Embed Size (px)
Citation preview
i | P a g e
National Guideline For
Kala-azar Case Management 2016 3
rd Edition
National Kala-azar Elimination Program (NKEP)
Communicable Disease Control (CDC)
Disease control Unit
Directorate General of Health Services (DGHS)
Ministry of Health and Family Welfare (MoHFW)
Government of the People’s Republic of Bangladesh
ii | P a g e
NAMES OF THE MEMBERS IN UPDATING THE
NATIONAL GUIDELINE FOR KALA-AZAR CASE MANAGEMENT 2016
Chief Adviser:
Prof. Dr. Abul Kalam Azad
Director General
Directorate General of Health Services
Advisor
Prof. Dr. Sanya Tahmina
Director, Disease Control & Line Director, CDC
Directorate General of Health Services
Chairman Prof. Dr. Md. Ridwanur Rahman
Head Department of Medicine
Shaheed Suhrawardy Medical College Hospital, Dhaka
Member Secretary
Dr. A.F.M. Akhtar Hossain
Deputy Programme Manager, Kala-azar Elimination Program
Communicable Disease Control, Director General of Health Services
Technical Writer
Dr. M. G. Mostafa,
Technical Advisor, NKEP, CDC, DGHS-Dhaka
Board of Editors:
1. Prof. Dr. Baizid Khoorshid Riaz, Director, NIPSOM, Dhaka
2. Prof. Dr. Be-Nazir Ahmed, Dept. of Microbiology, NIPSOM, Dhaka
3. Prof. Dr. Akhtarun Nahar Nira, Dept. of Microbiology, SSMCH, Dhaka
4. Prof. Dr. Abul Khair Mohammad Shamsuzzaman, Dept. of Microbiology, RMCH, Rajshahi
5. Dr. Abdus Sobur, Deputy Director, CDC, DGHS-Dhaka
6. Dr. AKM Manjurul Islam, Deputy Director, M&PDC, CDC, DGHS-Dhaka
7. Dr. Kamar Rezwan, NPO, WHO-Bangladesh, Dhaka
8. Dr. Dinesh Mondal, Senior Scientist, icddr,b, Mohakhali, Dhaka
9. Dr. M. G. Mostafa, Technical Advisor, NKEP, CDC, DGHS-Dhaka
10. Dr. Robed Amin, Associate Professor, Medicine, DMCH, Dhaka
11. Dr. Shahjada Selim, Assistant Professor, Endocrinology, BSMMU, Dhaka
12. Dr. Md. Abdullah Yusuf, Assistant Professor of Microbiology, NINH, Dhaka
13. Dr. Mostafa Kamal, Civil Surgeon, Mymensingh District, Mymensingh
14. Dr. Parikshit Kumar Parh, Deputy Civil Surgeon, Mymensingh District, Mymensingh
15. Dr. Md. Moshihur Rahman, UH&FPO, Trishal UHC, Trishal, Mymensingh
16. Dr. Robiul Islam, RMO, Trishal UHC, Trishal, Mymensingh
17. Dr. Sabera Sultana, NPO, Neglected Tropical Disease, WHO-Bangladesh, Dhaka
18. Dr. Mizanur Rahman, National Consultant, KEP, WHO-Bangladesh, Dhaka
19. Dr. Ariful Basher, In charge of SKKRC, Infectious & Tropical Disease, MMCH, Mymensingh
20. Dr. Md. Mahbubur Rashid, SMO, Kala-azar Elimination Program, CDC, DGHS-Dhaka
21. Dr. AKM Kayum, SMO, Kala-azar Elimination Program, CDC, DGHS-Dhaka
22. M Mamun Huda, Assistant Scientist, icddr,b, Mohakhali, Dhaka
23. Dr. Mohammad Sohel Shomik, Deputy Program Coordinator, KalaCORE, Dhaka
24. Md. Shahadot Hossain, Manager, M&E, KEP, CDC, DGHS-Dhaka
25. Ms. Fahima Yeasmin Lira, Data Manager, KEP, CDC, DGHS-Dhaka
26. Ms. Shyla Faria, Procurement Officer, KEP, CDC, DGHS-Dhaka
27. Mr. Pankaj Kumar Ghose, Data Management Officer, KEP, CDC, DGHS-Dhaka
iii | P a g e
ABREVIATIONS
AIDS Acquired Immune Deficiency Syndrome
ARV Anti-retroviral Therapy
BCC Behavior Change Communication
CL Cutaneous Leishmaniasis
DDT Dichloro Diphenyl Trichloroethane
DGHS Directorate General of Health Services
H&FWC Health & Family Welfare Centre
HIV Human Immuno Deficiency Virus
ICT Immune-chromatographic test
IEDCR Institute of Epidemiology Disease Control and Research
IPD Inpatient department
IRS Indoor Residual Spray
IM Intramuscular
ITN Initial Training Network
IV Intravenous
KA Kala-azar
LAmB Liposomal Amphotericin B
MIS Management Information System
MO Medical Officer
MOU Memorandum of Understanding
NGO Non-Government Organization
NKA New Kala-azar
OPD Outpatient department
PCR Polymerase Chain Reaction
PKDL Post Kala-azar Dermal Leishmaniasis
RD Rural Dispensary
RDT Rapid Diagnostic Test
RKA Retreatment Kala-azar
rK39 RDT rK39 Rapid Diagnostic Test
RTAG Regional Technical Advisory Group
SC Sub Centre
SEARO South East Asian Regional Office
SOP Standard Operation Procedure
SSG Sodium Stibogluconate
TB Tubercle Bacillus
UHCs Upazila Health Complexes
UH&FPO Upazila Health and Family Planning Officer
WHO World Health Organization
iv | P a g e
Message Bangladesh has successfully accomplished and achieved numbers of targets under Millennium
Development Goal‟s (MDGs) and is committed to achieve ambitious set of targets under “Sustainable
Development Goals (SDGs)” aiming to transform Bangladesh a middle income country by 2030. The
country is committed to achieve “Good Health and Well-being (SDGs-3)” aiming to ensure healthy lives
and promote well-being for all; bring an end of wave of Malaria, Filaria, Kala-azar, Tuberculosis,
HIV/AIDS and other communicable diseases; attain universal health coverage; and provide access to
safe-effective medicines and vaccines for all.
Bangladesh seeks to create conditions whereby the people of the county have the opportunity to reach and
maintain the highest attainable level of health. The Ministry of Health & Family Welfare (MoHFW) being
the responsible ministry ensures health and well-being of the citizens by expanding access to quality and
equitable healthcare; develops people healthier, happier and economically productive; and make
Bangladesh a middle income country by 2021. We are also committed to achieving the universally agreed
goals in specific areas as set out in the declarations of various world summits including SDGs by 2030.
It is indeed very depressing information to learn that Kala-azar, a neglected tropical disease, claims more
than 50,000 lives every year worldwide. The disease being endemic to central and north part of
Bangladesh for many decades has created public health problems and affected poor and the vulnerable
group of people in the community. However, I feel very happy to know that the National Kala-azar
Elimination Program (NKEP) of Disease Control Division, Communicable Disease Control of Directorate
General of Health Services (DGHS) has developed strategies to eliminate the disease from the country.
I am pleased to know that NKEP has updated the existing treatment guideline: „National Guideline for
Kala-azar Case Management 2016‟. I believe this management guideline will provide strategies,
principles, course of actions and recommendations to the concerned health professionals and help them to
improve the approach of treatment, management, and prevention of Kala-azar at all levels of health
facilities in Bangladesh.
I would like to congratulate technical experts, clinicians, doctors, researchers and health managers for
taking active part in the development of „National Guideline for Kala-azar Case Management 2016‟. I
wish every success of National Kala-azar Elimination Program for taking a leadership role in the
elimination of Kala-azar disease from Bangladesh.
Joy Bangla, Joy Bangabandhu.
Long live Bangladesh
Photo
Honourable Prime Minister
Government of the People‟s Republic of
Bangladesh
v | P a g e
Message
Ministry of Health & Family Welfare (MoHFW) is committed to comprehend Vision 2021 by developing
healthier, happier and economically productive citizens of Bangladesh. The MoHFW being the leading
and responsible ministry has been creating conditions whereby the people will be able to achieve and
maintain the highest attainable level of health, and to ensure access to quality healthcare services in
Bangladesh. The MoHFW has been planning to improve quality, equity and efficiency towards universal
health coverage and would like to achieve Sustainable Development Goals (SDGs) by 2030.
The Kala-azar disease load, being very high in South-Asian region especially in Bangladesh, India and
Nepal, comprises more than fifty percent of the total global disease burden. The government of
Bangladesh, India and Nepal, therefore, signed a memorandum of understanding in 2005 and pledged
their commitment to eliminate Kala-azar from the region and reset a target to reduce the incidence rate of
KA less than 1 case per 10 000 populations by the year 2017. This target has been set in a WHO/SEARO
Regional Summit of Health Minister‟s Meeting held on 9 September 2014 in Dhaka, Bangladesh.
Signatories to this MoU were Bangladesh, Bhutan, India, Nepal and Thailand.
The National Kala-azar Elimination Program (NKEP) of Disease Control Division, Communicable
Disease Control (CDC) of Directorate General of Health Services (DGHS) has developed strategies to
eliminate the disease from the country with a goal to improve the health status of the vulnerable groups
and at-risk population living in Kala-azar endemic areas by eliminating the disease and achieving the
regional and national target by the year 2017. I am happy to know that the NKEP has already achieved the
national target in October 2016.
I have the pleasure to know that the NKEP has updated existing treatment guideline titled: “National
Guideline for Kala-azar Case Management 2016”. I believe the concerned health personnel at every
health facility will receive proper guidance from the national guideline in treating, managing and
preventing Kala-azar disease in the endemic areas of Bangladesh.
I would like to extend my sincere thanks and gratitude to all technical experts, clinicians, doctors,
researchers and health managers for taking active part in the development and updating the national
guideline for Kala-azar Case Management 2016‟. Last but not least, I would like to congratulate all the
staffs of NKEP of Disease Control Unit, CDC of DGHS-Dhaka.
Joy Bangla, Joy Bangabandhu.
Long live Bangladesh
Photo
Honourable Minister
Ministry of Health & Family Welfare
Govt. of the People‟s Republic of Bangladesh
vi | P a g e
Message
The Ministry of Health & Family Welfare (MoHFW) is the responsible ministry for improving quality,
equity and efficiency of health services towards attaining universal health coverage and achieving
sustainable development goals by 2030 through strengthening governance and stewardship of health
sectors; improving equitable access to and utilization of quality health services; and establishing a high
quality health workforce to be available across the health system. The MoHFW through its coordinated
efforts aims to comprehend long term impacts in the improvement of health indicators that are targeting to
reduce the disease mortality rates, improving nutritional situation, and preventing all types of
communicable and non-communicable diseases in Bangladesh. Bangladesh is a hot-humid tropical country providing an excellent breeding environment for the growth
and multiplication of sandflies, the only vector for Kala-azar disease to transmit within the poor
community. Despite high endemicity prevailing for a period of last few decades, the incidence rate of
Kala-azar, however, has been decreasing remarkably since 2005 as a result of coordinated efforts and
effective strategies implemented by the NKEP of Disease Control Division, Communicable Disease
Control (CDC) of Directorate General of Health Services (DGHS); and as of October 2016, the country
has achieved national target of incidence rate of less than 1 case per 10 000 populations. I am glad to know that NKEP of Disease Control Division, CDC of DGHS is going to publish „National
Guideline for Kala-azar Case Management 2016‟ which will be acting as a strategic guiding document for
all level of health facilities and will be using as a resource text for all physicians, clinicians, researchers
and nurses involved in the treatment and management of Kala-azar disease in Bangladesh.
I would like to congratulate and express my heartiest thanks and gratitude to all the staff of NKEP, CDC,
DGHS and all those experts and resource persons who were involved in every endeavor to the
development of this treatment guideline.
I wish every success of NKEP, Disease Control Division, CDC of DGHS for eliminating Kala-azar
disease from Bangladesh.
Joy Bangla, Joy Bangabandhu
Long live Bangladesh
Honourable State Minister
Ministry of Health & Family Welfare
Govt. of the People‟s Republic of Bangladesh
Photo

vii | P a g e
Message
The Ministry of Health & Family Welfare (MoHFW) has developed 4th Health Nutrition Population
Sector Program (HNPSP: 2017-2022) focusing to increase access to quality healthcare and improve
equity along with efficiency in both service delivery and health systems strengthening. The 4th HNPSP
aims to achieve Vision 2021 by materializing number of Operational Plans (OPs) and CDC‟s OP intends
to reduce the burden of communicable diseases from the country in general and achieve elimination of
Kala-azar, a neglected tropical communicable disease, by 2017.
We have identified number of issues and challenges that need attention to eliminate Kala-azar from the
country. The PKDL patients for example are acting as a potential reservoir and do not always come to the
treatment facilities, therefore, the low coverage of PKDL poses a great challenge; re-emergence of the
disease as a result of resistance to anti-leishmania drug may become a great threat; provisions of the early
diagnosis and prompt treatment may be jeopardized because of the patient‟s low level of health seeking
behavior; quality of integrated vector management will be at stake because of the non-availability of
effective insecticides; asymptomatic cases of Kala-azar may act a sources for transmission of disease in
the community; and cross-border issue may also contribute disease transmission.
We have set some functional activities to make the elimination of kala-azar faster and effective. In order
to able to make elimination successful, we should continue active case search to be done on a six month
interval within the next five years up to 2021; procure effective drugs, diagnostic kits, insecticides and
other logistics for the program; conduct operational research relevant to diagnose, treatment and vector
management; and carry out training and orientations for the clinicians, researchers, nurses, and other
relevant health staff using the “National Guideline for Kala-azar Case Management 2016 as resource
material.
I would like to express my great appreciation to the Disease Control Unit, Communicable Disease
Control (CDC) of DGHS for publishing „National Guideline for Kala-azar Case Management 2016‟ to
improve not only the cases but to prevent and control of Kala-azar from Bangladesh.
Secretary
Ministry of Health & Family Welfare
Photo
Honourable Secretary
Ministry of Health & Family Welfare
Govt. of the People‟s Republic of Bangladesh

viii | P a g e
Message
I am pleased to know that National Kala-azar Elimination Program (NKEP) of Disease Control Division,
Communicable Disease Control (CDC) of the Directorate General of Health Services (DGHS) has
developed “National Guideline for Kala-azar Case Management 2016”aming to train the clinicians,
doctors, nurses and other relevant health professional. I am confident that the clinicians will find the
present guideline as a ready reference text for consultation during the course of daily clinical works. I
believe the present guideline articulates the recent and upgraded treatment procedures and will serve as a
standard tool for the treatment and prevention of Kala-azar disease in Bangladesh.
Bangladesh Government is committed to eliminate Kala-azar from country by 2017 and the country has
already achieved national elimination target of less than 1 case of Kala-azar per 10 000 populations
(Incidence rate is 0.28 in October 2016) through implementing National Kala-azar Elimination Program
(NKEP) strategies and activities. Early diagnosis and prompt treatment with vector control are some of
the main approaches targeted for the elimination of the disease. A number of conventional and innovative
interventions including „Active Case Search‟ through index-based approach, camp-based approach, and
blanket house-to-house search applied during the 3rd HPNSD contributed in the achievement.
The production of “National Guideline for Kala-azar Case Management 2016” is regarded as an essential
resource to pursue policies and regulations in the management of drug therapy in all stages of kala-azar
disease recovery. This treatment guideline summarizes recommended treatments for common forms of
New Kala-azar (NKA), Post Kala-azar Dermal Leishmaniasis (PKDL) and Cutaneous Leishmaniasis
(CL); provides information to make the kala-azar treatment standardized throughout the health system;
assists clinicians and patients in making decisions about healthcare for specific clinical circumstances
such as Kala-azar Treatment Failure (KATF), Relapse Kala-azar (RKA) and Adverse Drug Reactions
(ADR); and promotes rational use of anti-leishmania drugs in hospitals, upazila health complexes and
other clinic settings.
I would like to extend my thanks and gratitude to all technical experts including clinicians, researchers,
health managers and other relevant health professional for updating the present guideline, evaluating the
effectiveness of anti-leishmania drug, assessing and controlling the adverse drug reactions, and proposing
the important strategy for improving medicine use in Kala-azar health care management system.
I wish all the members of NKEP a great success.
Prof. Dr. Abul Kalam Azad
Director General
Directorate General of Health services
Photo
Honourable Director General
Directorate General of Health Services Ministry of Health & Family Welfare

ix | P a g e
Message
Kala-azar is a major neglected tropical disease and a major public health problem in Bangladesh. The
disease commonly affects the poor members in the community in developing countries and has been
persisting in this sub-continent for quite a long period, and is responsible for number of deaths each year.
As a collateral benefit of blanket DDT spraying during malaria eradication program during 1960s, the
kala-azar disease was controlled to major extent in our country. However, in late 1980s it had re-emerged
and spread quickly in the central and north of Bangladesh.
The National Kala-azar Elimination Program (NKEP) has been initiated in 2007. Three indicators such as
kala-azar detection rate, treatment completion rate and vector control coverage rate have been set. The
early diagnosis and prompt treatment of the disease are ensured, the surveillance and monitoring system is
strengthened, and the indoor residual spraying (IRS) is instituted. We are committed to achieve national
goal by 2017. This optimistic and realistic goal could be apprehended by realizing the most important
favorable factors such as (i) biological factor where the human is only reservoir for Kala-azar parasite and
Phlebotomus argentipes sandfly is probably the only species transmitting disease in Bangladesh.
The Kala-azar eliminate strategies aim to diagnose and treat the cases and control the vector. Kala-azar
case detections and management along with the improvement of treatment outcome indicators are
regarded as the important criteria for monitoring the progress of activities. Moreover, the vector (sandfly)
management with characteristics of sandfly, its life cycle, behavior & bionomics and control measures are
also very important to eliminate the disease from the country. In Bangladesh, India and Nepal, there is
only one type of sandfly found which is very sensitive to all types of insecticides. The Indoor Residual
Spraying (IRS) is confined to only household and cattle shed, and limited to community in a geographical
areas affecting only to 98 upazilas of Bangladesh.
The recent and upgraded „National Guideline for Kala-azar Case Management 2016‟ in Bangladesh is
published with the aim to provide a handy and quick guideline to diagnose and treat a Kala-azar and
PKDL patient as well as effectively handle the IRS program, ensuring a robust and effective disease and
vector surveillance and develop public awareness through community participation.
At the end I would like to thank from my core of heart to all the technical experts, clinicians, researchers,
and health managers providing their kind support and scientific efforts to publish the „National Guideline
for Kala-azar Case Management 2016‟ in Bangladesh.
Dr. A.F.M. Akhtar Hossain
Deputy Program Manager
National Kala-azar Elimination Program
Photo
Deputy Program Manager, KEP, CDC
Directorate General of Health services
Govt. of the People’s Republic of Bangladesh
x | P a g e
Message
Diseases Control Division, Communicable Disease Control (CDC) of Directorate General of Health
Services (DGHS) has been implementing National Kala-azar Elimination Program (NKEP) since 2007,
pursuing WHO/SEARO Regional Strategic Framework for Elimination of Kala-azar from the South-East
Asia Region, setting goal to improve the health status of vulnerable groups and at-risk population, and
building target to reduce the annual incidence rate of Kala-azar less than 1 case per 10 000 populations at
all levels of endemic upazilas of Bangladesh by 2017.
The management and control of Kala-azar disease continues to be one of the highest public health
priorities in Bangladesh. The program strategy is aimed to reduce the Kala-azar disease burden and to
achieve national goals and targets. The country has also started a number of target-oriented health
programs to eliminate other communicable diseases like malaria, filaria, soil transmitted disease, rabies,
HIV/AIDS, hepatitis, nipah, avian influenza, etc under the leadership of Disease Control Division,
Communicable Disease Control of Directorate General of Health Services (DGHS).
The NKEP is implemented as a part of CDC OP (Operational Plan) under 3rd
Health, Population and
Nutrition Sector Development Program (HPNSDP: 2011-2015). The strategic objectives of the national
kala-azar elimination program is to ensure early diagnosis and complete management of the cases,
implement integrated kala-azar vector management (IVM), have effective patient and vector surveillance
system, conduct operational research, and build institutional capacity.
The revised WHO/SEARO Regional Framework for Elimination of Kala-azar Strategy: 2016-2020 has
been adopted by the country emphasing key indicators for elimination. The indicators are: (i) detection
rate – tracking all new cases of kala-azar in an endemic area within a given year; (ii) treatment completion
rate – the target for treatment complition rate in any endemic upazila should be above 90% with effective
anti-leishmania drug; and (iii) vector control for coverage rate – the number of households protected
through indoor residual spray (IRS) to be 100 percent.
It is my immense pleasure that the Disease Control Division, Communicable Disease Control (CDC) of
the Directorate General of Health Services (DGHS) is going to publish „National Guideline for Kala-azar
Case Management 2016‟ which will provide the latest treatment and management for Kala-azar patients.
I would like to express my heartiest thanks to all the resource persons, consultants, experts and physicians
who gave their valuable time; provided technical and financial support; and contributed to the revision
and updating the important guideline within the shortest possible time.
Prof. Dr. Sanya Tahmina
Director, Disease Control & Line Director, CDC
Directorate General of Health Services
Photo
Director, Disease Control & Line Director, CDC
Directorate General of Health services
Govt. of the People’s Republic of Bangladesh
xi | P a g e
CONTENT PAGE
Abbreviations………………………………………………………………………………………………… iii
Messages……………………………………………………………………………………….………….…… iv
Content Page………………………………………………………………………………….……………… xii
Executive Summary………………………………………………………………………………………… xvii
CHAPTER: ONE……………………………………………………………………………………….…… 1
1. INTRODUCTION ……………………………………………………………………………………. 2
1.1 Background – Kala-azar………….……………………………………………….…………………. 2
1.2 Current Global Burden of Visceral Leishmaniasis……………....…………………….…………...……. 2
1.3 Vector Sandfly – Characteristics, Life Cycle and Control Measures..………………………………….. 4
1.4 Life Cycle of Leishmania Parasite……………………………………………………………………….. 6
1.5 Factors favorable for Elimination of Kala-azar………………………………………………………….. 7
1.6 Present situation of Kala-azar in Bangladesh…………………………………………………………….. 8
1.7 Objectives of National Guideline for Kala-azar Case Management ……………….……………………. 13
1.8 Target Audiences for the National Guideline…………………….…….………………..….………...…. 14
1.9 Kala-azar Elimination Program in Bangladesh……………………………………...…………………… 15
1.10 Challenges for Kala-azar Elimination Program in Bangladesh……………………………………...…... 16
CHAPTER: TWO………………..…………………………………………………………………….…… 18
2. DIAGNOSIS OF KALA-AZAR, PKDL AND CL….……………….……..……………………. 19
2.1 Clinical Diagnosis of New Kala-azar (NKA) ……………………………….……………………...…… 19
2.2 Clinical Diagnosis of Post Kala-azar Dermal Leishmaniasis (PKDL) ……….…….…………...……… 20
2.3 Kala-azar with Co-infections…..……………………………………………….………….………..…… 22
2.4 Diagnosis of Kala-azar using rK39 RDT………………………………………………………………… 24
2.4.1 Types of diagnostic tests available for Kala-azar…………………...……………………...…… 24
2.4.2 Procedures of rK39 RDT…………………………………………………………………..…… 24
2.4.3 Interpretation of test of rK39 RDT……………………………………………………………… 25
2.4.4 Effectiveness of rK39 RDT in detecting Kala-azar………………………………………...…… 25
2.4.5 Advantages and disadvantages of rK39 RDT……………………………………………...…… 25
2.4.6 Use of rK39 RDT in National Kala-azar Elimination Program……………….………………… 26
CHAPTER: THREE……………………….…………………………………………………………….… 28
3. TREATMENT OF KALA-AZAR, PKDL AND CL.………………………………….…….…. 29
3.1 Treatment for New Kala-azar (NKA)……..…………………………………………...………………… 29
3.2 Treatment for Post Kala-azar Dermal Leishmaniasis (PKDL)………………………...………………… 32
3.3 Treatment of Cutaneous Leishmaniasis CL)……………………………………..………………………. 35
3.4 Diagnosis and Treatment of Kala-azar in Special Situation.…..………………………………………… 37
3.5 Complete treatment of Kala-azar…….…………………………………………………………………. 39
3.6 Clinical/treatment outcomes in Kala-azar……………..…………………………………………….…… 43
3.6.1 Monitoring of clinical/treatment outcomes rates ………..……………………………………… 45
3.6.2 Key indicators for treatment compliance rate of kala-azar……………………………………… 45
3.6.3 Monitoring of clinical/treatment outcomes variables…………………………………..………. 46
3.6.4 The clinical/treatment outcomes of PKDL………………………………………..……………. 46
3.6.5 Monitoring treatment of outcomes rates calculations…………………………………………… 47
xii | P a g e
3.7 Pharmaco-vigilance Activities……………..……………………………..……………………………… 48
3.7.1 Operational Plan for Pharmaco-vigilance activities……………………………………...……… 48
3.7.2 Indicators of Pharmaco-vigilance activities……………………………………………...……… 49
CHAPTER: FOUR……………………………………………………………..…………………..……… 51
4. KALA-AZAR SURVEILLANCE SYSTEM……...........................……………………………… 52
4.1 Introduction to surveillance…………………………………………………………………….………… 52
4.2 Types of Kala-azar Surveillance….……………………………………………………………………… 53
4.2.1 Passive Case Surveillance…………………………………..…………………………………… 53
4.2.2 Active Case Surveillance………………………………………………………………...……… 56
4.2.2.1 Blanket Approach …………………………………………………………………… 56
4.2.2.2 Camp Based Approach ……………………………………………………………… 56
4.2.2.3 Index Based Approach ……………………………………………………………… 56
4.2.2.4 Incentive Based Approach …………………………………………………………… 56
4.2.2.5 No Kala-azar Transmission Strategy………………………………………….……… 56
4.2.2.6 Approach to Asymptomatic Kala-azar Management…………………………………. 58
4.3 Management of Kala-azar Surveillance………………………………………………………………….. 60
4.3.1 Kala-azar Surveillance Units…………………………………..………………………………… 60
4.3.2 National Rapid Response Team…………………………………………………………………. 61
4.3.3 Surveillance Reporting from UHC………………………………………………………..……. 61
4.3.4 NKA and PKDL Detection from Community……………………………………………...…… 61
4.3.5 Reporting Format For Diagnosis of NKA and PKDL………………………………………...… 63
4.3.6 Reporting of Surveillance Information………………………………………………………..… 64
4.3.7 Web-based Reporting of Surveillance System…………………………………………………... 65
CHAPTER: FIVE…………………………………………………..……………………………….….…… 66
5. MONITORING AND EVALUATION (M&E)………………………….………………...…….. 67
5.1 The Monitoring & Evaluation Framework …………………….…………………………..…………… 67
5.2 Monitoring and Evaluation Team……………………………………………………………………….. 67
5.3 Indicators related to Kala-azar and PKDL Diagnosis……………………………………………………. 68
5.4 Indicators related to Kala-azar and PKDL Treatment……………………………………………………. 69
5.5 Indicators related to Kala-azar and PKDL Surveillance…………………………………………………. 70
xiii | P a g e
LIST OF TABLES:
Table 1: Health Facilities and Referral System for Kala-azar Treatment in Bangladesh…………………….. 14
Table 2: Clinical Case Definition for New Kala-azar, PKDL & CL.………………………………..………….. 21
Table 3: Diagnosis of Kala-azar in different level of health facilities in Bangladesh………….……………… 23
Table-4: Diagnostic test for suspected cases of KA using rK39 RDT ……………………………………………. 26
Table-5: Drug treatment of New Kala-azar (NKA) ………………………………………………..….…….……… 30
Table-6: Drug Treatment of RKA…………………………………………………………………..…….…….……… 31
Table-7: Treatment regimens for PKDL…………………………………………………………..…….…….……… 34
Table-8: Treatment of Cutaneous Leishmaniasis (CL)..………………………………………..…….…….………. 36
Table-9: The Clinical/Treatment Outcomes with Case Definitions of NKA……………...…….…….…….…… 43
Table-10: Early Treatment Outcomes with Case Definitions………………………………..….…….…….……… 44
Table-11: Final Treatment Outcomes with Case Definition: ………………………………..….…….…….……… 44
Table-12: Monitoring Clinical/treatment Outcomes Rates…………………………..……….…….…….……… 45
Table-13: Treatment Completion Rates…………………………….…….…….……………………………………… 46
Table-14: Treatment Outcomes in PKDL Patients………………………………………………..…….…….……… 46
Table-15: Names of drug with side effects and the types of laboratory tests indicated…………..…………….. 49
Table-16: Indicators and information for Passive Surveillance ………………………………..…….…….…… 54
Table -17: Indicators for Monitoring Passive Case Surveillance………………………………..…….…….…… 55
Table-18: Screening tool for diagnosis of New KA attending UHC (Check list)……….……………..……. 63
Table-19: Screening tool for “Suspected Cases of PKDL” attending UHC (Check List) …………...…………. 63
LIST OF FIGURES:
Figure -1: Life Cycle of Leishmania Parasite……………………………………………………………………… 6
Figure -2: Bangladesh Maps showing Year-wise Endemicity of Kala-azar: 2008-2014…………………. 8
Figure -3: Endemicity of Kala-azar in Bangladesh in 2014 & 2015……………………………………..……….. 10
Figure- 4: Endemicity of Kala-azar in Bangladesh in January – October 2016……………..………...………… 11
Figure-5: Trend of New Kala-azar Cases and Deaths during 2000-2015…………………..………...………… 12
Figure-6: Trend of VL and PKDL from 2010-2015 in Bangladesh………………………………………………. 12
Figuee-7 Procedures to perform RDT rK39 test………….…………..……..………….…………………………. 24
Figure-8 Interpretation rK39 Strip……………………………………………………..……………………………. 25
Figure-9 Diagnosis of Kala-azar……………………………………………..……………………………. 40
Figure- 10: Treatment Chart for NKA…………………………………………..………………….…………. 41
Figure-11: Treatment Chart for RKA, PKDL & CL.………………………..……………...………………. 42
Figure -12: Diagrammatic view of Activities and responsibilities of NRRTK in NKTA……………………… 57
Figure-13 Flow Chart for NKA and PKDL Detection from Community………………………………………… 62
Figure-14 Data Flow and M&E…………….……………………………….…………..….……………….. 71
xiv | P a g e
ANNEXTURE:
Annex-1: Household Survey Form ………………………………………………………..………………..……… 73
Annex-2: List of Suspected Cases Kala-azar Patient……………………………….………………….………… 74
Annex-3: Field Referral Form …………………………………………………………….……………….….……… 75
Annex-4: Registration and Follow-up Book…………………………………………..…….………..…………… 76
Annex-5: Treatment Card………………………………………………………………..…………….………….… 77
Annex-6: Follow-up Chart……………………………………………………………………………….………….. 79
Annex-7: Monthly Kala-azar Reporting Format………………………………………....………….…………… 80
Annex-8 Description of Drugs used for the Treatment of Kala-azar…………………………………………. 81
Annex-9 Monitoring of Treatment Outcomes Variables………………………………………………………… 85
Annex-10: Indicators of Kala-azar Treatment Effectiveness……………………………………………………… 85
Annex-11: Monthly/Quarterly Report Format on Early Treatment Outcomes…………………………………. 86
Annex-12: Monthly/Quarterly Report Format on Final Treatment Outcomes…………………………………. 87
Annex-13 Indicators showing the pharmacovigilance activities………………………………………………… 88
Annex-14: Web-based Registration of Kala-azar Cases and Follow-up Form………………………………… 89
Annex-15: SOP of AmBisome………………………………………………………………...…..…………………… 95
Annex-16 M&E Form for Facility Observation Checklist….………………………………..………..….……… 103
Annex-17 M&E for Monthly Reporting Format……………………………………………………………………. 104

xv | P a g e
EXECUTIVE SUMMARY
The updated version of the “National Guideline for Kala-azar Case Management 2016” is a product of
the National Kala-azar Elimination Program, Bangladesh. It aims to provide health managers, doctors,
clinicians, researchers, nurses and other relevant health professionals with a firsthand guide and tool for
diagnosis, treatment, health education and follow-up of cases with Kala-azar and Post-Kala-azar Dermal
Leishmaniasis (PKDL) in Bangladesh. The guideline was initially developed in 2013 with technical
support from World Health Organization (WHO), Bangladesh. This guideline comprises five chapters
with list of tables, figures and annexure.
Chapter-One describes general information about the New Kala-azar (NKA), Post Kala-azar Dermal
Leishmaniasis (PKDL) and Cutaneous leishmaniasis (CL) with current global burden of Leishmaniasis
and visceral Leishmaniasis as well as present Kala-azar situation in Bangladesh, brief description about
sandfly, the vector of Kala-azar, its characteristics, life cycle and control measures, short accounts of life
cycle of leishmania parasite; factors favourable for elimination of leishmania from Bangladesh, objectives
and target audiences for the national guideline, level of health facilities and referral system for Kala-azar
and PKDL case management; and summary of vision, mission, target, indicators, impact objectives,
elimination strategies and challenges of kala-azar elimination program in Bangladesh.
Chapter-Two deals mainly with clinical and confirmed case definitions of NKA, PKDL and CL. The
value of confirmatory such as microscopic examination of spleen/bone marrow aspirate or skin slit biopsy
or PCR. This chapter also describes the diagnosis of Kala-azar with co-infection such as tuberculosis,
hepatitis, hematological diseases, HIV/AID, diabetes, pregnancy and malaria. The unique diagnostic
services are made available in different level of health facilities such as upazila health complexes, district
hospitals, tertiary hospitals and specialized hospital in the endemic areas of Bangladesh. This chapter ends
by describing the types of diagnostic tests available for kala-azar, procedures of doing rK39 RDT at
simple laboratory setting, interpretation and effectiveness of rK39 RDT in detecting kala-azar, and
advantages and disadvantages of rK39 RDT for mass screening of Kala-azar in the community level.
Chapter-Three describes the treatment of Kala-azar, PKDL and CL using different types of anti-
leishmania drugs as a monotherapy or in combination and highlights the advantages of using single dose
Liposomal Amphotericin B (LAmB) for the attack phase of the National Kala-azar Elimination Program.
The recommended treatment regimens have been described indicating the importance of first line drug
treatment, value of alternative drug of choice, and effectiveness of combinations of drug therapy in New
Kala-azar (NKA), Kala-azar Treatment Failure (KATF), Relapse Kala-azar (RKA), and other form of
disease. This chapter includes the descriptions of anti-leishmania drugs such as Liposomal amphotericin
B (LAmB), Miltefosine, Paromomycin, Amphotericin B deoxycholate and Sodium stibogluconate with
their advantages, disadvantages and possible side effects. The early and final clinical/treatment outcomes
have been defined. Moreover, monitoring of clinical/treatment outcomes rates such as initial cure rate,
final cure rate, treatment failure rate, loss-to-follow up rate, treatment completion rate and mortality rate
have also been defined. The methods of collection of data on pharmacoepidemiology including detection,
assessment, documentation, and prevention of adverse drug reaction have been described along with the
importance of reporting and analyzing of adverse drug reaction caused as a result of treatment of disease.
Chapter-Four explains the importance of Kala-azar surveillance system and the roles of passive and
active surveillance in collecting, reporting, monitoring, evaluating, analyzing and interpreting Kala-azar
data for making empirical decision to improve the program activities. The management and composition
of Kala-azar surveillance units at upazila, district and national levels along with rules and regulations
xvi | P a g e
have been described. The roles and responsibilities of health managers at different surveillance units have
been highlighted. The sources of surveillance (health facilities) from where the data are generated have
been identified and components of surveillance system are described; for an effective disease
surveillance, the standard methods and frequency of reporting of Kala-azar disease have been organized;
the indicators for passive case detection have been defined and the corresponding reporting criteria have
been identified to document the disease events. The different methods and the criteria of active case
detection such as blanket approach, camp-based, index-based and incentive-based approaches have been
identified in order to play a more dynamic role in active case detection and to facilitate early diagnosis
and complete treatment of Kala-azar and PKDL cases.
The advantages of “No Kala-azar Transmission Activities”, a modified form of index-based case
approach for the acceleration of active case detection, have been described and the benefits of this
approach to implement the activities for stopping further transmission of the disease within the endemic
community are identified. The approaches and strategies to manage asymptomatic Kala-azar carrier have
been described and empirical value of mass screening of family members and immediate neighboring
contacts of the index case have been documented. The chapter ends by describing the advantages of Web-
based Registration of Kala-azar and PKDL Cases and Follow-up, whereby the information generated
from web-based will be used by the program personnel to take immediate actions to prevent the
transmission of the disease in the epidemic and outbreak situation, and help the program managers to
make better decision to improve the Kala-azar elimination program activities in Bangladesh.
Chapter-Five describes monitoring and evaluation (M&E) component of Kala-azar elimination program.
The importance of M&E for the provision of quality of data on the scope, coverage and effectiveness are
described. The uses of M&E data to monitor progress on inputs, process, outputs, outcomes and impacts
levels have been highlighted. The role of routine monitoring, periodic assessment, supervision and
evaluation to ensure effective implementation is described. A set of objectively verifiable indicators used
to measure progress and to assess the achievement of elimination target in line with national Kala-azar
strategy are defined. The checklists or formats have been designed for regular M&E to identify gaps of
the ongoing activities. The importance of M&E Framework and its different elements are described.
Indicators for NKA, PKDL and CL in relation to diagnosis, treatment and surveillance are described
using log frame, a tool for improving the planning, implementation, management, monitoring and
evaluation of the program activities that organize the main elements of Kala-azar elimination program and
systematize the logical linkages between them.

xvii | P a g e
PHOTOGRAPHS OF KALA-AZAR PATIENTS
Kala-azar Post Kala-azar Dermal Leishmaniasis
Cutaneous Leishmaniasis Post Kala-azar Dermal Leishmaniasis
(PKDL)

xviii | P a g e
xix | P a g e
1 | P a g e
CHAPTER: ONE
INTRODUCTION TO KALA-AZAR
Sandfly, the Vector of Kala-azar
2 | P a g e
INTRODUCTION TO KALA-AZAR
1.1 BACKGROUND – KALA-AZAR
Leishmaniasis is a group of neglected tropical disease caused by more than 20 different types of species of
protozoan parasites of Leishmania genus known to be infective to humans and is transmitted by the bite of
infected female phlebotomine sandflies. Leishmaniasis was first identified in 1824 in Jessore District of
Bangladesh. In 1903, a Scottish Physician Professor William Leishman and an Irish Physician Professor
Charles Donovan worked independently in India and identified the causative organism of Kala‐azar from
splenic aspirates. They published their discoveries almost simultaneously in the same year in British
Medical Journal in May 1903 and July 1903 respectively.
The greatest authority on parasitology at the time, Sir Ronald Ross took up investigations on the parasite of
kala‐azar in Kolkata, India. In 1903, he ended all controversy and jointly accredited Professor William
Leishman and Professor Charles Donovan for their discovery of the parasite of kala‐azar. Ronald Ross
named the parasite in honor of the two greatest medical scientists as “Leishmania donovani”. Today, the
name kala‐azar is used interchangeably with the scientific name visceral leishmaniasis for the most acute
form of the disease caused by L. donovani. Clinical manifestations range from cutaneous ulcers to systemic
multi-organ disease. Visceral leishmaniasis (VL) is caused primarily by the two related species Leishmania
donovani and Leishmania infantum (synonym Leishmania chagasi).
1.2 CURRENT GLOBAL BURDEN OF VISCERAL LEISHMANIASIS
There are three main types of leishmaniasis: i) Visceral leishmaniasis, often known as kala-azar and the
most serious form of the disease (VL); ii) Cutaneous leishmaniasis, the most common (CL); and iii)
Mucocutaneous. A recent review shows that over 98 countries and territories are endemic for leishmaniasis.
Visceral leishmaniasis (VL): VL also known as kala‐azar is highly endemic in Indian subcontinent
(Bangladesh, India and Nepal), and in East Africa (North Sudan, Kenya and Ethiopia). An estimated
200 000 to 400 000 new cases of VL occur worldwide each year. Over 90% new cases of VL occur in 6
countries such as Bangladesh, Brazil, Ethiopia, India, Sudan and South Sudan. VL is caused by two
leishmanial species, L. donovani or L. infantum, depending on the geographical area. L. infantum infects
mostly children and immuno-suppressed individuals, whereas L. donovani infects all age group. There are
two types of VL, which differ in their transmission characteristics: (i) Zoonotic VL is transmitted from
animal to vector to human and (ii) Anthroponotic VL is transmitted from human to vector to human. In the
Zoonotic VL, humans are occasional hosts and animals, mainly dogs, are the reservoir of the parasites.
Zoonotic VL is found in areas of L. infantum transmission, whereas Anthroponotic VL is found in areas of
L. donovani transmission.
Cutaneous leishmaniasis (CL): Cutaneous leishmaniasis is more widely distributed, about 90% of CL
cases occurring in each of three epidemiological regions, the Americas, the Mediterranean basin, and
western Asia from the Middle East to Central Asia. Over two-thirds of the new CL cases occur in 6
countries such as Afghanistan, Algeria, Brazil, Colombia, Iran and the Syrian Arab Republic. An estimated
0.7-1.3 million new CL cases occur worldwide annually. CL is the most common form of leishmaniasis and
causes skin lesions; the patient generally presents with one or several ulcer(s), on exposed parts of the
body, leaving life‐long scars and serious disability. Different species of Leishmania can infect the
3 | P a g e
macrophages in the dermis, with variable clinical presentations and prognosis. The ulcers heal
spontaneously, although slowly, in immunocompetents individuals, but cause disfiguring scars..
Muco-cutaneous leishmaniasis: Almost 90% of muco-cutaneous leishmaniasis cases occur in the
Plurinational State of Bolivia, Brazil and Peru. In Mucocutaneous leishmaniasis, the patients suffer from
progressively destructive ulcerations of the mucosa, leading to partial or total destruction of mucous
membranes of the nose, mouth and throat including pharynx and larynx. These lessons are not self-healing
and are usually seen months or years after a first episode of cutaneous leishmaniasis, when the macrophage
of the naso-oropharyngeal mucosa become colonized. Leishmania braziliensis is responsible for most cases
of muco-cutaneous leishmaniasis..
Post Kala-azar Dermal Leishmaniasis (PKDL): PKDL is characterized by a macular, maculo-papular or
nodular rash and is a complication of VL that is frequently observed after treatment of VL. It can also occur
in immuno-suppressed individuals in L. infantum-endemic areas. The interval between treated VL and
PKDL is 0-6 months in Sudan and 6 months to 3 years in Bangladesh, Indian and Nepal. PKDL cases are
highly infectious because the nodular lesions contain many parasites and such cases are the presumed
reservoir for Anthroponotic VL between epidemic cycles.
PKDL has been reported sporadically in patients who do not give a past history of VL. In the Indian Sub-
continent, PKDL is not self-healing. PKDL cases are a potential reservoir of the parasite as sand flies get
infected from biting them. In endemic areas, children and young adults are the principal victims. Kala-azar
with TB or HIV or malaria co-infection also has emerged as a health problem in recent years.
Kala-azar is the disease of poverty and mostly affects the socially marginalized and the poorest
communities of the rural population and is recognized as Neglected Tropical Disease (NTD). Nearly 2.4
million Disability-adjusted life years (DALYs) are lost each year due to kala-azar globally. South-East Asia
Region accounts for the loss of about 400 000 DALYs. The economic burden of the disease in the affected
areas is also very large. About 67% of the global disease burden of Kala-azar is harbored in Bangladesh,
India and Nepal. About 200 million populations are at risk of kala-azar in Indian sub-continent.
Visceral leishmaniasisis one of the clinical forms of Leishmania with its complication such as Post Kala-
azar Dermal Leishmaniasis (PKDL), Cutaneous Leishmaniasis (CL) and muco-cutaneous Leishmaniasis
(ML) and is caused by the protozoa Leishmania donovani. In Indian sub-continent it is transmitted by
female sand fly named Phlebotomus argentipes. The disease is characterized by prolonged fever (≥2
weeks) with splenomegaly, anemia, weight loss and darkening of skin. Kala-azar is fatal if not treated
properly.

4 | P a g e
1.3 VECTOR: SANDFLY - CHARACTERISTICS, LIFE CYCLE AND
CONTROL MEASURES
Habits of Sandfly: Sandfly that caused visceral leishmaniasis belongs to Phlebotomus genus and the
Phlebotomus argentipes is the common species. The sandfly is most commonly distributed in the warm
countries; only female sandfly can bite in the dwelling at night. The sandfly is characterized by its densely
hairy wings, giving them a moth-like appearance. It takes shelter during day in holes and crevices in wall,
in dark room and store room etc. The eggs are laid in damp and dark places in cattle sheds and poultry.
The species are mostly nocturnal in habit. The range of flight is on average 200 yards from their breeding
places; however, they cannot fly but can only hop and hop only short distance. The average life of
sandfly is about 2 weeks. The males and females feed on nectar and other plant juices, but females require
a blood meal in order to mature a second batch of eggs. The blood meal hosts include white-tailed deer,
horses, donkeys, mules, dog, cattle, swine, raccoons, rodents, birds and humans. Sand flies are active
during the early morning and evening hours when temperatures are cooler and humidity is lower.
General Characteristics of Sandfly: The body of sandfly consists of three parts: (i) The head bears a
pair of long and hairy antenna. Palpi and proboscis and one pair of prominent black eyes are present; (ii)
The thorax bears a pair of wings and three pair of legs. The wings are upright in shape and hairy. The
2nd
longitudinal vein is branched twice. The legs are long and slender and out of proportion to the size of
the body; and (iii) the abdomen has ten segments and is covered with hairs. In the female the tip of
abdomen is rounded while in male claspers are attached to last abdominal segment.
Life Cycle of Sandfly: The life cycle of sandfly is characterized by complete metamorphosis, having 4
developmental stages as flows:
Egg: Adult females require blood meal to develop eggs. The female generally lays eggs in the damp dark places
in the cattle sheds and poultry. The eggs vary from 40-50 in numbers, elongated oval shaped, and
brownish in color. The eggs measure about 0.4 mm in length. Eggs hatch in 1-2 weeks;
Larva: The larva is maggot like structure with pale cream in color, having large head, thorax and abdomen and
two long bristle on last abdominal segment. Caterpillar-like larvae hatch from eggs through a J-shaped
crack. Four different stages, or instars, of larval development occur over a period of around two weeks,
each one larger than the one before. The newly hatched first instar larvae have two rear bristles, or
whiskers, while all later larval developments have four rear bristles. Larvae feed on dead organic matter
and are found living in moist areas, such as in animal burrows. Larva becomes a pupa in about 2 weeks.
Pupa: Pupae are obtect, measuring approximately 2.6 mm in length looking much like a butterfly pupa. To
prepare for the pupal stage, the sand fly larvae attach themselves to a substrate. During this stage, each
larva develops into adults and grows wings. Sand flies are immobile during this life cycle stage and do not
eat. The pupal stage occurs over a period of five to ten days.
Adult: Sand flies emerge from their pupal stage as adults at night, shortly after they develop their wings, which
are a characteristic V shape when erected. Adults are small, on average 2.5 mm in length, silvery-
brownish in color, long-legged flies with narrow bodies. The wings are less than 3 mm long, and are held
erect above the body. Sexual dimorphism is marked between the male and female flies. Males have
conspicuous external terminalia with a relatively small and slender abdomen compared to the female. The
total time from egg to adult takes 5 weeks. The average life of a sandfly is about 2 weeks.
5 | P a g e
Behavior and Bionomics: The life cycle of sandfly develops in moist microhabitats rich in organic
matter. They thrive best in alluvial soil, in areas with relatively even temperature, high humidity and
abundance of cattle. They are not aquatic but eggs and larvae can withstand the immersion in water for a
period of 5 days, and the larvae of the fourth stage can withstand the immersion for a period of 14 days.
Thus they can survive even flooding. Breeding places are found within a radius of about 20-50 meters
from a dwelling. There is no information on the life expectancy of sandfly but thought that they can
survive not more than 35 days. Only the female suck blood and they prefer cattle blood because it
required a blood-meal for egg development. The sandfly shifts from cattle to humans only it has
exhausted the option of blood meal from cattle.
Sandflies rest comparatively in cool and humid places including bedrooms; latrines; basements; fissures
in walls, rocks, soil, crakes and crevices; dense vegetation; tree holes and buttresses; burrows of rodent
and other mammals; bird‟s nests. In the cattle sheds, the favorite breeding place is underneath cattle
troughs. Female sandflies of many species are predominantly exophagic (biting outdoor) and exophilic
(resting outdoors during maturation of eggs), and cannot be controlled by spraying internal walls of
houses with insecticide. In contrast, species that are endophilic (resting indoors during maturation of
eggs) can be controlled by spraying.
Control Measures: Sandflies are easily controlled because they do not move long distance from their
breeding places. (i) Insecticide: Deltamethrin, Lindane, some other insecticides have been proved
effective against sandfly. Spraying should be done in the human dwellings, cattle sheds and poultry. Its
residue may remain effective for a period of 3 months; and (ii) Sanitation: Removal of shrubs and
vegetation, filling of cracks and crevices in the wall and floor, and distance of cattle sheds and poultry
from human habitations may improve the sanitation and wipe out the habitats of sandfly.
Adult sandflies are active after dark, while during the day they escape into their resting shelters. The
indoor habitats of sandflies have implications for the effectiveness of control measures. The sandflies can
hop but cannot fly, and can hop only short distances. They cannot reach above a height of six feet. The
highest risk of disease transmission for Bangladesh, India and Nepal is in the months of June to October
when the humidity is high. Susceptibility test have shown that the sandfly continues to be susceptible to
all insecticides.
The vector behavior and bionomics that make interruption of transmission achievable in this subcontinent
include the following: (i) There is probably only one type of sandfly that causes kala-azar in Bangladesh,
India and Nepal, (ii) The vector is so far sensitive to all the insecticides, (iii) The insecticide spraying can
be done with economy since the spraying is required up to a height of about two meters (6 feet) only, (iv)
The operations may be confined to only the households and cattle sheds, (v) The operations of IRS is to
be limited to community in a geographical areas affecting only 98 upazilas of Bangladesh, (vi) The cross-
border collaboration in IRS operations can interrupt the transmission of the disease, and (vii) There is
historical evidence of interruption of transmission as a collateral benefit of malaria eradication program
when kala-azar was virtually eliminated from the subcontinent as a result insecticide spraying.
