-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
1/88
N A T I O N A L B R E A S T A N D C E R V I C A L C A N C E R E
A R L Y D E T E C T I O N P R O G R A M
detection
early
Summarizing the First 12 Years of Partnerships andProgress
Against Breast and Cervical Cancer
1 9 9 1 2 0 0 2 N A T I O N A L R E P O R T
U.S. Department of Health and Human Services
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
2/88
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
3/88
National Breast and Cervical CancerEarly Detection Program
19912002 National Report
A. Blythe Ryerson, MPH
Vicki B. Benard, PhDEpidemiology and Applied Research Branch
Anne C. Major
Program Services Branch
For additional copies of this report, please contact the
Centers for Disease Control and Prevention,
National Center for Chronic Disease Prevention and Health
Promotion
Division of Cancer Prevention and Control
Attn: Publications, Mail Stop K-64
4770 Buford Highway, N.E.
Atlanta GA 30341-3717
An electronic version of this report is available
athttp://www.cdc.gov/cancer/nbccedp/Reports/NationalReport/index.htm
All materials in this report are in the public domain and may be
reproduced or copiedwithout permission. However, citation of CDC as
the source is appreciated.
i 19912002 N A T I O N A L R E P O R T
http://www.cdc.gov/cancer/nbccedp/Reports/NationalReport/index.htmhttp://www.cdc.gov/cancer/nbccedp/Reports/NationalReport/index.htm
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
4/88
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
5/88
Table of Contents
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . iv
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . v
Executive Summary . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . vi
Overview of the NBCCEDP . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . 1History of the NBCCEDP . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . 4
Components of the NBCCEDP . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . 5
NBCCEDP Research and Evaluation . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. 9
Screening Results and Outcomes in the NBCCEDP . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9
Breast Cancer Screening. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . .10
Breast Cancer Screening Participation . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.10
Breast Cancer Screening Results . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.12
Breast Cancer Screening Diagnostic Follow-Up . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14
Breast Cancer Detection. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.14
Positive Predictive Value of Abnormal Mammograms . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . .17
Stage of Invasive Breast Cancer at Time of Diagnosis. . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
Cervical Cancer Screening . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. .18
Cervical Cancer Screening Participation . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.19
Cervical Cancer Screening Results. . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
20
Cervical Precancer and Cancer Detection . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Positive Predictive Value of Abnormal Pap Tests . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23
Stage of Invasive Cervical Cancer at Time of Diagnosis . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Future Directions. . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . 25
Data Tables . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . 27
Appendix IThe Minimum Data Elements . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
67
Appendix IINBCCEDP Publications . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
70
Appendix IIIMethods. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . 73
Breast Cancer Screening Analysis . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
73
Cervical Cancer Screening Analysis . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.74
References. . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . .75
iii 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
6/88
AcknowledgmentsThe Centers for Disease Control and Prevention
(CDC) would like to acknowledge the following contributors:
The state, territorial, and American Indian/Alaska Native tribes
and tribal organizations that are part of theNational Breast and
Cervical Cancer Early Detection Program (NBCCEDP) for their
commitment to providinghigh-quality breast and cervical cancer
screening, follow-up, and treatment to women in underserved
populations throughout the United States.
Program and scientific staff from CDCs Division of Cancer
Prevention and Control for their early planningand promotion of
this report, including Vicki Benard, PhD; Donald Blackman, PhD;
Christie Eheman, PhD;Herschel Lawson, MD; Nancy C. Lee, MD; Janet
Royalty, MS; and Sandra F. Thames.
Information Management Services ( IMS)especially William Helsel,
MS; William Kammerer; ChristaAnderson; and William Howe, for their
assistance with this report and for their management of the
MinimumData Elements.
Program, scientific, and editorial staff from CDCs National
Center for Chronic Disease Prevention andHealth Promotion,
including Kevin T. Brady, MPH; Ralph Coates, PhD; Christie Eheman,
PhD; Linda G. Elsner;James Gardner, MSPH; Cherie Gray, MA; Judy
Hannan, RN, MPH; Herschel Lawson, MD; Kevin Moran;
Steven L. Reynolds, MPH; Phyllis Rochester, PhD; Janet Royalty,
MS; Florence Tangka, PhD; Susan True, MEd;and Mary White, ScD,
MPH.
Contributors to the development and editing of this report from
the NBCCEDP state, territorial, and tribalgrantees, including
Pamela W. Balmer, Illinois Department of Public Health; Dianah
Bradshaw, RN, MSHA,North Carolina Department of Health and Human
Services; Helena Calhoun, Illinois Department of PublicHealth;
Sherrell Holtshouser, MPH, RN, Alaska Department of Health and
Social Services; Bradley J. Hutton,MPH, New York State Department
of Health; Cheryl M. Jones, RN, Oklahoma State Department of
Health;Chris Knutson, MN, ANP, Alaska Department of Health and
Social Services; Nikki L. Lyttle, MS, WestVirginia Department of
Health and Human Resources; Lana Nelson, Kaw Nation of Oklahoma;
ConradOtterness, MPH, South Carolina Department of Health and
Environmental Control; and Hyral Smith, RN,
Iowa Tribe of Oklahoma. Palladian Partners, Inc., for their
graphics, layout, and design services.
All national and local partners of the NBCCEDP for their
continued support in increasing womens access toscreening and
treatment services, developing strategies for improving rescreening
rates, and implementingpublic education and outreach strategies to
reach NBCCEDP-eligible women in priority populations.
iv 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
7/88
ForewordBy Susan True, MEd, Director, NBCCEDP
The National Breast and Cervical Cancer Early Detection Program
(NBCCEDP), which was created in responseto the Breast and Cervical
Cancer Mortality Prevention Act passed by Congress in 1990, is both
the first andthus far the only national cancer screening program in
the United States. As a consequence, its successesand challenges
are relevant not only to those who manage, implement, and are
served by the program, but
to policy makers, the health care system, the public health
community, and the general public as well. CDC ispleased to offer
this summary of the accomplishments of the NBCCEDP from 19912002.
Through it the readermay gain insight into the complexity of this
program designed to improve the quality of breast and cervical
cancer screening and early detection services and assure access to
them for women who, for a variety of reasons,would otherwise not
receive these services.
Clients of the NBCCEDP have no health insurance that covers
screening, and little or no discretionary income;they often have no
medical home. They represent minority populations and those who are
geographically orculturally isolated from existing services. Most
are over 40 but not yet 65often working as well as caring
forgrandchildren or aging parentswith little social support or
scheduling flexibility. Educating and motivatingthese women to want
screening; ensuring that services are convenient, accessible, and
provided in a respect
ful, culturally competent manner; and effectively communicating
results, recalling, and assisting women whoneed additional services
are among the responsibilities of every funded program. Grantees
are held to highstandards for reporting services provided, their
appropriateness, timeliness, and outcomes. Quality
assurance,including provider education and the development of data
review processes to identify problems, is a criticalcomponent of
this work.
This report summarizes the first 12 years of the NBCCEDP. During
this period, the program grew from 8 to 68grantees and from serving
thousands to serving hundreds of thousands of women each year. Both
CDC andMedicare policy changes influenced which women were served,
and how they were served, during this periodThe program has had a
rich history, with many lessons assimilated into the way NBCCEDP is
managed, implemented, and evaluated today.
Perhaps even more exciting, however, is the programs future. A
strategic evaluation plan will guide our assessment of program
components and outcomes for the next 5 years. We are exploring the
impact of infrastructurechoices on grantees costs to deliver
services and their success in eliminating disparities among women
in theprogram. An evolving performance-based system for making
awards is ensuring that federal dollars are wellspent. By
strengthening partnerships with our sister federal programs,
private partners, and comprehensive cancer control programs, we are
ensuring an environment in which the NBCCEDP can increasingly be a
significantcatalyst for reducing the illness and death associated
with breast and cervical cancer in communities across theUnited
States.
This report demonstrates our growing capacity to accomplish that
goal. Future reports will update the data andshow the impact of our
performance improvement initiatives.
Susan True, MEd
v 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
8/88
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
9/88
Executive SummaryThe Division of Cancer Prevention and Control
at the Centers for Disease Control and Prevention is pleasedto
release the first programmatic summary report of the National
Breast and Cervical Cancer Early DetectionProgram (NBCCEDP). The
NBCCEDP helps low-income, uninsured, and underserved women gain
access topotentially lifesaving screening programs for the early
detection of breast and cervical cancer.
In 2004, an estimated 215,990 new cases of invasive breast
cancer and 10,520 new cases of invasive cervica
cancer will be diagnosed in the United States, and about 44,010
women will die of these diseases combined.1Many of these deaths
could be avoided by increasing the cancer screening rates among
women at risk. TheU.S. Preventive Services Task Force (USPSTF)
recommendations state that timely mammography screeningamong women
aged 40 years or older could prevent a significant number of all
deaths from breast cancer.2
Papanicolaou (Pap) tests can detect cervical cancer at an early
stage when it is most curable, and can preventthe disease
altogether when precancerous lesions are found during the test and
are treated in a timely manner.
