Embed Size (px)
Citation preview

National Taipei University of Nursing and Health Sciences
College of Nursing
Department of Nurse-Midwifery and Women Health
Graduate Institute of Nurse-Midwifery
Master Thesis
Factors Associated with Six Months of Exclusive Breastfeeding
among Employed Mothers After Returning to Work in
Karanganyar Regency of Central Java, Indonesia
Siska Ningtyas Prabasari
Advisor : Meei-Ling Gau, CNM, PhD
June 2020

Acknowledgements
First of all, I would like to thank Allah SWT, the almighty God who has given me the favors
of guidance, the favors of faith, the favors of health and the blessings of opportunity so that I
can complete this Master program.
Mr. Sarwoto and Mrs. Jalimah thank you for your motivation, support, guidance, and
prayers that you will never stop giving to your child. I am grateful to have you both.
My husband Rizal, My siblings Iwan, Bayu and Indra who always provide support,
understanding to solve difficulties in the preparation of this thesis.
Professor Meei-Ling Gau as the supervisor of my thesis, Professor Chieh-Yu Liu as the
supervisor of statistical analysis and Stephanie as a medical English editor, thanks for
providing guidance and direction in the preparation of this thesis.
Friends of National Taipei University of Nursing and Health Science especially for
international class of 2018-2020, thank you for all our moments together, hopefully we can
all achieve our goals according to each other's expectations.

i
Abstract
Background: The short- and long-term benefits of breastfeeding for babies and
mothers are widely recognized. Breastfeeding is associated with decreased incidence and
severity of infectious diseases, such as diarrhea, respiratory tract infections and otitis media.
In Indonesia, the rate of exclusive breastfeeding until six months was 42% in 2012, according
to the Indonesian Demographic and Health Survey. Over a three-year period the rate of
exclusive breastfeeding increased dramatically, rising to 55.7% by 2015. In 2017, the rate of
exclusive breastfeeding in the province of Central Java was close to the national average, but
it rose by only 0.2% that year. This study will be done in Karanganyar Regency, which
ranked 30th out of 35 regencies in Central Java, with about 23% of women breastfeeding
exclusively for the first six months of their infant’s life. This figure is far from the target rate
of 80% set out by the national government. Indonesia’s government has recognized the
importance of breastfeeding and breast milk, and has enacted policies aimed at improving
breastfeeding rates. Indonesian Health Law No. 36 was enacted in 2009, calling for every
baby to be breastfed for the first six months of life, unless impossible due to a medical
condition. Though this law aims to increase breastfeeding, workplaces are not well regulated,
and employersre not held accountable for providing support to new mothers who must
breastfeed or pump breast milk at work.
Purpose of the study: to explore factors related to exclusive breastfeeding among
employed mothers returning to work, in particular, assessing whether breastfeeding-friendly
workplace practices are actually succeeding.
Methodology: A descriptive correlational design was used to collect data using
written questionaire. The adapted questionnaire, which included the Multidimensional scale
of perceived social support, Breastfeeding and employment study, Iowa infant feeding
attitude scale, and demographic characteristics, was administered to 208 employed mothers
ii
who consented to participate in Karanganyar Regency from July to November 2019. A binary
logistic regression was used to calculate adjusted odds ratios (AdjORs) and 95% confidence
intervals (CIs) for exclusive breastfeeding practice.
Results: The analysis used seven demographic variables, including age, education,
monthly family income, parity, mode of delivery, and previous breastfeeding experience,
along with different dimensions of social support for breastfeeding, which included family
support, support from friends and significant others (husbands and health workers), and
workplace organizational and management support. Only support from workplace support
(BESt) (p-value = .002 ,odds ratio of 1.034) showed a significant association with successful
exclusive breastfeeding among working women. Social support was not significantly
associated with exclusive breastfeeding in this study.
Conclusion: Lack of workplace support was the dominant factor that predicted failure
to breastfeed exclusively among employed mothers. Breastfeeding-friendly workplace
policies must be implemented and carried out with regular evaluations. Health workers
should do outreach to companies to educate management and co-workers about the
importance of breastfeeding and ways to integrate it with work.
Keywords : exclusive breastfeeding, employed mothers, breastfeeding-friendly
workplace, social support

iii
Contents
Abstract .......................................................................................................................... i
Contents ........................................................................................................................ ii
List of Tables .............................................................................................................. vi
List of Figures ............................................................................................................ vii
List of Abbreviations ................................................................................................. viii
Chapter One Introduction ............................................................................................. 1
1.1 Research Background ...................................................................................... 1
1.2 Significance of the Study ................................................................................. 3
1.3 Research Purpose ............................................................................................. 3
1.4 Research questions ........................................................................................... 3
1.5 Definition of Major Concepts ........................................................................... 4
Chapter Two Literature Review .................................................................................... 6
2.1 Geography of Karanganyar Regency ............................................................... 6
2.2 Maternal and Infant Statistics ........................................................................... 8
2.3 Breastfeeding ................................................................................................... 9
2.4 Exclusive Breastfeeding ................................................................................... 9
2.4.1 Definition .................................................................................................. 9

iv
2.4.2 The Type of Infant Feeding .................................................................... 10
2.4.2 Benefits of Breastfeeding .......................................................................... 10
2.4.3 Factors Related to Exclusive Breastfeeding ............................................... 11
2.5 Conclusion ..................................................................................................... 18
Chapter Three Methodology ....................................................................................... 20
3.1 Research Design ............................................................................................ 20
3.2 Research Setting ............................................................................................ 20
3.3 The Inclusion Criteria and Exclusion Criteria ................................................. 21
3.4 Sample Size .................................................................................................. 21
3.5 Instruments .................................................................................................... 23
3.6 Translation and Pilot Study ............................................................................ 25
3.7 Data Collection ............................................................................................... 29
3.8 Data Analysis ................................................................................................ 32
3.9 Ethical Consideration ..................................................................................... 35
Chapter Four Results ................................................................................................. 36
4.1 Characteristics of Research Subjects ............................................................. 36
4.2 Descriptive statistics of the outcomes variables .............................................. 37
4.3 Relationship between personal factors, breastfeeding and employment study and
social support towards breastfeeding types .................................................... 43
4.4 Factors associated with adherence to six months exclusive breastfeeding ....... 46
v
Chapter Five Discussion ............................................................................................ 48
5.1 Finding of this study .................................................................................... 48
5.1.1 Personal Factors ...................................................................................... 48
5.1.2 Breastfeeding Workplace Friendly Factors ............................................. 52
5.1.3 Social Support Factors ............................................................................ 54
Chapter Six Conclusion, Limitation and Recommendation ......................................... 56
6.1 Conclusion ..................................................................................................... 56
6.2 Limitations ................................................................................................... 56
6.3 Recommendations ......................................................................................... 57
References
Appendix

vi
List of Tables
Table 3.1 Table Data of Analysis ................................................................................ 33
Table 4. 1 Demographic Characteristics of the study participants................................. 37
Table 4. 2.1 Descriptive Statistics of Breastfeeding and Employment Study ................ 39
Table 4. 2.2 Descriptive Statistics of MSPSS ............................................................... 42
Table 4. 2.3 Descriptive Statistics of Iowa Infant Feeding Attitude Scale ..................... 43
Table 4. 3.1 Relationship between personal factors and breastfeeding types ................. 43
Table 4. 3.2 Relationship between BEsT and breastfeeding types ................................ 45
Table 4. 3.3 Relationship between social support and breastfeeding types.................... 46
Table 4. 4 Factors associated with adherence to six months exclusive breastfeeding .... 47

vii
List of Figures
Figure 2.1 Geography of Karanganyar Regency .......................................... 7
Figure 2.2 Conceptual Framework .............................................................. 19
Figure 3.2 Data Collection .......................................................................... 31

viii
List of Abbreviations
WHO
UNICEF
World Health Organization
United Nations International Children’s Emergency Fund
IMR Infant Mortality Rate
BFW Breastfeedingf Friendly Workplace
ASI Air Susu Ibu (Mother’s Breastmilk)
IIFAS Iowa Infant Feeding Attitude Scale
BESt Breastfeeding and Employment Study
MSPSS
IRB
Multidimensional Scale of Perceived Social Support
Institutional Review Board
1
Chapter One
Introduction
1.1 Research Background
Breastfeeding is widely known for short-term and long-term health benefits for babies
and the mothers. Breastfeeding is associated with decreasing incidence and severity of
infectious diseases, such as diarrhea, respiratory tract infections and otitis media (Tang, Lee,
& Binns, 2014).
The World Health Organization (WHO, 2019) recommends that new born babies
breastfeed until the age of six months without providing other food or fluids, except vitamins,
minerals, and drugs that have been allowed for medical reasons. According to the United
Nations International Children's Emergency Fund (UNICEF, 2012), every three years, 30,000
infant deaths in Indonesia and 10 million under-five deaths around the world can be
prevented by exclusive breastfeeding for six months after the birth of the baby without
providing additional food and drink.
The Indonesian Demographic and Health Survey in 2012 showed the rate of exclusive
breastfeeding until six months was 42%. Nationally, there was a rather dramatic increase over
a three-year period, with the rate of exclusive breastfeeding for infants 0-6 months rising to
55.7% by 2015. Although in the province of Central Java the rate of exclusive breastfeeding
in 2017 was close to the national average, it rose by only 0.2% that year. The lowest
exclusive breastfeeding rate in the province was in Temanggung Regency at 8.4% (451
babies) and the highest was in the town of Magelang City at 87.2% (458 babies). This study
will be done in Karanganyar Regency (a regency is an administrative unit similar to a large
city), which, at 22.82 is ranked 30th out of 35 regencies (Central Java Health Profile, 2018).
This figure is far from the target rate of 80% set out in the national government’s Minimum
Service Standards.

2
The infant mortality rate in Karanganyar Regency fluctuated over the five years from
2012 to 2017, with the lowest rate in 2013 at 9.9/1000 and the highest at 14.2/1000 in 2016
(In 2012 it was 10.1/1000, 9.9/1000 in 2013, 10.5/1000 in 2014, 12.8/1000 in 2015,
14.2/1000 in 2016 and 12.7/1000 in 2017). In 2017, there were 134 cases of infant mortality,
the most in the Karanganyar Primary Health Center at 17 cases and the least in the
Ngargoyoso Community Health Center with 2 cases (Central Java Health Profile, 2018).
Indonesia Governments have recognized the importance of breastfeeding and breast
milk, and they have enacted policies with the intention of improving breastfeeding rates. In
2009, Indonesian Health Law No. 36 was enacted, calling for every baby to be breastfed for
the first six months of life, unless impossible due to a medical condition (Indonesia Health
Profil, 2012). Though this law aims to increase breastfeeding. Workplaces are not well
regulated, and employers are not held accountable for providing aid to new mothers who
must breastfeed or pump breast milk at work.
Since a woman’s breast milk supply responds to demand, when she is unable to
release milk regularly, milk production decreases. Although employers are not being actively
regulated, the law states that women can face fines and/or jail time for not providing their
child with breast milk for the required amount of time (Alves, Dowling, & Mahan, 2017). In
urban areas where more mothers are working to make a living, it’s harder to breastfeed their
babies properly and regularly. Workplaces do not yet support the practice of breastfeeding,
for example, private space for pumping breast milk and proper means to store it are often
lacking. Also, most workplaces do not provide on-site child care facilities so that working
mothers could breastfeed their babies at certain times (Central Java Health Profile, 2018). In
addition, there are many other factors that influence working mothers’ ability to breastfeed
exclusively. Mothers who are employed postpartum are less likely to continue breastfeeding
than mothers who are not formally employed. However, as employment is increasingly

3
necessary for the majority of new mothers, it is important to investigate factors that influence
the continuation of breastfeeding among employed mothers (Bai, Wunderlich, & Weinstok,
2015).
1.2 Significance of the Study
The results of this study should help us understand the relationship between exclusive
breastfeeding and personal factors, social support for breastfeeding among employed
mothers, and breastfeeding-friendly workplace practices. The information provided should
offer a basis for designing practical guidelines for midwives to educate society and to
improve the implementation of exclusive breastfeeding among employed mothers returning
to work, which may further increase the exclusive breastfeeding rate.
1.3 Research Purpose
The purpose of this study is to explore factors related to exclusive breastfeeding among
employed mothers returning to work especially the breastfeeding-friendly workplace
practices. The research objectives were:
1.3.1 To examine breastfeeding-friendly workplace practices including workplace
organizational support, manager support, co-worker support, time support and physical
environment support for exclusive breastfeeding among employed mothers returning to work.
1.3.2 To examine personal factors related to exclusive breastfeeding among employed
mothers returning to work, including demographic and obstetrical data and personal attitudes
about breastfeeding.
1.3.3 To examine factors relating to social support among family, friends and others for
employed mothers to exclusively breastfeed after returning to work.
1.4 Research questions
1.4.1 What is the relationship between exclusive breastfeeding rates among employed
mothers returning to work and breastfeeding-friendly workplace practices, such as
4
organizational support, manager support, co-worker support, time support and physical
environment support for breastfeeding?
1.4.2 What are the relationships between personal factors, including demographic and
obstetrical factors, and attitudes towards exclusive breastfeeding among employed mothers
returning to work?
1.4.3 What is the relationship between social support and exclusive breastfeeding among
employed mothers returning to work?
1.4.4 Which factors—personal, workplace, and social support—are the most important
for predicting exclusive breastfeeding among employed mothers returning to work?
1.5 Definition of Major Concepts
1.5.1 Exclusive Breastfeeding
Concept definition:
Exclusive breastfeeding refers to infants receiving only breast milk during the first six
months of life, and not food or even water, including other liquids like tea and herbal
preparations, except for doctor-recommended vitamins, mineral supplements, or medicines
(WHO, 2009).
Operational definition:
A measure of exclusive breastfeeding among mothers will use the definition from WHO
including the types of infant feeding practice, which include exclusive breastfeeding, mix
breastfeeding and replacement feeding (formula) (Bai et al., 2009; Thurman & Allen, 2008;
WHO, 2009;)
1.5.2 Breastfeeding-friendly Workplace
Concept definition:
Workplace support for breastfeeding powerfully influences whether or not mothers
succeed at exclusive breastfeeding. Examples include places for pumping breast milk, proper

5
storage for breast milk, and childcare. In addition, work hours also affect the success of
breastfeeding, including the type and duration of work (Novayelinda, 2012).
Operational definition:
A measure of how breastfeeding-friendly workplaces support mothers to breastfed their
children exclusively. The measurement in this study uses Breastfeeding Employment Study
(BEESt) (Greene, Wolfe & Olson, 2008).
1.5.3 Social support
Concept definition:
Nursalam (2009) states that people involved in providing social support for breastfeeding
include spouses, parents, children, relatives, friends, health teams, and counselors.
Operational definition:
Using the Multidimensional Scale of Perceived Social Support (MSPSS). This instrument
is used to measure the social support factors which contains of three subscales: The
Significant Other Subscale, the Family Subscale and the Friends Subscale (Zimet, Dahlem,
Zimet & Farley, 1988).
1.5.4 Attitude
Concept definition:
Attitude is a reaction or response that is still closed from someone to stimulus or
object, attitude is not yet an action or activity, but it is a predisposition of an act of behavior
(Notoadmodjo, 2012).
Operational definition:
Using the Iowa Infant Feeding Attitude Scale (IIFAS) whch consist of 17 attitude questions,
half of which are favorable to breastfeeding and the remaining favorable to artificial feeding
(De la Mora, Russell, Dungy, Losch, & Dusdieker, 1999).
6
Chapter Two
Literature Review
2.1 Geography of Karanganyar Regency
Karanganyar Regency is one of 35 Regencies / Cities in Central Java Province located
110°40°-100°70° east longitude and 7°28° - 7°46° south latitude (Figure 1). The average
height is 511 meters above sea level, has a tropical climate with temperatures of 22° C - 31°
C Surakarta dan Kabupaten Boyolali. North is bordered by Sragen Regency; East side
borders with East Java Province; The South is bordered by Sukoharjo and Wonogiri
Regencies; The west is bordered by Surakarta City and Boyolali Regency.
Topographically, Karanganyar Regency is a land and mountains with a very varied
altitude. The height of the region up to 100 meters above sea level, covering the District of
Jaten and Kebakkramat (8.11%). The height of 101-500 meters above sea level covers
Jumantono, Karanganyar, Tasikmadu, Colomadu, Gondangrejo, Mojogedang and Kerjo
(45.32%), 501-1,000 meters above sea level, covering Jatiyoso, Jatipuro, Matesih,
Tawangmangu (partly), Ngargoyoso (partly), Karangpandan and some of Jenawi Subdistrict
(36.59%). And the altitude of 1,000 meters above sea level, covers part of the District of
Tawangmangu, Ngargoyoso and Jenawi (9.98%). While the total area is 773.8 km2 or 2.73%
of the total area of Central Java Province.
Based on data from the Population and Civil Registry Service (Disdukcapil), Karanganyar
Regency in 2017 has a population of 896,991 people. the largest population in Karanganyar
Subdistrict is 82,381 and the lowest population is in Jenawi Subdistrict District Health Profile
Karanganyar 2017 6 as many as 27,221 people.

