Embed Size (px)
Citation preview
Na+ Disorders: Not so Elementary, Watson.
Polly A. Glover, DVM, DACVECC Animal Emergency Critical Care at The Life Centre
TLC Veterinary Forum October, 2015
Topics
Total Body Water
Osmolality & Osmotic Pressure
Regulation of Plasma Osmolality
Hypernatremia
Hyponatremia
Sodium Concentration [Na+] Disorders
Why do they matter?
Alterations in plasma [Na+] are associated with poor outcomes in critically ill humans & veterinary patients
Even changes within the normal range carry an increased mortality risk
Is increased risk a function of [Na+] changes being detrimental or are [Na+] changes a hallmark of more severe disease processes?
[Na+] Disorders
Most cases of Na+ disorders are problems with water handling in the body (osmoregulation) rather than increases or decreases in [Na+]
Total Body Water (TBW)
Body water = 60% of adult animal’s body weight
0.6 x lean BWkg = Liters of TBW
Intracellular Fluid (ICF) = 2/3 of TBW
Extracellular Fluid (ECF) = 1/3 of TBW -Interstitial space = 75% of ECF -Intravascular space = 25% of ECF
Osmolality & Osmotic Pressure
Osmolality & Osmotic Pressure
Osmole = 1 mole of any fully dissociated substance dissolved in H2O
NaCl = Na + Cl = 1 mole Na + 1 mole Cl = 2 moles total
Osmolality = Concentration of osmoles in a mass of a substance (mOsm/kg of H2O)
Osmolarity = Concentration of osmoles in a volume of solvent (mOsm/L of H2O)
In physiologic systems, no appreciable difference – use ‘osmolality’ for remainder of presentation
Osmolality & Osmotic Pressure
Every molecule dissolved in TBW contributes to osmolality
Molecular size, weight, charge and composition DO NOT matter
