Embed Size (px)
Citation preview
MINISTERIO DE SALUD
National Alcohol Strategy: Reduction of High-Risk Alcohol Consumption
and its Social and Health Consequences A Bicentennial Challenge Proposal for Chile
Interministerial Committee
Working Document. Interministerial Committee. Ministry of Health Publication
2 National Alcohol Strategy - Chile
Contents I. EXECUTIVE SUMMARY* ................................................................................ 9 II. INTRODUCTION ....................................................................................... 14 III. WHY DOES CHILE NEED A NATIONAL ALCOHOL STRATEGY? .................. 19
a. Because the loss of lives and quality of life associated with alcohol injures the country. ............................................................................................................................................…19 b. Because there is a concern and desire to achieve higher levels of public safety. . 32 c. Because it seeks equitable development and social protection ................................... 34 d. Because its social and economic development is threatened by the costs of harmful use of alcohol. ................................................................................................................... 35
IV.- WHAT MAKES IT POSSIBLE FOR A NATIONAL STRATEGY ON ALCOHOL TO BE EFFECTIVE? ............................................................................................. 38
a. The regulatory system for alcohol control and its practical application, although still weak, is well-oriented and also perfectible. .................................................................... 38 b. Accumulated evidence that measure the differential effectiveness of various public policies on alcohol. ........................................................................................................................... 41 c. The lessons garnered from international experiences. ................................................... 43 d. The WHO initiative and activities of its regional offices ................................................. 45
V. – DEFINITIONS, RIGHTS, DETERMINANTS, AND MODELS OF INTERVENTION ..................................................................................................................... 46
a. Basic Definitions .......................................................................................................................... 46 b. Rights .............................................................................................................................................. 46 c. Social determinants of health and the National Strategy on Alcohol ......................... 47 d. Intervention Model...................................................................................................................... 49
VI. LINES OF ACTION AND PROPOSAL FOR CONCRETE MEASURES ............... 52
LINE OF ACTION № 1. PUBLIC INFORMATION AND ADVERTISING CONTROL. ........... 52 LINE OF ACTION №2: ALCOHOL AVAILABILITY ..................................................................... 53 LINE OF ACTION № 3: ALCOHOL TAXES AND RETAIL SALE PRICES .............................. 55 VI. LINE OF ACTION № 4: ALCOHOL DISPENSING AND RETAIL SALE POLICIES ...... 57 LINE OF ACTION № 5: TRAFFIC, ACCIDENTS AND HARMFUL ALCOHOL CONSUMPTION .................................................................................................................................. 58 LINE OF ACTION № 6: HAZARDOUS ALCOHOL CONSUMPTION AND HEALTH CARE. 63 LINE OF ACTION № 7: COMMUNITY ACTION AND LOCAL GOVERNMENTS (MUNICIPALITIES) ........................................................................................................................... 64 LINE OF ACTION N° 8: EDUCATION, PERSONNEL AND JOB TRAINING ......................... 65 LINE OF ACTION № 9. MONITORING AND EVALUATION .................................................... 68
VII: ORGANIC STRUCTURE AND DEVELOPMENT ROUTE FOR THE NATIONAL ALCOHOL STRATEGY ..................................................................................... 71 VIII. IMMEDIATE STEPS AND CONCLUSIONS ............................................... 73 IX. - REFERENCES ......................................................................................... 76
3 National Alcohol Strategy - Chile
PREFACE
At the dawn of the country’s 200th Anniversary, we offer to the consideration of our citizens the National Alcohol Strategy to reduce harmful consumption and its detrimental health and social consequences, a necessary step towards further development as a nation.
Its purpose should not be underestimated: to change the way Chileans relate to
alcohol in such a manner as to maintain the advantages and benefits of the economic activity it sustains, while dramatically reducing the negative consequences which derive from the growing pattern of hazardous drinking, i.e. premature deaths, impairment of life quality for millions of people and families, the rising issues of public safety, and other harmful effects on our economic and social development as a nation, that in many cases go unnoticed. Given its size, complexity and potential, such a purpose sets a great Bicentennial Challenge for Chile.
Currently, the National Alcohol Strategy represents both a response to the constructive and reflexive debate engaged by all realms of society, as well as a roadmap for a powerful and concerted State policy which is inclusive of all sectors and is sustained by the scientific evaluation of experiences developed in several nations.
The document, carefully developed by the technical bodies (professional advisors) from several ministries besides Health, reveals a range of alternatives that go beyond what have up to now been well-intentioned but isolated or poorly applied laws and policies, and even more, scarcely effective in reducing the negative effects of harmful alcohol consumption.
The National Strategy posits nine lines of action that apply to a wide variety of
aspects such as pricing policies; retail sales practices; alcohol marketing; information for the public; education; effective action regarding traffic accidents associated with alcohol consumption; early and adequate detection and treatment of those affected by hazardous use. It also considers civil participation and the roles that local, municipal and regional authorities may play in the National Alcohol Strategy
Only by implementing a strategy that contemplates the various factors at play and influences the culture, habits and practices of the population as a whole, will it be possible to succeed in the specific actions aimed at high risk groups that engage in harmful drinking and the groups exposed to the effects of harmful drinking by others. It is this conviction which underlies the World Health Organization initiative to develop similar strategies in each nation.
The health sector has made significant progress in this area over recent years and has increased its welfare resources, perfecting its practices and facilitating access to the affected population. At the same time, it leaves work in progress for the immediate future. Indeed, in 2010, the government will initiate the progressive implementation of brief interventions for alcohol problems through Primary Health Care Network, one of the proposals of the National Strategy that specifically falls under its mandate as a sector. Also, it has included among the regional health plans, the dissemination and citizen debate of key ideas of the National Alcohol Strategy, in order to provide support to each regional government to be able to launch those feasible measures within their own mandate, which may attract political and civic agreement and commitment.

4 National Alcohol Strategy - Chile
The National Alcohol Strategy emerges during the final phase of a State administration that will be remembered, among other things, for its decided efforts towards the protection of the more needed people and for having identified and confronted social vulnerabilities and inequities. Within the same framework, it passes on to the incoming authorities a useful tool for opening a new dimension for the protection of society and in this manner carry on with the work at hand. Dr. Álvaro Erazo Latorre Ministro de Salud (Minister of Health) Santiago de Chile, January, 2010
5 National Alcohol Strategy - Chile
PREFACE
The Health administration that starts in March 2010 has set itself the task of focusing on those health conditions that if left untreated become high risk factors for the population. The country has advanced in its objective of reaching acceptable standards in caring of the sick, but it does not show a similar progress regarding the control of the primary health risk factors, which as evidenced by obesity, excessive alcohol consumption, sodium rich diets, sedentary lifestyles, all help to condition the increase in burden of disease and preventable deaths. The harsh effects of the February 27th earthquake and tsunami this year demand greater urgency and effort towards achieving these objectives.
The reconstruction of hospitals and damaged services, the normalization of health care programs, the recovery of basic conditions for the effective and satisfactory performance of health care workers, are all essential goals for the country to be able to protect and recover the health of those Chileans that become ill.
At the same time, however, it is necessary to improve health levels within the general population. This, besides demanding new and major enhancements to the healthcare system, makes it essential to convene with other sectors and with the society in general, objectives that influence lifestyles of many people, in the economic activity and in cultural practices. Actually, these are the variables and factors at stake that protect health or make it more vulnerable, and that derive, sooner or later, in a good or bad quality of life of individuals, families, and the whole society. It is the case of quality of foods, physical activity levels, recreation, workplace security, routes, streets, homes and various others.
A particular example is the case of high-risk consumption of alcoholic beverages. Doubtlessly, Chile is facing a major challenge in this area. The studies of burden of disease rank alcohol consumption as the risk factor that most negatively influences life expectancy and overall quality of life of Chileans. Other solid studies inform us about strategies and alcohol policy measures that have proven to be highly effective in reducing the negative social and health effects of harmful alcohol use.
The World Health Organization is requiring that Member States take more active and effective measures to reduce harmful alcohol consumption and is preparing to make decisions that will bring the international community to share and collaborate in this goal.
The preparatory work of the past years regarding a national policy directed at reducing harmful alcohol consumption in Chile is going in the right direction, and this administration takes the task of continuing on itself.
The present work document will let citizens, social actors, and all decision makers become aware of the current state of available information, open up a space for advising and debate and so that progressively, the country reaches a sufficient level of agreement for carrying out, among all, the necessary measures to achieve a healthier and more harmonious relationship between Chileans and alcohol.
Dr. Jaime Mañalich Muxi Department of Health (Health Ministry)
6 National Alcohol Strategy - Chile
PARTICIPANTS IN THE ELABORATION OF THIS REPORT A. Parties responsible for the document Alfredo Pemjean Gallardo Médico Psiquiatra Asesor en Salud Mental Departamento de Salud Mental, Ministerio de Salud, Chile Profesor de Psiquiatría y Salud Mental Facultad de Medicina, Universidad Diego Portales Alberto Minoletti Scaramelli Médico Psiquiatra Jefe Departamento de Salud Mental División de Prevención y Control de Enfermedades Subsecretaría de Salud Pública Ministerio de Salud, Chile B. Final drafting team (Secretaría Técnica de la Estrategia) Fernando Poblete Arrué Médico de Familia, MPH, Departamento de Medicina Familiar Escuela de Medicina, P. Universidad Católica de Chile Marcelo Villalón Calderón Médico Especialista, MSP Escuela de Salud Pública, Universidad de Chile Jorge Ramírez Flores Médico-Cirujano, Escuela de Salud Pública, Universidad de Chile Ximena Barros Rubio Trabajadora Social, P. Universidad Católica de Chile Eduardo Bronstein Alonso Médico-Cirujano, Universidad Católica de Chile Paula Fernández Elgueta Psicóloga, Ministerio de Salud Chile Irina Toro Salgado Periodista, Ministerio de Salud, Chile A. Document content consulting and editing team Norman Giesbrecht
Senior Scientist Centro de Adicciones y Salud Mental, CAMH Toronto, Canadá Judith Márquez Contró Centro de Adicciones y Salud Mental, CAMH Toronto, Canadá Jaime Sapag Centro de Adicciones y Salud Mental, CAMH Toronto, Canadá. D. Collaborative consultants for base document Akwatu Khenti Oficina de Salud Internacional, Centro de Adicciones y Salud Mental,CAMH Jurgen Rehm Departamento de Investigación de Política de Salud. Centro de Adicciones y Salud Mental, CAMH Luis Gliksman Departamento de Investigación de Política de Salud Centro de Adicciones y Salud Mental, CAMH Maristela Monteiro Organización Panamericana de la Salud, OPS Marg Rylett Departamento de Investigación de Política de Salud Centro de Adicciones y Salud Mental, CAMH Svetlana Popova Departamento de Investigación de Política de Salud Centro de Adicciones y Salud Mental, CAMH Yedy Israel Jacard Academia de Ciencias de Chile E. English Document Translation Renato Cerro MSW, University of Washington (Trabajador Social); English Teacher, Instituto Chileno Norteamericano
7 National Alcohol Strategy - Chile
Rodrigo Suárez P. Magíster Literatura Spanish / English Teacher, Instituto Chileno Norteamericano F. Interministerial Committee for the elaboration of the National Alcohol Strategy Mónica Abual O. Ministerio Secretaría General de la Presidencia Enrique Azúa Ministerio de Educación Silvio Banfi Piazza Ministerio de Agricultura Bárbara Barrios Aguirre Ministerio de Agricultura Antonio Bayas F. Ministerio de Relaciones Exteriores Patricio Cañete Lizama Ministerio de Defensa Nacional María Clarisa Céspedes Goycochea Ministerio de Obras Públicas María Soledad Coca Herrera Consejo Nacional para el Control de Estupefacientes Pedro Antonio Díaz González Ministerio de Justicia René Donoso Sereño Consejo Nacional para el Control de Estupefacientes Dionisio Faulbaum Mayorga Ministerio de Agricultura Loreto Flores P. Ministerio de Trabajo y Previsión Social Carola González Gallinato Instituto Nacional de la Juventud Ximena Guzmán Ministerio de Justicia Adrian G. Jobt Sotomayor Ministerio de Defensa Nacional Marcela Lobo Barrientos
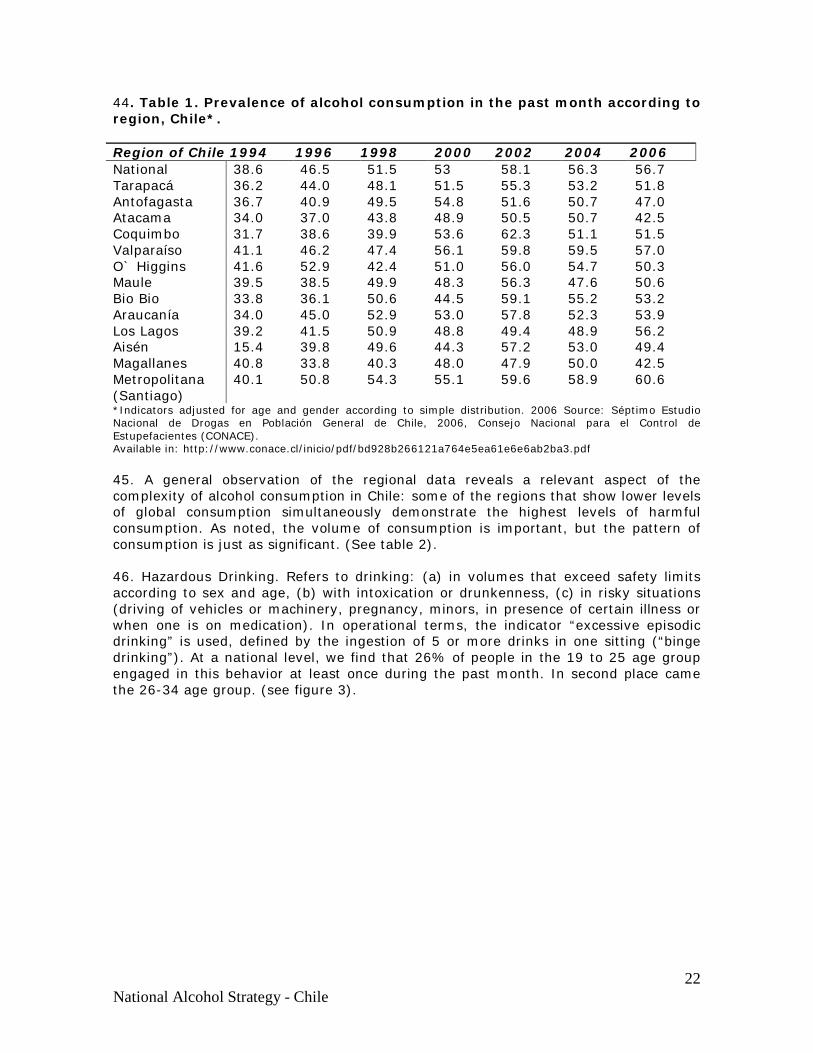
Comisión Nacional de Seguridad de Tránsito Karina López Monsalve Secretaría General de Gobierno Danica Mimica Porras Comisión Nacional de Seguridad de Tránsito Mariano Montenegro Consejo Nacional para el Control de Estupefacientes Claudia Morales Moraga Comisión Nacional de Seguridad de Tránsito Felipe Moreno Godoy Ministerio del Interior Andrés Núñez T. Ministerio de Obras Públicas Alexander Pérez Méndez Ministerio de Comisión Nacional de Energía Pamela Pérez González Ministerio de Obras Públicas David Poblete Huanel Consejo Nacional de la Cultura y las Artes Mauricio Quintana Díaz Ministerio de Bienes Nacionales Sebastián Salazar Ministerio del Interior Paula Sierralta Roldán Ministerio de Planificación James Spencer Olave Ministerio de Obras Públicas Alejandro Soto Stuardo Ministerio de Justicia Guillermo Toro Avendaño Ministerio de Minería Sandra Vera Servicio Nacional de la Mujer G. Collaborators (Members of expert workshop (Taller Experto en Seminario Internacional 2009)) Martín Arcila Martínez Comunidad Terapéutica Talitakum Karin Ávila Benavides

8 National Alcohol Strategy - Chile
Servicio de Salud Metropolitano Oriente Maribel Bustos Costa Seremi de Salud, Magallanes Álvaro Campos Muñoz Servicio de Salud Metropolitano Sur Oriente Anselmo Cancino Sepúlveda Ministerio de Salud Ruth Depaux Vega Sociedad Chilena de Atención Primaria Ramón Florenzano Urzúa Servicio de Salud Metropolitano Oriente Tito Gallardo Olmedo Ministerio de Educación David Jernigan Johns Hopkins Bloomberg School Of Public Health. USA Tomo Kanda OPS/OMS Chile Paula Margozzini Maira Facultad de Medicina Pontificia Universidad Católica de Chile Sergio Martínez Gutiérrez Servicio de Salud Metropolitano Iquique Sergio Naser Japaz Pastoral de Alcohol y Drogas, Episcopado Nacional Pablo Norambuena Cárdenas Ministerio del Interior Hugo Sánchez Reyes Instituto de Nutrición y Tecnología de los Alimentos, Inta Lilia Sánchez Beltrán Ministerio de Obras Públicas Julia Sanhueza Santander Seremi de Salud de la Región del Bío Bío Rafael Sepúlveda Jara C.D.T. Hospital Barros Luco
Patricio Silva Rojas Universidad Diego Portales Francisca Werth Weiner Fundación Paz Ciudadana G. Health Ministry collaborators and technical support units Helia Molina Milman División Políticas Públicas y Saludables Marisol Acuña Anfossi División Políticas Públicas y Saludables Ximena Rayo Urrutia Unidad de Gestión de Redes de Salud Mental Irma Rojas Moreno Departamento de Salud Mental Cristián Palma Biepefeld Departamento de Salud Mental Orielle Solar Hormazabal Gabinete Subsecretaría Salud Pública Lucy Poffald Angulo Gabinete Subsecretaría Salud Pública Patricia Narváez Espínola Departamento de Salud Mental María Angélica Caprile Departamento de Salud Mental Pamela Bernales Gabinete Subsecretaría Salud Pública H. Health Ministry Authorities that mandated the elaboration of the National Alcohol Strategy Dr. Álvaro Erazo Latorre Ministro de Salud Dra. Jeannette Vega Morales Subsecretaria de Salud Pública Dr. Julio Montt Vidal Subsecretario de Redes Asistenciales
9 National Alcohol Strategy - Chile
I. EXECUTIVE SUMMARY*
*
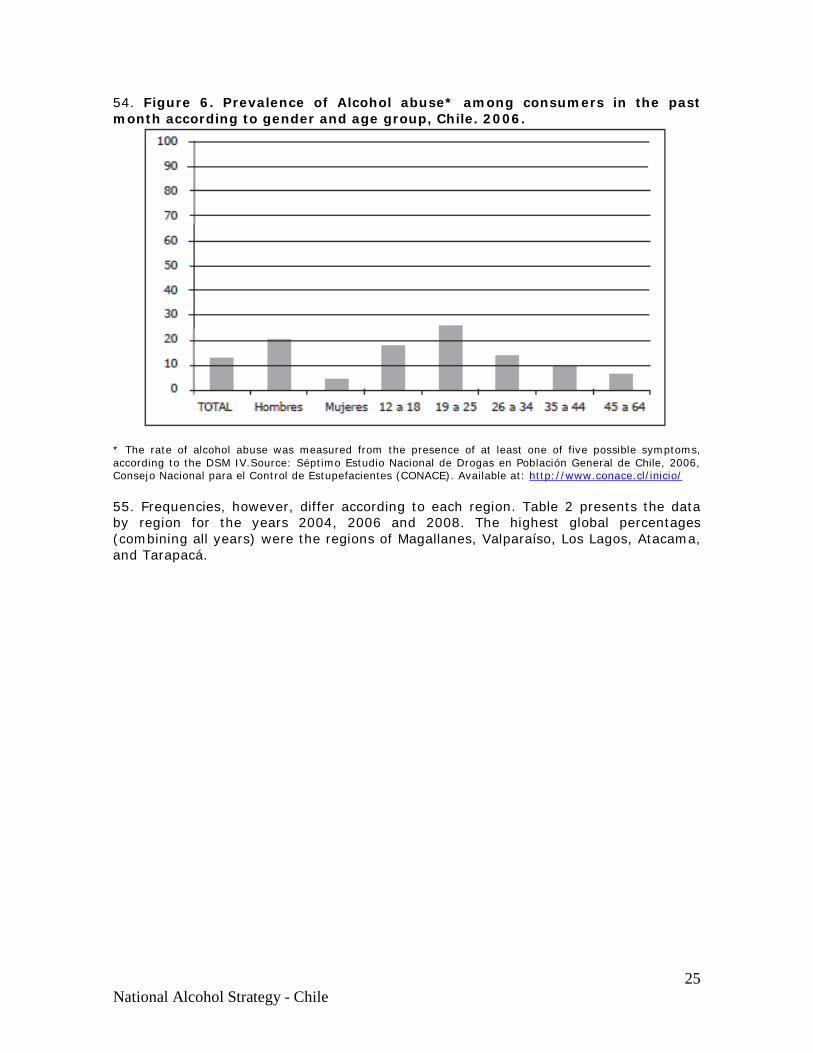
I. it is no longer necessary nor ethically acceptable for Chile to maintain a stance of passive resignation regarding the damages, suffering and losses that harmful alcohol consumption causes to its people, to social fabric, its coexistence and development, given the sufficient and adequate information now available on how to effectively address the issues of alcohol abuse, prevention and treatment. II. The National Alcohol Strategy deals with this is theme. After reviewing all the available information, it proposes to the public, its authorities, and institutions; a plan consisting of several lines of actions that would allow a substantial reduction of harmful alcohol consumption and its consequences over the next ten years. III. Due to the size and scope of this task, the National Alcohol Strategy poses a genuine Bicentennial Challenge for Chile. IV. Chileans have a long term relationship with alcoholic beverages, which in turn have associated costs and benefits: production and marketing of alcohol create job places for many people, high-quality wine exports are part of Chile’s international image, currency supply and tax revenue generate important fiscal income. V. On the other hand damaging effects to the consumer are generate by drinking alcohol above certain limits, but unlike any other product or merchandise, it not only affects the consumer, but third parties as well, including the social body as a whole. VI. Even though Chile has an average adult per capita consumption qualified as medium by international standards (8.2 liters of pure alcohol per year per person 15 years or older), the drinking pattern of a significant proportion of its population places Chile among nations with a high levels of risk and related harm. VII. The pattern of hazardous drinking refers to drinking in quantities that exceed limits that are manageable for the body (3 and 4 standard units of alcohol or “drinks” for women and men respectively, up to 5 days in the week) or in the form of episodic heavy drinking (more than 5 drinks at one sitting); drinking until intoxication or drunkenness (regardless of the degree of motor coordination); drinking in situations where small quantities cause risk to oneself or to others (driving vehicles or machinery, during pregnancy, by minors, in the workplace). VIII. The rapid transition from traditional problem consumption in Chile (mainly men who drink to the point of drunkenness on the weekend), towards a hazardous consumption pattern observable in a growing number of people, particularly youth, added to the increase of habitual consumption among women, the pressure of alcohol marketing and availability, the weak regulation of sales to minors and other factors, seem to explain the relatively uncomfortable position of Chile in comparison with other nations that have higher levels of consumption per capita, but exhibit lower rates of alcohol-related harm and negative consequences.
* This summary presents the main ideas of the "National Strategy on Alcohol. " For more precision and depth, please refer to the document extended and its annexes. The paragraph numbers are independent from those presented in the document issued.
10 National Alcohol Strategy - Chile
IX. The proportion of people that drank alcohol during the past month, an indicator of regular consumption, has been measured biennially in Chile since 1994. After strongly growing from the first survey (38.6%) until 2002 (58.1%), it stabilizes (until 2006) and even drops in 2008 (49.8%), though this trend has to prove consistency in upcoming surveys. XI. From the general population that declares having drunk alcohol during the past month, one out of eight people presented probable alcohol abuse (5 or more clinical symptoms). However, in the 19 to 35 age group, one of the most important groups in terms of productivity, the rate doubles (one out of four). XI. In the general adult population (15+ years old), one person out of six (16%) presents one or more problems regarding health, family or workplace derived from their consumption habits. This is five times more frequent among men than women. XII. One of the risk indicators, drinking five or more glasses of alcohol at one sitting (binge drinking), is an experience that is already present among 12% of students from the 8th grade of elementary school through the 12th grade of secondary education (4º año de Enseñanza Media), with a rapid progression from 9th grade or “1º medio” (one student out of 13) to 11th grade “3º medio” or (one out of six). XIII. Public safety on streets and highways seems seriously threatened by alcohol consumption. Over a span of 8 years (2000 – 2008), slightly more than 8% of traffic accidents and over 20% of all of the immediate deaths (within the first 24 hours) of pedestrians, drivers and passengers, occur under the influence of alcohol. Similarly, one out of two immediate deaths in traffic accidents are products of car/pedestrian collisions and of those, one out of five, the pedestrian tested positive for alcohol. Nevertheless, a wider perspective that takes into consideration larger number of sources as well as including all deaths, not only immediate ones, reveals that the mortality trend due to traffic accidents in Chile continues to rise. XIV. A relevant study done by the Segundo Estudio de la Carga de Enfermedad en Chile (Second Chilean Burden of Disease Study) with information from 2007, showed that alcohol dependency and hepatic cirrhosis are found among the five primary illnesses that lead to years of life lost due to premature death and disability. Cardiac diseases, hypertension, unipolar depression, gall bladder illnesses, traffic accidents, anxiety disorder and violent conditions are other maladies that, with differences between both sexes, top the list. Many of them are linked to alcohol consumption. XV. In addition, alcohol consumption was identified as the isolated risk factor, in 16 study subjects, which on its own explains the major proportion of years of life lost due to premature disability and death (12%). The next risk factor is obesity, accounting for 6%. Then comes hypertension, and at a lower level, sodium consumption, tobacco and hypoglycemia among others. XVI. On the other hand, even though high income sectors consume more alcohol in terms of volume than those of lower income, it’s the latter that concentrate the greatest proportion of problems associated with alcohol consumption. The measures to implement alcohol policies should take into account this unnoticed factor of inequity associated with alcohol consumption.
11 National Alcohol Strategy - Chile
XVII. Citizens worry about and wish to attain higher levels of public safety. Studies show that up to one of every fourteen crimes with high public impact (homicide, rape, injuries) is committed under the influence of alcohol. The frequency is much higher when studying offenses separately, where alcohol accounts for one out of six homicides and one out of four criminal injuries. XVIII. In the same manner, the country and its people aspire to continue advancing and taking definite steps to reach levels of economic and social development comparable with industrialized countries. XIX. A 1998 study on the costs pertaining to high-risk alcohol consumption, determined that they amount to four times the alcohol-related revenues to the country. The cash figures, in 1995 currency, may yield very different results from what the figure would be today (almost $3 billion dollars, or $209 dollars per capita annually), but were equivalent to a 3.4% of the GDP of that year. This includes indirect costs (lower productivity when workers are problem drinkers, because of premature death and absenteeism) and direct costs (health costs, police, accidents, destruction of assets). The economic benefits on the other hand reached US $602 million or US$59.00 per capita (exports, employed workforce, taxes) XX. Even though the balance and relation between damages and benefits does not seem to have changed in Chile, and its results are not that distinct from those that are found in other countries that have carried out similar research, an updating of this information is of utmost importance. The National Alcohol Strategy proposes the completion of this study for the year 2010 as one of its lines of action, in conjunction with an approach on avoidable costs. XXI: The choice of legal instruments, including regulations, sanctions and supervision, that Chile has enacted in order to better deal with problems related to alcohol consumption, although well guided, have been weakly enforced. Therefore, there is consensus on the precarious effectiveness of these measures. XXII. This is especially evident in information management inside municipal governments. The available data is scarce and there does not seem be an integrated system for regular data collection and analysis. It is at the local level that the implementation of public policies has the most to win or lose. With such a complex matter as alcohol, this entails a very good coordination between actors and institutions, as for example: municipal councils, local police judges, and community development, environment, public safety and health departments, among others. XXIII. The present Strategy seeks to relieve the role of municipal, as well as regional authorities, optimizing certain administrative procedures that contribute to the effectiveness of the existing regulatory framework. XXIV. The most crucial variable for implementing a State Policy with a renewed focus on these issues is the accumulated evidence collected by international evaluation studies regarding the effectiveness of certain strategic measures. A good example of a relevant study is the one performed by an outstanding group of researchers who analyzed thirty-four distinct strategies, and then organized them in the following areas: physical availability of alcoholic beverages, taxing and pricing, alcohol consumption context, education and persuasion, alcohol advertising, drinking and driving countermeasures, and treatments and early interventions.
12 National Alcohol Strategy - Chile
XXV. New studies and numerous publications have confirmed the specific measures that have shown the greatest effectiveness and influence on hazardous drinking behavior, both in the general population and in the most vulnerable groups. These are: (a) decreasing the physical availability of alcoholic beverages, regulating days and hours of retail sales, regulating density and location of alcohol outlets, strict enforcement of the prohibition of sale to minors; (b) reducing the economic availability through mechanisms that increase prices of alcoholic beverages; (c) reducing the upper limit for Blood Alcohol Content for drivers, random sobriety tests by the police, strict sanctions with an emphasis on the suspension of drivers licenses (d) active detection of at-risk drinkers and early interventions (Brief Intervention). XXVI. Both the recommendations of experts and the experience of those countries that have implemented national alcohol strategies, such as Australia, Scotland and New Zealand, suggest that simultaneous action is needed in order to significantly influence the consumer and risk groups, as well as the general population and the social and cultural context. An interesting Canadian simulation study estimated mortality reductions and burden of disease rates of about 18%, due to the effect of jointly implementing a reduction of legal blood alcohol content to 0.5%, raising the legal drinking age from 18 to 21 years, implementing brief interventions for high-risk drinkers and raising taxes XXVII. As for Chile as well, the proposed lines of action not only affect consumers, but take into account the market and the context. It does not seem fair that all responsibility for harmful drinking should fall on the individual. It is not reasonable to expect positive results when those preventive measures that the society organizes (information, education, limits, sanctions), aim to influence only the decisions and behavior of individual consumers. The strong cultural and social determinants of alcohol consumption should also be subjects of a national alcohol policy. A succinct and guiding formulation of the objectives of the National Alcohol Strategy would be the following: “Drink responsibly”, as well as “Sell responsibly” and “Advertise responsibly”. XXVIII. Harmful alcohol consumption not only affects Chile. The globalization of information, of markets and of cultural aspects regarding the transaction of consumer goods, coincides with an increase in alcohol consumption and related problems in many nations that until recently evidenced a cultural pattern of moderate consumption. XXIX. The WHO, alarmed by the contribution of alcohol to the global burden of disease and influence in certain Regions and countries, reactivated its leading role in the field of alcohol consumption and initiated a process of progressive construction of a global strategy to reduce harmful effects of alcohol consumption. This will be considered and voted on by the World Health Assembly in 2010. This is the framework and stimulus for the Chilean Strategy on the matter. XXX. The National Alcohol Strategy proposed for Chile makes reference to a framework of respect for the rights of (a) children, teens, and adults, to develop and live in safety and protection with respect to the risks and damages that they could suffer, based on harmful alcohol consumption of third parties and, (b) the rights of people affected by physical and mental illnesses determined by or associated with alcoholic beverage consumption, to have access to health services and other benefits, in the same manner as if they had been afflicted by any other kind of disease.
13 National Alcohol Strategy - Chile
XXXI. The National Alcohol Strategy focuses on the following priority areas:
a) Children and adolescents, due to their special biological and psychological vulnerability to alcohol;
b) Pregnant women and their unborn children who are susceptible to persistent harm in varying degrees.
c) The lives lost or damaged of those injured in traffic accidents related to alcohol consumption.
d) The social cost related to consumption of alcohol in especially sensitive areas such as domestic and criminal violence, absenteeism and workplace accident probability.
e) The incidence of alcohol use in a broad variety of illnesses and its contribution to the burden of disease
XXXII. The National Alcohol Strategy sets out nine lines of action and a series of concrete measures for each one (see summary of in Annex 1). These are:
1. Information to the public and control of advertising. 2. Availability of alcohol 3. Alcohol taxes and retail prices 4. Alcohol and policies on retail sales 5. Traffic accidents and harmful alcohol consumption 6. Hazardous alcohol consumption and health care services 7. Community action, and local governments (municipal) 8. Education, training, and personal development 9. Monitoring, evaluation and follow up.
XXXIII. With the gradual and consorted implementation of these lines of action, progress can be made towards accomplishing these goals that however difficult, are necessary for changing the relationship of Chileans to alcohol:
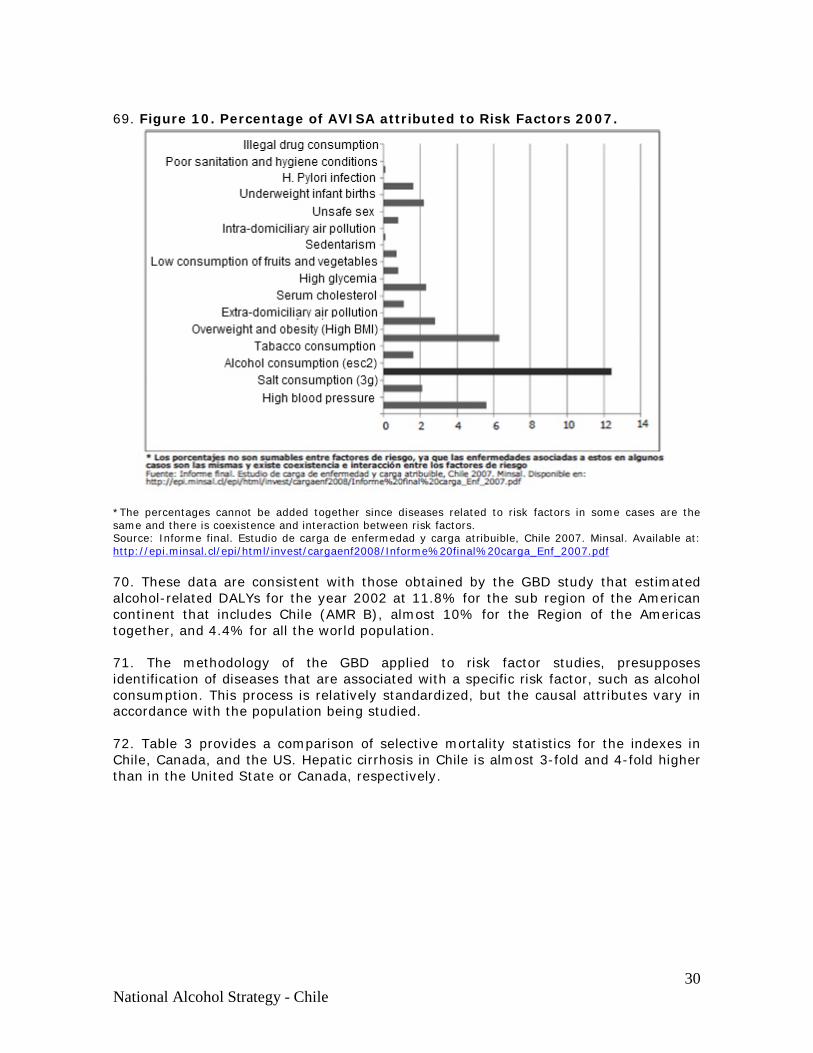
a) A more protective physical, social and cultural environment that promotes alcohol consumption without risk;
b) People with greater freedom to choose not drink alcohol or to drink at levels without risk;
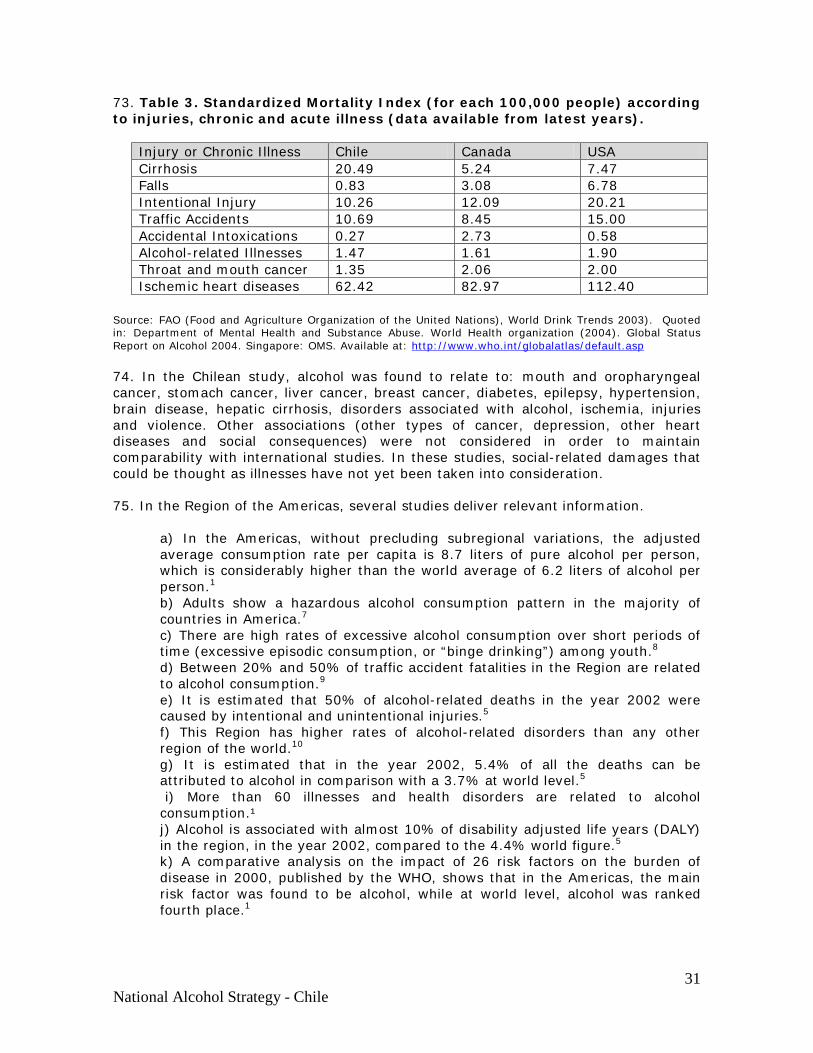
c) More control over availability and access to alcoholic beverages; d) Increased protection for victims of harmful alcohol drinking e) Increased access to adequate treatment for affected persons.
XXXIV. Some intermediate results that should be subject to constant monitoring express themselves in changes in the patterns of consumption among risk groups: a lower number and proportion of youth and adults who drink until intoxication; have five or more drinks at one sitting; and/or drink and drive; and a smaller number of women that drink during pregnancy. In turn, these changes generate positive social consequences as they reduce levels of absenteeism and labor-related injuries, domestic violence, disease burden, and the number of children with brain injuries or disorders. XXXV. Ultimately, a healthier, safer, and more developed Chile will be possible thanks to significant mediate gains: healthier individuals and families, safer and more confident communities, increased work productivity, lower social costs as well as lower expenses in the health and justice areas.
14 National Alcohol Strategy - Chile
XXXVI. The National Alcohol Strategy will require of a potent management infrastructure, that could include a Rector Organism wherein rests the responsibility of the entire government, in a similar manner to a National Council, integrated by several Secretaries of State, in addition to the Department of Health and presided over by the Ministry for National Planning. Moreover, this includes an Executive Technical Secretary, entrusted with the implementation of the decisions of the National Council, and the effective coordination between the participating sectors and the dialogue with civil society, the community and other interested sectors. XXXVII. The organic development of the National Alcohol Strategy requires an implementation that is both task and process oriented. It should develop through stages that do not recognize precise boundaries between them. The first phase consists of closely delimited process of consultations to institutions of the political, social, entrepreneurial, labor-related, academic worlds and to the general public from which new focuses, proposals and cautions will arise - all of them useful and necessary. XXXVIII. The formulation of the National Alcohol Strategy document in Chile coincides with the arrival of a new government administration. This scenario could establish itself as an even better opportunity, given that, from the objective analysis of the proposals included, it is clear that this strategy leads to a path of global development for the country, and for the health and safety of its people. These are objective pursued by all new governments.
II. INTRODUCTION
1. The National Alcohol Strategy sets a Bicentennial Challenge to the country, its institutions, its and authorities to: substantially reduce harmful alcohol consumption and its consequences over the next ten years. 2. To present core ideas so that Chile may put forth a state policy with this objective in mind. If it is approved by the citizenship, consistently implemented and demonstrates effectiveness, it will constitute an exceptional step towards harmonious human, social and economic development.
3. The scope of its benefits could be enormous as has been the case of other successful public health policies in our country’s history.
