Embed Size (px)
Citation preview

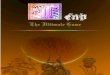
Treat other pulmonary
conditions if misdiagnosed
Consider referring patient to an
asthma specialist
• Start with non-invasive testing (allergy testing, IgE level, blood eosinophil count and FeNO* level) *Fractional nitric oxide concentration in exhaled breath.• If poor response to therapy continues, consider induced sputum di�erential for eosinophil and neutrophil counts and/or bronchoscopy with endobronchial biopsy and BAL
DETERMINE INFLAMMATORY PHENOTYPE/ ENDOTYPE FOR PERSONALIZED TREATMENT SELECTION
E
HealthNational Jewish
© 2019 National Jewish Health
ADOES THE PATIENT HAVE ASTHMA?
• Rhinosinusitis/nasal polyps• Gastroesophageal re�ux • Obstructive sleep apnea• Vocal cord dysfunction• Allergic bronchopulmonary aspergillosis• Eosinophilic granulomatosis with polyangiitis
• Obesity• Psychological factors (personality, depression, anxiety)• Drug side e�ects aspirin, NSAIDs, beta-blockers, ACE inhibitors• Aspiration
Diagnose and manage comorbidities
IS ASTHMA STILL UNCONTROLLED, DESPITE TREATMENT WITH HIGH-DOSE ICS + LABA AND A NON-BIOLOGIC ADD-ON THERAPY?
B EVALUATE COMORBIDITIES AND COMPLICATING FACTORS
NO
YES
DCONSIDER ADDING A NON-BIOLOGIC THERAPY• Tiotropium• Leukotriene modi�er• Theophylline
• Macrolide antibiotic• Oral corticosteroid (short course)
YES
C IS ASTHMA UNCONTROLLED, DESPITE STEPPING UP TO A HIGH-DOSE ICS+LABA?Asthma is uncontrolled when any 1 of the 4 criteria below is present: Poor symptom control ACQ >1.5, ACT < 20, or per GINA/NAEPP guidelines Systemic corticosteroids ≥ 2 bursts for asthma exacerbations in the past year Hospitalizations ≥ 1 hospitalization for asthma in the past year Pulmonary function FEV1 < 80% predicted when not taking short- or long-acting bronchodilators
F
• Con�rm variable air�ow limitation: review/repeat pulmonary function tests with bronchodilator • Consider methacholine or exercise challenge tests if spirometry inconclusive and clinical response to treatment is absent or limited• Exclude other conditions (eg, airway tumor, foreign body, COPD, bronchiectasis, vocal cord dysfunction, CF, aspiration)
Navigating Asthma Control A Severe
Asthma Roadmap
Address environmental factors• Allergen exposures (indoor, outdoor, pets)• Occupational exposures• Respiratory infections (eg, viruses)• Second-hand cigarette smoke• Tra�c-related pollution• Respiratory irritants
Asthma education and health maintenance
eating healthyvaccinationsmoking cessationexercise
Consider safety and potential e�ects of long-term oral corticosteroids (OCS) 1. Counsel patients about long term e�ects of OCS2. Optimize chronic OCS dose (establish current dose is truly needed)3. Use objective criteria to control taper (PEF, symptoms score, SABA use)4. Counsel patients regarding symptoms of adrenal insu�ciency and steroid withdrawal (”go slow when low”)5. Manage steroid related adverse e�ects
RxCaution
Evaluate Adherence and Optimize Inhaler Technique• Use a shared-decision making approach to select treatment• Choose best device for patient and individualize education• Assess barriers to proper medication use • Assess knowledge and attitudes about medication• Educate patient about strategies to reduce side e�ects• Check and correct inhaler technique at each visit
!
YES
This reference aid was developed as part of an educational activity supported by independent educational grants from AstraZeneca Pharmaceuticals LP, GlaxoSmithKline and Novartis Pharmaceuticals Corporation.
ReferencesGlobal Initiative for Asthma (GINA) Global Strategy for Asthma Management and Prevention. 2019. www.ginasthma.org | US National Heart, Lung, and Blood Institute (NHLBI) National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. 2007. www.nhlbi.nih.gov/�les/docs/guidelines/asthgdln.pdf | Chung KF, et al. International ERS/ATS guidelines on de�nition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343-7 | Israel E, Reddel HK. Severe and di�cult-to-treat asthma in adults. N Engl J Med. 2017;377(10):965-976. | Wechsler ME. Getting control of uncontrolled asthma. Am J Med. 2014;127(11):1049-59 | Bousquet J, et al. Care pathways for the selection of a biologic in severe asthma. Eur Respir J. 2017;50(6). | Chipps BE, et al. Asthma Yardstick: Practical recommendations for a sustained step-up in asthma therapy for poorly controlled asthma. Ann Allergy Asthma Immunol. 2017;118(2):133-142 | Volmer, T. E�enberger, T. Trautner, C. & Buhl, R. Consequences of long-term oral corticosteroid therapy and its side-e�ects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J. 2019;52:1-12.
NO
Close follow-up.
Reduce treatment intensity after at
least 3–6 months of stable, good
control
Non-Type 2Neutrophilic airway
in�ammation or Paucigranulocytic
Biomarkers No T2 biomarkers
• Blood eosinophil <150 µL AND• FeNO < 20 ppb AND• Sputum or BAL eosinophil < 2%
ORIf sputum BAL neutrophils also < 40-60% = pauciinflammatory
Associated Phenotypes• Obesity• Smoking History• Infections• Lack of response to corticosteroids
Anti-IgE Omalizumab Anti-IL-5 Mepolizumab, Reslizumab Anti-IL-5Rα Benralizumab Anti-IL-4Rα/13 Dupilumab
Anti-IgE Omalizumab Anti-IL-4Rα/13 Dupilumab
Allergic Eosinophilic Asthma
Anti-IL-4Rα/13 Dupilumab• Atopic Dematitis
Anti-IgE Omalizumab• Chronic Idiopathic Urticaria
Anti-IL-4Rα/13 Dupilumab*• Chronic Rhinosinusitis and Nasal Polyps
Allergic Noneosinophilic Asthma
Anti-IL-4Rα/13 Dupilumab*
OCS Dependence
Eosinophilic Asthma who:• Are nonallergic OR• Do not respond to anti-IgE treatment OR• Are out of dosing range for anti-IgE treatment
Type 2IL-4, IL-5, IL-13 or IgE mediated
in�ammation with high eosinophils or FeNO
Biomarkers • Blood eosinophils > 150 µL• FeNO > 20 ppb• Sputum or BAL eosinophils > 2%• Elevated IgE
Associated Phenotypes • Early age onset• History of allergies• Chronic Rhinosinusitis/Nasal Polyps
Anti-IL-5 Mepolizumab, Reslizumab Anti-IL-5Rα Benralizumab Anti-IL-4Rα/13 Dupilumab
Select Add-on Biologic Therapy
Considerations for Related Type 2 Phenotypes
Consider patient preference factors related to route/frequency/location of administration and cost.
Close follow-up.
Reduce treatment intensity after at
least 3–6 months of stable, good
control
NO
- Weight loss- Bariatric surgery- Macrolide antibiotics- Bronchial Thermoplasty
† Consider experimental therapy from clinical trials with Anti-TSLP, Anti-IL-6, Anti-IL-17 or other drugs in development.
- Secretion clearance- Pulmonary rehabilitation
Treatment
*While Dupilumab has the FDA indication for OCS dependence, both Mepolizumab and Benralizumab have shown e�cacy.
Type 2 patients with: