-
Non-communicable diseasesA global overviewDavid Leon
-
*OutlineDefinition Non-communicable disease mortality
worldwideThe Epidemiological TransitionGlobal Burden of Disease
StudyMajor risk factorsBlood pressureCholesterolSmokingInfection
and non-communicable diseases
-
*What are non-communicable diseases?
-
*Classifying deaths and diseases(WHO)Communicable diseases
[Group I]Those where death is directly due to the action of a
communicable agentNon-communicable diseases Diseases [Group
II]Cancer, diseases of various organ systems (eg respiratory,
cardiovascular etc.), diabetes, mental health etc.External causes
(injuries, poisonings and violence) [Group III]
-
*Importance of non-communicable diseases mortality
-
*A global problemIn 2004 there were 59 million deaths
world-wideNon-communicable diseases accounted for 60% of these
deaths and injuries and violence 10%. By 2020 it is estimated that
non-communicable disease will account for 73% of all deathsGBD 2004
Update, 2008
-
*The epidemiologic transition(Omran, 1971)Change in the balance
of disease in a population from communicable diseasesto
non-communicable disease
-
*Decline in proportion of total mortality due to infectious
diseases
England & Wales, 1911-94, by age
-
*Different countries at different stages of the epidemiological
transition
-
*Non-communicable diseases as % of all deaths by global region
(all ages)
WORLDWIDE59%N.America; W Europe88%China, W Pacific, + some SE
Asia75%Latin America + Caribbean67%S E Asia including
India51%Sub-Saharan Africa21%
-
*Urbanisation
-
*http://www.indiaimages.com/street/street_life2_large.jpg
-
*Urbanisation
-
*Drivers of the epidemiological transition in low and middle
income countriesPopulation ageingMajor socio-economic changes
(especially urbanisation)changes in risk factors such as diet,
physical activity, smoking etc.
-
*Global Burden of Disease (GBD) Study
-
*GBD 2001 mortality estimates107 countries had collected useable
information on cause of death from registration systems55 countries
(42 in sub Saharan Africa) no information on adult
mortalityEstimates based on many assumptions and extrapolations
-
*Global Burden of Disease StudyFirst GBD study started in 1992
by World Bank.Second GBD study (in collaboration with WHO)
conducted 2001Extensive synthesis of all available data to give set
of mortality estimates by age, sex, region and cause worldwide for
the first time2001 GBD study covers 135 causes of death, 17
sub-regions, based on aggregation of country-level information
-
Global Burden of Disease2004 Update (published
2008)http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf*
-
Distribution of deaths in the world by sex, 2004*GBD report 2004
update, 2008
-
Mortality rates among men and women aged 1559 years, region and
cause-of-death group, 2004*GBD report 2004 update, 2008
-
Projected global deaths for selected causes, 20042030*GBD report
2004 update, 2008
-
Effect of key risk factors on mortality*
-
Combining data Prospective studies collaboration *
-
Prospective Studies Collaboration Established chiefly to
investigate associations of blood pressure and cholesterol with
cause-specific mortality
Individual data on 900 000 participants without any previous
history of vascular disease from 61 prospective cohort studies
55 000 vascular deaths (34 000 ischaemic heart disease [IHD], 12
000 stroke, 10 000 other)
-
Blood pressure and cardiovascular mortality*
-
December 02*
Cardiovascular mortality: Age-specific effects for 20mmHg lower
usual SBP55 345 deaths at ages 40-89
*
-
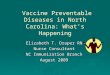
Cholesterol and cardiovascular mortality*
-
80-8970-7960-6950-5940-49Age
atriskUDV3:[VEP.PSC.FIGURES.TCHOL.240907]ihd-by-agesex-hettrend.ctrl:
24-SEP-2007 14:47:08.14 Usual total cholesterol
(mmol/L)4050607080051248163264128256Hazard ratio( 95% CI)Ischaemic
Heart Disease mortality (33 744 deaths) and total cholesterol
-
Different for stroke*
-
UDV3:[VEP.PSC.FIGURES.TCHOL.240907]stroke-by-agecause-trend.ctrl:
24-SEP-2007 14:47:18.56 Usual total cholesterol
