Embed Size (px)
Citation preview
National Outcomes of Cataract Extraction Retinal Detachment and Endophthalmitis after Outpatient Cataract Surgery
Jonathan C. Javitt, MD, MPH, 1•2
•3 Debra A Street, MPH,1
James M. Tielsch, PhD, 2•3 Qin Wang, MS, 1 Margaret M. Kolb, DrPH, 3
Oliver Schein, MD, MPH, 2•3 Alfred Sommer, MD, MHS, 2•3•4
5 6Marilyn Bergner, PhD, 5 Earl P. Steinberg, MD, MPP,3• •
On Behalf of the Cataract Patient Outcomes Research Team
Background: A near-total shift to cataract extraction on an outpatient basis occurred as a result of an administrative ruling by the Health Care Financing Administration. No national study has been conducted to assess the possible effects of that decision on clinical outcomes of surgery. The authors compared the rates of retinal detachment (RD) repair and hospitalization for endophthalmitis after extracapsular cataract E::'Xtraction (ECCE) (including phacoemulsification) in 1986 and 1987 with those following inpatient cataract extraction in 1984.
Methods: Using the 5% random sample of Medicare beneficiaries, we analyzed the claims of all individuals 66 years of age or older who underwent ECCE by nuclear expression or phacoemulsification in 1986 and 1987. A total of 57,103 patients were identified and followed to the end of 1988. Cumulative probability of RD repair and hospitalization for endophthalmitis was calculated by standard lifetable methods. These findings were compared with the cumulative probability of the same complications in a cohort of 330,000 patients who underwent cataract extraction on an inpatient basis in 1984.
Results: In the 1986-to-1987 cohort, the cumulative probability of RD within 3 years after cataract surgery was 0.81% and the cumulative probability of endophthalmitis within 1 year was 0.08%. The rate of RD is similar to that which we previously reported for 330,000 patients who underwent inpatient surgery in 1984, but the rate of endophthalmitis is significantly lower in the 1986-to-1987 outpatient cohort (0.08% versus 0.12%; z = 2.42; p = 0.01 ).
Conclusions: The shift to outpatient cataract surgery was accompanied by no significant increase in the probability of RD repair and possibly a significant decrease in the rate of hospitalization for endophthalmitis. Ophthalmology 1994;101:100-106
Originally received: November 8, 1992. Revision accepted: May 3, 1993. 1 Worthen Center for Eye Care Research, Department ofOphthalmology, Georgetown University Medical Center, Washington, DC. 2 Dana Center for Preventive Ophthalmology, Wilmer Ophthalmological Institute, Johns Hopkins University, Baltimore. 3 The Johns Hopkins Program for Medical Technology and Practice Assessment, Johns Hopkins Medical Institutions, Baltimore. 4 Office of the Dean, Johns Hopkins University School of Hygiene and Public Health, Baltimore. 5 Department of Health Policy and Management, Johns Hopkins University School of Hygiene and Public Health, Baltimore.
6 Department of Medicine, Johns Hopkins University, School of Medicine, Baltimore. Presented at the American Academy of Ophthalmology Annual Meeting, Dallas, November 1992 Supported in part by grant POl HS06280 from the Agency for Health Care Policy and Research, Rockville, Maryland; grant ROI EY08805 from the National Eye Institute, National Institutes of Health, Bethesda, Maryland; and grant SlO RR06758 from the Division of Research Resources, National Institutes of Health, Bethesda, Maryland. Reprint requests to Jonathan C. Javitt, MD, MPH, Worthen Center for Eye Care Research, Center for Sight, 3800 Reservoir Rd, N.W., Washington, DC 20007.
100

]avitt et al · National Outcomes of Cataract Extraction
The concept of performing cataract extraction on an ambulatory basis became increasingly accepted during the 1970s. 1•
2 By 1984, approximately one half of all cataract surgery reimbursed by Medicare was performed on an outpatient basis. Because of its perceived safety, and presumed lower cost, the Health Care Financing Administration (HCF A), which oversees the Medicare program, adopted a policy requiring that all cataract surgery be performed in the outpatient setting, unless prior approval to perform inpatient surgery was granted based on ocular or medical co-morbidity. This policy was implemented on a carrier-by-carrier basis between 1983 and 1985.
