Embed Size (px)
Citation preview
Nadin Abdel Razeq, PhD
ObjectivesTo gain awareness of the proper procedure of
peripheral IV access in pediatrics To review types of IV fluids used in children To review basics of maintenance and deficit
fluid and electrolyte requirementsTo gain awareness of the proper procedure of
IV-formula preparation and administration in pediatrics
To review basics of IV medications administration in children!
Proper Procedure of Peripheral IV Access in Children
Let us watch a Video First … Then Let us Focus on Some
Important ConceptsAll procedures at a treatment room Scalp Site and Arterial insertion To Get Better IV access you can…Number of IV access Attempts…
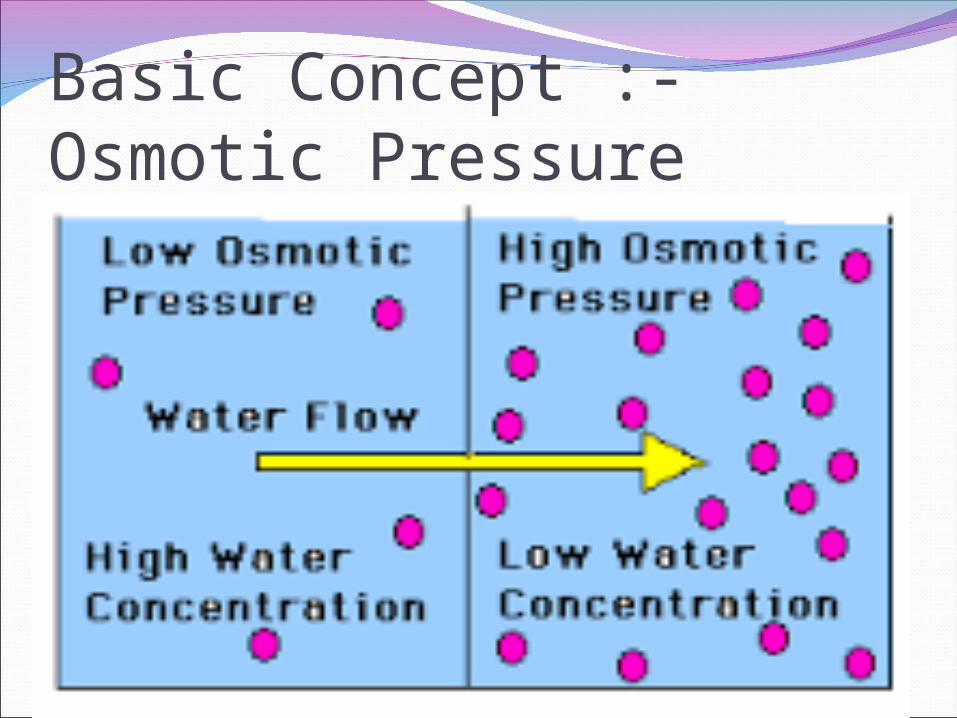
Basic Concept :-Osmotic Pressure
Basic Concept :-Osmolality of the blood Isotonicity of Blood = 275-295 mOsm/LSolutions having the same osmotic
pressure as that of blood are said to be isotonic with blood.
