Embed Size (px)
Citation preview
NAUSEA RELIEF AND PURPOSEFUL TOUCH: DECREASING
DISTRESS BY ALTERING THE PERCEPTUAL FIELD
A DISSERTATION
SUB:MITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS
FOR THE DEGREE OF DOCTOR OF PIIlLOSOPHY
IN THE GRADUATE SCHOOL OF THE
TEXAS WOMAN'S UNIVERSITY
COLLEGE OF NURSING
BY
LINDA S. DUNE, M.S.
DENTON, TEXAS
MAY2002
TEXAS WOMAN'S UNIVERSITY
DENTON, TEXAS
December 13, 2001
To the Dean of Graduate Studies and Research
I am submitting herewith a dissertation written by Linda S. Dune entitled "Nausea Relief and Purposeful Touch: Decreasing Distress by Altering the Perceptual Field." I have examined this dissertation for form and content and recommend that it be accepted in partial fulfillment of the requirements for the degree of Doctor of Philosophy, with a major in nursing.
We have read this dissertation and recommend its acceptance
Dean of Graduate Studies and Research

Copyright © Linda S. Dune, 2002 All rights reserved
ACKNOWLEDGMENTS
My sincere appreciation is offered to the members ofmy committee, Drs. Jeanette
Kernicki, Ann Young, and Joan Killen, for their support and guidance. Deep
appreciation is extended _to:
The patients and staff of the emergency center where this study was conducted.
Dr. Mary Watson for her statistical counseling.
, Rosa Lee Bachtel for her expert editorial skills.
IV
NAUSEA RELIEF AND PURPOSEFUL TOUCH: DECREASING
DISTRESS BY ALTERING THE PERCEPTUAL FIELD
LINDA S. DUNE, M.S.
MAY 2002
ABSTRACT
This study explored nausea levels after purposeful touch (PT) in patients who
presented to an emergency center (EC). PT is a commonly used nursing intervention that
can provide comfort in times of distress. Patient responses to distress were decreased by
the sensation of touch applied to a sensory pathway that communicates within the same
neuronal pool. PT decreased nausea by altering the perceptual field through stimulating
somatosensory peripheral areas that alter one or more of the nausea pathways. An
experimental two-group before-after design was used to determine the effects of PT or no
PT on the level of nausea of EC patients. The experimental group received PT while the
control group did not. The study sample included 140 patients randomly assigned to
either group based on order of presentation to the EC. The instruments used for data
collection included a Demographic Data Tool and a 100-mm visual analog nausea scale
(VANS). The patients in the experimental group received a 5-second bimanual touch to
the dominant hand and shoulder of the patient. The study groups were compared based
V
on demographics and findings. Frequencies and percentages were performed on the
variables of age, gender, ethnic origin, reason for EC visit, reactions to nausea, and history
of nausea. The analysis of covariance (ANCOVA) was used to analyze pretouch as the
covariate and experimental/control group data as recorded by each participant on the
VANS. Mean nausea intensity score among EC patients receiving PT to alter their
perceptual field was found to be significantly lower than the mean nausea intensity score
among the EC patients not receiving PT to alter their perceptual field (ANCOV A,
F= 27.22, df= 1, 139,p < 0.0005). These data supported the use of PT as an effective
nursing intervention to decrease nausea in EC patients with the common complaints of
gastrointestinal distress, pain, and headache.
VI
TABLE OF CONTENTS
ACKNOWLEDGI\ffiNTS... ... ...... ............ ... ... ... ... ... ...... ...... ... ... ... ... .... lV
ABSTRACT................................................................................... V
LIST OF TABLES ............... -........................................................ :... lX
LIST OF FIGURES.......................................................................... X
CHAPTER
1. Introduction .............................................................................................. . Problem of Study ................................................................................. . Rationale of Study ............................................................................... . Theoretical Framework ........................................................................ . Assumptions ........................................................................................ . Hypothesis ........................................................................................... . Definition of Terms .............................................................................. .
1 2 2
15 18 18 19
Limitations....................................................................................... . . . . . 20 Summary.............................................................................................. 21
2. Review of Literature................................................................................. . . 22 Nausea as a Focal Stimulus.................................................................... 23 Touch as a Focal Stimulus..................................................................... 34 Touch as a Nursing Intervention........................................................ . . . . 40 Stimuli Alteration for Nausea Relief....................................................... 45 Summary.............................................................................................. 58
3. Procedure for Collection and Treatment of Data.......................................... 60 Setting................................................................................................... 61 Population and Sample........................................................................... 61 Protection of Human Subjects................................................................ 63 Instruments ...................................... ·................................................. . . . . . 64 Data Collection.................................................................................. . . . . 69 Pilot Study............................................................................................. 71 Treatment of Data ........................................... ;.................................. . . . . 7 4 Summary............................................................................................ ... 75
vu
CHAPTER
4. Analysis ofData.......................................................................................... 76 Description of Sample........................................................................... 77 Findings............................................................................................. . . . 84 Summary of Findings............................................................................ 88
5. Summary of the Study................................................................................ 89 Summary............................................................................................. 89 Discussion of Findings....................................................................... . . . 92 Conclusions....................................................................................... . . . 98
Implications...................................................................................... . . . . 99
Recommendations for Further Study.................................................. . . . 99
REFERENCES...................................................................................................... 102
APPENDIX
A. AGENCY APPROVALS ............................................................................ 116 B. INFO�D CONSENT ............................................................................ 119
C. DEMOGRAPIDC DATA TOOL ................................................................ 123 D. VISUAL ANALOG NAUSEA SCALE...................................................... 125
vm
LIST OF TABLES
Table
1. Nursing Interventions to Decrease Physiological Effects of Nausea... . . . .. . . . . 6
2. Studies Reporting Significant Outcomes of Therapeutic TouchInterventions........................................................................................ ... .... 56
3. Descriptive Statistics for VANS by Age and Treatment Group...................... 78
4. Descriptive Statistics for VANS by Gender, Ethnic Originand Treatment Group.................................................... ... ... ... ... ... ... ... ... 80
5. Frequencies and Percentages of Primary Reason for EC Visit . . . . . . . . . . . . . . . . . . . . 81
6. Frequencies and Percentages of Symptoms with Nauseaby Treatment Group...................................................... . . . . . . . . . . . . . . . . . . . . . . . . 83
7. Bivariate Frequency Distribution of 140 VANS ScoresPretouch and Posttouch............................................................... . . . . . . . . . . . . . 86
8. Means and Mean Differences for VANS Scoresfor the Total Group ............................................................................ ...... 87
9. Analysis of Covariance for Mean Nausea Intensity Scores.......................... 87
lX
LIST OF FIGURES
Figure
1. Scatterplot Pre and Posttouch VANS by Group ............ ·...................... . . . . . . 85
X
CHAPTER!
INTRODUCTION
The basic and often used nursing actions ameliorating the effect of nausea are
sporadic in the current literature. Based on estimates from the National Health Interview
Survey in 1996, there were at least three episodes of nausea that contributed to at least
seven and one-half restricted activity days per 100 persons per year (Adams, Hindershot,
& Morano, 1999). Patients consider nausea to be so distressful that they will avoid
medications and treatments for life threatening diseases to avoid the sensation (Pervan,
1993).
The patient becomes vulnerable to the nausea stimuli through the perceptive
pathways of smell, sight, taste, or hearing. Nausea also can occur as a result of internal
stimuli caused by neurological dysfunctions, gastrointestinal inflammation, or chemical
poisonous substances. Nurses can use the focal stimulus of touch to interfere with one or
more of the nausea pathways in order to decrease the intensity of the distress.
Touch remains a fundamental nursing intervention that has been researched for
overall improvement in the patient's condition (Waddell, 1979). Nurses often touch the
patient to comfort or relieve patient distress (Barnard & Brazelton, 1990; Triplett &
Arneson, 1979). Nurses intervene on the patient's behalf by blocking or removing noxious
stimuli or stressors from the perceptual field (Ujhely, 1979). Physicians often administer
I
medications that block the nausea impulse in the central nervous system or use multiple
medications to alleviate the nausea distress. Side effects and medication interactions
increase proportionally to compounded medication use (Al-Sadi, Newman, & Julious,
1997). A single medication or one nursing intervention will not consistently alleviate the
distress of nausea. If nursing interventions and medications are used together, the distress
can be decreased beyond just the single medication effect (Arakawa, 1997).
Problem of Study
Nursing interventions combined with medication has ihe potential of decreasing
nausea. This study was conducted to answer the question: Will purposeful touch (PT)
applied to specific nerve pathways decrease nausea levels in patients who present to an
emergency center (EC) with nausea as a primary or secondary complaint?
Rationale for Study
Even though nausea research has been conducted and reported in the literature,
there are few reported studies on touch interventions for the distress of nausea.
Interviews conducted by the investigator revealed that nurses used different interventions
based on previous personal experiences rather than documented research. C. R. King
(200 I) identified that practical interventions need to be developed to relieve nausea and
vomiting immediately to avoid interference with the patient's daily activities and quality of
life. According to Quinn, Brown, Wallace, and Asbury (1994), postoperative nausea
remained as the most negative aspect of having surgery. Tobias ( 1993) reported that
2
patients preferred to be in pain rather than have nausea as a side effect of pain
medications. In addition to the nausea itself, patients reported multiple physiological and
psychosocial effects (Muth, Stem, Thayer, & Koch, 1996). Even though nausea and
vomiting effect the physical, psychological, social and spiritual well-being domains of
quality of life (Grant, 1997), there were no documented studies on the nursing intervention
of touch to relieve nausea for the EC patient.
Physiological Effects
Nausea is an overwhelming, unpleasant sensation in the back of the throat that may
precede vomiting (Hawthorn, 1995). Since nausea does not always result in vomiting, the
two concepts should not be used interchangeably (Rhodes, McDaniel, & Johnson, 1995).
The physical effects of nausea are well documented in nursing textbooks and research
(lgnatavicius, Workman, & Mishler, 1999; Muth et al., 1996). Responses to nausea
include changes in nutritional and functional status, fluid and electrolyte imbalances,
fatigue, and self-care deficits. Patients experiencing nausea report weakness often severe
enough to discourage any physical movement. Nausea is a syndrome of all-consuming
physical symptoms including: sweating, pallor, salivation, gastric stasis, drowsiness,
diarrhea, or hypotension (Muth et al., 1996� Rhodes et al., 1995). Arakawa (1997)
reported that the physical syndrome of nausea increases with activity of the autonomic
nervous system and visceral efferent nerves.
3
The sensation of nausea can be a response to stimulation of intestinal, meningeal,
gastric, and other receptors which can include direct chemical stimulation of the nausea
center, afferent integrated pathways, and the cerebral cortex (Edwards, 1996; Mannix,
1999). Nausea is believed to be a reaction to a complex physiology of stimulation of
receptors by the neurotransmitters dopamine, serotonin, 5-hydroxytryptamine ( 5-HT),
histamine, and somatostatin. These neurotransmitters are released from multiple sites
which include, but are not exclusively located in, the gastrointestinal tract, central nervous
system, cardiac muscle, bladder, and uterus (Hawtho� 1995; Hogan & Grant, 1993; C.
R. King, 200 I; Mannix, 1999). Since there are multiple numbers of neurotransmitters and
receptors, the nausea syndrome can be initiated by many physiological etiologies including
Addison's disease, anesthetic agents, anoxia, ascites, autonomic nervous system failure,
bruxism, cancer, cerebral infection, chemotherapy, congestive heart failure, constipation,
diabetic gastroparesis, diabetic ketoacidosis, diarrhea, disgusting sights, foul smells,
gastritis, gastroesophageal reflux, gastrointestinal irritation, hepatitis, hypercalcemia,
increased intracranial pressure, infection, intestinal obstruction, labyrinthitis, medications,
mesenteric ischemia, myocardial infarction, opiate analgesics, overindulgence, pain,
pancreatitis, peptic ulcer, pregnancy, premenstrual syndrome, pyloric stenosis, radiation,
Rey's syndrome, side effects of medications, surgical procedures, travel, toxins, tumor
lysis syndrome, and uremia (Bianchi, Grelot, Miller, & King, 1992; Hawthorne, 1995;
Mannix, 1999). Edwards ( 1996) summarized these etiologies according to the physiologic
4
input pathways of the cerebral cortex, chemoreceptor trigger zone (CTZ), sympathetic
visceral afferents, vagal visceral afferents, and vestibulocerebellar afferents.
The nausea syndrome stimulates the release of neurotransmitters that communicate
with the detectors in cranial nerves and visceral afferent nerve fibers. The nerves carry the
resulting impulses directly to the CTZ in the area postrema (AP) (Jablonski, 1993) or by
way of the nucleus tractus solarius (NTS) and the reticular formation to the AP (Hartman,
1992). Other detectors are located in the labyrinth of inner ear and higher brain centers.
The CTZ can detect substances in the circulating blood and cerebrospinal fluid since it is
located at the floor of the fourth ventricle and is not restricted by the blood-brain barrier
(Guyton & Hall, 1996). Once the nerve impulses are interpreted by the vomiting center,
messages are sent via the efferent pathways and sympathetic nervous system to the
respiratory, cardiovascular, and gastrointestinal systems to prepare the body for vomiting.
These sensations, created by the efferent pathways, result in some of the symptoms that
accompany nausea (Hogan & Grant, 1997).
Nursing interventions to relieve the physical effects of nausea have been used to
halt the initial response or the resultant sensations of nausea (Table 1 ). Other interventions
reported as anecdotally helpful include preparing cold food to avoid the odor of cooked
food and use of ice orally or placed on the abdomen or forehead. In this study, touch was
explored as an additional nursing intervention for nausea that can create or inhibit impulses
communicating to the central nervous system by way of the autonomic nervous system
and the peripheral nervous system (Lederman, 1997; Tovar & Cassmeyer, 1989).
5
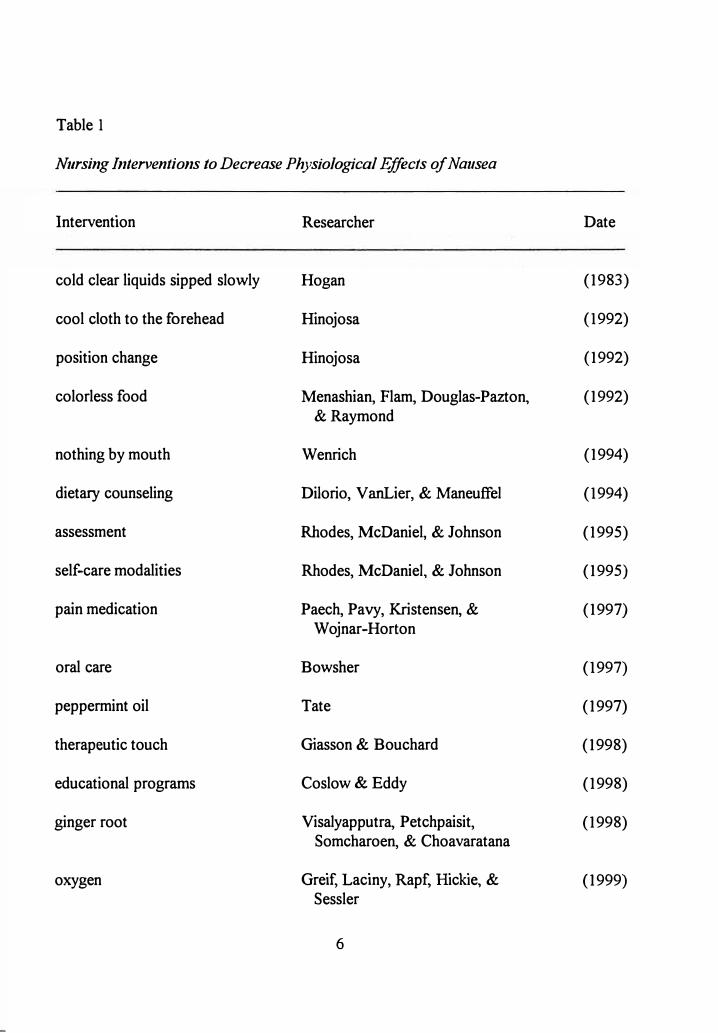
Table I
Nursing Interventions to Decrease Physiological Effects of Nausea
Intervention Researcher Date
cold clear liquids sipped slowly Hogan (1983)
cool cloth to the forehead Hinojosa (1992)
position change Hinojosa (1992)
colorless food Menashian, Flam, Douglas-Pazton, (1992) &Raymond
nothing by mouth Wenrich (1994)
dietary counseling Diiorio, V anLier, & Maneuffel (1994)
assessment Rhodes, McDaniel, & Johnson (1995)
self-care modalities Rhodes, McDaniel, & Johnson (1995)
pain medication Paech, Pavy, Kristensen, & (1997) Wojnar-Horton
oral care Bowsher (1997)
peppermint oil Tate (1997)
therapeutic touch Giasson & Bouchard (1998)
educational programs Coslow & Eddy (1998)
ginger root Visalyapputra, Petchpaisit, (1998) Somcharoen, & Choavaratana
oxygen Greif, Laciny, Rapf, Hickie, & (1999) Sessler
6
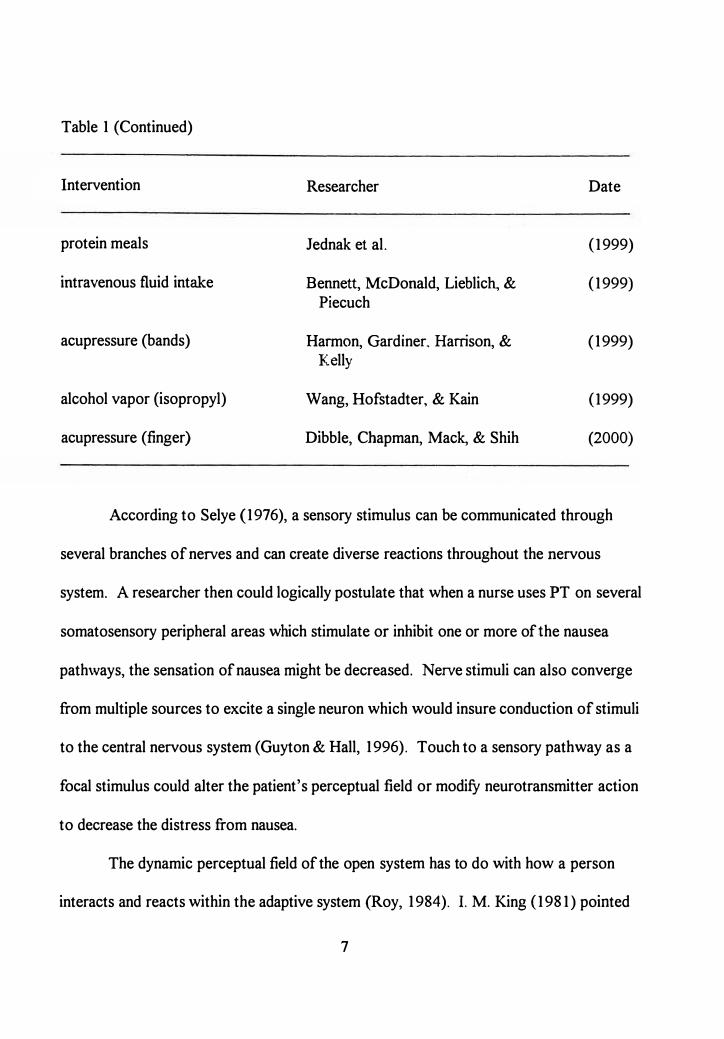
Table 1 (Continued)
Intervention Researcher Date
protein meals J ednak et al. (1999)
intravenous fluid intake Bennett, McDonald, Lieblic� & (1999) Piecuch
acupressure (bands) Harmon, Gardiner, Harrison, & (1999) Kelly
alcohol vapor (isopropyl) Wang, Hofstadter, & Kain (1999)
acupressure (finger) Dibble, Chapman, Mack, & Shih (2000)
According to Selye (1976), a sensory stimulus can be communicated through
several branches of nerves and can create diverse reactions throughout the nervous
system. A researcher then could logically postulate that when a nurse uses PT on several
somatosensory peripheral areas which stimulate or inhibit one or more of the nausea
pathways, the sensation of nausea might be decreased. Nerve stimuli can also converge
from multiple sources to excite a single neuron which would insure conduction of stimuli
to the central nervous system (Guyton & Hall, 1996). Touch to a sensory pathway as a
focal stimulus could alter the patient's perceptual field or modify neurotransmitter action
to decrease the distress from nausea.
The dynamic perceptual field of the open system has to do with how a person
interacts and reacts within the adaptive system (Roy, 1984). I. M. King (1981) pointed
7
out that human beings are open systems who interact with the environment. Nurses can
treat the distress of nausea by altering the perceptual field of the patient through
introducing stimuli via the senses that act as input into the central nervous system, after
which the patient can adapt to nausea (Roy & Andrews, 1999).
Touch as a Physiological Nursing Intervention
Purposeful touch (PT) was defined by Snyder and Nojima ( 1998) as intentional
physical contact by the nurse for the intent of helping. A wide range of touch
interventions was identified in the literature, such as: (a) caring, (b) protective,
(c) affective, (d) connecting, (e) working, (f) orienting, (g) therapeutic, (h) relaxation,
(i) healing, and G) social (Bottorff, 1992; Estabrooks, 1989; Meehan, 1998; Silva, 1992;
Wardell & Mentgen, 1999). The nursing intervention of PT differs in intent from other
types of touch since it is planned as a therapeutic intervention based upon scientific
rationale for a specific patient complaint. PT differs from therapeutic touch because it
utilizes tactile stimulation rather than the manipulation of energy fields. Estabrooks
defined PT as a physical, working kind of touch used during emergent or crisis situations.
Since patients identify nausea as an overwhelming distress, an emergent type of nursing
intervention would be appropriate.
PT is an intentional, planned nursing intervention that can be used for helping the
patient. According to Weiss ( 1986), there are four qualities of touch to be considered
when applying the external independent environmental stimuli: (a) intensity, (b) action,
8
( c) location, and ( d) duration of touch. Moderate intensity was identified as optimal since
too light a pressure would be minimally perceived and not even create a response and
strong pressure could cause distortions in neural conduction. In addition, the technique of
using stroking, rubbing, holding, or squeezing on a cutaneous area was identified as
meaningful by Weiss. The duration of touch was identified as important because the
length of the contact provided time for the patient to integrate the stimulus. Finally,
location was identified as a consideration, since the degree of enervation depends upon the
amount of somatosensory stimulation that results from the touch (Lamb, Ingram, Johnson,
& Pitman, 1980; Weiss, 1986). According to Guyton and Hall ( 1996), the sensory system
provides input to the central nervous system through mechanoreceptors that are sensitive
to touch, pressure, warmth, cold, and pain sensations. The transmissions of the touch
sensations adapt rapidly. These sensations continue as long as the stimuli are present and
may last minutes or hours beyond the initial stimulus.
According to Schoenhofer (1989), intensive care nurses touch the hand and
shoulder of their patients most often. The investigator has made similar observations in
which nurses used the same type of touch to calm patients in crisis, to support patients
during painful procedures, and/or to soothe patients in pain or with nausea. Based on
these observations, PT to the shoulder and handshake position was chosen as the
somatosensory areas for the purposes of this study. The areas of the touch were to the
patient's shoulder between the midclavicle and the lateral surface of the neck and the
handshake position. According to Holmes (2001 ), the touch to the shoulder area would
9
stimulate sensory neurons of the transverse cervical nerve and the supraclavicular nerves
of the superficial cervical plexus. The handshake position would stimulate the superficial
branch of the radial, the proper palmar digital branches and the palmar branches of the
· median, and the superficial and dorsal branches of the ulnar nerves of the brachia! plexus
(Holmes, 2001). The use of this bimanual touch could decrease nausea since afferent
nerve areas inclusive of dermatomes from cervical spine nerves three, four, six, seven, and
eight are stimulated simultaneously in order to alter the patient's perceptual field. The
resulting stimuli are communicated through multiple tracts to the thalamus and cerebral
cortex (Guyton & Hall, 1996). The touch could conceivably alter the focal stimulus of
nausea.
Psychological Effects
Roy ( 1984) identified nausea as an unpleasant sensation reported as a feeling of
sickness that can be stimulated by several intrinsic and extrinsic factors. Nausea can be
described as an overwhelming distress with pre learned anticipatory responses based on
previous focal stimuli. The person experiencing nausea generally reports feelings of
helplessness, overwhelming distress, and an increased need for nursing interventions to
relieve the nausea (Golberg, 1998). Other reported occurrences of nausea were attributed
to stressful situations or conversations, memories of nausea, phobias, or mental images of
chemotherapy (Redd, Dadds, Futterman, Taylor, & Bovbjerg, 1993). Anxiety is one of
the most documented psychological responses that contribute to nausea and vomiting.
------- -- ----
10
F essele ( 1996) identified that anxiety can be related to multiple factors of fear of
treatment, pain, or anticipatory expectations.
In addition to the stimuli that cause nausea, patients described experiences with
nausea as signifying suffering, demoralizing, and demeaning (Mannix, 1999). Patients
often apologize and seem embarrassed when experiencing nausea and vomiting (Renouf,
1998). These patients express concerns about causing a mess or creating offensive odors.
Concerns about the symptoms and their possible meaning were identified as anxiety
producing enough to exacerbate distress (Lenz, Pugh, Milligan, Gift, & Suppe, 1997).
