Embed Size (px)
Citation preview

Actualizacion y revision de los avances en cancer de
prostata resistente a la castracion
Enrique Gallardo [email protected] - @EnriqueGallar12

• Consultant or Advisory Role: Sanofi, Janssen, Astellas,
Pfizer, Bayer, Roche, Ipsen.
• Speaking: Astellas, Janssen, Sanofi, Bayer.
• Grant support: Astellas, Janssen, Sanofi, Bayer.
• Participation in clinical trials: Sanofi, Astellas, Pfizer, Bayer,
Ipsen, Bavarian-Nordic, Roche, Clovis.
CONFLICTS OF INTEREST

ÍNDICE
• Introducción
• Ensayos recientes en cáncer de próstata resistente a castración M0
–PROSPER
– SPARTAN
• Discusión
• Conclusiones

PROSTATE CANCER LANDSCAPE AND THERAPIES IN 2017
Scher HI, et al. J Clin Oncol 2016;34:1402-1418
Clinical Metastases: Noncastrate
Clinically Localized Disease
Rising PSA
Noncastrate
nmCRPC
mCRPC: 1st line
mCRPC: 2nd line
mCRPC: “n” line
Abiraterone Docetaxel
Abiraterone Enzalutamide
Docetaxel Cabazitaxel Radium-223
Castration
Castration
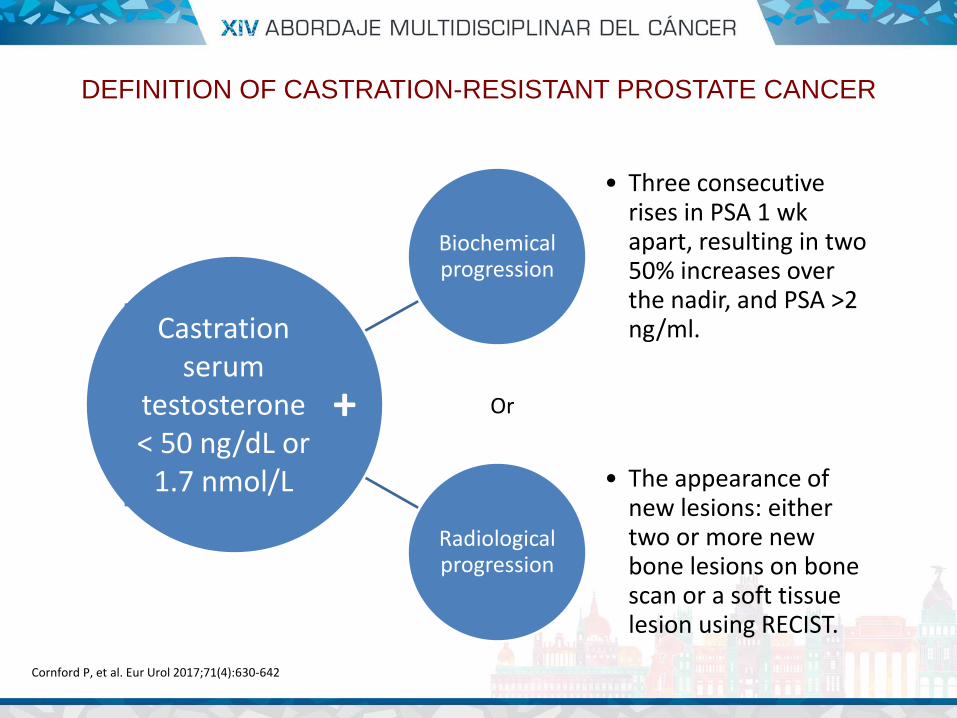
Biochemical progression
• Three consecutive rises in PSA 1 wk apart, resulting in two 50% increases over the nadir, and PSA >2 ng/ml.
Radiological progression
• The appearance of new lesions: either two or more new bone lesions on bone scan or a soft tissue lesion using RECIST.
DEFINITION OF CASTRATION-RESISTANT PROSTATE CANCER
Cornford P, et al. Eur Urol 2017;71(4):630-642
Castration serum
testosterone < 50 ng/dL or
1.7 nmol/L
Or +