Despite the availability of screening tests, deaths from breast
and cervical cancer occur more frequently amongwomen who are
uninsured or under-insured. Mammography and Pap tests are underused
by women who haveless than a high school education, are older, live
below the poverty level, or are members of certain racial andethnic
minority groups.3 To help improve access to breast and cervical
cancer screening among these at -risk
populations in the United States, Congress passed the Breast and
Cervical Cancer Mortality Prevention Actof 1990, which created the
NBCCEDP. The program, funded at $30 million in fiscal year (FY)
1991, eventually grew to a nationwide program that received over
$192 million in FY 2002. During this time, 1,175,759women received
2,038,118 mammograms, and 1,329,523 women received 2,305,936 Pap
tests through theNBCCEDP.
The intent of this report is to summarize the first 12 years of
the NBCCEDP, from 1991 through 2002.Information on the programs
framework and history are given in addition to data on breast and
cervicalcancer screening results and outcomes for women served
through the program. This report provides a basis forresearchers to
develop research questions that can be answered with more specific
and advanced analysesusing both the national and program-specific
data. Individual programs can use these data to help guide
activities to improve program management, evaluation, data
management, and outreach activities.
The NBCCEDPs comprehensive approach to breast and cervical
cancer control ensures that not only medicallyunderserved women
benefit from this early detection effort, but that all women gain
from the educational activities, public and private partnerships,
and quality assurance standards implemented in our funded
programs.At the state and community level, the development of early
detection programs has resulted in a new organizational capacity
and infrastructure for cancer control, increased staff resources
and expertise, enabled multiplecollaborative partnerships in the
private and public sectors, built state and community coalitions,
and promoteda greater understanding of the challenges in delivering
preventive health services to women who are medicallyunderserved.
By presenting this report, the NBCCEDP hopes to demonstrate the
continued momentum and commitment of federal and state governments
to comprehensive screening programs that work to close the gap
inhealth disparities, improve early detection rates, and reduce the
illness and death from all cancers.
vii 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
10/88
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
11/88
Overview ofthe NBCCEDP
Early detection throughscreening is our best
defense against morbidity
and mortality from breastand cervical cancers andprecancers.
Julie Louise Gerberding, MD, MPHDirector, Centers for Disease
Control
and Prevention
The National Breast andCervical Cancer EarlyDetection
Program
(NBCCEDP) is a nationwide,comprehensive public healthprogram
that helps uninsured andunderserved women gain accessto screening
services for the earlydetection of breast and cervicalcancer.
Breast cancer is the most commonly diagnosed cancer and
thesecond leading cause of cancer
death among women in the UnitedStates.1 Screening for and
earlydetection of breast and cervical cancer reduces death ratesand
greatly improves cancerpatients survival.2 However, thereis a
disproportionately low rate ofscreening among women of
certainracial and ethnic minorities andamong under- or uninsured
women,which creates a wide gap in health
outcomes between such womenand other women in the UnitedStates.3
To address this healthdisparity, Congress authorized theNBCCEDP in
1990, giving CDCthe ability to implement a nationalstrategic effort
to increase access tomammography and Pap test screenings for women
in need.
The NBCCEDP is implementedthrough cooperative agreementswith
state and territorial healthdepartments, tribes, and
tribalorganizations (grantees). Sixtypercent of federal funds
receivedby a grantee must be expendedon direct services for
women.
The other 40% of federal fundscan be used to support
programmanagement, public and providereducation, quality assurance,
andsurveillance and evaluation activities. The NBCCEDP is
intendedto be the payer of last resort forscreening services;
therefore, grantmonies cannot be used to pay forservices if other
coverage is available through any state fund, private
health insurance, or other government health benefits
programsuch as Medicaid or Medicare.Grantees are also required to
contribute $1 for every $3 of federalfunds. Grantees contract with
abroad range of provider agencies to deliver screening and
otherservices, and each grantee hasdeveloped its own delivery
systembased on available resources.
The NBCCEDP is directed to low-income, uninsured women aged1864
from priority populations.The program provides clinical
breastexaminations, mammograms, andPap tests for eligible women
whoparticipate in the program as well asdiagnostic testing for
women whosescreening outcome is abnormal.Although treatment
services are not
directly paid for by the NBCCEDP,programs have always
beenrequired to identify resources forthe treatment of breast and
cervicalcancer found through the program.To assist programs in
identifyingthese resources, in 2000 Congressgave the states the
option to providemedical assistance for treatmentthrough Medicaid
(PL 106-354). Inaddition to screening and diagnostic
services, the legislation authorizingthe NBCCEDP (PL 101-354)
pro-vided for public and professionaleducation, quality assurance,
and
1 19912002 N A T I O N A L R E P O R T
surveillance and evaluation systemsto monitor program
activities. Eachgrantee reports to CDC a subsetof program data
known as the
minimum data elements (MDEs).The MDEs are a set of standardized
data elements considered tobe minimally necessary for granteesand
CDC to monitor client demographics and clinical outcomes ofwomen
screened with NBCCEDPfunds. The MDEs also are usedto establish
NBCCEDP policiesand practices, assess the nationalprograms
screening outcomes, and
respond to the information needsof CDC stakeholders and
partners.A description of the MDEs can befound inAppendix I.
Since the NBCCEDP began in1991, CDC has expanded theprogram to
all 50 states, 4 U.S.territories, the District of Columbia,and 13
American Indian/AlaskaNative tribes or organizations.
Through the hard work of dedicated national partners,
statehealth officials, community leaders, medical care providers,
andothers involved in the program,the NBCCEDP has provided morethan
4 million breast and cervicalcancer screening and diagnostictests
to almost 1.75 million low-income, uninsured women. From1991
through 2002, 1,175,759
women have received 2,038,118mammograms, and 1,329,523women have
received 2,305,936Pap tests through the NBCCEDP(Figures 14).
Because of thesescreenings, 9,956 cases of breastcancer, 12,187
cases of precancerous cervical lesions, and 832 casesof invasive
cervical cancer werediagnosed.
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
12/88
Figure 1. Number of Women Receiving Mammograms Through the
NBCCEDP, 19912002*
300,000
Women returning for at least one subsequent program mammogram
Women receiving a first program mammogram
9,309
494
250,000
135,268
men 200,000 130,769
90,392
rofWo 116,803101,421
66,047 90,808
150,00043,305e
Numb
100,000 25,288149,469
134,806127,622 119,584 121,364102,309 118,453 118,084
50,000 78,26067,82637,982
0 1991/ 1993 1994 1995 1996 1997 1998 1999 2000 2001
20021992
Calendar Year
*During this period, 1,175,759 women received at least one paid
mammogram through the NBCCEDP.
Figure 2. Number of Mammography Screenings Provided Through the
NBCCEDP, 19912002*
300,000
250,000
200,000
150,000
100,000
50,000
0
292,601dediv 260,119or 242,048P 230,504 227,544s 214,877ma
198,193rgomm 148,896a
ofM
105,940
re 78,527
Numb
38,869
1991/ 1993 1994 1995 1996 1997 1998 1999 2000 2001 20021992
Calendar Year
*During this period, 2,038,118 mammograms were paid for directly
with program funds, and 309,229 unpaid mammograms wereprovided to
women receiving at least one other NBCCEDP-funded service.
2 19 9 1 2 0 0 2 N AT I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
13/88
Figure 3. Number of Women Receiving Pap Tests Through the
NBCCEDP, 19912002*
300,000
men
250,000
rofWo200,000
e 150,000
Numb
100,000
50,000
0
Women returning for at least one subsequent program Pap test
Women receiving a first program Pap test
130,222
128,86195,52375,268 120,421107,567
97,304
55,674
15,79438,335
150,9662,234 137,364 129,002 131,813 136,955
142,799121,965119,516
98,069 100,466
60,608
1991/ 1993 1994 1995 1996 1997 1998 1999 2000 2001 20021992
Calendar Year
*During this period, 1,329,523 women received at least one paid
Pap test through the NBCCEDP.
Figure 4. Number of Pap Test Screenings Provided Through the
NBCCEDP, 19912002*
300,000
250,000
200,000
150,000
100,000
50,000
0
291,966284,591
269,754de 250,699div 236,120 229,158o 225,015rsPst 184,888
apTe
147,531
ofP
120,574
re
Numb
65,640
1991/ 1993 1994 1995 1996 1997 1998 1999 2000 2001 20021992
Calendar Year
*During this period, 2,305,936 Pap tests were paid for directly
with program funds, and 85,783 unpaid Pap tests were provided
towomen receiving at least one other NBCCEDP-funded service.
3 19 9 1 2 0 0 2 N AT I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
14/88
History of theNBCCEDPBegi
ildi
l lic)
ll
Nati i
i li l
i ( lic)
l )
2000
( l )
l
i lf ( l )
1991
nning of the NBCCEDP
1992
Implementation of the Capacity Bu ng
Program
1993
Amendment of the Breast and CervicalMorta ity Prevention Act of
1990 (PubLaw 103-183
1996
Estab ishment of mammography ageguide ines
1997
onw de expansion of the NBCCEDP
1998
Exclusion of Med care-e gib e women
Passage of Womens Health Research and
Prevent on Amendments of 1998 PubLaw 105-340
1999
Passage of Balanced Budget RefinementAct of 1999 (Pub ic Law
106-113
Implementation of Breast and CervicalCancer Prevention and
Treatment Act of2000 Pub ic Law 106-354
Cervical cancer screening po icy change
2001
Passage of Native American Breast andCervical Cancer Treatment
Techn caAmendment Act o 2001 Pubic Law 107-121
Prior to 1990, CDCs Division ofCancer Prevention and Control
laidthe groundwork for building earlydetection programs by funding
a
few states to work on the designand implementation of breast
andcervical cancer screening services for medically
underservedwomen. In part through the advocacy of CDCs national
partners,Congress recognized the importance of establishing a
nationwideprogram and passed the Breastand Cervical Cancer
MortalityPrevention Act of 1990. This
landmark legislation authorizedCDC to establish the
NationalBreast and Cervical CancerEarly Detection Program(NBCCEDP).
