon D. Transient mitochondrial permeability transition pore opening mediates preconditioning-induced protection. Circulation 109(14), 1714–1717 (2004).
62 Hausenloy DJ, Yellon DM. The mitochondrial permeability transition pore in myocardial preconditioning. Cardiovasc. J. S. Afr. 15(4 Suppl. 1), S5 (2004).
63 Hausenloy DJ, Yellon DM. New directions for protecting the heart against ischaemia-reperfusion injury: targeting the Reperfusion Injury Salvage Kinase (RISK)-pathway. Cardiovasc. Res. 61(3), 448–460 (2004).
64 Isobe N, Oshima S, Taniguchi K et al. Does repeated balloon inflation during coronary angioplasty induce ischemic tolerance? Analysis based on regional work. Heart Vessels 15, 117–123 (2000).
65 Bolli R, Becker L, Gross G et al. Myocardial protection at a crossroads: The need for translation into clinical therapy. Circ. Res. 95, 125–134 (2004).
Affiliations
• Jakob Vinten-Johansen, PhD
Carlyle Fraser Heart Center, Cardiothoracic Research Laboratory,Carlyle Fraser Heart Center of Emory Crawford Long Hospital, 550 Peachtree Street NE, Atlanta,GA 30308–2225, USATel.: +1 404 686 2511Fax: +1 404 686 [email protected]
• Zhi-Qing Zhao, MD
Carlyle Fraser Heart Center, Cardiothoracic Research Laboratory,Carlyle Fraser Heart Center of Emory Crawford Long Hospital/Emory University, 550 Peachtree Street NE, Atlanta, GA 30308–2225, USATel.: +1 404 686 2511Fax: +1 404 686 [email protected]
• Rong JiangCarlyle Fraser Heart Center, Cardiothoracic Research Laboratory,Carlyle Fraser Heart Center of Emory Crawford Long Hospital/Emory University, 550 Peachtree Street NE, Atlanta, GA 30308–2225, USATel.: +1 404 686 2511Fax: +1 404 686 [email protected]
• Amanda J Zatta, PhD
Carlyle Fraser Heart Center, Cardiothoracic Research Laboratory,Carlyle Fraser Heart Center of Emory Crawford Long Hospital/Emory University, 550 Peachtree Street NE, Atlanta, GA 30308–2225, USATel.: +1 404 686 2511Fax: +1 404 686 [email protected]