6 | P a g e
1.4 LIFE CYCLE OF LEISHMANIA PARASITE
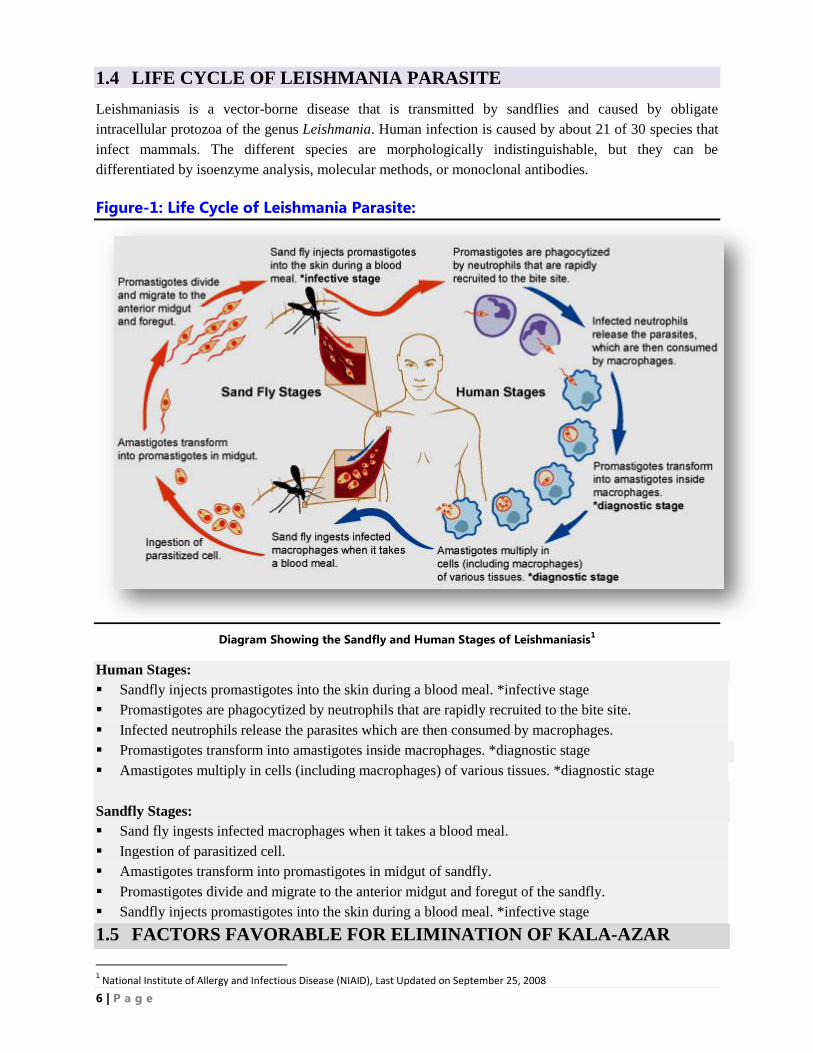
Leishmaniasis is a vector-borne disease that is transmitted by sandflies and caused by obligate
intracellular protozoa of the genus Leishmania. Human infection is caused by about 21 of 30 species that
infect mammals. The different species are morphologically indistinguishable, but they can be
differentiated by isoenzyme analysis, molecular methods, or monoclonal antibodies.
Figure-1: Life Cycle of Leishmania Parasite:
Diagram Showing the Sandfly and Human Stages of Leishmaniasis1
Human Stages:
Sandfly injects promastigotes into the skin during a blood meal. *infective stage
Promastigotes are phagocytized by neutrophils that are rapidly recruited to the bite site.
Infected neutrophils release the parasites which are then consumed by macrophages.
Promastigotes transform into amastigotes inside macrophages. *diagnostic stage
Amastigotes multiply in cells (including macrophages) of various tissues. *diagnostic stage
Sandfly Stages:
Sand fly ingests infected macrophages when it takes a blood meal.
Ingestion of parasitized cell.
Amastigotes transform into promastigotes in midgut of sandfly.
Promastigotes divide and migrate to the anterior midgut and foregut of the sandfly.
Sandfly injects promastigotes into the skin during a blood meal. *infective stage
1.5 FACTORS FAVORABLE FOR ELIMINATION OF KALA-AZAR
1 National Institute of Allergy and Infectious Disease (NIAID), Last Updated on September 25, 2008
7 | P a g e
The morbidity and mortality of VL in Bangladesh, India and Nepal is high about 67% of the global disease
burden, the governments of these countries have declared this disease as a public health problem and have
launched a Regional VL Elimination Program implementing strategies to reduce the annual incidence of
VL. Bangladesh, India and Nepal signed a memorandum of understanding (MoU) in 2005 and pledged
their commitment to eliminate kala-azar from the region by 2015. Thereafter a “Regional Strategic
Framework for Elimination of Kala-azar from the South-East Asia Region: 2011-2015” was adopted with
clear goal, target, indicators and objectives. On 9th September 2014 in Dhaka, the MoU has been extended
including two countries Bhutan and Thailand, with the aim of reducing annual incidence of kala-azar less
than 1 case per 10,000 populations in the endemic areas by 2017. This optimistic and realistic aim could be
apprehended by realizing two most important favorable factors as follows:
1.5.1 Biological Factors: Biological factors favorable for elimination of kala-azar are in the South-East
Asia Region are:
Man is known to be the only reservoir host for kala-azar parasite (Leishmania donovani),
Phlebotomus argentipes sandfly is probably the only species amongst about 50 phlebotomine
species that transmits kala-azar to humans in Bangladesh, India and Nepal.
1.5.2 Technical Factors: The technical factors favorable for elimination of kala-azar are:
rK39 Rapid Diagnostic Test kit: rK39 Rapid Diagnostic Test kit is available for the diagnosis of
kala-azar. , which is very reliable with high sensitivity and specificity, easy-to-use,;
Availibility of Anti-leishmaniasis Drug: The first line drugs such as oral Miltefosine and single
dose injection Liposomal Amphotericin B are available for the treatment of kala-azar. These
drugs are reasonably safe and effective; Alternative effective drug such as Paromomycin is also
available;
Vector Control Measures: Vector control using indoor residual spraying (IRS) with effective
insecticide is available;
Strong political commitment in the three countries including Bhutan and Thailand favors
feasibility of elimination of the disease; and
The disease is limited to only 90 districts in the Indian subcontinent (26 Bangladesh, 52 India and
12 Nepal). Some districts in Bhutan and Thailand are also affected with sporadic cases. Hence,
elimination efforts should be focused in the five endemic countries.
8 | P a g e
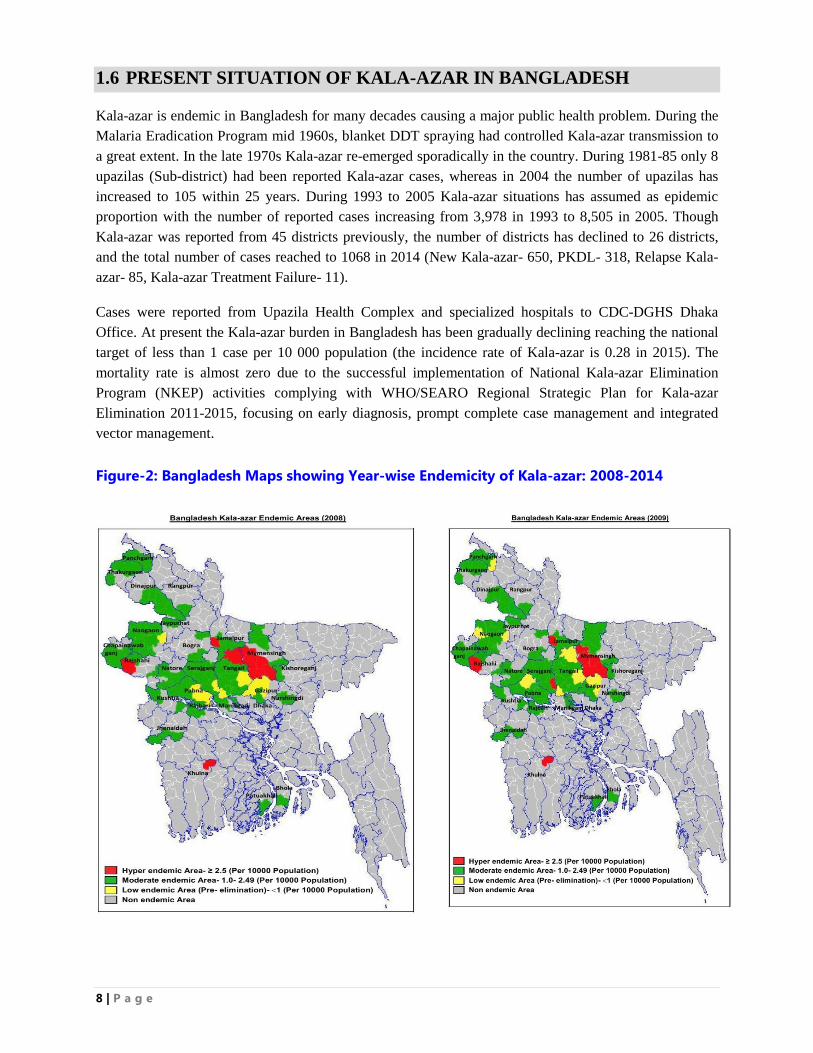
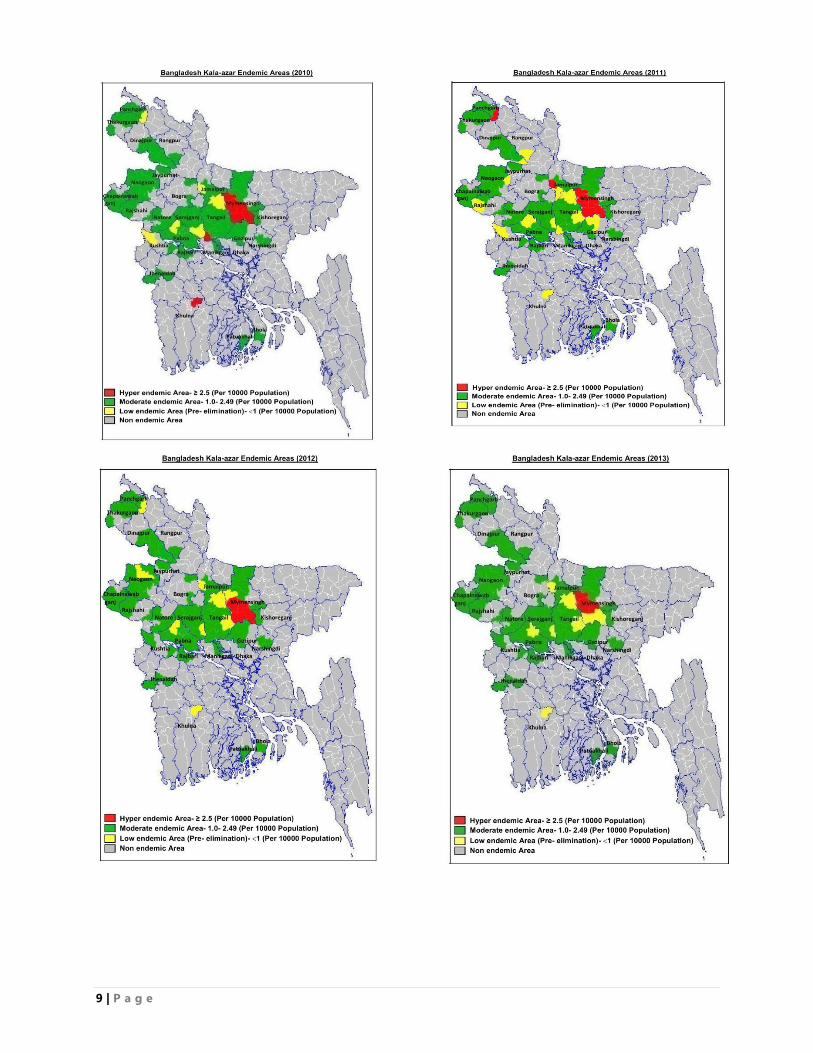
1.6 PRESENT SITUATION OF KALA-AZAR IN BANGLADESH
Kala-azar is endemic in Bangladesh for many decades causing a major public health problem. During the
Malaria Eradication Program mid 1960s, blanket DDT spraying had controlled Kala-azar transmission to
a great extent. In the late 1970s Kala-azar re-emerged sporadically in the country. During 1981-85 only 8
upazilas (Sub-district) had been reported Kala-azar cases, whereas in 2004 the number of upazilas has
increased to 105 within 25 years. During 1993 to 2005 Kala-azar situations has assumed as epidemic
proportion with the number of reported cases increasing from 3,978 in 1993 to 8,505 in 2005. Though
Kala-azar was reported from 45 districts previously, the number of districts has declined to 26 districts,
and the total number of cases reached to 1068 in 2014 (New Kala-azar- 650, PKDL- 318, Relapse Kala-
azar- 85, Kala-azar Treatment Failure- 11).
Cases were reported from Upazila Health Complex and specialized hospitals to CDC-DGHS Dhaka
Office. At present the Kala-azar burden in Bangladesh has been gradually declining reaching the national
target of less than 1 case per 10 000 population (the incidence rate of Kala-azar is 0.28 in 2015). The
mortality rate is almost zero due to the successful implementation of National Kala-azar Elimination
Program (NKEP) activities complying with WHO/SEARO Regional Strategic Plan for Kala-azar
Elimination 2011-2015, focusing on early diagnosis, prompt complete case management and integrated
vector management.
Figure-2: Bangladesh Maps showing Year-wise Endemicity of Kala-azar: 2008-2014
9 | P a g e
10 | P a g e
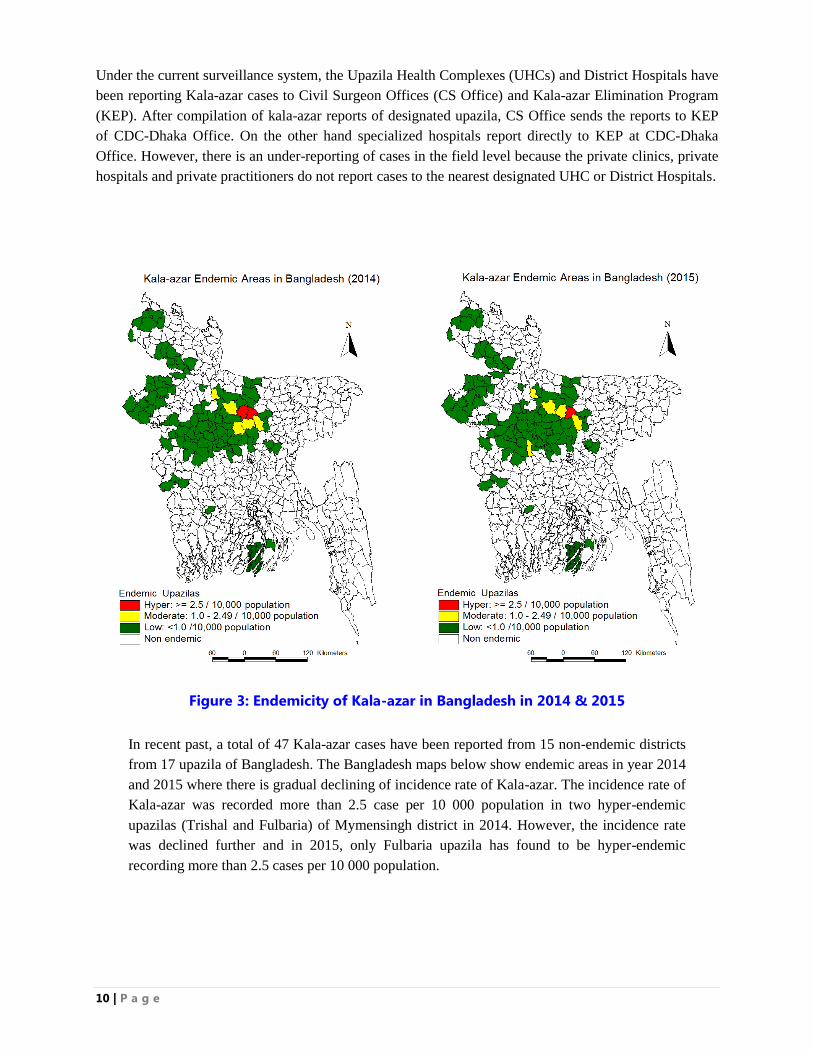
Under the current surveillance system, the Upazila Health Complexes (UHCs) and District Hospitals have
been reporting Kala-azar cases to Civil Surgeon Offices (CS Office) and Kala-azar Elimination Program
(KEP). After compilation of kala-azar reports of designated upazila, CS Office sends the reports to KEP
of CDC-Dhaka Office. On the other hand specialized hospitals report directly to KEP at CDC-Dhaka
Office. However, there is an under-reporting of cases in the field level because the private clinics, private
hospitals and private practitioners do not report cases to the nearest designated UHC or District Hospitals.
Figure 3: Endemicity of Kala-azar in Bangladesh in 2014 & 2015
In recent past, a total of 47 Kala-azar cases have been reported from 15 non-endemic districts
from 17 upazila of Bangladesh. The Bangladesh maps below show endemic areas in year 2014
and 2015 where there is gradual declining of incidence rate of Kala-azar. The incidence rate of
Kala-azar was recorded more than 2.5 case per 10 000 population in two hyper-endemic
upazilas (Trishal and Fulbaria) of Mymensingh district in 2014. However, the incidence rate
was declined further and in 2015, only Fulbaria upazila has found to be hyper-endemic
recording more than 2.5 cases per 10 000 population.
11 | P a g e
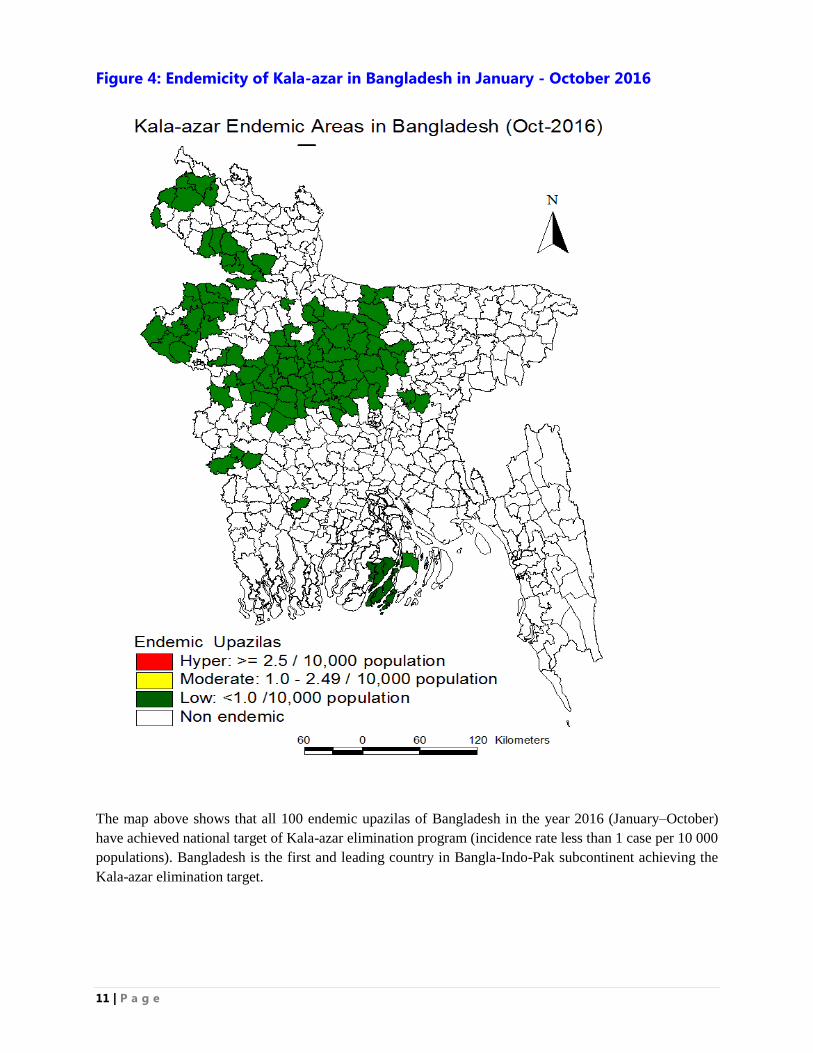
Figure 4: Endemicity of Kala-azar in Bangladesh in January - October 2016
The map above shows that all 100 endemic upazilas of Bangladesh in the year 2016 (January–October)
have achieved national target of Kala-azar elimination program (incidence rate less than 1 case per 10 000
populations). Bangladesh is the first and leading country in Bangla-Indo-Pak subcontinent achieving the
Kala-azar elimination target.
12 | P a g e
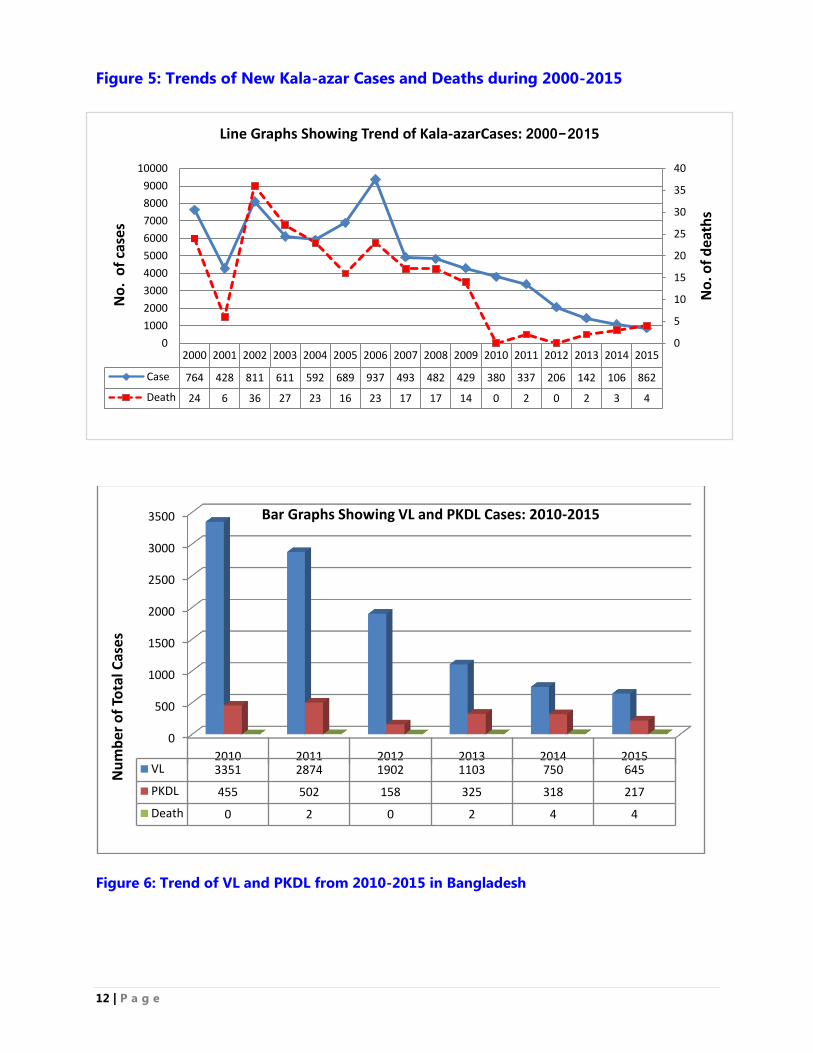
Figure 5: Trends of New Kala-azar Cases and Deaths during 2000-2015
Figure 6: Trend of VL and PKDL from 2010-2015 in Bangladesh
0
500
1000
1500
2000
2500
3000
3500
2010 2011 2012 2013 2014 2015VL 3351 2874 1902 1103 750 645
PKDL 455 502 158 325 318 217
Death 0 2 0 2 4 4
Nu
mb
er o
f To
tal C
ase
s
Bar Graphs Showing VL and PKDL Cases: 2010-2015
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Case 764 428 811 611 592 689 937 493 482 429 380 337 206 142 106 862
Death 24 6 36 27 23 16 23 17 17 14 0 2 0 2 3 4
0
5
10
15
20
25
30
35
40
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
No
. of
dea
ths
No
. o
f ca
ses
Line Graphs Showing Trend of Kala-azarCases: 2000-2015
13 | P a g e
1.7 OBJECTIVES: NATIONAL GUIDELINE FOR KALA-AZAR CASE
MANAGEMENT
With technical support from Technical Working Group (TWG) Bangladesh, Kala-azar Elimination
Programme (KEP) has developed „National Guideline for Kala-azar Case Management‟ with the
following objective and the contents as follows:
Objective: The primary objective of the National Guideline for Kala-azar Case management is to orient
the health care providers with tools for diagnosis, treatment, surveillance and M&E of Kala-azar.
Contents of the guideline: The treatment guideline would content the following topics:
Identification of suspected cases of Kala-azar at community and hospital level
Diagnosis, detection and confirmation of Kala-azar at Upazila Health Complex, District Hospitals,
Medical College Hospital and Specialized Hospital
Provision of treatment modalities, availability of treatment, doses and administration of drugs
Establishment of effective referral system for Kala-azar patients
Institutionalizing supervision, monitoring and evaluation of Kala-azar Elimination Program
Surveillance system with passive and active case detection and activities for Kala-azar
Reporting system of Kala-azar
In 2015 the guideline has been updated with the following purposes:
To include the latest Data of Kala-azar Elimination Program
To orient with new terminology
To update the treatment modalities for Kala-azar, SOPs of Kala-azar drugs and diagnostics
To orient web-based reporting and Pharmaco-vigilance of Kala-azar drugs
To implement supervision, monitoring and evaluation tools for better management of Kala-azar
Elimination Program
14 | P a g e
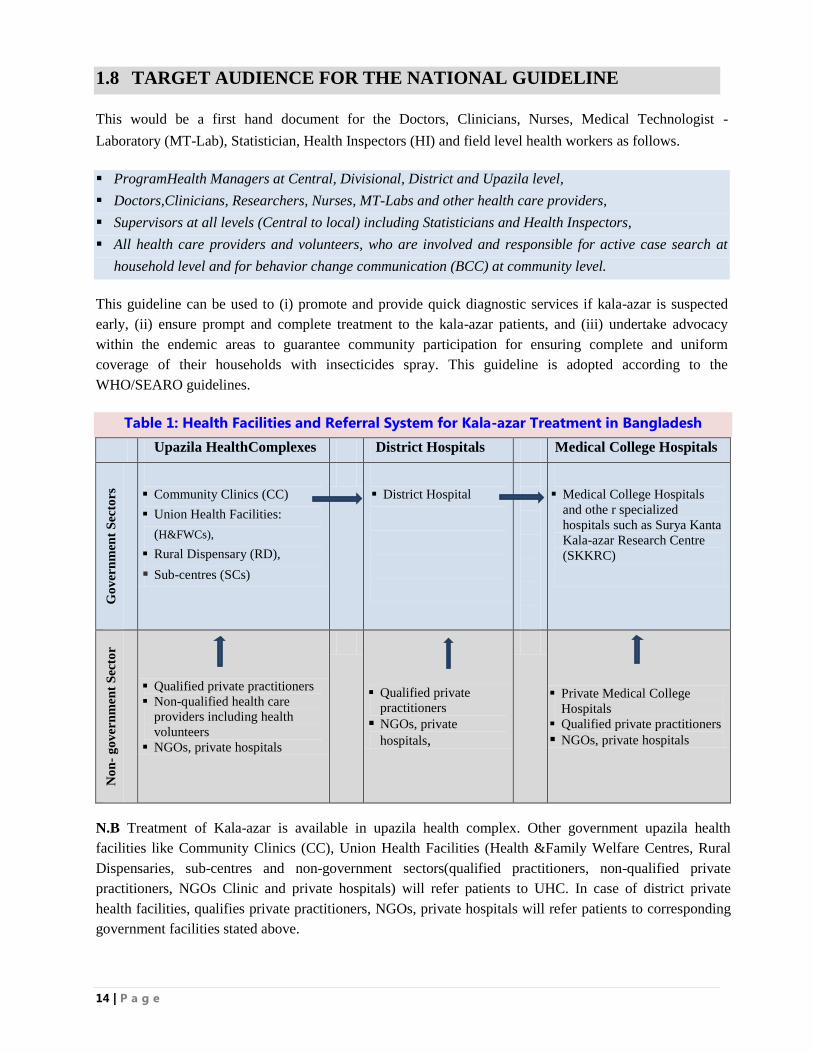
1.8 TARGET AUDIENCE FOR THE NATIONAL GUIDELINE
This would be a first hand document for the Doctors, Clinicians, Nurses, Medical Technologist -
Laboratory (MT-Lab), Statistician, Health Inspectors (HI) and field level health workers as follows.
ProgramHealth Managers at Central, Divisional, District and Upazila level,
Doctors,Clinicians, Researchers, Nurses, MT-Labs and other health care providers,
Supervisors at all levels (Central to local) including Statisticians and Health Inspectors,
All health care providers and volunteers, who are involved and responsible for active case search at
household level and for behavior change communication (BCC) at community level.
This guideline can be used to (i) promote and provide quick diagnostic services if kala-azar is suspected
early, (ii) ensure prompt and complete treatment to the kala-azar patients, and (iii) undertake advocacy
within the endemic areas to guarantee community participation for ensuring complete and uniform
coverage of their households with insecticides spray. This guideline is adopted according to the
WHO/SEARO guidelines.
Table 1: Health Facilities and Referral System for Kala-azar Treatment in Bangladesh
Upazila HealthComplexes District Hospitals Medical College Hospitals
Go
ver
nm
ent
Sec
tors
Community Clinics (CC)
Union Health Facilities:
(H&FWCs),
Rural Dispensary (RD),
Sub-centres (SCs)
District Hospital
Medical College Hospitals
and othe r specialized
hospitals such as Surya Kanta
Kala-azar Research Centre
(SKKRC)
No
n-
go
ver
nm
ent
Sec
tor
Qualified private practitioners
Non-qualified health care
providers including health
volunteers
NGOs, private hospitals
Qualified private
practitioners
NGOs, private
hospitals,
Private Medical College
Hospitals
Qualified private practitioners
NGOs, private hospitals
N.B Treatment of Kala-azar is available in upazila health complex. Other government upazila health
facilities like Community Clinics (CC), Union Health Facilities (Health &Family Welfare Centres, Rural
Dispensaries, sub-centres and non-government sectors(qualified practitioners, non-qualified private
practitioners, NGOs Clinic and private hospitals) will refer patients to UHC. In case of district private
health facilities, qualifies private practitioners, NGOs, private hospitals will refer patients to corresponding
government facilities stated above.
15 | P a g e
For the success of the program, it is important to develop referral linkages from community to medical
college hospitals and specialized hospital. The district focal point should be responsible for sustaining the
linkages. The details of collaboration between the public and private sector need to be worked out with
the objective of obtaining uniform standards of practices.
1.9 KALA-AZAR ELIMINATION PROGRAM IN BANGLADESH
Vision: Kala-azar free Bangladesh by 2020.
Goal: To contribute to improving the health status of vulnerable groups and at-risk population living in
Kala-azar endemic areas of Bangladesh by the elimination of Kala-azar.
Target: To reduce the incidence rate of the disease to less than 1 case per 10000 populations at the
upazila level in Bangladesh by the year 2017.
Indicators: Three indicators have been set: (i) Kala-azar Detection Rate should be close to 100%, (ii)
Treatment Completion Rate should be ≥ 90% and (iii) Vector Control Coverage Rate (HH coverage
through IRS) should be close to 100%.
Impact Objectives: To reduce the incidence of New Kala-azar and PKDL to less than 1 case per 10
000 populations at the upazila level in Bangladesh by the end of 2017 by:
Reducing incidence of KA in the poor, vulnerable and un-reached populations in the endemic areas.
Reducing case fatality rates from Kala-azar to negligible level.
Reducing cases of PKDL to interrupt transmission of kala-azar, and
Preventing and treating Kala-azar-HIV-TB co-infections in the endemic areas.
Elimination strategies: A regional strategic framework for elimination of Kala-azar of WHO/SEARO
2011-2015 has been endorsed by the Regional Technical Advisory Group (RTAG). It comprises of the
following components:
1. Early diagnosis and complete treatment: All suspected cases of Kala-azar and PKDL should have
access to recommended diagnosis and treatment.
2. Integrated vector management (IVM): The IVM strategy aims to prevent and decrease vector
(sandfly) spread within the community and reduce human-vector-pathogen contact, and is done by
controlling vector through IRS in households and distributing LLIN within the kala-azar patients.
3. Effective disease surveillance: An effective surveillance system should be strengthen to ensure early
diagnosis, provide prompt treatment, undertake active case detection, and report kala-azar cases from
the public and private sector.
4. Social mobilization and building partnerships: For community participation and social mobilization
for behavioral change communication (BCC) at community level; and partnership building would help
to achieve the goal of Kala-azar elimination program.
5. Operational research: Operational research aims to explore strategies, interventions, tools and
knowledge that can monitor the quality, coverage, effectiveness and performance of the kala-azar
elimination program activities and evaluate the drug efficacy, insecticide resistance, quality of drugs,
treatment compliance, pharmaco-vigilance and LLIN use.
16 | P a g e
1.10 CHALLENGES FOR NKEP IN BANGLADESH
The programme activities have contributed to reduce the incidence rate of kaka-azar remarkably over the
years in Bangladesh, however, the following areas need to be addressed and prioritized as follows:
1.6.1 The epidemiological surveillance systems need to be strengthened further at the upazila and
district level with the focus to capture data from all sources including private sector and NGOs.
1.6.2 Health-seeking behaviour: Kala-azar patients seek treatment not only from the government
facilities but also from the private practitioners, Ayurvedhic, Homeopathy, Unany and even form
village quacks. It is indeed a challage to get data from these non-governmane sources.
1.6.3 PKDL patients do not always come to a treatment facility. They act as a potential reservoir in the
community for transmission of the disease.
1.6.4 Emergence of drug resistance in L. donovani:There was a documented 60% failure rate of VL
cases with Antimonials in North Bihar of India, and parasite resistance was established in the
laboratory. Resistance to anti-kala azar drug is not documented in bangladesh.
1.6.5 Increasing relapse rates on miltefosine has been observed in India and Nepal where upto up to
20% after 12 months has been observed in the latter.
1.6.6 Asymptomatic cases of Kalaa-zar: Asysmptomatic cases of Kala-azar may act as sources of
transmission of disease in the community.

17 | P a g e

18 | P a g e
CHAPTER: TWO
DIAGNOSIS OF KALA-AZAR AND PKDL
19 | P a g e
2. DIAGNOSIS OF KALA-AZAR, PKDL AND CL
The evolution and advancement of different serological diagnostic tests that have been used to diagnosis
kala-azar and PKDL include globulin content of the blood, globulin ring test, globulin precipitation test,
globulin opacity test, aldehyde test, direct agglutination test both fridge and dried, rK39 rapid diagnostic
test (RDT), and polymerase chain reaction (PCR) to diagnose leishmaniasis. The confirmation of kala-
azar is also done by examination of bone marrow/spleen aspirate for LD bodies.
The KEP is using rK39 RDT, which is the latest diagnostic test with high sensitivity and specificity
suitable for screening mass population within the kala‐azar endemic areas. The rK39 RDT is usually used
in the upazila health complexes (sub‐district hospital of Bangladesh). The parasitological diagnostic tests
are regarded as confirmatory tests identifying for the presence of parasites (LD bodies) in splenic
aspirates, bone marrow biopsy and slit‐skin biopsy. The confirmatory tests are usually done at tertiary
hospitals. Once the case is diagnosed as Kala-azar, the patient is treated with first line of anti‐leishmania
drug. In some complicated cases of kala-azar in which rK39 RDT found to be negative and therefore
splenic puncture for LD bodies or PCR to detect the antibody or culture may be indicated in those cases.
2.1 CLINICALDIAGNOSIS OF NEW KALA-AZAR (NKA)
Case Definition of New Kala-azar (NKA): The most important diagnostic strategy is to describe a
standard case definition for New Kala-azar (NKA). The Technical Members of WHO in a country
consultation meeting formulated kala-azar case definition and the Regional Technical Advisory Group
(RTAG) of WHO endorsed the case definition as follows:
History of prolonged fever more than two weeks,
History of living or travelling in the kala-azar endemic area, and
Splenomegaly (palpable spleen), that is enlarge spleen.
Additional signs include weight loss, anemia and enlarge liver (Table-2).
This case definition is more sensitive than specific, holding the basis of surveillance system in the kala-azar
elimination program, and forming the basis of setting rules for the early diagnosis and complete treatment of
kala-azar cases.
Clinical Diagnosis of NKA: The second most important diagnostic approach is to conduct the screening
test using “rK39 RDT” for all new cases who meet the above case definition with fever of more than two
weeks and/or splenomegaly. If the rK39 RDT is found to be positive and if the patient has no history of
treatment of kala-azar before, the patients should be diagnosed as New Kala-azar (NKA) and should be
treated with effective first line anti-leishmania drug.
In cases with past history of kala-azar or those with high suspicion of KA but with negative rK39 RDT,
confirmation should be done by examining spleen/bone marrow aspirate for LD bodies. Treatment of
kala-azar in these circumstances should only be started after the diagnosis is confirmed.
20 | P a g e
2.2 CLINICAL DIAGNOSIS OF PKDL
Case Definition of PKDL: The strategy for case definition of Post Kala-azar Dermal Leishmaniasis
(PDKL has been adopted from WHO/TDR2.The approved clinical indicators for PKDL case definition are
as follows:
History of previous kala-azar,
History of living in the previous kala-azar endemic area, and
Skin manifestation with multiple hypo-pigmented macule, papule and or nodule with skin sensation
(Table-2).
With these above three clinical indicators, the patient is labeled as “Suspected PKDL Case”. The
suspected case of PKDL is further screened with diagnostic test kit rK39 RDT and if the result of rK39
RDT kit is positive along with the above three clinical indicators, the patient is labeled as “Probable
PKDL Case”. The strategy adopted for Probable PKDL Case is to treat them with effective anti Kala-azar
drug. The patient is labeled as “Confirmed PKDL Case” if they meet the criteria for Probable PKDL
along with confirmed parasites (LD Bodies) in slit-skin smear or skin biopsy. In this situation the
Confirmed PKDL Case should also be treated with effective anti-kala-azar drugs.
Skin lesions in PKDL cases have been not been graded in National Kala-azar Elimination Program
(NKEP) in Bangladesh. However, some countries have graded PKDL cases into three major categories as
follows: Grade I includes scattered maculo-papular or nodular rash in the face with or without some
involvement in the upper chest or arm; Grade II includes maculo-papular or nodular rash mostly on face
and extending to the chest, back upper arms, and legs; and Grade III includes maculo-papular or nodular
rash covering most part of the body, including hands and feet.
In some cases of PKDL, there may be a history of NKA and in some cases, there may not be past history.
All suspected cases of PKDL should be subjected to rK39 RDT. A negative test with rK39 RDT in
macular lesions does not rule out the possibility of PKDL. In such cases and also in nodular and papular
lesions, the diagnosis may be confirmed by biopsy or scraping of slit-skin. PCR tests with skin biopsy or
slit-skin smear is much more sensitive. The rK39 RDT is usually positive in both papular and nodular
lesions.
Bangladesh has adopted this case definition of NKA and PKDL and continued implementing this
standard process in its NKEP. Early diagnosis with case detection and prompt treatment will improve the
prognosis of patients and reduce the transmission of the disease in the endemic area.
2 WHO (2010). Indicators for monitoring and evaluation of the kala-azar elimination programme. August 2010, WHO & TDR, p 6-7.
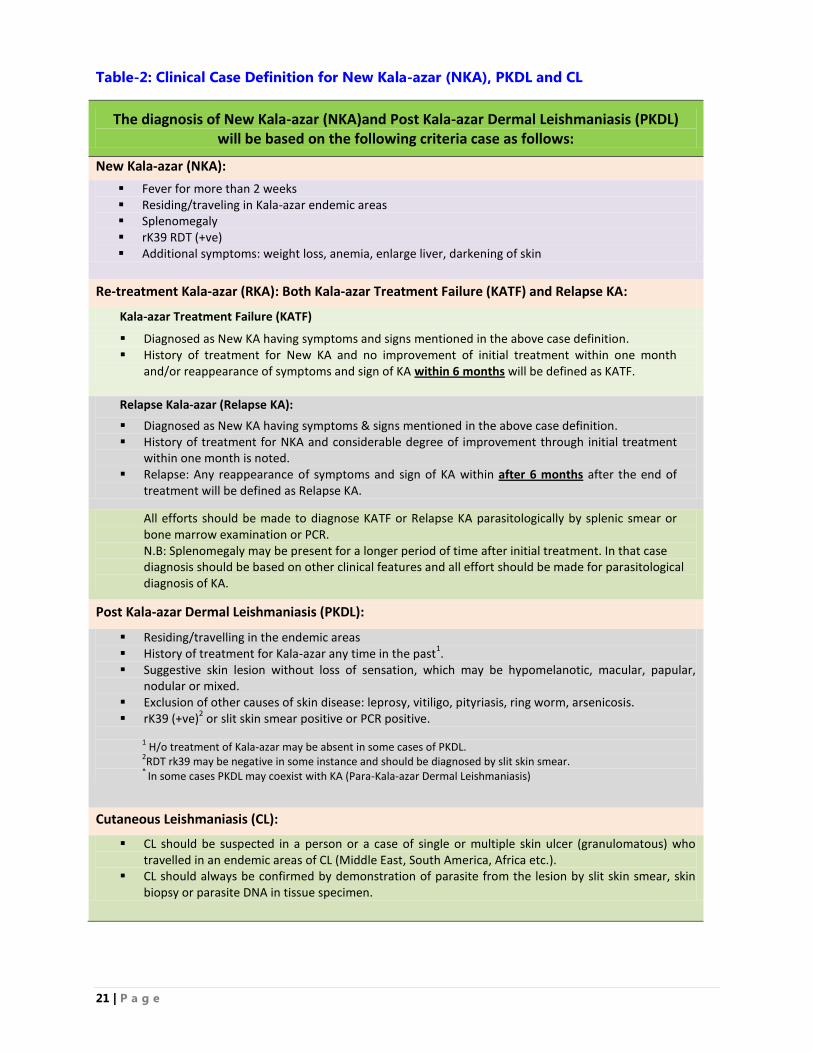
21 | P a g e
Table-2: Clinical Case Definition for New Kala-azar (NKA), PKDL and CL
The diagnosis of New Kala-azar (NKA)and Post Kala-azar Dermal Leishmaniasis (PKDL) will be based on the following criteria case as follows:
New Kala-azar (NKA):
Fever for more than 2 weeks Residing/traveling in Kala-azar endemic areas Splenomegaly rK39 RDT (+ve) Additional symptoms: weight loss, anemia, enlarge liver, darkening of skin
Re-treatment Kala-azar (RKA): Both Kala-azar Treatment Failure (KATF) and Relapse KA:
Kala-azar Treatment Failure (KATF)
Diagnosed as New KA having symptoms and signs mentioned in the above case definition. History of treatment for New KA and no improvement of initial treatment within one month
and/or reappearance of symptoms and sign of KA within 6 months will be defined as KATF.
Relapse Kala-azar (Relapse KA):
Diagnosed as New KA having symptoms & signs mentioned in the above case definition. History of treatment for NKA and considerable degree of improvement through initial treatment
within one month is noted. Relapse: Any reappearance of symptoms and sign of KA within after 6 months after the end of
treatment will be defined as Relapse KA.
All efforts should be made to diagnose KATF or Relapse KA parasitologically by splenic smear or bone marrow examination or PCR. N.B: Splenomegaly may be present for a longer period of time after initial treatment. In that case diagnosis should be based on other clinical features and all effort should be made for parasitological diagnosis of KA.
Post Kala-azar Dermal Leishmaniasis (PKDL):
Residing/travelling in the endemic areas History of treatment for Kala-azar any time in the past
1.
Suggestive skin lesion without loss of sensation, which may be hypomelanotic, macular, papular, nodular or mixed.
Exclusion of other causes of skin disease: leprosy, vitiligo, pityriasis, ring worm, arsenicosis. rK39 (+ve)
2 or slit skin smear positive or PCR positive.
1 H/o treatment of Kala-azar may be absent in some cases of PKDL.
2RDT rk39 may be negative in some instance and should be diagnosed by slit skin smear.
* In some cases PKDL may coexist with KA (Para-Kala-azar Dermal Leishmaniasis)
Cutaneous Leishmaniasis (CL):
CL should be suspected in a person or a case of single or multiple skin ulcer (granulomatous) who travelled in an endemic areas of CL (Middle East, South America, Africa etc.).
CL should always be confirmed by demonstration of parasite from the lesion by slit skin smear, skin biopsy or parasite DNA in tissue specimen.
22 | P a g e
2.3 KALA-AZAR WITH CO-INFECTIONS
The most frequent causes of death of Kala azar patients are due to presence of co-morbidities. The
common co-morbid illness are Kala-azar-TB co-infection, Kala-azar hepatitis co-infection, Kala-azar with
hematological diseases, Kala-azar-HIV co-infection, Kala-azar with Diabetes, Kala-azar in pregnancy,
Kala-azar Malaria co-infection, etc. All efforts should be made to diagnose KA with co-morbid illness by
parasitological examination of splenic smear or bone marrow or PCR. In cases of Kala-azar HIV co-
infection 'rK39' test may be negative. Patients with Kala-azar in special situations should be referred to
the required level of health facilities as appropriate.
Bangladesh is a country where both TB and Kala-azar exist. SK-KRC, a specialized research centre, had
diagnosed four cases of NKA having pulmonary tuberculosis, two cases of NKA with malaria, and six
cases NKA with Hepatitis in 2014 (Dr. Ariful Basher, SK-KRC). Hasnain et al (2013) reported a first case
of Kala-azar TB co-infection from a village of Trishal Upazila, one of the hyper-endemic areas of
Mymensingh District. The case was first identified as TB and was treated with TB drug according to the
National TB Guideline of Bangladesh. After taking 5-week of anti-TB drug the patient was diagnosed as
Kala-azar and was treated with AmBisome. With completion of successful treatment, the patient
recovered fully from TB and Kala-azar.3
Kala-azar HIV/AIDS co-infection has been appeared to be an increasing problem in countries such as
Ethiopia, Sudan and Brazil where both infections are becoming more and more prevalent. In Asia, co-
infections are increasingly being reported in India, which also has the highest global burden of Kala-azar.
KA-HIV coinfection is currently reported for 2-9% of all cases in given countries of endemicity. In India,
the first case of KA-HIV coinfection was reported in 1999; the KA-HIV coinfection rate has increased
from 0.88% in 2000 to 2.18% in 2006. In a case series from India, rate of HIV positive among PKDL
patients ranged from 1.5% to 6.3%. One hospital-based study in India reported a KA prevalence of 2.84%
among HIV-positive patients in 2006.
In Nepal, a study conducted for a period of one year from June 2003 to May 2004 in 39 hospitals showed
that 140 of 854 febrile patients had New Kala-azar and 8 of these were HIV positive (5.7%). Both NKA
and PKDL patients co-infected with any type of infection may act as an important reservoir of parasites
with high potential to maintain infection rates.
In Bangladesh, no case of Kala-azar HIV/AIDS co-infection has been reported so far. The diagnosis of
Kala-azar HIV co-infection is difficult because the clinical signs and symptoms are non-specific, and
splenomegaly is less frequent and most of these patients have other associated opportunistic infections
with similar symptoms, which usually complicate the clinical diagnosis.
3 Hasnain MG, et al (2013). Clinical Case Reports: First case of pulmonary tuberculosis and visceral leishmaniasis co-infection
successfully treated with anti-TB drug and AmBisome. Center for nutrition and food security, icddrb, Dhaka, Bangladesh.
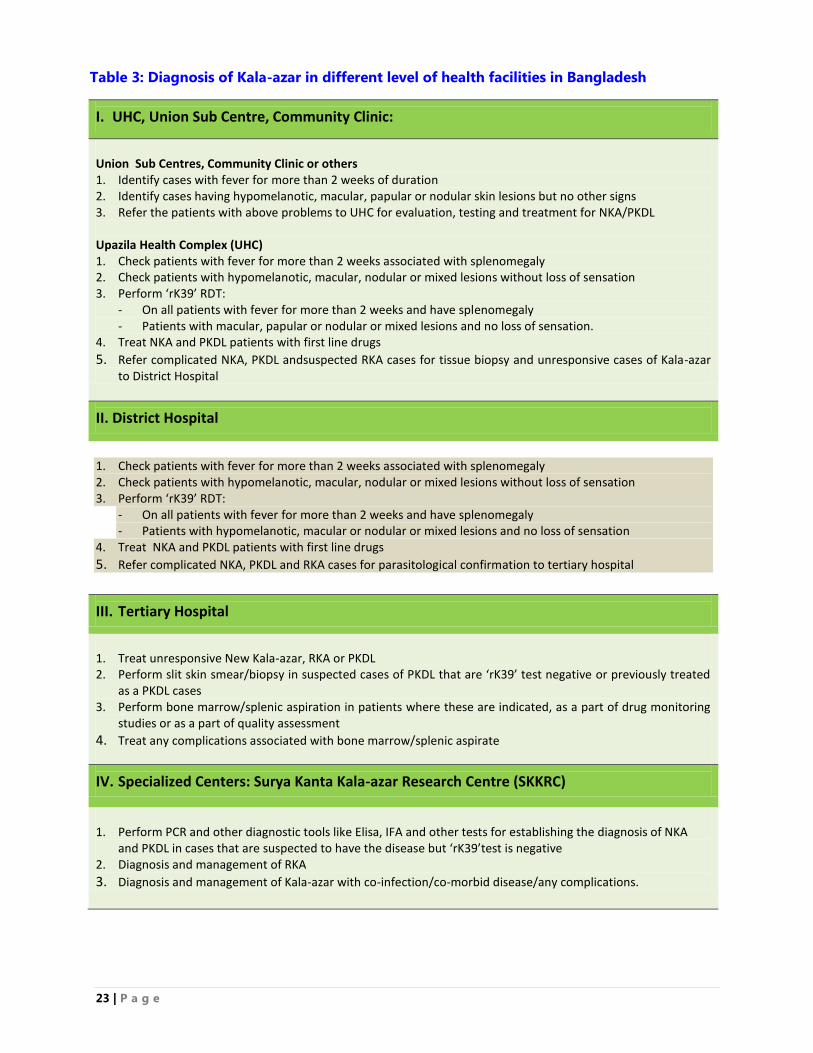
23 | P a g e
Table 3: Diagnosis of Kala-azar in different level of health facilities in Bangladesh
I. UHC, Union Sub Centre, Community Clinic:
Union Sub Centres, Community Clinic or others 1. Identify cases with fever for more than 2 weeks of duration 2. Identify cases having hypomelanotic, macular, papular or nodular skin lesions but no other signs 3. Refer the patients with above problems to UHC for evaluation, testing and treatment for NKA/PKDL Upazila Health Complex (UHC) 1. Check patients with fever for more than 2 weeks associated with splenomegaly 2. Check patients with hypomelanotic, macular, nodular or mixed lesions without loss of sensation 3. Perform ‘rK39’ RDT:
- On all patients with fever for more than 2 weeks and have splenomegaly - Patients with macular, papular or nodular or mixed lesions and no loss of sensation.