To date, only two reports from individual hospitals have compared eye-related complications after inpatient and outpatient cataract extraction. Bloom and Krueger3
observed a slight decrease in the rate of endophthalmitis after outpatient, compared with inpatient cataract surgery, among patients who underwent extracapsular cataract extraction (ECCE) in a single Philadelphia hospital. Holland and co-workers4 examined the experience of600 patients who underwent ECCE in a single Los Angeles hospital and found no statistically significant difference in rates ofcomplication among patients undergoing inpatient versus outpatient surgery. In this report, we compare the rates of retinal detachment (RD) and endophthalmitis among Medicare beneficiaries who underwent ECCE in 1986 and 1987, after the mandated shift to outpatient surgery, with those that we have reported previously as having occurred among Medicare beneficiaries who underwent inpatient ECCE in 1984. 5•6
Materials and Methods
Patients included in the 1984 inpatient cohort consisted of a 100% sample of all Medicare beneficiaries, 65 years ofage and older, who underwent surgery in United States hospitals in 1984. These patients were followed through the end of 1987.5•6 Patients included in the 1986-to-1987 outpatient cohort were drawn from a 5% random sample of all Medicare beneficiaries from 1986 to 1987. These patients were followed through the end of 1988. The reason for the difference in sampling strategy is that HCFA historically has maintained hospital data on 100% of Medicare beneficiaries but, before 1991, maintained physician claims, hospital outpatient records, and ambulatory surgical center bills only on a 5% random sample of beneficiaries. 7
We have reported previously the methods and coding criteria used to identify probable cases of cataract extraction from both the 1984 and the 1986-to-1987 cohorts. 5•6•8
As described in the original reports, the 1984 cohort was analyzed based on International Classification ofDisease (ICD-9-CM) diagnosis and procedure codes, which are used in the hospital files. 9 The 1986-to-1987 cohort was analyzed using the ICD-9-CM classification system for hospital records, as well as the HCFA Common Procedure Classification System 10 codes, which are generally equivalent to Physicians Current Procedural Terminology codes11 for analysis of physician and Ambulatory Surgical
Center (ASC) bills.* Criteria used to ascertain RD and endophthalmitis in the 1984 cohort are detailed in our previous reports. 5•
6 Ascertainment criteria for RD in the 1986-to-1987 cohort also have been reported previously.8
In brief, RD was ascertained based on an ophthalmologist's bill for repair of RD and/or a hospital claim with a primary diagnosis of RD or a procedure code for repair ofRD. In previous reports, we classified possible episodes of RD repair as level 1 or 2, based on the amount of evidence found in the claims database. 8 In this report, we include all level 1 and level 2 episodes of RD repair. Endophthalmitis was ascertained based on a hospital discharge diagnosis (primary or secondary) of endophthalmitis. Because no procedure code specifically indicates treatment for endophthalmitis, and physician bills from 1986 to 1987 did not include diagnosis codes, only hospital claims were used in ascertaining episodes of endophthalmitis.
These ascertainment criteria differed between the two cohorts, in that, in the 1984 cohort, RD was only ascertained when a patient was hospitalized, whereas in the 1986-to-1987 cohort, data were available from physician bills, ASC bills, and hospital outpatient records that enabled us to ascertain RD repair in the outpatient setting. Therefore, for the purpose ofcomparing the RD rate after cataract extraction in 1984, we defined RD in two ways: (1) as defined for the 1984 cohort (i.e., an ICD-9 discharge diagnosis code for RD on a Medicare inpatient hospital record); or (2) as defined previously for our 1986-to-1987 cohort (i.e., using both ICD-9 and HCFA Common Procedure Classification System (CPT) codes. 8 When using the second ascertainment scheme, both definite (level 1) and probable (levels 1 or 2) cases of RD were included. Because we believe that virtually all patients with true endophthalmitis are likely to be hospitalized and because there is no procedure code that uniquely identifies management of endophthalmitis, we ascertained endophthalmitis in the 1986-to-1987 cohort based only on a discharge diagnosis (primary or secondary) ofendophthalmitis during an inpatient hospital stay (ICD-9-CM 360.0), just as we did in the 1984 cohort. The date of hospital admission was considered to represent the date of onset of endophthalmitis for lifetable analyses.
Our primary statistical analysis was based on actuarial survival analysis (PROC LIFETEST) using SAS, version 6.07 (SAS Institute, Inc, Cary, NC). 12 Patients were entered into the analysis on the date of their cataract extraction and were followed to the end of the study (December 31, 1988), unless one of the following events occurred, at which time patients were withdrawn from the study (censored): (l) a subsequent intraocular procedure, including a second cataract extraction, (2) entry into a Medicare HMO or loss of either Medicare Part A or Part B benefits, or (3) death, as ascertained in the Medicare denominator file. The reasons for discontinuing patient follow-up subsequent to a second intraocular procedure
* A complete list of codes used in the ascertainment of possible cases of cataract surgery and subsequent complications may be obtained from the corresponding author on written request.
101
Ophthalmology Volume 101, Number 1, January 1994
Table 1. Demographic Characteristics of Patients Who Underwent Extracapsular Cataract Extraction on an Outpatient or Inpatient Basis from 1986 to 1987 and the Proportion with Subsequent Retinal
Detachment (3-year follow-up) or Endophthalmitis (1-year follow-up)
No.(%) of No. Patients with RD
Variable (n = 57,103) (n = 261)
Age (yrs) 66-69 6844 (12) 65 70-79 28,972 (51) 149 80-89 18,914 (33) 45 ~90 2373 (4) 2
Sex M 19,543 (34) 110 F 37,560 (66) 151
Race Black 3237 (6) 12 White 52,363 (92) 242 Other 572 (1) 1 Unknown 931 (2) 6
RD = retinal detachment.