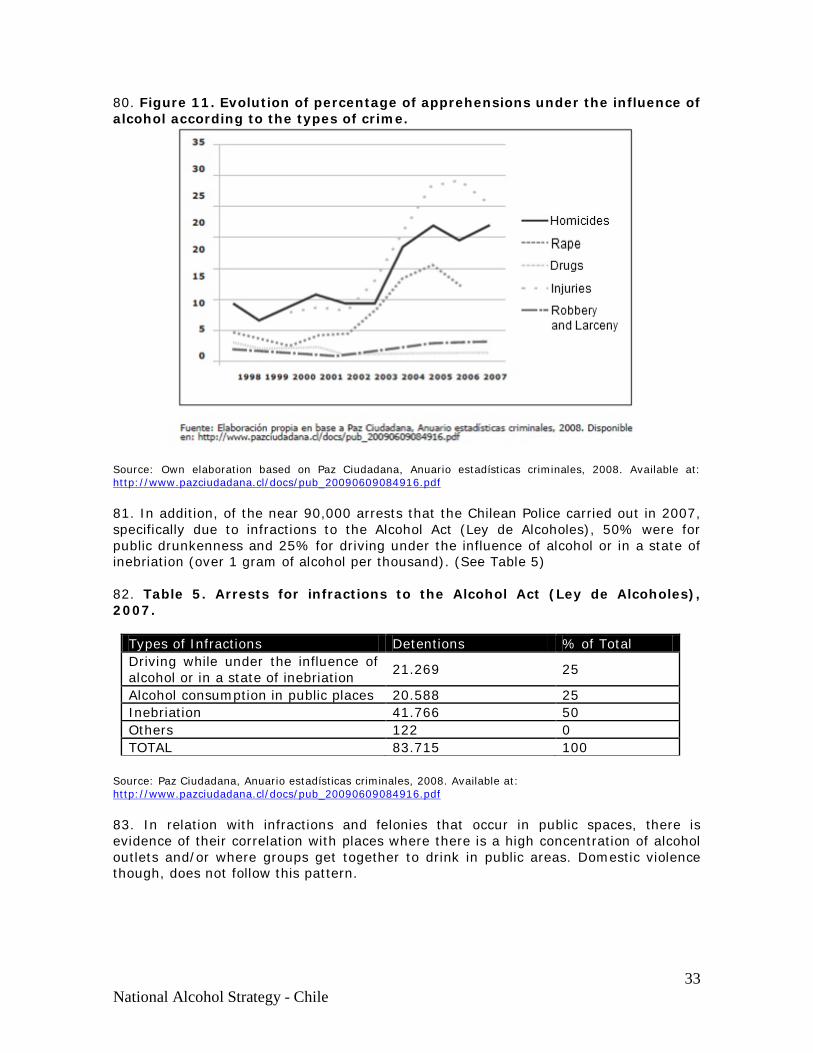
4. The National Alcohol Strategy, based on the solid support of evidence, will be able to complement and harmonize the diverse approaches and policies that operate simultaneously; the economy (production and productivity, income for the population that labors in the alcohol sector, for the industry and for the State, associated costs, etc.); the judicial system (security, police, trials and sanctions at the local, family, labor, penal and economic levels ) and welfare (coexistence, income and benefits, sports and recreation, etc.) 5. The Strategy seeks a cultural change in the relationship of Chileans with alcohol which will ultimately lead most of the population into adhering to and participating in a pattern of low risk alcohol consumption. 6. A still far off, but possible objective, is that by the end of the decade following Chile’s Bicentennial, the country will count on having a well-structured state policy that has elicited social consensus and strikes an acceptable balance between the benefits of
15 National Alcohol Strategy - Chile
the alcohol related economy and the protection required from the damages and avoidable negative consequences of alcohol consumption. 7. As a consequence of this policy, there will be a substantial reduction in deaths, injuries, disabilities because of accidents, violence and illnesses related to the consumption of alcohol. The losses in lower productivity as well as health, police, and justice expenses related to alcohol consumption will also decrease. 8. Industry and commerce will perfect creative and effective forms of achieving public health protection objectives. Nevertheless, the effects of this policy are not meant to impinge on their legitimate earnings and investments. 9. Families, young people and society as a whole will be envisioning forms of coexistence, recreation and socialization in which the non-consumption or responsible consumption of alcohol become more frequent, as well as socially accepted and reinforced behaviors. 10. The National Alcohol Strategy will have been a determinant factor in these results. 11. The National Alcohol Strategy proposed here began its first phase of elaboration at the end of 2008, with a collaboration agreement reached between the Ministry of Health, the Pan American Health Organization (PAHO) and the Centre for Addiction and Mental Health (CAMH) in Canada. That same year Chile was recognized for its development of mental health care inside the Primary Health Care system and for the evident advances made in coverage, diversity and quality of service for those affected by mental health problems due to, among other reasons, alcohol abuse and dependence. However, the data from the Second Study of Burden of Disease showed that alcohol consumption was by far the greatest contributing factor in mental diseases and it was already known that indicators of Health Objectives for the Decade evinced poor results relative to the consequences of alcohol consumption. 12. A first document - a report with conceptual input, a compilation of experiences in other countries and recommendations- was commissioned and elaborated by a CAMH consultant, Professor Norman Giesbrecht, in collaboration with professionals from the CAMH and the Chile’s Ministry of Health. 13. In June 2009, the first International Seminar allowed nearly two hundred people from health sectors, state sectors and academia, to analyze this first report, with strong support from international experts. The industry was also invited as an observer. An expert workshop, in the framework of the seminar, drew up a “roadmap” for transforming the recommendations into proposals and concrete measures through the careful elaboration and editing work done by a small group (office of the Technical Secretary of the National Strategy), to be validated by a broad representative group of the state sectors (an Interministerial Committee for the elaboration of the National Strategy), and then, having reached a level of sufficient basic agreement within the State domain, the next step is to offer such agreements to civil society and open and inclusive debate. 14. The Technical Secretary finished its task in December 2009. The Inter-ministerial committee convened on six occasions between July 2009 and January 2010. The present document is the work result of professional groups among the Secretaries of State.
16 National Alcohol Strategy - Chile
15. In the following stage, it is necessary to embark on a period of consultation and debate with all involved sectors. Opinions and positions on this topic will be legitimately diverse and conflicting. For these to be properly assessed, considered and integrated, it is essential that they be presented in terms of pieces of information whenever possible, supported by objective or objectified data in such a way that conclusions and final decisions rest upon a rational base, susceptible to evaluations and modifications over time. 16. The significant goals that the Strategy seeks to achieve: reductions in harmful alcohol consumption and its consequences as well as changes in the relationship between Chileans and alcohol are expected to yield results in an estimated time of no less than 10 years, over the course of which the assumptions made in the proposals of this Strategy will be put to the test. 17. It will be necessary to resolutely support carrying out studies to unveil areas not often explored (such as the effects and costs of public policies implemented up to now in the country, social representations that underlie harmful drinking practices of specific segments of the population), in order to confirm or refute several of the Strategy’s assumptions, as well as the arguments to the contrary that will most likely arise. This should be an important part of the implementation of its proposals. BACKGROUND
18. Chile has a longstanding relationship with alcohol. Before the arrival of Europeans, indigenous peoples used alcohol in a pattern characterized by regulated and ritual consumption, although related to episodes of collective intoxication several times per year. As time passed, through miscegenation and colonial transculturalization, the majority of the population adopted a pattern of wine, and later of beer, consumption that is defined as being almost exclusively male and by episodic drinking during weekends apart from meals until reaching the point of inebriation. 19. Over the last 40 years, and with increasing speed, this “traditional” pattern is suffering important changes due to the incorporation of women into a culture of frequent consumption, at times reaching levels of intoxication which not long ago were socially-sanctioned, and also of adolescents at increasingly younger ages, who drink mainly on weekends with the intention of becoming intoxicated in very visible minority groups. The changes of this last phase clearly correlate with the phenomena of globalization of customs and the market economy. The wide availability and accessibility to alcoholic beverages in the physical and cultural environment, because of the manner it is offered, as well as for its relatively low prices, increases the pressure towards consumption, which is proven by the sustained decrease of the proportion of alcohol abstainers in the population and the onset of consumption at increasingly at younger ages 20. The introduction of vineyards in the country began early in the colony. Since early on, people appreciated the quality of the climate and soil. However, the boom of agriculture of vineyards and industrialization is fairly recent. Today, alcoholic drinks constitute a vigorous commercial product. Chilean wines are promoted as one of the country’s main presentation card among other nations; beer and liquor imports have grown and the internal consumption shows a sustained growth, a result of the increase in wages.
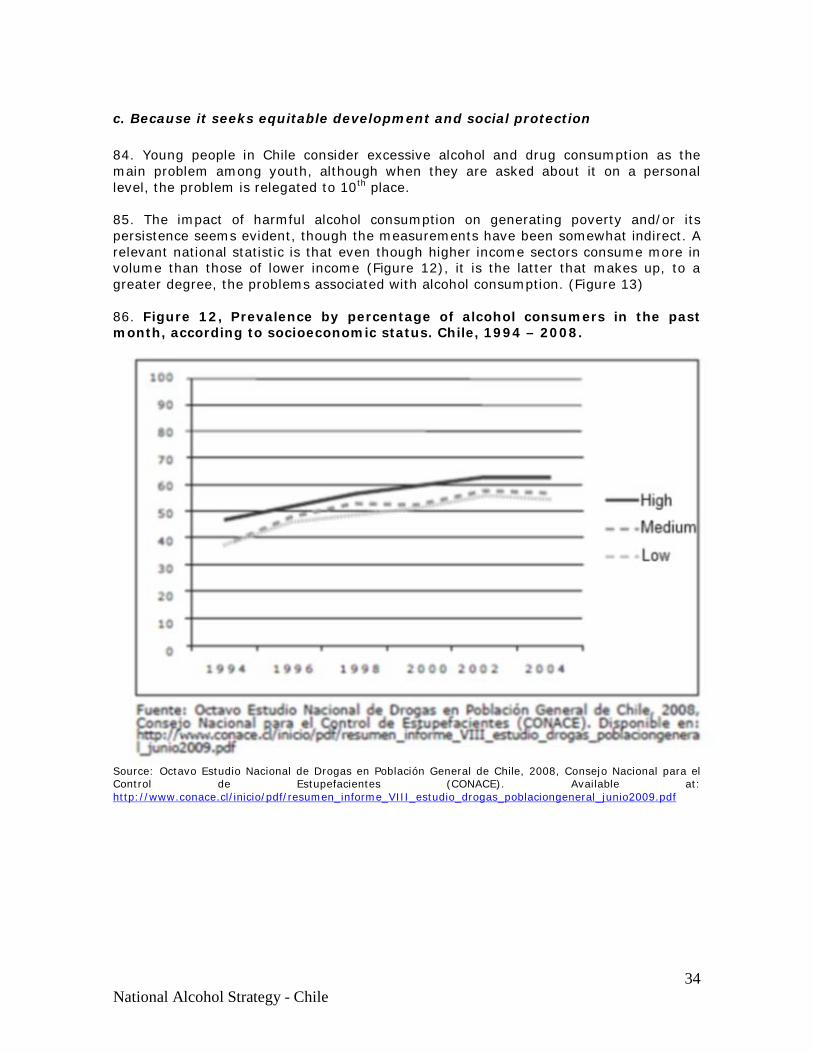
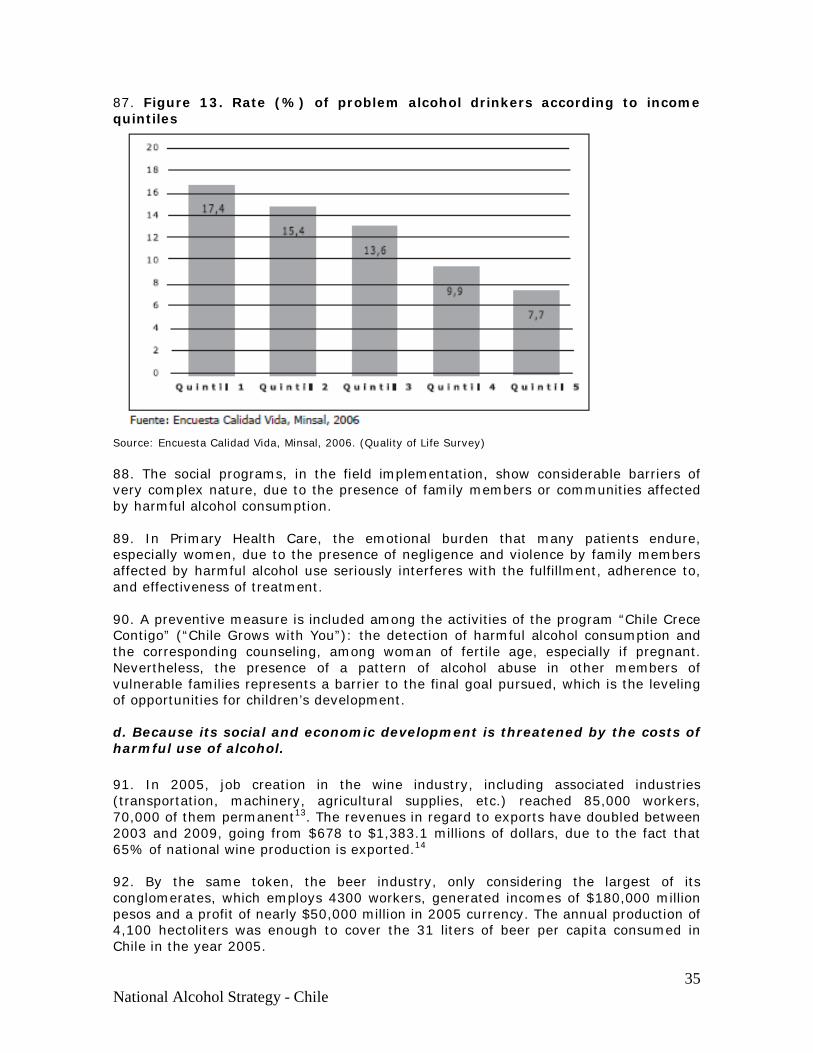
17 National Alcohol Strategy - Chile
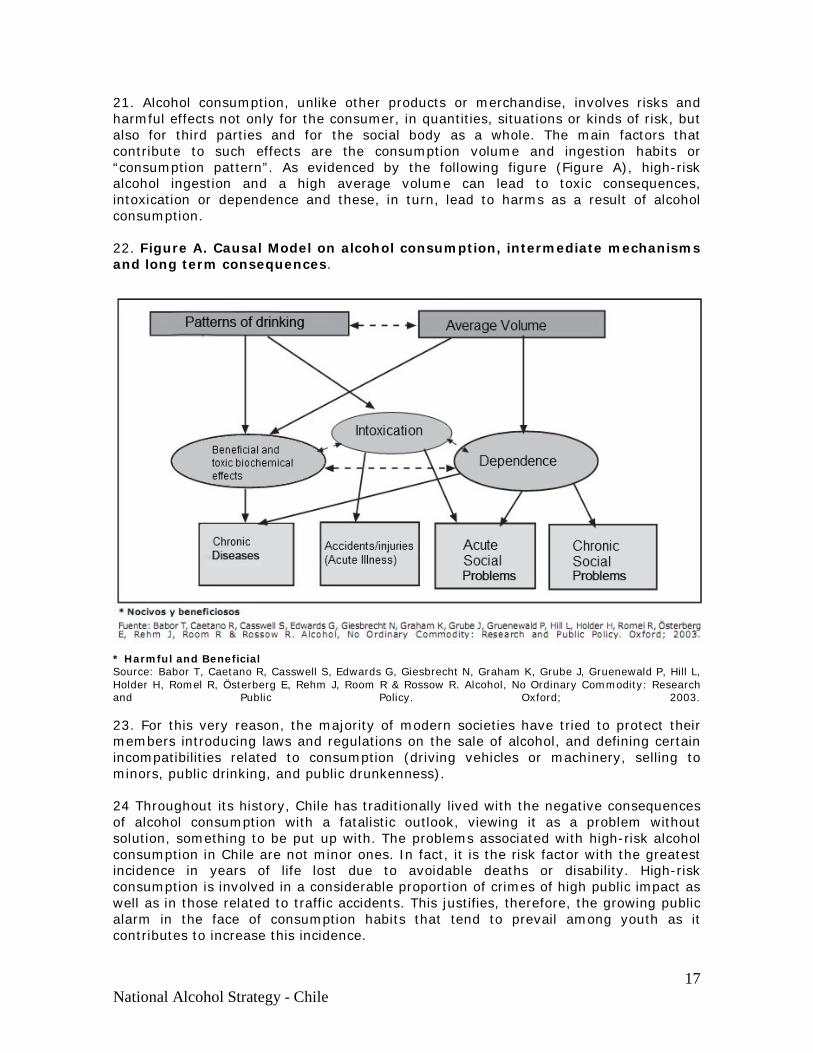
21. Alcohol consumption, unlike other products or merchandise, involves risks and harmful effects not only for the consumer, in quantities, situations or kinds of risk, but also for third parties and for the social body as a whole. The main factors that contribute to such effects are the consumption volume and ingestion habits or “consumption pattern”. As evidenced by the following figure (Figure A), high-risk alcohol ingestion and a high average volume can lead to toxic consequences, intoxication or dependence and these, in turn, lead to harms as a result of alcohol consumption. 22. Figure A. Causal Model on alcohol consumption, intermediate mechanisms and long term consequences.
* Harmful and Beneficial Source: Babor T, Caetano R, Casswell S, Edwards G, Giesbrecht N, Graham K, Grube J, Gruenewald P, Hill L, Holder H, Romel R, Österberg E, Rehm J, Room R & Rossow R. Alcohol, No Ordinary Commodity: Research and Public Policy. Oxford; 2003. 23. For this very reason, the majority of modern societies have tried to protect their members introducing laws and regulations on the sale of alcohol, and defining certain incompatibilities related to consumption (driving vehicles or machinery, selling to minors, public drinking, and public drunkenness). 24 Throughout its history, Chile has traditionally lived with the negative consequences of alcohol consumption with a fatalistic outlook, viewing it as a problem without solution, something to be put up with. The problems associated with high-risk alcohol consumption in Chile are not minor ones. In fact, it is the risk factor with the greatest incidence in years of life lost due to avoidable deaths or disability. High-risk consumption is involved in a considerable proportion of crimes of high public impact as well as in those related to traffic accidents. This justifies, therefore, the growing public alarm in the face of consumption habits that tend to prevail among youth as it contributes to increase this incidence.
18 National Alcohol Strategy - Chile
25. The policies and plans that Chile has set for itself to confront these problems have been weak. Legal changes have resulted in prolonged and ineffectual controversies, and political support and financing has been scant. Furthermore, the measures taken have been, in general, biased, isolated, inconsistent, weakly regulated and insufficiently evaluated. In the end, the sought-after objectives and results have been elusive and unsatisfactory. 26. Additionally, the use of “alcoholism”, the most common designation, has contributed to dealing with the problem in a biased and reductionist manner. In effect, the major proportion of negative consequences related to the pattern of alcohol consumption are not provoked by individual alcoholics (alcohol dependants), but rather by those who, while not sharing this condition, do drink to the point of intoxication, drink large quantities in one sitting, drive vehicles under the influence of alcohol, or diminish their productivity and work efficiency due to their alcohol ingestion habits which in these cases does not necessarily imply alcohol dependency. 27. The terms “harmful alcohol consumption” (consumo nocivo), and “hazardous consumption” (consumo de riesgo) will be used interchangeably with respect to this document, though the WHO describes them as somewhat separate ideas. Both include not only the behavior of one or various individuals in the face of alcoholic beverages, but also a wide and complex grouping of factors that influence or determine these behaviors, not infrequently, despite the will of the individuals involved.
28. Countries that have compared gains and losses due to alcohol use have systematically concluded that the latter is considerably greater. This is also the case in Chile, making it necessary to envision and move towards a new and improved balance between gains and losses. 29. Over the past years, several well proven studies have directed attention towards alcohol consumption, hazardous drinking and the harm derived from alcohol consumption. These studies show that within the Americas, these figures are 40% higher than the global average. 30. The State has the right and also the duty to protect its citizens from the harms related to alcohol consumption, especially those most vulnerable, as is the case of children. Citizens should also be protected from alcohol-related harms caused by third parties. For this to be possible, it is necessary that decision-makers and the general population handle a sufficient level of updated information, based on objective evidence, so that they are not inhibited in giving the required support to the implementation of alcohol policies.
19 National Alcohol Strategy - Chile
III. WHY DOES CHILE NEED A NATIONAL ALCOHOL STRATEGY?
31. There are various answers to this question:
a. Because the loss of lives and diminished quality of life associated with alcohol injures the country.
b. Because Chile is concerned about and desires to achieve higher levels of public safety.
c. Because it seeks equitable development and social protection. d. Because its social and economic development is threatened by the
costs caused by the harmful use of alcohol.
a. Because the loss of lives and diminished quality of life associated with alcohol injures the country. 32. Chile has suffered, suffers, and will continue to suffer from death and damage to the quality of life of its inhabitants caused by alcohol consumption. The ways in which alcohol gives rise to these effects are varied and range from the most known, such as alcoholism and cirrhosis, to others less known and visible such as certain types of cancer, cardiovascular diseases and mental health disorders as well as other illnesses. 33. Alcohol consumption not only causes harm to the individual consumer, but also to third parties. The expectant mother inevitably does injure herself as well as her unborn child. The father can also negatively affect the development of the children if he demonstrates a hazardous consumption pattern or if he gives rise to an adverse parenting environment due to alcohol abuse. 34. Drivers and pedestrians that consume alcohol also cause deaths and injuries to third parties in traffic accidents. In the same way, we all endure public annoyances and insecurity due to violence and crime related to alcohol consumption in public spaces. 35. The relation between the volume of alcohol consumption within the population and the negative effects of the same is not simple. In general terms, the higher the level of consumption per capita, the higher the proportion of high-risk drinkers, and in turn, the higher the frequency of negative effects; nevertheless, the last appear to be determined more by the proportion of high-risk drinkers and the pattern of prevalent consumption. This explains why countries and regions that have an elevated per capita consumption rate show less alcohol related harm than others with lower consumption per capita. 36. Chile has an average per capita alcohol consumption that falls in the medium range, but a high incidence of alcohol-related harm in the areas of health, safety and productivity as will be demonstrated in the following pages. To a much larger extent, the latter is due to the pattern of hazardous consumption within its population, rather than to average consumption. 37. Alcohol consumption, hazardous consumption, and problem drinking (abuse) Alcohol Consumption. The prevalence of alcohol consumers in Chile (measured by the number of people reporting having consumed alcohol in the past year or month)
20 National Alcohol Strategy - Chile
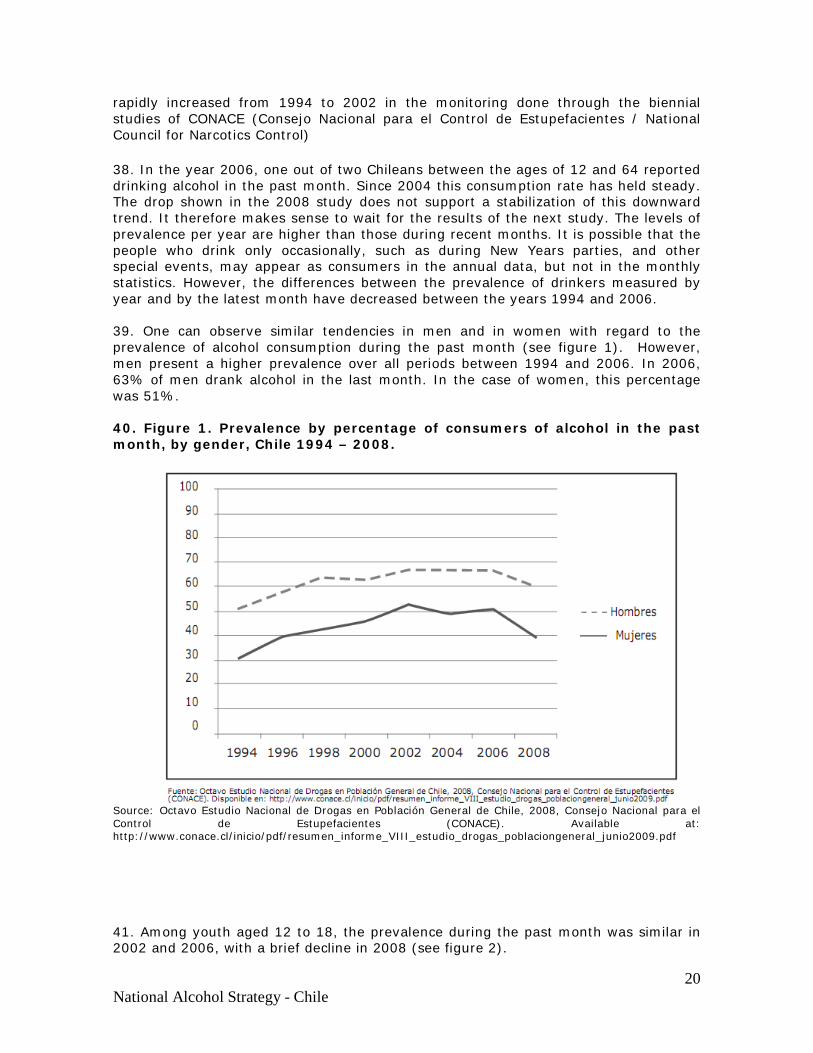
rapidly increased from 1994 to 2002 in the monitoring done through the biennial studies of CONACE (Consejo Nacional para el Control de Estupefacientes / National Council for Narcotics Control) 38. In the year 2006, one out of two Chileans between the ages of 12 and 64 reported drinking alcohol in the past month. Since 2004 this consumption rate has held steady. The drop shown in the 2008 study does not support a stabilization of this downward trend. It therefore makes sense to wait for the results of the next study. The levels of prevalence per year are higher than those during recent months. It is possible that the people who drink only occasionally, such as during New Years parties, and other special events, may appear as consumers in the annual data, but not in the monthly statistics. However, the differences between the prevalence of drinkers measured by year and by the latest month have decreased between the years 1994 and 2006. 39. One can observe similar tendencies in men and in women with regard to the prevalence of alcohol consumption during the past month (see figure 1). However, men present a higher prevalence over all periods between 1994 and 2006. In 2006, 63% of men drank alcohol in the last month. In the case of women, this percentage was 51%. 40. Figure 1. Prevalence by percentage of consumers of alcohol in the past month, by gender, Chile 1994 – 2008.
Source: Octavo Estudio Nacional de Drogas en Población General de Chile, 2008, Consejo Nacional para el Control de Estupefacientes (CONACE). Available at: http://www.conace.cl/inicio/pdf/resumen_informe_VIII_estudio_drogas_poblaciongeneral_junio2009.pdf 41. Among youth aged 12 to 18, the prevalence during the past month was similar in 2002 and 2006, with a brief decline in 2008 (see figure 2).
21 National Alcohol Strategy - Chile
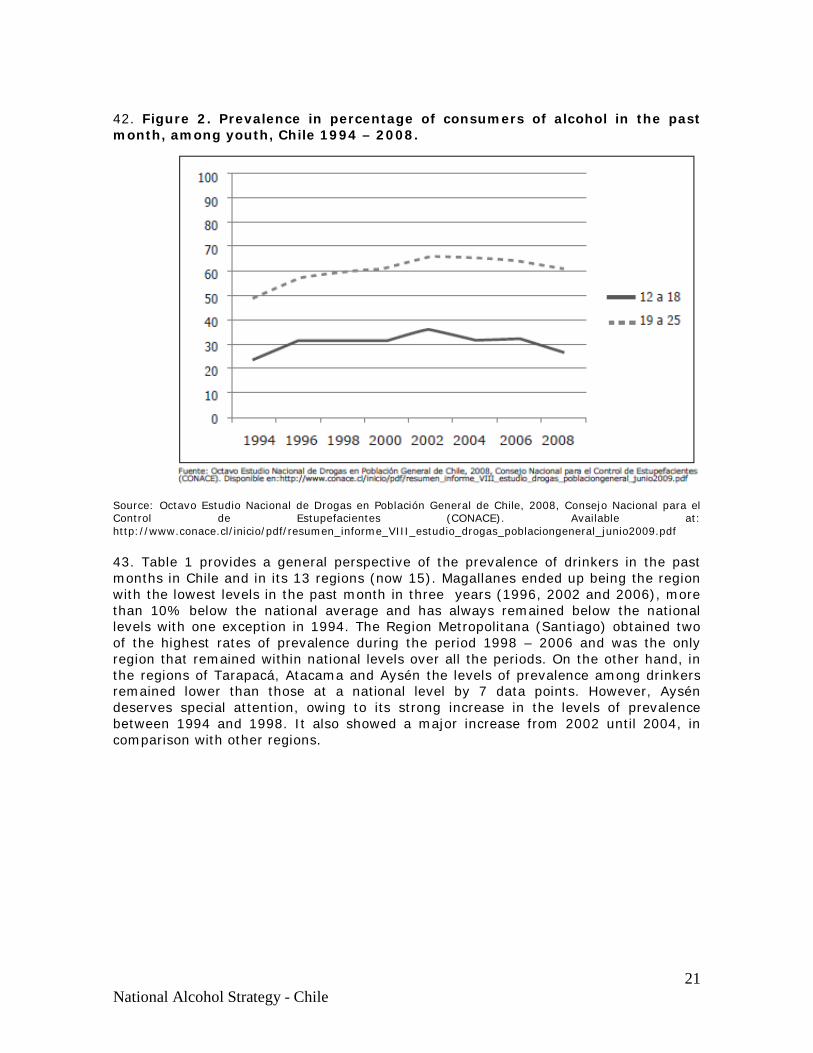
42. Figure 2. Prevalence in percentage of consumers of alcohol in the past month, among youth, Chile 1994 – 2008.
Source: Octavo Estudio Nacional de Drogas en Población General de Chile, 2008, Consejo Nacional para el Control de Estupefacientes (CONACE). Available at: http://www.conace.cl/inicio/pdf/resumen_informe_VIII_estudio_drogas_poblaciongeneral_junio2009.pdf 43. Table 1 provides a general perspective of the prevalence of drinkers in the past months in Chile and in its 13 regions (now 15). Magallanes ended up being the region with the lowest levels in the past month in three years (1996, 2002 and 2006), more than 10% below the national average and has always remained below the national levels with one exception in 1994. The Region Metropolitana (Santiago) obtained two of the highest rates of prevalence during the period 1998 – 2006 and was the only region that remained within national levels over all the periods. On the other hand, in the regions of Tarapacá, Atacama and Aysén the levels of prevalence among drinkers remained lower than those at a national level by 7 data points. However, Aysén deserves special attention, owing to its strong increase in the levels of prevalence between 1994 and 1998. It also showed a major increase from 2002 until 2004, in comparison with other regions.
22 National Alcohol Strategy - Chile
44. Table 1. Prevalence of alcohol consumption in the past month according to region, Chile*. Region of Chile 1994 1996 1998 2000 2002 2004 2006 National 38.6 46.5 51.5 53 58.1 56.3 56.7 Tarapacá 36.2 44.0 48.1 51.5 55.3 53.2 51.8 Antofagasta 36.7 40.9 49.5 54.8 51.6 50.7 47.0 Atacama 34.0 37.0 43.8 48.9 50.5 50.7 42.5 Coquimbo 31.7 38.6 39.9 53.6 62.3 51.1 51.5 Valparaíso 41.1 46.2 47.4 56.1 59.8 59.5 57.0 O` Higgins 41.6 52.9 42.4 51.0 56.0 54.7 50.3 Maule 39.5 38.5 49.9 48.3 56.3 47.6 50.6 Bio Bio 33.8 36.1 50.6 44.5 59.1 55.2 53.2 Araucanía 34.0 45.0 52.9 53.0 57.8 52.3 53.9 Los Lagos 39.2 41.5 50.9 48.8 49.4 48.9 56.2 Aisén 15.4 39.8 49.6 44.3 57.2 53.0 49.4 Magallanes 40.8 33.8 40.3 48.0 47.9 50.0 42.5 Metropolitana (Santiago)
40.1 50.8 54.3 55.1 59.6 58.9 60.6
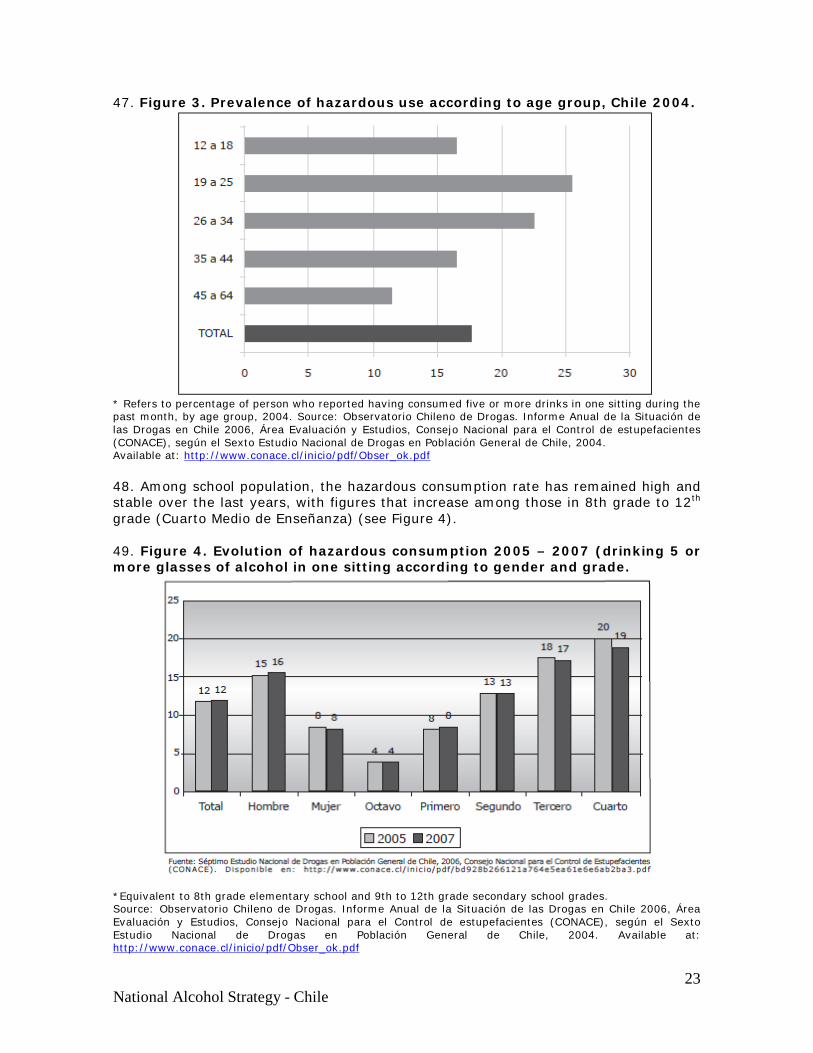
*Indicators adjusted for age and gender according to simple distribution. 2006 Source: Séptimo Estudio Nacional de Drogas en Población General de Chile, 2006, Consejo Nacional para el Control de Estupefacientes (CONACE). Available in: http://www.conace.cl/inicio/pdf/bd928b266121a764e5ea61e6e6ab2ba3.pdf 45. A general observation of the regional data reveals a relevant aspect of the complexity of alcohol consumption in Chile: some of the regions that show lower levels of global consumption simultaneously demonstrate the highest levels of harmful consumption. As noted, the volume of consumption is important, but the pattern of consumption is just as significant. (See table 2). 46. Hazardous Drinking. Refers to drinking: (a) in volumes that exceed safety limits according to sex and age, (b) with intoxication or drunkenness, (c) in risky situations (driving of vehicles or machinery, pregnancy, minors, in presence of certain illness or when one is on medication). In operational terms, the indicator “excessive episodic drinking” is used, defined by the ingestion of 5 or more drinks in one sitting (“binge drinking”). At a national level, we find that 26% of people in the 19 to 25 age group engaged in this behavior at least once during the past month. In second place came the 26-34 age group. (see figure 3).
23 National Alcohol Strategy - Chile
47. Figure 3. Prevalence of hazardous use according to age group, Chile 2004.
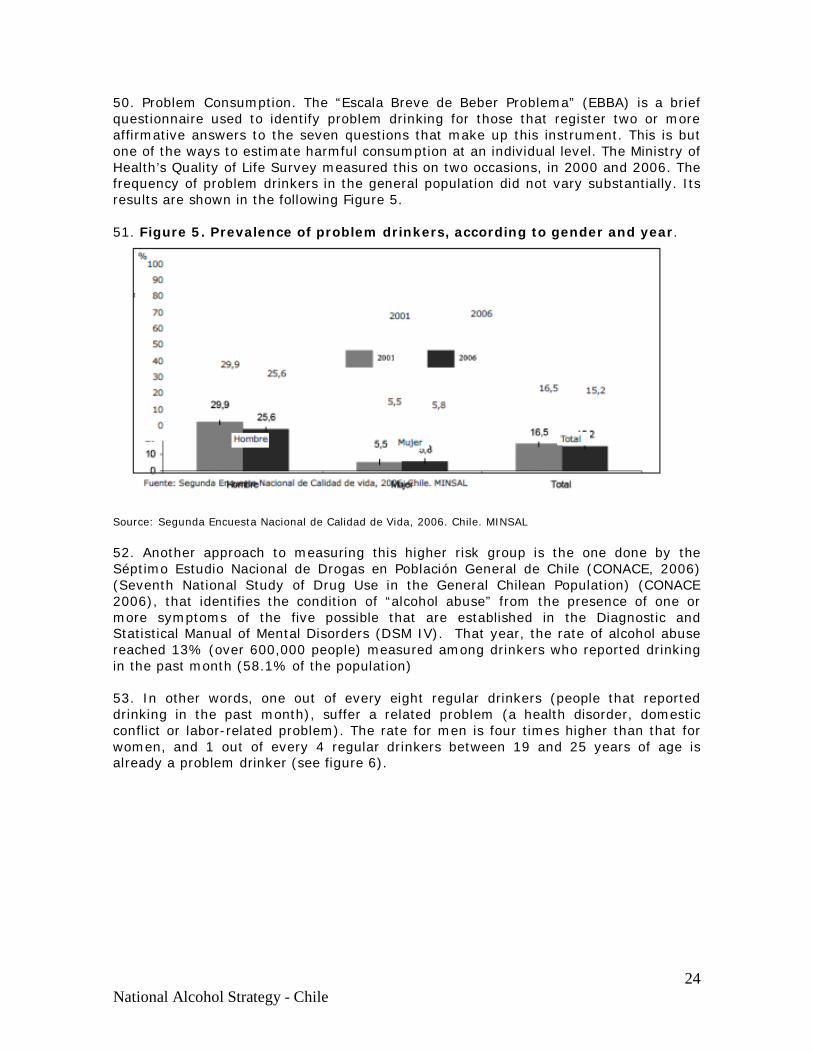
* Refers to percentage of person who reported having consumed five or more drinks in one sitting during the past month, by age group, 2004. Source: Observatorio Chileno de Drogas. Informe Anual de la Situación de las Drogas en Chile 2006, Área Evaluación y Estudios, Consejo Nacional para el Control de estupefacientes (CONACE), según el Sexto Estudio Nacional de Drogas en Población General de Chile, 2004. Available at: http://www.conace.cl/inicio/pdf/Obser_ok.pdf 48. Among school population, the hazardous consumption rate has remained high and stable over the last years, with figures that increase among those in 8th grade to 12th grade (Cuarto Medio de Enseñanza) (see Figure 4). 49. Figure 4. Evolution of hazardous consumption 2005 – 2007 (drinking 5 or more glasses of alcohol in one sitting according to gender and grade.
*Equivalent to 8th grade elementary school and 9th to 12th grade secondary school grades. Source: Observatorio Chileno de Drogas. Informe Anual de la Situación de las Drogas en Chile 2006, Área Evaluación y Estudios, Consejo Nacional para el Control de estupefacientes (CONACE), según el Sexto Estudio Nacional de Drogas en Población General de Chile, 2004. Available at: http://www.conace.cl/inicio/pdf/Obser_ok.pdf
24 National Alcohol Strategy - Chile
50. Problem Consumption. The “Escala Breve de Beber Problema” (EBBA) is a brief questionnaire used to identify problem drinking for those that register two or more affirmative answers to the seven questions that make up this instrument. This is but one of the ways to estimate harmful consumption at an individual level. The Ministry of Health’s Quality of Life Survey measured this on two occasions, in 2000 and 2006. The frequency of problem drinkers in the general population did not vary substantially. Its results are shown in the following Figure 5. 51. Figure 5. Prevalence of problem drinkers, according to gender and year.
Source: Segunda Encuesta Nacional de Calidad de Vida, 2006. Chile. MINSAL 52. Another approach to measuring this higher risk group is the one done by the Séptimo Estudio Nacional de Drogas en Población General de Chile (CONACE, 2006) (Seventh National Study of Drug Use in the General Chilean Population) (CONACE 2006), that identifies the condition of “alcohol abuse” from the presence of one or more symptoms of the five possible that are established in the Diagnostic and Statistical Manual of Mental Disorders (DSM IV). That year, the rate of alcohol abuse reached 13% (over 600,000 people) measured among drinkers who reported drinking in the past month (58.1% of the population) 53. In other words, one out of every eight regular drinkers (people that reported drinking in the past month), suffer a related problem (a health disorder, domestic conflict or labor-related problem). The rate for men is four times higher than that for women, and 1 out of every 4 regular drinkers between 19 and 25 years of age is already a problem drinker (see figure 6).
25 National Alcohol Strategy - Chile
54. Figure 6. Prevalence of Alcohol abuse* among consumers in the past month according to gender and age group, Chile. 2006.