AGENT/TRIAL STATUS CONTROL ARM OS (MONTHS) HAZARD RATIO P VALUE
SIPULEUCEL-T IMPACT
QT naïve Placebo 25.8 0.78 0.03
ABIRATERONE-P COU-AA-302
QT naïve Prednisone 34.7 0.81 0.0033
ENZALUTAMIDE PREVAIL
QT naïve Placebo 32.4 0.70 <0.0001
DOCETAXEL-P TAX-327
QT naïve Mitoxantrone-P 18.9 0.76 0.009
ABIRATERONE-P COU-AA-301
Post-docetaxel Prednisone 15.8 0.74 <0.0001
ENZALUTAMIDE AFFIRM
Post-docetaxel Placebo 18.4 0.63 <0.0001
CABAZITAXEL-P TROPIC
Post-docetaxel Mitoxantrone-P 15.1 0.70 <0.0001
RADIUM 223 ALSYMPCA
Pre&Post-docetaxel Placebo 14.9 0.70 <0.001
DENOSUMAB* Bone mets Zoledronic 20.7* 0.82 0.008
PHASE III TRIALS IN METASTATIC CASTRATION-RESISTANT PROSTATE CANCER
Kantoff PW, et al. N Engl J Med 2010;363:411-22. Ryan CJ, et al. Lancet Oncol 2015;16(2):152-60. Tannock IF, et al.N Engl J Med 2004;351(15):1502-12. De Bono JS, et al. Lancet 2010;376:1147-54. Fizazi K, et al. Lancet Oncol 2012;13(10):983-92. Scher HI, et al. N Engl J Med 2012;367(13):1187-97. Parker C, et al. N Engl J Med 2013;369:213-23. Fizazi K, et al. Lancet 2011;377(9768):813-22. Beer TM, et al. N Engl J Med 2014;371(5):424-33.

PRESENT THERAPIES IN CASTRATION-RESISTANT PROSTATE CANCER
Lorente D, et al. Lancet Oncol 2015:16(6):e279-92

PROSTATE CANCER LANDSCAPE AND THERAPIES IN 2017
Scher HI, et al. J Clin Oncol 2016;34:1402-18
Clinical Metastases: Noncastrate
Clinically Localized Disease
Rising PSA
Noncastrate
nmCRPC
mCRPC: 1st line
mCRPC: 2nd line
mCRPC: “n” line
Abiraterone Docetaxel
Abiraterone Enzalutamide
Docetaxel Cabazitaxel Radium-223
Castration
Castration
NO STANDARD THERAPY

ANNUAL PROGRESSION AND MORTALITY RATES FOR THE BASE-CASE MODEL IN 2009 AND 2020 PROJECTIONS
Scher HI, et al. PLOS One 2015;10:e0139440

Scher HI, et al. PLOS One 2015;10:e0139440
BASE CASE MODEL 2009

Scher HI, et al. PLOS One 2015;10:e0139440
OUTCOMES WITH INTRODUCTION OF NEW THERAPY
mCRPC incidence mCRPC prevalence mCRPC mortality

Smith MR, et al. J Clin Oncol 2013;31(30):3800-3806

Smith MR, et al. J Clin Oncol 2013;31(30):3800-3806
ODAC – FDA voted “No” to recommend denosumab indication to prevent bone mets development in high-risk M0
CRPC.
ODAC Chairman, Dr. Wilson: “There’s an assumption that delaying bone metastases is beneficial. We are looking at a
radiographicbenefit here; this is a completely artificial endpoint”.

