Embed Size (px)
Citation preview

Proc. Nati. Acad. Sci. USAVol. 84, pp. 7503-7507, November 1987Biochemistry
Myoglobin-mediated oxygen delivery to mitochondria of isolatedcardiac myocytes
(electron transport/heart cells/cytochrome oxidase)
BEATRICE A. WITTENBERG* AND JONATHAN B. WITTENBERGDepartment of Physiology and Biophysics, Albert Einstein College of Medicine, Bronx, NY 10461
Communicated by Berta Scharrer, July 20, 1987 (received for review May 5, 1987)
ABSTRACT Myoglobin-mediated oxygen delivery to in-tracellular mitochondria is demonstrated in cardiac myocytesisolated from the hearts of mature rats. Myocytes are held athigh ambient oxygen pressure, 40-340 torr (5-45 kPa);sarcoplasmic myoglobin is fully oxygenated. In this conditionoxygen availability does not limit respiratory rate; myoglobin-facilitated diffusion contributes no additional oxygen flux and,since oxygen consumption is measured in steady states, thestorage function of myoglobin vanishes. Carbon monoxide,introduced stepwise, displaces oxygen from intracellularoxymyoglobin without altering the optical spectrum of thelargely oxidized intracellular mitochondria. A large part,about one-third, of the steady-state oxygen uptake is abolishedby carbon monoxide blockade of myoglobin oxygenation. Themyoglobin-dependent component of the oxygen uptake de-creases linearly with decreasing fraction of intracellularoxymyoglobin, with a slope near unity. Studies using inhibitorsof mitochondrial electron transport indicate- that myoglobin-delivered oxygen uptake depends on electron flow through themitochondrial electron transport chain. We conclude thatcardiac mitochondria accept two additive simultaneous flows ofoxygen: a flow of dissolved oxygen to cytochrome oxidase anda flow of myoglobin-bound oxygen to a mitochondrial termi-nus. Myoglobin-mediated oxygen delivery supports ATP gen-eration by heart cells at physiological ambient oxygen pressure.
Myoglobin is an oxygen-binding monomeric hemeproteinfound in the cytosol of cardiac myocytes and of thosevertebrate muscle fibers that do sustained work (1). Themyoglobin content of muscles increases with exercise (1-3)and is proportional to the cytochrome oxidase content (2, 4,5). Myoglobin, by facilitating oxygen diffusion, maintains anample free oxygen concentration at the muscle mitochon-drion (2, 4, 6). Blockade of myoglobin function decreasesoxygen uptake (7, 8), work output (8, 9), and ATP generation(10) of cardiac and skeletal muscle.
Facilitation of oxygen diffusion through the sarcoplasm ofthe myocyte has often been taken as the sole function ofmyoglobin in muscles in the steady state. Here we show anadditional function: myoglobin-mediated oxygen delivery tomitochondria. This is most clearly demonstrated in isolatedcardiac myocytes flooded with superabundant oxygen (11,12). In this circumstance, the maximum diffusive flow ofdissolved oxygen across the sarcoplasm exceeds the mito-chondrial oxygen demand at least 100-fold (13, 14); sarco-plasmic myoglobin is essentially fully oxygenated, and facil-itated diffusion contributes no additional oxygen flux (2, 4, 6).Since oxygen uptake is in steady states, the storage functionof myoglobin vanishes (7). Intracellular gradients of oxygenpressure, always shallow (15-18), now are small relative toambient oxygen pressure.
Cytochrome oxidase, half-oxidized when ambient oxygenpartial pressure (Po2) is 0.07 torr (1 torr = 133 Pa) (16), in thecircumstance described here experiences oxygen pressures20- to 200-fold the pressure required to maintain the normal,largely oxidized, state seen in resting myocytes (16). Carbonmonoxide in this circumstance blocks oxygenation ofsarcoplasmic myoglobin selectively without perturbing theoptical spectrum of intracellular cytochrome oxidase. Weconclude that cardiac mitochondria accept two additivesimultaneous flows of oxygen: the well-known flow of dis-solved oxygen to cytochrome oxidase and a flow ofmyoglobin-bound oxygen to a mitochondrial terminus. Themyoglobin-mediated oxygen flow supports ATP generationin the physiological range of oxygen pressure.
MATERIALS AND METHODSIsolated Cardiac Myocytes. These were prepared from the
hearts of mature rats by enzymatic digestion, purified onPercoll (Pharmacia) density gradients, and suspended to afinal density of 0.5-1.0 x 106 cells per ml (19, 20).