4. Treat NKA and PKDL patients with first line drugs
5. Refer complicated NKA, PKDL andsuspected RKA cases for tissue biopsy and unresponsive cases of Kala-azar to District Hospital
II. District Hospital
1. Check patients with fever for more than 2 weeks associated with splenomegaly 2. Check patients with hypomelanotic, macular, nodular or mixed lesions without loss of sensation 3. Perform ‘rK39’ RDT:
- On all patients with fever for more than 2 weeks and have splenomegaly - Patients with hypomelanotic, macular or nodular or mixed lesions and no loss of sensation
4. Treat NKA and PKDL patients with first line drugs
5. Refer complicated NKA, PKDL and RKA cases for parasitological confirmation to tertiary hospital
III. Tertiary Hospital
1. Treat unresponsive New Kala-azar, RKA or PKDL 2. Perform slit skin smear/biopsy in suspected cases of PKDL that are ‘rK39’ test negative or previously treated
as a PKDL cases 3. Perform bone marrow/splenic aspiration in patients where these are indicated, as a part of drug monitoring
studies or as a part of quality assessment
4. Treat any complications associated with bone marrow/splenic aspirate
IV. Specialized Centers: Surya Kanta Kala-azar Research Centre (SKKRC)
1. Perform PCR and other diagnostic tools like Elisa, IFA and other tests for establishing the diagnosis of NKA and PKDL in cases that are suspected to have the disease but ‘rK39’test is negative
2. Diagnosis and management of RKA
3. Diagnosis and management of Kala-azar with co-infection/co-morbid disease/any complications.
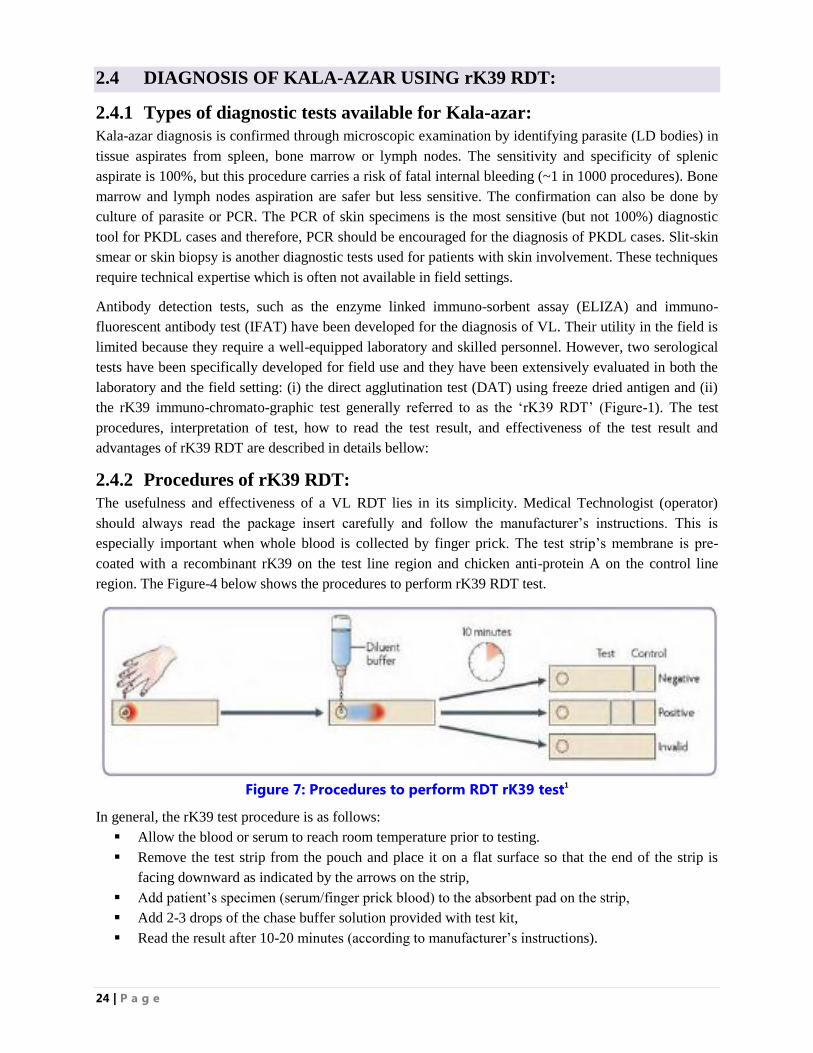
24 | P a g e
2.4 DIAGNOSIS OF KALA-AZAR USING rK39 RDT:
2.4.1 Types of diagnostic tests available for Kala-azar:
Kala-azar diagnosis is confirmed through microscopic examination by identifying parasite (LD bodies) in
tissue aspirates from spleen, bone marrow or lymph nodes. The sensitivity and specificity of splenic
aspirate is 100%, but this procedure carries a risk of fatal internal bleeding (~1 in 1000 procedures). Bone
marrow and lymph nodes aspiration are safer but less sensitive. The confirmation can also be done by
culture of parasite or PCR. The PCR of skin specimens is the most sensitive (but not 100%) diagnostic
tool for PKDL cases and therefore, PCR should be encouraged for the diagnosis of PKDL cases. Slit-skin
smear or skin biopsy is another diagnostic tests used for patients with skin involvement. These techniques
require technical expertise which is often not available in field settings.
Antibody detection tests, such as the enzyme linked immuno-sorbent assay (ELIZA) and immuno-
fluorescent antibody test (IFAT) have been developed for the diagnosis of VL. Their utility in the field is
limited because they require a well-equipped laboratory and skilled personnel. However, two serological
tests have been specifically developed for field use and they have been extensively evaluated in both the
laboratory and the field setting: (i) the direct agglutination test (DAT) using freeze dried antigen and (ii)
the rK39 immuno-chromato-graphic test generally referred to as the „rK39 RDT‟ (Figure-1). The test
procedures, interpretation of test, how to read the test result, and effectiveness of the test result and
advantages of rK39 RDT are described in details bellow:
2.4.2 Procedures of rK39 RDT:
The usefulness and effectiveness of a VL RDT lies in its simplicity. Medical Technologist (operator)
should always read the package insert carefully and follow the manufacturer‟s instructions. This is
especially important when whole blood is collected by finger prick. The test strip‟s membrane is pre-
coated with a recombinant rK39 on the test line region and chicken anti-protein A on the control line
region. The Figure-4 below shows the procedures to perform rK39 RDT test.
Figure 7: Procedures to perform RDT rK39 test1
In general, the rK39 test procedure is as follows:
Allow the blood or serum to reach room temperature prior to testing.
Remove the test strip from the pouch and place it on a flat surface so that the end of the strip is
facing downward as indicated by the arrows on the strip,
Add patient‟s specimen (serum/finger prick blood) to the absorbent pad on the strip,
Add 2-3 drops of the chase buffer solution provided with test kit,
Read the result after 10-20 minutes (according to manufacturer‟s instructions).
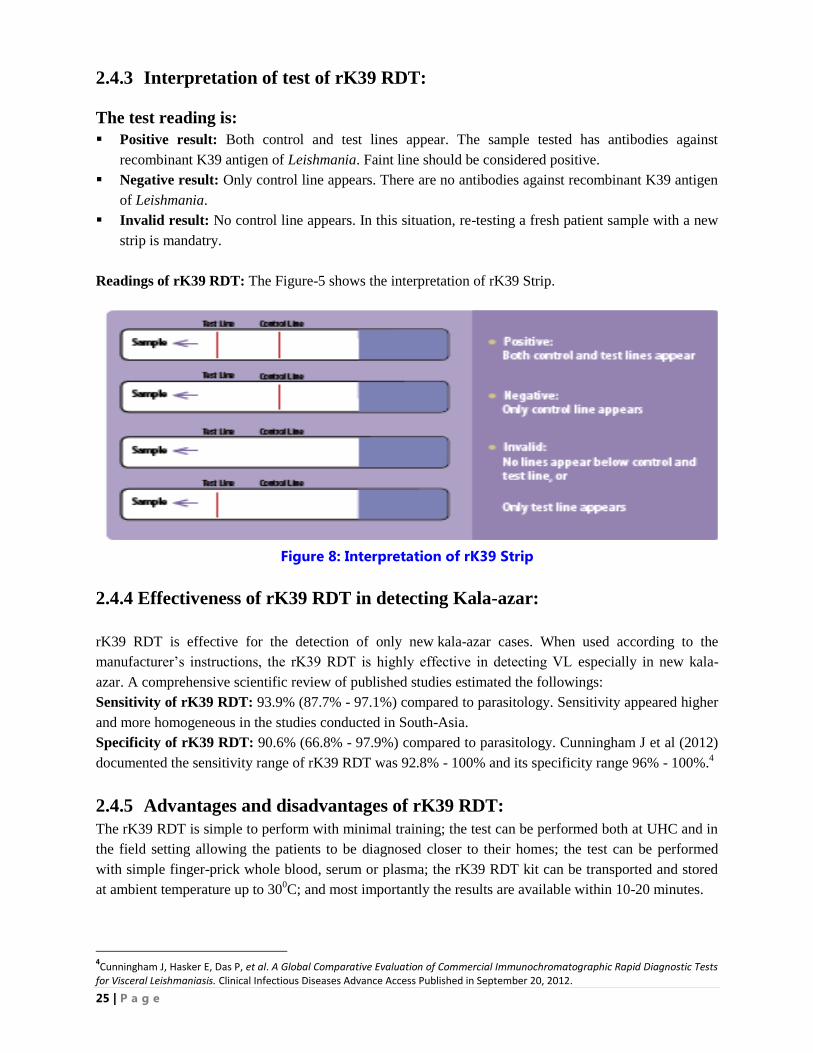
25 | P a g e
2.4.3 Interpretation of test of rK39 RDT:
The test reading is:
Positive result: Both control and test lines appear. The sample tested has antibodies against
recombinant K39 antigen of Leishmania. Faint line should be considered positive.
Negative result: Only control line appears. There are no antibodies against recombinant K39 antigen
of Leishmania.
Invalid result: No control line appears. In this situation, re-testing a fresh patient sample with a new
strip is mandatry.
Readings of rK39 RDT: The Figure-5 shows the interpretation of rK39 Strip.
Figure 8: Interpretation of rK39 Strip
2.4.4 Effectiveness of rK39 RDT in detecting Kala-azar:
rK39 RDT is effective for the detection of only new kala-azar cases. When used according to the
manufacturer‟s instructions, the rK39 RDT is highly effective in detecting VL especially in new kala-
azar. A comprehensive scientific review of published studies estimated the followings:
Sensitivity of rK39 RDT: 93.9% (87.7% - 97.1%) compared to parasitology. Sensitivity appeared higher
and more homogeneous in the studies conducted in South-Asia.
Specificity of rK39 RDT: 90.6% (66.8% - 97.9%) compared to parasitology. Cunningham J et al (2012)
documented the sensitivity range of rK39 RDT was 92.8% - 100% and its specificity range 96% - 100%.4
2.4.5 Advantages and disadvantages of rK39 RDT:
The rK39 RDT is simple to perform with minimal training; the test can be performed both at UHC and in
the field setting allowing the patients to be diagnosed closer to their homes; the test can be performed
with simple finger-prick whole blood, serum or plasma; the rK39 RDT kit can be transported and stored
at ambient temperature up to 300C; and most importantly the results are available within 10-20 minutes.
4Cunningham J, Hasker E, Das P, et al. A Global Comparative Evaluation of Commercial Immunochromatographic Rapid Diagnostic Tests
for Visceral Leishmaniasis. Clinical Infectious Diseases Advance Access Published in September 20, 2012.
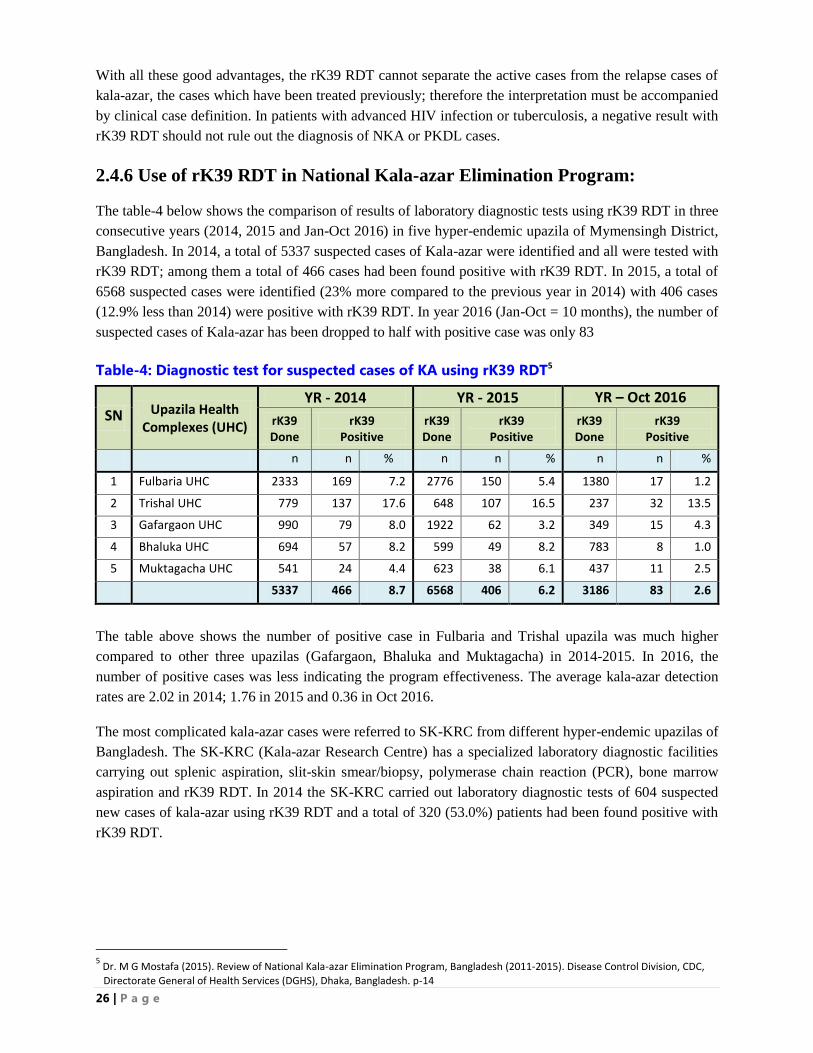
26 | P a g e
With all these good advantages, the rK39 RDT cannot separate the active cases from the relapse cases of
kala-azar, the cases which have been treated previously; therefore the interpretation must be accompanied
by clinical case definition. In patients with advanced HIV infection or tuberculosis, a negative result with
rK39 RDT should not rule out the diagnosis of NKA or PKDL cases.
2.4.6 Use of rK39 RDT in National Kala-azar Elimination Program:
The table-4 below shows the comparison of results of laboratory diagnostic tests using rK39 RDT in three
consecutive years (2014, 2015 and Jan-Oct 2016) in five hyper-endemic upazila of Mymensingh District,
Bangladesh. In 2014, a total of 5337 suspected cases of Kala-azar were identified and all were tested with
rK39 RDT; among them a total of 466 cases had been found positive with rK39 RDT. In 2015, a total of
6568 suspected cases were identified (23% more compared to the previous year in 2014) with 406 cases
(12.9% less than 2014) were positive with rK39 RDT. In year 2016 (Jan-Oct = 10 months), the number of
suspected cases of Kala-azar has been dropped to half with positive case was only 83
Table-4: Diagnostic test for suspected cases of KA using rK39 RDT5
SN Upazila Health Complexes (UHC)
YR - 2014 YR - 2015 YR – Oct 2016
rK39 Done
rK39 Positive
rK39 Done
rK39 Positive
rK39 Done
rK39 Positive
n n % n n % n n %
1 Fulbaria UHC 2333 169 7.2 2776 150 5.4 1380 17 1.2
2 Trishal UHC 779 137 17.6 648 107 16.5 237 32 13.5
3 Gafargaon UHC 990 79 8.0 1922 62 3.2 349 15 4.3
4 Bhaluka UHC 694 57 8.2 599 49 8.2 783 8 1.0
5 Muktagacha UHC 541 24 4.4 623 38 6.1 437 11 2.5
5337 466 8.7 6568 406 6.2 3186 83 2.6
The table above shows the number of positive case in Fulbaria and Trishal upazila was much higher
compared to other three upazilas (Gafargaon, Bhaluka and Muktagacha) in 2014-2015. In 2016, the
number of positive cases was less indicating the program effectiveness. The average kala-azar detection
rates are 2.02 in 2014; 1.76 in 2015 and 0.36 in Oct 2016.
The most complicated kala-azar cases were referred to SK-KRC from different hyper-endemic upazilas of
Bangladesh. The SK-KRC (Kala-azar Research Centre) has a specialized laboratory diagnostic facilities
carrying out splenic aspiration, slit-skin smear/biopsy, polymerase chain reaction (PCR), bone marrow
aspiration and rK39 RDT. In 2014 the SK-KRC carried out laboratory diagnostic tests of 604 suspected
new cases of kala-azar using rK39 RDT and a total of 320 (53.0%) patients had been found positive with
rK39 RDT.
5 Dr. M G Mostafa (2015). Review of National Kala-azar Elimination Program, Bangladesh (2011-2015). Disease Control Division, CDC,
Directorate General of Health Services (DGHS), Dhaka, Bangladesh. p-14

27 | P a g e

28 | P a g e
CHAPTER: THREE
TREATMENT OF NEW KALA-AZAR (NKA),
POST KALA-AZAR DERMAL LEISHMANIASIS (PKDL)
AND CUTANEOUS LEISHMANISIS (CL)
29 | P a g e
3. TREATMENT OF KALA-AZAR, PKDL AND CL
The primary objective of treatment for Kala-azar is to cure the patient, prevent complications of the
disease, minimize side effects of medicines, prevent emergence of drug resistance, and reduce the risk of
spread of kala-azar from the country. The secondary objective is to diagnose and treat appropriately the
complications and concomitant disease conditions if any arises.
3.1 TREATMENT OF NEW KALA-AZAR (NKA):
The Regional Technical Advisory Group (RTAG) of WHO/SEARO at its meeting in Dhaka in 2009
recommended introducing single dose Liposomal Amphotericin B (LAmB), which is safe, highly
effective and guarantee 100 percent treatment compliance. The NKEP of Bangladesh has sorted out
several issues while including LAmB (AmBisome) in the program and ensured maintenance cold chain
and space for drug storage; ensure supply of electricity round the clock or availability of generator;
conduction of training of doctors, nurses and other health care delivery workers for treatment of kala-azar
with AmBisome ensuring knowledge of Good Clinical and Laboratory Practices.
The NKEP has accepted the recommendation of RTAG and has approved the policy of introducing
LAmB (AmBisome) single dose as the drug of choice for the 1st line of treatment. Evidence obtained
from the randomized controlled trial shows that a total dose of ≥ 10 mg/kg body weight results in a cure
rate of more than 95% in Bangladesh, India and Nepal. In India, a 90% cure rate was found with a single
dose of 5 mg/kg body weight, and a 98% cure rate was achieved with a single dose of 10 mg/kg.
In case of drug reaction with LAmB (AmBisome), alternative choice to 1st line of treatment is
Miltefosine, the dose of which is depended on age and body weight of the patients to be administered for
28 days. On the other hand, Paromomycin 15 mg/kg body weight in intramuscular form is another
alternative choice to 1st line of treatment to be dispensed daily for 21 days. Three different combination
of drug, which are alternative choice to 1st line treatment, are available, these are: (i) Miltefosine and
Paromomycin daily for 10 days; or (ii) LAmB (AmBisome) in single dose and Miltefosine daily for 7
days; or (iii) LAmB (AmBisome) in single dose and Paromomycin daily for 10 days (Table-6).
It has been reported that various combination regimens of LAmB (AmBisome), Miltefosine and
Paromomycin are highly effective and safe, all are above 95% efficacious; the program‟s choice can
depend on cost and availability. Combination therapy is expected to prevent or delay the development of
resistance of Leishmania donovani. The choice between monotherapy or combination therapy is a
complex one, and the context should be very carefully considered.
When we compare the efficacy of single dose infusions of LAmB (AmBisome) with that of combination
therapy, we found a single-dose infusion has a clear advantage over other drugs. However, it should be
administered in a safe and correct way, monitored and evaluated patients during infusion, maintained
quality, ensured cold chain, and stored the drug in a safe space with round the clock electricity supply. In
the absence of the above criteria a choice for a combination regimen seems the better option.
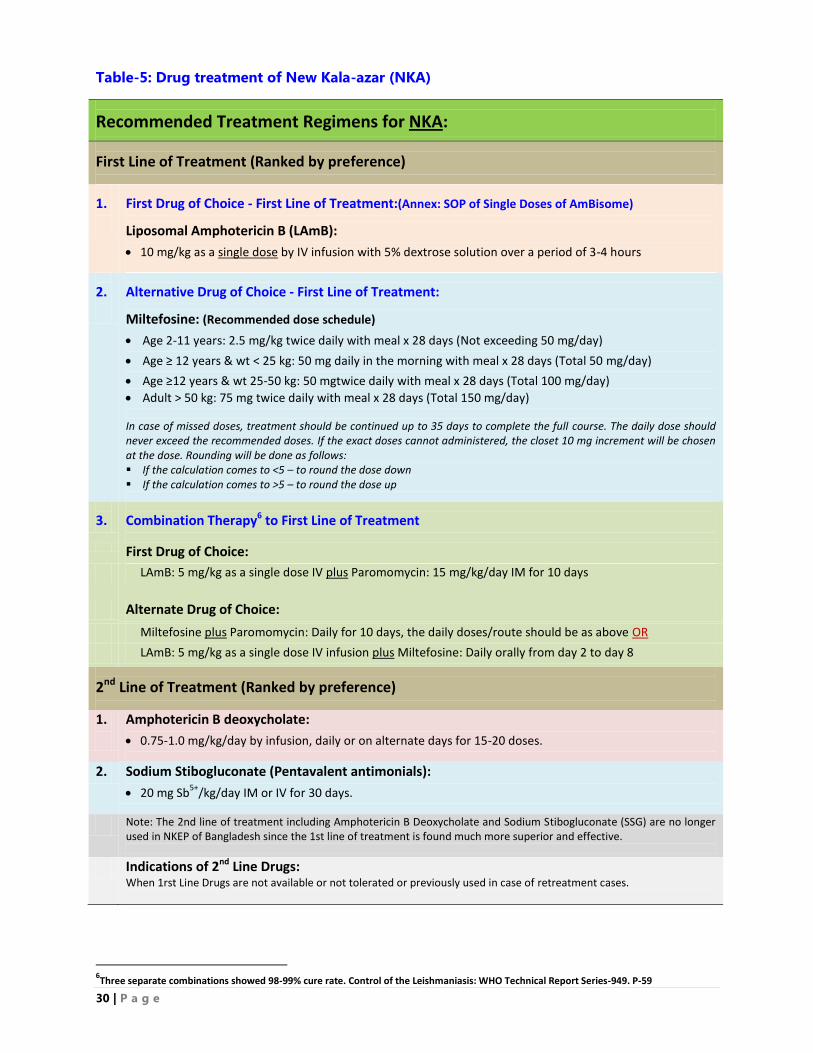
30 | P a g e
Table-5: Drug treatment of New Kala-azar (NKA)
Recommended Treatment Regimens for NKA:
First Line of Treatment (Ranked by preference)
1.
First Drug of Choice - First Line of Treatment:(Annex: SOP of Single Doses of AmBisome)
Liposomal Amphotericin B (LAmB):
10 mg/kg as a single dose by IV infusion with 5% dextrose solution over a period of 3-4 hours
2.
Alternative Drug of Choice - First Line of Treatment:
Miltefosine: (Recommended dose schedule)
Age 2-11 years: 2.5 mg/kg twice daily with meal x 28 days (Not exceeding 50 mg/day)
Age ≥ 12 years & wt < 25 kg: 50 mg daily in the morning with meal x 28 days (Total 50 mg/day)
Age ≥12 years & wt 25-50 kg: 50 mgtwice daily with meal x 28 days (Total 100 mg/day)
Adult > 50 kg: 75 mg twice daily with meal x 28 days (Total 150 mg/day)
In case of missed doses, treatment should be continued up to 35 days to complete the full course. The daily dose should never exceed the recommended doses. If the exact doses cannot administered, the closet 10 mg increment will be chosen at the dose. Rounding will be done as follows: If the calculation comes to <5 – to round the dose down If the calculation comes to >5 – to round the dose up
3.
Combination Therapy6 to First Line of Treatment
First Drug of Choice:
LAmB: 5 mg/kg as a single dose IV plus Paromomycin: 15 mg/kg/day IM for 10 days
Alternate Drug of Choice:
Miltefosine plus Paromomycin: Daily for 10 days, the daily doses/route should be as above OR
LAmB: 5 mg/kg as a single dose IV infusion plus Miltefosine: Daily orally from day 2 to day 8
2nd Line of Treatment (Ranked by preference)
1.
Amphotericin B deoxycholate:
0.75-1.0 mg/kg/day by infusion, daily or on alternate days for 15-20 doses.
2. Sodium Stibogluconate (Pentavalent antimonials):
20 mg Sb5+
/kg/day IM or IV for 30 days.
Note: The 2nd line of treatment including Amphotericin B Deoxycholate and Sodium Stibogluconate (SSG) are no longer used in NKEP of Bangladesh since the 1st line of treatment is found much more superior and effective.
Indications of 2nd Line Drugs: When 1rst Line Drugs are not available or not tolerated or previously used in case of retreatment cases.
6Three separate combinations showed 98-99% cure rate. Control of the Leishmaniasis: WHO Technical Report Series-949. P-59
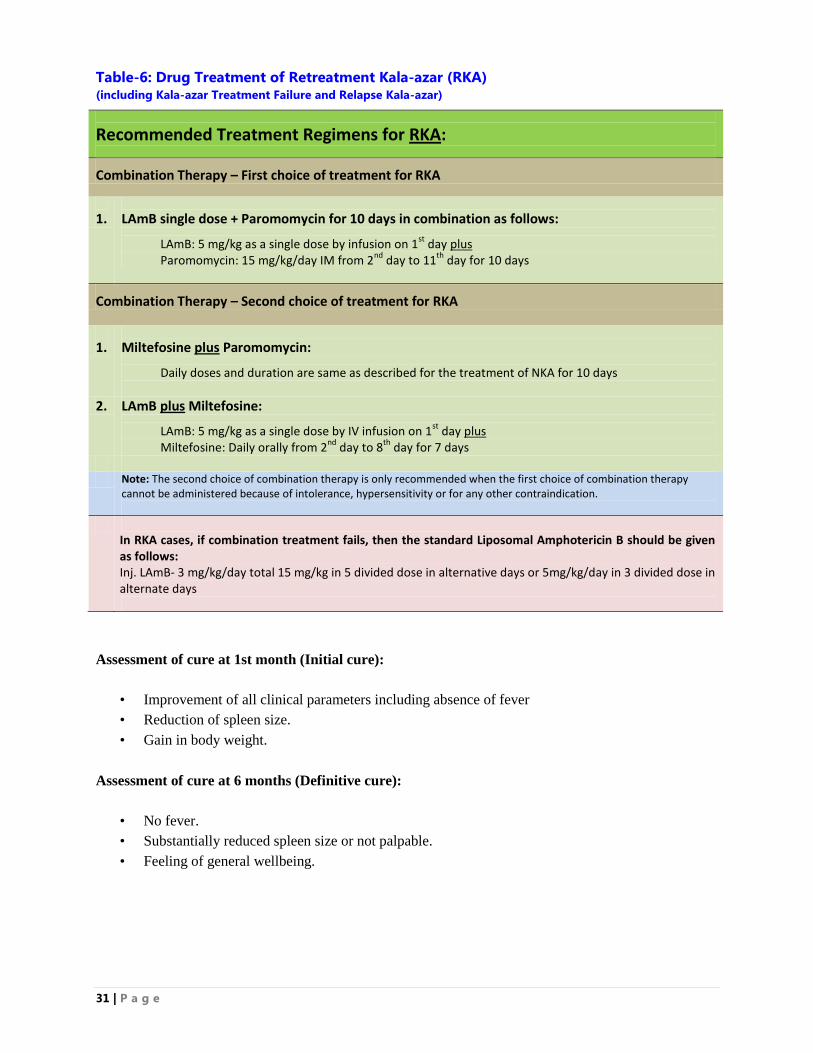
31 | P a g e
Table-6: Drug Treatment of Retreatment Kala-azar (RKA) (including Kala-azar Treatment Failure and Relapse Kala-azar)
Recommended Treatment Regimens for RKA:
Combination Therapy – First choice of treatment for RKA
1.
LAmB single dose + Paromomycin for 10 days in combination as follows:
LAmB: 5 mg/kg as a single dose by infusion on 1st
day plus Paromomycin: 15 mg/kg/day IM from 2
nd day to 11
th day for 10 days
Combination Therapy – Second choice of treatment for RKA
1.
Miltefosine plus Paromomycin:
Daily doses and duration are same as described for the treatment of NKA for 10 days
2. LAmB plus Miltefosine:
LAmB: 5 mg/kg as a single dose by IV infusion on 1st
day plus Miltefosine: Daily orally from 2
nd day to 8
th day for 7 days
Note: The second choice of combination therapy is only recommended when the first choice of combination therapy
cannot be administered because of intolerance, hypersensitivity or for any other contraindication.
In RKA cases, if combination treatment fails, then the standard Liposomal Amphotericin B should be given as follows: Inj. LAmB- 3 mg/kg/day total 15 mg/kg in 5 divided dose in alternative days or 5mg/kg/day in 3 divided dose in alternate days
Assessment of cure at 1st month (Initial cure):
• Improvement of all clinical parameters including absence of fever
• Reduction of spleen size.
• Gain in body weight.
Assessment of cure at 6 months (Definitive cure):
• No fever.
• Substantially reduced spleen size or not palpable.
• Feeling of general wellbeing.
32 | P a g e
3.2 TREATMENT OF POST KALA-AZAR DERMAL LEISHMANIASIS
Pathogenesis: The pathogenesis of Post Kala-azar Dermal Leishmaniasis (PKDL) occurs usually after the
treatment of visceral leishmaniasis (VL) in a proportion of patients, and is considered to be triggered
immunologically7. In VL the predominant immune response is a Th2 response; whereas in PKDL there is
a mixed Th1 and Th2 response with persistence of interleukin 10 (IL-10). It is difficult to predict who will
develop PKDL. Inadequate treatment for VL for example, treatment with a low dose of medicine or for a
short/incomplete duration, young age generally 5-17 years, malnutrition, HIV infection and antiretroviral
treatment may play a part in the development of PKDL. There are no proven predictors of PKDL, such as
the degree of splenomegaly or hepatomegaly during VL. PKDL occurs almost exclusively in patients with
VL caused by L. donovani. In biopsy samples, PKDL in India shows a diffuse dermal infiltrate of
macrophages, lymphocytes and plasma cells.
The inflammatory cells are mainly CD3+ cells; IL-10 is predominant in the lesions; interferon-gamma is
found uniformly; and IL-4 is present in varying amounts. Diminished expression of Th1-Type Cytokines
(interferon-gamma) receptor 1 (R-1) and tumour necrosing factor R1 and R2 receptors during PKDL may
interfere with an effective host response. IL-10 expressing CD3+CD8+ lymphocytes are prominent, and
their level decreases with treatment. Patients with PKDL present raised levels of immunoglobulins (G3
and G1) and increased serum levels of IL-10. High serum concentrations of IL-10 during visceral
leishmaniasis correlate with subsequent development of PKDL. Anti-retroviral treatment during
HIV/AIDS co-infection can lead to PKDL. Favorable outcomes for patients with PKDL are predicted by a
positive leishmanin skin test or when levels of interferon-gamma (pro-inflammatory responses) are higher
than levels of IL-10 (anti-inflammatory response).
Clinical Manifestation: PKDL patients with their mild skin rash do not normally present to a health
facility. They do not have fever, and the physical examination is usually normal with no splenomegaly.
But in course of the disease, the skin manifestations may cause significant social and clinical discomfort.
Sometimes the lesions of PKDL are extensive covering mucosa of the lips and palate. In PKDL cases,
sensation over the lesions is preserved in contrast to leprosy where lesions have no sensations.
In Indian subcontinent, most of the patients have a polymorphic presentation comprising macular, papular
or nodular skin lesions, with prediction for the area around the chin and mouth. This presentation can be
subdivided into different forms as monomorphic (macular and nodular), polymorphic or mixed (both
macules and indurated lesions such as papules are present) and rare presentations (for example,
erythrodermic). The severity may be described as: mild with few skin lesions usually on the face;
moderate with lesions easily visible and generalized; and sever with dense coverage with lesions and little
normal skin remains.
Diagnosis: The cases of PKDL usually do not have any signs of kala-azar like fever, splenomegaly, or
anemia because 85-90% of them appear after the cure of kala-azar. It is documented that 15% of cases of
PKDL occur without the preceding history of kala-azar. Therefore, PKDL should be suspected in patients
7 T-Lymphocytes (T helper cells) are regarded as being the most prolific cytokine producers. T helper cells are subdivided into Th1 and
Th2, and the cytokines they produce are known as “Th1-Type Cytokines (interferon gamma)” and “Th2-Type Cytokines (interleukins 5, 9, 10, & 13)”. Cytokines (Th1-Type Cytokines and Th2-Type Cytokines) are the hormonal messengers responsible for most of the biological effects in the immune system, such as cell mediated immunity and allergic type of responses. The optimal scenario is that humans will produce well balanced Th1 and Th2 response, suited to the immune challenge.
33 | P a g e
in endemic areas who present with a skin rash combined with previous or concomitant visceral
leishmaniasis. The diagnosis can be made using clinical criteria or by identifying parasite, or both.
Clinical diagnosis is made by assessing the presence of the typical rash, its distribution, whether the
patient has a history of VL, or PKDL can also occur without previous VL; whether the patient lives in an
endemic area or has a recent history of travel to endemic area.
The rK39 RDT is usually positive in both papular and nodular lesions. A negative diagnostic test with
rK39 RDT in macular lesions does not rule out the possibility of PKDL. In such cases and also in nodular
and papular lesions, the diagnosis may be confirmed by biopsy or scraping of slit-skin in which the
smears are more likely to show amastigotes form of parasites; samples are least likely to show
amastigotes if taken from macular lesions. Culture can be attempted but it takes time and contamination is
common. Skin biopsies may also be examined by histopathology and immuno-histo-chemistry.
Polymerase chain reaction (PCR) tests performed with skin biopsy samples or slit-skin smear is much
more sensitive. The sensitivity of this test varies depending on the PCR method used and the type of
lesions. Quantitative PCR used to assess slit-skin specimens has been shown to be highly sensitive.
Treatment: The PKDL, a primary complication of NKA, is acting as potential reservoir for transmission
of visceral leishmaniasis. PKDL develops within a median time of 21 months (range, 0-120 months) after
VL, and most often is untreated. A severe form of the PKDL disease is very difficult to treat in some
patients. The most important challenges for the clinicians for the treatment of PKDL cases are the reliable
estimates of the burden of infection, infectiousness, pathogenesis, clinical presentations, determination of
the most infective types of PKDL lesions, effective treatment and control. The incidence of PKDL is
reducing in Bangladesh and India after introduction of Liposomal Amphotericin B (LAmB) and
Miltefosine for the treatment of NKA. An initial cure rate of 95% has been achieved with miltefosine for
the treatment of PKDL. However, the efficacy of combination therapy should be explored to reduce the
treatment duration and hence to improve treatment compliance. Younis BM, et al (2015) documented that
Paromomycin and SSG combination therapy was effective, time-saving and safe in treating PKDL cases
within 30 days8 (Table-8).
The objective of treatment of PKDL is the disappearance of all skin lesions of the patients; however, there
is no self-healing of the lesions in the Indian subcontinent. The treatment of PKDL at present is
unsatisfactory, although various regimens have been tried with variable success. There is no standard
treatment of PKDL approved by the national programme. In Bangladesh the number of VL cases are
decreasing, however, true PKDL rates are not known because of the inadequate and losses to follow-up of
PKDL cases. The frequent adverse effects of Miltefosine, 12 week long duration of drug treatment,
potential for emergence of resistance, compliance to Miltefosine treatment, and losses to follow-up are
some of the great concern for the treatment of PKDL patients in Bangladesh.
Treatment of PKDL requires long courses of therapy and very few clinical trials have been conducted to
compare the different regimens. The NKEP of Bangladesh has adopted and approved the policy to treat
PKDL patients with oral Miltefosine for a period of 12 weeks. The dose of Miltefosine is depended on
age and body weight and should be dispensed in divided doses with meal (Table-8).
8 Younis BM, et al (2015). Cure of post kala-azar dermal leishmaniasis with paromomycin/sodium stibogluconate combination: a proof of concept. Int J Res Med Sci. 2015; 3(1):16-21.
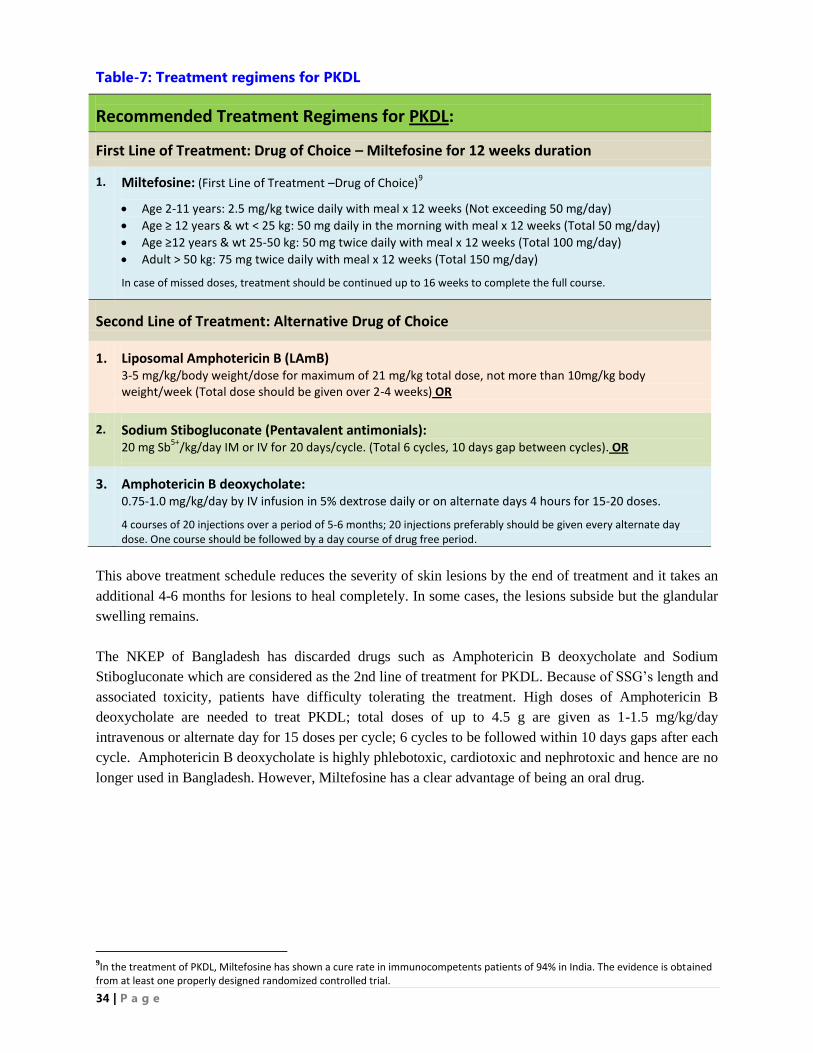
34 | P a g e
Table-7: Treatment regimens for PKDL
Recommended Treatment Regimens for PKDL:
First Line of Treatment: Drug of Choice – Miltefosine for 12 weeks duration
1.
Miltefosine: (First Line of Treatment –Drug of Choice)9
Age 2-11 years: 2.5 mg/kg twice daily with meal x 12 weeks (Not exceeding 50 mg/day)
Age ≥ 12 years & wt < 25 kg: 50 mg daily in the morning with meal x 12 weeks (Total 50 mg/day)
Age ≥12 years & wt 25-50 kg: 50 mg twice daily with meal x 12 weeks (Total 100 mg/day)
Adult > 50 kg: 75 mg twice daily with meal x 12 weeks (Total 150 mg/day)
In case of missed doses, treatment should be continued up to 16 weeks to complete the full course.
Second Line of Treatment: Alternative Drug of Choice
1.
Liposomal Amphotericin B (LAmB) 3-5 mg/kg/body weight/dose for maximum of 21 mg/kg total dose, not more than 10mg/kg body weight/week (Total dose should be given over 2-4 weeks) OR
2.
Sodium Stibogluconate (Pentavalent antimonials): 20 mg Sb
5+/kg/day IM or IV for 20 days/cycle. (Total 6 cycles, 10 days gap between cycles). OR
3.
Amphotericin B deoxycholate: 0.75-1.0 mg/kg/day by IV infusion in 5% dextrose daily or on alternate days 4 hours for 15-20 doses.
4 courses of 20 injections over a period of 5-6 months; 20 injections preferably should be given every alternate day dose. One course should be followed by a day course of drug free period.
This above treatment schedule reduces the severity of skin lesions by the end of treatment and it takes an
additional 4-6 months for lesions to heal completely. In some cases, the lesions subside but the glandular
swelling remains.
The NKEP of Bangladesh has discarded drugs such as Amphotericin B deoxycholate and Sodium
Stibogluconate which are considered as the 2nd line of treatment for PKDL. Because of SSG‟s length and
associated toxicity, patients have difficulty tolerating the treatment. High doses of Amphotericin B
deoxycholate are needed to treat PKDL; total doses of up to 4.5 g are given as 1-1.5 mg/kg/day
intravenous or alternate day for 15 doses per cycle; 6 cycles to be followed within 10 days gaps after each
cycle. Amphotericin B deoxycholate is highly phlebotoxic, cardiotoxic and nephrotoxic and hence are no
longer used in Bangladesh. However, Miltefosine has a clear advantage of being an oral drug.
9In the treatment of PKDL, Miltefosine has shown a cure rate in immunocompetents patients of 94% in India. The evidence is obtained from at least one properly designed randomized controlled trial.
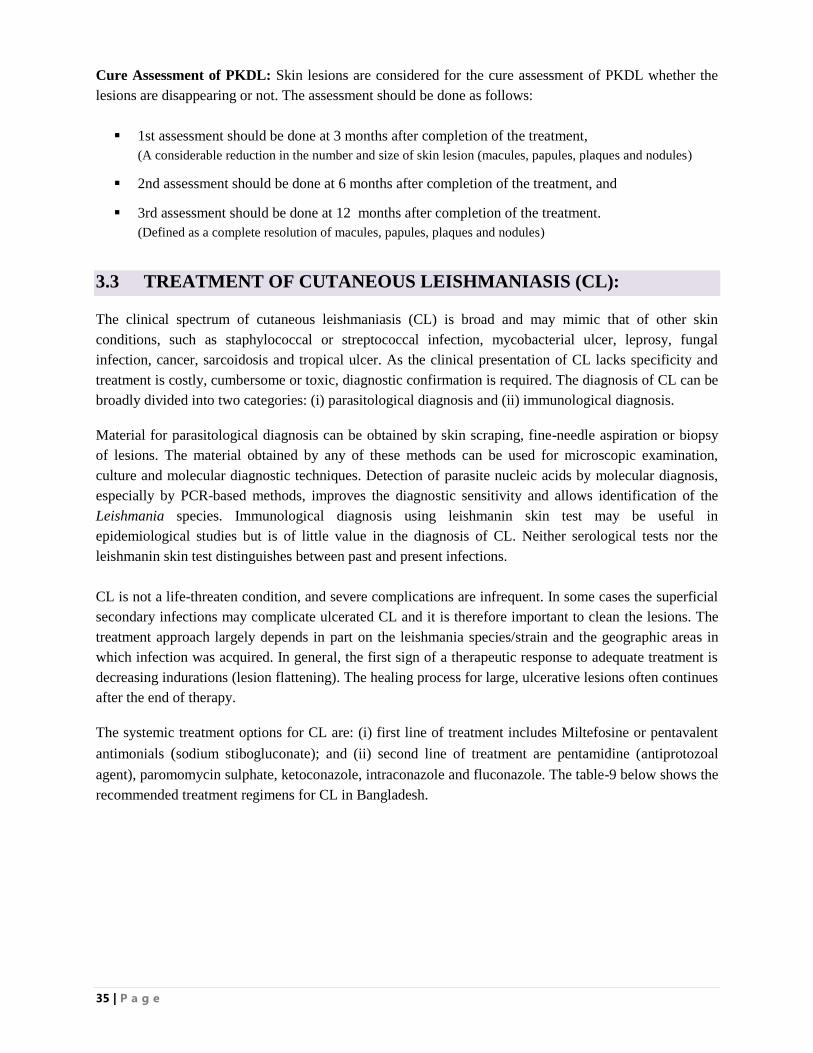
35 | P a g e
Cure Assessment of PKDL: Skin lesions are considered for the cure assessment of PKDL whether the
lesions are disappearing or not. The assessment should be done as follows:
1st assessment should be done at 3 months after completion of the treatment,
(A considerable reduction in the number and size of skin lesion (macules, papules, plaques and nodules)
2nd assessment should be done at 6 months after completion of the treatment, and
3rd assessment should be done at 12 months after completion of the treatment.
(Defined as a complete resolution of macules, papules, plaques and nodules)
3.3 TREATMENT OF CUTANEOUS LEISHMANIASIS (CL):
The clinical spectrum of cutaneous leishmaniasis (CL) is broad and may mimic that of other skin
conditions, such as staphylococcal or streptococcal infection, mycobacterial ulcer, leprosy, fungal
infection, cancer, sarcoidosis and tropical ulcer. As the clinical presentation of CL lacks specificity and
treatment is costly, cumbersome or toxic, diagnostic confirmation is required. The diagnosis of CL can be
broadly divided into two categories: (i) parasitological diagnosis and (ii) immunological diagnosis.
Material for parasitological diagnosis can be obtained by skin scraping, fine-needle aspiration or biopsy
of lesions. The material obtained by any of these methods can be used for microscopic examination,
culture and molecular diagnostic techniques. Detection of parasite nucleic acids by molecular diagnosis,
especially by PCR-based methods, improves the diagnostic sensitivity and allows identification of the
Leishmania species. Immunological diagnosis using leishmanin skin test may be useful in
epidemiological studies but is of little value in the diagnosis of CL. Neither serological tests nor the
leishmanin skin test distinguishes between past and present infections.
CL is not a life-threaten condition, and severe complications are infrequent. In some cases the superficial
secondary infections may complicate ulcerated CL and it is therefore important to clean the lesions. The
treatment approach largely depends in part on the leishmania species/strain and the geographic areas in
which infection was acquired. In general, the first sign of a therapeutic response to adequate treatment is
decreasing indurations (lesion flattening). The healing process for large, ulcerative lesions often continues
after the end of therapy.
The systemic treatment options for CL are: (i) first line of treatment includes Miltefosine or pentavalent
antimonials (sodium stibogluconate); and (ii) second line of treatment are pentamidine (antiprotozoal
agent), paromomycin sulphate, ketoconazole, intraconazole and fluconazole. The table-9 below shows the
recommended treatment regimens for CL in Bangladesh.
36 | P a g e
Table-8: Treatment of Cutaneous Leishmaniasis (CL)
Recommended Treatment Regimens for CL:
First Line of Treatment: Drug of Choice
1. Miltefosine:
Age 2-11 years: 2.5 mg/kg twice daily with meal x 28 days (Not exceeding 50 mg/day)
Age ≥ 12 years & wt < 25 kg: 50 mg daily in the morning with meal x 28 days (Total 50 mg/day)
Age ≥12 years & wt 25-50 kg: 50 mg twice daily with meal x 28 days (Total 100 mg/day)
Adult > 50 kg: 75 mg twice daily with meal x 28 days (Total 150 mg/day)
In case of missed doses, treatment should be continued up to 35 days to complete the full course. OR
2. Liposomal Amphotericin B (LAmB)
3-5 mg/kg/body weight/dose for maximum of 21 mg/kg total dose, not more than 10mg/kg body
weight/week (Total dose should be given over 2-4 weeks) OR
3. Sodium Stibogluconate (Pentavalent antimonials)
20 mg Sb5+
/kg/day IM or IV for 20 days.(10 days may suffice based on clinical judgment).
Second Line of Treatment
1. Ketokonazole: 600 mg daily for 28 days, OR
2. Itraconazole: 200 mg twice daily for 28 days, OR
3. Fluconazole:200 mg daily for 6 weeks (for adult)
Note: The description of drugs used for the treatment of Kala-azar is attached in Annex-8.
37 | P a g e
3.4 DIAGNOSIS AND TREATMENT OF KALA-AZAR IN SPECIAL
SITUATIONS:
The diagnosis and treatment of Kala-azar can be difficult in the following special situations such as:
children under 2 years old, pregnancy, married women of reproductive age who are not using
contraceptives regularly, women who are breast feeding their babies, and severe anemia (Hemoglobin
less than 5 g/dl).