According to Roy ( 1984 ), the person has innate ways of adapting to the environment and
uses both the cognator and regulator subsystems to adapt to stimuli. The person has the
ability to respond to nausea through a process of forming perceptions and using
information processing, learning, judgment, and emotion to adapt to the stimulus (Roy &
Andrews, 1999).
Nurses can treat the distress of nausea by altering the perceptual field of the patient
through introducing stimuli via the senses that act as input into the central nervous system,
after which the patient can adapt to nausea (Roy & Andrews, 1999). Behavioral
interventions identified in the literature for psychological causes or responses to nausea
are effective because they produce relaxation, distraction, feelings of control, have no side
effects, and can be used by the patient without the therapist being present (C.R. King,
2001). Some of the interventions identified were self-hypnosis, altered states of
consciousness, progressive muscle relaxation, biofeedback, imagery, distraction,
11
desensitization, and music therapy. O'Brien, Relyea, and Lidstone (1997) described
interventions such as deep breathing, resting, silence, soft music and quiet conversation to
be beneficial to decreasing nausea caused by visual or auditory stimuli. Hogan ( 1983)
suggested that empowering the patient by allowing for previous interventions that have
been successful during times of illness in the past would decrease anxiety and thus help
manage nausea. Hawthorn ( 1995) suggested the following nursing interventions for
psychological effects of nausea: (a) take time to explain treatment, (b) reassure that
vomiting is not inevitable but be realistic about it occurring, ( c) inform the patient that
anti emetics will be available, ( d) use vocabulary familiar to the patient, ( e) remove any
exacerbating factors" (p. 136). PT could be employed to provide comfort in times of
distress along with other nursing interventions that introduce stimuli into the cognator
subsystem to be processed so that the patient's adaptive responses to nausea can be
produced.
Social Effects
The social effects of nausea extend beyond just costly outcomes or lost school or
lost work days to include a direct influence upon activities of daily living and social
interactions. Nausea experienced by anyone within a group detracts from the types and
meaning of interactions. Family and friends may continue to eat but report a lack of
enjoyment of the meal (O'Brian & Naber, 1992). Nausea adds complexity to already
severe illnesses. Fifty percent of patients with myocardial infarction complained of nausea
12
(Ahmad, 1978; Ingram, Fulton, Protal, & Aber, 1980). Nausea is costly because of the
influence upon the ability of a person to work or attend school during times of illness.
Rhodes (1990) reported that among the symptoms of viral respiratory infections, nausea
and vomiting are the most common causes of employee absenteeism. Patients reported
weakness and alterations in activities of daily living and a resultant inability to work when
nausea is a concern (Engstrom, Hernandez, Haywood, & Lilenbaum, 1999). Even though
nurses can decrease nausea, it remains a distress associated with multiple diseases and the
most common complication of anesthesia despite antiemetic medications and
nonpharmacologic treatments such as acupressure (Ferrara-Love, Sekeres, & Bircher,
1996). Carroll, Miederhoff, and Cox ( 1994) reported that postoperative nausea and
vomiting costs averaged as much as $1,040 per patient with the cost for additional
supplies of at least $16 per patient. Patients who experience the distress of nausea will
spend more time in an EC, use more supplies, and require more medications than the
patients who do not have nausea (Carroll et al., 1994). If more time is required to treat
patients in the EC, other presenting patients may have to wait for care in the triage area.
According to Marley ( 1996), concerns of optimal facility usage and the inability to
provide timely care for all patients arose when there was an increased amount of care
needed for the patients with nausea in the outpatient setting. Patients who require an
increased level of care related to nausea contribute to a backup in services, and additional
holding areas may be required to allow for control of medication side effects and needed
monitoring after conventional therapies for nausea. More staff would be needed to
13
J - ---�- --��
operate the additional beds, and thus other patients may receive decreased time with health
care professionals. Individual patients who stayed longer in EC because of nausea
treatment delayed care that other patients required because of the lack of available beds
during busy times. Patients waiting for services may become more ill and require more
time to reverse symptoms which might decrease the patient satisfaction with care.
Carroll et al. (1994) reported nausea extended the length of post anesthesia time
by an average of 24 minutes. A waiting time of 24 minutes in an EC could translate into
significant loss of revenue and decreased patient satisfaction. In today's health care
environment, the cost of health care signifies an enormous concern to patients and nurses,
and relieving nausea could decrease these costs and, as a result, the concern.
Implementation of nursing interventions for nausea can provide cost-effective care with
clinically useful patient outcomes. Many of the nonpharmacologic techniques help
decrease nausea and improve the patient's quality oflife without an increase in cost. By
using PT, the nurse can support the patient until nausea medication can be administered
and augment the nausea medication effects so that a lower dose might be needed. A
lowered dose could decrease the amount of time that the EC patient spends in recovering
from the sedation side effects for many antinausea medications. PT can be implemented as
a part of nursing care without additional care time. In addition, this study of PT and
nausea relief contributed to the number of individualized interventions possible for the
patient with nausea and added to the body of nursing knowledge.
14
Theoretical Framework
A theory base is an important component of nursing research. The theoretical
basis of this study was Roy's adaptation model (Roy, 1984; Roy & Andrews, 1999).
Nausea, one of the signs and symptoms of disturbed gastrointestinal function, often occurs
with stressors to the human system in general. Since nausea can be a symptom resulting
from stress or a stressful event that often accompanies illness, groups of reactions must be
considered when assisting the patient to adapt to nausea as a pattern of response to
stressors.
The response of the person to nausea as a stressor can result from physical or
psychological stimuli from multiple pathways that can influence adaptation. Nurses can,
according to Roy and Andrews ( 1999), "promote adaptation in situations of health and
illness and enhance the interaction of human systems with the environment" (p. 55).
Human beings are adaptive systems which are more than just individual parts that function
as a whole. Human beings interact with the environment by use of internal and external
stimuli. Stimuli that catch the patient's attention and energies are called focal stimuli.
These focal stimuli can enter into the human adaptive system as input along with
contextual and residual stimuli. Stimuli and internal input result in the adaptation level.
The adaptation level remains in constant flux of change because human beings and the
environments tend to readjust constantly.
Compensatory processes may be triggered to assist with adaptation (Roy &
Andrews, 1999). The nerve impulses influence the functioning of neurotransmitters and
15
many other organ systems including the gastrointestinal tract. The endocrine glands
attempt to defend against stressors by producing adaptive hormones that cause local and
systemic changes to combat the organic effect of stress. Adaptation, as a group of
inhibitory and activating reactions to stress, integrates into a pattern of responses and not
just a single reaction (Selye, 1976). The regulator and cognator processes identified by
Roy ( 1984) can work together or as separate systems to assist with the adaptation of the
human being as part of the pattern of response. Both processes have input, internal
systems, and output. The regulator subsystem includes inputs of chemical, neural, and
endocrine stimuli that result in automatic channeling and an automatic, unconscious
response. The cognator subsystem consists of internal systems that enable the patient to
use perceptual and information processing, learning, judgment, and emotion that result in
problem solving and decision making with the output as relief from anxiety. The
autonomic processes or reflexes that may follow as a result of the body's response to
stimuli are considered outputs from the regulator subsystem (Roy & Roberts, 1981).
Nurses identify adaptation to nausea by assessing the patient's behavior during
autonomic body responses of diaphoresis, skin pallor, hypersalivation, and hypotension
(Cole, l 996� Muth et al., 1996) or by the patient's verbal complaints of nausea. In
addition, behaviors identified by Roy and Andrews (1999), such as eating patterns, sense
of taste, sense of smell, food allergies, pain, and altered ingestion, would need to be
assessed. Focal, contextual, and residual stimuli such as the structural integrity of the
digestive tract, functions of digestion, conditions of eating, or cues for eating are assessed
16
in order to identify the factors that influence the patient's digestive processes. The
sensation of nausea enters into the regulator subsystem as either internal or external
stimuli (Roy & Andrews, 1999). Nausea stimulates the system processes by way of
neural, chemical, or endocrine stimulation of the gastrointestinal tract, peripheral nerves,
cerebral cortex, cerebrospinal fluid, and the chemoreceptor trigger zone ( CTZ) ( Arakawa,
1997).
Once the stimuli and behavioral responses are identified, then barriers to
adaptation can be considered and goals established. A decision then must be made
regarding how to best assist the human system toward adaptation and which nausea
pathway can be influenced by direct intervention. As indicated by Roy and Andrews
(1999), nursing interventions promote adaptation by "altering, increasing, decreasing,
removing or maintaining" stimuli (p. 86).
According to Roy and Andrews (1999), nurses promote adaptation by altering
focal stimuli. Since the NTS is the primary relay of messages between the AP and the
respiratory, circulatory, and gastrointestinal tract, it could be deduced that a change in
external stimuli could change the focal stimulus of nausea and promote adaptation.
Nurses can use PT to change or eliminate the focal stimulus of nausea by decreasing the
associated autonomic behaviors and thus increasing the patient's ability to cope with
nausea (Roy & Andrews, 1999). As a result of this study, another focal stimulus, PT, that
enhances adaptive responses as described within the Roy adaptation model, was
supported.
17
Assumptions
This study was based on assumptions from the conceptual framework derived from
Roy's (1984; Roy & Andrews, 1999) adaptation model:
1. Human beings are adaptive systems that are more than just parts, but components
that function as whole systems (Roy & Andrews, 1999).
2. Human beings interact with the environment by use of internal and external stimuli
that enter through regulator and cognator subsystems (Roy & Andrews, 1999).
3. Nurses identify adaptive processes of illness by assessing behavior, patients'
complaints, and the focal, contextual, and residual stimuli (Roy & Andrews, 1999).
4. Nursing interventions promote adaptation by altering, removing, or decreasing
stimuli t�at can enter through the regulator subsystem (Roy & Andrews, 1999).
Hypothesis
It has been proposed that purposeful touch serves as an effective nursing
intervention to decrease the intensity of the sensation of nausea for individuals who
present to an EC treatment area with a primary or secondary complaint of nausea. The
hypothesis for this study can be stated as:
The mean nausea intensity score among emergency center patients receiving
purposeful touch to alter their perceptual field will be significantly lower than the
mean nausea intensity score among the emergency center patients not receiving
purposeful touch to alter their perceptual field.
18
Definition of Terms
For the purpose of this study, the following terms were conceptually and
operationally defined:
1. Nausea: Conceptually, nausea was defined as the feeling of distress and loss of
control of bodily functions in anticipation of vomiting (Rhodes & Watson, 1987).
Nausea was operationally measured on a 0-100 millimeter visual analog nausea
scale (VANS) with 0 being none and the 1 OD-millimeter mark described as the
worst nausea ever felt.
2. Patient: Patient was conceptually defined as a human system functioning as a
whole, who, as the focus of nursing activities, can adapt to environmental changes
(Roy & Andrews, 1999). Operationally, patient included any adult male or female
more than 18 years of age presenting to the emergency room or emergency center
complaining of nausea without history of chemotherapy, radiation therapy, or
current abdominal pathology. The patients were able to self-report nausea and
mark the degree of nausea on the VANS with their dominant hand.
3. Purposeful touch (PT): Conceptually, PT was defined as an intentional physical
- contact by a nurse intended to activate nerve impulses that can change the focal
stimulus of nausea and influence adaptation. The physical contact was the stimulus
of the nurse's hands on the patient's anterior shoulder to stimulate sensory neurons
of the transverse cervical nerve and the supraclavicular nerves of the superficial
cervical plexus and in a handshake position to stimulate the superficial branch of
19
the radial, the proper palmar digital branches and the palmar branches of the
median, and the superficial and dorsal branches df the ulnar nerves of the brachial
plexus prior to receiving other nursing or medical interventions for nausea
(Holmes, 2001 ). The operational definition of PT was an intentional physical
contact exemplified as a bimanual touch performed by a nurse, which lasted 5
seconds (Schoenhofer, 1989; Weiss, 1979) and was moderate in pressure so there
was a shallow skin indentation with no resultant change in the patient's skin color
during the time of contact (Weiss, 1986).
Limitations
The study was limited by the following:
1. Severely nauseated patients may be unable to assess or respond to the visual
analog scale for nausea.
2. Patients with a history of previous episodes of nausea or vomiting are at an
increased risk of developing nausea from sights, smells, sounds, or taste because of
a well-developed reflex arc or conditioned reflex (C.R. King, 1997; White &
Shafer, 1988).
3. Generalizability may be limited to patients of emergency rooms o,r emergency
centers.
20
Summary
The purpose of this study was to explore differences in nausea pre and post
nursing interventions between a control group (no nursing intervention) and a test group
(PT). The theoretical framework for this study, based on Roy's adaptation model,
supported PT as a method to change the sensation of nausea and the resultant distress of
the symptom. Nurses use PT to reduce anxiety, support patients during painful times, and
soothe stressful situations (Schoenhofer, 1989). Therefore, the question explored in this
study was: Will purposeful touch (PT) applied to specific nerve pathways decrease nausea
levels in patients who present to an emergency center (EC) with nausea as a primary or
secondary complaint? Assumptions were presented, the hypothesis was stated, concepts
were defined, and the limitations of this study were identified.
21
LtREWMlfl ■
CHAPTER2
REVIEW OF LITERATURE
The use of touch as a comfort measure has been described in nursing, sociology,
and psychology literature. Nurses use touch to support patients during difficult
treatments or distress (Morse, 1983; Weiss, 1986). The planned nursing intervention of
purposeful touch (PT) as a sensory stimulus, based on a scientific rationale for action,
helps relieve patient distress. Bottorff (1992) described a similar type of touch as being
provided not only for comfort but also for "calming, soothing, quieting, reassuring, or
encouraging" (p. 55). PT was not the typical physical nurse-patient contact occurring
with routine nursing procedures, but it was a nursing intervention based on the intentional
stimulation of sensory receptors of touch.
Nausea presents as a common but unique symptom for everyone (Hawthorn,
1995). "Nausea is a conscious awareness of the need to vomit" (Cole, 1996, p. 792).
Many researchers have explored vomiting but have failed to explore the distress of
nausea (Jenns, 1994). Many nursing interventions exist for relief of nausea; however,
few researchers have reported touch nursing interventions for_ nausea. The distress of
nausea has been trivialized in the past (Jablonski, 1993).
This study was designed to investigate the symptom of nausea after PT and
determine the effectiveness of PT as an intervention between a control group (no PT) and
22
""" -
a test group (PT). The related literature was reviewed and was categorized into the
following topics: (a) nausea as a focal stimulus, (b) stimuli alteration for nausea relief, (c)
touch as a focal stimulus, and ( d) touch as a nursing intervention.
Nausea as a Focal Stimulus
Almost everyone experiences nausea sometime during life. Nausea has been a
concern for people since the earliest times of human history. Hippocrates (400 B.C.E.)
described the sequencing of appetite symptoms as indicators of poor or good health.
Most of the early documented history described vomiting but omitted nausea as a form of
distress. Nausea during the Roman times was believed to result from indigestion after
eating exceptionally large meals. Roman authors also documented the occurrence of
nausea maris [sic] or seasickness (Bianchi & Grelot, 1992).
Nau sea and vomiting continued to be researched and described throughout
history, but nausea was included with vomiting rather than as a separate symptom
(Rhodes, 1990, 1997; Rhodes, McDaniel, & Johnson, 1995). Patients began making
decisions on health care based on quality of life and comfort level post chemotherapy and
would withdraw from curative treatments because of distress from nausea and vomiting
(Rhodes & Watson, 1987). Medications were developed for nausea and vomiting, but
nausea remained an overwhelming distress experienced by patients that was difficult to
measure and to research. Since nausea symptoms have a subjective nature, a valid animal
model has not been found to test medications for complaints of nausea (Fox, 1992). The
lack of specific nausea medications then increased the importance of nonpharmacologic
23
----·· ·- ·---�-- ----·- - · -· ·
interventions (C. R. King, 1997). According to Grant (1997), nurses were essential in
relieving the side effects of chemotherapy and contributing to the resultant enhanced
quality of life. Although nausea has been documented throughout history and occurs in
almost every lifetime, there continues to be little research that supports nursing
interventions for the distress of nausea.
In this review of nausea as a focal stimulus, the distress and complaints of
different patient groups were explored. Multiple causes for nausea and bodily responses
were identified in the literature. Studies were conducted to detect etiologies and
responses among groups of patient with nausea resulting from therapeutic procedures or
treatments. Many articles have been written about the causes of nausea and vomiting.
However, few studies have been concentrated on nausea as an isolated event.
NI edications and Anesthetic Agents
Nausea was a common postoperative complaint often related to medications,
fasting, anesthetic agents, or length of the operative procedure. Bellville, Bross, and
Howland ( 1960) documented factors contributing to postoperative nausea in a large
metropolitan hospital in New York City. They tested the efficiency of commonly used
medications for nausea and collected other demographic data to establish contributing
factors. Data were collected from 3,794 patients regarding medical history, previous
treatment, anesthesia, operation, and recovery room course. The researchers found that
nausea and vomiting were significantly higher among women, after mask administered
anesthesia gases, among patient groups who become hypotensive during surgery, with
24
I
.
I
I
longer anesthesia times, with abdominal surgeries, and with obese patients. Multiple
etiologies for nausea continued to be identified as medication therapies were tested.
Other researchers found that the same factors identified by earlier studies as
contributing factors to developing nausea continued even with the development of new
antiemetic medications and anesthetic agents. M. Cohen, Duncan, DeBoer, and Tweed
( 1994) reported that nausea and vomiting continued at a rate of 20% to 3 0% for the
postoperative patient. The descriptive data collected in four large hospitals in the Eastern
United States and Canada included 15,992 patients who were interviewed within 72
hours postoperative. A visual analog scale was used to allow patients to detect severity
of nausea. Analysis of data was based on crude relative odds and adjusted relative odds
of each risk factor established. Multiple logistic regressions were used to control for
variables such as the role of gender and type of surgical procedure or the type of patients
treated in different hospital sites. The factors that contributed to postoperative nausea
included: (a) being of a younger age, (b) being of the female gender, (c) being intubated
for anesthesia, ( d) having a decreased physical status, ( e) having no preoperative medical
conditions, (f) experiencing a longer anesthesia time, (g) having an elective operation,
(h) receiving opioids intra operative, and (i) being a nonsmoker. Postoperative nausea
continued to be a problem for patients and had not diminished over the years (M. Cohen
et al., 1994).
Patients with middle ear., gynecologic, cardiothoracic, and abdominal surgeries
reported nausea more often than other patients (Cetindag, Boley, Magee, & Hazelrigg,
25
longer anesthesia times, with abdominal surgeries, and with obese patients. Multiple
etiologies for nausea continued to be identified as medication therapies were tested.
Other researchers found that the same factors identified by earlier studies as
contributing factors to developing nausea continued even with the development of new
antiemetic medications and anesthetic agents. M. Cohen., Duncan., DeBoer
., and Tweed
( 1994) reported that nausea and vomiting continued at a rate of 20% to 3 0% for the
postoperative patient. The descriptive data collected in four large hospitals in the Eastern
United States and Canada included 15.,992 patients who were interviewed within 72
hours postoperative. A visual analog scale was used to allow patients to detect severity
of nausea. Analysis of data was based on crude relative odds and adjusted relative odds
of each risk factor established. Multiple logistic regressions were used to control for
variables such as the role of gender and type of surgical procedure or the type of patients
treated in different hospital sites. The factors that contributed to postoperative nausea
included: (a) being of a younger age., (b) being of the female gender, (c) being intubated
for anesthesia, (d) having a decreased physical status, (e) having no preoperative medical
conditions, (f) experiencing a longer anesthesia time, (g) having an elective operation,
(h) receiving opioids intra operative, and (i) being a nonsmoker. Postoperative nausea
continued to be a problem for patients and had not diminished over the years (M. Cohen
et al., 1994).
Patients with middle ear., gynecologic
., cardiothoracic, and abdominal surgeries
reported nausea more often than other patients (Cetindag, Boley, Magee, & Hazelrigg,
25
1999; Grapp, Savage, & Hall, 1996; Honkavaara & Pyykko, 1998). Quinn, Brown,
Wallace, and Asbury (1994) identified common patterns of nausea in their descriptive
study based on nominal data collected from 3,850 postoperative patients. The sample
included patients between the ages of 11 and 91 years, with a total of 1,365 male and
1,879 female participants. Over two-thirds (37%) of the 3,244 patients who received a
general anesthetic and one-fifth (20%) of the 606 patients who received a local anesthetic
reported nausea. Chi-square, Mann-Whitney, or the Kruskal-Wallis tests were used for
analysis of data. However, the results of the statistical tests were not specified but some
percentages and noted median scores were reported. Complaints of nausea were
significantly higher among women (72.2%, p < 0.0001) and the younger age group
( median = 4 7 years., inter quartile range = 3 2 years, p < 0.0001 ). A significant difference
was found between nausea and level of pain (with general anesthesia, M = 4.3 pain level,
with local anesthesia, M = 3. O pain level), placement on a gynecology postoperative unit
(with general, 52%, and with local anesthesia, 50%), anxiety (with general, 40.9%, and
with local anesthesia, none). Twenty percent of all patients reported nausea
postoperatively, with increased numbers within the groups of patients with gynecological,
cardiothoracic, and general surgery. The researchers concluded that nausea was a
multifaceted problem that would require multiple strategies to treat successfully. Thus,
the researchers suggested a multiple medication approach to prevention of postoperative
nausea and vomiting. Postoperative nausea continued to be a problem in at least 23% of
all patients receiving general anesthetics (Quinn et al., 1994 ).
26
Contributing Factors of Age and Gender
Age and gender were identified as significant factors to consider when assessing
nausea as a primary complaint. Rub, Andrews, and Whitehead ( 1992) recruited 596
participants from various social groups, government offices, banks, schools, family
planning clinics, and day care centers for the elderly from a European city. Of the
respondents, 54% reported at least one episode of nausea in the past 12 months. Data
were analyzed with the chi-square test. No significant relationship was found between
nausea and gender. The researchers, in this non experimental descriptive study,
discovered a significant decrease in nausea with increasing age (X2 = 114.1, p < 0.0001 ).
Postmenopausal women were less likely to experience nausea (n = 175, X2 = 74.89,
p < 0.0001) than menstruating women. In healthy populations, nausea was more severe
in the 18-30 year old group than in the 31-60 or in the > 60 year old groups. Age was a
contributing factor in complaints of nausea as a primary complaint and could be a factor
for patients' responses to medications (Rub et al., 1992).
According to Dodd, Onishi, Dibble, and Larson ( 1996), age could be a factor in
outpatient chemotherapy nausea. The researchers conducted a 4-month study including
127 participants from 18 different outpatient settings. The study used a nonexperimental
design to establish differences in nausea between lesser than 64- and greater than
65-year-old patient groups. The Rhodes Index of Nausea and Vomiting Form 2 and a
behavior checklist developed by the researchers were used to determine distress from
nausea and vomiting and self-care measures that patients used to decrease the symptoms.
27
The average age of the younger group was 47.5 years (n = 40), while the older group
mean was 70.4 years (n = 6). Although the older group experienced less nausea and
vomiting than the younger group at 24 hours after the first cycle of chemotherapy, a two
way ANOVA revealed no significant differences between groups (F = 0.92, with the p
expressed as nonsignificant). Both groups reported doing the same interventions for
nausea. The only significant finding in this study was that the older group used
distraction-type behaviors more often than the younger group based on chi-square
analysis (X2 = 7.14, p = < 0.004). The researchers suggested that more precise
instruments are needed to establish outcomes of interventions and larger groups of
participants in future studies. According to the researchers, further research needs to be
done to determine effectiveness of nursing interventions for the symptoms of nausea and
vomiting in the chemotherapy patient (Dodd et al., 1996).
Anoxia
As pointed out by Ingram, Fulton, Protal, and Aber (1980), myocardial ischemia
can cause nausea and vomiting by stimulating left
ventricular receptors that result in
gastric relaxation. In a descriptive study, Grapp and associates ( 1996) documented
gastrointestinal symptoms in a group of 122 adult patients post cardiac surgery. The
researchers used the Gastrointestinal Symptom Frequency, Symptom Distress Scale and
The Center for Epidemiologic Studies Depression Scale to collect data post intensive care
and at 2 weeks and 6 weeks after discharge. The post discharge data collection was
completed by telephone interview. Nausea was a concern in the postoperative group.
28
One-third (34%) of the subjects reported nausea during the hospitalization, while only
10% continued to report nausea 6 weeks after being discharged. Based on a logistic
regression analysis, subjects who had higher depression scores reported significantly
higher nausea levels while in the hospital (n = 33, odds ratio = 0.264, p < 0.01), and 2
weeks after discharge (n = 18, odds ratio = 3.917, p < 0.05). Reported nausea was
significantly higher among patients receiving antiarrhythmic medications while in the
hospital (n = 33, odds ratio = 0.264,p < 0.01). There was no relationship found between
blood pressure, mixed venous oxygen saturation, and subject age in this study. The
researchers suggested that nurses should be aware of this potential distress and provide
more detailed nutritional instructions for home care after any cardiac surgery (Grapp et
al., 1996).
Psychological Factors
Mental images of treatment increased or created the sensation of nausea among
patients thinking about chemotherapy. Redd, Dadds, Futterman, Taylor, and Bovbjerg
( 1993) explored the possibility of mental images of chemotherapy as causes of nausea.
