Embed Size (px)
Citation preview

ABSTRACT: Largely initiated by studies among Greenland Es-kimos in the early 1970s, great attention has been given to thepossible effects of the very long chain n-3 polyunsaturated fattyacids (PUFA) in a variety of cardiovascular disease states. A se-ries of possibly positive effects on pathogenetic mechanisms incardiovascular disease has evolved from laboratory studies incell cultures and animals as well as in humans, focusing mainlyon eicosanoid metabolism with reduced activities of plateletsand leucocytes, reduced plasma triglycerides and, antiarrhyth-mic effects in the myocardium. A rationale for a positive effectof very long chain n-3 PUFA in the secondary prophylaxis afterrevascularization procedures obviously also exists. The positiveclinical effects based on prospectively randomized trials aresummarized as follows. After coronary artery bypass grafting(CABG), the SHOT study showed statistically significant reduc-tion in angiographic vein graft occlusion in 610 patients after 1yr with supplementation of 3.4 g/d of highly concentrated verylong chain n-3 PUFA. The reduction in occlusion rates was sig-nificantly related to the change in the n-3 PUFA concentrationin serum phospholipids during the study period with the occlu-sion rate in the upper quartile of such changes at only ~50% ofthat in the lower quartile. These results were also clearly relatedto the presence of angina pectoris and occurrence of myocar-dial infarction after 1 yr. Several studies were conducted in pa-tients after percutaneous transluminal coronary angioplasty(PTCA). By 1993, two meta-analyses indicated a positive effecton the restenosis rate, a significant problem after otherwise suc-cessful PTCA. During the late 1990s, three large prospectiverandomized placebo-controlled angiographic studies were con-ducted with very long n-3 PUFA 5.1–8.0 g/d, all with com-pletely negative results. Today, therefore, very long chain n-3PUFA supplementation cannot be recommended to reduce theincidence of restenosis after PTCA. All studies were performedwithout stenting of the coronary lesion. In the very specialrevascularization procedure of heart transplantation, evolvinghypertension and accelerated atherosclerosis have been majorclinical problems. In other studies, positive effects by supple-mentation with very long chain n-3 PUFA (3.4–5.7 g/d) wereobtained on the surrogate end points coronary vasoreactivity toacetylcholine and hypertension, respectively. On the basis ofthe presently available literature from clinical studies, recom-mendations for supplementation with very long chain n-3 PUFAcan be given to patients after venous CABG (up to 3.4 g/d), andafter heart transplantation (3.4–5.7 g/d) but not to patients aftertraditional PTCA. In fact, data from substudies suggested the
possibility that large doses (5.1 g/d) of very long chain n-3 PUFAmight be contraindicated because they induce a proinflamma-tory state in patients under oxidative stress.
Paper no. L8804 in Lipids 36, S103–S106 (2001).
Largely initiated by the reports of Bang, Dyerberg, andcoworkers in the 1970s that a low prevalence of coronaryartery disease among Greenland Eskimos possibly was asso-ciated with their special diet rich in n-3 polyunsaturated fattyacids (PUFA) (1,2), great attention has been given to the in-fluence of these very long chain PUFA on a variety of cardio-vascular disease states.
In addition, a large number of laboratory studies in cellculture and animal models have pointed out a series of possi-ble beneficial effects of very long chain n-3 PUFA on thepathogenetic mechanisms of cardiovascular disease, focusingmainly on eicosanoid metabolism with reduced activities ofplatelets and leucocytes, lowering of plasma triglycerides,and also antiarrhythmic effects in the myocardium.
The possibility of a rationale for positive effects in rela-tion to various revascularization procedures is obviously pres-ent, and I will try to summarize the evidence that positiveclinical effects of supplementation with very long chain n-3PUFA can be expected.
Today the primary vascularization procedures includecoronary artery bypass grafting (CABG) and percutaneoustransluminal coronary angioplasty (PTCA) for coronary heartdisease; I will focus mainly on these therapeutic approaches.In addition, I will include some interesting data obtained inthe very special revascularization procedure of heart trans-plantation.
Starting with the last-mentioned data, Fleischhauer andcoworkers in 1993 (3) elegantly demonstrated in a randomizedstudy of heart transplant patients that supplementation of 5.7 g/dof very long chain n-3 PUFA normalized the pathologic reac-tivity of their coronary arteries to intracoronary injection ofacetylcholine. Thus, endothelial-dependent vasodilatationwas reestablished.