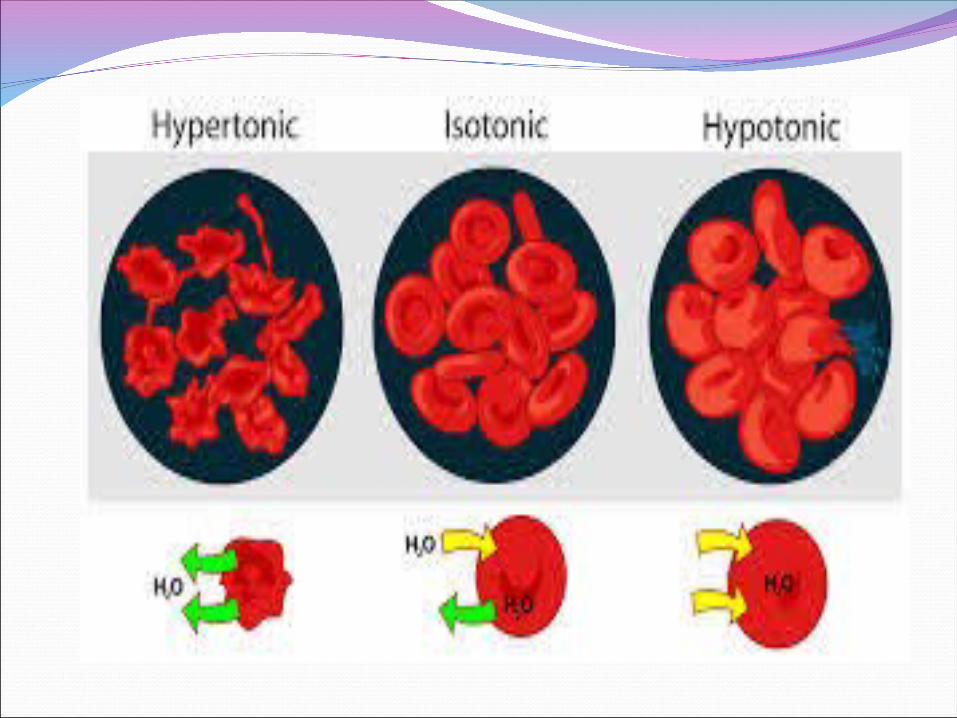
Solutions with a higher osmotic pressure than body fluids are called hypertonic
Solutions with a lower osmotic pressure are called hypotonic.
Types of IV fluids in children5% glucose in
water 0.9% NaCl
(Normal Saline)
Types of IV fluids in children25% or 50%
glucose in water Never as an infusion
Only used in NICU and at low vol eg. 1-2mls/hr via central line
10% glucose in water
--------------------------15% or 20% glucose
in water Give only via a
central line as a 1-2ml/kg bolus for hypoglycaemia. Monitor blood glucose
Types of IV fluids in children0.9% NaCl with 5% dextrose (Normal
saline with glucose)
Osmolarity: 560
Types of IV fluids in children0.18% NaCl and 4%
dextrose (4% and 1/5th normal saline)
0.45% NaCl with 5% dextrose
(1/2 Normal saline with glucose and no potassium
Types of IV fluids in childrenRinger Lactate :0-10 gram glucose/100cc
Na 130 mEq/LNaHCO3 28 mEq/L as
lactate K 4 mEq/L273 mOsm/L
Water for injection
