Embed Size (px)
Citation preview
Lead ing 21 s t Century Heal thcare
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
Bulletin of theNational Center for Healthcare Leadership
www.nchl.org
3 Meeting the Demands for Improved Healthcare
5 Transformational Excellence:The Key to Tomorrow’s Healthcare Leaders
9 The Foundation of Leadershipin Baldrige Winning Organizations
Geoffrey S. CalhounDirector, Business Excellence, Baxter International
John R. GriffithAndrew Pattullo Collegiate ProfessorDepartment of Health Management & PolicyUniversity of Michigan School of Public Health
Marie E. SiniorisPresident and CEO, National Center for Healthcare Leadership
21 Commentaries on The Foundation of Leadershipin Baldrige Winning Organizations
Changing for the BetterJames H. Hinton, President and CEOPresbyterian Healthcare Services
Competent CommunitiesDavid C. Leach,MD, Former Executive DirectorAccreditation Council for Graduate Medical Education
Baldrige as a Path to ExcellenceRichard P. Miller, President and CEO,Virtua Health
27 Thomas M. Priselac Talks About Leadership and theInevitability of Change in Healthcare
December 2007
F O RT H E
CongratulationsTom Priselac
President & CEO, Cedars-Sinai Health SystemWinner of 2007 National Healthcare Leadership Award
Modern Healthcare commends your leadership and commitment to healthcare.
Modern Healthcare is the industry’s most trusted, credible and relied-upon news source. In print and online,Modern Healthcare examines the most pressing healthcare issues and provides executives with comprehensiveinformation they need to make the most informed business decisions and lead their organizations to success.For this reason, Modern Healthcare is a “must-read” by the who’s who in healthcare.
To subscribe to our products, please call Modern Healthcare at 888.446.1422 or email us at [email protected].
360 N. Michigan Avenue | Chicago, IL 60601 | 312.649.5499 | ModernHealthcare.com

We salute the
for its commitment to fostering quality leadership andhigh standards of excellence
among healthcare systems nationwide
and we heartily congratulate tonight’s honoree
THOMAS M. PRISELAC
Saul B. KatzCHAIRMAN, BOARD OF TRUSTEES
Michael J. DowlingPRESIDENT AND CHIEF EXECUTIVE OFFICER
3December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
3
Dear Reader,
With the presidential election less than a year away, reforming our nation’shealthcare has emerged as the hot button issue of the campaign season.Citizens are demanding it, politicians are promising it, and the healthcareindustry is eager to speed up reform so that high quality, effective, affordable,and patient-centered healthcare becomes equally accessible across the nation.
In that same vein, NCHL has witnessed a growing demand to accelerate organi-zational improvement in healthcare and to reach a broader segment of thefield with its evidence-based programs and best practices. What we know is thatexcellent leaders are required if healthcare organizations are going to undergothe kind of transformation that is needed in today’s environment whereaccountability, quality, and patient safety are demanded. We are committedto helping organizations achieve that excellence.
This issue of the Bulletin of theNational Center for Healthcare Leadership presentsa persuasive white paper on“The Foundation of Leadership in Baldrige WinningOrganizations”by Jeff Calhoun, John Griffith, and Marie Sinioris, which exploresthe principles and framework that defines the Malcolm Baldrige NationalQuality Award in helping organizations achieve excellence. As the whitepaper says,“while the Baldrige program is not the only avenue to higher per-formance, it embodies leadership and management principles now recog-nized by both practitioners and academicians as fundamental to success.”
The Bulletin also provides insight into how one leader inspires organizationalexcellence. In an interview, Thomas M. Priselac, President and CEO of Cedars-Sinai Health System in Los Angeles and recipient of the 2007 NationalHealthcare Leadership Award said he is inspired by the people who work atCedars where the“commitment to excellence is palpable.”
NCHL’s response to the national call for broader and deeper industry-wideimprovement has been its collaboration with GE Healthcare to create theInstitute for Transformational Healthcare Leadership, while continuing itsground-breaking research through its LENS (Leadership Excellence Networks)and university demonstration sites. The Bulletin details these efforts, all ofwhich have the same goal: helping organizations achieve a higher level ofperformance that will in turn improve the health of the public.
We hope the Bulletin brings you new thinking on healthcare leadershipdevelopment and organizational excellence.
Gail L. Warden Marie E. SiniorisPresident Emeritus President and CEOHenry Ford Health System National Center for Healthcare LeadershipChairNational Center for Healthcare Leadership
NCHL BOARD OF DIRECTORS
Diane P. AppleyardHealthcare Research & DevelopmentInstitute of America
John BabiarzARAMARK Healthcare
George ChavelSodexho Health Care Services
Brenita CrawfordAmara Management Resources
Michael J. DowlingNorth Shore-LIJ Health System
William M.DwyerCerner Corporation
David J. FineSt. Luke’s Episcopal Health System
Richard P. GustafsonHeidrick & Struggles
George J. Isham,MDHealthPartners
David C. Leach,MDAccreditation Councilfor Graduate Medical Education
Stephen F. Loebs, PhDThe Ohio State University
Gary A.MecklenburgWaud Capital Partners
William E.MoellerUnitedHealthcare of Illinois
Lee H. PerlmanGNYHA Ventures
Marla E. Salmon, ScD, RNEmory University
Stephen M. Shortell, PhDUniversity of California, Berkeley
Marie E. Sinioris (ex-officio)National Center for Healthcare Leadership
Joseph R. SwedishTrinity Health
Gail L.WardenHenry Ford Health System
LIAISON BOARD MEMBERS
Janet M. Corrigan, PhDNational Quality Forum
Jack C. EbelerConsultant
SENIOR ADVISOR TO THE BOARD
John R. GriffithUniversity of Michigan
Bul let in of the Nat iona l Center for Heal thcare Leader sh ip
EDITORS
Janet M. Corrigan, PhDNational Quality Forum
David J. FineSt. Luke’s Episcopal Health System
MANAGING EDITORJoyce AnneWainioNational Center for Healthcare Leadership
CONTRIBUTING EDITORLisabethWeinerLisabeth Weiner Consultants, Inc.Chicago
ART DIRECTORLisa KleinPisa Design, Inc.Chicago
JOURNAL COMMITTEEJanet M. Corrigan, PhD, Co-chairPresident & CEONational Quality Forum
David J. Fine, Co-chairPresident & CEOSt. Luke’s Episcopal Health System
John BabiarzGroup PresidentARAMARK Healthcare
Melanie BarstadPresident, Women’s Healthcare InitiativesJohnson & Johnson
Elizabeth H. Bradley, PhDAssociate Professor of Public Health &Director, Health Management ProgramYale School of Medicine
John R. GriffithAndrew Pattullo Collegiate ProfessorUniversity of Michigan
David C. Leach,MDFormer Executive DirectorAccreditation Councilfor Graduate Medical Education
Thomas M. PriselacPresident & CEOCedars-Sinai Health System
Stephen C. ReynoldsPresident & CEOBaptist Memorial Health Care
Marie E. Sinioris (ex-officio)President & CEONational Center for Healthcare Leadership
National Center for Healthcare Leadership515 North State Street, Suite 2000Chicago, Illinois 60610telephone: 312.755.5017fax: 312.755.7498
For more information about NCHLvisit our Web site at www.nchl.org.
Copyright © 2007
Bulletin of the National Center of Healthcare Leadership.
All rights reserved.No part of this publicationmay be reproduced or
transmitted in any form or by any means, electronic or mechanical,
including photocopy, recording, or any information storage and
retrieval system,without written permission.
Baptist Memorial Healthcarecongratulates
NCHL’s NationalHealthcare Leadership
A W A R D R E C I P I E N T
Thomas M. PriselacPresident & CEO, Cedars-Sinai Health System
We salute your achievements,leadership and ongoing commitmentto providing quality health care.
Memphis, TN
5December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
If healthcare is going to successfully confront the challenges ofa complex, rapidly changing environment, then it will needforward thinking, insightful, and highly competent leaders whoare prepared to transform the industry.
For the past six years, NCHL has pursued its mission to be anindustry-wide catalyst to assure the availability of this high-quality, relevant, and accountable health management leader-ship. The NCHL strategy has remained the same; however, onegoal in recent years has been to extend the reach and penetra-tion of its research-driven, peer-reviewed leadership develop-ment programs to a wider audience to help raise quality, safety,and leadership in healthcare to new levels. An ideal solution isits recently announced collaboration with GE Healthcare tomeld state-of-the-art learning with NCHL’s research-basedHealth Leadership Competency Model, blending the best ofGE’s proven management systems and NCHL’s expertise in lead-ership innovation, research, evaluation, and benchmarking.
NCHL Strategy
• Span the industry reaching comprehensively across:
- Career levels: career-entry, mid-career, advanced career
- Industry sectors: providers, suppliers, insurers, policy
- Professional disciplines: administration, nursing, medicine,behavioral health
- Academia and Practice
• Develop programs based upon sound research and globalbest practices
• Focus on rapid development, testing, and deployment of programs
• Accelerate adoption of best practices through learningcollaboratives and benchmarking
• Systematically evaluate programs to assess learning outcomesand performance improvement—evidence-based managementpractice
• Broad dissemination to the field via publications and strategiccollaboration
Although healthcare is making important strides, the currentenvironment requires continued attention and commitment todeveloping leaders and teams. The result is the new Institutefor Transformational Healthcare Leadership, whose focus is todrive healthcare leadership and high performance through the
development of organizational capabilities and individualleadership skills. By building on each organization’s expertise,the Institute will drive the development of programs to equipleaders with the right skills at the right point—key mile-stones—in their careers. The result will be highly competentleaders who have the knowledge and resources to transformtheir organizations into top centers of healthcare excellence.
The uniqueness of the Institute’s learning programs and leader-ship systems is that it combines world-class practices of leadershipdevelopment informed by NCHL’s design team of leadinghealthcare executive practitioners, evidenced-based manage-ment research, rigorous independent evaluation,and continuousrevision of all programs. This approach will set a new standardfor the entire industry.
Emphasizing action learning and team-based methods,the Institute seeks to eliminate the silos that may be basedon profession, career stage, or industry sectors as it tacklesthe problems that face hospitals and health systems. Theframework of the programs always incorporate and balancethe values-based, mission-driven goals of healthcare with theglobal best practices required for talent management andorganizational excellence.
Industry Environment
• Industry quality performance has improved but moresubstantial improvements in cost, quality, and access arebeing demanded
• National and state healthcare reform efforts underscore theimportance of leadership development
• Leadership development is being addressed by somelarger systems, but gaps remain in industry segments(e.g., freestanding community, rural, mental health) as well assystemic changes in the larger systems
• Awareness and adoption of best practices mustbe accelerated
• More effective collaboration between the academiccommunity and practice has begun and must be built upon
• Health management accreditation has adopted a competency-based approach, but professional certification standardsremain unchanged
• Vigorous action is required to assure diversity in leadership
Transformational Excellence:The Key to Tomorrow’s Healthcare Leaders
6 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
�omas M. Priselacrecipient of the2007 National Healthcare Leadership Award,for his lifetime of work to improvethe field of healthcare leadership.
