Embed Size (px)
Citation preview

1690
Journal of Food Projection, Vol. 69, No. 7, 2006, Paces 1690-1698Copyright s., international Association for Food Protection
Mysterious Outbreaks of Gastrointestinal Illness Associatedwith Burritos Supplied through School Lunch Programst
ELLEN B. STEINBERG,. 2 ALDEN HENDERSON, 3 ADAM KARPATI,-- t MIKE HOEKSTRA,NINA MARANO,' JENNIFER MARTINELLI SOUZA, 4 MEG SIMONS, 5 KIRBY KRUGER,5 JENNIFER GIROUX,17
HELEN S. ROGERS, 3 MICHAEL K. HOFFMAN, 5 ABDEL-RAZAK M. KAI)RY,° PATRICIA M. GRIFFIN,'AND THE BURRITO WORKING GROUP:::
Foodh<,rne and Diary/teal Diseases 8,-one/i, Dn-i.s,on of I/arterial and Mvroiir Disea.vi'.i, Notional (stier br lit/ct -tail, i Diciot'.y. -Lpulennr lnie//iç'eni-rSen-ic e. Lpideintoiog3 Program Office. and I-lea/il, Studies Branch. Dii'ision of Ent-ironmenial Hazards and Health 87/ic-nt ,jVatjona/ (enter /Environmental Health, Cciitersfi)r Doente Control and P,'et'e,tiim,,A,/onto Geo,rttia .iO333: 8ost017 Universit y Medical ('en/Cr 7/5 Al/ton y Street,Boston, Ma.,sac/tuie//s 02118: 5I,tdian Iqeaft/t ,Seo-,c-e, P.O. I/or 160, Be/court, iVo,i/, Dakota 58316: 'North Dakota Deportment of Henit/t. 600 EastBon/et-orci Avenue, Bmsn,ork, North Dakota 58805: lniha,t He(1/fit Service, 5300 Honiettead Road N.E., A/htmquem-que, New Mexico 87110: and tuc
Depot-/meat of Agricuiiui-c', Food Safeit- and lnspectiomt Sent-ice, Aerospace Center, Room 334, 901 0 Street S. W, Washington, /).0 20024. USA
MS 05-301: Reecised 30 June 2005/Accepted 12 October 2005
ABSTRACT
From October 1997 through March1998, three outbreaks of gastrointestinal illness among school children were linkedto company A burritos. In September 1998, a similar outbreak occurred in three North Dakota schools following lunches thatincluded company B bonitos. We conducted ail to dctcrminc the source of the North Dakota outbreak, identifyother similar outbreaks, characterize the illness, and gather evidence about the cause. The investigation included epidemiologicanalyses, environmental investigation, and laboratory analyses. In North Dakota, a case was defined as nausea, headache.abdominal cramps, vomiting, or diarrhea after lunch on 16 September 1998. Case definitions varied in the other states. InNorth Dakota, 504 students and staff met the case definition: predominant symptoms were nausea (72%), headache (68c ),abdominal cramps (54%-). vomiting (24%). and diarrhea 11 The median incubation period was 35 min and median durationof illness was 6 Ii. Eating burritos was significantl y associated with illness (odds ratio, 2.6: 95% confidence interval. 1.6 to4.2). We identified 16 outbreaks that occurred in seven states from October 1997 throu gh October 1998, affecting more than1.900 people who ate burritos from two unrelated companies. All tortillas were made with wheat flour, but the fillings differed,suggesting that tortillas contained the etiologic agent. Results of plant inspections. tracehacks. and laboratory investigationswere unrevealing. More than two million pounds of hurritos were recalled or held from distribution. The short incubationperiod, symptoms, and laboratory data suggest that these outbreaks were caused by all undetected toxin or an agent notpreviously associated with this clinical syndrome. Mass psychogenic illness is an unlikely explanation because of the largenumber of sites where outbreaks occurred over a short period, the similarity of symptoms, the common food item, the lackOf publicity, and the link to only two companies. A network of laboratories that can rapidly identify known and screen forunknown agents in food is a critical part of protecting the food supply against natural and intentional contamination.
Gastroenteritis among school-aged children is a con-i-mon phenomenon leading to numerous missed school daysfor students and missed workdays for parents. Gastrointes-tinal symptoms among groups of school children followinga meal have sometimes been considered psychogenic (1,11, 18). In this article, we describe 16 related school-basedoutbreaks of gastrointestinal illness. Some were initiallyconsidered psychogenic; we present evidence that theywere due to an undetected toxin or an agent not previouslyassociated with foodborne gastrointestinal illness.
-- Author for correspondence. Present address: Ellen Steinberti Sics eitsoit.Emer y Unveii-stt School of Medicine. Department of Pediatrics. 1405Clifton Road, 3C Annex. Atlanta, GA 30322. LISA. Tel: 404-785-6104:Fax: 404 . 785-1462: E-mail: [email protected] opinions expressed ill this paper are those of the authors) and donot necessarily reflect the views of the Indiat, 1-lealth Service.Paul A. Blake, Vasucttia Reddv, Hat-old Davis. Clifford Purdy, PhyllisSparting. Charles Lattuacta. Mar y Trucksess, tin, Pruckten Eliot Gregos,T Monroe, Sonja J. Olsen. tail-ant t.ingappa. Negash Belay, RichardThurnherg. Reginald W Bennett. and Charles Warner.
From October 1997 through March 1998, three out-breaks of acute gastrointestinal illness among school chil-dren occurred in Kansas, Florida. and Geor gia. Epidemio-logic investigations identified an association between illnessand eating bonitos from company A. The illnesses werecharacterized by nausea, headache, abdominal cramps, andvomiting beginning within 60 nun of eating the burritosand lasting less than 24 h. In April 1998. company A but-ritos were recalled, and no further outbreaks linked to com-pany A were reported. Despite extensive laboratory testingof the burritos. the causative agent remained a mystery. Thepossibility of mass psychogenic illness was raised.