The NUMBER of dissolved molecules determine osmolality & therefore osmotic pressure
Most abundant molecules in ECF: -Na+ -Glucose -Urea
Osmolality & Osmotic Pressure
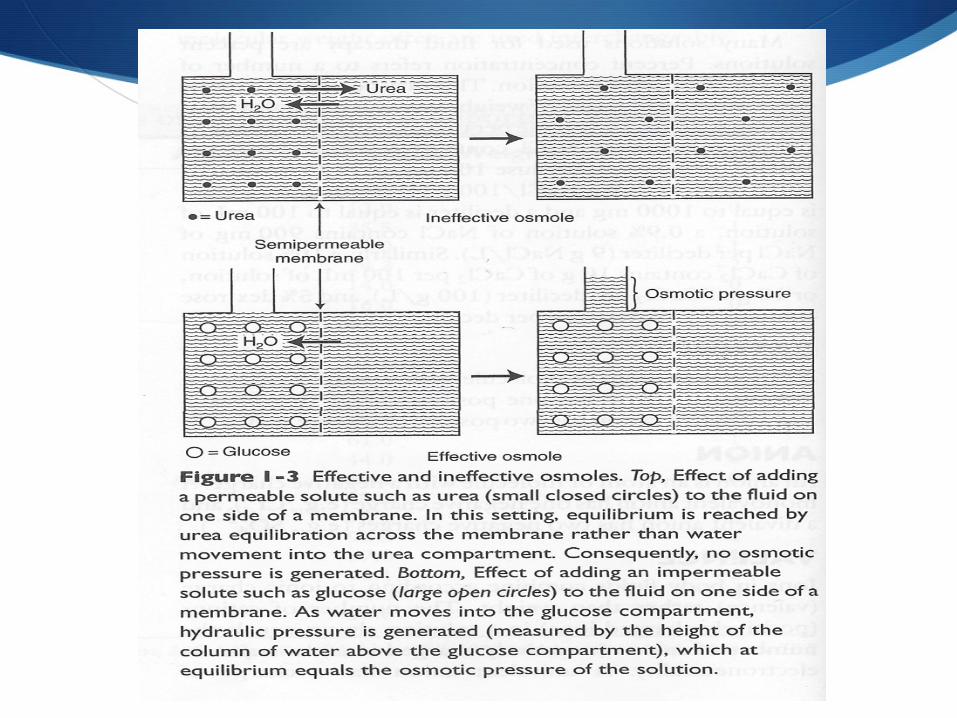
Effective osmoles: Do not freely cross semi-permeable cell membrane (Na+, K+); exert osmotic pressure across cell membrane
Ineffective osmoles: Freely cross semi-permeable cell membrane (glucose, urea); do not normally exert osmotic pressure across cell membrane
Osmotic pressure causes H2O to move from area of lower osmolality (higher [H2O]) to area of higher osmolality (lower [H2O]) down its concentration gradient
Occurs until osmolality in compartments equal
Osmolality & Osmotic Pressure
Na+, glucose, urea = main determinants of plasma osmolality in healthy dogs & cats
Plasma Osmolality
Dog: 290 – 310 mOsm/kg
Cat: 290 – 330 mOsm/kg
Measured plasma osmolality via freezing-point depression osmometry
Calculated plasma osmolality =
2 (Na+ + K+) + (BUN/2.8) + (Glucose/18)
*2.8 and 18 are conversion factors (mg/dL to mmol/L)
Regulation of Plasma Osmolality
Hypothalamic osmoreceptors sense changes in plasma osmolality
Osmolality changes of 2-3 mOsm/kg induce compensatory mechanisms to return plasma osmolality to hypothalamic set point
Two major physiologic mechanisms: 1. Antidiuretic hormone system (ADH) 2. Thirst
ADH/Vasopressin
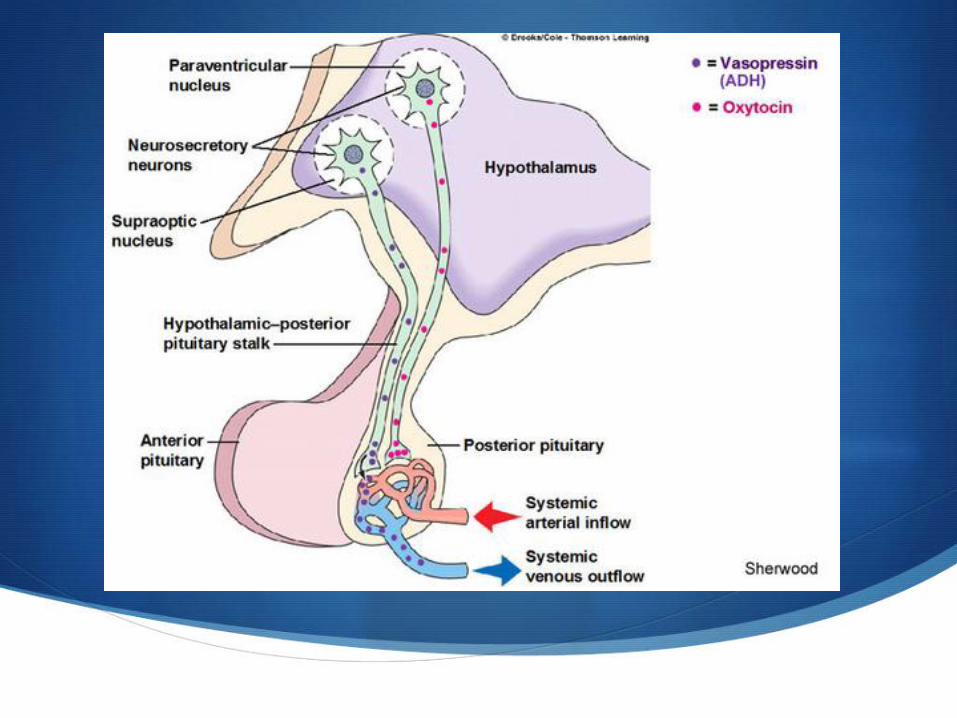
Small peptide secreted by posterior pituitary gland
Two major stimuli for release: 1. Elevated plasma osmolality 2. Decreased effective circulating volume (ECV)
ECV = Volume of arterial blood effectively perfusing tissue. Dynamic quantity – not a measureable, distinct compartment.