was that, after the second procedure, we were less certain that the RD or endophthalmitis was associated with the index cataract extraction. Entry into a Medicare HMO or loss ofeither Medicare Part A or Part B benefits meant we could no longer ascertain RD or endophthalmitis on those patients because follow-up data were not available. This analytic approach is comparable with that used in our previous analysis of the 1984 cohort. 5•6 It differs from the approach used in our previous report on the association between neodymium:YAG (Nd:YAG) capsulotomy and risk of RD, in that, for the capsulotomy analysis, we chose to use a second identified episode of cataract extraction as a covariate in the multivariate analysis, rather than as a censoring variable. 8 Because of this difference, more RDs were counted in the capsulotomy analysis than in the current study (337 versus 261). It is important to note that our purpose in the capsulotomy analysis was to compare the risk of RD in patients who did and did not undergo capsulotomy, whereas in the current analysis our purpose is to compare rates ofRD (and endophthalmitis) in the 1984 versus 1986-to-1987 cohorts.
Cox's proportional hazards model (SAS: PHREG procedure) was used to evaluate potential risk factors for RD or endophthalmitis, while controlling for other covariates.1 3 The z statistic was used to compare rates of RD and endophthalmitis across years.
Results
A total of 57,103 Medicare beneficiaries were identified as having undergone ECCE (including phacoemulsification) in 1986 to 1987. Ofthese, 54,807 underwent surgery in the outpatient setting and 2,296 were admitted to a
%with No. with %with RDin Endophthalmitis Endophthalmitis
Stratum (n = 44) in Stratum
0.95 6 0.09 0.51 20 0.07 0.24 13 0.07 0.08 5 0.21
0.56 15 0.08 0.40 28 0.08
0.37 2 0.06 0.46 37 O.D7 0.17 1 0.17 0.64 4 0.43
hospital for cataract surgery. Approximately half of this cohort (Table 1) was between 70 and 79 years of age, and the majority was white (92%) and female (66%).
A total of 261 cases of probable or definite RD were ascertained over the entire period of follow-up; 44 persons were hospitalized for endophthalmitis within 12 months after cataract extraction.
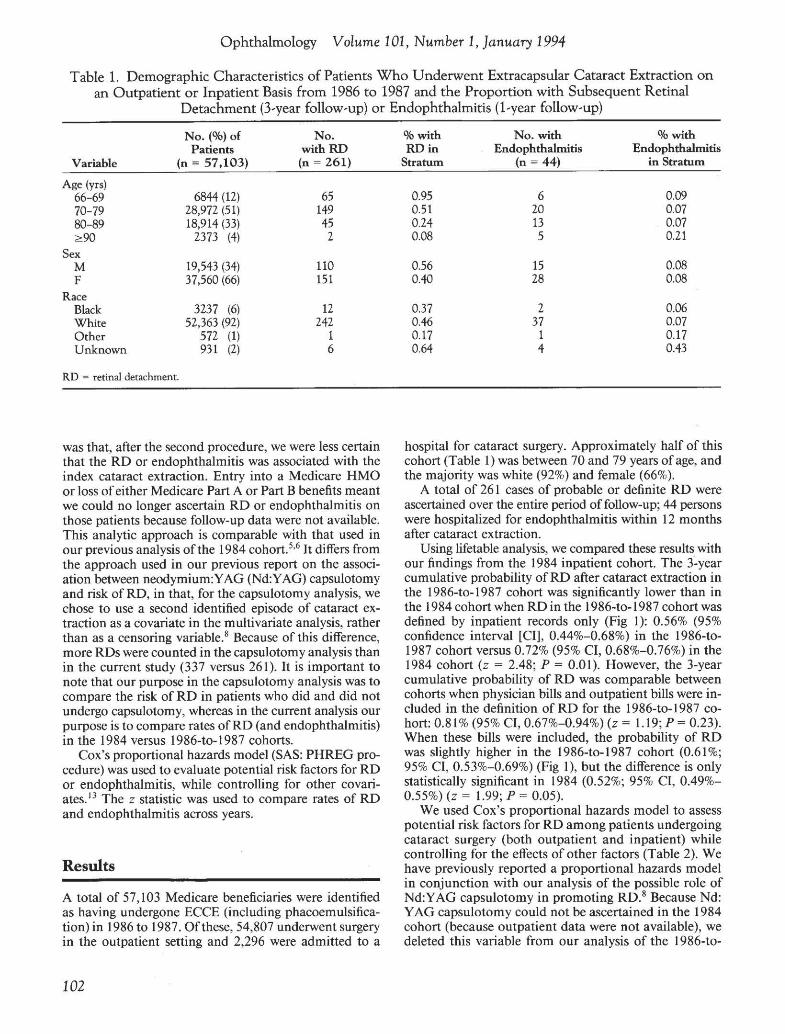
Using lifetable analysis, we compared these results with our findings from the 1984 inpatient cohort. The 3-year cumulative probability of RD after cataract extraction in the 1986-to-1987 cohort was significantly lower than in the 1984 cohort when RD in the 1986-to-1987 cohort was defined by inpatient records only (Fig 1): 0.56% (95% confidence interval [CI], 0.44%-0.68%) in the 1986-to1987 cohort versus 0.72% (95% CI, 0.68%-0.76%) in the 1984 cohort (z = 2.48; P = 0.0 l ). However, the 3-year cumulative probability of RD was comparable between cohorts when physician bills and outpatient bills were included in the definition of RD for the 1986-to-1987 cohort: 0.81 % (95% CI, 0.67%-0.94%) (z = 1.19; P = 0.23). When these bills were included, the probability of RD was slightly higher in the 1986-to-1987 cohort (0.61 %; 95% CI, 0.53%-0.69%) (Fig 1), but the difference is only statistically significant in 1984 (0.52%; 95% CI, 0.49%0.55%) (z = 1.99; P = 0.05).