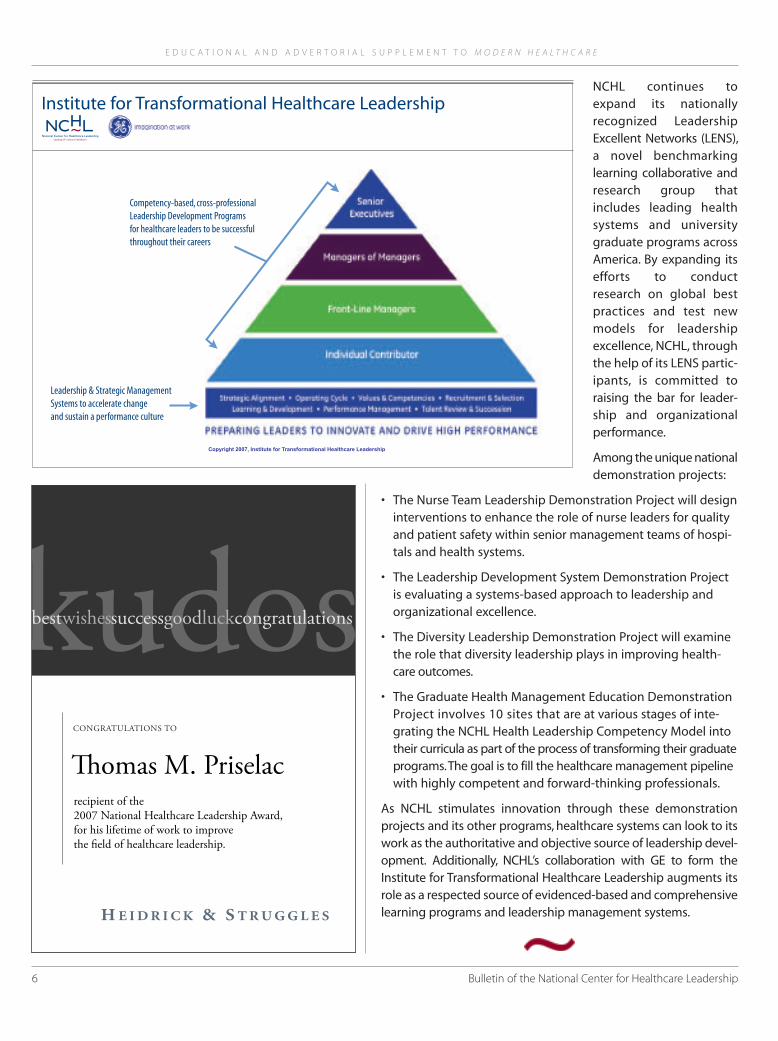
NCHL continues toexpand its nationallyrecognized LeadershipExcellent Networks (LENS),a novel benchmarkinglearning collaborative andresearch group thatincludes leading healthsystems and universitygraduate programs acrossAmerica. By expanding itsefforts to conductresearch on global bestpractices and test newmodels for leadershipexcellence, NCHL, throughthe help of its LENS partic-ipants, is committed toraising the bar for leader-ship and organizationalperformance.
Among the unique nationaldemonstration projects:
• The Nurse Team Leadership Demonstration Project will designinterventions to enhance the role of nurse leaders for qualityand patient safety within senior management teams of hospi-tals and health systems.
• The Leadership Development System Demonstration Projectis evaluating a systems-based approach to leadership andorganizational excellence.
• The Diversity Leadership Demonstration Project will examinethe role that diversity leadership plays in improving health-care outcomes.
• The Graduate Health Management Education DemonstrationProject involves 10 sites that are at various stages of inte-grating the NCHL Health Leadership Competency Model intotheir curricula as part of the process of transforming their graduateprograms.The goal is to fill the healthcare management pipelinewith highly competent and forward-thinking professionals.
As NCHL stimulates innovation through these demonstrationprojects and its other programs, healthcare systems can look to itswork as the authoritative and objective source of leadership devel-opment. Additionally, NCHL’s collaboration with GE to form theInstitute for Transformational Healthcare Leadership augments itsrole as a respected source of evidenced-based and comprehensivelearning programs and leadership management systems.
Copyright 2007, Institute for Transformational Healthcare Leadership
Competency-based, cross-professionalLeadership Development Programsfor healthcare leaders to be successfulthroughout their careers
Leadership & Strategic ManagementSystems to accelerate changeand sustain a performance culture
Institute for Transformational Healthcare Leadership
Congratulations on receiving the 2007 National Healthcare Leadership Award.
Connecting members.Delivering results.
Thomas M. Priselac, M.P.H.President and CEO
Cedars-Sinai Health System
VHA values the contributions you
make to our Alliance and the communities
you serve.
Tom,
Congratulations on this
well-deserved National
Healthcare Leadership Award.
Cedars-Sinai Medical Group and
Cedars-Sinai Health Associates thank you
for your 1,000% support of all our efforts.
It has not gone unnoticed.
With Love and Thanks,
John C. LawChairman
Cedars-Sinai HealthSystem
Association ofAmerican Medical
Colleges
AtlantiCare
Chamberlain Group
Rush UniversityMedical Center
Surgical CareAffiliates
congratulationsto Thomas M. Priselac
Your valuesand leadership
are an inspirationto this and future
generations.
9December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
Geoffrey S. CalhounDirector, Business ExcellenceBaxter International
John R.GriffithAndrew Pattullo Collegiate ProfessorDepartment of Health Management & PolicyUniversity of Michigan School of Public Health
Marie E. SiniorisPresident and CEONational Center for Healthcare Leadership
INTRODUCTION
Improved performance in healthcare is a clear mandate for thecoming decade. Although many hospitals and healthcare sys-tems face substantial challenges in responding to this man-date,1 a growing number have achieved superior performance,and even more have begun a journey to excellence. Theseorganizations deliver high-quality services, satisfy patients andcaregivers, and keep their costs low enough to enable them tothrive financially on standard Medicare and insurance pay-ments. Their successes have been consistent and stable; no onein these organizations is pressing for a return to the old ways.Operating across a broad spectrum of metropolitan and ruralAmerica,2 these organizations have followed paths based onsound organizational theory and documented successes inother industries. What they have accomplished and how canserve as valuable guidance for organizations seeking to makesimilar achievements.
One of the best documented examples of excellence in hospi-tal management is provided by recipients of the MalcolmBaldrige National Quality Award. (Box 1 summarizes the reviewprocess used to make the awards.) Congress established thisprogram in the late 1980s to stimulate improvement in thequality and efficiency of American industry. 3 Applicants for theawards must submit a 50-page application responding toCriteria for Performance Excellence covering seven major orga-nizational elements: leadership, strategy, customers, informa-tion and knowledge, work force, operations, and results.4
While the Baldrige program is not the only avenue to high per-formance, it embodies leadership and management principlesnow recognized by both practitioners and academicians asfundamental to success. Given the rigor and standardization of
the award process, the recipients represent an audited and reli-able model of excellence.To articulate this model, the NationalCenter for Healthcare Leadership analyzed the recipients’ pub-lished applications for the years 2002 to 2006, with emphasison healthcare but attention to other industries.5 We endeav-ored to identify the recipients’ leadership style, including boththeir common leadership processes and examples of particu-larly successful practices. We interviewed senior managersfrom all healthcare recipients and three recipients from otherindustry sectors, soliciting responses to three critical questions:
• What were the key actions that qualified your organizationto receive the award?
• How has your organization sustained its excellence in leader-ship since receiving the award?
• What advice would you give to someone in a position like yourswithin an organization undertaking the Baldrige process?
The Foundation of Leadershipin Baldrige Winning Organizations
Box 1.The Baldrige Review Process
• All applications are reviewed by teams of trainedexaminers.
• Assessments are based on evidence of approach—development of sound, evidence-based plans,processes, measures, and actions; deployment—achievement of uniformity across all units of theorganization; learning—refinement through cyclesof evaluation and encouragement of breakthroughchange; and integration—the harmonization ofplans, information, resources, and analyses tosupport key organization-wide goals.
• In scoring, 45 percent is related to results and12 percent to leadership; no other process variablereceives more than 9 percent.
• Potential award recipients are selected for a sitevisit by the examiner team, which verifies applicationstatements and presents findings to a panelof judges.
• Award recipients must commit to public sharingof information and best practices.

10 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
The interviews were recorded and summarized by the inter-viewer. Interviewees were given the opportunity to correct orexpand the portions of these summaries used in this paper.
The results of these efforts show clearly that the award recipients,like other documented high-performing healthcare organiza-tions, operate in ways that distinguish them from the average.Their operating processes can be grouped under two majorthemes: (1) leadership—creating a culture and climate ofsupport and responsiveness for all patients, workers, and otherstakeholders; and (2) continuous process improvement—an ongoing program of performance measurement andevidence-based analysis of work processes focused by a set ofsound strategies.
LEADERSHIP
The leadership style and organizational culture of excellentorganizations have shifted steadily from a “transactional” to a“transformational” approach. Transformational organizationsplace strong emphasis on a shared vision, collaborative effort,and personal rewards from work.6,7,8,9 In his book Good to Greatand the Social Sector, Jim Collins elaborates the core concept as“Level 5 leadership” or “legislative leadership.” The healthcareexecutives we interviewed sometimes call it “servant leader-ship.” According to Collins, transformational leadershipemploys“persuasion,political currency,and shared interests.” It“builds enduring greatness through a paradoxical blend of per-sonal humility and professional will,” and it is demonstratedwhen employee stakeholders “follow when they have the free-dom not to.”10 This leadership style must be supported by allmanagers in the organization—hundreds or thousands of peo-ple with a consistent message. In Baldrige recipient hospitals,transformational leadership is implemented through specific,carefully managed processes guided by common concepts:
• Empowering workers—encouraging them to participatein goal achievement rather than simply contributingspecific efforts.
• Negotiating workplace goals rather than issuing orders.
• Making managers accountable to their subordinates—obligating them to answer questions and eliminate factorsthat limit worker performance.
The remainder of this section reviews five essential aspects oftransformational leadership: (1) a focus on mission, vision, andvalues; (2) a culture of teamwork and change; (3) communicationand transparency; (4) rewards and recognition; and (5) leader-ship development.
Focus on Mission,Vision, and Values
The healthcare award recipients we interviewed universallyemphasize a strong patient focus in their mission, vision, andvalues.These commitments are reviewed annually by the exec-utive team and governing board and updated periodically withextensive stakeholder participation. Once established, the mis-sion, vision, and values are widely distributed and referencedsuch that most workers (employees, physicians, volunteers, andcontract workers) receive daily reinforcement.
All new associates are introduced to the organization’s mission,vision, and values early in the recruiting process. Most awardrecipients ask applicants for positions in the organization tosign a statement attesting that they understand and will sup-port them. Management’s commitment to transformationalapproaches is also made clear during orientation for new workers.Senior managers commonly meet and personally educate newassociates. Mentors are provided. Questions are encouraged,and transformational leadership is illustrated by example.