Mitochondria. Mitochondria were prepared by the methodof Palmer et al. (21) from adult rat hearts that had beenperfused with balanced saline solution to remove erythro-cytes.Gas Partial Pressures and Oxygen Uptake. All measure-
ments were made in steady states (7, 16) of constant oxygenpressure and oxygen uptake. The measuring chamber hadboth liquid and gas phases (16, 22). The gas phase composi-tion was set by a mass flow controller (Tylan, Torrance, CA).Since carbon monoxide is not consumed, solution Pco isknown from the composition of the gas phase. Solutionoxygen pressure was monitored by a sensitive polarographicoxygen electrode and is the balance of oxygen entering andoxygen consumed by the myocytes. At constant temperatureand stirring rate, oxygen uptake is known from the differencebetween solution Po2 in the absence of myocytes (equal togas-phase Po2) and the actual solution Po2 in the presence ofmyocytes, using a mass transfer coefficient that is determineddaily (16, 22, 23). The temperature was 30'C in all experi-ments.
Optical Spectra. The chamber was held in a thermostattedblock placed in the sample light beam of a Cary model 17recording spectrophotometer (Varian) equipped with a Caryscattered transmission accessory. Data were acquired digi-tally from 650 to 350 nm, and difference spectra wereconstructed by subtraction, using an Aviv data acquisitionsystem (Aviv Laboratories, Lakewood, NJ). The spectralcontribution of myoglobin dominates the myocyte opticalspectrum (16). Under the conditions of our experiments,
Abbreviations: CCCP, carbonyl cyanide m-chlorophenylhydrazone;MbO2, oxymyoglobin; MbCO, carbon monoxide myoglobin; Po2,partial pressure of oxygen; Pco, partial pressure of carbon monox-ide.*To whom reprint requests should be addressed.
7503
The publication costs of this article were defrayed in part by page chargepayment. This article must therefore be hereby marked "advertisement"in accordance with 18 U.S.C. §1734 solely to indicate this fact.

7504 Biochemistry: Wittenberg and Wittenberg
intracellular myoglobin is essentially completely ligated; oxy-and carbon monoxide myoglobin are the dominant speciespresent. The contribution of myoglobin was calculated fromthe spectral changes occurring at 409 and 424 nm, whenintracellular oxymyoglobin was converted fully to carbonmonoxide myoglobin, and was subtracted from myocytespectra to obtain a residuum dominated by the spectralcontribution of the mitochondria. The fraction of carbonmonoxide myoglobin at any Pco was calculated from spectralchanges observed at 409 and 424 nm. Excellent isosbesticitywas maintained at 415 and 438 nm.
Energetics of Cardiac Myocytes. Suspensions of myocyteswere incubated in the measuring chamber for 60 min. Oxygenuptake, intracellular ATP, intracellular phosphocreatine, andaccumulated lactate (final minus initial) were determined aspreviously (16, 20).
RESULTS
The partition of intracellular myoglobin between carbonmonoxide and oxygen, M = ([MbCO] x Po2)/([MbO2] x
Pco), was determined graphically as the slope of the line inFig. 1. 'The partition coefficient, M = 20 at 30'C, is not largelydifferent from that of purified rat heart myoglobin, M = 29 at30'C, which we determined by conventional procedures (24,25). The reasonable value of the slope, together with thelinearity of the relation found, indicates near equilibriumbetween sarcoplasmic myoglobin, oxygen, and carbon mon-oxide.The effect of carbon monoxide on steady-state respiration
of cardiac myocytes is presented in Fig. 2. Within eachexperiment, the fraction of oxygen in the gas phase was heldconstant at 10-25% and the fraction of carbon monoxide was
increased stepwise. Steady-state solution oxygen pressure,steady-state oxygen uptake, and optical spectra were moni-tored. The oxygen uptake of cardiac myocytes held at highPo2 decreases initially as Pco is increased, stays nearlyconstant in a prolonged plateau in which myoglobin is fullysaturated with carbon monoxide, and finally, above 95%carbon monoxide, in the gas phase, declines to zero as carbonmonoxide combines with cytochrome oxidase (Fig. 2a). Theearly decrease clearly follows the increasing fractional satu-ration of cytoplasmic myoglobin with carbon monoxide (Fig.2b). This part of the respiration may be called the myoglobin-dependent oxygen uptake.
