8/14/2019 Myotonic Muscular Dystrophy[1]
1/2
JAPI VOL. 55 MARCH 2007 www.japi.org 249
[b] a significant number of cases occurring below 50years of
age, [c] Absence of gastric cancer as part ofcancer family
syndrome, [d] additional risk posed byfried food. Since patient
number was small, these resultsneed confirmation by larger field
studies.
G Ray+, S Dey*, S Pal++Senior Medical Officers; *Post Graduate
[DNB] Trainee,Gastroenterology Unit, Department of Medicine, B.R.
Singh(Central) Hospital, Eastern Railway, Sealdah, Kolkata.Received
: 28.5.2005; Revised : 12.12.2006; Accepted :30.1.2007
REFERENCES1. Cancer. In: K Park, Ed. Parks Textbook of
Preventive and
Social Medicine (18th edition). Jabalpur: M/S Banarsidas
BhanotPublisher. 30210.
2. Development of An Atlas of Cancer in India. First All
IndiaReport 20012002. Nandakumar A, Gupta PC, Eds. NationalCancer
Registry Programme (ICMR), Bangalore, 2004.
3. Malhotra SL. Geographic distribution of gastrointestinal
cancerin India with special reference to causation. Gut
1967;8:36172.
Myotonic Muscular Dystrophy
Sir,
The disease is seen worldwide with a particularlyhigh frequency
in French Canadians in Quebec where allcases can be traced to a
single ancestor.1-3 The molecular basis of disease lies in
expansion of a trinucleotide(cytosine thymine guanine CTG) repeat
sequencein the 3untranslated region of the myotonic
dystrophyprotein kinase (DMPK) gene on chromosome 19q. Thisexpanded
gene is unstable and its size increases withage. The size of repeat
on gene is directly proportional
to clinical severity of disease and has inverse relationwith age
of onset of the disease.1-3
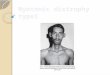
25-years-old male presented with decreased powerof gripping,
which progressed to difficulty in holdingobjects in hands over 5
years. There was difficulty inholding neck while getting up from
lying down positionand dysphagia, and nasal intonation of voice
alongwith nasal regurgitation of fluids for last 3 years. Therewas
no family history of the disease. On examinationatrophy of muscles
of face (hatchet shaped face),temporalis, masseter along with
sternocleidomastoid bilaterally was noted (Fig. 1). Percussion
myotonia
could be demonstrated both on thenar muscles (Fig.2) and tongue.
Rest of neurological examination andsystemic examination was
normal. EMG studies showedmyotonia along with decreased amplitude
of actionpotentials and polyphasic potentials. Muscle
biopsyrevealed muscle fibers of variable size with atrophy
offibers. There was presence of central nuclei and ringfibers.
`Classical form' of the disease is seen in adolescentor early
adult life with variable presenting features.Muscular weakness,
myotonia, mental retardation,cataract, neonatal problems are common
symptoms
and about 18% remain asymptomatic.1, 3 The clinicalseverity of
the disease ranges from death in utero to
mild symptoms without physical signs in old age.2Superficial
facial muscles, levator palpebral superioris,temporalis,
sternocleidomastoid, distal muscles offorearm and dorsiflexors of
foot are most prominentlyaffected. The atrophy of facial muscles
gives typicalhatchet shaped appearance to face.
Quadriceps,diaphragm, intercostals, palatal muscles,
pharyngealmuscles, and extraocular muscles are also
commonlyinvolved. Muscles of pelvic girdle, hamstrings,soleus, and
gastrocnemius are spared.1 Smooth muscleinvolvement of
gastrointestinal tract may lead todysphagia and irritable bowel
syndrome like symptoms.
Fig. 1 : Clinical photograph of patient showing atrophy of
facialmuscles, muscles of mastication (hatchet facies) and atrophy
of
neck muscle.
Fig. 2 : Percussion myotonia in thenar muscle of hand.
8/14/2019 Myotonic Muscular Dystrophy[1]
2/2
250 www.japi.org JAPI VOL. 55 MARCH 2007
Conduction defect and cardiomyopathy denotes cardiacinvolvement.