Trial Enrollment Treatment Primary endpoint
PROSPER (NCT02003924) 1401 Enzalutamide 160 mg once daily vs
placebo Metastasis-free survival
SPARTAN (NCT01946204) 1207 Apalutamide 240 mg once daily vs
placebo Metastasis-free survival
ARAMIS (NCT02200614) 1509 Darolutamide 600 mg twice daily vs
placebo Metastasis-free survival
Positive results from the SPARTAN and PROSPER trials. ARAMIS ongoing with recruitment stopped.
M0 CASTRATION-RESISTANT PROSTATE CANCER:
THE RIGHT PATIENT FOR CLINICAL TRIAL



ClinicalTrials.gov: NCT02003924
PROSPER TRIAL
Enzalutamide
160 mg QD
Placebo QD
R 2:1
N=1401
Non-metastatic (M0) CRPC
Testosterone ≤50 ng/dL
Progressive disease with ongoing ADT
Asymptomatic
PSADT ≤10 months
• PROSPER is a multinational, Phase 3, randomised, double-blind, placebo-controlled trial
• Primary endpoint: Metastasis-free survival
MFS BENEFIT
Secondary endpoints:
• OS
• Time to pain progression
• Time to opiate use for prostate cancer pain
• Time to first use of cytotoxic chemotherapy
• Time to first use of new antineoplastic therapy
• Time to PSA progression
• PSA response rates
• QoL
• Safety

MECANISMO DE ACCIÓN DE ENZALUTAMIDA

ENZALUTAMIDE HAS PROVED SURVIVAL BENEFIT IN 1ST & 2ND LINES IN
MCRPC
Scher HI, et al. N Engl J Med 2012;367(13):1187-97 Beer TM, et al. N Engl J Med 2014;371:424-33

PROSPER – BASELINE CHARACTERISTICS
Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)

PROSPER
Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)

PROSPER
Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)

Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)
PROSPER

Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)
PROSPER

Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)
PROSPER

Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)
PROSPER

FACT-P: mean change over time (PMM analysis)
PMM assumes data missing not at random
As expected, patients in both treatment arms experienced meaningful decline in FACT-P total score (>10 points) over time; the rate of decline was significantly slower in patients treated with enzalutamide
PROSPER: longitudinal analysis of FACT-P total scores in patients with nm-CRPC
Median FACT-P value over time
In PROSPER, good HRQoL was maintained during the treatment period in both groups
Deterioration in HRQoL would be expected as patients progress and age
PMM=pattern mixed model
Tombal B, et al. 2018 EAU Meeting, Copnehagen

Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)
PROSPER

Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)
PROSPER
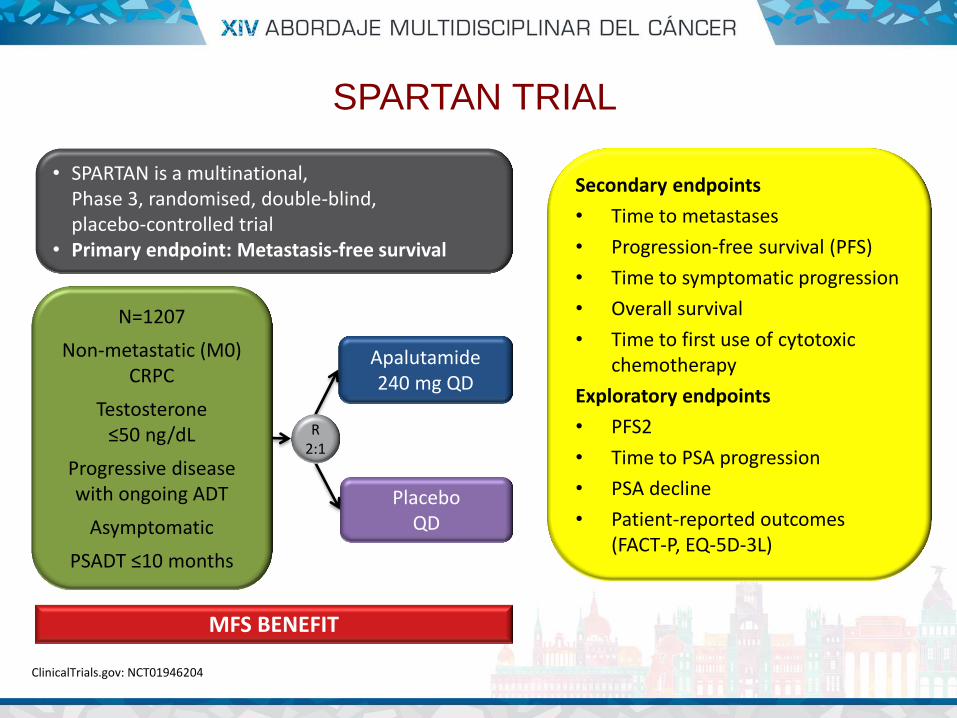
ClinicalTrials.gov: NCT01946204
SPARTAN TRIAL
Apalutamide
240 mg QD
Placebo QD
R 2:1
N=1207
Non-metastatic (M0) CRPC
Testosterone ≤50 ng/dL
Progressive disease with ongoing ADT
Asymptomatic
PSADT ≤10 months
• SPARTAN is a multinational, Phase 3, randomised, double-blind, placebo-controlled trial
• Primary endpoint: Metastasis-free survival
MFS BENEFIT
Secondary endpoints
• Time to metastases
• Progression-free survival (PFS)
• Time to symptomatic progression
• Overall survival
• Time to first use of cytotoxic chemotherapy
Exploratory endpoints
• PFS2
• Time to PSA progression
• PSA decline
• Patient-reported outcomes (FACT-P, EQ-5D-3L)