To begin the effort,Congress appropriated $30 million in fiscal
year (FY) 1991 tofund efforts by the first eight statesto establish
early detection programs. Early lessons showing thatindividual
programs needed more
time for capacity building led tothe development of a
two-stagefunding process. The CapacityBuilding Program offered
granteesthe opportunity to recruit personneland design service
delivery. Afterthey developed their infrastructure,grantees were
funded through acompetitive application process tobegin screening
women primarilyfrom low-income, under- or unin
sured, and racial or ethnic minoritygroups. Since then, the
NBCCEDPhas experienced substantial growthand a number of
legislative andpolicy changes.
1991Beginning of theNBCCEDP. CDC funded eightstates in fiscal
year (FY) 91 andadded four more in FY 92.
1992Implementationof the Capacity BuildingProgram. CDC funded
anadditional 18 states to developthe infrastructure necessary
todeliver screening programs.
1993Amendment of
the Breast and CervicalMortality PreventionAct of 1990 (Public
Law103-183). This amendmentauthorized NBCCEDP fundingfor American
Indian/AlaskaNative tribes and tribal organizations and required
CDC togive funding priority to thosestates with a high
diseaseburden from breast or cervical
cancer. 1996Establishment
of mammography ageguidelines. The NBCCEDPestablished a goal that
75% offederally funded mammogramsbe provided to women 50 yearsof
age or older.
1997Nationwide expansion of the NBCCEDP.
Funding was provided to 50states, the District of Columbia,5
territories, and 13 tribes ortribal organizations.
1998Exclusion ofMedicare-eligible women.As a result of Medicare
adding these cancer screeningservices under the Part B coverage
option, women enrolled in
MedicarePart B were excludedfrom the
NBCCEDP-eligiblepopulation.
1998Passage of WomensHealth Research andPrevention Amendments
of1998 (Public Law 105-340).Congress allowed the NBCCEDPto add case
management asa program component and
4 19 9 1 2 0 0 2 N AT I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
15/88
enabled program grantees tocontract with for-profit
entities.
1999Passage ofBalanced BudgetRefinement Act of 1999(Public Law
106-113).Congress allowed the NBCCEDP
to raise the reimbursementrate for Pap tests from $7.15 to$14.60
and to adjust the rateannually for inflation.
2000Implementation ofBreast and Cervical CancerPrevention and
Treatment
Act of 2000 (Public Law106-354). Congress gavestates the option
to providemedical assistance throughMedicaid to eligible womenwho
were screened and foundto need treatment for breast orcervical
cancer or precancerousconditions.
2000Cervical cancerscreening policy change.NBCCEDP grantees
wereencouraged to focus cervicalcancer screening on women
who had rarely or never beenscreened and to decrease
over-screening of women enrolled inthe program.
2001Passage of NativeAmerican Breast andCervical Cancer
TreatmentTechnical Amendment Actof 2001 (Public Law 107121).
Congress amended Title
XIX of the Social Security Act toclarify that Indian women
withbreast or cervical cancer whoare eligible for health
servicesprovided under a medical careprogram of the Indian
HealthService or of a tribal organization should be included in
theoptional Medicaid eligibility category of breast or cervical
cancerpatients added by the Breast and
Cervical Cancer Prevention andTreatment Act of 2000.
As a result of the extensive systemof data collection, analysis,
andongoing communication with grantees, the NBCCEDP has
successfullyenacted modifications to improve
the programs structure and to moreclosely define those eligible
forscreening services. The changesthat have had the most impact
onthe program were the issuanceof mammography guidelines in1996,
which required that 75% ofprogram-paid mammograms beprovided to
women 50 years ofage and older, and the exclusion
ofMedicare-eligible women in 1998,
which resulted in a temporarydecrease in the number of
womenreceiving screening servicesthrough the NBCCEDP (Figures14).
The program establishedother specific policies not listedabove that
have had the cumulative effect of focusing the deliveryof services
on women most likelyto be rarely or never screened andthose at or
below 250% of the
poverty level.4
Through the hardwork of those at state and territorial health
departments, tribes, andtribal organizations, and with
theassistance of national, voluntary,and private organizations,
theNBCCEDP has grown significantlyand is now filling a critical gap
inthe screening for and early detection of breast and cervical
cancerin the United States.
Components ofthe NBCCEDPBreast cancer and cervical cancerare two
very distinct diseases andrequire markedly different methods for
their detection, diagnosis,and treatment. For breast cancer,
a combination of clinical breastexamination (CBE) and
mammography can generally detect anabnormality at an early stage
ofthe disease. For cervical cancer,Pap tests can detect
precancerous lesions years before invasivecancer becomes apparent.
While
these screening services are key toearly detection of breast and
cervical cancer, their existence alone isnot sufficient to achieve
a reductionin the illness and death associatedwith these diseases.
Other activitiesmust also occur to support directscreening
services. The NBCCEDPhas eight major components.
Program Management
The overarching goal of programmanagement is to implement
allprogram components in accordance with established policiesand
procedures; to identify andleverage resources; and to provide
leadership in planning,coordination, implementation, andevaluation.
Program managers arerequired to
Establish a sound fiscal systemthat tracks and monitors program
expenditures.
Develop an accurate budgetrequest that corresponds with
theprograms work plan.
Recruit and develop a qualifiedand technically diverse
staff.
Develop an annual work plancontaining specific,
measurable,time-phased, and realistic goalsbased on a thorough
understanding of program components.
Evaluation
The NBCCEDP defines evaluationas the systematic documentationof
the operations and outcomes
5 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
16/88
of a program and the compari
son of these results with a set ofexplicit standards or
objectives.Evaluation activities must becarefully planned and
implemented to ensure that programdata are credible and useful.
Thisinformation is critical to guidingoperations and ensuring
programsuccess.
NBCCEDP Conceptual Framework
at
Daa M nagement
ya
Qulit Assurance
Q tu enalityImprove
m
Program Management
Results
Professional Screening &Development
DiagnosticPartnerships Services
Case ManagementTracking
Recruitment Follow-upPublic EducationOutreachInreach
Healthy Women
Evaluation
Partnerships
Partnerships are critical to theNBCCEDP cancer control efforts.A
successful national program tocontrol breast and cervical
cancerdepends on the involvement of avariety of committed partners
atthe local, state, and national levels. Such partners help
strengthenand maintain the NBCCEDP bycontributing their expertise,
connec
tions, resources, and enthusiasm tothe activities of the
program.
PARTN ERSH IP The Iowa Tribe of Oklahoma, the Kaw Nation Breast
and Cervical Cancer EarlyDetection Program (BCCEDP), and the
Oklahoma Take Charge! Program of theOklahoma BCCEDP are
collaborating to serve the women living in and around therural
Payne County community of Perkins in north-central Oklahoma.
The Iowa Tribe operates a clinic in Perkins that serves tribal
and other community members. The Tribal Health Director wanted to
be sure that all women in the area had access to the BCCEDP. The
collaboration of the three programs allows services to be provided
for tribal members through the Kaw Nation BCCEDP, for other
eligible women through the Take Charge! Program, and for insured
women through the clinics medical staff. Mammography services are
provided by a mobile unit operated by the Oklahoma Breast Care
Center in Oklahoma City.
Outreach strategies include displaying posters in community
businesses and tribaloffices, placing announcements in local and
tribal papers, and setting up boothsat tribal functions. The
population of eligible women in the area is small and
clinicutilization is limited; to date, the program has served 50
women. However, thepartners remain committed to making the services
available to all area women.
ProfessionalDevelopment
Professional development activitiesin the NBCCEDP are designed
toimprove the ability of health careproviders to screen for and
diagnose breast and cervical cancer
so that women receive appropri-ate and high-quality screeningand
diagnostic services. Related
activities include increasing theimpact of the program on
breastand cervical cancer mortality andimproving providers
performancein following up on abnormalscreening results.
Recruitment
The purpose of recruitment is toincrease the number of women
in
priority populations receiving clinical screening services by
raisingawareness, addressing barriers,
and motivating women to usethese screening services.
Raisingawareness through public education involves the systematic
designand delivery of clear and consistent messages about breast
andcervical cancer and the benefits ofearly detection using a
variety ofoutreach and inreach strategies topromote the clinical
services avail-able for program-eligible women.
6 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
17/88
Outreach relies on comprehensive,tailored, population-specific
strategies designed to reach and bringwomen from NBCCEDP
prioritypopulations into clinical screening services. Inreach
involvesapproaching program-eligible priority women who are using
otherhealth services (e.g., getting a flushot, receiving care for
diabetes)
and recruiting them into NBCCEDP.
The essential elements of recruitment are
Obtaining input from partners,including representatives
frompriority population groups, inassessing needs and developing
comprehensive plans forpublic education, outreach, and
inreach. Developing or revising, as
needed, a public education andcomprehensive outreach workplan
that includes an appropriatemix of broad-based awareness-raising,
community education, andone-on-one outreach strategies.
