Embed Size (px)
Citation preview
VICSERV
TRAINING NEEDS
ANALYSIS REPORT
2010
Acknowledgements
Glossary
ExecutiveSummary
MethodologyKeyfindings
Recommendations
SECTION1Introduction
ObjectivesOverviewPsychiatricDisabilityRehabilitationandSupport(PDRS)inVictoriaPsychiatricDisabilityServicesofVictoria(Vicserv)Strategiccontext
SECTION2Methodology
OverviewNotesontheprocess
SECTION3Findings
Overview
SECTION3.1DevelopmentneedsforPDRSsupportworkers
CriticaldevelopmentneedsrelatedtoperformancebenchmarksandstrategicprioritiesAdditionalcriticaldevelopmentneedsTrainingprioritiesPreferencesformeetingdevelopmentneedsSupportingevidenceofdevelopmentneedsfromotherrecentstudies
04
05
06
08
09
16
14
18
VICSERV TRAININGNEEDSANALYSISREPORT•2010
CONTENTS
The Training Needs Analysis Reportispublishedby
PsychiatricDisabilityServicesofVictoria(VICSERV)Level2,22HorneStreet,ElsternwickVictoria3185AustraliaT0395197000,[email protected]
EditorsSueDurham,TrainingManagerJohnKatsourakis,DevelopmentManager,TrainingKristieLennon,ResourcesCoordinator
CopyrightAllmaterialpublishedinthisreportiscopyright.Organisationswishingtoreproduceanymaterialcontainedinthisreportmayonlydosowiththepermissionoftheeditors.
DesignedbyStudioBinocular
02
SECTION4Recommendations
SECTION5Bibliography
SECTION6Appendices
Appendix1:Literaturereview
Appendix2:Summariseddevelopmentneedsmappedtojobfunctionsforsupportworkers
Appendix3:Profileofthesupportworker
Appendix4:Profileofthemanager
Appendix5:DevelopmentcurrentlyavailabletothePDRSsector
32
36
37
45
53
31
SECTION3.2DevelopmentneedsforPDRSmanagers
CriticaldevelopmentneedsrelatedtoperformancebenchmarksandstrategicprioritiesAdditionalcriticaldevelopmentneedsTrainingprioritiesPreferencesformeetingdevelopmentneeds
SECTION3.3Trainingcurrentlyavailabletomeetdevelopmentneeds
GapsinexistingtrainingcoverageStructuralissuesDisincentivesDesignissuesOpportunitiesforaddressingissues
SECTION3.4Workforcesustainabilityissuesrelatedtodevelopmentneeds
22
25
27
28
30
CONTENTS 03
ThisreportwouldnothavebeenpossiblewithoutthevaluedcooperationandeffortofVictoria’sPsychiatricDisabilityRehabilitationandSupport(PDRS)servicesectororganisationsandindividualrespondentsacrossthestate.VICSERVandtheCommunityServices&HealthIndustryTrainingBoard(CS&HITB)wouldliketoexpresstheirappreciationtoallwhotookthetimeandefforttoparticipateandgivetheirvaluableinsightsandassessments.
TheprojectteamwouldalsoliketothankmemberswhoprovidedinputandadviceontheTrainingNeedsAnalysis’structureandcontentincluding:
•VICSERVTrainingAdvisoryGroup•DepartmentofHealth(formerlyDepartmentofHumanServices)•SouthernMentalHealthAssociation(ReachOutMentalHealth)•HealthCareChaplaincyCouncilofVictoria•NeamiLimited•AnxietyRecoveryCentre•HomeGroundServices•MindAustralia•SNAPGippsland•StLuke’sAnglicare
•BallaratCommunityHealthCentre•WimmeraUnitingCare•CentacareBallarat•GippslandAccommodationRehabilitationSupportService•ERMHA•ARAFEMI•MentalIllnessFellowshipVictoria•PrahranMission•InnerEastMentalHealthServicesAssociation
Inaddition,VICSERVwouldliketoacknowledgethefundingandassistanceprovidedbytheSectorQuality&WorkforceDevelopmentUnit,MentalHealth&DrugsOperationsBranch,DepartmentofHealthandtheMentalHealthCouncilofAustralia.