Smith MR, et al. Eur Urol 2016;70:963-970
Platinum Priority – Prostate CancerEditorial by Daniel M. Geynisman, Elizabeth R. Plimack and Matthew Zibelman on pp. 971–973 of this issue
Phase 2 Study of the Safety and Antitumor Activity of
Apalutamide (ARN-509), a Potent Androgen Receptor Antagonist,
in the High-risk Nonmetastatic Castration-resistant Prostate
Cancer Cohort
Matthew R. Smitha,*, Emmanuel S. Antonarakisb, Charles J. Ryanc, William R. Berryd,
Neal D. Shoree, Glenn Liu f, Joshi J. Alumkal g, Celestia S. Higanoh, Edna Chow[17_TD$DIFF]Maneval i[5_TD$DIFF],
Rajesh Bandekar j, Carla J. deBoer k, Margaret K. Yu l, Dana E. Rathkopf m
aMassachusetts General Hospital Cancer Center and Harvard Medical School, Boston, MA, USA; bSidney Kimmel Comprehensive Cancer Center at Johns
Hopkins University, Baltimore, MD, USA; cUCSF Helen Diller Family Comprehensive Cancer Center, San Francisco, CA, USA; dCancer Centers of North
Carolina, Raleigh, NC, USA; eCarolina Urologic Research Center, MyrtleBeach, SC, USA; f University of Wisconsin CarboneCancer Center, Madison, WI, USA;gOregonHealth& ScienceUniversity,Knight Cancer Institute,Portland,OR,USA; hUniversity of Washington,FredHutchinsonCancer ResearchCenter,Seattle,WA,
USA; i Aragon Pharmaceuticals, San Diego, CA, USA; j Janssen Research & Development, [18_TD$DIFF]Spring House, PA, USA; kJanssen Biologics, B.V., Leiden, TheNetherlands;l Janssen Research [19_TD$DIFF]& Development, LosAngeles, CA, USA; mMemorial Sloan KetteringCancer Center and Weill Cornell Medical College, New York, NY, USA
EUROPEAN UROLOGY 70 ( 2016) 963–970
avai lable at www.sciencedi rect .co m
journal homepage: www.europeanurology.com
Article info
Article history:
Accepted April 21, 2016
Associate Editor:
James Catto
Keywords:
Antitumor activity
Apalutamide
Castration-resistant prostate
cancer
Safety
Abstract
Background: Apalutamideisapotent androgenreceptor (AR) antagonist that targetstheARligand-binding
domain and preventsARnuclear translocation,DNAbinding, and transcription of ARgenetargets.
Objective: To evaluate the activity and safety of apalutamide in patients with high-risk nonmetastatic
castration-resistant prostate cancer (nmCRPC).
Design,setting, and participants: Weconducted amulticenter phase2 study of nmCRPCpatientswith a
high risk for progression (prostate-specific antigen [PSA] 8 ng/ml or PSA doubling time [PSA DT] 10
mo).
Intervention: Patients received 240mg/d apalutamide while continuing on androgen-deprivation ther-
apy.
Outcome measurements and statistical analysis: Primary end point was 12-wk PSA response (Prostate
Cancer WorkingGroup 2 criteria). Secondary end pointsincluded safety, timetoPSAprogression (TTPP),
and metastasis-free survival (MFS).
Resultsand limitations: Atotal of 51 patientswereenrolled; [20_TD$DIFF]four patients with metastatic diseasewere
excluded from theefficacy analysis.Patient characteristicsincluded median age,71 yr; Eastern Coopera-
tiveOncology Group performance status 0 (76%); Gleason score 7 (57%); median PSA10.7 ng/ml; and
PSADT 10 mo(45%).At median follow-up of 28.0 mo,18patients (35%) remained in thestudy. Overall,
89%of patients had 50%PSAdecline at 12 wk.Median TTPPwas24.0 mo (95%confidence interval [CI],
16.3mo–not reached[NR]); medianMFSwasNR(95%CI,33.4mo–NR).Most of thepatientsdiscontinued
study treatment (n=33) due to diseaseprogression (n=11 [22%]) or adverse events (AEs) (n=9 [18%]).
Themost common AEwas fatigue (any grade, n=31 [61%]) although grade 3 fatigue wasuncommon
(n=2 [4%]). These represent the first apalutamide nmCRPCpatient clinical data.
Conclusions: In high-risk nmCRPCpatients,apalutamidewassafewith robust activity based on durable
PSA responses and disease control.
Patient summary: Antitumor activity and the safety of apalutamide in patients with nonmetastatic
castration-resistant prostate cancer support continued development in this setting.
Trial registration: ClinicalTrials.gov identifier NCT01171898
# 2016 European Association of Urology. Published by Elsevier B.V. This isan open accessarticle under
the CCBY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
* Corresponding author. Massachusetts General Hospital Cancer Center, Yawkey 7030, 55 Fruit
Street, Boston, MA 02114, USA. Tel. +1 617 724 5257; Fax: +1 617 726 4899.
E-mail address: [email protected] (M.R. Smith).
http://dx.doi.org/10.1016/j.eururo.2016.04.023
0302-2838/# 2016 European Association of Urology. Published by Elsevier B.V. This is an open access article under the CC
BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Downloaded for Anonymous User (n/a) at Parc Tauli Fundation from ClinicalKey.com by Elsevier on April 09, 2018.For personal use only. No other uses without permission. Copyright ©2018. Elsevier Inc. All rights reserved.