Under the above special circumstances, the diagnosis and treatment should be decided cautiously.
Patients with Kala-azar in special situations should be referred to the required level of facility as
appropriate. The patient‟s treatment outcomes should be closely monitored.
The diagnosis and treatment of Kala-azar in special situations is recommended in centers where
appropriate clinical expertise and health facilities are available. The following conditions can be
considered as special situations:
Pregnancy:
In pregnancy, rK39 RDT may be negative due to altered immunity in pregnancy. The confirmation of
diagnosis can be done by either PCR or parasitological diagnosis through spleen puncture or bone
marrow aspiration in specialized centre. Risk of treatment should be weighed against benefit.
Treatment should be prioritized according to the severity. If a pregnant mother is diagnosed as NKA
during 1st trimester, she should be treated at 2
nd trimester, or if she diagnosed as NKA during 3
rd
trimester then she should be treated after delivery. Kala-azar with pregnancy should be treated with
LAmB as there is proven safety profile for using LAmB in pregnancy in SKKRC. Preferable doses
for Liposomal Amphotericin B will be 5 mg/kg body weight on alternate days for 3 doses or 3mg/kg
body weight for 5 doses in alternate days. Miltefosine and Sodium Stibogluconate are contraindicated
in case of pregnancy.
In Bangladesh a total of 4 cases of New Kala-azar (NKA) in pregnancy have been reported and
treated in SK-KRC in 2014. All four cases of NKA have been found positive with rK39 RDT and
treated with Injection AmBisome. The encouraging result is that all pregnant women delivered
healthy babies. One of 4 women developed PKDL after one year of treatment but the child was found
free from kala-azar. However, one of 4 babies was positive with rK39 RDT and has splenomegaly at
the age of one and half month (Dr. Ariful Basher of SK-KRC).
Rahman KM, et al (2014) described Kala-azar in pregnancy, a case identified from Fulbaria Upazila
of Mymensingh, using a method of social autopsy.10
Miah MT, et al (2010) in their retrospective
study conducted during 2005 to 2009 and documented a total of 16 Kala-azar cases in pregnancy, of
which 11 cases experienced miscarriage with no maternal deaths.11
The abortion took place mostly
between 22 to 24th day of treatment with Sodium Antimony Gluconate (SAG). The researchers in
their conclusion suggested that the kala-azar in pregnancy cases should not be treated with SAG in
early or mid-pregnancy.
10
Rahman KM, et al (2010). Kala-azar in Pregnancy in Mymensingh, BD: A Social Autopsy. PloS, Negl Trop Dis. 2014 May; 8(5) e2710. 11
Miah MT, Ayaz FM, Maniruzzaman M, et al (2010). Kala-azar in Pregnancy. Mymensingh Med J 19: 529-532 PubMed.
38 | P a g e
Married women of reproductive age who are not using contraceptives regularly:
The diagnosis in this situation will be as usual for KA or other patients. The rK39 based diagnosis
will be sufficient for case definition. The drug of choice is single dose Liposomal Amphotericin B
(Miltefosine is contraindicated).
Women who are breast feeding their babies:
The diagnosis in this situation will be as usual for KA or other patients. The rK39 based diagnosis
will be sufficient for case definition .The drug of choice is Liposomal Amphotericin B but temporary
discontinuation of breast feeding for 2 weeks should be advised.
Kala-azar with severe anemia (Hemoglobin less than 5 g/dl):
The diagnosis in this situation will be as usual for KA or other patient .There should be transfusion of
whole blood to raise hemoglobin ≥6 gm/dl prior to commencement of treatment.
Kala-azar with TB:
The diagnosis in this situation will be as usual for KA or other patients. Only disseminated
tuberculosis may need confirmed diagnosis through PCR or parasitological confirmation through
bone marrow aspiration or spleen puncture. Treatment of both diseases should be continued
simultaneously and KA will be treated as NKA or RKA as per case definition.
Kala-azar HIV/AIDS co-infection:
In HIV/AIDS, rK39 may be negative due to immmunosuppression. The confirmation of diagnosis can
be done by either PCR or parasitological diagnosis through Spleen puncture or bone marrow
aspiration in specialized centre. It will be treated with Liposomal Amphotericin B with multiple
doses. ARV should be continued for HIV/AIDS.
Kala-azar in a patient suffering from another serious disease:
In serious diseases, rK39 may be negative due to altered immune reaction. The confirmation of
diagnosis can be done by either PCR or parasitological diagnosis through spleen puncture or bone
marrow aspiration in specialized centre. All the cases of Kala-azar with serious co-morbidities should
be treated under specialized supervision. Liposomal Amphotericin B will be the drug of choice and
treatment should be given in a tertiary care facility.
Asymptomatic Parasitaemia:
There is no recommendation to use any drugs for asymptomatic parasitaemia. The parasitological or
PCR based diagnosis should be followed up for development of symptom. As soon as symptom
develops, patient should be treated as NKA.
39 | P a g e
3.5 COMPLETE TREATMENT OF KALA-AZAR:
Efforts should be made to ensure the complete treatment of kala-azar. The following measures are
recommended to complete the treatment:
Counseling: Every patient should be counseled so that the patient and family understand the
importance of complete treatment and the consequences of the incomplete treatment.
Free Medicine: All treatment should be free of cost to eliminate the economic constrains as a reason
for discontinuation of treatment.
Treatment Box: Each patient should have a separate treatment box kept at the health facility. The
box contains full dose of drugs labeled with the name, individual identification number, and number
of days the treatment received by the patients.
Follow-up patient: It is highly advisable to follow-up the patient during treatment, immediately after
treatment, and up to 12 months year (at 1st, 5th, 9th and 12th month). The treatment should be
directly observed as per SOP.
Coordination: There should be coordination amongst the public and private sector providers, and a
follow up plan should be develop for each patient.
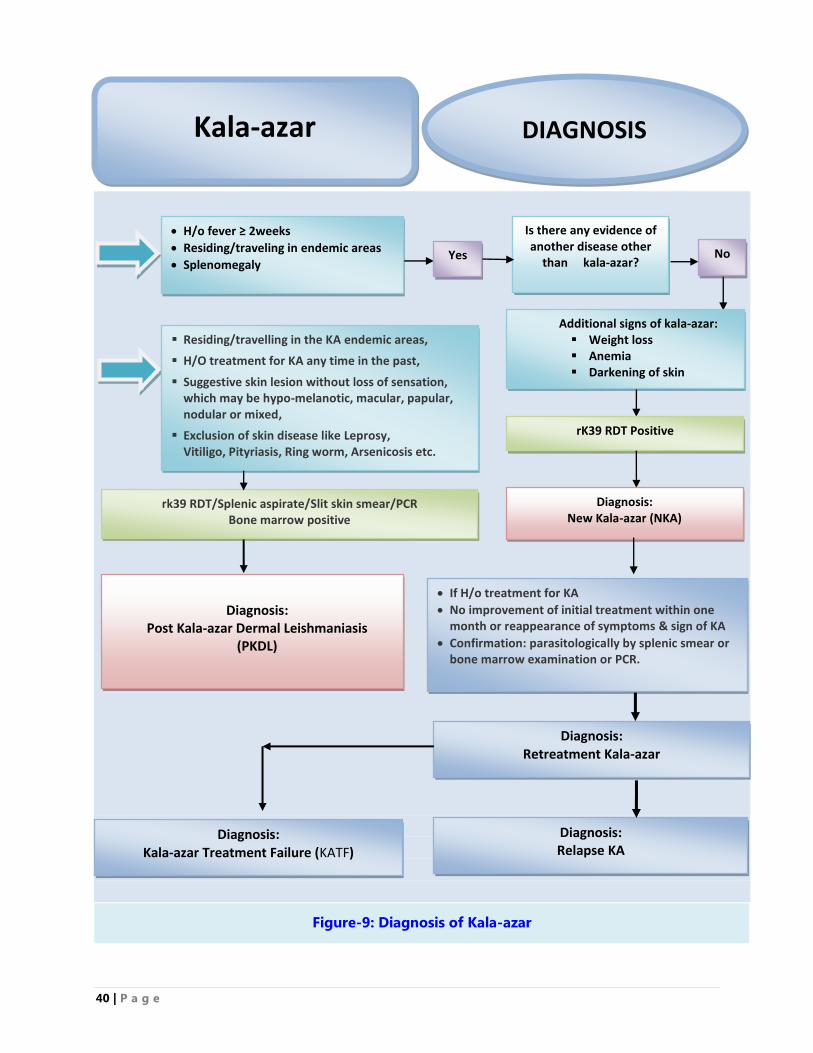
40 | P a g e
Is there any evidence of another disease other
than kala-azar? Yes
Additional signs of kala-azar: Weight loss Anemia Darkening of skin
rK39 RDT Positive
Diagnosis: New Kala-azar (NKA)
No
Diagnosis: Post Kala-azar Dermal Leishmaniasis
(PKDL)
Diagnosis: Retreatment Kala-azar
Residing/travelling in the KA endemic areas,
H/O treatment for KA any time in the past,
Suggestive skin lesion without loss of sensation, which may be hypo-melanotic, macular, papular, nodular or mixed,
Exclusion of skin disease like Leprosy, Vitiligo, Pityriasis, Ring worm, Arsenicosis etc.
H/o fever ≥ 2weeks
Residing/traveling in endemic areas
Splenomegaly
If H/o treatment for KA
No improvement of initial treatment within one month or reappearance of symptoms & sign of KA
Confirmation: parasitologically by splenic smear or bone marrow examination or PCR.
rk39 RDT/Splenic aspirate/Slit skin smear/PCR Bone marrow positive
DIAGNOSIS
Kala-azar
Figure-9: Diagnosis of Kala-azar
Diagnosis: Kala-azar Treatment Failure (KATF)
Diagnosis: Relapse KA
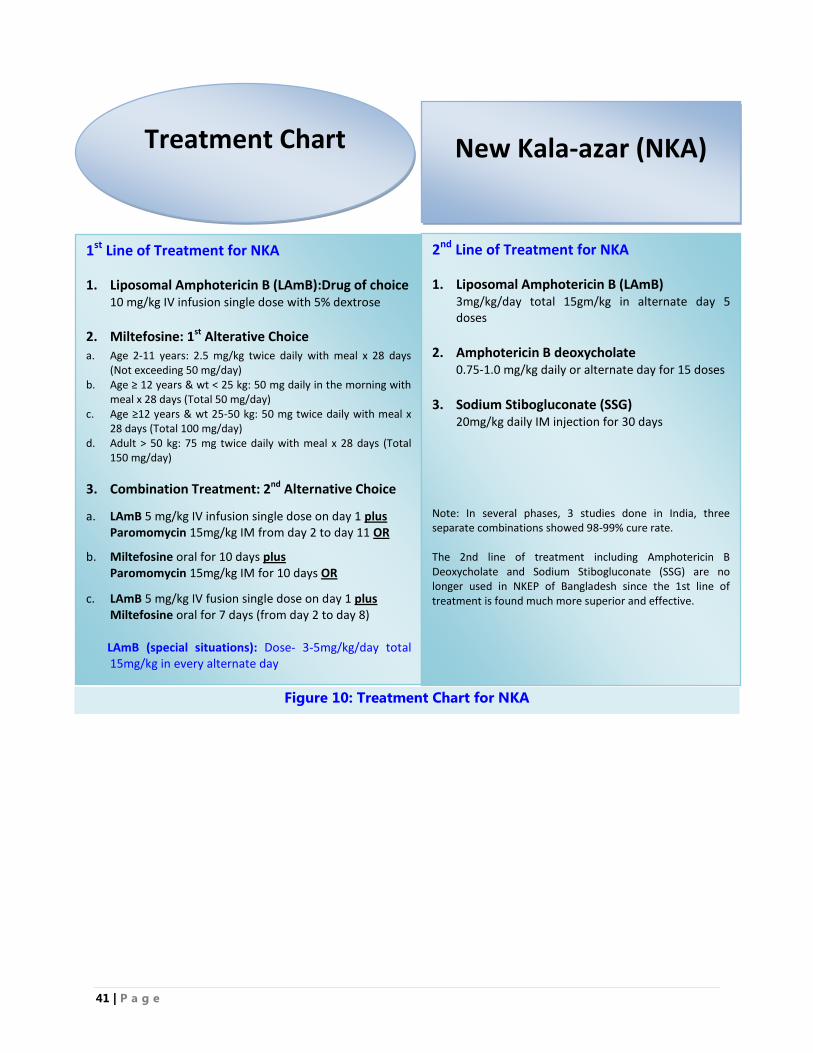
41 | P a g e
Figure 10: Treatment Chart for NKA
Treatment Chart
New Kala-azar (NKA)
1st Line of Treatment for NKA
1. Liposomal Amphotericin B (LAmB):Drug of choice 10 mg/kg IV infusion single dose with 5% dextrose
2. Miltefosine: 1st Alterative Choice a. Age 2-11 years: 2.5 mg/kg twice daily with meal x 28 days
(Not exceeding 50 mg/day) b. Age ≥ 12 years & wt < 25 kg: 50 mg daily in the morning with
meal x 28 days (Total 50 mg/day) c. Age ≥12 years & wt 25-50 kg: 50 mg twice daily with meal x
28 days (Total 100 mg/day) d. Adult > 50 kg: 75 mg twice daily with meal x 28 days (Total
150 mg/day)
3. Combination Treatment: 2nd Alternative Choice
a. LAmB 5 mg/kg IV infusion single dose on day 1 plus Paromomycin 15mg/kg IM from day 2 to day 11 OR
b. Miltefosine oral for 10 days plus Paromomycin 15mg/kg IM for 10 days OR
c. LAmB 5 mg/kg IV fusion single dose on day 1 plus Miltefosine oral for 7 days (from day 2 to day 8)
LAmB (special situations): Dose- 3-5mg/kg/day total 15mg/kg in every alternate day
2nd Line of Treatment for NKA
1. Liposomal Amphotericin B (LAmB) 3mg/kg/day total 15gm/kg in alternate day 5 doses
2. Amphotericin B deoxycholate
0.75-1.0 mg/kg daily or alternate day for 15 doses
3. Sodium Stibogluconate (SSG)
20mg/kg daily IM injection for 30 days
Note: In several phases, 3 studies done in India, three separate combinations showed 98-99% cure rate. The 2nd line of treatment including Amphotericin B Deoxycholate and Sodium Stibogluconate (SSG) are no longer used in NKEP of Bangladesh since the 1st line of treatment is found much more superior and effective.
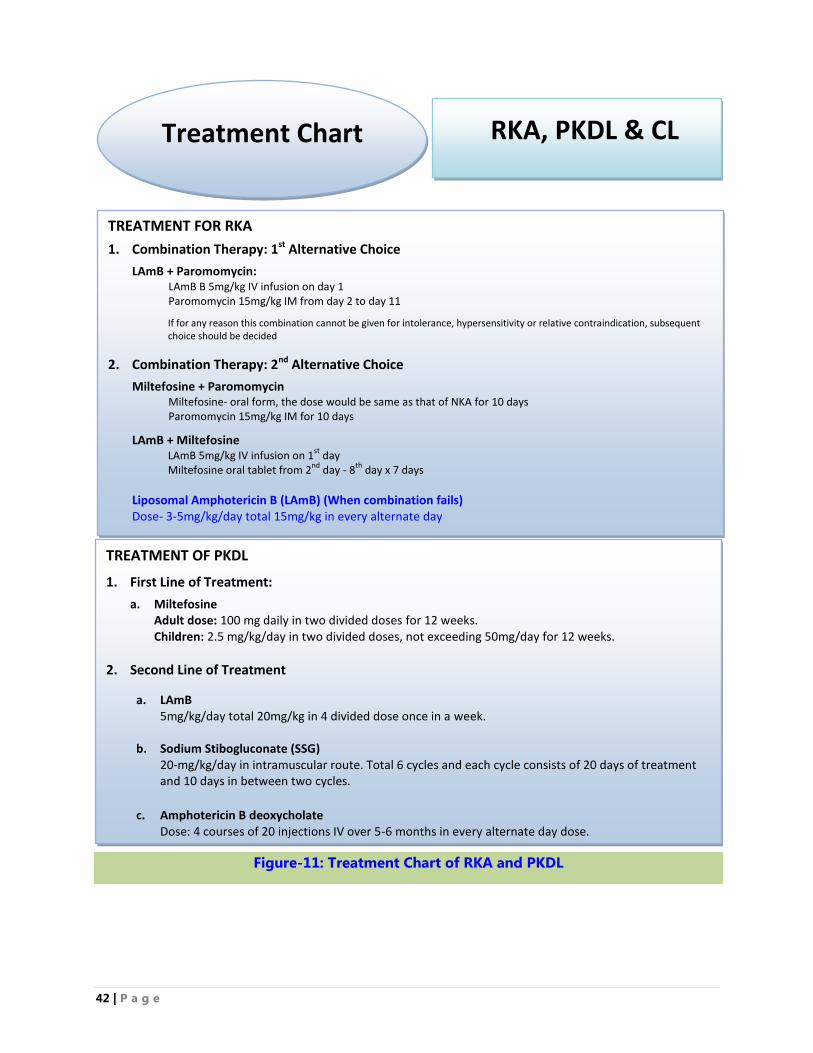
42 | P a g e
TREATMENT OF PKDL
1. First Line of Treatment:
a. Miltefosine Adult dose: 100 mg daily in two divided doses for 12 weeks. Children: 2.5 mg/kg/day in two divided doses, not exceeding 50mg/day for 12 weeks.
2. Second Line of Treatment
a. LAmB 5mg/kg/day total 20mg/kg in 4 divided dose once in a week.
b. Sodium Stibogluconate (SSG) 20-mg/kg/day in intramuscular route. Total 6 cycles and each cycle consists of 20 days of treatment and 10 days in between two cycles.
c. Amphotericin B deoxycholate
Dose: 4 courses of 20 injections IV over 5-6 months in every alternate day dose.
TREATMENT FOR RKA
1. Combination Therapy: 1st Alternative Choice
LAmB + Paromomycin: LAmB B 5mg/kg IV infusion on day 1 Paromomycin 15mg/kg IM from day 2 to day 11
If for any reason this combination cannot be given for intolerance, hypersensitivity or relative contraindication, subsequent choice should be decided
2. Combination Therapy: 2nd Alternative Choice a.
Miltefosine + Paromomycin Miltefosine- oral form, the dose would be same as that of NKA for 10 days Paromomycin 15mg/kg IM for 10 days
LAmB + Miltefosine LAmB 5mg/kg IV infusion on 1
st day
Miltefosine oral tablet from 2nd
day - 8th
day x 7 days
Liposomal Amphotericin B (LAmB) (When combination fails) Dose- 3-5mg/kg/day total 15mg/kg in every alternate day
Treatment Chart
RKA, PKDL & CL
Figure-11: Treatment Chart of RKA and PKDL
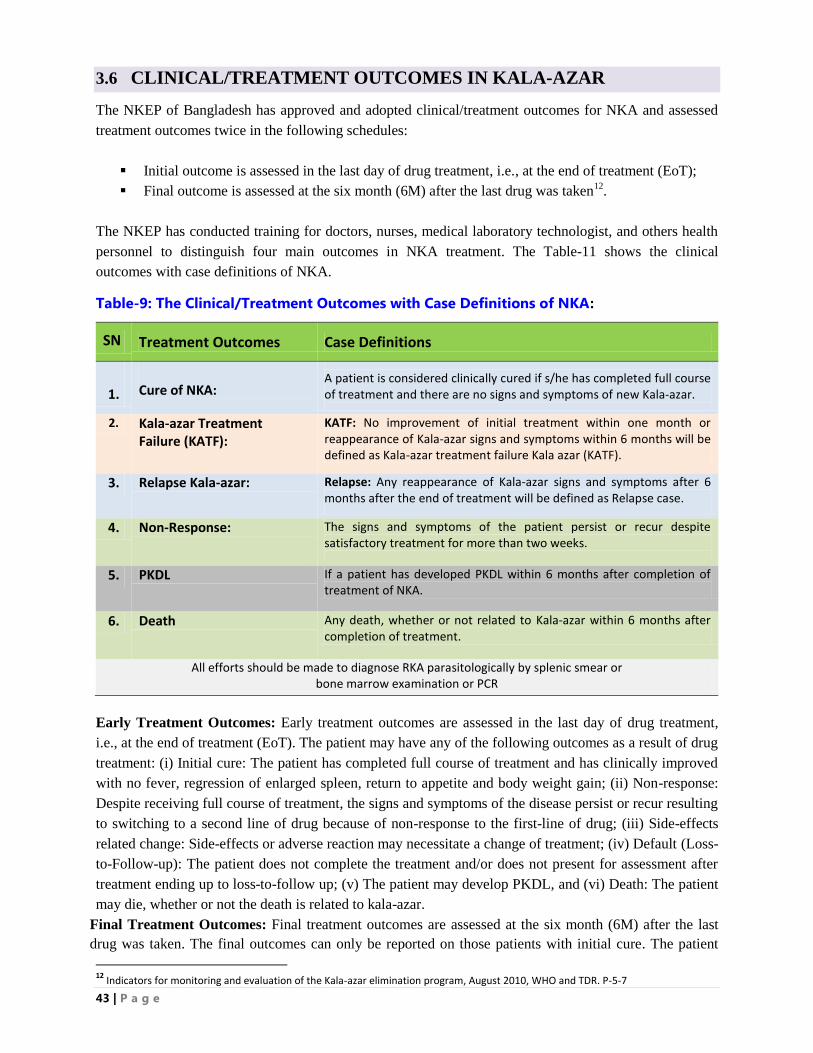
43 | P a g e
3.6 CLINICAL/TREATMENT OUTCOMES IN KALA-AZAR
The NKEP of Bangladesh has approved and adopted clinical/treatment outcomes for NKA and assessed
treatment outcomes twice in the following schedules:
Initial outcome is assessed in the last day of drug treatment, i.e., at the end of treatment (EoT);
Final outcome is assessed at the six month (6M) after the last drug was taken12
.
The NKEP has conducted training for doctors, nurses, medical laboratory technologist, and others health
personnel to distinguish four main outcomes in NKA treatment. The Table-11 shows the clinical
outcomes with case definitions of NKA.
Table-9: The Clinical/Treatment Outcomes with Case Definitions of NKA:
SN Treatment Outcomes Case Definitions
1.
Cure of NKA:
A patient is considered clinically cured if s/he has completed full course of treatment and there are no signs and symptoms of new Kala-azar.
2. Kala-azar Treatment Failure (KATF):
KATF: No improvement of initial treatment within one month or reappearance of Kala-azar signs and symptoms within 6 months will be defined as Kala-azar treatment failure Kala azar (KATF).
3. Relapse Kala-azar: Relapse: Any reappearance of Kala-azar signs and symptoms after 6 months after the end of treatment will be defined as Relapse case.
4. Non-Response: The signs and symptoms of the patient persist or recur despite satisfactory treatment for more than two weeks.
5. PKDL If a patient has developed PKDL within 6 months after completion of treatment of NKA.
6. Death Any death, whether or not related to Kala-azar within 6 months after completion of treatment.
All efforts should be made to diagnose RKA parasitologically by splenic smear or bone marrow examination or PCR
Early Treatment Outcomes: Early treatment outcomes are assessed in the last day of drug treatment,
i.e., at the end of treatment (EoT). The patient may have any of the following outcomes as a result of drug
treatment: (i) Initial cure: The patient has completed full course of treatment and has clinically improved
with no fever, regression of enlarged spleen, return to appetite and body weight gain; (ii) Non-response:
Despite receiving full course of treatment, the signs and symptoms of the disease persist or recur resulting
to switching to a second line of drug because of non-response to the first-line of drug; (iii) Side-effects
related change: Side-effects or adverse reaction may necessitate a change of treatment; (iv) Default (Loss-
to-Follow-up): The patient does not complete the treatment and/or does not present for assessment after
treatment ending up to loss-to-follow up; (v) The patient may develop PKDL, and (vi) Death: The patient
may die, whether or not the death is related to kala-azar.
Final Treatment Outcomes: Final treatment outcomes are assessed at the six month (6M) after the last
drug was taken. The final outcomes can only be reported on those patients with initial cure. The patient
12
Indicators for monitoring and evaluation of the Kala-azar elimination program, August 2010, WHO and TDR. P-5-7
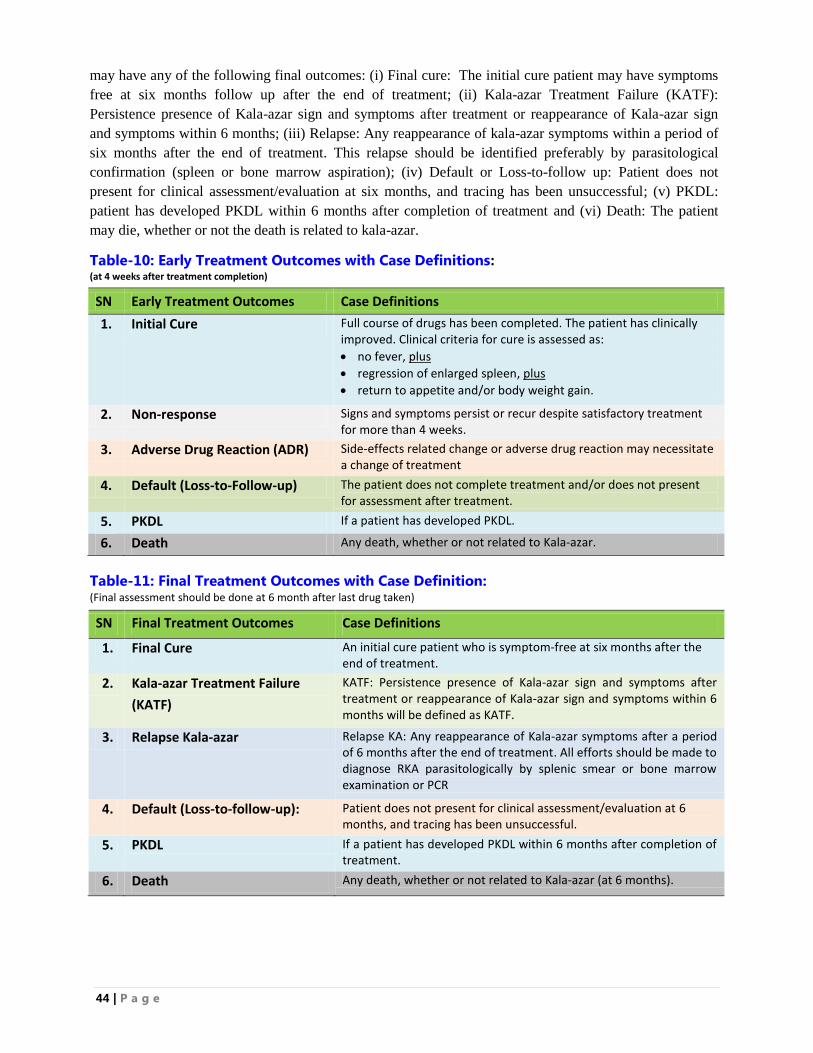
44 | P a g e
may have any of the following final outcomes: (i) Final cure: The initial cure patient may have symptoms
free at six months follow up after the end of treatment; (ii) Kala-azar Treatment Failure (KATF):
Persistence presence of Kala-azar sign and symptoms after treatment or reappearance of Kala-azar sign
and symptoms within 6 months; (iii) Relapse: Any reappearance of kala-azar symptoms within a period of
six months after the end of treatment. This relapse should be identified preferably by parasitological
confirmation (spleen or bone marrow aspiration); (iv) Default or Loss-to-follow up: Patient does not
present for clinical assessment/evaluation at six months, and tracing has been unsuccessful; (v) PKDL:
patient has developed PKDL within 6 months after completion of treatment and (vi) Death: The patient
may die, whether or not the death is related to kala-azar.
Table-10: Early Treatment Outcomes with Case Definitions: (at 4 weeks after treatment completion)
SN Early Treatment Outcomes Case Definitions
1. Initial Cure Full course of drugs has been completed. The patient has clinically improved. Clinical criteria for cure is assessed as:
no fever, plus
regression of enlarged spleen, plus
return to appetite and/or body weight gain.
2. Non-response Signs and symptoms persist or recur despite satisfactory treatment for more than 4 weeks.
3. Adverse Drug Reaction (ADR) Side-effects related change or adverse drug reaction may necessitate a change of treatment
4. Default (Loss-to-Follow-up) The patient does not complete treatment and/or does not present for assessment after treatment.
5. PKDL If a patient has developed PKDL.
6. Death Any death, whether or not related to Kala-azar.
Table-11: Final Treatment Outcomes with Case Definition: (Final assessment should be done at 6 month after last drug taken)
SN Final Treatment Outcomes Case Definitions
1. Final Cure An initial cure patient who is symptom-free at six months after the end of treatment.
2. Kala-azar Treatment Failure
(KATF)
KATF: Persistence presence of Kala-azar sign and symptoms after treatment or reappearance of Kala-azar sign and symptoms within 6 months will be defined as KATF.
3. Relapse Kala-azar Relapse KA: Any reappearance of Kala-azar symptoms after a period of 6 months after the end of treatment. All efforts should be made to diagnose RKA parasitologically by splenic smear or bone marrow examination or PCR
4. Default (Loss-to-follow-up): Patient does not present for clinical assessment/evaluation at 6 months, and tracing has been unsuccessful.
5. PKDL If a patient has developed PKDL within 6 months after completion of treatment.
6. Death Any death, whether or not related to Kala-azar (at 6 months).
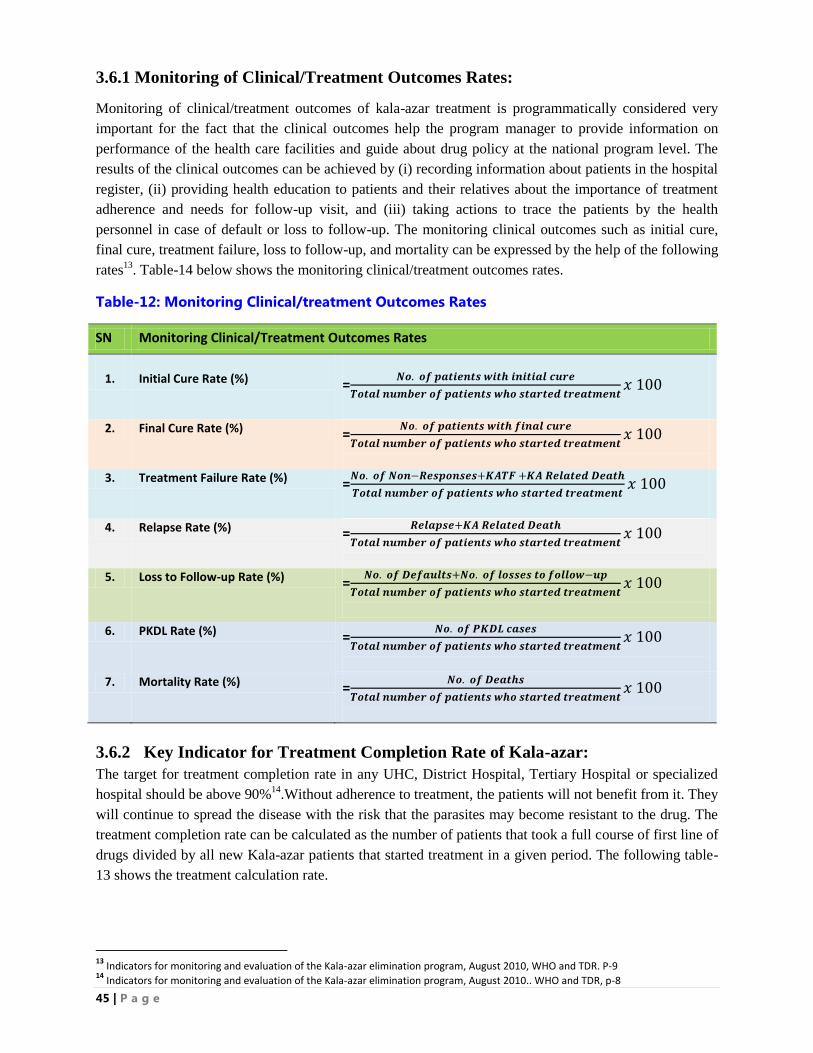
45 | P a g e
3.6.1 Monitoring of Clinical/Treatment Outcomes Rates:
Monitoring of clinical/treatment outcomes of kala-azar treatment is programmatically considered very
important for the fact that the clinical outcomes help the program manager to provide information on
performance of the health care facilities and guide about drug policy at the national program level. The
results of the clinical outcomes can be achieved by (i) recording information about patients in the hospital
register, (ii) providing health education to patients and their relatives about the importance of treatment
adherence and needs for follow-up visit, and (iii) taking actions to trace the patients by the health
personnel in case of default or loss to follow-up. The monitoring clinical outcomes such as initial cure,
final cure, treatment failure, loss to follow-up, and mortality can be expressed by the help of the following
rates13
. Table-14 below shows the monitoring clinical/treatment outcomes rates.
Table-12: Monitoring Clinical/treatment Outcomes Rates
SN Monitoring Clinical/Treatment Outcomes Rates
1.
Initial Cure Rate (%)
=𝑵𝒐. 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒊𝒕𝒉 𝒊𝒏𝒊𝒕𝒊𝒂𝒍 𝒄𝒖𝒓𝒆
𝑻𝒐𝒕𝒂𝒍 𝒏𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒉𝒐 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕𝑥 100
2. Final Cure Rate (%) =𝑵𝒐. 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒊𝒕𝒉 𝒇𝒊𝒏𝒂𝒍 𝒄𝒖𝒓𝒆
𝑻𝒐𝒕𝒂𝒍 𝒏𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒉𝒐 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕𝑥 100
3. Treatment Failure Rate (%) =𝑵𝒐. 𝒐𝒇 𝑵𝒐𝒏−𝑹𝒆𝒔𝒑𝒐𝒏𝒔𝒆𝒔+𝑲𝑨𝑻𝑭 +𝑲𝑨 𝑹𝒆𝒍𝒂𝒕𝒆𝒅 𝑫𝒆𝒂𝒕𝒉
𝑻𝒐𝒕𝒂𝒍 𝒏𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒉𝒐 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕𝑥 100
4. Relapse Rate (%) =𝑹𝒆𝒍𝒂𝒑𝒔𝒆+𝑲𝑨 𝑹𝒆𝒍𝒂𝒕𝒆𝒅 𝑫𝒆𝒂𝒕𝒉
𝑻𝒐𝒕𝒂𝒍 𝒏𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒉𝒐 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕𝑥 100
5. Loss to Follow-up Rate (%) =𝑵𝒐. 𝒐𝒇 𝑫𝒆𝒇𝒂𝒖𝒍𝒕𝒔+𝑵𝒐. 𝒐𝒇 𝒍𝒐𝒔𝒔𝒆𝒔 𝒕𝒐 𝒇𝒐𝒍𝒍𝒐𝒘−𝒖𝒑
𝑻𝒐𝒕𝒂𝒍 𝒏𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒉𝒐 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕𝑥 100
6. PKDL Rate (%) =𝑵𝒐. 𝒐𝒇 𝑷𝑲𝑫𝑳 𝒄𝒂𝒔𝒆𝒔
𝑻𝒐𝒕𝒂𝒍 𝒏𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒉𝒐 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕𝑥 100
7. Mortality Rate (%) =𝑵𝒐. 𝒐𝒇 𝑫𝒆𝒂𝒕𝒉𝒔
𝑻𝒐𝒕𝒂𝒍 𝒏𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒘𝒉𝒐 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕𝑥 100
3.6.2 Key Indicator for Treatment Completion Rate of Kala-azar:
The target for treatment completion rate in any UHC, District Hospital, Tertiary Hospital or specialized
hospital should be above 90%14
.Without adherence to treatment, the patients will not benefit from it. They
will continue to spread the disease with the risk that the parasites may become resistant to the drug. The
treatment completion rate can be calculated as the number of patients that took a full course of first line of
drugs divided by all new Kala-azar patients that started treatment in a given period. The following table-
13 shows the treatment calculation rate.
13
Indicators for monitoring and evaluation of the Kala-azar elimination program, August 2010, WHO and TDR. P-9 14
Indicators for monitoring and evaluation of the Kala-azar elimination program, August 2010.. WHO and TDR, p-8
46 | P a g e
Table-13: Treatment Completion Rates
Treatment Completion Rate (%)
Treatment Completion Rate (%):
=𝑵𝒖𝒎𝒃𝒆𝒓 𝒐𝒇 𝒑𝒂𝒕𝒊𝒆𝒏𝒕𝒔 𝒕𝒉𝒂𝒕 𝒕𝒐𝒐𝒌 𝒂 𝒇𝒖𝒍𝒍 𝒄𝒐𝒖𝒓𝒔𝒆 𝒐𝒇 𝒇𝒊𝒓𝒔𝒕 𝒍𝒊𝒏𝒆 𝒅𝒓𝒖𝒈𝒔
𝑨𝒍𝒍 𝒏𝒆𝒘 𝑲𝑨 𝒄𝒂𝒔𝒆𝒔 𝒕𝒉𝒂𝒕 𝒔𝒕𝒂𝒓𝒕𝒆𝒅 𝒕𝒓𝒆𝒂𝒕𝒎𝒆𝒏𝒕 𝒊𝒏 𝒂 𝒈𝒊𝒗𝒆𝒏 𝒑𝒆𝒓𝒊𝒐𝒅 (𝒀𝑹)𝑥 𝟏𝟎𝟎
3.6.3 Monitoring of Clinical/Treatment Outcomes Variables:
In order to be able calculate the monitoring of treatment outcomes rates such as initial cure rate, final cure
rate, treatment failure rate, loss-to-follow-up rate, mortality rate, treatment completion rate, case detection
rate, and coverage rate of vector control in Kala-azar endemic areas within a given period of time (usually
in one quarter and one year), the NKEP should plan and design the functional strategy with annual action
plan and budget well ahead of time, develop appropriate forms and register book, and train the health
personnel how to fill-up the register book and different monitoring forms with an accuracy so that the all
relevant data flow from the UHC, hospitals and specialized centre to the NKEP, CDC- Dhaka. The annex-
9 shows monitoring clinical/treatment outcomes variables with starting and evaluation treatment.
3.6.4 The Clinical/Treatment Outcomes of PKDL:
Treatment outcomes in PKDL are also clinically assessed at primary health care level. The UHC facilities
should have the clinical capacity to resolve at least 80% cases of macules and/or a decrease in erythema
and flattening of lesions. These cases should be followed up in accordance with 4 follow up visit
schedules and among them 2 visits will be done for initial cure and final cure assessment:
1st visit: Immediately after completion of treatment
2nd
visit: 3 months after completion of treatment
3rd
visit: 6 months after completion of treatment
4th visit: 12 months after completion of treatment
The Treatment Outcomes of PKDL are shown in the table-14 as follows:
Table-14: Treatment Outcomes in PKDL Patients
SN Treatment Outcomes Case Definitions of PKDL
1. Initial Cure: Clinical improvement at the end of treatment that defined as a considerable reduction in the number and size of skin lesions in PKDL cases.
2. Final Cure: Clinical cure at 12 months after the end of treatment that defined as a complete resolution of macules, papules, plaques and nodules.
3. Partial Response More than 50% reduction in skin lesions (number and/or size of lesions) at one year only (on examination and/or as per patients statement)
4. PKDL Treatment Failure Less than 50% reduction in skin lesions (number and/or size of lesions) at one year only (on examination and/or as per patients statement)
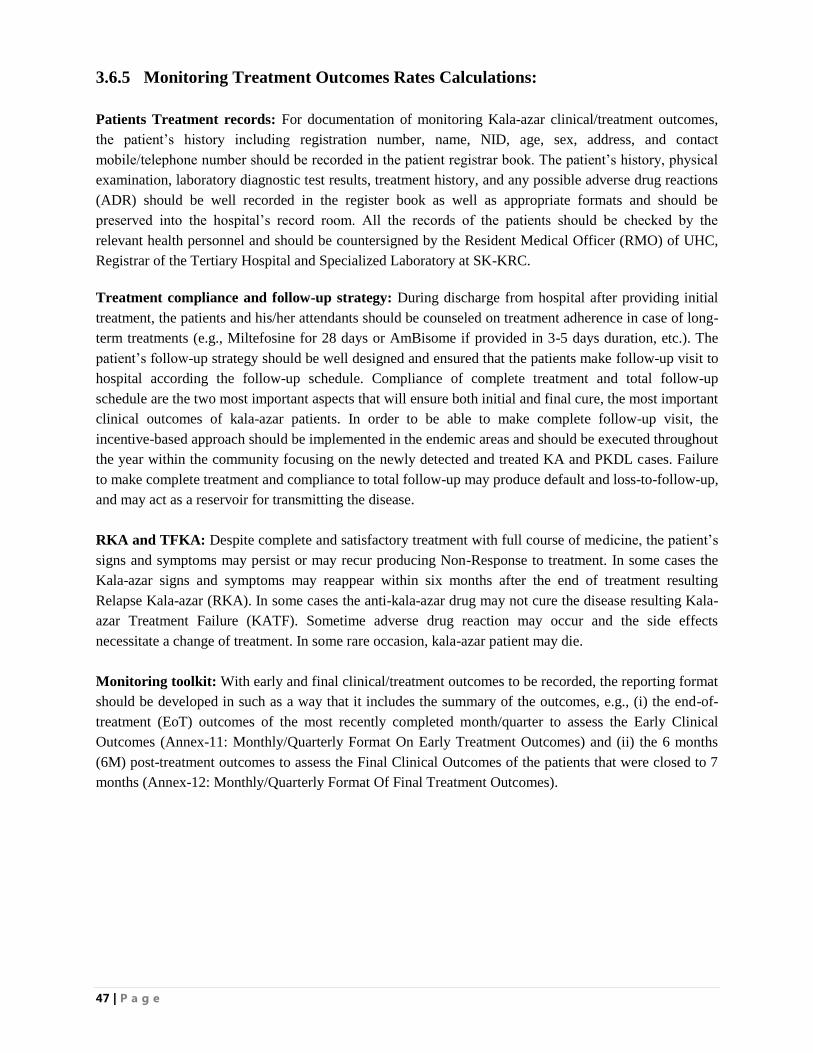
47 | P a g e
3.6.5 Monitoring Treatment Outcomes Rates Calculations:
Patients Treatment records: For documentation of monitoring Kala-azar clinical/treatment outcomes,
the patient‟s history including registration number, name, NID, age, sex, address, and contact
mobile/telephone number should be recorded in the patient registrar book. The patient‟s history, physical
examination, laboratory diagnostic test results, treatment history, and any possible adverse drug reactions
(ADR) should be well recorded in the register book as well as appropriate formats and should be
preserved into the hospital‟s record room. All the records of the patients should be checked by the
relevant health personnel and should be countersigned by the Resident Medical Officer (RMO) of UHC,
Registrar of the Tertiary Hospital and Specialized Laboratory at SK-KRC.
Treatment compliance and follow-up strategy: During discharge from hospital after providing initial
treatment, the patients and his/her attendants should be counseled on treatment adherence in case of long-
term treatments (e.g., Miltefosine for 28 days or AmBisome if provided in 3-5 days duration, etc.). The
patient‟s follow-up strategy should be well designed and ensured that the patients make follow-up visit to
hospital according the follow-up schedule. Compliance of complete treatment and total follow-up
schedule are the two most important aspects that will ensure both initial and final cure, the most important
clinical outcomes of kala-azar patients. In order to be able to make complete follow-up visit, the
incentive-based approach should be implemented in the endemic areas and should be executed throughout
the year within the community focusing on the newly detected and treated KA and PKDL cases. Failure
to make complete treatment and compliance to total follow-up may produce default and loss-to-follow-up,
and may act as a reservoir for transmitting the disease.
RKA and TFKA: Despite complete and satisfactory treatment with full course of medicine, the patient‟s
signs and symptoms may persist or may recur producing Non-Response to treatment. In some cases the
Kala-azar signs and symptoms may reappear within six months after the end of treatment resulting
Relapse Kala-azar (RKA). In some cases the anti-kala-azar drug may not cure the disease resulting Kala-
azar Treatment Failure (KATF). Sometime adverse drug reaction may occur and the side effects
necessitate a change of treatment. In some rare occasion, kala-azar patient may die.
Monitoring toolkit: With early and final clinical/treatment outcomes to be recorded, the reporting format
should be developed in such as a way that it includes the summary of the outcomes, e.g., (i) the end-of-
treatment (EoT) outcomes of the most recently completed month/quarter to assess the Early Clinical
Outcomes (Annex-11: Monthly/Quarterly Format On Early Treatment Outcomes) and (ii) the 6 months
(6M) post-treatment outcomes to assess the Final Clinical Outcomes of the patients that were closed to 7
months (Annex-12: Monthly/Quarterly Format Of Final Treatment Outcomes).
48 | P a g e
3.7 PHARMACOVIGILANCE ACTIVITIES:
3.7.1 Operational Plan for Pharmacovigilance Activities: The NKEP of Bangladesh has developed a guideline titled: “Operational Plan for Pharmacovigilance
Activities for Visceral Leishmaniasis in Bangladesh” and implemented the plan since September 2014
(25). The objective of the operational plan is to detect, assess, understand, document and prevent adverse
drug reaction (ADR) of the various regimens used to treat kala-azar patients and to improve the clinical
and treatment outcomes. The operational plan recommends the collection of safety and ADR of the drugs
such as Liposomal Amphotericin B, Miltefosine, Paromomycin, and Amphotericin B deoxycholate used
to treat kala-azar patients. The serious adverse events due to drug reactions may result in death, life
threatening or risk of dying, require inpatient hospitalization or prolongation of hospitalization, result in
persistent or significant disability or incapacity, and cause congenital anomaly or birth defect.
The scope of the operational plan is to orient and educate all healthcare professionals engaged with
diagnosis and treatment of Primary Kala-azar (PKA) and Post Kala azar Dermal Leishmaniasis (PKDL).
The followings are broad functions of pharmacovigilance articulated in operational plan such as:
detection and study of adverse reactions; measurement of risk; measurement of effectiveness; benefit and
harm evaluation; dissemination of information; education; early warning; and rational and safe use of
medicines. The functions of pharmacovigilance is also applicable to those dispensing drugs for kala-azar
patients, providing nursing care to such patients or other personnel directly involved in the collection and
analysis of adverse drug reaction data.
Kala-azar Elimination Program (KEP) in collaboration with icddr,b Dhaka, conducted training on
“Pharmacovigilance Activities for Kala-azar in Bangladesh” in two phases (first phase: 18-19 October
2014 and second phase: 14-15 November 2014). A total of 230 health care professionals (Doctors-78,
Nurses-73 and Statisticians-79) from 80 endemic upazilas of 26 districts received training on
pharmacovigilance activities. Health care professionals are expected to monitor for signs and symptoms
indicative of adverse drug reactions, and record promptly in the treatment sheet. Senior Staff Nurse (SSN)
of each UHC and other health facilities is the focal point person responsible to fill up the ADR Form and
the Doctor/RMO will check and sign the form and send it to KEP and icddr,b Dhaka Office on a monthly
basis (Annex: ADR Form). A soft copy should also be sent to icddr,b Dhaka Office. Sending report on a
monthly basis is applicable to non-fatal cases only. However, for fatal cases, the ADR report should be
sent to icddr,b Dhaka Office within seven days.
Analysis of the reported ADR information: The ADR data collected at KEP will be shared with the
Directorate General of Drug Administration (DGDA), Government of Bangladesh. Data Quality will be
checked and medically evaluated and causality will be assessed according to the WHO-UMC causality
assessment algorithm (Annex: WHO-UMC Causality Assessment Algorithm). The data are analyzed for
signals or alerts. Based on the data processing and analysis, appropriate recommendations and risk
mitigation plans will be developed and communicated to the relevant stakeholders. An expert committee
at KEP, Dhaka will review the data and generate information on a half yearly basis and make
recommendations to kala-azar elimination program.
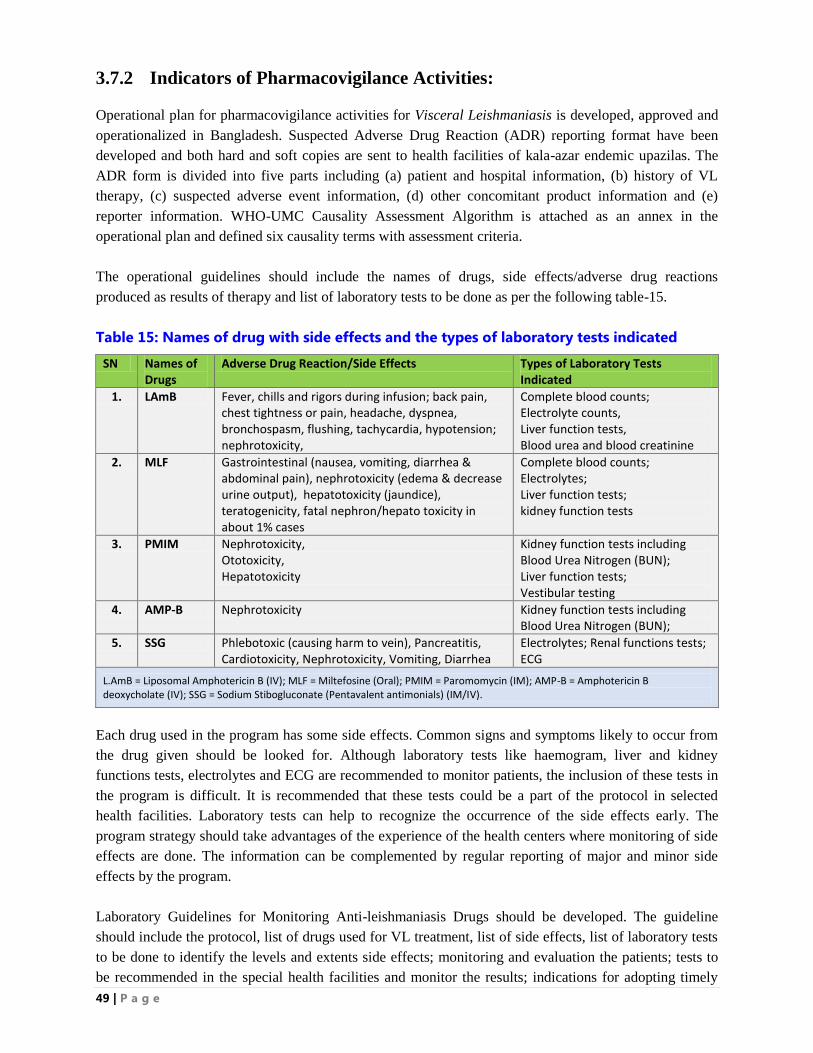
49 | P a g e
3.7.2 Indicators of Pharmacovigilance Activities: Operational plan for pharmacovigilance activities for Visceral Leishmaniasis is developed, approved and
operationalized in Bangladesh. Suspected Adverse Drug Reaction (ADR) reporting format have been
developed and both hard and soft copies are sent to health facilities of kala-azar endemic upazilas. The
ADR form is divided into five parts including (a) patient and hospital information, (b) history of VL
therapy, (c) suspected adverse event information, (d) other concomitant product information and (e)
reporter information. WHO-UMC Causality Assessment Algorithm is attached as an annex in the
operational plan and defined six causality terms with assessment criteria.