7
Figure 1: Karanganyar Geography

8
2.2 Maternal and Infant Statistics
The maternal mortality rate is the number of mothers who die from pregnancy, childbirth
and childbirth in a particular area per 100,000 birth live within one year. Maternal mortality
rates can describe nutritional status and maternal health, environmental health conditions and
the level of health services, especially for pregnant women, mothers of childbirth and
postpartum mothers. According to Karanganyar Regency Health Profile (2017) the maternal
mortality rate in Karanganyar in 2017 was 72.6 / 100,000 birth live, down compared to 2016
of 30.79 / 100,000 birth live, while in 2015 amounted to 123.3 /100,000 birth live, in 2014
amounted to 138.5 /100,000 birth live, in 2013 amounted to 68.3 /100,000 birth live, and in
2012 amounted to 127.1 /100,000 birth live. The number of cases of maternal deaths in 2017
was 9 cases spread in the Jumantono, Tawangmangu, Karangpandan, Colomadu II,
Gondangrejo, Kebakkramat I and Jenawi health centers as many as 1 case of maternal death,
while in Karanganyar Health Center there were 2 cases of maternal deaths.
Infant Mortality Rate (IMR) is the number of infant deaths (0-11 months) per 1,000 birth
live in one year. AKB describes the level of public health problems related to the factors that
cause infant mortality, the level of antenatal care, the nutritional status of pregnant women,
the success rate of the MCH and family planning programs, and environmental conditions
and economic issues. The infant mortality rate in Karanganyar Regency in 2017 was 12.7 /
1,000 birth live, a decrease compared to 2016 of 14.2 /1,000 birth live, while in 2015 it was
12.8 /1,000 birth live, 2014 was 10.5 /1,000 birth live, while in 2013 it was 9, 9 /1,000 birth
live, and in 2012 amounted to 10.1 /1,000 birth live. In 2017 there were 134 cases of infant
mortality, the most in the Karanganyar health center, which were 17 cases and the lowest in
the Ngargoyoso community health center in 2 cases.

9
2.3 Breastfeeding Policy
The Exclusive ASI Policy in Indonesia is regulated in Decree of the Minister of Health
No. 450 / MENKES / SK / IV / 2004 concerning Giving Breast Milk Exclusively to Infants in
Indonesia, PP No. 33 of 2012 concerning Exclusive Breastfeeding. In addition, the
government also supports it with Law No. 36 of 2009 concerning 29 Health Article 129
paragraph (2), PERMENKES No. 15 of 2013 concerning Procedures for Provision of
Breastfeeding Facilities and Minister of Women's Empowerment and Child Protection
Regulation No. 3 of 2010 concerning Application of Ten Steps to the Success of
Breastfeeding (Indonesia’s data and information center of Ministry of Health, 2017).
Article 35 of Government Regulation no. 33/2012 on Granting Exclusive Breastfeeding
obliges the workplace manager and the administrator of public facilities to introduce internal
regulations that support and aid successful breastfeeding programs. Such internal regulations
demonstrate enterprise support of breastfeeding and allow the enterprise to implement an
effective BFW policy through the following means: Establish decent workplace facilities for
working mothers to breastfeed/ breast-pump (nursing room), give working mothers the
opportunity to breastfeed/ express breast milk during working hours, ensure that the policy on
3 month maternity leave is more flexible. It will not always be necessary to have a 1.5 (one-
and-a half) month’s period of rest before giving birth and a 1.5 month’s period of rest after
giving birth, but it is advisable that the maternity leave is adjusted closer to the date of birth,
based on a reference letter from the doctor. This will allow a mother to have more time to
breastfeed after the birth and to prepare for her to return to work (Better Work Indonesia,
2013).
10
2.4 Exclusive Breastfeeding
2.4.1 Definition
According to the World Health Organization (2009), exclusive breastfeeding means that
the infant receives only breast milk. No other liquids, such as tea or herbal preparations, or
food are given – not even water – with the exception of oral dehydration solution, or
vitamins, minerals, or medicines in liquid form. If this practice is not continued for at least
six months, it does not meet the definition of exclusive breastfeeding. The WHO
recommends six months of exclusive breastfeeding for all newborns (Kumala, 2017; WHO,
2009).
2.4.2 The types of infant feeding
Two types of infant feeding, exclusive breastfeeding and complementary feeding.
Exclusive breastfeeding as receiving only breast milk and no other liquids or solids except
drops syrups consisting of vitamins, minerals, or medicines and complementary feeding as
the term which used for giving other foods and drinks in addition to breastfeeding after the
completion of the 6 months exclusive breastfeeding period. Including of replacement feeding
(formula) and mix feeding (breast milk and replacement feeding). According to WHO, this
process covers the period of growth during which infants are at high risk of nutrient
deficiencies and illnesses (Bai et al., 2009; Thurman & Allen, 2008; WHO, 2009).
2.4.3 Benefits of Breastfeeding
Breastfeeding has an extraordinary range of benefits. It has profound impact on a child’s
survival, health, nutrition and development. Breast milk provides all of the nutrients, vitamins
and minerals for infant needs for growth for the first six months, and no other liquids or food
are needed. Breastfeeding for the first six months decreases the infant’s risk of immune-
related diseases in the future. One reason is that breast milk carries antibodies from the
mother that help combat disease (Hirani, Karmaliani, Christie, Parpio & Rafique, 2013).
11
Breastfeeding also encourages mothers to pay closer attention to their infants’ mental and
physical health (Alves, Dowling, & Mahan, 2017).
Babies who get breast milk should develop good vision because breast milk contains
omega 3 fatty acids. Breastfeeding can also help babies learn to speak more quickly because
when breastfeeding the baby makes strong sucking movements that strengthen the cheek
muscles. In addition to being beneficial for babies, exclusive breastfeeding is also beneficial
for the mother. Breastfeeding the baby immediately after birth not only produces the
hormones that stimulate milk secretion, it can stimulate contractions of the muscles of the
uterus and prevent postpartum bleeding. In this way, it may also prevent iron deficiency
anemia and blood deficiency. Exclusive breastfeeding will also reduce maternal weight, as
the number of calories burned may be 200 to 500 calories (Roesli, 2009).
2.4.4 Factors Related to Exclusive Breastfeeding
A characteristic of personal factors, including demographic such as maternal age, marital
status, mother’s education, monthly family income, parity, mode of delivery, breastfeeding
experience and attitude so does breastfeeding-friendly workplace factors and social support
factors have been associated with exclusive breastfeeding.
2.4.4.1 Personal factors
More mature age will increase maturity in attitude and action (Arisdiani & Livana, 2016).
Mother who was young at first becoming a mother is also less to start breastfeeding
(Griffiths, Tate & Dezateux, 2005). Based on Silva et al. (2018) in their findings, maternal
age was statistically associated (p < .003) with exclusive breastfeeding, it is very likely that
older mothers have accumulated a more substantial prior experience, either because of
previous pregnancies or because of their receptiveness to the formal contacts with health
services where they were assisted during prenatal care, delivery and puerperium. As for
adolescents or young mothers, almost always with low or no parity, they face the demands of

12
pregnancy with greater insecurity, including the willingness to breastfeed. Dewi (2016) also
found that respondents aged between 18-35 years were more likely to breastfeed than
respondents who were <18 years old and the results of statistical tests proved there was an
influence between maternal age and breastfeeding status.
Previous studies have shown that marital status affects breastfeeding and showed that
married mothers are more likely to practice exclusive breastfeeding compared to unmarried
or widowed mothers (Jones, Kogan, Singh, Dee & Gummer-Strawn, 2011). This might be
related to greater family support for exclusive breastfeeding practices among married
mothers. For example, family members may help a new mother perform other household
tasks allowing her more time and energy for breastfeeding (Dhakal, Lee, & Nam, 2017).
According to Ferreira, Oliveira, Bernando, Almeida, Aquino, & Pinheiro (2018), women who
are not married but have significant others also are more likely to practice breastfeeding
exclusively than those without a life partner, suggesting that the key factor in studies linking
marital status and breastfeeding is social support. Because Ferreira included “significant
other” as a category, marital status did not show a significant statistical association with
exclusive breastfeeding (p=.90). Hunegnaw, Gezie and Teferra (2017) likewise found no
statistically significant relationship between exclusive breastfeeding and marital status
(p=.20).
Mothers’ education has been found to be related to exclusive breastfeeding. Ambarwati
and Wulandari (2010) found that, in Indonesia, a mother’s level of knowledge and education
has a positive effect on the frequency and pattern of breastfeeding. Another study conducted
in Indonesia likewise found that higher education was positively associated with exclusive
breastfeeding (Ratnasari, Paramashanti, Hadi, Yusistyowati, & Nurhayati, 2017). To explain
this finding, Ratnasari et al. proposed that highly educated people respond more rationally to
information they receive and use reason to weigh the benefits they might get from an idea.

13
For some mothers, Ratnasari et al. observed, breastfeeding is a natural and instinctive action.
Therefore, they assume that breastfeeding does not need to be studied. However, most
mothers in the study were less aware of the importance of breast milk as the baby's main
food. They only knew that breast milk was food that babies need, without being aware of the
specific benefits it confers (Ratnasari et al., 2017). But results of different studies may vary
regarding the effect of education on breastfeeding. For example, Hunegnaw et al. (2017)
found that mothers’ education had no statistically significant association with exclusive
breastfeeding. An Indonesian study by Kumala (2017) also found no significant relationship
between mother’s education and exclusive breastfeeding, with a p value of .202.
Family income is income from all family members living in one home that is used for
family shopping (Wendirati, Subagio, & Wijayanti, 2017). Some studies group family
income into two categories, high and low income (Wendirati et al., 2017).
A study conducted on 10,519 mothers in the US revealed that women with a higher
family income were more likely to exclusively breastfeed their infants than their lower
income counterparts (US Department of Health and Human Services, 2011). This might be
explained by an association between higher education and higher income, with higher income
mothers more aware of the benefits of breastfeeding. Conversely, studies from Saudi Arabia,
Peru and the Philippines all found that higher family income was associated with a reduced
initiation and duration of breastfeeding (UNICEF, 2011). This finding might be explained by
the fact that formula feeding is associated with higher status or higher income in some
countries. Many studies have shown that parity has an effect on the health of mothers and
children and directly affects breastfeeding (Mursyida & Wadud, 2013). A study conducted to
Ferreira et al. (2018) found that mothers who had experienced pregnancy and childbirth
before were more open to breastfeeding compared to mothers who had not. In a study by
Kaneko et al., 2006), the prevalence of exclusive breastfeeding increased with the number of

14
children a mother had. Mothers were more likely to breastfeed exclusively if they had three
or more children. They were more likely to use exclusive breastfeeding for the third child
compared to the second and first, so there was a significant relationship between parity and
exclusive breastfeeding. The study conducted by Kitano et al. (2016) also found that parity
was significantly associated with exclusive breastfeeding initiation.
A study by Fischer and colleagues (2013) found that both mode of conception and mode
of delivery affected the likelihood that a mother would breastfeed her baby exclusively.
Despite having a clear intention to do so, women who became pregnant through assisted
reproductive technologies such as IVF and those who had cesarean sections were more likely
to introduce infant formula before discharge from hospital. They were also more likely to
stop breastfeeding in the first four months after birth (Fisher et al., 2013). A study by
DiFrisco and colleagues found similar results, explaining that one of the consequences of
caesarean section is separating the mother and baby after delivery. This may disrupt the
relationship between them, as the first contact between mother and baby is not optimal, so the
mother is less likely to breastfeed the baby exclusively (DiFrisco et al., 2011).
Atindanbila, Mwini, Abasimi, Benneh & Avane (2014) likewise found that the mode of
birth impacted breastfeeding. Participants who had caesarian sections reported having
initiated breastfeeding a day after delivery, because nurses scheduled feeding times for babies
of mothers who had undergone caesarean section. By contrast, mothers who had spontaneous
vaginal deliveries initiated breastfeeding hours after delivery. DiFrisco and colleagues (2011)
found that mothers who breastfed within the first hour of birth were significantly more likely
to be exclusively breastfeeding at two-to-four weeks after discharge, than mothers who did
not breastfeed within the first hour of birth (DiFrisco et al., 2011).These results are similar
those of a study conducted in Western Australia which found that mothers who had a vaginal
delivery were almost twice as likely to breastfeed exclusively at hospital discharge compared
15
to mothers who had caesarean deliveries. This could be because the mothers who had
caesarean section deliveries were less comfortable and felt fatigue after the caesarean
procedure (Weber, Janson, Nolan, Wen, & Rissel (2011).
Mothers who have experienced lactation before tend to be better at breastfeeding than
mothers who have not, according to a study done in Indonesia. This prior experience made it
easier for such mothers to breastfeed exclusively (Purwanti, 2004). Similarly, Roig et al.
(2010) observed that not having breastfed a child previously was the variable with the highest
independent risk factor for abandoning exclusive breastfeeding within four months or less.
Mothers who successfully breastfed a previous child were more likely to succeed at
breastfeeding a second one.
Attitude is a reaction or response that is still closed from someone to stimulus or object,
attitude is not yet an action or activity, but it is a predisposition of an act of behavior
(Notoadmodjo 2012). According to Eagly and Chaiken (1993) in Leone (1995) review,
attitudes can be positioned as a result of evaluations of attitude objects, which are expressed
in cognitive, affective, and behavioral processes. So that the outline of the attitude consists of
cognitive components (ideas that are generally related to conversation and learning), behavior
(tends to affect the appropriate and inappropriate responses), and emotions (causing
consistent responses) (Wawan & Dewi, 2010). Attitudes towards and practices of exclusive
breastfeeding may differ among individuals, ethnic groups, countries, and even across
continents (Atindanbila et al., 2014).). In a study on attitudes and practices associated with
exclusive breastfeeding, Atindabila et al. (2014) found that most participants had a negative
attitude toward breastfeeding and did not practice exclusive breastfeeding effectively. These
findings were similar to a study conducted in Indonesia by Pertamasari et al. (2018) which
found that negative attitudes towards breastfeeding were significantly associated with weaker
or no intention to breastfeed exclusively.
16
2.4.4.2 Workplace friendly factors
Many studies have found that returning to work after childbirth affects breastfeeding.
Mothers who work full time generally worry about their babies and children at home. As
breastfeeding is the optimal nutrition for newborns and infants; with sufficient support in the
workplace, such as breastfeeding rooms and provision of childcare services on site, mothers
can both work and breastfeed their children at the same time (Ufamily, 2013). However, few
employers provide such facilities. A study conducted by Elyas, Mekasha, Admasie & Assefa
(2017) found that employed mothers had less opportunity to stay at home, compromising
their ability to breastfeed exclusively. Working mothers may have to leave their babies. Elyas
et al. (2017) found that only 43% of employed mothers breastfed their child for six months,
whereas mothers who were not working outside the home were 13% more likely to breastfeed
than working mothers. In addition, type of work and working hours also affect women’s
success at breastfeeding, in particular, length of the work day (Novayelinda, 2012).
Breastfeeding-friendly workplace policies can greatly influence women’s success at
exclusively breastfeeding their infants (Novayelinda, 2012). For example, some employers
provide a lactation room for pumping breast milk, equipment to store breast milk, and
babysitting services.
A recent study in Taiwan by Tsai (2013) supports the importance of a breastfeeding-
friendly workplace, finding that such policies figured into a complicated decision-making
process among employed mothers regarding whether and when to return to work. Women
employed in a labor-intensive work environment by a large electronics company who had
recently taken maternity leave completed questionnaires about their perceptions of
breastfeeding support at their workplace. They reported that they had access to a lactation
room and support for breastfeeding when raising their most recently born child. However, the
policies’ effectiveness was undermined by other aspects of the work environment including

17
pressure on the job; even though 85% of the mothers had access to a dedicated lactation
room, a substantial majority (63.8%) did not use pumping breaks, and more than half did not
continue to breastfeed after returning to work (Tsai, 2013).
Arranging physical facilities for breastfeeding in the workplace is one of the most
powerful interventions to promote breastfeeding among working mothers according to a
literature review by Hirani, Karmaliani, Christie, Parpio and Rafique (2013) that used only
studies with peer reviewed databases. Corroborating these findings, Yimyam and Hanpa
(2014) found that implementing a workplace breastfeeding support program significantly
raised the rate of exclusive breastfeeding and any breastfeeding at six months. The key to
success at exclusive breastfeeding for working mothers lies in the methods of expressing and
storing breast milk (breastfeeding management), according to a study on obstacles to
breastfeeding among working women (Better Work Indonesia, 2013). They found that the
difficulty of pumping and the risk of breast milk spoiling are the most common reasons why
working mothers stop breastfeeding. Therefore, it is important that workplaces have a
suitable nursing room and allow enough time for working mothers to express their breast
milk for the sake of children’s health (Better Work Indonesia, 2013). These studies
recommend that a breastfeeding room should offer privacy, accommodate breast pumps
(sufficient electrical outlets), and refrigerated storage facilities for breast milk, as well as
childcare facilities on site (Better Work Indonesia, 2013; Hirani et al., 2013).
2.4.4.3 Social support factors
Nursalam (2009) states that individuals included in providing social support include
spouses, parents, children, relatives, friends, health teams or counselors. According to
Ratnasari et al. (2017), support from the family will improve exclusive breastfeeding
compliance if health workers explain to the family the benefits of breast milk for babies after
returning to work, so that they will encourage the woman. Families can help out by providing
18
childcare, buying or making food, and also feeding the child expressed breast milk. Ratnasari
and colleagues concluded that adequate family support was significantly associated with
practicing exclusive breastfeeding. This finding is consistent with results from other studies
that also found family support can increase the rate of exclusive breastfeeding (Permatasari et
al., 2018; Sari, Yosi, & Nella, 2015).
A study conducted by Palupi and Devi (2016) in Indonesia showed that social support
tended to be positive but low. Low support led the mothers to give up on breastfeeding when
they encountered obstacles that were relatively hard for them to overcome, even though the
situations would have been surmountable if the mothers had received adequate information
and been highly motivated to breastfeed.
2.5 Conclusion and Conceptual Framework
Exclusive breastfeeding is influenced by a range of factors, including personal factors
such as demographic characteristics, social support, and workplace breastfeeding policies.
However, information about exclusive breastfeeding among employed mothers has received
limited attention so far. Of all these factors, having a breastfeeding friendly workplace is one
of the most impactful. Hence, understanding the factors related to exclusive breastfeeding
may help employed mothers continue to breastfeed their children after returning to work.