Maintenance Electrolyte RequirementsMaintenance K
Requirements: IV: 1-2 mEq/100ml of water/day
OR 1-2mEq/kg/dayIndications : Administration: Added only once the
urine output is established.
Strength:Calculate :
• Side effect: ECG monitoring Frequent testing
•\
Maintenance Electrolyte RequirementsMaintenance Ca
Requirements: IV: 60 to 100 mg/kg/day
Indications : Administration: Strength:
Calculate : Side effect:

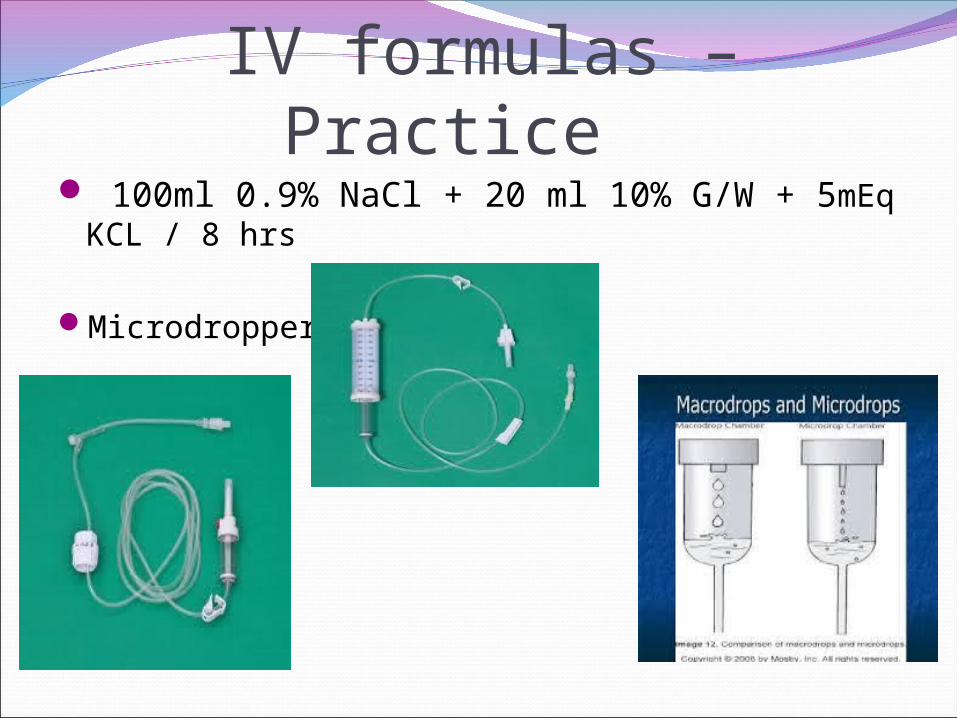
IV formulas – Practice 100ml 0.9% NaCl + 20 ml 10% G/W + 5mEq
KCL / 8 hrs
Microdropper
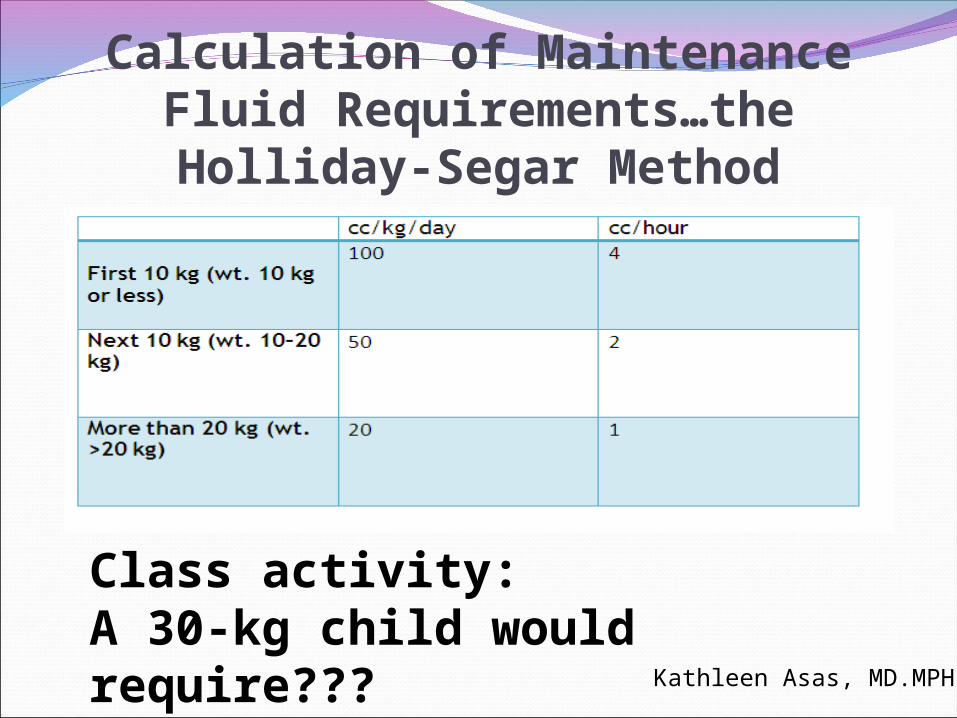
Calculation of Maintenance Fluid Requirements…the Holliday-Segar Method
Class activity: A 30-kg child would require??? Kathleen Asas, MD.MPH
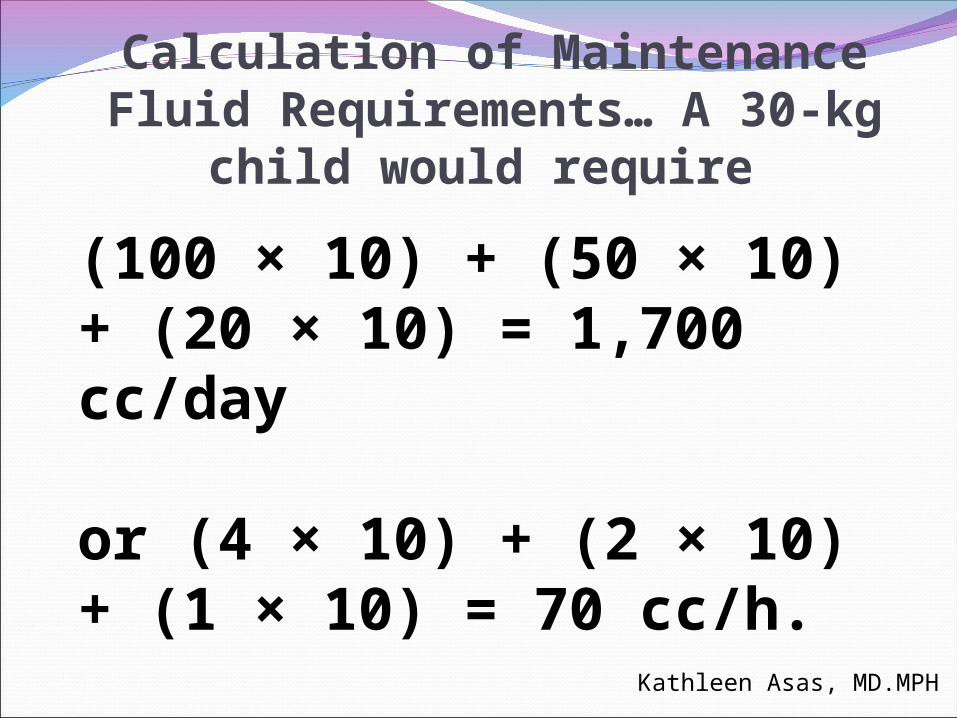
Calculation of Maintenance Fluid Requirements… A 30-kg child would
require
(100 × 10) + (50 × 10) + (20 × 10) = 1,700 cc/day
or (4 × 10) + (2 × 10) + (1 × 10) = 70 cc/h.
Kathleen Asas, MD.MPH