The operational guidelines should include the names of drugs, side effects/adverse drug reactions
produced as results of therapy and list of laboratory tests to be done as per the following table-15.
Table 15: Names of drug with side effects and the types of laboratory tests indicated
SN Names of Drugs
Adverse Drug Reaction/Side Effects Types of Laboratory Tests Indicated
1. LAmB Fever, chills and rigors during infusion; back pain, chest tightness or pain, headache, dyspnea, bronchospasm, flushing, tachycardia, hypotension; nephrotoxicity,
Complete blood counts; Electrolyte counts, Liver function tests, Blood urea and blood creatinine
2. MLF Gastrointestinal (nausea, vomiting, diarrhea & abdominal pain), nephrotoxicity (edema & decrease urine output), hepatotoxicity (jaundice), teratogenicity, fatal nephron/hepato toxicity in about 1% cases
Complete blood counts; Electrolytes; Liver function tests; kidney function tests
3. PMIM Nephrotoxicity, Ototoxicity, Hepatotoxicity
Kidney function tests including Blood Urea Nitrogen (BUN); Liver function tests; Vestibular testing
4. AMP-B Nephrotoxicity Kidney function tests including Blood Urea Nitrogen (BUN);
5. SSG Phlebotoxic (causing harm to vein), Pancreatitis, Cardiotoxicity, Nephrotoxicity, Vomiting, Diarrhea
Electrolytes; Renal functions tests; ECG
L.AmB = Liposomal Amphotericin B (IV); MLF = Miltefosine (Oral); PMIM = Paromomycin (IM); AMP-B = Amphotericin B deoxycholate (IV); SSG = Sodium Stibogluconate (Pentavalent antimonials) (IM/IV).
Each drug used in the program has some side effects. Common signs and symptoms likely to occur from
the drug given should be looked for. Although laboratory tests like haemogram, liver and kidney
functions tests, electrolytes and ECG are recommended to monitor patients, the inclusion of these tests in
the program is difficult. It is recommended that these tests could be a part of the protocol in selected
health facilities. Laboratory tests can help to recognize the occurrence of the side effects early. The
program strategy should take advantages of the experience of the health centers where monitoring of side
effects are done. The information can be complemented by regular reporting of major and minor side
effects by the program.
Laboratory Guidelines for Monitoring Anti-leishmaniasis Drugs should be developed. The guideline
should include the protocol, list of drugs used for VL treatment, list of side effects, list of laboratory tests
to be done to identify the levels and extents side effects; monitoring and evaluation the patients; tests to
be recommended in the special health facilities and monitor the results; indications for adopting timely
50 | P a g e
measures even before the signs appear; revision of reports of major and minor side effects obtained from
UHC; regular reporting the side effects on the ADR Reporting Forms to be sent to icddr,b Dhaka Office
once in a month for review and feedback. This will help guide the program in recommending tests that
should be done to monitor the patients on treatment. The Annex-13 shows the indicators for
monitoring pharmacovigilance activities.
51 | P a g e
CHAPTER: FOUR
KALA-AZAR SURVEILLANCE SYSTEM
52 | P a g e
4. KALA-AZAR SURVEILLANCE SYSTEM
4.1 INTRODUCTION TO SURVEILLANCE
Bangladesh, an endemic country, is committed to eliminate Kala-azar and the country has declared Kala-
azar as a reportable disease. It is therefore mandatory for every health facility including upazila health
complexes, clinic/hospitals to report kala-azar cases to Diseases Control Unit (CDC), Directorate General
of Health Services (DGHS) of the Ministry of Health and Family Welfare (MoHFW). Since the disease
surveillance is mandated by the Government of Bangladesh and since the reporting of cases of kala-azar
is required by rules and regulation, the disease surveillance system should be far more complete.
Therefore, it is important to improve and strengthen disease surveillance system and data management
skills at program level.
Kala-azar disease surveillance is an information-based activity involving the systematic collection,
analysis and interpretation of outcome-specific data originating from a variety of sources such as
community, upazila health facilities, and secondary and tertiary health facilities. The information collated
is then used in a number of ways as follows: (i) to evaluate the effectiveness of health measures for kala-
azar prevention, control and elimination program, (ii) to monitor changes in kala-azar agents including the
trends in development of anti-kala-azar drug resistance, (iii) to support national kala-azar elimination
strategic plan and the allocation of appropriate resources within the healthcare system, (iv) identify high
risk populations or areas to target interventions, and (v) provide a valuable archive of disease activity for
future reference. To be effective, the collection of kala-azar surveillance data must be standardized on a
national basis and be made available at local, regional and national level.
The main role of kala-azar disease surveillance is to predict, observe, and minimize the harm caused by
outbreak, epidemic, and pandemic situations, as well as increase knowledge about which factors
contribute to such circumstances. A key part of modern kala-azar disease surveillance is the practice of
disease case reporting.
Kala-azar Surveillance System Components: The components of a kala-azar surveillance system
include:
1. Health facilities such as upazila health complexes, clinics and/or hospitals for the collection of primary data,
for example the number of NKA and PKDL cases, based on established case definitions and structured
reporting formats (paper and/or electronic);
2. Standard methods and frequencies of reporting, collating and monitoring of kala-azar disease as whole;
3. Description and definition of activities and initiates for public health actions, for example the number of NKA
cases within an endemic area that triggers an outbreak investigation (i.e., Index case search, No Kala-azar
Transmission Activities and/or indoor residual spraying);
4. Continuous monitoring and evaluation of the system for timeliness and effectiveness; and
5. Regular analysis of collated data for trends over time and space.
The kala-azar surveillance system is unlikely to capture all the cases of kala-azar and therefore, it is
essential to evaluate differences in reporting over time and between surveillance sites for interpretation of
data. In the design of such a system, evaluation is greatly facilitated by the use of indicators of
effectiveness, which are collated and monitored as part of surveillance. Surveillance data should also be
collated from the private health sector and non-governmental organizations. A surveillance protocol or
53 | P a g e
guidelines should be designed for monitoring the burden of Kala-azar and trends in Kala-azar co-
infections and for evaluating the effectiveness of control measures.
Kala-azar Surveillance System comprises of passive case surveillance and active case detection of cases
and vector surveillance. Passive case surveillance includes reporting of all cases of New Kala-azar (NKA)
and PKDL (Web-based Patient Registration). To make the disease surveillance effective, it is necessary to
organize a method of systemic surveillance activity, regular reporting, and analysis of data, review,
feedback and dissemination of information. Regular reporting and exchange information should be
organized upwards, downwards and laterally in the system that comprises government, private sector,
NGOs and the community as partners. Feedback linked to surveillance system is a critical element of the
kala-azar elimination program. Surveillance of the disease should also be used for sharing of reports
periodically to higher authorities on a regular basis to facilitate and rationalize the planning of elimination
program. Surveillance is useful for planning indoor residual spray of the endemic areas to be sprayed and
in monitoring the trends of kala-azar.
4.2 TYPES OF KALA-AZAR SURVEILLANCE
4.2.1 Passive Case Surveillance
Passive case surveillance of kala-azar includes reporting of cases of New Kala-azar (NKA) and Post
Kala-azar Dermal Leishmaniasis (PKDL). The passive surveillance is the basic foundation of the kala-
azar elimination program. The National Kala-azar Elimination Program (NKEP) has started with
reporting of cases, who seek diagnosis and treatment of kala-azar from a level of upazila health
complexes, tertiary hospitals and specialized hospitals in the government health facilities since beginning
from its implementation. However, the passive surveillance of NKEP does not provide real time true
picture since (i) a portion of kala-azar cases visit private doctors including Homeopathic, Unani and other
unqualified practitioners as there is no reporting of cases from these health care providers; (ii)
asymptomatic cases of kala-azar remains undiagnosed and untreated, and act as continuous foci of
transmission of disease; (iii) treatment is often started without a definitive diagnosis of kala-azar specially
by the unqualified doctors; and (iii) many cases do not seek health care at all because of poverty and
socio-cultural conditions.
Despite the variety of information needs, many elements of data collected in surveillance are very similar
and the data source is often the same individual or facility. However, there may be differences in: (i) the
specific case detection method used (passive vs. active case detection); (ii) the speed at which data need
to flow through the system (routine vs. immediate); (iii) the rapidity of response required (immediate
investigation of cases or clusters of cases vs. analysis of data on a regular basis with subsequent
adjustments to a control program). For the surveillance system to function as an early warning system,
reporting, confirmation, decision-making and response must be rapid. On the other hand, for kala-azar
endemic disease, the aim may be to carefully consider data collected in order to adjust or target the
control program. The national surveillance system should therefore be able to accommodate both needs,
and will require two-speed reporting mechanisms.
The NKEP has improved over the period of times, the capacity has increased, and the passive case
detection at the health facilities in the endemic areas has improved. Passive surveillance has been done on
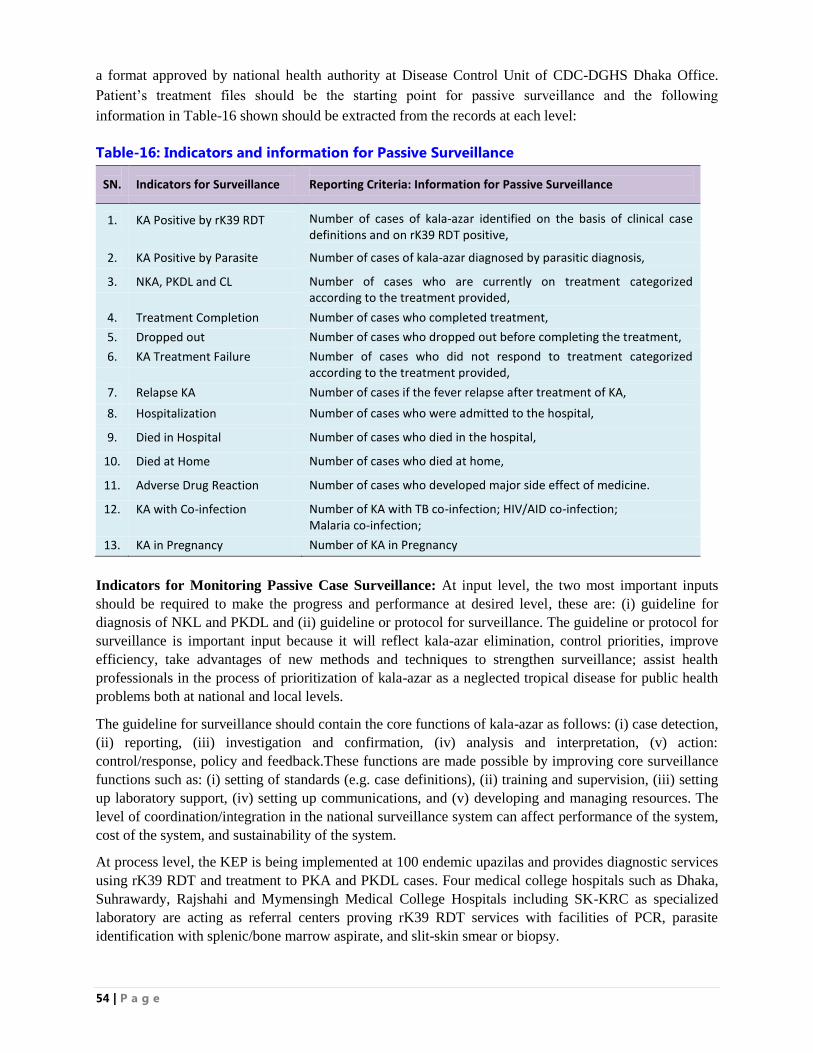
54 | P a g e
a format approved by national health authority at Disease Control Unit of CDC-DGHS Dhaka Office.
Patient‟s treatment files should be the starting point for passive surveillance and the following
information in Table-16 shown should be extracted from the records at each level:
Table-16: Indicators and information for Passive Surveillance
SN.
Indicators for Surveillance
Reporting Criteria: Information for Passive Surveillance
1.
KA Positive by rK39 RDT
Number of cases of kala-azar identified on the basis of clinical case definitions and on rK39 RDT positive,
2. KA Positive by Parasite Number of cases of kala-azar diagnosed by parasitic diagnosis,
3. NKA, PKDL and CL Number of cases who are currently on treatment categorized according to the treatment provided,
4. Treatment Completion Number of cases who completed treatment,
5. Dropped out Number of cases who dropped out before completing the treatment,
6. KA Treatment Failure Number of cases who did not respond to treatment categorized according to the treatment provided,
7. Relapse KA Number of cases if the fever relapse after treatment of KA,
8. Hospitalization Number of cases who were admitted to the hospital,
9. Died in Hospital Number of cases who died in the hospital,
10. Died at Home Number of cases who died at home,
11. Adverse Drug Reaction Number of cases who developed major side effect of medicine.
12. KA with Co-infection Number of KA with TB co-infection; HIV/AID co-infection; Malaria co-infection;
13. KA in Pregnancy Number of KA in Pregnancy
Indicators for Monitoring Passive Case Surveillance: At input level, the two most important inputs
should be required to make the progress and performance at desired level, these are: (i) guideline for
diagnosis of NKL and PKDL and (ii) guideline or protocol for surveillance. The guideline or protocol for
surveillance is important input because it will reflect kala-azar elimination, control priorities, improve
efficiency, take advantages of new methods and techniques to strengthen surveillance; assist health
professionals in the process of prioritization of kala-azar as a neglected tropical disease for public health
problems both at national and local levels.
The guideline for surveillance should contain the core functions of kala-azar as follows: (i) case detection,
(ii) reporting, (iii) investigation and confirmation, (iv) analysis and interpretation, (v) action:
control/response, policy and feedback.These functions are made possible by improving core surveillance
functions such as: (i) setting of standards (e.g. case definitions), (ii) training and supervision, (iii) setting
up laboratory support, (iv) setting up communications, and (v) developing and managing resources. The
level of coordination/integration in the national surveillance system can affect performance of the system,
cost of the system, and sustainability of the system.
At process level, the KEP is being implemented at 100 endemic upazilas and provides diagnostic services
using rK39 RDT and treatment to PKA and PKDL cases. Four medical college hospitals such as Dhaka,
Suhrawardy, Rajshahi and Mymensingh Medical College Hospitals including SK-KRC as specialized
laboratory are acting as referral centers proving rK39 RDT services with facilities of PCR, parasite
identification with splenic/bone marrow aspirate, and slit-skin smear or biopsy.
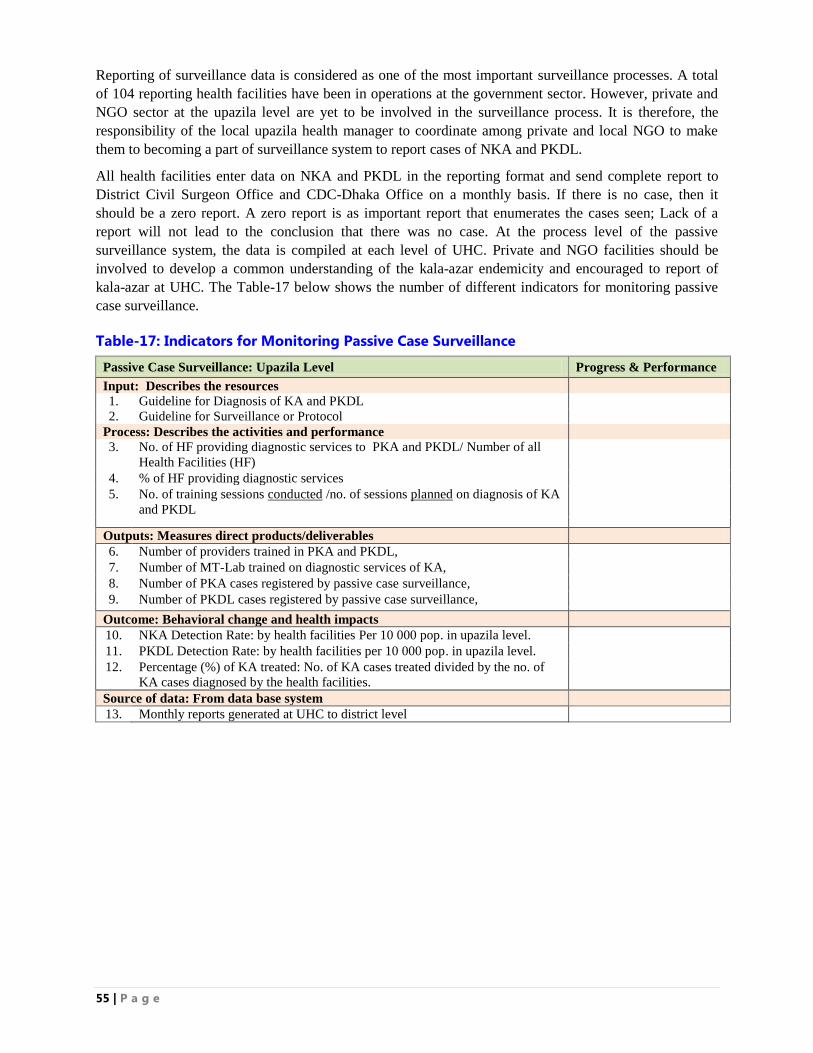
55 | P a g e
Reporting of surveillance data is considered as one of the most important surveillance processes. A total
of 104 reporting health facilities have been in operations at the government sector. However, private and
NGO sector at the upazila level are yet to be involved in the surveillance process. It is therefore, the
responsibility of the local upazila health manager to coordinate among private and local NGO to make
them to becoming a part of surveillance system to report cases of NKA and PKDL.
All health facilities enter data on NKA and PKDL in the reporting format and send complete report to
District Civil Surgeon Office and CDC-Dhaka Office on a monthly basis. If there is no case, then it
should be a zero report. A zero report is as important report that enumerates the cases seen; Lack of a
report will not lead to the conclusion that there was no case. At the process level of the passive
surveillance system, the data is compiled at each level of UHC. Private and NGO facilities should be
involved to develop a common understanding of the kala-azar endemicity and encouraged to report of
kala-azar at UHC. The Table-17 below shows the number of different indicators for monitoring passive
case surveillance.
Table-17: Indicators for Monitoring Passive Case Surveillance
Passive Case Surveillance: Upazila Level Progress & Performance
Input: Describes the resources
1. Guideline for Diagnosis of KA and PKDL
2. Guideline for Surveillance or Protocol
Process: Describes the activities and performance
3. No. of HF providing diagnostic services to PKA and PKDL/ Number of all
Health Facilities (HF)
4. % of HF providing diagnostic services
5. No. of training sessions conducted /no. of sessions planned on diagnosis of KA
and PKDL
Outputs: Measures direct products/deliverables
6. Number of providers trained in PKA and PKDL,
7. Number of MT-Lab trained on diagnostic services of KA,
8. Number of PKA cases registered by passive case surveillance,
9. Number of PKDL cases registered by passive case surveillance,
Outcome: Behavioral change and health impacts
10. NKA Detection Rate: by health facilities Per 10 000 pop. in upazila level.
11. PKDL Detection Rate: by health facilities per 10 000 pop. in upazila level.
12. Percentage (%) of KA treated: No. of KA cases treated divided by the no. of
KA cases diagnosed by the health facilities.
Source of data: From data base system
13. Monthly reports generated at UHC to district level
56 | P a g e
i. Active Case Surveillance
Active disease surveillance plays a more dynamic role in data gathering in kala-azar elimination program.
The active case detection is more resource intensive and is usually done in association with passive
surveillance. The basic principle and criteria of any disease elimination program is to have a robust active
case detection system that will contribute to early diagnosis and complete treatment of kala-azar cases.
Moreover, active case detection is recognized as one of the most important indicators for monitoring kala-
azar elimination activities at village/union level.
Four approaches of active case detection (ACD) have been validated for its utility in NKA and PKDL
case detection. These are Blanket Approach, Camp Based Approach, Index Based Approach, and
Incentive Based Approach.
4.2.2.1 Blanket Approach: In blanket approach, the trained health workers make house-to-house visit in
the entire endemic areas for the detection of NKA and PKDL cases; The blanket approach is considered
the „gold standarnd‟, but due to the additional high cost incurred with this method, it is only
recommended in outbreak situations.
4.2.2.2 Camp Based Approach: The camp approach is done by organizing health camp in defined kala-
azar endemic areas where screening of kala-azar is done by mobile health teams of medical officers,
nurses, lab technician, health inspectors, assistant health inspectors, health workers and health volunteers;
The camp based approach is a sensitive tool for the detection of new kala-azar and PKDL cases
particularly in high KA endemic areas.
4.2.2.3 Index Case-based Approach: The index case-based approach includes the search of kala-azar
cases among the households members through house-to-house search around a house (radius of 50 meters
or 100 HHs were searched) of a recently diagnosed cases of kala-azar usually in the previous six months;
For the moderate to low KA endemic areas and in those areas where households are scattered, the index
based approach is the prefered method for active case detection; and
4.2.2.4 Incentive Based Approach: In the incentive based approach, the search for new kala-azar cases
is done through health workers who receive an incentive for each newly detected case. The use of the
incentive based approch can be useful method which can be applied particulary in low KA endemic
upazilas or in combination with any of the approaces mentioned above. The incentive based approach of
case detection may initiate the snow ball technique for NKA and PDKL case finding. However, this
method needs meticulaous supervision and monitoring to prevent misuse of funds. Incentive based ACD
is currently practiced in India and by some research teams in Bangladesh15
.
4.2.2.5 No Kala-azar Transmission Activity (NKTA): The KEP in its ACD strategy have implemented
index based approach. While doing index based approach IRS has been done to about 60-100 HHs. The
objective of conduction of IRS under the index case approach is to stop further transmission of new cases
of kala-azar from the index case. This strategy is known as “No Kala-azar Transmission Activity
(NKTA)”. During the implementation of NKTA under index based approach, the epidemiological team
consisting of medical officer use to investigat the index case and conduct active searching for NKA &
15 Regional Strategic Framework for Elimination of Kala-azar from South-East Asia Region, 2016-2020 WHO/SEARO
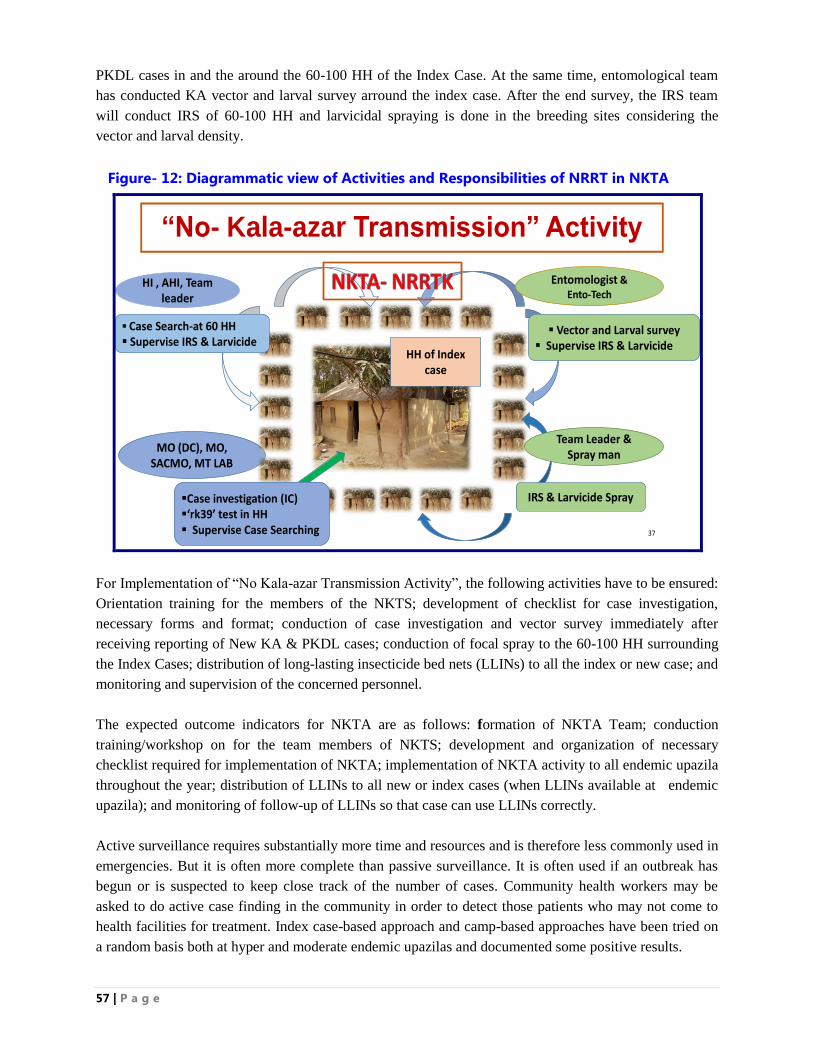
57 | P a g e
PKDL cases in and the around the 60-100 HH of the Index Case. At the same time, entomological team
has conducted KA vector and larval survey arround the index case. After the end survey, the IRS team
will conduct IRS of 60-100 HH and larvicidal spraying is done in the breeding sites considering the
vector and larval density.
Figure- 12: Diagrammatic view of Activities and Responsibilities of NRRT in NKTA
“No- Kala-azar Transmission” Activity
37
Team Leader & Spray man
MO (DC), MO, SACMO, MT LAB
IRS & Larvicide Spray
HI , AHI, Team leader
Entomologist & Ento-Tech
Case Search-at 60 HH Supervise IRS & Larvicide
Vector and Larval survey Supervise IRS & Larvicide
HH of Index case
Case investigation (IC)‘rk39’ test in HH Supervise Case Searching
For Implementation of “No Kala-azar Transmission Activity”, the following activities have to be ensured:
Orientation training for the members of the NKTS; development of checklist for case investigation,
necessary forms and format; conduction of case investigation and vector survey immediately after
receiving reporting of New KA & PKDL cases; conduction of focal spray to the 60-100 HH surrounding
the Index Cases; distribution of long-lasting insecticide bed nets (LLINs) to all the index or new case; and
monitoring and supervision of the concerned personnel.
The expected outcome indicators for NKTA are as follows: formation of NKTA Team; conduction
training/workshop on for the team members of NKTS; development and organization of necessary
checklist required for implementation of NKTA; implementation of NKTA activity to all endemic upazila
throughout the year; distribution of LLINs to all new or index cases (when LLINs available at endemic
upazila); and monitoring of follow-up of LLINs so that case can use LLINs correctly.
Active surveillance requires substantially more time and resources and is therefore less commonly used in
emergencies. But it is often more complete than passive surveillance. It is often used if an outbreak has
begun or is suspected to keep close track of the number of cases. Community health workers may be
asked to do active case finding in the community in order to detect those patients who may not come to
health facilities for treatment. Index case-based approach and camp-based approaches have been tried on
a random basis both at hyper and moderate endemic upazilas and documented some positive results.
58 | P a g e
Implementation of Active Case Detection: The KEP had implemented active search during the last
operational plan and the strategy has been found to be effective in identifying case of kala-azar as
follows:
Formation of Kala-azar Active Search Team: This team is consisted of 2-3 volunteers and AHI/HI as the
first line supervisor. One team has to conduct active search to about 60-100 HH/day surrounding an index case
and refer the suspected cases of kala-azar to UHC for diagnosis with rK39 RDT;
Formation of IRS Team: The IRS team is a 6-member team with spray man and mixture man. The team is
supervised by AHI/HI. The IRS team would search suspected case of kala-azar during indoor residual spraying
(IRS) and refer the cases to UHC for proper diagnosis; and
Formation of Kala-azar Search Volunteer (KSV): During the camp based approach, the KSV have
conducted searching for new suspected cases of kala-azar in 100 HH/day in every village of a designated union
of hyper-endemic upazilas. Suspected cases of NKA detected by the KSV are referred to a central search camp
based at the community, where the MT-Lab performed test using rK39 RDT following a camp-based approach
and refer the positive cases to UHC for treatment.
4.2.2.6 Approach to Manage Asymptomatic Kala-azar Cases
The approach or strategy for the management of asymptomatic kala-azar infection poses an important
challenge because of the two critical reasons. First, the identification of asymptomatic cases and the
management of the carriers have become a great threat for kala-azar elimination program in the country.
Second, the absence of validated markers for asymptomatic infection poses another challenge. An
asymptomatic infective host may serve as silent reservoir and jeopardize the sustainability of elimination
program activities if their role in transmission is confirmed. However, the potential of asymptomatic
infections as a reservoir is not clearly understood.
The number of asymptomatic cases is much higher than the number of infected cases presenting with
clinical illness. Recent studies have revealed that the ratio of full-blown kala-azar cases to asymptomatic
kala-azar infection varies from 1: 2.4 in Sudan, 1:4 in Bangladesh, 1:4 in Kenya, 1:6 in Ethiopia, 1:9 in
Indian and Nepal, and 1:18 in Brazil16
. Many people infected with Leishmania species develop an
effective immune response and do not manifest clinical disease. It is, therefore, important from the
program point of view to know how many infected persons will develop full blown disease and how
many of they can be diagnosed before they show clinical manifestation.
Asymptomatic kala-azar infection is not well defined, but is usually ascertained by a positive serological
test, PCR or Leishmanin Skin Test in the healthy populations living in the endemic areas. The role of
asymptomatic carriers in transmission or the prognosis of asymptomatic infection at the individual level is
not fully explained. Epidemiological studies should be undertaken to identify the factors that lead to the
development of disease in asymptomatic infections.
Genetic factors, poverty, poor housing, mud-wall house, ownership of cattle and poor nutritional status
have been shown to increase the risk of progression from asymptomatic infection to clinical kala-azar;
children with moderate to severe protein energy malnutrition have been found to have nine-fold increased
risk of developing kala-azar. Malnutrition is considered to be associated with impaired immune responses
16 Om Prakash Singh,, et al, (2014). Asymptomatic leishmania infection: A new challenge for leishmania control. Oxford Journal of Clinical Infectious Diseases (CID,) February 27, 2014
59 | P a g e
against the parasite and can weaken both innate as well as T cell immunity. This, however, requires a
longitudinal prospective follow-up design study that allows for the exploration of the combination of
epidemiological, parasitological, immunological and genetic risk factors in the same population.
Sarman S, et. al, (2002) 17
in his research reported their findings on the host immune responses against
L. donovani specific antigen (recombinant K39) and its value in predicting the development of clinical
disease. A total of 240 clinical kala-azar cases and 150 asymptomatic family members and neighbors of
the index case patients were tested for anti-rK39 immunoglobulin G (IgG) and IgA. Fifty five (36.7%)
asymptomatic cases were found to be seropositive. These individuals were monitored every 3 months for
1 year. On follow-up, 24 cases (43.9%) of the asymptomatic seropositive contacts develop kala-azar
within the first 3 months, and a cumulative total of 38 cases (69%) developed kala-azar within 1 year. The
rest 17 (31%) seropositive cases remained asymptomatic and the infection got self-healed in the
subsequent period. The study concluded that the mass screening of family members and immediate
neighboring contacts by using rK39 ELISA could be a highly reliable tool for early diagnosis and to plan
prophylactic treatment of latently infected asymptomatic carriers to eradicate kala-azar.
Based on the research finding, the National Kala-azar Elimination Program will adopt the following
strategy and conduct the following activities:
1. Index Case Search: Index case search should be made mandatory under the kala-azar elimination
program activity. During the index case search, all the names of the family members of the index
cases and the immediate neighboring contact should be listed using prescribed formats.
2. Diagnosis: All the family members and the immediate neighbor should be tested with rK39 antigen.
The names of the asymptomatic seropositive cases with rK39 RDT should be listed using prescribed
format.
3. Distribution of LLIN: Long Lasting Insectiside Impregnated Bednets (LLIN) will be used
selectively to prevent the transmission of disease to the other healthy population.
4. Follow-up and Counseling: Both the index cases and asymptomatic seropositive cases should be
followed-up every 3 months for at least 1 year (Follow-up Formats). The asymptomatic cases should
be health education and counseling. Mobile follow-up may cost effective.
5. Treatment: Asymptomatic seropositive cases who develop clinical symptoms and signs should be
treated with 1st line of anti-leishmania drug and should be follow-up.
6. Sand Fly Density Survey and IRS: The Entomological team should conduct sandfly density survey
to each area arround the index case and conducte IRS to about 60-100 households arround the index
case.
The above program strategy would help correctly diagnosed all most 100% of cases who are
exposed to L. donovani. The program could also predict the disease development in the family
and neighborhood contacts of the patients by using anti-rK39 test. However, it would be difficult
17 Sarman Sing, Veena Kumari and Niti Sing (2002). Predicting Kala-azar Disease Manifestation in Asymptomatic Patients with Latent Leishmania donovani Infection by Detection of Antibody against Recombinant K39 Antigen. Clinical and Diagnostic Laboratory Immunology, May 2002.
60 | P a g e
to rule out re-infection as opposed to re-activation of latent infection in asymptomatic
individuals, who are still residing in the endemic area.
4.3 MANAGEMENT OF KALA-AZAR SURVEILLANCE
Kala-azar surveillance is a part of web-based national disease surveillance system centrally managed by
Kala-azar Elimination Program (KEP), Disease Control Unit of Communicable Disease Control (CDC) of
the Directorate General of Health Services (DGHS). Kala-azar Elimination Program having specific
indicators have been incorporated in the reporting format. In order to strengthen Kala-azar surveillance
system, KA Surveillance Unit has been set up at upazila and district level.
4.3.1 Kala-azar Surveillance Unit:
A. UHC Level: Upazila Kala-azar Surveillance Unit
Head: Upazila Health and Family Planning Officer (UH&FPO)
Focal person: Medical Officer (Disease Control)
Senior Staff Nurse (SSN) and
Statistician
B. District Level: District Kala-azar Surveillance Unit:
Head: Civil Surgeon (CS)
Focal Person: MO (CS/DC)
District Public Health Nurse (DPHN) and
Statistical Assistant
C. Government Medical College Hospitals:
Director (Hospital)
Focal Person: to be assigned by the Hospital Director
Senior Staff Nurse (SSN) and
Statistical Officer/Statistician
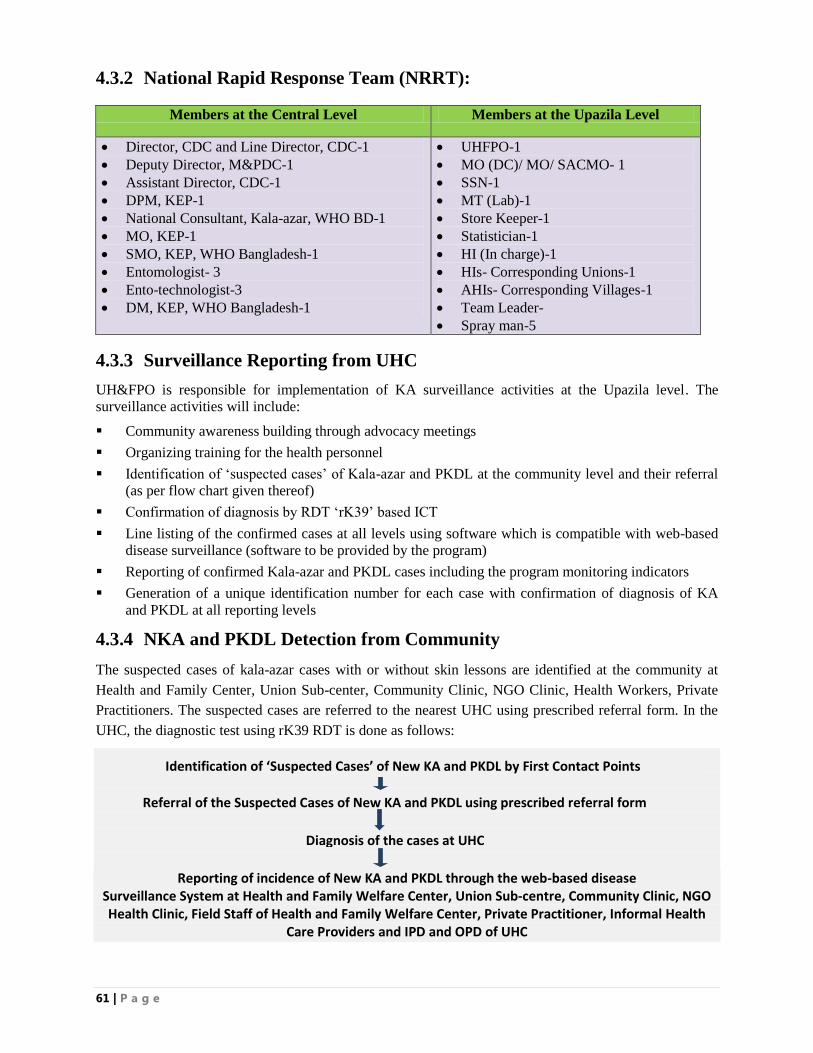
61 | P a g e
4.3.2 National Rapid Response Team (NRRT):
Members at the Central Level Members at the Upazila Level
Director, CDC and Line Director, CDC-1
Deputy Director, M&PDC-1
Assistant Director, CDC-1
DPM, KEP-1
National Consultant, Kala-azar, WHO BD-1
MO, KEP-1
SMO, KEP, WHO Bangladesh-1
Entomologist- 3
Ento-technologist-3
DM, KEP, WHO Bangladesh-1
UHFPO-1
MO (DC)/ MO/ SACMO- 1
SSN-1
MT (Lab)-1
Store Keeper-1
Statistician-1
HI (In charge)-1
HIs- Corresponding Unions-1
AHIs- Corresponding Villages-1
Team Leader-
Spray man-5
4.3.3 Surveillance Reporting from UHC
UH&FPO is responsible for implementation of KA surveillance activities at the Upazila level. The
surveillance activities will include:
Community awareness building through advocacy meetings
Organizing training for the health personnel
Identification of „suspected cases‟ of Kala-azar and PKDL at the community level and their referral
(as per flow chart given thereof)
Confirmation of diagnosis by RDT „rK39‟ based ICT
Line listing of the confirmed cases at all levels using software which is compatible with web-based
disease surveillance (software to be provided by the program)
Reporting of confirmed Kala-azar and PKDL cases including the program monitoring indicators
Generation of a unique identification number for each case with confirmation of diagnosis of KA
and PKDL at all reporting levels
4.3.4 NKA and PKDL Detection from Community
The suspected cases of kala-azar cases with or without skin lessons are identified at the community at
Health and Family Center, Union Sub-center, Community Clinic, NGO Clinic, Health Workers, Private
Practitioners. The suspected cases are referred to the nearest UHC using prescribed referral form. In the
UHC, the diagnostic test using rK39 RDT is done as follows:
Identification of ‘Suspected Cases’ of New KA and PKDL by First Contact Points
Referral of the Suspected Cases of New KA and PKDL using prescribed referral form
Diagnosis of the cases at UHC
Reporting of incidence of New KA and PKDL through the web-based disease
Surveillance System at Health and Family Welfare Center, Union Sub-centre, Community Clinic, NGO Health Clinic, Field Staff of Health and Family Welfare Center, Private Practitioner, Informal Health
Care Providers and IPD and OPD of UHC
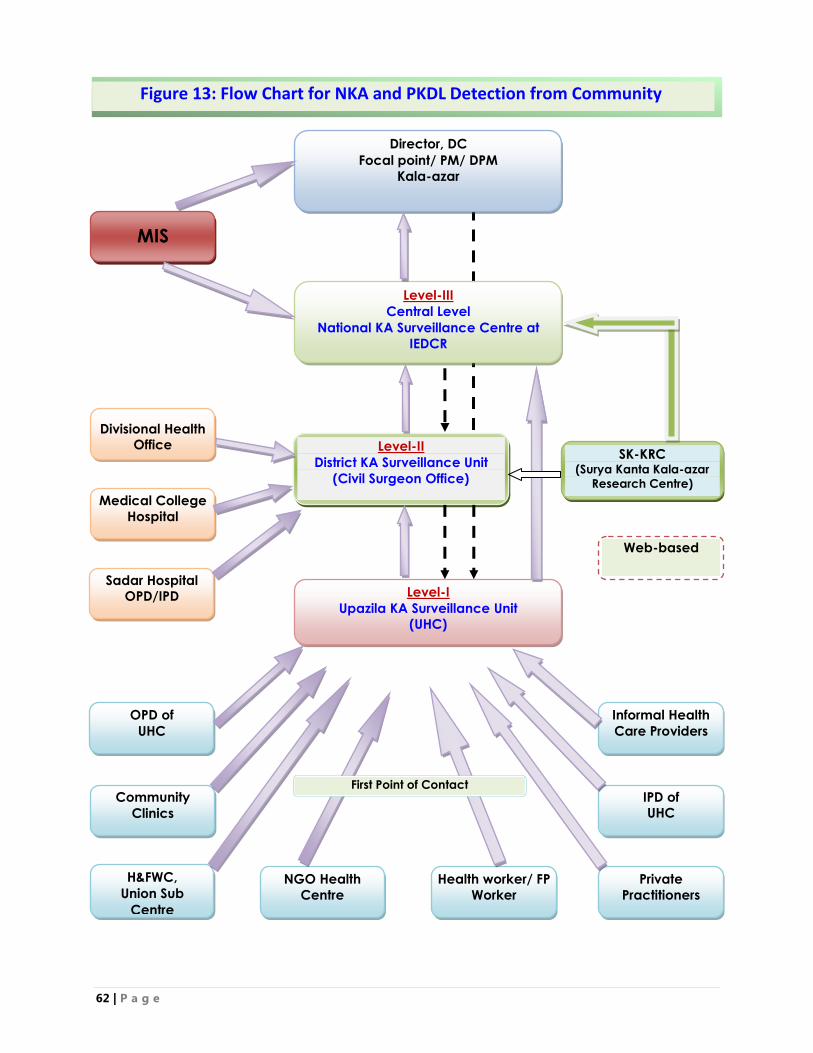
62 | P a g e
OPD of
UHC
IPD of UHC
Community
Clinics
Informal Health
Care Providers
H&FWC,
Union Sub
Centre
Private
Practitioners
NGO Health
Centre
Health worker/ FP
Worker
Level-I
Upazila KA Surveillance Unit (UHC)
Level-II
District KA Surveillance Unit
(Civil Surgeon Office)
Level-III
Central Level
National KA Surveillance Centre at
IEDCR
Director, DC
Focal point/ PM/ DPM
Kala-azar
Web-based
SK-KRC (Surya Kanta Kala-azar
Research Centre)
Sadar Hospital OPD/IPD
Medical College
Hospital
Divisional Health Office
MIS
Figure 13: Flow Chart for NKA and PKDL Detection from Community
First Point of Contact
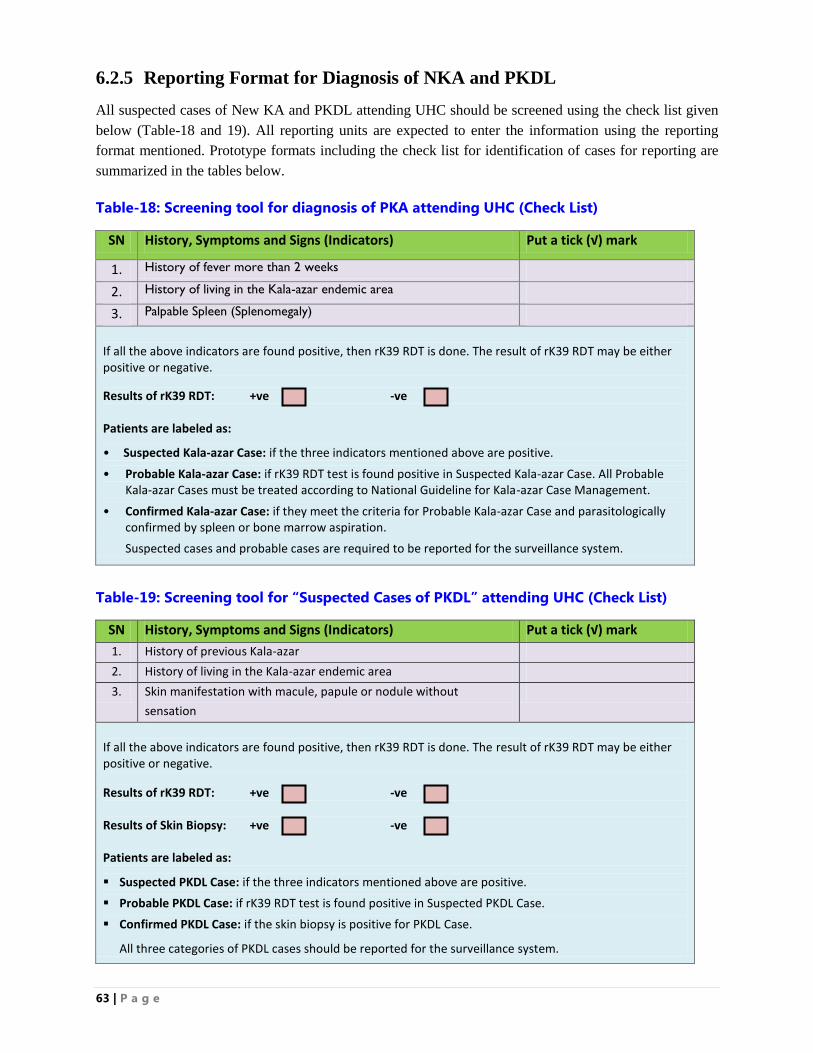
63 | P a g e
6.2.5 Reporting Format for Diagnosis of NKA and PKDL
All suspected cases of New KA and PKDL attending UHC should be screened using the check list given
below (Table-18 and 19). All reporting units are expected to enter the information using the reporting
format mentioned. Prototype formats including the check list for identification of cases for reporting are
summarized in the tables below.
Table-18: Screening tool for diagnosis of PKA attending UHC (Check List)
SN History, Symptoms and Signs (Indicators) Put a tick (√) mark
1. History of fever more than 2 weeks
2. History of living in the Kala-azar endemic area
3. Palpable Spleen (Splenomegaly)
If all the above indicators are found positive, then rK39 RDT is done. The result of rK39 RDT may be either positive or negative.
Results of rK39 RDT: +ve -ve Patients are labeled as:
• Suspected Kala-azar Case: if the three indicators mentioned above are positive.
• Probable Kala-azar Case: if rK39 RDT test is found positive in Suspected Kala-azar Case. All Probable Kala-azar Cases must be treated according to National Guideline for Kala-azar Case Management.
• Confirmed Kala-azar Case: if they meet the criteria for Probable Kala-azar Case and parasitologically confirmed by spleen or bone marrow aspiration.
Suspected cases and probable cases are required to be reported for the surveillance system.
Table-19: Screening tool for “Suspected Cases of PKDL” attending UHC (Check List)
SN History, Symptoms and Signs (Indicators) Put a tick (√) mark
1. History of previous Kala-azar
2. History of living in the Kala-azar endemic area
3. Skin manifestation with macule, papule or nodule without
sensation
If all the above indicators are found positive, then rK39 RDT is done. The result of rK39 RDT may be either positive or negative.
Results of rK39 RDT: +ve -ve Results of Skin Biopsy: +ve -ve Patients are labeled as:
Suspected PKDL Case: if the three indicators mentioned above are positive.
Probable PKDL Case: if rK39 RDT test is found positive in Suspected PKDL Case.
Confirmed PKDL Case: if the skin biopsy is positive for PKDL Case.
All three categories of PKDL cases should be reported for the surveillance system.
64 | P a g e
4.2.6 Reporting of Surveillance Information
The data flow for reporting of cases of New KA and PKDL should follow the flow chart shown in Fig 7.
Upazila Kala-azar surveillance unit should send complete information on Kala-azar to the district focal
point once in a month before the first Wednesday of each month and directly to Program Manager of
Kala-azar Elimination Program through hard and soft copy. After compilation Focal Person (Kala-azar)
will send the report to Central Level. Once web-based surveillance is in place, surveillance data should be
uploaded to the server maintained at Kala-azar Elimination Program, Disease Control Unit of DGHS from
all levels.
A unique identifier should be used for each case during diagnosis to avoid duplication of reporting. If
there are no cases then it should be a zero report. The data should be compiled at each level for the
government, private and facilities, and reported mainly at Upazila and District levels in a coordinated
way. Data from tertiary level health facilities including the medical college hospitals may be reported
through District level or uploaded directly to web-based surveillance system if the facilities are available.
There should be a feedback mechanism to make the best use of surveillance data by the government,
private and NGO facilities for a common understanding of the problems that will lead to identification of
possible solutions. The reports after compilation should be submitted to MO (Kala-azar elimination) of
the UHC. The statistical Assistant will compile information from the reporting units from the
government, private and NGO facilities and add their own.
A consolidated report should be sent to the district. The data will cover information for the preceding
month. In the district, the information from each reporting facility should be entered on the computer and
will send to the central level.
Report on review and feedback: The focal points at all levels have the responsibility to provide
regular written feedback to relevant stakeholders every month. Review and feedback are important at all
levels to take appropriate action. The written feedback from upazila and district will have to be copied to
the program.
Report on treatment: Information available from the treatment cards provided to patients and registers
will be used for preparing treatment report. The basic information recorded is:
Personal information about the patient including address, age, sex, weight, marital status,
pregnancy and lactating status
Contact Number (Mobile Number)
Drugs used for treatment of Kala-azar
Number of days treatment provided
If treatment course has been completed or not
Side effects of drugs
Outcome of treatment
Treatment provider (public, private, NGO)

65 | P a g e
Report on hospitalized cases: Separate reports are needed for the indoor patients of Kala-azar. This
should include the total number of admissions, the total number of patients admitted for Kala-azar, the
total number of deaths and the total number of deaths due to Kala-azar. The report should be categorized
according to age (under five, 5-14 and 15 and above) and sex. Information on pregnant women should be
included separately in the monthly report. The outcome should be summarized as (a) improved (b)
referred (c) died. To indicate the number of patients who worsened and were referred. The report should
indicate the number of patients who used the referral services. The monthly report should indicate the
number of patients who completed the treatment and the number of patients who are being treated but
have not completed treatment. It is also necessary to indicate the number of patients who were started
treatment but have dropped out.