SSM Health Care, the first healthcare award recipient andthe only complete system to be recognized by the Baldrigeprogram, provided the following model:
Nearly 3,000 employees and physicians participated infocus groups across the system to define the organiza-tion’s mission and values during 1999. Out of this discus-sion came recommended wording for a single, more con-cise, and memorable mission statement and core values.During 2000, educational sessions were conductedat each of the entities to communicate the new missionand core values to all physicians and employees. Theeducation, designed to give definition to the mission andvalues, included group discussions of the personalmeaning of the mission and values to individuals. A“Meeting in a Box” tool kit, including a video, brochures,and pocket cards, was used to facilitate consistentdeployment. Educational programs conducted in2001…served to reinforce the mission and values.11
Sr. Mary Jean Ryan, CEO of SSM Health Care, added inher interview:
It was a very proud time for us when we developed ourmission statement. It involved every level of the organiza-tion from every facility. Some people probably thoughtthey did not want to be involved, but after it was donethey thought it was a wonderful experience. I hadabsolutely nothing to do with it other than to ask that itbe short enough that I could remember it. When 3,000people know that they have had a significant role indeveloping the mission, it’s not mine, it’s theirs.

11December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
Culture of Teamwork and Change
An emphasis on common goals promotes teamwork,discouragesblame, and creates a culture in which change is expected andwelcome. In hospitals, an emphasis on process and measure-ment shifts the culture from one of silos and domains ofauthority to one of evidence-based analysis and collaborativeprocess improvement.
At Saint Luke’s Hospital of Kansas City:
The leadership structure is characterized by a strongfoundation for collaboration between administrationand the medical staff. The medical staff is representedin each component of the governance structure.12
Richard Hastings, President and CEO of Saint Luke’s Hospitalof Kansas City and Saint Luke’s Health System, added:
This structure is in place to ensure medical staff leadersshare responsibility as perspective leaders in our high-level measurement architecture, our balanced scorecard.By having one member of the medical staff share respon-sibility with each administrative perspective leader,Saint Luke’s ensures that high-level strategy flowsthrough the organization. This enhances the alignmentof our organization in the five strategic areas on ourbalanced scorecard: People, Clinical and AdministrativeQuality, Customer Satisfaction, Growth and Development,and Financial.
Another important initiative that enhances our culture ofteamwork is our nursing shared governance program.Saint Luke’s Hospital of Kansas City first initiated sharedgovernance in nursing nearly two decades ago and nowevery hospital within the Saint Luke’s Health Systemstructures nursing management around our five strategicperspectives using shared governance.
We live our mission, “the best place to get care, thebest place to give care.” Achieving the level of successthat earned us the Malcolm Baldrige National QualityAward didn’t come without growing pains. We hadsome doubters when we were first planning dramaticchange and then adopted Baldrige as our managementmodel back in the 1990s. Now the doubters recognizethe value Baldrige has brought to our organization.Among other things, earning this level of high perform-ance helps us recruit top-notch physicians and clinicians,and has helped us maintain a record-low nursingturnover rate of less than six percent.
Communication and Transparency
Leadership entails a strong commitment to two-way commu-nication at all levels.Multiple means are used to hear from bothpatients and associates. All leaders are trained in listening andoffering constructive responses to the needs of customers andworkers. Senior managers make a critical contribution, ensur-ing that their actions reinforce the organization’s commitmentand respond to all needs identified through the communicationprocess. As defined by Al Stubblefield, President and CEO ofBaptist Health Care, Pensacola, transparency “becomes howyour organization thinks and behaves everyday.”
At Robert Wood Johnson University Hospital Hamilton:
Senior leaders role model service behaviors and havesigned a formal Senior Leadership Commitment Agreement.[The hospital] provides an environment where employeesunderstand their role and are empowered to achievepersonal and organizational goals through innovativeapproaches. There are several mechanisms that facilitateempowerment and innovation, including:
• Team Talk
• Shared Governance
• Best Practice Sharing Technology [an intranet site]
• External Benchmarking
• Voice of the Customer [a systematic approach usedto aggregate, track, and trend employee andpatient concerns]
• Service Recovery Process
• Employee Satisfaction, Work-Life Balance, DiversityCommittees13
David Spong, Chair of The Foundation for the Malcolm BaldrigeNational Quality Award and retired Boeing Company VicePresident, is one of two leaders to have guided two organiza-tions to receipt of the Baldrige award (the other is John Heer,quoted below). According to Spong:
Only the senior leader can sustain the effort.The leader ofthe organization is a true believer who is willing to puthim or herself on the line and also understands the needto stay the course. But after a while, Baldrige thinkingbecomes habit. At one Boeing unit, we worked on theBaldrige for nine years before I left. My successors werenot quite as passionate about Baldrige, but now, sevenyears later, the workers still use the Baldrige approach.
The Leadership Criterion asks“how do your senior leaderslead?” That’s an interesting question. One way to answerit is get feedback on how your workers think you lead.
12 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
You survey your workers, trying to use revealing ques-tions. You get groups together to tell you what theythink.We used a 360-review process and reported back tomanagers. We had each manager pick the two thingsthey scored worst on and solve them by involving theworkers. The lesson is that you don’t have to solve everyproblem,you just have to try, to show good faith.After wedid this, our survey response rates went to the high 90s.People knew we were serious. Survey feedback related toa formal communications plan deployed by the seniorleaders, [and] was used to improve that plan.
Rewards and Recognition
Transformational leadership rewards success. It is forward looking,analyzing opportunities for improvement, negotiating goals,and scrupulously avoiding blame. The reward process beginswith goals that are realistic and achievable. Good goals areaccepted by the team, usually because they are backed bycarefully developed improvements in work processes, and theyare almost always achieved.The rewards are personal satisfactionfrom achievement, public recognition, and material gain.Achievement is celebrated, publicized, and reinforced withcash and prizes, often supported by the personal participationof senior leaders. Managers expect to achieve their goals andoften receive substantial pay incentives for doing so. Extensionof incentive compensation to all employees is widespread.
Bronson Methodist Hospital, for example, maintains “a cultureof fun and fabulous prizes” characterized by:
• Thank-you notes
• On-the-spot recognition
• Leader recognition toolbox
• Celebrations (tied to goal achievement) and prizes
• Hospital Week, Nurses’Week, Employee Appreciation
• Annual events—picnic, holiday banquet, children’sholiday party
• Service awards and annual recognition banquet
• Nursing Excellence Awards
• President’s Team Awards
• Bonuses (gainshare, key contributor, productivity, pre-ceptor, certification/advanced degree completion)14
At Bronson Methodist:
Effective reward and recognition of all employeesreinforces a culture of excellence.The executive team hascultivated a culture that celebrates success with fun andfabulous prizes. Be it the annual service awards banquet,employee picnic, or a special occasion, employees may
receive pre-paid gas cards, delicious treats, or the chanceto spin the BMH Wheel of Fortune for a $500 voucher.Theexecutive team participates in all formal and informalrecognition events, administers key contributor bonuspools, allots department-specific recognition funds, andwrites thank you notes to recognize staff for their efforts.15
According to Michele Serbenski, Bronson Methodist’s ExecutiveDirector of Corporate Effectiveness and Customer Satisfaction:
Leadership visibility is an important reward. We alwayssay thank you, we always take the opportunity for a paton the back, a round of applause, as opposed to somebig, expensive program.We [have] hardwired that leaderswill round and be available. All our leaders need to knowhow to recognize and reward.We spent an entire trainingsession on “loving them or losing them.” We teach howto round, and why we round, how to use recognitiontool kits—things you can buy from your budget, likemovie tickets, “Bronson bucks” usable in our shopsand cafeterias—and why thank you notes should behandwritten. It’s not rocket science…but you needto teach people how to do those things and why theyare important.
Leadership Development
Among Baldrige recipients, all leaders are expected to developand grow, acquiring additional skills they need to operateeffectively in a transformational culture. The necessary compe-tencies include communication, coaching, and rewarding andrecognizing staff and employees.The recipient organizations haveleadership succession plans.All managers have personal develop-ment plans and access to a wide variety of learning opportunities.Leadership skills are taught explicitly using a variety of methods,including classes,dramatizations,demonstrations, rounds,coaches,and discussion groups. Often leadership training is formalized inquarterly meetings with broad attendance.
According to North Mississippi Medical Center’s Baldrigeapplication:
We believe that leadership is an honor and an obligation:a responsibility to “enable” the ability of every employee,physician and volunteer who chooses to spend theircareers with us. [Our] leadership system is designed toleverage the potential of every leader, front-line employeeand key partner.16
The Center’s leadership development process:
…begins each year with the individual employee submit-ting their Performance Plan (aligned with the critical

13December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
success factors and strategic goals) to their supervisor forreview and approval. The Performance Plan has specificactions under each critical success factor and measurableresults and/or observable behaviors. Employees recordtheir Performance Plan on KEYS TO SUCCESS cards. Eachemployee (all areas, not just direct patient care) includesa patient satisfaction goal as a personal goal to strength-en our emphasis on patient-centered care. As part of anongoing process, performance is formally reviewed afterthe first 90 days of employment and then biannually.During the mid-cycle and annual review process, feed-back is solicited from at least six of each employee’s cus-tomers and/or co-workers to produce a 360-degree eval-uation profile on each of the critical success factors.Employees are rewarded with merit increases basedon performance.17
John Heer, the Center’s President and CEO, expanded on theorganization’s leadership model:
The principles of servant leadership are humility,patience, kindness, selflessness, respect, honesty, integrity,but also a very high level of accountability and respectfor environment. We communicate those in a four-hourseminar format. We use a leadership skills inventory. It’s a360-degree evaluation—your boss, your peers, yourreports. What do you think about this person’s humility?Are they honest? Do you trust them? Are they selfless?Do they respect others? We have nine people do the surveyfor each leader, anonymously, using an online system.
The report has each of the questions with the leader’sown response, and the distribution of other responses.The questions are rank ordered from high score to low,and there are written comments at the end. The leaderdevelops a 90-day action plan that’s specific, and measur-able. Then they meet with their boss and a“consultant”—a person trained in how to review these forms. There’sdiscussion about the action plan and agreement.There’s aprogress report every month. After 180 days, we resurvey.We’ve surveyed senior managers four times. Departmentheads are on their second round. Managers are finishingtheir first round. First-line managers are just starting.
We had several people who were shocked about howthey were viewed. Some of our weaker people left, about5 of 350. Some who had that epiphany really upped theirgame. We asked our leaders to sit down with the peoplein their departments and share the results. We called it“opening our kimonos”—asking for help in areas where[they] have opportunities for improvement.Then they allcome together and work to the common goal.
I have no earthly idea what this process costs. Whateverit costs, it’s worth it, because of what it’s done for theorganization.What it’s done is get people focused on theright thing. I don’t know how to put a value on that. Butthere’s a reason why leadership in the Baldrige is scored120 points, while everything else is scored 85. Everythingstarts with leadership, and in order to become a world-class organization,you have to have great leaders,workingin a humble, servant leadership-type environment. Thisplace is not the same culturally as it was three years ago.Retention has gotten better. We’re now headed for 91.5to 92 percent.