ThekeycontributorstothisreportwereJacquieO’Brien,GeoffSheehanandCindyCurranfromtheCS&HITBwithextensiveassistancefromSueDurhamandJohnKatsourakisfromVICSERV,andGregoryEvansfromHypatiaConsulting.
ACKNOWLEDGEMENTS
VICSERV TRAININGNEEDSANALYSISREPORT•2010 404
GLOSSARY/ACKNOWLEDGEMENTS
CALDCulturallyandLinguisticallyDiversereferstoindividualpeople,communitiesorpopulationswhohaveaspecificculturalorlinguisticconnectionthroughbirth,ancestryorreligion
ClinicalsectorVictoria’sstate-fundedclinicalmentalhealthservicesareknownasAreaMentalHealthServices(AMHS)astheyaredeliveredonthebasisofadistinctgeographiccatchmentarea.EachAMHSprovidesarangeofcommunitybasedservicesandinpatientfacilitiesforpeoplewhoareacutelyunwell
ConsumerApersonwhoisexperiencing,orhasexperienced,amentalillness,whoreceivessupportfrompsychologicalorPDRSservicesorhasarelationshipwiththeservicewheretheyaregivenachoiceintreatmentandhavesomeinfluenceonservicedelivery
DevelopmentneedsDevelopmentneedsexistwhenthereisadeficitbetweentheskillsandknowledgerequiredtoperformajobtothebenchmarkstandard,andthe
employee’sactuallevelsofskillandknowledge.Developmentneedsmaybeaddressedbytraining,coaching,specificworkassignments,mentoring,performancesupporttoolsandrelatedactivities
ManagerAnindividualperformingamanagementand/orleadershiprolewithinaPDRSserviceprovider
PDRSPsychiatricDisabilityRehabilitationandSupport
SupportworkerAnindividualemployedtoprovidedirectcareorsupporttoapersonwithapsychiatricdisability
TNATrainingNeedsAnalysis
VICSERVPsychiatricDisabilityServicesofVictoriaInc.(VICSERV)
GLOSSARY
05
The Victorian PDRS sector is undergoing considerable and rapid growth in response to consumer demand and government directions for improving the care of people affected by, or at risk of, mental illness.
TheDepartmentofHumanServices’Because mental health matters: Victorian mental health reform strategy 2009–2019,recognisesthatPDRSserviceswillbe‘atthecentreofthementalhealthservicesystem,’1andthereforetheneedtobuildthecapacityandexpertiseofthePDRSsectortomeetincreasingdemand.
Inresponse,Shaping the future: The Victorian mental health workforce strategy, 2009,outlinesarangeofstrategicinitiativestodevelopthePDRSsectoraccordingly.Theseactionsinclude:
• ProfilingthecapabilitiesrequiredbythePDRSworkforce
• CreatingmoreattractiveopportunitiesforgraduateentrytothePDRSroles
• EstablishingaMentalHealthEducationandTrainingInstitute
• Supportingleadershipdevelopment
• MakingbetteruseoftheCertificateIVinMentalHealth,CommunityServicestrainingpackage.2
ThisTNAwascommissionedtosupporttheseinitiativesbyproviding:
• Reliable,comprehensivedataontheVictorianPDRSsectorworkforce’scurrentcapabilities
• AnassessmentofthePDRSsectorworkers’traininganddevelopmentneeds
• Recommendationstoaddresssignificanttraininganddevelopmentneeds.