19
Figure 2.2 Conceptual framework
Personal factors:
1. Age
2. Marital Status
3. Mothers Education
4. Monthly Family Income
5. Parities
6. Attitude
7. Mode of Delivery
8. Breastfeeding Experience
Social support factors:
1. Family support
2. Friends
3. Significant others
Workplace friendly factors:
1. Workplace organization
support
2. Manager support
3. Co-worker support
4. Time support
5. Physical Environment
Support
6-month Exclusive
Breastfeeding types
1. Exclusive
breastfeeding
2. Not Exclusive
breastfeeding

20
Chapter Three
Methodology
This study was carried out among employed mothers in Karanganyar Regency who have
returned to work after having a child. A descriptive correlational design was used to identify
factors that influence exclusive breastfeeding. These included personal factors such as age,
marital status, mother’s education, monthly family income, parity, mode of delivery,
breastfeeding experience and attitude. The study also explored breastfeeding-friendly
workplace factors, such as workplace organization support, manager support, co-workers’
support, time provided for breastfeeding, and the physical environment for breastfeeding at
work. The study also investigated social support factors related to exclusive breastfeeding,
which included support from family, friends, and significant others. The instruments
(Appendix 1) used to explore our research questions were a demographic questionnaire for
the personal factors, the lowa Infant Feeding Attitude Scale (IIFAS), the Breastfeeding and
Employment Study (BESt) for assessing workplace-related factors, and the Multidimensional
Scale of Perceived Social Support (MSPSS).
3.1 Research Design
A descriptive correlational design was used among the employed mothers who were
willing to take part in this study. A convenience sampling was made to choose research
subjects and to ensure that they agreed to participate in the study by signing a consent inform
(Appendix 2).
3.2 Research Setting
Karanganyar Regency, one of the cities in Central Java, is a land and mountains with a
very varied altitude. The height of the region up to 100 meters above sea level, covering the
District of Jaten and Kebakkramat (8.11%). The height of 101-500 meters above sea level
covers Jumantono, Karanganyar, Tasikmadu, Colomadu, Gondangrejo, Mojogedang and

21
Kerjo (45,32%), 501-1,000 meters above sea level, covering Jatiyoso, Jatipuro, Matesih,
Tawangmangu (partly), Ngargoyoso (partly), Karangpandan and some of Jenawi Subdistrict
(36.59%). And the altitude of 1000 meters above sea level, covers part of the District of
Tawangmangu, Ngargoyoso and Jenawi (9.98%). While the total area is 773.8 km2 or 2.73%
of the total area of Central Java Province.
This study was carried out on Primary Health Center in Karanganyar. Based on data from
the Population and Civil Registry Service (Disdukcapil), Karanganyar Regency in 2017 has
21 Primary Health Cares they are primary health care of Jatipuro, Jatiyoso, Jumapolo,
Jumantono, Matesih, Tawangmangu, Ngargoyoso, Karangpandan, Karanganyar, Tasikmadu,
Jaten I, Jaten II, Colomadu I, Colomadu II, Gondangrejo, Kebakkramat I, Kebakkramat II,
Mojogedang I, Mojogedang II, Kerjo and Jenawi.
3.3 The Inclusion Criteria and Exclusion Criteria
3.3.1 Inclusion Criteria
The target population for the study was comprised all an employed mothers after
returning to work and who met the following criteria : Mothers whose infants aged 6-12
months (even though WHO recommendation for breastfeeding is up to 2 years, the researcher
only limited the sample aged only 6-12 months due to memory recall issues), mothers who:
work outside home, gave birth by vaginal or cesarean section delivery, were 18 years and
older, were able to read and write Indonesia language, agreed to participate in the study.
3.3.2 Exclusion Criteria
Infants who were adopted, severely ill (hospitalized in intensive care units), infants who
had medical indications to receive breast milk substitutes mothers.
3.4 Sample Size

22
The sample size was determined based on the calculation validated by G-Power software
version 3.1.2 (Faul, Erdfelder, Buchner, & Lang, 2009). Based on logistic regression where
Power = .8, alpha (α) = .05, assuming the probability of a mother giving breastfeeding is
50% and the mother with better workplace one more likely to have higher probability
assuming 60 % so the calculation of the odd ratio is with 1.5 thus suggesting a sample size of
208 subjects (Figure 3). Sample was collected from 21 primary health cares. Each primary
health care was drawn 13 or more respondents and data was collected in 4 months (July -
November 2019).

23
3.5 Instruments
Three instruments were used in this study including demographic data sheet. In order to
collect the data related factors which associated with exclusive breastfeeding among
employed mothers were used three kind instruments, they are Iowa Infant Feeding Attitude
Scale (IIFAS) for the Attitude, breastfeeding and employment study (BESt) for the workplace
friendly factors and the multidimensional scale of perceived social support (MSPSS) for
social support factors. Permission to use these questionnaires was obtained via email contact
with the authors, who provide a copy of the questionnaire to the researcher (Appendix 3, 4
and 5).
3.5.1 Exclusive Breastfeeding
Exclusive breastfeeding refers to infants receiving only breast milk during the first six
months of life, and not food or even water, including other liquids like tea and herbal
preparations, except for doctor-recommended vitamins, mineral supplements, or medicines
(WHO, 2009).
The dependent variable of this study is Exclusive breastfeeding and a measurement was
used of Exclusive breastfeeding in this study is the types of infant feeding practice, which
included exclusive breastfeeding, mix breastfeeding and formula feeding, for the exclusive
breastfeeding was coded as “1”, mix breastfeeding and formula feeding were coded as “0”.
3.5.2 Demographic Information
The researcher created the demographic information for this study using factors from
previous studies found to be associated with exclusive breastfeeding. The demographic
information including 8 items, including maternal age, marital status, education level, parity,
family monthly income, modeof birth, breastfeeding experience, and attitude toward to
breastfeeding. Marital status was categorized into single which was coded “0” and married
which was coded as “1”. Mother education was categorized into juniro high school which

24
was coded ‘0” and senior high school or above was coded “1”. Parity was categorized into
primigravida which will was coded “0” and multigravida was coded as “1”. Monthly family
income, the District or City Minimum Wage of Karanganyar Regency is 1.833.000 IDR
based on Central Java Governor Decree No. 560/68/2018 so for monthly family income was
divided into low income (< 1,833,000 IDR) which was coded ‘0” and high income
(≧1,833,000 IDR) was coded as “1”. Mode of delivery was categorized into vaginal delivery
which was coded “0”, caesarean section was coded as “1”. Breastfeeding experience was
categorized into experienced which was coded “0” and not experienced which was coded as
“1”. Attitude which used The IIFAS (Iowa Infant Feeding Attitude Scale, the IIFAS appears
to be very reliable, with Cronbach's alpha ranging from .85 to .86 (De la Mora et al., 1999).
The IIFAS consist of 17 attitude questions, half of which are favorable to breastfeeding and
the remaining favorable to artificial feeding. Higher IIFAS score means more positive
attitude toward to breastfeeding. Items of favorable to artificial feeding were reverse
computing the score.
3.5.3 Breastfeeding and employment study (BESt)
It was used to collect data (Greeneet al., 2008). BESt contains 41 items that require either
categorical yes/no or Likert scale responses, the categorical yes has score 1 and no has score
0 and the Likert scale has 4 score for strongly agree, 3 for agree, 2 for disagree and 1 for
strongly disagree. The survey items are grouped together to evaluate five aspects of the work
climate : organization support (11 items), manager support ( 12 items), co-worker support
(six items), time support (three items) and physical environment support (nine items) and this
instrument has 5 items negative and it will be reverse in computer for scoring the result.
Internal consistency reliability coefficients of the BESt were high (.87 and .89) and the
correlation between the subscales was moderately strong (r =.68) in the pilot study (n=104)
(Greene et al., 2008). The item of organization support, the highest score is 44 (low support:

25
1- 14, moderate: 15 - 28 and high support: 29 - 44). The Management support is 48 (low
support: 1 - 16, moderate: 17 - 32 and high support: 33 - 48). Co-worker support is 24 (low
support: 1 - 8, moderate: 9 - 18 and high support: 19 - 24). Time is 12 (low support: 1 - 4,
moderate: 5 - 8 and high support: 9 - 12). Physical environment is 24 (low support: 1 - 8,
moderate: 9 - 16 and high support: 17 - 24).
3.5.4 Multidimensional scale of perceived social support (MSPSS)
This study measured social support using the MSPSS. The MSPSS was developed by
Zimet et al. in 1988. The MSPSS is a 12-item instrument. It measures social support on three
subscales: (1) the Significant Other Subscale (items 1, 2, 5, & 10); (2) the Family Subscale
(items 3, 4, 8, & 11), and (3) the Friends Subscale (items 6, 7, 9, & 12). For the Significant
Other, Family, and Friends subscales, the alpha values were .91, .87, and .85, respectively.
Reliability of the overall scale was .88 (Zimet et al., 1988). Each item is rated according to a
seven-point Likert-type response format, with 1 indicating very strongly disagree and 7
indicating very strongly agree. An overall any mean scale score ranging from 1 to 2.9 could
be considered low support; a score of 3 to 5 could be considered moderate support; a score
from 5.1 to 7 could be considered high support.
3.6 Translation and Pilot Study
This study was carried out among employed mothers in Indonesia especially in
Karanganyar Regency. Validation of cross-cultural research instruments is very important
because of the variety of the global population (Sousa & Rojjanasrirat, 2011).
To ensure the quality of the instrument, the researcher arranged for the translation and the
results was examined with a forward and backward translation. The questionnaire of this
study was translated by three translators (Appendix 6, 7 and 8) with the following steps.
26
3.6.1 Translating from the source to the target language
The first translator translated the original English version into the target language,
Indonesian.
3.6.2 Blindly translating back from the target to the source
Re-translation is translating from the newly translated version back to the original source
language (Brislin, 1970). The second translator re-translated the instrument from the first
translator’s new Indonesian version back into English.
3.6.3 Comparing the two versions in the original language
It is possible to evaluate the equivalence of the instrument in its original language and the
target language version of the instrument (Brislin, 1970). The results of the two previous
translations were examined by an English language medical editor with 18 years of
experience editing medical journal articles.
The researcher and the two translators together evaluated the original text of the
instrument and the two translations, one in Indonesian and the back-translation into English.
After reaching agreement, the researcher then had a discussion with an expert, the English
language medical editor mentioned above. There were several points of difference between
the translated English version and the original one.
On item no 2, “I will be able to get information about combining work and
breastfeeding,” thetranslated version was, “I will get information about the regulation at work
while breastfeeding.” The Indonesian version used the word “regulation” while the original
question did not. “Regulation” in Bahasa is peraturan, while the original version only
mentioned “information,” informasi in Bahasa. So the researcher and the medical editor
agreed to delete the terms “regulation” and “peraturan” in the English and Indonesian
translations. The new Indonesian version says roughlyi, “I will get information about
breastfeeding at work.”

27
On item no 6, the original version “My job sould be at risk”,the back-translated version
was, “becomes risky,” while the original version used “at risk.” The editor pointed out that
the phrase “becomes risky” sounds like the job becomes physically dangerous. Indonesian,
“becomes risky,” beresiko, has a meaning similar to the meaning of the original version,
while the original term, “my job is at risk” means “I could lose the job.” So the researcher
and the medical editor agreed to substitute the term “at risk” for “becomes risky.”
On item no 8, the original version “I would feel comfortable asking for accommodations
to help me breastfeed” uses the term “accommodations” which mean a place or facility, while
the back-translated version did not mention it. In Indonesian, the translator only used
membantu, which means “helping.The back-tranlsated English was, “I feel comfortable
asking the company to help me breastefeed or pump breastmilk at the workplace.” “in
Indonesian, in the phrase is “menyediakan sesuatu untuk memenuhi kebutuhan,” means
approximately, “to provide something to fulfill a need.” In the back-tranlsated English
version, it sounds as if the company might literally help by squeezing a breast. So the
researcher and the editor agreed to put the term “menyediakan sarana” into the Indonesian
version.
In item no 13, “My manager would help me combine breastfeeding and work” the
original item used the term, “combine,” while the back-translated version did not. The
original phrase, “the manager will help me combine breastfeeding and work,” which means
that the manager will help arrange the work schedule and workload, while the Indonesian
version did use the term “combine.” In Bahasa combine means “menggabungkan beberapa
hal”. So researcher and the editor agreed to put term “combine” into the sentence.
In item no 18, the original version “my manager would consider it part of his/her job to
help me combine breastfeeding and work” while the back-traslated mention “my manager
will assume that one of his/her duties is helping me to breastfeed while working”,.the back-

28
translated version mentioned “helping to breastfeed while working” while the original
version said “ helping combine breastfeeding and work”. The term of “while working” is
slightly different than “at work”. In Indonesian, “while working” means “selama bekerja”
and “at work” means “saat bekerja”. The editor pointed out that the back translated version
suggested the respondent would be simultaneously breastfeeding while working. So the
researcher and the editor agreed to make sure the Indonesian version carried the idea of
“enabling the employee to breastfeed while at work”.
Item no 19, the original version mentioned “my manager would think less of workers who
choose to breastfeed or pump breast milk at work”, while the back-translated version
mentioned “manager will think that a few employees”, meaning “a small number of the
employees” while the original version used the phrase “the manager will think less of
workers.” The meaning differed from the original. To think less of someone—the original
text—means to look down on that person, to respect them less than before. So the researcher
and the editor decided to put Indonesian term “meremehkan”. The new Indonesian version
says roughly “think less/ to look down on that person”.
Item no 20, the translated version mentioned “will assure my work is handled”, which
seems to say that the manager will be confident that the worker is handling it. While the
original version mentioned “the job will covered,” which means that the manager will assign
another employee to cover the responsibilities while the respondent is breastfeeding or
pumping breast milk. So the researcher and the medical editor decided to put “digantikan
sementara” meaning roughly “the job will covered”.
Item no 28, the translated version included the word “replace” which in Indonesian is
“menggantikan”. While in original version used the word “covered” which in Indonesian is
“ditutupi/ digantikan”. The back-translated term “replace” sounds like the respondent is
permanently losing the job. The English word “cover” means to temporarily fill in for

29
someone else. So researcher and the medical editor decided to put sentence “digantikan”
meaning roughly, “to temporarily play someone’s role.”
The Iowa Infant Feeding Attitude Scale. Item no 6, the original version mentioned
“Breasfed babies are more likely to be overfed than formula-fed babies”, while in the back-
translated instrument,”A breastfed baby will have greater appetite than baby with milk
formula” using the phrase, “have greater appetite,” while the original version used the phrase
“to be overfed”. Those two meanings differ. “Have greater appetite” means
“to desire more food,” while “overfed” means to ingest too many calories. So the researcher
and the medical editor decided not to put “have greater appetite” but put the term “resiko
kegemukan”, meaning approximately, “to be overfed”.
A pilot study was carried out with five participants to check whether the questionnaire
would be easy for participants to follow.
3.7 Data Collection
Sample of this study were employed mothers. Researcher got the data of employed
mothers from the midwife in primary health care. The researcher made a permission letter
which forwarded to the Health Department of Karanganyar Regency. After receiving the
permission, the researcher handed the permission letter (Appendix 9) from Health
Department to Primary Health Care at Karanganyar Regency. Researcher have two persons
who helped her to collect the data, they had been trained by following the researcher how to
collect it. Then the respondents were approached door to door in their homes.
In Primary Health Care, the researcher got the data about the participant then screening
the participant to see if they meet inclusion criteria. Researcher explained the purpose of the
study to the participants. Those participants were signed the consent form and were given a
self-administered questionnaire. Once the participant was through answering the
questionnaire, the researcher went over the data collection forms to ensure their
30
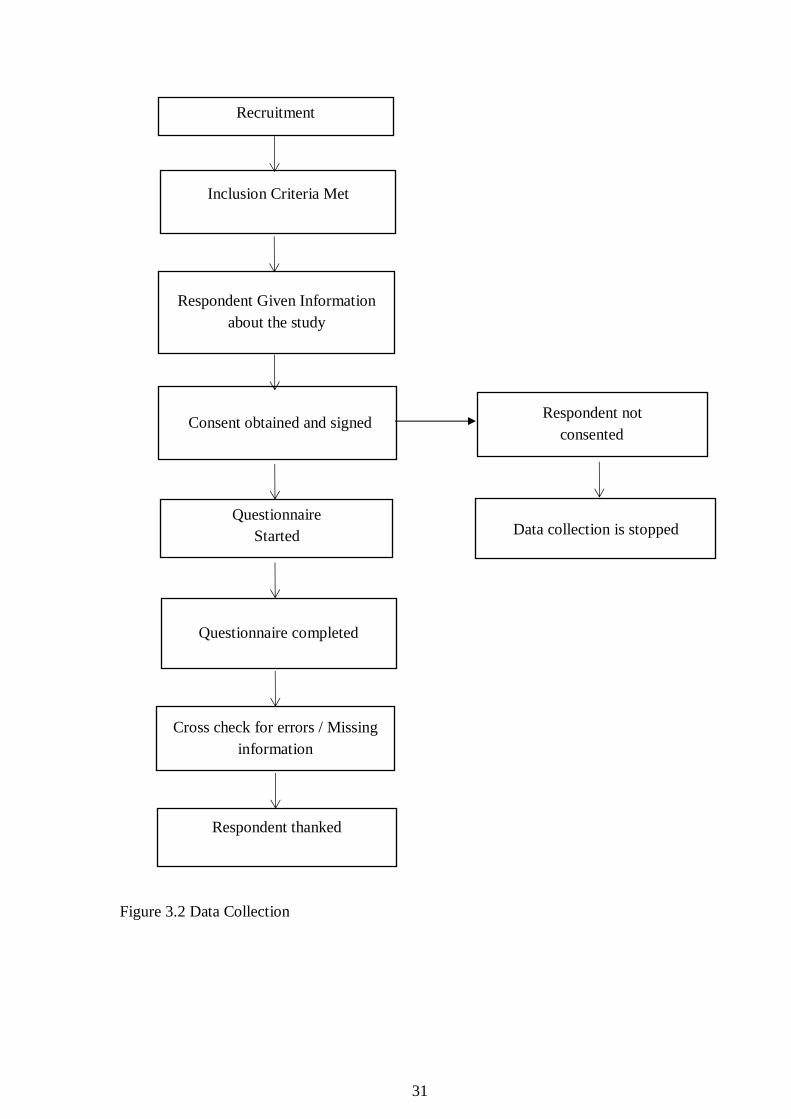
completeness. Then the questionnaire was collected by the researcher (Figure 3.2). The
instrument was used in this study included the Exclusive breastfeeding mode at six months,
the breastfeeding and employment sudy (BESt), the Multidimensional Scale ofPerceived
Support (MSPSS) and the demographic information.
31
Figure 3.2 Data Collection
Recruitment
Inclusion Criteria Met
Respondent Given Information
about the study
Consent obtained and signed
Questionnaire
Started
Cross check for errors / Missing
information
Questionnaire completed
Respondent thanked
Respondent not
consented
Data collection is stopped

32
3.8 Data analysis
Each participant was provided with a unique code. Data was entered into Microsoft excel
and then was analyzed using SPSS 22.0 software. Descriptive statistics including frequency
and percentage were used for the discontinuous variables. Mean and standard deviation were
used for continuous variables. The t-test was applied to compare the mean differences
between feeding types and workplace friendly, personal factors (age, monthly family income)
and social factors. Chi-Square was applied to determine the relationship between feeding
types and personal factors (education, marital status, parity, attitude, mode of delivery and
breastfeeding experience). Furthermore, the significant variables were entered into binary
logistic regression analysis to identify the predictors of dependent variables.