Oil September 1998, an outbreak similar to the threedescribed above occurred following lunch at the elemen-tary, middle, and high schools in a rural North Dakota town(population 12.000). At the elementary school, the fire de-partment was summoned to hose down the school play-ground because so many children had vomited: 38 childrenwere sent to the local hospital emergency department. All

\ 7 BURRITO OUTBREAKS1691
C hildren in these schools received free lunch in the schocicafeteria. The elementar y and middle (EM) schools werehoused in the same building and shared a kitchen: the highschool used a separate kitchen and was located nearby inanother building. The food served in the three schools wassimilar.
We initiated an investigation to determine the sourceand extent of the outbreak in North Dakota. determinewhether similar outbreaks occurred in other parts of thecountry, characterize the clinical syndrome, and gather ev-idence to identify the cause of the outbreak.
MATERIALS AND METHODS
Epidemiologic studies: North Dakota investigation. Allchildren in the FM schools who attended school on 16 Septemberand ate in the school cafeteria were eligible br inclusion in aretrospective cohort stud y . A ease was defined as nausea, head-ache. abdominal cramps. vomiting, or diarrhea in a person whoate lunch from the school cafeteria on 16 September 1998 andwhose symptoms began within the 3 (la ys following lunch. In theEM schools. only 52 1/c of ill students had eaten breakfast fromthe cafeteria, but all ill students had eaten lunch from the cafeteria.Thus, we conducted a cohort study of the EM school studentswho had eaten tunch in the school cafeteria on 16 September todetermine if a specific food item was associated with illness andto institute control measures. We included only students less than16 years old who satisfactorily completed tIle questionnaire. Weexcluded two students who reported onl y fever and three whoreported only chills. We defined the incubation period as the in-terval between lunch and the onset of nausea, headache. abdom-inal cramps. vomiting, or diarrhea, and we defined illness durationas the time between the onset and resolution of symptoms. Wealso conducted retrospective cohort investigations among the EMschool staff and high school students. Other than age, the criteriafor inclusion were the same as for tile study of EM students.
For children in kindergarten through third grade. question-naires were completed one-on-one with school or health depart-ment staff. Students in grades tour through twelve and staff com-pleted the questionnaire themselves. On the original questionnaire.EM school students were asked yes-no questions about all foodsthey ate for breakfast and lunch and the presence and timing ofclinical symptoms. A follow-up questionnaire administered to thesame students included questions about the number of burritosthey had eaten, the part of the hurrito eater), and a description ofthe taste of the burritos. The high school students and EM staffcompleted one questionnaire that included questions from both theoriginal and follow-up EM school questionnaire.
Leftover meals from the EM school kitchen were routinelydonated to a local housing development. The coordinator for thesedaily food deliveries provided a list of the 14 households thatreceived burritos on 16 September. A door-to-door to survey wasconducted anlong these households to assess illness.
We reviewed the charts of the 39 patients from the threeschools who were seen in the faced hospital emergency departmenton 16 and 17 September 1998. Information collected included dateand time of arrival, chief complaint, history of present illness.food history, past medical history. physical examination, and lab-oratory results. In addition, we interviewed physicians from theonly other hospital in the surrounding area and reviewed the emer-gency department log for 16 and 17 September.
Epidemiologic studies: national investigation. To identifyother outbreaks, we solicited reports of outbreaks from county and
state heal ill departments via phone calls and a letter faxed to allstate and territorial epidemiologists and public health laboratories.In addition, we contacted the manufacturers of the suspect burn-tos. companies A and B. schools, and one juvenile detention cen-1cr that reported illness to company B. For the purpose of thispiper. we henceforth refer to the juvenile detention center as aschool. Some outbreak sites involved multiple schools iil the samecounty but were counted as a single outbreak for the purpose ofanalysis. To explore the possibility of intentional contaminationcaused by a supplier or disgruntled emplo yee. we reviewed workrecords, interviewed employees and nlanagers. and researchedlinks between suppliers and manufacturers.
Environmental investigation: North Dakota. Local satli-tarians inspected the school kitchens and interviewed the staffbetween 16 and 21 September. We met with the dietician, sani-iarians, and kitchen staff, and reviewed the inspections. burritohandling, and cooking procedures. The school provided us withleftover intact frozen burritos from the same lot that was servedon 16 September. and we recovered leftover partially eaten bur-ritos from the local landfill: both were sent for laboratory testing.We conducted a tracehack of the burritos and their nigredients thatextended to all distributors and the manufacturer.
Environmental investigation: national. In other outbreaklocations, school kitchens were inspected by local sanitarians andwe reviewed the inspections. biirrito handling. and cooking pro-cedures through written reports and conference calls. We request-ed that the other involved schools and health departments obtainburrito samples and clinical specimens. conducted a nationaltracehaek of products from companies A and B and their tortillasuppliers, and reviewed the results of product recalls initiated bythe U.S. Department of Agriculture (USDA) and the burrito man-ufacturers.
We conducted extensive plant investigations of company Band its tortilla suppliers. Tile ilvestigatilg teanl, which includedinspectors and epidemiologists from the earlier nlvestigatiOns ofcompany A and its tortilla suppliers, reviewed reports fronl thecompany A investigation: examined burrito preparation, cooking,freezing. storage. and shipping processes: evaluated chemical us-age, maintenance procedures. pest control, and employee practic-es. compared the procedures of companies A and B: and reviewedlocal health department inspection reports of company B's tortillasuppliers.
Laboratory investigation: patients. In North Dakota. conl-plete blood counts and serum electrolyte and glucose levels weremeasured for 23 of the 38 patients during the emergency depart-ment evaluation of'of patients. A vonlitus sample fronl one patientwas cultured. The USDA, Food Safety and Inspection Servicearranged for the analysis of one vomit sample for heavy metalsand a general drug screen. No further chemical analysis of thevonlitus was done because the sample was discarded. The analysiswas performed at the Clinical Toxicology Laboratory. New JerseyMedical School. university of Medicine and Dentistry of NewJersey. Newark. No clinical specimens were available from theother outbreaks.