3 -
0~~~~~~~~~~~~~~~
0~~~~~~~~~~~
0o ...0H
0.05 0.1 0.15
PCO/ P°2
FIG. 1. Partition of intracellular myoglobin between oxygen andcarbon monoxide. Data are from six experiments. Solution oxygenpressures ranged from 40 to 340 torr in different experiments. Thepartition coefficient M = 20 at 30'C.
a
w0uBy
zw
x0
00
0w
I-
a.
z
0
b1.0I
me - _ _
A.~*U- S~- -
0.5 /U/,0//0/
/00 I400 10 20 30 40
Pco torr
FIG. 2. Steady-state oxygen uptake of suspensions of cardiacmyocytes as a function of carbon monoxide partial pressure. Res-piratory rate [14.4 ± 3.3 nmol of oxygen per min per ml per 106 cells(mean ± SD; n = 29) in these experiments] is normalized, taking theuninhibited rate in each experiment as unity. Data are from threeexperiments. m, 15% oxygen in the gas phase (solution P92 = 80-90torr); e, 20% oxygen (solution Po2 = 100-120 torr); A, 25% oxygen(solution Po2 = 155-160 torr). (a) Pco = 0-730 torr. (b) The samedata presented over a limited range; the fractional saturation ofsarcoplasmic myoglobin in one experiment is presented (o--- o;20%o oxygen in the gas phase). The myoglobin-dependent componentof the oxygen uptake is taken as the difference between theuninhibited rate and the plateau value reached as sarcoplasmicmyoglobin approaches saturation with carbon monoxide.
The myoglobin-dependent component of oxygen uptakedecreases linearly 'with increasing fractional saturation ofsarcoplasmic myoglobin with CO, with a slope near -1.1(Fig. 3). This indicates that the myoglobin-dependent oxygenuptake is proportional to the fraction of sarcoplasmicoxymyoglobin.The state of intracellular mitochondria of cardiac myocytes
exposed to carbon monoxide in the presence of oxygen, theplateau region of Fig. 2, was determined from optical spectra.Myocyte spectra (Pco = 295 torr, Po2 = 36 torr) after thespectral contribution of intracellular carbon monoxidemyoglobin is subtracted scarcely differ from spectra of thesame cell suspension in oxygen alone (Po2 = 35 torr) after thespectral contribution of intracellular oxymyoglobin is sub-tracted (Fig. 4). The absence of spectral difference near 428,445, 590, and 606 nm between the upper and middle traces ofFig. 4 indicates that cytochrome a3 of cytochrome oxidasehas not ligated appreciably to carbon monoxide even at a Pco(295 torr) far greater than that required to inhibit myoglobin-dependent oxygen uptake (95% inhibition near Pco = 50 torr,Fig. 2a).The absence of spectral difference near 445 and 603 nm
indicates that the extent of steady-state oxidation/reductionof cytochrome oxidase is unchanged. The absence of thediagnostic intense maximum of reduced cytochrome c (550nm) in the upper trace of Fig. 4 indicates that the level ofreduction of cytochrome c likewise is largely unchanged.Taken together, these spectral findings indicate that mito-chondria of myocytes in the plateau region of Fig. 2 (Pco =
Proc. Natl. Acad Sci. USA 84 (1987)

Proc. Natl. Acad. Sci. USA 84 (1987) 7505
I.0w
By
A7-
w D0 x
o <t
Z LLo
z z
aIJJ F
7_ E-m0
0lo
0.8~
0.6
0.4
0.2
0.2 0.4 0.6 0.8 1.0
[MbCo]/([ MbCo] + [MbO2 ])
FIG. 3. Myoglobin-dependent oxygen uptake of suspensions ofcardiac myocytes as a function of the fraction of sarcoplasmicmyoglobin ligated to carbon monoxide. Myoglobin-dependent oxy-gen uptake, defined in the legend to Fig. 2, is normalized, taking themaximal value in each experiment as unity. Results of five experi-ments are shown. *, Two experiments with solution Po2 = 40-60torr; *, solution Po2 = 70-90 torrP e, solution Po2 = 100-120 torr; El,
a single experiment with solution Po2 = 340 torr (precision ofmeasuring oxygen uptake is less in this experiment). Pco at halfsaturation of sarcoplasmic myoglobin in different experiments was3-15 torr. The solid line is a least-squares fit to the data of the fourexperiments represented by solid symbols. The slope is -1.1 (r =0.98).
50-300 torr) are in the state expected for myocytes in oxygenand are not affected by carbon monoxide.