ADH/Vasopressin
Increased plasma osmolality hypothalamic osmoreceptor shrinkage neural impulses to posterior pituitary ADH release
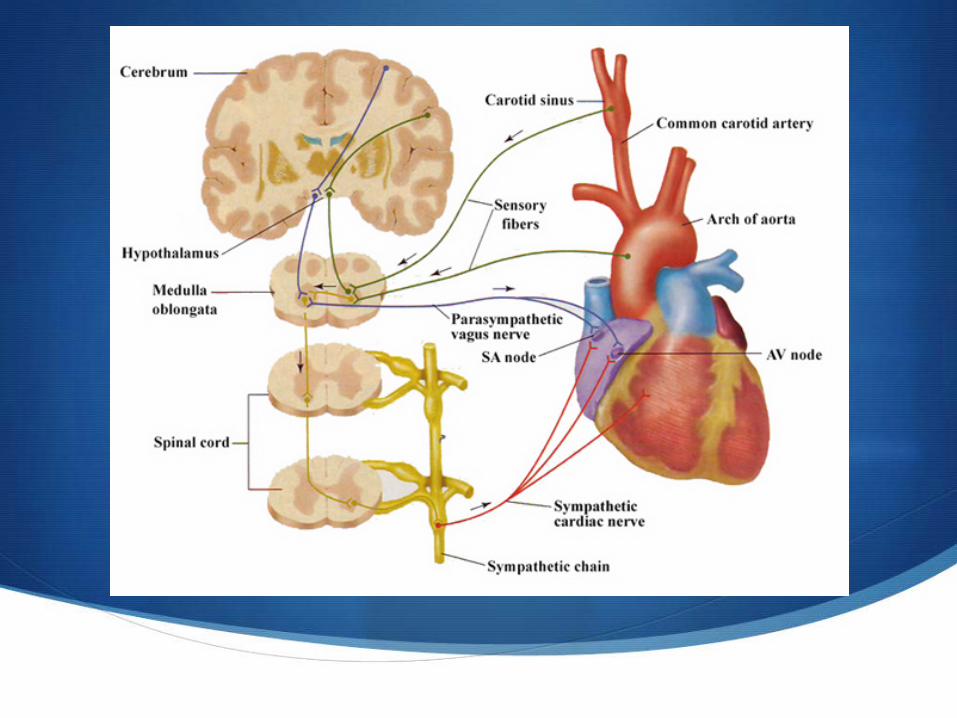
Low ECV Aortic arch & carotid bodies’ baroreceptor cells stimulated neural impulses to posterior pituitary ADH release
ADH/Vasopressin
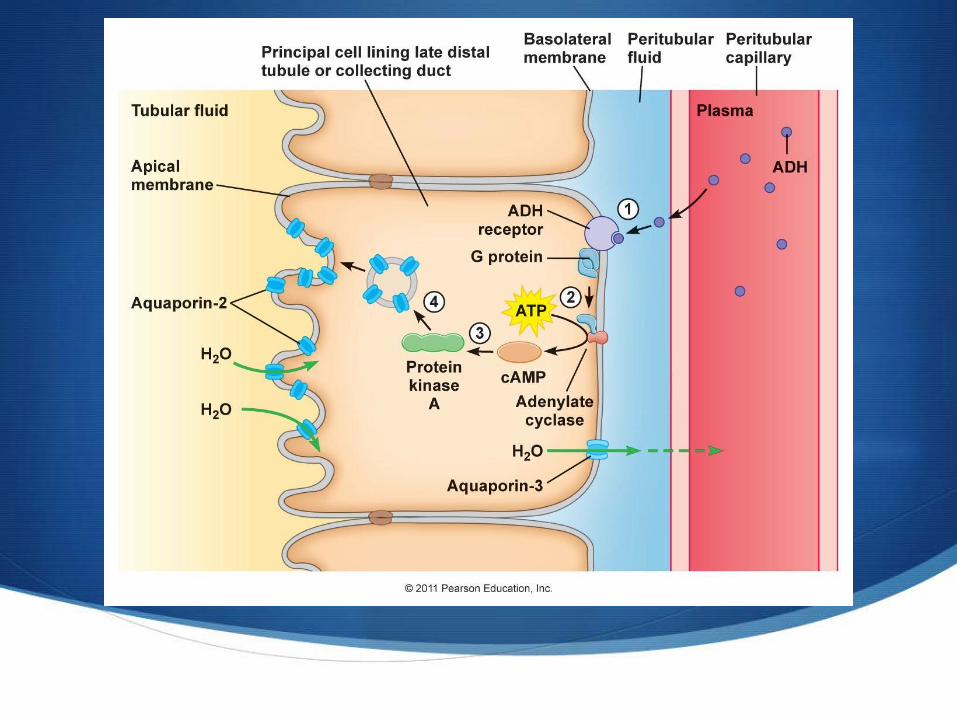
No ADH renal tubular collecting ducts relatively impermeable to H2O
ADH activates V2 receptors on collecting duct cells to insert AQP-2 molecules into membrane
AQP-2 molecules form water pores H2O moves into cells down osmotic gradient into hyperosmolar renal medulla
If no hyperosmolar renal medulla (renal ‘washout’) – ADH will not work!