We used Cox's proportional hazards model to assess potential risk factors for RD among patients undergoing cataract surgery (both outpatient and inpatient) while controlling for the effects of other factors (Table 2). We have previously reported a proportional hazards model in conjunction with our analysis of the possible role of Nd:YAG capsulotomy in promoting RD. 8 Because Nd: Y AG capsulotomy could not be ascertained in the 1984 cohort (because outpatient data were not available), we deleted this variable from our analysis of the 1986-to
102
]avitt et al · National Outcomes of Cataract Extraction
0.9 -·---···············································-······················-·····-···------·--
0.8 -························································································-··-·-···--0 a: 0.7 ···················· .2 5 0.6 ···············
~ 0.5 .............. ~ a. 0.4 ......... 0 "' .l:
~
*' 0.2 .......
6 12 18 24 30 36
Time following cataract extraction (months)
Figure 1. Cumulative probability of retinal detachment repair after extracapsular cataract extraction (ECCE) and phacoemulsification (PHACO) performed on an outpatient or inpatient basis in 1986 and 1987 compared with surgery performed on an inpatient basis in 1984. Because only hospital records were available for the 1984 cohort, whereas hospital, outpatient department, ambulatory surgical center, and physician bills were available for the 1986-to-1987 cohort, retinal detachment was ascertained in the 1986-to-1987 cohort in two ways: (1) using only hospital records (asterisk) and (2) using all available records.
1987 cataract surgery cases for the sake of comparison with the 1984 data. The proportional hazards model (Table 2) shows that women were at lower risk of RD than were men, and that risk of RD decreased as age increased. These findings are consistent with those that we reported from the 1984 cohort. 5 Although AfricanAmericans were less likely than whites to experience an RD, only a mild decrease in risk for African-Americans was seen in the 1986-to-1987 cohort. This may be a function of the smaller sample size and, hence, smaller power to detect a difference, in the later cohort.
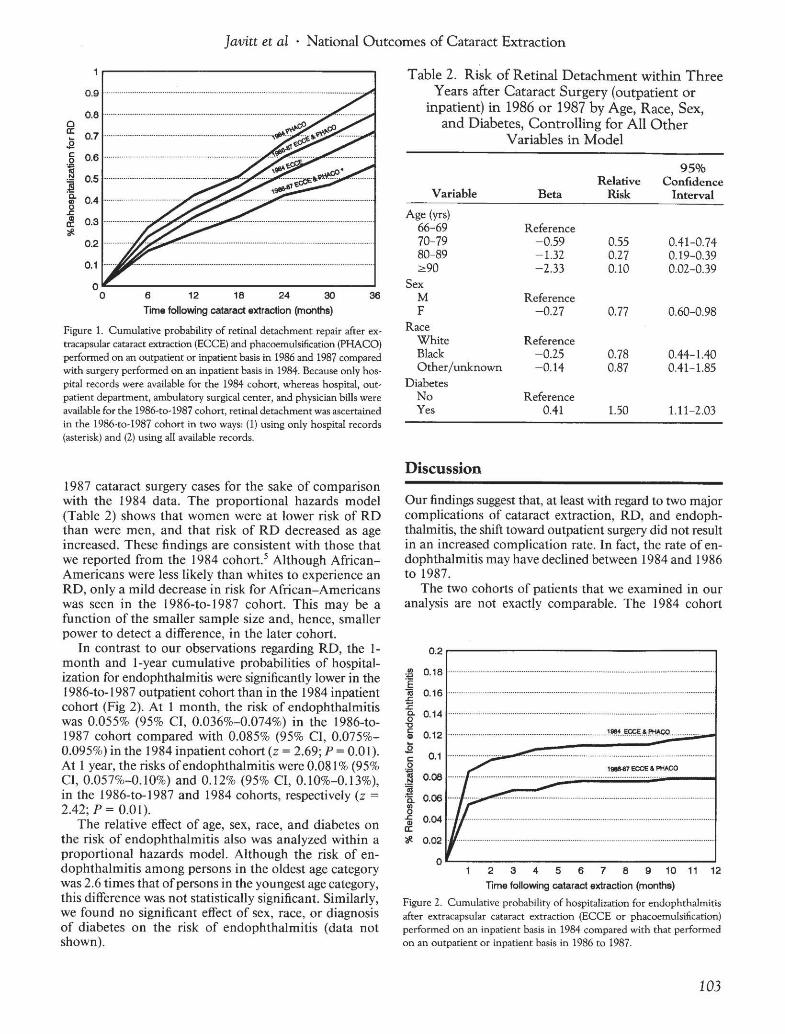
In contrast to our observations regarding RD, the 1month and 1-year cumulative probabilities of hospitalization for endophthalmitis were significantly lower in the 1986-to-1987 outpatient cohort than in the 1984 inpatient cohort (Fig 2). At 1 month, the risk of endophthalmitis was 0.055% (95% CI, 0.036%-0.074%) in the 1986-to1987 cohort compared with 0.085% (95% CI, 0.075%0.095%) in the 1984 inpatient cohort (z = 2.69; P = 0.01). At 1 year, the risks ofendophthalmitis were 0.081% (95% CI, 0.057%-0.10%) and 0.12% (95% CI, 0.10%-0.13% ), in the 1986-to-1987 and 1984 cohorts, respectively (z =
2.42; p = 0.01 ). The relative effect of age, sex, race, and diabetes on
the risk of endophthalmitis also was analyzed within a proportional hazards model. Although the risk of endophthalmitis among persons in the oldest age category was 2.6 times that ofpersons in the youngest age category, this difference was not statistically significant. Similarly, we found no significant effect of sex, race, or diagnosis of diabetes on the risk of endophthalmitis (data not shown).