Spectral features near 430, 537, and 563 nm, seen in themyocyte but not the mitochondrial spectra of Fig. 4, indicatethat cytochrome b of ubiquinone-cytochrome c oxidoreduc-tase [429 and 562-564 nm (refs. 26-28)], oxidized in fullyoxidized isolated mitochondria, is detectably reduced in theaerobic isolated myocyte. Spectral contributions fromcytochrome b of succinate-ubiquinone oxidoreductase [424and 560 nm (refs. 28-30)] or from cytochrome b5 [423 and 556nm (refs. 31-33)] are easily distinguished and are excluded.The final decrease in respiration occurs at about 95%
carbon monoxide in the gas phase (Pco = 700 torr; solutionPo2 = 7 torr). Concomitant with inhibition of respiration,optical spectra first indicate ligation of cytochrome a3 tocarbon monoxide. The spectral change is complete at 100%carbon monoxide in the gas phase (Fig. 5).The spectral contribution of myoglobin cancels in the
difference between spectra of cells exposed to 100% carbonmonoxide and cells on the plateau region of Fig. 2 (Fig. 5,upper trace). The spectrum is essentially similar to thedifference spectrum of isolated mitochondria exposed tocarbon monoxide minus those in air (Fig. 5, lower trace),except for a feature near 563 nm in the mitochondrialspectrum ascribed to differential reduction of cytochrome b.Spectral features near 550, 445, and 605 nm seen in bothtraces indicate increased reduction of cytochrome c andcytochrome oxidase in the absence of oxygen. A spectralfeature near 593 nm seen in both traces is ascribed to carbonmonoxide-ligated cytochrome a3 of cytochrome oxidase.This confirms that intracellular mitochondria of cells exposedto carbon monoxide in air are in an oxidized steady state.A small maximum near 419 nm appears in the difference
between spectra of myocytes exposed to carbon monoxideand oxygen and those in oxygen alone (difference between
Wd /\430Ql *w
'.
Cf)m
350 400 450 500 550 600 650
WAVELENGTH, nm
FIG. 4. Optical spectra of a suspension of cardiac myocytes,compared to spectra of isolated mitochondria. Bottom trace, spec-trum of an oxygenated suspension of rat heart mitochondria. Middletrace, spectrum ofa suspension ofcardiac myocytes (106 cells per ml;solution Po2 = 35 torr) minus the spectral contribution of 5.2 AuMMbO2. At this solution oxygen pressure the intracellular myoglobinis %% oxygenated (16). Upper trace, spectrum of the same cellsuspension (solution Po2 = 36 torir; Pco = 295 torr) minus thespectral contribution of 5.2 ,M MbCO. This trace corresponds to apoint on the respiratory plateau of Fig. 2, where the myoglobin-dependent respiration is fully inhibited, and intracellular myoglobinis fully saturated with carbon monoxide. The myocyte spectra arenearly the same in the absence and presence of carbon monoxide,differing only slightly in the Soret region.
upper and middle traces of Fig. 4, not presented). This is theonly spectral change (other than the changes ascribed to
430
550 603
0.05 ~~~520LiJ
0
z
350 400 450 500 550 600 650
WAVELENGTH, nm
FIG. 5. Optical difference spectrum of cardiac myocytes. Intra-cellular myoglobin is fully saturated with carbon monoxide in eachparent myocyte sample, and the spectral contribution of MbCO iscancelled in the difference. This is compared to a mitochondrialdifference spectrum. Upper trace, spectrum of a suspension ofcardiac myocytes (0.5 x 101 cells per ml) in carbon monoxide alone(Pco = 730 torr) minus the spectrum of the same suspension, takenearlier (solution Po2 = 195 torr, Pco = 370 torr; this corresponds toabout the midpoint of the respiratory plateau of Fig. 2). Lower trace,spectrum of a suspension of isolated rat heart mitochondria in thepresence of succinate and carbon monoxide minus the spectrum ofthe same suspension taken earlier in the presence of oxygen. Thetraces are largely the same except for a greater prominence of afeature near 563 nm in the mitochondrial trace. Cytochrome b, towhich this feature is ascribed, is always detectably reduced inmyocytes (Fig. 4) and is fully reduced in anaerobic mitochondria.
i ~
on *
0
a 0*
Biochemistry: Wittenberg and Wittenberg
7506 Biochemistry: Wittenberg and Wittenberg
myoglobin) consistently accompanying binding of intracellu-lar myoglobin to carbon monoxide and is observed evenwhen myoglobin-dependent oxygen uptake is decreased inthe presence of antimycin, myxothiazol, or cyanide. Thisfeature is not observed in spectra of isolated mitochondriaexposed to 50% carbon monoxide in oxygen. Candidates forthe origin of this difference are many. It may reflect increasedreduction ofcytochrome c or ofcytochrome c1 ofubiquinone-cytochrome c oxidoreductase [reduced minus oxidized dif-ference spectrum, 418, 523, and 553 nm (refs. 34 and 35)]. Orit may reflect a ferryl or a low-spin ferric form of myoglobinor possibly a minor perturbation in the steady state ofcytochrome oxidase.