* The rate of alcohol abuse was measured from the presence of at least one of five possible symptoms, according to the DSM IV.Source: Séptimo Estudio Nacional de Drogas en Población General de Chile, 2006, Consejo Nacional para el Control de Estupefacientes (CONACE). Available at: http://www.conace.cl/inicio/ 55. Frequencies, however, differ according to each region. Table 2 presents the data by region for the years 2004, 2006 and 2008. The highest global percentages (combining all years) were the regions of Magallanes, Valparaíso, Los Lagos, Atacama, and Tarapacá.
26 National Alcohol Strategy - Chile
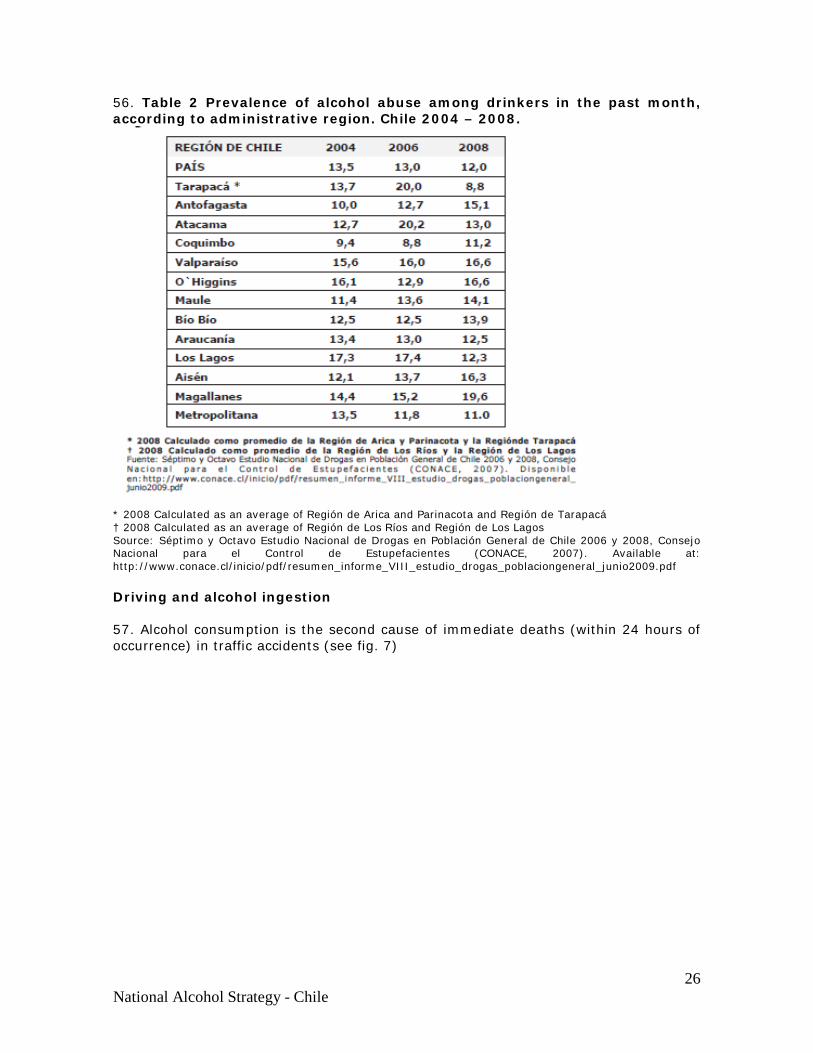
56. Table 2 Prevalence of alcohol abuse among drinkers in the past month, according to administrative region. Chile 2004 – 2008.
* 2008 Calculated as an average of Región de Arica and Parinacota and Región de Tarapacá † 2008 Calculated as an average of Región de Los Ríos and Región de Los Lagos Source: Séptimo y Octavo Estudio Nacional de Drogas en Población General de Chile 2006 y 2008, Consejo Nacional para el Control de Estupefacientes (CONACE, 2007). Available at: http://www.conace.cl/inicio/pdf/resumen_informe_VIII_estudio_drogas_poblaciongeneral_junio2009.pdf Driving and alcohol ingestion 57. Alcohol consumption is the second cause of immediate deaths (within 24 hours of occurrence) in traffic accidents (see fig. 7)
27 National Alcohol Strategy - Chile
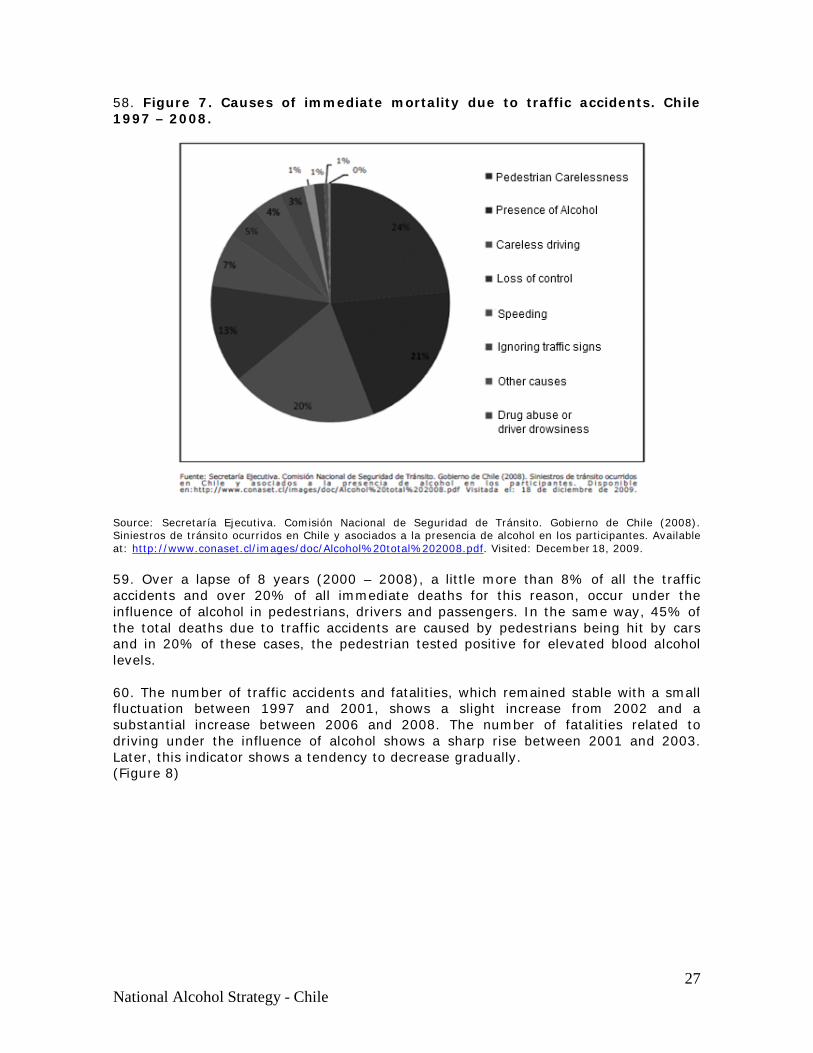
58. Figure 7. Causes of immediate mortality due to traffic accidents. Chile 1997 – 2008.
Source: Secretaría Ejecutiva. Comisión Nacional de Seguridad de Tránsito. Gobierno de Chile (2008). Siniestros de tránsito ocurridos en Chile y asociados a la presencia de alcohol en los participantes. Available at: http://www.conaset.cl/images/doc/Alcohol%20total%202008.pdf. Visited: December 18, 2009. 59. Over a lapse of 8 years (2000 – 2008), a little more than 8% of all the traffic accidents and over 20% of all immediate deaths for this reason, occur under the influence of alcohol in pedestrians, drivers and passengers. In the same way, 45% of the total deaths due to traffic accidents are caused by pedestrians being hit by cars and in 20% of these cases, the pedestrian tested positive for elevated blood alcohol levels. 60. The number of traffic accidents and fatalities, which remained stable with a small fluctuation between 1997 and 2001, shows a slight increase from 2002 and a substantial increase between 2006 and 2008. The number of fatalities related to driving under the influence of alcohol shows a sharp rise between 2001 and 2003. Later, this indicator shows a tendency to decrease gradually. (Figure 8)
28 National Alcohol Strategy - Chile
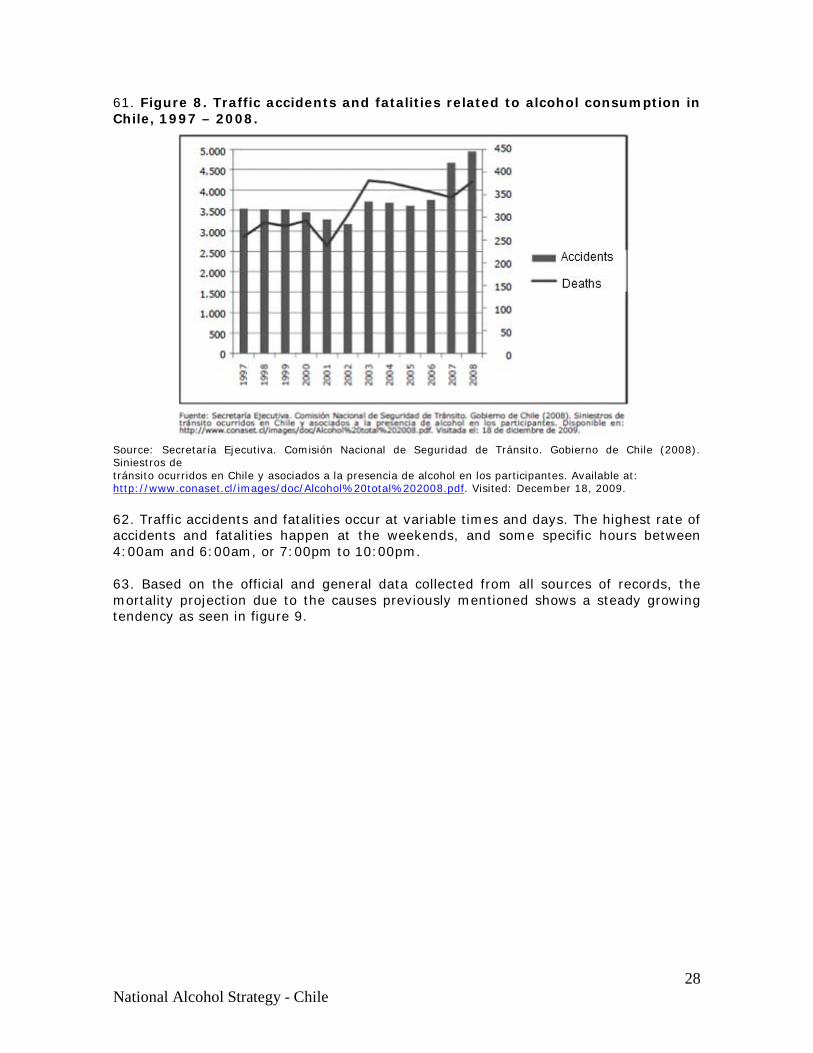
61. Figure 8. Traffic accidents and fatalities related to alcohol consumption in Chile, 1997 – 2008.
Source: Secretaría Ejecutiva. Comisión Nacional de Seguridad de Tránsito. Gobierno de Chile (2008). Siniestros de tránsito ocurridos en Chile y asociados a la presencia de alcohol en los participantes. Available at: http://www.conaset.cl/images/doc/Alcohol%20total%202008.pdf. Visited: December 18, 2009. 62. Traffic accidents and fatalities occur at variable times and days. The highest rate of accidents and fatalities happen at the weekends, and some specific hours between 4:00am and 6:00am, or 7:00pm to 10:00pm. 63. Based on the official and general data collected from all sources of records, the mortality projection due to the causes previously mentioned shows a steady growing tendency as seen in figure 9.
29 National Alcohol Strategy - Chile
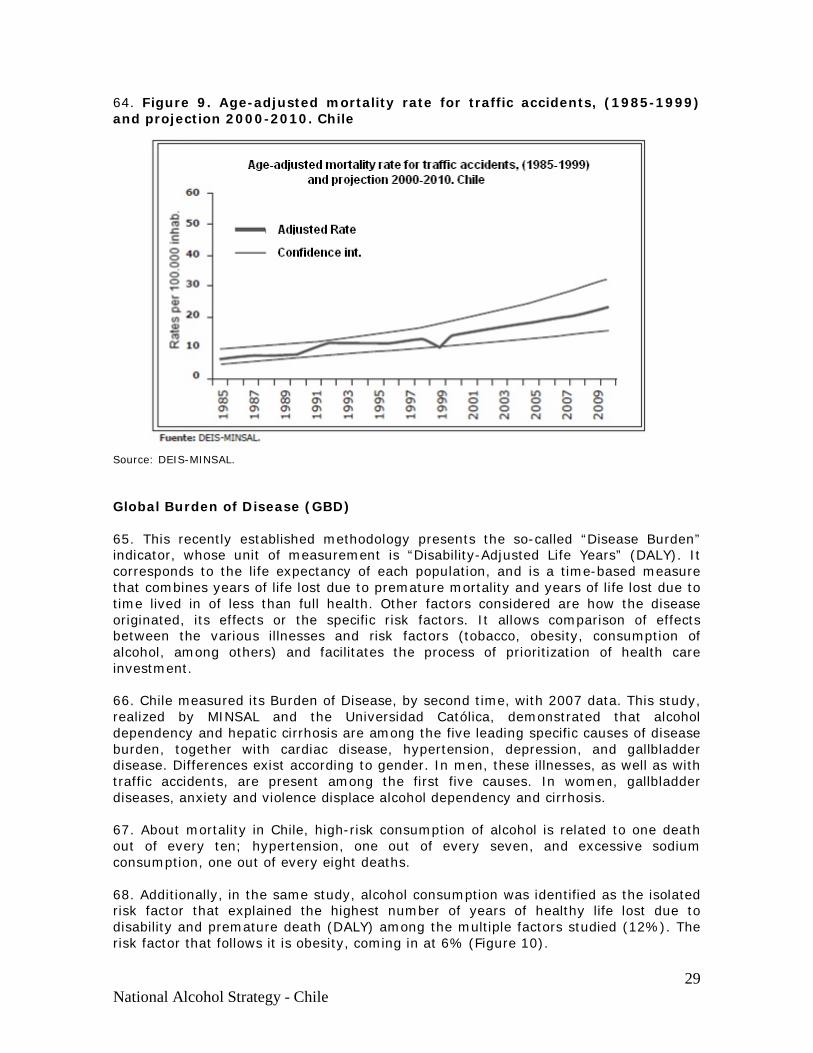
64. Figure 9. Age-adjusted mortality rate for traffic accidents, (1985-1999) and projection 2000-2010. Chile
Source: DEIS-MINSAL. Global Burden of Disease (GBD) 65. This recently established methodology presents the so-called “Disease Burden” indicator, whose unit of measurement is “Disability-Adjusted Life Years” (DALY). It corresponds to the life expectancy of each population, and is a time-based measure that combines years of life lost due to premature mortality and years of life lost due to time lived in of less than full health. Other factors considered are how the disease originated, its effects or the specific risk factors. It allows comparison of effects between the various illnesses and risk factors (tobacco, obesity, consumption of alcohol, among others) and facilitates the process of prioritization of health care investment. 66. Chile measured its Burden of Disease, by second time, with 2007 data. This study, realized by MINSAL and the Universidad Católica, demonstrated that alcohol dependency and hepatic cirrhosis are among the five leading specific causes of disease burden, together with cardiac disease, hypertension, depression, and gallbladder disease. Differences exist according to gender. In men, these illnesses, as well as with traffic accidents, are present among the first five causes. In women, gallbladder diseases, anxiety and violence displace alcohol dependency and cirrhosis. 67. About mortality in Chile, high-risk consumption of alcohol is related to one death out of every ten; hypertension, one out of every seven, and excessive sodium consumption, one out of every eight deaths. 68. Additionally, in the same study, alcohol consumption was identified as the isolated risk factor that explained the highest number of years of healthy life lost due to disability and premature death (DALY) among the multiple factors studied (12%). The risk factor that follows it is obesity, coming in at 6% (Figure 10).
30 National Alcohol Strategy - Chile
69. Figure 10. Percentage of AVISA attributed to Risk Factors 2007.
*The percentages cannot be added together since diseases related to risk factors in some cases are the same and there is coexistence and interaction between risk factors. Source: Informe final. Estudio de carga de enfermedad y carga atribuible, Chile 2007. Minsal. Available at: http://epi.minsal.cl/epi/html/invest/cargaenf2008/Informe%20final%20carga_Enf_2007.pdf 70. These data are consistent with those obtained by the GBD study that estimated alcohol-related DALYs for the year 2002 at 11.8% for the sub region of the American continent that includes Chile (AMR B), almost 10% for the Region of the Americas together, and 4.4% for all the world population. 71. The methodology of the GBD applied to risk factor studies, presupposes identification of diseases that are associated with a specific risk factor, such as alcohol consumption. This process is relatively standardized, but the causal attributes vary in accordance with the population being studied. 72. Table 3 provides a comparison of selective mortality statistics for the indexes in Chile, Canada, and the US. Hepatic cirrhosis in Chile is almost 3-fold and 4-fold higher than in the United State or Canada, respectively.
31 National Alcohol Strategy - Chile
73. Table 3. Standardized Mortality Index (for each 100,000 people) according to injuries, chronic and acute illness (data available from latest years).
Injury or Chronic Illness Chile Canada USA Cirrhosis 20.49 5.24 7.47 Falls 0.83 3.08 6.78 Intentional Injury 10.26 12.09 20.21 Traffic Accidents 10.69 8.45 15.00 Accidental Intoxications 0.27 2.73 0.58 Alcohol-related Illnesses 1.47 1.61 1.90 Throat and mouth cancer 1.35 2.06 2.00 Ischemic heart diseases 62.42 82.97 112.40
Source: FAO (Food and Agriculture Organization of the United Nations), World Drink Trends 2003). Quoted in: Department of Mental Health and Substance Abuse. World Health organization (2004). Global Status Report on Alcohol 2004. Singapore: OMS. Available at: http://www.who.int/globalatlas/default.asp 74. In the Chilean study, alcohol was found to relate to: mouth and oropharyngeal cancer, stomach cancer, liver cancer, breast cancer, diabetes, epilepsy, hypertension, brain disease, hepatic cirrhosis, disorders associated with alcohol, ischemia, injuries and violence. Other associations (other types of cancer, depression, other heart diseases and social consequences) were not considered in order to maintain comparability with international studies. In these studies, social-related damages that could be thought as illnesses have not yet been taken into consideration. 75. In the Region of the Americas, several studies deliver relevant information.
a) In the Americas, without precluding subregional variations, the adjusted average consumption rate per capita is 8.7 liters of pure alcohol per person, which is considerably higher than the world average of 6.2 liters of alcohol per person.1
b) Adults show a hazardous alcohol consumption pattern in the majority of countries in America.7
c) There are high rates of excessive alcohol consumption over short periods of time (excessive episodic consumption, or “binge drinking”) among youth.8
d) Between 20% and 50% of traffic accident fatalities in the Region are related to alcohol consumption.9
e) It is estimated that 50% of alcohol-related deaths in the year 2002 were caused by intentional and unintentional injuries.5 f) This Region has higher rates of alcohol-related disorders than any other region of the world.10 g) It is estimated that in the year 2002, 5.4% of all the deaths can be attributed to alcohol in comparison with a 3.7% at world level.5
i) More than 60 illnesses and health disorders are related to alcohol consumption.¹ j) Alcohol is associated with almost 10% of disability adjusted life years (DALY) in the region, in the year 2002, compared to the 4.4% world figure.5
k) A comparative analysis on the impact of 26 risk factors on the burden of disease in 2000, published by the WHO, shows that in the Americas, the main risk factor was found to be alcohol, while at world level, alcohol was ranked fourth place.1
32 National Alcohol Strategy - Chile
b. Because there is a concern and desire to achieve higher levels of public safety.
76. During recent years, criminal acts of violence have been profusely covered by the media and this information exposed to the scrutiny of public opinion. On several occasions, delinquency has been presented as the second most important national problem.11
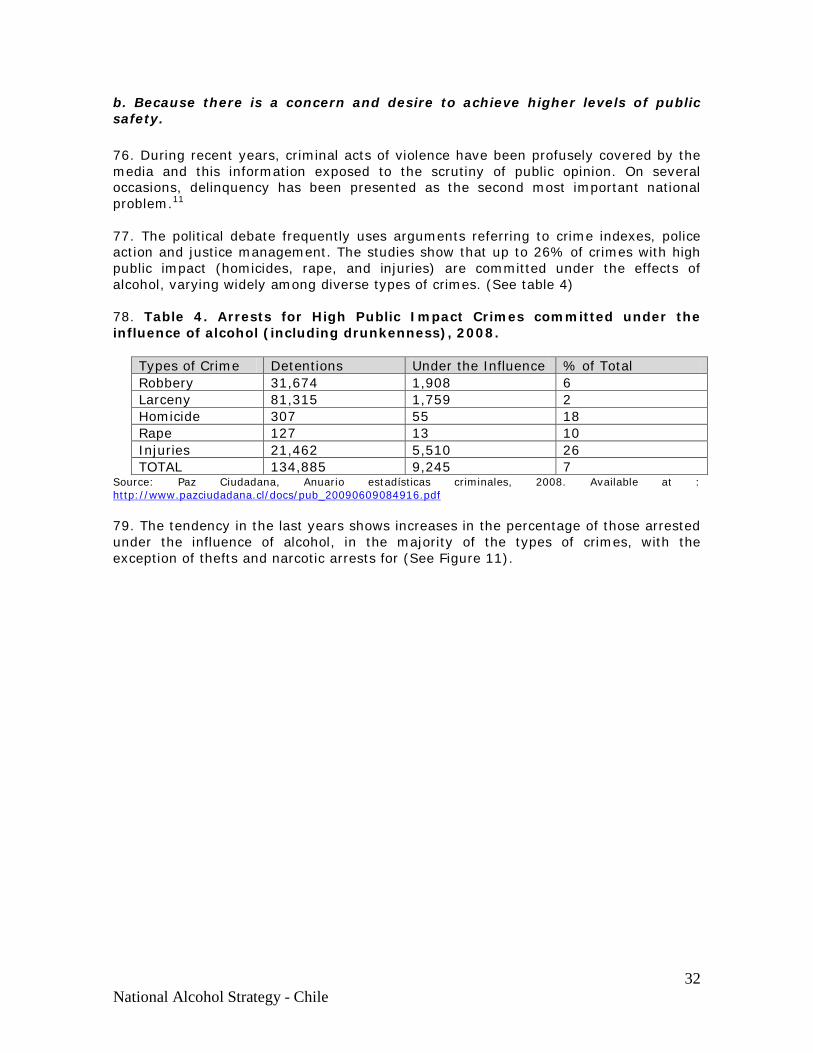
77. The political debate frequently uses arguments referring to crime indexes, police action and justice management. The studies show that up to 26% of crimes with high public impact (homicides, rape, and injuries) are committed under the effects of alcohol, varying widely among diverse types of crimes. (See table 4) 78. Table 4. Arrests for High Public Impact Crimes committed under the influence of alcohol (including drunkenness), 2008.
Types of Crime Detentions Under the Influence % of Total Robbery 31,674 1,908 6 Larceny 81,315 1,759 2 Homicide 307 55 18 Rape 127 13 10 Injuries 21,462 5,510 26 TOTAL 134,885 9,245 7
Source: Paz Ciudadana, Anuario estadísticas criminales, 2008. Available at : http://www.pazciudadana.cl/docs/pub_20090609084916.pdf 79. The tendency in the last years shows increases in the percentage of those arrested under the influence of alcohol, in the majority of the types of crimes, with the exception of thefts and narcotic arrests for (See Figure 11).
33 National Alcohol Strategy - Chile
80. Figure 11. Evolution of percentage of apprehensions under the influence of alcohol according to the types of crime.
Source: Own elaboration based on Paz Ciudadana, Anuario estadísticas criminales, 2008. Available at: http://www.pazciudadana.cl/docs/pub_20090609084916.pdf 81. In addition, of the near 90,000 arrests that the Chilean Police carried out in 2007, specifically due to infractions to the Alcohol Act (Ley de Alcoholes), 50% were for public drunkenness and 25% for driving under the influence of alcohol or in a state of inebriation (over 1 gram of alcohol per thousand). (See Table 5) 82. Table 5. Arrests for infractions to the Alcohol Act (Ley de Alcoholes), 2007.
Types of Infractions Detentions % of Total Driving while under the influence of alcohol or in a state of inebriation
21.269 25
Alcohol consumption in public places 20.588 25 Inebriation 41.766 50 Others 122 0 TOTAL 83.715 100
Source: Paz Ciudadana, Anuario estadísticas criminales, 2008. Available at: http://www.pazciudadana.cl/docs/pub_20090609084916.pdf 83. In relation with infractions and felonies that occur in public spaces, there is evidence of their correlation with places where there is a high concentration of alcohol outlets and/or where groups get together to drink in public areas. Domestic violence though, does not follow this pattern.
34 National Alcohol Strategy - Chile
c. Because it seeks equitable development and social protection
84. Young people in Chile consider excessive alcohol and drug consumption as the main problem among youth, although when they are asked about it on a personal level, the problem is relegated to 10th place. 85. The impact of harmful alcohol consumption on generating poverty and/or its persistence seems evident, though the measurements have been somewhat indirect. A relevant national statistic is that even though higher income sectors consume more in volume than those of lower income (Figure 12), it is the latter that makes up, to a greater degree, the problems associated with alcohol consumption. (Figure 13) 86. Figure 12, Prevalence by percentage of alcohol consumers in the past month, according to socioeconomic status. Chile, 1994 – 2008.
Source: Octavo Estudio Nacional de Drogas en Población General de Chile, 2008, Consejo Nacional para el Control de Estupefacientes (CONACE). Available at: http://www.conace.cl/inicio/pdf/resumen_informe_VIII_estudio_drogas_poblaciongeneral_junio2009.pdf
35 National Alcohol Strategy - Chile
87. Figure 13. Rate (%) of problem alcohol drinkers according to income quintiles
Source: Encuesta Calidad Vida, Minsal, 2006. (Quality of Life Survey) 88. The social programs, in the field implementation, show considerable barriers of very complex nature, due to the presence of family members or communities affected by harmful alcohol consumption. 89. In Primary Health Care, the emotional burden that many patients endure, especially women, due to the presence of negligence and violence by family members affected by harmful alcohol use seriously interferes with the fulfillment, adherence to, and effectiveness of treatment. 90. A preventive measure is included among the activities of the program “Chile Crece Contigo” (“Chile Grows with You”): the detection of harmful alcohol consumption and the corresponding counseling, among woman of fertile age, especially if pregnant. Nevertheless, the presence of a pattern of alcohol abuse in other members of vulnerable families represents a barrier to the final goal pursued, which is the leveling of opportunities for children’s development.
d. Because its social and economic development is threatened by the costs of harmful use of alcohol.
91. In 2005, job creation in the wine industry, including associated industries (transportation, machinery, agricultural supplies, etc.) reached 85,000 workers, 70,000 of them permanent13. The revenues in regard to exports have doubled between 2003 and 2009, going from $678 to $1,383.1 millions of dollars, due to the fact that 65% of national wine production is exported.14
92. By the same token, the beer industry, only considering the largest of its conglomerates, which employs 4300 workers, generated incomes of $180,000 million pesos and a profit of nearly $50,000 million in 2005 currency. The annual production of 4,100 hectoliters was enough to cover the 31 liters of beer per capita consumed in Chile in the year 2005.

36 National Alcohol Strategy - Chile
93. A study on the economy of alcohol in Chile (1998) concluded that the costs and expenses that are caused by the patterns of consumption in the country amounted to four times the income that this same economic activity returned to the country. Indeed, the direct and indirect costs related to excessive alcohol consumption, in 1995 currency, amounted to US$2,969,000,000, equivalent to 3.4% of the GDP or US$209 per capita. This includes indirect costs (low worker productivity when they are problem drinkers, premature death and absenteeism), and direct costs (expenses in health, police, accidents, destruction of assets). The economic benefits, on their part, reached US $59.00 per capita (exports, employed workforce, taxes) (see Annex 2). In fifteen years time, the situation may have well changed, hence making an update to this information highly necessary. 94. The effects of harmful alcohol use in the workplace occur fundamentally in the decrease of secondary productivity; in accidents in workplaces (20 to 25% of these are related to alcohol consumption); with the ease of access to alcohol at workplaces; the requests for medical leave (3 times more probable among workers that are problem drinkers); disability pensions due to the consequences of traumas (5 times more frequent); absenteeism (2 to 3 times more frequent). Recent alcohol consumption reached 15.2% among male workers that suffered severe accidents. 95. In Canada 2002, the costs associated with illicit drug, alcohol and tobacco use measured in medical services expenses, law enforcement and workplace productivity losses amounted to US$8.2 billion in regard to illicit drugs, US$14.6 billion to alcohol, and US$17.0 billion to tobacco. In other words, these three substances together, added up to a total of US$39,8 billion. It should be noted that, although the expenses associated with alcohol are almost double those associated with illicit drugs, the investment in promotion, prevention, and treatment associated with alcohol does not reach the sixth part of the budget destined to similar purposes for illicit drugs.17
96. Tendency in alcohol consumption per capita. In the last 10 years, the records on per capita alcohol consumption among adults of 15 years of age or older have increased gradually. It must be emphasized that obtaining this data was a difficult task, often varying depending on the consulted source. This can be seen in Table 6. For the calculations, standard concentrations were used (11% wines, 40% liquors, and 5% beers), according to WHO methodological recommendations.18
97. Table 6. Estimated alcohol consumption in Chile, 1998 – 2007, in liters of pure ethanol per person of 15 years of age or older, according to several sources.
YEAR WHO FAO ODEPA 1998 - 6.66 7.23 1999 - 6.50 6.90 2000 6.25 6.68 6.45 2001 6.11 6.12 6.58 2002 6.08 6.52 5.74 2003 6.39 6.57 6.85 2004 6.46 - 7.15 2005 6.81 - 7.50
Sources: WHO. Americas Region of WHO and information provided by S. Popova, J. Rehm & M. Rylett. FAO. Own elaboration based on FAOSTAT. Consumption. Crops Primary Equivalent.
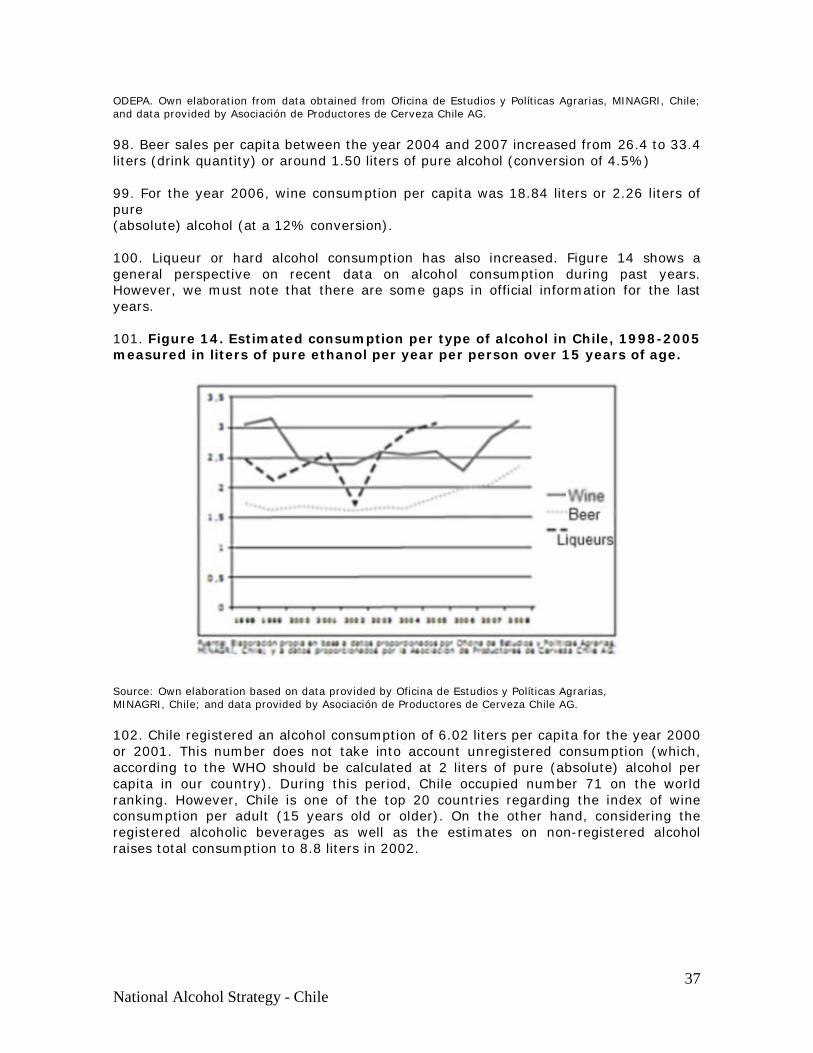
37 National Alcohol Strategy - Chile
ODEPA. Own elaboration from data obtained from Oficina de Estudios y Políticas Agrarias, MINAGRI, Chile; and data provided by Asociación de Productores de Cerveza Chile AG. 98. Beer sales per capita between the year 2004 and 2007 increased from 26.4 to 33.4 liters (drink quantity) or around 1.50 liters of pure alcohol (conversion of 4.5%) 99. For the year 2006, wine consumption per capita was 18.84 liters or 2.26 liters of pure (absolute) alcohol (at a 12% conversion). 100. Liqueur or hard alcohol consumption has also increased. Figure 14 shows a general perspective on recent data on alcohol consumption during past years. However, we must note that there are some gaps in official information for the last years. 101. Figure 14. Estimated consumption per type of alcohol in Chile, 1998-2005 measured in liters of pure ethanol per year per person over 15 years of age.
Source: Own elaboration based on data provided by Oficina de Estudios y Políticas Agrarias, MINAGRI, Chile; and data provided by Asociación de Productores de Cerveza Chile AG. 102. Chile registered an alcohol consumption of 6.02 liters per capita for the year 2000 or 2001. This number does not take into account unregistered consumption (which, according to the WHO should be calculated at 2 liters of pure (absolute) alcohol per capita in our country). During this period, Chile occupied number 71 on the world ranking. However, Chile is one of the top 20 countries regarding the index of wine consumption per adult (15 years old or older). On the other hand, considering the registered alcoholic beverages as well as the estimates on non-registered alcohol raises total consumption to 8.8 liters in 2002.
38 National Alcohol Strategy - Chile
IV.- WHAT MAKES IT POSSIBLE FOR A NATIONAL STRATEGY ON ALCOHOL TO BE EFFECTIVE?
103. Today it is possible to set up an effective public alcohol strategy due to the following factors:
a) The regulatory system for alcohol control and its practical application, although still weak, are well-headed and perfectible.
b) The accumulated evidence that measure the differential effectiveness of various public policies on alcohol, allow for decision-making with improved safety margins.
c) The lessons garnered from international experiences. d) The WHO initiative regarding a global strategy towards reducing
alcohol abuse provides a framework of goodwill and cooperation among nations and places the issue in the world development agenda.
a. The regulatory system for alcohol control and its practical application, although still weak, is well-oriented and also perfectible. 104. Over the last 30 years, the production, diversification, exportation and marketing of higher quality wines has increasingly dominated the economic and commercial policies related to alcohol in so much as to be assimilated as an important part of a collective national consciousness that takes pride in the image of Chile as an exporting nation. 105. Diverse measures have been taken to regulate internal consumption of alcoholic beverages. There are laws concerning the alcohol industry, retail sales to the public, regulations on minimum age, public spaces and drinking and driving. However, as we shall see, alcoholic beverages are still highly available to the population. 106. This will be the framework in which the National Strategy on Alcohol proposes new measures, modifications for current ones, as well as a starting point for new perspective on public policies.

39 National Alcohol Strategy - Chile
107. Summary of the main regulations and their problems in Chile is shown as follows (Table A) 108. Table A. Alcohol regulations in Chile. 2009 Area Regulations Comments Alcohol industry regulations
Act Nº 18.455 (1985) on production, development and marketing of ethyl alcohols, alcoholic beverages and others, aims to ensure legitimacy of alcohol related products, their quality and safety for human consumption. Moreover it seeks to oversee the distribution of alcohol related products and their availability to end-consumers. Decree-Act No. 1606 includes changes made to Act No. 19716, which modified tax rates affecting alcoholic beverages in accordance to WHO norms.
These regulatory measures are compromised by obligations assumed by Chile on international trade agreements (Ex. The European Community protests on tax rates applied to whisky in Chile). Consequently, some alcohol taxes have been reduced. This scenario must be taken into account when designing a new price policy on alcohol-related products
Sales, Retail Sales and Alcohol Consumption
Act No. 19.925 on selling and alcohol consumption (2004) prohibits drinking in public spaces; establishes the minimum age for selling alcohol at 18; prohibits selling or serving alcohol to minors in bars, restaurants and similar; and prohibits selling alcohol to any person in an obvious state of intoxication. The Act restricts the number and density of alcohol points of sale by legally establishing a proportion of licenses in respect to population (1 per 600)*
Supervision of this Act is very limited and tends to lean on low-income young adults (weekend controls).
. Alcohol selling is allowed seven days a week and sale hours depend on POS.
Drunkenness in public spaces is punished only when repeated. Medical treatment may be indicated, but so far it is seldom applied. There is no explicit prohibition of alcohol intake for minors less than 18 years of age. (They can consume if in presence of their parents). Restrictions on number and density do not include restaurants, hotels and other such businesses, where the sale of alcohol is permitted on the premises. There are also a large number of POS per capita with no restrictions on opening days.
* Comparatively speaking, these constitute moderate restrictions on outlet density. For example,
Ontario, with a population of around 14 million, has approximately 1300 off-license Points of Sale of alcoholic beverages, equivalent to 1 POS for every 10,769 people. Furthermore, Ontario has near to 19,000 establishments with licenses to sell alcohol (pubs, restaurants or clubs) or selling and consumption on the premises. In Ontario, the combined density of off and on-license Points of Sale is around 1 POS per 736 inhabitants.
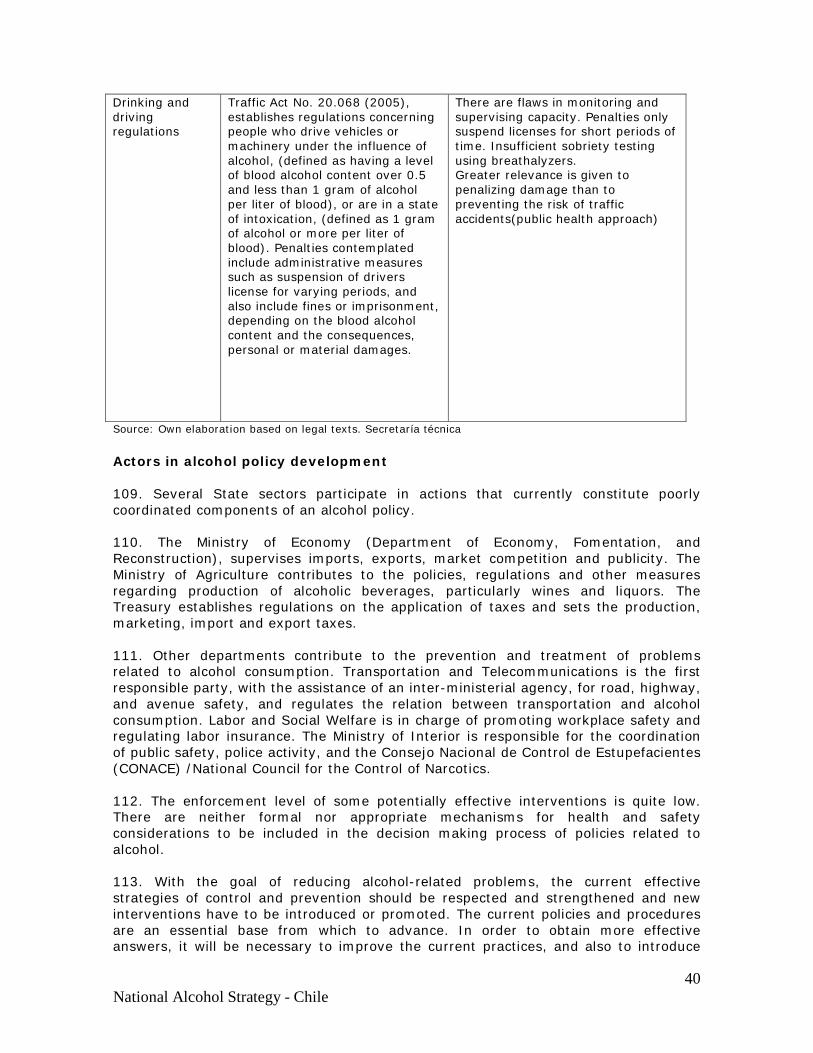
40 National Alcohol Strategy - Chile
Drinking and driving regulations
Traffic Act No. 20.068 (2005), establishes regulations concerning people who drive vehicles or machinery under the influence of alcohol, (defined as having a level of blood alcohol content over 0.5 and less than 1 gram of alcohol per liter of blood), or are in a state of intoxication, (defined as 1 gram of alcohol or more per liter of blood). Penalties contemplated include administrative measures such as suspension of drivers license for varying periods, and also include fines or imprisonment, depending on the blood alcohol content and the consequences, personal or material damages.