It is well known that heart transplant patients as a groupbecome hypertensive (related to their cyclosporin therapy)and experience accelerated coronary atherosclerosis. In thisconnection, Andreassen and coworkers (4) in 1997 publishedtheir results from a randomized study of 28 heart transplantpatients in which supplementation with 4 g/d of n-3 fattyacids significantly reduced the blood pressure compared witha group given corn oil. In fact, after 6 mon the systolic blood
Copyright © 2001 by AOCS Press S103 Lipids, Vol. 36, Supplement (2001)
*Address correspondence at Ullevål University Hospital, Oslo, Norway.E-mail: [email protected]: CABG, coronary artery bypass grafting; CI, confidence interval;OR, odds ratio; PDGF, platelet-derived growth factor; PTCA, percutaneoustransluminal coronary angioplasty; PUFA, polyunsaturated fatty acids.
n-3 Fatty Acids and Revascularization ProceduresHarald Arnesen*
Ullevål University Hospital, Oslo, Norway

pressure was lower than preoperatively in the n-3 fatty acidgroup compared with an increase of 17 mm Hg in the corn oilgroup. In the same period, the diastolic blood pressure had in-creased by 21 mm Hg in the corn oil group compared withonly 10 mm Hg in the n-3 fatty acid group. Of course the datamentioned relate to surrogate end points, but might give agood indication of possible clinical effects for patients in thisspecial group.
For the revascularization procedure of CABG, it is wellrecognized that up to 50% of patients experience occlusion ofvenous aortocoronary grafts by angiographic examinationafter 1 yr. The figures for occlusion of arterial grafting withthe internal mammary artery are significantly lower, ap-proaching ~15% after 5 yr.
The vein graft disease, with a high frequency of occlusionafter 1 yr, is thought to be caused initially by thrombotic occlu-sion during the first weeks, and thereafter by a specialized inti-mal hyperplasia with possible secondary thrombotic occlusion.More traditional atherosclerotic lesions may be seen in veingrafts within the first postoperative year, but generally a periodof >1 yr seems to be required for their development. Thus,processes of thrombosis, intimal hyperplasia, and traditionalatherosclerosis seem to be involved in the pathophysiology ofvein graft occlusion. Related to possible antiatherosclerotic ef-fects of n-3 PUFA, both antithrombotic and antimitogenicmechanisms might be operative.
To date, only one large prospective randomized study onthe effect of n-3 PUFA on the incidence of graft occlusion rateshas been published. This is the so-called SHOT study by Erits-land and coworkers from our research group (5). In this study,610 patients undergoing coronary artery bypass grafting wereassigned randomly to either supplementation with 4 g/d ofhighly concentrated n-3 PUFA or a control group. Simultane-ously, all patients by stratification received antithrombotictreatment with aspirin or warfarin. Both diet and serum phos-pholipid fatty acid profiles were monitored and the primaryend point was 1-yr graft patency assessed by repeat angiogra-phy. The latter procedure was completed in 95% of the pa-tients, and data on the serum phospholipid fatty acids indicatedvery good compliance with the study medication.
Vein graft occlusion rates per distal anastomoses were27% in the n-3 PUFA group and 33% in the control group.That gives an odds ratio (OR) of 0.77 with a 95% confidenceinterval (CI) of 0.6–0.99 and a P-value of 0.034. When calcu-lated on a patient basis, 43% in the n-3 PUFA group had oneor more occluded vein grafts compared with 51% in the con-trol group. That gives an OR of 0.72 with a 95% CI of0.51–1.01 and a P-value of 0.05.
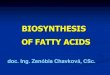
Interestingly, there was a significant trend to fewer patientswith vein graft occlusions with increasing relative change inserum-phospholipid n-3 fatty acids during the study period(P for linear trend = 0.0037) (Fig. 1). No effect on a muchlower occlusion rate (13.5%) was found for supplementationwith n-3 PUFA for the internal mammary artery grafts.
From this study one could conclude that dietary supple-mentation with 4 g/d of highly concentrated n-3 PUFA
reduced the incidence of vein graft occlusion after 1 yr andthat an inverse relation between relative change in serumphospholipid n-3 fatty acids and vein graft occlusions was ob-served.