Inhibitors of the mitochondrial respiratory chain (36) wereused to elucidate the relation of myoglobin-mediated oxygenuptake to mitochondrial function. Cyanide (1 mM) ormyxothiazole (2 ,uM) inhibit 80-85% of the respiratoryoxygen uptake ofcardiac myocytes. In the presence of either,myoglobin-mediated oxygen flux is abolished. Oxygen up-take can be inhibited partially (50-60% of control) at lowerconcentrations of cyanide (10-50 ,uM) or of antimycin (0.6pM). At this level of inhibition, difference spectra (50 uMcyanide minus control) exhibit features near 550 and 600 nm,attributed to increased reduction of cytochrome c and toperturbation of cytochrome oxidase. Difference spectra(antimycin minus control) exhibit well-resolved maxima near430 and 563 nm, attributed to additional reduction ofcytochrome b of ubiquinone-cytochrome c oxidoreductase(36, 37). In these partially inhibited states of cellular respi-ration, carbon monoxide (10-40% in the gas phase) bringsabout only a small inhibition (11 + 5%; n = 7) of oxygenuptake in each experiment. Optical spectra indicate nofurther reduction of cytochrome c or perturbation ofcytochrome oxidase. An increased absorbance is noted near419 nm.To demonstrate the effect of myoglobin blockade on cell
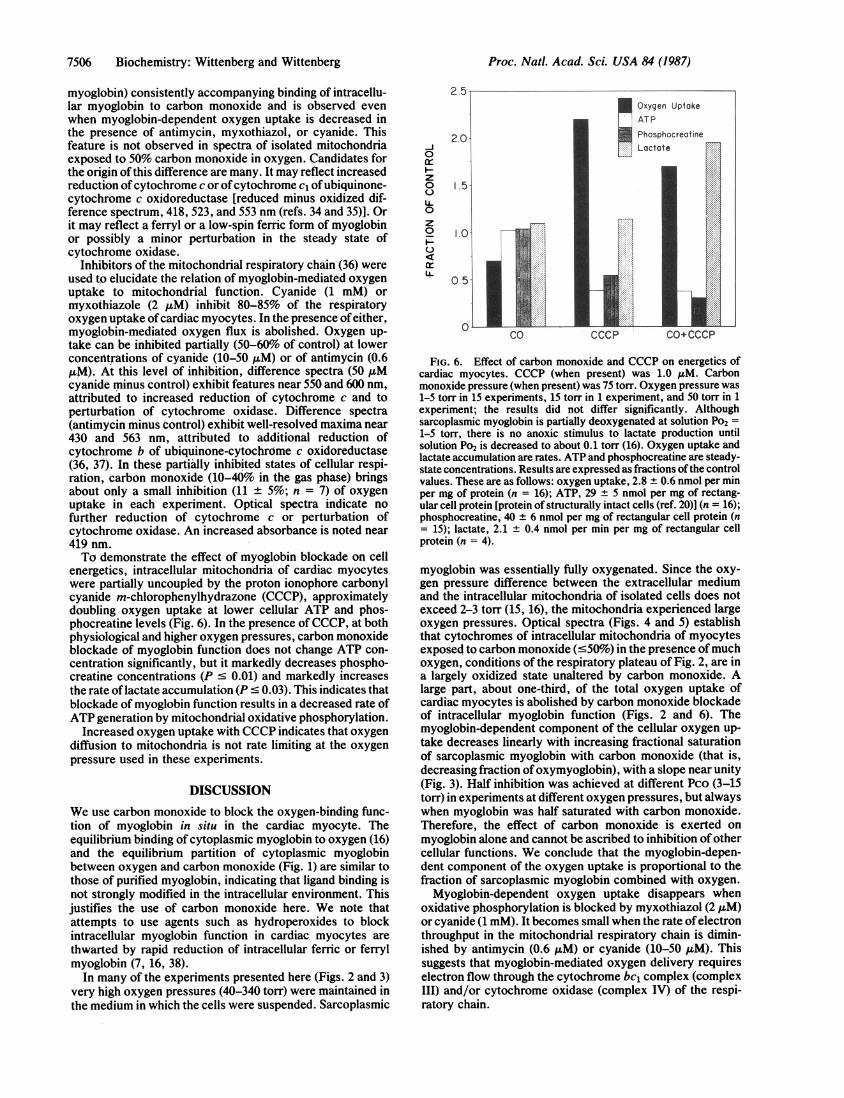
energetics, intracellular mitochondria of cardiac myocyteswere partially uncoupled by the proton ionophore carbonylcyanide m-chlorophenylhydrazone (CCCP), approximatelydoubling oxygen uptake at lower cellular ATP and phos-phocreatine levels (Fig. 6). In the presence of CCCP, at bothphysiological and higher oxygen pressures, carbon monoxideblockade of myoglobin function does not change ATP con-centration significantly, but it markedly decreases phospho-creatine concentrations (P c 0.01) and markedly increasesthe rate oflactate accumulation (P - 0.03). This indicates thatblockade of myoglobin function results in a decreased rate ofATP generation by mitochondrial oxidative phosphorylation.