4.2.7 Web-based Registration of Kala-azar Cases and Follow-up Form:
The overall goal of the Web-based Registration of Kala-azar Cases and Follow-up Form is to record
all Kala-azar cases diagnosed and treated at health care facilities (Upazila Health Complexes, District
Hospitals and Tertiary & Specialized Hospitals) and ensure required numbers of follow-up visits. The
information generated from the web-based registration will help the health program personnel to take
immediate actions to prevent the transmission of the disease in the epidemic and outbreak situation, and
help the program managers to make better decision to improve the Kala-azar elimination program
activities. Every health facilities situated at the endemic areas are equipped with computer and data are
entered using statistical package called “Health Management Information System 2 (DHIS2)”.
KEP will be able to manage its operations more effectively, monitor processes and improve
communication with help of DHIS 2. DHIS 2 is typically used as national health information systems at
DGHS-Dhaka for data management and analysis purposes, for health program monitoring and evaluation,
as facility registries and service availability mapping, for logistics management and for mobile tracking of
pregnant mothers in rural communities. With the help of DHIS 2, KEP will be able to capture data on any
type of device, including desktops, laptops, tablets, smartphones and feature phones. It works in most
solutions in work-offline, enabling improved reach in locations with poor connectivity. DHIS 2 provides
a wide range of solutions based on HTML5, SMS and Java.
The Web-based Registration of Kala-azar Case and Follow-Form has following subsections:
1. General Information (of the patients)
2. Patient‟s Information (Before Treatment)
3. Patient‟s Information (After Treatment and beofre Discharge)
4. Suspected Adverse Drug Reaction (ADR) and List of Adverse Events
5. Follow-up Information
The web-based registration form is attached in Annex-13 (Page___)
66 | P a g e
CHAPTER: FIVE
MONITORING AND EVALUATION (M&E)
67 | P a g e
5. MONITORING AND EVALUATION:
The availability and use of quality data is essential for evidence based decision making to improve
program activities. The lack of accurate and timely data can be an impediment to progress in
implementation. The monitoring and evaluation component of the program will provide important data on
the scope, coverage and effectiveness on the programs activities. The M&E data will be used to monitor
progress in key program outcomes as well as provide data on inputs and outputs.
Routine monitoring, periodic assessment and evaluation would be done by the program at all levels to
ensure effective implementation of different activities as per plan. A set of objectively verifiable
indicators will be used to measure progress and assess the achievement of elimination program in line
with national Kala-azar strategy. For regular monitoring checklists or formats will be used to see any gaps
of the ongoing activities. Further, impact evaluations will be obtained from external independent
organization who competent authority will do the evaluation.
In this chapter the activities mentioned in the national guideline for Kala-azar case management will be
monitored and evaluated; however “national guideline for M&E for the NKEP” will be used to monitor
and evaluate the NKEP.
5.1 The Monitoring & Evaluation Framework
The following input-output-outcome-impacts framework is used for monitoring and evaluation of the
activities mention in the national Kala-azar case management guideline.
Input: describes the resources allocated to an activity.
Process: describes the activities and performance within the services.
Output: measures the direct products (deliverables) of an activity.
Outcome: describes the effect of these activities in terms of behavioral change
Impact: describes the status of health (not covered by this chapter)
A set of objectively verifiable indicators has been developed to measure progress and assess the
achievement of the planned activities. The indicators, operation definition of the indicators, sources of
verification and the responsible person to collect these indicators are summarized in sub-chapter 5.3 to 5.5
in the nest pages. Data flow of the M&E is presented in Figure-13.
5.2 Monitoring and Evaluation Team
For monitoring and supervision there different teams will be deployed.
Central level District/Tertiary level Upazila level
Line Director (DC)
Assistant director (DC)
Deputy Program Manager-
Kala-azar
Surveillance Medical
Officer- Kala-azar
Monitoring & Evaluation
Manager
Civil Surgeon
Deputy Civil Surgeon
Director, Tertiary level
Hospital
Consultant, Tertiary level
Hospital
Upazila Health & Family
planning officer
MO (DC)
Sr. Staff Nurse (SSN)
MT (Lab)
Statistician
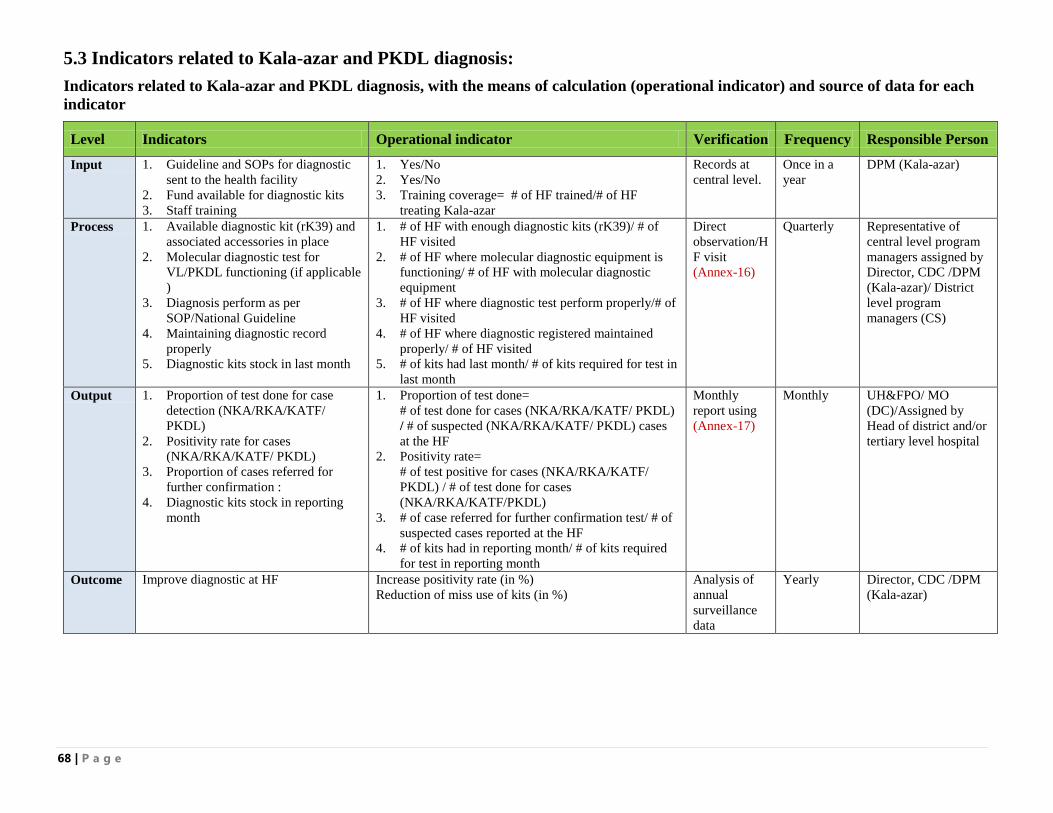
68 | P a g e
5.3 Indicators related to Kala-azar and PKDL diagnosis:
Indicators related to Kala-azar and PKDL diagnosis, with the means of calculation (operational indicator) and source of data for each
indicator
Level Indicators Operational indicator Verification Frequency Responsible Person
Input 1. Guideline and SOPs for diagnostic
sent to the health facility
2. Fund available for diagnostic kits
3. Staff training
1. Yes/No
2. Yes/No
3. Training coverage= # of HF trained/# of HF
treating Kala-azar
Records at
central level.
Once in a
year
DPM (Kala-azar)
Process 1. Available diagnostic kit (rK39) and
associated accessories in place
2. Molecular diagnostic test for
VL/PKDL functioning (if applicable
)
3. Diagnosis perform as per
SOP/National Guideline
4. Maintaining diagnostic record
properly
5. Diagnostic kits stock in last month
1. # of HF with enough diagnostic kits (rK39)/ # of
HF visited
2. # of HF where molecular diagnostic equipment is
functioning/ # of HF with molecular diagnostic
equipment
3. # of HF where diagnostic test perform properly/# of
HF visited
4. # of HF where diagnostic registered maintained
properly/ # of HF visited
5. # of kits had last month/ # of kits required for test in
last month
Direct
observation/H
F visit
(Annex-16)
Quarterly Representative of
central level program
managers assigned by
Director, CDC /DPM
(Kala-azar)/ District
level program
managers (CS)
Output 1. Proportion of test done for case
detection (NKA/RKA/KATF/
PKDL)
2. Positivity rate for cases
(NKA/RKA/KATF/ PKDL)
3. Proportion of cases referred for
further confirmation :
4. Diagnostic kits stock in reporting
month
1. Proportion of test done=
# of test done for cases (NKA/RKA/KATF/ PKDL)
/ # of suspected (NKA/RKA/KATF/ PKDL) cases
at the HF
2. Positivity rate=
# of test positive for cases (NKA/RKA/KATF/
PKDL) / # of test done for cases
(NKA/RKA/KATF/PKDL)
3. # of case referred for further confirmation test/ # of
suspected cases reported at the HF
4. # of kits had in reporting month/ # of kits required
for test in reporting month
Monthly
report using
(Annex-17)
Monthly UH&FPO/ MO
(DC)/Assigned by
Head of district and/or
tertiary level hospital
Outcome Improve diagnostic at HF Increase positivity rate (in %)
Reduction of miss use of kits (in %)
Analysis of
annual
surveillance
data
Yearly Director, CDC /DPM
(Kala-azar)
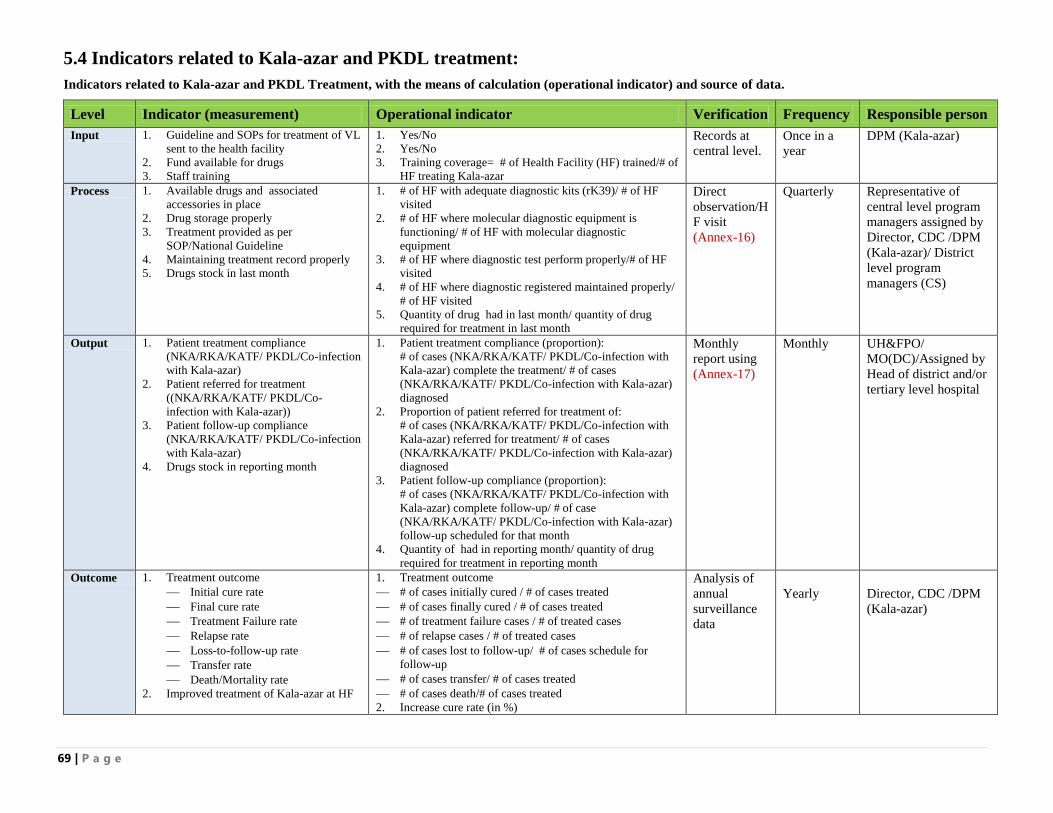
69 | P a g e
5.4 Indicators related to Kala-azar and PKDL treatment:
Indicators related to Kala-azar and PKDL Treatment, with the means of calculation (operational indicator) and source of data.
Level Indicator (measurement) Operational indicator Verification Frequency Responsible person
Input 1. Guideline and SOPs for treatment of VL
sent to the health facility
2. Fund available for drugs
3. Staff training
1. Yes/No
2. Yes/No
3. Training coverage= # of Health Facility (HF) trained/# of
HF treating Kala-azar
Records at
central level.
Once in a
year
DPM (Kala-azar)
Process 1. Available drugs and associated
accessories in place
2. Drug storage properly
3. Treatment provided as per
SOP/National Guideline
4. Maintaining treatment record properly
5. Drugs stock in last month
1. # of HF with adequate diagnostic kits (rK39)/ # of HF
visited
2. # of HF where molecular diagnostic equipment is
functioning/ # of HF with molecular diagnostic
equipment
3. # of HF where diagnostic test perform properly/# of HF
visited
4. # of HF where diagnostic registered maintained properly/
# of HF visited
5. Quantity of drug had in last month/ quantity of drug
required for treatment in last month
Direct
observation/H
F visit
(Annex-16)
Quarterly Representative of
central level program
managers assigned by
Director, CDC /DPM
(Kala-azar)/ District
level program
managers (CS)
Output 1. Patient treatment compliance
(NKA/RKA/KATF/ PKDL/Co-infection
with Kala-azar)
2. Patient referred for treatment
((NKA/RKA/KATF/ PKDL/Co-
infection with Kala-azar))
3. Patient follow-up compliance
(NKA/RKA/KATF/ PKDL/Co-infection
with Kala-azar)
4. Drugs stock in reporting month
1. Patient treatment compliance (proportion):
# of cases (NKA/RKA/KATF/ PKDL/Co-infection with
Kala-azar) complete the treatment/ # of cases
(NKA/RKA/KATF/ PKDL/Co-infection with Kala-azar)
diagnosed
2. Proportion of patient referred for treatment of:
# of cases (NKA/RKA/KATF/ PKDL/Co-infection with
Kala-azar) referred for treatment/ # of cases
(NKA/RKA/KATF/ PKDL/Co-infection with Kala-azar)
diagnosed
3. Patient follow-up compliance (proportion):
# of cases (NKA/RKA/KATF/ PKDL/Co-infection with
Kala-azar) complete follow-up/ # of case
(NKA/RKA/KATF/ PKDL/Co-infection with Kala-azar)
follow-up scheduled for that month
4. Quantity of had in reporting month/ quantity of drug
required for treatment in reporting month
Monthly
report using
(Annex-17)
Monthly UH&FPO/
MO(DC)/Assigned by
Head of district and/or
tertiary level hospital
Outcome 1. Treatment outcome
Initial cure rate
Final cure rate
Treatment Failure rate
Relapse rate
Loss-to-follow-up rate
Transfer rate
Death/Mortality rate
2. Improved treatment of Kala-azar at HF
1. Treatment outcome
# of cases initially cured / # of cases treated
# of cases finally cured / # of cases treated
# of treatment failure cases / # of treated cases
# of relapse cases / # of treated cases
# of cases lost to follow-up/ # of cases schedule for
follow-up
# of cases transfer/ # of cases treated
# of cases death/# of cases treated
2. Increase cure rate (in %)
Analysis of
annual
surveillance
data
Yearly
Director, CDC /DPM
(Kala-azar)
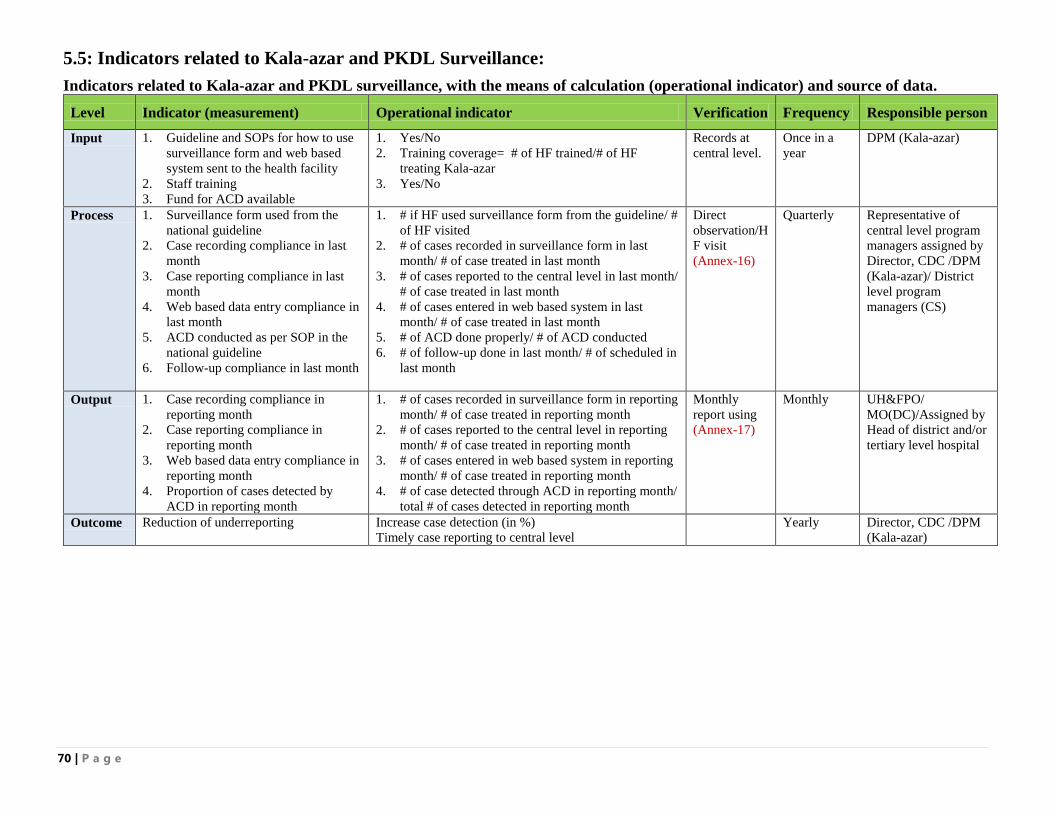
70 | P a g e
5.5: Indicators related to Kala-azar and PKDL Surveillance:
Indicators related to Kala-azar and PKDL surveillance, with the means of calculation (operational indicator) and source of data.
Level Indicator (measurement) Operational indicator Verification Frequency Responsible person
Input 1. Guideline and SOPs for how to use
surveillance form and web based
system sent to the health facility
2. Staff training
3. Fund for ACD available
1. Yes/No
2. Training coverage= # of HF trained/# of HF
treating Kala-azar
3. Yes/No
Records at
central level.
Once in a
year
DPM (Kala-azar)
Process 1. Surveillance form used from the
national guideline
2. Case recording compliance in last
month
3. Case reporting compliance in last
month
4. Web based data entry compliance in
last month
5. ACD conducted as per SOP in the
national guideline
6. Follow-up compliance in last month
1. # if HF used surveillance form from the guideline/ #
of HF visited
2. # of cases recorded in surveillance form in last
month/ # of case treated in last month
3. # of cases reported to the central level in last month/
# of case treated in last month
4. # of cases entered in web based system in last
month/ # of case treated in last month
5. # of ACD done properly/ # of ACD conducted
6. # of follow-up done in last month/ # of scheduled in
last month
Direct
observation/H
F visit
(Annex-16)
Quarterly Representative of
central level program
managers assigned by
Director, CDC /DPM
(Kala-azar)/ District
level program
managers (CS)
Output 1. Case recording compliance in
reporting month
2. Case reporting compliance in
reporting month
3. Web based data entry compliance in
reporting month
4. Proportion of cases detected by
ACD in reporting month
1. # of cases recorded in surveillance form in reporting
month/ # of case treated in reporting month
2. # of cases reported to the central level in reporting
month/ # of case treated in reporting month
3. # of cases entered in web based system in reporting
month/ # of case treated in reporting month
4. # of case detected through ACD in reporting month/
total # of cases detected in reporting month
Monthly
report using
(Annex-17)
Monthly UH&FPO/
MO(DC)/Assigned by
Head of district and/or
tertiary level hospital
Outcome Reduction of underreporting Increase case detection (in %)
Timely case reporting to central level
Yearly Director, CDC /DPM
(Kala-azar)
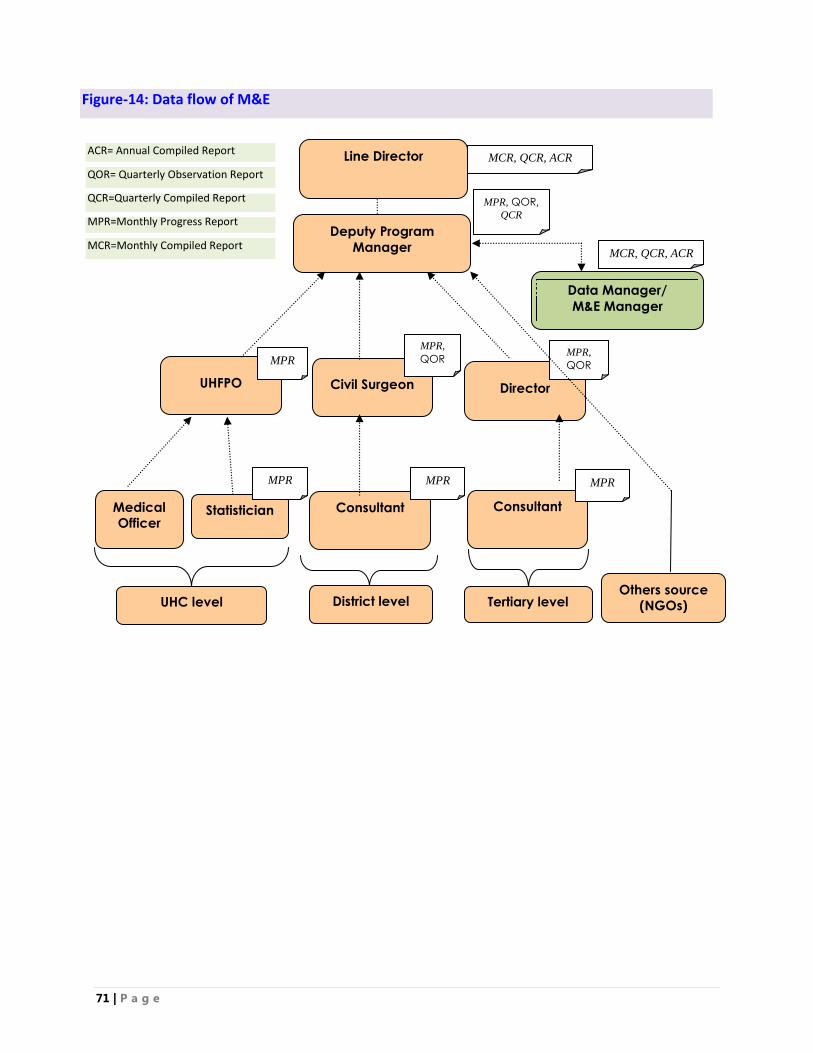
71 | P a g e
MCR, QCR, ACR
UHC level District level Tertiary level
UHFPO
Statistician
Medical Officer
Consultant
Civil Surgeon
Director
Consultant
Deputy Program
Manager
Data Manager/
M&E Manager
Line Director
MPR
MCR, QCR, ACR
MPR MPR
MPR,
QOR
MPR,
QOR MPR
Others source (NGOs)
MPR, QOR,
QCR
Figure-14: Data flow of M&E
MPR=Monthly Progress Report
MCR=Monthly Compiled Report
QCR=Quarterly Compiled Report
ACR= Annual Compiled Report
QOR= Quarterly Observation Report
72 | P a g e
ANNEXURES
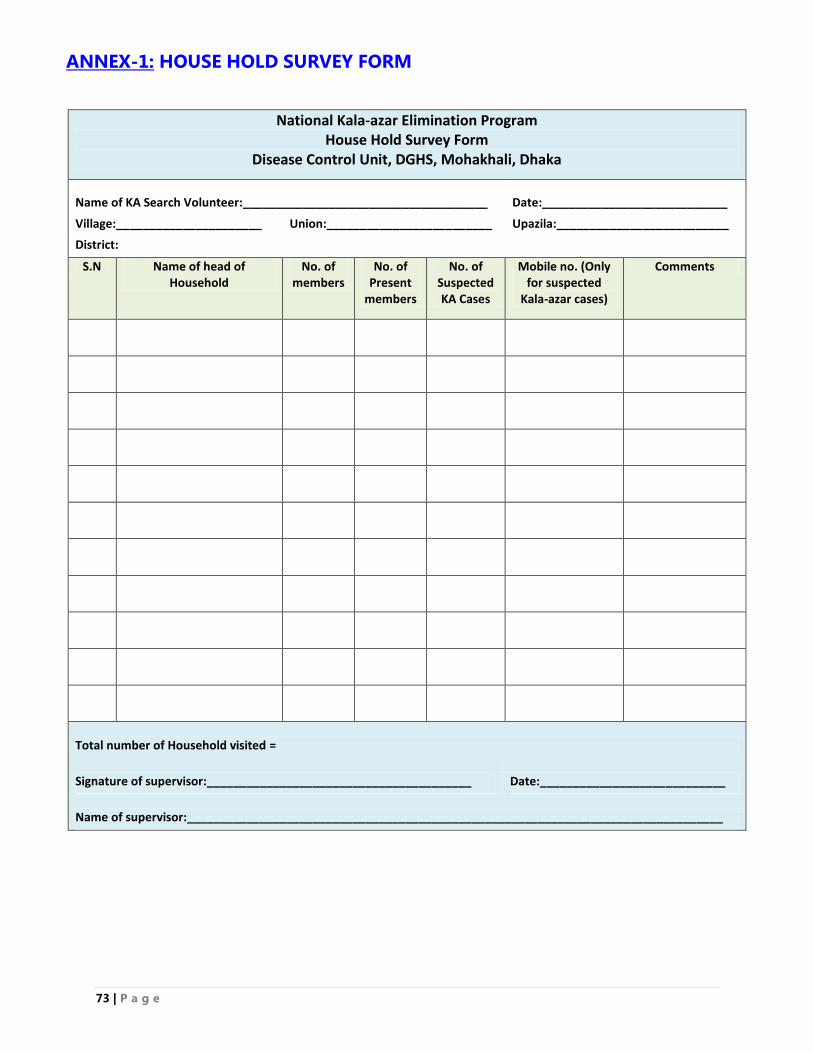
73 | P a g e
ANNEX-1: HOUSE HOLD SURVEY FORM
National Kala-azar Elimination Program House Hold Survey Form
Disease Control Unit, DGHS, Mohakhali, Dhaka
Name of KA Search Volunteer:_____________________________________ Date:____________________________
Village:______________________ Union:_________________________ Upazila:__________________________
District:
S.N Name of head of Household
No. of members
No. of Present
members
No. of Suspected KA Cases
Mobile no. (Only for suspected
Kala-azar cases)
Comments
Total number of Household visited =
Signature of supervisor:________________________________________ Date:____________________________
Name of supervisor:_________________________________________________________________________________
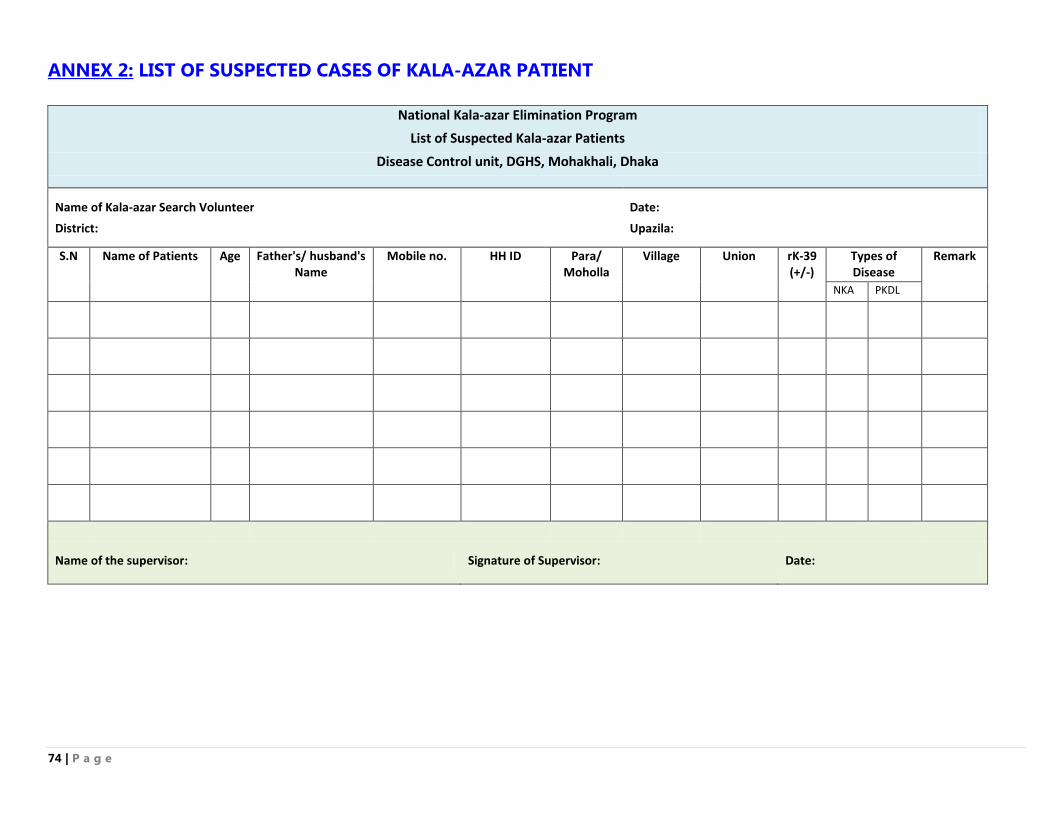
74 | P a g e
ANNEX 2: LIST OF SUSPECTED CASES OF KALA-AZAR PATIENT
National Kala-azar Elimination Program
List of Suspected Kala-azar Patients
Disease Control unit, DGHS, Mohakhali, Dhaka
Name of Kala-azar Search Volunteer
Date:
District: Upazila:
S.N Name of Patients Age Father's/ husband's Name
Mobile no. HH ID Para/ Moholla
Village Union rK-39 (+/-)
Types of Disease
Remark
NKA PKDL
Name of the supervisor: Signature of Supervisor: Date:
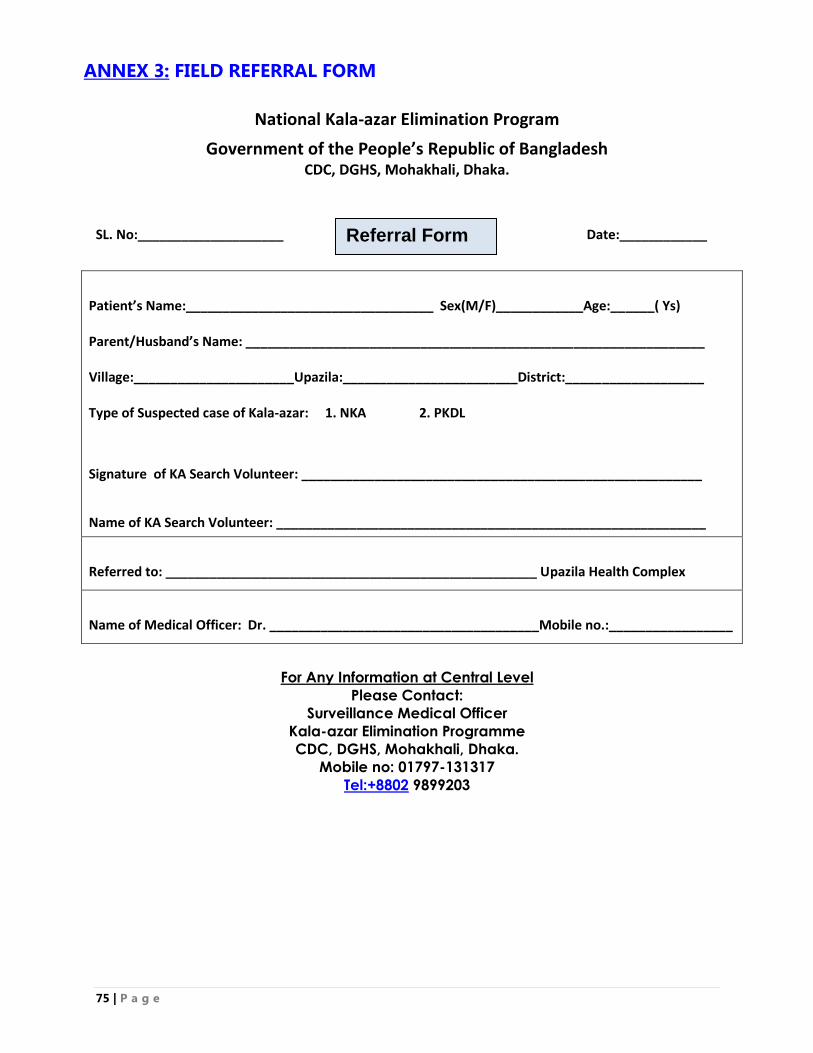
75 | P a g e
ANNEX 3: FIELD REFERRAL FORM
National Kala-azar Elimination Program
Government of the People’s Republic of Bangladesh CDC, DGHS, Mohakhali, Dhaka.
SL. No:____________________ Date:____________
Patient’s Name:__________________________________ Sex(M/F)____________Age:______( Ys)
Parent/Husband’s Name: _______________________________________________________________
Village:______________________Upazila:________________________District:___________________
Type of Suspected case of Kala-azar: 1. NKA 2. PKDL
Signature of KA Search Volunteer: _______________________________________________________
Name of KA Search Volunteer: ___________________________________________________________
Referred to: ___________________________________________________ Upazila Health Complex
Name of Medical Officer: Dr. _____________________________________Mobile no.:_________________
For Any Information at Central Level
Please Contact:
Surveillance Medical Officer
Kala-azar Elimination Programme
CDC, DGHS, Mohakhali, Dhaka.
Mobile no: 01797-131317
Tel:+8802 9899203
Referral Form
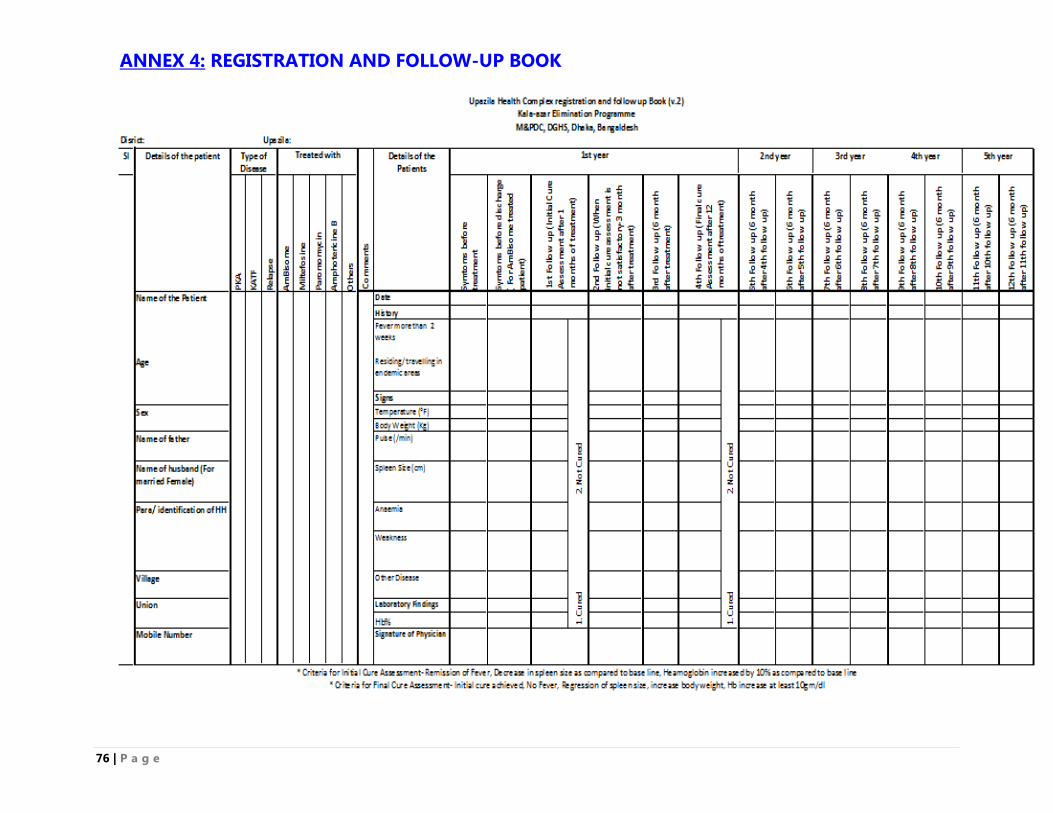
76 | P a g e
ANNEX 4: REGISTRATION AND FOLLOW-UP BOOK
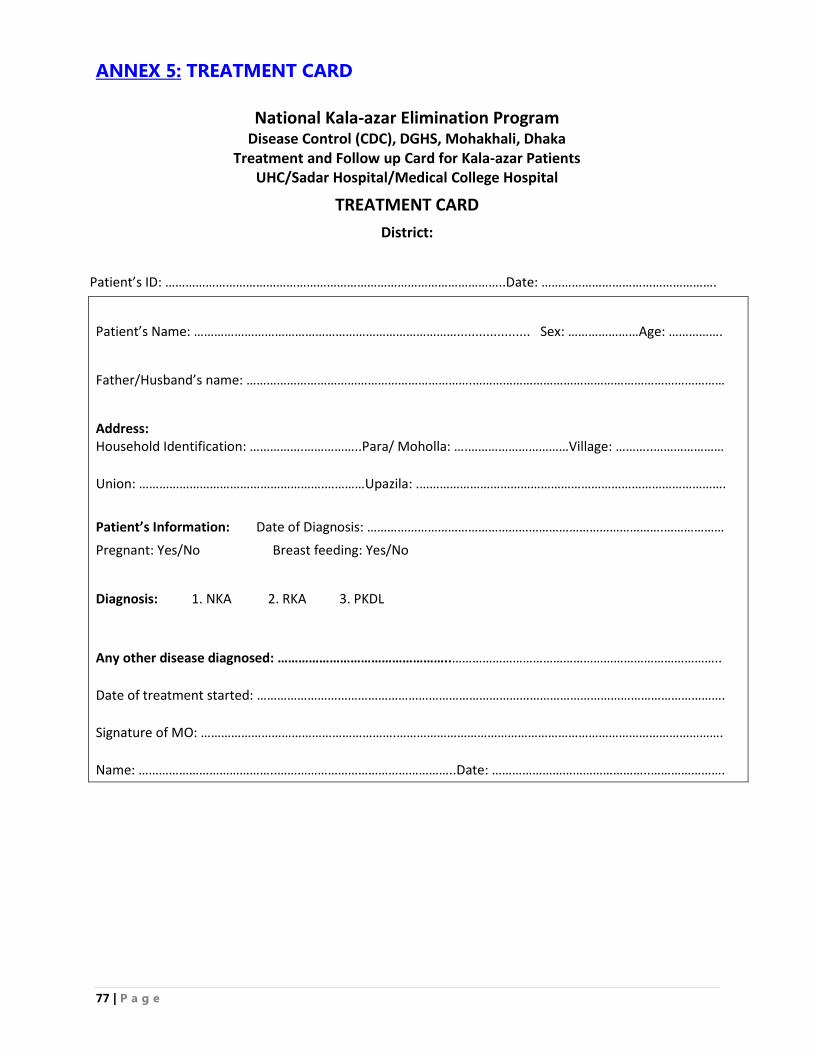
77 | P a g e
ANNEX 5: TREATMENT CARD
National Kala-azar Elimination Program Disease Control (CDC), DGHS, Mohakhali, Dhaka
Treatment and Follow up Card for Kala-azar Patients UHC/Sadar Hospital/Medical College Hospital
TREATMENT CARD
District:
Patient’s ID: ………………………………………………………………………………………..Date: …………………………………………….
Patient’s Name: …………………………………………………………………….................... Sex: …………………Age: …………….
Father/Husband’s name: ………………………………………………………….…………………………………………………………………
Address: Household Identification: …………….……………..Para/ Moholla: ….…………………………Village: ………..………………… Union: ……………………………………………….…………Upazila: .……………………………………………………………………………….
Patient’s Information: Date of Diagnosis: …………………………………………………………………………….………………
Pregnant: Yes/No Breast feeding: Yes/No
Diagnosis: 1. NKA 2. RKA 3. PKDL
Any other disease diagnosed: …………………………………………..…………………………………………………………………….. Date of treatment started: …………………………………………………………………………………………………………………………. Signature of MO: ………………………………………………….……………………………………………………………………………………. Name: …………………………………..……………………………………………..Date: ………………………………………..………………….
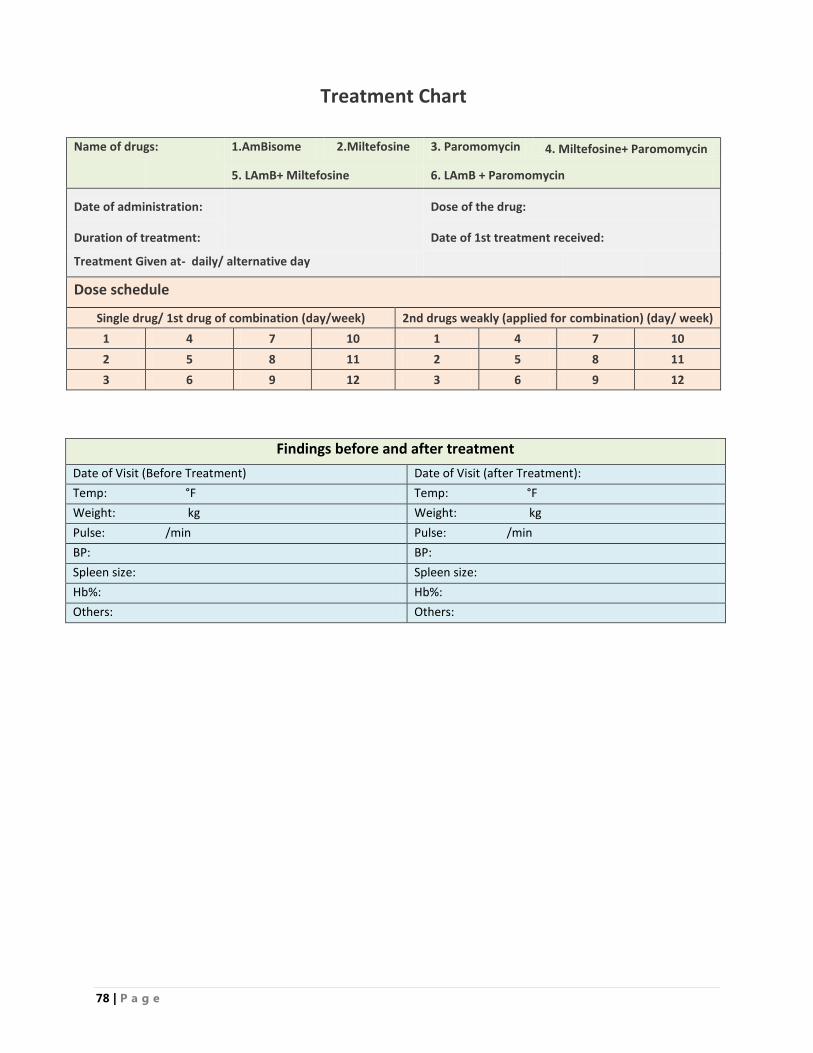
78 | P a g e
Treatment Chart
Name of drugs: 1.AmBisome 2.Miltefosine 3. Paromomycin 4. Miltefosine+ Paromomycin
5. LAmB+ Miltefosine 6. LAmB + Paromomycin
Date of administration:
Dose of the drug:
Duration of treatment:
Date of 1st treatment received:
Treatment Given at- daily/ alternative day
Dose schedule
Single drug/ 1st drug of combination (day/week) 2nd drugs weakly (applied for combination) (day/ week)
1 4 7 10 1 4 7 10
2 5 8 11 2 5 8 11
3 6 9 12 3 6 9 12
Findings before and after treatment
Date of Visit (Before Treatment) Date of Visit (after Treatment):
Temp: °F Temp: °F
Weight: kg Weight: kg
Pulse: /min Pulse: /min
BP: BP:
Spleen size: Spleen size:
Hb%: Hb%:
Others: Others:
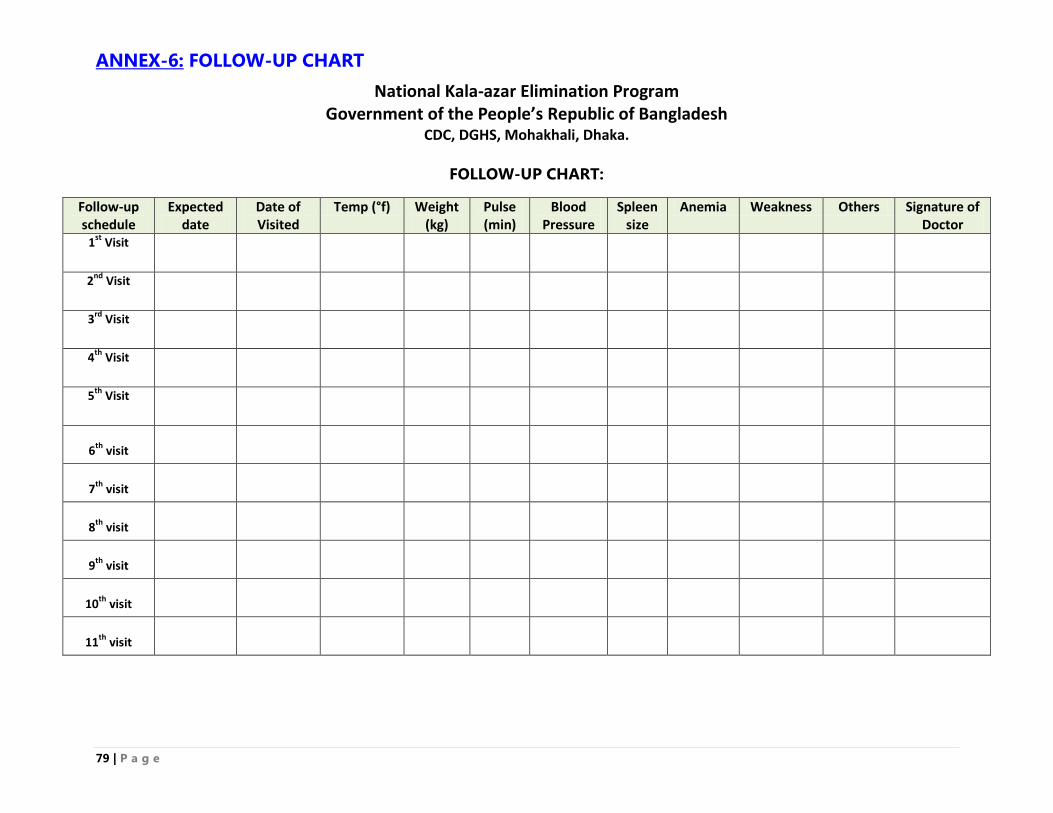
79 | P a g e
ANNEX-6: FOLLOW-UP CHART
National Kala-azar Elimination Program Government of the People’s Republic of Bangladesh
CDC, DGHS, Mohakhali, Dhaka.
FOLLOW-UP CHART:
Follow-up schedule
Expected date
Date of Visited
Temp (°f) Weight (kg)
Pulse (min)
Blood Pressure
Spleen size
Anemia Weakness Others Signature of Doctor
1st
Visit
2nd
Visit
3rd
Visit
4th
Visit
5th
Visit
6th
visit
7th
visit
8th
visit
9th
visit
10th
visit
11th
visit
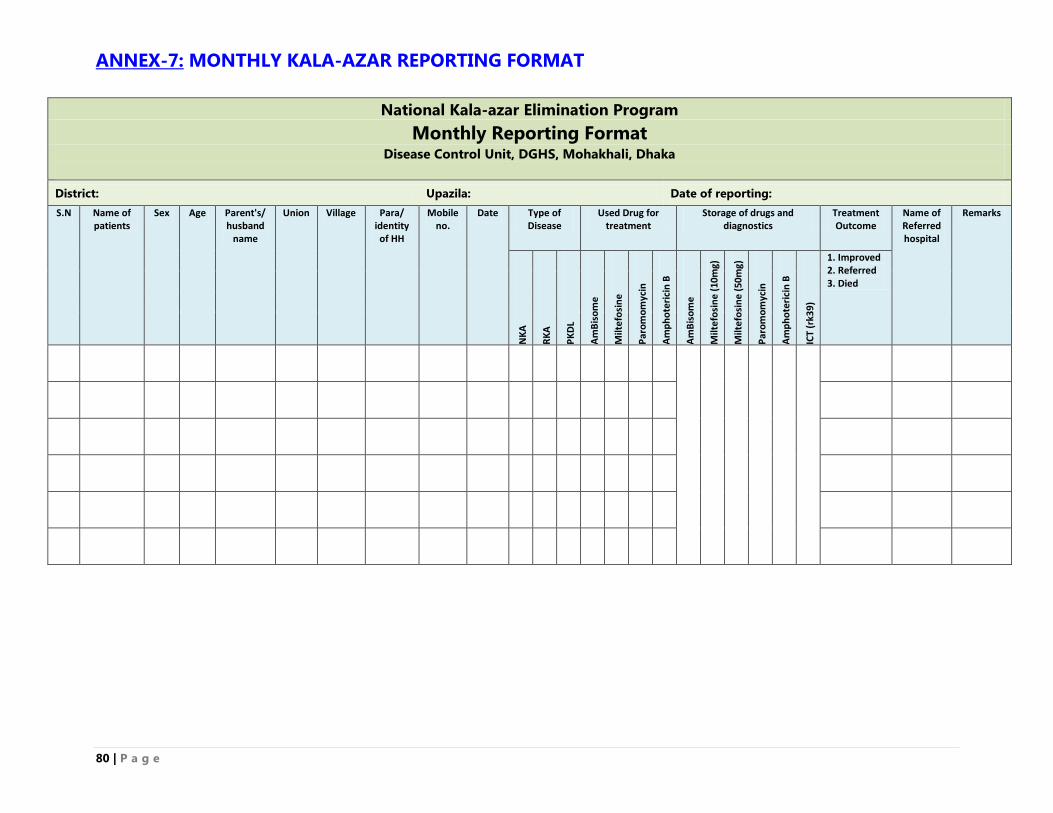
80 | P a g e
ANNEX-7: MONTHLY KALA-AZAR REPORTING FORMAT
National Kala-azar Elimination Program
Monthly Reporting Format Disease Control Unit, DGHS, Mohakhali, Dhaka
District: Upazila: Date of reporting:
S.N Name of patients
Sex Age Parent's/ husband
name
Union Village Para/ identity of HH
Mobile no.