Ten women with histories of post chemotherapy nausea were observed and videotaped
during imagery scenarios introduced by a psychologist. This experimental study was
designed to explore three scenarios described as: ( a) a walk in a pastoral setting, (b) a non
cancer medical treatment, and ( c) chemotherapy. Participants were interviewed in an
outpatient setting separate from the chemotherapy center. The dependent variables were
nausea, anxiety, and vivid imagery ranked on a 0-100 scale. The independent variables
29
were thoughts of medical treatment and chemotherapy. The results of this study
suggested that the cause of nausea among potential chemotherapy patients could be
associated with mental images of chemotherapy and expectations of the patients. The
researchers suggested that future research should be focused on the conditioned response
of post chemotherapy patients. Redd et al. also suggested nausea research could be done
to develop interventions for cessation for the conditioned response.
Depressed and anxious patients have been identified with complaints of
gastrointestinal distress including complaints of nausea (Langeluddecke, Goulston, &
Tennent, 1990; Talley, Fung, Gilligan, McNeil, & Piper, 1986). Handa and associates
(1999) collected data in Japan from 71 patients complaining of functional dyspepsia.
Patients who complained of epigastric pain (group one) nausea, vomiting, and heartburn
(group two) were evaluated for underlying physical or psychiatric etiologies for their
distress. A control group was assigned from 20 healthy volunteers. All subjects received
esophageal manometry, provocative tests for chest pain, and a State-Trait Anxiety
Inventory assessment. The Mann-Whitney U, chi-square, and Kruskal-W allis tests were
used to compare age, gender, duration of illness, manometry, provocative tests, and the
anxiety inventory results. Results were reported as means, medians, and probability.
There was a probability of 0.0508, based on the chi-square test with Yates' correction
that depression (n = 39, 48.7%) and anxiety (n = 8, 20.5%) can influence the symptoms
. of nausea, vomiting, and heartburn. Randa et al. added that cultural differences must be
considered before this research could be generalized to other patient groups.
30
Pregnancy
Whitehead, Andrews, and Chamberlain (1992) identified that nausea, vomiting�
and taste aversions are common symptoms of pregnancy as early as 4 weeks past the last
menses. The researchers reported that at least 85% of the 1,000 surveyed women, who
were attending an antenatal clinic in a European city, experienced nausea. Several
etiologies for nausea were explored. A chi-square statistic was used to analyze the data
collected from a detailed questionnaire. The results of data· analysis were reported as
totals, percentages, and probabilities only. The groups with nausea as a significant
reported symptom were women: (a) with pre menstrual tension (11 = 283., X2 not reported,
p < 0.005), (b) who developed food cravings (45%, X2 not reported,p < 0.05), and
(c) with planned pregnancies (63%, X2 not reported,p < 0.05). Nausea in pregnancy,
according to the researchers, was not explained by hormones or other circulating factors
but could be caused by complex neuronal circuitry that develops with pregnancy
(Whitehead e� al., 1992).
The complex hormonal and physiological interactions that occur with pregnancy
also may contribute to nausea and vomiting of pregnancy. van Lier, Manteuffel, Diiorio,
and Stalcup ( 1993) investigated the relationship between the nausea and fatigue of
pregnancy. The researchers identified their study as a descriptive correlational design
that included 51 pregnant women 20-41 years of age who visited a nurse-midwifery
clinic in a large southeastern city. The two instruments used were the Pearson-Byars
fatigue-feeling checklist and researcher-developed nausea scale rating nausea and distress
31
from nausea on a Likert scale. The dependent variable was fatigue, and the independent
variable was nausea. The researchers used a t test to compare mean level of reported
fatigue with reported nausea. van Lier et al. reported that women with nausea are no
more likely to complain about fatigue (t = 0.92, p = 0.363) than those without nausea.
Fatigue scores increased with increasing nausea severity scores (t = -1.96, p = 0.055), but
the differences were not significant. Women with severe nausea complained of greater
fatigue based on a Spearman's rank correlation coefficient (rho = 0.46,p = 0.001). The
researchers recommended that helping the gravid women to schedule their day to include
sufficient rest periods might decrease nausea (van Lier et al., 1993).
Many variables may contribute to nausea and vomiting of pregnancy other than
complex physiological interactions and fatigue. O'Brien and Zhou ( 1995) used the
Rhodes Inventory of Nausea and Vomiting (INV) and the 16 Personality Factor (16PF)
questionnaire to establish relationships between symptoms of nausea and vomiting
(dependent variable) and maternal age, occupation, parity, cigarette smoking, infant
gender, and the personality trait ofindependence (independent variables). The 126
pregnant women were observed from their 'first antenatal visit until the postpartum visit
to obstetric and nurse-midwife practices in the Midwestern United States. Demographics
and The Rhodes INV were completed during the first visit at less than 16 weeks of
gestation. The participants completed the 16 Personality Factor questionnaire between 24
and 29 weeks gestation. Based on multiple regression analysis, nausea significantly
correlated with age of gravid women, work outside the home, parity, and independence
32
(F= 4.73,p < 0.01). The inadequate sample size may have contributed to the inability of
the researchers to predict the presence and severity of nausea and vomiting. Further
studies were planned to explore the maternal response to interacting hormones (O'Brien
& Zhou, 1995).
In summary, this review identified the ages, genders, groups, and diagnoses most
affected by nausea. As previously reported, younger age groups between the ages of 18
through 3 0 experience nausea more often than older adult age groups greater than 3 1,
although all age groups used the same interventions for nausea and received similar
medications. A greater risk for developing nausea was identified among pre menopausal
female patients. Surgery also was identified as a cause influencing the development of
nausea. Types of surgery, events in preparation for surgery, and events occurring during
operative procedures were identified as risk factors for developing postoperative nausea.
According to the researchers, nausea was associated with preoperative medications,
preoperative fasting, types of anesthetic agents, length of the operative procedure
( anesthesia time), types of operative procedure, having an elective procedure, being
intubated for general anesthesia, hypotension during the operative procedure, having no
preoperative medical conditions, receiving opioids during surgery, being a nonsmoker,
level of pain, anxiety, and obesity. Nausea most often occurs with middle ear,
gynecologic, cardiothoracic, and abdominal surgical procedures. Nausea also was
associated with mental images of chemotherapy, radiation therapy, and patient
expectation of treatment outcomes. As documented in this review of literature,
33
depression, anxiety, myocardial ischemia, and antiarrhythmic medications also contribute
to nausea. The complex hormonal, neuronal, and physiological interactions that occur
with pregnancy also can contribute to nausea. Women most likely to have nausea and
vomiting were summarized as having the following risk factors: (a) pre menstrual
tension, (b) food cravings, ( c) planned pregnancies, ( d) fatigue, ( e) age of less than 3 5
years, (f) occupations requiring exposure to odors, (g) nulliparity, (h) nonmoving, and
(i) male gender embryos. As demonstrated in this research review, nausea was a
multifaceted problem that requires larger sample sizes, more precise instruments for
assessing, further research to develop nursing interventions, and outcome analyses to
validate patient responses to the multiple interventions needed for nausea relief
Touch as a Focal Stimulus
According to Barnett ( 1972), touch has been used since the beginning of
humankind and was used in nursing from the very beginnings of professional practice.
Barnett described touch as integral to nursing interventions and essential for
communication. McCorkle and Hollenbach (1990) recognized touch as an act of
communication and not as a therapeutic event. However, touch was identified by
S. Cohen (1987) as one of the earliest healing techniques documented in history. The
Egyptians used techniques of touch for medical purposes as early as 1553 B.C. The
ancient Greeks also used touch to cure illness. Around 400 B.C., Greek internists used
their palms and fingers to heal various illnesses (S. Cohen, 1987).
34
1:WTI ""
Touch was a universal healing method in the early church and was found in at
least nine chapters of the Holy Bible (1611). According to the New Testament, Jesus ·
Christ used the power of touch to heal illnesses: "And whenJesus was come into Peter's
house, he saw his wife's mother laid, and sick of a fever. And he touched her hand, and
the fever left her: and she arose, and ministered unto them" (Matthew 8:14-15).
However, little evidence of ancient touch for healing specific ailments has survived since
the early church (Grad, 1965; Ruckman, 1980). Montagu (1986) described touch as a
basic behavioral need essential for normal growth and development that contributes to the
overall efficient functioning of the nervous and immunological systems. Several research
projects followed since then establishing the influence of touch as a focal stimulus.
McCorkle (1974) researched the effects of touch on 60 seriously ill hospitalized
medical surgical patients between the ages of 20 and 64. This experimental study
consisted of a control group and an experimental group of equal numbers based on an
alternate assignment of participants. The participants were selected based on age,
sensory intactness, chance of recovery, orientation to surroundings, freedom from oxygen
masks, and freedom of one arm from intravenous or other treatments that would restrict
touch of the wrist. The dependent variable was identified as positive acceptance
responses, and the independent variable was touching and verbal stimuli. The Interaction
Behavior Worksheet was used by the researcher to focus on the patient's nonverbal
behaviors to initiate the interaction, and the Intrusa-Gram Worksheet was used to classify
35
the nonverbal behavior observed into either facial expressions, body movements, eye
contact, and general response of the patient.
After the interaction, the patients were questioned about their perceptions of
comfort and interest that the nurses portrayed. The data from the worksheets and Bales'
Interaction Process were analyzed using the Kolmogorov-Smimov two-sample test. The
researcher reported a significantly greater number of patients measured by facial
expression within the experimental group as responding positively to touch (D = -0. l 7,
p = 0.01). No significant differences were found between the groups when changes in
body movement, eye contact, length of nurses' verbalization, or EKG changes were
· analyzed. The results of this study supported the use of touch to communicate caring to
seriously ill patients. McCorkle (1974) suggested that touch should be considered as one
aspect of communicating and that nurses need to develop other methods of nonverbal
communication and touch to help the seriously ill patients.
Mills, Thomas, Lynch, and Katcher (1976) explored the effect of touch (taking a
pulse) on 62 coronary care patients. A total of 171 pulse palpations was monitored with a
3-minute resting time before and after the intervention. The independent variable was the
use of touch, and the dependent variables were supra ventricular and ventricular cardiac
arrhythmias. A significant increase in cardiac arrhythmias was found in all participants
who were touched based on chi-square statistical analysis (X2 = 5.26, p < 0.01). The
researchers concluded, based on the outcome of this study, that the changes in cardiac
arrhythmia frequency could be associated with autonomic activity resulting from social
36
interactions. These researchers did not explore other neurogenic or psychogenic factors
that could contribute to myocardial irritability. The findings suggested that, despite other
environmental stimuli in critical care settings, touch was a potent enough
neurophysiologic stimulus to cause a change in the patient condition (Mills et al., 1976).
Drescher, Gantt., and Whitehead (1980) also investigated heart rate and response
to touch (talcing a pulse). They explored the effect of touch on four men and four women
participants with an average age of26.4 years. The environment for the study was
controlled, and a closed circuit television camera monitored the action. A polygraph
machine with skin and ear electrodes was used to record the heart rate. Each participant
received the same interventions--door closed, door open before touching; hand on
participants' wrist, door open after touching., and door closed. There was a significant
increase in heart rate (t = 2.68, p < 0.05) when the researchers entered the rooms and a
significant decrease when the researchers touched the wrist for 30 seconds (F= 10.7,
p < 0.001).
Drescher et al. (1980) then replicated the study to discover if the change in heart
rate was from touch alone or could be the result of touch by another person. Heart rates
of a new group composed of five women and three men (average age of25.8) were
compared with the same design with the addition of the action of the subjects taking their
own pulse. The results showed that touch by the researcher decelerated pulse rates
(t = 3.67, p < 0.05) between the subjects and that self-touch slightly accelerated pulse
rates. Touch influenced the pulse rate of both healthy and coronary care patients. This
37
cardiac response was similar to one noted in infants as a potent reaction to touch
(Drescher et al., 1980).
Knable ( 1981) researched hand holding to determine its effect on vital signs and
nonverbal communication gestures made by patients and to describe reasons for use and
situations where the technique might be used. Fifteen critically ill patients were selected
from a sample in a community hospital in the Eastern United States. All patients were
monitored by electrocardiogram, and vital signs were taken by one of 12 female nurses
involved in the patients' care. The researcher described the facial expressions, body
movements, eye contact, and general responses recorded on the Intrusa-Gram Worksheet
used by trained observers. The observer documented three different responses among
participants: positive, neutral, or negative. Nurses chose the times to touch the patients,
and the touch was described as purposeful and nonprocedural in nature. Vital sign
changes were reported from hand holding. The patients responded to 25 touches as
genuinely interested, and 221 out of 3 06 reported touches were evaluated as nonverbally
positive by the observers. The nurses described hand holding for providing emotional
support for patients who were alone or apprehensive (Knable, 1981 ). This research did
not establish statistical significance. However, the researcher suggested that hand
holding should be used as a nursing intervention to enhance nonverbal communications.
Glick ( 1986) postulated there was a relationship between procedural and caring
touch and anxiety experienced by the patient with a myocardial infarction in the
intermediate care unit. The researcher defined procedural touch as "the use of the hands
38
in completing nursing duties and caring touch as non task related, conscious, nonverbal
communication in which one's hands or anns make contact with another person, in the
promotion of that individual's inherent uniqueness" (Glick, 1986, p.63). In the quasi
experimental study, 40 male and female patients were systematically assigned to study
groups. Anxiety was the dependent variable measured by the State-Trait Anxiety
Inventory. The type of touch was the independent variable. However, the analysis of
data using analysis of variance (ANOVA) revealed no significant difference between
groups (n = 33, experimental group pre touch (PRE) M = 35.31, post touch (POST)
M = 33.93; control group PREM= 34.39 and POST M = 34. 78 with total groups'
ANOV A between F = 0.00, p = 0.9949). Thus, the results did support previous research
regarding touch and scientific rationale suggested by other authors, such as the sensory
influence of the skin and the ability of touch to reduce tension (Glick, 1986). Glick
erroneously assumed levels of anxiety to be high but they were not assessed as such by
the participants. The researcher also underestimated the effect of age and preexisting
coronary artery disease in this study.
Research and early historical writings support touch as a potent stimulus that can
comfort patients in distress. Since early human history to current times, human touch has
been effective but research has not empirically established the significance of touch
therapies. Touch as more than just nonverbal communication can influence cardiac
rhythm, emotions, blood pressure, pulse, and respirations. Nurses change patient
39
behavior by altering, changing, removing, or maintaining stimuli (Roy & Andrews,
1999). The research cited established the fact that touch can be a strong focal stimulus.
Touch as a Nursing Intervention
According to Barnett ( 1972), registered nurses touch twice as often as other health
care personnel. · Durr ( 1971) used a nonexperimental research design to explore reactions
to touch in 13 medical-surgical patients. The six men and seven women included in this
study were able to identify physical contact between themselves and the nurses as
beneficial. These patients reported a feeling of physical support, an increased level of
understanding, and verification of verbal communication based on the physical contact
between the research subjects and the nurses. The researcher suggested that touch and
physical closeness facilitate patient comfort as long as the interactions are therapeutically
relevant. However, actual practices of touch between patients and health professionals
still needed to be identified (Durr, 1971).
Barnett ( 1972) conducted a survey of the frequency of touch to determine the
practice of touch between patients and health team members. The researcher observed
540 patients and 900 health team personnel for a total of 452 touches over a 4-week
observation period in all patient care units. These units were in both a church-supported
and tax-supported facility in a large metropolitan medical center. Patients were touched
significantly more often (F = 4.1849, p < 0.001) in the tax-supported facility by personnel
between the ages of 18 and 32. Other analyses of data were reported as percentages of
touch occurrences. The researcher reported that health personnel's use of touch
40
T -
decreased with age, which refutes the claims of other researchers that touch was equated
with sexual intent and usually avoided unless with friends in the American culture.
Female personnel touched 85% more often than males. Registered nurses touched twice
as often as other personnel. Personnel reporting to be among the White race touched
more often than the other races (73%) .. The patients' extremities were touched 60% more
frequently than other parts of the body. Touch was used more often in the pediatric, labor
and delivery, recovery room, comatose, and intensive care units in both hospitals.
Patients who were listed in good or fair conditions were touched 70% of the time as
opposed to patients in serious or critical condition. Patients between the ages of 26 and
33 (25%), White (66%), and female (53%) were touched more often than the other
groups. The researcher reported data to support and identify factors involved with the
intervention of touch but failed to establish statistical significance between groups other
than differences in frequencies of touch between types of hospitals. Health care workers
did not touch the more affluent patients as often (Barnett, 1972).
Copstead ( 1980) pointed out that touch communicated caring to the elderly adult.
The researcher investigated touch, nurse/patient interaction appraisal, and self-appraisal
scores between the elderly patient and registered nurses. The dependent variables were
the nurse/patient interaction and self-appraisals of the patient. The independent variable
was the use of touch. This study had a control group with no touch and an experimental
group of patients receiving physical body contact with a nurse at any time of the
nurse/patient interaction. A random sample of 3 3 permanent residents of three nursing
41
homes was included in the study. The participants were included in the study if they
were able to feel the nurse's touch, follow directions, respond verbally in English to direct
questions, read and write in English, and had known the medication nurse for at least one
month. Self-appraisal scores were significantly higher in the experimental group
(p = 0.001) based on a Pearson's correlation coefficient (r = .86). Since the interaction
times in the experimental group ranged from 5.40 to 197.69 seconds and 6.24 to 38.78 in
the control group, the researchers postulated that touch lengthens interaction durations.
However, the interactions times could have contributed to the heightened self-appraisal
scores rather than touch alone. Since the use of touch lengthened interactions, the
researcher suggested that more time be allocated for routine nursing procedures so that
touch could be used during nursing procedures, even while administering medications to
the elderly, to enliven the lived experience (Copstead, 1980).
Langland and Panicucci ( 1982) postulated that touch preserved relational aspects
of communication with elderly confused patients. This experimental study used a
selected sample of 32 elderly confused participants who were divided into control and
experimental groups. The researchers were exploring the effect of the independent
variables of touch and verbal request on the dependent variables of attention, relevant
verbal responses, and action responses. A significant increase in attention was found
when touch was used based on analysis by the Wilcoxon rank sum test ( experimental
11 = 16, sum of scores = 315.00; control n = 16.,
sum of scores = 213, andp = 0.05).
However, the other dependent variables were not supported as significant by the data
42
analysis. Although verbal and action responses of the patients were not influenced by
touch in this study, the researchers felt that significance could be established with more
participants and more experiences of touch (Langland & Panicucci, 1982).
In one study, affectional touch was primarily used for transmitting signals of
recognition, acceptance, protection, and caring. Schoenhofer ( 1989) collected data to
establish qualitative and quantitative factors involving affectional touch in critical care
nursing. The researcher used a convenience sample of 30 nurse-patient groups in three
intensive care units in two Midwestern hospitals. Instances, form, qualitative factors,
accompaniments, stimuli, and proximity without touch were the six observed factors.
Patients in this study received affectional touch by nursing personnel an average of2.8
times per hour. Nurses used sustained stationary touch (f = 26) to a hand (f = 29) or
shoulder (f = 23) most often. The researcher identified that the shoulders were the most
common touch location which was reported as the least touched area by Copstead (1980).
The motivation underlying touch and assessment for the need for touch were identified as
essential for further formalization of a nursing theory for touch (Schoenhofer, 1989).
Weaver (1989), in a qualitative pilot study, explored the meaning of touch for
obstetrical nurses. Eleven registered nurses practicing in labor and delivery were
interviewed using a semi-structured interview guide. The sample was composed of
nurses with an average age of 31, with five graduates from baccalaureate programs and
having an average of 4. 5 years of obstetrical experience. The researcher concluded that
touch: (a) was an essential strategy, (b) was potentially a powerful modality, (c) was used
43
by nurses based on experience and sensitivity, ( d) included both giving and receiving,
( e) could be a learned competency, and (f) could be perceived by patients as negative if
withheld. The researcher suggested further study to clarify the use of touch for specific
medical diagnoses and to develop the ability to teach the use of touch. Nurses shared self
with patients by using touch (Weaver, 1989).
Bottorff ( 1992, 1993) pointed out that touch forms an important aspect of nursing
practice. The researcher used qualitative ethology to identify types of touch and
attending types used by nurses. Five types of touch were identified by analysis of video
taped nurse-patient interactions with eight oncology patients. These touches were similar
to procedural and caring touch as identified by other researchers but offered more
comprehensive descriptors of touch techniques. Comforting, connecting, working,
orienting, and social were identified as types of touch used while nurses attended patients
with cancer. The types of attending (Bottorff, 1992; Bottorff & Morse, 1994) identified
by the researchers supported the premise that the context of touch was critical to
understanding the use of touch. The types of touch and caring methods can be changed
to meet the needs of each patient (Bottorff, 1993).
Based on the previously cited research, touch contributed to feelings of physical
support, increased levels of understanding, and verification of communication between
patients and nurses. Furthermore, touch can be a learned competency and must be
therapeutically relevant to transmit signals of recognition, acceptance, protection, and
caring. In some studies, the patients' extremities were touched most often by female
44
nurses in the pediatric, labor and delivery, recovery room, intensive care, and in not-for
profit hospital settings. Additionally, some uses of touch identified by the researchers
included: (a) an essential strategy identified by nurses as a way to share self with patients,
(b) a potentially powerful modality, (c) a determinant factor of nurses' experience,
sensitivity, giving, and receiving, (d) a way of lengthening nurse/patient interactions, and
( e) a contributor to heightened self appraisals and increased quality of life. Touch could
be perceived by patients as negative if withheld. In one study conducted within critical
care units, nurses used a stationary touch to a hand or shoulder most often (Schoenhofer,
1989). Another study identified five types of touch: (a) comforting, (b) connecting,
(c) working, (d) orienting, and (e) social (Bottorff, 1992). The researchers also identified
that further research will be needed to explore the influence of the context of touch, types
of touch as caring methods for meeting the needs_ of each patient, actual practices of
touch between patients and health professionals, use of touch to intervene on specific
medical diagnoses, and formulation of a nursing theory for touch.
Stimuli Alteration for Nausea Relief
Even though acupressure (AP) and therapeutic touch (TT) are interventions that
require different techniques than the PT identified in this study, they are reviewed as
interventions to activate stimuli that could relieve nausea. AP is the use of a deep,
constant pressure on exact points along acupuncture meridians which have a relationship
with various physiological functions (Tappan, 1988). According to Krieger (1987), TT
represents a human field phenomenon that uses a human energy transfer from the healer
45
to the ill person via electron transfer resonance to restore the vital flow in the patient's
open system.
Acupressure
Ulett, Han, and Han (1998) identified acupuncture as an umbrella term that
included acupressure (APr Uses for acupuncture include but are not limited to headache,
menstrual cramps, fibromyalgia, low back pain, carpal tunnel syndrome, asthma, and
nausea. Acupuncture is an ancient system of healing developed from the traditional
medicine of China and other Eastern countries over 2,500 years ago. The practice began
with the idea that stimulation of areas of the skin can influence organ functioning. The
skin areas are located on specific locations that are believed to lie on energy channels or
meridians. Acupuncture is the practice of inserting needles in these energy channels to
either stimulate or depress organ actions associated with the skin areas. Acupressure is a
therapy that utilizes the same skin areas and the meridians of acupuncture to identify
points where finger friction and pressure can improve organ function (Ulett et al., 1998).
According to The National Institute of Health (1997), acupuncture can have therapeutic
effects for pain conditions, nausea and vomiting in adult postoperative, chemotherapy
patients, and nausea of pregnancy. A similar statement regarding AP was not included in
The National Institute of Health Consensus Statement (1997).
Researchers have established scientific rationale for the use of AP over the P-6 or
ST-38 points to relieve nausea. The P-6 point was located two thumb-breadths (two cun
[sic]) "above the ventral wrist fold between the tendons of palrnaris longus and flexor
46
carpi radialis" (Tappan, 1988, p.151 ). The ST-36 point was located "one cun lateral and
distal to the tibial tuberosity" (Tappan, 1988, p. 152). AP activates the same points to
relieve nausea as the corresponding acupuncture point. In all of the following reported
research, the dependent variable was nausea and the independent variable was the
technique of finger AP or AP bands.
Dundee, Sourial, Ghaly, and Bell (1988) conducted a prospective study to test the
efficacy of AP in preventing morning sickness of pregnancy. The sample included 350
pregnant outpatients randomly assigned to one of three groups. The patients in the P-6
experimental group were instructed to press the P-6 point for 5 minutes every 4 hours for
four consecutive days. The second group was to press a dummy point near the right
elbow with the same frequencies. The control group was to report emetic symptoms with
the same frequencies. The grading of emetic symptoms was a 5-descriptor Likert scale
which allowed the participants to rank the nausea from none to severe. Only 50% of the
acupressure group, 52% of the dummy group, and 70% of the control group returned
completed data cards. Data were analyzed using chi-square tests. Significant differences
occurred between the experimental, control, and dummy groups. The experimental group
experienced less nausea than the dummy (X2 = 21.9,p < 0.0005) or control group
(X2 = 36.4,p < 0.0005). There was also a significant decrease in the dummy group's
nausea as compared to the control group (X2 = 13.4, p < 0.01). Chi-square analyses were
reported as comparisons between two groups rather than an overall significance with post
hoc investigation. The researchers reported there was a beneficial effe�t of P-6 AP
47
despite the high attrition rate. They asserted that AP was a safe technique that can be
used for morning sickness instead of medications which frequently cannot be used with
the gravid female because of side effects (Dundee et al., 1988).