Table 2. Risk of Retinal Detachment within Three Years after Cataract Surgery (outpatient or
inpatient) in 1986 or 1987 by Age, Race, Sex, and Diabetes, Controlling for All Other
Variables in Model
95% Relative Confidence
Variable Beta Risk Interval Age (yrs)
66-69 Reference 70-79 -0.59 0.55 0.41-0.74 80-89 -1.32 0.27 0.19-0.39 2::90 -2.33 0.10 0.02-0.39
Sex M Reference F -0.27 0.77 0.60-0.98
Race White Reference Black -0.25 0.78 0.44-1.40 Other/unknown -0.14 0.87 0.41-1.85
Diabetes No Reference Yes 0.41 1.50 1.11-2.03
Discussion
Our findings suggest that, at least with regard to two major complications of cataract extraction, RD, and endophthalmitis, the shift toward outpatient surgery did not result in an increased complication rate. In fact, the rate of endophthalmitis may have declined between 1984 and 1986 to 1987.
The two cohorts of patients that we examined in our analysis are not exactly comparable. The 1984 cohort
0.2.--------------------,
1988-87 ECCE & PHACO
2 3 4 5 6 7 8 9 10 11 12
Time following cataract extraction (months)
Figure 2. Cumulative probability of hospitalization for endophthalmitis after extracapsular cataract extraction (ECCE or phacoemulsification) performed on an inpatient basis in 1984 compared with that performed on an outpatient or inpatient basis in 1986 to 1987.
103

Ophthalmology Volume 101, Number 1, January 1994
consisted both of patients with co-morbidities requiring inpatient care and of patients who underwent inpatient surgery because of the practice style at that time. Given the summary nature of insurance claims data, we cannot distinguish between the former group, who were presumably most ill, and those who would likely have undergone outpatient surgery in later years. Although we could have made a distinction between the experience ofpatients who underwent inpatient versus outpatient cataract extraction in our 1986-to-1987 cohort, we elected not to do so because of the selection bias that would have been introduced. As a result, 96% of patients in the 1986-to-1987 cohort underwent cataract surgery on an outpatient basis. Presumably, those who were operated on inhospital had co-morbidities that required inpatient care. Removing the 2296 cases of inpatient cataract extraction from our 1986to-1987 cohort does not alter our findings (data not shown).
An exact comparison of rates of RD among patients who underwent cataract surgery in 1984 versus 1986-to1987 also is not possible because only inpatient records on RD are available for the 1984 cohort, whereas both inpatient and outpatient data are available for the 1986to-1987 cohort. As shown in Figure 1, when only cases of hospitalization for RD are counted in the 1986-to-1987 cohort, the cumulative probability of RD within 3 years after surgery is significantly lower than in the 1984 cohort (0.56% versus 0.72%; P < 0.5). However, when, in addition, cases of RD repair performed in the outpatient setting on patients in the 1986-to-1987 cohort are considered, there is no significant difference between the rates. We cannot determine whether a significant number of detachments were repaired on an outpatient basis in the 1984 cohort. Thus, there are two possible conclusions: (I) the rate ofRD after cataract extraction did not change significantly over the time period, or (2) the rate of RD after cataract extraction did decline over the interval in question, but we did not detect the decline in RD rate because we were not able to identify outpatient repair of RD performed on the 1984 cohort. The essential point, however, is that outpatient surgery with immediate ambulation was not associated with an observed increase in the rate of this complication.