33
No Research Question Variable Variable Type
Analysis
Strategy
1
What is the
relationship between
exclusive
breastfeeding rates
among employed
mothers returning to
work and
breastfeeding-friendly
practice ?
DV : Types of
breastfeeding
practices
IV: Breastfeeding-
friendly workplace
practice
DV : Categorical
IV: Continuous
t-test
2
What are the
relationships between
personal factors
including
demographic,
obstetrical, attitudes
and exclusive
breastfeeding among
employed mothers
after returning to
work ?
DV : Types of
Breastfeeding
practices
IV : Personal Factor :
(1) Education,
Marital Status, Parity,
Mode of Delivery,
Monthly Family
Income and
Breastfeeding
Experience
(2) Age and Attitude
DV: Categorical
IV :
(1) Categorical
(2) Continuous
1. Chi-
Square
2. t-test
3
What is the
relationship between
social support and
DV : Types of
Breastfeeding
DV : Categorical
t-test

34
No Research Question Variable Variable Type
Analysis
Strategy
exclusive
breastfeeding among
employed mothers
returning to work ?
practices
IV : Social Support
IV : Continuous
4
Which factors-personal
(demographic,
obstetric and attitude),
workplace and social
support- are the most
important for
predicting exclusive
breastfeeding among
employed mothers
returning to work ?
DV : Types of
Breastfeeding
practices
IV : Personal factors,
breastfeeding
workplace-friendly
and social support
DV : Categorical
IV : Continuous
or categorical
Binary
Logistic
Regression
Table. 1: Table of Data Analysis

35
3.9 Ethical Consideration
The study was granted permission prior to its commencement during summer vacation.
Researcher was applied and obtained the permission to conduct this study from Institutional
Review Board (IRB) in Indonesia (Appendix 10). A letter of request was sent to Department
of Health in Karanganyar then was forwarded to the Primary Health Care. Participant who
agreed to fill in the questionnaire were informed about the importance of the study and its
main purpose. Those participants in this study were given the inform consent. For protecting
the data subjects, researcher provided guarantees in the use of research subjects by not giving
or including the name of the respondent on the measuring sheet and only writing the code for
the data collection sheet or the results of the research to be presented. All information that
were collected is guaranteed confidentiality by researcher; only certain data groups was
reported on the results of research.

36
Chapter Four
Results
In this chapter, the results from this research on factors associated with six months of
exclusive breastfeeding among employed mothers after returning to work are discussed under
the following headings: characteristics of demographic variables, workplace breastfeeding
friendly and social support.
4.1 Characteristics of Research Subjects
This study was conducted in August 2019 in Karanganyar, one of the cities in Central
Java. The researcher went door-to-door to talk with working women with children ages 6 to
12 months, as shown in Table 4.1. A total of 208 subjects completed the questionnaires.
The ages of the subjects participating in this study ranged from 18 to 40 years with
mean age of 28.80 (SD 5.46). All of the respondents in this study (100 %, n=208) were
married. The mean age of their babies was 8.95 months (SD 1.89).
The women’s level of education is expressed as a binary category: elementary school
and junior high school on the one hand, and senior high school, diploma (one to three years
of college), or bachelor (completed four years) on the other hand. Less than half of the study
participants (39%, n=39) had completed junior high school, while the majority of them 81%
(n=169) were categorized as senior high school/diploma/bachelor.
More than two-thirds of the respondents 60% (n=125) had monthly family income
≥1,833,000 IDR. For the parity, 39% (n=81) were primigravidas. About 65% (n = 130) of the
respondents had experienced vaginal delivery. Most of the study participants (61%, n=127)
had experience breastfeeding.

37
Table 4.1 Demographic characteristics of the study participants (N=208)
Variables n % Mean SD
Age (yrs) 28.80 5.46
Age of Baby (months) 8.95 1.89
Marital Status
Married 208 100
Education
Junior High School 39 19
Senior High School/Above 169 81
Monthly Family Income (IND)
< 1.833.000 83 40
≥ 1.833.000 125 60
Parity
Primigravida 81 39
Multigravida 127 61
Mode of Delivery
Vaginal delivery 130 63
Cesarean Section 75 36
Forceps/Vacuum 3 1
Previous Breastfeeding experience
No
Yes
6 Months of Exclusive Breastfeeding
Not breastfeeding exclusively
Exclusive breastfeeding
81
127
55
153
39
61
26
74
4.2 Descriptive statistics of the outcomes variables
Descriptive statistics for this study consist of the total scores on three instruments: the
Breastfeeding and Employment Study (BESt) (which includes organization support, manager
support, co-worker support, time support and physical environment support); the

38
Multideminsional Subscales of Perceived Social Support (MSPSS) (which includes family,
friends, and significant others); and scores on the Iowa Infant Feeding Attitude Scale
(IIFAS).
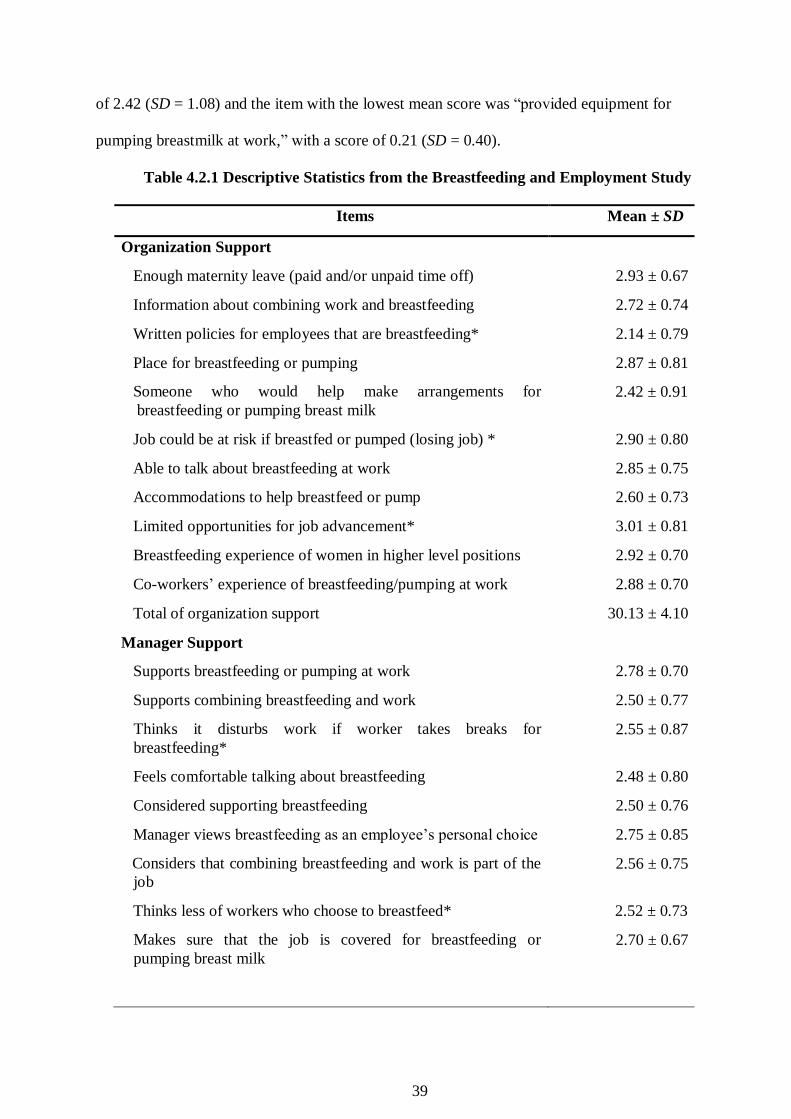
4.2.1 Breastfeeding and Employment Study (BESt)
The categories of the breastfeeding and employment survey included organization
support, manager support, co-worker support, time support, and physical environment
support. The organization support consisted of 11 items, which were all continuous variables.
According to Table 4.2.1, the item with the highest mean score was “limited opportunities for
job advancement” with a score 3.01 (SD = 0.81) and the item with the lowest mean score was
“written policies for employees that are breastfeeding” with a score 2.14 (SD = 0.79).
Manager support consisted of 12 items and the item with the highest mean score was
“support for breastfeeding or pumping at work,” with a score of 2.78 (SD = 0.70) and the
item with the lowest mean score was “Suitable schedule to allow the employee to breastfeed
or pump breast milk,” with a score of 2.30 (SD = 0.62). Co-worker support consisted of six
items. The item with the highest mean score was “thought of supporting breastfeeding” with
a score of 2.93 (SD = 0.65) and the item with the lowest mean score was “covered others’ job
duties to allow mothers to breastfeed or pump,” with a score of 2.53 (SD = 0.70). Time
support, meaning adequate time for breastfeeding or pumping milk, consisted of three items.
The item with the highest mean score was “Frequent enough breastfeeding or pumping breast
milk (at work),” with a score of 2.86 (SD = 0.80) and the item with the lowest mean score
was “time (at work) long enough for breastfeeding or pumping breast milk,” with a score of
2.63 (SD = 0.80). For physical environment support, which means having sufficient facilities,
space, tools and privacy, consisted of nine items. The item with the highest mean score was
“a designated place was available for breastfeeding or pumping when needed,” with a score
39
of 2.42 (SD = 1.08) and the item with the lowest mean score was “provided equipment for
pumping breastmilk at work,” with a score of 0.21 (SD = 0.40).
Table 4.2.1 Descriptive Statistics from the Breastfeeding and Employment Study
Items Mean ± SD
Organization Support
Enough maternity leave (paid and/or unpaid time off) 2.93 ± 0.67
Information about combining work and breastfeeding 2.72 ± 0.74
Written policies for employees that are breastfeeding* 2.14 ± 0.79
Place for breastfeeding or pumping 2.87 ± 0.81
Someone who would help make arrangements for
breastfeeding or pumping breast milk
2.42 ± 0.91
Job could be at risk if breastfed or pumped (losing job) * 2.90 ± 0.80
Able to talk about breastfeeding at work 2.85 ± 0.75
Accommodations to help breastfeed or pump 2.60 ± 0.73
Limited opportunities for job advancement* 3.01 ± 0.81
Breastfeeding experience of women in higher level positions 2.92 ± 0.70
Co-workers’ experience of breastfeeding/pumping at work 2.88 ± 0.70
Total of organization support 30.13 ± 4.10
Manager Support
Supports breastfeeding or pumping at work 2.78 ± 0.70
Supports combining breastfeeding and work 2.50 ± 0.77
Thinks it disturbs work if worker takes breaks for
breastfeeding*
2.55 ± 0.87
Feels comfortable talking about breastfeeding 2.48 ± 0.80
Considered supporting breastfeeding 2.50 ± 0.76
Manager views breastfeeding as an employee’s personal choice 2.75 ± 0.85
Considers that combining breastfeeding and work is part of the
job
2.56 ± 0.75
Thinks less of workers who choose to breastfeed* 2.52 ± 0.73
Makes sure that the job is covered for breastfeeding or
pumping breast milk
2.70 ± 0.67

40
Items Mean ± SD
Makes suitable schedule to allow the employee to breastfeed or
pump breast milk
2.30 ± 0.62
Helps dealing with the workload to allow for breastfeeding or
pumping
2.38 ± 0.74
Embarrassed to speak about breastfeeding* 2.66 ± 0.61
Total of Manager Support 30.21 ± 5.63
Co-Worker Support
Thinks less of workers who choose to breastfeed* 2.54 ± 0.66
Feels comfortable speaking about breastfeeding 2.85 ± 0.60
Considered supporting breastfeeding 2.93 ± 0.65
Willing to switch the break times to breastfeed 2.64 ± 0.71
Covered the job duties to allow mothers breastfed or pumped 2.53 ± 0.70
Embarrassed to speak about breastfeeding* 2.72 ± 0.75
Total of Co-Worker Support 15.71 ± 2.47
Time Support
Frequent enough opportunities for breastfeeding or pumping
breast milk at work
2.86 ± 0.80
Long enough time for breastfeeding or pumping breast milk 2.63 ± 0.80
Adjust the break schedule in order to breastfeed or pump 2.80 ± 0.92
Total of Time Support 8.28 ± 2.29
Environment Support
Considering buying or borrowing the equipment for
breastfeeding or pumping breast milk
0.73 ± 0.44
Company provides equipment for pumping breastmilk at work 0.21 ± 0.40
Company provides place to store expressed breast milk at work 0.41 ± 0.50
There is a company-designated place for women to breastfeed
or pump milk during the workday
0.67 ± 0.47
There is a designated place for breastfeeding or pumping
available when needed
2.42 ± 1.08
The designated place is close enough to the work area to use
during a break
2.31 ± 1.04
The designated place is comfortable for breastfeeding or
pumping
2.28 ± 1.13

41
Items Mean ± SD
The designated place for breastfeeding or pumping is
satisfactory
2.19 ± 1.08
The designated place for breastfeeding or pumping includes
everything needed
2.06 ± 1.04
Total of Environment Support 13.27 ± 6.30
* Reverse items have been recoded
4.2.2 Multidimensional Scale of Perceived Social Support Scores (MSPSS)
Multideminsional Subcales of Perceived Social Support (MSPSS) includes the
categories of family, friends, and significant others. The descriptive analysis is in
Table 4.2.2. The family support consisted of four items. The item with the highest
mean score was “my family is willing to help me make decisions” with a score of
6.04 (SD = 0.73) and the item with lowest mean score was “I can talk about my
problems with my family,” with a score of 5.88 (SD = 0.84).
Support from friends consisted of four items. The item with the highest mean
score was “I have friends with whom I can share my joys and sorrows” with a score
of 5.62 (SD = 1.03) and the item with the lowest mean score was of “I can count on
my friends when things go wrong” with a score of 5.33 (SD = 1.15).
Support from significant others, which in this study included husbands and
health workers, consisted of four items. The item with the highest mean score was
“There is a special person in my life who cares about my feelings” with a score of
6.08 (SD = 0.78) and the item with the lowest mean score “There is a special person
who is around when I am in need” with a score of 5.75 (SD = 1.02).

42
Table 4.2.2 Descriptive Statistics of Multidimensional Scale of Perceived Social Support
Items Mean ± SD
Family
My family really tries to help me 5.98 ± 0.79
I get the emotional help and support I need from my family 5.93 ± 0.89
I can talk about my problems with my family 5.88 ± 0.84
My family is willing to help me make decisions 6.04 ± 0.73
Total Family Support 23.82 ± 2.51
Friends
My friends really try to help me 5.60 ± 1.05
I can count on my friends when things go wrong 5.33 ± 1.15
I have friends with whom I can share my joys and sorrows 5.62 ± 1.03
I can talk about my problems with my friends 5.60 ± 1.05
Total Friends Support 22.14 ± 3.47
Significant Others
There is a special person who is around when I am in need 5.75 ± 1.02
There is a special person with whom I can share my joys and sorrows 5.76 ± 0.95
I have a special person who is a real source of comfort to me 5.94 ± 0.80
There is a special person in my life who cares about my feelings 6.08 ± 0.78
Total Significant Others Support 23.53 ± 2.72
4.2.3 Iowa Infant Feeding Attitude Scale (IIFAS)
The IIFAS consists of 17 items, half of which are favorable to breastfeeding and the
remaining are favorable to artificial feeding. The mean score obtained for the IIFAS was 58.9
(SD = 7.96).