Date Type of Disease
Used Drug for treatment
Storage of drugs and diagnostics
Treatment Outcome
Name of Referred hospital
Remarks
NK
A
RK
A
PK
DL
Am
Bis
om
e
Milt
efo
sin
e
Par
om
om
ycin
Am
ph
ote
rici
n B
Am
Bis
om
e
Milt
efo
sin
e (
10m
g)
Milt
efo
sin
e (
50m
g)
Par
om
om
ycin
Am
ph
ote
rici
n B
ICT
(rk3
9)
1. Improved 2. Referred 3. Died
ANNEX-8: DESCRIPTION OF DRUGS USED FOR THE TREATMENT OF
KALA-AZAR
1. LIPOSOMAL AMPHOTERICIN B (LAMB):
Apart from treating serious systematic fungal infection and primary amoebic meningoencephalitis,
Liposomal Amphotericin B (LAmB) is first line of treatment of drug of choice for the treatment of
visceral leishmaniasis (VL). The drug has the following advantages:
LAmB has the best safety profile, well tolerated and widened the narrow therapeutic window.
LAmB can be given in a single intravenous infusion at a dose of 10 mg/kg for a period not less
than 3 hours duration. Therefore, the drug provides excellent treatment compliance.
In special situations, like Retreatment cases (relapse or failure cases), children of less than 5
years, in pregnancy, and co-infection with HIV/ AIDS could be treated with multiple dose of
LAmB (5mg/kg body weight on alternate days for 3 doses, or 3mg/kg body weight for 5 days. For
retreatment cases, this standard liposomal amphotericin B should be prescribed if the combination
treatment fails.
For standard use of LAmB please see the Annex 7: Standard operation Procedure for LAmB
(AmBisome).
For combination of first line treatment in Bangladesh, Injection Liposomal Amphotericin B would
be given as 5mg/kg body weight IV infusion for single day. It will be followed by either oral drug
(Miltefosine) or injection drug (Paromomycin) according to schedule.
LAmB (AmBisome) must be reconstituted using sterile water for injection (without a Bacteriostatic
agent) and diluted in dextrose solution (5%, 10% or 20%) for infusion only to be administered over a
period of 3-4 hours. AmBisome is not compatible with saline and must not be reconstituted or diluted
with saline or administered through an intravenous line that has previously been used for saline unless
first flushed with dextrose solution (5%, 10% or 20%) for infusion. If this is not feasible, AmBisome
should be administered through a separate line.
AmBisome should be administered by admitting the patient in a hospital during the entire period of
treatment for close supervision and monitoring of side effects. Each vial contains as active ingredient
50 mg of amphotericin B (50,000 units) encapsulated in liposomes. After reconstitution, the
concentration contains 4 mg/ml amphotericin B. AmBisome is indicated as the primary therapy of VL
in immuno-competent patients including both adult and children. AmBisome is also indicated as the
primary therapy of VL in immuno-compromised patients e.g., HIV positive.
Test Dose of AmBisome: In order to avoid anaphylaxis and anaphylactoid reactions, a test dose
should be administered initially. If a severe anaphylactic/anaphylactoid reaction occurs, the infusion
should be discarded. AmBisome has been shown to be substantially less toxic; however, adverse
reactions including renal adverse reactions may still occur.
Undesirable Side Effects of AmBisome: Fever and chills/rigors are the most frequent infusion-
related reactions expected to occur during AmBisome administration. Less frequent infusion-related
reactions such as hypotension, anorexia, nausea, vomiting, headache, dyspnea and tachypnea,
drowsiness, and generalized weakness, back pain, chest tightness or pain, bronchospasm, flushing,
and tachycardiamay occur. These resolve rapidly on stopping the infusion and may not occur on
82 | P a g e
subsequent dose. If any severe hypersensitivity reaction occurred then standard hypersensitivity
management protocol should be followed.
Precaution before using LAmB: Hb% of KA patients should be investigated before LAmB
administration. If Hb% is less than 6mg/dl, then 1 or 2 unit blood should be transfused to increase
Hemoglobin level more than 6 mg/dl and then LAmB should be infused. AmBisome should be
administered with caution in case of renal , hepatic or cardiac compromised patients
Contraindications: AmBisome is contraindicated in those patients who have demonstrated or have
known hypersensitivity to Amphotericin B deoxycholate or any other constituents of the product
unless, in the opinion of the treating physician, the benefit of therapy outweighs the risk.
Indications for alternative 1st line drugs (Oral miltefosine and Injection Paromomycin
combination)
When Liposomal Amphotericin B is not indicated due to hypersensitivity, intolerance,
contraindication
When Liposomal Amphotericin B is not available.
2. MILTEFOSINE:
Miltefosine, an oral relatively safe drug, is used as an alternative choice of 1st line of treatment of KA
in NKEP in Bangladesh. The dose of Miltefosine is depended on age and body weight, and should be
administered daily in two divided doses with meal for a period of 28 days. In case of missed doses,
treatment up to 35 days is recommended to complete the full course.
Evidence obtained from at least one properly designed randomized controlled trial shows that total
doses with 28 days treatment with Miltefosine has shown a cure rate in immuno-competent patients of
more than 94% in India and about 90% in Ethiopia18
. Disappearance of the lesions at a 12-month
follow-up visit was taken as the criterion of cure, including parasitological as well as clinical cure.
Since this drug is given for 28 days, patient compliance to treatment is a serious concern. Analysis of
data from the upazila health complexes, tertiary hospitals and SK-KRC of Bangladesh would be
useful to document the issue of compliance. Similar to the development of drug resistance in case of
any monotherapy, resistance of parasite to Miltefosine can also develop.
When to avoid the use of Miltefosine: Miltefosine is the preferred drug of choice for the treatment
of NKA and PKDL in the kala-azar elimination program. However, the drug is not recommended in
the following situations: (i) women during pregnancy, (ii) married women of child-bearing age who
are not using contraceptives regularly and are at risk of becoming pregnant, (iii) women who are
breast-feeding their babies, and (iv) children less than two years of age.
Miltefosine may not be the ideal drug for the following patients of Kala-azar: Miltefosine may
not be the ideal drug for patients of kala-azar who are severely undernourished having severe anemia
and patients with known history of kidney or liver failure. For patients with severe anemia and severe
under nutrition, before starting miltefosine treatment, patients should be built up by blood transfusion
to correct anemia and appropriate feeding to correct severe under nutrition. If dehydration is present,
it should be corrected with fluids, preferably oral rehydration solution. This would help in reducing
the side effects of the drug. Married women of childbearing age should not be given miltefosine
18
Control of the Leishmaniases: WHO Technical Report Series-949. Report of a meeting of the WHO Expert Committee on the Control of Leishmaniases, Geneva, 22-26 March 2010, WHO; p-58.
83 | P a g e
treatment if couples do not agree to use contraceptive methods to prevent pregnancy during treatment
and until three months thereafter.
Adverse reactions of Miltefosine treatment: Adverse reactions to Miltefosine are mostly mild.
Mild to moderate vomiting is seen in 40% patients and mild diarrhea in 15-20% patients. These
adverse effects are seen usually during the 1st week of treatment. There may be liver-or-kidney-
related side effects like puffiness of the eyes, jaundice or decrease urine. If any of the symptoms are
reported, the patients should be referred to a Level-2 or Level-3 health facility for advice and
treatment. Adverse reactions to Miltefosine are mostly mild. Mild to moderate vomiting is seen in
40% patients and mild diarrhea in 15-20% patients. These usually occur during first week of
treatment.
Duration of treatment of Miltefosine:
Miltefosine should not be given as mono-therapy for kala-azar cases as there is increasing resistance
of the drug used as mono-therapy. This drug should be prescribed as combination with either
Liposomal Amphotericin B or Paromomycin. If Liposomal Amphotericin B is used in combination,
Miltefosine should be prescribed as standard dose from 2nd
day to 8th day, while in combination with
Paromomycin, Miltefosine should be given from day 1 to day 10.
3. PAROMOMYCIN:
Paromomycin is an aminoglycoside antibiotic, used to treat intestinal infections such as
cryptosporidiosis and amoebiasis, and other diseases such as kala-azar. Paromomycin was
demonstrated to be effective against cutaneous leishmaniasis (CL) in clinical studies in the USSR in
the 1960s, and in trials with visceral leishmaniasis (VL) in the early 1990s. The route of
administration is intramuscular injection and in oral in capsule form. Paromomycin topical cream with
or without gentamicin is an effective treatment for ulcerative cutaneous leishmaniasis (according to
the results of a phase-3, randomized, double-blind, parallel group–controlled trial). Sundar S and Jaya
Chakravarty (2008) in their research reported that paromomycin, with its excellent efficacy, low cost,
shorter duration of administration and good safety profile has the potential to be used as a first-line
drug for the treatment of leishmaniasis19
.
Musa AM, et al (2010)conducted a research to investigate the treatment efficacy with paromomycin in
kala-azar patients and documented that at end of treatment (EoT), 85% of patients in the 20
mg/kg/day group and 90% of patients in the 15 mg/kg/day group had parasite clearance. Six months
(6M) after treatment, efficacy was 80.0% and 81.0% in the 20 mg/kg/day and 15 mg/kg/day groups,
respectively20
. There were no serious adverse events. Pharmacokinetic profiles suggested a difference
between the two doses, although numbers of patients recruited were too few to make it significant (n
= 3 in the 20 mg/kg/day and n = 6 in the 15 mg/kg/day groups respectively). Conclusion: Data suggest
that both high dose regimens were more efficacious. The dose of 15 mg/kg sulfate is equivalent to 11
mg/kg of base, and 20 mg/kg sulfate is equivalent to 15 mg/kg of base. A combination therapy of
AmBisome (single dose) and Paromomycin for 10 days with 15 mg/kg/day has been found to be
effective in treating kala-azar cases.
Mild pain at the injection site is the commonest adverse event. Reversible ototoxicity occurs in few
cases. Renal toxicity is rare. Some patients may develop hepatotoxicity, indicated by raised hepatic
19 Sunder S and Chakravarty. Paromomycin in the treatment of leishmaniasis. Banaras Hindu University, Institute of Medical Sciences, Department of Medicine, Varanasi-221005, India. May 2008, Vol. 17, No. 5 , Pages 787-794 20 Musa AM, Younis B, Fadlalla A, et al. Paromomycin for the Treatment of Visceral Leishmaniasis in Sudan: A Randomized, Open-Label, Dose-Finding Study. PloS Neglected Tropical Disease. October 2010, Volume 4, Issue 10, e855
84 | P a g e
enzyme concentration; tetany has also been reported. A topical formulation is available for cutaneous
leishmaniasis.
4. AMPHOTERICIN B DEOXYCHOLATE:
Recommended second line drug for treatment of New Kala-azar and RKA is Amphotericin B
deoxycholate. This drug is also an effective drug. But it has high toxicity profile and thus pushed to
second line. The recommended dose is 1 mg/kg daily or alternate day in the form of intravenous
infusion (in 5% Dextrose solution 500 ml) for 15 doses having a cure rate of ≥90%. A test dose
should be given before administration of Amphotericin B deoxycholate. After preparation of solution,
5 drops/minute for 30 minutes, then 10 drops/minute for another 30 minutes and if there is no reaction
occurs, then the infusion should be given slowly over a period of 4-6 hours.
5. SODIUM STIBOGLUCONATE (SSG)
SSG is an effective and widely used drug for KA and KATF. But the drug is pushed to second line
because of its cardiac toxicity and is recommended by WHO to be phased out gradually. The drug
should be given at a dosage of 20mg/kg body weight, daily IM injection for 30 days. It is essential to
weigh the patient before starting treatment. Clinical cardiac monitoring should be done throughout the
treatment period. The preferred route of administration recommended is by deep intramuscular (IM)
injection. It is better not to give the drug intravenously (IV) to avoid the risk of cardiovascular
collapse.
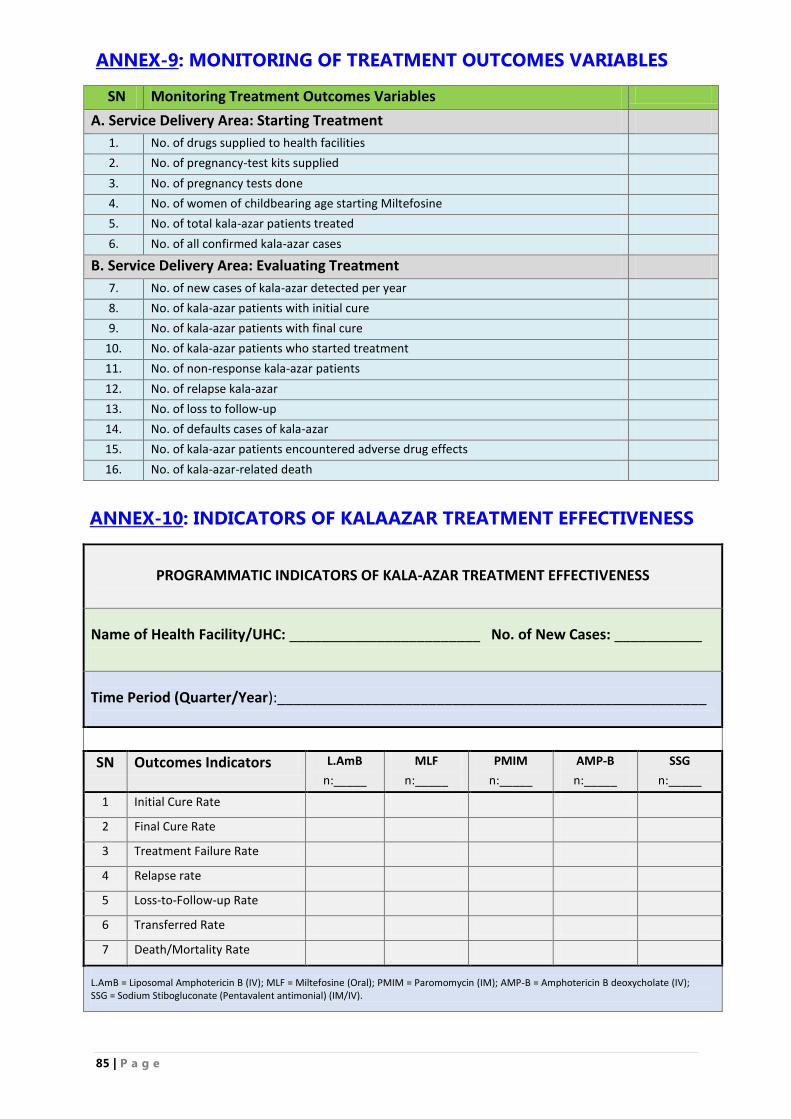
85 | P a g e
ANNEX-9: MONITORING OF TREATMENT OUTCOMES VARIABLES
SN Monitoring Treatment Outcomes Variables
A. Service Delivery Area: Starting Treatment
1. No. of drugs supplied to health facilities
2. No. of pregnancy-test kits supplied
3. No. of pregnancy tests done
4. No. of women of childbearing age starting Miltefosine
5. No. of total kala-azar patients treated
6. No. of all confirmed kala-azar cases
B. Service Delivery Area: Evaluating Treatment
7. No. of new cases of kala-azar detected per year
8. No. of kala-azar patients with initial cure
9. No. of kala-azar patients with final cure
10. No. of kala-azar patients who started treatment
11. No. of non-response kala-azar patients
12. No. of relapse kala-azar
13. No. of loss to follow-up
14. No. of defaults cases of kala-azar
15. No. of kala-azar patients encountered adverse drug effects
16. No. of kala-azar-related death
ANNEX-10: INDICATORS OF KALAAZAR TREATMENT EFFECTIVENESS
PROGRAMMATIC INDICATORS OF KALA-AZAR TREATMENT EFFECTIVENESS
Name of Health Facility/UHC: ________________________ No. of New Cases: ___________
Time Period (Quarter/Year):______________________________________________________
SN Outcomes Indicators L.AmB
n:_____
MLF
n:_____
PMIM
n:_____
AMP-B
n:_____
SSG
n:_____
1 Initial Cure Rate
2 Final Cure Rate
3 Treatment Failure Rate
4 Relapse rate
5 Loss-to-Follow-up Rate
6 Transferred Rate
7 Death/Mortality Rate
L.AmB = Liposomal Amphotericin B (IV); MLF = Miltefosine (Oral); PMIM = Paromomycin (IM); AMP-B = Amphotericin B deoxycholate (IV); SSG = Sodium Stibogluconate (Pentavalent antimonial) (IM/IV).
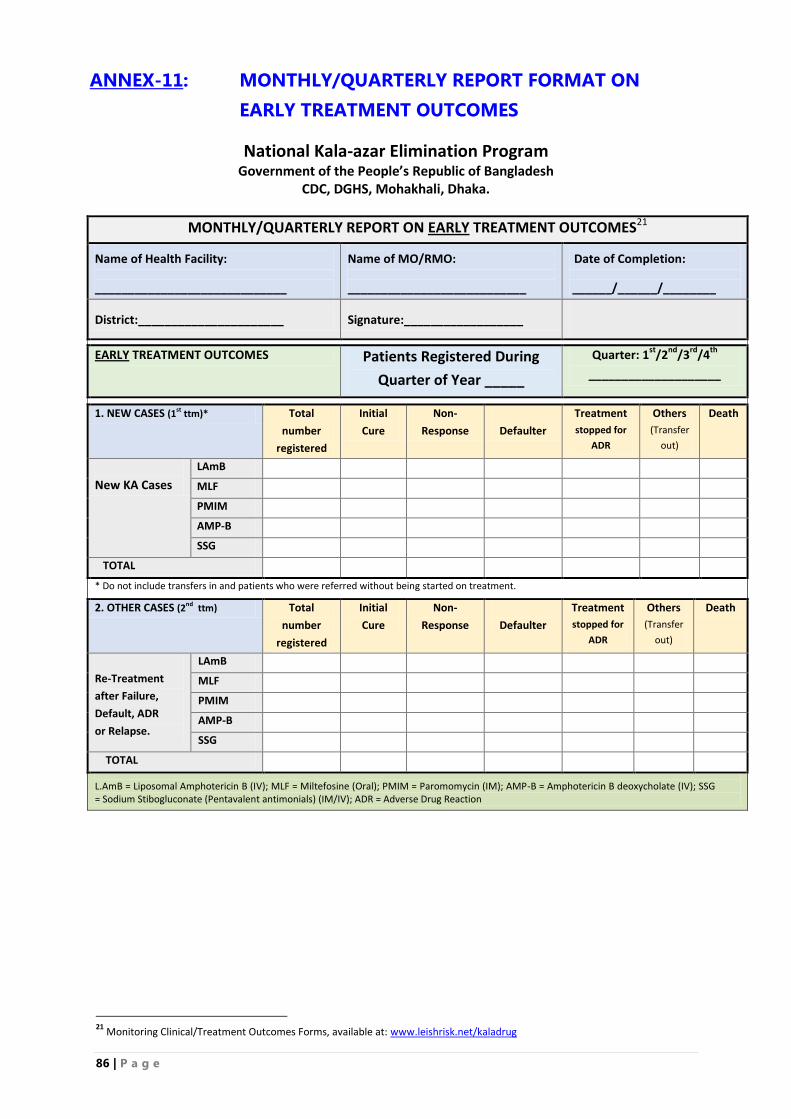
86 | P a g e
ANNEX-11: MONTHLY/QUARTERLY REPORT FORMAT ON
EARLY TREATMENT OUTCOMES
National Kala-azar Elimination Program Government of the People’s Republic of Bangladesh
CDC, DGHS, Mohakhali, Dhaka.
MONTHLY/QUARTERLY REPORT ON EARLY TREATMENT OUTCOMES21
Name of Health Facility:
_____________________________
Name of MO/RMO:
___________________________
Date of Completion:
______/______/________
District:______________________
Signature:__________________
EARLY TREATMENT OUTCOMES Patients Registered During
Quarter of Year _____
Quarter: 1st
/2nd
/3rd
/4th
____________________
1. NEW CASES (1st ttm)* Total
number
registered
Initial
Cure
Non-
Response
Defaulter
Treatment
stopped for
ADR
Others
(Transfer
out)
Death
New KA Cases
LAmB
MLF
PMIM
AMP-B
SSG
TOTAL
* Do not include transfers in and patients who were referred without being started on treatment.
2. OTHER CASES (2nd ttm) Total
number
registered
Initial
Cure
Non-
Response
Defaulter
Treatment
stopped for
ADR
Others
(Transfer
out)
Death
Re-Treatment
after Failure,
Default, ADR
or Relapse.
LAmB
MLF
PMIM
AMP-B
SSG
TOTAL
L.AmB = Liposomal Amphotericin B (IV); MLF = Miltefosine (Oral); PMIM = Paromomycin (IM); AMP-B = Amphotericin B deoxycholate (IV); SSG = Sodium Stibogluconate (Pentavalent antimonials) (IM/IV); ADR = Adverse Drug Reaction
21
Monitoring Clinical/Treatment Outcomes Forms, available at: www.leishrisk.net/kaladrug
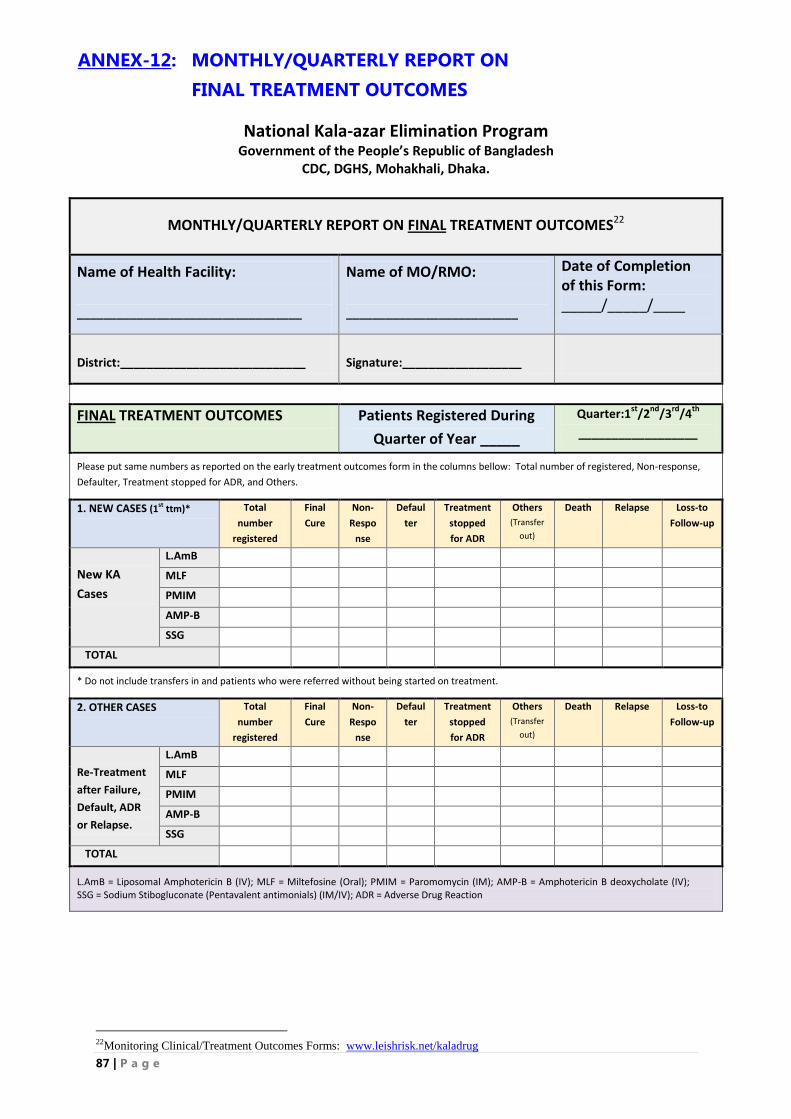
87 | P a g e
ANNEX-12: MONTHLY/QUARTERLY REPORT ON
FINAL TREATMENT OUTCOMES
National Kala-azar Elimination Program Government of the People’s Republic of Bangladesh
CDC, DGHS, Mohakhali, Dhaka.
MONTHLY/QUARTERLY REPORT ON FINAL TREATMENT OUTCOMES22
Name of Health Facility:
__________________________________
Name of MO/RMO:
__________________________
Date of Completion of this Form: _____/_____/____
District:____________________________
Signature:__________________
FINAL TREATMENT OUTCOMES Patients Registered During
Quarter of Year _____
Quarter:1st
/2nd
/3rd
/4th
__________________
Please put same numbers as reported on the early treatment outcomes form in the columns bellow: Total number of registered, Non-response,
Defaulter, Treatment stopped for ADR, and Others.
1. NEW CASES (1st ttm)* Total
number
registered
Final
Cure
Non-
Respo
nse
Defaul
ter
Treatment
stopped
for ADR
Others
(Transfer
out)
Death Relapse Loss-to
Follow-up
New KA
Cases
L.AmB
MLF
PMIM
AMP-B
SSG
TOTAL
* Do not include transfers in and patients who were referred without being started on treatment.
2. OTHER CASES Total
number
registered
Final
Cure
Non-
Respo
nse
Defaul
ter
Treatment
stopped
for ADR
Others
(Transfer
out)
Death Relapse Loss-to
Follow-up
Re-Treatment
after Failure,
Default, ADR
or Relapse.
L.AmB
MLF
PMIM
AMP-B
SSG
TOTAL
L.AmB = Liposomal Amphotericin B (IV); MLF = Miltefosine (Oral); PMIM = Paromomycin (IM); AMP-B = Amphotericin B deoxycholate (IV); SSG = Sodium Stibogluconate (Pentavalent antimonials) (IM/IV); ADR = Adverse Drug Reaction
22Monitoring Clinical/Treatment Outcomes Forms: www.leishrisk.net/kaladrug
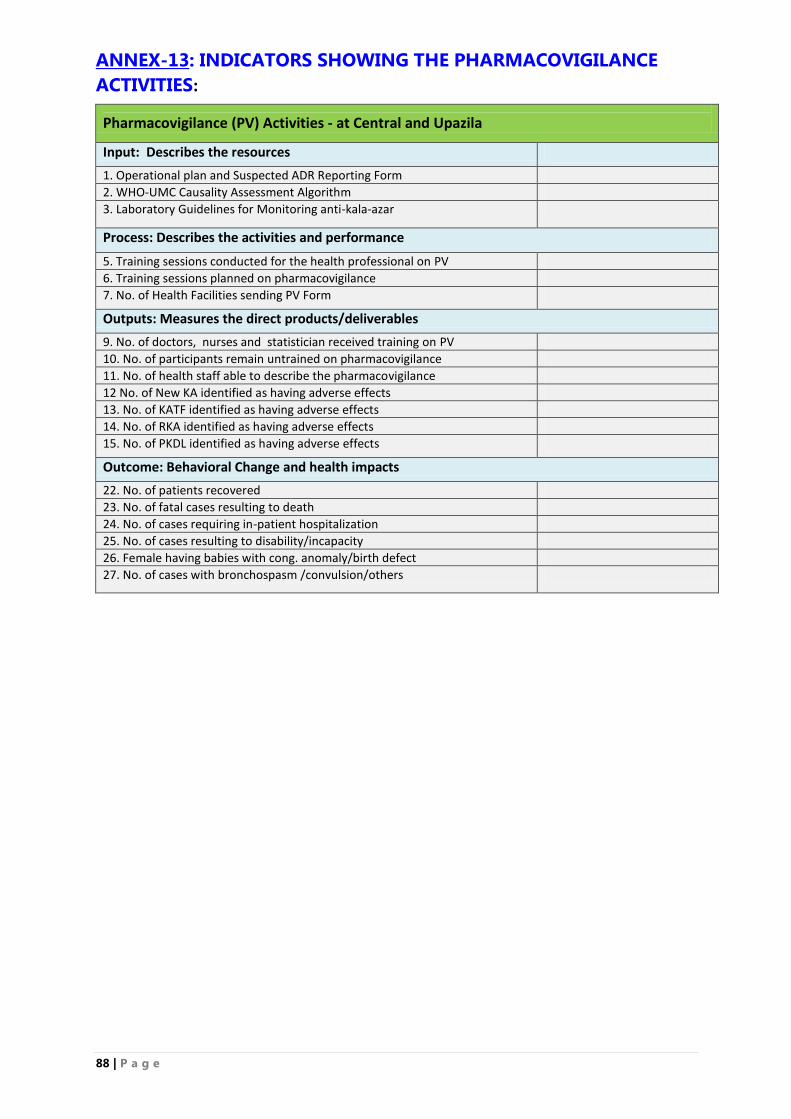
88 | P a g e
ANNEX-13: INDICATORS SHOWING THE PHARMACOVIGILANCE
ACTIVITIES:
Pharmacovigilance (PV) Activities - at Central and Upazila
Input: Describes the resources
1. Operational plan and Suspected ADR Reporting Form
2. WHO-UMC Causality Assessment Algorithm
3. Laboratory Guidelines for Monitoring anti-kala-azar
Process: Describes the activities and performance
5. Training sessions conducted for the health professional on PV
6. Training sessions planned on pharmacovigilance
7. No. of Health Facilities sending PV Form
Outputs: Measures the direct products/deliverables
9. No. of doctors, nurses and statistician received training on PV
10. No. of participants remain untrained on pharmacovigilance
11. No. of health staff able to describe the pharmacovigilance
12 No. of New KA identified as having adverse effects
13. No. of KATF identified as having adverse effects
14. No. of RKA identified as having adverse effects
15. No. of PKDL identified as having adverse effects
Outcome: Behavioral Change and health impacts
22. No. of patients recovered
23. No. of fatal cases resulting to death
24. No. of cases requiring in-patient hospitalization
25. No. of cases resulting to disability/incapacity
26. Female having babies with cong. anomaly/birth defect
27. No. of cases with bronchospasm /convulsion/others
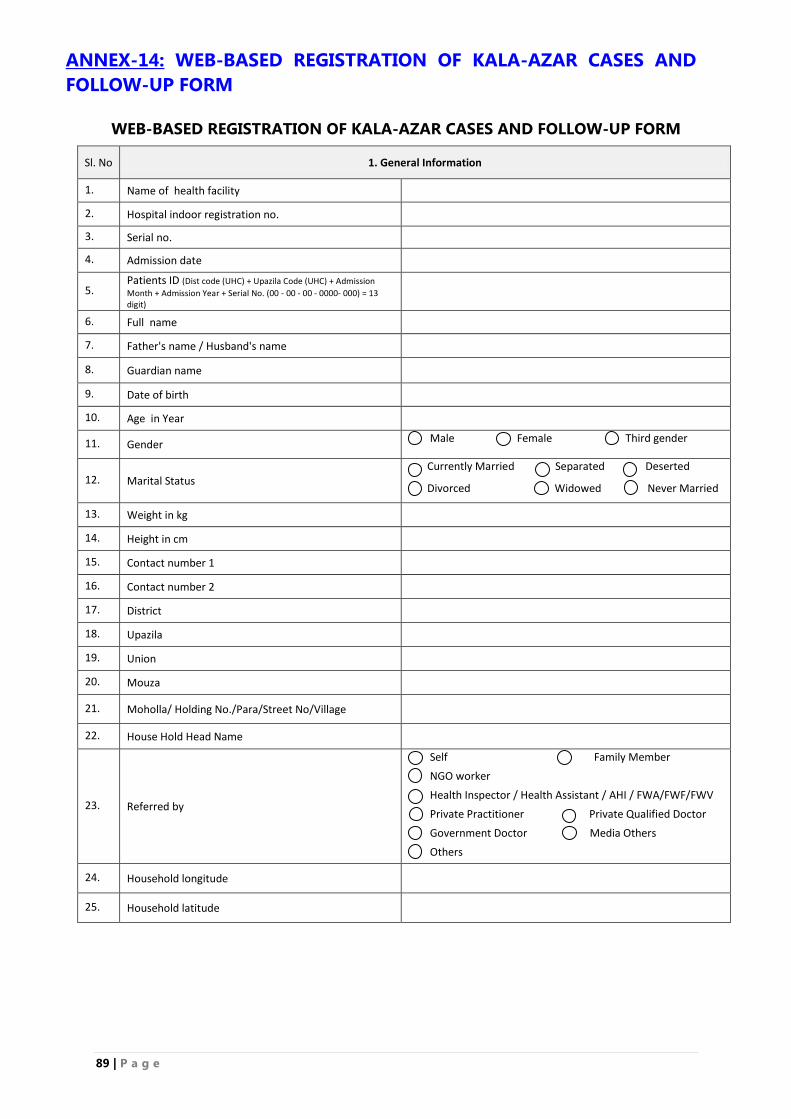
89 | P a g e
ANNEX-14: WEB-BASED REGISTRATION OF KALA-AZAR CASES AND
FOLLOW-UP FORM
WEB-BASED REGISTRATION OF KALA-AZAR CASES AND FOLLOW-UP FORM
Sl. No 1. General Information
1. Name of health facility
2. Hospital indoor registration no.
3. Serial no.
4. Admission date
5. Patients ID (Dist code (UHC) + Upazila Code (UHC) + Admission
Month + Admission Year + Serial No. (00 - 00 - 00 - 0000- 000) = 13 digit)
6. Full name
7. Father's name / Husband's name
8. Guardian name
9. Date of birth
10. Age in Year
11. Gender Male Female Third gender
12. Marital Status Currently Married Separated Deserted
Divorced Widowed Never Married
13. Weight in kg
14. Height in cm
15. Contact number 1
16. Contact number 2
17. District
18. Upazila
19. Union
20. Mouza
21. Moholla/ Holding No./Para/Street No/Village
22. House Hold Head Name
23. Referred by
Self Family Member
NGO worker
Health Inspector / Health Assistant / AHI / FWA/FWF/FWV
Private Practitioner Private Qualified Doctor
Government Doctor Media Others
Others
24. Household longitude
25. Household latitude
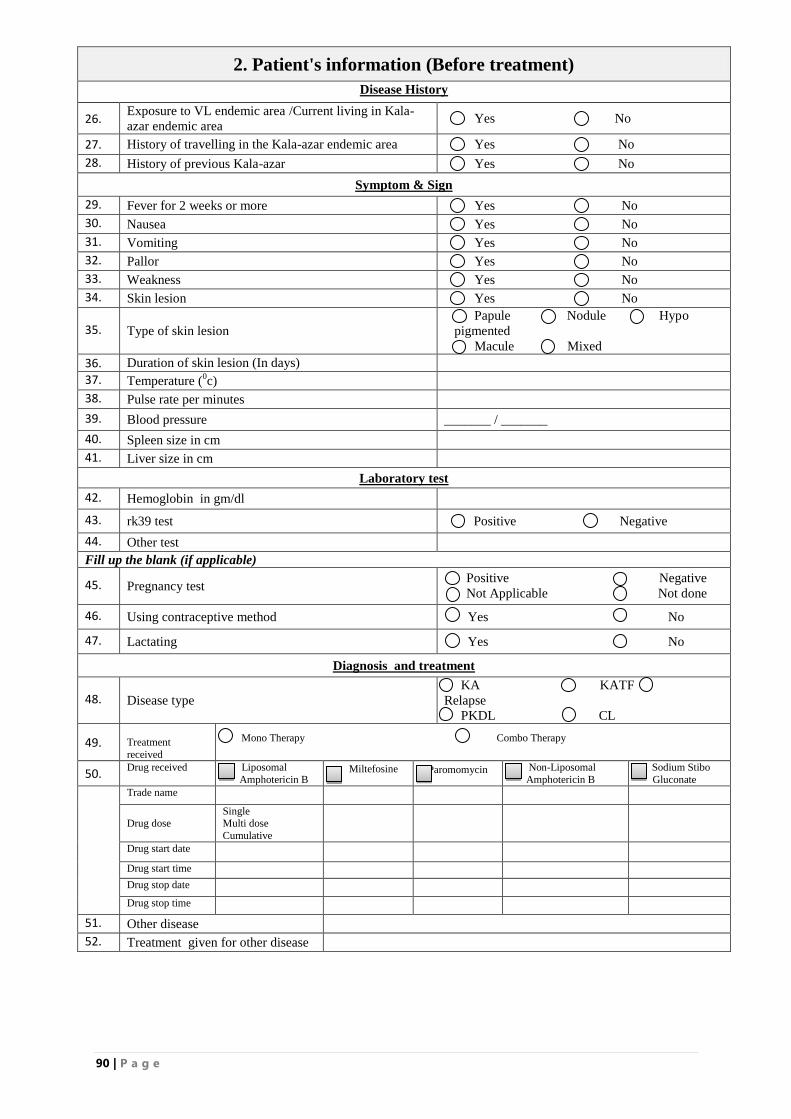
90 | P a g e
2. Patient's information (Before treatment)
Disease History
26. Exposure to VL endemic area /Current living in Kala-
azar endemic area Yes No
27. History of travelling in the Kala-azar endemic area Yes No
28. History of previous Kala-azar Yes No
Symptom & Sign
29. Fever for 2 weeks or more Yes No
30. Nausea Yes No
31. Vomiting Yes No
32. Pallor Yes No
33. Weakness Yes No
34. Skin lesion Yes No
35. Type of skin lesion
Papule Nodule Hypo
pigmented
Macule Mixed
36. Duration of skin lesion (In days)
37. Temperature (0c)
38. Pulse rate per minutes
39. Blood pressure _______ / _______
40. Spleen size in cm
41. Liver size in cm
Laboratory test
42. Hemoglobin in gm/dl
43. rk39 test Positive Negative
44. Other test
Fill up the blank (if applicable)
45. Pregnancy test Positive Negative
Not Applicable Not done
46. Using contraceptive method Yes No
47. Lactating Yes No
Diagnosis and treatment
48. Disease type
KA KATF
Relapse
PKDL CL
49.
Treatment
received
Mono Therapy Combo Therapy
50. Drug received
Liposomal
Amphotericin B Miltefosine Paromomycin Non-Liposomal
Amphotericin B
Sodium Stibo
Gluconate
Trade name
Drug dose Single Multi dose
Cumulative
Drug start date
Drug start time
Drug stop date
Drug stop time
51. Other disease
52. Treatment given for other disease
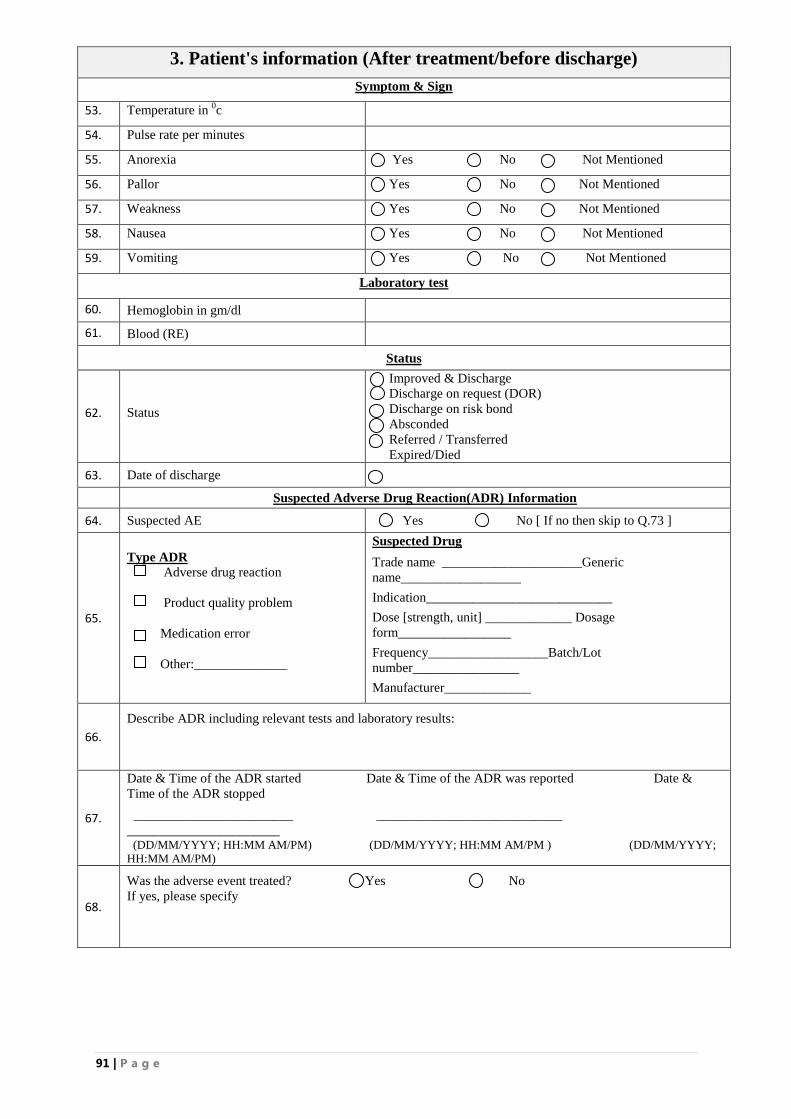
91 | P a g e
3. Patient's information (After treatment/before discharge)
Symptom & Sign
53. Temperature in 0c
54. Pulse rate per minutes
55. Anorexia Yes No Not Mentioned
56. Pallor Yes No Not Mentioned
57. Weakness Yes No Not Mentioned
58. Nausea Yes No Not Mentioned
59. Vomiting Yes No Not Mentioned
Laboratory test
60. Hemoglobin in gm/dl
61. Blood (RE)
Status
62. Status
Improved & Discharge
Discharge on request (DOR)
Discharge on risk bond
Absconded
Referred / Transferred
Expired/Died
63. Date of discharge
Suspected Adverse Drug Reaction(ADR) Information
64. Suspected AE Yes No [ If no then skip to Q.73 ]
65.
Type ADR
Adverse drug reaction
Product quality problem
Medication error
Other:______________
Suspected Drug
Trade name _____________________Generic
name__________________
Indication____________________________
Dose [strength, unit] _____________ Dosage
form_________________
Frequency__________________Batch/Lot
number________________
Manufacturer_____________
66.
Describe ADR including relevant tests and laboratory results:
67.
Date & Time of the ADR started Date & Time of the ADR was reported Date &
Time of the ADR stopped
________________________ ____________________________
_______________________ (DD/MM/YYYY; HH:MM AM/PM) (DD/MM/YYYY; HH:MM AM/PM ) (DD/MM/YYYY;
HH:MM AM/PM)
68.
Was the adverse event treated? Yes No
If yes, please specify
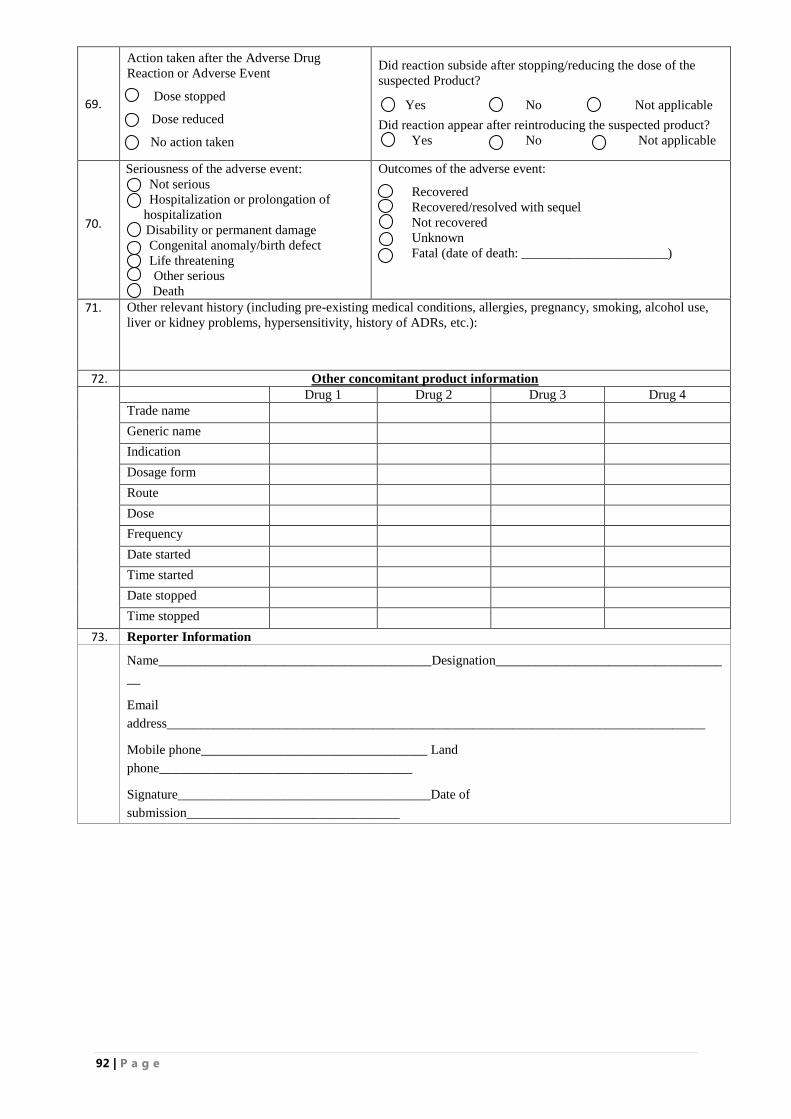
92 | P a g e
69.
Action taken after the Adverse Drug
Reaction or Adverse Event
Dose stopped
[ Dose reduced
No action taken
Did reaction subside after stopping/reducing the dose of the
suspected Product?
Yes No Not applicable
Did reaction appear after reintroducing the suspected product?
Yes No Not applicable
70.