Laboratory investigation: food. Burritos and tortillas wereanalyzed by laboratories at the USDA. U.S. Food and Drug Act-ministration (FDA). and Centers for Disease Control and Preven-tion (CDC) as well as by the North Dakota Department of HealthDivision of Chemistry. the California Food and Agricultural Lab-oratory. and the North Dakota State University Veterinary Toxi-cology Laboratory. Multiple laboratories were involved becauseof their expertise in the various analyses performed.

1692STEINBERG ET AL, J. Food Prot., Vol. 69, No
TABLE I. Characteristics of illness among elementar y and middle school students, high school students, and elementary and middleschool staff in North Dakota on 16 September 1998
Elementaryand middle
school students(ii375)
CharacteristicsNausea (%) 72Headache (%) 65Cramps (%) 54Vomiting (%) 26Diarrhea (%) 12
Incubation, median (h) 0.6Duration, median (h) 6.2
ElementaryHigh school and middle
students school staff Total(it = 98) (it = 31) (it = 504)
73 68 7285 53 6851 58 5418 10 2426 32 16
1.2 1.5 0.76 12 6
We conducted careful analysis of lot numbers and shipmentsto ensure that the burritos analyzed were from lots associated withillness. In total, burrito and tortilla samples from five outbreaksites were analyzed. Burritos collected from a USDA lunch pro-gram and a commercial market that were not associated with anyoutbreak served as negative controls.
Burritos and tortillas from the live outbreaks were analyzedfor Bacillus cereus, Staph vlococcal aureus and their emetic tox-ins, mycotoxins (e.g., deoxynivalenol [DON], acetyl-deoxynival-enol, and other tricothecenes), trace metals, nonmetal ions (e.g..fluorine), plant toxins (e.g., alkaloids), pesticides (e.g., pyrethrins,organophosphates, and chlorinated hydrocarbons), food additives(e.g., glutamate), and spoilage factors (e.g., biogenic amines). Inaddition, cell culture assays, brine shrimp assays, mouse feedingstudies, and gas chromatography and mass spectrometry were per-formed in an attempt to detect new classes of agents or toxins.
Following completion of the epidemiologic investigation andlaboratory analysis, a veterinary toxicologist (A.-R. M. Kadry)reviewed the outbreak reports as did a medical toxicologist (M.Belson), assisted by the use of two databases (12, 13) to helpidentify chemical, medicinal, and biologic agents that could havecaused these outbreaks.
Statistical analysis. We conducted statistical analyses withEpi Info version 6.04 (CDC. Stone Mountain, Ga.) and SAS 8
No. caw',700
906070605040302010
0.511.522.533.54 >4
1-lours after lunch
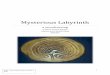
FIGURE 1. Onset of s ymptoms by quarter-hour after lunch amongelementary-middle school students, September 1998, North Da-kota (n = 266 with data).
(SAS Institute Inc, Cary, N.C.). We calculated frequencies of clin-ical characteristics for the three cohorts in North Dakota both in-dividually and combined and examined factors possibly associatedwith disease with bivariate and multivariate techniques; we con-sidered a P-value of 0.05 to be significant. Logistic regressionwas used to examine multivariable models.
RESULTS
Epidemiologic and clinical investigations: NorthDakota. In total, 975 EM school students reported that theyate the school lunch served on 16 September. Of the 950(97%) of them who ate the lunch and satisfactorily com-pleted the questionnaire, 375 (40%) had illness that met thecase definition. The most common symptoms among thosewho were ill were nausea (72%), headache (65%), abdom-inal cramps (54%), vomiting (26%), and diarrhea (12%)(Table I). The median incubation period was 35 mm (Fig.1), and the median duration of illness was 6.2 h. Nineteenpercent of ill students sought health care: none were hos-pitalized or died. Fifty-six percent of ill students and 44%of well students were female. The median age was 11 years(range 5, to 15 years) among ill students and 8 years (range,5 to 14 years) among well students. Most children ate thesame foods because the same six food items were placedon every child's lunch tray. Children ate by grade level,and the lower grades generally ate earlier.
Children in higher grades were more likely to be ill(chi-square for trend, P < .001). Controlling for children'sgrade level in a multivariate logistic regression model, wefound that ill students were significantly more likely thanwell students to have eaten burritos (91 versus 84%; oddsratio [OR], 2.6; 95% confidence interval [CIJ, 1.6 to 4.2)(Table 2). Ill students were also more likely to have eatentaco sauce. Although this association was marginally sig-nificant after we adjusted for burrito consumption (OR, 1.5:95% Cl. 1.0 to 2.1), the two exposures were colinear. Inaddition, case exposure for sauce was substantially less thanfor burritos; therefore, we did not include sauce in the de-scriptive model. Too few students responded to the follow-up questionnaire for us to formally categorize observed bur-rito taste, and there was no consistent pattern to the re-sponses. Taste descriptions ranged from moldy to sour tometallic; none of the students reported a soapy taste. Too

[¼()J I>N1.. \o]. (()• No -, B RRl I () 01 I I ILl \K I 603
TABLE 2. Lunch items consumed by elementary and middleschool students in North Dakota on 16 September 1998"
IllWellstudentsstudents
(n = 375) (n575)Lunch item( 9)("4)OR"95" ClP-value
Burrito91842.61.6-4.2<0.001Taco sauce69551.81.3-2.5<0.00!Milk89891.50.97-2.50.07Rice44481.30.96-1.80.09Carrots57671.10.78-1.50.68Orange64790.750.54-1.10.09
OR, odds ratio: Cl, confidence interval.Adjusted for student's grade level.
few students ate only one component of the burrito, tortillaor filling, for us to assess an association of these specificcomponents with illness.