Similarly, Bronson Methodist Hospital invests heavily inleadership development:
A key element of creating organizational sustainability isbeing sure that there are strong leaders today and in thefuture. The executive team takes a lead role in the devel-opment of future organizational leaders. The boards ofdirectors and CEO annually review a formal successionplan for the executive-level staff, including emergent orshort- and long-term plans for replacement of the CEO.The executive team annually reviews performanceappraisal results and formally discusses potential succes-sion opportunities for high achievers. Through activeoversight and participation in the leadership initiative,the executive team guides the process for developingand growing BMH leaders. Executive team membersactively participate in the new management mentor pro-gram as executive coaches. Through the StaffPerformance Management System, each executive talkswith his/her leaders about career progression and futuresuccession opportunities.18
Michele Serbenski added:
Organizational and personal development was hugefor our organization; to invest in leaders in a way thatthey have the skills they need to be effective. We believethat people don’t leave an organization; they leave aleader. They are leaving somebody, because they can’twork with them or for them, rather than some place. Weknew we couldn’t go farther unless we addressed theneeds of all leaders, got the right leaders in each position,and had an ongoing commitment to that.
The successful transition to a transformational culture througheffective leadership processes and leadership developmentovercomes resistance to change and promotes processimprovement. Managers and staff become engaged in thepursuit of excellence in performance through the clear and

14 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
consistent communication of mission, vision, and values; role-model behavior by leaders throughout the organization; anorganizational shift from silos to cross-functional teams; andreinforcement by means of comprehensive reward and recog-nition practices. Leadership, beginning with senior leaders,must develop new skills and change the way time is allocatedto create such a culture. The use of formal and informalprocesses to develop leadership capacity throughout theorganization supports the transition to this culture.
CONTINUOUS PROCESS IMPROVEMENT
As noted above, excellence in performance depends on a com-bination of leadership and continuous process improvement.W. Edwards Deming has articulated the essential synthesis ofthese two foundations.17 The importance of Deming’s balancedapproach has been recognized and documented by manyanalysts in a variety of non-healthcare fields,19, 20, 21, 22, 23, 24 as wellas in healthcare organizations.25, 26, 27, 28, 29 Since Deming’s workwas published, highly sophisticated process improvementmethods have been developed, such as Six Sigma, the ToyotaProduction System, and Lean Manufacturing. These methodsall have their place, but in context. Context, to Baldrige recipi-ents, is leadership plus measurement, strategic alignment,sound governance, and ongoing improvement.
Measurement, Benchmarking, and Performance Analysis
Among recipients of the Baldrige award, performance is carefullymeasured, transparently reported, and systematically bench-marked against outside information.The recipients use scorecardsshowing results for key measures that reflect their critical successfactors.These measures are tracked at the board level and usedto determine incentive pay. They are supplemented by severalhundred more specific measures tailored to individual workteams, covering outcomes and process quality, cost, financialmanagement, patient satisfaction, and associate satisfaction.Many measures are benchmarked by being compared rigorouslywith the best values reported by other organizations.The Resultssection of the Baldrige application reports actual progress andbenchmarks for all aspects of the organization. The trend istoward the use of more measures. North Mississippi MedicalCenter, for example, reported 103 different measures, and SSMHealth Care 68. All these measures are aligned with the keystrategies and overall objectives of the organization.
Measurement is a scientific skill in itself. Each measure must beprecisely defined, acquired through a consistent process, andanalyzed to understand both elements outside the control ofthe system operators and causes of random variation.Benchmarking requires that these processes be stable across
all the contributing sites. Premier, Inc., the hospital performancealliance that received the Baldrige award as a service industryapplicant in 2006, offers both measurement design andcomparative data for benchmarking among its services, as do anumber of competing organizations.
Baptist Hospital developed a reporting system that manysubsequent healthcare recipients have copied and expanded.Senior leaders continually monitor key performance indicatorsvia the monthly Dashboard Report, Budget AccountabilityReport, Clinical Accountability Report of Excellence (a compre-hensive tool that uses an index scoring methodology fordepartmental and hospital-wide results), and 90-day plans inorder to discover opportunities for improvement. If a resultvaries negatively compared to historical, budgeted, or bestpractice targets in cross-departmental areas,a team is assignedto analyze the variance and develop a plan of action accept-able to senior leadership.30
The measures used feed the performance improvementsystem, which analyzes processes and provides the foundationfor new and better goals. At North Mississippi Medical Center:
The senior leadership team focus on action is based on aNO EXCUSES/RESULTS ORIENTATION.The incorporation offacts and results identified via key reporting mechanismsenables an evidence-based focus…Issues identifiedthrough these reports often become subjects of perform-ance improvement teams and may become performancescorecard indicators. Once an [opportunity for improve-ment] is identified, the senior leadership team determinesthe approach to the [opportunity for improvement] andits priority. If it is a minor project, the [senior leadershipteam] will assign the problem assessment and processimprovement to the appropriate leader or [processimprovement] team. If,however, the [process improvement]project is expected to affect the critical success factor-based goals or require substantial financial commitment,the…initiative is reviewed by the board of directors. Thesenior leadership team sets and monitors deadlines forall improvements.31
According to Richard Hastings:
Our balanced scorecard serves as our ultimate measure-ment tool, because it reports our performance in our fivestrategic focus areas. The quarterly report is presented ina way that everyone in our organization can understand.Hospitals employ many individuals with wide ranges ofeducational backgrounds. In my 33 years as a hospitaladministrator, I have found the balanced scorecard to bethe best performance analysis tool. For most employees,

15December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
the balanced scorecard provides a color-coded report bywhich they can see if we are performing below, at, orabove goal as is indicated by the colors green, blue, or red.
At other levels in the organization, such as with themedical staff and our board of directors, the balancedscorecard quantitative results provide color-coded indi-cations of performance and quantitative results that canbe analyzed in depth.
To continually challenge our high performance, we adaptand occasionally change a balanced scorecard measureas part of a refinement cycle for improvement.For example,we are discussing where to place additional resources forpatient safety since we currently perform in the top fivepercent of America’s hospitals in patient safety indicators.We consider benchmarks for ratings where we alreadyperform in the top decile nationally, but the measures onour balanced scorecard represent areas we are targetingfor improvement. Our scorecard measures are set to helpus dive into areas that need improvement to move us totop decile performance.
Jena Abernathy, Senior Vice President, Human Resources andWorkplace Resources at Premier, explained:
We bring everybody together around data. Start withyour data and compare yourself to whatever peer groupmakes you comfortable. We will not base decisions onopinions, we will look at data. You can use these data toidentify opportunities and create consensus among yourstakeholders. You can sit down with your physicians andshow the comparisons.
Strategic Alignment and Integration
The strategic process for Baldrige recipients emphasizes ongoinglistening to all stakeholders; a systematic annual surveillancereport shared by governance, senior management, medicalstaff leadership, and many middle managers; governanceagreement on major goals and directions; and a cascade ofthose directions down to individual work units.The senior leadersof the organization own the planning process and use it to createan organization-wide focus on what is most important. Overtime, the list of what is most important is usually narrowed to avital few. At North Mississippi Medical Center, senior leadersestablished 5 Critical Success Factors: people, service, quality,financial, and growth, in order of importance. Similarly, RobertWood Johnson University Hospital Hamilton established5 Pillars, and Bronson Hospital created a focus on the 3C’s:clinical excellence, customer and service excellence, and corpo-rate effectiveness.
In most organizations, these focal points form the basis for thescorecard, communications, and all meeting agendas. The finalstrategy adopted by the board cascades from core businessrequirements to organizational objectives, supporting actionplans for each team and, in most organizations, individualassociates. At each level, realistic goals are carefully negotiatedbased on measured performance, benchmarks, and stakehold-er needs. Goals are achieved through systematic analysis andimprovement of work processes.
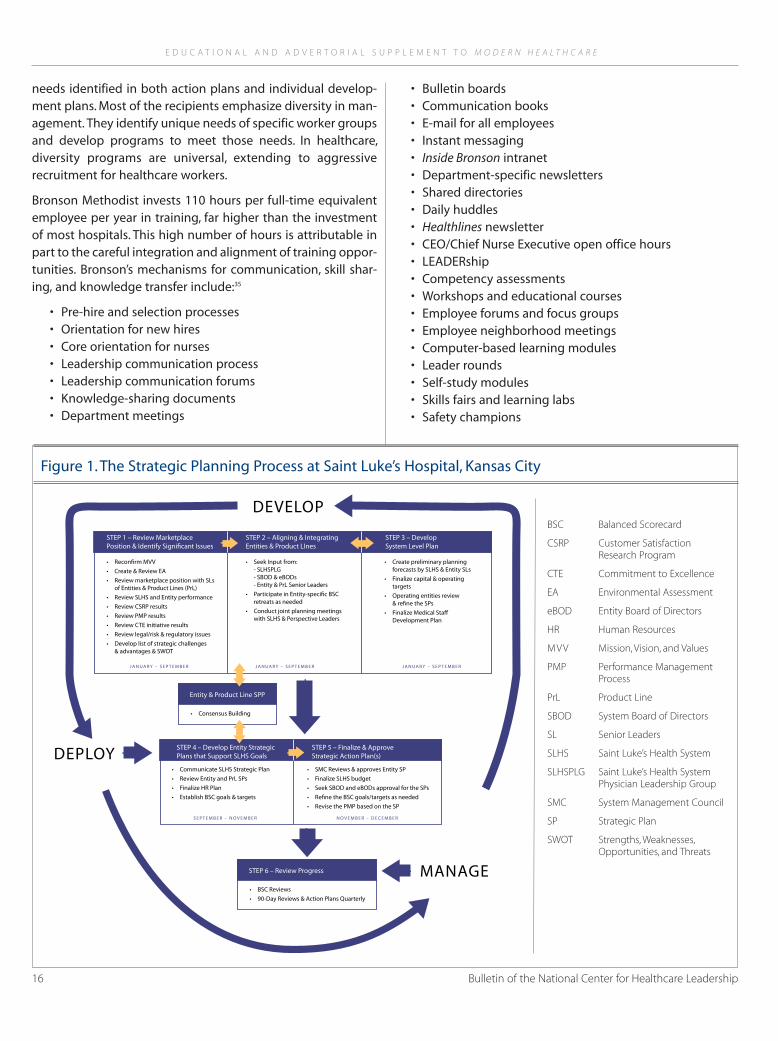
The model used by Saint Luke’s is not as detailed as some.However, it contains the key elements (Figure 1).32 At Saint Luke’s:
A framework to promote a culture of clinical and techno-logical advancement has also been established…[that]includes the establishment of centers of excellence,medical education endowed chairs, shared governancewithin the nursing department, visiting professors,resident and medical student education, allied healtheducation programs and Saint Luke’s College of Nursing.33
According to Richard Hastings:
We align with three approaches: the balanced scorecard,the strategic plan, and the 90-day action plan. Employeeand administrative performance evaluations are alsoaligned with these. In order to enhance communicationand maximize our strategic efforts, we hold five retreatseach year during which we spend a full day on each oneof the five strategic focus areas, which are also the fivebalanced scorecard perspectives.