Developing and using methodsto evaluate the effectiveness of
comprehensive outreach andinreach strategies, as well aspublic
education messages, inrecruiting women into screening.
Placing priority for using program resources on
implementingactivities that are most effective
in recruiting eligible women frompriority populations for
screening
) i
ll
( li l
l ii
ll l
l implll l i l iate
i l ll i l
i ini i ll
PROFESS ION AL DEV ELOPMEN T
Alaskas Breast & Cervical Health Check (BCHC program staff
has begun us ng amultifaceted approach to improving mammography
rates. BCHC awarded a $15
bonus fee to c inics for each woman aged 5064 who had amammogram
within 60 days of her c inical breast examination CBE). Program
data were used to identify BCHC c inicsites w th ow mammography
rates. These sites were notifiedof their rates and shown comparison
rates from simi ar-s zedsites where rates were higher. These data
were accompan edby information about strategies for improving
mammographyrates, inc uding the use of motivational communications
basedon the Stages of Change Theory. C inics were supp ied
withspecially designed tick ers that help s ify and makereca
efforts reliab e and t mely. The tick ers are approprfor use with
any patient in the providers practice, reducing
his or her impulse to put time into mp ementing multip e
tracking systems. Tips fora Qua ity Mammogram cards were d
stributed to patients at all BCHC c inics. Layoutreach staff
received ntensive tra ng n motivational interviewing ski ls basedon
Stages of Change Theory. C inicians were offered training in the
vertical stripmethod of CBE and breast diagnostic algorithms.
ll
i l
in i il
l i i
l l il l il and
ii
l i ill l
l ii
l
ill i
R E C R U I T M E N T
On April 1, 2003, the I inois Breast and CervicalCancer Program
launched a statewide enrollment campaign target ng African
American, rura , and Hispanicwomen between the ages of 50 and 64.
Focus groupswere used to obta nput on everyth ng from appropri
ate take-home messages to which co or scheme was most visually
appealing. Theresu t was a h ghly nteractive campaign incorporating
mass media and face-to-face communications encouraging women to
take charge of their health. Tacticsinc uded direct mail, coa ition
bu ding, enrol ment day events, radio advert sements, faith-based
outreach, and a peer advocates program. Direct mai
radio advertisements turned out to be the two most successful
strateg es in thiscampa gn.
Direct mai pieces conta ned the toll-free Womens Health-L ne
number for womento ca for referrals, as well as a postage-free rep
y card that could be torn off andmai ed back. Paid rad o
advertisements ran in 60-second spots, promoting theprogram and the
Womens Health-Line. Combined, these two strateg es resulted inmore
than 2,200 referrals. Overall, the campaign motivated approximate y
4,500women to contact the program during a 9-month period. In terms
of actual enrollments, 2,900 more women signed up for the program
than enrolled during thesame time period the previous year. This
represented a 49% increase n enrollmentovera and a 48% increase in
enrollment by racial or ethnic m nority women.
Data Management
The collection, analysis, and useof quality data are essential
forguiding program efforts. To meet
CDCs data management expectations, a grantee is required to
Establish and maintain a datasystem for collecting, editing,and
managing the data neededto track a womans receipt ofscreening,
rescreening, diagnostic, and treatment services.
Establish mechanisms forreviewing and assessing the
completeness, accuracy, andtimeliness of data collected.
Establish protocols to ensure thesecurity and confidentiality of
alldata collected.
Collaborate with other existingsystems to collect and
analyzepopulation-based information
7 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
18/88
on breast and cervical cancer,including incidence and mortality
rates, cancer stage atdiagnosis, and the demographicprofile of
cancer patients.
Quality Assurance
The NBCCEDP provides guidanceon quality assurance and
improvement methods that use data toidentify training needs,
improveservices, and ultimately ensurewomen receive high-quality
care.The overarching intent of qualityassurance and improvement
(QA/QI) activities is to
Ensure the quality of services
delivered through the NBCCEDP.
Describe the role of QA/QIwithin the broader context ofpublic
health.
Promote best-practice outcomesas benchmarks for
improvingclinical services for programwomen.
Health agencies that participate inthe NBCCEDP use
mammographyfacilities certified by the AmericanCollege of Radiology
and cytology laboratories that follow theClinical Laboratory
ImprovementAmendments of 1988. CDC provides screening and
diagnosticguidelines to all NBCCEDP grantees and helps them
evaluate theappropriateness and quality oftheir clinical services.
Under CDCs
guidance, all grantees developstrategies to ensure that
womenreceive the best care possible.
ion
Q U A L I T Y A S S U R A N C E
The foundation of any program for the early detection of breast
and cervicalcancer is quality data. Surveillance plays an important
role in identifying dataproblems and establishing successful
quality assurance activities to correct thoseproblems. One of the
challenges that the West Virginia Breast and CervicalCancer
Screening Program (WVBCCSP) faced was reaching a minimum of 20%in
the never or rarely screened category (percentages ranged from 3.9%
to8.7%). Program staff knew this high-risk population of women
existed in West
Virginia, but the challenge was figuring out why they were not
being capturedin the data. During 2002, routine data
surveillanceidentified an unusual increase in the number of
womenwho answered unknown to the question abouthaving had a prior
Pap test. This increase promptedfurther investigation and resulted
in a chart audit.Program researchers suspected that the key to
solvingthe problem was related to the unknown prior Paptests.
Indeed, the chart audit identified a misconceptamong WVBCCSP
providers. Many thought that if a woman did not recall theexact
date of her previous Pap test, they had to mark unknown on her
Patient
Data Form. Once the WVBCCSP staff recognized this misconception,
they workeddiligently to correct the problem by communicating with
providers and reassuringthem that partial or estimated dates were
acceptable. To date, the WVBCCSPhas performed three chart audits,
and each has been essential in increasing theprograms never or
rarely screened percentages. Prior to the implementation ofroutine
chart audits, the WVBCCSPs overall never or rarely screened
percentage was 4.5%. That percentage increased to 24.9% following
the completionof the first chart audit and has since remained above
the mandated 20%.While chart audits proved to be a valid method of
recapturing never or rarelyscreened populations for the WVBCCSP,
they alsoperhaps more importantlyemphasized the impact of provider
education on data quality.
SCREEN IN G
The heart of theNorth CarolinaBreast and CervicalCancer
ControlProgram (NCBCCCP) case management training is its Case
Management Kit.The NC BCCCP compares the kitto a cookbook.
Experienced cooksand new cooks use a cookbookdifferently. The Case
ManagementKit is designed to provide as muchguidance as possible to
new casemanagers but still allow experienced case managers to
modifytheir approaches with creativity andconfidence.
The Case Management Kit is ahalf-inch, indexed 3-ring binderthat
contains everything the NCBCCCP coordinator needs to fol-low the
case management system.Contents include an overview ofNorth
Carolinas case managementrationale and philosophy; PowerPointnotes;
an algorithm used in trainingon the case management process;all
forms needed to document casemanagement, including a
needsassessment form and six care plantemplates; and the NC BCCCP
case
management policies.
Screening
Screening and diagnostic servicesare the heart of the
program.
Screening encompasses five distinctly different program
activities:screening, tracking, follow-up, casemanagement, and
rescreening.These activities work together toensure that women in
the programreceive timely and appropriatefollow-up. The NBCCEDP
reimburses states and other granteesfor clinical breast exams,
screening mammograms, pelvic exams,
8 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
19/88
Pap tests, and some diagnosticprocedures. State health
agenciescontract with a broad range ofagencies to coordinate and
deliverscreening and diagnostic services.
NBCCEDPResearch andEvaluationThe data collected by theNBCCEDP
facilitate the identification, analysis, and resolution ofimportant
issues in the provision ofbreast and cervical cancer screening to
underserved women. Eachgrantee submits to CDC minimum
data elements (MDEs) that areuseful for planning and evaluation
functions and as a basis forscientific studies. A selected list
ofscientific publications illustratingthe breadth and importance
ofresearch using the MDEs is includedinAppendix II. As noted in
thislist of publications, researchers haveexamined such issues as
how frequently Pap tests are needed once
a series of tests are reported asnegative,5 differences in
screeningmammography between the UnitedStates and the United
Kingdom,6
and racial and ethnic differences inscreening outcomes.7
Additionally,analysis of NBCCEDP data hasbeen valuable in
determining thatlinkage of the MDEs with statecancer registries is
important in consistently and accurately reportingcancer-stage
data. This has led togreater cooperation between unitsin the health
departments and fromthe community at large.
Of equal importance is the contribution of the MDE data set
topublic health practice. Designedto monitor the extent to
whichfunded programs in the NBCCEDPachieve the objectives of
the
authorizing legislation, the MDEsprovide demographic,
service,and outcome data that have had adramatic impact on policy
and program development. For example,
Descriptive reports of MDE dataallow CDC to quickly identify
programs struggling to meetclinical or service standards setfor
the national program andprovide technical assistancebefore quality
declines. Thesereports also guide the development of training for
grantees andcontribute to the identification ofbest practices for
dissemination.
Monitoring the MDEs may resultin the identification of common
deficiencies that suggestthat system-wide changes areneeded. New
national policiesor partnerships may result. Anexample is the
relationship CDChas developed with the MigrantClinicians Network to
enhancethe cancer-related case management of migrant, homeless,
andmobile people.