Again, vein graft occlusion is a surrogate end point and thequestion arises about the clinical relevance of these data. TheSHOT study was not designed to evaluate the clinical effects.However, evaluation of the clinical results showed that post-operative angina pectoris was significantly more often relatedto one or more vein graft occlusions which were present in67.6% of patients with angina pectoris compared with 40.1%in patients with no postoperative angina (P < 0.0001) (6).
In larger prospective studies on CABG patients, there isalso a clear correlation between long-term patency of venousaortocoronary grafts and morbidity and mortality after aorto-coronary bypass grafting. Finally, it should be mentioned thatin the SHOT study no differences in the prevalence of shuntocclusions were observed in the two stratified subgroups ofantithrombotic treatment. Thus, it seems reasonable to advo-cate the supplementation of n-3 PUFA to patients after aorto-coronary bypass grafting. According to the limited literatureavailable, supplementation with 3–4 g/d n-3 PUFA concen-trates seems reasonable.
The third procedure of revascularization that I will discussis the potential effect of n-3 PUFA on the phenomenon ofrestenois after PTCA. This procedure was introduced by Gru-entzig in 1977; in most cardiological centers, more patientswith coronary heart disease are now being treated with PTCAthan with aortocoronary bypass surgery for myocardialrevascularization. Although the initial success rate withPTCA is high (~90%), restenosis occurs in up to 50% of thepatients after 3–6 mon and obviously represents a largemethodological problem and a therapeutic challenge today.The use of intracoronary stenting in parallel with PTCA hasreduced the tendency to clinically important restenosis to~50%. But restenosis remains an important threat to a lastingsuccessful PTCA.
The process of restenosis should be looked on as a re-sponse to intimal damage brought about by repeated balloonpressures of ~10 atm. The restenosis process is composed ofpassive elastic vascular recoil, thrombus formation, and
S104 H. ARNESEN
Lipids, Vol. 36, Supplement (2001)
Odds Ratio
1
0.8
0.6
0.4
0.2
0Q1 Q2 Q3 Q4
FIG. 1. Patients with vein graft occlusion in quartiles of the relativechange in polyunsaturated n-3 fatty acids; n = 524 patients with veinshunts. P for trend = 0.0037 (5).

mainly intimal smooth muscle cell proliferation, extracellularmatrix formation, and vessel remodeling. The process includesthe active participation of thrombogenic, mitogenic, and va-soactive factors, in which platelet aggregation, inflammation,and cell proliferation are major components. Special attentionhas been given to platelet-derived growth factor (PDGF) as animportant factor for smooth muscle cell chemotaxis. Becausen-3 PUFA are known to reduce platelet activation, downregu-late leucocytic inflammatory activity, and reduce synthesis ofPDGF, a solid rationale for a possible inhibitory effect on theprocess of restenosis is present.
From 1987 to 1992, seven clinical trials with n-3 PUFAwere undertaken to evaluate the possible effect on restenosisafter PTCA. The studies varied with respect to type anddosage of n-3 PUFA, time point of starting the supplementa-tion, and diagnostic preciseness toward restenosis. In 1992and 1993, two meta-analyses were published, the first byO’Connor and coworkers (7), the second by Gapinski andcoworkers (8). On the basis of these trials, they concludedthat there was a beneficial effect of n-3 PUFA on restenosis,with an OR of 0.71 (95% CI 0.54–0.94, P = 0.016) (7). In ad-dition, Gapinski and coworkers (8) pointed out a possibledose-response effect based mainly on the studies with angio-graphic end-point evaluation. Both studies recommendedlarger prospective randomized studies to further establish thepossible effect.
In the years from 1994 to 1999, three large, prospectiveplacebo-controlled trials of n-3 PUFA in patients undergoingPTCA were published, i.e., Leaf et al. in Circulation in 1994(9), Cairns et al. in Circulation in 1996 (10), and Johansen etal. in the Journal of the American College of Cardiology in1999 (11). The studies were of equal size with patient num-bers from 500 to 653; the dosage of n-3 PUFA was from 5.1to 8.0 g/d; and all studies used corn oil as placebo. The n-3PUFA supplementation was started from 7 to 14 d before thePTCA, and the presence of restenosis was evaluated by quan-titative coronary angiography after 18 wk to 6 mon. Therewere no significant differences between the n-3 PUFA groupand the placebo group with respect to restenosis.