The methodology for the TNA involved:
1 Clarifyingtheobjectivesandcontextfortheanalysisbyinterviewingkeystakeholdersandreviewingrelevantliterature
2 Identifyingappropriateperformancestandardsagainstwhichtrainingneedscouldbeassessed
3 Conductingasurveyof231respondents(165supportworkersand66managers)toobtainaself-assessmentofcapabilityagainsteachperformancestandardandtheimportanceofthestandardinrelationtoworkperformance
4 Ananalysisofthecollatedsurveydata
5 ValidationofinitialfindingsandrecommendationsthroughconsultationwithseniorPDRSstakeholders
6 Documentingandreportingoffindingsandrecommendations.
Methodology
References
1 DepartmentofHumanServices,(2009),Becausementalhealthmatters:Victorianmentalhealthreformstrategy2009–2011,MentalHealthandDrugsDivision,DHS,Melbourne
2 DepartmentofHealth,(2009),ShapingtheFuture,TheVictorianMentalHealthWorkforceStrategy,FinalReport,DoH,Melbourne,p5
EXECUTIVESUMMARY
VICSERV TRAININGNEEDSANALYSISREPORT•2010 06
07
Support workers
• BaselinefoundationskillsforPDRSworkers
•ASISTplusFirstAidskills
• Workingwithfamilies–takingafamily-centredapproach
• Physicalhealth,housingandeconomicparticipation
•Workersafety
•Peerworker
•Recovery
•Earlyintervention
•Understandingtrauma
•Workingwithyoungpeople
• Workinginpartnershipswithotherservices
•WorkingwithCALDclients
•Rightsandresponsibilitiesofclients
•Crisispreventionandintervention
• Monitoringandmanagingtheadverseaffectsofphysicalhealth,medicationandothermedicaltreatments
•Supportingfamilymembersandchildren
•Dualdiagnosis
Managers
•Managingchange
•Reflectivepractice
•Applyingqualityprinciples
• Applyingdataandoutcomemeasurementstoimproveservicesdelivery
•Legislativecompliance
• Managingcomplexstakeholderissuesthatareintegraltothechangeprocess
•Writingtendersandsubmissions
• Developingandmanagingcomplexbudgets
• Interpretingstateandfederalpolicyandplans
Keyfindings
EXECUTIVESUMMARY
The following points outline the highest priority development needs for the PDRS workforce: The following indicates other critical training and development-related needs:
•TherearegapsintheexistingtrainingavailabletotheVictorianPDRSsector,particularlyforsupportworkers.Thesegapsincludeworkingwithfamilies,earlyintervention,workingwithyoungpeople,peerworkerandhealth.
•UndergraduatetrainingformentalhealthworkersdoesnothaveadequatecoverageofPDRSphilosophyandapproachestoprovidingservices.
•Allsurveyrespondentsindicatedastrongpreferenceforface-to-facetraininganddevelopment,andexpressedconsiderableenthusiasmforaccreditedtraining.Onlinetraininganddevelopmentwasnotthepreferredtrainingdeliverymedium.
•TherearestructuralissuesconcerningthesupplyanddemandofPDRStraining:
SomePDRSservicesareunabletomakeuseofmany,muchneeded,availabledevelopmentopportunitiesduetolackofresourcing.
Therearebarrierstoparticipationinfoundationskillstraining,includingduration,availabilityandfinancialdisincentivesforPDRSworkerswithhigherqualifications.
•Currentworkforcesustainabilityissuesthreatentoundermineanyinvestmentintraininganddevelopment.Forty-sevenpercentofsurveyrespondentsindicatedtheyareconsideringand/orplanningtoleavethesector.
SOMEPDRSSERVICESAREUNABLETOMAKEUSEOFMANY,MUChNEEDED,AVAILABLEDEVELOPMENTOPPORTUNITIESDUETOLACKOFRESOURCING.