Increased oxygen uptake with CCCP indicates that oxygendiffusion to mitochondria is not rate limiting at the oxygenpressure used in these experiments.
DISCUSSIONWe use carbon monoxide to block the oxygen-binding func-tion of myoglobin in situ in the cardiac myocyte. Theequilibrium binding of cytoplasmic myoglobin to oxygen (16)and the equilibrium partition of cytoplasmic myoglobinbetween oxygen and carbon monoxide (Fig. 1) are similar tothose of purified myoglobin, indicating that ligand binding isnot strongly modified in the intracellular environment. Thisjustifies the use of carbon monoxide here. We note thatattempts to use agents such as hydroperoxides to blockintracellular myoglobin function in cardiac myocytes arethwarted by rapid reduction of intracellular ferric or ferrylmyoglobin (7, 16, 38).
In many of the experiments presented here (Figs. 2 and 3)very high oxygen pressures (40-340 torr) were maintained inthe medium in which the cells were suspended. Sarcoplasmic
0-~~~-- LII]~~~Lactate0
zo 1.5
0z
0
CO CCCP CO+CCCP
FIG. 6. Effect of carbon monoxide and CCCP on energetics ofcardiac myocytes. CCCP (when present) was 1.0 ,uM. Carbonmonoxide pressure (when present) was 75 torr. Oxygen pressure was1-5 torr in 15 experiments, 15 torr in 1 experiment, and 50 torr in 1experiment; the results did not differ significantly. Althoughsarcoplasmic myoglobin is partially deoxygenated at solution Po2 =1-5 torr, there is no anoxic stimulus to lactate production untilsolution Po2 is decreased to about 0.1 torr (16). Oxygen uptake andlactate accumulation are rates. ATP and phosphocreatine are steady-state concentrations. Results are expressed as fractions ofthe controlvalues. These are as follows: oxygen uptake, 2.8 ± 0.6 nmol per minper mg of protein (n = 16); ATP, 29 ± 5 nmol per mg of rectang-ular cell protein [protein of structurally intact cells (ref. 20)] (n = 16);phosphocreatine, 40 ± 6 nmol per mg of rectangular cell protein (n= 15); lactate, 2.1 ± 0.4 nmol per min per mg of rectangular cellprotein (n = 4).
myoglobin was essentially fully oxygenated. Since the oxy-gen pressure difference between the extracellular mediumand the intracellular mitochondria of isolated cells does notexceed 2-3 torr (15, 16), the mitochondria experienced largeoxygen pressures. Optical spectra (Figs. 4 and 5) establishthat cytochromes of intracellular mitochondria of myocytesexposed to carbon monoxide (50%) in the presence of muchoxygen, conditions of the respiratory plateau of Fig. 2, are ina largely oxidized state unaltered by carbon monoxide. Alarge part, about one-third, of the total oxygen uptake ofcardiac myocytes is abolished by carbon monoxide blockadeof intracellular myoglobin function (Figs. 2 and 6). Themyoglobin-dependent component of the cellular oxygen up-take decreases linearly with increasing fractional saturationof sarcoplasmic myoglobin with carbon monoxide (that is,decreasing fraction of oxymyoglobin), with a slope near unity(Fig. 3). Half inhibition was achieved at different Pco (3-15torr) in experiments at different oxygen pressures, but alwayswhen myoglobin was half saturated with carbon monoxide.Therefore, the effect of carbon monoxide is exerted onmyoglobin alone and cannot be ascribed to inhibition of othercellular functions. We conclude that the myoglobin-depen-dent component of the oxygen uptake is proportional to thefraction of sarcoplasmic myoglobin combined with oxygen.
Myoglobin-dependent oxygen uptake disappears whenoxidative phosphorylation is blocked by myxothiazol (2 AM)or cyanide (1 mM). It becomes small when the rate ofelectronthroughput in the mitochondrial respiratory chain is dimin-ished by antimycin (0.6 pM) or cyanide (10-50 pM). Thissuggests that myoglobin-mediated oxygen delivery requireselectron flow through the cytochrome bc, complex (complexIII) and/or cytochrome oxidase (complex IV) of the respi-ratory chain.