Cataract, frontal baldness in male, gonadalatrophy, hypersomnia,
mild endocrinal anomalies, bonechanges and abnormalities of
immunoglobulins can beother associated disorders.1-3
`Congenital form ' is evident at birth with history
ofpolyhydramnios and poor fetal movement in pregnancy.
There can be respiratory and feeding difficulty inneonatal
period with death of few, in those survivinguntil late teens or
early adulthood, hypotonia resolvesand motor function improves but
during adolescencethe features of classic adult form appear. The
late onsetform' is associated with a small CTG-repeat expansionand
is typically asymptomatic or oligosymptomatic.1-3Death is usually
due to respiratory infections or cardiaccause.
There is currently no specific therapy. The surgicalprocedures
are avoided due to associated anestheticsensitivit y,
postoperativel y respiratory muscle
inadequacy with high incidence of arrhythmias. Thesepatients
require regular, general, and neuromuscularassessment for detection
and correction of systemicdisorders and for better quality of life.
Physiotherapy,occupational advice, and speech therapy all have
a
role in such patients. Genetic counseling by means ofchorionic
villous sampling can be offered for screeningto the members of
family affected.1-3
SK Mahajan*, BR Sood*, V Chauhan**, S Thakur***,LS
Pal+*Registrar, **Post Graduate, ***Associate Professor,
+Professorand Head, Department of Medicine, I. G. Medical
College,Shimla (H. P.).Received : 13.10.2003; Revised : 17.8.2004;
Re-revised : 1.2.2007;Accepted : 8.2.2007
REFERENCES1. Brook JD. Molecular basis of myotonic dystrophy:
expansion of a
trinucleotide (CTG) repeat in the 3 end of a transcript
encodinga protein kinase family member. Cell 1992;68:799-808.
2. Harper PS. Myotonic dystrophy and other autosomal
musculardystrophies. In Scriver CS, Blaudet AL, Sly W S et al
(Edi).The Metabolic and Molecular Basis of Inherited disease
7thEdi. Mcgraw Hill, Inc Health Profession Division New
York1995;III:4227-41.
3. Hilton-Jones D. Myotonia. Oxford Textbook of Medicine.
WarrelDA, Cox TM, Firth JD, et al (Edi) 4th Edi Oxford University
Press.
Oxford 2003;I:480-1.
STATEMENT OF OWNERSHIP
Statement about ownership and other particulars about newspaper
(Journal of the Association of Physicians of India) to
be published in the first issue every year after last day of
February.
Form IV (see Rule B)
1. Place of publication Turf Estate, Unit No. 6 and 7, Opp.
Shakti Mill Compound,Off Dr. E Moses Road, Mahalaxmi (W), Mumbai
400 011.
2. Periodicity of its publication Monthly
3. Printer's name Dr. Shashank R JoshiNationality IndianAddress
Turf Estate, Unit No. 6 and 7, Opp. Shakti Mill Compound,
Off Dr. E Moses Road, Mahalaxmi (W), Mumbai 400 011.
4. Publisher's name Dr. Shashank R JoshiNationality
IndianAddress Turf Estate, Unit No. 6 and 7, Opp. Shakti Mill
Compound,
Off Dr. E Moses Road, Mahalaxmi (W), Mumbai 400 011.
5. Editor's name Dr. Shashank R Joshi
Nationality IndianAddress Turf Estate, Unit No. 6 and 7, Opp.
Shakti Mill Compound,Off Dr. E Moses Road, Mahalaxmi (W), Mumbai
400 011.
6. Name and address of individuals Association of Physicians of
India.who own the newspaper and partners Turf Estate, Unit No. 6
and 7, Opp. Shakti Mill Compound,or shareholders holding more than
one Off Dr. E Moses Road, Mahalaxmi (W), Mumbai 400 011.per cent of
the total capital
I, Dr. Shashank R Joshi, hereby declare that the particulars
given above are true to the best of my knowledge and belief.
Sd/-Dr. Shashank R Joshi
Signature of Publisher