Boeing Aerospace began using the Baldrige criteria as a frame-work for its own internal improvement cycle. Boeing is a largeorganization, providing information and training, aircraft mod-ifications, maintenance, and modernization to customersaround the world. To develop a uniform approach to theformulation of strategic questions and goal negotiations, eachof its 10 sites structured its annual budgeting and improve-ment identification process according to the Baldrige criteria.The result was a common framework and language, and aneffective vehicle for sharing best practices. Valuable gains inprocesses were achieved, and several of the local sites wonstate awards. Most important, the process led to improvementsin customer service that have helped Boeing maintain a strongcompetitive position and to improvements in efficiency thathave increased profit margins.34
Learning and Personal Development
Organizational and personal development is supported by arich learning environment. The Baldrige recipients systemati-cally develop training and education programs to address
16 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
needs identified in both action plans and individual develop-ment plans. Most of the recipients emphasize diversity in man-agement. They identify unique needs of specific worker groupsand develop programs to meet those needs. In healthcare,diversity programs are universal, extending to aggressiverecruitment for healthcare workers.
Bronson Methodist invests 110 hours per full-time equivalentemployee per year in training, far higher than the investmentof most hospitals. This high number of hours is attributable inpart to the careful integration and alignment of training oppor-tunities. Bronson’s mechanisms for communication, skill shar-ing, and knowledge transfer include:35
• Pre-hire and selection processes• Orientation for new hires• Core orientation for nurses• Leadership communication process• Leadership communication forums• Knowledge-sharing documents• Department meetings
• Bulletin boards• Communication books• E-mail for all employees• Instant messaging• Inside Bronson intranet• Department-specific newsletters• Shared directories• Daily huddles• Healthlines newsletter• CEO/Chief Nurse Executive open office hours• LEADERship• Competency assessments• Workshops and educational courses• Employee forums and focus groups• Employee neighborhood meetings• Computer-based learning modules• Leader rounds• Self-study modules• Skills fairs and learning labs• Safety champions
STEP 1 – Review MarketplacePosition & Identify Signi�cant Issues
STEP 2 – Aligning & IntegratingEntities & Product LInes
STEP 3 – DevelopSystem Level Plan
• Recon�rm MVV• Create & Review EA• Review marketplace position with SLs
of Entities & Product Lines (PrL)• Review SLHS and Entity performance• Review CSRP results• Review PMP results• Review CTE initiative results• Review legal/risk & regulatory issues• Develop list of strategic challenges
& advantages & SWOT
• Seek Input from:- SLHSPLG- SBOD & eBODs- Entity & PrL Senior Leaders
• Participate in Entity-speci�c BSCretreats as needed
• Conduct joint planning meetingswith SLHS & Perspective Leaders
• Create preliminary planningforecasts by SLHS & Entity SLs
• Finalize capital & operatingtargets
• Operating entities review& re�ne the SPs
• Finalize Medical Sta!Development Plan
J A N U A R Y – S E P T E M B E R J A N U A R Y – S E P T E M B E R J A N UA R Y – S E P T E M B E R
STEP 4 – Develop Entity StrategicPlans that Support SLHS Goals
• Communicate SLHS Strategic Plan• Review Entity and PrL SPs• Finalize HR Plan• Establish BSC goals & targets
STEP 6 – Review Progress
• BSC Reviews• 90-Day Reviews & Action Plans Quarterly
STEP 5 – Finalize & ApproveStrategic Action Plan(s)
• SMC Reviews & approves Entity SP• Finalize SLHS budget• Seek SBOD and eBODs approval for the SPs• Re�ne the BSC goals/targets as needed• Revise the PMP based on the SP
S E P T E M B E R – N O V E M B E R N O V E M B E R – D E C E M B E R
Entity & Product Line SPP
• Consensus Building
DEPLOY
DEVELOP
MANAGE
BSC Balanced Scorecard
CSRP Customer SatisfactionResearch Program
CTE Commitment to Excellence
EA Environmental Assessment
eBOD Entity Board of Directors
HR Human Resources
MVV Mission, Vision, and Values
PMP Performance ManagementProcess
PrL Product Line
SBOD System Board of Directors
SL Senior Leaders
SLHS Saint Luke’s Health System
SLHSPLG Saint Luke’s Health SystemPhysician Leadership Group
SMC System Management Council
SP Strategic Plan
SWOT Strengths,Weaknesses,Opportunities, and Threats
Figure 1.The Strategic Planning Process at Saint Luke’s Hospital, Kansas City

17December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
• Preceptors• Externships/internships• Management mentor program• Shared governance• Teams, work groups, councils, and committees• Staff performance management system
While other recipients may not be as thorough in capturinglearning opportunities, the themes are the same. At BaptistHospital:
A change in process may involve a number of staffmembers who must be fully engaged for the change tobe successful. If this is the case, a problem-specific educa-tional program may be developed and round-the-clocksessions held to educate staff on the need for the changeand the effect the change will have on their daily respon-sibilities. Key partners, including dietary and environ-mental services vendors, submit and comply with 90-dayplan requirements. Key physician partners undercontract, including emergency room physicians andhospitalists, are also subject to 90-day performanceexpectations of their respective departments.36
Richard Hastings of Saint Luke’s noted that all leaders must beprepared to support the new culture:
Saint Luke’s encourages knowledge sharing and organi-zational learning.Each Saint Luke’s employee participatesin education programs. Clinical education is alwaysimportant but we also focus employee training programson enhancing customer service.
To help employees embrace learning and personal develop-ment, I talk with them when I make hospital rounds. I alsohost employee forums and send regular communicationsabout our performance and about change. I alwaysdiscuss new balanced scorecard measures and explainwhy the measure is important. Our employees share thevision to be the best so encouragement helps them gainconfidence in what they are doing to carry out the vision.In our employee satisfaction surveys, we are in the 99thpercentile on the question, “I am proud to work at SaintLuke’s.” This level of employee pride cultivates an envi-ronment that helps me encourage new learning.Employees are eager to further their personal develop-ment to align with the vision when trust and pride arealive in an organization’s culture.
Educational processes, like any other processes, must be meas-ured and improved. Many of the Baldrige recipients use theKirkpatrick four-level measurement framework of reaction,learning, transfer, and business results.37 That is, they know
whether the associate appreciated, understood, applied, andwas successful in using the training content.
Governance
Effective governance is a high priority for any successful organ-ization.38 Baldrige recipients build it by systematically measuringand improving board performance; aggressively managingconflicts of interest; and using active audit, compensation, andcompliance committees that often maintain reportingarrangements bypassing the CEO.
At Robert Wood Johnson University Hospital Hamilton:
The new [in 2004] Finance, [Human Resources] and AuditCommittee reviews external and internal audits as well asSarbanes-Oxley compliance, which exceeds the not-for-profit industry standard. The Corporate ComplianceOfficer regularly reports to the Board of Trustees onaccreditation, legal and regulatory compliance as well asethics and governance.39
At North Mississippi Medical Center:
Senior leaders continuously reinforce what is acceptableand what is not. In conjunction with the CorporateCompliance Committee of the NMMC board of directors,the leadership team established a strict zero-tolerancepolicy for unethical or illegal activities by any member ofthe organization…The [senior leaders] personallypromote ethical behavior through [the organization’s]NO SECRETS culture and by intentionally raising ethicalissues during their leadership rounds.40
David Spong of The Foundation for the Malcolm BaldrigeNational Quality Award commented:
In some ways, governance is an annoyance. All theserules, compliance officers, and so on. But these are thedevices that keep the organization on track.They remindpeople of what’s important.Under Sarbanes-Oxley, all theBoeing vice presidents had to sign and attest that theirquarterly reports were “true and accurate.” What’s thatmean? We all know how complicated those calculationsare. It makes you stop and think.
Ongoing Improvement
None of the Baldrige recipients is backing away from theBaldrige commitment or approach. All have plans to reapply.(A recipient must wait 5 years before reapplying. SSM HealthCare is now making its second application; Saint Luke’s is nowapplying as a system.) Thus the Baldrige commitment is aphilosophical one. As part of that commitment, leadership
18 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
processes—recruitment, orientation, training, personal devel-opment, the reward structure—and process improvementactivities—measurement, benchmarking, strategic planning,goal setting, performance improvement—are themselvessystematically studied and improved. Advice offered by threeof the CEOs interviewed—Sr. Mary Jean Ryan of SSM HealthCare, David Spong of The Foundation for the Malcolm BaldrigeNational Quality Award, and Richard Hastings of Saint Luke’s—is presented in Box 2.
CONCLUSION
The award recipients are clear on the sources of their success.Support for transformational leadership, combined withsystematically measured and improved performance, allowsthese organizations to achieve top-quartile and benchmarkperformance (see Box 3). The approach sustains and enhancesexcellence, and simultaneously satisfies associates andstakeholders. The recipients’ advice to other CEOs is, as Sr.Mary Jean said,“Do it.”And they are following their own advice,continuing to work on opportunities for improvement,expanding use of the Baldrige approach, and working activelytoward reapplication.
Box 2. Advice from CEO to CEO
Sr.Mary Jean Ryan, FSM
It’s not about winning, it’s about getting better. We’vesaid that everybody who is eligible for a state awardshould apply, not to win the award, but to go throughthe process, because it requires you to answer a lot ofquestions you would not normally ask. And you submityour answers to outsiders.
There’s always some who resist, but when the processeswe put in place really did improve things, they camearound. In one of our markets, we’d had significant loss-es. With the improvements we made with [continuousquality improvement] and Baldrige, they had a $50 mil-lion turnaround in two years.
We picked Baldrige because it’s a whole organizationalimprovement. It isn’t just administrative, or clinical, orfinancial, it’s all of those things. It’s about satisfaction. It’sabout how we take care of our employees. Every singleaspect of the organization is subjected to review.
If you are a CEO or a board member, why would you notdo this? Yes, I know it’s a lot of work. But if you claim thatyou are really about improving the quality of patientcare, then do something. A few CEOs I’ve talked to say,“I couldn’t get my board to agree to this.” I’m trying tofigure out why not. My advice is “do it.”The reality is, youwill never be ready. I say to them,“Why wait?” The scoredoesn’t really matter, except to identify where you needto improve.
E. David Spong
I’d advise people starting the Baldrige [process] that it’snot as tough a struggle as it might look. A lot of peoplesay, “I’d like to do Baldrige, but…” There are all thesefires to fight. That’s kind of the antithesis to Jim Collins’Good to Great. Baldrige actually helps.There are alwaysfires to fight, and the first year is struggle. By the secondyear, the fires are less.The third year is a breeze.
G. Richard Hastings
First, you must have a vision. If you don’t know whereyou are going, you can’t lead there. You must establishmeasurable goals that you can communicate toemployees and medical staff. Engaging in Baldrigerequires thought, deep study, and discussion with otherhospitals and other CEOs. Boeing has been key to SaintLuke’s, because they manage with Baldrige principlesand have earned the award too.
Second, hospital administrators need to spend a lot oftime with their medical staff. CEOs keep the vision alivewhen the medical staff is reinforcing it.By tapping greatmedical staff leaders, hospital administrators can helpphysicians understand how using Baldrige principleswill also positively affect their practices.
My third point of advice to other CEOs is to spend qualitytime with the chair of your board so he or she shares theorganization’s vision as well. Strategy is ignited whenadministrators and hospital boards share vision.
19December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
Box 3. Examples of Performance Excellence Reportedby Healthcare Recipients of the Baldrige Award
• Composite quality score of 96, above the 90thpercentile in HQIDP (Hospital Quality Indicators).