43
Table 4.2.3 Descriptive Statistics of Iowa Infant Feeding Attitude Scale
Items Mean ± SD
The benefit of breastmilk lasts only as long as the baby is fed* 3.31 ± 1.19
Formula feeding is more convenient than breastfeeding* 3.12 ± 1.27
Breastmilk is lacking in iron* 2.51 ± 1.05
Formula feeding is the better choice if the mother plans to go out to work* 3.32 ± 1.11
Women should not breastfeed in public places* 3.70 ± 1.15
Breastfed babies are more likely to be overfed than formula-fed babies* 3.45 ± 0.90
Fathers feel left out if a mother breastfeeds* 2.28 ± 0.87
Formula is as healthy for an infant as breast milk* 2.80 ± 1.10
A mother who occasionally drinks alcohol should not breastfeed her baby* 3.68 ± 1.11
Breastfeeding increases mother-infant bonding 4.30 ± 0.70
Formula-fed babies are more likely to be overfed than breastfed babies 3.32 ± 0.96
Mothers who formula feed miss one of the great joys of motherhood 3.05 ± 1.10
Breastfed babies are healthier than formula fed babies 3.83 ± 1.03
Breastmilk is the ideal food for babies 4.36 ± 0.67
Breastmilk is more easily digested than formula 4.34 ± 0.69
Breastfeeding is more convenient than formula 4.40 ± 0.58
Breastfeeding is cheaper than formula 4.46 ± 0.60
Total Score 58.9 ± 7.96
* Reverse items have been recoded
4.3 Relationship between personal factors, breastfeeding and employment study scores,
and social support for different types of breastfeeding
To identify whether there is robust evidence about the relationship, univariate
analyses were performed using the independent samples t-test and Chi-Square. The
results are summarized in Tables 4.3.1, 4.3.2 and 4.3.3.

44
4.3.1 Relationship between personal factors and different breastfeeding types
A univariate analysis to identify associations between personal factors
(demographic characteristics) and exclusive breastfeeding was performed using the
independent sample t-test (continuous variables with breastfeeding types) and Chi-
square (categorical variables with breastfeeding types). None of the personal variables
and obstetrics variables were statistically significantly related to breastfeeding type (p
>.05).
Table 4.3.1 Relationships between personal factors and breastfeeding types (N=208)
Variables Total N (%)/
Mean ± (SD)
Exclusive
Breastfeeding
Not Exclusive
Breastfeeding
t/χ2 p
Age 28.80 ± 5.46 29.08 ± 5.32 28.07 ± 5.80 1.191a .235
Age of Baby 8.95 ± 1.89 9.11 ± 1.86 8.63 ± 1.92 1.643a .102
Marital Status
Married
151 (72.6)
57 (27.4)
Education
Junior High School
Senior High School/ Above
26 (17.2)
125 (82.8)
13 (22.8)
44 (77.2)
0.848b
.357
Monthly Family Income
< 1.833.000
≥ 1.833.000
59 (39)
92 (61)
24 (42.1)
33 (57.9)
0.1b
.690
Parity
Primigravida
Multigravida
58 (38.5)
93 (61.5)
23 (40.4)
34 (59.6)
0.066b
.798
Mode of Delivery
Vaginal delivery
Cesarean section
Vacuum/ Forceps’
95 (63)
54 (36)
2 (1)
35 (61)
21 (37)
1 (2)
0.082b
.960
Breastfeeding Experience
Yes
No
93 (62)
58 (38)
34 (60)
23 (40)
0.066b
.798
Attitude 58.9 ± 7.96 58.9 ± 7.86 58.8 ± 8.30 0.094 a .926
a Independent Samples t-Test

45
b Chi-Square Tests
4.3.2 Relationship between breastfeeding-friendly workplace factors and breastfeeding
types
Independent t test was used to analyze the relationship between breastfeeding friendly
factors and breastfeeding types. The results showed that higher organization support (t =
2.924, p = .004), manager support (t =2.062, p = .041), physical environment support (t =
2.000, p = .047), and time support (t = 2.974, p = .003) increased the likelihood of exclusive
breastfeeding. There was no significant association between the co-worker support score and
exclusive or non-exclusive breastfeeding type (t = 1.725, p = .086).
Table 4.3.2 Relationships between breastfeeding workplace friendly factors
and breastfeeding types
Variables Exclusive
Breastfeeding
Not Exclusive
Breastfeeding
t p
Organization Support 30.64 ± 3.93 28.81 ± 4.27 2.924 .004*
Manager Support 30.70 ± 5.60 28.91 ± 5.56 2.062 .041*
Co-Worker Support 15.89 ± 2.40 15.23 ± 2.60 1.725 .086
Time Support 8.56 ± 2.20 7.53 ± 2.35 2.974 .003*
Environment Support 13.80 ± 6.10 11.86 ± 6.61 2.000 .047*
Note : * p < .05
4.3.3 Relationships between social support factors and breastfeeding types
A univariate analysis to identify associations between social support and breastfeeding types
was run using the independent sample t-test. There were no statistically significant
associations between social support and breastfeeding types for all the support subscales (p
>.05).
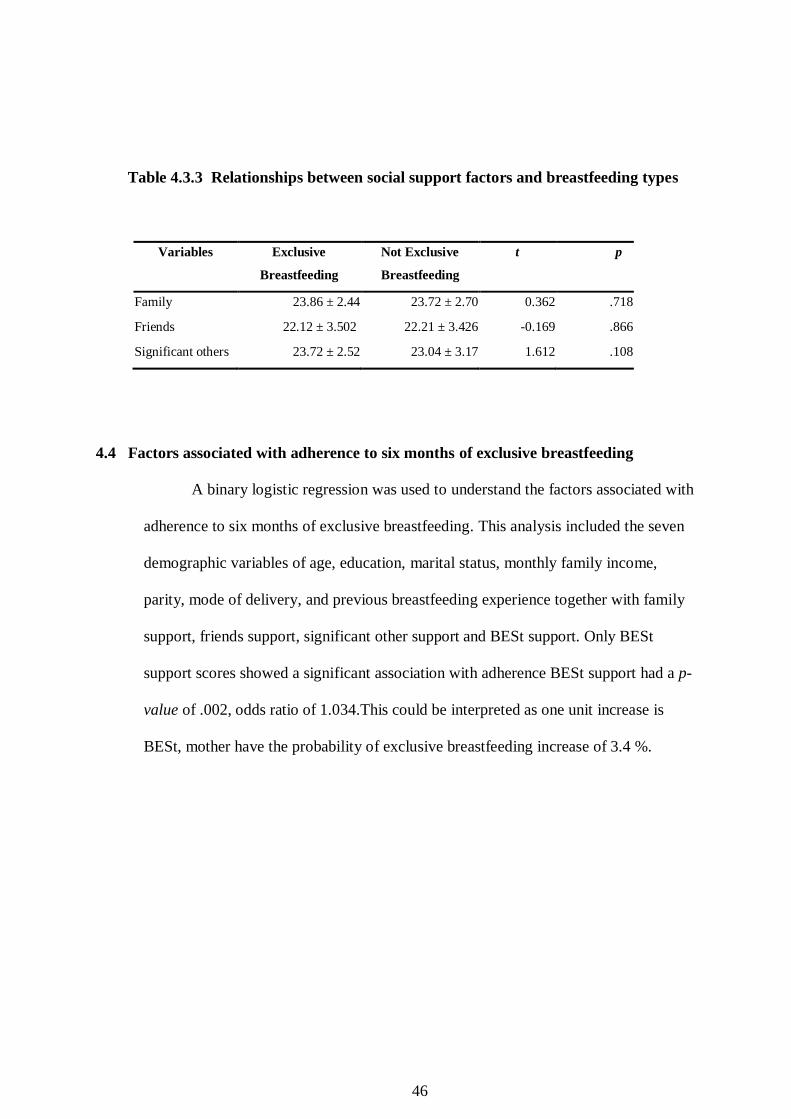
46
Table 4.3.3 Relationships between social support factors and breastfeeding types
Variables Exclusive
Breastfeeding
Not Exclusive
Breastfeeding
t p
Family 23.86 ± 2.44 23.72 ± 2.70 0.362 .718
Friends 22.12 ± 3.502 22.21 ± 3.426 -0.169 .866
Significant others 23.72 ± 2.52 23.04 ± 3.17 1.612 .108
4.4 Factors associated with adherence to six months of exclusive breastfeeding
A binary logistic regression was used to understand the factors associated with
adherence to six months of exclusive breastfeeding. This analysis included the seven
demographic variables of age, education, marital status, monthly family income,
parity, mode of delivery, and previous breastfeeding experience together with family
support, friends support, significant other support and BESt support. Only BESt
support scores showed a significant association with adherence BESt support had a p-
value of .002, odds ratio of 1.034.This could be interpreted as one unit increase is
BESt, mother have the probability of exclusive breastfeeding increase of 3.4 %.

47
Table 4.4 Factors associated with adherence to six months of exclusive breastfeeding
B S.E. p-value OR
95% CI for EXP(B)
Lower Upper
Age 0.045 .032 .169 1.046 0.981 1.114
Education (junior high school
vs senior high school or
above)
0.562 .418 .179 1.754 0.772 3.983
Monthly family income:
<1,833,000 vs ≥1,833,000 -0.071 .354 .841 0.932 0.465 1.866
Parity: primigravida vs
multigravida -0.122 .368 .740 0.885 0.431 1.819
Birth Mode: vaginal delivery
vs Cesarean section -0.027 .338 .936 1.034 1.012 1.057
Social Support -0.111 .023 .634 0.989 0.945 1.035
Attitude -0.007 .021 .745 .993 .954 1.035
BESt 0.027 .0338 .002 1.034 1.012 1.057
Constant -2.727 2.156 .206 .065
Note: BESt (Breastfeeding Employment study for breastfeeding friendly workplace)

48
Chapter Five
Discussion
This chapter discusses the findings of this study, which aimed to understand the
factors associated with six months of exclusive breastfeeding among employed mothers after
returning to work in Karanganyar Regency, Central Java, Indonesia. The following variables
were investigated: personal factors including demographic data and attitudes; social support
factors, and breastfeeding-friendly workplace factors.
5.1 Findings of this study
Four main variables were used to explore the factors associated with continued
exclusive breastfeeding among employed mothers after returning to work in Karanganyarar
Regency: demographic factors (include of age, education, monthly family income, parity,
birth mode and previous experience), attitude, social support factors (include of family
support, friend support and significant other support) and workplace breastfeeding friendly
factors.
5.1.1 Personal Factors
The personal factors investigated in this study included demographic characteristics
and also attitudes. Characteristics included age, marital status, education, monthly family
income, parity, mode of delivery and previous breastfeeding experience.
The result on demographic characteristics showed that 74% of employed mothers
practiced breastfeeding exclusively. This prevalence was high, almost reaching the target rate
of 80% set out by the Indonesian goverment’s target. By contras, studies conducted by Danso
(2014) and Chhetri, Rao, and Guddattu (2018) found that the prevalence of exclusive
breastfeeding practice among working mothers was found to be low. A study done in East
Java, Indonesia by Pujiani and Rahmawati (2014) found that mothers within the age range 18
to 35 were 3.188 times more likely to practice exclusive breastfeeding than than those under

49
age 18 or over age 35. Their study was consistent with previous studies (Cristiana, 2016;
Kassahun, 2019; Kingston, Heaman, Fell, & Chalmers, 2012; Tsai, 2013;). In contrast,
some studies, including this one, did not find a signficant relationship between the age of
mothers and the practice of exclusive breastfeeding (Lenggogeni, 2016; Setegn et al., 2012).
Highly educated mothers may have more control over their jobs and work schedules,
meaning they are able to enjoy a more breastfeeding-friendly work environment (Li Bay,
Tak Fong, & Tarrant, 2015). Ratnasari et al. (2017) as well as Ambarwati and Wulandari
(2010) found that the education of mothers had a positive effect on the frequency and pattern
of breastfeeding. This may be because highly educated people are better able to absorb
information they receive and weigh the benefits they might get from a recommendation, such
as exclusive breastfeeding. It is generally assumed that educational status would be
associated with having more in-depth information regarding the practice of exclusive
breastfeeding.
In contrast, in this study, education was not a significant factor in exclusive
breastfeeding, which indicates no significant association between education and the practice
of exclusive breastfeeding. In this study, education was a binary variable. Among the 208
respondents, 169 had obtained senior high school education or above and 125 of those
breastfed their children exclusively. Of the remaining women who had junior high school
education (n=39), only 13 breastfeed their children exclusively. However, the difference in
exclusive breastfeeding rates by education was not statistically significant in this study. The
companies that employed women in this study generally required workers to have senior high
school education or above. Because all the women in this study were employed, they tended
to have higher than average levels of education than Indonesian women in general. The fact
that all the women in this study were more highly educated than average meant there was not
sufficient difference between them to find a significant association between exclusive

50
breastfeeding and education. If the study had included women with less education, the result
might have been different. This result is consistent with another study on breastfeeding and
employment conducted in Indonesia by Khayati and Kusumaningrum (2019) which likewise
found that the education level of the mothers did not have a significant correlation to the
practice of exclusive breastfeeding.
Some studies have found that families with higher monthly incomes are more likely to
practice exclusive breastfeeding. This is partly explained by their ability to buy extra food,
such as milk formula, that could be given to infants in addition to breastmilk (Baale, 2014).
However, the results of this study found no significant relationship between monthly family
income and exclusive breastfeeding practice. This finding is similiar with studies conducted
by Rosita (2016) and Wendiranti et al. (2017) who found that monthly family income did not
have a significant relationship with the practice of exclusive breastfeeding. In this study, the
lack of clear relationship between income and exclusive breastfeeding could be because this
study gathered data only about the wife’s income rather than household income.
Previous studies found that parity has a significant correlation to the practice of
exclusive breastfeeding (Ferreira et al., 2016; Kassahun, 2019; Keneko, 2006; Kitano et al.,
2016; Kusumastuti, 2014). Mothers are more likely to breastfeed exclusively if they have
three or more children. Moreover, they are more likely to use exclusive breastfeeding for the
third child compared to the second and first. On the contrary, this and other studies found that
parity had no significant correlation to the practice of exclusive breastfeeding (Hunegnaw et
al., 2017; Kumala, 2017).
Studies have likewise shown that parity also has a relation to the prior exprience of
exclusive breastfeeding. Mothers with one or two children often have problems giving milk
to their babies because the nipple blisters due to lack of breastfeeding experience or because
the mother is psychologically unready to breastfeed (Aprizal, & Deniati, 2018). In this study,

51
prior experience of breastfeeding unexpectedly did not show a significant association to the
practice of exclusive breastfeeding. By contrast, a study by Maharloue et al. (2018) found
that prior history of breastfeeding did have a significant association with the practice of
exclusive breastfeeding. These different results might be due to the different characteristics of
the study participants. The participants in that study included both employed mothers and
unemployed mothers, whereas all the women in this study were employed. Because all the
women in this study were working, and working is often an obstacle to breastfeeding, prior
experience had no influence on exclusive breastfeeding practice. In other words, working
might mediate the relationship between prior breastfeeding experience and exclusive
breastfeeding practice.
Previous studies have found that mode of delivery was associated with the practice of
exclusive breastfeeding, with mothers who received cesarean sections less likely to breastfeed
exclusively (Alves et al., 2017; Chekol, Biks, Gelaw, & Melsew, 2017; Maharlouei et al.,
2018). This could be due to the condition mothers who have had cesarean section face in the
first hours after delivery as they may be experiencing pain and a lack of energy. Also, early
initiation of breastfeeding is an important factor in a woman’s success at exclusive
breastfeeding; women who initiate breastfeeding sooner are more likely to succeed at it. On
the contrary, women who give birth to their baby vaginally are readier to start breastfeeding
in the first hours after delivery because they are in good physical condition. However, in this
study, the results showed that there was no significant association between mode of delivery
and practicing exclusive breastfeeding. This might be possibly the sample size for this study
was too small to reveal the connection. Also, this study did not ask a question about early
initiation of breastfeeding, which may be a mediating factor between mode of delivery and
breastfeeding practice. This finding is consistent with a study conducted in South East
Ethiopia by Setegn et al. (2012).
52
Studies on how attitude affects the practice of exclusive breastfeeding show mixed
results. Septiani, Hanulan; Budi, Artha; Karbito.,(2017) found that attitude has a significant
correlation with practice of exclusive breastfeeding. They found that respondents who had a
positive attitude towards exclusive breastfeeding were 3.7 times more likely to practice
exclusive breastfeeding than those who had a negative attitude towards exclusive
breastfeeding. Lack of knowledge and inappropriate beliefs are the major obstacles to
exclusive breastfeeding (Hillowis, 2016). For example, a study conducted in Somalia showed
that attitude toward breastfeeding is strongly influenced by maternal grandmothers and other
elderly women in the community. Most children start breastfeeding two or three days after
birth and mothers do not feed the infant colostrum as it is considered dirty. But results of this
study showed that the attitude did not have a significant correlation with exclusive
breastfeeding. One reason for this finding may be that all the women in this study were
employed. Even if they had a positive attitude about breastfeeding, practical obstacles might
prevent them from doing it.
5.1.2 Breastfeeding Workplace Friendly Factors
The breastfeeding workplace friendly factors investigated in this study included
organization support, manager support, coworker support, time support and environment
support.
The number of working women in Indonesia has begun to increase due to the demand
to improve family welfare (Ratnasari, Paramashanti, Hadi, Yugistyowati & Nurhayati, 2017).
A study conducted by Li Bay, Tak Fong, and Tarrant (2015) found that breastfeeding
workplace friendly has significant assosiated with the practice of exclusive breastfeeding for
employment mothers. According to the result showed that four of the breastfeeding
workplace friendly factors variables has a significant association with the practice of