There are flaws in monitoring and supervising capacity. Penalties only suspend licenses for short periods of time. Insufficient sobriety testing using breathalyzers. Greater relevance is given to penalizing damage than to preventing the risk of traffic accidents(public health approach)
Source: Own elaboration based on legal texts. Secretaría técnica
Actors in alcohol policy development 109. Several State sectors participate in actions that currently constitute poorly coordinated components of an alcohol policy. 110. The Ministry of Economy (Department of Economy, Fomentation, and Reconstruction), supervises imports, exports, market competition and publicity. The Ministry of Agriculture contributes to the policies, regulations and other measures regarding production of alcoholic beverages, particularly wines and liquors. The Treasury establishes regulations on the application of taxes and sets the production, marketing, import and export taxes. 111. Other departments contribute to the prevention and treatment of problems related to alcohol consumption. Transportation and Telecommunications is the first responsible party, with the assistance of an inter-ministerial agency, for road, highway, and avenue safety, and regulates the relation between transportation and alcohol consumption. Labor and Social Welfare is in charge of promoting workplace safety and regulating labor insurance. The Ministry of Interior is responsible for the coordination of public safety, police activity, and the Consejo Nacional de Control de Estupefacientes (CONACE) /National Council for the Control of Narcotics. 112. The enforcement level of some potentially effective interventions is quite low. There are neither formal nor appropriate mechanisms for health and safety considerations to be included in the decision making process of policies related to alcohol. 113. With the goal of reducing alcohol-related problems, the current effective strategies of control and prevention should be respected and strengthened and new interventions have to be introduced or promoted. The current policies and procedures are an essential base from which to advance. In order to obtain more effective answers, it will be necessary to improve the current practices, and also to introduce
41 National Alcohol Strategy - Chile
and implement new methods and prevention strategies. This will bring benefits to the general population as well as to individuals that show high levels of harm due to alcohol consumption.
b. Accumulated evidence that measure the differential effectiveness of various public policies on alcohol.
114. In the last 15 years a notable effort has been made to compile and carry out solid scientific studies that allow identification and appraisal of those strategies effective in reducing alcohol consumption, hazardous drinking and related harms.20
115. An outstanding example is the study carried out by Babor and a group of sixteen researchers in 200320, together with the WHO. They analyzed thirty-four prevention strategies, applied in various areas and moments, in relation to their effectiveness in determining objectifiable changes (decrease in general consumption or in harmful consumption, reduction of accidents, or crimes, among others. Thus, they evaluated the solidity and breadth of the sustaining research, the intercultural applicability and costs of implementation. They enumerated ten principal strategies by cost effectiveness, classified in seven fields: physical availability, taxes and prices, alteration of alcohol consumption context, education and persuasion, alcohol promotion, countermeasures to drinking and driving, and early treatment and interventions. 116. The strategies are directed to modify some determinants of context (context factors), certain targeted behaviors, or the consequences of harmful alcohol consumption, as one sees in the following: CONTEXT FACTORS OR DETERMINANTS
ECONOMIC AVAILABILITY
a) Pricing and Taxation*
PHYSICAL AVAILABILITY:
b) Regulating availability: total or partial sales prohibitions, government monopoly on off-premise sales*, alcohol licenses for on-premise sales, restrictions on days and hours of sale*, identifying and locating points of sale and density of retail outlets
c) Limiting requirements for buying and selling alcohol: rationing, minimum
legal purchase age* and legal responsibility of those who sell or serve alcohol
d) Regulating beverage availability according to alcohol content
DRINKING CONTEXT
e) Promotion of alcohol-free activities and events
42 National Alcohol Strategy - Chile
f) Training for personnel that serve and/or sell alcoholic beverages to promote responsible drinking and plans of practices to prevent intoxication and underage drinking
g) Application of alcohol rationing practices and potential legal liability h) Adoption of Voluntary Codes of Practice in retail sales
i) Personnel training programs for the prevention and management of
aggression and other behavior problems
j) Community mobilization k) Regulation of alcohol promotion: industry self-regulation as to alcohol
advertising standards; governmental prohibitions and controls on advertising for: types of beverages, types of media, advertising times and hours, contents and sponsors
TARGET BEHAVIOURS
l) Countermeasures for drinking and driving: lowering BAC (blood alcohol
concentration) limits*, zero tolerance blood alcohol testing for young drivers*, sobriety checkpoints*, random breath testing*, administrative license suspension*, treatments to prevent recidivism, engine startup blocking devices, graduated licensing for novice drivers*, designated driver program services to prevent driving while under the influence
REDUCING CONSEQUENCES
m) Education and persuasion strategies: public service announcements and
counter advertising, warning labels, guidelines on low-risk alcohol consumption*, continuous programs in schools, universities and other higher education institutions.
n) Treatment and early intervention: brief interventions with high-risk
drinkers*, specialized treatment for alcohol related problems, attendance to self-help groups and group therapy, and mandatory treatment for reoffending drivers
117. The strategies marked with asterisks (*) above, are considered the most effective. (See Annex 3 for a summarized list of evidences on the effectiveness of a series of policies and interventions). 118. In Avoidable Costs of Alcohol Abuse in Canada 2002 by Rehm et al.23, researchers calculated the avoidable costs of alcohol in correlation to seven of the interventions highlighted by Babor et al (2003). The methodology included the use of criteria from Collins et al.24, which were based upon the results of the proven effective major interventions. The impact was calculated based in reference to costs obtained from Second Canadian Study of Social Costs Attributable to Substance Abuse (Rehm et al, 2006) where six interventions were used with proven effectiveness in reducing harm. In addition, this study analyzed the effects of an important political change that was debated in Canada in that very year – a transition from a government monopoly on alcohol retail sales to privatization. The avoidable costs were estimated in terms of
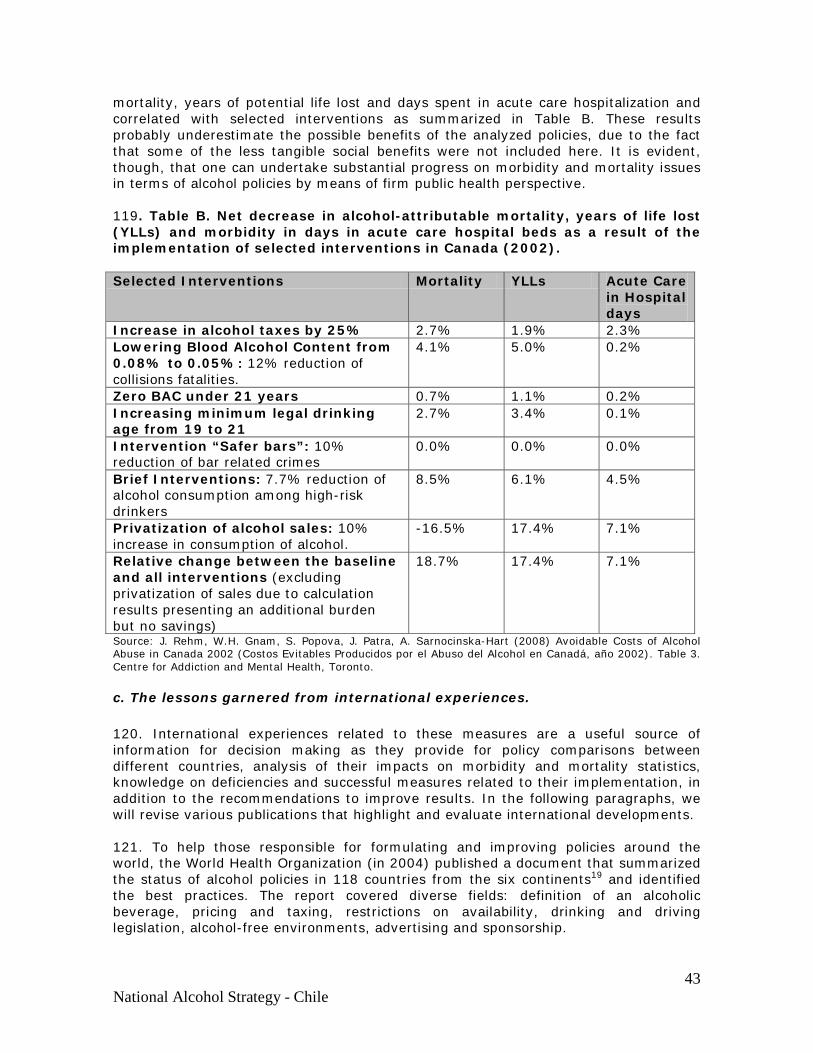
43 National Alcohol Strategy - Chile
mortality, years of potential life lost and days spent in acute care hospitalization and correlated with selected interventions as summarized in Table B. These results probably underestimate the possible benefits of the analyzed policies, due to the fact that some of the less tangible social benefits were not included here. It is evident, though, that one can undertake substantial progress on morbidity and mortality issues in terms of alcohol policies by means of firm public health perspective. 119. Table B. Net decrease in alcohol-attributable mortality, years of life lost (YLLs) and morbidity in days in acute care hospital beds as a result of the implementation of selected interventions in Canada (2002). Selected Interventions Mortality YLLs Acute Care
in Hospital days
Increase in alcohol taxes by 25% 2.7% 1.9% 2.3% Lowering Blood Alcohol Content from 0.08% to 0.05%: 12% reduction of collisions fatalities.
4.1% 5.0% 0.2%
Zero BAC under 21 years 0.7% 1.1% 0.2% Increasing minimum legal drinking age from 19 to 21
2.7% 3.4% 0.1%
Intervention “Safer bars”: 10% reduction of bar related crimes
0.0% 0.0% 0.0%
Brief Interventions: 7.7% reduction of alcohol consumption among high-risk drinkers
8.5% 6.1% 4.5%
Privatization of alcohol sales: 10% increase in consumption of alcohol.
-16.5% 17.4% 7.1%
Relative change between the baseline and all interventions (excluding privatization of sales due to calculation results presenting an additional burden but no savings)
18.7% 17.4% 7.1%
Source: J. Rehm, W.H. Gnam, S. Popova, J. Patra, A. Sarnocinska-Hart (2008) Avoidable Costs of Alcohol Abuse in Canada 2002 (Costos Evitables Producidos por el Abuso del Alcohol en Canadá, año 2002). Table 3. Centre for Addiction and Mental Health, Toronto.
c. The lessons garnered from international experiences. 120. International experiences related to these measures are a useful source of information for decision making as they provide for policy comparisons between different countries, analysis of their impacts on morbidity and mortality statistics, knowledge on deficiencies and successful measures related to their implementation, in addition to the recommendations to improve results. In the following paragraphs, we will revise various publications that highlight and evaluate international developments. 121. To help those responsible for formulating and improving policies around the world, the World Health Organization (in 2004) published a document that summarized the status of alcohol policies in 118 countries from the six continents19 and identified the best practices. The report covered diverse fields: definition of an alcoholic beverage, pricing and taxing, restrictions on availability, drinking and driving legislation, alcohol-free environments, advertising and sponsorship.
44 National Alcohol Strategy - Chile
122. Based on the number of measures considered in the alcohol policy survey, the WHO concluded that few countries had truly comprehensive policies. There were some countries that did not register any of the measures included and most fell somewhere between these opposite realities. In order to strengthen policy effectiveness, the WHO report highlighted the importance of enforcing current policies and promoting collaborative efforts between institutions and organizations at the local and regional levels. Finally, the report suggests that, depending on context, each country can design and implement a policy that includes a blend of some or all of the following proven measures: establishment of a sufficiently low alcohol content in the definition of an alcoholic beverage to include the majority of alcoholic beverages consumed in the country; government control over retail sales; effective enforcement of minimum age purchasing limit and blood alcohol content levels while driving; restriction of sales according to time and place; promotion of lower or non-alcoholic beverages by reducing prices in relation to alcoholic beverages; higher taxes; regulation of time, place and media for advertising and alcohol sponsorship; restriction of alcohol consumption in public places; treatment and early intervention of those affected. 123. Another recent WHO document25 describes in general terms, ten proposed policy options or target areas: raising awareness and political commitment; health sector response; community action, drinking and driving policies and prevention; pricing policies; availability of alcoholic beverages; marketing of alcoholic beverages; harm reduction; and reducing the public health impact of illegal and informal alcohol; monitoring and surveillance. 124. A recent comparative analysis between policies directed towards influencing harmful alcohol consumption, in terms of economic costs, and its effects on preventing burden of disease26 concluded that taxation is the most cost-effective strategy while random alcohol breath tests and brief advice or counseling in primary health care, are the effective interventions with the highest relative cost. The main conclusions established that in regions with high levels of harmful alcohol use, a brief advice by a physician and taxation can have notable impact on the health of the population; and in regions where high-risk drinking behavior represents less of a burden to public health, restrictions on supplies or on the promotion of alcoholic beverages seem to be useful. In both situations, governments should embrace an important role in promoting risk reducing strategies 125. In Comparative Analysis of Alcohol Control Policies in 30 Countries (Brand et al. 2007) the authors developed an Alcohol Policy Index to estimate strength of alcohol policies (ranges between 0 and 100 points) and established a relation between policy score and alcohol consumption per capita. In those countries, the 16 chosen policies were grouped together in five regulatory domains20: physical availability of alcohol, alcohol consumption context, pricing, alcohol advertising, and the driving of motorized vehicles. 126. The median score was 42.4%. The scores registered a wide variation, from 14.5% in Luxembourg to 67.3% in Norway. Regarding availability, Iceland and the US obtained higher scores of 24 and 23, respectively, of a possible 32. In relation to alcohol consumption, Norway, Poland, Iceland, Finland, Ireland, Holland and Switzerland obtained the highest score (8), meanwhile Poland, Slovakia, and Mexico obtained high scores in the pricing area. Norway, Poland, Sweden, Finland, Turkey, Spain, Italy and Germany obtained highest scores in advertising, and finally, in the field of operating motorized vehicles, Norway (28), Sweden (28) and Poland (25) were the leaders (of 34 possible points). Consequently, the ten countries that lead the
45 National Alcohol Strategy - Chile
ranking are: Norway, Poland, Iceland, Sweden, Australia, Finland, Slovakia, Canada and Hungary. 127. The authors also discovered a relatively strong negative correlation between alcohol consumption and the score obtained on the Alcohol Policy Index; a 10-point increase in the score was associated with a decrease in absolute alcohol consumption of one liter per capita per year. In other words, a higher score in the application of alcohol policies is linked to a lower consumption per capita. 128. In summary, although there are few studies that analyze the cost-effectiveness of alcohol policies in the international context and with a cost-effective plan, there are some common conclusions. Some strategies have demonstrated being more cost-effective than others, such as the application of pricing and taxation, the regulation of physical availability, measures preventing driving and drinking and early interventions in health problems. These strategies also have a positive impact on consumption levels per capita, on high-risk alcohol consumption, and alcohol-related harms. The authorities and communities, at the local and regional level have to choose and implement a viable mixture of these measures, constantly monitoring and watching over its progress in accomplishing goals, in order to reach the objectives of health promotion, prevention and the reduction of the consequences related to alcohol consumption.28
129. In Annex 4, we can see summaries of the experiences in Canada (British Columbia, and Nova Scotia), Spain, Australia, New Zeland, and England.
d. The WHO initiative and activities of its regional offices
131. The World Health Report 2002 highlights that, worldwide, 4% of morbidity (DALYs) and 3.2% of mortality rates are attributable to alcohol abuse and represents the principal health risk factor for developing countries with low levels of mortality and the third, in developed countries”. The report recognizes that habits, context and general alcohol consumption level influence the health of the entire population and that harmful consumption habits are among the principal causes of illness, injuries, violence (especially domestic violence against women and children), disability, social problems and premature deaths. Alcohol abuse is also related to mental health problems, has serious repercussions on human welfare, affecting families, communities, and society as a whole and contributes to social and health inequalities. The report additionally emphasizes the risk of harmful effects related to alcohol consumption, particularly in the context of driving motor vehicles, in the workplace, and during pregnancy. 132. In 2004, the WHO retook its role in the field of world health and alcohol consumption, initiating a gradual construction process of a world strategy to reduce harmful alcohol use. Through successive consultations, documents and Resolutions, the moment has arrived for the proposal to be considered and voted on in the World Health Assembly of 2010. In Annex 5 (only available in Spanish), there is a summary of the WHO initiative and the charter of Rights of the WHO European Region.
46 National Alcohol Strategy - Chile
V. – DEFINITIONS, RIGHTS, DETERMINANTS, AND MODELS OF INTERVENTION
a. Basic Definitions
133. Policies refer to government authority decisions taken after going through a process that brings together diverse opinions and influences and are put into action through laws, norms and regulations. 134. The main purpose of an alcohol policy is to prevent, reduce or treat the negative social and health related consequences of harmful alcohol consumption. It includes measures and strategies aimed at the general population, specific organizations as well as individuals, serving the interests of public health and welfare20. Alcohol policies are the most effective manner of stimulating individual and cultural changes regarding alcohol consumption and behavior29. 135. There are, however other policies that can stimulate hazardous alcohol consumption, increase the associated harms and generate higher social and economic costs. For example, policies that drive prices lower than advisable, policies that permit price wars of alcoholic beverages or those that increase the number of alcohol outlet licenses. 136. The Alcohol Strategy refers to a proposal for State action that is systematic, interconnected and collaborative for reducing harm related to alcohol consumption at the general population, community, and individual levels. 137. Alcohol policies typically set out to strike a balance between the rights and responsibilities of the individuals, of the society as a whole, and the interests and benefits of specific sectors such as those that deal with government income, public safety programs, production and commerce; all of which are encompassed in the global context of shared social responsibility. 138. The success and reach of these policies are influenced by the commitments and constant participation of diverse sectors of society, including government, private and public institutions as well as the general public. 139. The formulation of alcohol policies should be goal-oriented, community-based, well designed, and must be willing to tackle the myriad of associated risks. This includes strategies to: improve health standards, and prevent problems associated with alcohol consumption in the general population; prevention programs aimed at specific risk groups; detection and early intervention among hazardous and excessive alcohol consumers; and individualized treatment and rehabilitation.30
b. Rights
140. The National Alcohol Strategy responds to the people’s rights, with the idea that the institutions, national community and citizens promote and protect these rights, specifically: a) Children, youth, and adults have the right to grow up and live in safety and
protection with respect to the risks and harm that they may suffer due to third party alcohol consumption or the illnesses related to it, in the areas of family, work,
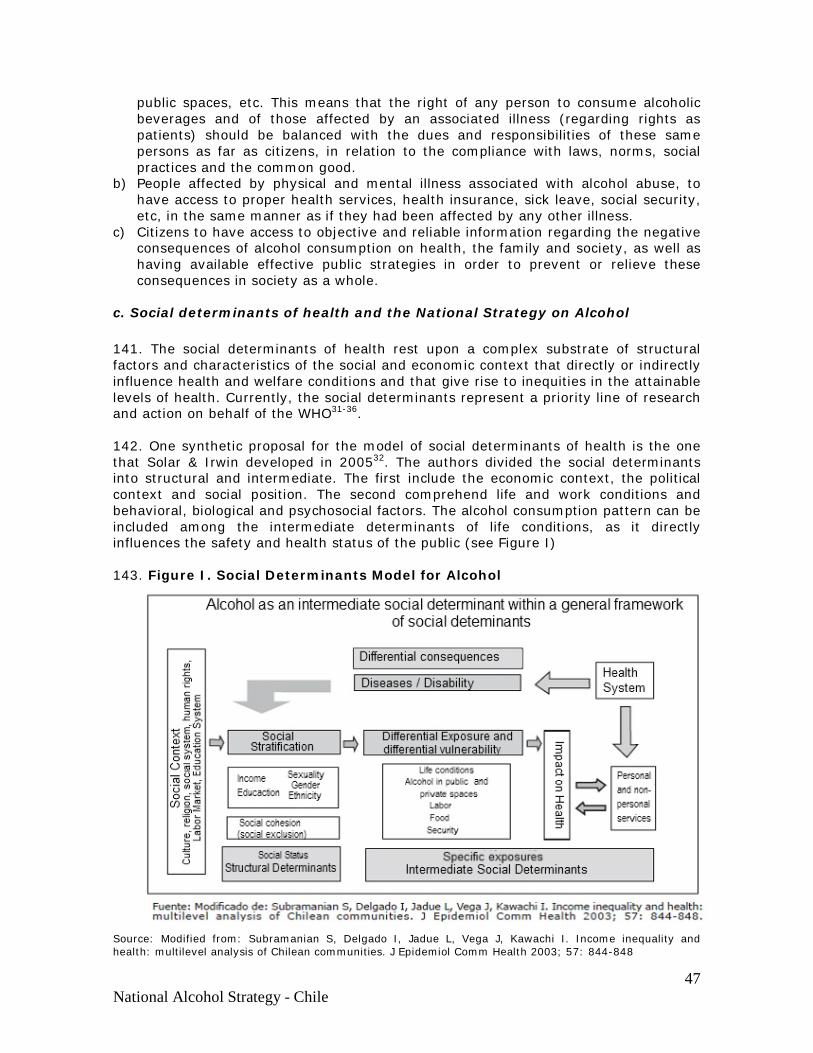
47 National Alcohol Strategy - Chile
public spaces, etc. This means that the right of any person to consume alcoholic beverages and of those affected by an associated illness (regarding rights as patients) should be balanced with the dues and responsibilities of these same persons as far as citizens, in relation to the compliance with laws, norms, social practices and the common good.
b) People affected by physical and mental illness associated with alcohol abuse, to have access to proper health services, health insurance, sick leave, social security, etc, in the same manner as if they had been affected by any other illness.
c) Citizens to have access to objective and reliable information regarding the negative consequences of alcohol consumption on health, the family and society, as well as having available effective public strategies in order to prevent or relieve these consequences in society as a whole.
c. Social determinants of health and the National Strategy on Alcohol 141. The social determinants of health rest upon a complex substrate of structural factors and characteristics of the social and economic context that directly or indirectly influence health and welfare conditions and that give rise to inequities in the attainable levels of health. Currently, the social determinants represent a priority line of research and action on behalf of the WHO31-36. 142. One synthetic proposal for the model of social determinants of health is the one that Solar & Irwin developed in 200532. The authors divided the social determinants into structural and intermediate. The first include the economic context, the political context and social position. The second comprehend life and work conditions and behavioral, biological and psychosocial factors. The alcohol consumption pattern can be included among the intermediate determinants of life conditions, as it directly influences the safety and health status of the public (see Figure I) 143. Figure I. Social Determinants Model for Alcohol
Source: Modified from: Subramanian S, Delgado I, Jadue L, Vega J, Kawachi I. Income inequality and health: multilevel analysis of Chilean communities. J Epidemiol Comm Health 2003; 57: 844-848
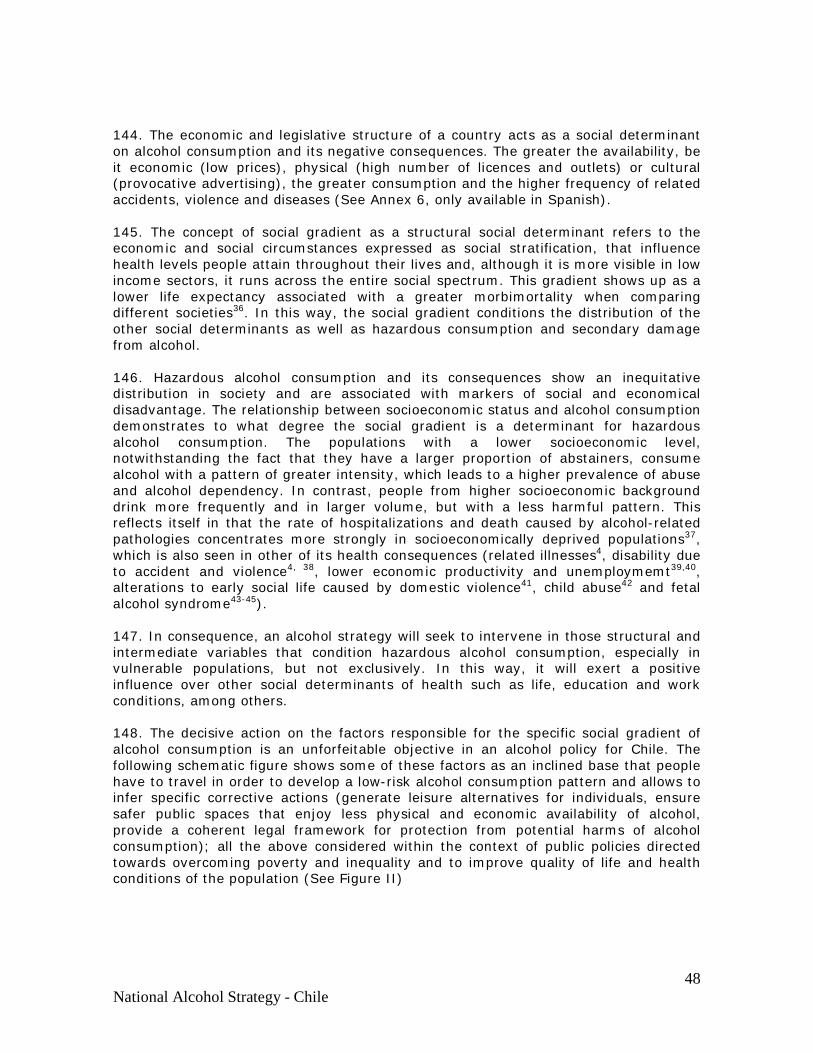
48 National Alcohol Strategy - Chile
144. The economic and legislative structure of a country acts as a social determinant on alcohol consumption and its negative consequences. The greater the availability, be it economic (low prices), physical (high number of licences and outlets) or cultural (provocative advertising), the greater consumption and the higher frequency of related accidents, violence and diseases (See Annex 6, only available in Spanish). 145. The concept of social gradient as a structural social determinant refers to the economic and social circumstances expressed as social stratification, that influence health levels people attain throughout their lives and, although it is more visible in low income sectors, it runs across the entire social spectrum. This gradient shows up as a lower life expectancy associated with a greater morbimortality when comparing different societies36. In this way, the social gradient conditions the distribution of the other social determinants as well as hazardous consumption and secondary damage from alcohol. 146. Hazardous alcohol consumption and its consequences show an inequitative distribution in society and are associated with markers of social and economical disadvantage. The relationship between socioeconomic status and alcohol consumption demonstrates to what degree the social gradient is a determinant for hazardous alcohol consumption. The populations with a lower socioeconomic level, notwithstanding the fact that they have a larger proportion of abstainers, consume alcohol with a pattern of greater intensity, which leads to a higher prevalence of abuse and alcohol dependency. In contrast, people from higher socioeconomic background drink more frequently and in larger volume, but with a less harmful pattern. This reflects itself in that the rate of hospitalizations and death caused by alcohol-related pathologies concentrates more strongly in socioeconomically deprived populations37, which is also seen in other of its health consequences (related illnesses4, disability due to accident and violence4, 38, lower economic productivity and unemploymemt39,40, alterations to early social life caused by domestic violence41, child abuse42 and fetal alcohol syndrome43-45). 147. In consequence, an alcohol strategy will seek to intervene in those structural and intermediate variables that condition hazardous alcohol consumption, especially in vulnerable populations, but not exclusively. In this way, it will exert a positive influence over other social determinants of health such as life, education and work conditions, among others. 148. The decisive action on the factors responsible for the specific social gradient of alcohol consumption is an unforfeitable objective in an alcohol policy for Chile. The following schematic figure shows some of these factors as an inclined base that people have to travel in order to develop a low-risk alcohol consumption pattern and allows to infer specific corrective actions (generate leisure alternatives for individuals, ensure safer public spaces that enjoy less physical and economic availability of alcohol, provide a coherent legal framework for protection from potential harms of alcohol consumption); all the above considered within the context of public policies directed towards overcoming poverty and inequality and to improve quality of life and health conditions of the population (See Figure II)
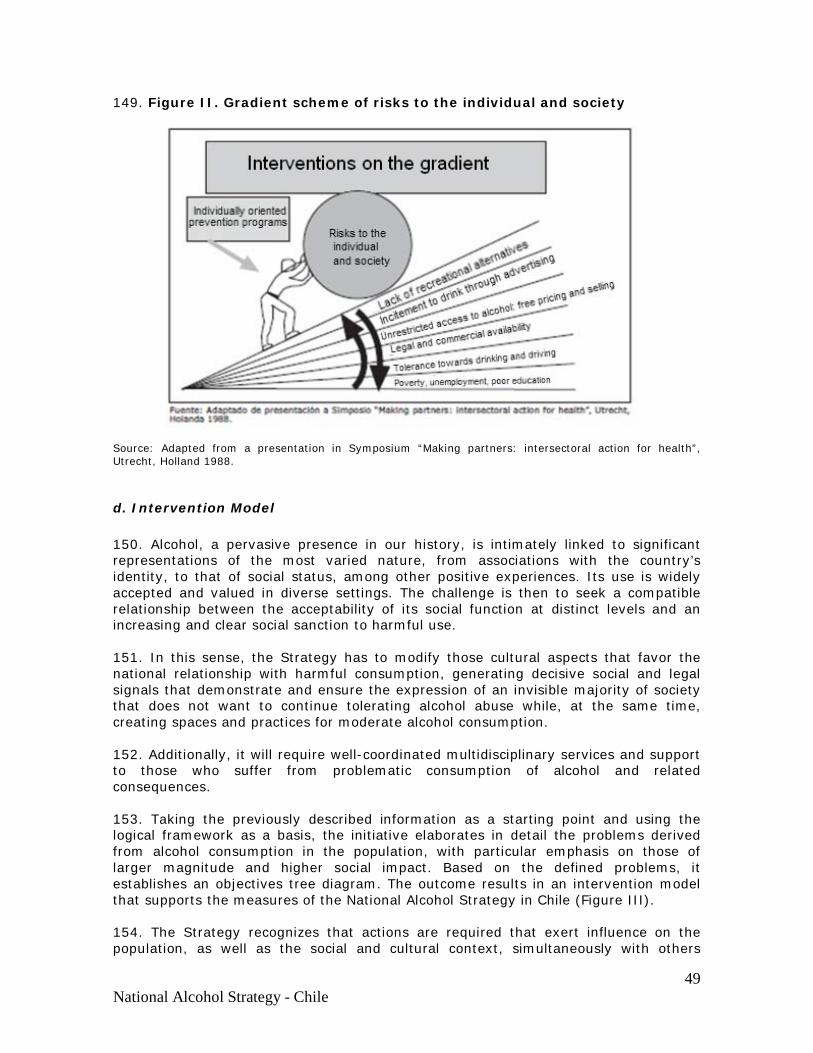
49 National Alcohol Strategy - Chile
149. Figure II. Gradient scheme of risks to the individual and society
Source: Adapted from a presentation in Symposium “Making partners: intersectoral action for health”, Utrecht, Holland 1988.
d. Intervention Model
150. Alcohol, a pervasive presence in our history, is intimately linked to significant representations of the most varied nature, from associations with the country’s identity, to that of social status, among other positive experiences. Its use is widely accepted and valued in diverse settings. The challenge is then to seek a compatible relationship between the acceptability of its social function at distinct levels and an increasing and clear social sanction to harmful use. 151. In this sense, the Strategy has to modify those cultural aspects that favor the national relationship with harmful consumption, generating decisive social and legal signals that demonstrate and ensure the expression of an invisible majority of society that does not want to continue tolerating alcohol abuse while, at the same time, creating spaces and practices for moderate alcohol consumption. 152. Additionally, it will require well-coordinated multidisciplinary services and support to those who suffer from problematic consumption of alcohol and related consequences. 153. Taking the previously described information as a starting point and using the logical framework as a basis, the initiative elaborates in detail the problems derived from alcohol consumption in the population, with particular emphasis on those of larger magnitude and higher social impact. Based on the defined problems, it establishes an objectives tree diagram. The outcome results in an intervention model that supports the measures of the National Alcohol Strategy in Chile (Figure III). 154. The Strategy recognizes that actions are required that exert influence on the population, as well as the social and cultural context, simultaneously with others
50 National Alcohol Strategy - Chile
focused on vulnerable groups. All of these constitute priorities for the National Strategy. 155. The priority groups proposed by the Strategy are the following:
a) Adolescents and youth are the most vulnerable populations facing alcohol abuse. As mentioned earlier, youth populations present a greater risk of problematic alcohol consumption the younger they start drinking. At the same time, advertising exercises a more powerful effect on this group regarding initiation. Whatever harm at this age, in particular those associated to violence and accidents, can decisively impact later adolescent development and as well as that of the family.
b) The pregnant woman and unborn child. Alcohol consumption on the part of the
pregnant mother has proven to have damaging effects in the short and/or long term, without it being possible to establish a safe level of consumption.
156. Also, there will be a priority action focus by the National Alcohol Strategy on the negative consequences of harmful alcohol use that are no longer acceptable to the country and that are today, susceptible to modification. These are:
a) Early loss of lives and damages due to effects of alcohol-related traffic accidents. This problem carries with it a huge social repercussion: pain and suffering that many innocent people experience as victims of drinking and driving related accidents.
b) Burden and social cost associated with harmful alcohol consumption. There are two highly sensitive examples: domestic and criminal violence as well as absenteeism and workplace injuries.
c) Damages to health and mortality due to multiple causes. Alcohol consumption is the specific factor which most damage causes to population health expressed through years of life lost, and premature and avoidable deaths and disabilities
157. Based on the priorities highlighted above, we present an intervention model for the National Alcohol Strategy. The Lines of Action seek (first column) to influence specific targets (second column). The resulting effects will be expressed at different levels, on the consumption pattern and on related damages (columns 3 and 4). Any process of social and cultural change takes time and requires the application of multiple strategies in a synergetic and persistent manner. These efforts are rewarded with the gain of collective benefits (column 5). The expected final result is a safer, better developed and healthier Chile (see Figure III).
51 National Alcohol Strategy - Chile
158. Figure III. Intervention Model. National Strategy on Alcohol Source: Adapted from: Laurence Gruer. Reducing alcohol-related harm in Scotland. The evidence base and a logic model for action. Board Meeting: 16 may 2008. HS Paper 14/08. Secretaría Técnica.
52 National Alcohol Strategy - Chile
VI. LINES OF ACTION AND PROPOSAL FOR CONCRETE MEASURES
159. Below, we specify the Lines of Action proposed by the National Alcohol Strategy, in addition to the concrete measures required for each one. The background and evidence that support the proposal are found detailed in Annex 6 (only available in Spanish).
LINE OF ACTION № 1. PUBLIC INFORMATION AND ADVERTISING CONTROL.
160. The National Strategy on Alcohol proposes establishing and implementing a powerful continuous information mechanism directed to the general public as well as to specific groups, to increase the base of objective information for decisions and debates that arise from its own launching. This includes data about social, economic and health harms related to alcohol consumptions and also how to attenuate them. 161. The long term goal is to strengthen the cultural model that normalizes consumption behavior in a way that is not harmful or risky. Included is “non-use” or “abstinence”, which cancels out positive social representations of people under the influence of alcohol. This constitutes a social right to adequate protection from the risks and harm due to hazardous consumption by third parties. 162. The advertising and marketing techniques used in promotion of the alcoholic beverages have demonstrated to be effective in inducing young people to start drinking and in increasing consumption in those who have already started46. Concrete Measures Information for the public 163. Select and disseminate sufficient amount of information content to enable the general public, having such knowledge, to move from a passively tolerant attitude to that of self-protection, defending their rights face to face against the most serious issues that alcohol abuse causes to its surrounding environment. 163. Organize and execute an extensive plan of dissemination and promotion of the National Alcohol Strategy, demonstrating its importance as a mechanism to generate a protective environment against hazards associated with high-risk drinking behaviors. Of the multiple instruments available, the hosting of civic forums in specific regions of the country is one that has been considered for the first phase. Also, an interactive website is being contemplated to conduct seminars and forums of technical nature, supplying evidence and updates directed at decision making, surveys, and opinion studies, etc. 165. To establish a procedure in order to register, collect, and systematize the conclusions, propositions, and suggestions that are generated by various civic forums and thematic meetings throughout the country, initially organized by the Regional Secretary of Health (SEREMI de Salud), and other SEREMI officials that are involved in the construction process of the National Alcohol Strategy, and later on, by regional governments.
53 National Alcohol Strategy - Chile
166. Design, agree on, establish and finance a system, a plan, a milestone calendar and dissemination contents of the National Alcohol Strategy 167. Design, agree upon, establish and finance a procedure and plan that facilitates continual communication between the civil society and institutions towards the National Alcohol Strategy, and vice versa. Regulating Alcohol Marketing 168. To move an urgency motion on the bill that includes measures on warning labels for alcoholic beverage containers, advertising and sponsorship (though approved by the House of Representatives after two years of debate, the bill currently remains dormant in the Senate, where it has been for over one year). 169. The following are the bill’s legal dispositions sanctioned until now:
a) Labeling: Labels and containers must state the following message: “Warning: Drinking in excess causes health injuries and can be harmful to third parties”.
Furthermore, at least one of the following sentences should be added at the choice of producer or manufacturer. I. Pregnant women should not drink alcohol II. Alcohol consumption decreases a person’s capacity to drive III. Alcohol consumption by minors affects their physical and intellectual development The same warning will be also included on all graphic or audiovisual media.
b) Advertising: “Advertising on television could be shown only between 11:00pm and 6:00am; advertising of alcoholic beverages, directly or indirectly, on the radio, between 4:00pm – 6:00pm will be prohibited. This includes: prohibition of alcoholic beverage advertising on streets, freeways, any form of commercial or non-commercial advertising, as well as direct or indirect advertising during sporting events and activities. Prohibition will be in force for all the products, activities, or publications, whatever their format – physical, virtual, aimed at minors, sporting articles for mass distribution such as shirts, uniforms and others, and any merchandising connected with sport activities, can not contain alcoholic beverage advertising.
170. Short term evaluation (one year) and incorporation of new measures for a second phase. 171. Establish and monitor self-regulation industry commitments with the regulatory authority. These commitments should be accessible to the public.
LINE OF ACTION №2: ALCOHOL AVAILABILITY
172. The physical availability of alcoholic beverages (supply, access) has direct bearing on consumption behavior in general and on excessive consumption as well. “The greater the supply, the greater the demand” is a basic rule of the economy.
54 National Alcohol Strategy - Chile
173. For the National Alcohol Strategy, it is necessary to design and agree upon provisions and practices so that the sales and supply of alcoholic beverages contribute to the reduction of excessive alcohol consumption in the nation. 174. Management of these strategies is a complex task. The proposed measures here refer to the density, concentration and mix of alcohol outlets; hours of sale and minimum purchasing age. These measures are based on effectiveness studies from international literature and/or are based on the general recommendations for Chile by expert organizations. Each measure can also cause collateral effects or risks that should be foreseen, one of them being the increase of extralegal activity. Concrete measures Reinforce and innovate on current legislation and norms on alcohol sales. Alcohol licensing 175. Establish a set of explicit requirements of binding character for the holders of alcohol licenses in order that they promote “Responsible sales”, (avoiding or minimizing the individual and social damages, for example: saying “no” to alcohol sales to minors; to those already intoxicated; to neighborhood noise disturbances; to promotions that facilitate access to alcohol). Monitoring such a measure would require systematizing the information that is received from various sources, such as local police courts, neighborhood committees, and health establishments, among others. 176. Decrease the number of maximum alcohol licenses from 1 per every 600 to 1 per thousand inhabitants. Included in this figure are all types of establishments that sell or serve alcohol. Detailed information with respect to the lifecycle of liquor licenses has to be included in the yearly municipal public account. 177. Authorize liquor licenses for set time periods, for example 3 to 5 years, and significantly increase the costs of such licenses. 178. Establish supplementary state support for municipalities that decrease the number of licenses issued. 179. Study reinsertion mechanisms and plans for merchants unable to continue in business and who need to diversify sales into non-alcohol related areas. 180. Study the feasibility and cost-effectiveness of relocating the instance for issuing alcohol licenses to a more centralized level, such as provincial and regional governments, in order to reach a more organic planning of outlet distribution. 181. Notwithstanding the foregoing, it is necessary to regulate for a more active regional government role in the control of lifecycles of alcohol licenses issued by the municipalities. Detailed information with respect to the lifecycle of liquor licenses has to be included in the yearly municipal public account Enforcement and sanctions 182. Establish a procedure to centralize the incoming information from local police courts, SEREMI de Salud, community organizations, and other relevant participants, on
55 National Alcohol Strategy - Chile
the lifecycles of liquor licenses, using this information for decision making with respect to issuing and postponement or expiration of licenses. 183. Strengthen effectiveness of municipal enforcement with respect to compliance with requirements of liquor license lifecycles. 184. Assign a more active role to the Intendants (regional government) for collaboration, supervision, and enforcement of guidelines to follow at municipal level. 185. Stricter sanctions (revoking of licenses and penalization) for offenders that break the rules specific to: selling alcohol to minors; the presence of minors in places that sell alcohol. Alcoholic beverage sale hours 186. Modify regulations on hours established by law, maintaining current norms that for those locales serving alcohol for consumption within the premises and with food (restaurants, cafés, etc) and restricting the alcohol sale hours in stores, bars and clubs (until 11:00pm, Sunday to Thursday, and until 1:00am of the following day on Friday and Saturday). This modification should be uniform at least at a regional level (eventual role of Intendants). Carry out a diagnosis 187. To study the current traits of alcohol availability in Chile. It should take into consideration the true density and distribution by locales, degree of compliance with the hours of sale, and the minimum purchase age, etc. Its objective will be to determine critical points that have bearing on high-risk alcohol consumption behavior, taking into account the related individual and social damages. 188. To study the benefits and feasibility of introducing strategies for outlet concentration associated with less harmful or risky alcohol consumption, favoring a higher geographical concentration of locales that serve alcohol accompanied by food on the premises. These strategies could be included, for example, inside the framework of a communal or regional development plan.