In the 1984 cohort, we noted that the cumulative probability ofRD after phacoemulsification was 0.92%, 3 years after cataract extraction, compared with a rate of 0.72% after standard ECCE (P < 0.001 ). 5 In the 1986-to-1987 cohort, we are not able to distinguish cases of phacoemulsification from cases ofstandard ECCE with lens implantation because both are identified by the same CPT code (CPT 66984). Because of the shift of RD repair to the outpatient setting (as discussed above), there is no way to determine from these data whether the increased popularity ofphacoemulsification affected the rate ofRD in the 1986-to-1987 cohort.
In examining the cumulative probability of endophthalmitis (Fig 2), it appears that the difference in the incidence of endophthalmitis between 1984 and 1986 to 1987 is nearly all due to a difference that occurred by the first month after surgery. One possible explanation for the
observed difference in the cumulative probability of endophthalmitis is that patients who undergo surgery on an ambulatory basis are exposed to fewer or different pathogens compared with patients who remain in the hospital after surgery. It is also possible that changes in surgical management, such as advances in operative technique, wound closure, management of intraocular irrigating fluids, and antibiotic prophylaxis, over the 4-year interval from 1984 to 1987 resulted in a decrease in the rate of endophthalmitis.
There is a possibility that endophthalmitis was more likely to be managed on an outpatient basis in 1986 to 1987 than in 1984. If so, this could account for the decrease in the likelihood of hospitalization for endophthalmitis that we observed. Although the ophthalmologic literature strongly supports the approach of hospitalization, vitrectomy, and both systemic and intravitreal antibiotics for endophthalmitis, 14- 16 examples of outpatient management with a diagnostic vitreous tap and instillation of antibiotics have been reported. 17 We cannot assess the degree to which such practice affected our findings, because there is no outpatient procedure code that is specific for intravitreal instillation of antibiotics.
In our previous reports, we discussed the possibility that coding errors in the Medicare database might have affected our results. Recently, Fisher and co-workers18 reported that procedure codes for cataract surgery in the Medicare hospital file are 96% sensitive and 100% specific for cataract surgery having occurred. We recently have found that physicians' bills for cataract surgery are similarly 95% accurate with respect to type of surgery (intracapsular cataract extraction versus ECCE) with a predictive value of99% for surgery having occurred. 19 To date, no study has been performed validating diagnosis and procedure coding for endophthalmitis and RD repair. However, if the coding error rates associated with these clinical entities are comparable with those associated with cataract surgery, the error rate in the Medicare database is unlikely to affect our conclusions in any significant way.
There is also the possibility that sampling error could account partly for the difference in findings for the two cohorts because the entire population of Medicare beneficiaries, who were 65 years of age and older and who underwent inpatient cataract extraction comprised the 1984 cohort, whereas all patients in a 5% sample ofMedicare beneficiaries who were 66 years ofage and older and who underwent outpatient or inpatient cataract extraction comprised the 1986-to-1987 cohort; however, a comparison of the two cohorts shows that demographic characteristics ofthe 1986-to-1987 5% random sample are nearly the same as those ofthe 1984 total cohort (age, sex, and race are similar; persons in the 1984 cohort tend to be slightly younger; Table 1 and reference 5, Table 3).
Our ascertainment criterion for endophthalmitis is based on a hospital discharge diagnosis (primary or secondary) ofendophthalmitis, rather than on culture-proven endophthalmitis. Using this criterion, we identified nine cases of endophthalmitis that occurred between 1 month and I year after cataract surgery. Chronic endophthalmitis, caused by fungi, propionibacteria, etc., is likely to
104

]avitt et al · National Outcomes of Cataract Extraction
be diagnosed well after the initial episode of cataract surgery, because of its more indolent presentation?0- 22 These cases are thought to be rare; the nine late cases of endophthalmitis represent a cumulative probability of hospitalization of0.02%. We recently saw a patient in whom a fulminant panophthalmitis developed, caused by an ahemolytic Streptococcus organism, after suture removal I year after the initial cataract surgery. A rare complication of this nature also would have been detected by us as a case of endophthalmitis after cataract surgery.
In conclusion, we find that, between 1984 and 1986 to 1987, during which there was a mandated shift to outpatient cataract extraction, there either was no change or a decrease in the probability of RD repair after cataract surgery, and there is evidence of a decrease in the rate of hospitalization for endophthalmitis.
Acknowledgments The authors thank the members of the advisory board of the Cataract Patient Outcomes Research Team: Donald Doughman, MD, Merton Flom, OD, Thomas Harbin, MD, Harry Knopf, MD, Thomas Lewis, OD, Stephen Obstbaum, MD, Denis O'Day, MD, Walter Stark, MD, Arlo Terry, MD, and C. Pat Wilkinson, MD.
References
I. Galin MA, Baras I, Barasch K, Boniuk V. Immediate ambulation and discharge after cataract extraction. Trans Am Acad Ophthalmol Otolaryngol 1974;78:0P43-9.
2. Galin MA, Boniuk V, Obstbaum S, Glasser M. Out-patient cataract surgery. Trans Ophthalmol Soc UK 1975;95:425.
3. Bloom BS, Krueger N. Cost and quality effects of outpatient cataract removal. Inquiry 1988;25:383-7.
4. Holland GN, Earl DT, Wheeler NC, et a!. Results of inpatient and outpatient cataract surgery. A historical cohort comparison. Ophthalmology 1992;99:845-52.