Quality assurance (QA) is amajor outcome of effective useof
MDEs. Grantees can evaluatethe work of individual providersagainst
a standard and identifyoutliers for whom QA interventions may be
needed. TheMDE system provides essentialinformation on the
timeliness,adequacy, and appropriatenessof follow-up of clinical
care,
ensuring that problems areaddressed and changes made.
Outcomes of MDE reportingactivities have resulted in
significantly increased funding, allowingadditional women to be
screenednationwide for breast and cervical cancer. In addition,
MDEdata are useful in evaluating andinfluencing the development
of
updated national cancer screeningrecommendations and
guidelines,tracking cancer rates amongwomen who are never or
rarelyscreened, testing the efficacyof screening technologies,
anddeveloping models to addressother cancers. Data from the
NBCCEDP support performance-based budgeting and the
effectivestewardship of taxpayers dollarsand public trust. Data
about who isbeing served, with what services,within what time
frame, and withwhat results allow CDC and itspartners to assure the
public thatthe NBCCEDP provides high-quality services to eligible
womenand contributes significantly to the
reduction of the breast and cervicacancer burden in the
country.
ScreeningResults andOutcomes inthe NBCCEDPThis report summarizes
the datasubmitted by grantees from 1991through 2002 on breast and
cervical cancer screening participation,screening test results,
diagnosticprocedures performed, and finaldiagnoses. In addition to
summaryresults, more detailed data are presented by time period
(19911995,19962000, and 20012002) inthe Data Tablessection.
Most
screening outcomes are reportedby first and subsequent screening
round because outcomesfrom the subsequent rounds in theNBCCEDP are
more likely to reflectincidence of disease rather thanprevalence. A
womans first program screening round is defined asher first NBCCEDP
mammogram orPap test. In reporting subsequentscreening rounds, we
excluded
9 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
20/88
results for women whose initialexam led to a final diagnosis
ofcancer. All screening result distributions, diagnostic follow-up
rates, andcancer detection rates estimatedfor racial/ethnic groups
wereage-adjusted to the populationof women receiving mammo
grams and Pap tests through theNBCCEDP in 2000 using the
directmethod.8 A more detailed description of the methods used to
obtainall breast and cervical cancerscreening results and outcomes
canbe found inAppendix III.
Breast Cancer
ScreeningIn the NBCCEDP, breast cancerscreening includes both
mammography and clinical breast examinations(CBEs). Mammography is
currentlythe best available procedure fordetecting breast cancer in
itsearliest, most treatable stageanaverage of 1 to 3 years
beforethe woman can feel the lump.9
Additionally, CBEs are able todetect some of the few breast
cancers that screening mammographymay miss.10 Thus, NBCCEDP
breastcancer screening includes bothtypes of examinations.
In the NBCCEDP, a breast cancerscreening round can be initiated
byeither a mammogram or a CBE .11
Mammography test results arecategorized using the American
College of Radiology (ACR) BreastImaging Reporting and
DataSystem (BI-RADS).12 This system isa quality assurance tool
designedto standardize mammographicreporting and facilitate
outcomemonitoring. Abnormal mammogram results that signal the
needfor additional diagnostic testinginclude suspicious
abnormalities
(BI-RADS category 4), thosethat are highly suggestive of
amalignancy (BI-RADS category5), and incomplete assessments(BI-RADS
category 0). Diagnostictesting also is considered if themammogram
was done outsidethe program but the results arethought to have been
abnormal. If
a suspicious abnormality is foundduring a CBE, diagnostic
work-upis required regardless of the initialmammogram findings. If
diagnosticwork-up is required or initiated inthe NBCCEDP,
documentation ofdiagnostic tests performed andthe final diagnosis
is expected.Additionally, for women diagnosedwith breast cancer,
documentationof the cancers stage at diagnosis,
the tumor size, the status of treatment, and the date of
treatmentinitiation is required.
The Breast and Cervical CancerMortality Prevention Act of
1990requires programs to take all appropriate measures to ensure
thatwomen with abnormal screeningresults receive the necessary
follow-up services. CDC requiresprograms to establish and
maintaina proactive surveillance systemfor the timely and
appropriatereferral and follow-up for womenwith abnormal or
suspicious testresults whose clinical services arepaid for in whole
or in part by the
NBCCEDP funds. The NBCCEDPpays for select diagnostic
services,including diagnostic mammography, repeat CBEs,
breastultrasounds, fine-needle aspirations, surgical consultations,
andbreast biopsies.
Breast Imaging Reporting and DataSystem (BI-RADS)
Assessment Categories
Category 0Assessment incompleteneed additional
imagingevaluation
Category 1Negative
Category 2Benign finding
Category 3Probably benignshortinterval follow-up suggested
Category 4Suspicious abnomal-itybiopsy should beconsidered
Category 5Highly suggestive ofmalignancyappropriate
action should be taken
Breast CancerScreening Participation
When the NBCCEDP began in1991, CDC followed recommendations for
breast cancer screeningthat emphasized the value ofscreening
mammography bothfor women aged 4049 andfor women aged 50 or
older.All CDC-funded programs couldscreen women in both of theseage
groups. In 1996, however, theNBCCEDP established a more strin
gent age policy for funding breastcancer screening that would
allowthe best use of limited resources.The new NBCCEDP policy
requiredthat 75% of mammograms paidwith NBCCEDP funds be providedto
women 50 years of age orolder. Consistent with the current age
guidelines, most womenscreened in the program between1991 and 2002
were 5064
years of age at the time of their firstscreening (Figure 5).
Figure 6 illustrates the age distribution of women screened
inthe program between 2001 and2002. The recent shift in the
agedistribution of women receivingmammograms through the programis
primarily due to a change in1998 to exclude women 65 years
10 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
21/88
of age and older who are eligiblefor Medicare Part B
coverage.
Figure 5. Age* Distribution of Women Receiving Mammograms
Through the NBCCEDP, 19912002
65+10%
16%
404930%
6064
505944%
*Age at time of first mammogram.
Figure 6. Age* Distribution of Women Receiving Mammograms
Through the NBCCEDP, 20012002
65+3%
606416% 4049
29%
505952%
*Age at time of first mammogram.
The racial and ethnic distributionof women receiving mammography
through the NBCCEDP isshown in Figures 7 and 8. Since
the beginning of the program,approximately 88% of the
womenscreened have been Hispanic/Latina, white, and black or
AfricanAmerican (Figure 7). However,during 2001 and 2002 a
slightly
higher percentage of womenscreened were Hispanic/Latinaand
Asian/Native Hawaiian/Other Pacific Islander (Figure 8).
11 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
22/88
Figure 7. Racial/Ethnic Distribution of Women Receiving
Mammograms Through the NBCCEDP, 19912002
Other/Unknown3%
21%Hispanic/Latina
White50%
American Indian/Alaska Native
5%
Asian/Native Hawaiian/Other Pacific Islander
4%
Black/AfricanAmerican
17%
Figure 8. Racial/Ethnic Distribution of Women Receiving
Mammograms Through the NBCCEDP, 20012002
Other/Unknown4%
27% White43%
American Indian/Alaska Native
4%
Asian/Native Hawaiian/Other Pacific Islander
Hispanic/Latina
6%Black/African American16%
Breast CancerScreening Results
Figure 9 illustrates the age-specificpercentage of screening
mammograms that are abnormal duringthe first and subsequent
screen-
ing rounds for women screenedthrough the NBCCEDP between1991 and
2002. Overall, thepercentage of abnormal screening mammograms
decreases withincreasing age, and the percentage of women with
abnormal
mammography results is higherin the first screening round.
Anunknown number of women arereferred to the program or seekout the
NBCCEDP themselves afterpresenting with symptoms or afterhaving an
abnormal CBE or
12 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
23/88
Figure 9. Percentage of Screening Mammograms That Are Abnormal*
Among Women in the NBCCEDP,by Age Group and Screening Round,
19912002
)
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
10.9
9,309
6.8
12.3
8.2
11.1
6.9
9.9
6.4 6.7
4.6
Fi
Percent(%
rst-round mammogramsSubsequent-round mammograms
>Total 4049 5059 6064 _65**
Age Group
*Includes the following mammogram results: suspicious
abnormality, highly suggestive of malignancy, and
assessmentincomplete.**Most women 65 years of age or older were not
served through the NBCCEDP because of eligibility for Medicare Part
B coverage.
Figure 10. Age-Adjusted* Percentage of Screening Mammograms That
Are Abnormal** Among Women inthe NBCCEDP, by Race/Ethnicity and
Screening Round, 19912002
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
10.9 11.0
7.0 6.9
10.7
8.3
6.1
10.7
6.6
7.6 7.9
11.5
)
Percent(%
First-round mammograms
Subsequent-round mammograms
Total* White Black/African Asian/Native American
Hispanic/LatinaAmerican Hawaiian/Other Indian/Alaska
Pacific Islander Native
Race/Ethnicity
*Age-adjusted to the 2000 NBCCEDP population.**Includes the
following mammogram results: suspicious abnormality, highly
suggestive of malignancy, and assessment incomplete.
13 19 91 2 0 0 2 N AT ION A L R E P OR T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
24/88
mammogram elsewhere. As aresult, the percentage of
womenreporting symptoms was alsogreater in the first screening
round(11.0%) than in subsequent rounds(6.7%).