Oral Rehydration: Key ConceptsMild to moderate dehydration may be
managed successfully with oral rehydration in the majority of cases.
Oral rehydration solutions should contain glucose and sodium in a ratio not to exceed 2:1
Amount of rehydration solution to be given is based on the estimated percentage of dehydration by weight.
Kathleen Asas, MD.MPH
Oral RehydrationPatient vomiting
– 5-10mL Q 5-10 minutes and increase as tolerated
Mild Dehydration– Deficit replacement: 50 mL/kg over 4 hours
Moderate Dehydration– Deficit replacement: 100 mL/kg over 4 hours
Kathleen Asas, MD.MPH
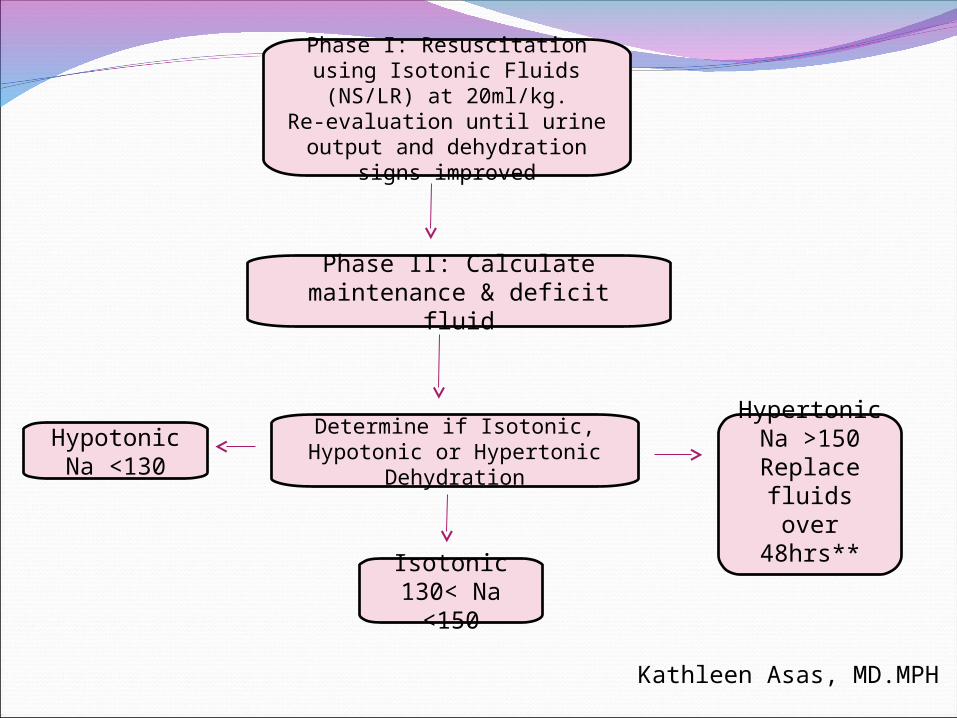
Phase I: Resuscitation using Isotonic Fluids (NS/LR) at
20ml/kg.Re-evaluation until urine
output and dehydration signs improved
Phase II: Calculate maintenance & deficit fluid
Determine if Isotonic, Hypotonic or Hypertonic
Dehydration
HypotonicNa <130
Isotonic130< Na
<150
HypertonicNa >150Replace
fluids over 48hrs**
Kathleen Asas, MD.MPH