08
The following recommendations have been developed through a consideration of the findings, and are aligned with the strategic actions outlined in The Department of Health’s Shaping the Future: The Victorian Mental Health Workforce Strategy, 2009:
1 Conductastudytoidentifystrategiesforaddressingrecruitment,retentionandcareerpathwaychallenges,andothermattersrelatedtoworkplacesustainabilityfactors.
2 VICSERVtoprovideinputonthePDRSsectorphilosophyandapproachestoundergraduatetrainingproviders.
3 OfferunitsofaccreditedtrainingbeyondthePDRSsectortosupporttheneedtoimproveworkinginpartnershipswithotherservices.(VICSERVhastrainingthatisofsignificantvaluetootherservices.)
4 Offerskill-setstrainingtoparticipantsotherthanthoseundergoingaccreditedtraining.
5 BuildthecapacityoftheregionalPDRStrainingworkforcetocatertothestrongpreferenceforlocal,face-to-facedevelopment.
6 Examinethefeasibilityofprovidingappropriateonlinelearning,aspartofablendeddevelopmentstrategy.Thefeasibilitystudyshouldincludeexaminingcosts,accessibilityandthebestuseofavailableresources.ThismayincludeapproachingtheNationalMentalHealthProfessionalOnlineDevelopment(MHPOD)projectfortheuseand/oradaptationofrelevantonlineresources.
7 VICSERVtoundertakefurtheractivitiestosupport:
• Facilitationofqualificationpathways
• Avenuesforskillsrecognitionandflexiblecoursedeliveryshouldbeenhanced
• Professionalopportunitiesforworkerswhoareatanintermediate/advancedskilllevel.
8 VICSERVtocontinuetooffertheDiplomaofManagement,SupervisionandQualitytraining.
9 Identifyriskmanagementrequirementsformanagersandprovidedevelopmentaccordingly.
10 VICSERVmaybewellsituatedtoprovideleaderswhoarenewtoseniorpositionsinthePDRSsector(suchasCEOsndgeneralmanagers)withorientationtotheirroles.
11 ObtainfundingexemptionsforCertificateIVparticipantspossessinghigherqualificationswhootherwisewouldn’tqualifyforfunding.
12Obtainfundingtoincreasethescopeofthefoundationskillspackagetoinclude:
• Workingwithfamilies
• Earlyintervention
• Workingwithyoungpeople
• Peerworker
• Health
13 IdentifystrategiestoenablePDRSservicestomakebetteruseofthedevelopmentopportunitiesavailabletothem.ThismayrequireadeeperanalysisofthestructuralissuesinthesupplyanddemandforPDRStraininginVictoria.
RECOMMENDATIONS
VICSERV TRAININGNEEDSANALYSISREPORT•2010

The objectives of the PDRS Training Needs Analysis are to:
1 IdentifytrainingneedsforthePDRSsectorinVictoria
2 PrioritisetrainingandrelatedneedsforthePDRSsectorinVictoria
3 Identifyrealisticactionstoaddresstheprioritisedtrainingneeds.
This section provides context for the Training Needs Analysis. It comprises information on:
• PsychiatricDisabilityRehabilitationandSupportinVictoria
• PsychiatricDisabilityServicesofVictoriaInc.(VICSERV)
•Strategiccontext:
SupplyanddemandintheVictorianPDRSsector
StrategicdirectionsfortheVictorianPDRSsector
StrategicactionstosupporttheVictorianPDRSsector
ATNAtoinformstrategicdecision-making
Objectives Overview
SECTION1•VICSERVTRAININGNEEDSANALYSISREPORT2010
INTRODUCTION–
10
PsychiatricDisabilityRehabilitationandSupport(PDRS)inVictoria
PsychiatricDisabilityServicesofVictoria(VICSERV)
Victoria has a strong tradition of PDRS service provision by the non-government sector.
PDRSserviceprovisionisaspecialistfunction,underpinnedbyacommitmenttotheprinciplesofpsychosocialrehabilitationandaphilosophyofprovidingprogramsforpeoplewithpsychiatric
disabilities.Theseservicesarenotavailablethroughgenericcommunityservices.