Proc. Natl. Acad. Sci. USA 84 (1987)
Proc. Natl. Acad. Sci. USA 84 (1987) 7507
Resting myocytes at physiological ambient Po2 (1-5 torr)maintain their energy reserves in the face of blockade ofmyoglobin function. Partial uncoupling of mitochondrialoxidative phosphorylation roughly doubles respiratory oxy-gen uptake and establishes a new steady state, simulating thatin the working heart. The phosphocreatine reserve is less andATP concentration is near a minimum working level. Carbonmonoxide blockade of myoglobin oxygenation impairs theability of these myocytes to meet the demand for ATP (Fig.6). The steady-state concentration of intracellular ATP isitselfconserved, but a sharp fall in the standing concentrationof phosphocreatine and a dramatic increase in the rate oflactate accumulation indicate that the rate of oxidativephosphorylation has decreased, and the short fall in ATPgeneration has been compensated by a shift in the balancebetween phosphocreatine and creatine and by increasedaerobic glycolysis to meet the fixed demand for ATP.Intracellular myoglobin function, therefore, supports ATPgeneration at extracellular oxygen pressures close to thepressure expected for intact cardiac muscle.Oxymyoglobin supporting mitochondrial ATP generation
may deliver its oxygen to mitochondria. Alternatively,sarcoplasmic oxymyoglobin might accept electrons frommitochondria, with concomitant reduction of heme iron-ligated oxygen to water. Our evidence cannot distinguishbetween these two formal possibilities. Either mechanismrequires interaction between oxymyoglobin and mitochon-dria.Myoglobin-dependent oxygen delivery to mitochondria,
demonstrated here in myocytes, finds a strong parallel inleghemoglobin-mediated oxygen delivery to nitrogen-fixingsymbiotic bacteria of the soybean root nodule. Oxygendelivered by leghemoglobin supports ATP generation in theintact nodule (39) and in a broken cell system (40-43).Dissolved oxygen, in contrast, although consumed rapidly,supports only limited ATP generation. The bacterialoxidase(s), presumably located in the cell membrane, isseparated from leghemoglobin by the bacterial cell wall. Wedo not yet know how leghemoglobin-delivered oxygen istransferred across the bacterial wall, just as we do notunderstand how myoglobin-bound oxygen is delivered acrossthe outer mitochondrial membrane to the inner membrane.We conclude that a dominant function of myoglobin in the
cardiac myocyte is myoglobin-mediated oxygen delivery tomitochondria. The myoglobin-mediated oxygen flow sup-ports ATP generation at physiological oxygen pressures. Wesuggest that myoglobin-mediated oxygen delivery may con-tribute importantly to the ability of the heart to sustainmaximum work output. Loss of this function may explain thecardiac toxicity of subacute carbon monoxide poisoning.
We thank Drs. C. A. Appleby, D. Mauzerall, and M. Wikstrom forhelpful discussion and Chui Fan Wong for technical assistance. Thiswork was supported in part by a grant in aid from the New YorkHeart Association (to B.A.W.), by Grants HL 19299 and HL 33655from the U.S. Public Health Service (to B.A.W.), and by ResearchGrants DMB 84-16001 and PCM 84-16016 (to J.B.W.) from the U.S.National Science Foundation. J.B.W. is Research Career ProgramAwardee 1-K6-733 of the U.S. National Heart, Lung and BloodInstitute.
1. Millikan, G. A. (1939) Physiol. Rev. 19, 503-523.2. Wittenberg, J. B. (1970) Physiol. Rev. 50, 559-636.3. Pattengale, K. & Holloszy, J. 0. (1967) Am. J. Physiol. 213,
783-785.4. Wittenberg, J. B. & Wittenberg, B. A. (1981) in Oxygen and
Living Processes, ed. Gilbert, D. L. (Springer, New York), pp.177-199.
5. Lawrie, R. A. (1950) J. Agric. Sci. 40, 356-366.6. Murray, J. D. (1977) Lectures on Nonlinear-Differential-Equa-
tion Models in Biology (Clarendon, Oxford), pp. 42-82.7. Wittenberg, B. A., Wittenberg, J. B. & Caldwell, P. R. B.
(1975) J. Biol. Chem. 250, 9038-9043.8. Cole, R. P. (1983) Respir. Physiol. 53, 1-14.9. Driedzic, W. R. (1983) Comp. Biochem. Physiol. A 76,
487-493.10. Taylor, D. J., Matthews, P. M. & Radda, G. K. (1986) Respir.