SPARTAN – BASELINE CHARACTERISTICS
Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]
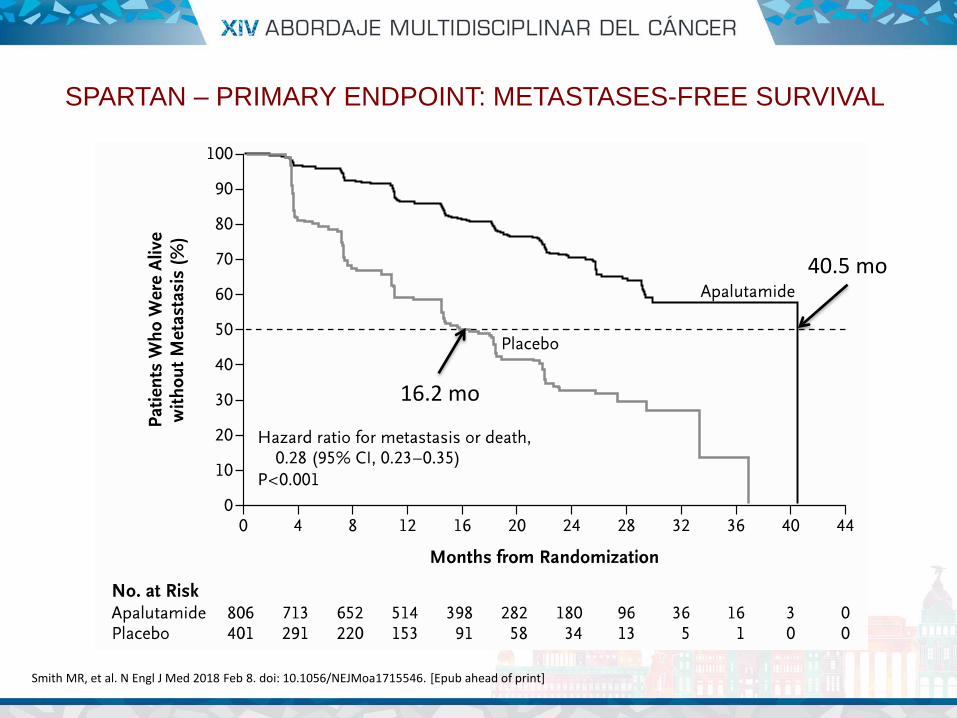
SPARTAN – PRIMARY ENDPOINT: METASTASES-FREE SURVIVAL
Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]
40.5 mo
16.2 mo