53
exclusive breastfeeding on employment mothers, there are organization support, manager
support, time support and environment support.
A mother's dual role between caring for her child including giving breastfeeding and
working to help the family economy often makes it difficult for a mother to cope. Some
barriers to the success of exclusive breastfeeding programs in the workplace included the
unavailability of private lactation areas to express the breastmilk, the absence of a flexible
schedule or time, bad relation with the other employers or the supervisor. The result of the
multiple logistic regression showed that mothers with the support from organization,
manager, time also environment are more likely to have exclusive breastfeeding practices
1.034 times than those who doesn’t have support. Also this result showed the p-value .002
which mean that breastfeeding workplace friendly support has a significant correlation with
the practice of exclusive breastfeeding. Similiar finding by Septiani et al. (2017) showed
that manager support has significant relationship toward practice of exclusive breastfeeding.
Support that comes from manager will influence the success of exclusive breastfeeding in the
workplace included support in combining breastfeeding and work aslo giving suitable time to
allow the employee for breastfeeding or pumping breast milk.
Previous studies mentioned that working hours was associated with the practice of
exclusive breastfeeding (Novayelinda, 2012; Wendiranti, Subagio, & Wijayanti, 2017).
Some workplaces provide lactation space but limition time is given to express the breast
milk, it can also be the barrier of success exclusive breastfeeding practice in the workplace.
Despite the place to express the breast milk and place for storing the breast milk (Wendiranti
et al., 2017).
Although the organization or the employee already understood about the advantage of
breastfeeding, there were still no efforts made to support the exclusive breastfeeding
programs in the workplace (Sariet al., 2015). The possible reason might be employement

54
rules and regulations such as maternity leave and employed mohters have less opportunity to
stay at home, compromising exclusive breastfeeding and lack of child care facilities close to
the workplace (Elyas et al., 2017). Novayelinda (2012) as well as Yimyam and Hanpa (2014)
found that breastfeeding-friendly workplace policies can greatly influence women’s success
at exclusively breastfeeding their infants. In Indonesia the regulation has been set up by the
State Minister for Women Empowerment, the Minister of Manpower and Transmigration and
the Minister of Health in 2012 on increasing breastfeeding during working time in the
workplace. But the application and evaluation of this regulation is not yet known clearly and
in detail so it requires further study.
5.1.3 Social Support Factors
The social support factors investigated in this study included family support, support
from friends, and support from significant others. The results showed social support factor
variables had no significant association with the practice of exclusive breastfeeding among
employed mothers.
The finding that support from family did not increase the likelihood of exclusive
breastfeeding in this study was contrary to results of other studies. For example, in another
Indonesian study, family support significantly increased the likelihood of exclusive
breastfeeding (Ratnasari et al., 2017). The researchers observed that family can help out by
providing childcare, buying or making food, and also feeding the child expressed breast milk
(Ratbnasari et al, 2017). Other studies have come to similar conclusions, that family support
increases the likelihood of exclusive breastfeeding (Chekol et al,, 2017; Permatasari et al.,
2018; Rahmawati, 2016; Rosita, 2016; Sari, Yosi & Nella, 2015; Sephani et al., 2017; Umami
& Margawati, 2018).
However, this study did not find a significant relationship between family support and
practice of exclusive breastfeeding; there may be several explanations for this result. First,

55
women living with extended family may have more difficulty controlling what other people
feed their infants. In some families, a woman may not have the authority to ask her parents or
in-laws not to feed the baby anything but breast milk. Other family members may feed the
baby honey, juice, or porridge. This might explain why support from family was not
positively associated with exclusive breastfeeding practice in this study.
Another reason that family support was not associated with exclusive breastfeeding
among women in this study might be related to the fact that all participating women were
employed and employed women were more likely to live with only their husband and
children, rather than with an extended family. In this living situation, support from extended
family members for (or against) exclusive breastfeeding had less impact on their daily lives
and child feeding practices.
The statistical results showed that support from friends was not significantly associated
with exclusive breastfeeding.This finding was in agreement with results of studies conducted
by Septiani et al. (2017) and Ariani, Ariescha, & Vera (2019)) which likewise showed that
support from friends did not improve the mother’s ability to provide exclusive breastfeeding.
Other studies, however, showed that women who reported strong support from friends were
significantly more likely to practice exclusive breastfeeding Astutik (2018).The difference in
results might be due to the different characteristics of the respondents. Also, in this study,
friend support can be define as a friend who can be the listener when the respondent has any
problems but it was not clearly explained about the problems which they faced about.
In contrast with results of other studies, support from significant others was
significantly correlated with the practice of exclusive breastfeeding Rosita (2016); Umami
and Margawati (2018). In other words, women who reported more support from significant
others were more likely to breastfeed exclusively than those who did not. The stastitical result
of this study did not show this association.

56
Chapter VI
Conclusion
In this chapter contains the summary of the findings, conclusions, limitations
and recommendations:
6.1 Conclusion
A descriptive correlational design was adopted to collect data using
questionnaires to identify the factors associated with six-months of exclusive
breastfeeding among employed mothers after returning to work in Karanganyar
Regency Central Java, Indonesia.
Lack of workpace support was the dominant predictive factor that could
potentially derail exclusive breastfeeding. Breastfeeding friendly workplace factors
identified as key to a breastfeeding-friendly workplace were found to be significantly
associated with the practice of exclusive breastfeeding among employed mothers.
Support which comes from the company where they work, such us organizational
support, support from the manager, having time available for breastfeeding, and also a
breastfeeding-appropriate environment, are essential for employed mothers.
6.2 Limitations and Recommendations for Future Research
Even though this study has several strengths, including a reasonably large
sample size and use of well-established instruments, it also has several limitations.
First, the manner of recruiting participants introduces a high risk of selection bias,
because respondents worked in government offices, some of which already conform
to breastfeeding-friendly workplace guidelines, and the rest worked in well-known
big companies with many employees, rather than in small shops. Future research
could include a wider range of workplaces such as smaller businesses and schools.
Moreover, it would be informative to clearly identify the types of work the women

57
were engaged in. Second, this study relied on Likert-scale questionnaires that offer
pre-determined responses. Qualitative research that asks open-ended questions is
needed to know more deeply about barriers to practicing exclusive breastfeeding.
A live interview might establish better rapport and elicit more detailed and honest
responses.
6.3 Recommendations
6.3.1 Recommendations for Goverment
This research provides a basis for government agencies to conduct routine
evaluations of how well workplaces have implemented breastfeeding-friendly policies
to enable workers to perform exclusive breastfeeding for six months. In addition,
government should collaborate with health workers to design programs for outreach
aimed at educating both workers and management about the importance of exclusive
breastfeeding for working mothers. Government and health workers should help
employers comply with the government’s policy to promote exclusive breastfeeding,
Perbup Karanganyar No. 82 of 2015.
6.3.2 Recommendations for Health Providers
Currently, health workers counsel women in healthcare settings about
exclusive breastfeeding and its benefits, as well as addressing practical issues like
breastfeeding techniques, how to store breast milk, and how to combine exclusive
breastfeeding with work .
However, if working women are to succeed at breastfeeding, it is essential to
have breastfeeding-friendly workplaces, not just in name only, but as a reality. Some
mothers in this study were hesitant to claim the right to breastfeed or pump milk at
work out of concern that it would burden their co-workers or annoy their managers.
Women will not use their right to breastfeed if they are concerned that they could lose
58
their job or lose a promotion. Therefore, since most companies do not hire health
workers on site, health workers must conduct outreach into the workplace, in order to
provide counselling not only to employed mothers themselves, but also to their co-
workers and managers in the workplace. Government should pay health workers extra
for visiting companies to perform such outreach for this purpose.
6.3.3 Recommendations for Companies
Companies are expected to create a working environment that supports
exclusive breastfeeding through the provision of breastfeeding facilities in the
workplace and via work policies that enable female workers to practice exclusive
breastfeeding.

59
References
Alves, N., Dowling, M., & Mahan, M. (2017). Supporting breastfeeding mothers at work and
at home in Indonesia. An Interactive Qualifying Project: Worcester Polytechnic
Institute.
Ambarwati, E. R & Wulandari, D. (2010). Asuhan Kebidanan Nifas. Nuha Medika:
Yogyakarta.
Aprizal, S. H & Deniati, E. N. (2018). Faktor-Faktor Yang Berhubungan Dengan Asi
Eksklusif Pada Ibu Di Banjarmasin, Kalimantan Selatan. Jurnal Ilmu Kesehatan
Masyarakat, 9(2), 115-124. doi.org/10.26553/jikm.2018.9.2.115-124
Ariani, P., Ariescha, P & Vera, J. (2019). Analisis Faktor Yang Berhubungan Dengan
Pemberian Asi Eksklusif Pada Ibu Pekerja. Jurnal Kebidanan Kestra (JKK), 2(1), e-
ISSN 2655-0822. doi.org/10.35451/jkk.v2i1.244
Arisdiani, T & Livana. (2016). Gambaran Sikap Ibu Dalam Pemberian Asi Eksklusif
(Describe The Mother's Attitude About Exclusive Breastfeeding). Jurnal
Keperawatan, 4(2), 137-140
Astutik, L. P. (2018). Dukungan Teman Sejawat Di Jejaring Sosial Dalam Pemberian Asi
Eksklusif. Jurnal Medika Karya Ilmiah Kesehatan,,3(2), 25-30. doi : 10.35728/
jmkik.v3i2.44
Atindanbila, S., Mwini-Nyaledzigbor, P. P., Abasimi, E., Benneh, C. O., & Avane, M. A.
(2014). Attitude and practices associated with exclusive breastfeeding (EBF) of
nursing mothers in Bolgatanga Municipality. International Journal of Humanities
Social Sciences and Education,(7), 114-120.
Baale, E. (2014). Determinants of early initiation, exclusiveness and duration of
breastfeeding in Uganda. Journal Health Population Nutrition; 32 (2), 249-260
60
Bai, Y. K., Wunderlich, S. M., & Weinstok, M. (2012). Employer’s readiness for the mother-
friendly workplace: an elicitation study. Maternal & Child Nutrition, 8(4), 483-491.
https://doi.org/10.1111/j.1740-8709.2011.00334.x
Better Work Indonesia (2012). Law and Regulations on Breastfeeding. Retrieved April 11,
2019, from http://betterwork.org/indonesia/
Brislin, R. W. (1970). Back-Translation for Cross-Cultural Research. Journal of Cross-
Cultural Psychology, 1(3), 185–216. https://doi.org/10.1177/135910457000100301
Central Java Health Cervice. (2018). Central Java Health Profile in 2017 (Profil Kesehatan
Jawa Tengah Tahun 2017). Jakarta : Ministry of Health
Chekol, D. A., Biks, G. A., Gelaw, A. Y & Melsew, Y. A. (2017). Exclusive breastfeeding
and mothers’ employment status in Gondar town, Northwest Ethiopia: A
comparative cross-sectional study. International Breastfeeding Journal, 12, 27.
https://doi.org/10.1186/s13006-017-0118-9
Chhetri, S., Rao, R, A., & Guddattu, V. (2018). Factors affecting exclusive breastfeeding
(EBF) among working mothers in Udupi taluk, Karnataka. Clinical Epidemiology
and Global Health, 6(4), 216-219. doi.org/10.1016/j.cegh.2018.06.008.
Cristiana, E. N. (2016). Faktor-Faktor Yang Berhubungan Dengan Pemberian ASI Eksklusif
Pada Ibu muda Di Wilayah Kerja Puskesmas Banyudono 1 dan Banyudono 2,
Boyolali. Publikasi Ilmiah FIK Universitas Muhammadiyah Surakarta
Danso, J. ( 2014). Examining the practice of exclusive breastfeeding among professional
working mothers in Kumasi Metropolis of Ghana. International Journal of Nursing.
(1), 1.
De la Mora, A., Russell, D. W., Dungy, C. I., Losch, M., & Dusdieker, L. (1999). The Iowa
infant feeding attitude scale: Analysis of reliability and validity. Journal of Applied
Social Psychology 29(11), 2362-2380.doi.org/10.1111/j.1559-1816.1999.tb00115.x
61
Dewi, U. M. (2016). Pengaruh Karakteristik Ibu Terhadap Pemberian Asi Eksklusif Pada
Bayi Usia 0-6 Bulan di BPM Nurul Trianawati, SST Surabaya (Effect of maternal
characteristics on exclusive breastfeeding on babies 0-6 months in BPM Nurul
Trianawati, SST Surabaya). Journal of Health Sciences, 9(2), 146-150.
Dhakal, S., Lee, T.H., & Nam, E. W. (2017). Exclusive breastfeeding practice and its
association among mothers of under 5 children in Kwango Distric, DR Congo.
International Journal of Environmental Research and Public Health, 14(5), 455.
https://doi.org/10.3390/ijerphl4050455
DiFrisco, E., Goodman, K. E., Budin, W. C., Lilienthal, M. W., Kleinman, A., & Holmes, B.
(2011). Factors associated with exclusive breastfeeding 2 to 4 weeks following
discharge from a large, urban, academic medical center striving for baby-friendly
designation. Journal of Perinatal Education, 20(1), 28-35. doi.org/10.1891/1058-
1243.20.1.28
Elyas, L., Mekasha, A., Admasie, A., & Assefa, E. (2017). Exclusive breastfeeding practice
and associated factors among mothers attending private pediatric and child clinics,
Addis Ababa, Ethiopia: A cross-sectioanl study. International Journal of
Pediatrics,Volume : 2017, Pages 8546192 https://doi.org/10.1155/2017/8546192.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using
G*Power 3.1: Tests for correlation and regression analyses. Behavior Research
Methods, 41, 1149-1160. doi:10.3758/BRM.41.4.1149.
Ferreira, H. L. O. C., Oliveira, M. F. D., Bernado, E. B. R., Almeida, P. C. D., Aquino, P. D.
S., & Pinheiro, A. K. B. (2018). Factors associated with adherence to the exclusive
breastfeeding. Ciencia & Saude Coletiva, 23(3), 683-690.
https://doi.org/10.1590/1413-81232018233.06262016
62
Fisher, J., Himmelberg, K., Wynter, K., McBain, J., Gibson, F., Boivin, J., & McMahon, C.
(2013). Assisted conception, maternal age and breastfeeding: An Australian cohort
study. Acta Paediatrica : Nurturing The Child, 102(10), 970-976.
https://doi.org/10.1111/apa.12336
Greene, S. W., Wolfe, E.W., & Olson, B.H. (2008). Assessing the validity of measures of an
instrument designed to measure employees’ perceptions of workplace breastfeeding
support. Breastfeeding Medicine, 3(3), 159-163.
https://doi.org/10.1089/bfm.2007.0029
Griffiths, L. J., Tate, A. R., & Dezateux, C. (2005). The contribution of parental and
community ethicity to breastfeeding practices: Evidence from the millenium cohort
study. International Journal Epidemiology, 34(6), 1378-1386.
https://doi.org/10.1093/ije/dyi162
Hillowis, H. (2016). Improving nutrition behaviours through a care group model project in
Somalia. Nutrition Exchange, 6, 24. www.ennonline.net/nex/6/improvingnutsomalia
Hirani, S. A. A., Karmaliani, R., Christie, T., Parpio, Y., & Rafique, G. (2013). Perceived
Breastfeeding Support Assessment Tool (PBSAT): Development and testing of
psychometric properties with Pakistani urban working mothers. Midwifery, 29(6),
599-607. https://doi.org/10.1016/j.midw.2012.05.003
Hunegnaw, M. T., Gezie, L. D., & Teferra, A. S. (2017). Exclusive breastfeeding and
associated factors among mothers in Gozamin district, northwest Ethiopia: A
community based cross-sectional study. International Breastfeeding Journal, 12(1),
30. https://doi.org/10.1186/s13006-017-0121-1
Indonesia Demographic and Health Survey. (2012). Jakarta, Indonesia: BPS, BKKBN,
Kemenkes, and ICF International

63
Indonesian Ministry of Health. (2018). Indonesia Health Profile in 2017 (Profil Kesehatan
Indonesia Tahun 2018). Jakarta : Ministry of Health
Jones, J. R., Kogan, M.D., Singh, G. K., Dee, D. L., & Grummer-Strawn. L. M. (2011).
Factors associated with exclusive breastfeeding in the United States. Pediatric,
128(6), 1117-1125. https://doi.org/10.1542/peds.2011-0841
Kaneko, A., Kaneita, Y., Yokoyama, E., Miyake, T., Harano, S., Suzuki, K., . . . Ohida, T.
(2006). Factors associated with exclusive breast-feeding in Japan: For activities to
support child-rearing with breast-feeding. Journal of Epidemiology, 16, 57-63,
https://doi.org/10.2188/jea.16.57
Kassahun, M. (2019). Exclusive breastfeeding practices and associated factors among
working mothers in Qera Meberat Hayel Condeminium, Addis Ababa, Ethiopia.
Thesis : College of Development Studies Center For Population Studies.
Khayati, N, F & Kusumaningrum, R, P. (2019). Analisis Faktor Pemberian ASI Eksklusif
pada Ibu Bekerja di Instansi Pemerintah. Gaster : Jurnal Kesehatan, (17), 2.
doi.org/10.30787/gaster.v17i2.410.
Kingston, D., Heaman, M., Fell, D., & Chalmers, B. (2012). Comparison of adolescent,
young adult, and adult women’s maternity experiences and practices.Official Journal
of the American Academy of Pediatrics,129(5), 1228-1237.
https://doi.org/10.1542/peds.2011-1447
Kitano, N., Nomura, K., Kido, M., Murakami, K., Ohkubo, T., Ueno, M., & Sugimoto, M.
(2016). Combined effects of maternal age and parity on successful initiation of
exclusive breastfeeding. Preventive Medicine Report, 3, 121-126.
https://doi.org/10.1016/j.pmedr.2015.12.010