Resuscitation phaseGoal: Restore circulation, re-perfuse brain,
kidneysMild-Moderate
20 mL/kg bolus given over 30 – 60 minutesSevere
May repeat bolus as needed (ideally up to 60ml/kg)
Fluids – something isotonic such as NS or lactated ringers (LR)
Kathleen Asas, MD.MPH
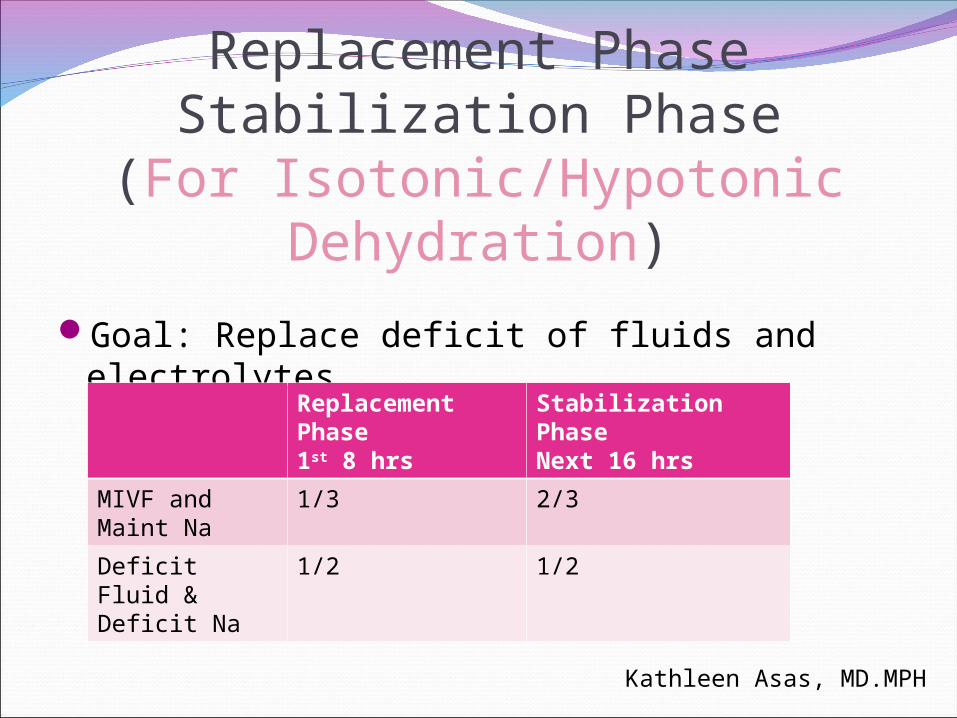
Replacement PhaseStabilization Phase
(For Isotonic/Hypotonic Dehydration)Goal: Replace deficit of fluids and electrolytes
Replacement Phase1st 8 hrs
Stabilization PhaseNext 16 hrs
MIVF and Maint Na
1/3 2/3
Deficit Fluid & Deficit Na
1/2 1/2
Kathleen Asas, MD.MPH
IV Medications
IV Medications - basic Concepts Correct :
Patient Drug Dose Rout,
IV or Oral ----- check IV site , Time, Time of Other Medications Documentation
IV Medications - basic Concepts Administration :
Micro-dropper for each MedMinimum dilution of drugs What to Do with the extra fluids Type of solution and computability
Meds Never with blood product Duration of administration – Time of Other Medication