• Industry-leading, 99th percentile patientsatisfaction scores.
• Fully 98 percent of all patients would recommendthe hospital.
• Physician satisfaction 97 percent overall, above thePress-Ganey 90th percentile.
• Operating margins of 7 percent.
• Community support a minimum of 25 percentof operating profits.
• AAA or AA bond rating.
• Registered nurse retention rate of 98 percent,above the national benchmark.
• Overall employee retention rate of 98 percent,above the national benchmark.
• Medicare adjusted length of stay of 3.4 days,below best practice of 3.6 days.
The overall Baldrige business model and criteria for performanceexcellence are based on a series of core values, concepts thatare embedded in the beliefs and behaviors of high-performingorganizations. The first of these core values is visionary leader-ship, which describes the role of senior leaders in both health-care provider and operational and administrative positions.These fundamental responsibilities are to:
• Set directions and create a patient focus, clear and visiblevalues, and high expectations,
• Inspire, motivate, and encourage your entire workforce tocontribute, to develop and learn, to be innovative, and to becreative, and
• Serve as role models through their ethical behavior andtheir personal involvement in planning, communications,coaching, development of future leaders, review of organi-zational performance, and staff recognition
The set of Baldrige winners is both small and self-selected. Theirachievement may reflect unique factors that other institutions can-not duplicate,such as a uniquely supportive environment or specif-ic resources.Similarly,neither this paper nor the longer applicationsummaries fully reflect the whole story.There may be critical events
in the Baldrige process. It is known that other, similar institutionshave begun the Baldrige journey and discontinued it. We do notknow how many organizations have done so, or whether the dis-continuances represent failures or adoption of an alternative,morepromising approach.
Despite these limitations, what these model organizations showis that organizational excellence is within reach for many if notmost American healthcare providers. What has been done inTupelo can be done in Tacoma,Tallahassee, or Toledo. Excellenceis achieved through systematic efforts to change leadership style,organizational culture, skills, and specific work processes. AllBaldrige award recipients enhanced leadership performance atall levels of management and across all boundaries.Through thisapproach they were able to change the organization’s perform-ance culture.Leadership built a committed and trained workforcein a results-oriented culture that expects improvement.
The transformational leader helps team members achieveexcellence, demonstrates resolve, channels his/her personalambition into the organization, takes a legislative approach togoal setting, gives credit for success to others, and takes fullresponsibility for poor results. One of the most daunting issuesin the near future is competition for talent and the ability toattract leaders to the healthcare industry who can assumethese responsibilities. At the heart of the solution to this issueis the ability to develop leadership talent within a nurturingand effective culture. The Baldrige award recipients haveshown how these efforts can succeed.
REFERENCES
1 Griffith, JR, Alexander, JA, Jelinek, RC, Foster, DA.“Is anybody managing thestore? National trends in hospital performance.” Journal of HealthcareManagement.51(6): 392-405; discussion 405-6, November-December, 2006.
2 Griffith, JR,White, KR.“The Revolution in Hospital Management.” Journal ofHealthcare Management.50(3): 170-190, 2005.
3 Baldrige National Quality Award program history and description:http://www.quality.nist.gov/Improvement_Act.htm. Accessed 5/31/07.
4 Ibid.
5 Healthcare winners were SSM Health Care, St. Louis and Baptist Hospital,Pensacola, FL, 2003; St. Luke’s Hospital of Kansas City, MO, 2003; Robert WoodJohnson University Hospital Hamilton, NJ, 2004; Bronson Methodist Hospital,Kalamazoo,MI, 2005; and North Mississippi Medical Center, Tupelo, MS, 2006.The full list of winners and their applications is available at Baldrige NationalQuality Award website: http://www.quality.nist.gov/Contacts_Profiles.htm.Accessed 5/31/07.
6 Pawar, BS, Eastman, KK.“The nature and implications of contextual influenceson transformational leadership: A conceptual examination.”The Academy ofManagement Review.22(1): 80-109, January, 1997.
7 Flamholtz, E, Randle,Y.Changing the Game: Organizational Transformations ofthe First, Second, and Third Kinds.New York: Oxford University Press, 1998.
8 Calhoun, JG, Dollett, L, Sinioris, ME,Wainio, JA, Butler, PW, Griffith, JR,Warden,GL.“Core competencies for healthcare leadership in the 21st century: TheNational Center for Healthcare Leadership competency model.” In press.
9 National Center for Healthcare Leadership, Health Leadership CompetencyModel: Summary. http://www.nchl.org/ns/documents/CompetencyModel-short.pdf. Accessed 8/10/07.
10 Collins, J.Good to Great and the Social Sector.Boulder: Collins, 2005. pp. 9-13.

20 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
11 SSM Health Care, 2002 Baldrige Award Application, p. 1.http://baldrige.nist.gov/2002_Application_Summaries.htm. Accessed 8/6/07.
12 St. Luke’s Hospital of Kansas City, 2003 Baldrige Application, p. 9.http://www.baldrige.nist.gov/2003_Application_Summaries.htm.Accessed 8/6/07.
13 Robert Wood Johnson University Hospital Hamilton, 2004 Baldrige AwardApplication, p. 7. http://baldrige.nist.gov/2004_Application_Summaries.htm.Accessed 8/6/07.
14 Bronson Methodist Hospital, 2005 Baldrige Award Application, pp. 2-3.http://baldrige.nist.gov/2005_Application_Summaries.htm. Accessed 8/6/07.
15 Bronson Methodist Hospital Applications, pp. 2-3.
16 North Mississippi Medical Center, 2006 Baldrige Award Application, pp. 22-23.http://baldrige.nist.gov/2006_Application_Summaries.htm. Accessed 8/6/07.
17 Ibid, p. 1.
18 Bronson Methodist Hospital Application, p. 27.
19 Deming,WE.Out of the Crisis.Cambridge,MA:The MIT Press, 1986.
20 Bell, RR, Elkins, SA.“A balanced scorecard for leaders: Implications of theMalcolm Baldrige National Quality Award criteria.” S.A.M.AdvancedManagement Journal.69(1): 12, 2004.
21 Ghosh, S, Handfield, RB, Kannan, VR, Tan, KC.“A structural model analysis of theMalcolm Baldrige National Quality Award framework.” International Journal ofManagement & Decision Making.4(4): 289, 2003.
22 Seanor, DD.Analysis of the leadership of UW-Stout in winning theMalcolm BaldrigeNational Quality Award in education.Lincoln,NE:The University of Nebraska, 2004.
23 Ahire, SL, Golhar, DY,Waller, MA.“Development and validation of TQM imple-mentation constructs.”Decision Sciences.27(1): 23-77, 1996.
24 Black, SA, Porter, LJ.“Identification of the critical factors of TQM.”DecisionSciences.27(1): 1-22, 1996.
25 Cunningham, AD. Leadership development in Catholic healthcare: A study onservant leadership.St. Louis, MO: Saint Louis University, 2003.
26 Goldstein, SM, Schweikhart, SB.“Empirical support for the Baldrige Awardframework in U.S. hospitals.”Health Care Management Review.27(1): 62-75, 2002.
27 Hirtz, PD. Effective leadership for Total Quality Management.Rolla, MO: Universityof Missouri, 2002.
28 Ryan,MJ.“The spirit of leadership and a commitment to quality transformSSM health care system.” Journal of Organizational Excellence.23(3): 15, 2004.
29 Goonan, KJ, Stoltz, PK. Leadership and management principles for outcomes-oriented organizations.Medical Care.42(4) Supplement: III 31-38, 2004.
30 Baptist Hospital, 2003 Baldrige Award Application, pp. 3-4.http://baldrige.nist.gov/2003_Application_Summaries.htm. Accessed 8/6/07.
31 North Mississippi Medical Center Application, p. 3.
32 St. Luke’s Hospital of Kansas City, 2003 Baldrige Award Application, p. 15.http://www.baldrige.nist.gov/2003_Application_Summaries.htm.Accessed 8/6/07.
33 Ibid, p. 11.
34 Boeing Aerospace Baldrige Application, 2003 Baldrige Award Application,p.3. http://baldrige.nist.gov/2003_Application_Summaries.htm.Accessed 8/6/07.
35 Bronson Methodist Hospital Application, p. 19.
36 Baptist Hospital, 2003 Baldrige Award Application, p.4.http://www.baldrige.nist.gov/2003_Application_Summaries.htm.Accessed 8/6/07.
37 Kirkpatrick, J. “The Hidden Power of Kirkpatrick.” Training+Development.pp. 34-37, August 2007. Kirkpatrick, DL. Evaluating Training Programs:The FourLevels. San Francisco: Berrett-Koehler Publishers, 1998.
39 Bryant, LE, Jacobson, PD.“Best practices for measuring the effectiveness ofnonprofit healthcare boards.”Bulletin of the National Center for HealthcareLeadership.pp. 8-12. December 5, 2006.
39 Robert Wood Johnson University Hospital Hamilton Application, p. 8.
40 North Mississippi Medical Center Application, p. 1.
Sutter Health Proudly Congratulates
Thomas M. PriselacPresident and CEO
of Cedars-Sinai Health System
For advancing health careacross the nation
and inspiringfuture health care leaders.
2007 National HealthcareLeadership Award
~
~
Congratulations!Thomas M. Priselac
President & CEOCedars-Sinai Health System
Upon receiving the 2007 National Healthcare
Leadership Award
For your leadership and contributions to hospitals
and health care, and your commitment to excellence in
patient care, research, education and community service.
21December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
Changing for the BetterBy James H.Hinton, President and CEO,Presbyterian Healthcare Services
Let me begin by stating that as New Mexico’s only private, non-profit healthcare system and it’s largest provider of care, wehave been on the Malcolm Baldrige National Quality Awardjourney for the past five years, and I fully support and appreci-ate the conclusions in the paper.
Healthcare must undergo fundamental changes to respond tochanging customer needs, delivering benchmark clinical results,and providing affordable services.That is why we chose Baldrigeas the performance framework to accelerate our progress.
Even though Presbyterian Healthcare Services is a 99-year-oldorganization that has a history of stability and market-leadingperformance and preference, a few years ago our leadershipteam and Board made the decision to work for national excel-lence. While it’s tempting to settle for being “good,” we con-sciously challenged our organization for greatness. We believedeeply that our patients and members deserve nationallyexcellent healthcare. We chose Baldrige. We believed then,andare even more convinced today, that it is the best way for us toget better, faster. It has turned out to one of the best decisionsour leadership team and Board have ever made.
Our organization has applied to Baldrige twice and was fortu-nate to receive a site visit both times and the rigor and stan-dardization of the award process is a sound model. The criteriadrive our organization to focus on the right things, strive forbenchmark performance (versus local market), and createprocesses that attain sustainable results.The feedback receivedfrom the Baldrige process is brutally honest and provides acatalyst for change.
Like many of the organizations and CEOs that you interviewed,we have fundamentally redesigned our leadership and gover-nance model (which was cited as best practice at both site vis-its); we have become dogged about measurement tied tonational comparative data; and are continuously focusing onimproving our processes to reduce waste and improve care.We view Baldrige as a worldwide standard for best-in-classcompanies who have a systemic, company-wide approach toachieving excellence in every arena of company activities.