High school officials did not detect an outbreak of ill-nesses in their school, and in our review of the schoolnurse's records, we found no increase in the number ofvisits for illness compared with the previous week. How-ever, questionnaire responses revealed that many of thesestudents and many EM school staff also became ill follow-ing the 16 September lunch. Symptom profiles for highschool students and EM school staff were similar to thoseof the EM school students except that the incubation periodwas slightly longer (Table I). In response to an open-endedquestion about the taste of the burritos, high school studentsand EM school staff also described a range of tastes withouta consistent pattern; three noted a metallic taste and two asoapy taste. We found no dose-response relationship or dif -ference in attack rate associated with when respondents atelunch. In total, 97% of ill high school students and 92% ofill FM school staff ate burritos. Overall. 504 (41%) of the1,253 students and staff met the case definition.
Interviewers were able to contact someone in 4 of the14 households that received leftover burritos from the EMschool kitchen. In these households, two people reportedbeing ill within 24 h after eating food left over from the 16September lunch; both had consumed a burrito. Theirsymptoms included nausea and abdominal cramps.
We reviewed the medical charts of 39 people treatedin the emergency department: 36 EM students, two highschool students, and one staff member. In our analysis, weexcluded one patient because he developed symptoms be-fore 16 September. All had eaten burritos at the schoollunch on 16 September and were evaluated the same day.The most common symptoms were vomiting (58%), nausea(53%), abdominal cramps (50%), and headache (11%).Twenty-one patients (55%) had abdominal tenderness,which was reported as mild in 12 (58%) patients and severein 9 (42%). No other muscarinic, nicotinic, or central ner-vous system findings were noted. No students or staff werehospitalized. No visits because of similar illness to the othernearby hospitals were identified.
Epidemiologic and clinical investigations: national.Including the North Dakota outbreak, we identified 16 out-breaks of similar illness in seven states between October1997 and October 1998 that were associated with eatingburritos served in schools. These outbreaks occurred inFlorida (5), Georgia (4), Illinois (2), Kansas (2), Indiana(I), North Dakota (I), and Pennsylvania (1). A total of1,908 people in 125 schools at these 16 sites reported beingill. All outbreaks occurred in schools. Although case find-ing was not done for adults in most outbreaks, 41 adultillnesses were documented. The extent of case finding andepidemiologic investigation in the different outbreaks var-ied; formal epidemiologic investigations done in only sevenof them (Table 3). In addition, case definitions varied. Insome outbreaks for which no formal epidemiologic inves-tigations were conducted, only people who vomited werecounted as cases; whereas, in others, people with vomiting,diarrhea, or abdominal cramps were counted. Outbreaks inFlorida, Georgia, and Illinois occurred on the same date asthe outbreak in North Dakota.
The clinical characteristics of illness were similar in all16 outbreaks. Nausea, cramps, or vomiting were present inpatients in all outbreaks. Headache was present in morethan 30% of patients in five of six outbreaks where thisinformation was obtained. The median incubation periodranged from 10 min to I h.
Burritos were epidemiologically implicated in sevenoutbreaks (Table 3). In the nine other outbreaks for whichlimited epidemiologic investigations were conducted, mostor all ill people ate burritos. All of the burritos were madeby the same two unrelated companies (companies A andB).
Environmental investigation. In North Dakota, wefound no major deficiencies in sanitation, food-handling, orburrito-preparation procedures. No kitchen staff at eitherschool had gastrointestinal illness before the lunch. In theother 15 outbreaks, no major deficiencies were reported.
The first three outbreaks, which occurred from October1997 through March 1998, were linked to burritos manu-factured by company A. No major deficiencies or violationswere noted in reports of inspections of company A and itstortilla supplier. After company A burritos were recalled inApril 1998, no further outbreaks were linked to companyA. The next 13 outbreaks, which occurred from Maythrough October 1998, were linked to company B (Fig. 2).All of the outbreaks were linked to burritos made with tor -tillas from a single supplier Y. In September 1998, companyB recalled burritos made with tortillas from supplier Y. Therecall was restricted to such products because the outbreaksbegan a few months after company B changed from tortillasupplier X to supplier Y. Although two outbreaks occurredafter the recall, both were linked to product made beforethe recall. More than two million pounds of burritos wererecalled or held from distribution.
Burritos consist of meat or vegetable filling wrappedin a corn or wheat flour tortilla. North Dakota company Bburrito filling consisted of water, beef, beans, seasoning(salt, spices, sugar, paprika, paprika extract, onion powder,
A

1694STEINBERG ET AL. Food Prot.. Vol. 69. No. 7
TABLE 3. Burriro-asociated outbreaks .161- which formal epidemiologic evaluations were conducted in the United States trout October1997 through October 1998°
Associationwith burritoMeasure of
Date State No. ill"CompanyconsumptionOR or RR95% CI
October 1997February 1998March 1998August 1998September 1998September 1998October 1998
KansasFloridaGeorgiaFloridaNorth DakotaGeorgiaFlorida
226 AOR21.2
18 ARR14.8
155ARR 7.1
635 BOR40.0
500B OR 5.5
107B RR 2.2
58B OR 8.8
5.8-101.33.4-64.03.8-13.05.0-850.01.5-24.01.5-3.21.8-47.6
° OR, odds ratio: RR, relative risk; Cl, confidence interval.Case definitions varied from more inclusive (e.g., North Dakota: nausea, headache, abdominal cramps, vomiting, or diarrhea) to morerestrictive (e.g.. Kansas: nausea, abdominal cramps, or vomiting).
dehydrated garlic, dextrose), textured vegetable protein(TVP) (soy protein concentrate, caramel color, zinc oxide,niacin amide, ferrous sulfate, copper gluconate, vitamin Apalmitate, calcium pantothenate, thiamine mononitrate, pyr-idoxine hydrochloride, riboflavin, cyanocobalamin), andtortillas consisted of enriched bleached wheat flour (flout;malted barley flour, niacin, reduced iron, thiamine mono-nitrate, riboflavin, folic acid), water, vegetable shortening(partially hydrogenated soybean and cottonseed oil),ding (sodium acid phosphate, sodium bicarbonate, corn-starch, monocalcium phosphate), salt, calcium propionate,potassium sorbate, monosodium phosphate, annatto color.The fillings of the burritos served in the 16 outbreaks var-ied: beef and pinto beans in 13 outbreaks, chicken and pintobeans in 1 outbreak, pork-sausage and egg in 1 outbreak,and beef in I outbreak. The tortillas in all 16 outbreakswere made with wheat flour. Company A and its tortillasupplier were located in Colorado; company B and its tor-tilla suppliers were located in Illinois.