5. Javitt JC, Vitale S, Canner JK, et a!. National outcomes of cataract extraction. I. Retinal detachment after inpatient surgery. Ophthalmology 1991 ;98:895-902.
6. Javitt JC, Vitale S, Canner JK, eta!. National outcomes of cataract extraction. Endophthalmitis following inpatient surgery. Arch Ophthalmol 1991 ;109:1085-9.
7. Lave J, Dobson A, Walton C. The potential use of Health Care Financing Administration data sets for health care services research. Health Care Finane Rev 1983;5:93-8.
8. Javitt JC, Tielsch JM, Canner JK, eta!. National outcomes ofcataract extraction. Increased risk of retinal complications associated with Nd:YAG laser capsulotomy. Ophthalmology 1992;99: 1487-98.
9. The International Classification of Diseases, 9th revision. Clinical Modification. ICD-9-CM, 3rd ed. Vol. 1: Diseases,
Tabular List. [Washington, DC]: US Dept. Health Human Services, 1989.
10. HCFA Common Procedure Coding System (HCPCS), 1989 (non CPT-4). [Baltimore]: Health Care Financing Administration, 1989.
II . CPT: Physicians' Current Procedural Terminology, 4th ed. Chicago: American Medical Association, 1977.
12. SAS Institute Inc. SAS/STAT User's Guide: Version 6, 4th ed., Vol. 2. Cary, NC: The Institute, 1990:1027-70.
13. Cox DR. Regression models and life-tables. J R Stat Soc 1972;34:187-220.
14. Doft BH. The endophthalmitis vitrectomy study [editorial]. Arch Ophthalmol 1991 ; I 09:487-9.
15. Driebe WT Jr, Mandelbaum S, Forster RK, eta!. Pseudophakic endophthalmitis. Diagnosis and management. Ophthalmology 1986;93:442-8.
16. Olson JC, Flynn HW Jr, Forster RK, Culbertson WW. Results in the treatment of postoperative endophthalmitis. Ophthalmology 1983;90:692-9.
17. Pavan PR, Brinser J H. Exogenous bacterial endophthalmitis treated without systemic antibiotics. Am J Ophthalmol 1987;104:121-6.
18. Fisher ES, Whaley FS, Krushat WM, et a!. The accuracy of Medicare's hospital claims data: progress has been made, but problems remain. Am J Public Health 1992;82:243-8.
19. Javitt JC, McBean AM, Sastry S, DiPaolo FJ. Accuracy of Medicare Part-B coding for cataract extraction. Arch Ophthalmology 1993;111:605-7.
20. Meisler DM, Palestine AG, Vastine DW, eta!. Chronic Propionibacterium endopthalmitis after extracapsular cataract extraction and intraocular lens implantation. Am J Ophthalmol 1986; 102:733-9.
21. McManaway JW III, Weinberg RS, Coudron PE. Coryneform endophthalmitis. Two case reports. Arch Ophthalmol 1990;108:942-4.
22. Jaffe GJ, Whitcher JP, Biswell R, Irvine AR. Propionibacterium acnes endophthalmitis seven months after extracapsular cataract extraction and intraocular lens implantation. Ophthalmic Surg 1986;17:791-3.
Appendix
The Cataract Patient Outcomes Research Team is composed of: Earl P. Steinberg, MD, MPP (principal investigator), Marilyn Bergner, PhD, (co-principal investigator), Alfred Sommer, MD, MHS (co-principal investigator), Gerard F. Anderson, PhD, Eric B. Bass, MD, MPH, Joseph Canner, MHS, Alan M. Gittelsohn, PhD, Jonathan Javitt, MD, Margaret M. Kolb, DrPH, Marcia Legro, PhD, Neil R. Powe, MD, Oliver P. Schein, MD, MPH, Phoebe Sharkey, SeD, Donald M. Steinwachs, SeD, and James M. Tielsch, PhD.
105

Ophthalmology Volume 101, Number 1, January 1994
Discussion by
PaulP.Lee,~,PD
Dr. Javitt and his group again have made significant contributions to our understanding ofcataract surgery. There are at least three important implications that should be highlighted: (I) the safety of outpatient surgery, (2) insights into risk factors for complications, and, perhaps most importantly, (3) the potential uses of the data contained within the study.
First, the rate of two of the most feared complications of cataract surgery-retinal detachment (RD) and endophthalmitis-have not increased with a move toward outpatient surgery .1 Unlike earlier single-site studies, 2 this national study has sufficient power to detect clinically significant differences in otherwise rare or unusual events. Thus, we can conclude that cataract surgery may be safely performed in the outpatient setting, but we cannot automatically generalize that all ophthalmic surgery can be so safely performed. Similarly, not all cataract surgery can be performed on an outpatient basis.
Second, the 1984 and 1987 study populations show insights into the risks of complications developing. In both studies, the risk of developing an RD was both statistically and clinically significantly higher for younger cohorts. 1•3 If this trend can be extrapolated to those younger than 65 years of age, careful consideration of the risks and expected benefits in younger patients must be undertaken. Because the Medicare databases do not contain information about axial length, we cannot say anything about this important risk factor for detachment.