Our strategy is to be nationally excellent as measured by theachievement of the “3 Things:” 1) Earning “AA” ratings on our
financial performance; 2) hitting top 10 percent results inpatient safety; and, 3) of course, earning the Malcolm BaldrigeNational Quality Award. The reason for the “3 Things” is not forrecognition, but rather, these things are external validations ofexcellence. It is not “us telling ourselves” we have achievedsomething, but reaching national standards that confirm it.The clarity and rigor of Baldrige lends itself to healthcareextremely well and it has really guided us on this journey. Wehave seen first-hand how Baldrige is changing our organiza-tion for the better. How it focuses us more clearly on ourpatients and members. How it sharpens our concentration onwhat matters most to the people we serve.
It’s no accident that Baldrige puts its greatest focus on results,and the bottom line for us is that we can track our performanceover the journey and point to specific achievements that mat-ter to our patients and members. Baldrige has helped us docu-ment the lives we have saved in our hospitals; manage a healthplan that is only one of nine in the country to have attained an“excellent” rating by the National Committee for QualityAssurance in all products; attain a “AA” rating for our financialstewardship; and care for our diabetic patients with outcomessurpassing the 90th percentile nationwide.
For me, Baldrige really connected where we have beento where we want to go. Presbyterian has always beenfortunate to have great people. Baldrige has taught us tocreate the processes to support our great people. In manyrespects, we have “burned the boats” on quality. Never willwe retreat to a disconnected, haphazard approach toperformance excellence.
I appreciate your work on this white paper and am hopeful thatit will encourage other healthcare organizations to adopt thisframework for performance excellence to improve our indus-tries’ outcomes for those we have the privilege of serving.
Competent CommunitiesBy David C. Leach,MD, Former Executive Director,Accreditation Council for Graduate Medical Education
It is said that the second Buddha may come as a community;perhaps reflection on the article offered by Calhoun, Griffith,and Sinioris in this supplement can prompt us to think aboutthe importance of community in improving healthcare. The
Commentaries on The Foundation of Leadershipin Baldridge Winning Organizations

22 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
first Buddha was enlightened and compassionate; what wouldan enlightened and compassionate community look like?
The people in organizations and the relationships they havewith one another can either inhibit or facilitate purpose. Whathelps them facilitate purpose? As to people, aside from raresociopaths, most people show up to work actually wanting tohelp. Dee Hock has said that the following criteria should beused in judging people: integrity, motivation, capacity, under-standing, knowledge, and experience.1 He says the criteriamust be used in the order given and for good reason; for exam-ple, if someone lacks integrity and is highly motivated they canget the organization in deep trouble. Transformational leader-ship, as illuminated by the interviews in the Calhoun piece,could also make use of these criteria. The focus on empowerment,communication, and transparency are enhanced by integrity,motivation,and capacity.The trouble with Hock’s approach is thatthe most important criteria are the hardest to measure – hence wetend to overweight experience (show me the resume) and under-weight integrity (how would I measure that?).
Once people are convened their relationships become crucialto the achievement of purpose. Some of the relationships aredictated or heavily influenced by structure (anatomy)—whereare folks on the organizational chart—but much is determinedby physiology—how the various people interact. Deep atten-tion to purpose and principle, harvesting the wisdom of thoseclosest to the front line, incorporating improvement into thework in a way that makes it part of the work rather than anextraordinary event, all depend on reducing barriers betweendecision-makers and decision-implementers.The anatomy canget in the way. A better model might be the “microsystem”model of Paul Batalden that is more aligned with the wayhealthcare is actually delivered. Perhaps the “C-Suite” shouldstand for the “Caring Suite” and include all who care.
It may be best to work with rather than against human nature.Every human comes equipped with an intellect (that seekstruth), a will (that seeks goodness), and an imagination (thatseeks beauty).The work of healthcare is aligned with these fac-ulties: to discern and tell the truth; to make good administra-tive and clinical decisions; and to do so in ways that are creativeand sometimes even beautiful.
Using people to get the work done is probably a wrongheadedmodel for transformational leadership; instead we should usethe work to improve the formation of people. Healthcare isnoble work; it has to be done, why not use it to build on andenhance people’s native capacities? The Calhoun articleemphasizes the linkage of transformational leadership, system-atic measurement of performance, and continuous improve-ment of performance. Likewise, Batalden argues that the quali-ty of patient care, the quality of health professional formation,
and the quality of system performance are inextricably linked.2
Metrics should be linked with these three variables to judgeorganizational excellence.
Individual competence is a habit; it is the demonstrated habit ofreflective practice; perhaps organizational competence can bedefined as the demonstrated habit of reflective practice as well.The organizations interviewed in the Calhoun piece seem tohave found a way to use the Baldrige Award system to measureand reflect upon performance at the community level.Some arereapplying in order to carry the conversations, reflections, andmeasurements forward in an attempt to improve even further.Those of us in healthcare can learn from these leaders.We needto transform the industry as well as each organization.
1 The Trillion Dollar Vision of Dee Hock.Fast Company, October, 1996.
2 Batalden, P. Personal communication, July, 2007.
Baldrige as a Path to ExcellenceBy Richard P. Miller, President and CEO,Virtua Health
CEO’s, Senior Leaders, and Board Members are acutely awarethat the mandate for change in American healthcare is clear—improve patient safety and quality, reduce costs, and make theresults of your organization transparent and public. Calhoun,Griffith, and Sinioris have provided a valuable reference forhealthcare leaders clearly showing HOW this can be achievedusing the Baldrige criteria as a path to excellence.They providean executive overview of the two key aspects of healthcareBaldrige Winners:
• The key role leadership serves in establishing a culturewhere mission, vision, and values are alive and activelysupport and align staff in caring for patients
• The critical contribution of measurement and relentlessperformance improvement
At a time of major internal and external stressors to the health-care industry, the Baldrige Criteria are a blueprint for organizationimprovement and sustainability.
By studying the Baldrige winners both inside and outside ofthe healthcare industry, the authors identify key factors forsuccess in using and applying the criteria. This work alsounderscores the fact that this is a leadership-driven processthat cannot be delegated.The results achieved become a mirrorof the leadership team’s ability.They highlight the fact that thecriteria are a tool for improvement—an assessment ofstrengths and weaknesses as seen by objective examiners whoonly have the organization’s success as their focus.This is not aregulatory body, a customer, or a payer—this is a group of
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
consultants who delve deeply into the organization with a setof criteria that is closely correlated with success.
The message is clear that an organization has to take the firststep. You hear it from the “voices” of past winners: you beginwhere you are and grow from there. Sister Mary Jean Ryan ofSSM, CEO of the first healthcare Baldrige winner is quotedmaking the point that it is not about winning the award, it isabout getting better as an organization.The Baldrige Criteria canbe a bit complicated and daunting by its length and language.The white paper is a primer for leaders and covers the majorhighlights of most of the categories. It helps translate keyaspects for Senior Leaders who want to take their first step.
Virtua Health has had experience with two applications at thestate level using the Baldrige Criteria.The Senior Team relies ona core group of writers to put the application together for theirreview. The feedback reports have been invaluable as a sourceof guidance for improvement efforts. As we move to apply onthe national level, this white paper will be helpful to promoteunderstanding of their role in leading this journey.
An opportunity to strengthen this white paper or to perform acompanion document would be to delve further into some of thekey elements that examiners look for when reading an applica-tion such as describing“how’s”and“what’s”and discussing with
a bit more clarity the fact that they are looking for an organiza-tion’s: Approaches, Deployment, Learning, and Integration.
The review of the evaluation of results came across with moreclarity that examiners and Senior Leaders should look carefullyat what they measure (customer requirements, key processes,etc.) and that they look for industry and best-in-class bench-marks. Organizations are judged not only on their currentresults but their improvement over time, current trends, andcomparison to industry and best-in-class benchmarks.
It is fitting that the National Center for Healthcare Leadershipwrite this article and provide a tool for CEO’s and their teams tofind a better approach to succeeding in today’s complex andchallenging environment. Given the rigor and standardizationof the award process, the recipients represent an audited andreliable model of excellence. They are uniquely qualified toidentify and share key success factors in the use and applica-tion of the criteria. Calhoun, Griffith, and Sinioris focus onBaldrige as a path to excellence provides senior leaders withthe critical success factors, styles, and practices to make theirorganization healthcare industry leaders. Organization’s thatuse the criteria for organizational transformation and sustainedimprovement clearly have an advantage.
Herman Miller, Inc., commends Thomas M. Priselac,2007 National Healthcare Leadership Awardrecipient, and his commitment to leadership in the Healthcare industry.
�omas Priselac, on years of innovation, commitment, and leadership.
Intermountain Healthcare would like to congratulate
�omas M. Priselac of Cedars-Sinai Health System
for his achievements, leadership and continued
commitment to quality healthcare. �ank you
for your example of excellence in every
aspect of medicine.
CONGRATULATIONS TO
FOR HIS
LEADERSHIP & COMMITMENT
TO PATIENTS,
HEALTHCARE STAFF
AND COMMUNITIES.
TThhoommaass MM.. PPrriisseellaacc
Cedars-Sinai Health SystemPresident and CEO
American Hospital AssociationChair-Elect
National Center for HealthcareLeadership 2007 Award Recipient
Overall Great Guy
www.uhc.edu
THE POWER OF COLLABORATION
The University HealthSystem Consortiumand its members proudly honor:
Thomas M. Priselac Recipient of the 2007
National Healthcare Leadership Award
Thank you for your remarkable dedication to academic medicine, performance improvement, and
the next generation of healthcare leaders.
© 2007 University Hospitals 07-MIS-026
Congratulations!
Thomas F. Zenty lll, CEO,Achilles A. Demetriou, M.D., Presidentand the University Hospitalscommunity applaud Tom Priselac,recipient of the 2007 National Healthcare Leadership Award.
In conjunction with its proud support of the
National Center for Healthcare Leadership
Johnson & Johnson
Health Care Systems Inc.
honors
THOMAS M. PISELAC2007 recipient of the
nchl national healthcare
leadership award
© Johnson & Johnson Health Care Systems Inc. 2007
To a person making a difference.
From the people of Cedars-Sinai.
Congratulations.
Congratulations to our own Thomas M. Priselac onreceiving the 2007 National Healthcare Leadership Award.
Your commitment to quality healthcare sets the standard.
www.cedars-sinai.edu
C
27December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
A few things are deeply embedded in Tom Priselac’s make up. Firstare values—including the importance of community—that wereinstilled by his parents. Second is the inspiration from a collegeathletics coach who taught him about commitment and passion.And third, the quest to continually improve. Those are the attrib-utes Priselac has brought to Cedars-Sinai Health System in his roleas President and CEO, and which have been a perfect fit with theculture and mission of Cedars-Sinai. When you put it all togetherthe result is one of the nation’s most widely respected academicmedical centers.
How do you lead a large, complex healthcare systemlike Cedars-Sinai?