Postoperative nausea and vomiting can be decreased by AP, as reported by
Dundee et al. (1989). Fifty-one women were selected with similar weights, ages,
anesthesia times, and type of anesthesia. AP bands were used on the dominant arm at the
P-6 AP point and were pushed by the patients for 5 minutes each hour during the time of
the study, as encouraged by the nurses who accompanied the patients during the
postoperative period. Data were collected at 1 hour and 6 hours postoperative as nausea,
vomiting, or no nausea/vomiting. Chi-square analysis indicated a significant difference
between the AP group and the control group within the first hour only (X2 = 31.4,
p < 0.001). Since this AP study was part of a larger study on the effects of acupuncture
on postoperative nausea and vomiting, the control participants were used for analysis in
both the acupuncture and the AP groups.(Dundee et al., 1989).
Dundee and Yang (1990) used AP bands to prolong the antiemetic effects of
acupuncture in 40 patients receiving chemotherapy. The AP bands were applied to the
patients' dominant arms immediately after the pre-chemotherapy acupuncture procedure,
and the patients were instructed to press the stud on the AP band for 5 minutes every 2
hours. Significance was not established in this descriptive study. Percentages of
effectiveness over time were reported as 95% of the patients having beneficial anti emetic
48
effects for 24 hours after acupuncture on a scale of good, moderate, slight, or nil [sic]
benefits from P-6 AP (Dundee & Yang, 1990).
According to Brown, North, Marvel, and Fons (1992), nausea and vomiting may
be a major distress for terminally ill patients. In an attempt to decrease medication use
and resultant side effects, the effectiveness of AP was explored in this six-subject study.
The researchers used a 4-item abbreviated Rhodes Index of Nausea and Vomiting rating
scale to collect data after the three interventions of an AP wrist band, a placebo wrist
band, and no wrist band. The subjects were not able to complete the study and data were
incomplete. No decrease in nausea was reported by the researchers to justify the use of
AP bands for terminally ill patients (Brown et al., 1992).
. In an experimental study using AP bands for nausea and vomiting in pregnancy,
Stone ( 1993) recruited 31 participants in their first 12 weeks of pregnancy who were
visiting a university-based health care clinic for prenatal care. The experimental group
wore AP bands and the control group wore placebo bands for a total of 7 days for all
participants. Data were analyzed using a t test for independent samples. A significant
difference (t = -2.04, df= 27, and two tailedp = 0.0520) was found between the 17
experimental group scores (M = 0.3232, SD = 1.128) and 14 control group scores
(M = -0.3978, SD = 0.657). The control group bands were found to be more effective
than the experimental AP bands. The small sample size and the lack of ability to do
follow-up on the correct· application of the AP bands during the length of the study were
identified as limitations (Stone, 1993).
49
Phillips and Gill ( 1993) reported that postoperative nausea could be reduced when
AP wristbands were used. Their sample of 80 female patients between the ages of 18 and
81 were admitted for major gynecological surgical procedures. In this experimental
study, groups were randomized into two groups. The experimental group wore AP bands
on both wrists prior to and for 2 days after surgery, while the control group received no
bands. The nausea levels were evaluated using a 0- to 9-point scale and by measuring the
total amount of antiemetic medications given. Data were analyzed with a Student's Ltest
for paired samples. The experimental group required fewer doses of antiemetics (11 = 28,
M = 1. 5, SD not reported, t not reported, p = 0.001) than the control group ( n = 28,
M = 3.5). The I-test scores or standard deviations were not reported in the data analysis
of this study. There was a significant difference between groups regarding severity of
symptoms (p = 0.002). The researchers suggested that, since the AP bands were effective
in this study, the potential savings in postoperative antinausea medications use would
warrant further research in AP band use for postoperative patients (Phillips & Gill, 1993).
AP was identified as a modality to help decrease the nausea and vomiting of
pregnancy in this randomized blind study (Belluomini, Litt, Lee, & Katz, 1994). Ninety
pregnant women less than 12 weeks gestation referred from midwife and physician
practices were randomly assigned to groups testing the effectiveness of AP. The
experimental group (n =30) was taught how to apply AP to the Neiguan point and the
control group (n =30) was taught to apply AP to a placebo point. The participants were
told not to apply AP during the first 3 days so that those days could be used as control.
50
The instrument used was the Rhodes index of nausea and vomiting. A Student's t test
was used for data analysis of differences between group means �th an ANOV A for
repeated measures of data over time. The reported scores for the experimental group
(PRE,M= 12.64, SD= 5.1 and POST,M= 8.69, SD= 5.0)were significantly lower than
the control group scores (PRE, M = 11.47, SD= 4.9 and POST, M = 10.03, SD= 4.6).
The researchers reported that both groups improved significantly over time (F1,ss = 21. 7,
p < 0. 000 I) but that the nausea in the experimental group improved significantly more
(F1,s& = 10.4,p < 0.0021). According to Belluomini et al. (1994), the use of AP was a
safe, low cost, and an easily learned technique that can decrease nausea in pregnancy.
Ho, Hseu, Tsai, and Lee (1996) researched the effect of AP bands on patients
experiencing nausea and vomiting after epidural morphine for post cesarean section pain
relief Participants were randomized into groups for this experimental study. AP bands
were applied to both wrists for participants enrolled in the experimental group (n = 30)
and placebo bands were applied to both wrists for participants in the control group
(n = 30) prior to spinal anesthesia. Data were collected by an independent
anesthesiologist who was not aware of group assignments. The data collected were vital
signs, pain severity, postoperative analgesic requirements, nausea, vomiting, retching,
respiratory rate, length of time wearing the bands, side effects of pruritus, dizziness,
herpes simplex labialis, and nausea and vomiting at 0, 5, 15, 30, 45 minutes, 1, 2, 4, 8,
12, 24, 36, and 48 hours after the epidural morphine. Data were reported as absolute
values or percentages. The incidence of nausea in the experimental group (3 % ) was
51
significantly less than the control group (43%) (p < 0.05) based on analysis with the
Student's t test. The researchers suggested that AP bands can reduce the incidence of
nausea and vomiting after cesarean section pain relief with morphine (Ho et al., 1996).
O'Brien, Relyea, and Taerum (1996) researched the use of AP in the treatment of
nausea during pregnancy. Of the women who completed the protocol (n = 149), 54 had
been assigned to the treatment group, 53 to the placebo group, and 54 to the control
group. AP bands were properly applied in the treatment group, applied over a non
treatment area for the placebo, and no AP bands were given to the control group.
Participants were given 13 copies of the Rhodes Inventory of Nausea and Vomiting to
record their symptoms every 12 hours at home. A research assistant called each
participant daily to record symptoms and to make sure that the symptoms were
appropriately assessed. Data were analyzed with an ANOV A of difference scores.
Between group differential effects were not discovered in this study (F = 4.64,
M squares = 6.55, df = 24, p = 0.98 for nausea scores). The researchers did not establish
the effectiveness of AP bands. Since the participants completed data collection every 12
hours, this data collection would be influenced by sleep/awake patterns or relief of nausea
while sleeping or in a supine position (O'Brien et al., 1996).
Concerns of the efficacy of anti emetic medications post laparoscopy was a
rationale for the research conducted by Harmon, Gardiner, Harrison, and Kelly (1999).
This randomized, double-blind study included 104 patients, 19 to 43 years old, receiving
standard anesthesia by different anesthetists. The experimental group (n=52) received the
52
AP bands in correct position on the right arm prior to anesthesia and the control group
(n = 52)., received AP bands placed on non AP points. The participants were evaluated in
the recovery room, 2 hours, and 24 hours after the operation for nausea ranks of none,
mild, moderate, or severe. The Student's t test was used to compare groups. Data were
reported as frequencies of nausea/vomiting complaints with the first 24 hours after the
laparoscopy. The experimental group reported 10 complaints of nausea/vomiting
compared with 22 in the control group. There was a significant reduction in nausea for
the experimental group (p = 0.02). The researchers suggested that AP bands can be used
as an effective treatment to decrease postoperative nausea/vomiting in postoperative
laparoscopy patients (Harmon et al., 1999).
Dibble, Chapman, Mack, and Shih (2000) explored the use of finger AP to
decrease nausea in women receiving chemotherapy for breast cancer. The researchers
used the Rhodes Inventory ofNausea, Vomiting, and Retching (INVR), a nausea
intensity scale, and the Chemotherapy Problem Checklist to assess nausea in 17 women
receiving the combination therapy of cyclophosphamide, methotrexate, and fluorouracil
or doxorubicin in an outpatient oncology clinic for treatment of breast cancer. The
participants completed the daily log each evening for 21 days. The experimental group
·· (11 = 8) was taught how to access and hold pressure to the P-6 and ST-36 AP points for
treatment of nausea and how to complete the daily log. The control group was taught
how to complete the daily log. Repeated measures ANOV A were used to analyze the
data. The overall nausea experience measured on the INVR was significantly less for the
53
RlllilElllall TIM91PI w nr
experimental group (F = 10.44, p < 0.01 ). Nausea intensity was less severe for the
experimental group (F= 5.255,p < 0.04). Analysis of the retrospective Chemotherapy
Problem Checklist, however, revealed no significant differences between the
experimental (M= 2.83, SD =1.6) and control (M= 3.00, SD= 0.58) groups of average
nausea symptoms experienced over the previous month of therapy. The researchers
suggested that AP might be useful in decreasing the nausea intensity for women receiving
chemotherapy for breast cancer (Dibble et al., 2000).
AP was explored as a complementary healing modality to decrease the incidence
of postoperative nausea and vomiting in a quasi-experimental study on patients
recovering from anesthesia (Windle, Borromeo, Robles, & Ilacio-Uy, 2001 ). Participants
(n = 157) in this study were divided into five groups. The randomly assigned groups
were: (a) AP bands with AP on both wrists (n = 29), (b) AP bands with acupressure on
one wrist (n = 34), (c) wristbands without AP on both wrists (n = 30), (d) wristband
without AP on one wrist (n = 35), (e) no wristband (n = 29). Analysis of incidence of
nausea based on retrospective chart audit on nurse's documentation and ANCOVA
revealed no significant differences between groups. The researchers suggested that
significant findings might be obtained with a larger sample size and longer patient
exposure to AP bands postoperative (Windle et al., 2001).
Therapeutic Touch
The Rogerian theory that human beings and the environment are energy fields
interacting mutually form the basis for TT (Krieger, 1987). According to Krieger, the
54
?"3
nurse's hands are used to assess imbalances in the energy field and then balance the field
to enable the patient's own healing processes to intervene. Egan (1998) attributed the
patient healing process to be a result of the intentional and specific interaction between
the healer's and patient's energy field to restore order and harmony to the energy pattern
of the patient.
TT has been examined in myriad research studies (Table 2); however, only the
following study that described its effect upon the relief of nausea was found in the
literature. According to Giasson and Bouchard (I 998), non contact TT significantly
increased the scores on the researcher-developed Well-Being Scale of persons with
tenninal cancer. Non contact TT was a process of energy exchange in which the nurse's
hands were used to re-pattern the human energy field. The components of the scale were
the subjective feelings of physical and emotional comfort that included absence of pain,
nausea, depression, and anxiety. The presence of activity, appetite, relaxation, and inner
peace were also assessed. The dependent variables were the subjective feelings of
physical and emotional comfort, and the independent variable was TT. The instrument
was a visual analog type horizontal scale with one line for each item of well-being
identified by the researcher. The reliability and validity were established by correlation
and coefficients prior to use with the study group.
Twenty adults with terminal cancer admitted to a palliative care unit served as
subjects for this experimental time-series research. The participants were randomly
assigned to either the experimental or control group. The experimental group received
55
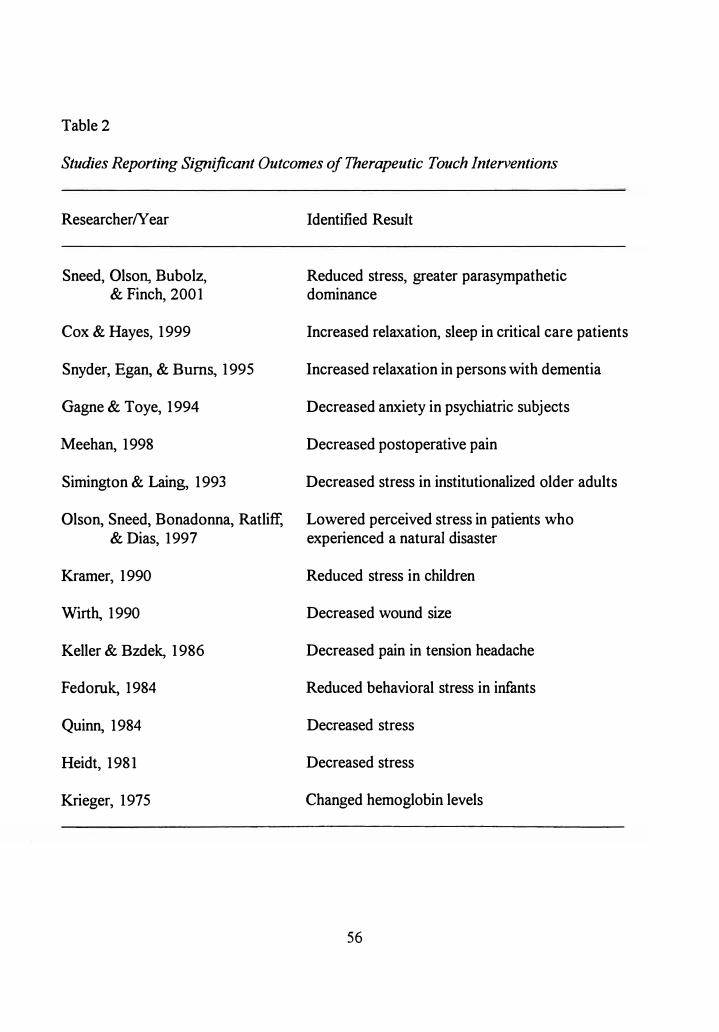
- - r ••
Table 2
Studies Reporting Significant Outcomes of Therapeutic Touch Interventions
ResearcherNear
Sneed, Olson, Bubolz, & Finch, 2001
Cox & Hayes, 1999
Snyder, Egan, & Burns, 1995
Gagne & Toye, 1994
Meehan, 1998
Simington & Laing, 1993
Olson, Sneed, Bonadonna, Ratliff, & Dias, 1997
Kramer, 1990
Wirth, 1990
Keller & Bzdek, 1986
F edoruk, 1984
Quinn, 1984
Heidt, 1981
Krieger, 1975
Identified Result
Reduced stress, greater parasympathetic dominance
Increased relaxation, sleep in critical care patients
Increased relaxation in persons with dementia
Decreased anxiety in psychiatric subjects
Decreased postoperative pain
Decreased stress in institutionalized older adults
Lowered perceived stress in patients who experienced a natural disaster
Reduced stress in children
Decreased wound size
Decreased pain in tension headache
Reduced behavioral stress in infants
Decreased stress
Decreased stress
Changed hemoglobin levels
56
TT treatments for 15-20 minutes one hour after analgesics. The control group underwent
rest periods for the same amount of time, and the researcher sat next to the participants
and completed mental mathematical problems to prevent any centering or energy
exchanges. No significant differences in groups emerged considering sociodemographics
and analgesic use based on chi-square and t tests. An ANOV A was used for data analysis
and indicated a significant interaction (F=l 1.89,p < 0.001). A significant increase
occurred in the well-being score of the experimental group (M = 1. 70, SD = 1.28) and a
decrease was found in the control group (M= 0.31, SD= 1.12). The experimental well
being scores increased significantly over time (F= 14.02,p < 0.001), and the control
group scores (F = 1 . 07, no p reported) decreased over time. Data were not reported
regarding nausea-specific results after TT. This study cannot be used to support the use
of TT to decrease nausea (Giasson & Bouchard, 1998).
The reported research on interventions for nausea to activate stimuli that can
relieve nausea included the use of AP bands, AP, and TT. The effectiveness of AP bands
has not been established by research. Riddled by attrition rates, small sample sizes, data
collection instruments lacking established reliability/validity statistics, incidental
inclusion in larger studies, and possible incorrect placement of the AP bands, results of
research on the use of AP bands remained controversial. The use of AP bands was
supported as an effective technique for use with patients who complain of postoperative
nausea and the nausea of pregnancy. No decrease in nausea was reported to justify the
use of AP bands for terminally ill patients. The effects were viewed as successful if some
57

nausea was relieved because the side effects of medications were avoided and a potential
decrease in health care costs would result if AP bands were effective. Further study will
need to be done to establish the effectiveness of the AP bands. The use of finger AP,
however, was found to be a safe, _low cost, and an easily learned technique that decreased
nausea in pregnancy and chemotherapy for breast cancer. The Rhodes INVR was used
for data collection in studies of finger AP. Further studies are indicated to investigate
other patients who would benefit from finger AP. The effectiveness of TT for use with
nausea patients has not been established. TT significantly increased the scores of well
being for terminal cancer patients but improvement in nausea could not be established.
Summary
This review of the literature explored the relationships between nausea and the
use of nursing touch. Nausea was described as a multifaceted problem resulting from
_ stress or a stressful event that often accompanies illness and also as a focal stimulus that
catches the patient's attention and energy. Future nausea research will require larger
sample sizes, more precise instruments for assessing, and outcome analyses to validate
patient responses to the multiple interventions needed for nausea relief.
Other techniques of use of stimuli to relieve nausea were reviewed. The use of
finger AP was found to be a safe, low cost, and easily learned technique that decreased
nausea in pregnancy and chemotherapy for breast cancer. Further studies are indicated to
investigate other patients who would benefit from finger AP. The effectiveness of TT for
use with nausea patients has not been established.
58
Touch, as a healing technique, has been documented in early human history.
Scientific rationale for touch techniques have been established and used to decrease or
relieve human distress. Registered nurses use touch as a focal stimulus that can enter into
the human adaptive system as input along with contextual and residual stimuli. Touch
was supported as a mode of caring communication but not as an intervention for nausea.
A need for further research was identified to establish a nursing model for development
of touch intervention that is patient-response specific.
59
CHAPTER3
PROCEDURE FOR COLLECTION AND TREATMENT OF DATA
An experimental two-group before and after design was used to determine the
effects of purposeful touch (PT) and no touch on nausea of patients who present in the
emergency center (EC) complaining of nausea as a primary or secondary complaint.
According to Huck and Cormier (1996), this type of design not only enabled the
researcher to investigate a cause and effect relationship but allowed rigor in exploring how
the independent variable affected the dependent variable. The experimental two-group
design with random assignments to groups reduced external variability due to
experimental error or biased treatment effects (Kirk, 1982). Participants in both groups
were asked to evaluate levels of nausea on a 100-millimeter (mm) scale as pretest and
posttest measures. The experimental group received PT, while those in the control group
did not receive PT. The independent variable of this study was PT, and the dependent
variable was nausea. Since the goal of research is efficiently to draw valid conclusions
about the effects of the independent variable, analysis of covariance and randomization
were used in this experimental study as ways to control for extraneous variables (Kirk,
1982).
60
Setting
The study was conducted in an EC of a private not-for-profit hospital. The large
medical center hospital functions as a teaching facility for a medical school in a
metropolitan area of the southeastern United States. The facility reported a total of 1,200
inpatient beds and 31,626 emergency visits in 2000. The hospital is an internationally
known referral center for many medical specialties.
The participants were assessed in the EC triage area (triage) by hospital personnel
and escorted into a treatment area. Staff nurses recruited the participants by asking if the
patients would like to be involved in the research study. The investigator approached the
participants, who had already agreed to be included in the study, in the EC treatment area
that consisted of rooms or cubicles with curtains or doors that allowed for patient privacy.
The patient remained· in this area until after emergent assessment, interventions, and
evaluations were completed and the patient was released from the EC either by admission
to the facility or discharged to home.
Population and Sample
The population of the study included all patients who presented to a large medical
center hospital EC with complaints of nausea. Data were collected from March 25, 2001
through June 3, 2001. The researcher collected data during afternoon and evening hours
on weekend days for 2 months of the study and then on consecutive days until data
collection was completed.
61
The study sample included a total of 140 patients who presented to the EC with
complaints of nausea. A power analysis determined that a sample size of 70 participants
per group was necessary to achieve a power size of .80, with an effect size of .35, and a
level of significance of0.05 (J. Cohen, 1988). The .35 effect size was based on previous
testing of the visual analog scales (Borjeson et al. 1996; Coppola, Yealy, & Leibold,
1996). If a mean nausea score was 10 points greater than the pre touch mean score, it
was considered important with a documented standard deviation of 29. The effect size
was then computed as .3 5.
Each of the two study groups included patients randomly assigned to either the
experimental or control group. Patients who met the following criteria were included in
the study: (a) arrived in the EC complaining of nausea without a history of chemotherapy,
radiation therapy, or current abdominal pathology, (b) were at least 18 years of age at the
time of data collection, ( c) were able to read, write, and speak English, and ( d) were
willing to participate in the study as indicated by signing the informed consent. All
persons meeting the criteria were asked to participate in the study. A random assignment
technique at the beginning of the study was used to assign participants to the experimental
or control group. A table of random numbers was used to select a group of 70 numbers
from a total count of 140. A toss of a coin then was used to assign control or
experimental group status to the selected numbers. The remaining random numbers were ·
assigned to the other group (Waltz, Strickland, & Lenz, 1991). The random assignment
was based on the order of patient presentation to the EC treatment area.
62
Protection of Human Subjects
Permission to conduct the study was obtained from the Human Subjects Review
Committee of Texas Woman's University (Appendix A). Agency permission was granted
for the hospital through The Institutional Review Board for Human Subjects Research for
Affiliated Hospitals (Appendix A). The guidelines for protection of human subjects were
followed. The study subjects were informed that participation was voluntary and that they
could withdraw from the study at any time (Appendix B). The subjects were told that
there would be no benefit to them if they agreed to participate in the study. They were
informed that the investigator was staying on the site to answer questions or concerns they
had. The results of the study, reported in group format only, were available on request to
the group. Subjects were informed that completion of the signed consent and the two
visual analog scales indicated their consent to participate in the study.
The subjects were informed that all information was confidential. Any data
collection forms were coded so that neither the subject's name nor the name of the
institution appeared on any of the forms or results of the study. A code number was
placed on the upper right comer of each instrument at the time of data collection so that
the results of the pretest and posttest data could be matched.
All data were kept in a locked cabinet during the data collection, and only the
investigator had access to the cabinet. The collected information was destroyed on
completion of the study to further insure confidentiality.
63
Instruments
Two instruments were used to collect data in this study. The first instrument was
the Demographic Data Tool (Appendix C). This instrument included the date of data
collection, assigned treatment group code, age, gender, ethnic origin, reason for EC visit,
current reactions to nausea, and history of nausea. The other instrument was the 100-mm
visual analog nausea scale (Appendix D).
Demographic Data Tool
The Demographic Data Tool (DDT) was used to determine attributes of the
sample of the study. Each component of the DDT was substantiated by research,
including the autonomic reactions and the history of nausea, as potential contributors to
individual variations of the threshold to nausea or confounding variables that could
influence the results of the study. The demographic variables of nausea as identified by
other researchers were also explored in this study to identify sample characteristics.
According to previous researchers, younger patients ( < 60) reported higher nausea
scores and reported nausea more often than older patients(> 60) (Dodd, Onishi, Dibble,
& Larson, 1996; Rub, Andrews, & Whitehead, 1992). M. Cohen, Duncan, DeBoer, and
Tweed ( 1994) found that being of a younger age contributed to the incidence of
postoperative nausea. Quinn, Brown, Wallace, and Asbury ( 1994) also reported a
significantly higher incidence of postoperative nausea in the younger age group. In
addition, Rub et al. identified a significant decrease in nausea with increasing age. Age
64
. i
was a contributing factor in complaints of nausea as a primary complaint and could be a
factor for patients' responses to medications. Since Rub et al. recruited from general
populations in Europe, age groupings were replicated so that significant differences could
be identified between ages in the gen�ral population and this EC study sample.
Since gender influences the frequency of nausea and patient responses to touch
(Porter, Redfern, Wilson-Barnett, & LeMay, 1986; Rub et al., 1992), it was included in
data collection to allow for generalization of the results. Mann ( 1998) reported that
emetic symptoms occur three times more often in women than men. Women who receive
chemotherapy and are younger than 50 are more likely to experience nausea and
anticipatory nausea than are women over 50 (Goodman, 1997). To determine if gender
was a factor for EC patients with nausea, gender was recorded on the DDT.
Barnett ( 1972) and Porter et al. (1986) noted cultural differences in response to
touch. Ethnic group information was included on the DDT to allow for analysis of data to
determine if significant differences existed between ethnic groups and if the convenience
sample was representative of the population at large to allow for generalization of the
findings. Since different cultures have different spacial norms (Barnett, 1972), the analysis
of ethnic groups also would allow identification of differing responses among the groups.
According to Hawthorn (1995), the onset and severity of nausea can vary greatly
based on the etiology. Therefore, the reason for the EC visit needed to be determined.
Patients with a history of nausea experience more nausea with chemotherapy, radiation
therapy, or in the postoperative situation (Hinojosa, 1992; Redd, Dadds, Futterman,
65
Taylor, & Bovbjerg, 1993). According to Rhodes (1990), nausea is an expected symptom
of some specific pathophysiologic conditions. Other researchers identified multiple causes
of nausea, such as: after traumatic injuries, with gastrointestinal infections, headaches,
transient ischemic attacks, anoxia as a result of respiratory or cardiovascular disease,
metabolic disorders, burns, overdoses, and alcohol poisoning (Brechenridge, Larry, &
Mazzaferri, 1996; Grapp, Savage, & Hall, 1996; Hawthorn, 1995; Hepburn et al., 1991;
Rhodes, 1990). Patients with these types of conditions commonly present to the EC with
nausea. The influence of the chief complaint of nausea was explored as it related to the
use of PT.