Figure 10 displays the age-
adjusted percentage of abnormalscreening mammograms by racialand
ethnic origin of the programparticipants. From 1991 through2002 the
age-adjusted percentageof abnormal screening mammograms for all
women in theNBCCEDP was 10.9% and 7.0%for first and subsequent
screeningrounds, respectively. Hispanic/Latina women had the
highest
percentage of abnormal mammography screening results for both
firstand subsequent rounds.
Tables 1.11.3 and Tables 2.12.3in the Data Tablessection ofthis
report show the distribution,by time period, of all breast cancer
screening results for womenscreened through the NBCCEDP. Ingeneral,
the percentage of abnor
mal mammograms increased overthe 12-year time period covered
inthis report.
Breast CancerScreening DiagnosticFollow-Up
Diagnostic follow-up in theNBCCEDP can be initiated basedon
either an abnormal screeningresult or the level of concern ofthe
patient or clinician. Diagnosticfollow-up is defined as any
surgical or imaging procedures otherthan the screening mammogram
orCBE, including additional mammographic views, ultrasound, a
repeatCBE or surgical consultation, a
fine-needle or cyst aspiration, andbiopsy or lumpectomy. The
age-specific biopsy rates per 1,000mammograms in the NBCCEDPare
illustrated in Figure 11. Biopsyrates were inversely related
towomens age. Figure 12 showsthe age-adjusted biopsy rates
byracial/ethnic group. Regardless ofage, race, or ethnicity, the
biopsyrates were substantially lower in
subsequent rounds. This result isexpected since many of the
womenscreened for the first time in theNBCCEDP report having
symptoms, have not been screenedbefore, or are referred to the
program by another clinician due to asuspicious finding.
Tables 3.13.3 and Tables 4.14.3in the Data Tablessection ofthis
report show, by time period,the rates of all diagnostic follow-up
in women screened throughthe NBCCEDP. During the 12-yeartime period
covered in this report,the rate of diagnostic follow-upincreased in
all age groups.
Figure 11. Biopsy* Rates Among Women in the NBCCEDP, by Age
Group and Screening Round, 19912002
Rateper1,000Mammograms
40.0 First-round mammograms Subsequent-round mammograms
35.0
30.0
25.0
20.0
15.0
10.0
5.0
0.0
Total 4049 5059 6064 _65
30.7
9,309
16.1
36.5
20.4
29.8
16.0
28.7
15.2
19.6
12.1
>
Age Group
*Diagnostic follow-up may be initiated on the basis of an
abnormal CBE, abnormal mammogram, or a high level of concern by
thepatient or clinician.
Breast CancerDetection
Figure 13 shows age-specific cancer detection rates (invasive
and insitu combined) per 1,000 mammograms in the NBCCEDP. Thecancer
detection rates generallyincrease with age; however, thereis a
slight drop in rates for women65 years of age or older. The
age-
14 19 9 1 2 0 0 2 N AT I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
25/88
adjusted cancer detection rates areillustrated in Figure 14.
Figure 12. Age-Adjusted* Biopsy** Rates Among Women in the
NBCCEDP, by Race/Ethnicity and ScreeningRound, 19912002
Rateper1,000M
ammograms
40.0
35.0
30.0
25.0
20.0
15.0
10.0
5.0
0.0
30.5
16.5
35.6
18.420.2 20.9
11.8
30.8
17.2
11.1
13.7
23.5
First-round mammogramsSubsequent-round mammograms
Total* White Black/African Asian/Native American
Hispanic/LatinaAmerican Hawaiian/Other Indian/Alaska
Pacific Islander Native
Race/Ethnicity
*Age-adjusted to the 2000 NBCCEDP population.**Diagnostic
follow-up may be initiated on the basis of an abnormal CBE,
abnormal mammogram, or a high level of concern by the patient or
clinician.
Figure 13. Rates of Breast Cancer* Among Women in the NBCCEDP,
by Age Group and Screening Round,19912002
Rateper1,000Mamm
ograms
12.0
10.0
8.0
6.0
4.0
2.0
0.0
9.1
3.7
8.1
3.2
9.0
3.5
11.3
4.4
8.9
4.0
First-round mammogramsSubsequent-round mammograms
>Total 4049 5059 6064 _65
Age Group
*Includes invasive breast cancer, Lobular Carcinoma in Situ
(LCIS), Ductal Carcinoma in Situ (DCIS), and all other Carcinoma in
Situ.
Overall,and adjusted for age, there are 9.4cases of invasive or
in situ breastcancer diagnosed per 1,000 mammograms in the NBCCEDP.
Thisrate is higher in white women, butlower in all other racial and
ethnic
groups. Regardless of age, race,or ethnicity, the detection
ratesfor carcinoma in situ and invasivecancer were substantially
lower insubsequent rounds, since many ofthe women screened during
the firstround were previously unscreened,symptomatic, or referred
to the pro
gram by another clinician due to asuspicious finding.
Tables 3.13.3 and Tables 4.14.3in the Data Tablessection ofthis
report show, by time period,the invasive and in situ
carcinomadetection rates in women screened
15 19 91 2 0 0 2 N AT I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
26/88
Figure 14. Age-Adjusted* Rates of Breast Cancer** Among Women in
the NBCCEDP, by Race/Ethnicity andScreening Round, 19912002
0.0
2.0
4.0
6.0
8.0
10.0
12.0
9.4
3.6
11.5
4.0
7.0 7.1
3.4
9.3
4.0
3.1
2.3
5.8
Fi t
Rateper1,000Mammogram
s
rs -round mammogramsSubsequent-round mammograms
Total* White Black/African Asian/Native American
Hispanic/LatinaAmerican Hawaiian/Other Indian/Alaska
Pacific Islander Native
Race/Ethnicity*Age-adjusted to the 2000 NBCCEDP
population.**Includes invasive breast cancer, Lobular Carcinoma in
Situ (LCIS), Ductal Carcinoma in Situ (DCIS), and all other
Carcinoma in Situ.
Figure 15. Positive Predictive Value (PPV)* of Abnormal
Mammography Results** Among Women in theNBCCEDP, by Age Group and
Screening Round, 19912002
6.4
10.9
l
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
7.9
5.1
6.1
3.5
7.7
4.8
6.4
10.9
12.5
7.8
Fi
PPV*and95%ConfidenceInterva
rst-round mammograms
Subsequent-round mammograms
_Total 4049 5059 6064 >65
Age Group
*The positive predictive value (PPV) was calculated by dividing
the number of abnormal mammogram results leading to a
finaldiagnosis of cancer by the total number of abnormal mammogram
results.**Includes the following mammogram results: suspicious
abnormality, highly suggestive of malignancy, and
assessmentincomplete.
16 19 9 1 2 0 0 2 N AT I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
27/88
through the NBCCEDP. In gen-eral, cancer detection rates
haveincreased since the beginning ofthe program.
Positive PredictiveValue of AbnormalMammograms
The diagnostic value of a proce-dure is often defined by its
positivepredictive value, or the measure(%) of times a positive
test resultleads to diagnosis of disease.Here, the positive
predictive value(PPV) of abnormal mammograms isdefined as the
proportion of abnor-mal mammograms that lead to afinal diagnosis of
breast cancer.
Figure 15 illustrates age-specificPPVs of abnormal
mammograms
among women in the NBCCEDP.In general, first-round
abnormalmammograms have a PPV of7.9, whereas
subsequent-roundabnormal mammograms havea significantly lower PPV
of 5.1.The PPVs are smaller for youngerwomen but increase with
increas-
ing age. The variation by racialand ethnic group is shown
inFigure 16. The PPV is signifi-cantly higher in black or
AfricanAmerican women and whitewomen when compared to the PPVin
Asian/Native Hawaiian/OtherPacific Islander and Hispanic/Latina
women.
Tables 5.15.3 in the Data
Tablessection of this report showthese results by time
period.
Figure 16. Positive Predictive Value (PPV)* of Abnormal
Mammography Results** Among Women in theNBCCEDP, by Race/Ethnicity
and Screening Round, 19912002
PPV*and95%Confidence
Interval
12.0 First-round mammograms Subsequent-round mammograms
10.0
8.0
6.0
4.0
2.0
0.0White Black/African Asian/Native American Hispanic/Latina
9.7
5.8
8.2
4.1
4.9
6.1 6.47.0
2.8
4.5
American Hawaiian/Other Indian/Alaska
Pacific Islander Native
Race/Ethnicity
*The positive predictive value (PPV) was calculated by dividing
the number of abnormal mammogram results leading to a
finaldiagnosis of cancer by the total number of abnormal mammogram
results.**Includes the following mammogram results: suspicious
abnormality, highly suggestive of malignancy, and
assessmentincomplete.
Stage of InvasiveBreast Cancer at Timeof Diagnosis
The goal of screening for breastcancer is to detect the disease
atits earliest and most treatable stageof development. Figure 17
illus
trates the age-specific distributionof early- versus late-stage
detection of invasive breast cancer inthe NBCCEDP. From 1991
through2002, 9,956 women had a diagnosis of invasive breast
cancer,and 74.0% of these cancers wereidentified at an early
stage.
Tables 6.16.3 in the DataTablessection of this report showall
breast cancer staging results byage and time period.
17 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
28/88
Figure 17. Distribution (%)* of Early vs. Late Stage** Invasive
Cancer at Time of Diagnosis in WomenScreened Through the NBCCEDP,
by Age Group, 19912002
Percent(%)*
90.0
80.0 Early stage*** Late stage****70.0 Unknown stage
60.0
50.0
40.0
30.0
20.0
10.03.0
0.0Total 4049 5059 6064 _65
74.0
21.5
4.4
24.9
70.3
4.8 4.1
73.2
22.1
76.5
19.4
81.8
15.2
4.7
>
Age Group
*Totals may not add to 100% due to rounding.
**Staging information in the NBCCEDP data may not be consistent
with that from cancer registries due to variation in type of
information reported by individual programs.***Includes AJCC Stage
I and II, and SEER summary local stage.****Includes AJCC Stage III
and IV, and SEER summary regional and distant stage.Abbreviations:
AJCC=American Joint Committee on Cancer; SEER=Surveillance,
Epidemiology, and End Results.
CervicalCancer
ScreeningCervical cancer is largely preventable with appropriate
screening.The standard screening method forearly detection of
cervical carcinoma is the Pap test. This screeningtest has helped
reduce the cervical cancer morbidity and mortalityrates and is the
most cost-effectivecancer screening method avail-able.13 The U.S.
Preventive ServicesTask Force strongly recommendsthat women between
the ages of21 and 65 be screened regularlyfor cervical cancer.2
2001 Bethesda System Categories Used in the NBCCEDP
Negative for intraepithelial lesion or malignancy.
Atypical squamous cells of undetermined significance
(ASCUS).
Low-grade squamous intraepithelial lesion (LSIL) encompassing:
HPV,mild dysplasia/CIN I.
Atypical squamous cells of undetermined significancecannot
exclude
HSIL (ASCH). High-grade squamous intraepithelial lesion (HSIL)
encompassing:
moderate and severe dysplasia, CIS/CIN II and III.
Squamous cell carcinoma.
Atypical glandular cells including atypical, endocervical
adenocarci-noma in situ and adenocarcinoma.
Other.
In the NBCCEDP, a cervical cancerscreening round is initiated by
aPap test. The Pap test results arecategorized using the
BethesdaSystem.14 This system is a quality assurance tool designed
to stan
dardize Pap test reporting andfacilitate outcome
monitoring.Abnormal Pap test results that signalthe need for
additional diagnostic
testing include low-grade squamous
intraepithelial lesion (LSIL), high-grade squamous
intraepitheliallesion (HSIL), squamous cell cancer(SqCa), atypical
glandular cells
(AGC), and atypical squamous
18 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
29/88
cellscannot exclude HSIL (ASC-H),which was added to the
reportingsystem in 2001. If diagnostic workup is required or
initiated in theNBCCEDP, documentation of diagnostic tests
performed and the finaldiagnosis is expected. Additionally,for
women diagnosed with cervi
cal cancer, documentation of thecancers stage at diagnosis,
tumorsize, status of treatment, and dateof treatment initiation is
required.
The Breast and Cervical CancerMortality Prevention Act of
1990requires programs to take allappropriate measures to ensurethat
women with abnormal screening results are provided with
necessary follow-up services. TheNBCCEDP pays for
diagnosticservices, including colposcopy andcolposcopy-directed
biopsy.
Although the overall rate of screening for cervical cancer in
theUnited States has increased, many
subpopulations are not beingadequately screened. More than60% of
the women with a diagnosis of cervical carcinoma hadnever been
screened or had notbeen screened within the previous5 years of
diagnosis.15 In 1999,CDC and an external work group
conducted a careful review of thescientific literature, the
cervicalcancer guidelines of professionalorganizations, and NBCCEDP
dataon Pap screening outcomes andcollaborated on the developmentand
implementation of a new cervicalcancer screening policy. This
policyencouraged all NBCCEDP granteesto focus cervical cancer
screeningon women who had rarely or never
been screened and to decreaseover-screening of women enrolledin
the program.
At the same time, CDC changedthe screening guidelines
thatrecommended yearly Pap tests for
all women. The new guidelinesrecommend a Pap test every 3years
after a woman has hadthree consecutive normal Pap testresults
within a 5-year period. Forwomen who have not had threeconsecutive
Pap tests with normalor benign findings within a 5-year
period, annual screening is stillrecommended.
Cervical CancerScreening Participation
Figure 18. Age* Distribution of Women Receiving Pap Tests
Through the NBCCEDP, 19912002
65+6% 182910%
606410%
303912%
505929%
404933%
*Age at time of first Pap test.
Figure 18 illustrates the age distribution of women receiving
aPap test in the NBCCEDP sincethe onset of the program, andFigure
19 shows the distribution
for 2001 and 2002 only. Morethan half of the women screenedin
the program are 4059 yearsof age. Only 22% of clients receiving
cervical cancer screening duringthis entire period were underage
40. In the more recent time
19 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
30/88
period, these younger age groupsrepresent only 17% of the
totalpopulation, which likely reflects theprograms increasing
emphasis onthe recruitment of never or rarelyscreened women.
Figure 19. Age* Distribution of Women Receiving Pap Tests
Through the NBCCEDP, 20012002
65+ 18296064 2% 7%10%
303910%
505932%
404939%
*Age at time of first Pap test.
Figure 20. Racial/Ethnic Distribution of Women Receiving Pap
Tests Through the NBCCEDP, 19912002
Other/Unknown2%
21%Hispanic/Latina
14%
White53%American Indian/Alaska Native
6%
Asian/Native Hawaiian/Other Pacific Islander
4%
Black/African American
The racial/ethnic distributionof women receiving a Pap test
through the NBCCEDP is shown inFigures 20 and 21. For all
yearscombined, slightly less than half(47%) of the women were
fromracial/ethnic minority groups.For the most recent time
period(20012002), the percentage fromminority groups is slightly
morethan half (51%).
Cervical CancerScreening Results
Figure 22 illustrates the age-specificpercentage of screening
Paptests with abnormal results duringthe first and subsequent
screening rounds for women screenedthrough the NBCCEDP between
20 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
31/88
1991 and 2002. For all womenscreened for the first time,
thepercentage of abnormal screen-ing results was 2.7% from
1991through 2002. Overall, the per-centage of abnormal Pap
testresults decreases with increasingage, and the percentage of
women
with abnormal Pap test results ishigher in the first screening
round.
Figure 21. Racial/Ethnic Distribution of Women Receiving Pap
Tests Through the NBCCEDP, 20012002
Other/Unknown4%
Hispanic/Latina23%
White49%
American Indian/Alaska Native
5%
Asian/Native Hawaiian/Other Pacific Islander
5%
Black/African American14%
Figure 22. Percentage of Screening Pap Tests That Are Abnormal*
Among Women in the NBCCEDP, byAge Group and Screening Round,
19912002
Perc
ent(%)*
12.0 First-round Pap tests Subsequent-round Pap tests
10.0
8.0
6.0
4.0
2.0
0.0
2.7
1.4
9.7
4.1
5.0
2.5
1.0
2.1
1.5 1.41.1
0.8 0.60.9
>Total 1829 3039 4049 5059 6064 _65
Age Group
*Includes the following Pap test results: low-grade squamous
intraepithelial lesions (LSIL), high-grade squamous intraepithelial
lesions(HSIL), atypical squamous cells of undetermined
significancecannot exclude HSIL (ASC-H), atypical glandular cells
(AGC), andsquamous cell cancer.
**Most women 65 years of age or older were not served through
the NBCCEDP because of eligibility for Medicare Part B
coverage.
Figure 23 displays the age-adjusted percentage of abnormalPap
test results by racial and ethnicorigin. For both first and
subse-quent screening rounds, AmericanIndian/Alaska Native women
had
the highest percentage of abnormal Pap test results.
Tables 7.17.3 in the Data Tablessection show the distribution of
allcervical cancer screening resultsby age and time period.
Tables8.18.3 show the age-adjusted dis-tribution by race/ethnicity
for the
21 19912002 NA T I O NA L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
32/88
three time periods. There were nosubstantial changes in the
percentage of abnormal Pap tests duringthe 12-year time period
covered inthis report.
Figure. 23 Age-Adjusted* Percentage of Screening Pap Tests That
Are Abnormal** Among Women in theNBCCEDP, by Race/Ethnicity and
Screening Round, 19912002
Percent(%)*
3.0
2.5
2.0
1.5
1.0
0.5
0.0
2.1
1.4
2.1
1.4 1.4
2.6
1.8
2.0
1.5
1.2
1.4
2.0
Fi t t
rs -round Pap testsSubsequen -round Pap tests
Total* White Black/African Asian/Native American
Hispanic/LatinaAmerican Hawaiian/Other Indian/Alaska
Pacific Islander Native
Race/Ethnicity
*Age-adjusted to the 2000 NBCCEDP population.**Includes the
following Pap test results: low-grade squamous intraepithelial
lesions (LSIL), high-grade squamous intraepithelial lesions(HSIL),
atypical squamous cells of undetermined significancecannot exclude
HSIL (ASC-H), atypical glandular cells (AGC), andsquamous cell
cancer.
Figure 24. Rates of Biopsy-Confirmed Cervical Intraepithelial
Neoplasia (CIN) II or Worse* Among Womenin the NBCCEDP, by Age
Group and Screening Round, 19912002
30.0 Fi t ts
1.3 1.1
rs -round Pap testsSubsequent-round Pap tes
25.0
20.0
15.0
10.0
5.0
0.0
26.7
10.8
RatePer1,000PapTests
14.1
6.3
8.1
2.6
6.2
2.63.9
1.6
3.42.7
Total 1829 3039 4049 5059 6064
Age Group
_>65
*CIN II or worse includes CIN II, CIN III, carcinoma in situ,
and invasive cervical cancer.