64
Kumala, A. (2017). Factors associated with exclusive breastfeeding at Primary Health Care in
Indonesia. 10th World Pediatrics Congress, 7(4), 2161-0665.
https://doi.org/10.4172/2161-0665-C1-043
Kusumastuti, D, A. (2014). Korelasi Faktor Sosio Demografi Dengan Pelaksanaaai
Pemberian Asi Eksklusif Di Kabupaten Kudus. JIKK (Jurnal Keperawatan dan
Kebidanan), 5(2) 6A-69.
Lenggogeni, P. (2016). Examining exclusive breastfeeding practice in Indonesia, and its
association to maternal socio-demographic determinants, to inform intervention
efforts aimed at reducing infant mortality. Thesis, Georgia State University, 2016.
https://scholarworks.gsu.edu/iph_theses/462
Leone, C. (1995). A review: Eagly, A. H., & Chaiken, S. (1993). The psychology of attitudes.
New York: Harcourt, Brace, & Janovich. Psychology and Marketing, 12, 459-466.
Li Bay, D., Tak Fong, D, Y & Tarrant, M. (2015). Factors associated with breastfeeding
duration and exclusivity in mothers returning to paid employment postpartum.
Maternal Child Health Journal. (19), 990–999. DOI 10.1007/s10995-014-1596-7.
Maharlouei, N., Pourhaghighi, A., Raeisi., Hadi., Zohoori., Dariush., Lankarani & Kamran.
(2018). Factors Affecting Exclusive Breastfeeding, Using Adaptive LASSO
Regression. International Journal of Community Based Nursing and Midwifery, 6,
260-271.
Mursyida, A., & Wadud, S. (2013). Hubungan Umur Ibu dan Paritas dengan Pemberian ASI
Eksklusif pada Bayi Berusia 0-6 bulan di Puskesmas Pembina Palembang.
Dipublikasikan untuk Poltekkes Kemenkes Palembang, Jurusan Kebidanan
Notoatmodjo, S. (2012). Promosi Kesehatan dan Perilaku Kesehatan. Jakarta: PT Rineka
Cipta. p. 138-147

65
Novayelinda, R. (2012). Telah literatur: pemberian asi dan ibu bekerja. Jurnal Ners
Indonesia, 2(2), 177-184.
Nursalam. (2009). Konsep dan Penerapan Metodologi Penelitian Ilmu Keperawatan. Jakarta:
Salemba Medika
Palupi, R. A., & Devy, S.R. (2016). Role of social in breastfeeding for adolescent mothers.
The 2nd International Meeting of Public Health.
https://doi.org/10.18502/kls.v4i4.2281
Permatasari, T. A. E., Sartika, R. A. D., Achadi, E. L., Purwono, U., Irawati, A., Ocviyanti,
D., & Martha, E. (2018). Exclusive breastfeeding intention among pregnant women.
National Public Health Journal, 12(3), 134-141.
https://doi.org/10.21109/kesmas.vl2i3.1446
Pujiani & Rahmawati, M. (2014). Analisis Faktor Pemberian Asi Eksklusif. Journal
Eduhealth, (4), 1
Purwanti. (2004). Konsep Penerapan ASI Eksklusif (Exclusive breastfeeding concept).
Bandung: Cendekia.
Rahmawati, N.I. (2016). Dukungan Informasional Keluarga Berpengaruh Dalam Pemberian
Asi Ekslusif di Desa Timbulharjo Sewon Bantul. Jurnal Ners dan Kebidanan
Indonesia, 4(2), 75-78. doi.org/10.21927/jnki.2016.4(2).75-78
Ratnasari, D., Paramashanti, B. A., Hadi, H., Yugistyowati, A., & Nurhayati, E. (2017).
Family support and exclusive breastfeeding among Yogyakarta mothers in
employment. Asia Pacific Journal of Clinical Nutrition, 26, S31-S35.
https://doi.org/10.6133/apjcn.062017.s8
Roesli, U. (2009). Inisiasi Menyusu Dini Plus ASI Eksklusif. Jakarta: Pustaka Bunda
Roig, A. O., Martínez, M. R., García, J. C., Hoyos, S. P., Navidad, G. L., Álvarez, J. C. F.,
González, R. G. d. L. (2010). Factors associated to breastfeeding cessation before 6

66
months. Revista Latino-Americana de Enfermagem, 18. 373-380.
https://doi.org/10.1590/S0104-11692010000300012
Rosita, N, A. (2016). Peran Dukungan Orang Tua Faktor Yang Paling Berpengaruh Terhadap
Pemberian Asi Ekslusif. Unnes Journal of Public Health, 5(4) 2252-
6781.http://journal.unnes.ac.id/sju/index.php/ujph
Sari, Y. P., Yosi, S., & Nella, V. (2015). The exclusive breastfeeding experiences of working
mothers in West Sumatera (Sumbar) Peduli ASI Community. International Journal
of Research in Medical Sciences, 3(10), 2599-2604, https://doi.org/10.18203/2320-
6012.ijrms20150798
Septiani, Hanulan; Budi, Artha; Karbito. (2017). Faktor-Faktor yang Berhubungan dengan
Pemberian ASI Eksklusif Oleh Ibu Menyusui yang Bekerja Sebagai Tenaga
Kesehatan. Jurnal Aisyah: Jurnal Ilmu Kesehatan, 2 (2), 159 – 174.
Setegn, T., Belachew, T., Gerbaba, M., Deribe, K., Deribew, A & Biadgilign, S.
(2012). Factors associated with exclusive breastfeeding practices among mothers in
Goba district, south east Ethiopia: a cross-sectional study. International Breastfeed
Journal 7, 17. doi.org/10.1186/174 6-4358-7-17
Silva, V.A.A.L., Caminha, M.F.C., Silva, S.L., Serva, V.M.S.B.D., Azevedo, P.T.A.C.C., &
Filho, M.B. (2018). Maternal breastfeeding: Indicators and factors associated with
exclusive breastfeeding in a subnormal urban cluster assisted by the Family Health
Strategy. Journal de Pediatria, 95(3), 298-305.
https://doi.org/10.1016/j.jped.2018.01.004
Sousa, V.D., & Rojjanasrirat, W. (2011). Translation, adaptation and validation of
instruments or scales for use in cross-cultural health care research: A clear and user-
friendly guideline. Journal of Evaluation in Clinical Practice, 17(2), 268-274.
https://doi.org/10.1111/j.1365-2753.2010.01434.x
67
Tang, L., Lee, A. H., & Binns, C.W. (2014). Factors associated with breastfeeding duration:
A prospective cohort study in Sichuan Province, China. World Journal of Pediatric,
11(3), 232-238. https://doi.org/10.1007/s12519-014-0520-y
Thurman, S. E., & Allen, P.J. (2008). Integrating lactation consultants into primary health
care service: Are lactation consultants affecting breastfeeding success?. Pediatric
Nursing, 34(5), 419-425.
Tsai, S.Y. (2013). Impact of a breastfeeding-friendly workplace on an employed mother’s
intention to continue breastfeeding after returning to work. Breastfeeding Medicine,
8, 210-216. https://doi.org/10.1089/bfm.2012.0119
Ufamily. (2013). Workplace breastfeeding initiative. Retrieved April 2019. From
http://www.ufamily.org.sg/about_us/
Umami, W & Margawati, A. (2018). Faktor-Faktor Yang Mempengaruhi Pemberian Asi
Eksklusif. Diponegoro Medical Journal,7(4), 1720-1730
U.S. Department of Health and Human Services. (2011). The Surgeon General’s Call to
Action to Support Breastfeeding. Washington, DC: U.S. Department of Health and
Human Services, Office of the Surgeon General. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK52682/
United Nations Children's Fund. (2011). Programming guide infant and young child feeding.
Retrieved from
http://www.unicef.org/nutrition/files/Final_IYCF_programming_guide_2011.pdf
United Nations Children's Fund. (2012). Mari jadikan Asi eksklusif prioritas nasional. Pusat
Media UNICEF. http://www.unicef.org/indonesia/id/media_19265.html
Wawan, A & Dewi, M. (2010). Teori & Pengukuran, Sikap, dan Prilaku Manusia. Nuha
Medika: Yogyakarta.
68
Weber, D., Janson, A., Nolan, M., Wen, L. M., & Rissel, C. (2011). Female employees'
perceptions of organisational support for breastfeeding at work: findings from an
Australian health service workplace. International Breastfeeding Journal, 6(1), 19.
https://doi.org/10.1186/1746-4358-6-19
Wendiranti, C.,Subagio, H & Wijayanti, H. (2017). Faktor Risiko Kegagalan ASI Eksklusif.
Journal of Nutrition College, 6. 241. Doi :10.14710/jnc.v6i3.16916.
World Health Organization [WHO]. (2009). Infant and young child feeding: Model chapter
for textbook for medical students and allied health professionals. Maternal,
Newborn, Child and Adolescent Health, Switzerland.
World Health Organization, United Nations Children's Fund and Partners. (2010). Indicators
for assessing infant and young child feeding practices. Part 3: country profiles.
Switzerland: World Health Organization.
World Health Organization. (2014). Indonesia’s breastfeeding challenge is echoed the world
over. Bulletin of World Health Organization, 92(4), 234-235.
https://doi.org/10.2471/BLT.14.020414
World Health Organization. (2019). Exclusive Breastfeeding. Retrieved 26 March 2019, from
https://www.who.int/nutrition/topics/exclusive_breastfeeding/en/
Yimyam, S., & Hanpa, W. (2014). Developing a workplace breastfeeding support model for
employed lactating mothers. Midwifery, 30(6), 720-724.
https://doi.org/10.1016/j.midw.2014.01.007
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional
scale of perceived social support. Journal of Personality Assessment, 52(1), 30-41.
https://doi.org/10.1207/s15327752jpa5201_2

69
Appendix
Appendix 1
QUESTIONNAIRE
ASSOCIATED FACTORS OF SIX MONTHS BREASTFEEDING AMONG
EMPLOYED MOTHERS AFTER RETURNING TO WORK
A. General Instructions
1. Fill in the identity completely and correctly
2. Give a check (√) to the answer column that you think is correct
3. Answer honestly according to your conscience
4. Choose one answer in each question
5. All questions must be read all nothing has been missed
B. Characteristics of Respondents
1 Age ……………… years
2 Marital Status
Married
Single
3 Education
Elementary School
Junior High School
Senior High School/ So
4 Monthly Family Income
< 1,833,000 IDR
≥ 1,833,000 IDR
5 Parity
Primigravida
Multigravida
6 Mode of Delivery
Vaginal Delivery
Cesarean Section
Vacuum
Forceps
7 Previous Breastfeeding Experienced:
Yes

70
No
8 How old is your baby now ? ….……... months
9 Whatt is your feeding mode currently 1. Exclusive breastfeeding
2. Partially breastfeeding
3. Formula
4. Solid foods
(If you choose exclusive breastfeeding, go to
number 10)
(If you choose partially breastfeeding or
formula or solid food go to number 11)
10. For how many months did you feed
your children only with breast milk
without any liquid or food (except for
medical condition)?
………… months
11. At what age did you stop giving
your baby only breastmilk ?
………… months

71
Organizational Support
This section asks about the overall support you feel would be provided by your
company if you wanted to combine breastfeeding and work.
Strongly
Agree Disagree
Strongly
agree disagree
1. I would have enough maternity leave (paid and/or
unpaid time off) to get breastfeeding started before
going back to work.
2. I would be able to get information about combining
work and breastfeeding from my company.
3. I’m certain my company has written policies for
employees that are breastfeeding or pumping breast
milk.
4. I’m certain there is a place I could go to breastfeed
or pump breast milk at work.
5. There is someone I could go to at work that would help
me make arrangements for breastfeeding or pumping
breast milk.
6. My job could be at risk (e.g. lose my job or get fewer
scheduled hours) if I breastfed or pumped breast milk at work.
7. I would be able to talk about breastfeeding at work.
8. I would feel comfortable asking for accommodations to help me breastfeed or pump breast milk at work.
9. My opportunities for job advancement would be limited
if I breastfed or pumped breast milk at work.
10. I’m certain that women in higher-level positions have
breastfed or pumped breast milk at my workplace.
11. I’m certain coworkers have breastfed or pumped
breast milk at my workplace.
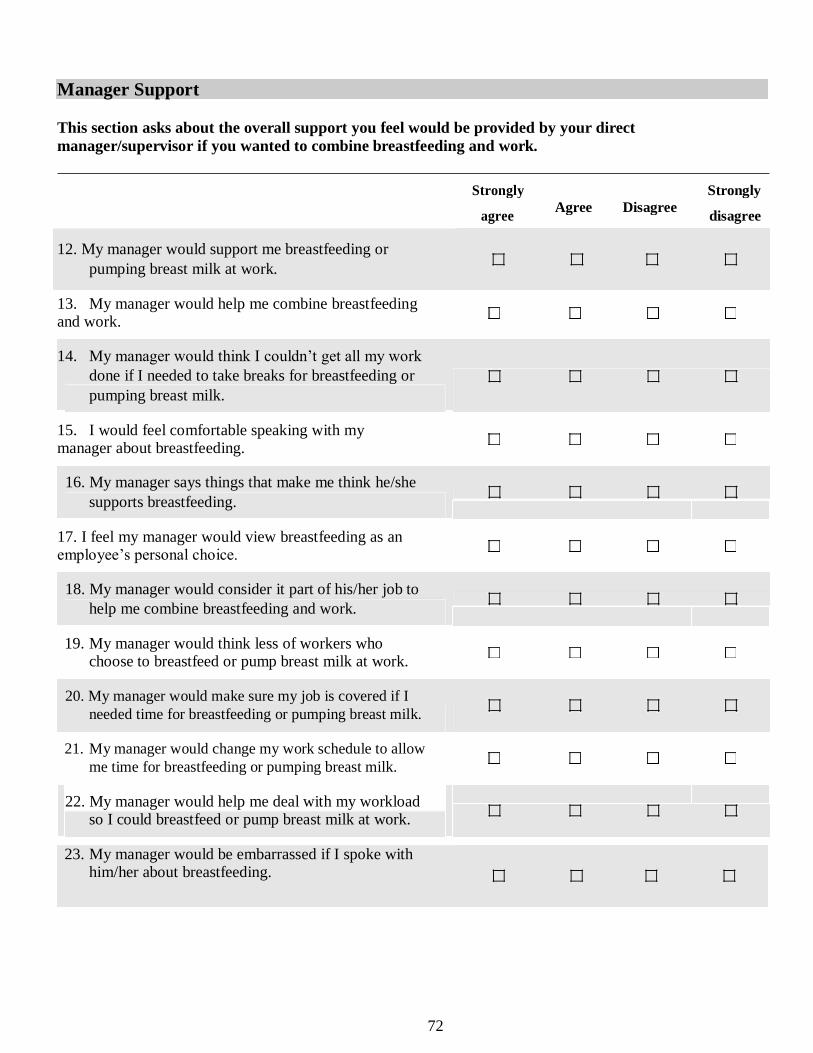
72
Manager Support
This section asks about the overall support you feel would be provided by your direct
manager/supervisor if you wanted to combine breastfeeding and work.
Strongly
Agree Disagree
Strongly
agree disagree
12. My manager would support me breastfeeding or pumping breast milk at work.
13. My manager would help me combine breastfeeding and work. 14. My manager would think I couldn’t get all my work
done if I needed to take breaks for breastfeeding or pumping breast milk.
15. I would feel comfortable speaking with my manager about breastfeeding.
16. My manager says things that make me think he/she supports breastfeeding.
17. I feel my manager would view breastfeeding as an employee’s personal choice.
18. My manager would consider it part of his/her job to help me combine breastfeeding and work.
19. My manager would think less of workers who choose to breastfeed or pump breast milk at work.
20. My manager would make sure my job is covered if I
needed time for breastfeeding or pumping breast milk.
21. My manager would change my work schedule to allow
me time for breastfeeding or pumping breast milk.
22. My manager would help me deal with my workload so I could breastfeed or pump breast milk at work.
23. My manager would be embarrassed if I spoke with him/her about breastfeeding.

73
Co-worker Support
This section asks about the overall support you feel would be provided by your coworkers if you
wanted to combine breastfeeding and work.
Strongly
Agree Disagree
Strongly
agree disagree
24. My coworkers would think less of workers that choose to breastfeed or pump breast milk at work.
25. I would feel comfortable speaking with my coworkers about breastfeeding.
26. My coworkers say things that make me think they support breastfeeding.
27. My coworkers would change their break times with me so that I could breastfeed or pump breast milk.
28. My coworkers would cover my job duties if I needed
time for breastfeeding or pumping breast milk.
29. My coworkers would be embarrassed if I spoke with them about breastfeeding.
Time
This section asks about the pace of your job and available time you would have during your workday
to breastfeed or pump breast milk.
Strongly
Agree Disagree
Strongly
agree disagree
30. My breaks are frequent enough for breastfeeding or pumping breast milk.
31. My breaks are long enough for breastfeeding or pumping breast milk.
32. I could adjust my break schedule in order to breastfeed or pump breast milk.

74
Physical Environment
This section asks about the physical environment of your workplace for breastfeeding
or pumping breast milk after returning to work.
33. I could buy or borrow the equipment I would need for pumping breast milk.
No
Yes
34. My company would supply the equipment I would need for pumping breast milk at work.
No
Yes
35. I could find a place to store expressed breast milk at work.
No Yes
36. There is a company-designated place for women to breastfeed or pump milk during the
workday.
No
Yes
Strongly
Agree Disagree
Strongly
agree disagree
37. The designated place for breastfeeding or
pumping breast milk at work would be
available when I needed it.
38. The designated place for breastfeeding or pumping
breast milk is close enough to my work area to use during my breaks.
39. I would feel comfortable breastfeeding or pumping breast milk in the designated place.
40. The designated place for breastfeeding or pumping breast milk is satisfactory.
41. The designated place for breastfeeding or pumping breast milk includes everything I need.