Physiol. 63, 275-283.11. Wittenberg, B. A., Wong, C. F. & Wittenberg, J. B. (1986)
Biophys. J. 49, 242a (abstr.).12. Wittenberg, B. A. & Wittenberg, J. B. (1987) Biophys. J. 51,
406a (abstr.).13. Kawashiro, T., Nusse, W. & Scheid, P. (1975) Pflugers Arch.
359, 231-251.14. Mahler, M., Louy, C., Homsher, E. & Peskoff, A. (1985) J.
Gen. Physiol. 86, 105-134.15. Katz, I. R., Wittenberg, J. B. & Wittenberg, B. A. (1984) J.
Biol. Chem. 259, 7504-7509.16. Wittenberg, B. A. & Wittenberg, J. B. (1985) J. Biol. Chem.
260, 6548-6554.17. Gayeski, T. E. J. & Honig, C. R. (1986) Am. J. Physiol. 251,
H789-H799.18. Clark, A., Clark, P. A. A., Connett, R. J., Gayeski, T. E. J. &
Honig, C. R. (1987) Am. J. Physiol. 252, C583-C587.19. Wittenberg, B. A. & Robinson, T. (1981) Cell Tissue Res. 216,
231-251.20. Wittenberg, B. A., White, R. L., Ginzberg, R. D. & Spray,
D. C. (1986) Circ. Res. 59, 143-151.21. Palmer, J. W., Tandler, B. & Hoppel, C. L. (1977) J. Biol.
Chem. 252, 8731-8739.22. Cole, R. P., Sukanek, P. C., Wittenberg, J. B. & Wittenberg,
B. A. (1982) J. Appl. Physiol. 53, 1116-1124.23. Degn, H. & Wohlrab, H. (1971) Biochim. Biophys. Acta 245,
347-355.24. Giardina, B. & Amiconi, G. (1981) Methods Enzymol. 76,
417-427.25. Gill, S. J. (1981) Methods Enzymol. 76, 427-438.26. Yu, C. A., Yu, L. & King, T. E. (1974) J. Biol. Chem. 249,
4905-4910.27. Riccio, P., Schagger, H., Engel, W. D. & von Jagow, G. (1977)
Biochim. Biophys. Acta 459, 250-262.28. Reddy, K. V. S. & Hendler, R. W. (1983) J. Biol. Chem. 258,
8568-8581.29. Weiss, H. & Kolb, H. J. (1979) Eur. J. Biochem. 99, 139-149.30. Hatefi, Y. & Galante, Y. M. (1980) J. Biol. Chem. 255,
5530-5537.31. Strittmatter, P. & Velick, S. F. (1956) J. Biol. Chem. 221,
253-264.32. Strittmatter, P. (1960) J. Biol. Chem. 235, 2492-2497.33. Spatz, L. & Strittmatter, P. (1971) Proc. Natl. Acad. Sci. USA
68, 1042-1046.34. Li, Y., Leonard, K. & Weiss, H. (1981) Eur. J. Biochem. 116,
199-205.35. King, T. E. (1983) Adv. Enzymol. Relat. Areas Mol. Biol. 54,
267-366.36. von Jagow, G. & Link, T. A. (1986) Methods Enzymol. 126,
253-271.37. Wikstrom, M. & Saraste, M. (1984) in Bioenergetics, ed.
Ernster, L. (Elsevier, Amsterdam), pp. 49-94.38. Tamura, M., Araki, R., Ishikawa, T., Sagisaka, K. &
Yamazaki, I. (1980) J. Biochem. (Tokyo) 88, 1211-1213.39. Bergersen, F. J., Turner, G. L. & Appleby, C. A. (1973)
Biochim. Biophys. Acta 292, 271-282.40. Wittenberg, J. B., Bergersen, F. J., Appleby, C. A. & Turner,
G. L. (1974) J. Biol. Chem. 249, 4057-4066.41. Wittenberg, J. B. (1980) in Nitrogen Fixation, eds. Orme-
Johnson, W. H. & Newton, W. E. (University Park Press,Baltimore), Vol. 2, pp. 53-67.
42. Appleby, C. A. (1984) Annu. Rev. Plant Physiol. 35, 443-478.43. Bergersen, F. J. (1982) Root Nodules of Legumes: Structure
and Functions (Research Studies Press, Wiley, Chichester,U.K.).
Biochemistry: Wittenberg and Wittenberg


























![Influencia Personal[7507]](https://img.pdfslide.net/doc/110x75/55cf9503550346f57ba5f392/influencia-personal7507.jpg)