LINE OF ACTION № 3: ALCOHOL TAXES AND RETAIL SALE PRICES
189. Raising prices of alcoholic beverages to the public is one of the most effective and sustainable policy measures for decreasing the level of excessive alcohol consumption per capita, as well as the associated negative consequences. Modifying tax rates is one possible mechanism, but not the only one. 190. This area of the economy is one in which a price hike on a particular product, through intelligent planning, could result in a balance between seemingly conflicting objectives: benefitting consumers, through individual and public health indicators, without affecting the revenues of the implied economic agents. Concrete measures Obtaining essential information for decision making
56 National Alcohol Strategy - Chile
191. Begin the necessary studies to obtain objective and reliable information on two essential issues for the due consideration and analysis of measures on prices and taxes.
a) Balance between costs and benefits of alcohol consumption for Chile in terms of economic activity. b) Avoidable costs of harmful alcohol consumption in Chile and cost-effectiveness of necessary measures to that end.
Entity for regulating of minimum retail prices of alcoholic beverages 192. Establish an entity for the analysis, assessment and economic regulation consisting of one or more representatives from the Ministry of Treasury, Economy, Agriculture, Health and Planning, among others, in roles to be defined in the areas of:
a) Modifications for raising or lowering alcoholic beverages tax rates, within a specific range determined by law (similar to a price band) in response to the effects on public health parameters to be defined. b) Propositions for legal modifications that allow for minimum price fixing of retail sales for alcoholic beverages in agreement with the outlined principles. c) Fixing minimum retail prices of alcoholic beverages in agreement with legislation. d) Design and maintain in continuous operation, a monitoring system of social, economic, sanitary impacts that the applied measures produce on taxes and prices, and that contribute to decision making. e) Propose incentives so that producer companies and alcoholic beverage marketers increase the export of their products and the diversification of their activities towards other areas. f) Propose technical support, loans and subsidies so that small and medium-sized companies based mainly on producing and marketing alcoholic beverages shift towards the exportation of their products, and begin diversifying their activities in other areas. This would not affect those small producers for whom the measures proposed in this document are not viable due to several reasons (soil, climate or traditional grape stocks).
Increase alcoholic beverage taxes with the purpose of raising retail prices. 193. Review and modify current tax legislation on alcoholic beverages (Decree Act № 1.606 on Sales and Services Tax and Act № 19.716, which adapts the surtax on Value-Added Tax affecting alcoholic beverages to World Trade Organization rules. For this to occur, we propose two alternatives that generate two different estimated results in terms of the reduction of alcohol consumption by the population if a conservative elasticity of -0.5 is applied to the tax raise proposed according to the two meta-analyses done up to now (see Annex № 6 on Evidence, only available in Spanish):
a) Alternative 1. Differentiated increase of taxes between 5% and 20% according to absolute alcohol volume, resulting in the following figures:
57 National Alcohol Strategy - Chile
I. Beer and other alcoholic beverages, with an absolute alcohol by
volume between 0° and 9°, a tax rate of 20% (currently 15%). II. Wines, champagnes, “chichas”, ciders, and other alcoholic
beverages with an ABV between 10° and 19°, a 25% tax rate (currently 15%).
III. Liquors and other alcoholic beverages with an ABV between 20°
and 29°, a 42% tax rate (currently 27%). IV. Liquors, piscos, whisky, aguardientes (brandy), distilled, and
other alcoholic beverages with an ABV of 30° or more, a 47% tax rate (currently 27%).
In this case, the objective is to decrease alcohol intake by 2.5% for beer,
5% for wines, 7.5% for liquors of 20° to 29° and by 10% for liquors of 30° or more. b) Alternative 2: An across the board tax increase of 10% for all alcoholic beverages, resulting in the following figures:
I. Beer and other alcoholic beverages, with an ABV between 0° and
9°, a tax rate of 25% (currently 15%). II. Wines, champagnes, “chicas”, ciders, and other alcoholic
beverages with an ABV between 10° and 19°, a 25% tax rate (currently 15%).
III. Liquors, piscos, whisky and other alcoholic beverages with an
ABV of 20° and up, a 37%% tax rate (currently 27%).
In this case, the goal is to decrease alcohol intake by 5% equally for beers, wines and liquors.
Self-regulation of minimum quality of alcoholic beverages to reach a minimum high price.
194. In accordance with the manufacturing industry, agree upon a procedure that allows the industry to self-regulate the raising of acceptable standards of product quality for domestic consumption in such a manner that the minimum sales price is sufficiently high enough to reach public health goals (reducing consumption among adolescents and groups at risk).
195. Eventually, consider the usefulness and feasibility of establishing product quality control, either within the regulatory framework contained in the Reglamento Sanitario de Alimentos (Decreto Supremo № 977/96) (Food Sanitation Regulations) or under other regulations, and thus to acquire tools to influence the raising of the minimum sale price to the public.
VI. LINE OF ACTION № 4: ALCOHOL DISPENSING AND RETAIL SALE POLICIES
58 National Alcohol Strategy - Chile
196. The proposed measures in this line of action point towards sales practices regarding alcoholic beverages, either for consumption on the premises (restaurants, bars, pubs, etc) or off them (liquor stores, supermarkets, etc). The goal of these measures is to protect the consumers, minors, and the population situated near outlets and the community as a whole. There is relevant evidence and experience that should be examined in order to determine the best way of implementing them. Concrete measures Restriction of promotions that increase low-priced sales 197. Restrict the advertising and realization of types of sales that involve discounts and gifts. For example, specials offered at supermarkets, alcoholic drinks as gifts, clearance sales, two for one prices, happy hour, etc. Moreover, to strictly prohibit these kinds of activities at sporting events or others that involve youth. 198. Study the potential effects, feasibility and cost-efficiency of separating alcohol sales from other non-alcoholic products in supermarkets, for example: having exclusive cash register lines especially for alcohol-related sales. Sales policies 199. Design and implement an explicit outlet sale policy, whose rules pertain directly to those running the establishment, directed to generating non-risk selling of alcohol that could also be named “Responsable sales”. This policy takes into consideration educational slogans on menus and walls of the establishment, measures to prevent inebriation in locales of alcohol consumption; preventing drinking and driving; recognition and incentives for establishments that comply with the policy; training for waiters and sellers on persuasion strategies and conflict management of intoxicated customers, etc. 200. Participation and active leadership by owners and workers of locales is fundamental and should be taken into account when attracting cooperation for these measures as opposed to imposing them from above. Initial Diagnosis and follow up 201. Establish a line of studies which try to determine a sales pattern in locales, for consumption on or off premises. The goal of these studies will be to understand the critical environmental issues that could generate more harmful alcohol consumption on a national level, depending on the type of establishment.The baseline results and successive follow ups will provide information on the tendencies that support and sustain decision making.
LINE OF ACTION № 5: TRAFFIC, ACCIDENTS AND HARMFUL ALCOHOL CONSUMPTION
202. Many of the measures that the National Alcohol Strategy proposes in this line of action are completely or partially included in the bills that modify other legal bodies, in some state institutional plans or in proposals by corporate institutions. It represents a convergence and consensus regarding its convenience and opportunity.
59 National Alcohol Strategy - Chile
Concrete Measures Reduce and unify the alcohol blood level legally permitted for driving vehicles and the operation of machinery 203. We propose implementing a legal modification of the Traffic Act № 18.290 that reduces permissible blood alcohol levels to 0.5 grams per liter and increases the sanctions for infractions, in particular, the suspension of drivers licenses. A preparatory period would allow for an evaluation process to study and agree upon criteria to synchronize the magnitude and quality of afflictive and financial penalties with those of other legal bodies. Ensure the effective enforcement on civilian drivers done by Chilean Police (Carabineros), through means of two complimentary measures. 204. Increase the frequency and redirect enforcement procedures until a base level of success demonstrating positive results is achieved. 205. Certify the application of alcohol breath tests (alcotest) carried out according to ad hoc protocol, as sufficient scientific and legal proof for legal and administrative purposes. The measuring equipment (alcotest) must be adequately and precisely calibrated at all times. 206. Such procedures should include highly visible random enforcement to increase drivers’ awareness of the possibility of being monitored which, according to studies on effectiveness, acts as a prevention measure. 207. Applying this measure will speed up the control process, currently hampered, and in some ways, nullified by the delay in obtaining blood samples in health care centers. The technology of today’s measurement equipment (breath alcohol testing) is highly reliable, and can be used in short time periods– considerably faster than taking blood samples. In all cases, if the person being tested so demands, that person is entitled to have a blood sample taken to determine the blood alcohol content in places previously accredited by the Health Authority which already have police officers who act as attesters (at emergency health centers). 208. The “alcotest” (breathalyzer) technology today is considered to be just as reliable as or more so than blood alcohol testing. The police apply an apparatus that functions, independently of the person’s physical movements. The implementation protocol provides a more uniform and detailed account of all the users (this will include two successive applications 10 minutes apart, as well as other easily implemented conditions). 209. The legal disposition supposes that the provision of the alcotest equipment to police departments will be sufficient (in all cases, considerably more than today) and assigning human resources and time that demonstrate satisfactory results, according to evidenced based criteria. Introduce mandatory participation in health evaluation directed at detection and diagnosis of problem drinking for all reoffending drivers. Included in this process would be, in necessary cases, the treatment of mental disorders and associated consumption behaviors, and “safe driver” reeducation.
60 National Alcohol Strategy - Chile
210. The evaluation and treatment will begin in health centers and/or clinics that have implemented the appropriate procedure, subject to the medical authorization, issued and enforced by the Health Authority. Among its obligations will be the due and timely communication of the state of progress of the evaluation and treatment procedures to the corresponding judicial authority. 211. Safe driver reeducation could be implemented by agents from the public sector (municipalities, health centers), or private (education centers, work-related accident insurance organization – “ACHS”; NGOs; and others), properly authorized by the Department of Transportation and Telecommunications. The corresponding Health Authority will participate in the design, execution and evaluation of the reeducation program and ensure that the contents on low and high risk alcohol consumption levels are included. 212. All costs associated with the evaluation and reeducation of the “safe driver” will be assumed by the State.
Increase the intensity of administrative sanctions (suspension of drivers licenses) to offending drivers for driving under the influence of alcohol (drinking and driving)
213. The current provisions regarding drivers license suspensions do not give precise indications regarding criteria and suspension periods to judges handing down sentences. As a result, enforcement is at best uneven. 214. On the other hand, the evidence shows that suspending drivers licenses as promptly as possible and for suspension periods considerably longer than current ones is the most effective dissuasive measure in reducing repeat offenses and ulterior accidents. 215. Reinstating a suspended license for this cause has as an added pre-requisite: submitting to an evaluation and re-education training. Besides, precise criteria exist for definite license revocation at a certain level of repeat offenses. These measures would probably raise the effectiveness in modifying behavior. 216. The specifications about the suspension periods that heighten the effectiveness of the measure are not goals of the Alcohol Strategy, but of the plans and projects that arise from it. 217. When possible, this proposal will be merged with the provisions for the drivers icense point system project. In any case, the tightening of sanctions based on license suspension proposed here, affects the current legislation which will work in parallel with the point system.
Other possible measures that require further study 218. Establish greater demands in the process of license issuing and renewal for professional drivers regarding alcohol consumption pattern and sanctions for related offenses committed while in the performance of his duties which involve responsibility for the safety of others.

61 National Alcohol Strategy - Chile
219. Establish a “first” short-term license for drivers under 20 years and novices of any age. Integrate the various existing registration systems and procedures into one national unified epidemiology surveillance system on traffic accidents in general and those related to alcohol consumption in particular.
220. Although the National Alcohol Strategy will rely on a monitoring and general evaluation system for all of its lines of action, traffic accident monitoring already has its own systems and records that include those associated with alcohol consumption. 221. Such systems of records can and need to be perfected and strengthened by means of the unification and integration of information collected by the Chilean Police, CONSASET, DEIS-MINSAL, Registro Civil (Office of Vital Records), Servicio Médico Legal (Medical Examiner’s Office), Ministerio Público, and others if necessary. This includes observation points and procedures for a proper registration process to extract reliable and timely information. 222. Both information sources and records should be coordinated together to widen their specific perspectives and avoid duplication. Restructure the “state of health evaluation” component in the issuing and/or renewing of drivers licenses in a way that includes a more effective and reliable early health risk detection related to alcohol consumption.
223. The current procedure includes a medical evaluation in urgent need of improvement and strengthening. In such cases, it could have a high potential for early detection of not only hazardous or harmful alcohol consumption, but also other risk conditions for driving vehicles. 224. This could be accomplished if the intervention of a physician is performed in the framework of a proper health intervention, most likely in a health establishment. In the case of hazardous use of alcohol, it would facilitate the use of proven and effective detection instruments as well as ensuring that a brief intervention referral for hazardous drinking is done in a voluntary manner or as a requirement for license authorization. Prioritize and guarantee prevention area of traffic accidents associated with alcohol consumption in the Regional Commissions on Traffic Safety (Comisiones Regionales de Seguridad de Tránsito). 225. The Regional Commissions on Traffic Safety have been organizing themselves progressively over recent years. They are directed by regional intendants, while the SEREMI (Regional Ministry Office) of Transportation acts as regional coordinator. The Commissions are integrated by the sectors belonging to CONASET (National Commission on Traffic Safety).
226. The labor and effectiveness of this coordination effort can become highly relevant for activities such as studying, informing and advocating on the local realities of road safety risks; maintaining a high level of awareness and preventive behavior in the regional population, and activating and innovating best practices in diverse regional institutions.
62 National Alcohol Strategy - Chile
227. One of its possible functions should focus on strengthening and putting into effect traffic accident preventions plans related to alcohol which up to now have been weakly implemented. This mission can be accomplished through the granting of more substantial structural support, resources and assistance by local and national authorities. Promoting municipal prevention plans is another strategy, which although incipient, has great potential if empowered with creativity, normative sustainability and resources. 228. Producing an annual evaluative report for the Regional Intendant on the actions taken by the Regional Commission in this area could become a technical, political and public evaluation instrument that helps to guarantee adequate prioritization of the subject matter. Improve driver school study plans 229. Introduce a module in drivers school education and training plans that is subject to specific evaluation on alcohol consumption, its risk levels, influence on drivers and pedestrians, damages related to high risk consumption, strategies to reduce consumption and other correlated matters. Innovate on protective measures regarding pedestrians and cyclists under the effects of alcohol. 230. Pedestrian safety should be a special concern both because pedestrians are the most vulnerable of road users and international experience does not have much communicated evidence on the effectiveness of protection measures. 231. In general terms, the construction of suburban and rural roads and highways does not take into consideration the use that pedestrians need to make of their shoulders, crosswalks, and surfaces. 232. Pedestrians that have consumed alcohol, especially the inebriated, are in a vulnerable position, being a risk to themselves, as well as to third parties. The general protection measures for all pedestrians will also contribute to the safety of those impaired by drinking, although specific measures are needed for pedestrians under the influence of alcohol.
Prevention measures that require voluntary compliance from the private sector 233. Designated Driver programs implemented as policies in restaurants, institutions, company events and parties, educational centers, municipalities and neighborhoods. 234. Educational information on drinking and driving included in sponsorship and advertising of commercial products related to and also to those not related to alcoholic beverages. Add the issue of traffic accidents to the public safety agenda. Consider traffic accidents as one of the indicators used in measuring safety and for inclusion in “state of the nation” public disclosures. 235. Deaths and injuries from traffic accidents are more frequent than deaths associated with criminal violence.

63 National Alcohol Strategy - Chile
236. Although the citizens and the media do not consider traffic safety as a part of the perception on public security/insecurity; vehicular traffic conditions, including those associated with drinking and driving, can objectively have a negative effect on public safety and quality of life. 237. Local authorities, opinion leaders and the media, have a role to play in the proper use of the concept of “public safety”.
LINE OF ACTION № 6: HAZARDOUS ALCOHOL CONSUMPTION AND HEALTH CARE.
238. The health sector’s task increases within the framework of a National Alcohol Strategy. It has to anticipate and provide effective services to those affected by the more than 60 illnesses related to alcohol consumption while it simultaneously contributes to a State policy that faces this challenge as a national problem, relying on a solid public health focus. Concrete measures 239. Boost effectiveness of the primary care system (APS: Atención Primaria de Salud) and institute a routine alcohol risk level detection system to be implemented for patients and the registered population of APS facilities. In addition, carry out brief interventions on hazardous alcohol consumption. This implies the elaboration of the corresponding protocol, extensive personnel training, gradual procedure implementation, and proper registration of evaluation processes. This would allow for necessary corrections and adjustments required to reach needed effectiveness and efficiency 240. The national and regional health authority will provide. through the most effective measures possible, a flow of objective information to the general public that allows it to identify social and individual behavior factors that underlie responsible alcohol consumption, as well as responsible selling and advertising. It should also allow the public to exert its rights and duties respecting such practices. 241. Health services will revise and adapt their health care programs for women, adolescents, adults, the elderly, mental health, families, in order to include an appropriate procedure to detect and intervene in the hazardous alcohol consumption existing among its users, providing continued care along the health care network. 242. Specialized psychiatric and mental health teams will participate as APS consultants or practitioners, if so required, in the treatment plan for those patients with problematic consumption issues (harmful or dependent). Whenever possible, such decisions will be made as a team and the treatment plan will also be implemented by the team. Clinical guides, technical guidelines and protocols provide criteria and in some cases, mandatory steps. In general, they are reference points for the decisions made by the team on a case by case basis. This includes the increasingly frequent cases of alcohol dependence related to illicit substance abuse or a psychiatric comorbidity. 243. The existing mental health, alcohol, and drug programs in health services will improve the quality of services offered to those sanctioned by judicial institutions (local police and family courts, Public Prosecutors Office, etc), for infractions and offenses
64 National Alcohol Strategy - Chile
related to alcohol consumption, in order to facilitate rehabilitation and recidivism prevention of people attended by those services, working within it specific health role and complementing that of other institutions involved in this task. 244. The existing mental health, alcohol, and drug programs in health services will improve the quality of services offered to children, adolescents, in close coordination and collaboration with municipal plans directed at these and other risk groups; in order to make them more accessible, attractive and flexible, in accordance with the culture and needs of these groups. 245. The various health SEREMI offices will actively collaborate with the local governments so that they implement plans or actions in order to affect the social determinants, the social and cultural context, as well as the most vulnerable groups. The ways of collaborating are diverse and should adapt to local realities. Among other actions, we mention the following: provide updated information based on evidence on the most effective public strategies for reducing hazardous drinking; help to form intersectoral workshops for elaborating, approving and implementing municipal alcohol plans; identify the most vulnerable or damaged groups and/or zones and ensure the access to municipal health care network and Health Services. It is necessary to mention the situation of ethnic minorities, children of alcoholics, migrants, the homeless and people in other situations of exclusion. 246. From the knowledge and interaction that university educational centers acquire through their contact with the National Alcohol Strategy in the areas of teaching-health care and research, it is expected that they progressively but promptly update and introduce into academic training of future health professionals and graduates, the knowledge and tools necessary for the proper management of this problem in the affected population, as well as in public health actions.
LINE OF ACTION № 7: COMMUNITY ACTION AND LOCAL GOVERNMENTS (MUNICIPALITIES) 247. Alcohol consumption, its social dynamics and problems typically appear at the municipal level. It is here where we observe the interaction between residential sectors, alcohol outlets, streets and spaces where neighbors, friends, and youth meet, where they hold parties and where the stimulation to partake in alcohol consumption is found. 248. Both the neighbors and the municipality experience problems related to alcohol consumption by various means: public drinking or inebriation; loitering, excessive noise, littering and other nuisances around outlets; public spaces occupied by groups drinking alcohol, making the area unsafe for passers-by; domestic violence; street fights and crime, etc. 249. Each of the above factors contributes to the overall community suffering and/or inconvenience and generates a demand for municipal services. 250. A public policy such as the National Alcohol Strategy that seeks to influence life habits and social coexistence, in the end reaches its objectives in the social milieu where people live, meet and spend leisure time. Concrete Measures
65 National Alcohol Strategy - Chile
251. Revise, with broad participation of municipalities as well as other pertinent bodies, the current laws on municipal functions and competencies in order to propose the necessary legal amendments that confer clear roles on local governments. In addition, consider the necessary attributions to implement the National Alcohol Strategy for the Reduction of Harmful Alcohol Consumption on a municipal level to protect public health and the safe social coexistence within its jurisdiction. 252. Develop a grounded technique and legal basis that provides a means of support to future regulations and policies of social action to various sectors on various themes. For example:
a) Retail sale policies on alcoholic beverages with a protection component to minors and drinkers at risk. b) Municipal policies on alcoholic beverage advertising and promotion on streets, in public spaces, at cultural, sporting or recreational events, all of which involve minors. c) Identification and development of local collaborative activities that make “service activities on a community level” possible, considered as alternative sanctions in laws related to consumption of alcohol and drugs.
253. Create a financing fund accessible to municipalities that implement local plans of a preventive and reparatory nature both on the social environment as well as for people. Priority would be set on those plans that use this financing in conjunction with municipal funds (matching funds) already available, collected in the form of fines for infractions to Act N° 19.925 and of others corresponding to programs being carried out with other proposals, but which allow several kinds of integration for confronting problems associated with alcohol consumption (of health, education, sports, recreation, community development, etc). 254. Implement a procedure ensuring that municipal authorities have a broad, updated and pertinent source of information and understanding available. This supports the community strategies related to problem consumption the local government has decided to carry out during the course of its mandate. 255. Collect, concentrate, study and disseminate practices and experiences originating in group initiatives, base organizations and institutions (voluntary, non-profit, mutual aid, etc) directed towards reducing harmful alcohol use in order to facilitate proper social and political valuation, as well as its replication as an instrument that fosters social participation in this area.
LINE OF ACTION N° 8: EDUCATION, PERSONNEL AND JOB TRAINING
256. The majority of countries that have widely relied on education as an instrument of preventing or modifying harmful alcohol use and abuse, in various target populatoins: Students of grade schools, universities and technical training centers, workers, the general public, etc 257. A wide range of educational interventions have been evaluated at an international level. Though they show increases in information levels and positive changes in attitudes among the intervened groups, they have been systematically unable to show
66 National Alcohol Strategy - Chile
consistent evidence demonstrating immediate or long-term changes on alcohol consumption behavior. 258. Though the aforementioned result is discouraging, the researchers’ conclusion is that educational programs should still be actively used, but in narrow association and complemented by other measures that bear upon the availability and access to alcohol, and advertising control while prioritizing activities between peers and always involving parents. 259. Addressing the problem of harmful alcohol consumption in its due measure, that is, as the prime factor of avoidable death and disability in the country, requires a technical and professional body of highly qualified experts in various sectors (Economy, Planning and Development, Work, Education, Sports and Recreation, Ministry of Interior and Public Safety, local governments from each municipality, and Public Health). 260. The process of training competencies should incorporate initiatives in education at the university and post graduate level, in many areas of study and disciplines as well as personnel training in multiple public and private institutions. 261. Finally, the impetus and streamlining of research is also critical for the sustainability and renovation of the National Alcohol Strategy. Concrete Measures Modifications to the formal education curriculum, interventions in the educative community as a whole, and training plans with a focus on content delivery. 262. Revision of the formal curriculum and elaboration of a report with recommendations on necessary topic updates related to alcohol consumption to be considered in a future process of curricular adjustment or change. 263. Revision of curricular framework, study programs and other curriculum instruments such as study texts and progress maps with contents relative to harmful alcohol consumption. Identify and strengthen systems of school culture practices that prevent, decrease, or avoid harmful alcohol consumption among members of the grade school community. 264. Identify those school culture practices that represent potential opportunities for the prevention of harmful alcohol use at periodic events, in recreational spaces, within codes of conduct, in the student center, at parent-teacher meetings and of educational institutional projects, etc. 265. Elaborate and distribute guidelines and orientations destined to strengthen the identified systems of practices, as well as modifying and eradicating those that promote, facilitate or stimulate harmful alcohol usage. 266. Make available to educational communities, the strategies, methodologies, didactic materials, and dissemination materials for the prevention of harmful alcohol
67 National Alcohol Strategy - Chile
usage. When articulated with the formative purpose of the curriculum, they bolster the achievement of the goals set by the curriculum. 267. In addition, a training procedure for teachers currently working and for those studying for teaching careers is required in order to ensure the quality of education on this issue. Educational pilot interventions focused on behavioral change 268. Design, execute and evaluate the behavioral change aspects of educational interventions, as pilot programs that propose methodological innovations and complement other simultaneous measures directed at life context of students. 269. For this phase of pilot interventions, the following settings and emphasis are proposed:
a) Elementary/Grade School. Develop pilot interventions in at least three critical stages of development: preschool (preventive emphasis); elementary (preventive emphasis); secondary (high school) (preventive and harm reduction emphasis).
b) Universities. Among students. Emphasis: preventive, early detection and harm reduction
c) Work places. Emphasis: prevention, detection, and harm reduction. Tax incentives for companies that demonstrate permanency of interventions
Higher Education and Technical Education 270. An occasion for updating and deepening the knowledge and competencies on alcohol, consumption, its consequences and the urgency of relying on measures of control at a national level needs to be included in the criteria of accreditation and re-accreditation of the minimum curriculum at the level of higher education, courses in the field of Education, Health and others. 271. Study the convenience and feasibility of incorporating in the criteria of accreditation and re-accreditation of higher education programs and establishments, a policy for education, prevention and reduction of harm from alcohol consumption among students and employees. This policy should incorporate the criteria of the National Alcohol Strategy. 272. Include and prioritize the issues of alcohol consumption, its risks, and effective preventive interventions within the various forms of continuing education, professional training and enhancement for health professionals and technicians and those from other public and private institutions. 273. Ensure that education and training programs for Primary Health Care and Health Service professionals include as one of its priorities, the development of competencies for prevention, treatment and rehabilitation of at-risk alcohol consumers and those with disorders associated with alcohol, to actively participate in tasks specific to the National Alcohol Strategy. Other measures
68 National Alcohol Strategy - Chile
274. Study the convenience and feasibility of an institute or studies center dedicated to alcohol issues, preferably contributing to the generation and evaluation of related public policies. 275. Procure resources and incentive mechanisms for educational activities of higher education centers that enhance and update the competencies of professional and technical workers to participate in their respective scopes of actions related to the National Alcohol Strategy. 276. Procure resources and incentive mechanisms for research in multi-disciplinary themes and areas that contribute to the success of the achieving fundamental objectives of the National Strategy on Alcohol.
LINE OF ACTION № 9. MONITORING AND EVALUATION 277. A fundamental aspect for the National Alcohol Strategy’s efficacy is to develop a monitoring and evaluation system that reports on concrete advances in each line of action and the intervention model as a whole. 278. Four components are proposed for the construction of this system: a baseline of initial conditions; determination of adequate indicators for specific aspects (economic, social, legal, and cultural) of each line of action; monitoring protocol for each line of action; evaluation protocol for the Strategy as a whole and for each line of action. Concrete Measures Baseline and new indicators 279. The following statistical indicators are to be considered:
a) Per capita alcohol consumption in liters of pure alcohol among those 15 years of age or older
b) Prevalence of drinkers, measured as consumption in the past month and year.
c) Hazardous alcohol consumption is defined as the proportion of drinkers who consume five or more drinks in one sitting at least once per month.
d) Prevalence of risk drinkers, problem drinking and dependence e) Number of alcohol-related traffic accidents. f) Number and proportion of alcohol-related traffic accidents. g) Adjusted mortality rates of illnesses causally related to alcohol (standardized
figures per 100,000 inhabitants). h) Economic costs of alcohol use i) Economic benefits of alcohol consumption. j) Police arrests for infractions of alcohol laws. k) Disability Adjusted Life Years related to alcohol consumption. l) Work force in the alcohol economic activity. m) Average price of alcohol units.
280. Notwithstanding the aforementioned, the challenge of relating these global indicators to the proposed lines of actions of the National Alcohol Strategy stems from disaggregated or local evaluation of said indicators and the fact that these indicators seem unrelated to one another and randomly spread out.
69 National Alcohol Strategy - Chile
281. The implementation of the National Alcohol Strategy displays two complimentary fronts. One can be considered a centripetal force, represented by expected effects from structural, legal and economic measures that influence and pass down to local governments, neighborhoods, families and individuals (example: taxes and alcoholic beverage prices; changes to legislation in relation to advertising, availability, duty fees, and dispensing of alcoholic beverages; traffic legislation) and a front with centrifugal force with an initial focus on increasing the information and participation of the diverse social actors, such as citizens, authorities and managers; social, administrative and political institutions; national, regional and municipal institutions.
282. This focuses on local realities and regards alcohol as a social determinant that is distributed in an unequal pattern throughout the population. Some complementary indicators to those mentioned in the first point are:
a) Measurement of local alcohol consumption (estimate according to alcohol sales at a local level in relation to populations older than 15) and local consumption pattern (estimate of consumption prevalence obtained from municipal surveys)
b) Measurement of local alcohol availability, based on the objectification of alcohol outlet number and density and of local advertising.
c) Estimate of local social risks related to alcohol: rates of morbid-mortality, accidents, traumas, violence and crime.
d) Estimate of social representations of alcohol in the community based on validated qualitative techniques (for example, grounded theory).
e) Local evaluation of the implementation and effectiveness of health care protocols though quantitative indicators: number of medical consultations and people attended; results measured by socio-clinical and harm reduction parameters; efficiency in the application of suggested protocols such as brief interventions.
f) Evaluation of number of hours dedicated to education on responsible alcohol drinking, in educational settings-
Monitoring Protocol
283. The “concrete measures” that are included in each line of action will be the objectives to be monitored.
284. The analysis, communication and recording instrument for monitoring could be a roadmap, which incorporates the dates of events, the actions taken in support of achieving the goals, the assigning of resources, the problems that arise, important events such as accomplished goals, the external changes that have bearing on the objectives and other variables. Evaluation Protocol 285. Evaluation criteria should be designed and established with global and specific indicators for each line of action according to its objectives. These allow sequential and/or comparative measurements. Some examples:
286. For Line of Action №1:
70 National Alcohol Strategy - Chile
a) Periodic measurement of the degree of knowledge, approval and public opinion respecting the preventive information messages that are utilized for the general public and for selected groups. b) Evaluation of the impact before and after the eventual launching of the restrictive measures on advertising schedules and modalities that are currently in Congress on the opinion, information, attitude, and behavior of the population, c) Arrest on the part of the Chilean Police for infractions of the alcohol laws.
287. For Lines of Action №2 and 4:
a) Measurement of the physical availability of alcohol starting from the objectification of number and density of outlets in specific periods (for example: every 5 years). And in representative areas of diverse realities: urban-rural, neighborhoods, municipalities, etc.
b) Quantitative and qualitative measurements of the effects of changes in sale practices and dispensing of alcohol (selling hours, sales policies, etc)
288. Line №3:
a) Epidemiological studies using time series methodology (historical evolution) that determine effects of alcohol price increases (via taxes and price fixing) in secondary morbid-mortality
289. Line №4:
a) Measurement of local alcohol consumption (estimation according to alcohol sales at the local level in relation to population number over 15 year of age) and pattern of local consumption (estimation of prevalence of consumptions based on municipal surveys) taking into account indicators for risk-related consumption.
290. Line №5:
a) Variations in the number and proportion of traffic accidents and related consequences (deaths, injuries, etc) associated with alcohol consumption, according to legal modifications, regulations or the degree of enforcement of the aforementioned in specific areas and/or moments. b) Measure levels of acceptance and participation, immediate and mediate results of the application of health evaluation and of activities for the re-education of offenders for driving under the influence of alcohol. c) Evaluations of the effects on attitudes and behaviors of drivers and pedestrians of specific educational campaigns directed towards preventing driving under the influence of alcohol.
291. Line №6:
a) Periodic evaluation of the implementation and effectiveness of health service protocols through process and result indicators (number and characteristics of
71 National Alcohol Strategy - Chile
people attended with special focus on youth, drinkers at risk, rehabilitation and harm reduction levels)
b) Study of social and clinical results of programs especially designed for specific populations: ethnic minorities, children of alcoholics, migrants, the homeless.
c) Adjusted mortality rates of illnesses causally related to alcohol (standardized indicators per each 100,000 inhabitants)
e) Evaluation of social representations of alcohol in patients with positive and negative evolution (critical case studies)
292. Line №7:
a) Time variation of indicators that demarcate levels of social and health risks associated with alcohol consumption in municipal jurisdictions: rates of morbi-mortality, accidents, trauma, violence and crime. b) Evaluation of social representations of alcohol in the community based on validated qualitative techniques. c) Evaluation of social representations of alcohol among members of the health team.
293. Line №8:
a) Continued compilation of studies that show results based on education plans on alcohol consumption implemented in schools, universities, workplace, etc.
VII: ORGANIC STRUCTURE AND DEVELOPMENT ROUTE FOR THE NATIONAL ALCOHOL STRATEGY
294. The National Alcohol Strategy will require a powerful management infrastructure. This could include: 295. Governing organism of the National Alcohol Strategy: the National Alcohol Strategy is a responsibility of the entire government which can delegate the governing tasks to a National Council, formed by the Ministers of Health, Interior, Transport and Communication, Economy, Foment and Reconstruction, Education, Labor, INJUV (Institute for Youth), Culture and the Minister of Planning, who will preside. 296. Executive Technical Office: in charge of executing and implementing the decisions of the National Council, of the effective coordination between participant sectors in order to ensure that the objectives of the National Strategy are approached with a coherent technical and political balance. In the same way, it has to interact with civil society, the community and the diverse stakeholders. Each Ministry in the Council will appoint a representative in this office.
72 National Alcohol Strategy - Chile
297. Executive Technical Officer or Secretary: shall be appointed by the Council from a short list of three candidates presented by the Health Minister. 298. The Executive Technical Office will structure its task through a triennial Action Plan based on a set of strategic objectives to which various institutions and social organizations will concur. Each one of them will have diverse degrees of regulatory binding, some mandatory, some optional, and others voluntary. The Plan will include goals for public knowledge and disclosure during clearly stipulated periods. Moreover, it will acknowledge indicators and procedures for monitoring and periodic evaluation that facilitate both the necessary controls over the effectiveness of the Action Plan, as well as relying on the adhesion to and support of the citizens, their institutions, industries, etc. 299. The National Alcohol Strategy is a social construct more than a ruling or decision from a centralized policy. For this to happen, community participation and an informed public opinion are essential. If not understood, the chances of successfully reaching the main objective of reducing harmful alcohol consumption are scarce. 300. From the very beginning, it has been stated that a National Alcohol Strategy functions as State policy in the totality of State and government sectors. 301. The role that the National Health Authority (Health Ministry) has played up to now is that of a driving force of the National Alcohol Strategy, acting in consort with representatives from other Ministries. In the near future, it will maintain its role as an information provider and catalyst, but not necessarily an executor, without precluding those measures that enjoy a broad consensus or previous developments, either in their own health area or as complements to others. An example of the first is the inclusion of the modality called Brief Interventions in Primary Health Care, and the evaluation and reeducation of drivers sanctioned for driving under the influence. 302. The organic development of the National Alcohol Strategy refers to its installation as task and process that takes place in stages without clearly defined boundaries between them; namely, a consultation process with institutions of the political, social, entrepreneurial, labor-related, academic worlds and with the general public; implementation of those measures on which there is sufficient agreement or progress (Brief intervention in Primary Health Care); workshops in all regional governments and some municipal ones; Preparation and launching studies that contribute to major decision making (updated balance of cost-benefits of alcohol consumption regarding economic activity; studies of avoidable costs related to hazardous drinking; specification of the magnitude of alcohol-related burden of disease in specific groups, public opinion on specific measures; best practices in controlling sales to minors, drinking and driving, etc.); preparation of bills, regulations and ordinances. (See section “Immediate Steps and Conclusion” below). 303. The National Alcohol Strategy requires ongoing communication and dialogue between those directly responsible for its development, the general public, its individual members, organized groups, institutions and social organizations, both public and private. 304. In this respect, many positive experiences are observed in other countries or cultures that have carried out similar processes. These results should be carefully examined before applying them in Chile.
73 National Alcohol Strategy - Chile
305. The Health and Welfare Secretary in Scotland, for example, carried out a wide public consultation when it presented the National Strategy, gathering and assembling an important body of data from the 472 responses received, eventually becoming an annex to the latter. Among other issues submitted for this public survey was the promotion of alcoholic beverages at discount prices; consistent information to parents; raising the legal age for buying alcoholic beverages; imposing a “social responsibility” tariff to retail alcohol sales.49
306. The Australian government also sponsored, in an early stage, a public consultation about its Alcohol Strategy for 2006-2009, a document “designed to stimulate discussion” was included on the Health and Aging Department Website and was extensively disseminated inviting public opinions and feedback. Printed documents were also sent to specific audiences, resulting in responses from 23 forums, 600 answer forms, 42 written opinions and ten responses on the website were collected. This input data was used for the elaboration of the definitive document50. Similar work was carried out in New Zealand51 and England52. 307. Building alliances with those in key positions in diverse sectors of social life is also a recommendation garnered from countries who have implemented policies or plans to reduce alcohol consumption-related problems.53
308. Doubtlessly, collaboration, mutual understanding and respect should characterize the relationship between government and State sector, on one hand, and the private sector dealing with the alcohol-related economy, on the other. This sector includes businesses involved in alcoholic beverage production; alcohol wholesale and retail marketing; hospitality, tourism and leisure industries; alcohol advertising and promotion. In the case of Chile, there are already significant examples that can serve as starting points such as definitions of corporate social responsibility, self-regulation advertising which does not exploit underage models; inserted messages in advertising which refer to responsible consumption such as not drinking and driving or in the forming of an association of producers and importers with the objective of promoting responsible consumption (APROCOR). 309. There are international examples which the industry, particularly large producers, can adopt with regard to advertising and marketing self-regulation, education initiatives, and support and financing of risk prevention programs. A recent industry publication states that there are ample opportunities of innovation for industry actions that reduce harmful alcohol use and that collaborating with government institutions and other sectors is the most effective and desirable path to success.
VIII. IMMEDIATE STEPS AND CONCLUSIONS
310. The National Alcohol Strategy projects itself as a permanent policy. Its first stage of national agreement and implementation is estimated to last ten years. 311. The objectives and efforts required for the implementation of the plan are a “Bicentennial Challenge”. Its rewards, if successful, may become a relevant milestone in the development and history of the country. 312. In this final section, we specify a horizon of short-term and foreseeable actions as of the submission of this document to the consideration of the respective authorities:
74 National Alcohol Strategy - Chile
a) Analysis and approval of the Health Authority, an essential condition to initiate the consultation process. b) Beginning of the consultation to stakeholders from the political, social, entrepreneurial, labor, academic and community spheres. c) The consultation will be public in nature, open on certain occasions and in others, limited to territorial, thematic, institutional levels, as well as others. d) The respective conclusions will be recorded and systematized. The participants in the consultations shall receive feedback through summaries and conclusions. e) Towards the end of this step, a consolidated body of opinions, proposals and suggestions will be disseminated on a national level (foreseen duration: March to September 2010) f) Implementation and/or expediting of those measures on which there is sufficient agreement or progress: Brief intervention in Primary Health Care; setting-up of workshops in all regional governments and some municipal ones with the objective of getting to getting acquainted with and applying the National Strategy at those jurisdiction levels; pushing forward with related bills and law projects already in Congressional discussion. g) Setting-up the coordinating governing organism for the National Alcohol Strategy. h) Begin studies that contribute to filling information gaps necessary for major decision making: updated balance of cost-benefits of alcohol consumption regarding economic activity; avoidable costs related to hazardous drinking; specify the magnitude of alcohol-related burden of disease in particular loci: harm to the fetus and manifestations in the child’s psychosocial development, most frequent non-transmissible chronic diseases, occupational diseases; effect of alcohol consumption in labor productivity; Neighborhood security/safety perception levels in relation to alcohol outlets, etc. i) Preparation of bills, regulations and ordinances on those topics that have received opinions, respecting qualitative contributions and submitting to the democratic resolution of the competent agencies. Among others are the following: a new stricter framework on drinking and driving; modernization and adaptation of procedures for issuing drivers licenses; new framework for the process of issuing alcohol licenses; reconsiderations of the attributions that the law grants to municipalities regarding control over availability of alcoholic beverages in their jurisdiction as well as other. j) First evaluation of National Alcohol Strategy process (Estimated date: November 2010) k) Elaboration of the global triennial Action Plan 2011-2013 (Estimate date: November 2010)
75 National Alcohol Strategy - Chile
313. The present document has outlined the framework of proposals that appear to be technically advisable and feasible to the Interministerial Committee, for its submission to the country’s political authorities. 314. One of the fundamental proposals made is that of initiating a broad and reflective consultation with all sectors that becomes an exercise in information, awareness and democratic decision making regarding the paths towards reducing harmful alcohol consumption and it social and health consequences. 315. The process of consultations, approval and implementation of the National Alcohol Strategy will be marked by an intense and in all probability, passionate debate that will reveal the diverse approaches to the problem. 316. This is something necessary and beneficial and will enrich the framework of proposals. Besides, it will separate what is possible from what can be delayed or ruled out. 317. This current process will be long, complex and difficult, but its successful conclusion will certainly push Chile towards greater levels human, economic and social development.