(mmol/L)4050607080124816326480-89 70-79 60-69 40-59 Age Hazard
ratio(& 95% CI)Stroke mortality (11 663 deaths) and total
cholesterol by age
-
*Smoking
-
*% of deaths aged 35-69 years attributable to smoking in
2000Source : http://www.deathsfromsmoking.net/
MenWomenBelarus33%0%Russia33%3%Ukraine32%3%Central Asia
(8)23%4%Estonia31%3%Latvia30%2%Lithuania29%0%United
Kingdom25%21%Germany29%11%
-
*Risk of myocardial infarction increases with every single
cigarette smoked per dayNumber of cigarettes smoked per dayOdds
Ratio of Myocardial InfarctionNever 1-2 3-4 5-6 7-8 9-10 11-12
13-14 15-16 17-18 19-20 >=21Source : K. K. Teo et al Tobacco use
and risk of myocardial infarction in 52 countries in the INTERHEART
studyLancet 368 (9536):647-658, 2006.INTERHEART study 52 countries
12 461 cases, 14 637 controls
-
*Smoking causes more deaths from cardiovascular disease than
cancerDeaths attributed to smoking among men (all ages) in Russia,
2000
All cancers = 77,000
Cardiovascular disease = 148,000Source :
http://www.deathsfromsmoking.net/
-
*Things are getting worse not better
-
*Smoking in men in Russia is not decliningRuralUrbanSt
Petersburgh/MoscowSource : Perlman et al Tob.Control 16
(5):299-305, 2007Russian Longitudinal Monitoring Survey
-
*Smoking in women in Russia is increasingRuralUrbanSt
Petersburgh/MoscowRussian Longitudinal Monitoring SurveySource :
Perlman et al Tob.Control 16 (5):299-305, 2007
-
Giving up smoking reduces risk*
-
*
-
Some non-communicable diseases have infectious etiology*
-
Trends in stomach cancer mortality*Source : WHO HFA databaseAge
standardised mortality per 100,000
Chart1
198013.2132.5529.2532.9946.45198017.65
198112.7431.9628.2829.4445.53198117.05
198212.0130.5826.929.6745.34198216.19
198311.8629.3926.5728.7744.69198316.38
198411.6428.0126.1329.4643.6198415.94
198510.8126.072528.6341.88198515.23
198610.725.924.1927.1641.21198614.63
16.5910.0124.7923.927.1640.7710.5914.35
15.699.9924.822.9726.8439.9410.2714.07
15.469.2224.2821.8126.8838.899.8513.37
13.669.0324.3621.1826.7538.429.6612.76
13.158.4723.6720.2324.7737.379.4412.21
11.858.1423.5219.9224.8636.58.8511.88
12.048.0222.6918.9523.535.678.1710.79
11.187.4922.0718.3322.134.428.1110.79
10.567.2721.0717.8822.8733.317.189.97
10.57.0619.2916.9721.4431.647.269.51
10.26.7919199720.6230.427.429.15
8.916.8418.91199819.6529.726.628.95
8.376.5918.0115.3920.0329.246.798.45
8.226.2916.7715.2119.4528.246.162000
8.026.0516.5114.6318.6727.266.277.65
8.046.0316.0714.317.9626.136.147.4
7.625.6915.3413.8517.1825.6820036.93
7.66200414.3813.3616.4825.0920046.67
7.43200512.82005200524.120052005
Finland
France
Hungary
Poland
Portugal
Russian Federation
Sweden
United Kingdom
Sheet1
Column1Column2
YearsFinlandFranceHungaryPolandPortugalRussian
FederationSwedenUnited Kingdom
198013.2132.5529.2532.9946.4517.65
198112.7431.9628.2829.4445.5317.05
198212.0130.5826.929.6745.3416.19
198311.8629.3926.5728.7744.6916.38
198411.6428.0126.1329.4643.615.94
198510.8126.072528.6341.8815.23
198610.725.924.1927.1641.2114.63
198716.5910.0124.7923.927.1640.7710.5914.35
198815.699.9924.822.9726.8439.9410.2714.07
198915.469.2224.2821.8126.8838.899.8513.37
199013.669.0324.3621.1826.7538.429.6612.76
199113.158.4723.6720.2324.7737.379.4412.21
199211.858.1423.5219.9224.8636.58.8511.88
199312.048.0222.6918.9523.535.678.1710.79
199411.187.4922.0718.3322.134.428.1110.79
199510.567.2721.0717.8822.8733.317.189.97
199610.57.0619.2916.9721.4431.647.269.51
199710.26.791920.6230.427.429.15
19988.916.8418.9119.6529.726.628.95
19998.376.5918.0115.3920.0329.246.798.45
20008.226.2916.7715.2119.4528.246.16
20018.026.0516.5114.6318.6727.266.277.65
20028.046.0316.0714.317.9626.136.147.4
20037.625.6915.3413.8517.1825.686.93
20047.6614.3813.3616.4825.096.67
20057.4312.824.1
-
*Helicobacter pylori bacterium - a causal factor for stomach
cancer
-
*Marshall BJ,.Warren JR. Unidentified curved bacilli in the
stomach of patients with gastritis and peptic ulceration. Lancet
1984;1:1311-5.Marshall BJ, Armstrong JA, McGechie DB, Glancy RJ.