75
Multidimensional Scale of Perceived Social Support
Instructions: We are interested in how you feel about the following statements. Read each
statement carefully. Indicate how you feel about each statement.
Give a check (√) in the column “1” if you Very Strongly Disagree Give a check (√) in the column “2” if you Strongly Disagree
Give a check (√) in the column “3” if you Mildly Disagree
Give a check (√) in the column “4” if you are Neutral
Give a check (√) in the column “5” if you Mildly Agree
Give a check (√) in the column “6” if you Strongly Agree
Give a check (√) in the column “7” if you Very Strongly Agree
No Questions 1 2 3 4 5 6 7
1. There is a special person who is around when I am in
need.
2. There is a special person with whom I can share my
joys and sorrows.
3. My family really tries to help me.
4. I get the emotional help and support I need from my
family.
5. I have a special person who is a real source of
comfort to me.
6. My friends really try to help me.
7. I can count on my friends when things go wrong.
8. I can talk about my problems with my family.
9. I have friends with whom I can share my joys and
sorrows.
10. There is a special person in my life who cares about
my feelings.
11. My family is willing to help me make decisions.
12. I can talk about my problems with my friends.

76
Iowa Infant Feeding Attitude Scale
Instructions: We are interested in how you feel about the following statements. Read each
statement carefully. Indicate and give a check (√) how you feel about each statement.
No Infant-Feeding Attitude Strongly
Agree Agree Moderate Disagree
Strongly
Disagree
1 The benefits of breastmilk last only as long as
the baby is fed
2 Formula feeding is more convenient than breastfeeding
3 Breastmilk is lacking in iron
4 Formula feeding is the better choice if the
mother plans to go out to work
5 Women should not breast-feed in public places
6 Breastfed babies are more likely to be overfed
than formula-fed babies
7 Fathers feel left out if a mother breast-fed
8 Formula is as healthy for an infant as breast
milk
9 A mother who occasionally drinks alcohol
should not breast-feed her baby
10 Breastfeeding increases mother-infant bonding
11 Formula-fed babies are more likely to be over
fed than breastfed babies
12 Mothers who formula feed miss one of the great joys of motherhood
13 Breastfed babies are healthier than formula fed
babies
14 Breastmilk is the ideal food for babies
15 Breastmilk is more easily digested than
formula
16 Breastfeeding is more convenient than formula
17 Breastmilk is cheaper than formula

77
KUESIONER
FAKTOR-FAKTOR YANG BERHUBUNGAN DENGAN 6 BULAN ASI EKSKLUSIF
PADA IBU SETELAH KEMBALI BEKERJA
A. Petunjuk Umum
1. Isilah identitas anda dengan lengkap dan benar
2. Berilah tanda centang(√) pada kolom jawaban yang menurut anda benar
3. Jawablah dengan jujur sesuai dengan hati nurani anda
4. Pilihlah satu pilihan jawaban disetiap pertanyaan
5. Semua pertanyaan harus terisi dan jangan sampai ada yang terlewatkan
B. Karakteristik Responden
1. Umur ……………… tahun
2. Status Pernikahan
Menikah
Belum menikah
3. Pendidikan
SD
SMP
SMA/ DIII/ SI/ SII
4. Pendapatan Keluarga
< 1,833,000
≥ 1,833,000
5. Kehamilah ke
Pertama
Kedua/ lebih
6. Tipe persalinan Pervaginam
CS/ Sesar
Vakum
Forcep

78
7. Pengalaman menyusui
Pernah
Tidak pernah
8. Berapa usia bayimu sekarang ….……... tahun
9. Tipe menyusui saat ini 1. Asi Eksklusif
2. Asi dan MPASI
3. Formula
4. Makanan padat
(Jika kamu memilih asi eksklusif, silahkan
langsung ke nomor 10)
(Jika kamu memilih asi/ MPASI, formula dan
makanan padat, silahkan langsung ke nomor 11)
10. Selama berapa bulan anda memberi
makan anak anda hanya dengan ASI
tanpa cairan atau makanan ? (kecuali
pada kondisi medis) ?
…………bulan
11. Pada usia berapa anda berhenti
memberi bayi anda hanya ASI tanpa
cairan atau makanan lain ?
………… bulan

79
C. Dukungan Tempat Kerja
Bagian ini menanyakan tentang dukungan-dukungan yang menurut anda akan
diberikan oleh tempat kerja jika anda ingin menyusui.
No Pernyataaan Sangat
Setuju Setuju
Tidak
Setuju
Sangat
tidak
setuju
1 Saya akan mendapatkan cuti melahirkan yang
cukup untuk menyusui bayi saya baik digaji
maupun tidak digaji
2 Saya akan mendapatkan informasi tentang bekerja
sambil menyusui ditempat saya bekerja
3 Saya yakin bahwa tempat kerja saya memiliki
kebijakan tertulis bagi karyawan yang sedang
menyusui atau mempompa ASI
4 Saya yakin ada tempat yang bisa saya gunakan
untuk menyusui atau mempompa ASI ditempat
saya bekerja
5 Ada seseorang yang bisa membantu saya
mengatur persiapan menyusui atau mempompa
ASI ditempat kerja saya
6 Pekerjaan saya bisa beresiko jika saya menyusui
atau mempompa ASI ditempat saya bekerja,
misalnya kehilangan pekerjaan atau pengurangan
jam kerja
7 Saya dapat membicarakan perihal menyusui
ditempat kerja
8 Saya merasa nyaman meminta fasilitas dalam
membantu saya menyusui atau mempompa ASI
9 Kesempatan saya untuk naik jabatan akan dibatasi
jika saya menyusui atau mempompa ASI

80
D. Dukungan Atasan
Bagian ini menanyakan tentang dukungan-dukungan yang menurut anda akan
diberikan oleh atasan anda jika ingin menyusui.
10 Saya yakin bahwa wanita dengan jabatan tinggi
ditempat saya bekerja pernah menyusui atau
mempompa ASI ditempat kerja
11 Saya yakin rekan kerja saya juga pernah
menyusui atau mempompa ASI ditempat saya
bekerja
No Pernyataaan Sangat
Setuju Setuju
Tidak
Setuju
Sangat
tidak
setuju
12 Atasan saya akan mendukung saya untuk
menyusui atau mempompa ASI ditempat saya
bekerja
13 Atasan saya akan membantu saat saya menyusui
sambil bekerja
14 Atasan saya akan berpikir bahwa semua pekerjaan
saya tidak akan selesai jika saya butuh istirahat
untuk menyusui atau mempompa ASI
15 Saya akan merasa nyaman membicarakan perihal
menyusui dengan atasan saya
16 Atasan saya mengatakan sesuatu yang membuat
saya berpikir bahwa dia mendukung perihal
menyusui ditempat kerja
17 Saya merasa atasan saya akan memandang bahwa
menyusui adalah pilihan pribadi setiap karyawan
18 Atasan saya akan mempertimbangkan bahwa
membantu saya untuk menyusui sambil bekerja
81
E. Dukungan Rekan Kerja
Bagian ini menanyakan tentang dukungan-dukungan yang menurut anda akan
diberikan oleh rekan kerja anda jika anda ingin menyusui.
adalah salah satu tugasnya
19 Atasan saya akan berpikir bahwa sedikit
karyawan yang memilih menyusui dan
mempompa ASI ditempat kerja
20 Atasan saya akan memastikan pekerjaan saya
selesai meskipun saya membutuhkan waktu untuk
menyusui atau mempompa ASI
21 Atasan saya akan merubah jadwal bekerja saya
untuk memberikan saya waktu menyusui atau
mempompa ASI
22 Atasan saya akan membantu saya menangani
beban kerja saya, sehingga saya bisa menyusui
atau mempompa ASI ditempat saya bekerja
23 Atasan saya akan merasa sungkan jika saya
membicarakan periihal menyusui dengannya
No Pernyataaan Sangat
Setuju Setuju
Tidak
Setuju
Sangat
tidak
setuju
24 Rekan kerja saya akan berpikir bahwa sedikit
karyawan yang memilih untuk menyusui atau
mempompa ASInya ditempat kerja
25 Saya akan merasa nyaman membicarakan perihal
menyusui dengan rekan kerja saya
26 Rekan kerja saya mengatakan sesuatu yang
membuat saya berpikir mereka mendukung
perihal menyusui ditempat kerja

82
F. Waktu
Bagian ini menanyakan perihal waktu yang tersedia untuk menyusui atau
mempompa ASI pada jam kerja
G. Lingkungan Fisik
Bagian ini menayakan tentang lingkungan fisik dimana anda bekerja sambil
menyusui atau mempompa ASI
33. Saya dapat membeli atau meminjam peralatan yang saya butuhkan untuk
mempompa ASI saya.
Tidak
Ya
27 Rekar kerja saya akan menukar waktu
isitirahatnya dengan saya sehingga saya bisa
menyusui atau mempompa ASI
28 Rekan kerja saya akan menyelesaikan pekerjaan
saya jika saya membutuhkan waktu untuk
menyusui atau mempompa ASI
29 Rekan kerja saya akan merasa sungkan jika saya
membicarakan perihal menyusui dengannya
No Pernyataaan Sangat
Setuju Setuju
Tidak
Setuju
Sangat
tidak
setuju
30 Saya cukup sering mendapatkan waktu istirahat
untuk menyusui atau mempompa ASI
31 Waktu istirahat saya cukup lama untuk menyusui
atau mempompa ASI
32 Saya dapat menyesuaikan jadwal istirahat saya
untuk menyusui atau mempompa ASI

83
34. Tempat saya bekerja akan menyediakan peralatan yang saya butuhkan untuk
mempompa ASI saya ditempat kerja
Tidak
Ya
35. Saya dapat menemukan tempat untuk menyimpan ASI yang telah dipompa ditempat
kerja
Tidak
Ya
36. Ditemapat saya bekerja, tersedia ruangan menyusui/ mempompa ASI selama jam
kerja
Tidak
Ya
No Pernyataaan Sangat
Setuju Setuju
Tidak
Setuju
Sangat
tidak
setuju
37 Ruangan menyusui atau mempompa ASI ditempat
kerja saya kan dibuka ketika saya memerlukannya
38 Ruangan menyusui atau mempompa ASI cukup
dekat dengan lokasi saya bekerja untuk digunakan
saat waktu istirahat
39 Saya akan merasa nyaman menyusui atau
mempompa ASI diruang menyusui
40 Ruangan untuk menyusui atau mempompa ASI
memuaskan
41 Ruangan menyusuil atau mempompa ASI terdapat
segala sesuatu yang saya perlukan

84
H. Skala Multidimensional Dukungan Sosial I.
Intruksi : Kami tertarik pada bagaimana perasaan anda tentang pernyataan berikut dan
berilah tanda centang(√) pada kolom.
No Pernyataan
San
gat
tid
ak
set
uju
Tid
ak
setu
ju
Agak
tid
ak
setu
ju
Net
ral
Agak
set
uju
Set
uju
San
gat
setu
ju
1 Ada orang khusus yang ada disekitar ketika saya
membutuhkan
2 Ada orang khusus dengan siapa saya dapat berbagi
suka dan duka saya
3 Keluarga saya benar-benar mencoba untuk
membantu saya
4 Saya mendapatkan bantuan emosiaonal dan
dukungan yang saya butuhkan dari keluarga saya
5 Saya punya orang khusus yang merupakan sumber
nyata kenyamanan bagi saya
6 Teman-teman saya benar-benar mencoba untuk
membantu saya
7 Saya dapat mengandalkan teman-teman saya ketika
ada sesuatu yang salah
8 Saya dapat berbicara tentang masalah saya dengan
keluarga saya
9 Saya punya teman dengan siapa saya dapat berbagi
suka dan duka saya
10 Ada orang istemewa dalam hidup saya yang peduli
tentang perasaan saya
11 Keluarga saya bersedia untuk membantu saya
membuat keputusan
12 Saya dapat berbicara tentang masalah saya dengan
teman-teman saya

85
I. Iowa Skala Sikap Menyusui
Berilah tanda centang(√) pada kolom.
No Infant-Feeding Attitude
Str
on
gly
Agre
e
Agre
e
Mod
erate
Dis
agre
e
Str
on
gly
Dis
agre
e
1 Manfaat ASI hanya bertahan selama bayi menyusui
ibunya
2 Susu formula lebih memudahkan dari pada ASI
3 Kandungan zat besi pada ASI sangat kurang
4 Susu formula merupakan pilihan yang lebih baik jika ibu
berencana bekerja diluar rumah
5 Ibu seharusnya tidak menyusui di tempat umum
6 Bayi yang disusui ASI cenderung minum berlebih
dibandingkan bayi yang diberikan susu formula
7 Para ayah akan merasa diabaikan jika ibu menyusui
bayinya
8 Untuk bayi, susu formula sama sehatnya dengan ASI
9 Seorang ibu yang terkadang minum alkohol seharusnya
tidak menyusui bayinya
10 Menyusui dapat meningkatkan ikatan ibu dan bayi
11 Bayi yang diberi susu formula cenderung minum
berlebih dibandingkan bayi yang diberikan ASI
12 Ibu yang memberikan susu formula pada bayinya
kehilangan sebuah kebahagiaan menjadi seorang ibu
13 Bayi yang disusui ASI lebih sehat dari pada bayi yang
diberi susu formula
14 ASI merupakan makanan yang ideal untuk bayi
15 ASI lebih mudah dicerna dari pada susu formula
16 ASI lebih memudahkan dari pada susu formula
17 ASI lebih murah dari pada susu formula

86
Appendix 2
INFORM SHEET
Accosiated Factors of Six Months Breastfeeding among Employed Mothers after
Returning To Work
My name is Siska Ningtyas Prabasari, a Master Student at National Taipei University
of Nursing and Health Sciences. I am conducting study about factors related to exclusive
breastfeeding among employed mothers after returning to work. This study is intended to
fulfill an academic requirement.
I will ask you few questions relating to exclusive breastfeeding, breastfeeding
workplace-friendly and sosial support. There are four sections to this questionnaire. The first
is personal factors including demographic and attitude factors, second is breastfeeding
workplace-friendly factors and social support factors. This will take little bit your time
approximately 30 minutes. The information you will provide me will be made confidential
and will not be shared to a third party. After signing the consent form, a copy of
questionnaire will be given to you, kindly answer all question honestly and completely.
Thank you for giving me privilege of sharing your experiences and for taking your
time to participate in my research study.
Sincerely,
Siska Ningtyas Prabasari
Master Student
National Taipei University of Nursing and Health Sciences

87
LEMBAR INFORMASI
Faktror-faktor yang mempengaruhi ASI Eksklusif pada ibu pekerja setelah kembali bekerja
Nama saya Siska Ningtyas Prabasari, seorang Mahasiswa Magister Ilmu Kebidanan
dan Kesehatan Universitas Nasional Taipei. Saya sedang melakukan studi tentang faktor-
faktor yang berhubungan dengan pemberian ASI eksklusif di antara ibu yang bekerja setelah
kembali bekerja. Studi ini dimaksudkan untuk memenuhi persyaratan akademik.
Saya akan mengajukan beberapa pertanyaan kepada anda terkait pemberian ASI
eksklusif, lingkungan di tempat kerja dan dukungan sosial. Ada empat bagian untuk
kuesioner ini. Yang pertama adalah faktor pribadi termasuk faktor demografi dan sikap,
kedua adalah faktor ramah tempat kerja menyusui dan faktor dukungan sosial. Ini akan
menghabiskan sedikit waktu anda sekitar 30 menit. Informasi yang anda berikan kepada saya
akan dirahasiakan dan tidak akan dibagikan kepada pihak ketiga. Setelah menandatangani
formulir persetujuan, salinan kuesioner akan diberikan kepada anda, silakan jawab semua
pertanyaan dengan jujur dan lengkap.
Terima kasih telah memberi saya hak istimewa untuk berbagi pengalaman dan untuk
meluangkan waktu Anda untuk berpartisipasi dalam studi penelitian saya.
Hormat kami,
Siska Ningtyas Prabasari
Mahasiswa Master
Universitas Nasional Ilmu Keperawatan dan Kesehatan Taipei

88
CONSENT FORM
After been provided with clear explanation of the study, I know and understand purpose of
this study. I believe that researcher will acknowledge my rights as a respondents and this
study does not have a negative impact on me. I understand my participation will help
researcher and nurse to improve nursing services.
Hereby, I state willing to be a respondent in the study and my signature is evidence to
confirm my consent to participate in this study.
Date : / /2019
Respondent,
Signature or thumb print
( Name )

89
LEMBAR PERSETUJUAN
Setelah diberikan penjelasan yang jelas tentang penelitian ini, saya tahu dan mengerti tujuan
dari penelitian ini. Saya percaya bahwa peneliti akan mengakui hak-hak saya sebagai
responden dan penelitian ini tidak berdampak negatif pada saya. Saya mengerti partisipasi
saya akan membantu peneliti dan perawat untuk meningkatkan layanan keperawatan.
Dengan ini, saya menyatakan bersedia menjadi responden dalam penelitian ini dan tanda
tangan saya adalah bukti untuk mengkonfirmasi persetujuan saya untuk berpartisipasi dalam
penelitian ini.
Tanggal: / / 2019
Termohon,
Cetak tanda tangan atau ibu jari
(Nama)

90
Appendix 3

91
Appendix4
92
Appendix 5

96
Appendix 7

100
Appendix 9

101

102

103
104
Appendix 10




![College of Medicine, Nursing & Health Sciences [CMNHS] College of Medicine, Nursing & Health Sciences [CMNHS] School of Medicine School of Nursing](https://img.pdfslide.net/doc/110x75/56649dbe5503460f94ab1b37/college-of-medicine-nursing-health-sciences-cmnhs-college-of-medicine.jpg)
