76 National Alcohol Strategy - Chile
IX. - REFERENCES 1. Rehm J, Monteiro M. Alcohol consumption and burden of disease in the Americas: implications for alcohol policy. Pan American Journal of Public Health. 2005; 18 (4/5):241-8. 2. Orpinas P VM, Pemjeam A, Florenzano R, Nogueira R, Hernández J. Validación de una escala breve para la detección de beber anormal (EBBA). Santiago, Chile; 1991. 3. Association AP. The Diagnostic and Statlstlcal Manual of Mental Disorders, DSM-IV. 4th ed: American Psychiatrlc Publishing, Inc; 2000. 4. MINSAL. Segundo Estudio de Carga de Enfermedad y Cargabatribuible, Chile 2007: Departamento de Epldemiologla. Universidad Católica de Chile. Ministerio de Salud. Chile;2007. 5. Rehm J, Patra J, Baliunas D, Popova S, Roerecke M & Taylor B. Alcohol consumption and the global burden of disease, 2002. Geneva: WHO Department of Mental Health and Substance Abuse, Management of Substance Abuse; 2006.Monteiro MG. Alcohol and public health in the Americas: a case for action. Washington, D.C.: Pan American Health Organization; 2007. 7. WHO. Base Mundial de Datos 8. Carlini-Cotrim B. Country profile on alcohol in Brazil. In: Riley LM, M, editor. Alcohol and public health in 8 developing countries. Geneva: World Health Organization; 1999. p. 13-35. 9. WHO. World report on road traffic injury preventlon. Geneva: World Health Organization; 2004. 10. Consorcio para la Encuesta Mundial de Salud Mental; 2004. 11. INE. Encuesta Nacional Urbana de Seguridad Ciudadana (ENUSC): Instituto Nacional de Estadísticas; 2007 12. INJUV. Quinta Encuesta Nacional de Juventud: Instituto Nacional de la Juventud, Chile; 2007. 13. Presentación a Comisión de Salud. Senado de la República. Valparaíso, Chile: Asociación de Viñas de Chile A.G.; 2006. 14. Boletln Mensual: Banco Central; 2010 Enero. 15. MINSAl. Impacto Económico del Uso de Alcohol en Chile: MINSAL (CHILE); 1998. 16. Trueco M, Rebolledo P, Bustamante M, González X, Acuña G, Correa A. Detección de consumo de alcohol y drogas en accidentes graves del trabajo. Boletln Cientlfico, Asociación Chilena de Seguridad. 1999. 17. Rehm J, Baliunas D, Brochu S, Fischer B, Gnam W, Patra J et al. The Costs of Substance Abuse in Canada 2002: Highlights. Ottawa: Canadian Centre on Substance Abuse; 2006. 18. WHO-OPS. Gula Internacional para vigilar el consumo del Alcohol y sus consecuencias sanitarias: World Health Organization; 2000. 19. WHO. Global Status Report: Alcohol Policy. Geneva, Switzerland: Department of Mental Health and Substance Abuse: World Health Organlzation; 2004. 20. Babor T, Caetano R, Casswell S, Edwards G, Giesbrecht N, Graham K, Grube J, Gruenewald P, Hill L, Holder H, Romel R, Ósterberg E, Rehm J, Room R & Rossow R. Alcohol, No Ordinary Commodity: Research and Public Policy. Oxford; 2003. 21. Frequently asked questions: California Department of Alcoholic Beverage Control. 22. Babor TF, Caetano R. Evidence-based alcohol policy in the Americas: strengths, weaknesses, and future challenges. Rev Panam Salud Publica. 2005 Oct-Nov;18(4-5):327-37. 23. Rehm J, et al. Avoidable cost of alcohol abuse in Canada 2002: Centre for Addiction and Mental Health 2008. 24. Collins D, lapsley H, Brochu S, Easton B, Perez-Gomez A, Rehm J & Single E. International Guldelines for the Estimation of the Avoidable Costs of Substance Abuse. Ottawa: Health Canada; 2006. 25. WHO. Towards a global strategy to reduce harmful use of alcohol. Discussion paper for regional technical consultations on harmful use of alcohol. Geneva: World Health Organization 2009. 26. Chisholm D, Doran C, Shibuya K, Rehm J. Comparative cost-effectiveness of policy instruments for reducing the global burden of alcohol, tobacco and illicit drug use. Drug Alcohol Rev. 2006 Nov;25(6):553-65. 27. Brand DA, Saisana M, Rynn LA, Pennoni F, Lowenfels AB. Comparatlve analysis of alcohol control pollcies in 30 countries. PLoS Med. 2007 Apr;4(4):e151. 28. Giesbrecht N, McAllister J. From a blueprint to a building: Challenges and resources for implementing alcohol policy frameworks. 35th Annual Alcohol Epldemiology Symposlum of the Kettil Bruun Society. Copenhagen, Denmark; 2009. 29.: Departamento de Salud, Promoción y Protección; 2007. 30. CCSA. Gulding principies for substance abuse pollcy. Ottawa: Canadian Centre on Substance Abuse; 2006. p. 1-8. 31. Krieger N. Theories for social epidemiology in the 21st century: an ecosocial perspective. Int J Epidemiol. 2001 Aug; 30(4): 668-77. 32. Subramanian SV, Delgado I, Jadue L, Vega J, Kawachi I. Income inequality and health: multilevel analysis of Chilean communities. J Epidemiol Community Health. 2003 Nov;57(11):844-8. 33. WHO. Towards a conceptual Framework for analysis and actlon on the social determlnants of Health. Ginebra: World Health Organization; 2005. 34. WHO. Priorities for research to take forward the health equity policy agenda. Ginebra: World Health Organization; 2005. 35. WHO. Determinantes sociales de la salud: Subsanar las desigualdades en una generación. Ginebra: Organización Mundial de la Salud; 2008. 36. WHO. Social determinants of health: The salid facts. Ginebra: Organización Mundial de la Salud; 2003. 37. Marmot M. Strategic Review of Health Inequalities in England post-2010; 2009. 38. Chaloupka FJ, Saffer H., Grossman M. Alcohol-control policies and motor-vehicle fatalities. J Legal Stud. 1993;22(161-86). 39. Ohsfeldt RL, Morrisey MA. Beer taxes, workers compensation, and industrial injury. Rev Econ Stat. 1997;79: 155-60. 40. Faxcroft DR, Ireland D, lister-Sharp DJ, Lowe G, Breen R. Prlmary preventian for alcohol misuse in young people. Cochrane Database Syst Rev. 2002(3):CD003024. 41. Markowitz S. The price of alcohol, wife abuse, and husband abuse. Southern Econ J. 2000;67:279-303. 42. Markowitz S, Grossman M. The effects of beer taxes on physical child abuse. J Health Econ. 2000 Mar;19(2):271- 82. 43. Aros S. Exposición fetal a alcohol. Rev Chil Pediatr. 2008;79 (1):46-50. 44. Aros S, Milis JL, Torres C, Henriquez C, Sources A, Capurro T, et al. Prospective identification of pregnant women drlnking four or more standard drinks (> or = 48 g) of alcohol per day. Subst Use Misuse. 2006;41(2):183-97. 45. Nazer J. Anomalías congénitas estructurales en el recién nacido. Revista Hospital Clínico Universidad de Chile. 2002; 13 (3). 46. Anderson P, Chisholm D, Fuhr DC. Effectlveness and cost-effectiveness of policles and programmes to reduce the harm caused by alcohol. Lancet. 2009 Jun 27;373(9682):2234-46.

77 National Alcohol Strategy - Chile
47. Giesbrecht N. Reducing alcohol-related damage in populations: rethinking the roles of education and persuasion Interventlons. Addiction. 2007 Sep; 102(9): 1345-9. 48. Foxcroft D. Alcohol misuse prevention for young people: A rapid review of recent evidence; 2006. 49. SCOTLAND. Changing Scotland's Relationship with Alcohol: A Framework for Action: The Scottish Government; 2009. 50. AUSTRAl1A. National Alcohol Strategy 2006 - 2009. Towards Safer Drinking Cultures: Ministerial Council on Drug Strategy; 2006. 51. NEW-ZEALAND. National Alcohol Strategy 2000-2003. Wellington, New Zealand: Alcohol Advisory Couneil of New Zealand and Ministry of Health 2001 52. ENGLAND. Safe. Sensible. Social. The next steps In the National Alcohol Strategy. London: Department of Health, Home Offiee, Department for Education and Skills and Department for Culture, Media and Sport; 2007. 53. WHO-EUROPA. Framework for alcohol policy in the WHO European Region. 2006. 54. Worklng together to reduce harmful drinking. Internacional Center for Alcohol Policies. Washington DC: Routledge; 2010.
Page 1 of 18 Annex 1. National Alcohol Strategy
ANNEX 1
SUMMARY TABLE
CONCRETE MEASURES BY LINE PF ACTION LINE OF THE NATIONAL
ALCOHOL STRATEGY
LINE OF ACTION Nº 1. PUBLIC INFORMATION AND ADVERTISING CONTROL ..................................................... 2
LINE OF ACTION Nº 2. ALCOHOL AVAILABILITY .......................................................................................................... 4
LINE OF ACTION Nº 3. ALCOHOL TAXES AND RETAIL SALE PRICES ...................................................................... 6
LINE OF ACTION Nº 4. ALCOHOL DISPENSING AND RETAIL SALE POLICIES ....................................................... 8
LINE OF ACTION Nº 5. TRAFFIC, ACCIDENTS AND HARMFUL ALCOHOL CONSUMPTION ................................ 9
LINE OF ACTION Nº 6. HAZARDOUS ALCOHOL CONSUMPTION AND HEALTH CARE. ..................................... 13
LINE OF ACTION Nº 7. COMMUNITY ACTION AND LOCAL GOVERNMENTS (MUNICIPALITIES) .................. 15
LINE OF ACTION Nº 8. EDUCATION, PERSONNEL AND JOB TRAINING ................................................................. 16
LINE OF ACTION Nº 9. MONITORING AND EVALUATION .......................................................................................... 18
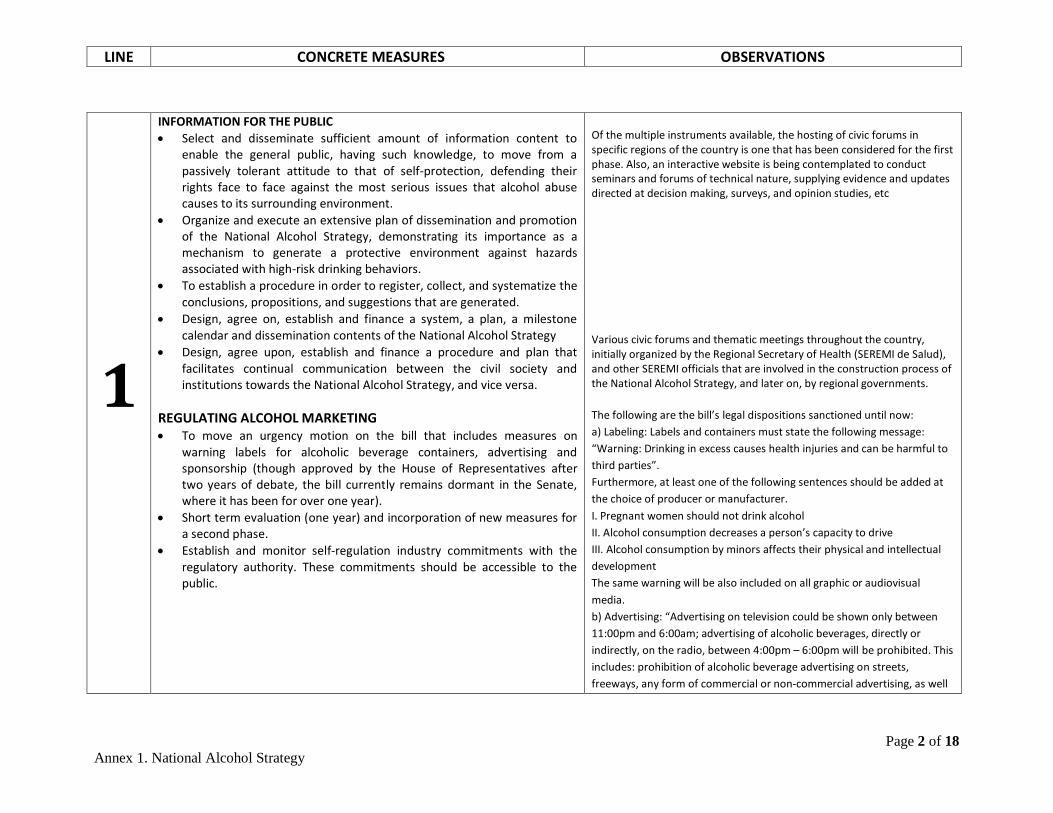
LINE CONCRETE MEASURES OBSERVATIONS
Page 2 of 18 Annex 1. National Alcohol Strategy
1
INFORMATION FOR THE PUBLIC • Select and disseminate sufficient amount of information content to
enable the general public, having such knowledge, to move from a passively tolerant attitude to that of self-protection, defending their rights face to face against the most serious issues that alcohol abuse causes to its surrounding environment.
• Organize and execute an extensive plan of dissemination and promotion of the National Alcohol Strategy, demonstrating its importance as a mechanism to generate a protective environment against hazards associated with high-risk drinking behaviors.
• To establish a procedure in order to register, collect, and systematize the conclusions, propositions, and suggestions that are generated.
• Design, agree on, establish and finance a system, a plan, a milestone calendar and dissemination contents of the National Alcohol Strategy
• Design, agree upon, establish and finance a procedure and plan that facilitates continual communication between the civil society and institutions towards the National Alcohol Strategy, and vice versa.
REGULATING ALCOHOL MARKETING • To move an urgency motion on the bill that includes measures on
warning labels for alcoholic beverage containers, advertising and sponsorship (though approved by the House of Representatives after two years of debate, the bill currently remains dormant in the Senate, where it has been for over one year).
• Short term evaluation (one year) and incorporation of new measures for a second phase.
• Establish and monitor self-regulation industry commitments with the regulatory authority. These commitments should be accessible to the public.
Of the multiple instruments available, the hosting of civic forums in specific regions of the country is one that has been considered for the first phase. Also, an interactive website is being contemplated to conduct seminars and forums of technical nature, supplying evidence and updates directed at decision making, surveys, and opinion studies, etc Various civic forums and thematic meetings throughout the country, initially organized by the Regional Secretary of Health (SEREMI de Salud), and other SEREMI officials that are involved in the construction process of the National Alcohol Strategy, and later on, by regional governments. The following are the bill’s legal dispositions sanctioned until now: a) Labeling: Labels and containers must state the following message: “Warning: Drinking in excess causes health injuries and can be harmful to third parties”. Furthermore, at least one of the following sentences should be added at the choice of producer or manufacturer. I. Pregnant women should not drink alcohol II. Alcohol consumption decreases a person’s capacity to drive III. Alcohol consumption by minors affects their physical and intellectual development The same warning will be also included on all graphic or audiovisual media. b) Advertising: “Advertising on television could be shown only between 11:00pm and 6:00am; advertising of alcoholic beverages, directly or indirectly, on the radio, between 4:00pm – 6:00pm will be prohibited. This includes: prohibition of alcoholic beverage advertising on streets, freeways, any form of commercial or non-commercial advertising, as well
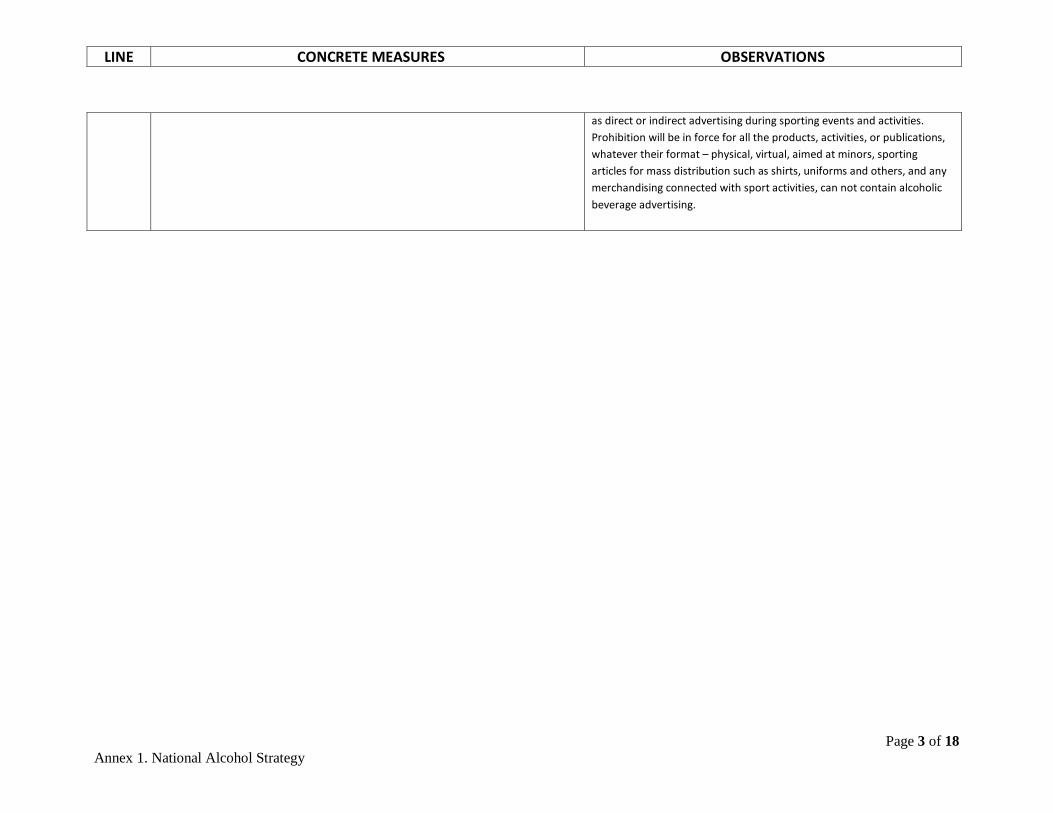
LINE CONCRETE MEASURES OBSERVATIONS
Page 3 of 18 Annex 1. National Alcohol Strategy
as direct or indirect advertising during sporting events and activities. Prohibition will be in force for all the products, activities, or publications, whatever their format – physical, virtual, aimed at minors, sporting articles for mass distribution such as shirts, uniforms and others, and any merchandising connected with sport activities, can not contain alcoholic beverage advertising.
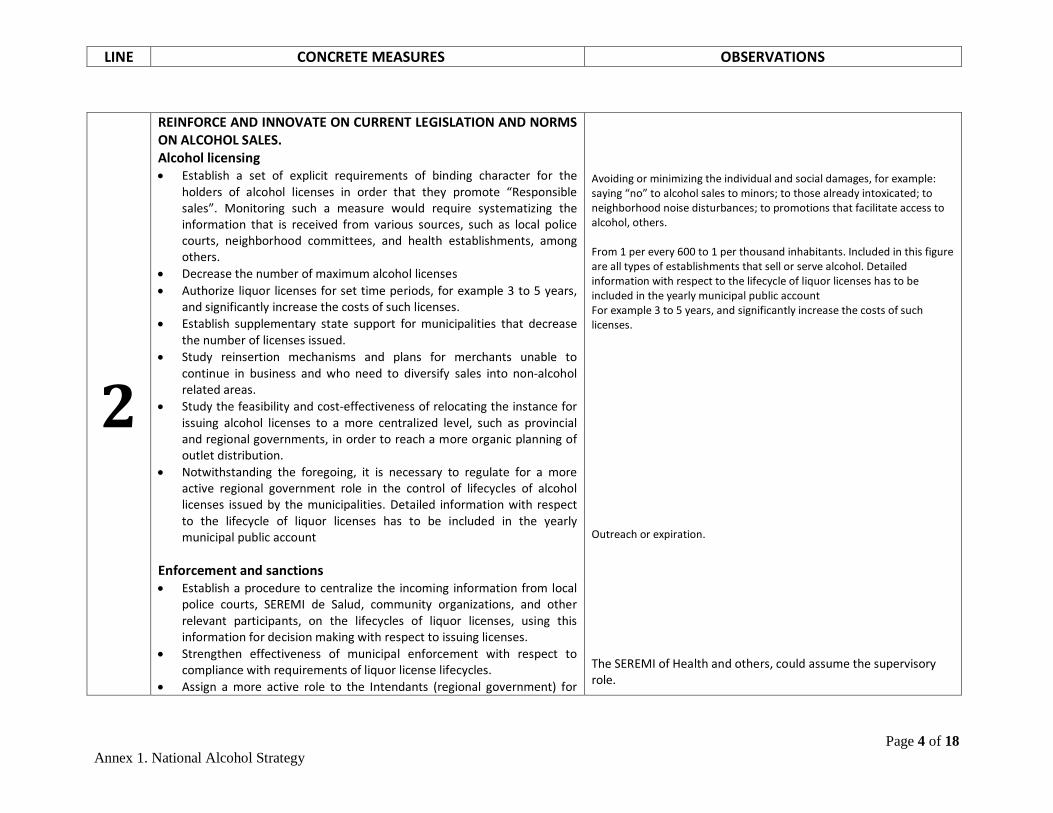
LINE CONCRETE MEASURES OBSERVATIONS
Page 4 of 18 Annex 1. National Alcohol Strategy
2
REINFORCE AND INNOVATE ON CURRENT LEGISLATION AND NORMS ON ALCOHOL SALES. Alcohol licensing • Establish a set of explicit requirements of binding character for the
holders of alcohol licenses in order that they promote “Responsible sales”. Monitoring such a measure would require systematizing the information that is received from various sources, such as local police courts, neighborhood committees, and health establishments, among others.
• Decrease the number of maximum alcohol licenses • Authorize liquor licenses for set time periods, for example 3 to 5 years,
and significantly increase the costs of such licenses. • Establish supplementary state support for municipalities that decrease
the number of licenses issued. • Study reinsertion mechanisms and plans for merchants unable to
continue in business and who need to diversify sales into non-alcohol related areas.
• Study the feasibility and cost-effectiveness of relocating the instance for issuing alcohol licenses to a more centralized level, such as provincial and regional governments, in order to reach a more organic planning of outlet distribution.
• Notwithstanding the foregoing, it is necessary to regulate for a more active regional government role in the control of lifecycles of alcohol licenses issued by the municipalities. Detailed information with respect to the lifecycle of liquor licenses has to be included in the yearly municipal public account
Enforcement and sanctions • Establish a procedure to centralize the incoming information from local
police courts, SEREMI de Salud, community organizations, and other relevant participants, on the lifecycles of liquor licenses, using this information for decision making with respect to issuing licenses.
• Strengthen effectiveness of municipal enforcement with respect to compliance with requirements of liquor license lifecycles.
• Assign a more active role to the Intendants (regional government) for
Avoiding or minimizing the individual and social damages, for example: saying “no” to alcohol sales to minors; to those already intoxicated; to neighborhood noise disturbances; to promotions that facilitate access to alcohol, others. From 1 per every 600 to 1 per thousand inhabitants. Included in this figure are all types of establishments that sell or serve alcohol. Detailed information with respect to the lifecycle of liquor licenses has to be included in the yearly municipal public account For example 3 to 5 years, and significantly increase the costs of such licenses. Outreach or expiration. The SEREMI of Health and others, could assume the supervisory role.
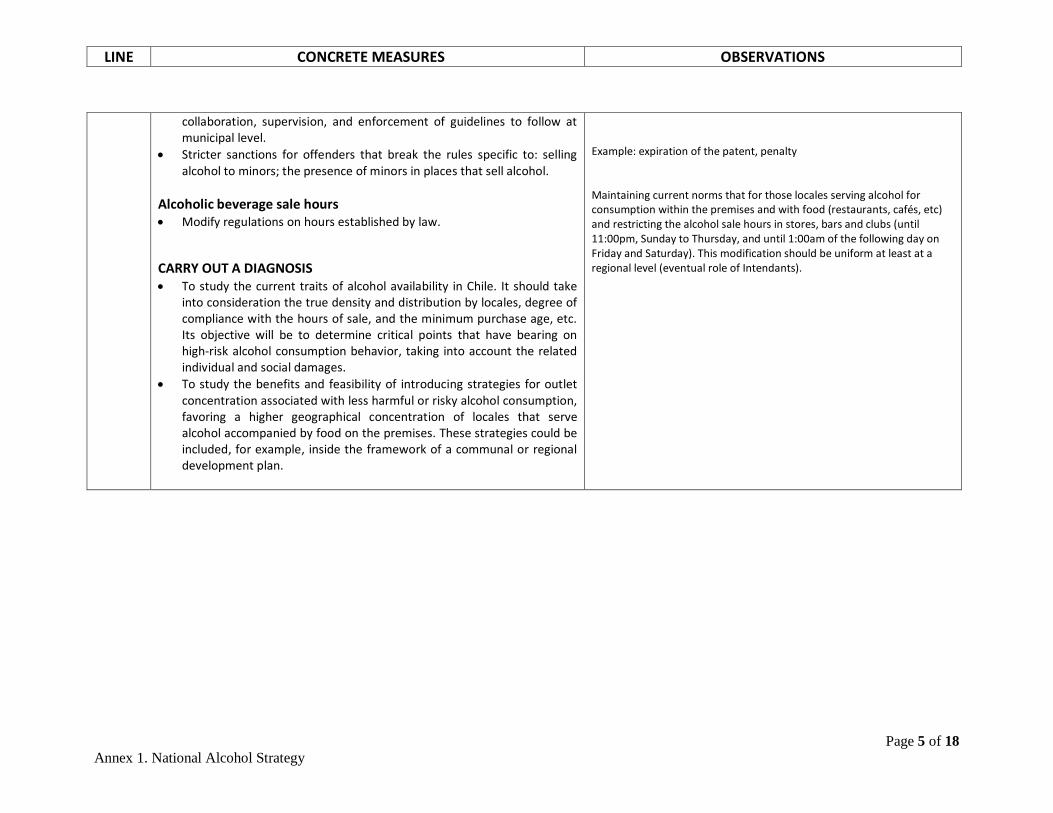
LINE CONCRETE MEASURES OBSERVATIONS
Page 5 of 18 Annex 1. National Alcohol Strategy
collaboration, supervision, and enforcement of guidelines to follow at municipal level.
• Stricter sanctions for offenders that break the rules specific to: selling alcohol to minors; the presence of minors in places that sell alcohol.
Alcoholic beverage sale hours • Modify regulations on hours established by law.
CARRY OUT A DIAGNOSIS • To study the current traits of alcohol availability in Chile. It should take
into consideration the true density and distribution by locales, degree of compliance with the hours of sale, and the minimum purchase age, etc. Its objective will be to determine critical points that have bearing on high-risk alcohol consumption behavior, taking into account the related individual and social damages.
• To study the benefits and feasibility of introducing strategies for outlet concentration associated with less harmful or risky alcohol consumption, favoring a higher geographical concentration of locales that serve alcohol accompanied by food on the premises. These strategies could be included, for example, inside the framework of a communal or regional development plan.
Example: expiration of the patent, penalty Maintaining current norms that for those locales serving alcohol for consumption within the premises and with food (restaurants, cafés, etc) and restricting the alcohol sale hours in stores, bars and clubs (until 11:00pm, Sunday to Thursday, and until 1:00am of the following day on Friday and Saturday). This modification should be uniform at least at a regional level (eventual role of Intendants).
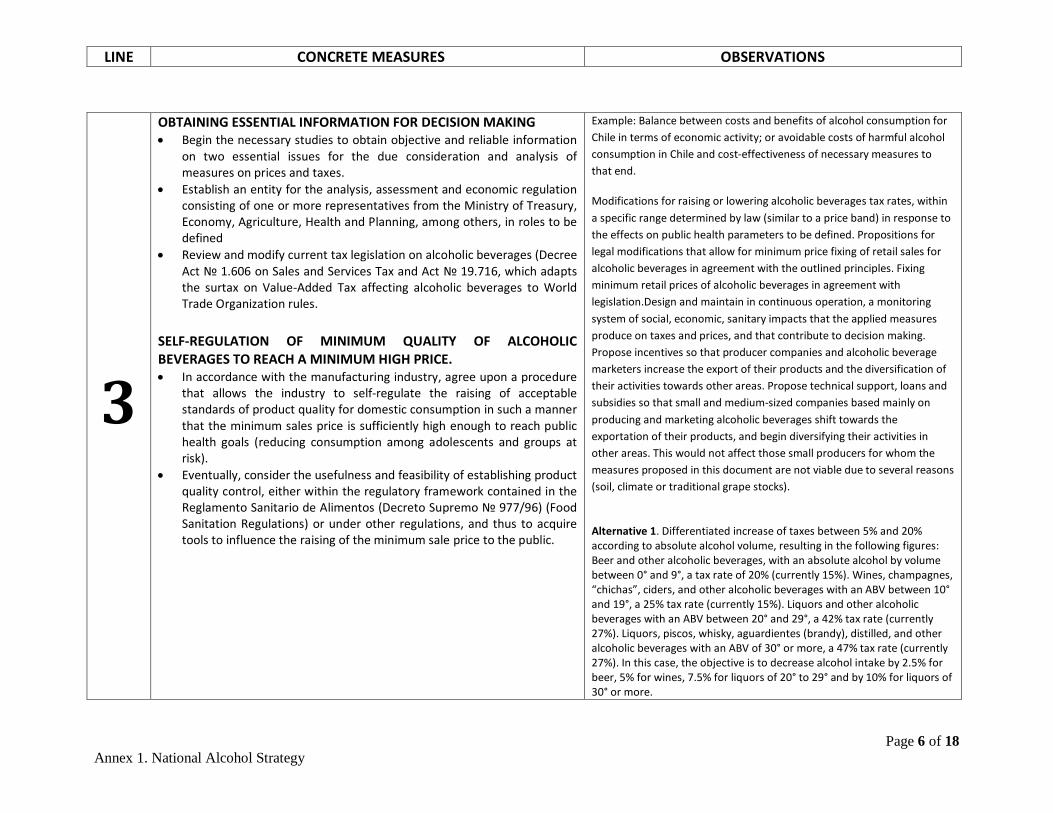
LINE CONCRETE MEASURES OBSERVATIONS
Page 6 of 18 Annex 1. National Alcohol Strategy
3
OBTAINING ESSENTIAL INFORMATION FOR DECISION MAKING • Begin the necessary studies to obtain objective and reliable information
on two essential issues for the due consideration and analysis of measures on prices and taxes.
• Establish an entity for the analysis, assessment and economic regulation consisting of one or more representatives from the Ministry of Treasury, Economy, Agriculture, Health and Planning, among others, in roles to be defined
• Review and modify current tax legislation on alcoholic beverages (Decree Act № 1.606 on Sales and Services Tax and Act № 19.716, which adapts the surtax on Value-Added Tax affecting alcoholic beverages to World Trade Organization rules.
SELF-REGULATION OF MINIMUM QUALITY OF ALCOHOLIC BEVERAGES TO REACH A MINIMUM HIGH PRICE. • In accordance with the manufacturing industry, agree upon a procedure
that allows the industry to self-regulate the raising of acceptable standards of product quality for domestic consumption in such a manner that the minimum sales price is sufficiently high enough to reach public health goals (reducing consumption among adolescents and groups at risk).
• Eventually, consider the usefulness and feasibility of establishing product quality control, either within the regulatory framework contained in the Reglamento Sanitario de Alimentos (Decreto Supremo № 977/96) (Food Sanitation Regulations) or under other regulations, and thus to acquire tools to influence the raising of the minimum sale price to the public.
Example: Balance between costs and benefits of alcohol consumption for Chile in terms of economic activity; or avoidable costs of harmful alcohol consumption in Chile and cost-effectiveness of necessary measures to that end.
Modifications for raising or lowering alcoholic beverages tax rates, within a specific range determined by law (similar to a price band) in response to the effects on public health parameters to be defined. Propositions for legal modifications that allow for minimum price fixing of retail sales for alcoholic beverages in agreement with the outlined principles. Fixing minimum retail prices of alcoholic beverages in agreement with legislation.Design and maintain in continuous operation, a monitoring system of social, economic, sanitary impacts that the applied measures produce on taxes and prices, and that contribute to decision making. Propose incentives so that producer companies and alcoholic beverage marketers increase the export of their products and the diversification of their activities towards other areas. Propose technical support, loans and subsidies so that small and medium-sized companies based mainly on producing and marketing alcoholic beverages shift towards the exportation of their products, and begin diversifying their activities in other areas. This would not affect those small producers for whom the measures proposed in this document are not viable due to several reasons (soil, climate or traditional grape stocks).
Alternative 1. Differentiated increase of taxes between 5% and 20% according to absolute alcohol volume, resulting in the following figures: Beer and other alcoholic beverages, with an absolute alcohol by volume between 0° and 9°, a tax rate of 20% (currently 15%). Wines, champagnes, “chichas”, ciders, and other alcoholic beverages with an ABV between 10° and 19°, a 25% tax rate (currently 15%). Liquors and other alcoholic beverages with an ABV between 20° and 29°, a 42% tax rate (currently 27%). Liquors, piscos, whisky, aguardientes (brandy), distilled, and other alcoholic beverages with an ABV of 30° or more, a 47% tax rate (currently 27%). In this case, the objective is to decrease alcohol intake by 2.5% for beer, 5% for wines, 7.5% for liquors of 20° to 29° and by 10% for liquors of 30° or more.
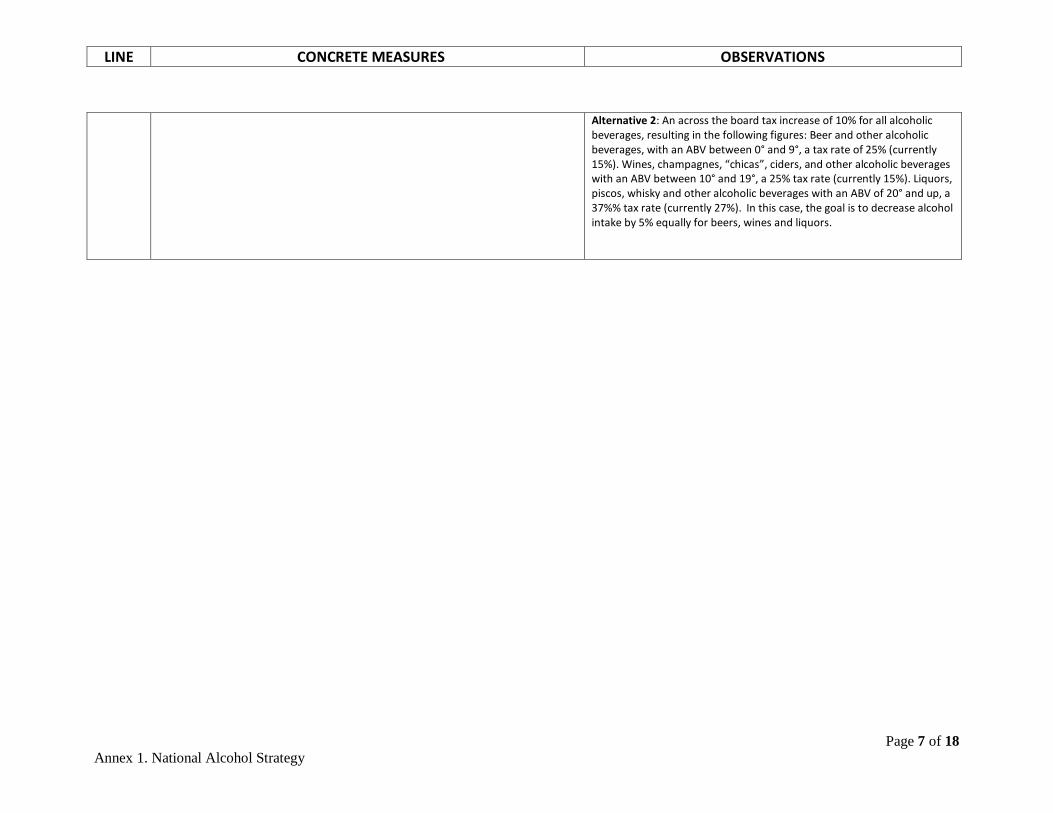
LINE CONCRETE MEASURES OBSERVATIONS
Page 7 of 18 Annex 1. National Alcohol Strategy
Alternative 2: An across the board tax increase of 10% for all alcoholic beverages, resulting in the following figures: Beer and other alcoholic beverages, with an ABV between 0° and 9°, a tax rate of 25% (currently 15%). Wines, champagnes, “chicas”, ciders, and other alcoholic beverages with an ABV between 10° and 19°, a 25% tax rate (currently 15%). Liquors, piscos, whisky and other alcoholic beverages with an ABV of 20° and up, a 37%% tax rate (currently 27%). In this case, the goal is to decrease alcohol intake by 5% equally for beers, wines and liquors.
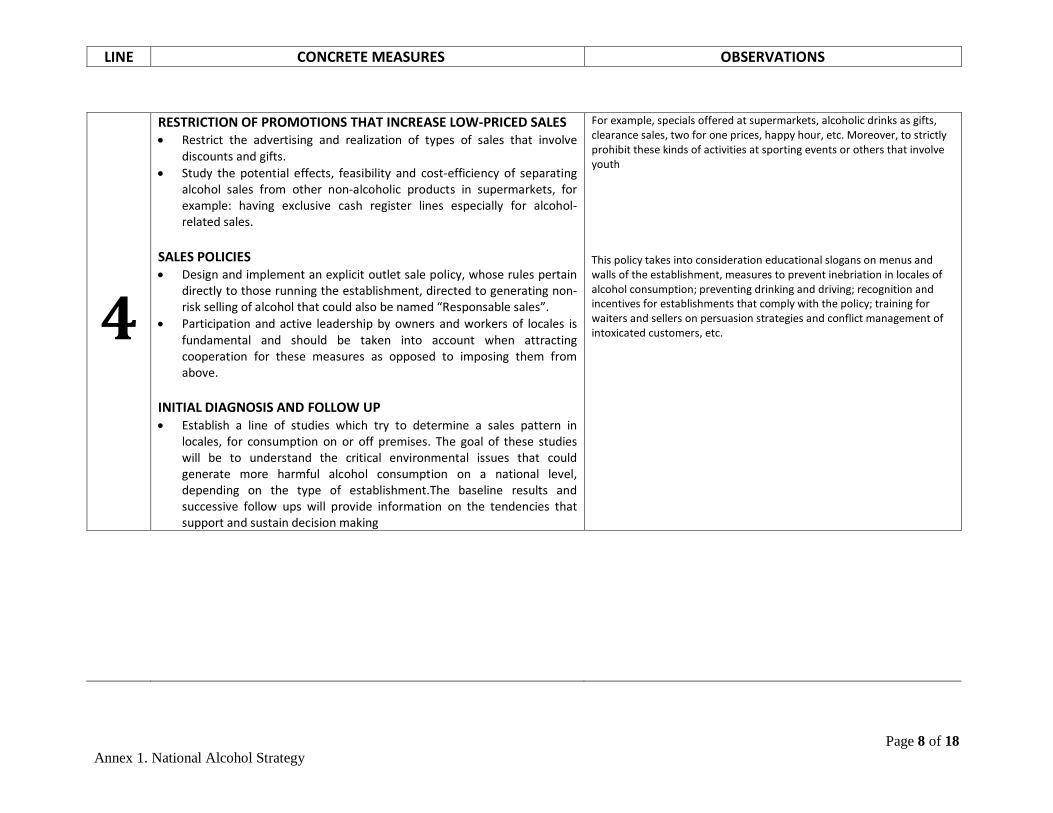
LINE CONCRETE MEASURES OBSERVATIONS
Page 8 of 18 Annex 1. National Alcohol Strategy
4
RESTRICTION OF PROMOTIONS THAT INCREASE LOW-PRICED SALES • Restrict the advertising and realization of types of sales that involve
discounts and gifts. • Study the potential effects, feasibility and cost-efficiency of separating
alcohol sales from other non-alcoholic products in supermarkets, for example: having exclusive cash register lines especially for alcohol-related sales.
SALES POLICIES • Design and implement an explicit outlet sale policy, whose rules pertain
directly to those running the establishment, directed to generating non-risk selling of alcohol that could also be named “Responsable sales”.
• Participation and active leadership by owners and workers of locales is fundamental and should be taken into account when attracting cooperation for these measures as opposed to imposing them from above.