A key role for people in leadership is communication: I tryto spend a lot of time communicating with a wide variety ofpeople and groups in Cedars-Sinai tackling issues as well asunderstanding changes in the external environment andengaging people in identifying what our response to theseissues should be. Face-to-face communication is an importantpart of the culture of Cedars-Sinai. E-mail alone would notwork. In this setting a lot of personal presence, personal atten-tion, and carrying the message directly is required. We do itwith regularly scheduled medical staff, management, andemployee opportunities. I try to use whatever opportunitiesI can to reinforce our messages. Personal communication mustalso come from the other members of the management teamas well as our medical staff leadership. In addition to having anexcellent management team, I am fortunate to have an enlight-ened medical staff and medical staff leaders who share ourcommitment to quality and carry that message to theircolleagues throughout the institution.
What is the most significant thing you do in yourleadership role?
The job of a leader in a healthcare system like Cedars-Sinai—one that is large and complex—is to help translate the externalenvironment and realities to everyone involved in the organi-zation and then to work with them to identify a common visionabout what we need to do to continue as a national leader inproviding outstanding patient care, research, and education.
Thomas M. Priselac Talks About Leadership and theInevitability of Change in Healthcare
The National Center for HealthcareLeadership is proud to present the2007 National Healthcare LeadershipAward to Thomas M. Priselac, Presidentand Chief Executive Officer of theCedars-Sinai Health System in LosAngeles. During his nearly 30-yearhealthcare career, Tom has earneda reputation for commitment to excel-lence at every level of Cedars-Sinai—patient care, research, education, andcommunity service. As president of aleading academic medical center,he ishighly regarded for his willingness toinnovate, take bold moves, create newknowledge, and share his findingswith the field. Under his guidance,
Cedars-Sinai has earned and maintained a stellar reputation for its patient-centered care, biomedical research,and inspired learning environment for allhealth professions. Tom has made lasting improvements to the health fieldand important contributions to future leaders.For his dedication to advancingthe nation’s healthcare, NCHL salutes Tom Priselac and thanks him for hisinspiration to the next generation of healthcare leaders.
Thomas M. PriselacPresident & CEOCedars-Sinai Health System
EducationBA, BiologyWashington and Jefferson College
MPH, Public Health, Health ServicesAdministration and PlanningUniversity of Pittsburgh
CareerMontefiore HospitalPittsburgh (1975 – 1979)
Cedars-Sinai Health System(1979 – Present)
1988 – Executive Vice President
1994 – President and CEO
Boards and other affiliationsChair-electAmerican Hospital Association
Past ChairAssociation of AmericanMedical Colleges
Chair, Healthcare CommitteeLos Angeles Chamber of Commerce
Adjunct faculty memberUCLA School of Public Health
About Cedars-Sinai Health SystemFounded in 1902, Cedars-Sinaihas more 2,000 physicians, 9,000employees and 2,000 volunteers.In 2007 it was named to the U.S.News andWorld Report “BestHospitals” Honor Roll for excellencein 10 medical specialties. For thepast 19 years, it has been named LosAngeles’ most preferred hospital forall health needs in an independentsurvey of area residents. In additionto its 952-bed medical center,Cedars-Sinai Health System comprisesa Medical Delivery Network (includ-ing the Cedars-Sinai Medical Groupand Cedars-Sinai Health Associates)and the Burns & Allen ResearchInstitute. Cedars-Sinai is internation-ally renowned for its diagnostic andtreatment capabilities, breakthroughsin biomedical research, and out-standing medical education.

Are you bothered that a few people still think ofCedars-Sinai primarily as the“hospital to the stars?”
While it speaks to our quality that people who can go anywherein the world for healthcare choose to come here, celebrities areactually a very small portion of the patients we care for. A lotof people aren’t aware of the fact that Cedars-Sinai has one ofthe largest Medicaid patient volumes of any hospital inCalifornia, and that we provided more than $135 million incommunity benefit last year.
So your job as a leader is to inspire and motivateyour staff?
I’ve learned over the years that a big part of the art of leader-ship is to make sure we have agreement and understandingabout our goals and our assignments, and then I try not tomicromanage.At the same time,we have effective accountabil-ity mechanisms in place to help people achieve their goals.Cedars-Sinai attracts employees, medical staff, and traineeswho are high-achievement oriented.
What other tools do you think are critical to be asuccessful leader?
I come out of a planning background, so part of my nature isthe extensive use of planning tools. I have found that creatingthe right kinds of tools and committing to making them relevantwill drive communication. We use a dashboard that reportsdesired outcomes for different aspects of our institution’s mission.We also have very active quality committees. We continuallyreview “red-green” reports that show targets met and not met,which allows us to focus on how to overcome obstacles to success.
Beyond the tools, what does your leadership stylelook like?
If you go beyond the tools, I think the role of the leader is torecognize that the need for change is inevitable, and then toembrace it. Part of what you have to do as a leader is embracechange and have an ongoing commitment to excellence. And aleader needs a deep personal commitment to what he is doing.Healthcare is a very collaborative endeavor, so people can quicklyascertain the nature and extent of a leader’s commitment.
What are the big issues healthcare and Cedars-Sinaiare facing?
The increasing demand for value in healthcare is the biggestchallenge. We are doing a lot of work on this in our setting.We have the good fortune of having a reputation for excellentquality. But our cost structure—because of our academic
mission and because of the nature and volume of our high-endspecialty clinical services, research, and teaching—is higher.We are working on ways within our mission to be moreefficient and more effective. This relates to operations andeffective resource management.
How does Cedars-Sinai approach leadershipdevelopment?
We have organized programs to provide leadership andmanagement development that crosses different career stagesand career paths. One of the things we are proudest of is ourphysician leadership development program, which is availableto all members of our medical staff. This program, designed bythe physicians, has involved physicians from every department.Each physician takes on a current issue facing the institutionand works with other physicians and administrative leaders toreach consensus on solutions. A recent project focused on theturnaround time on imaging reports. The projects oftenintegrate physician issues with some part of our broader qualitystrategies, such as hand hygiene. So a couple of physiciansmight tackle interventions to increase compliance and comeup with strategies that can be effectively implemented. Westrive to find issues that are relevant to their individual inter-ests as well as being relevant to the entire medical staff.
What is one of the thorniest leadership issues health-care faces?
During the ‘90s and early part of this century, graduateprograms in healthcare management, like other healthcareprofessions, lost their attractiveness for a lot of young people.That is starting to turn around, but still remains an issue: weneed to have sufficient numbers of people with master’sdegree educations—that is critical. The other crucial need is tostrengthen the depth of leadership skills in our managers andsupervisors. It is a big challenge for hospitals to find time forleadership development. Currently, a lot of leadership skillscome about from experience, which is fine, but it needs to beaugmented by formal opportunities for leadership development.
What is the role of teamwork in managing alarge hospital?
Caring for patients is the ultimate team sport, especially in ateaching hospital where a patient may come in contact with asmany as 70 people in a 24-hour period.You cannot take care ofsomeone well or efficiently without a substantial team effort.A good example is our participation in the nationalTransforming Care at the Bedside initiative, which engages ournurses, other members of the healthcare team, and patients
28 Bulletin of the National Center for Healthcare Leadership
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
29December 2007
E D U C A T I O N A L A N D A D V E R T O R I A L S U P P L E M E N T T O M O D E R N H E A L T H C A R E
and their families in designing and testing new patient-cen-tered approaches. Another initiative is our MD/RNCollaborative, which is in every operating unit of the hospital.The whole purpose is to look at the interaction of thenurse/physician team to get their ideas about how to worktogether to provide the best possible care for each patient.
What is the role for a prominent healthcare leader inthe political arena?
There’s no question that politicians are anxious to hear fromhospitals and the healthcare field. Those of us in healthcareleadership need to articulate the critical role that hospitals playin their communities and give objective advice to others whowill be involved in making policy decisions, to help themunderstand how these changes will impact our communities.We also need to listen carefully to the concerns expressed byother constituencies about healthcare, and take thoseconcerns to heart.
As a past chair of the AAMC (Association of AmericanMedical Colleges) and current chair-elect of the AHA(American Hospital Association) you have taken yourleadership skills beyond Cedars-Sinai.Why is thatinvolvement important to you?
Hospitals need to make sure that real-life information is beingincluded when broader policy decisions are being made thataffect hospitals, physicians, or other parts of the deliverysystem.So it is in the best interest of all hospitals to have a pres-ence and voice at the larger policy platform. Despite the extrawork, this involvement was instilled in me from the beginningof my career in hospital administration—that participating isthese organizations is part of what I signed up for.
Kaiser Permanente
salutes the National
Center for Healthcare
Leadership and its
honoree Tom Priselac
for their dedication
and commitment
to the health of our
communities.
For more information about Kaiser Permanente, call 1-800-464-4000 (toll free) or visit kaiserpermanente.org
©20
07Ka
iser
Perm
anen
te
congratulations
to a manwho gets
the
BIGpictureand the
L I T T L E
pictureright.
I live because of your talentsand the gifts of those you lead.
ALL THE BESTSari Weiner
Healthcare Executive& CS Patient
�
�
Abbott salutes Tom Priselac for his outstanding professional and personal commitment to developing our next generation of healthcare leaders.
www.spencerstuart.com
spencer stuart recognizes great leaders.
it’s our business.
Spencer Stuart is a proud sponsor of the 2007 National Healthcare Leadership Award.
We congratulate Thomas M. Priselac, president and chief executive officer of Cedars-
Sinai Health System and this year’s recipient of the National Healthcare Leadership
Award. An admired leader in the healthcare community for more than two decades, he
has helped set the standard for community service, dedicated leadership and outstand-
ing philanthropic commitment.
Spencer Stuart joins NCHL in saluting him for his efforts in advancing the nation’s
healthcare and for his inspiration to future healthcare leaders.
Healing People,Strengthening CommunitiesCatholic Healthcare West is pleased to congratulate Thomas Priselac on being honored with the 2007 National Healthcare Leadership Award. We are humbled by his work to improve the healthcare landscape and we applaud his accomplishments in shaping healthcare policy and practice.
42 Hospitals in California, Arizona & Nevada
50,000 Employees,$10.5 Billion in Assets
In 2007, Provided Over $922 Million in Community Benefits and Care for the Poor
California’s LargestNot-for-Profit Hospital Provider
Over 4 Million PatientsAssisted Annually
Baxter employees share your commitment to making a meaningful difference in people’s
lives. At Baxter, we apply our expertise in biotechnology, medical devices and specialty
pharmaceuticals to develop innovative therapies that save and sustain lives around the
world. It is this higher purpose that binds us as a company and as global citizens.
baxter.com
Baxter is proud to support the 2007 Invitational Symposium and National Healthcare Leadership Award
2007 Nat iona l Hea l thcare Leader sh ip Award
Thank you to all who support NCHLand honor and celebrate the lifelong
accomplishments of distinguished leadersin our field.
The National Center for Healthcare Leadership
IS PLEASED TO PRESENT
Thomas M. Pr i se lacPRESIDENT AND CHIEF EXECUTIVE OFFICER, CEDARS-SINAI HEALTH SYSTEM
WITH THE
H O N O R I N G H I S L I F E T I M E O F W O R K T O I M P R O V E T H E H E A LT H C A R E F I E L D
S A V E T H E D A T E
2008 National Healthcare Leadership AwardThursday, December 4, 2008