ADH/Vasopressin
Circulating ADH & its effects on the normal kidney are the primary
physiologic determinants of free H2O retention & excretion.
Thirst
Hyperosmolality & decreased ECV stimulate thirst
Mechanisms similar to pathways for ADH secretion
Thirst + H2O consumption are main determinants of free H2O intake
Osmolality versus ECV
Normal physiologic conditions: -RAAS monitors & fine-tunes ECV -ADH system maintains plasma osmolality
Maintenance of ECV always prioritized over maintenance of normal plasma osmolality
Patients with poor ECV will have increased thirst & ADH release regardless of plasma osmolality
Hypernatremia
Plasma [Na+]
Normal plasma [Na+]:
-Dog: 145 - 150 mEq/L
-Cat: 155 - 160 mEq/L
*Moderate hypernatremia: [Na+] > 170
*Severe hypernatremia: [Na+] > 180 mEq/L
*Both species by convention
Hypernatremia (HyperNa+)
Most cases due to free or hypotonic H2O loss, not excessive Na+ intake or
retention
HyperNa+: Clinical Signs
In many cases, there are no specific signs.
All cells with Na+-K+/ATPase pumps shrink as H2O moves out of cell & down concentration gradient to interstitium
Neurons clinically least tolerant to changes in cell volume
If severe or rapid in onset: -Obtundation Coma -Head-pressing -Seizures -Death
HyperNa+: Adaptation
Slow development of hyperNa+ allows adaptation
Patient less symptomatic or asymptomatic
Brain has multiple ways to protect against & reverse neuronal H2O loss
HyperNa+: Early Adaptation
Within minutes to hours of hyperosmolar state:
Neuronal H2O lost to hyperNa+ circulation, neurons shrink
As plasma osmolality increases further, Na+ moves rapidly from CSF cerebral tissue
Minimizes brain volume loss – H2O follows Na+ into interstitium & neurons
Early fluid & ionic shifts protect brain from magnitude of volume loss expected for given plasma hyperosmolality
HyperNa+: Late Adaptation
Within 24 hours to 7 days:
Neurons accumulate organic solutes to increase ICF osmolality & shift H2O back into ICF
Idiogenic osmoles
-Inositol -Glutamine -Glutamate -Others
HyperNa+: Treatment
Hypernatremia should be treated, even if no clinical signs are present.
HyperNa+: Treatment
The most important questions:
1. What caused the hypernatremia?
2. How rapidly did the hypernatremia occur?
3. What are the neurologic, hydration, & IV volume statuses of my patient?
4. What IV crystalloid should I use?
5. What should the IV fluid rate (IVFR) be?
6. How often should I be monitoring plasma [Na+] & performing neurologic exams on my patient?
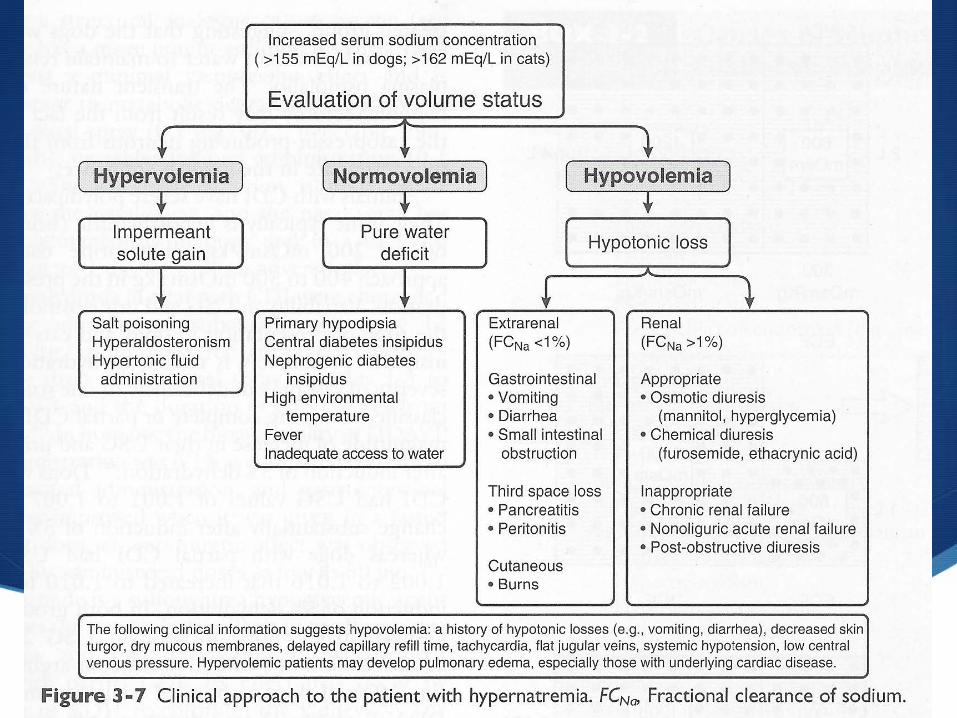
HyperNa+: Causes of Free Water Deficit
Denied H2O access for extended period
Prolonged panting – high environment/body temperature
Diabetes Insipidus
Hypodipsic hyperNa+ (Miniature Schnauzers)
HyperNa+: Causes of Hypotonic Fluid Deficit
GI loss: Vomiting, diarrhea
Third-space fluid loss
Renal disease: CKD, nonoliguric AKI
Postobstructive diuresis
Osmotic diuresis: Mannitol, diabetes mellitus
Activated charcoal + sorbitol
Low Na+ polyuria (diuretics)
HyperNa+: Causes of Na+ Excess
Hyperaldosteronism
Hyperadrenocorticism
Salt poisoning (rock salt, chemicals, seawater, brackish water, beef jerky, homemade play dough)
Sodium phosphate enemas
Hypertonic saline
NaHCO3 infusion
Parenteral nutrition
HyperNa+: Treatment
Must assess volume status of your patient! Hydration ≠ Perfusion
Hydration issues (dog & cat): Dry mucous membranes, loss of eye sheen, sunken eyes, skin tent, dandruff/dry coat, dry rectal mucosa, hard/firm feces
Early perfusion issues (dog): Tachycardia, normo- or hypertension, bounding/thready pulses, CRT < 1 second, typically normothermic
Early perfusion issues (cat): Bradycardia, normo- or hypotension, fair/weak pulses, CRT unreliable, normo- to hypothermic
HyperNa+: Treatment
In small animal medicine, most hyperNa+ patients will have hypotonic fluid losses resulting in some level of dehydration and/or intravascular volume depletion.
HyperNa+: Treatment
Must know onset of primary clinical signs!
-Profuse vomiting/diarrhea for 12 hours or 2-3 days?
-Outside in summer heat 1 hour ago or 24 hours ago?
-Large ingestion of beef jerky today or on NFL Sunday?
Rapidity of hyperNa+ onset will dictate how quickly you can normalize plasma [Na+] in your patient.