PDRSservicesassistclientstoregainordevelopskillstheyneedinordertoactivelyparticipateindailylife,inpersonalandsocialinteractionsandincommunitylifeandactivities.
VICSERV is a membership-based organisation and the peak body representing community-managed mental health services in Victoria.
VISION
VICSERVenvisagesasocietywherementalhealthandsocialwellbeingareanationalpriorityand:
• Everyonehasaccesstotimelymentalhealthtreatmentandsupport
•Mentalhealthservicesarerecoveryoriented
• Peopleparticipateindecision-makingabouttheirownlivesandtheircommunity
• Peopleaffectedbymentalillnesshaveaccessto,andafairshareof,communityresourcesandservices
• Allpeopleareinvolvedasequals,withoutdiscrimination
MISSION
Asthepeakbodyforthecommunity-managedmentalhealthsectorinVictoria,VICSERVpursuesthedevelopmentandreformofmentalhealthservices.
VICSERVsupportsmembersby:
•Promotingrecoveryorientedpractice
•Buildinganddisseminatingknowledge
•Providingleadership
•Buildingpartnershipsandnetworks
• Undertakingworkforcedevelopment,trainingandcapacitybuilding
•Promotingqualityinservicedelivery
• Undertakingadvocacyandcommunityeducation
VALUES
•Collaboration
•Courage
• Inclusiveness
• Integrity
• Flexibility
VICSERV TRAININGNEEDSANALYSISREPORT•2010
SECTION1
INTRODUCTION
Strategiccontext
SupplyanddemandintheVictorianPDRSsector
ASThEPEAKBODYFORThECOMMUNITY-MANAGEDMENTALhEALThSECTORINVICTORIA,VICSERVPURSUESThEDEVELOPMENTANDREFORMOFMENTALhEALThSERVICES.
This section provides a brief account of factors influencing the availability of skilled workers in the PDRS sector, beginning with an overview of some of the forces that shape the market for PDRS services in Victoria, then providing an overview of the strategic directions for the Victorian PDRS sector.
TheneedforaTNAtoinformdecision-makingaroundhowbesttosupportthestrategicdirectionsisthenoutlined.
The PDRS sector is undergoing considerable and rapid growth in response to consumer demand and government directions for improving responses to people affected by, or at risk of, mental illness.
TheVictorianGovernmentiscommittedtostrengtheningandsupportingthePDRSsector,inrecognitionofitssuccessinpromotingintegrationandsupportingthesignificantnon-clinicalneedsofpeoplewithamentalillnessandtheircarers.
Crucialtothedevelopmentofthisservicesectorhasbeenthecommitmentofindividuals,groupsandorganisationstoadvocatefortherightsofpeoplewithpsychiatricdisabilitiesandimproveopportunitiesandconditionsforpeoplewithpsychiatricdisabilitieslivinginthecommunity.1
Forthepurposesofthisreport,psychiatricdisabilitiesaredefinedas‘theeffectsofamentalillness,whichtovaryingdegreesimpair
functioningindifferenceaspectsofaperson’slifesuchastheabilitytoliveindependently,maintainfriendshipsormaintainemployment.’2
Despitethisgoodwill,thePDRSworkforcehasinsufficientcapacityinitscurrentstatetomeetgrowthrequirementsorsupportthestrategicdirectionsofmentalhealthinVictoria.
ThedemandforPDRSserviceshasneverbeenhigher.Driversofdemandinclude:
•Theageingdemographicsofconsumers
• Theincreasinglycomplexissuesofconsumers
• Rapidchangesintherapies,technology,regulatoryregimesandrelatedmatters.
Atthesametime,supplyofskilledworkersisconstrainedby:
• Insufficientdevelopmentopportunities
•Anageingworkforce
• Lownumbersofqualifiedworkersenteringthesector
• Indistinctcareerpaths
• Relativelylowremunerationcomparedtotheclinicalsector,andtherelativewagedisparitybetweenthoseworkinginnot-for-profitorganisationscomparedtogovernmentorganisations.