In addition, we know from earlier studies that vitreous loss requiring anterior vitrectomy increases the relative risk of postoperative RD and endophthalmitis four to five times.3- 5 Similarly, neodymium:Y AG capsulotomy is known to increase the risks of detachment. Results of the earlier study and this study suggest that men, whites, and those with diabetes also may be at higher risk for RDY
An interesting point is the significantly lower rate of endophthalmitis in the 1986-to-1987 cohort. 1 A case-control study has suggested that the use ofpolypropolene haptics is associated with a higher rate of endophthalmitis than PMMA haptics. 5 One additional possibility deals with whether treatment for suspected endophthalmitis differed in the two cohorts. While separated in time by no more than 3 years, the barriers to retaining an inpatient for suspected endophthalmitis may be significantly different than those of rehospitalizing an outpatient. As such, both case definition and case treatment may have favored a relative underdiagnosis of endophthalmitis in the later cohort.
Third, we now have results from a national sample ofpatients confirming case series and single-site studies as to typical rates ofRD and endophthalmitis after cataract surgery. Together with past and future studies on anterior vitrectomy, corneal decompensation, and neodymium:YAG capsulotomy, a more complete picture of expected outcomes after cataract surgery is being developed.
With a certainty ofan increased emphasis on managed care,6
the data from this study may find its most profound implications in their incorporation into quality-monitoring guidelines by third-party payers and managed-care organizations. For the first time, we have national outcomes data on complications in the outpatient setting. Together with guidelines development to as-
From RAND, Santa Monica, and the Doheny Eye Institute, Los Angeles, California.
sess the appropriateness of surgery on the part of several organizations, continuous monitoring of the quality of surgical outcomes will be part of the practice experience ofophthalmologists in the coming years. 7 The Health Care Finance Administration has made the incorporation of explicit quality measures ofphysician performance a cornerstone of its approach in the coming era of managed care. 7
Given this profound possibility, we must take great care to ensure that the data used to create such standards are both accurate and realistic. For the most part, the Medicare databases, as used here, meet three critical concerns.
First, how accurate are the data? The data were collected for administrative and billing purposes and not for clinical study; as such, the level of detail and accuracy should be scrutinized. Although data regarding cataract surgery or the type of surgery performed are generally accurate (95% ), levels ofdetail may not be. Dr. Javitt's group has carefully reviewed this area and found that the Medicare databases do accurately reflect the operative note details.
Second, is sufficient detail present to allow careful analysis ofknown confounding factors? These databases may not contain enough information to allow refined case-mix analysis.
Third, can the coding systems accurately translate clinical reality into analytic codes? These databases share the limitations of the coding system being used, whether it be the ICD-9-CM or CPT codes, where one code could cover a tremendous amount ofvariation or be used to represent different entities or procedures by different providers. Fortunately, this study has addressed this last concern by explicitly including all likely codes for the complications being studied. However, as an example, it would have been valuable to have examined phacoemulsification separately from standard extracapsular extraction.
Thus, the challenge for ophthalmology will be to meet these concerns and construct databases with sufficient detail and accuracy that the data will be both accurate and realistic. To do otherwise would be to jeopardize the practice ofophthalmology and the care of our patients.
References
1. Javitt JC, Street DA, Tielsch JM, et a!. National outcomes of cataract extraction: retinal detachment and endophthalmitis following outpatient cataract surgery. Ophthalmology 1994; 101: 100-60.
2. Holland GN, Earl DT, Wheeler NC, et a!. Results of inpatient and outpatient cataract surgery. A historical cohort comparison. Ophthalmology 1992;99:845-52.
3. Javitt JC, Vitale S, Canner JK, eta!. National outcomes of cataract extraction. I. Retinal detachment after inpatient surgery. Ophthalmology 1991 ;98:895-902.
4. Javitt JC, Vitale S, Canner J, eta!. National outcomes of cataract extraction. Endophthalmitis following inpatient surgery. Arch Ophthalmol 1991;109:1085-9.
5. Menikoff JA, Speaker MG, Marmor M, Raskin EM. A casecontrol study of risk factors for postoperative endophthalmitis. Ophthalmology 1991 ;98: 1761-8.
6. Clinton B. The Clinton health care plan. N Eng! J Med 1992;327:804-7.
7. Jencks SF, Wilensky GR. The health care quality improvement initiative. JAMA 1992;268:900-3.
106









![Clinical Outcomes After Cataract Surgery With a New ...lentech.com.co/archivos/estudios/Clinical Outcomes... · Journal of Refractive Surgery ÊUÊ6 °ÊÎÓ]Ê °ÊÇ]ÊÓä£È](https://img.pdfslide.net/doc/110x75/5fa0346ee061442e0d6c2fd0/clinical-outcomes-after-cataract-surgery-with-a-new-outcomes-journal-of.jpg)



