HyperNa+: Free H2O Loss Treatment
What crystalloid should I use? 5% dextrose in water (D5W)
Free H2O Deficit =
([current [Na+]p ÷ normal [Na+]p] – 1) x (0.6 x BWkg) current [Na+]p = patient’s current plasma [Na+]
normal [Na+]p = Patient’s normal plasma [Na+] BWkg = Patient’s body weight in kg
HyperNa+: Free Water Loss Treatment
Free water replacement alone will not correct clinical dehydration or hypovolemia
2/3 of volume administered will enter cells
Relatively safe to replace free water in hypernatremic patients – even those with renal & cardiac disease
HyperNa+: Free Water Loss Treatment
What IVFR should I use?
If hypernatremia acute in onset, can correct plasma [Na+] rapidly with D5W – no idiogenic osmole formation
With more prolonged or unknown onset, use guidelines:
Moderate hyperNa+ (> 170 mEq/L): Decrease plasma [Na+] no more than 1.0 mEq/L/hr
Severe hyperNa+ (> 180 mEq/L): Decrease plasma [Na+] no more than 0.5 – 1.0 mEq/L/hr
HyperNa+: Free Water Loss Treatment
If there are severe neurologic signs present, rapidly administer serial 10-20
mL/kg aliquots of D5W until clinical signs improve.
HyperNa+: Hypotonic Fluid Loss
What crystalloid & rate should I use?
Plasma [Na+] < 170 mEq/L typically can use balanced electrolyte replacement solution for rehydration & resuscitation purposes
Plasma [Na+] > 170 mEq/L resuscitate with IVF that has [Na+] that matches patient +/- 6 mEq/L
Plasma [Na+] > 170 mEq/L rehydrate with IVF that has [Na+] lower than patient but will not drop plasma [Na+] over 10 mEq/L in 24 hour period or 18 mEq/L over 48 hours
THIS IS VERY HARD TO DO!
HyperNa+: Hypotonic Fluid Loss
Adding Na+ to a balanced electrolyte solution or 0.9% NaCl:
23.4% hypertonic saline = 4 mEq NaCl/mL solution
7.2% hypertonic saline = 1.2 mEq NaCl/mL solution
3% hypertonic saline = 0.5 mEq NaCl/mL solution
Add calculated volume to the fluid bag
Remember to factor in the Na+ already in the fluid bag!
HyperNa+: Hypotonic Fluid Loss
What crystalloid & rate should I use?
Resuscitation must happen fast! Up to 90 mL/kg IVF in 10-20 mL/kg aliquots
If [Na+] not immediately known – do not delay therapy waiting for results, treat with balanced electrolyte solution
Rehydration should always occur over a time frame that closely mirrors the onset of dehydration (hours or days?)
Rehydration volume (L) = (% dehydration x BWkg) + 60 mL/kg/d
HyperNa+: Iatrogenic IVF
What to do when plasma [Na+] starts to steadily climb while on replacement IVF therapy for rehydration?
Change to maintenance solution or 0.45% NaCl + 2.5% dextrose +/- KCl if patient well hydrated
‘Piggy-back’ 0.45% NaCl + 2.5% dextrose with balanced electrolyte solution if patient still dehydrated
If cardiac or renal patient, recommend changing to 0.45% + 2.5% dextrose IVF earlier to prevent volume overload
HyperNa+: Therapeutic Considerations
Consider nasoesophageal or nasogastric tube placement for enteral H2O administration in patients not vomiting
Consider furosemide for natriuresis in neurologic crises
Desmopressin therapy for diabetes insipidus
Monitor blood pressure closely & treat PRN – hypertension typically improves and/or resolves with plasma [Na+] reduction
HyperNa+: Therapeutic Complications
Primary complication = Cerebral edema
Clinical Signs: Obtundation, head pressing, coma, seizures, other disorders of behavior/movement
Remember to check plasma [Na+] – clinical signs may be related to treatment or worsening hypernatremia!