In the study of Leaf and coworkers (9), 551 patients were ran-domized to receive 8.0 g/d of an ethyl ester formulation of n-3PUFA or corn oil as placebo, starting 12–14 d before electivePTCA. At coronary angiography after 6 mon, 46% of thepatients receiving corn oil met the criteria for restenosis (<50%final luminal diameter and >30% increase in narrowing at thestenosis site), compared with 52% in the n-3 PUFA group(P = 0.37). Thus, the restenosis rate was actually somewhathigher in the n-3 PUFA group, although this difference was notsignificant. In this study, two-thirds of the patients additionallyreceived 200 mg α-tocopherol as antioxidant. The incidence ofrestenosis and the difference between the groups did not differamong patients receiving α-tocopherol and those who did not.They concluded that the supplement of 8 g/d of n-3 fatty acidsfailed to prevent the usual high rate of restenosis after PTCA.
In the EMPAR study by Cairns and coworkers fromCanada (10), 653 patients were randomized to receive 5.4 g/d
of n-3 PUFA in a triglyceride formulation or corn oil asplacebo with a median start 6 d before elective PTCA andcontinued until angiography after 18 wk. Again, coronary an-giography revealed equal frequency of restenosis defined asloss of >50% of the gain of luminal diameter achieved byPTCA. Thus, in the n-3 PUFA group, 46.5% of the patientsfulfilled the criteria for restenosis compared with 44.7% inthe placebo group. In this study, low-molecular-weight hep-arin was also tried in a 2 × 2 factorial design. The simultane-ous testing of low-molecular-weight heparin did not influencethese results. They concluded that there was no evidence fora clinically important reduction of restenosis by n-3 PUFAafter PTCA in this trial.
Finally, in the CART study by Johansen and coworkers fromour research group (11), 500 patients were randomly allocatedto supplementation with 5.1 g/d of highly concentrated n-3PUFA in an ethyl ester formulation or corn oil as placebostarting at least 2 wk before elective PTCA. Restenosis onquantitative coronary angiography after 6 mon was defined as>50% luminal stenosis or a late loss of at least 20% of diame-ter or an increase in stenosis of at least 0.7 mm. In this study,restenosis occurred in 45.9% of the patients in the n-3 PUFAgroup compared with 44.8% in the placebo group. That givesan OR of 1.05, a 95% CI of 0.69–1.59, and a P-value of 0.82.On the basis of treated stenoses, the restenosis rate was 40.6%in the n-3 PUFA group compared with 35.4% in the placebogroup (OR 1.25, 95% CI 0.87–1.80, P = 0.21). In this study,we concluded that supplementation with 5.1 g/d n-3 PUFAfor 6 mon initiated at least 2 wk before coronary angioplastydid not reduce the incidence of restenosis.
Given the results of these three large prospective random-ized trials, the issue of n-3 PUFA supplementation to coun-teract restenosis after PTCA has come to a final result: It isnot effective and should not be advocated for such use. Itshould be added that these trials were conducted before stent-ing became common in connection with PTCA. Today, mostPTCA procedures are accompanied by stenting. The latterprocedure has reduced the frequency of restenosis to abouthalf that of PTCA alone, but the process of restenosis seemsto be the same whether stenting is performed or not.
Finally, I would like to comment on the possibility of nega-tive effects on patients with coronary artery disease with thesehigh doses of highly concentrated n-3 PUFA. Thus, in the CARTstudy, the clinical results, although not the primary aim of thestudy, seemed to be somewhat poorer in the n-3 PUFA groupthan in the placebo group. Thus, when angina pectoris was clas-sified in the New York Heart Association classes after 6 mon,significantly more patients were in class 3 and 4 in the n-3 PUFAgroup than in the placebo group (22 vs. 13%, P = 0.032). In linewith this observation, the use of betablockers and nitrates wasmore frequent in the n-3 PUFA group than in the placebo group(39 vs. 30% and 28 vs. 18%, respectively). Whether these ob-servations are relevant to the recently described increase in solu-ble markers of inflammation after supplementation with highdoses of highly concentrated n-3 PUFA (12) remains hypotheti-cal, but obviously the possibility exists.