SPARTAN – MFS SUBGROUP ANALYSIS
Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]

SPARTAN – SECONDARY AND EXPLORATORY ENDPOINTS
Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]

Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]
SPARTAN – MAIN SECONDARY ENDPOINTS
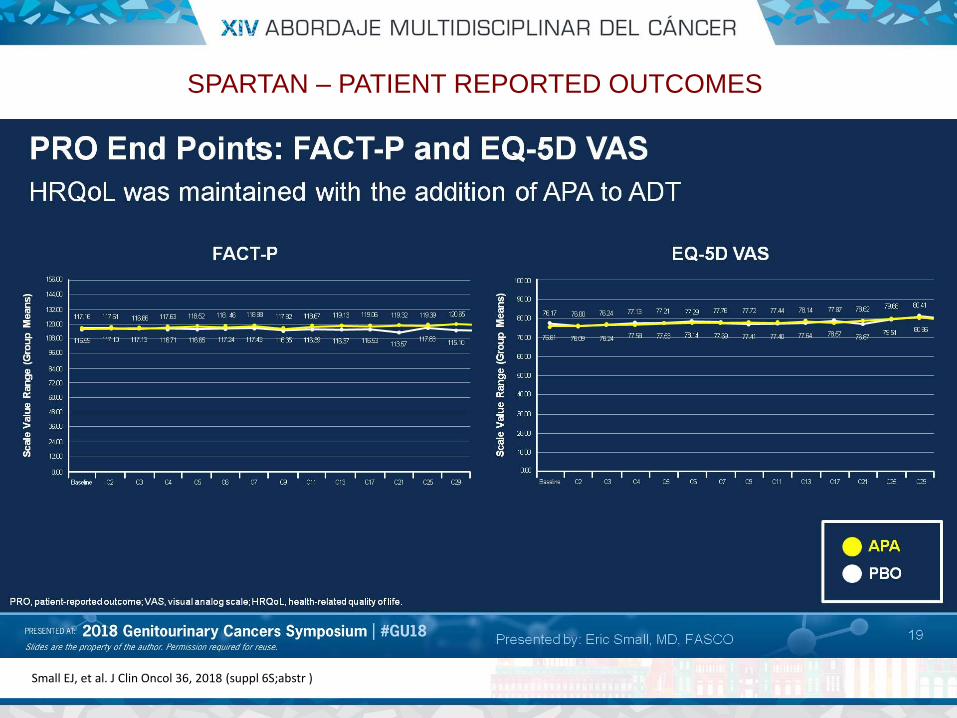
SPARTAN – PATIENT REPORTED OUTCOMES
Small EJ, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr )

Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]
SPARTAN – ADVERSE EVENTS

SPARTAN – CAUSES OF DEATH
Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]
16
Table S5. Causes of Death.
Apalutamide
(n=803)
Placebo
(n=398)
no. of patients (%)
All deaths within 28 days of last dose 10 (1.2) 1 (0.3)
Adverse event 7 (0.9) 1 (0.3)
Death due to prostate cancer 3 (0.4) 0
Other 0 0
Adverse events leading to death 10 1
Acute myocardial infarction 1 (0.1) 0
Cardio-respiratory arrest 1 (0.1) 1 (0.3)
Cerebral hemorrhage 1 (0.1) 0
Myocardial infarction 1 (0.1) 0
Multiple organ dysfunction 1 (0.1) 0
Pneumonia 1 (0.1) 0
Prostate cancer 2 (0.2) 0
Sepsis 2 (0.2) 0

SPARTAN – SUBSEQUENT THERAPIES
Small EJ, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr )

• Enzalutamide and apalutamide have
demonstrated a significant benefit in
Metastases-free survival, primary endpoint in
PROSPER and SPARTAN vs. placebo, with HR
0.29 and 0.28, and median MFS of 36.6 and
40.5 months, respectively.
• Also, benefit was present in secondary
objectives.
• However, some caveats may be considered.
PROSPER & SPARTAN
1. Do asymptomatic and M0 patients need to be
treated?
2. Is MFS an adequate endpoint?
3. Do clinical benefit balance side effects? Do
prolonged exposure to drugs provoke safety
concerns?
4. Do benefit justify costs?
PROSPER & SPARTAN

PSA DOUBLING TIME: PREDICTOR OF RISK OF METASTASES
Smith MR, et al. J Clin Oncol 2005;23(13):2918-25 Smith MR, et al. J Clin Oncol 2013;31(30):3800-6 Howard LE, et al. BJU Int 2017;120:E80-E86

Howard LE, et al. BJU Int 2017;120:E80-E86
PSA DOUBLING TIME: PREDICTOR OF SURVIVAL

M0 CRPC: SOME PATIENTS ARE REAL M1
Lorente D, et al. Lancet Oncol 2015:16(6):e279-92
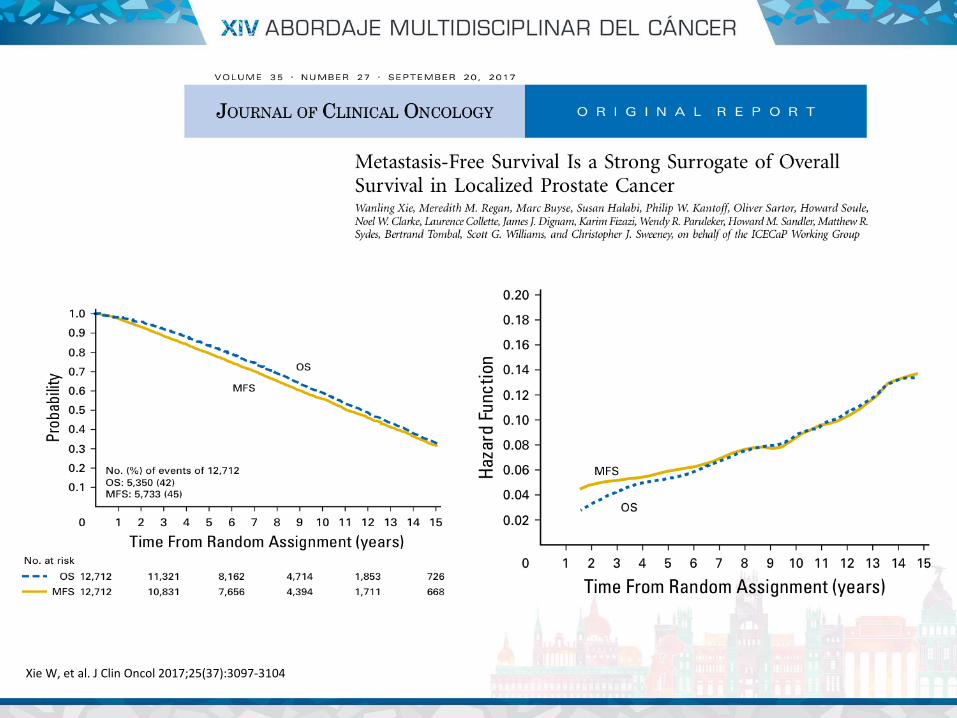
Xie W, et al. J Clin Oncol 2017;25(37):3097-3104