Seriousness of the adverse event:
Not serious
Hospitalization or prolongation of
hospitalization
Disability or permanent damage
Congenital anomaly/birth defect
Life threatening
Other serious
Death
Outcomes of the adverse event:
Recovered
Recovered/resolved with sequel
Not recovered
Unknown
Fatal (date of death: ______________________)
71. Other relevant history (including pre-existing medical conditions, allergies, pregnancy, smoking, alcohol use,
liver or kidney problems, hypersensitivity, history of ADRs, etc.):
72. Other concomitant product information
Drug 1 Drug 2 Drug 3 Drug 4
Trade name
Generic name
Indication
Dosage form
Route
Dose
Frequency
Date started
Time started
Date stopped
Time stopped
73. Reporter Information
Name_________________________________________Designation__________________________________
__
address_________________________________________________________________________________
Mobile phone__________________________________ Land
phone______________________________________
Signature______________________________________Date of
submission________________________________
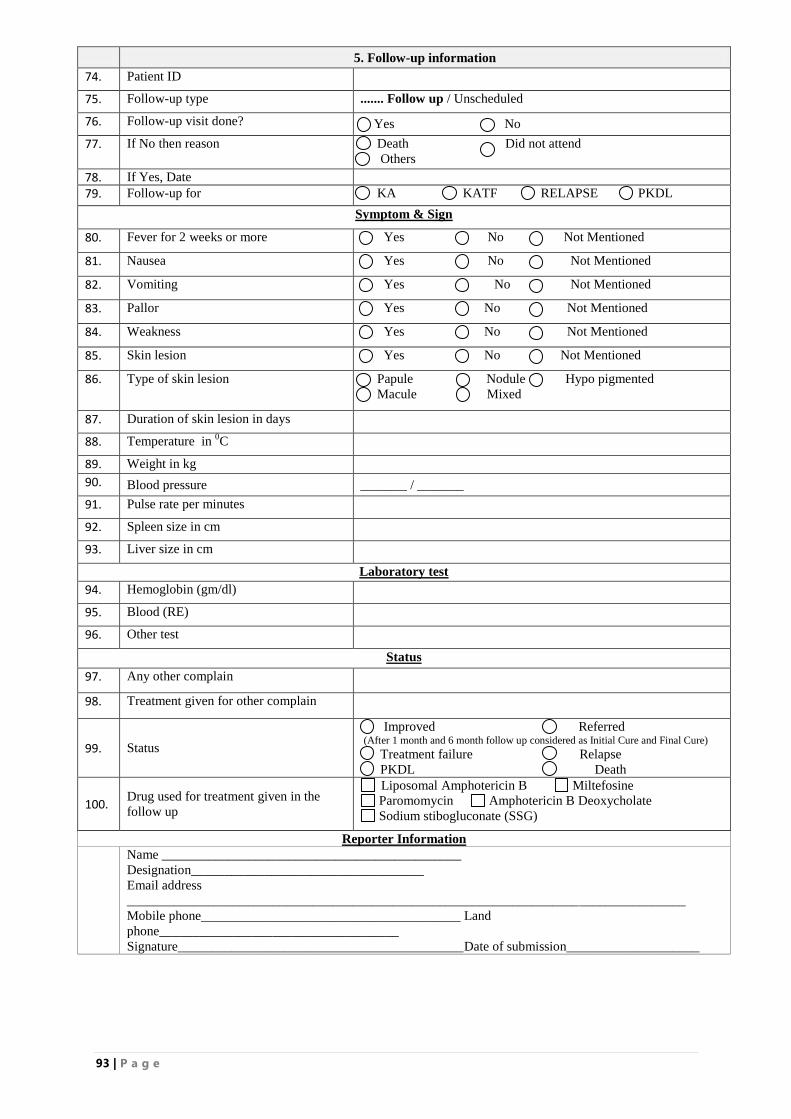
93 | P a g e
5. Follow-up information
74. Patient ID
75. Follow-up type ....... Follow up / Unscheduled
76. Follow-up visit done? Yes No
77. If No then reason Death Did not attend
Others
78. If Yes, Date
79. Follow-up for KA KATF RELAPSE PKDL
Symptom & Sign
80. Fever for 2 weeks or more Yes No Not Mentioned
81. Nausea Yes No Not Mentioned
82. Vomiting Yes No Not Mentioned
83. Pallor Yes No Not Mentioned
84. Weakness Yes No Not Mentioned
85. Skin lesion Yes No Not Mentioned
86. Type of skin lesion
Papule Nodule Hypo pigmented
Macule Mixed
87. Duration of skin lesion in days
88. Temperature in 0C
89. Weight in kg
90. Blood pressure _______ / _______
91. Pulse rate per minutes
92. Spleen size in cm
93. Liver size in cm
Laboratory test
94. Hemoglobin (gm/dl)
95. Blood (RE)
96. Other test
Status
97. Any other complain
98. Treatment given for other complain
99. Status
Improved Referred (After 1 month and 6 month follow up considered as Initial Cure and Final Cure) Treatment failure Relapse
PKDL Death
100. Drug used for treatment given in the
follow up
Liposomal Amphotericin B Miltefosine
Paromomycin Amphotericin B Deoxycholate
Sodium stibogluconate (SSG)
Reporter Information
Name _____________________________________________
Designation___________________________________
Email address
____________________________________________________________________________________
Mobile phone_______________________________________ Land
phone____________________________________
Signature___________________________________________Date of submission____________________
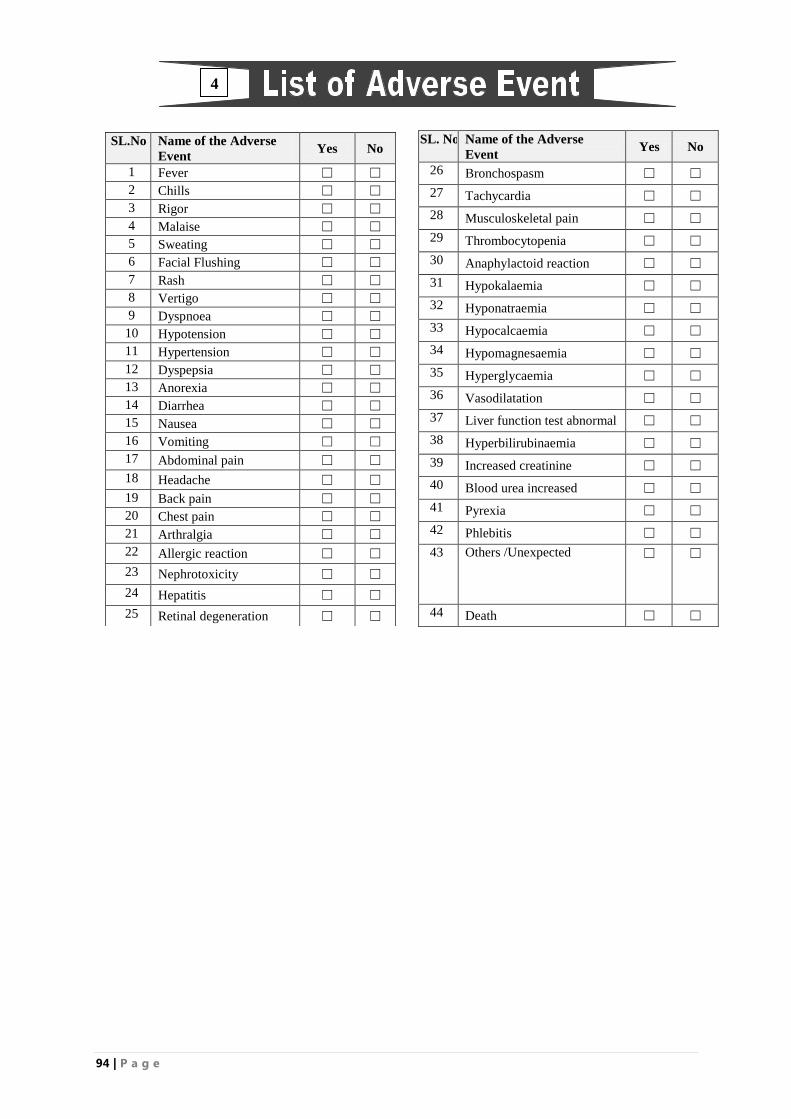
94 | P a g e
SL.No Name of the Adverse
Event Yes No
1 Fever ☐ ☐
2 Chills ☐ ☐
3 Rigor ☐ ☐
4 Malaise ☐ ☐
5 Sweating ☐ ☐
6 Facial Flushing ☐ ☐
7 Rash ☐ ☐
8 Vertigo ☐ ☐
9 Dyspnoea ☐ ☐
10 Hypotension ☐ ☐
11 Hypertension ☐ ☐
12 Dyspepsia ☐ ☐
13 Anorexia ☐ ☐
14 Diarrhea ☐ ☐
15 Nausea ☐ ☐
16 Vomiting ☐ ☐
17 Abdominal pain ☐ ☐
18 Headache ☐ ☐
19 Back pain ☐ ☐
20 Chest pain ☐ ☐
21 Arthralgia ☐ ☐
22 Allergic reaction ☐ ☐
23 Nephrotoxicity ☐ ☐
24 Hepatitis ☐ ☐
25 Retinal degeneration ☐ ☐
SL. No Name of the Adverse
Event Yes No
26 Bronchospasm ☐ ☐
27 Tachycardia ☐ ☐
28 Musculoskeletal pain ☐ ☐
29 Thrombocytopenia ☐ ☐
30 Anaphylactoid reaction ☐ ☐
31 Hypokalaemia ☐ ☐
32 Hyponatraemia ☐ ☐
33 Hypocalcaemia ☐ ☐
34 Hypomagnesaemia ☐ ☐
35 Hyperglycaemia ☐ ☐
36 Vasodilatation ☐ ☐
37 Liver function test abnormal ☐ ☐
38 Hyperbilirubinaemia ☐ ☐
39 Increased creatinine ☐ ☐
40 Blood urea increased ☐ ☐
41 Pyrexia ☐ ☐
42 Phlebitis ☐ ☐
43 Others /Unexpected ☐ ☐
44 Death ☐ ☐
4
95 | P a g e
ANNEX-15: SOP OF AMBISOME
Standard Operating Procedure (SOP) of
AmBisome DESCRIPTION
AmBisome for Injection is a sterile, non-pyrogenic lyophilized product for intravenous infusion. Each
vial contains 50 mg of amphotericin B, USP, intercalated into a liposomal membrane consisting of
approximately 213 mg hydrogenated soy phosphatidylcholine; 52 mg cholesterol, NF; 84 mg
Distearoyl phosphatidyl glycerol; 0.64 mg alpha tocopherol, USP; together with 900 mg sucrose, NF;
and 27 mg disodium succinate hexahydrate as buffer. Following reconstitution with Sterile Water for
Injection, USP and the resulting pH of the suspension is between 5-6.
Mechanism of Action:
The active ingredient of AmBisome acts by binding to the sterol component, ergosterol of the cell
membrane of susceptible fungi. By forming a trans-membrane channel it leads to alterations in cell
permeability which causes leak out of monovalent ions (Na+, K+, H+ and Cl+) from the cell and
finally causes cell death. Amphotericin B has higher affinity for the ergosterol component of the
fungal cell membrane and also binds with cholesterol component of the mammalian cell leading to the
cytotoxicity. The liposomal preparation of Amphotericin B (AmBisome) has been shown to penetrate
the cell wall of both extracellular and intracellular forms of susceptible fungi.
Adverse effects:
AmBisome is well tolerated. AmBisome has a lower incidence of chills, hypertension, hypotension,
tachycardia, hypoxia, hypokalemia, and various events related to decreased kidney function as
compared to Amphotericin B deoxycholate. There have been a few reports of flushing, back pain with
or without chest tightness, and chest pain associated with AmBisome administration; on occasion this
has been severe. Where these symptoms noted, the reaction developed within a few minutes after the
start of infusion and disappeared rapidly when the infusion is stopped. The symptoms do not occur
with every dose and usually do not recur on subsequent administrations when the infusion rate is
slowed.
Infusion Related Reactions
In Study 94-0-002, the large, double-blind study of pediatric and adult febrile neutropenic patients, no
premedication to prevent infusion related reaction was administered prior to the first dose of study
drug (Day 1). AmBisome-treated patients had a lower incidence of infusion related fever (17% versus
44%), chills/rigors (18% versus 54%) and vomiting (6% versus 8%) on Day 1 as compared to
Amphotericin B deoxycholate-treated patients.
Contraindications:
AmBisome is contraindicated in those patients who have demonstrated or have known
hypersensitivity to Amphotericin B deoxycholate or any other constituents of the product unless, in
the opinion of the treating physician, the benefit of therapy outweighs the risk.
Administration of AmBisome
Objective of SOP: To administer single dose intravenous AmBisome accurately and with proper
aseptic precaution.
Materials required:
1. A pair of disposable hand gloves.
2. Disposable IV cannula of appropriate size.
3. Ball of cotton.
4. Chlorohexidine / 70% isopropyl alcohol/ spirit.
96 | P a g e
5. Micropore 2 inches.
6. Disposable infusion set.
7. Saline stand.
8. A 10 ml syringe containing test dose of AmBisome 1 mg (0.25 of dissolved AmBisome with
distilled water) prepared according to SOP for AmBisome preparation.
9. Measured Total dose of AmBisome diluted in 5% DA prepared according to SOP guideline.
Procedure:
1. Explain the procedure to the patient and give assurance that it is a very simple procedure.
2. Patient should be lying on bed with the head on a soft pillow.
3. Wash your hands with soap and water vigorously before preparation.
4. Take proper aseptic precaution.
5. Wear a pair of gloves.
6. Bind the tourniquet in the arm of the patient to make the cubital vein prominent.
7. Take a ball of cotton soaked with chlorohexidine and gently rub the site of injection.
8. Wait until it is dried up.
9. Take the IV canula and prick the vein and ensure that it is placed in the vein.
10. Fix the canula with micropore.
11. Take the syringe loaded with the test dose of AmBisome as described above.
12. Start pushing the plunger very slowly and give the whole 10ml of test dose AmBisome in 10
minutes through i.v. canula.
13. Look for any hypersensitivity reaction.
14. If any hypersensitivity reaction occurs then give:
a. Tab. Chlorpheniramine 4mg in Adult and 0.1-0.2mg/kg body weight in children orally
(maximum 4mg per dose).
b. Tab. Paracetamol (500mg ) in Adult and 15-20mg/g body weight in Children orally.
15. If the symptoms do not disappear, then call the duty / study physician.
16. If there is any evidence of hypersensitivity reaction the patient should not be given the
AmBisome infusion.
17. After finishing the test dose wait for 30 minutes and closely observe the patient for any
adverse drug reaction.
18. If there are no symptoms or signs of hypersensitivity reaction after 30 minutes then take a
disposable infusion set and fix it with the bottle/pack containing Measured Total dose of
AmBisome diluted in 5% DA (please see SOP for preparation of AmBisome and the table for
calculation of AmBisome)
19. Label the bottle/pack with patient‟s initial and ID, time of starting and drops per minutes to be
infused.
20. Give oral premedication with paracetamol 10mg/kg and Chlorpheniramine 0.1-0.2 mg/kg
(maximum 4 mg per dose)
21. Measure vital parameter (respiratory rate, blood pressure, pulse) before the start of infusion.
22. Start the IV channel very slowly initially.
23. Then calculate the drops per minute to give the whole volume in a period of 3-4 hours.
24. Observe the patient closely for any adverse drug reaction for 30 minutes.
25. Discard all the sharp instruments in Red colored waste disposal container.
26. Discard all the soft materials in the yellow colored waste disposal container.
27. Monitor vital parameters at one hour after infusion, at the end of infusion and one hour later
after completion of infusion.
Responsible person: Trained Staff nurse of Upazila Health complex is responsible for the task but
the whole procedure should be in close observation by hospital duty physician.
Applicability to other SOP: This SOP is applicable to the SOP for preparation and calculation of
AmBisome.

97 | P a g e
Glossary/ Definition:
1. IV- Intravenous
2. 5% DA- 5% dextrose in aqua
3. Kg- Kilogram
4. Ml- Milliliter
Reference:
Leaflet provided with the AmBisome vial
Glossary/ Definition:
5. 5% DA: 5% dextrose in aqua
6. Kg: Kilogram
7. Ml: Milliliter
8. UHC: Upazila Health Complex
9. Icddr,b: International Centre For Diarrheal Disease Research, Bangladesh
Reference:
Leaflet provided with the AmBisome vial
Guideline provided by Scientist Shyam Sundar
SOP used in AmBisome preparation in trial in India
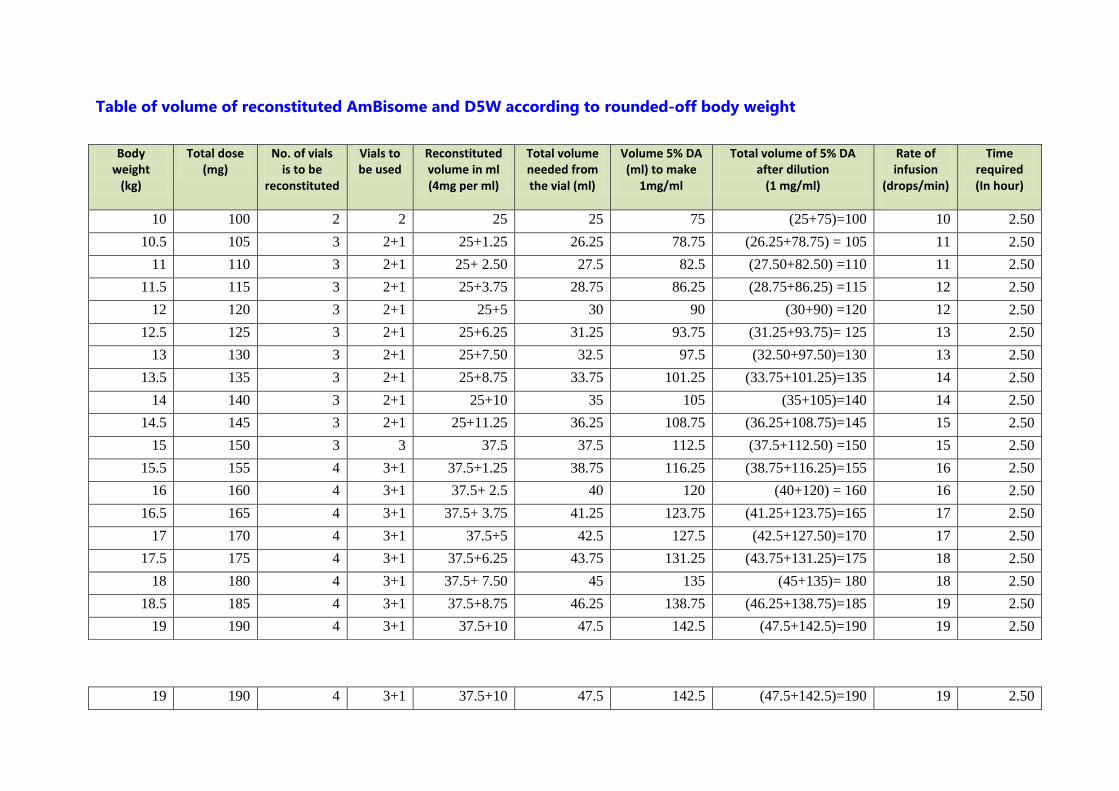
Table of volume of reconstituted AmBisome and D5W according to rounded-off body weight
Body weight
(kg)
Total dose (mg)
No. of vials is to be
reconstituted
Vials to be used
Reconstituted volume in ml (4mg per ml)
Total volume needed from the vial (ml)
Volume 5% DA (ml) to make
1mg/ml
Total volume of 5% DA after dilution
(1 mg/ml)
Rate of infusion
(drops/min)
Time required (In hour)
10 100 2 2 25 25 75 (25+75)=100 10 2.50
10.5 105 3 2+1 25+1.25 26.25 78.75 (26.25+78.75) = 105 11 2.50
11 110 3 2+1 25+ 2.50 27.5 82.5 (27.50+82.50) =110 11 2.50
11.5 115 3 2+1 25+3.75 28.75 86.25 (28.75+86.25) =115 12 2.50
12 120 3 2+1 25+5 30 90 (30+90) =120 12 2.50
12.5 125 3 2+1 25+6.25 31.25 93.75 (31.25+93.75)= 125 13 2.50
13 130 3 2+1 25+7.50 32.5 97.5 (32.50+97.50)=130 13 2.50
13.5 135 3 2+1 25+8.75 33.75 101.25 (33.75+101.25)=135 14 2.50
14 140 3 2+1 25+10 35 105 (35+105)=140 14 2.50
14.5 145 3 2+1 25+11.25 36.25 108.75 (36.25+108.75)=145 15 2.50
15 150 3 3 37.5 37.5 112.5 (37.5+112.50) =150 15 2.50
15.5 155 4 3+1 37.5+1.25 38.75 116.25 (38.75+116.25)=155 16 2.50
16 160 4 3+1 37.5+ 2.5 40 120 (40+120) = 160 16 2.50
16.5 165 4 3+1 37.5+ 3.75 41.25 123.75 (41.25+123.75)=165 17 2.50
17 170 4 3+1 37.5+5 42.5 127.5 (42.5+127.50)=170 17 2.50
17.5 175 4 3+1 37.5+6.25 43.75 131.25 (43.75+131.25)=175 18 2.50
18 180 4 3+1 37.5+ 7.50 45 135 (45+135)= 180 18 2.50
18.5 185 4 3+1 37.5+8.75 46.25 138.75 (46.25+138.75)=185 19 2.50
19 190 4 3+1 37.5+10 47.5 142.5 (47.5+142.5)=190 19 2.50
19 190 4 3+1 37.5+10 47.5 142.5 (47.5+142.5)=190 19 2.50
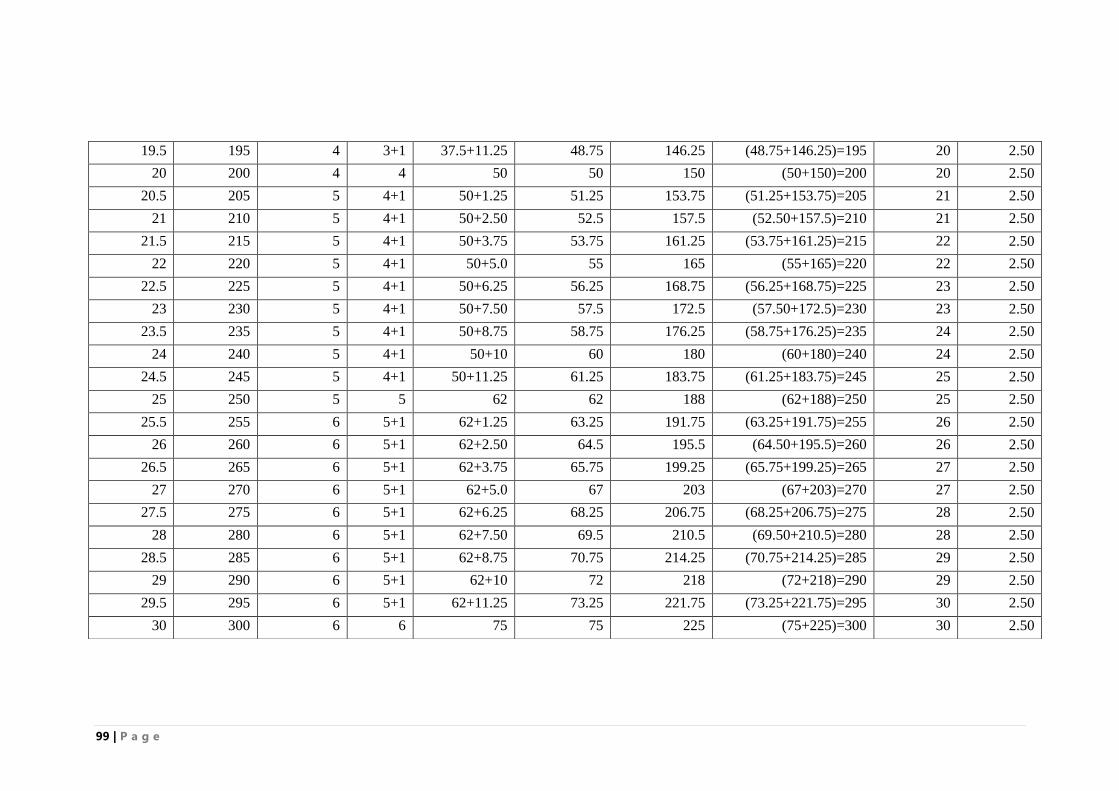
99 | P a g e
19.5 195 4 3+1 37.5+11.25 48.75 146.25 (48.75+146.25)=195 20 2.50
20 200 4 4 50 50 150 (50+150)=200 20 2.50
20.5 205 5 4+1 50+1.25 51.25 153.75 (51.25+153.75)=205 21 2.50
21 210 5 4+1 50+2.50 52.5 157.5 (52.50+157.5)=210 21 2.50
21.5 215 5 4+1 50+3.75 53.75 161.25 (53.75+161.25)=215 22 2.50
22 220 5 4+1 50+5.0 55 165 (55+165)=220 22 2.50
22.5 225 5 4+1 50+6.25 56.25 168.75 (56.25+168.75)=225 23 2.50
23 230 5 4+1 50+7.50 57.5 172.5 (57.50+172.5)=230 23 2.50
23.5 235 5 4+1 50+8.75 58.75 176.25 (58.75+176.25)=235 24 2.50
24 240 5 4+1 50+10 60 180 (60+180)=240 24 2.50
24.5 245 5 4+1 50+11.25 61.25 183.75 (61.25+183.75)=245 25 2.50
25 250 5 5 62 62 188 (62+188)=250 25 2.50
25.5 255 6 5+1 62+1.25 63.25 191.75 (63.25+191.75)=255 26 2.50
26 260 6 5+1 62+2.50 64.5 195.5 (64.50+195.5)=260 26 2.50
26.5 265 6 5+1 62+3.75 65.75 199.25 (65.75+199.25)=265 27 2.50
27 270 6 5+1 62+5.0 67 203 (67+203)=270 27 2.50
27.5 275 6 5+1 62+6.25 68.25 206.75 (68.25+206.75)=275 28 2.50
28 280 6 5+1 62+7.50 69.5 210.5 (69.50+210.5)=280 28 2.50
28.5 285 6 5+1 62+8.75 70.75 214.25 (70.75+214.25)=285 29 2.50
29 290 6 5+1 62+10 72 218 (72+218)=290 29 2.50
29.5 295 6 5+1 62+11.25 73.25 221.75 (73.25+221.75)=295 30 2.50
30 300 6 6 75 75 225 (75+225)=300 30 2.50
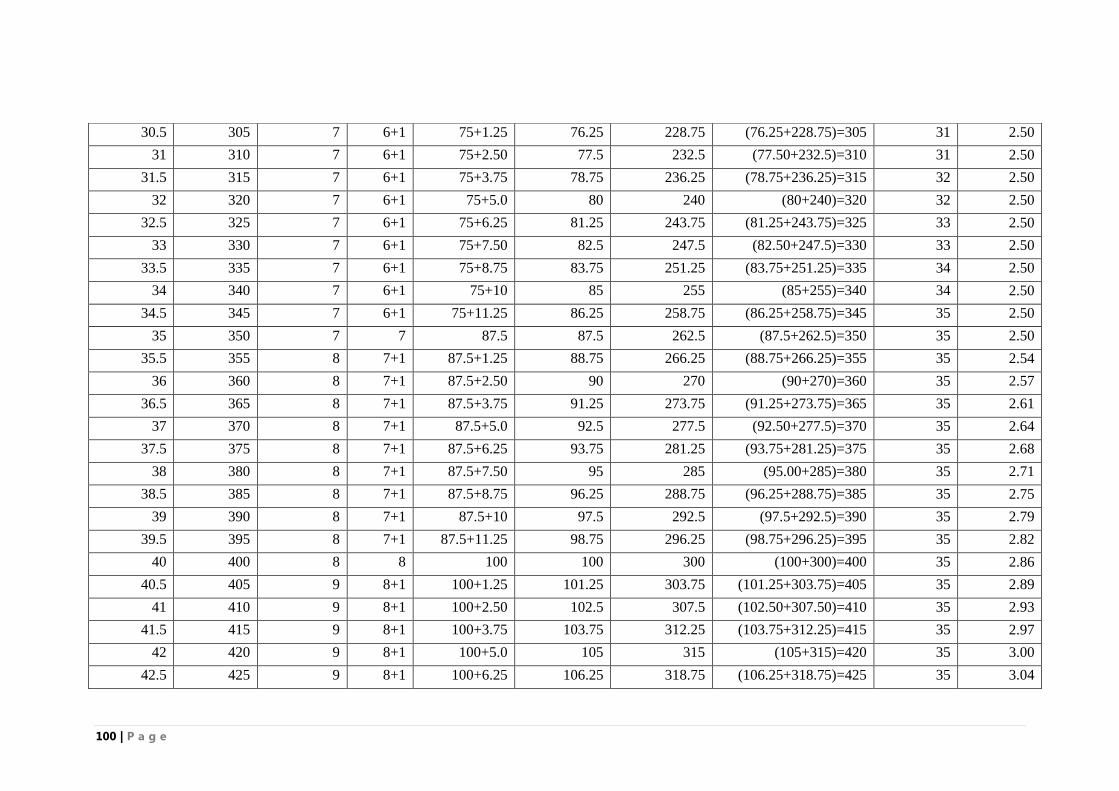
100 | P a g e
30.5 305 7 6+1 75+1.25 76.25 228.75 (76.25+228.75)=305 31 2.50
31 310 7 6+1 75+2.50 77.5 232.5 (77.50+232.5)=310 31 2.50
31.5 315 7 6+1 75+3.75 78.75 236.25 (78.75+236.25)=315 32 2.50
32 320 7 6+1 75+5.0 80 240 (80+240)=320 32 2.50
32.5 325 7 6+1 75+6.25 81.25 243.75 (81.25+243.75)=325 33 2.50
33 330 7 6+1 75+7.50 82.5 247.5 (82.50+247.5)=330 33 2.50
33.5 335 7 6+1 75+8.75 83.75 251.25 (83.75+251.25)=335 34 2.50
34 340 7 6+1 75+10 85 255 (85+255)=340 34 2.50
34.5 345 7 6+1 75+11.25 86.25 258.75 (86.25+258.75)=345 35 2.50
35 350 7 7 87.5 87.5 262.5 (87.5+262.5)=350 35 2.50
35.5 355 8 7+1 87.5+1.25 88.75 266.25 (88.75+266.25)=355 35 2.54
36 360 8 7+1 87.5+2.50 90 270 (90+270)=360 35 2.57
36.5 365 8 7+1 87.5+3.75 91.25 273.75 (91.25+273.75)=365 35 2.61
37 370 8 7+1 87.5+5.0 92.5 277.5 (92.50+277.5)=370 35 2.64
37.5 375 8 7+1 87.5+6.25 93.75 281.25 (93.75+281.25)=375 35 2.68
38 380 8 7+1 87.5+7.50 95 285 (95.00+285)=380 35 2.71
38.5 385 8 7+1 87.5+8.75 96.25 288.75 (96.25+288.75)=385 35 2.75
39 390 8 7+1 87.5+10 97.5 292.5 (97.5+292.5)=390 35 2.79
39.5 395 8 7+1 87.5+11.25 98.75 296.25 (98.75+296.25)=395 35 2.82
40 400 8 8 100 100 300 (100+300)=400 35 2.86
40.5 405 9 8+1 100+1.25 101.25 303.75 (101.25+303.75)=405 35 2.89
41 410 9 8+1 100+2.50 102.5 307.5 (102.50+307.50)=410 35 2.93
41.5 415 9 8+1 100+3.75 103.75 312.25 (103.75+312.25)=415 35 2.97
42 420 9 8+1 100+5.0 105 315 (105+315)=420 35 3.00
42.5 425 9 8+1 100+6.25 106.25 318.75 (106.25+318.75)=425 35 3.04
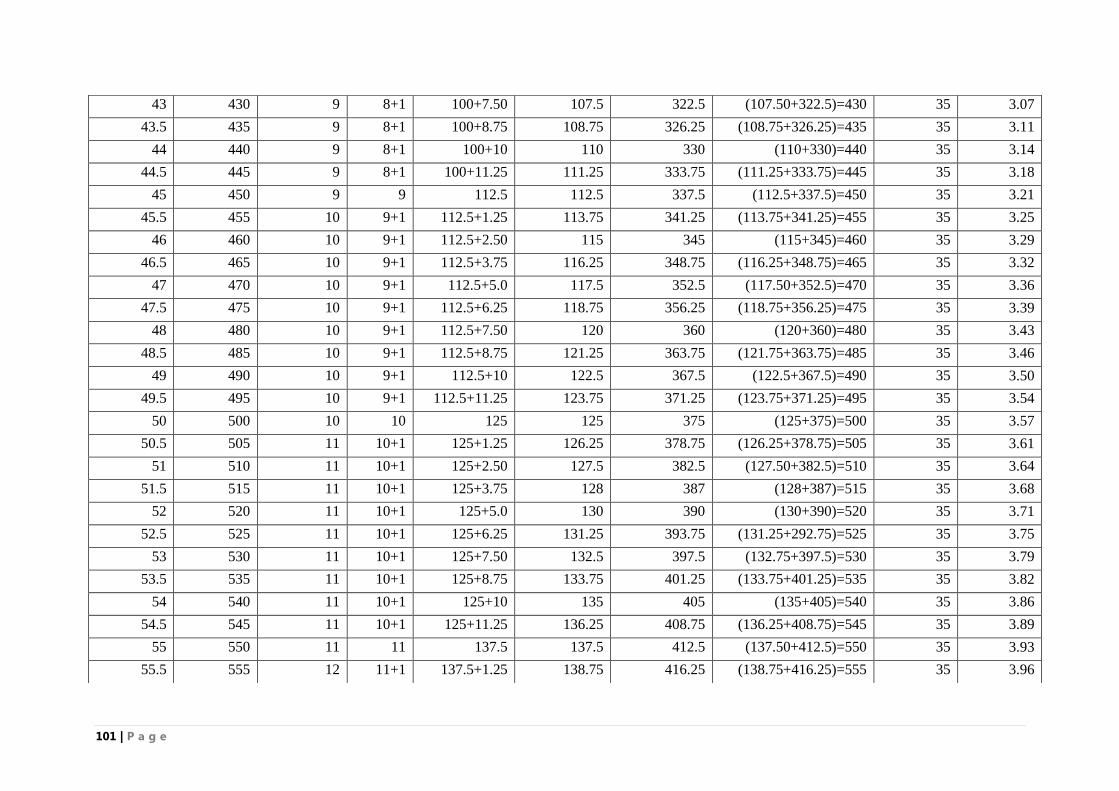
101 | P a g e
43 430 9 8+1 100+7.50 107.5 322.5 (107.50+322.5)=430 35 3.07
43.5 435 9 8+1 100+8.75 108.75 326.25 (108.75+326.25)=435 35 3.11
44 440 9 8+1 100+10 110 330 (110+330)=440 35 3.14
44.5 445 9 8+1 100+11.25 111.25 333.75 (111.25+333.75)=445 35 3.18
45 450 9 9 112.5 112.5 337.5 (112.5+337.5)=450 35 3.21
45.5 455 10 9+1 112.5+1.25 113.75 341.25 (113.75+341.25)=455 35 3.25
46 460 10 9+1 112.5+2.50 115 345 (115+345)=460 35 3.29
46.5 465 10 9+1 112.5+3.75 116.25 348.75 (116.25+348.75)=465 35 3.32
47 470 10 9+1 112.5+5.0 117.5 352.5 (117.50+352.5)=470 35 3.36
47.5 475 10 9+1 112.5+6.25 118.75 356.25 (118.75+356.25)=475 35 3.39
48 480 10 9+1 112.5+7.50 120 360 (120+360)=480 35 3.43
48.5 485 10 9+1 112.5+8.75 121.25 363.75 (121.75+363.75)=485 35 3.46
49 490 10 9+1 112.5+10 122.5 367.5 (122.5+367.5)=490 35 3.50
49.5 495 10 9+1 112.5+11.25 123.75 371.25 (123.75+371.25)=495 35 3.54
50 500 10 10 125 125 375 (125+375)=500 35 3.57
50.5 505 11 10+1 125+1.25 126.25 378.75 (126.25+378.75)=505 35 3.61
51 510 11 10+1 125+2.50 127.5 382.5 (127.50+382.5)=510 35 3.64
51.5 515 11 10+1 125+3.75 128 387 (128+387)=515 35 3.68
52 520 11 10+1 125+5.0 130 390 (130+390)=520 35 3.71
52.5 525 11 10+1 125+6.25 131.25 393.75 (131.25+292.75)=525 35 3.75
53 530 11 10+1 125+7.50 132.5 397.5 (132.75+397.5)=530 35 3.79
53.5 535 11 10+1 125+8.75 133.75 401.25 (133.75+401.25)=535 35 3.82
54 540 11 10+1 125+10 135 405 (135+405)=540 35 3.86
54.5 545 11 10+1 125+11.25 136.25 408.75 (136.25+408.75)=545 35 3.89
55 550 11 11 137.5 137.5 412.5 (137.50+412.5)=550 35 3.93
55.5 555 12 11+1 137.5+1.25 138.75 416.25 (138.75+416.25)=555 35 3.96
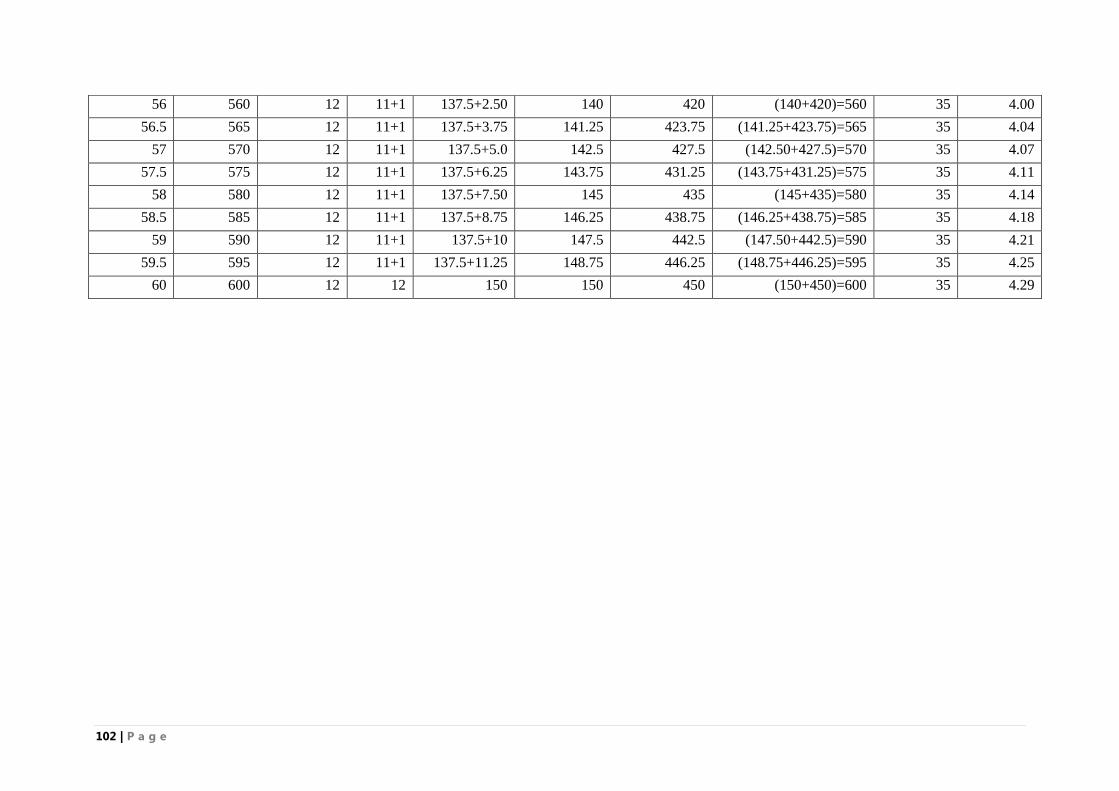
102 | P a g e
56 560 12 11+1 137.5+2.50 140 420 (140+420)=560 35 4.00
56.5 565 12 11+1 137.5+3.75 141.25 423.75 (141.25+423.75)=565 35 4.04
57 570 12 11+1 137.5+5.0 142.5 427.5 (142.50+427.5)=570 35 4.07
57.5 575 12 11+1 137.5+6.25 143.75 431.25 (143.75+431.25)=575 35 4.11
58 580 12 11+1 137.5+7.50 145 435 (145+435)=580 35 4.14
58.5 585 12 11+1 137.5+8.75 146.25 438.75 (146.25+438.75)=585 35 4.18
59 590 12 11+1 137.5+10 147.5 442.5 (147.50+442.5)=590 35 4.21
59.5 595 12 11+1 137.5+11.25 148.75 446.25 (148.75+446.25)=595 35 4.25
60 600 12 12 150 150 450 (150+450)=600 35 4.29
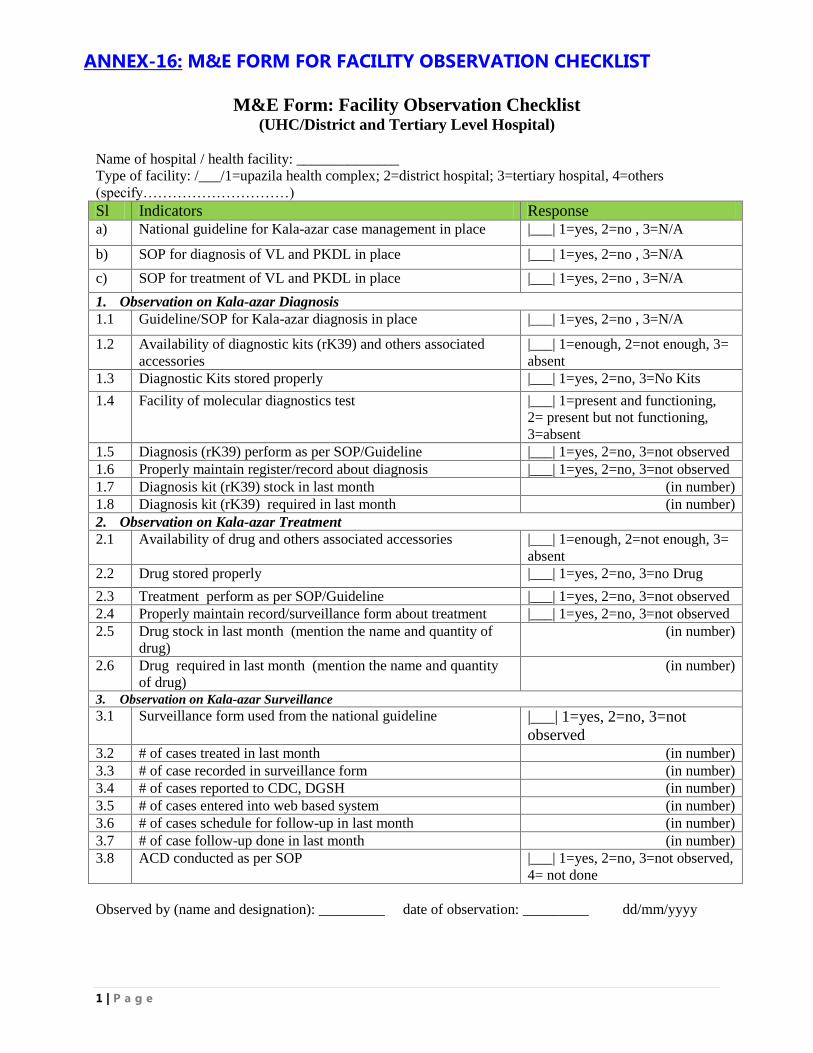
1 | P a g e
ANNEX-16: M&E FORM FOR FACILITY OBSERVATION CHECKLIST
M&E Form: Facility Observation Checklist (UHC/District and Tertiary Level Hospital)
Name of hospital / health facility: ______________
Type of facility: /___/1=upazila health complex; 2=district hospital; 3=tertiary hospital, 4=others
(specify…………………………)
Sl Indicators Response a) National guideline for Kala-azar case management in place |___| 1=yes, 2=no , 3=N/A
b) SOP for diagnosis of VL and PKDL in place |___| 1=yes, 2=no , 3=N/A
c) SOP for treatment of VL and PKDL in place |___| 1=yes, 2=no , 3=N/A
1. Observation on Kala-azar Diagnosis
1.1 Guideline/SOP for Kala-azar diagnosis in place |___| 1=yes, 2=no , 3=N/A
1.2 Availability of diagnostic kits (rK39) and others associated
accessories
|___| 1=enough, 2=not enough, 3=
absent
1.3 Diagnostic Kits stored properly |___| 1=yes, 2=no, 3=No Kits
1.4 Facility of molecular diagnostics test |___| 1=present and functioning,
2= present but not functioning,
3=absent
1.5 Diagnosis (rK39) perform as per SOP/Guideline |___| 1=yes, 2=no, 3=not observed
1.6 Properly maintain register/record about diagnosis |___| 1=yes, 2=no, 3=not observed
1.7 Diagnosis kit (rK39) stock in last month (in number)
1.8 Diagnosis kit (rK39) required in last month (in number)
2. Observation on Kala-azar Treatment
2.1 Availability of drug and others associated accessories |___| 1=enough, 2=not enough, 3=
absent
2.2 Drug stored properly |___| 1=yes, 2=no, 3=no Drug
2.3 Treatment perform as per SOP/Guideline |___| 1=yes, 2=no, 3=not observed
2.4 Properly maintain record/surveillance form about treatment |___| 1=yes, 2=no, 3=not observed
2.5 Drug stock in last month (mention the name and quantity of
drug)
(in number)
2.6 Drug required in last month (mention the name and quantity
of drug)
(in number)
3. Observation on Kala-azar Surveillance
3.1 Surveillance form used from the national guideline
|___| 1=yes, 2=no, 3=not
observed 3.2 # of cases treated in last month (in number)
3.3 # of case recorded in surveillance form (in number)
3.4 # of cases reported to CDC, DGSH (in number)
3.5 # of cases entered into web based system (in number)
3.6 # of cases schedule for follow-up in last month (in number)
3.7 # of case follow-up done in last month (in number)
3.8 ACD conducted as per SOP |___| 1=yes, 2=no, 3=not observed,
4= not done
Observed by (name and designation): _________ date of observation: _________ dd/mm/yyyy
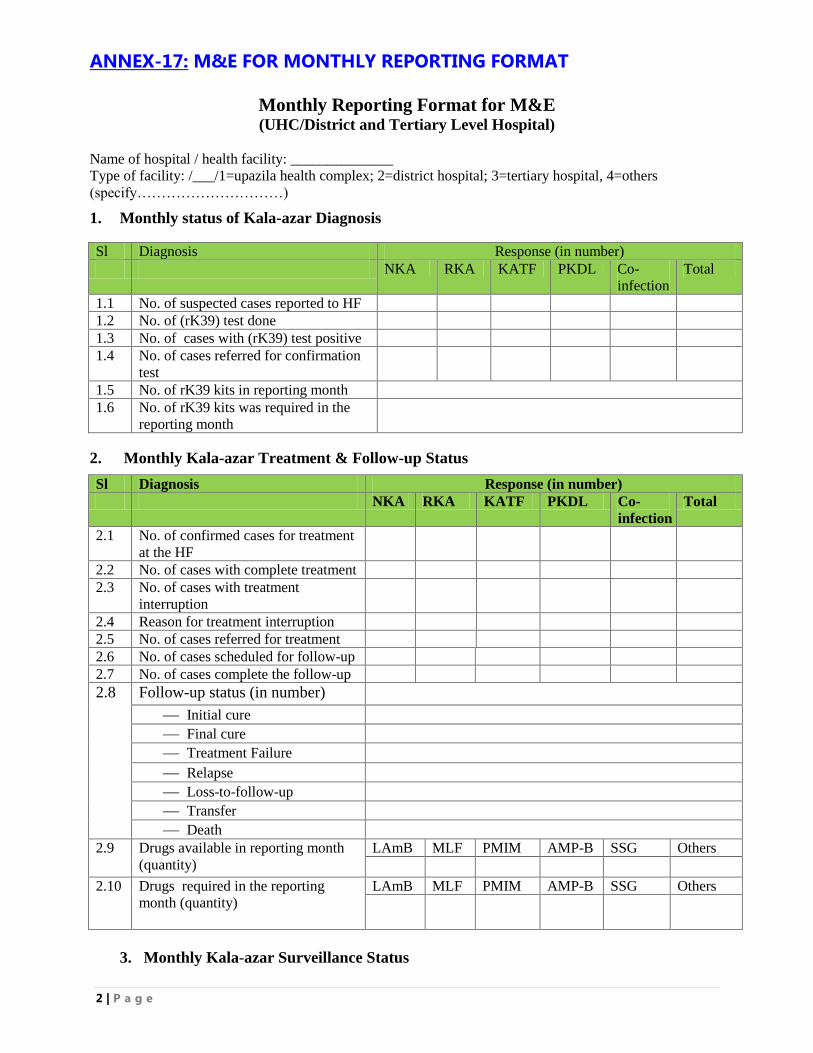
2 | P a g e
ANNEX-17: M&E FOR MONTHLY REPORTING FORMAT
Monthly Reporting Format for M&E (UHC/District and Tertiary Level Hospital)
Name of hospital / health facility: ______________
Type of facility: /___/1=upazila health complex; 2=district hospital; 3=tertiary hospital, 4=others
(specify…………………………)
1. Monthly status of Kala-azar Diagnosis
Sl Diagnosis Response (in number)
NKA RKA KATF PKDL Co-
infection
Total
1.1 No. of suspected cases reported to HF
1.2 No. of (rK39) test done
1.3 No. of cases with (rK39) test positive
1.4 No. of cases referred for confirmation
test
1.5 No. of rK39 kits in reporting month
1.6 No. of rK39 kits was required in the
reporting month
2. Monthly Kala-azar Treatment & Follow-up Status
Sl Diagnosis Response (in number)
NKA RKA KATF PKDL Co-
infection
Total
2.1 No. of confirmed cases for treatment
at the HF
2.2 No. of cases with complete treatment
2.3 No. of cases with treatment
interruption
2.4 Reason for treatment interruption
2.5 No. of cases referred for treatment
2.6 No. of cases scheduled for follow-up
2.7 No. of cases complete the follow-up
2.8 Follow-up status (in number)
Initial cure
Final cure
Treatment Failure
Relapse
Loss-to-follow-up
Transfer
Death 2.9 Drugs available in reporting month
(quantity)
LAmB MLF PMIM AMP-B SSG Others
2.10 Drugs required in the reporting
month (quantity)
LAmB MLF PMIM AMP-B SSG Others
3. Monthly Kala-azar Surveillance Status
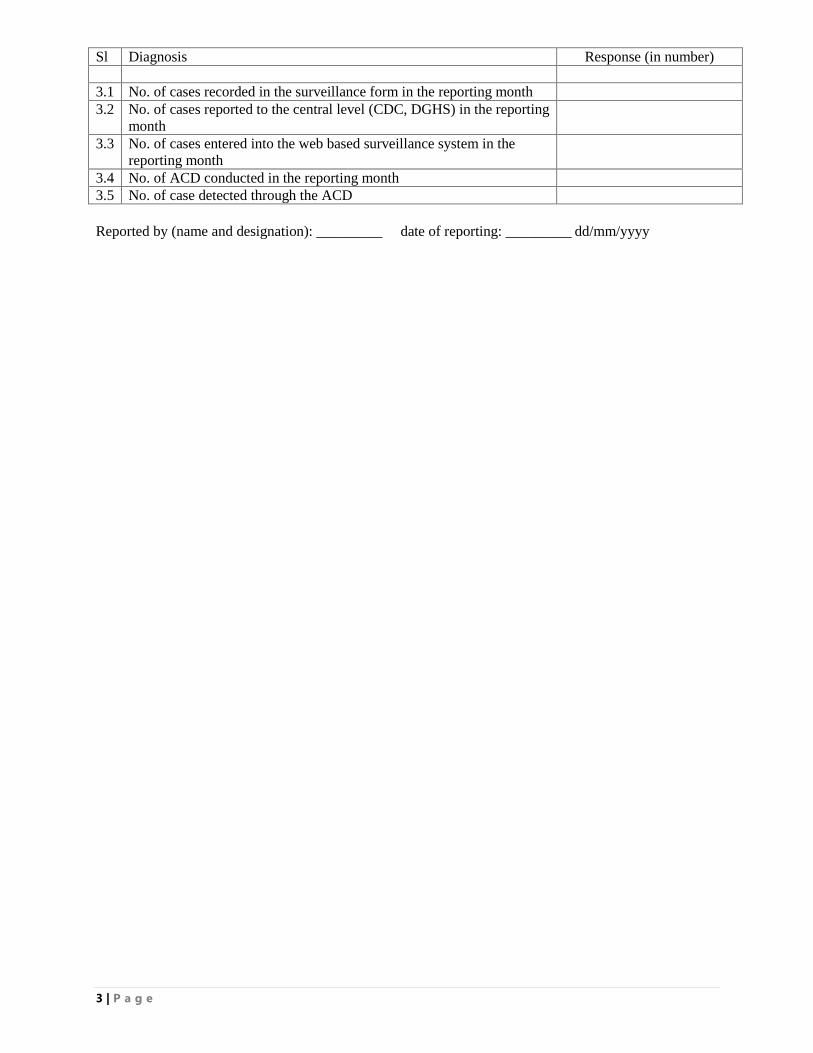
3 | P a g e
Sl Diagnosis Response (in number)
3.1 No. of cases recorded in the surveillance form in the reporting month
3.2 No. of cases reported to the central level (CDC, DGHS) in the reporting
month
3.3 No. of cases entered into the web based surveillance system in the
reporting month
3.4 No. of ACD conducted in the reporting month
3.5 No. of case detected through the ACD
Reported by (name and designation): _________ date of reporting: _________ dd/mm/yyyy

4 | P a g e