INITIAL DIAGNOSIS AND FOLLOW UP • Establish a line of studies which try to determine a sales pattern in
locales, for consumption on or off premises. The goal of these studies will be to understand the critical environmental issues that could generate more harmful alcohol consumption on a national level, depending on the type of establishment.The baseline results and successive follow ups will provide information on the tendencies that support and sustain decision making
For example, specials offered at supermarkets, alcoholic drinks as gifts, clearance sales, two for one prices, happy hour, etc. Moreover, to strictly prohibit these kinds of activities at sporting events or others that involve youth This policy takes into consideration educational slogans on menus and walls of the establishment, measures to prevent inebriation in locales of alcohol consumption; preventing drinking and driving; recognition and incentives for establishments that comply with the policy; training for waiters and sellers on persuasion strategies and conflict management of intoxicated customers, etc.
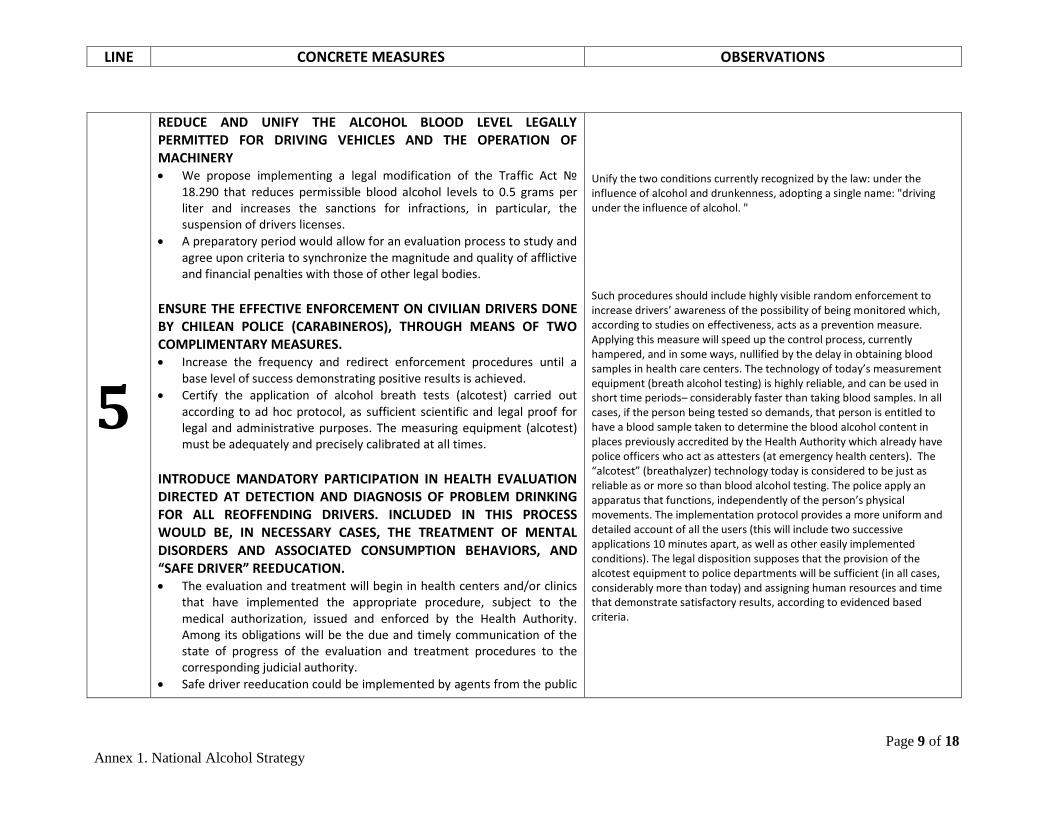
LINE CONCRETE MEASURES OBSERVATIONS
Page 9 of 18 Annex 1. National Alcohol Strategy
5
REDUCE AND UNIFY THE ALCOHOL BLOOD LEVEL LEGALLY PERMITTED FOR DRIVING VEHICLES AND THE OPERATION OF MACHINERY • We propose implementing a legal modification of the Traffic Act №
18.290 that reduces permissible blood alcohol levels to 0.5 grams per liter and increases the sanctions for infractions, in particular, the suspension of drivers licenses.
• A preparatory period would allow for an evaluation process to study and agree upon criteria to synchronize the magnitude and quality of afflictive and financial penalties with those of other legal bodies.
ENSURE THE EFFECTIVE ENFORCEMENT ON CIVILIAN DRIVERS DONE BY CHILEAN POLICE (CARABINEROS), THROUGH MEANS OF TWO COMPLIMENTARY MEASURES. • Increase the frequency and redirect enforcement procedures until a
base level of success demonstrating positive results is achieved. • Certify the application of alcohol breath tests (alcotest) carried out
according to ad hoc protocol, as sufficient scientific and legal proof for legal and administrative purposes. The measuring equipment (alcotest) must be adequately and precisely calibrated at all times.
INTRODUCE MANDATORY PARTICIPATION IN HEALTH EVALUATION DIRECTED AT DETECTION AND DIAGNOSIS OF PROBLEM DRINKING FOR ALL REOFFENDING DRIVERS. INCLUDED IN THIS PROCESS WOULD BE, IN NECESSARY CASES, THE TREATMENT OF MENTAL DISORDERS AND ASSOCIATED CONSUMPTION BEHAVIORS, AND “SAFE DRIVER” REEDUCATION. • The evaluation and treatment will begin in health centers and/or clinics
that have implemented the appropriate procedure, subject to the medical authorization, issued and enforced by the Health Authority. Among its obligations will be the due and timely communication of the state of progress of the evaluation and treatment procedures to the corresponding judicial authority.
• Safe driver reeducation could be implemented by agents from the public
Unify the two conditions currently recognized by the law: under the influence of alcohol and drunkenness, adopting a single name: "driving under the influence of alcohol. " Such procedures should include highly visible random enforcement to increase drivers’ awareness of the possibility of being monitored which, according to studies on effectiveness, acts as a prevention measure. Applying this measure will speed up the control process, currently hampered, and in some ways, nullified by the delay in obtaining blood samples in health care centers. The technology of today’s measurement equipment (breath alcohol testing) is highly reliable, and can be used in short time periods– considerably faster than taking blood samples. In all cases, if the person being tested so demands, that person is entitled to have a blood sample taken to determine the blood alcohol content in places previously accredited by the Health Authority which already have police officers who act as attesters (at emergency health centers). The “alcotest” (breathalyzer) technology today is considered to be just as reliable as or more so than blood alcohol testing. The police apply an apparatus that functions, independently of the person’s physical movements. The implementation protocol provides a more uniform and detailed account of all the users (this will include two successive applications 10 minutes apart, as well as other easily implemented conditions). The legal disposition supposes that the provision of the alcotest equipment to police departments will be sufficient (in all cases, considerably more than today) and assigning human resources and time that demonstrate satisfactory results, according to evidenced based criteria.
LINE CONCRETE MEASURES OBSERVATIONS
Page 10 of 18 Annex 1. National Alcohol Strategy
sector (municipalities, health centers), or private (education centers, work-related accident insurance organization – “ACHS”; NGOs; and others), properly authorized by the Department of Transportation and Telecommunications. The corresponding Health Authority will participate in the design, execution and evaluation of the reeducation program and ensure that the contents on low and high risk alcohol consumption levels are included.
• All costs associated with the evaluation and reeducation of the “safe driver” will be assumed by the State.
INCREASE THE INTENSITY OF ADMINISTRATIVE SANCTIONS (SUSPENSION OF DRIVERS LICENSES) TO OFFENDING DRIVERS FOR DRIVING UNDER THE INFLUENCE OF ALCOHOL (DRINKING AND DRIVING) • Reinstating a suspended license for this cause has as an added pre-
requisite: submitting to an evaluation and re-education training. Besides, precise criteria exist for definite license revocation at a certain level of repeat offenses. These measures would probably raise the effectiveness in modifying behavior.
• The specifications about the suspension periods that heighten the effectiveness of the measure are not goals of the Alcohol Strategy, but of the plans and projects that arise from it.
• When possible, this proposal will be merged with the provisions for the drivers icense point system project. In any case, the tightening of sanctions based on license suspension proposed here, affects the current legislation which will work in parallel with the point system.
OTHER POSSIBLE MEASURES THAT REQUIRE FURTHER STUDY • Establish greater demands in the process of license issuing and renewal
for professional drivers regarding alcohol consumption pattern and sanctions for related offenses committed while in the performance of his duties which involve responsibility for the safety of others.
• Establish a “first” short-term license for drivers under 20 years and novices of any age.
• Integrate the various existing registration systems and procedures into
The current provisions regarding drivers license suspensions do not give precise indications regarding criteria and suspension periods to judges handing down sentences. As a result, enforcement is at best uneven.
On the other hand, the evidence shows that suspending drivers licenses as promptly as possible and for suspension periods considerably longer than current ones is the most effective dissuasive measure in reducing repeat offenses and ulterior accidents.
LINE CONCRETE MEASURES OBSERVATIONS
Page 11 of 18 Annex 1. National Alcohol Strategy
one national unified epidemiology surveillance system on traffic accidents in general and those related to alcohol consumption in particular.
• Such systems of records can and need to be perfected and strengthened by means of the unification and integration of information collected by the Chilean Police, CONSASET, DEIS-MINSAL, Registro Civil (Office of Vital Records), Servicio Médico Legal (Medical Examiner’s Office), Ministerio Público, and others if necessary. This includes observation points and procedures for a proper registration process to extract reliable and timely information.
• Both information sources and records should be coordinated together to widen their specific perspectives and avoid duplication.
Restructure the “state of health evaluation” component in the issuing and/or renewing of drivers licenses in a way that includes a more effective and reliable early health risk detection related to alcohol consumption. Prioritize and guarantee prevention area of traffic accidents associated with alcohol consumption in the Regional Commissions on Traffic Safety (Comisiones Regionales de Seguridad de Tránsito). • One of its possible functions should focus on strengthening and putting
into effect traffic accident preventions plans related to alcohol which up to now have been weakly implemented. This mission can be accomplished through the granting of more substantial structural support, resources and assistance by local and national authorities. Promoting municipal prevention plans is another strategy, which although incipient, has great potential if empowered with creativity, normative sustainability and resources.
• Producing an annual evaluative report for the Regional Intendant on the actions taken by the Regional Commission in this area could become a technical, political and public evaluation instrument that helps to guarantee adequate prioritization of the subject matter.
Although the National Alcohol Strategy will rely on a monitoring and general evaluation system for all of its lines of action, traffic accident monitoring already has its own systems and records that include those associated with alcohol consumption.
The current procedure includes a medical evaluation in urgent need of improvement and strengthening. In such cases, it could have a high potential for early detection of not only hazardous or harmful alcohol consumption, but also other risk conditions for driving vehicles. This could be accomplished if the intervention of a physician is performed in the framework of a proper health intervention, most likely in a health establishment. In the case of hazardous use of alcohol, it would facilitate the use of proven and effective detection instruments as well as ensuring that a brief intervention referral for hazardous drinking is done in a voluntary manner or as a requirement for license authorization. Thus, we also evaluate the overall health of the applicant and professionally, his suitability to drive motorized vehicles. In this way the medical staff returns to its true role
he Regional Commissions on Traffic Safety have been organizing themselves progressively over recent years. They are directed by regional intendants, while the SEREMI (Regional Ministry Office) of Transportation acts as regional coordinator. The Commissions are integrated by the sectors belonging to CONASET (National Commission on Traffic Safety). The labor and effectiveness of this coordination effort can become highly relevant for activities such as studying, informing and advocating on the local realities of road safety risks; maintaining a high level of awareness and preventive behavior in the regional population, and activating and
LINE CONCRETE MEASURES OBSERVATIONS
Page 12 of 18 Annex 1. National Alcohol Strategy
Introduce a module in drivers school education and training plans that is subject to specific evaluation on alcohol consumption, its risk levels, influence on drivers and pedestrians, damages related to high risk consumption, strategies to reduce consumption and other correlated matters. Innovate on protective measures regarding pedestrians and cyclists under the effects of alcohol. • The general protection measures for all pedestrians will also contribute
to the safety of those impaired by drinking, although specific measures are needed for pedestrians under the influence of alcohol.
• Prevention measures that require voluntary compliance from the private sector • Educational information on drinking and driving included in sponsorship
and advertising of commercial products related to and also to those not related to alcoholic beverages.
Add the issue of traffic accidents to the public safety agenda. Consider traffic accidents as one of the indicators used in measuring safety and for inclusion in “state of the nation” public disclosures.
innovating best practices in diverse regional institutions.
Pedestrian safety should be a special concern both because pedestrians are the most vulnerable of road users and international experience does not have much communicated evidence on the effectiveness of protection measures. In general terms, the construction of suburban and rural roads and highways does not take into consideration the use that pedestrians need to make of their shoulders, crosswalks, and surfaces.Pedestrians that have consumed alcohol, especially the inebriated, are in a vulnerable position, being a risk to themselves, as well as to third parties
In example: Designated Driver programs implemented as policies in restaurants, institutions, company events and parties, educational centers, municipalities and neighborhoods.
Deaths and injuries from traffic accidents are more frequent than deaths associated with criminal violence. Although the citizens and the media do not consider traffic safety as a part of the perception on public security/insecurity; vehicular traffic conditions, including those associated with drinking and driving, can objectively have a negative effect on public safety and quality of life. Local authorities, opinion leaders and the media, have a role to play in the proper use of the concept of “public safety”.
LINE CONCRETE MEASURES OBSERVATIONS
Page 13 of 18 Annex 1. National Alcohol Strategy
6
• Boost effectiveness of the primary care system (APS: Atención Primaria de Salud) and institute a routine alcohol risk level detection system to be implemented for patients and the registered population of APS facilities. In addition, carry out brief interventions on hazardous alcohol consumption.
• The national and regional health authority will provide. through the most effective measures possible, a flow of objective information to the general public that allows it to identify social and individual behavior factors that underlie responsible alcohol consumption, as well as responsible selling and advertising. It should also allow the public to exert its rights and duties respecting such practices.
• Health services will revise and adapt their health care programs for women, adolescents, adults, the elderly, mental health, families, in order to include an appropriate procedure to detect and intervene in the hazardous alcohol consumption existing among its users, providing continued care along the health care network.
• Specialized psychiatric and mental health teams will participate as APS consultants or practitioners, if so required, in the treatment plan for those patients with problematic consumption issues (harmful or dependent). Whenever possible, such decisions will be made as a team and the treatment plan will also be implemented by the team.
• The existing mental health, alcohol, and drug programs in health services will improve the quality of services offered to those sanctioned by judicial institutions (local police and family courts, Public Prosecutors Office, etc), for infractions and offenses related to alcohol consumption, in order to facilitate rehabilitation and recidivism prevention of people attended by those services, working within it specific health role and complementing that of other institutions involved in this task.
• The existing mental health, alcohol, and drug programs in health services will improve the quality of services offered to children, adolescents, in close coordination and collaboration with municipal plans directed at these and other risk groups; in order to make them more accessible, attractive and flexible, in accordance with the culture and needs of these groups.
• The various health SEREMI offices will actively collaborate with the local
This implies the elaboration of the corresponding protocol, extensive personnel training, gradual procedure implementation, and proper registration of evaluation processes. This would allow for necessary corrections and adjustments required to reach needed effectiveness and efficiency. Clinical guides, technical guidelines and protocols provide criteria and in some cases, mandatory steps. In general, they are reference points for the decisions made by the team on a case by case basis. This includes the increasingly frequent cases of alcohol dependence related to illicit substance abuse or a psychiatric comorbidity. The ways of collaborating are diverse and should adapt to local realities. Among other actions, we mention the following: provide updated
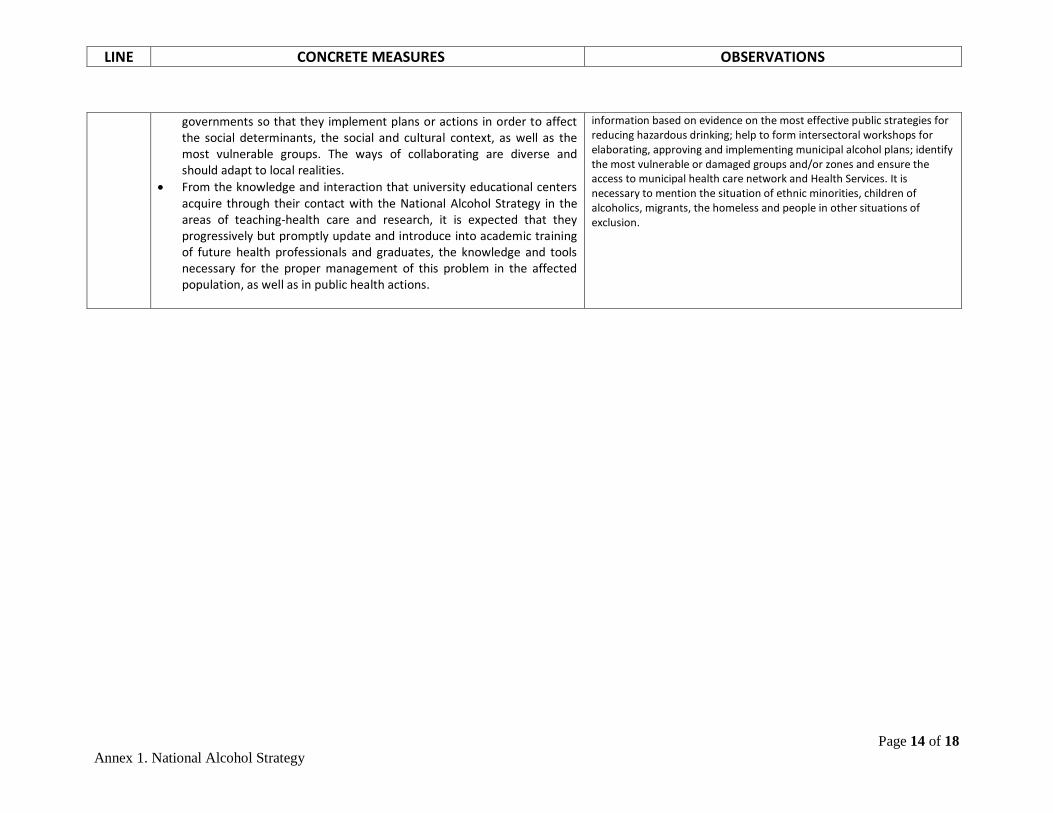
LINE CONCRETE MEASURES OBSERVATIONS
Page 14 of 18 Annex 1. National Alcohol Strategy
governments so that they implement plans or actions in order to affect the social determinants, the social and cultural context, as well as the most vulnerable groups. The ways of collaborating are diverse and should adapt to local realities.
• From the knowledge and interaction that university educational centers acquire through their contact with the National Alcohol Strategy in the areas of teaching-health care and research, it is expected that they progressively but promptly update and introduce into academic training of future health professionals and graduates, the knowledge and tools necessary for the proper management of this problem in the affected population, as well as in public health actions.
information based on evidence on the most effective public strategies for reducing hazardous drinking; help to form intersectoral workshops for elaborating, approving and implementing municipal alcohol plans; identify the most vulnerable or damaged groups and/or zones and ensure the access to municipal health care network and Health Services. It is necessary to mention the situation of ethnic minorities, children of alcoholics, migrants, the homeless and people in other situations of exclusion.
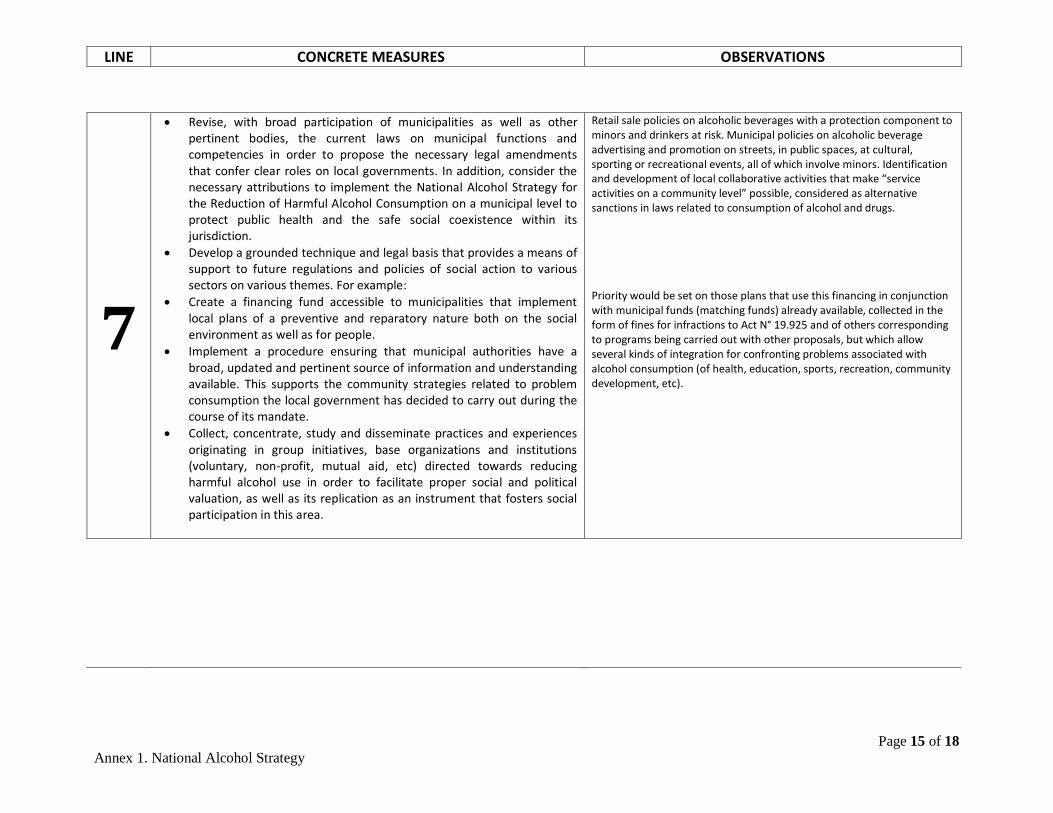
LINE CONCRETE MEASURES OBSERVATIONS
Page 15 of 18 Annex 1. National Alcohol Strategy
7
• Revise, with broad participation of municipalities as well as other pertinent bodies, the current laws on municipal functions and competencies in order to propose the necessary legal amendments that confer clear roles on local governments. In addition, consider the necessary attributions to implement the National Alcohol Strategy for the Reduction of Harmful Alcohol Consumption on a municipal level to protect public health and the safe social coexistence within its jurisdiction.
• Develop a grounded technique and legal basis that provides a means of support to future regulations and policies of social action to various sectors on various themes. For example:
• Create a financing fund accessible to municipalities that implement local plans of a preventive and reparatory nature both on the social environment as well as for people.
• Implement a procedure ensuring that municipal authorities have a broad, updated and pertinent source of information and understanding available. This supports the community strategies related to problem consumption the local government has decided to carry out during the course of its mandate.
• Collect, concentrate, study and disseminate practices and experiences originating in group initiatives, base organizations and institutions (voluntary, non-profit, mutual aid, etc) directed towards reducing harmful alcohol use in order to facilitate proper social and political valuation, as well as its replication as an instrument that fosters social participation in this area.
Retail sale policies on alcoholic beverages with a protection component to minors and drinkers at risk. Municipal policies on alcoholic beverage advertising and promotion on streets, in public spaces, at cultural, sporting or recreational events, all of which involve minors. Identification and development of local collaborative activities that make “service activities on a community level” possible, considered as alternative sanctions in laws related to consumption of alcohol and drugs. Priority would be set on those plans that use this financing in conjunction with municipal funds (matching funds) already available, collected in the form of fines for infractions to Act N° 19.925 and of others corresponding to programs being carried out with other proposals, but which allow several kinds of integration for confronting problems associated with alcohol consumption (of health, education, sports, recreation, community development, etc).
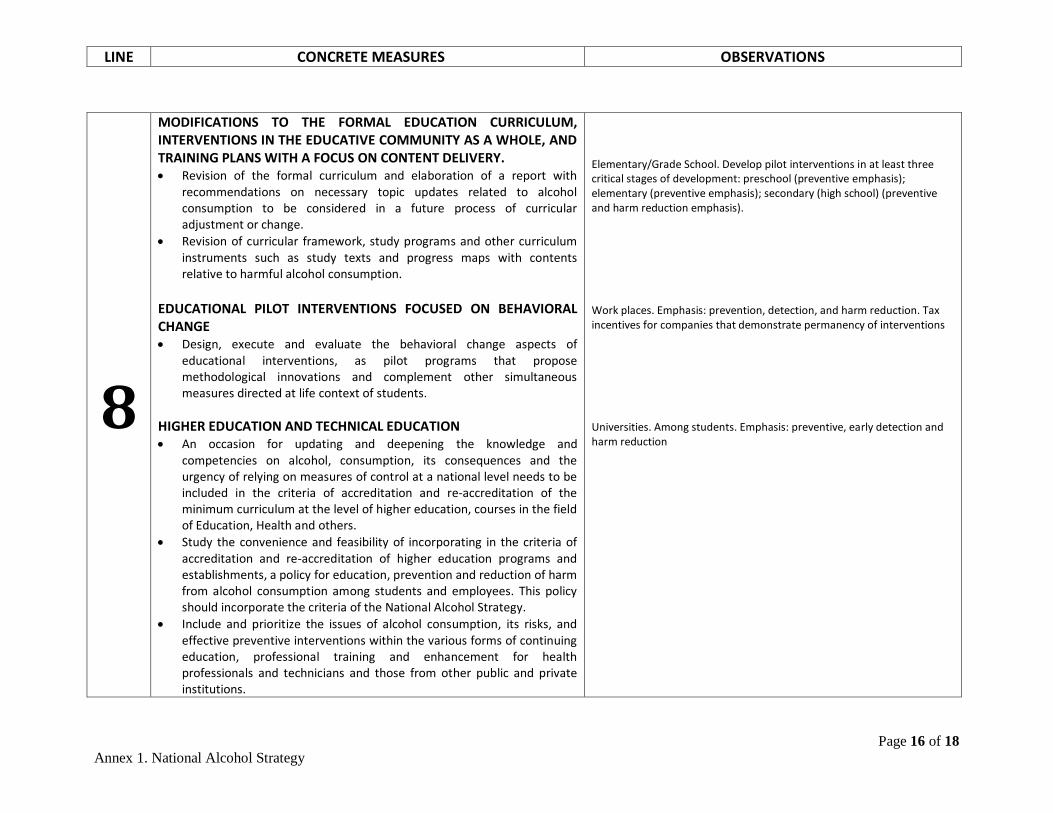
LINE CONCRETE MEASURES OBSERVATIONS
Page 16 of 18 Annex 1. National Alcohol Strategy
8
MODIFICATIONS TO THE FORMAL EDUCATION CURRICULUM, INTERVENTIONS IN THE EDUCATIVE COMMUNITY AS A WHOLE, AND TRAINING PLANS WITH A FOCUS ON CONTENT DELIVERY. • Revision of the formal curriculum and elaboration of a report with
recommendations on necessary topic updates related to alcohol consumption to be considered in a future process of curricular adjustment or change.
• Revision of curricular framework, study programs and other curriculum instruments such as study texts and progress maps with contents relative to harmful alcohol consumption.
EDUCATIONAL PILOT INTERVENTIONS FOCUSED ON BEHAVIORAL CHANGE • Design, execute and evaluate the behavioral change aspects of
educational interventions, as pilot programs that propose methodological innovations and complement other simultaneous measures directed at life context of students.
HIGHER EDUCATION AND TECHNICAL EDUCATION • An occasion for updating and deepening the knowledge and
competencies on alcohol, consumption, its consequences and the urgency of relying on measures of control at a national level needs to be included in the criteria of accreditation and re-accreditation of the minimum curriculum at the level of higher education, courses in the field of Education, Health and others.
• Study the convenience and feasibility of incorporating in the criteria of accreditation and re-accreditation of higher education programs and establishments, a policy for education, prevention and reduction of harm from alcohol consumption among students and employees. This policy should incorporate the criteria of the National Alcohol Strategy.
• Include and prioritize the issues of alcohol consumption, its risks, and effective preventive interventions within the various forms of continuing education, professional training and enhancement for health professionals and technicians and those from other public and private institutions.
Elementary/Grade School. Develop pilot interventions in at least three critical stages of development: preschool (preventive emphasis); elementary (preventive emphasis); secondary (high school) (preventive and harm reduction emphasis). Work places. Emphasis: prevention, detection, and harm reduction. Tax incentives for companies that demonstrate permanency of interventions Universities. Among students. Emphasis: preventive, early detection and harm reduction
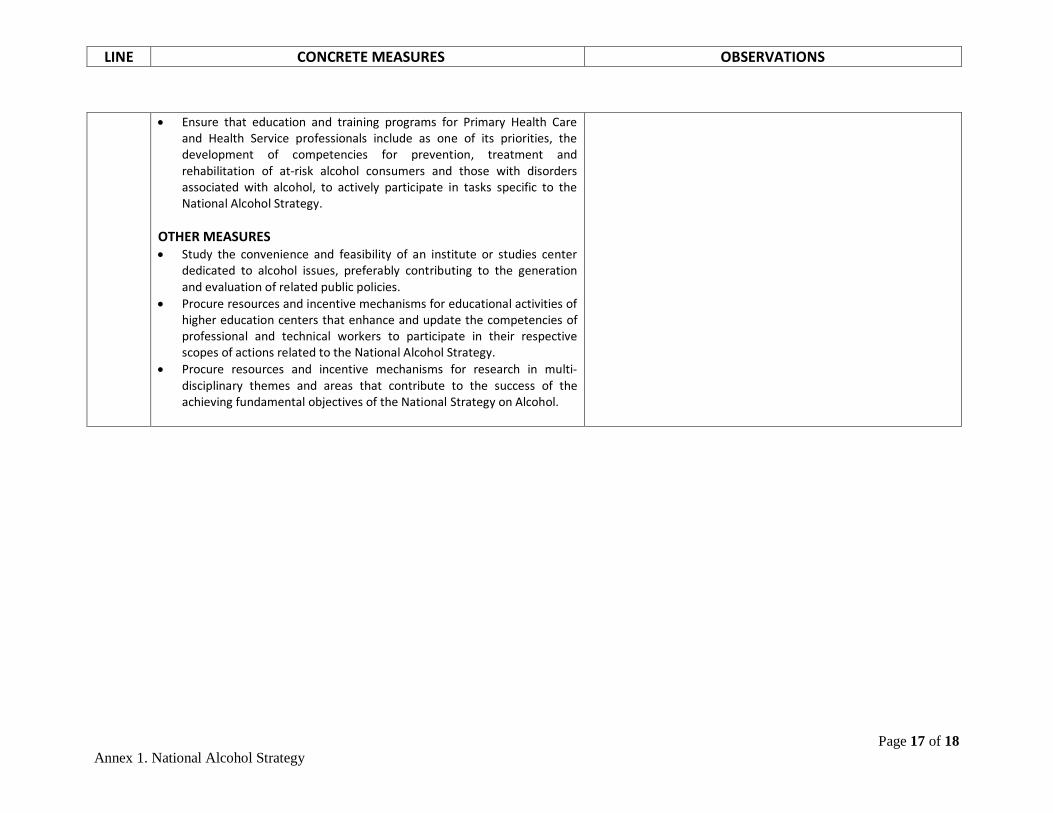
LINE CONCRETE MEASURES OBSERVATIONS
Page 17 of 18 Annex 1. National Alcohol Strategy
• Ensure that education and training programs for Primary Health Care and Health Service professionals include as one of its priorities, the development of competencies for prevention, treatment and rehabilitation of at-risk alcohol consumers and those with disorders associated with alcohol, to actively participate in tasks specific to the National Alcohol Strategy.
OTHER MEASURES • Study the convenience and feasibility of an institute or studies center
dedicated to alcohol issues, preferably contributing to the generation and evaluation of related public policies.
• Procure resources and incentive mechanisms for educational activities of higher education centers that enhance and update the competencies of professional and technical workers to participate in their respective scopes of actions related to the National Alcohol Strategy.
• Procure resources and incentive mechanisms for research in multi-disciplinary themes and areas that contribute to the success of the achieving fundamental objectives of the National Strategy on Alcohol.
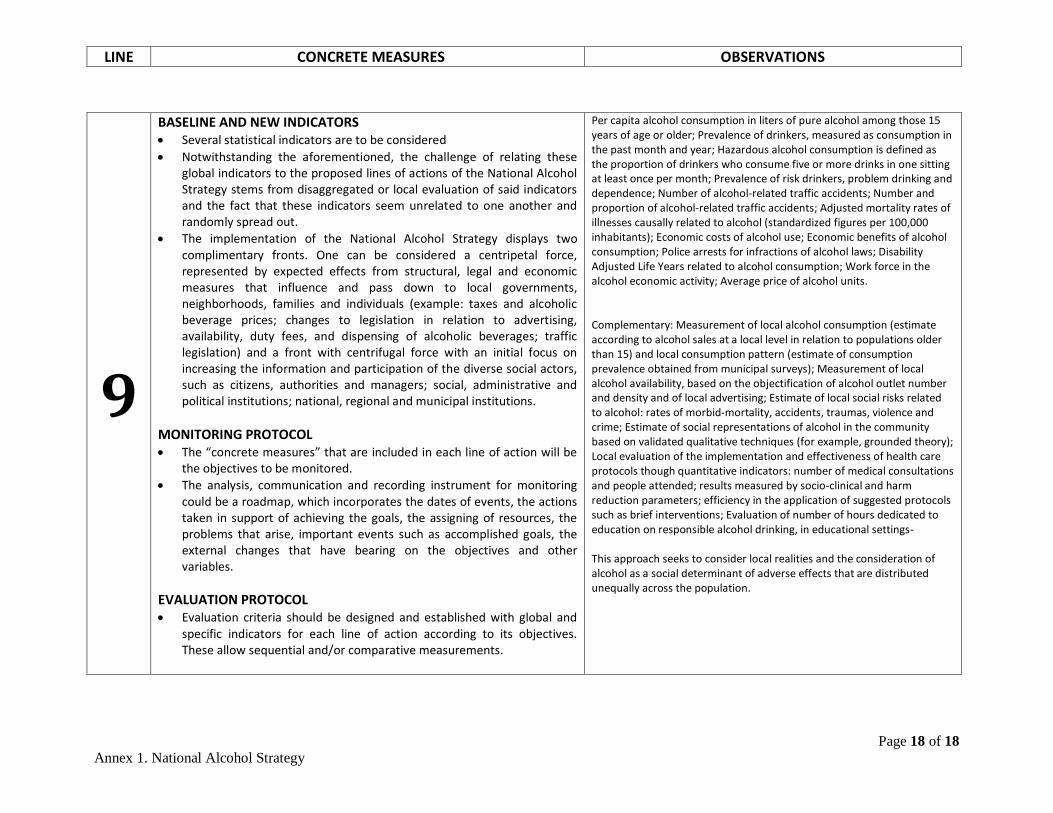
LINE CONCRETE MEASURES OBSERVATIONS
Page 18 of 18 Annex 1. National Alcohol Strategy
9
BASELINE AND NEW INDICATORS • Several statistical indicators are to be considered • Notwithstanding the aforementioned, the challenge of relating these
global indicators to the proposed lines of actions of the National Alcohol Strategy stems from disaggregated or local evaluation of said indicators and the fact that these indicators seem unrelated to one another and randomly spread out.
• The implementation of the National Alcohol Strategy displays two complimentary fronts. One can be considered a centripetal force, represented by expected effects from structural, legal and economic measures that influence and pass down to local governments, neighborhoods, families and individuals (example: taxes and alcoholic beverage prices; changes to legislation in relation to advertising, availability, duty fees, and dispensing of alcoholic beverages; traffic legislation) and a front with centrifugal force with an initial focus on increasing the information and participation of the diverse social actors, such as citizens, authorities and managers; social, administrative and political institutions; national, regional and municipal institutions.
MONITORING PROTOCOL • The “concrete measures” that are included in each line of action will be
the objectives to be monitored. • The analysis, communication and recording instrument for monitoring
could be a roadmap, which incorporates the dates of events, the actions taken in support of achieving the goals, the assigning of resources, the problems that arise, important events such as accomplished goals, the external changes that have bearing on the objectives and other variables.
EVALUATION PROTOCOL • Evaluation criteria should be designed and established with global and
specific indicators for each line of action according to its objectives. These allow sequential and/or comparative measurements.
Per capita alcohol consumption in liters of pure alcohol among those 15 years of age or older; Prevalence of drinkers, measured as consumption in the past month and year; Hazardous alcohol consumption is defined as the proportion of drinkers who consume five or more drinks in one sitting at least once per month; Prevalence of risk drinkers, problem drinking and dependence; Number of alcohol-related traffic accidents; Number and proportion of alcohol-related traffic accidents; Adjusted mortality rates of illnesses causally related to alcohol (standardized figures per 100,000 inhabitants); Economic costs of alcohol use; Economic benefits of alcohol consumption; Police arrests for infractions of alcohol laws; Disability Adjusted Life Years related to alcohol consumption; Work force in the alcohol economic activity; Average price of alcohol units. Complementary: Measurement of local alcohol consumption (estimate according to alcohol sales at a local level in relation to populations older than 15) and local consumption pattern (estimate of consumption prevalence obtained from municipal surveys); Measurement of local alcohol availability, based on the objectification of alcohol outlet number and density and of local advertising; Estimate of local social risks related to alcohol: rates of morbid-mortality, accidents, traumas, violence and crime; Estimate of social representations of alcohol in the community based on validated qualitative techniques (for example, grounded theory); Local evaluation of the implementation and effectiveness of health care protocols though quantitative indicators: number of medical consultations and people attended; results measured by socio-clinical and harm reduction parameters; efficiency in the application of suggested protocols such as brief interventions; Evaluation of number of hours dedicated to education on responsible alcohol drinking, in educational settings- This approach seeks to consider local realities and the consideration of alcohol as a social determinant of adverse effects that are distributed unequally across the population.
Page 1 of 3 ANNEXO 2. National Alcohol Strategy
ANNEX 2
COSTS AND BENEFITS ASSOCIATED
WITH ALCOHOL CONSUMPTION COSTS ASSOCIATED WITH EXCESSIVE ALCOHOL CONSUMPTION ........... ¡Error! Marcador no definido. BENEFITS ASSOCIATED WITH THE ALCOHOL MARKET ....... ¡Error! Marcador no definido.