Other sympathetic symptoms of nausea influenced the perceived distress from
nausea (Rhodes, McDaniel, & Johnson, 1995). The descriptors of effects of nausea,
identified on the DDT, were based upon the factors identified by Muth, Stem, Thayer, and
Koch (1996). According to Redd et al. (1993), classical conditioning can contribute to
the development of nausea even if the patient was distant from the associated treatment.
For example, a previous history of motion sickness increased the risk for developing
postoperative nausea and vomiting (Mann, 1998). The history factors to consider, listed
on the DDT, were extrapolated from Thompson (1999) and Hawthorn (1995). Data were
collected to discover if a history of nausea would influence the effect of PT.
66
Visual Analog Nausea Scale (VANS)
The I 00-mm visual analog nausea scale (VANS) used in this study to determine
the effects of touch on the severity of nausea was designed to measure the severity of
nausea, took only a few seconds to complete, and was used in an EC setting where nausea
was situational and nota recurring symptom. According to Contanch (1984), the VANS
is an easy way to quantify the subjective symptoms of patients. The VANS is a vertical
scale measuring exactly 100 mm, with zero at the lowest point and I 00 at the top of the
scale. Markings are located along the scale at 10-mm increments without labels. Zero is
labeled as "none" and I 00 as the "nausea as bad as it can possibly get." The VANS
measured both before and after purposeful touch or no touch on two separate original
sheets of the instrument. Each VANS was printed as an original to avoid the accidental
enlargement of the scale commonly experienced with duplicating machines.
Validity and Reliability
The DDT was designed as an interview instrument to be completed only by the
researcher. The DDT allowed for direct reliable answers since potential responses were
read for them, the researcher retained the ability to interpret the answers, and the
categories limited the potential responses to established variables (Fowler, 1984). The
questions progressed from general to specific with less distressing questions at the
beginning and more specific nausea questions at the end since there is a cognitive
component to nausea and the researcher did not wish to increase the discomfort for the
67
lli RETTT H
patient at the beginning of data collection (Bateson, 1984). Content validity of the DDT
was established by using language to describe nausea from the literature, investigator
observations in the EC, expert review by a three nurse specialists in oncology actively
involved in treatment of nausea, and expert review by two nurse researchers with
experience in instrument development (Waltz et al., 1991). The reliability of the DDT was
established during a pilot study of 20 patients. Since only one researcher was involved in
the intervention, interrater reliability was not required. The amount of time needed to
complete the DDT was established so that the EC staff and participants of the study could
be assured that the patient would not be detained longer than IO minutes.
Construct validity was established by correlation of the visual analog scale with
other scales for the measurement of sensations (Waltz et al., 1991). According to
Borjeson and associates ( 1996), there was a good concordance between the VANS and a
verbal category scale for complaints of nausea among patients receiving chemotherapy.
The researchers also suggested that the VANS. would be best used to detect small but
significant changes in a retest situation after interventions (Borjeson et al., 1996). Gift
( 1989) indicated that concurrent validity of the visual analog scale was established by use
in other studies on sensations of pain, depression, and dyspnea. Gift also reported
discriminate validity for the use of this scale in studies of quality of life and degrees of
airway obstruction.
The reliability of the VANS, according to Gift (1989) and Waltz et al. (1991), was
established in the test-retest method by demonstrating moderate to strong correlations.
68
Higher test-retest reliability coefficients (r = .92) were notedwhen the visual analog scale
was used to retest after 1 to 2 hours of the first test to evaluate a group of cancer
outpatients with nausea (Padilla et al., 1983). Fetting, Grochow, Folstein, Ettinger, and
Colvin (1982) reported a test/retest reliability of .83 on the VANS based on 27 pairs of
scores. Other forms of reliability testing have not been completed on the VANS. Since
literature establishing reliability for the use of the VANS with nausea patients in the EC
was not found, a pilot study was needed to pretest the applicability of the VANS for this
research.
Data Collection
Human subjects approval for the identified facility was obtained. All patients
meeting the study selection criteria were asked to participate in the study after they were
placed in the treatment area where privacy could be provided. A random assignment
· technique at the beginning of the study was used to assign participants to the experimental
or control group. Data collection forms were coded before the study was implemented.
The forms were selected and assigned in order based on the progression of patient
presentation to the EC treatment areas. The DDT and pre coded VANS (pretest and
posttest) were completed on each identified subject.
Each person agreeing to participate was informed that the purpose of the study
was to determine if nurses can decrease uncomfortable feelings of nausea by using touch.
The participants were then asked to read and sign the consent (Appendix B). After
69
obtaining consent, the researcher completed the DDT from information collected in triage
as documented on the patient chart and by interview. The patient was asked to complete
the pretest VANS while in a sitting position.
Patients included in the experimental group received a 5-second, bimanual touch to
the patient's shoulder between the midclavicle and the lateral surface of the neck and a
handshake position. The touch to the shoulder area stimulated sensory neurons of the
transverse cervical nerve and the ·supraclavicular nerves of the superficial cervical plexus.
The handshake position stimulated the superficial branch of the radial, the proper palmar
digital branches and the palmar branches of the median, and the superficial and dorsal
branches of the ulnar nerves of the brachia! plexus. The researcher remained in the
patient's room and stood 4 to 5 feet away from the foot of the patient's stretcher, while
the patient remained silent, napped, talked with their family, EC personnel, or the
researcher. Any conversations that occurred while the researcher was in the patient
examination room between completing the pretest, intervention, and posttest were patient
initiated. The patient was asked to complete the posttest VANS 2 minutes after the touch
in a sitting position. After the posttest VANS was marked, the patients were informed
that their participation was completed, asked if they had any questions, told that if they
had any questions later that the researcher would be in the area until discharge, and shown
the telephone number located on their copy of the consent form for questions after
discharge.
70
For the patients in the control group, the investigator stayed in the patient's room
for 2 minutes and stood 4 to 5 feet away from the foot of the patient's stretcher, while the
patient remain.ed silent, napped, talked with family members, EC personnel, or the
researcher. Any conversations that occurred while the researcher was in the patient
examination room between completing the pretest and posttest were patient initiated. The
patient was asked to complete the posttest VANS 2 minutes after the pretest VANS was
completed in a sitting position. After the posttest VANS was marked, the patients were
informed that the participation was completed, asked if they had questions, told that if
they had any questions later that the researcher would be in the area until discharge, and
shown the telephone number located on their copy of the consent form for questions after
discharge. If any of the participants were not able to complete the study pretest, posttest,
or asked to withdraw from the study, the collected data were not included in the data
analysis.
Pilot Study
Prior to data collection for the research, a pilot study was conducted to refine the
study design and establish reliability of the instruments for the proposed study. The
convenience sample consisted of 20 subjects randomly assigned to an experimental or
control group. Data for the pilot study were collected over one month in the EC
designated for the research.
71
An experimental two-group before and after design was used to determine the
effects of purposeful touch (PT) and no touch on the level of nausea of patients who
present in the emergency center (EC) of a private not-for-profit hospital complaining of
nausea as a primary or secondary complaint. The population of the study included all
patients who presented to EC with complaints of nausea. Data for the pilot study were
collected from March 25, 2001 through April 28, 2001 ·during high traffic times for the
EC. The sample size of20 was determined, based on approximately 15% of the overall
estimated sample size of 140 for the research. The guidelines for protection of human
subjects were followed and human subjects approval for the identified facility was
obtained.
Data collection forms were coded before the researcher approached the
participants. The forms were selected and assigned in order based on the progression of
patient presentation to the EC treatment areas. The DDT and pre coded VANS .(two
forms marked pretest and posttest) were completed on each identified subject. After
obtaining consent, the researcher completed the DDT from information collected in triage
documented on the patient chart and by interview. Patients included in the experimental
group received a 5-second, bimanual touch to the patient's shoulder between the
midclavicle and the lateral surface of the neck and the handshake position. The researcher
remained in the patient room, and stood 4 to 5 feet away from the foot of the patient's
stretcher, while the patient remained silent, napped, talked with their family, EC personnel,
or the researcher. The patient was asked to complete the posttest VANS 2 minutes after
72
PT in a sitting position. For the patients in the control group, the investigator stayed in
the patient's room for 2 minutes and stood 4 to 5 feet away from the foot of the patient's
.stretcher, while the patient remained silent, napped, talked with family members, EC
personnel, or the researcher. The patient was asked to complete the posttest VANS 2
minutes after the pretest VANS was completed in a sitting position.
The instruments for data collection and analysis were the DDT and the I 00-rnm
vertical visual analog nausea scale. The DDT contained the date of data collection,
assigned treatment group code, age, gender, ethnic origin, reason for EC visit, current
reactions to nausea, and history of nausea. Assessment data listed on the DDT were
obtained by the literature review. Content validity of the DDT was established by a
review by three oncology nurse specialists. lnterrater reliability was not established for
this instrument since the instrument was completed by the researcher only. Reliability and
validity for the VANS was established by previous research.
A total of 20 patients were included in the pilot study. Eleven of the patients were
included in the experimental group and 9 were in the control group based upon the
random assignment technique established for the proposed research. The participants
required more indepth information on how to complete the VANS than expected. Many
of the participants wanted to mark the level with an "X'' or a check mark instead of a
horizontal line. Ink pens were not used on the VANS because of the inconsistency of ink
flow for the marks. Newly sharpened pencils were provided for each participant and
discarded after each participant completed the posttouch VANS.
73
An analysis of covariance was used to establish adequacy of the covariate of
pretouch. The pretouch scores demonstrated adequacy as comparison data with a
significance of (F= 43.699,p < 0.0005). Each participant responded to the questions
regarding reactions and history of nausea. However, some of the terms were confusing to
the respondents. For example, the term palpitations was changed to "Any changes in your
heart beat?" during the interview. The pilot allowed for feedback into the script of the
research and led to improved modalities for communication with the study groups prior to
proceeding with the research. An anecdotal finding as a result of this pilot study was that ·
some staff nurses recruited more patients than others. More orientation sessions were
conducted before beginning the research to address concerns about recruiting patients, and
each triage nurs_e and EC physician was reoriented to the study before recruiting began
each shift.
Treatment of Data
To define the characteristics or attributes of the participants of this study,
demographic data were collected. The variables of gender, ethnic origin, reason for EC
visit, current reactions to nausea, and history of nausea were reported as frequencies and
percentages of nominal data. The age of the participants was reported as frequencies,
median, range, and percentages of resulting ordinal data. Once the demographics were
analyzed, the results of the study were applied to the groups identified (Polit & Hungler,
(1995).
74
The analysis of covariance (ANCOVA), an inferential statistical method, was used
to analyze data obtained from the visual analog nausea scale (VANS). According to
Pedhazur and Schmelkin (1991), the ANCOVA is the appropriate analysis for the
pretest/posttest, treatment/control design, where the pretest is treated as a covariate. The
ANCOV A enables a researcher to decrease the experimental error and to remove potential
sources of bias from the experimental effects (Kirk, 1982). The data were ratio level
based on a ruler measurement. The ruler was aligned along the central vertical line with
the zero of the ruler placed at the bottom of the scale designated by zero or no nausea and
the measurement was made at the bottoms of the marks made by the participants on the
VANS (Bums & Grove, 1997). The level of significance was set atp = 0.05.
Summary
An experimental study with a pretest and posttest design with randomization of
groups was conducted to determine the effectiveness of touch on decrease in nausea
scores. There was a total of 140 subjects with 70 participants in each of the two groups.
The independent variable was purposeful touch, and the dependent variable was nausea.
A DDT and visual analog nausea scale (VANS) were used to collect data on nausea.
Descriptive statistics and an ANCOVA were used to analyze the data from this study.
75
CHAPTER4
ANALYSIS OF DATA
The purpose of this experimental study was to determine if purposeful touch (PT)
applied to specific nerve pathways would decrease nausea in patients who present to an
emergency center (EC) with nausea as a primary or secondary complaint. This study with
a pretest and posttest design and random group assignments was conducted to determine
the effectiveness of touch on nausea. There was a total of 140 subjects with 70
participants in each of the two groups. The experimental group received PT (n = 70) and
the control group did not receive PT (n = 70). The independent variable was purposeful
touch, and the dependent variable was nausea. Both study groups were compared based
on demographics and study findings. Frequencies and percentages were performed on the
variables of gender, ethnic origin, reason for EC visit, reactions to nausea, and history of
nausea. Ages were reported as frequencies, median, range and percentages of the sample.
The analysis of covariance (ANCOVA), an inferential statistical method, was used to
analyze pretouch as the covariate, and experimental/control group data were recorded by
each participant on the visual analog nausea scale (VANS).
76
Description of Sample
Analysis of demographic data was completed to allow for comparisons and
generalization of the study results. The data reported was nominal and ordinal, so
statistics are reported as frequencies and percentages. The scores of pretouch and
posttouch associated with each demographic variable are reported as means and standard
deviations. The following data on age, gender, ethnic origin, reason for the EC visit,
symptoms, and history of nausea were described and used to compare the sample
characteristics between the experimental and control groups.
Age
This study sample consisted of 140 patients between the ages of 18 and greater
than 60. Of these patients, 24% were between the ages of 18-30, 50% between the ages
of 31-60, and 25. 7% greater than 60 years of age. The median range age group was
between the ages of 31-60. As shown in Table 3, the experimental group had more
(n = 20) in the greater than 60 age group and the control group had more (n = 20) in the
18-30 age group. The PT pre and post intervention VANS scores are summarized by age
on Table 3. Since there were lower reported pretouch nausea scores in the greater than
60 group, an a posteriori analysis of variance was completed to determine significance
between age groups. There were no significant differences between age in the pretouch or
posttouch groups even with the > 60 age range reporting less nausea prior to the
intervention.
77
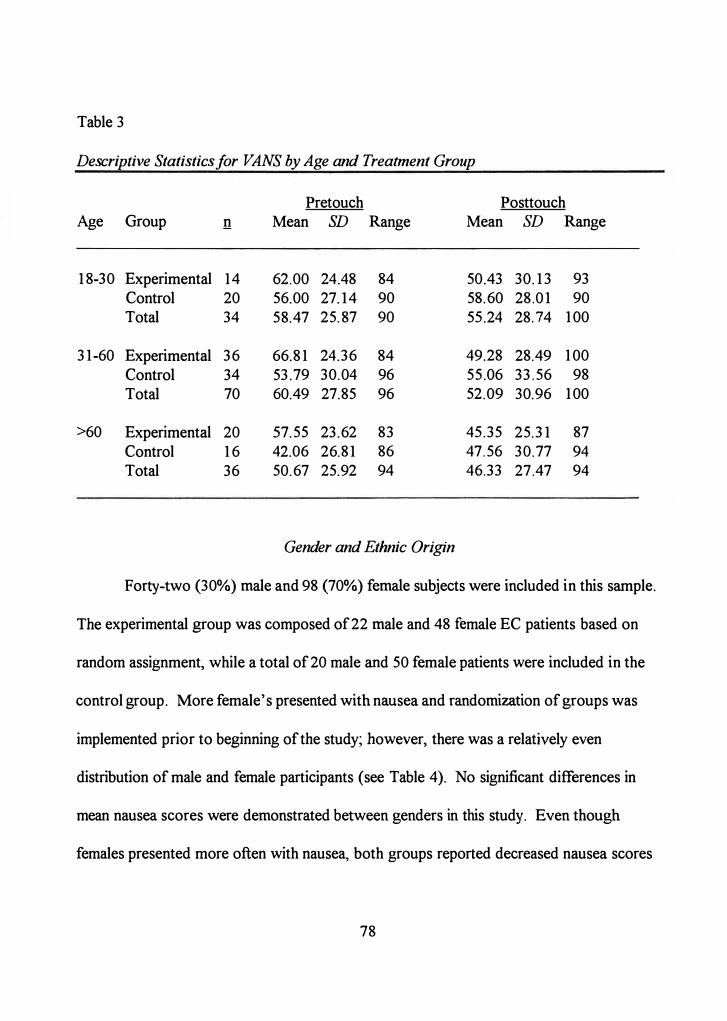
Table 3
Descriptive Statistics for ·VANS by Age and Treatment Group
Age Group !!
18-30 Experimental 14Control 20 Total 34
31-60 Experimental 36Control 34 Total 70
>60 Experimental 20 Control 16 Total 36
Pretouch Mean SD Range
62.00 24.48 84 56.00 27.14 90 58.47 25.87 90
66.81 24.36 84 53.79 30.04 96 60.49 27.85 96
57.55 23.62 83 42.06 26.81 86 50.67 25.92 94
Gender and Ethnic Origin
Posttouch Mean SD Range
50.43 30.13 93 58.60 28.01 90 55.24 28.74 100
49.28 28.49 100 55.06 33.56 98 52.09 30.96 100
45.35 25.31 87 47.56 30.77 94 46.33 27.47 94
Forty-two (30%) male and 98 (70%) female subjects were included in this sample.
The experimental group was composed of 22 male and 48 female EC patients based on
random assignment, while a total of 20 male and 50 female patients were included in the
control group. More female's presented with nausea and randomization of groups was
implemented prior to beginning of the study; however, there was a relatively even
distribution of male and female participants (see Table 4). No significant differences in
mean nausea scores were demonstrated between genders in this study. Even though
females presented more often with nausea, both groups reported decreased nausea scores
78
with PT ( male, decrease of mean scores = 15 .13 and female, decrease of mean
scores = .. 14.66).
The subjects included in this study consisted of 68 (48.6%) White, 58 (41.4%)
Black, JO (7.1%) Hispanic, and 4 (2.9%) other or Asian-American participants. The
distribution of those who received PT (experimental group) was 40 (58%) White, 27
(39%) Black, and 3 (4%) Hispanic participants. The control group participants not
receiving PT were composed of 28 (40%) Whites, 31 (44%) Blacks, 7 (10%) Hispanics,
and 4 (2.9%) other or Asian-Americans. PT used in_this study was applied to locations
without negative personal or cultural connotations. Even though different cultures have
different spacial norms (Barnett, 1972), no significant differences in posttouch scores were
noted between the groups (see Table 4).
Reason for EC Visit
The primary reasons for visiting· the EC included the most common complaint. of
79 (56.4%) gastrointestinal symptoms of vomiting, nausea, or pain, 23 (16.4%) headache,
and 13 (9.3%) with cardiac complaints of chest pain or congestive heart failure. These
data were obtained from the patient triage record (see Table 5). Less common reasons
were respir�tory, trauma, cerebrovascular, and other.
Symptoms Experienced with Nausea
The symptoms experienced with this episode of nausea were explored and
re�orded as reported by the participants. Many participants reported more than one
79
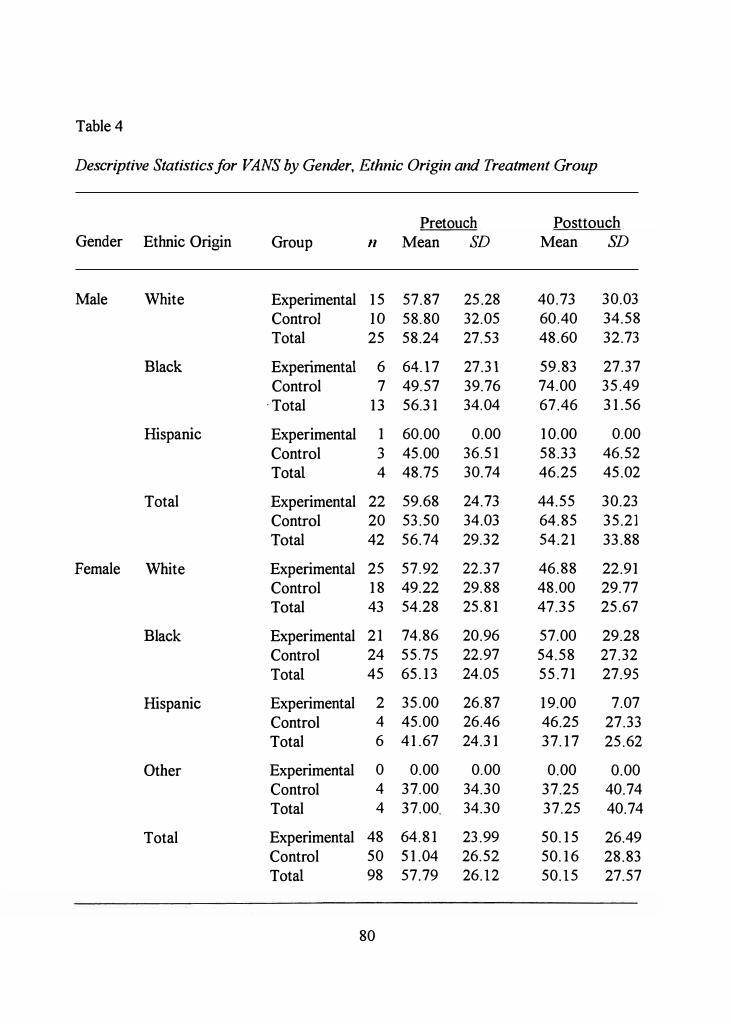
Table 4
Descriptive Statistics for VANS by Gender, Ethnic Origin and Treatment Group
Pretouch Posttouch Gender Ethnic Origin Group 11 Mean SD Mean SD
Male White Experimental 15 57.87 25.28 40.73 30.03
Contra] 10 58.80 32.05 60.40 34.58
I Total 25 58.24 27.53 48.60 32.73
Black Experimental 6 64.17 27.31 59.83 27.37
Control 7 49.57 39.76 74.00 35.49
· Total 13 56.31 34.04 67.46 31.56
Hispanic Experimental 1 60.00 0.00 10.00 0.00
Control 3 45.00 36.51 58.33 46.52
Total 4 48.75 30.74 46.25 45.02
Total Experimental 22 59.68 24.73 44.55 30.23
Control 20 53.50 34.03 64.85 35.21
Total 42 56.74 29.32 54.21 33.88
Female White Experimental 25 57.92 22.37 46.88 22.91
Control 18 49.22 29.88 48.00 29.77
Total 43 54.28 25.81 47.35 25.67
Black Experimental 21 74.86 20.96 57.00 29.28
Control 24 55.75 22.97 54.58 27.32
Total 45 65.13 24.05 55.71 27.95
Hispanic Experimental 2 35.00 26.87 19.00 7.07
Control 4 45.00 26.46 46.25 27.33
Total 6 41.67 24.31 37.17 25.62
Other Experimental 0 0.00 0.00 0.00 0.00
Control 4 37.00 34.30 37.25 40.74
Total 4 37.00. 34.30 37.25 40.74
Total Experimental 48 64.81 23.99 50.15 26.49
Control 50 51.04 26.52 50.16 28.83
Total 98 57.79 26.12 50.15 27.57
80
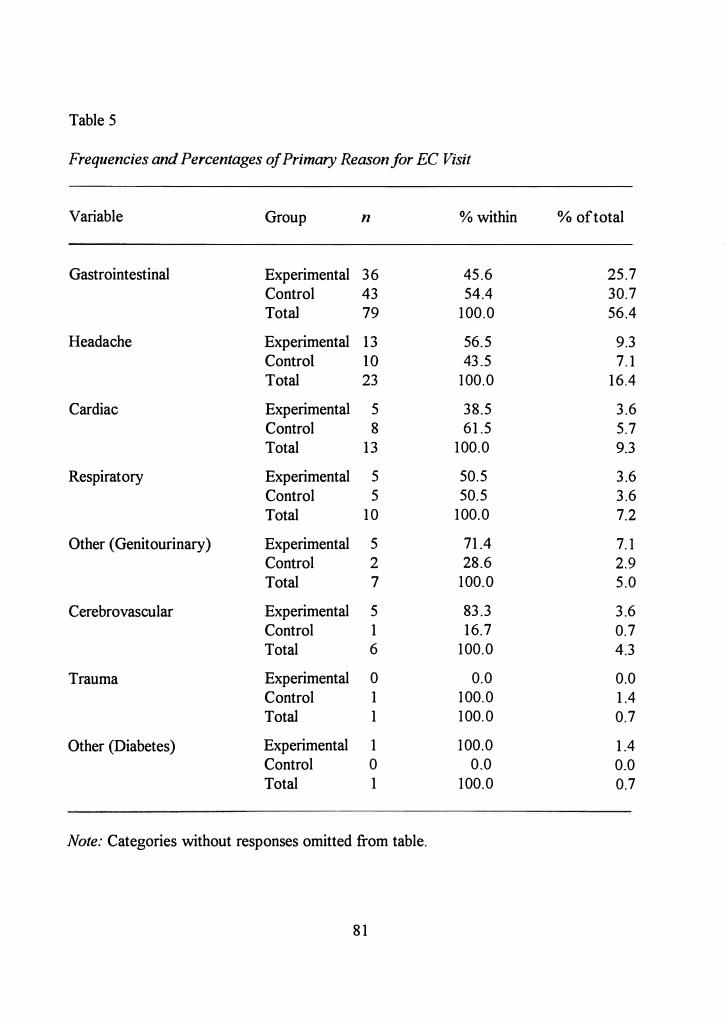
Table 5
Frequencies and Percentages of Primary Reason for EC Visit
Variable Group n % within
Gastrointestinal Experimental 36 45.6 Control 43 54.4 Total 79 100.0
Headache Experimental 13 56.5 Control 10 43.5 Total 23 100.0
Cardiac Experimental 5 38.5 Control 8 61.5 Total 13 100.0
Respiratory Experimental 5 50.5 Control 5 50.5 Total 10 100.0
Other (Genitourinary) Experimental 5 71.4 Control 2 28.6 Total 7 100.0
Cerebrovascular Experimental 5 83.3 Control 1 16.7 Total 6 100.0
Trauma Experimental 0 0.0 Control 1 100.0 Total 1 100.0
Other (Diabetes) Experimental 1 100.0 Control 0 0.0 Total 1 100.0
Note: Categories without responses omitted from table.