Consequently,thereisacriticalneedforreliableevidencetoinformstrategicdecisionsconcerningthedevelopmentofthesector’scapabilityandcapacity.
References
1 DepartmentofHumanServices,(2004),Standardsforpsychiatricdisabilityrehabilitationandsupportservices,DHS,Melbourne,p3
2 DepartmentofHumanServices,(2009),Becausementalhealthmatters:Victorianmentalhealthreformstrategy2009–2011,MentalHealthandDrugsDivision,DHS,Melbourne,p161
INTRODUCTION 11
StrategicdirectionsfortheVictorianPDRSsector
The critical role of the PDRS sector is acknowledged in Because mental health matters: Victorian mental health reform strategy 2009–2019, which recognises that ‘community-based services will be at the centre of the mental health service system’1.
Undertheheadingof‘Abalanced,networkedservicesystem,’thefollowingstrategicdirectionsforthePDRSsectorareoutlined:
• Expectationthatoverthecomingyears,PDRSwillconsolidateitsroleandbecomeamoreequalpartnerwithspecialistclinicalservicesandacentralpartofthesocialinclusionthrustofreform
• Overtime,thiswillrequirecapacitybuildingandchangestostaffingprofiles.Asaresultofthesechangesandotherfactors,thenamePDRSmaynolongerbeadequate–anewnameemphasisingpsychosocialrecoverymightbemoresuitable
• TheneedforthePDRSsectortobemorecloselycoordinatedwithclinicalservices,withoutlosingitsdistinctiveapproach.Thiswillbeassistedbyjointplanning,professionaltraininganddevelopment,andsharedmanagementofsomeactivities
• Thesectorwillbesupportedandencouragedtobuildonthestrengthinitsdiversityandlocalfocus,whileworkingtobecomelessfragmentedandcleareraboutthescopeofitsactivities.Asoundevidencebaseshouldunderpineffectivepsychosocialsupportandsectordevelopment
• Thesectoriswellplacedtoplaystrongerrolesinawiderrangeofrehabilitationandintermediatestep-downcare(bothbedbasedandoutreachsupport),andincarecoordinationforconsumersneedingsustainedcareandsupport
• TherearealsoopportunitiesforthePDRSsectortobemoreactiveatthe‘frontend’ofthecarepathway,deliveringearlyinterventionsthathelpavoidtheneedforacuteservices.
VICSERV TRAININGNEEDSANALYSISREPORT•2010
SECTION1(CONT’D)
INTRODUCTION
12
StrategicactionstosupporttheVictorianPDRSsector
INTRODUCTION
‘COMMUNITY-BASEDSERVICESWILLBEATThECENTREOFThEMENTALhEALThSERVICESYSTEM’1.
The positioning of the PDRS sector at the centre of the mental health service system is reinforced in Shaping the Future: The Victorian Mental Health Workforce Strategy, 2009, which proposes a number of short- and medium-term strategies to support the development of the sector2, including:
1 Developandimplementashort-term(12-month)recruitmentstrategytargetingworkerswhowouldtransitionintothespecialistmentalhealthworkforcetofillexistingvacancies.ThiswillinvolveanonlineservicethatwillconnectpublicclinicalandPDRSopportunities.
2 UndertakeaworkforceresearchprojectforthePDRSsectorthatfurtherinvestigatestheworkforceprofile,analysesskillneedsandidentifiesstrategiestoaddressrecruitment,retentionandcareerpathwaychallenges.
3 Identifyanappropriate,structured,paidundergraduateemploymentmodeltoenhanceearlyexposuretothementalhealthenvironment.
4 Establishamentalhealtheducationandtraininginstitutethatsupportsmultidisciplinaryandcross-sectoralapproachestodeliveringfurthereducationandtrainingforclinicalandPDRSserviceworkers,consumersandcarers.