Attempt to fulfil Koch's postulates for pyloric Campylobacter.
Med.J.Aust. 1985;142:436-9.
The Helicobacter pylori story ...
-
SummaryNon-communicable diseases are now the most common cause
of death world wideIncreasing rates in low and middle income
countries because of change in lifestyles (urbanisation)Key risk
factors have very large effectsInterventions are effective and can
reduce burdenThe need to combine results and have large
studies*
**Here we see the decline over time in the proportion of
mortality at different ages attributable to infections ranging from
tuberculosis to diuphtheria, measles and gastro-intestinal
infections. The downward spike in 1918 is because most excess
deaths were from pneumonia rather than influenza. Rates of
pneumonia were much lower than those for infectious diseases either
side of the 1918 Spanish flu making up less than 10% of all deaths
among those aged The sharp decline mid-century is not well
understood and is under-researched. The precise role of the
introduction and use of anti-biotics is important question..
Mackenbachs work suggesting that this played a role in the
Netherlands at least.With the decline of infectious diseases
life-expectancy in particular becomes more strongly related to the
influence of individual behaviours. This is apparent with the
widening gap in male to female life-expectancy over the 20th
Century which rose from 4 years in 1900 to a peak of just over 6
years in the late 1960s.
http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf
*The Prospective Studies Collaboration is a collaborative
meta-analysis combining data from existing prospective
observational studies that recorded both blood pressure and blood
cholesterol at baseline and that followed participants for
cause-specific mortality. Investigators from around the world have
collaborated to combine data from 61 existing prospective studies
involving a total of one million participants from Europe, North
America, Australia, Israel, China and Japan. During 12.7 million
person-years of follow-up there were 120000 deaths involving more
than 55000 vascular deaths (12000 stroke, 34000 ischaemic heart
disease [IHD], 10000 other vascular) and more than 65000 other
deaths.PSC: Age-specific relevance of usual blood pressure to
vascular mortalityLancet 2002; 360:1903-13*Figure 1(a): IHD
mortality (33 744 deaths) versus usual total cholesterol.
Age-specific associationsThe hazard ratios are plotted on a
floating absolute scale of risk (so each log hazard ratio has an
appropriate variance assigned to it.
NOTES: 1 mmol/L lower total cholesterol was associated with
about a half , a third and a sixth lower IHD mortality in both
sexes at ages 40-49, 50-69 & 70-89, respectively, throughout
the main range of cholesterol in most developed countries, with no
apparent threshold.Although the proportional differences in risk
decrease with age, the absolute effects of cholesterol on annual
IHD mortality rates are much greater at older than at younger ages.
For example, the absolute difference in the annual risk of IHD
death for a 1 mmol/L difference in total cholesterol was about 10
times greater at 80-89 than at 40-49 years of age. Figure 4(a).
Stroke mortality (11 663 deaths) versus usual total cholesterol.
Age-specific associations for total stroke.Conventions as in figure
1(a).
NOTES: There was a weak positive association between total
cholesterol and total stroke mortality at ages 40-59 years, but
little association at older ages. When the MRFIT and PSC findings
were combined (table 2, webfigure 7), there was a weak positive
association with total stroke at ages 40-59 and 60-69 years, but
not at older
ages.http://www.deathsfromsmoking.net/*http://www.deathsfromsmoking.net/**