81
% of total
25.7 30.7 56.4
9.3 7.1
16.4
3.6 5.7 9.3
3.6 3.6 7.2
7.1 2.9 5.0
3.6 0.7 4.3
0.0 1.4 0.7
1.4 0.0 0.7
additional symptom; therefore, all symptoms were recorded (see Table 6). Most
participants reported accompanying symptoms of weakness, dizziness, flushed feeling,
diaphoresis, anxiety, changes in respirations, palpitations, and pain. The most common
symptom experienced with nausea was the feeling of weakness (n = 70, 50%).
History of Nausea
Data were collected to discover if a previous experience of nausea would negate
the effect of PT. The study participants reported pain (n = 63, 45%), indigestion (n = 56,
40%), and odors (n = 55, 39.3%) to be the most common stimuli that caused nausea in the
past. Other causes of reported nausea were: (a) pregnancy (11 = 50, 35. 7%), (b) general
anesthesia from surgical procedures in the past (n = 39, 27.9%), (c) motion sickness
(n = 35, 25.0%), (d) medications (n = 35, 25.0%), (e) constipation (n = 31, 22.1 %),
(f) repulsive sights (n = 29, 20.7%), (g) with dysphagia (n = 24, 17.1%), and
(h) associated with thoughts of vomiting (n = IO, 7.1%). Six (4%) patients reported no
history of nausea. Although there were no significant differences between groups and
relief of nausea, the patients who reported a history of nausea with pain evidenced the
greatest mean difference in nausea scores (experimental group M = 5.00, control group
M = 4.00). Patients with a history of motion sickness reported the lowest mean difference
in nausea scores ( experimental group M = 0.30, control group M = 0.20).
82
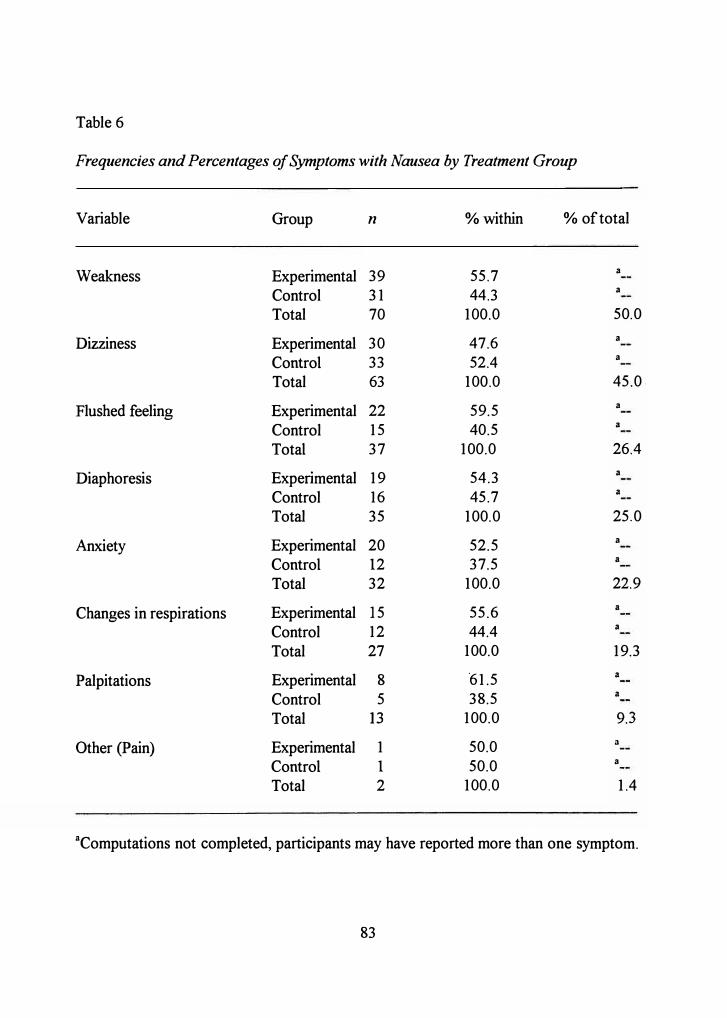
Table 6
Frequencies and Percentages of Symptoms with Nausea by Treatment Group
Variable Group n % within % of total
Weakness Experimental 39 55.7 a
Control 31 44.3 a
Total 70 100.0 50.0
Dizziness Experimental 30 47.6 a
Control 33 52.4 a
Total 63 100.0 45.0
Flushed feeling Experimental 22 59.5 a
Control 15 40.5 a
Total 37 100.0 26.4
Diaphoresis Experimental 19 54.3 a
Control 16 45.7 a
Total 35 100.0 25.0
Anxiety Experimental 20 52.5 a
Control 12 37.5 a
Total 32 100.0 22.9
Changes in respirations Experimental 15 55.6 a
Control 12 44.4 a
Total 27 100.0 19.3
Palpitations Experimental 8 '61.5 a
Control 5 38.5 a
Total 13 100.0 9.3
Other (Pain) Experimental 1 50.0 a
Control 1 50.0 a
Total 2 100.0 1.4
aComputations not completed, participants may have reported more than one symptom.
83
Findings
The hypothesis for this research study was:
The mean nausea intensity score among emergency center patients receiving
purposeful touch to alter their perceptual field will be significantly lower than the
mean nausea intensity score among the emergency center patients not receiving
purposeful touch to alter their perceptual field.
The analysis of covariance(ANCOVA), an inferential statistical method, was used to
analyze pretouch as the covariate and experimentaVcontrol group data recorded on the
visual analog nausea scale (VANS) as the dependent variable.
The level of nausea was assessed on patients pre and post intervention during one
EC visit. The scatter plot in Figure 1 illustrates the distribution.
The mean post intervention scores and standard deviations supported the findings
in that the experimental group mean (48.39) and standard deviation (27.62) were lower
than the control group (M= 54.36 and SD= 31.25) (see Table 7). The experimental
group reported higher pretouch scores than the control group, however. This finding can
be attributed to the increased numbers of patients enrolled in this study with
gastrointestinal complaints of nausea, vomiting, and pain.
The participants in this study also reported some greater differences in scores if
they experienced nausea with pain in the past. Further analysis revealed that the
participants who reported nausea greater than 7 5 on the pretouch scores from the
experimental group were 72% female, between the ages of 31-60 ( 61 % ) who reported
84
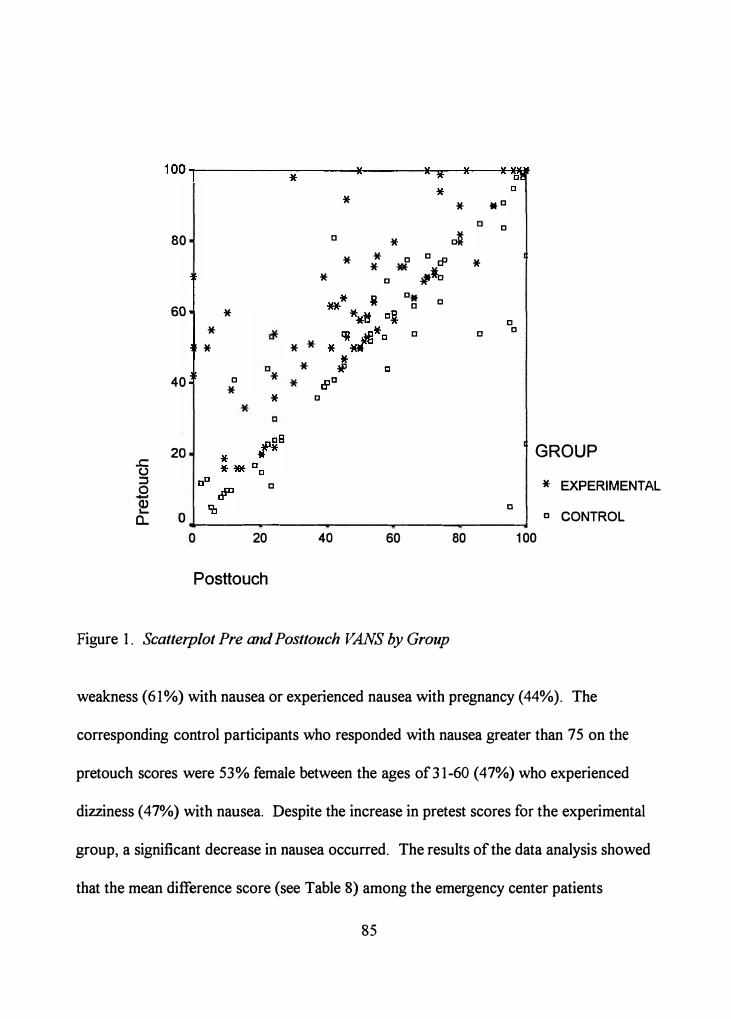
.c (.) :::, 0
80 a
60
40
20
* *
*
D *
* *
*
*
* a
C
*
*
* * D
* cl* D Ccfl * *
D W .-1o D*
D
a
C
C
D
C D
D
GROUP
* EXPERIMENTAL
D CONTROL � a. 0
---------...------------------...----.1
20 40 60 80 100
Posttouch
Figure 1. Scatterplot Pre and Posttouch VANS by Group
weakness (61%) with nausea or experienced nausea with pregnancy (44%). The
corresponding control participants who responded with nausea greater than 7 5 on the
pretouch scores were 53% female between the ages of31-60 (47%) who experienced
dizziness ( 4 7%) with nausea. Despite the increase in pretest scores for the experimental
group, a significant decrease in nausea occurred. The results of the data analysis showed
that the mean difference score (see Table 8) among the emergency center patients
85
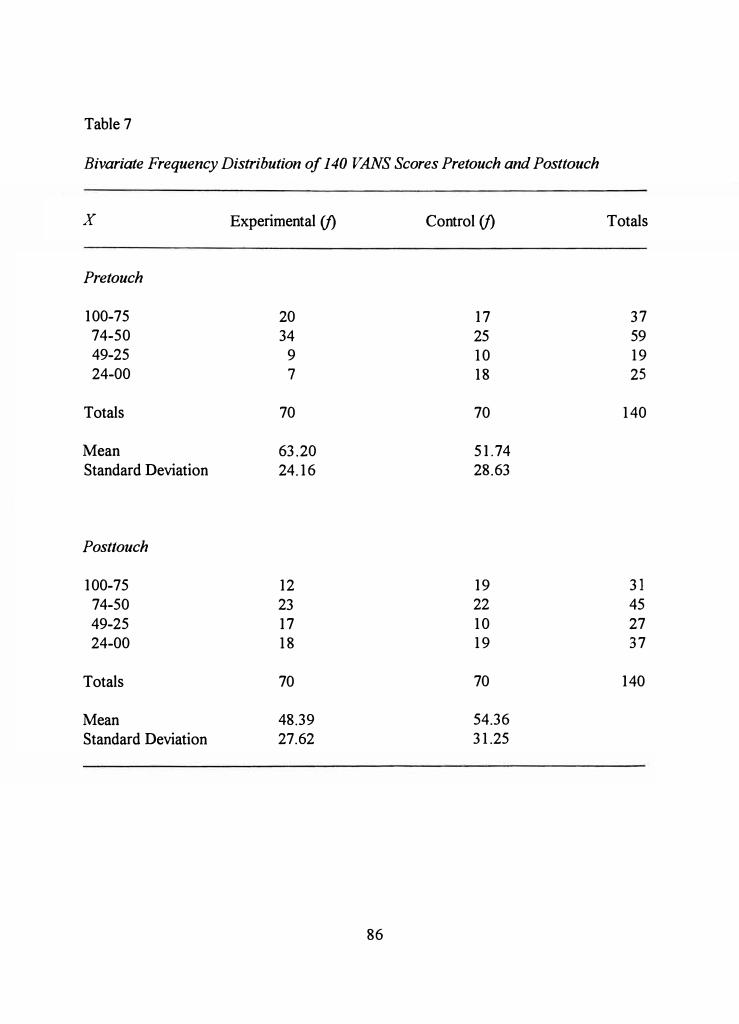
Table 7
Bivariate Frequency Distribution of 140 VANS Scores Pretouch and Posttouch
X Experimental (f) Control (f) Totals
Pretouch
100-75 20 17 37 74-50 34 25 59 49-25 9 10 19 24-00 7 18 25
Totals 70 70 140
Mean 63.20 51.74 Standard Deviation 24.16 28.63
Posttouch
100-75 12 19 31
74-50 23 22 45
49-25 17 10 27 24-00 18 19 37
Totals 70 70 140
Mean 48.39 54.36
Standard Deviation 27.62 31.25
86
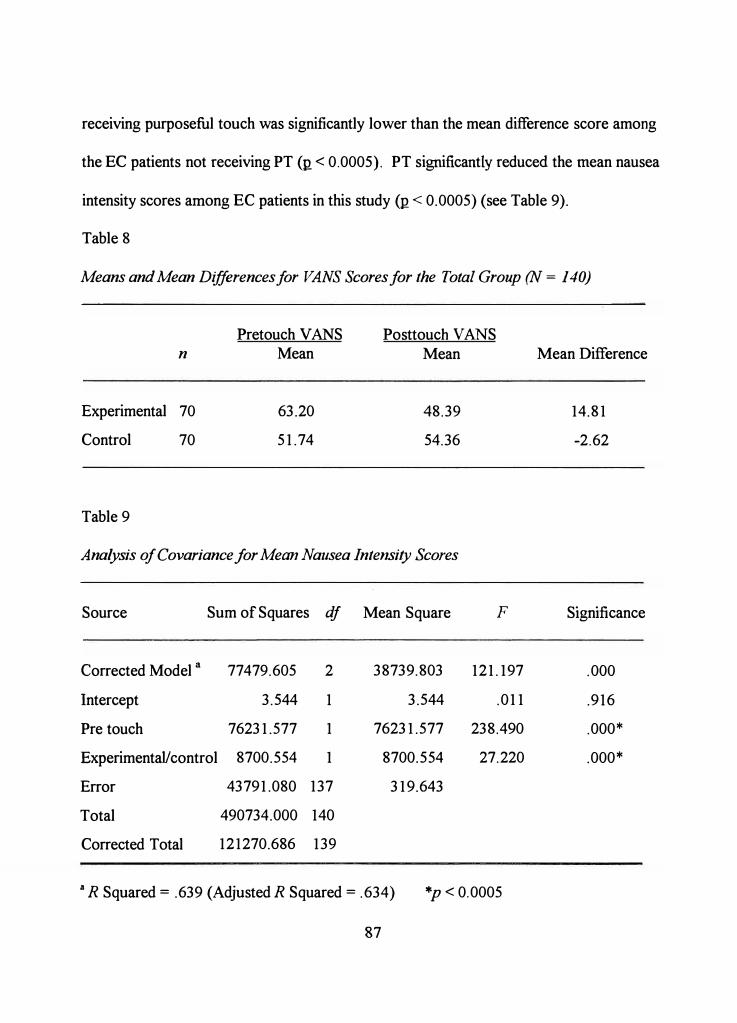
receiving purposeful touch was significantly lower than the mean difference score among
the EC patients not receiving PT (ti< 0.0005). PT significantly reduced the mean nausea
intensity scores among EC patients in this study (R < 0.0005) (see Table 9).
Table 8
Means and Mean Differences for VANS Scores for the Total Group (N = 140)
n
Experimental 70
Control 70
Table 9
Pretouch VANS Mean
63.20
51.74
Posttouch VANS Mean
48.39
54.36
Analysis of Covariance for Mean Nausea Intensity Scores
Source
Corrected Model a
Intercept
Pre touch
Sum of Squares df Mean Square
77479.605 2 38739.803
3.544 1 3.544
76231.577 1 76231.577
Experimental/ control 8700.554 1 8700.554
Error 43791.080 137 319.643
Total 490734.000 140
Corrected Total 121270.686 139
F
121.197
.011
238.490
27.220
., R Squared= .639 (Adjusted R Squared= .634) *p < 0.0005
87
Mean Difference
14.81
-2.62
Significance
.000
.916
.000*
.000*
Summary of Findings
The level of nausea was assessed on patients presenting to the EC complaining of
nausea as eith�r a primary or secondary complaint. The effects of PT were evaluated in
measurements of nausea based on the VANS. Measurements pre and post intervention
were completed on the experimental group receiving PT and the control group not
receiving it. Findings indicated that the mean nausea intensity score among the EC
patients receiving purposeful touch were significantly lower than the mean nausea ·intensity
score among the EC patients not receiving PT. This finding indicated a decrease in nausea
among participants who received PT.
88
CHAPTERS
SUMMARY OF THE STUDY
This study was designed to test the influence of purposeful touch (PT) on nausea
relief in patients who presented with nausea as a primary or secondary complaint in an
emergency center (EC). The Demographic Data Tool was used to determine attributes of
the sample of the study to allow for comparison between these and other research sample
characteristics. A vertical visual analog nausea scale (VANS) was used to measure nausea
between two randomly assigned groups of patients before and after PT or no PT. The
study is summarized, the findings are discussed, conclusions and implications are
summarized, and recommendations for future research are presented.
Summaiy
An experimental two-group before and after design was used to determine the
effects of PT and no touch on the nausea of patients who presented in the EC complaining
of nausea as a primaiy or secondaty complaint. The hypothesis for this study was:
The mean nausea intensity score among emergency center patients receiving
purposeful touch to alter their perceptual field will be significantly lower than the
mean nausea intensity score among the emergency center patients not receiving
purposeful touch to alter their perceptual field.
89
The study sample included a total of 140 patients who presented to the EC with
complaints of nausea. Each of the two study groups included 70 patients randomly
assigned to either the experimental or control group. The random assignment was based
on the order of patient presentation to the EC treatment area. The first 70 numbers
chosen were assigned as control or experimental based on the toss of a coin (heads as
experimental, tails as control). The remaining 70 random numbers were assigned control
or experimental by default. The numbers were then printed on two individualized original
VANS instruments for each participant and coded with the number assigned, pre- or
posttest, and the group designation as A ( control) or B ( experimental). The results of the
randomization were equal numbers in each group without duplicate numbers.
Participants included in the experimental group received a 5-second� bimanual
touch measured on the EC treatment room wall clocks. The touch was applied half way
between the shoulder and neck and a handshake to the dominant hand. Two minutes after
the touch, the patient was asked to complete the posttest visual analog nausea scale
(VANS), an instrument designed to measure the severity of nausea. The investigator
stayed in the room with the patients in the control group and retested them after 2
minutes.
Permission to conduct the study was obtained from the Human Subjects Review
Committee of Texas Woman's University. Agency permission was obtained for the
hospital through The Institutional Review Board for Human Subjects Research for
Affiliated Hospitals. The guidelines for protection of human subjects were followed.
90
The Demographic Data Tool was used to determine attributes of the sample of the
study and to allow for generalization of the study results. Differences in response to
nausea and touch have been documented in previous studies (Barnett, 1972; Porter,
Redfern; Wilson-Barnett, & LeMay, 1986). The variables identified in the research were
replicated for this study to allow for comparisons and explanations of the study results.
Gender, ethnic origin, reason for EC visit; previous history of nausea, and other symptoms
of nausea were reported as nominal level data. Age was reported as ordinal data based
upon differences in nausea and age as identified by Dodd, Onishi, Dibble, and Larson
(1996) and Rub, Andrews, and Whitehead (1992).
The VANS was used to detennine the effects of touch on the severity of nausea.
This.instrument was a vertical scale measuring exactly l00·mm, with Oat the lowest point
and 100 at the top of the scale. Markings were located along the scale at 10-mm
increments without labels. Zero was labeled as "no nausea" and 100 as the "nausea as bad
as itcan possibly be." In this study, the patient was asked to mark nausea levels on the
measured scale both before and after PT or no touch.
After the final mark on the VANS was completed, the researcher remained
available for questions. The participants shared their questions and comments freely. The
following are some of the questions and comments: (a) "My nausea went away while you
were touching me, but r�turned a few seconds after you stopped," (b) "I think you would
have better results if you had me mark the sheet right after the touch," (c) "Could you
teach my family how to do that?", ( d) "Could you teach me how to do that for this nausea
91
or stop the· nausea from coming back at all? It really has taken over my life," ( e) "Can you
touch me again? It's coming back worse than before," (f) "I can't believe that worked.
Are you a healer or something?", (g) "I would rather have had just a shot," (h) a family
member asked, "How can I help her get over this distress?", and (i) another family
member asked, "I am really surprised that worked. Can you teach that to me?". These
results were not predicted nor measured and can only be considered as suggestions or
ideas for future research.
Discussion of Findings
Findings of the study indicated that a 5-second, bimanual touch to the anterior
shoulder and along the median and ulnar nerve pathways to the dominant hand decreased
the mean nausea intensity score among EC patients (Q < 0.0005). The mean post
intervention scores and standard deviations supported the findings in that the experimental
group mean (48.39) and standard deviation (27.62) were lower than the control
(M = 54.36, SD= 31.25) group analysis. The identified pre touch score, used as the
covariate, was a predictor of posttouch with a probability ofp < 0.0005 based on analysis
of covariance. For purposes of comparison, there were no other published research
studies that compared the effect of PT and decreased nausea.
The decrease in nausea in this study was due to the alteration of the perceptual
field of the participant and a resulting decrease in the patient's degree of reaction
associated with the stress response to nausea. Touch researchers of the past attributed the
92
relief of symptoms or changes in vital signs related to touch or hand holding to autonomic
activity resulting from social interactions with a nurse (Drescher, Gantt, & Whitehead,
1980; Mills, Thomas, Lynch, & Katcher, 1976), rather than an actual alteration in the
perceptual field or changes in neural pathways. The findings of this study supported the ·
use of PT to decrease nausea. The experimental group responded to PT despite a higher
nausea pretouch score and somatic complaints that would increase the distracting stimuli
and resist the introduction of additional stimuli. PT seemed to work for these participants
because several nerve pathways were used to provide sufficient focal stimuli to change the
nausea pathway to the central nervous system. These results supported Roy's ( 1984)
adaptation model since the researcher used one focal stimulus (PT) to alter another
(nausea).
According to Pervan ( 1993 ), nausea can be so distressful that patients will refuse
medications and treatments to avoid it. In this study, patients reported other symptoms
that accompanied nausea, such as weakness, dizziness, flushed feeling, diaphoresis,
anxiety, changes in breathing patterns, palpitations, and pain. According to Selye (1976),
stress was a group of symptoms affecting the entire body system, not just any isolated
organ system. The underlying cause of gastrointestinal symptoms or the symptom of
nausea alone can produce stress to .the entire body system. The findings of this study
supported the documented research on nausea as a stressor and its effect on the autonomic
nervous system and the entire body system.
93
According to other researchers (Barnard & Braselton, 1990; Waddell, 1979),
touch remains a fundamental nursing intervention used to comfort or relieve patient
distress. Nerve impulses influenced the functioning of the central nervous system and
adaptation can be defined as a group of inhibitory and activating reactions to stress (Selye,
197 6). This study used PT as a technique to decrease nausea as a stressor and thus
supported Selye's (1976) definition of adaptation as it applies to nausea in this study.
Nurses intervene on the patient's behalf by blocking or removing noxious stimuli or
stressors from the perceptual field (Ujhely, 1979). The patient becomes vulnerable to the
nausea stimuli through the perceptive pathways of smell, sight, taste, or hearing. This
study explored the perceptive pathways that were commonly associated with nausea by
assessing the patient's history of past nausea events to identify the relationship between
the use of PT as a method to alter nausea stimuli. Gastrointestinal pain was reported as
one of the most common stimuli that contributed to nausea by EC patients. The senses
contributed little to the development of nausea with this study sample. However, PT was
effective in decreasing nausea within the experimental group. PT became a part of the
perceptual field of the system apart from the other stimuli that the participants were
receiving. Roy ( 1984) identified the dynamic perceptual field of an open system as how a
person interacts and reacts within the adaptive system. Nurses can treat the distress of
nausea by altering the p�rceptual field of the _patient by introducing stimuli through the
senses that act as input into the central nervous system that will decrease the patient's
stress response to nausea (Roy & Andrews, 1999). This study supported Roy's (1984)
94
adaptation model by further validating that focal stimuli can interfere with other stimuli to
decrease the intensity of a symptom.
In this study, the researcher used PT to alter focal stimuli pathways of patients
complaining of nausea. The sensation of nausea was diminished through the process of
convergence. Convergence can be described as the coming together of nerve signals from
multiple sources to excite a single neuron (Guyton & Hall, 1996), and as a result, touch to
the sensory pathway could alter the sensation of nausea.