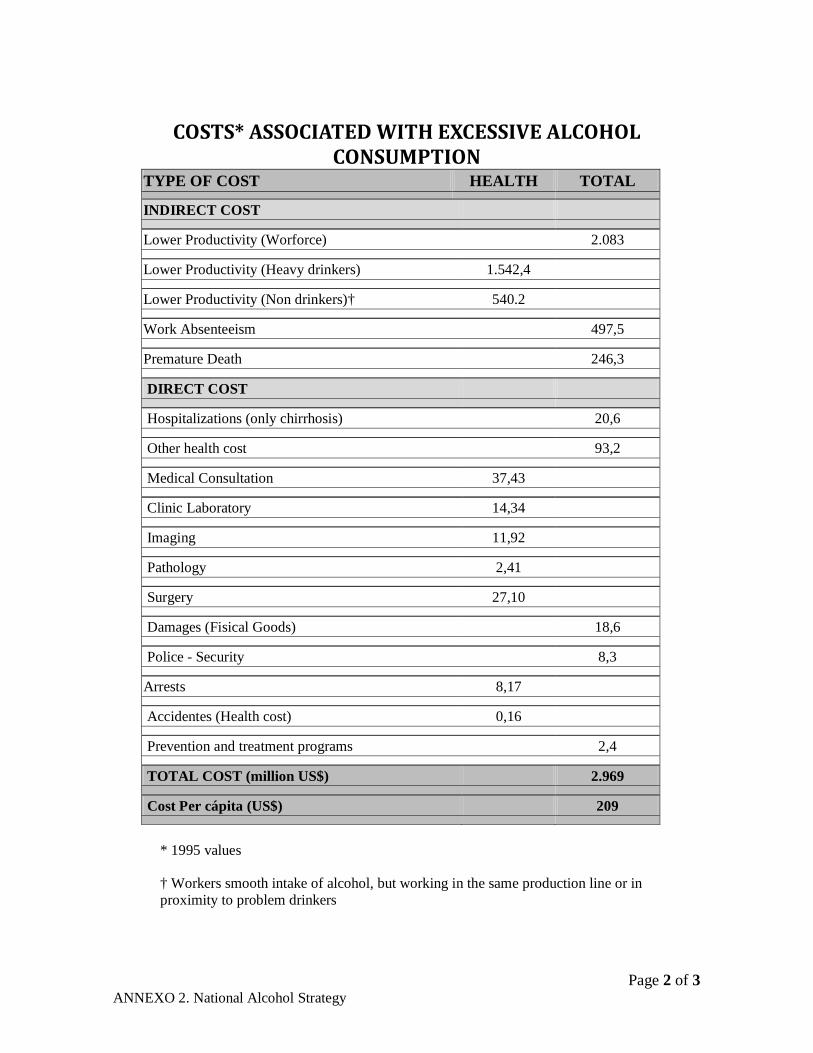
Page 2 of 3 ANNEXO 2. National Alcohol Strategy
COSTS* ASSOCIATED WITH EXCESSIVE ALCOHOL
CONSUMPTION TYPE OF COST HEALTH TOTAL
INDIRECT COST
Lower Productivity (Worforce) 2.083
Lower Productivity (Heavy drinkers) 1.542,4
Lower Productivity (Non drinkers)† 540.2
Work Absenteeism 497,5
Premature Death 246,3
DIRECT COST
Hospitalizations (only chirrhosis) 20,6
Other health cost 93,2
Medical Consultation 37,43
Clinic Laboratory 14,34
Imaging 11,92
Pathology 2,41
Surgery 27,10
Damages (Fisical Goods) 18,6
Police - Security 8,3
Arrests 8,17
Accidentes (Health cost) 0,16
Prevention and treatment programs 2,4
TOTAL COST (million US$) 2.969
Cost Per cápita (US$) 209
* 1995 values
† Workers smooth intake of alcohol, but working in the same production line or in proximity to problem drinkers
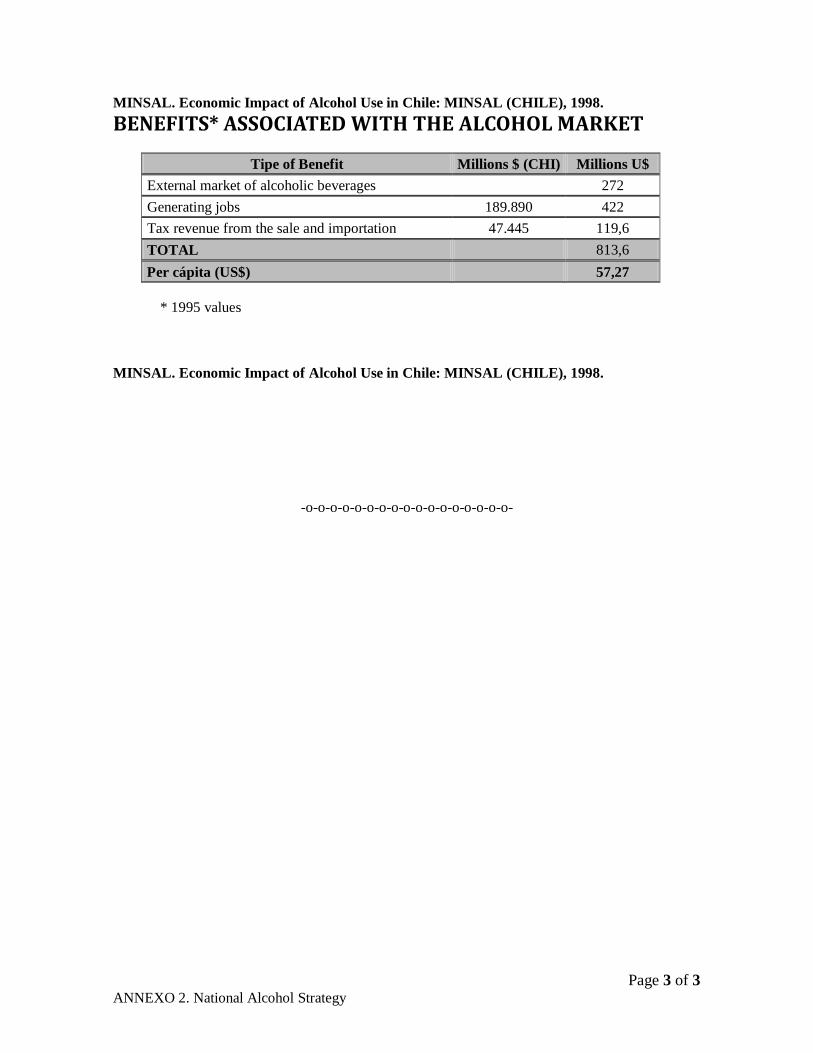
Page 3 of 3 ANNEXO 2. National Alcohol Strategy
MINSAL. Economic Impact of Alcohol Use in Chile: MINSAL (CHILE), 1998. BENEFITS* ASSOCIATED WITH THE ALCOHOL MARKET
Tipe of Benefit Millions $ (CHI) Millions U$ External market of alcoholic beverages 272 Generating jobs 189.890 422 Tax revenue from the sale and importation 47.445 119,6 TOTAL 813,6 Per cápita (US$) 57,27
* 1995 values
MINSAL. Economic Impact of Alcohol Use in Chile: MINSAL (CHILE), 1998.
-o-o-o-o-o-o-o-o-o-o-o-o-o-o-o-o-o-
Page 1 of 5
ANNEX 3. National Alcohol Strategy.
ANNEX 3
EFFECTIVENESS OF PUBLIC POLICY
MEASURES TO REDUCE THE DAMAGES RELATED TO ALCOHOL CONSUMPTION:
COMPARATIVE TABLES
1.- BABOR et al. (2005) Índices expertos de estrategias e intervenciones de políticas relevantes utilizadas en todo el mundo para prevenir o minimizar los problemas relacionados con el consumo de alcohol…………………………………………………………………………………………. 2
2.- ANDERSON et al. (2009) Resumen del efecto de medidas de política pública, con nivel de evidenciade acuerdo a disponibilidad de evidencia………………………………………………. 4
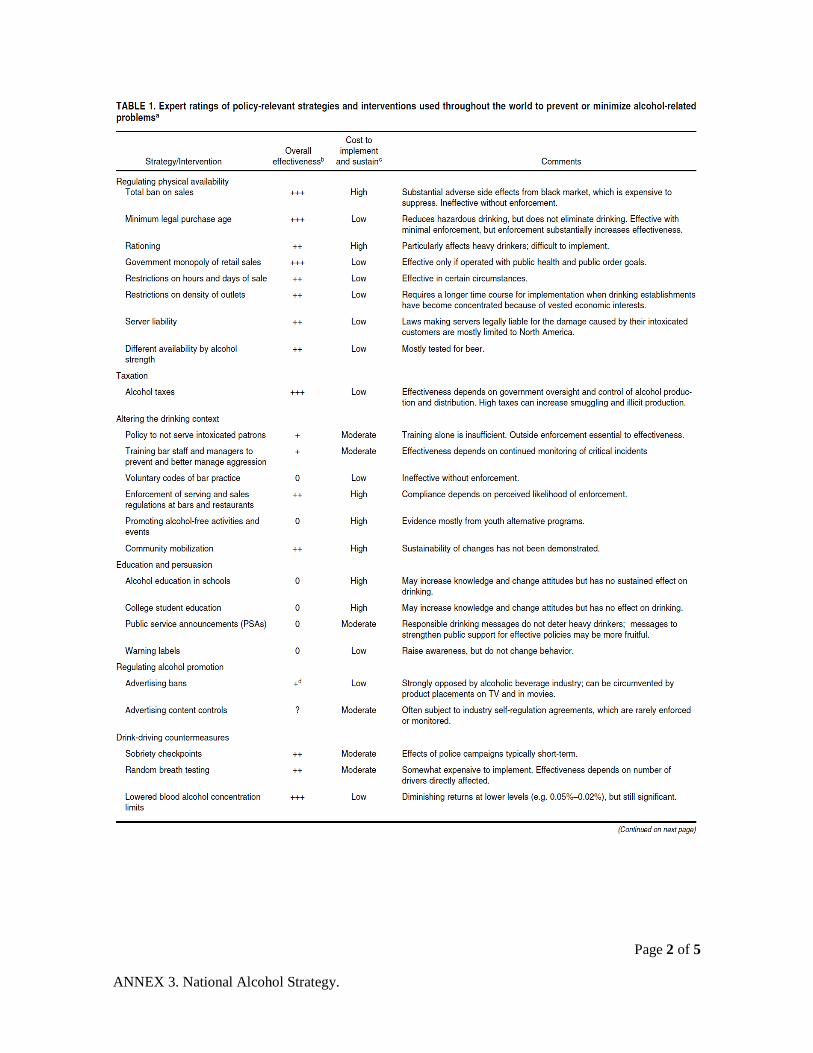
Page 2 of 5
ANNEX 3. National Alcohol Strategy.
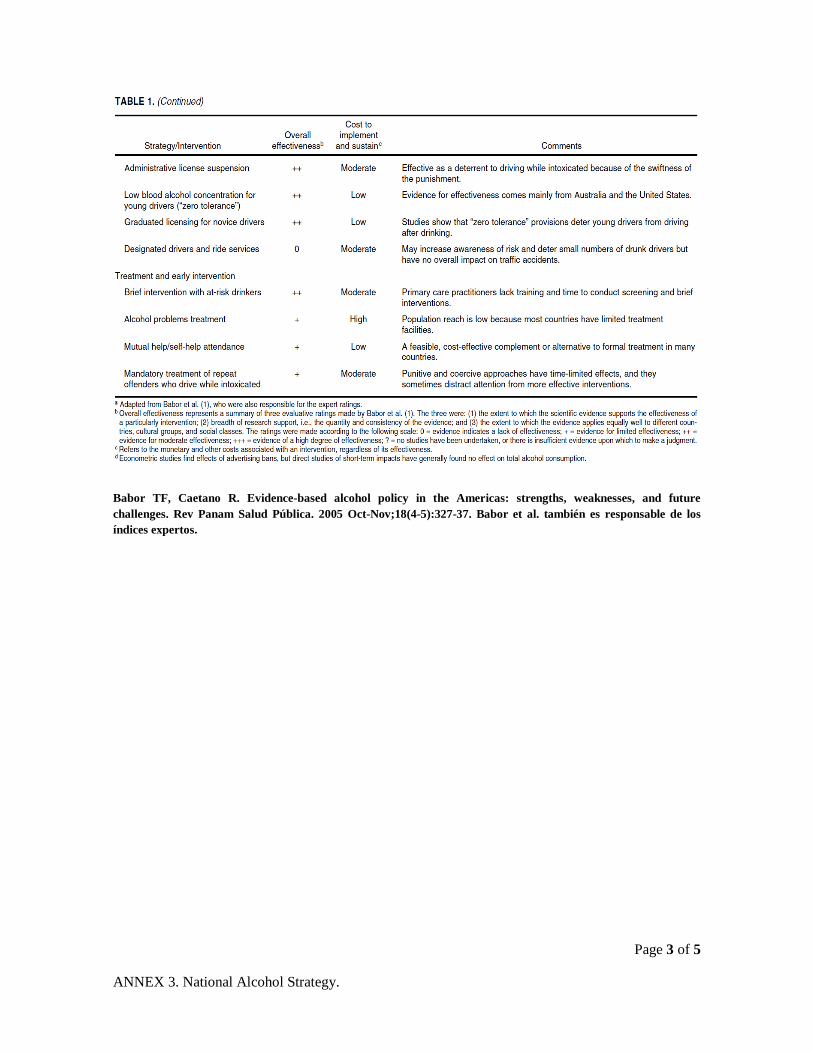
Page 3 of 5
ANNEX 3. National Alcohol Strategy.
Babor TF, Caetano R. Evidence-based alcohol policy in the Americas: strengths, weaknesses, and future challenges. Rev Panam Salud Pública. 2005 Oct-Nov;18(4-5):327-37. Babor et al. también es responsable de los índices expertos.
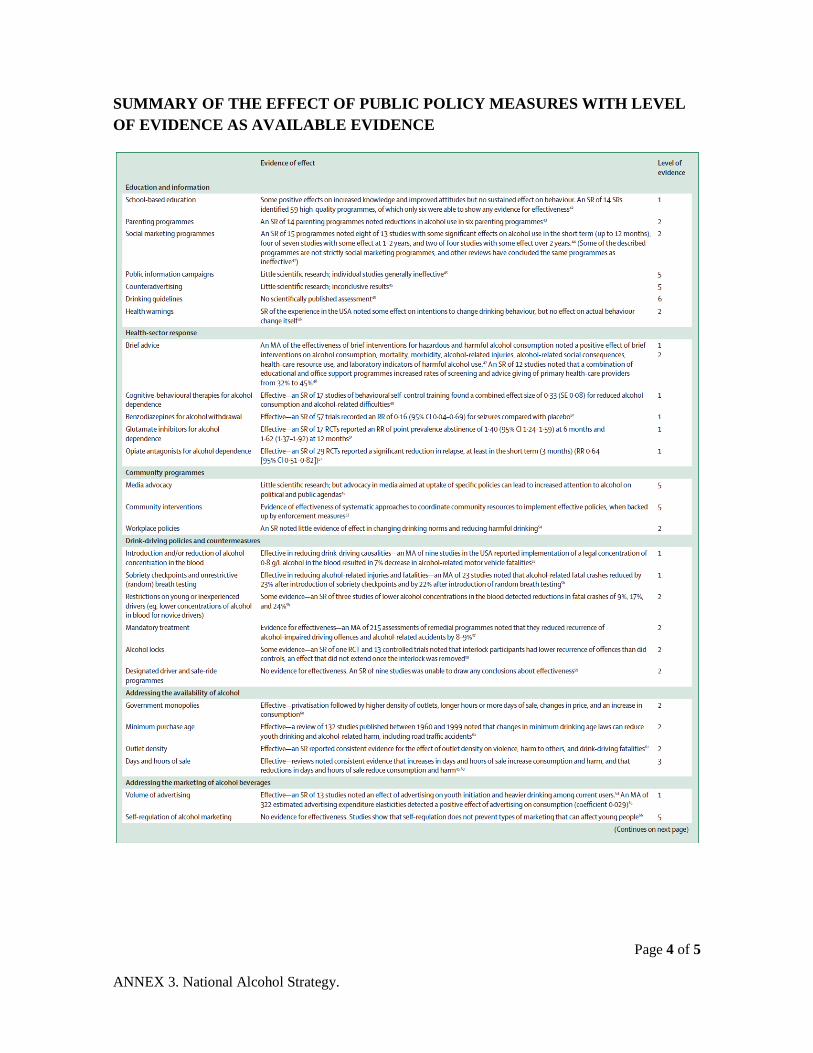
Page 4 of 5
ANNEX 3. National Alcohol Strategy.
SUMMARY OF THE EFFECT OF PUBLIC POLICY MEASURES WITH LEVEL OF EVIDENCE AS AVAILABLE EVIDENCE
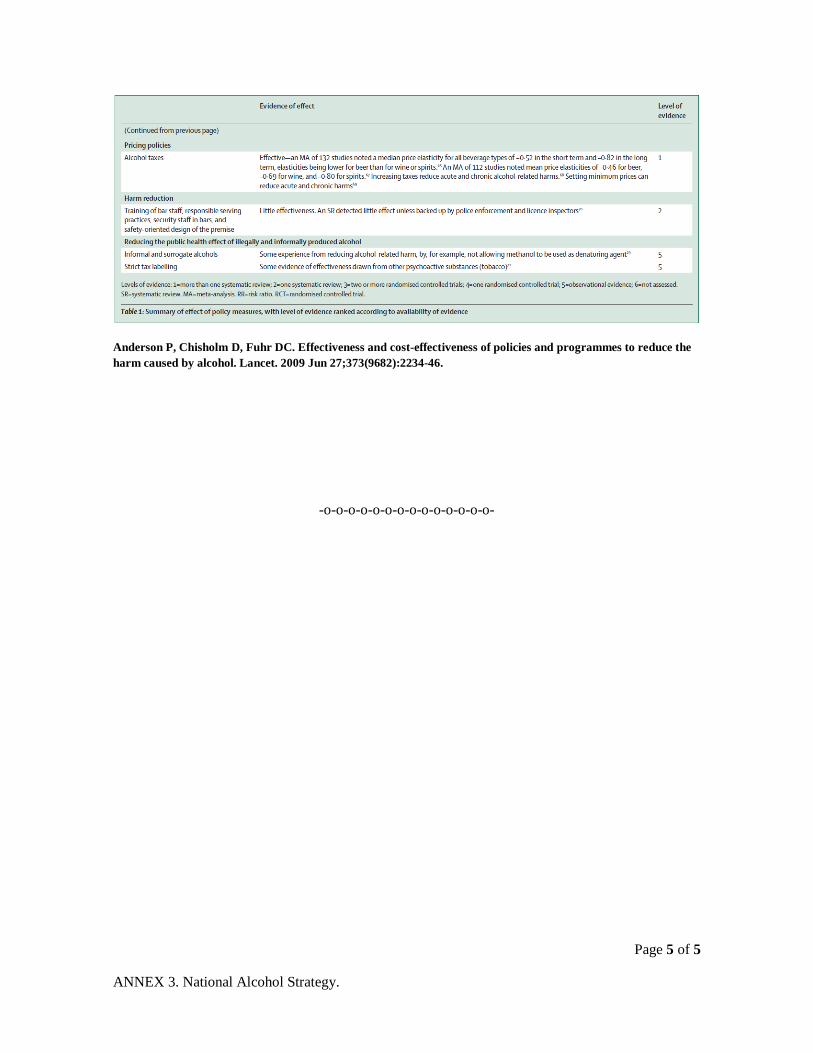
Page 5 of 5
ANNEX 3. National Alcohol Strategy.
Anderson P, Chisholm D, Fuhr DC. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet. 2009 Jun 27;373(9682):2234-46.
-o-o-o-o-o-o-o-o-o-o-o-o-o-o-
Page 1 of 11
ANNEX 4. National Alcohol Strategy
ANNEX 4
SUMMARY OF SPECIFIC NATIONAL AND
PROVINCIAL STRATEGIES (*)
a) Canada .................................................................................................................................2
b) British Columbia, Canada .....................................................................................................2
c) Nova Scotia, Canada .............................................................................................................4
d) Spain ....................................................................................................................................5
f) Australia ................................................................................................................................5
g) New Zealand .........................................................................................................................6
h) Inglaterra ..............................................................................................................................6
General View of the Alcohol Strategies, by country .................. ¡Error! Marcador no definido.
References .............................................................................................................................11
(*) by Norman Giesbrecht
Page 2 of 11
ANNEX 4. National Alcohol Strategy
The policies summarized here are not a comprehensive list of jurisdictions that have alcohol strategies, but rather, an illustrative collection. At the end of the annex, there is a table summarizing the current state of policy, noted above, in regions and countries, specifically in the areas and issues where there is evidence of effectiveness based on Babor et al. (2003).
a) Canada This summary is based on Thomas (2004) and the National Alcohol Strategy Working Group, 2007).
In 2002 alcohol related harms cost $14.6 billions or $463 for every living Canadian (Rehm et al. 2006b). Alcohol is one of the top three risk factors contributing to burden of disease, disability and death, 14% of the Canadians are high-risk drinkers, consumption levels has increased from 7.2 litres of absolute alcohol in 1997 to 7.9 per capita in 2004. The physical availability has been relaxed in recent years. Enforcement of regulations on liquor sales, however, is an ongoing issue in all provinces
The National Alcohol Strategy (NAS) was developed in recent years and document was made available in 2007. The main purposes are as follows: to develop a culture of moderation and responsibility in alcohol consumption and; to reduce the harms associated with alcohol misuse. It combines population level approaches and targeted interventions.
The document makes 41 recommendations in four areas of action:
1) Health promotion, prevention and education: to raise public awareness about responsible alcohol use and to enhance a culture of moderation through the understanding of what constitute a sensible drinking among population and the development and promotion of the national drinking guidelines);
2) to reduce health impacts and treatment through the expansion of screening measures, brief interventions and referrals by health professionals for people in risk or with alcohol-related problems and continuously address the contribution of alcohol to chronic diseases;
3) to better manage the availability of alcohol (liquor control boards, liquor licensing, minimum purchase age, taxation, prices (to control prices that discourage heavy drinking and maintain prices according to inflation, and advertising controls (to monitor, to ensure compliance), and;
4) to create safer communities and safer drinking environments.
Page 3 of 11
ANNEX 4. National Alcohol Strategy
b) British Columbia, Canada The recent report by Kendall et. al. (2008) is a revised and expanded version of an earlier report (Provincial Officer of Health (2002). British Columbia is the western most of Canada’s provinces, is the third most populated of the country. In 2002 the provincial government made some changes to the alcohol policy with the purpose of increase access to alcohol beverages and in that context the Provincial Health Officer recommended to monitor closely the possible impacts of those modifications and two reports has been released as a result of that suggestion. The last one titled “Public Health Approach to Alcohol Policy” (Kendall, 2008) reviews in detail levels and patterns of alcohol consumption in British Columbia (BC), rates and trends of alcohol related harms, the current cost-benefit profile of alcohol in the province and, the current alcohol policies in relation with best practice policies.
Since 2002 when the policy changes were implemented, there has been an increase in the number of retail liquor stores with the private stores showing the highest growth. The numbers of places that serve alcohol between 2003/2004 and 2007/2008 are positively and significant associated with consumption (Stockwell, Zhao, Macdonald, Pakula & Gruenland, 2008, cited in Kendall et. al., 2008).
Per capita consumption trend in BC (8.8 liters per person aged 15+ per year) is steadily increasing since 2002 and is still above then the national levels (8.1). It is noted that 44% of the population age 15 and older reported drinking at least weekly, and was the third highest percentage among the provinces in 2004. Self-reported rates of risky drinking at least monthly have increased since 2003.
Alcohol-related mortality rates continue to be stable among 2001-2006 but morbidity rates have increased 3.3% among 2002-2007, including number of hospitalizations and alcohol-involved road trauma. Although it is hard to estimate precisely the social and the economic costs and benefits related to alcohol, the authors suggest that the costs exceed the benefits in the health and economic sphere.
The main goals of the alcohol strategy in BC are to minimize alcohol related harms and lower costs and, maximize social and economic benefits. It has a combination of a population approach and one focusing on specific group targets.
The policy suggestions are directed to reinforce or restrict the current laws, specifically the ones related to economic and physical availability and drinking and driving, which are considered ones of the most cost-effective (Babor et al. 2003) such as limit the number of retail stores, density, hours of sales, prices and taxation and to improve drinking and driving measures. Also, the BC document refers to increasing capacity for routine screening, brief interventions and referrals; controlling alcohol advertising in quantity and quality; to improve the collection data on alcohol-involved morbidity and mortality; to create a small hard reduction levy on alcohol products with high alcohol content and; create programs to reduce violence around licensed establishments

Page 4 of 11
ANNEX 4. National Alcohol Strategy
There is also an emphasis on encouraging preventive strategies for target groups, such as youth and pregnant women. And finally, the report recommends support for a continuous monitoring arrangement.
c) Nova Scotia, Canada Nova Scotia is on the Atlantic Ocean, at the east side of Canada. In 2007 the Department of Health, Promotion and Protection developed and alcohol strategy for that province.
Since 2001, there has been a significant increase in the density of locations and the hours available in which to purchase alcohol. From 1999-2004, per capita consumption, aged 15+, in NS was slightly lower than the overall Canadian rate (7.57 and 7.76 liters respectively). However, there’s a 5.4% increase in per capita consumption between 2001 and 2005. It is noted that 23.4% of current drinkers in Nova Scotia exceeded low risk drinking guidelines designed to avoid acute and chronic alcohol related harms (developed by CAMH in Ontario) -- young adults followed by adolescents (15-19 years) had the highest rate of non-compliance.
The reports indicates that 76.1% of Nova Scotians of 15 years old and over drinking in the past 12 months. Mean age at onset of drinking is 18.2 years, 4.8% of all respondents consume +4 times per week, 43.5% in the past 12 months drank heavily at one sitting (5+ males or 4+ women) and, 7.1% weekly. Just 5.8% of the respondents consumed 8+ drinks in the past 12 months. 13.8% are hazardous drinkers with 3 times as many males drinking at these rates than females (22.5% versus 6.1%), most likely between 19-24 years (39.1%). Hazardous drinkers started consuming at a younger age (16), typically drank more at a single sitting (6.2 vs. 2.4) and over one third consuming more than 8 drinks at the same time against 1.6 among low risk consumers. The main reason to consume alcohol is to be sociable (80.3%), 87.5% most often location is at home, 57.2% drink in social situations (Schrans et al., 2008).
In 2002, per capita health, social and economic alcohol cost was $443 – 3rd lowest in Canada (Nunavut had the highest per capita costs for alcohol at $961 and Prince Edward Island the lowest at $385 – national average $463) (Nova Scotia Health Promotion and Protection, April 2006). For the five-year period 1999-2003, about 3000 hospital admissions a year can be attributed to alcohol use in Nova Scotia, with men twice as likely as women to be admitted for alcohol use. During the same time period, 1,149 deaths can be attributed to alcohol use (Graham, 2005).
“Changing the culture of alcohol use in Nova Scotia” constitutes a new alcohol strategy proposed by Addiction Services of the Department of Health Promotion and Protection. The main purpose of the strategy is reduce alcohol-related harms and costs and to do so by supporting a culture of moderation. In order to achieve its goal, the strategy proposes several key directions: Community capacity and partnership building; communication and social marketing; strengthening prevention, early intervention, and treatment; and, promoting research and evaluation.

Page 5 of 11
ANNEX 4. National Alcohol Strategy
The strategy has a health promotion and a balanced approach, which consider a balance between health protection, harm prevention, health benefits of moderation and costs and benefits to the economy. It is also population-based and concurrently focuses on under age drinkers, high-risk drinkers, alcohol consumption while pregnant and drinking and driving.
The main characteristics of this strategy are the focus on the cultural role of the alcohol as a tool to shift attitudes and harm-related behaviors. The shared responsibility between community and authorities related to health promotion and harm reduction is a central theme. The document proposes to set policies at a local level and then moving toward provincial and federal levels. This strategy encourages starting with education and early intervention and treatment, and also building support for, encouraging enforcement, and monitor best practices related to physical availability of alcohol and drinking-driving measures.
d) Spain Several resources were used in developing a brief snapshot of the situation in Spain including two World Health Organization reports (WHO, 2004; WHO Regional Office for EU, 2007)
There is not a national action plan on alcohol in Spain, just a national drug strategy 2005-2008.
Consumption was 9.9 liters in 2003 per capita consumption (i.e. total population, not aged 15+). Spain has highly developed drinking-driving campaigns, and moderately developed school based and local community programs. Health warning labels on bottles are required. There are not extensive training programs for primary health care; however, there are treatments for hazardous and harmful drinking and in non-governmental organizations too.
There is a prohibition of TV advertisements featuring beverages of >20º of alcohol content. Brief interventions are offered at emergency services and community interventions at local levels, programs for addicted pregnant women and programs that teach life skills. Treatment and rehabilitation of high-risk drinkers is provided via the national health system. There are server trainings at local levels. There is a voluntary arrangement for health warning labels. There are national information campaigns involving all media about alcohol’s impact on health, for prevention of alcohol consumption and of traffic safety.
f) Australia The following synopsis is based on the Ministerial Council on Drug Strategy (2006). A key issue is controlling intoxication. Many strategies are directed to encourage compliance to licensing laws in retail and serving alcohol places, enhance measures that encourage responsible service of alcohol and measures that increase community awareness of impacts of intoxication through labeling products and promoting alcohol guidelines. The goal of the Australian strategy is to prevent and minimize alcohol-relatd harm to individuals, families and communities in the context of developing safer and healthy drinking cultures in Australia.

Page 6 of 11
ANNEX 4. National Alcohol Strategy
Furthermore there are initiatives to identify licensed premises that may be serving alcohol irresponsibly. Queensland Police Party-Safe Program: provides practical tips to assist in holding successful, enjoyable and safe parties for everyone concerned including parents, hosts and guests. There is also a Party-Safe registration form so that party hosts can register their party with the local police.
g) New Zealand The National Alcohol Strategy is positioned under the New Zealand Health Strategy and the National Drug Policy, the first one identifies key priority health areas and the second one identifies the desired outcomes related to drug-related harm. In 1996, the government released a national policy statement on alcohol that intended to reduce or prevent alcohol-related harms.
Since the introduction of a Sale of Liquor Act 1989, there has been an increase of the physical availability of alcohol including, the number of liquor licenses, the range of places from which alcohol could be sold, the days and hours of sales (including Sundays), and also a decrease on the age of purchase (18 years old).
The strategy has several pillars.
• Supply control: Provide clear, comprehensible information on the provisions of the Act to persons responsible for administering it. Support intersect oral groups at a local level to monitor compliance with the Sale of Liquor Act, to actively enforce laws related to minimum age of purchase, measures to sale and supply alcohol to intoxicated patrons
• Demand reduction
• Problem limitation strategies
The total direct and indirect costs of alcohol misuse in New Zealand have been estimated as being between $1.5 billion and $2.4 billion (Devlin et al 1996). In 1982-83 the level of consumption per capita reached a historical high level of almost 12 litres per person aged 15 and older, and was declining steadily since then to 8.3 in 1997. New Zealand is ranked 20th in the world in terms of per capita alcohol consumption, one place below Australia, and one above the United Kingdom
h) England There have been other jurisdictions where there has been attention to alcohol policy issues in recent years, and in some cases this has followed on initiatives to several decades of increasing access to alcohol concurrent with an increase in trauma, social problems and chronic disease related to alcohol use.
Page 7 of 11
ANNEX 4. National Alcohol Strategy
For example, in England, on 5 June 2007, the Department of Health (DH) and the Home Office jointly issued a government strategy on alcohol which is a revision and updating of the Alcohol Harm Reduction Strategy for England ("Harm Reduction Strategy for England"), published in the year 2004 (ENGLAND 2007).
In England 90% of adults drink alcohol and only 13% of drinkers said that they kept a check on the number of units they drink. In 2003 per capita consumption was estimated in 9.29 liters of pure alcohol. The proportion of young people drinking has declined in recent years, but those who do drink are consuming more alcohol, more often. Excessive drinking costs more over 20 billion of euros each year. Alcohol-related deaths have more than doubled since 1979, with more people dying at a younger age. There are 180,000 alcohol-related hospital admissions per year. Violent crime has fallen 51% since 1995. In 2005/06 17% of all violent incidents were committed in or around pubs or clubs.
The strategy aim to reduce the harm caused by alcohol misuse through a program of joint government and industry action for:
• Better education and communication; using campaigns such as “know your limits” and “think” drinking and driving
• Improving health and treatment services; identifying and advising people in risk
• Combating alcohol-related crime and disorder and;
• Working with the alcohol industry: to include health information on bottles, to set up local partnerships schemes and to form an independent charity to promote sensible drinking.
England policy focuses on target groups or behaviors, especially underage drinking, 18-24 year old binge drinkers and harmful drinkers, alcohol-related violence and drinking and driving. Some of their successful strategies have been implemented at local levels, strengthening partnership between central and local authorities.
Some of the results of the national strategy are that new projects have increased levels in screening and intervention in primary health care. The campaign “know your limits” has successful raised awareness and has a high recall among young people. It has been claimed that “Think drink-driving” campaign contributed to the fall of death rate related to drinking and driving from more than 1,600 at the end of 1970 to 560 in 2005.
However, the UK approach to alcohol in the last decades has involved a number of developments that been considered to contribute to increasing risk and harm, rather than controlling damage. These have included a decline price of alcoholic beverages, extensive promotion and marketing, and increase in physical availability - including allowing 24-hour sales in off-premise and on-premise outlets. These are considered to be contributing factors in the high rates of liver cirrhosis mortality (Leon & McCambridge, 2006), and high rates of social disruption, drunkenness, property damage, and heavy drinking among youth (Heather, 2006; British Medical Association Board of

Page 8 of 11
ANNEX 4. National Alcohol Strategy
Science, 2008). Furthermore, attempts to control the dimensions of the strategy that were considered to lead to increased harm rather than reduce it, was confounded by the often close working relationship between the government and alcohol industries. This relationship was considered to contribute to rejection of evidence-based harm reduction policies in favour of those that would either be ineffective or increase drinking-related harm (Anderson, 2007).
.
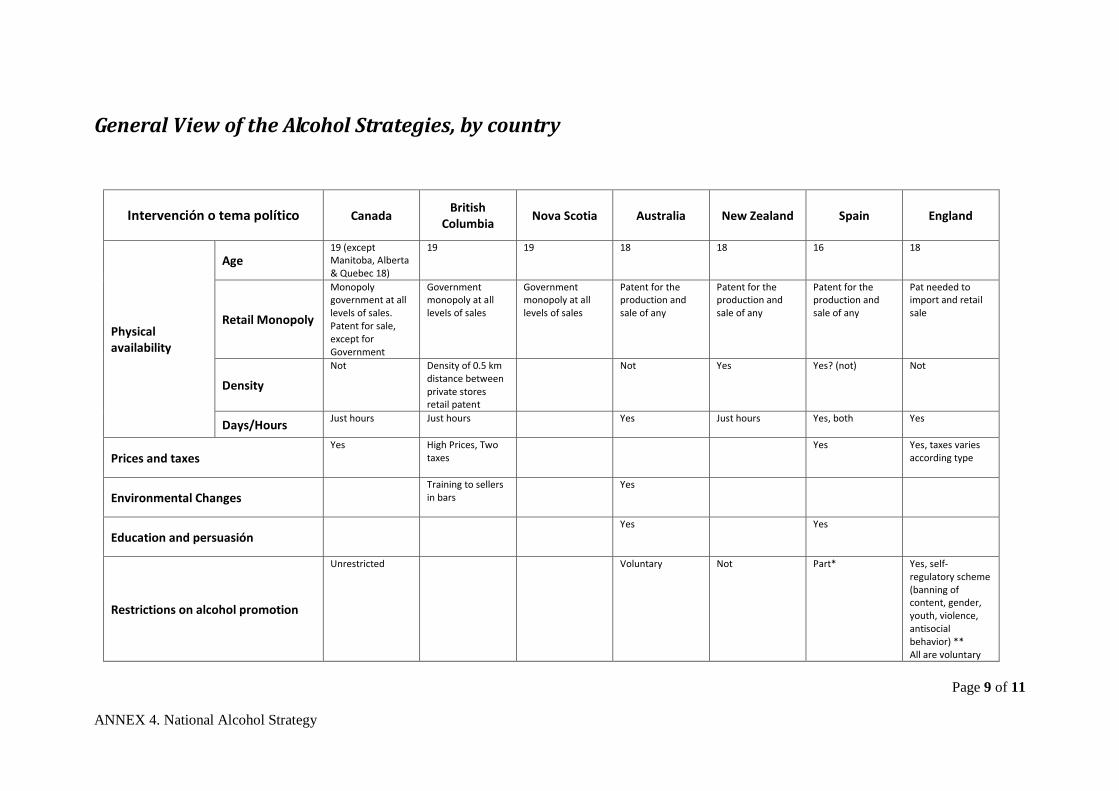
Page 9 of 11
ANNEX 4. National Alcohol Strategy
General View of the Alcohol Strategies, by country
Intervención o tema político Canada British
Columbia Nova Scotia Australia New Zealand Spain England
Physical availability
Age 19 (except Manitoba, Alberta & Quebec 18)
19 19 18 18 16 18
Retail Monopoly
Monopoly government at all levels of sales. Patent for sale, except for Government
Government monopoly at all levels of sales
Government monopoly at all levels of sales
Patent for the production and sale of any
Patent for the production and sale of any
Patent for the production and sale of any
Pat needed to import and retail sale
Density
Not Density of 0.5 km distance between private stores retail patent
Not Yes Yes? (not) Not
Days/Hours Just hours Just hours Yes Just hours
Yes, both Yes
Prices and taxes Yes
High Prices, Two taxes
Yes Yes, taxes varies according type
Environmental Changes Training to sellers
in bars
Yes
Education and persuasión
Yes
Yes
Restrictions on alcohol promotion
Unrestricted Voluntary Not Part* Yes, self-regulatory scheme (banning of content, gender, youth, violence, antisocial behavior) ** All are voluntary
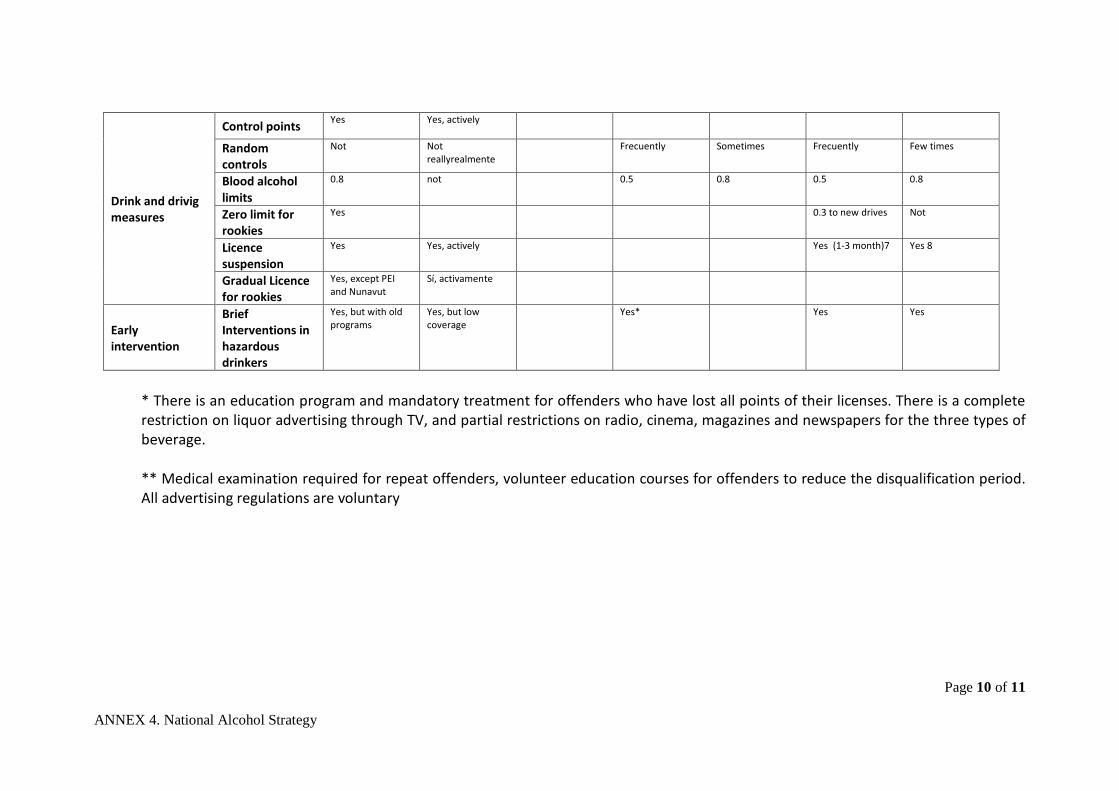
Page 10 of 11
ANNEX 4. National Alcohol Strategy
Drink and drivig measures
Control points Yes Yes, actively
Random controls
Not Not reallyrealmente
Frecuently Sometimes Frecuently Few times
Blood alcohol limits
0.8 not 0.5 0.8 0.5 0.8
Zero limit for rookies
Yes 0.3 to new drives Not
Licence suspension
Yes Yes, actively Yes (1-3 month)7 Yes 8
Gradual Licence for rookies
Yes, except PEI and Nunavut
Sí, activamente
Early intervention
Brief Interventions in hazardous drinkers
Yes, but with old programs
Yes, but low coverage
Yes* Yes Yes
* There is an education program and mandatory treatment for offenders who have lost all points of their licenses. There is a complete restriction on liquor advertising through TV, and partial restrictions on radio, cinema, magazines and newspapers for the three types of beverage. ** Medical examination required for repeat offenders, volunteer education courses for offenders to reduce the disqualification period. All advertising regulations are voluntary
Page 11 of 11
ANNEX 4. National Alcohol Strategy
References
(2006). The Costs of Substance Abuse in Canada 2002, Nova Scotia Health Promotion and
Protection. (2007). "National Strategy Working Group. Reducing alcohol related harm in Canada: Toward a
culture of moderation. Recommendations for a national alcohol strategy." Anderson, P. (2007). "A safe, sensible and social AHRSE: New Labour and alcohol policy."
AddictionAUSTRALIA (2006). National Alcohol Strategy 2006 - 2009. Towards Safer Drinking Cultures,
Ministerial Council on Drug Strategy.
102(10): 1515-21.
BMA (2008). Alcohol misuse: tackling the UK epidemic. London, Science and Education department of the Board of Science. British Medical Association Board of Science.
ENGLAND (2007). Safe. Sensible. Social. The next steps in the National Alcohol Strategy. London, Department of Health, Home Office, Department for Education and Skills and Department for Culture, Media and Sport.
Graham, L. (2005). Alcohol indicators report: A framework of alcohol indicators describing the consumption of use, patterns of use and alcohol-related harms in Nova Scotia. Province of Nova Scotia.
Heather, N. (2006). "Britain's alcohol problem and what the UK government is (and is not) doing about it." Adicciones
Kendall, P. (2008) "Public Health Approach to Alcohol Policy." Volume, DOI: 18(3): 225-235.
Leon, D. A. and J. McCambridge (2006). "Liver cirrhosis mortality rates in Britain, 1950 to 2002." Lancet
NEW-ZEALAND (2001 ). National Alcohol Strategy 2000–2003. Wellington, New Zealand, Alcohol Advisory Council of New Zealand and Ministry of Health
367(9511): 645.
Rehm, J., Baliunas D, Brochu S, Fischer B, Gnam W, Patra J et al. (2006). The Costs of Substance Abuse in Canada 2002: Highlights. Ottawa, Canadian Centre on Substance Abuse.
Thomas, G. (2004). Alcohol-related harms and control policy in Canada. Ottawa, Ontario, Canadian Centre on Substance Abuse: 1-38.
WHO-EUROPA (2007). EU Alcohol Strategy: Monitoring of Good Practices in EU-27 as of 1 January, World Health Organization Regional Office for Europe.
WHO (2004). Global Status Report: Alcohol Policy. Geneva, Switzerland, Department of Mental Health and Substance Abuse: World Health Organization.
-o-o-o-o-o-o-o-o-o-o-o-o-o-o-