All of the burritos were labeled as USDA-inspectedand supplied to school lunch programs. The North Dakotaschools purchased the burritos with federal funds for the
C'uinpans ACoiiipaim 3
No. outNrc,ik Recall B
Recall A
o'd.5.tS 540Q— 1997—I99s-
Month
FIGURE 2. Outbreaks of gastrointestinal illness associated withburritos, by month, United States, October 1007 through October1998 (n - 16).
National School Lunch Program: this information was notobtained for the other outbreaks. In 15 outbreaks, the bur-ritos were prepared and frozen at company A or B and thenheated at the schools. In the other outbreak, the filling wasprepared in the schools from ingredients purchased locallyand wrapped in tortillas supplied by company B. In thatoutbreak, company B had purchased tortillas from supplierY and repackaged them for distribution in a company B
The spices and minor ingredients did not vary substan-tially. Companies A and B had no common first-line sup-pliers of ingredients. However, the tortilla supplier for com-pany A obtained approximately 40% of its wheat fromNorth Dakota, and all the wheat for the tortillas used bycompany B was from North Dakota. Grain froni North Da-kota used to make the tortillas was reportedly stored in siloson farms and later as flour in silos at the tortilla producer'sfactory. During the season that the grain was harvested forthe tortillas, flooding had occurred in North Dakota, andfarmers and mill operators reported that some of the graincrop was moldy.
To allow for appropriate cooling. company B reportedthat burritos should be shipped 72 h or more after pack-aging. In reviewing records of shipping times, we foundthat burritos associated with outbreaks were often shippedearly. This analysis, however, was limited by incompleteshipping records. For example, at some outbreak sites, lotswere identified that were not listed in the shipping recordsand therefore could not be included in the analysis. Recordswere available for 858 lots shipped during the outbreakperiod from May through August 1998. These records in-cluded lots that were involved in outbreaks in seven schooldistricts. The lots were shipped from less than I day to 133days after being produced and packaged. Three (50%) ofsix lots shipped within 1 day of packaging were associatedwith outbreaks as were 3 (23%) of 13 lots shipped within2 days, and 2 (6%) of 32 lots shipped within three days ofpackaging (chi square = 0.047). Although the records wereless precise for lots shipped 3 or more days after packaging,only between I and 3% (between 11 and 22 of 807) of suchlots could be linked to outbreaks.
Plant inspections of companies A and B and their re-
leav-box.

hot.. Vol. 69. No. 7 BURRITO OUTBREAKS1695
spective tortilla suppliers did not reveal any other majorproblems in procedures or sanitation that could be linkedto the illness, and we found no relationship between com-panies A and B.
Laboratory investigation. All 23 patients from theemergency department evaluation in North Dakota hadcomplete blood counts, serum electrolytes, and glucose lev-els within normal laboratory reference ranges. The vomitussample collected at the hospital emergency departmentgrew a pure culture of Staph viococcus aureus: enterotoxintesting was not done.
Extensive chemical and microbiological testing wasperformed in nine laboratories (six federal, one state, andtwo academic) from November 1998 through February2001. The results for all analyses on burritos and tortillaswere negative (Table 4) with two exceptions. The aluminumconcentration was above the reference range. Octicizer, anorganophosphate ingredient used in the production of plas-tics, was detected in trace amounts in the burrito and tortillasamples that were associated with the outbreaks and in con-trol burritos. The concentration of octicizer could not bequantified; however, the amount in the control burritos waslower than in those associated with the outbreak.
DISCUSSION
We identified 16 outbreaks of a distinctive acute gas-trointestinal syndrome linked to burritos over a 13-monthperiod. The variety of fillings in outbreak-associated bur-ritos, the fact that outbreaks linked to company B bulTitosbegan shortly after that company changed its tortilla sup-plier, and the association of one outbreak with burritos pro-duced with locally made filling but tortillas from an impli-cated company strongly suggest that the etiologic agent wasin the tortillas. These outbreaks affected over 1,900 peopleparticipating in school lunch programs. A recall of burritoslikely prevented further cases. The remarkably short incu-bation period, the clinical symptoms, and negative labora-tory data suggest that these outbreaks were caused by anundetected toxin or an agent not previously associated withfoodborne illness.
Mass psychogenic illness is an unlikely explanation forthese outbreaks for several reasons: the number and loca-tion of sites where outbreaks occurred over a short period,the similarity of symptoms, the common food item, the lackof publicity, and the link to only two companies. However,it is possible that a psychogenic component contributed tothe number of reported cases of illness in some locations.
The short incubation period and the symptoms of theillness suggest that a preformed toxin or other short-actingagent that targets the stomach or upper intestine is the eti-ologic agent. However, the symptom complex in these out-breaks does not fit the usual clinical spectrum for the knowncauses of short-incubation gastrointestinal illness. Theagent's likely introduction in two unrelated tortilla plantsand the recognition of outbreaks with only certain batchesof tortillas both suggest that the agent was introduced in-termittently possibly via a contaminated ingredient or pieceof equipment. The early shipping of burritos before appro-
priate cooling may have provided an environment that al-lowed the causative agent to flourish or produce toxin if itwere living. Characteristics of the etiologic agent might in-clude the ability to survive the baking, storage, or reheatingprocesses: moderate to high potency: and indistinct organ-oleptic properties.