Current literature shows little research in support of nursing interventions for the
distress of nausea. However, studies have been conducted to determine etiologies and
responses among groups of patient diagnoses as a result of therapeutic procedures or
treatments (Cetindag, Boley, Magee, & Hazelrigg, 1999; M. Cohen, Duncan, DeBoer, &
Tweed, 1994; Grapp, Savage, & Hall, 1996; Honkavaara & Pyykko, 1998; Quinn, Brown,
Wallace, & Asbury, 1994 ). Many articles have been written about the causes of nausea
and vomiting (Dodd et al., 1996; Redd, Dadds, Futterman, Taylor, & Bovbjerg, 1993;
Rub et al., 1992). However, few studies have been concentrated on nausea as an isolated
event separate of vomiting.
Some techniques, identified in the literature, used perceptual stimuli to decrease
nausea. Acupressure (AP) and therapeutic touch (TT) were interventions that require
different techniques than the PT identified in this study. The techniques were reported to
decrease nausea. AP used deep, constant pressure on exact points along acupuncture
meridians which have a relationship with various physiological functions (Tappan, 1988).
95
Krieger (1987) defined TT as a human field phenomenon that uses a human energy
transfer from the healer to the ill person via electron transfer resonance to restore the vital
flow in the patient's open system. PT was defined as an intentional physical contact by a
nurse intended to activate stimuli that can change the permeability of receptor cells which ·
travel to the central nervous system in order to decrease nausea.
Belluomini, Litt, Lee, and Katz ( 1994) tested the use of AP to decrease nausea.
The researchers reported that nausea decreased over time with AP technique and was a
safe, low cost, and easily learned technique that can decrease nausea in pregnancy.
Dibble, Chapman, Mack, and Shih (2000) used AP to decrease nausea in chemotherapy
patients. They determined that the intervention might be effective in decreasing nausea for
the sample. PT was found to decrease nausea in the experimental group of this study with
the same safety, low cost, and ease of use as the AP research cited but within time
constraints dictated by the acuity of EC patients. Unfortunately, no research was found to
substantiate TT as an effective intervention for nausea.
Other explanations for the decrease in nausea with PT could be that the technique
can be employed to provide comfort in times of distress as a basic component of nursing
communication and sharing of self (Estabrooks, 1989; Lane, 1989; Langland & Panicucci,
1982; Mccorkle, 1974; Weaver, 1989). Touch and physical closeness also facilitate
patient comfort (Durr, 1971 ), communicate caring and enhance the lived experience
(Bottorff, 1992; Bottorff & Morse, 1994; Copstead, 1980). Even though other reasons
for the possible success of PT were not included as factors in this study, all of the above
96
factors co1:1ld not be excluded from overall results. To control for variations in the way in
which different nurses would comfort or share themselves with patients, the researcher
alone completed all the intervention or control communications on each of the 140
participants.
According to this study, PT decreased nausea in a group of EC patients. Claims
have been made that attached even more significance to touch than this study (Barnett,
1972). The analysis of PT data did uphold some of the other researchers' postulates about
PT being: (a) an essential strategy identified by nurses as a way to share self with patients
(Durr, 1971); (b) a potentially powerful modality (Mills et al., 1976), and (c) could be
perceived by patients as negative if withheld (McCorkle, 1974). The techniques and
locations of PT were supported in the early research on touch interventions (Bottorff
(1993). Schoenhofer (1989) reported that nurses used a stationary touch to a hand or
shoulder most often. Types of touch and touch interventions were identified by others
(Bottorff & Morse, 1994), but no research was found that used PT to decrease nausea.
Further research will be needed to explore the influence of the context of touch, types of
touch as caring methods for meeting the needs of patients, actual practices of touch
between patients and health professionals, using touch to intervene on specific medical
diagnoses, and to formulate a nursing theory for touch. This study on PT and nausea
added to nursing knowledge by identifying a specific technique that can be effective to
decrease nausea. This research was just the beginning in the formulation of a nursing
theory for touch to alter the perceptual field for decreasing nausea.
97
Conclusions
In this study, the hypothesis that mean nausea intensity scores, as measured by the
VANS, among EC patients receiving PT to alter their perceptual field was significantly
lower than mean nausea intensity scores among the EC patients not receiving PT was
supported. Bas_ed on these significant findings, it can be postulated that PT to sensory
areas on the hand and shoulder contributed to a decrease in nausea and that bimanual
touch enhances the overall effect of nausea reliefthrough_the process of convergence that
involve stimuli from two sensory pathways. Since nerve impulses influence the
functioning of the central nervous system and adaptation can be defined as a group of
inhibitory and activating reactions to stress, then nurses can foster adaptation by altering
the perceptual field of the patient. PT can be used as an effective, immediate nursing
intervention to decrease nausea in EC patients with the common complaints of
gastrointestinal distress, pain, and headache. This study further validated that PT applied
to nerve pathways when a patient was experiencing distress from the focal stimulus of
nausea may influence the process of adaptation and decrease the effect of nausea as a
stressor. This perceptual interface can converge with one or more of the nausea pathways
in order to decrease the intensity of the symptom as suggested by Guyton and Hall ( 1996).
Nurses can treat the distress of nausea by altering the perceptual field of the patient and
decreasing the patient's degree of reaction to avoid further complications associated with
the stress response (Roy, 1984; Selye, 1976) to nausea.
98
FT -· ■11
Implications
Since nausea is identified as a stressor and adaptation as a way in which nausea
could be decreased, nurses need to assess the patient's behavior and the focal, contextual,
and residual stimuli influencing the individual as a system (Roy & Andrews, 1999). The
patient's behavior and response to nausea include autonomic body reactions of
diaphoresis, skin pallor, hyper salivation, and hypotension (Cole, 1996 ;·Muth, Stern,
Thayer, & Koch, 1996), or by the patient's verbal complaints of nausea. Once the
assessment of nausea and the response to it are completed, nursing interventions to
promote adaptation by "altering, increasing, decreasing, removing or maintaining" stimuli
(Roy & Andrews, 1999, p. 86) can be implemented. The researcher suggests that nurses
can alter stimuli_ by using PT as a nursing intervention with patients who complain of
nausea in the EC. If PT decreases nausea, then nurses in current practice and student
nurses need to be instructed and encouraged to use the technique to decrease nausea. If
nausea can be decreased by nursing interventions, then the cost of additional anti nausea
medications will decrease, the side effects of the medications can be avoided, and EC costs
will decrease since the patients will need less time to recover from the complications of
nausea.
Recommendations for Further Study
Since this research was based on a convenience sample of EC patients, this study
should be replicated using a more diverse sample. Analysis of the data revealed consistent
99
LL rm
mean values and standard deviations among all variables. This sample was composed
primarily of white (58%) female (70%) patients between the ages of3 l-60 (50%) who
complained of gastrointestinal distress, pain, and headaches (79%). Future research might
explore specific gender, age group, or etiology for nausea, for example.
Other nursing interventions should be tested that are specific to causes and history
of nausea to develop scientific rationale for nausea interventions to help patients avoid the
potential summative and anticipatory causes of nausea. As suggested by Redd et al.
( 1993), a cool cloth to the forehead or to the back of the neck, the aroma of an alcohol
swab, chewing on ice chips, sipping cold ginger ale, dry crackers, pickles, lying flat in bed,
administering intravenous fluids, and anticipatory medications to prevent nausea from
occurring, are interventions that may relieve nausea. Further research may be needed to
establish effective nursing interventions for nausea which might include variations in PT.
This study should be replicated to explore the length of time the PT can be
sustained and how long the effects will last. No research has provided adequate
documentation on the amount of time suggested for this type of touch. According to
Guyton and Hall, ( 1996), all sensory receptors adapt after a period of time either over
seconds, minutes, or hours. It would also be of interest to explore if PT can be more
effective when applied as an alternating stimulus that would use the physiologic principle
of temporal summation rather than simple convergence.
Finally, the study should be replicated to determine the effects of PT on other
patient populations commonly suffering from nausea. For example, PT could be beneficial
100
for patients receiving medications, visiting physicians' offices, inpatient and outpatient
settings, and any location where patients request assistance for nausea symptoms. The
results of this study can only be generalized to the EC population tested. This population
was not receiving chemotherapy, radiation therapy, nor had any abdominal pathology.
However, the scores in this study were not significantly different between age groups.
Therefore, PT may be equally important to all ages of adults who are experiencing nausea.
101
REFERENCES
Adams, P. F., Hindershot, G. E., & Morano, M. A. (1999). Current estimates from the National Health Interview Sun,ey, 1996. Atlanta, GA: Centers for Disease Control and Prevention National Center for Health Statistics: Vital and Health Statistics.
Ahmad, S. (I 978). Significance of nausea and vomiting during acute myocardial infarction. American HeartJournal, 95, 671.
AI-Sadi, M., Newman, B., & Julious, S. A. (1997). Acupuncture in the prevention of postoperative nausea and vomiting. Anaesthesia,52, 658-661.
Arakawa, S. (1997). Relaxation to reduce nausea, vomiting and anxiety induced by chemotherapy in Japanese patients. CancerNursing, 20, 342-349.
Barnard, K., & Brazelton, T. B. (1990); Touch: The foundation of experience. Madison, WI: Johnson & Johnson/International Universities Press.
Barnett, K. (1972). A survey of the current utilization of touch by health team personnel with hospitalized patients. International Journal of Nursing Studies, 9, 195-209.
Bateson, N. (1984). Data construction in social surveys. London: Sage.
Belluomini, J., Litt, R. C., Lee, K. A., & Katz, M. (1994). Acupressure for nausea and vomiting of pregnancy: A randomized, blinded study. Obstetrics and Gynecology, 84, 245-248.
Bellville, J. W., Bross, I. D., & Howland, W. S. (1960). Postoperative nausea and vomiting IV: Factors related to postoperative nausea and vomiting. Anesthesiology, 21, 186-193.
Bennett, J., McDonald, T., Lieblich, S., & Piecuch, J. (1999). Perioperative rehydration in ambulatory anesthesia for dentoalveolar surgery. Oral Surgery, Oral Medicine, Oral Pathology, 88, 279-284.
102
_1
--
Bianchi, A. L., & Grelot, L. (1992). An historical overview of emesis. In A. L. Bianchi, L. Grelot, A. D. Miller, & G. L. King (Eds.), Mechanisms and control of emesis (pp.3-9). London: John Libbey Eurotext.
Bianchi, A. L., Grelot, L., Miller, A. D., & King, G. L. (Eds.). (1992). Mechanisms and control of emesis. London: John Libbey Eurotext.
Borjeson, S., Hursti, T. J., Peterson, C., Fredikson, M., Furst, C. J., Avall-Lundqvist, E., & Steineck, G. (1996). Similarities and differences in assessing nausea on a verbal category scale and a visual analogue scale. Cancer Nursing, 20, 260-266.
Bottorff, J. L. ( 1992). Nurse-patient interaction: Observations of touch. (Doctoral thesis,University of Alberta, 1992). Ottawa: Canadian Theses Services.
Bottorff, J. L. (1993). The use and meaning of touch in caring for patients with cancer. Oncology Nursing Forum, 20, 1531-1538.
Bottorff, J. L., & Morse, J.M. (1994). Identifying types of attending: Patterns of nurses' work. Image: Journal of Nursing Scholarship, 26, 53-60.
Bowsher, J. (1997). Oral care during pregnancy. Professional Care of Mother and Child, 7(4), 101-102.
Brechenridge, M. B., Larry, J. A., & Mazzaferri, E (1996, February 15). Confusion and nausea in a man who appeared to be drunk. Hospital Practice, 47-48.
Brown, S., North, D., Marvel, M. K., & Fons, R. (1992). Acupressure wrist bands to relieve nausea and vomiting in hospice patients: Do they work? American Journal of Hospice and Palliative Care, 9( 4), 26-29.
Burns, N., & Grove, S. K. (1997). The practice of nursing research: Conduct, critique, & utilization. Philadelphia: Saunders.
Carroll, N. V., Miederhoff, P.A., & Cox, F. M. (1994). Costs incurred by outpatient surgical centers in managing postoperative nausea and vomiting. Journal of Clinical Anesthesia, 6, 364-369.
Cetindag, I. B., Boley, T. M., Magee, M. J., & Hazelrigg, S. R. (1999). Postoperative gastrointestinal complications after lung volume reduction operations. Annuals of Thoracic Surgery, 68, 1029-1033.
103
Cohe°' J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum.
Cohe°' M. M., Duncan, P. G., DeBoer, D. P., & Tweed, W. A. (1994). The postoperative interview: Assessing risk factors for nausea and vomiting. Anesthesia & Analgesia, 78(1), 7-16.
Cohen, S.S. (1987). The magic of touch. New York: Harper & Row.
Cole, L. (1996). Anatomy and physiology of the gastrointestinal system. In S. D. Ruppert, J. G. Kernicki, & J. T. Dolan (Eds.), Dolan 's critical care nursing: Clinical management through the nursing process (2nd ed.) (pp. 777-790). Philadelphia: Davis.
Contanch, P. A. ( 1984). Measuring nausea and vomiting in clinical nursing research. Oncology Nursing Fonim, 11(3), 92-94.
Coppola, M., Yealy, D. M., & Leibold, R. A. (1995). Randomized, placebo-controlled evaluation of prochlorperazine versus metoclopramide for emergency department treatment of migraine headache. Annals of Emergency Medicine, 26, 541-546.
Copstead, L. C. ( 1980). Effects of touch on self-appraisal and interaction appraisal for pennanently institutionalized older adults. Journal of Gerontological Nursing, 6, 747-752.
Coslow, B. I., & Eddy, M. E. (1998). Effects of preoperative ambulatory gynecological education: Clinical outcomes and patient satisfaction. Journal of PeriAnesthesia Nursing, 13, 4-10.
Cox, C., & Hayes, J. (1999). Physiologic and psychodynamic responses to the administration of therapeutic touch in critical care. Intensive and Critical Care Nursing, 15, 363-368.
Dibble, S. L., Chapman, J., Mack, K. A., & Shih, A (2000). Acupressure for nausea: Results of a pilot study. Oncology Nursing Forum, 27(1), 41-47.
Diiorio, C., van Lier, D., & Manteuffel, B. (1994). Recommendations by cliniciansfor nausea and vomiting of pregnancy. Clinical Nursing Research, 3, 209-227.
104
Dodd, M. J., Onishi, K., Dibble, S. L., & Larson, P. L. (1996). Differences in nausea, vomiting, and retching between younger and older outpatients receiving cancer chemotherapy. Cancer Nursing, 19, 155-161.
Drescher, V. M., Gantt, W. H., & Whitehead, W. E. (1980). Heart rate response to touch. Psychosomatic Medicine, 42, 559-565.
Dundee, J. W. Ghaly, R. G., Bill, K. M., Chestnutt, W. N., Fitzpatrick, K. T., & Lynas, A G. (1989). Effect of stimulation of the P6 antiemtic point on postoperative nauseaand vomiting. British Journal of Anaesthesia, 63, 612-618.
Dundee, J. W., Sourial, F. B., Ghaly, R. G., & Bell, P. F. (I 988). P6 acupressure reduces morning sickness. Journal of the Royal Society of Medicine, 81, 456-457.
Dundee, J. W., & Yang, J. (1990). Prolongation of the antiemetic action of P6 acupuncture by acupressure in patients having cancer chemotherapy. Journal of the Royal Society of Medicine, 83, 360-362.
Durr, C. A (1971). Hands that help but how. Nursing Forum, 10, 392-400.
Edwards, J. N. ( 1996). Reliability and validity of the Edwards nausea assessment tool to measure nausea of cancer (UMI No. 9623074). Ann Arbor: UMI Dissertation Services.
Egan, E. C. (1998). Therapeutic touch. In M. Snyder, & R. Lindquist (Eds.), Complementary/alternative therapies in nursing (pp. 49-62). New York: Springer.
Engstrom, C., Hernandez, I., Haywood, J., & Lilenbaum, R. (1999). The efficacy and cost effectiveness of new antiemetic guidelines. Oncology Nursing Fon1m, 26, 1453-
1458.
Estabrooks, C. A (1989). Touch: A nursing strategy in the intensive care unit. Heart &Lung, 18, 392-401.
Fedoruk, R. B. (1984). Transfer of the relaxation response: Therapeutic touch as a method for reduction of stress in premature neonates. Dissertation Abstracts International, 46r 978B. (ADG 85-09162).
Ferrara-Love, R., Sekeres, L., & Bircher, N. G. (1996). Nonpharmacologic treatment of postoperative nausea. Journal of PeriAnesthesia Nursing, 11, 378-383.
105
Fessele, K. S. (1996). Managing the multiple causes of nausea and vomiting in the patient with cancer. Oncology Nursing Forum, 23, 1409-1417.
Petting, J. H., Grochow, L. B., Folstein, M. F., Ettinger, D. S., & Colvin, M. (1982). The course of nausea and vomiting after high-dose cyclophosphamide. Cancer Treatment Reports, 66, 1487-1493.
Fowler, F. J. (1984). Survey research methods. London: Sage.
Fox, R. A. (1992). Current status: Animal models of nausea. In A. L. Bianchi, L. Grelot, A. D. Miller, & G. L. King (Eds.), Mechanisms and controlof emesis (pp. 341-350). London: John Libbey Eurotext.
Gagne, D., & Toye, R. C. (1994). The effects of therapeutic touch and relaxation therapy in reducing anxiety. Archives of Psychiatric Nursing, 8, 184-189.
Giasson, M., & Bouchard, L. (1998). Effect of therapeutic touch on the well-being of persons with terminal cancer. Journal of Holistic Nursing, 16, 383-398.
Gift, A. G. ( 1989). Visual analogue scales: Measurement of subjective phenomena. Nursing Research, 38, 286-288.
Glick, M. S. (1986). Caring touch and anxiety in myocardial infarction patients in the intermediate cardiac care unit. Intensive Care Nurse, 2(2), 61-66.
Golberg, B. (1998). Connection: An exploration of spirituality in nursing care. Journal of Advanced Nursing, 27, 836-842.
Goodman, M. ( 1997). Risk factors and antiemetic management of chemotherapy induced nausea and vomiting. Oncology Nursing Forum, 24(7), 20-32.
Grad, B. R. (1965). Some biological effects of the "laying on of hands": A review of experiments with animals and plants. Journal of the American Society for Psychical Research, 59(2), 95-127.
Grant, M. (1997). Introduction: Nausea and vomiting, quality of life, and the oncology nurse. Oncology Nursing Forum, 24(7), 5-7.
Grapp, M. J., Savage, L., & Hall, G. B. (1996). The incidence of gastrointestinal symptoms in cardiac surgery patients through six weeks after discharge. Heart &Lung, 25, 444-450.
106
Greif, R., Laciny, S., Rapf, B.; Hickie, R. S., & Sessler, D. I. (1999). Supplemental oxygen reduces the incidence of postoperative nausea and vomiting. Anesthesiology, 91, 1246-1252.
Guyton, A. C., & Hall, J. E. (1996). Textbook of medical physiology (9th ed.). Philadelphia: Saunders.
Handa, M., Mine, Z., Yamamoto, H . ., Tsutsui, S . ., Hayashi, H., Kinukawa., N., & Kudo, C. (1999). _Esophageal motility and psychiatric factors in functional dyspepsia patients with or without pain. Digestive Diseases and Sciences, 44, 2094-2098.
Harmon, D., Gardiner, J., Harrison, R., & Kelly, A. (1999). Acupressure and the prevention of nausea and vomiting after laparoscopy. BritishJournal of Anaesthesia, 82, 387-390.
Hartman, F. (1992). Cranio-mandibular disorders inducing nausea and vomiting. In AL. Bianchi, L. Grelot, A D. Miller, & G. L. King (Eds.), Mechanisms and control of emesis (pp. 51-58). London: John Libbey Eurotext.
Hawthorn, J. ( 1995). Understanding and management of nausea and vomiting. Cornwall, UK: Blackwell Science.
Heidt, P. (1981). Effect of therapeutic touch on anxiety level of hospitalized patients. Nursing Research, 30, 32-37.
Hepburn, D. A., Deary, I. J., Frier, B. M., Patrick, A. W., Quinn, J. D., & Fisher, B. M. (1991). Symptoms of acute insulin-induced hypoglycemia in.humans with and without IDDM. Diabetes Care, 14, 949-957.
Hinojosa, R. J. (1992). Nursing interventions to prevent or relieve postoperative nausea and vomiting. Journal of Post Anesthesia Nursing. 7(1), 3-14.
Hippocrates. (400 B.C.E.). Aphorisms by Hippocrates. (F. Adams, Trans.). Retrieved November 10, 1999, From Massachusetts Institute of Technology, The Internet Classics Archive Web site: http://classics.mit.edu/Hippocrates/aphorisms.html
Ho, C. M., Hseu, S. K., Tsai, S. K., & Lee, T. Y. (1996). Effect of P-6 acupressure on prevention of nausea and vomiting after epidural morphine for post-Cesarean section pain relief Acta Anaesthesio/ogica of Scandinavica, 40, 372-375.
107
Hogan, C. M. (1983). Nausea and vomiting. In J. Yasko (Ed.), Guidelines for cancercare: Symptom management. (pp. 198-211). Reston, VA: Reston Publishing.
Hogan, C. M., & Grant, M. (1997). Physiologic mechanisms of nausea and vomiting in patients with cancer. Oncology Nursing Forum, 24(7), 8-12.
Hollinger, L. M. ( 1980). Perception of touch in the elderly. Joumal of GerontologicalNursing, 6, 741-746.
Holmes, H. N. (Ed.). (2001 ). Atlas of human anatomy. Springhouse, PA: Springhouse.
Holy Bible. (1611). Authorized (King James) Version. London: R. Barker.
Honkavaara, P., & Pyykko, I. (1998). Surgeon's experience as a factor for emetic sequelae after middle ear surgery. ACTA Anaesthesiologica Scandinavica, 42,1033-1037.
Huck, S. W., & Cormeir, W. H. (1996). Reading statistics and research (2nd ed.). New York: Harper Collins.
Ignatavicius, D. D., Workman, M. L., & Mishler, M. A (Eds.). (1999). Medical-surgicalnursing across the health care continuum. (3rd ed.). Philadelphia: Saunders.
Ingram, D. A., Fulton, R. A, Protal, R. W., & Aber, C. P. (1980) Vomiting as a diagnostic aid in acute ischaemic cardiac pain. British Medical Journal, 281, 636-637.
Jablonski, R. S. (1993). Nausea: The forgotten symptom. Holistic Nursing Practice, 7(2), 64-72.
Jednak, M. A., Shadigian, E. M., Kim, M. S., Woods, M. L., Hooper, F. G., Owyang, C., & Hasler, W. L. (1999). Protein meals reduce nausea and gastric slow wave dysrhythmic activity in first trimester pregnancy. American Journal of Physiology,277, G855-861.
Jenns, K. (1994). Importance of nausea. Cancer Nursing, 17, 488-493.
Keller, E., & Bzdek, V .. (1986). Effects of therapeutic touch on tension headache pain. Nursing Research, 35, 101-106.
108
i
i
King, C. R. ( 1997). N onpharmacologic management of chemotherapy induced nausea and vomiting. Oncology Nursing Forum, 24(1), 41-48.
King, C.R. (2001). Nausea and vomiting. In B. R. Ferrell, & N. Coyle (Eds.), Textbook of palliative nursing (pp. 107-121 ). Oxford: Oxford University Press.
King, I. M. ( 1981 ). A theory for ,mrsing: Systems, concepts, process. New York: John Wiley & Sons.
Kirk, R. E. (1982). Experimental design (2nd ed.). Pacific Grove, CA: Brooks/Cole.
Knable, J. ( 1981 ). Handholding: One means of transcending barriers of communication. Heart & Lung, JO, 1106-1110.
Kramer, N. A. (1990). Comparison of therapeutic touch and casual touch in stress reduction of hospitalized children. Pediatric Nursing, 16, 483-485.
Krieger, D. (1975). Therapeutic touch: The imprimatur of nursing. American Journal of Nursing, 75, 784-787.
Krieger, D. (1987). Living the therapeutic touch: Healing as a lifestyle. New York: Dodd, Mead & Company.
Lamb, J., Ingram, C., Johnson, I., & Pitman, R. (1980). Essentials of physiology. London: Blackwell Scientific.
Lane, P. L. (1989). Nurse-client perceptions: The double standard of touch. Issues in Mental Health Nursing, 10, 1-13.
Langeluddecke, P., Goulston, K., & Tennent, C. (1990). Psychological factors in dyspepsia of unknown cause: A comparison with peptic ulcer disease. Journal Psychosomatic Research, 34, 215-222.
Langland, R. M., & Panicucci, C. L. (1982). Effects of touch on communication with elderly confused clients. Journal of Gerontological Nursing, 8, 152-155.
Lederman, E. (1997). Fundamentals of manual therapy: Physiology, neurology, and psychology. New York: Churchill Livingstone.
109
Lenz, E. R., Pugh, L. C., Milligan, R. A., Gift, A., & Suppe, F. (1997). The middle-range theory of unpleasant symptoms: An update. Advances·in Nursing Science, ·19(3), 14-27.
Mann, A. (1998). A continuing postoperative complication: Nausea and vomiting--Who is affected, why, and what are the contributing factors? A review. CRNA: Clinical Forum for Nurse Anesthetists, 9(1), 19-29.
Mannix, K. A. (1999). Palliation of nausea and vomiting. In D. Doyle, G. W. Hanks, & N. MacDonald (Eds.), Oxford textbook of palliative medicine (2nd ed., pp. 489-499). New York: Oxford University Press.
Marley, R. A. ( 1996). Postoperative nausea and vomiting: The outpatient enigma. Journal of PeriAnesthesia Nursing, 11, 14 7-161.
McCorkle, R. (1974). Effects of touch on seriously ill patients. Nursing Research, 23, 125-132.
Mccorkle, R., & Hollenbach, M. (1990). Touch and the acutely ill. In K. Barnard & T. Brazelton (Eds.), Touch: The foundation of experience (pp. 517-540). Madison, WI: International University Press.
Meehan, T. C. (1998). Therapeutic touch as a nursing intervention. Journal of Advanced Nursing, 28(1), 117-125.
Menashian, L., Flam, M., Douglas-Pazton, D., & Raymond, J. (1992). Improved food intake and reduced nausea and vomiting in patients given a restricted diet while receiving cisplatin chemotherapy. Journal of the Americam Dietetic Association, 92(1), 58-61.
Mills, M. E., Thomas, S. A., Lynch, J. J., & Katcher, A.H. (1976). Effect of pulse
palpation on cardiac arrhythmia in coronary care patients. Nursing Research, 25,
378-382.
Montagu, A. (1986). Touching: The human significance of the skin (3rd ed.). New York:
Harper & Row.
Morse, J. M. (1983). An ethnoscientific analysis of comfort: A preliminary investigation.
Nursing Papers, 15(1), 6-20.
110
Muth, E. R., Stem, R. M., Thayer, J. F., & Koch, K. L. (1996). Assessment of the multiple dimensions of nausea: The nausea profile. Journal of Psychosomatic Research, 40, 511-520.
National Institute of Health. (1997).Acupuncture. NIH Consensus Statement, 15(5), l-34.
O'Brien, B., & Nabor, S. (1992). Nausea and vomiting during pregnancy: Effects on the quality of women's lives. Birth, 19, 138�143.
O'Brien, B., Relyea, J., & Lidstone, T. (1997). Diary reports of nausea and vomiting during pregnancy. Clinical Nursing Research, 6, 239-252.
O'Brien, B., Relyea, J., & Taerum, T. (1996). Efficacy of P6 acupressure in the treatment of nausea and vomiting during pregnancy. American Journal of Obstetrics and Gynecology, 174, 708-715.
O'Brien, B., & Zhou, Q. (1995). Variables related to nausea and vomiting during pregnancy. Birth, 22, 93-100.
Olson, M., Sneed, N., Bonadonna, R., Ratliff, J., & Dias, J. (1997). Therapeutic touch and post-Hurricaine Hugo stress. Journal of Holistic Nursing, 10(2), 120-136.
Padilla, G. V., Presant, C., Grant, M. M., Metter, B., Lipsett, J., & Heide, F. (1983). Quality of life index for patients with cancer. Research in Nursing and Health, 6(3), 117-126.
Paech, M. J., Pavy, T. J., Kristensen, J. H., & Wojnar-Horton, R. E. (1998). Postoperative nausea and vomiting: development of a management protocol. Anesthesia and Intensive Care, 26(2), 152-155.
Pedhazur, E. J., & Schmelkin, L. P. (1991). Measurement, design, and analysis: An integrated approach. Hillsdale, NJ: Lawrence Erlbaum.
Pervan, V. (1993). Understanding anti-emetics. Nursing Times, 89(10), 36-38.
Phillips, K., & Gill, L. ( 1993). A point of pressure: Use of acupressure wrist bands to relieve postoperative nausea. Nursing Times, 89( 45), 44-45.
Polit, D.F., & Hungler, B.P. (1995). Nursing research: Principles and methods.
Philadelphia: Lippincott.
111
Porter, L., Redfern, S., Wilso�-Barnett, J., & LeMay, A. (1986). The development of an observation schedule for measuring nurse-patient touch, using an ergonomic approach. International Journal of Nursing Studies, 23(1), 11-20.
Quinn, J. F. (1984). Therapeutic touch as energy exchange: Testing the theory. Advancesin Nursing Science, 6(2), 42-49.
Quinn, A. C., Brown, J. H., Wallace, P. G., & Asbury, A. J. (1994). Studies in postoperative sequelae. Nausea and vomiting--still a problem. Anaesthesia, 49(1),62-65.
Redd, W. H., Dadds, M. R., Futtennan, A. D., Taylor K. L., & Bovbjerg, D. H. (1993). Nausea induced by mental images of chemotherapy. Cancer, 72, 629-636.
Renouf, D. (1998). Hypnotically induced control of nausea: A preliminary report. Journalof Psychosomatic Research, 45, 295-296.
Rhodes, V. A. ( 1990). Nausea, vomiting, and retching. Nursing Clinics of North America,25, 885-900.
Rhodes, V. A. (1997). Criteria for assessment of nausea, vomiting, and retching. Oncology Nursing Forum, 24(7), 13-19.
Rhodes, V. A., McDaniel, R. W., & Johnson, M. H. (1995). Patient education: Self-care guides. Seminars in Oncology Nursing, 11, 298-304.
Rhodes, V. A., & Watson, P. M. (1987). Symptom distress--the concept: Past and present. Seminars in Oncology Nursing, 3, 242-24 7.
Roy, Sr. C. (1984). Introduction to nursing: An adaptation model. Englewood Cliffs, NJ: Prentice Hall.
Roy, Sr. C., & Andrews, H. (1999). The Roy adaptation model (2nd ed.). Stamford, CT: Appleton & Lange.
Roy, Sr. C., & Roberts, S. (Eds.). (1981). Theory construction in nursing: An adaptationmode 1. Englewood Cliffs, NJ: Prentice Hall.
Rub, R., Andrews, P. L., & Whitehead, S. A. (1992). Vomiting: incidence, causes, ageing and sex. In A. L. Bianchi, L. Grelot, A. D. Miller, & G. L. King (Eds.), Mechanisms and control of emesis (pp. 363-365). London: John Libbey Eurotext.
112
Ruckman, P. S. (1980). Tongues, signs and healing. Pensacola, Fl: Bible Baptist Bookstore.
Schoenhofer, S. 0. (1989). Affectional touch in critical care nursing: A descriptive study. Heart� Lung, 18, 146-154.
Selye, H. (1976). The stress of life (2nd ed.). New York: McGraw-Hill.
Silva, M.A. (1992). The effects of relaxation touch on the recovery level of postanesthesia abdominal hysterectomy patients. Unpublished doctoral dissertation. Texas Woman's University, Denton.
Simington,l A., & Laing, G. P. (1993). Effects of therapeutic touch on anxiety in the institutionalized elderly. Clinical Nursing Research, 2, 438-450.
Sneed, N. V., Olson, M., Bubolz, B., & Finch, N. (2001). Influences of a relaxation intervention on perceived stress and poser spectal analysis of heart rate variability. Progress in Cardiovascular Nursing, 15(2), 57-64.
Snyder, M., Egan, E. C., & Burns, K. R. ( 1995). Interventions for decreasing agitation behavio�s in persons with dementia. Journal of Gerontological Nursing. 21 (7), 34-40.
Snyder, M:, & Nojima,Y. (1998). Purposeful touch. In M. Snyder, & R. Lindquist (Eds.), Complementarylaltemative therapies in nursing (pp. 149-158). New York: Springer.
Stone, C. L. (1993). Acupressure wristbands for the nausea of pregnancy. Nurse Practitioner, 18(1 I), 15, 18, 23.
Talley, N. J., Fung, L. H., Gilligan, I. J., McNeil, D., & Piper, D. W. (1986). Association of anxiety, neuroticism, and depression with dyspepsia of unknown cause: A casecontrol study. Gastroenterology, 90, 886-892.
Tappan, F. M. (1988). Healing massage techniques: Holistic, classic, and emerging methods (2nd ed.). Norwalk, CT: Appleton & Lange.
Tate, S. ( 1997). Peppermint oil: A treatment for postoperative nausea. Journal of Advanced Nursing, 26, 543-549.
113
Thompson, H.J. (1999). The management of post-operative nausea and vomiting. Journal of Advanced Nursing, 29, 1130-1136.
Tobias, J. D. (1993). Management of minor adverse effects encountered during narcotic administration. Journal of Post Anesthesia Nursing, 8( 6), 96-100.
Tovar, M. K., & Cassmeyer, V. L. (1989). Touch: The beneficial effects for the surgical patient. Association of Operating Room Nursing Journal, 49, 1356-1363.
Triplett, J. L., & Arneson, S. W. (1979). The use of verbal and tactile comfort to alleviate distress in young hospitalized children. Research in Nursing and Health, 2(1), 17-23.
Ujhely, G. B. (1979). Touch: Reflections & perceptions. Nursing Forum, 18, 18-33.
Ulett, G. A., Han, J., & Han, S. (1998). Traditional and evidence-based acupuncture : History, mechanisms, and present status. Southern Medical Journal, 91, 1115-1120.
van Lier, D., Manteuffel, B., Diiorio, C., & Stalcup, M. (1993). Nausea and fatigue during early pregnancy. Birth, 2.0(4), 193-197.
Visalyaputra, S., Petchpaisit, N.·, Somcharoen, K., & Choavaratana, R. (1998). The efficacy of ginger root in the prevention of postoperative nausea and vomiting after outpatient gynecological laparoscopy. Anesthesia, 53, 486-510.
Waddell, E. (1979). Quality touching to communicate caring. Nursing Forum, 18, 288-293.
Waltz, C. F., Strickland, 0. L., & Lenz, E. R. (1991). Measurement in nursing research (2nd ed.). Philadelphia: Davis.
Wang, S., Hofstadter, M. B., & Kain, Z. N. (1999). An alternative method to alleviate postoperative nausea and vomiting in children. Journal of Clinical Anesthesia 11,
231-234.
Wardell, D; W., & Mentgen, J. (1999). Healing touch: An energy-based approach to healing. Imprint, 46(2), 35-36, 51.
Weaver, D. F. (1989). Nurses' views on the meaning of touch in obstetrical nursing practice. Journal of Obstetric Gynecologic Neonatology Nursing, 19(2), 157-160.
114
Weiss, S. J. (1979). The language of touch. Nursing Research, 2�, 76-80.
Weiss, S. J. (1986). Psycho physiologic effects of caregiver touch on incidence of cardiac dysrhythmia. Heart & Lung, 15, 495-504.
Wenrich, J. (1994). Epidural Diet Regimen. Journal of Post Anesthesia Nursing, 9, 283-284.
White, P. F., & Shafer, A. (1988). Nausea and vomiting: Causes and prophylaxis. Seminars in Anesthesia, 6, 300-308.
Whitehead, S. A., Andrews, P. L., & Chamberlain, G. V. (1992). Characterization of nausea and vomiting in early pregnancy: A survey of 1000 women. Journal of Obstetrics and Gynecology, 12, 364-369.
Windle, P. E., Borromeo, A., Robles, H., & Ilacio-Uy, V. (2001). The effects of acupressure on the incidence of postoperative nausea and vomiting in postsurgical patients. Journal of Perianestheris Nursing, 16, 158-162.
Wirth, D. P. (1990). The effect of non-contact therapeutic touch on the healing rate of full thickness dermal wounds. Subtle Energies,.}, 1-20.
115
I i
APPENDIX A
AGENCY APPROVALS
116
I
I
Department Of Pediatrics-Administration Mail Station: /
One Baylor Plaza
Houston, Texas 77030
Office of Research
(713) 798-6970
RE: #H-9564 • NAUSEA RELIEF AND PURPOSEFUL TOUCH: DECREASING DISTRESS
BY AL TEAING THE PERCEPTUAL FIELD
APPROVAL VALID FROM 2/6/01 TO 2/6/02
Dear
The Institutional Review Board for Human Subject Research for : Affiliated Hospitals (BCM IRB) is pleased to inform you that your above referenced research protocol and consent form were approved according to institutional guidelines and provided they receive the unaltered approval of any other institutional committees in which your research is involved.
1. Continued review will be required( ) a. After each subject's exposure( ) b. Quarterly( ) c. Semi-annually(X) d. Annually(X) e. Change in Protocol(X) f. Development of unexpected problems or unusual
complications( ) g. Other
2. Method of Review(X) a. IRB Renewal Form (IRB2) ( ) b. New Protocol( ) c. Interview with principal investigator( ) d. Other
If a consent form is being used for this protocol, only the IRB approved (and stamped) version should be used for obtaining consent from potential stud� subjects.
Sincerely yours
Kathleen J. Motil, M.D., Ph.D., Chair Institutional Review Board for Human Subject Research
& Affiliated Hospitals
KJM:mrt
humanap
117
'\C., '\S 16 77 j,r, .. ,, '\'?, ., ,;,·.-:··
11,.'l- • ,.·.
� 'I'
t HAR 2001
� RELEASED �
c\.�,
"•�=-=-- '-�· �,--· .·•'.
TEXAS WOMAN'S UNIVERSITY DENTON DALLAS HOUSTON
HUMAN SUBJEC� REVIEW COMMITIEE • HOUSTON CENTER
HSRC APPROVAL FORM
Name of lnvestigator(s) Linda S. Dune RN MS
Social Security Number(s) ____ . · . .a.• i __ ·___.....,;._.._ _________________ _
Name of Research Advisor(s) Jeanette Kemicki RN PhD
Address: -�""""1 __ 17 __ 0=3 __ M=ead=o=wtrail=·�Lan=::::.e __________________ _
Stafford Texas 77477-13S2
Dear: -----=L�in:.::da=-=D"'"un:..:ae=--------------------------
Your study entitled: Nausea relief and purposeful touch: Decre.ising distress by altering the perceptual
field
(11,e applicant must complete the top portion of this form)
has been reviewed by the Human Subjects Review Committee - Houston Center and it appears to meet our requirements in regard to protection of the individual's rights.
Please be reminded that both the University and the Department of Health and Human Services regulations typically require that signatures indicating infonned consent be obtained from all hwnan subjects in your study. These arc to be filed with the Human Subjects Review Committee Chairman. Any exc;eption to this requirement is noted below. Fwthcnnore, according to lll-lS regulations. another review by the HSRC is required if your project changes or if it es:tends beyond one year from this date of approval.
Any special provisions pertaining to your study are noted below:
______ The filing of signatures of subjects with the Human Subjects Review Committee is not :tquircd.
______ Other. sec attached sheet.
___ ./ ___ No special provisions apply.
Sincerely,
g J, IH-d>c "7t}J,_µ) .., '��.G�rsch. Ph.D. Chairperson., HSRC • Houston Center
Date
BSRC-H 1999 • 19
118
APPENDIXB
INFORMED CONSENT
119
PAGE 1 of3
AND AFFILIATES CONSENT TO PARTICIPATE IN A RESEARCH PROJECT (BPC) (9 9.6-08)
1. TITLE OF PROTOCOL
NAUSEA RELIEF AND PURPOSEFUL TOUCH: DECREASING DISTRESS BY ALTERING THE PERCEPTUAL FIELD
2. BACKGROUNDThere are few reported studies related to nausea and specific nursing actions that relieveit. Patients with nausea experience a feeling of helplessness and distress that may bedecreased with nursing care.
3. PURPOSE OF THE STIJDYThe purpose of this study is to detennine if nurses can decrease uncomfortable feelingsof nausea in patients who are in the emergency center by using touch. The length of thisstudy will be approximately six months.
4. PROCEDURESI understand that:[X] I will be .one of 140 subjects to be asked to participate in this trial.
I also understand that: 1. This study is to find out if a nurse's actions can make nausea (an upset stomach,
queasiness) stop or decrease.2. I will be asked to be available for fifteen (1 5) minutes to finish the study.3. I will only be participating in the study during this hospital emergency center visit.4. The researcher will explain the purpose of touch and feelings that I.might have from
the touch before beginning the study.5. I will be asked about my nausea and will be asked to mark a place on a paper sca1e to
let the researcher know how bad my nausea is.6. The researcher may touch my shoulder and hand for five (5) seconds.7. I will be asked to mark a place on another paper scale to let the researcher know how
bad my nausea is.8. I will receive all treatments as prescribed by the physician. My medica1 care will not
be slowed down because of my part in this study.9. I will be asked several questions about how I feel and any nausea that I have had in
the past.10. I can refuse to answer all or some of the questions.1 1. I may decide to stop the study at any time.
120
I
L __
PAGE2of3
5. RISKS/DISCOMFORTSI understand that the risks of participation in this study include:
1. Potential embarrassment from loss of privacy.2. Potential uneasiness, or a pressure sensation to the shoulder or hand when I am
touched.3. Potential that I may be identified in the research report.
6. BENEFITS
I have been told that the benefits of participating in this study may be partial or completerelief of nausea. However, I may receive no benefit from participating in this study.
7. ALTERNATIVESThe only al�emative to this study is non-participation.
8. FINANCIAL COSTS TO SUBJECTSThere will be no cost to subjects of this research study.
9. SUBJECT'S RIGHTSI have been informed that there may be unknown risks/discomforts involved, and that Iwill receive any new information discovered during the course of the study, concerningsignificant treatment findings that may affect my willingness to continue to participate.
Every effort will be made to maintain the confidentiality of my study records. The investigator, and agents of Baylor College of Medicine and The Methodist Hospital will be allowed to inspect sections of my medical and research records related to this study. The data from the study may be published; however I will not be identified by name. The confidentiality of the data will be maintained within legal limits.
In the event of injury resulting from this research, Baylor College of Medicine and/or The Methodist Hospital are not able to offer financial compensation nor to absorb the costs of medical treatment However, necessary facilities, emergency treatment and professional services will be available to research subjects,just as they are to the community generally. My signature below acknowledges my voluntary participation in this research project. Such participation does not release the investigator, or institutions from their professional and ethical responsibility to me.
My participation is voluntary and I may refuse to participate or may discontinue my participation AT ANY TIME, without penalty, loss of benefits, or change in my present or future care. The investigator has the right to withdraw me from the study at any time. My withdrawal from the study may be for reasons re1ated solely to me ( e.g. not following study-related directions from the Investigator; a serious adverse event reaction) or because the entire study has been tenninated.
121
PAGE3of3
The investigator has answered all of my questions. lfl have additional questions during the course ofthis study about the research or my rights as a research subject, I may address them to the Baylor Affiliates Review Board for Human Subject Research at (713) 798-6970. In the event of a research-related injury or if any other problems arise, I may
contact Linda Dune at (713) 793-1466.
I HA VE READ THE INFORMATION PROVIDED ABOVE (OR HA VE HAD IT READ TO ME) AND HAD MY QUESTIONS ANSWERED TO MY SATISFACTION. I VOLUNTARIL y AGREE TO PARTICIPATE IN nns STUDY. I WILL RECEIVE COPY OF nns CONSENT FORM.
Signature of Research Subject (Including children - when applicable)
Signature of Legal Representative or next of kin (If applicable)
(Relationship - i.e. Father, Mother, etc.)
Signature of Investigator or Designee Obtaining Consent
122
Date
Date
Date
NOT VALID WITHOUT THE INSTITUTIONAL
REVIEW BOARD STAMP OF CERTIFICATION - ······ ·
LID FOR 1 YEAR FROM ABOVE DATE

APPENDIXC
DEMOGRAPIIlC DATA TOOL
123
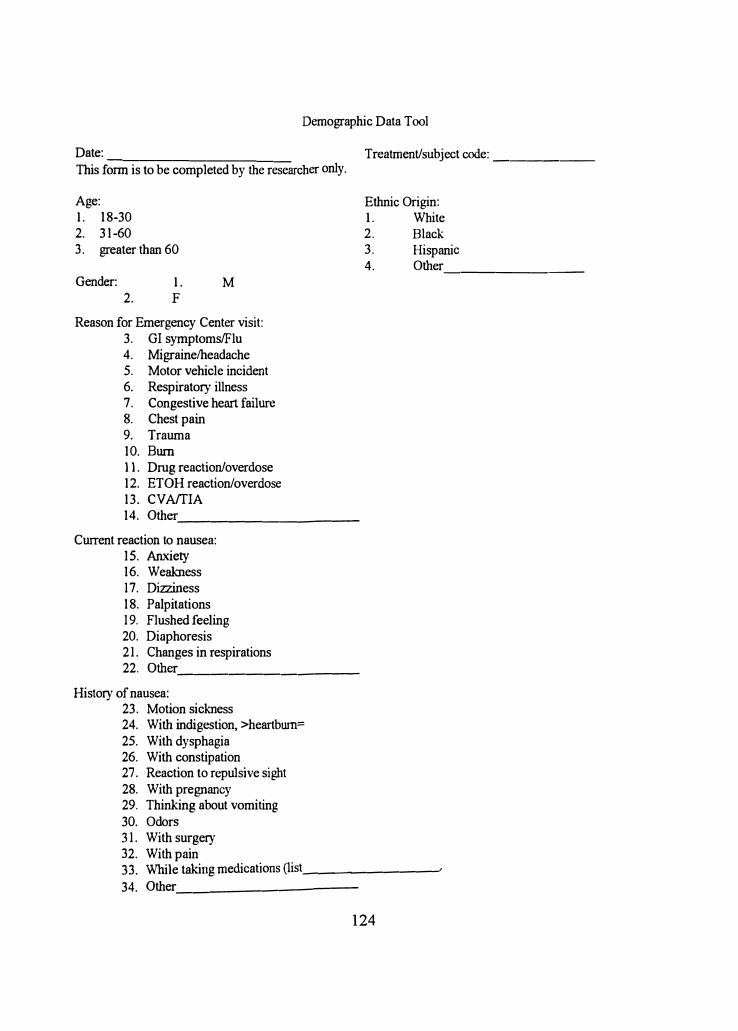
Demographic Data Tool
Date: -----------
This fonn is to be completed by the researcher only.
Age: I. 18-302. 31-603. greater than 60
Gender: 2.
I. F
M
Reason for Emergency Center visit: 3. GI symptoms/Flu4. Migraine/headache5. Motor vehicle incident6. Respiratory illness7. Congestive heart failure8. Chest pain9. Trauma10. Burn11. Drug reaction/overdose12. ETOH reaction/overdose13. CVAffIA
Treatment/subject code: _____ _
Ethnic Origin: I. White2. Black3. Hispanic4. Other _______ _
14. Other __________ _
Current reaction to nausea: 15. Anxiety16. Weakness17. Dizziness18. Palpitations19. Flushed feeling20. Diaphoresis21. Changes in respirations22. Other __________ _
History of nausea: 23. Motion sickness24. With indigestion, >heartburn=
25. With dysphagia26. With constipation27. Reaction to repulsive sight28. With pregnancy29. Thinking about vomiting30. Odors31. With surgery32. With pain33. While taking medications (list. __ __;,_ _____ __,
34. Other __________ _
124

APPENDIXD
VISUAL ANALOG NAUSEA SCALE
125
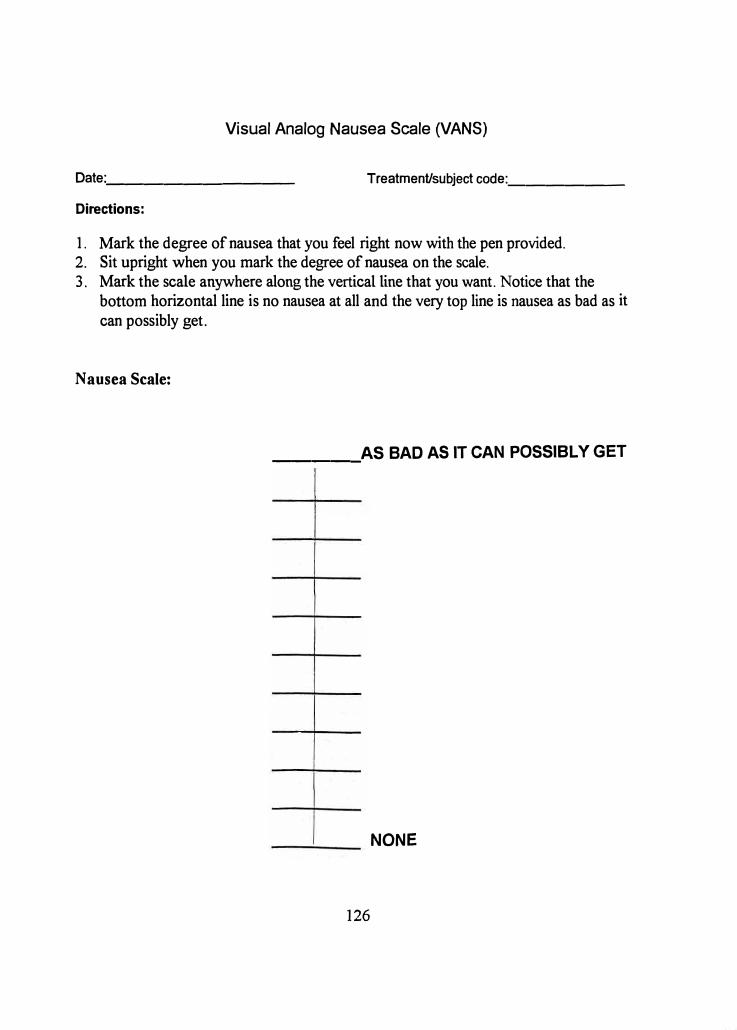
Visual Analog Nausea Scale (VANS)
Date:. _________ _ Treatment/subject code:. _____ _
Directions:
1. Mark the degree of nausea that you feel right now with the pen provided.2. Sit upright when you mark the degree of nausea on the scale.3. Mark the scale anywhere along the vertical line that you want. Notice that the
bottom horizontal line is no nausea at all and the very top line is nausea as bad as it
can possibly get.
Nausea Scale:
AS BAD AS IT CAN POSSIBLY GET -----
NONE
126
o , J I I '.� • -1�-...