Cervical Precancer andCancer Detection
Figure 24 shows age-specificrates of biopsy-confirmed cervical
intraepithelial neoplasia (CIN)II or worse (includes CIN II,
CIN
III, CIS, and invasive cancer) byscreening round per 1,000
Paptests in the NBCCEDP. The ratesof CIN II or worse decrease
withparticipants increasing age inboth first and subsequent
screeningrounds. The age-adjusted rates by
22 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
33/88
race and ethnicity are illustrated inFigure 25. Overall, and
adjustedfor age, there were 6.1 cases ofCIN II or worse per 1,000
Paptests. In the first round of screening,white women had the
highest age-adjusted rate (7.1 per 1,000 Pap
tests), followed by Hispanic/Latinawomen (5.7 per 1,000 Pap
tests).Regardless of age, race, or ethnic-ity, the detection rates
were lowerin subsequent rounds.
Tables 9.19.3 and Tables10.110.3 show the rates
ofbiopsy-confirmed CIN and invasivecervical cancer among womenin
the NBCCEDP. There were no
substantial changes in the precan-cerous and cancer detection
ratesbetween 1991 and 2002.
Figure 25. Age-Adjusted* Rates of Biopsy-Confirmed Cervical
Intraepithelial Neoplasia (CIN) II or Worse**Among Women in the
NBCCEDP, by Race/Ethnicity and Screening Round, 19912002
RatePer1,000
PapTests
8.0 First-round Pap tests Subsequent-round Pap tests7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0Total* White Black/African Asian/Native American
Hispanic/Latina
6.1
2.6
7.1
3.0
4.4 4.6
1.8
5.3
2.5 2.6
2.1
5.7
American Hawaiian/Other Indian/AlaskaPacific Islander Native
Race/Ethnicity
*Age-adjusted to the 2000 NBCCEDP population.**CIN II or worse
includes CIN II, CIN III, carcinoma in situ, and invasive cervical
cancer.
Positive PredictiveValue of AbnormalPap Tests
The diagnostic value of a proce-dure is often defined by its
positive
predictive value, or the measure(%) of times a positive test
resultleads to diagnosis of disease.Here, the positive predictive
value(PPV) of an abnormal Pap test isdefined as the proportion of
Paptest results of LSIL, ASC-H, HSIL,
AGC, or SqCa combined thatresult in a final diagnosis of CIN
IIor worse. Figure 26 illustrates theage-specific PPVs of abnormal
Paptests by screening round. Overall,in the first round the PPV is
25.4%,whereas subsequent rounds havea lower PPV of 14.1%. The
PPVsare highest for women in their 30s.The variation by racial and
ethnicgroup is shown in Figure 27. The
PPV is highest in white womenin the first round (29.0%) and
inAsian/Native Hawaiian/OtherPacific Islanders in the
subsequentrounds (16.3%).
Tables 11.111.3 in the DataTablessection of this report
showthese results by time period.
Stage of InvasiveCervical Cancer atTime of Diagnosis
Screening for cervical cancerallows for early detection whenthe
disease is at its earliest and
most treatable stage. Figure 28illustrates the detection of
invasivecervical cancer for women lessthan 50 years of age or 50
yearsand older in the NBCCEDP. A totalof 832 women were
diagnosedwith invasive cervical cancer from1991 through 2002 and
52.8% ofthese cases were identified as locadisease. Regardless of
age, mostcases were detected in an early
stage. However, women under 50years of age were more likely
thanwomen over 50 to be diagnosedwith local disease.
Tables 12.112.3 in the DataTablessection of this report showall
cervical cancer staging resultsby age and time period.
23 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
34/88
Figure 26. Positive Predictive Value (PPV)* of Abnormal Pap Test
Results** Among Women in the NBCCEDP,by Age Group and Screening
Round, 19912002
l Fi t ts
0
5
10
15
20
25
30
35
25.4
14.1
23.0
29.7
17.2
20.4
27.825.8
12.8
24.8
11.1
11.6
25.6
11.9
PPV*and95%ConfidenceInterva
rs -round Pap testsSubsequent-round Pap tes
_Total 1829 3039 4049 5059 6064 >65
Age Group
*The PPV was calculated by dividing the number of abnormal Pap
test results** leading to a biopsy-confirmed high-grade lesion
(CIN II or worse) by the total number of abnormal Pap test
results.**Includes the following Pap test results: LSIL, ASC-H,
HSIL, AGC, and squamous cell cancer. Abbreviations: CIN=cervical
intraepithelial neoplasia; HSIL=high-grade squamous intraepithelial
lesion; LSIL=low-grade squamousintraepithelial lesion; AGC=atypical
glandular cells; ASC-H=atypical squamous cells of undetermined
significancecannot exclude HSIL.
Figure 27. Positive Predictive Value (PPV)* of Abnormal Pap Test
Results** Among Women in the NBCCEDP,by Race/Ethnicity and
Screening Round, 19912002
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
29.0
15.9
21.7
10.3
16.3
26.7
14.8
12.7
23.5
12.7
l Fi ts
PPV*and95%ConfidenceInterva
rst-round Pap testsSubsequent-round Pap tes
White Black/African Asian/Native American
Hispanic/LatinaAmerican Hawaiian/Other Indian/Alaska
Pacific Islander Native
Race/Ethnicity
*The PPV was calculated by dividing the number of abnormal Pap
test results** leading to a biopsy-confirmed high-grade lesion(CIN
II or worse) by the total number of abnormal Pap test
results.**Includes the following Pap test results: LSIL, ASC-H,
HSIL, AGC, and squamous cell cancer. Abbreviations: CIN=cervical
intraepithelial neoplasia; HSIL=high-grade squamous intraepithelial
lesion; LSIL=low-grade squamousintraepithelial lesion; AGC=atypical
glandular cells; ASC-H=atypical squamous cells of undetermined
significancecannot exclude HSIL.
24 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
35/88
Figure 28. Distribution (%)* of Cancer Stage** at Time Invasive
Cervical Cancer Was Diagnosed in WomenScreened Through the NBCCEDP,
by Age Group, 19912002
29.7
12.8
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
52.8
35.5
5.6 6.1
60.8
45.9
29.6
5.73.9
8.15.6
40.5
>_50
(%)*
t *** i l st **** *****
Percent
Local s age
Reg ona age
Distant stageUnknown stage
Total _50
Age Group
*Totals may not add to 100% due to rounding.
**Staging information in the NBCCEDP data may not be consistent
with that from cancer registries due to variation in type of
information reported by individual programs.***Includes the
International Federation of Gynecology and Obstetrics (FIGO) Stage
I and the Surveillance, Epidemiology, and End Results (SEER) local
summary stage.****Includes FIGO/American Joint Committee on Cancer
(AJCC) Stage II and III and SEER regional summary
stage.*****Includes FIGO/AJCC Stage IV and SEER distant summary
stage.
FutureDirections
In cooperation with many localand national partners, theNBCCEDP
continues efforts toexpand screening services andimprove program
efficiency andeffectiveness. Currently, there areseveral special
projects adminis-tered by CDCs Division of CancerPrevention and
Control (DCPC)that are designed to improve ourunderstanding of
effective infra-
structure choices, costs, and bestpractices. With cooperation
fromour funded programs, the results ofthese special studies and
analyseswill enhance the success of ourprogram. The following
sectionhighlights some of the important projects underway.
Sharing NBCCEDPPerformance Data withthe General Public
In response to a congressionalinitiative to share
NBCCEDPperformance data with the gen-eral public, CDC is
developinga Web-based report accessiblethrough the CDC public Web
sitethat will provide a current summary of national and
program-specific screening and diagnostic servicesand outcomes.
The MDE ValidationProject
CDC regularly reviews the MDEdata for program monitoringpurposes
and also conductsanalyses of the national data forpublication in
appropriate reportsand professional journals. A list ofprevious
publications is providedinAppendix II. To better assess
the quality of these data, CDChas initiated a national
evaluationof the MDE data. To evaluate thequality of the national
database,
breast and cervical cancer screen-ing, diagnostic, and final
diagnosisMDE data from a sample ofNBCCEDP grantees will be compared
with data in the patients medical records.
Estimates of thePercentage of theEligible U.S.
PopulationScreened Through the
NBCCEDPEfforts are under way to estimatethe total number of
women in theUnited States who are eligiblefor the NBCCEDP as well
as thepercentage of age-appropriatewomen currently being
screenedthrough the program. The estimateswill be based on the MDEs
andthe Annual Social and Economic
25 19912002 N A T I O N A L R E P O R T
-
7/30/2019 National Breast and Cervical Cancer Early Detection
Program (a National Report)
36/88
Supplement of the U.S. CensusBureaus Current Population
Survey.This information will be used toinform the programs
estimatesof resources needed to expandservices, and may also be
usefulin ident











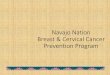




![DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for …€¦ · 3. Demonstration Population 13 [Women with Breast and Cervical Cancer]. Expenditures for women with breast and cervical](https://img.pdfslide.net/doc/110x75/5fbb81c1e0be7e1a172eefe9/department-of-health-human-services-centers-for-3-demonstration-population.jpg)