In outbreaks caused by B. cereus emetic toxin and S.aureus enterotoxin, headache is not a prominent feature,and the usual incubation period is 2 to 4 h (10, 14). BecauseS. aureus is routinely found in the oropharynx, we did notconsider a single culture of S. aureus isolated from a vom-itus sample to be significant. Moreover, food samples fromfive outbreaks were negative for B. cereus and S. aureusorganisms and toxins. In norovirus outbreaks, the incuba-tion period is longer (24 to 48 h), the duration of illnesslonger (12 to 60 h), and the proportion of patients withvomiting is higher (over 50%) than in the burrito-associatedoutbreaks. In addition, secondary transmission of norovi-ruses to household members occurs commonly (9) but wasnot reported in the burrito-associated outbreaks.
Pesticide poisoning typically causes additional symp-toms that were not described in these outbreaks, nor werepesticides, alkaloids, or biogenic amines detected in theburritos or tortillas. Some metals, such as cadmium, copper,iron, tin, barium, and zinc, can irritate mucosal membranesand cause sudden gastrointestinal illness; however, the onlymetal that was mildly elevated in the burritos was elementalaluminum, which has not been reported to cause thesesymptoms (3, 8). Calcium chloride ingestion can causerapid-onset nausea and vomiting, but in amounts largeenough to induce symptoms, the food would likely tastetoo salty to be palatable. Moreover, the calcium levels inthe burritos and tortillas were not elevated. Two metals notincluded in the screen were thallium and antimony. How-ever, thallium poisoning is typically associated with neu-rological symptoms, and antimony food poisoning usuallyoccurs when the metal is leached by acidic foods in a me-tallic container. Signs and symptoms of people who becameill were not compatible with thallium poisoning, and theburritos and tortillas were packaged in plastic bags or card-board boxes.
Several plant toxins, such as phytohemagglutinin, maysurvive cooking and cause gastrointestinal symptoms; how-ever, previous outbreaks associated with phytohemaggluti-nin have been linked to red kidney beans and not pintobeans, which were an ingredient in some of these burritos(17). Furthermore, beans were not in the filling of burritosassociated with two of the outbreaks, and results of testsfor these compounds were negative. The soy protein foundin TVP may cause gastroenteritis; however, TVP can alsocause other symptoms such as difficulty breathing, facialflushing, and swelling of the tongue, lips, or face (7). More-over, TVP was not an ingredient in burritos associated withtwo of the outbreaks.
Although octicizer was detected in trace amounts inoutbreak-associated burritos, this organophosphate seemsan unlikely cause of these outbreaks. Burritos were not indirect contact with plastic before consumption. They wereplaced in a cardboard box; the box was then wrapped in

'1)C-)
CC)
00
C)C)—
C
C)
30C-)z
C) C).3-3
C) C)C) C.)
V C)
CCz
C)
Oc
Sr.5
=
305 .3 3C33.
z
C-0
Sr
4C
C) C)
0 . CC
t C) SCC
zz
C)-C
-C) C) C)0 > >
Cl) C-C CLO ) C) C))ZZZ
C-)
-3CC CC
C)C.)C) C)C)C)
z z
Cl)
C.; C) C) C)COOC
C-
C C.).0 •
C)O C)
-C'
.9
C)CC
>- 0C.) C)
5C)
C) CCCC.C ;
C).-C-S
. CC
-C-UU
1696STEINBERG FT AL.
z <
3.LZ
- - .&C.')
Z ::)Z
UC
-oC•jC)C/5oP-2O. C-'
CC
C - C- .
U
UU-5----5uEC__)(3
I-
fj C;)
= = C-C C
C.; -C)1)C. ;l-).2-C)- C--S COC5CCC
- -C-C C)-
CCtj -C)
CC C)•_35_
C)3-
.5C)-5
.50 5 0 ,_.00_;I
5-.55
M L)
.rC - __C - > C) I C)C,•().. C) .:_t s. CC )_(( C 1<' C)__C .Cl)C)
zz'-CC —O2r - C55ç
C) - 2.)—.2C_-3-- E '-- -.-C.).— '- C) C)5_
S 5.0
-5
- C C >
-_)0 > —C) —
-5 C-> C) - V__S C)5
<0(3(33.
C)
2.s C)0C1< -C C-
=C)S .52--s
22C-—SE
5C)C) CCC.)C)
J. Food Piot.. Vol. 69, No. 7
-
V..-) .4)0
V-)-C- -
t-F
35 C C)3ZC-' o,L
C'
Cc)
0.C;CPV;-.)
C)
J;i-C--.CLLo.()C.3.
cr
wiIr
It
a-
CC.5 C (jC
p_S
C-)-___•C''
= C) . C)
—Uc C)-
V--S (IC CC.; .= -
03Cc_S
-C
--aC-CC.CVC)
C/R<
S
-5
.-5<czC)
U
-C 0 Ci) C)
CL)-) C)C'.-C
.EU..L>C.5-)tlj
C)•_ss2<
LLI
09= '1)<CCC.CIC3:<_S-CCCC.
CC.
o;
C-I.CC) C) C5CC .5. -
C.0
CC C) (IC
-ftC/_)CC-CC)
5 ? S <
S C).0 -C S.5.2.5 CCC) '
<CL; S- -5-s
E<
C;
U
3.C...
<C/DC/•) DUU
C.)C 5
-C;
H
H
0
0\
0.3
N. C3' t
C
0
3.
VC). <U
(I)
cr
U(U

-ud Prot.. Vol. 69, No. 7 BURRIFO OFIFRRNAKS1697
plustic. While tortillas were packaged in plastic bags, sev-cull tortillas were in each bag and only the tortillas thatvv etC on the outside had much direct contact with the baa.On the other hand, after the oLlibreak, investigators usedplastic to wrap the burrito samples that were shipped tolaboratories for testin g . This could have introduced octiciz-cc from the plastic into the burrito samples. Octicizer irri-tates the skin and, if ingested. may cause vomiting. Octi-ci/er, like other organophosphate compounds, may alsoproduce niuscarinic, nicotinic, and central nervous systemeffects such as nuosis, lacrimation. dvspnea. and frequenturination. These t ypes of symptoms were not reported inthese outbreaks and none of these findings were identifiedduring the emergency department chart review.