Mannitol 0.5 – 1.0 g/kg IV over 20-30 minutes
Hypertonic saline (7.2%) 3-5 mL/kg IV over 20 minutes -If no mannitol -If mannitol ineffective
HyperNa+: Monitoring
Monitor vital parameters & neurologic status every 2-4 hours or more frequently if necessary
Monitor plasma [Na+] initially every 4 hours, or immediately after any large volume IVF bolus
Majority of patients require several days in 24 hour referral hospital – exception are some free water loss patients
Further diagnostics need to be performed to determine underlying disease process
Be sure real-time plasma Na+ levels available to guide therapy
Hyponatremia
Plasma [Na+]
Normal [Na+]:
-Dog: 145 - 150 mEq/L
-Cat: 155 - 160 mEq/L
Moderate hyponatremia: [Na+] < 130 mEq/L
*Severe hyponatremia: [Na+] < 120 mEq/L
*Both species by convention
Hyponatremia (HypoNa+)
Clinically detrimental hypoNa+ uncommon in critically ill dogs & cats
Almost always free H2O retention in excess of Na+
retention
May have Na+ loss
Generation typically requires H2O intake + decreased H2O excretion
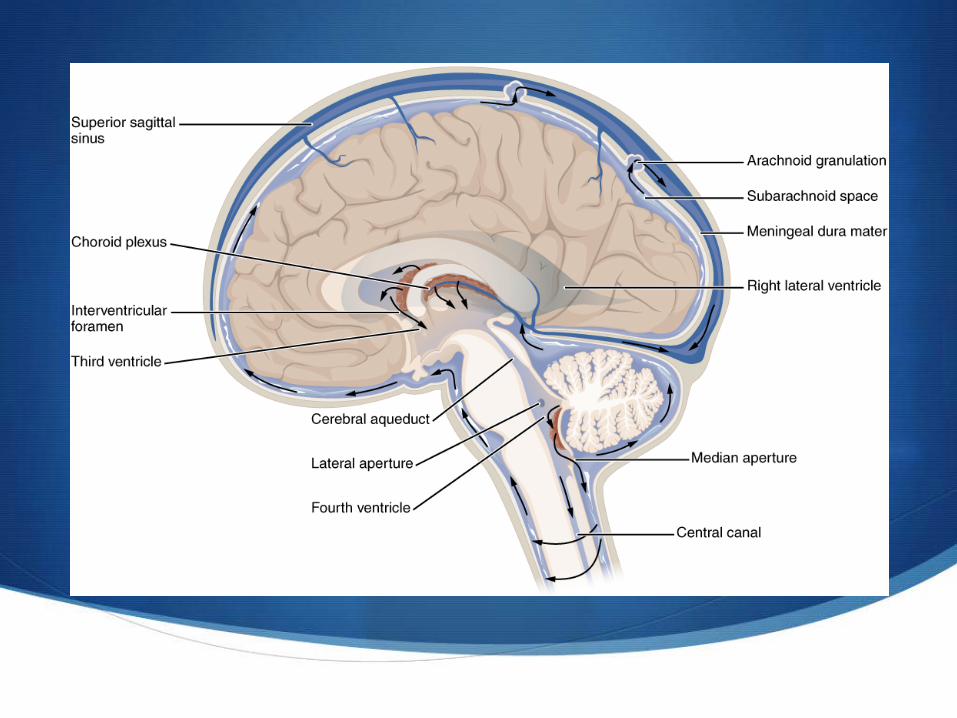
HypoNa+: Adaptation
ICF/interstitial edema in CNS increase in intracranial hydrostatic pressure
enhances fluid movement into CSF CSF flows out of cranium
subarachnoid space central spinal canal venous circulation
HypoNa+: Adaptation
Swollen neurons expel solutes: Na+, K+, organic osmolytes
Decreases intracellular osmolality & encourages H2O loss into ECF
Ion expulsion occurs rapidly
Loss of organic osmolytes requires hours to days
HypoNa+: Treatment
The most important questions are the same as with hyperNa+:
1. What caused the hyponatremia?
2. How rapidly did the hyponatremia occur?
3. What are the neurologic, hydration, & volume statuses of my patient?
4. What IV crystalloid should I use?
5. What should the IV fluid rate (IVFR) be?
6. How often should I be monitoring plasma [Na+] & performing neurologic exams in my patient?
HypoNa+: Causes
Decreased ECV
Hypoadrenocorticism
Diuretics
GI parasitism
Syndrome of Inappropriate ADH secretion (SIADH)
Infectious/inflammatory disease
Psychogenic polydipsia
Pregnancy
Cerebral salt-wasting syndrome (CSW, humans)
Artifact: Lipemic, hyperproteinemic samples
HypoNa+: Pseudohyponatremia
Diabetes mellitus
Diabetic ketoacidosis – Balanced electrolyte solution or 0.9% NaCl
Hyperglycemic hyperosmolar syndrome – recommend 0.9% NaCl therapy
Mannitol administration
HypoNa+: Clinical Signs
Mild to moderate [Na+] change usually no specific signs
If severe (Na+ < 120 mEq/L) or rapid occurrence – CNS signs same as with hyperNa+
All cells with Na+/K+-ATPase pumps swell as H2O moves into relatively hyperosmolar cell from hypoosmolar ECF
Neurons least tolerant of over hydration
HypoNa+: Asymptomatic Treatment
HypoNa+ due to decreased ECV most often mild (Na+ > 130) & self-corrects with treatment of underlying disease
Avoid IVF with [Na+] less than that of patient
HypoNa+: Symptomatic Treatment
If a patient is symptomatic, whether acute or chronic, it requires emergency
therapy;
however….
the best management style is controversial.
HypoNa+: Symptomatic Treatment
Goal = Raise plasma [Na+] enough to resolve clinical signs without causing
complications
HypoNa+: Symptomatic Treatment #1
1. Mannitol (0.5 g/kg IV) or furosemide (0.5 mg/kg IV) for electrolyte-free H2O loss
2. Replace fluid loss with a replacement crystalloid unless patient is overhydrated
3. Raise plasma [Na+] < 10 mEq/L over 1st 24 hours
4. Rate per day more important than rate per hour
5. Raise plasma [Na] < 18 mEq/L over 48 hr
HypoNa+: Symptomatic Treatment #2
Calculate Na+ deficit: (target [Na+]p – patient [Na+]p) x (0.6 x lean BWkg)
Target [Na+]p = desired patient plasma [Na+]
Target [Na+] = no more then 10-15% higher than current plasma [Na+] in 1st 24 hours
Calculated deficit determines amount of 3% hypertonic Na+ (0.5 mEq/mL) to be infused
HypoNa+: Symptomatic Treatment #2
Human medicine strategy:
1. Raise [Na+] by 10-15% in first 24 hours
2. Rate of correction as great as 15 mEq/L in 1st 24 hours
3. Not more than 2 mEq/L/hr increase in plasma [Na+] for first few hours
HypoNa+: Fluid Resuscitation
Plasma [Na+] < 130 mEq/L resuscitate with IVF with [Na+] that matches patient +/- 6 mEq/L
Balanced electrolyte solution with 130 mEq/L Na+ = lactated Ringer’s solution (LRS)
Add Na+ to maintenance solution to make [Na+] = patient’s plasma [Na+]
HypoNa+: Therapeutic Complications
Major complication = Thalamic myelinosis (dogs)
Neuronal shrinking away from myelin sheath as H2O moves out of neuron during correction of hypoNa+
Clinical signs occur many days after intervention
Overzealous correction paresis, ataxia, dysphagia, obtundation, other neurologic signs
Typically when [Na+] < 110 mEq/L & recommended replacement rates exceeded
HypoNa+: Therapeutic Complications
What to do if clinical signs develop during therapy:
Discontinue any hyperosmolar fluids
Immediately check plasma [Na+]
Treat with addition of free water (D5W)
Decreasing plasma [Na+] in already hypoNa+ patients can be difficult without concurrent loop diuretic
Preparedness Pearls
Collect blood samples prior to administering IVF every time if possible
Run electrolytes promptly – particularly if neurologic patient
Take stock of your crystalloids – recommend having replacement & maintenance solutions available +/- D5W
Keep hypertonic saline on the shelf (7.0 - 23.4%)
Prepare clients for potential neurologic complications – particularly if hyponatremic
Remember: Slow & steady wins the race!
Questions?