ROLE OF PUFA IN REVASCULARIZATION S105
Lipids, Vol. 36, Supplement (2001)

In summary, on the basis of the literature the followingconclusions seem warranted: (i) supplementation with3.4–5.7 g/d n-3 PUFA concentrate counteracts hypertensionand normalizes coronary vasoreactivity to acetylcholine inheart transplantation patients; (ii) supplementation with 3.4g/d n-3 PUFA concentrate counteracts occlusion of venousaortocoronary grafts 1 yr after by-pass operation; and (iii)supplementation with up to 8.0 g/d n-3 PUFA concentratedoes not counteract restenosis 6 mon after PTCA.
REFERENCES
1. Bang, H.O., Dyerberg, J., and Nielsen, A.B. (1971) PlasmaLipid and Lipoprotein Pattern in Greenlandic Eskimos, Lanceti, 1143–1145.
2. Dyerberg, J., Bang, H.O., Stoffersen, E., Moncada, S., andVane, J.R. (1978) Eicosapentaenoic Acid and Prevention ofThrombosis and Atherosclerosis? Lancet ii, 117–119.
3. Fleischhauer, F.J., Yan, W.D., and Fishell, T.A (1993) Fish Oil Im-proves Endothelium-Dependent Coronary Vasodilation in HeartTransplant Recipients, J. Am. Coll. Cardiol. 21, 9982–9989.
4. Andreassen, A.K., Hartmann, A., Offstad, J., Geiran, O.,Kvernebo, K., and Simonsen, S. (1997) Hypertension Prophy-laxis with Omega n-3 Fatty Acids in Heart Transplant Recipi-ents, J. Am. Coll. Cardiol. 29, 1324–1331.
5. Eritsland, J., Arnesen, H., Grønseth, K., Fjeld, N.B., and Abdel-noor, M. (1996) Effect of Dietary Supplementation with n-3Fatty Acids on Coronary Artery Bypass Graft Patency, Am. J.Cardiol. 77, 31–36.
6. Eritsland, J., Arnesen, H., Fjeld, N.B., Grønseth, K., and Abdel-noor, M. (1995) Risk Factors for Graft Occlusion After Coronary
Artery Bypass Grafting, Scand. J. Thorac. Cardiovasc. Surg. 29,63–69.
7. O’Connor, G.T., Malenka, D.J., Olmstead, S.M., Johnson, P.S.,and Hennekens, C.H. (1992) A Meta-analysis of RandomizedTrials of Fish Oil in Prevention of Restenosis Following Coro-nary Angioplasty, Am. J. Prev. Med. 8, 186–192.
8. Gapinski, J.P., Van Ruiswyk, J.V., Heudebert, G.R., and Schect-man, G.S. (1993) Preventing Restenosis with Fish Oils Follow-ing Coronary Angioplasty. A Meta-analysis, Arch. Intern. Med.153, 1595–1601.
9. Leaf, A., Jørgensen, M.B., Jacobs, A.K., Cote, G., Schoenfeld,D.A., Scheer, J., Weiner, B.H., Slack, J.D., Kellett, M.A.,Raizner, A.E., Weber, P.C., Mahrer, P.R., and Rossouw, J.E.(1994) Do Fish Oils Prevent Restenosis After Coronary Angio-plasty? Circulation 90, 2248–2257.
10. Cairns, J.A., Gill, J., Morton, B., Roberts, R., Gent, M., Hirsh, J.,Holder, D., Finnie, K., Marquis, J.F., Naqvi, S., and Cohen, E.(1996) Fish Oil and Low-Molecular-Weight Heparin for the Re-duction of Restenosis After Percutaneous Transluminal CoronaryAngioplasty. The EMPAR Study, Circulation 94, 1553–1560.
11. Johansen, O., Brekke, M., Seljeflot, I., Abdelnoor, M., andArnesen, H. (1999) n-3 Fatty Acids Do Not Prevent RestenosisAfter Coronary Angioplasty: Results from the CART Study, J.Am. Coll. Cardiol. 33, 1619–1626.
12. Johansen, O., Seljeflot, I., Høstmark, A.T., and Arnesen, H.(1999) The Effect of Supplementation with Omega-3 FattyAcids on Soluble Markers of Endothelial Function in Patientswith Coronary Heart Disease, Arterioscler. Thromb. Vasc. Biol.19, 1681–1686.
[Received April 26, 2001; accepted November 17, 2001]
S106 H. ARNESEN
Lipids, Vol. 36, Supplement (2001)