Morris MJ, et al. J Clin Oncol 2015;33 (12):1356-1363
rPFS MAY PREDICT OS

Rathkopf DE, et al. JAMA Oncoll 2018 Mar 8. doi: 10.1001/jamaoncol.2017.5808. [Epub ahead of print]
rPFS MAY PREDICT OS

Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]
SPARTAN – CLINICAL BENEFIT

SPARTAN – PATIENT REPORTED OUTCOMES
Small EJ, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr )

FACT-P: mean change over time (PMM analysis)
PMM assumes data missing not at random
As expected, patients in both treatment arms experienced meaningful decline in FACT-P total score (>10 points) over time; the rate of decline was significantly slower in patients treated with enzalutamide
PROSPER: longitudinal analysis of FACT-P total scores in patients with nm-CRPC
Median FACT-P value over time
In PROSPER, good HRQoL was maintained during the treatment period in both groups
Deterioration in HRQoL would be expected as patients progress and age
PMM=pattern mixed model
Tombal B, et al. 2018 EAU Meeting, Copnehagen

Small EJ, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr )
SPARTAN – ADVERSE EVENTS

SPARTAN – CAUSES OF DEATH
Smith MR, et al. N Engl J Med 2018 Feb 8. doi: 10.1056/NEJMoa1715546. [Epub ahead of print]
16
Table S5. Causes of Death.
Apalutamide
(n=803)
Placebo
(n=398)
no. of patients (%)
All deaths within 28 days of last dose 10 (1.2) 1 (0.3)
Adverse event 7 (0.9) 1 (0.3)
Death due to prostate cancer 3 (0.4) 0
Other 0 0
Adverse events leading to death 10 1
Acute myocardial infarction 1 (0.1) 0
Cardio-respiratory arrest 1 (0.1) 1 (0.3)
Cerebral hemorrhage 1 (0.1) 0
Myocardial infarction 1 (0.1) 0
Multiple organ dysfunction 1 (0.1) 0
Pneumonia 1 (0.1) 0
Prostate cancer 2 (0.2) 0
Sepsis 2 (0.2) 0

PROSPER
Hussain M, et al. J Clin Oncol 36, 2018 (suppl 6S;abstr 3)

• ¿Son enzalutamida y apalutamida nuevos SOC
en pacientes CRPC M0?
• Sí! Ensayos positivos con objetivo muy
probablemente adecuado (MFS), con
implicación estadística y clínicamente
significativa.
• Pero: Tener en cuenta exposición y toxicidades
a largo plazo, así como el coste de un
tratamiento muy prolongado.
CONCLUSIONES



PREGUNTAS

1. Tiempo hasta progresión del PSA
2. Tiempo hasta la progresión sintomática
3. Supervivencia libre de progresión
4. Supervivencia libre de metástasis
5. Supervivencia global
¿Qué objetivo consideras adecuado para la evaluación
del beneficio de un fármaco en cáncer de próstata?

1. Sí, porque son pacientes metastásicos.
2. Sí, porque retrasa la aparición de metástasis
y, por tanto, las complicaciones.
3. No, por el riesgo de efectos secundarios.
4. No, por el elevado coste y la falta de estudios
farmacoeconómicos.
5. No, porque no hay beneficio demostrado de
supervivencia global.
¿Indicarías enzalutamida o apalutamida en pacientes
con cáncer de próstata resistente a la castración M0
(con criterios de riesgo??