Outbreaks with symptoms similar to those described inthis report have occurred in China and India. where theyhave been linked to consumption of products made withgrains contaminated with fungi. Some fungi produce heat-stable ticothccene mycotox ins called vonli toxin or DON(6) that in high doses cause vomiting in pigs (19). In China.35 outbreaks affecting 7,818 people during 1961 through1985 were attributed to consumption of foods made withmoldy grain (15). Corn and wheat samples collected duringtwo outbreaks had higher levels of DON than those col-lected at other times. In 1987. 97 people in India becameill after consuming wheat products following heavy rains(5). DON and other trichothecene mycotoxins were detect-ed in the implicated wheat products, and the extracted tox-ins caused vomiting in puppies. Damp conditions, such asoccurred during the growing season ill North Dakota whengrail) was harvested for these tortillas, can cause molds toform. However, results of laboratory tests of burrito sam-ples showed DON levels to he within the acceptable FDAadvisory level of 1 ppm for finished wheat products (2).Testing for rare mycotoxins was also negative.
Several detergents and cleaning materials were presentin the building where bLirritos and tortillas were made.These compounds may cause nausea, vomiting, and abdom-inal cramps, but gooc1 screening tests for detergents in fooddo not exist. Although burritos were not specifically testedfor individual detergents, detergents often contain phos-phate, which was not elevated in the metal screen. In ad-dition, detergents generally have low toxicity, and a closehigh enough to cause illness would likely he accompaniedby a soapy taste, making the food unpalatable. Neverthe-less, we cannot eliminate the possibility that a detergentcaused these illnesses.
Although the hunito testing was broad and nlucll moreextensive than routine testing for toxins in food, laboratoryanalyses did not include tests for some toxic chemicals.such as boric acid, iodine, and nitrites, and some plant tox-ins. sucll as ricin and cardiac glycosides. We consideredmost of these toxins or chemicals unlikely to be the caus-ative agent for the following reasons: their likely degrada-tion in the preparation, storage, or cooking process; thepresence of incompatible symptoms or the absence of pa-ihognomonic symptoms: and the absence of typical organ-oleptic signs in case subjects. We considered other possibleagents to be unlikely because of the color of emesis and
the absence of particular symptoms (e.g.. autonomic dys-function suggesting nitrates; arrhythmias suggesting ricin oroleander). Alkaline cleaning solutions were thought unlike-ly to be the cause, given the absence of oropharyngeal in-volvement and the similar pH in outbreak and control bur-rims.
Many more cases of this illness likely occurred thanwere recognized. Most of these outbreaks came to the at-tention of public health officials because they occurred inschools where many people eat the same meal at the sametime in the same place. Some outbreaks may not have beenrecognized. such as the high school outbreak in North Da-kola, which was not initially detected. While the manufac-turers primarily produced burritos for purchase by schools,they also sold burritos and tortillas to restaurants and su-permarkets. Some other people who ate these products mayhave become ill: however, because their symptoms wouldlikely have been self-limited, they may not have recognizedthem as food related and may not have received medicalattention: thus, their illnesses would not have been reportedto public health authorities or the companies. The variationin symptom frequencies reported in the different outbreaksmay he related to differences in case finding methods andcase definitions.
Even outbreaks of mild illnesses ill school childrenelicit intense concerns among parents and school officials(4) and can have important implications for the communi-ties involved. For example. in North Dakota, some parentsof school children reportedly feared that the governmentwas poisoning their children and lost confidence in theschool lunch program. Following the outbreak, sonic chil-dren brought lunch from home, and the school stopped do-nating food to the local housing community. School offi-cials feared losing federal funding fronl the National SchoolLunch Program because of the decline in participating stu-dents.
Recognizing outbreaks of illness is key to ensuring thatinvestigations to identify the food item are conducted andthat control measures are instituted quickly. Parents andteachers should he encouraged to report possible outbreaksamong students to their local health department becausesome outbreaks may only be recognized in schools (16).Symptoms should not be dismissed too quickly as psycho-genic illness. The cause of these outbreaks remains a mys-tery. If future outbreaks of a similar illness should occur,occur,we recommend quickly obtaining clinical specimens (urine,serum, vonlitus. and stool) in consultation with the localhealth authorities and the CDC. It is also critical to saveleftover food samples, food shipping containers, and ic-ceipts; too often food is quickly discarded and thereforecannot be analyzed. The thorough and timely investigationof outbreaks among school children and other groups is animportant component of maintaining a safe food supply.Given the possibility of intentional contamination of thefood supply, a critical need exists for a network of labo-ratories that can rapidly test large numbers of clinical andfood specimens for a broad spectrum of agents and toscreen for unknown agents. To meet this need, the CDC isbuilding the Laboratory Response Network for Bioterror-

1698STEINBERG FT AL. J. Food Prol., Vol. 69. No. 7
ism. a multilevel system designed to link state and localpublic health laboratories with advanced capacity clinical,military, veterinary, agricultural, and water- and loud-test-ing laboratories.
Note added in proof. Ten similar outbreaks were re-ported to the Massachusetts Department of Public Healthand are described in the January 2006 Moth. Mortal. Wklv.Rep. ("Multiple outbreaks of gastrointestinal illness amongschool children associated with consumption of flour tor-tillas, Massachusetts 2003-2004").
ACKNOWLEDGMENTSWe thank the following individuals and organizations for their as-
sistance with the epidemiologic HINesti .gation and laborator y testing inthese outbreaks: II. Casper and B. Tacke, North Dakota State University,Veterinary Toxicolo gy Laborator y : G. Holcomb, Jr. and P. L. Lace y. HallCounty Environmental Health, Hall County Health Department. Georgia:T W. McCov and M. A. Stancil, Health District 2. Georgia: J. A. Benson.L. L. Cobb. M. L. Ray, M. M. Park, F. A. Franko, and M. F.Georgia Department of Human Resources: P. .1. Vukelic, I.. A. Shirele.and Del Streit,. North Dakota Department of Health: M. Friedman. N.Richey . and R. Hammond. Bureau of Environmental Epidemiolo gy . Flor-ida Department of Health: M. Lee. California Department of Food andAgriculture: L. Duphenais and J. Cheek, Indian Health Service: Centerfor Food Safety and Applied Nutrition and Office of Regional Operations,Food and Drug Administration. Office of Public Health and Science: C.L. Reding. M. Niernann. T. Hoepfnec L. Manis, D. Cromez-lrost, P. Rap-polee, D. Blank. M. Lankford. M. Prat. J. Hutchins. V. Cook. M. Head,B. Cray. J. Dreas. C. Henry. T. Mallinson. J. Groueck. F. Grand y , J.Donohue, K. Holland, R. Wilson. S. Hafner, A. Sell'. B. King. K. Guthrie.and B. Stancel, Food Safety and Inspection Service. U.S. Department ofAgriculture: W. P. Norred. C. W. Bacon. and K A. Voss. AgriculturalResearch Service, 'tOxicology and Mycotoxicology Research Unit, Athens,Ga.: M. Belson. Health Studies Branch, National Center for EnvironmentalHealth, CDC: C. A. Bopp. P Mead. and R. Tauxe. Divisiort of Bacterialand Mycotie Diseases, National Center for Infectious Diseases. CDC.
REFERENCES1. Anonymous. 1990. Sociogenic illness in a day care center-Florida.
Moth. Mortal. Wllv. Rep. 39:301-3042. Anon ymous. 1993. Industr y advisor y regarding deoxynivalenol
(DON) in wheat: letter to state agricultural directors, state Iced con-trol officials, and fond, feed, and grain trade organizations. AssociateCommissioner for Regulatory Affairs, U.S. Food and Drug Admin-istration. Rockville. Md.
3. Anonymous. 1997. Toxicological profile for aluminum. U.S. Dc-
partment of Health and Human Services, Agency for Toxic Sub-stances and Disease Registr y . Atlanta.
'I. Anonymous. 2002. Rashes amon g school children-27 states. Oc-tober 4, 200 I-June 3. 2002 Math. Motto!. WA/v. Rep. 51:524-527.
5. Bhat. R. V.. S. R. Beedu. Y. Ramakrisna. and K. L. Munshi. 1989.Outbreak of tricothecene invcotoxicosis associated ss ith consumptionof mold-damaged wheat products in Kashinir Valley . India. Lwrcet1:35-37.
6. Bullerman. L. 1997. Ftisaria and toxigenic molds other than itsper-i//i and P,',,jj//ja. p. 419-434. Ill P. Doyle. L. R. Beuchat. and
T J. Montville. (ed.) Food microbiology: fundamentals and frontiers.ASM Press. Washington. D.C.
7. Gunn. R....P R. Taylor. and F. J. G:ingarosa. 1981. Gastrointestinalillness associated with consumption of a so y protein extender. .1.low! Frye. 43:525-527.
8. Hall. A. H.. and V. 0. Robertson. 1990. Arsenic and other heavymetals. p. 1024-1034. Ill M. Haddad and J. F Winchester (ed.).Clinical management of poisoning and drug overdose. W. B. Saun-ders Co.. Philadelphia.
9. l-lcdherg. C.. and Ni. Osterholm. 1991 Outbreaks of food-borne andwaterhorne iral gastrocnteri tis. Cl/n. Micro/tb). Rev. 6:199-210.
10. Holmberg, S. D.. and P. A. Blake. 1984. Staph'. lococcal food poi-soning in the United States: new facts and old rriiscoitceptions. I., ,km. ,Wee/. /ISSOC. 251:487-489
II. Jones, L F, A. S. Craig. D. Hoy, E. W. Gtinter, D. L. Ashley. D. B.Barr. J. W. Brock, and V. Schaffner. 2000. Mass psychogenic illnessattributed to toxic exposure at a high school. V. Engl. .1. Med. 342:96-11)0.
11 Kimbrough. R. D.. K. R. Mahaffey. P. Grandjean. S. H. Sandoc, andD. D. Rutstein. 1989. Clinical effects of environmental chemicals: asoftware approach to etiological diagnosis. Hemisphere PublishingCompany. New York.
3. Lexi-Comp Inc. Lexi-Comp's clinical reference library, symptomsanalysis for toxicology. I.exi-Comp Inc., Hudson. Ohio.
14. I and, B. M. 1990. Fixtdhorne disease due to Bacillus and C/world-cvii species. Laernet 336:982-986.
15. Luo, X. Y. 1988. Outbreaks of moldy cereal poisonings in China. p.56-63. In Toxicology forum and the Chinese Aeadeln) of PreventiveMedicine. Issues in Food Safel y . Washington. D.C.
16. Mermin, J. H.. and P M. Griffin. 1999. Public health in crisis: out-breaks of Esc/u'ric/iill co/i 0157:H7 infections in Japan. Am. .1. Eje-,de,rrio/. I 50:797-803.
17. Noah. N. D.. A. E. Bender. G. B. Reach. and R. I.Gilberg . 1980.Food poisoning from raw red kidney beans. Br. Med..!. 281:236-237.
18. Philen. R. NI.. F. Ni. Krlhoarne, T. W McKinle y. and R. G. Parrish.1989. Mass sociogenic illness by proxy: parenterally reported epi-demic in an elementar y school. i_wg et 2:1372-1376.
19. Rotter. B. A. 1996. Toxicology of deoxynivalenol. I. To.vicol. Bit-iivon. Health 48:1-4.