5 Developprograms(suchasscholarships,shadowing,mentoring)thatidentifyemergingleadersinclinical,PDRSandmanagerialsectors,andprovidetheseworkerswithmanagementandleadershiptrainingtobetterplaceorganisationstomeetchangingservicedemands.Providecoachingandmentoringtopromotehigh-qualityleadershipatalllevelswithinanorganisation.
6 InvestigatethefeasibilityofincreasedscopeofpracticeforPDRSworkersthroughtheutilisationoftheCertificateIVinMentalHealth,CommunityServicesTrainingPackage.
References
1 DepartmentofHumanServices,(2009),Becausementalhealthmatters:Victorianmentalhealthreformstrategy2009–2011,MentalHealthandDrugsDivision,DHS,Melbourne,p56
2 DepartmentofHealth,(2009),ShapingtheFuture,TheVictorianMentalHealthWorkforceStrategy,FinalReport,DoH,Melbournep5–6
13
Overview
SECTION2•VICSERVTRAININGNEEDSANALYSISREPORT2010
METhODOLOGY–
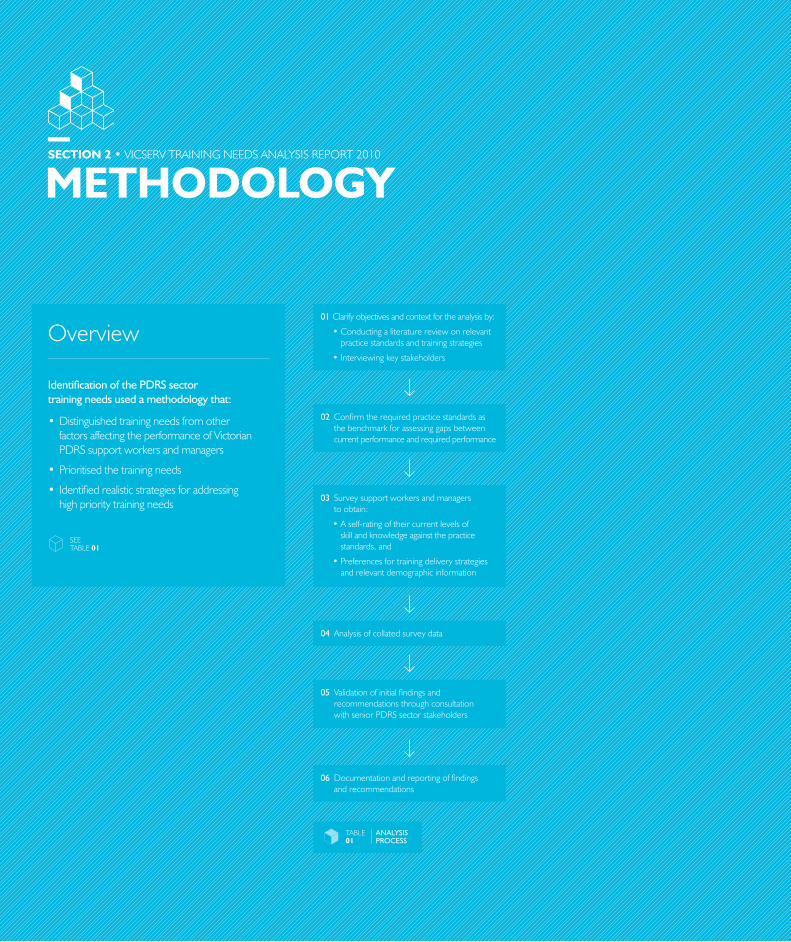
Identification of the PDRS sector training needs used a methodology that:
• DistinguishedtrainingneedsfromotherfactorsaffectingtheperformanceofVictorianPDRSsupportworkersandmanagers
•Prioritisedthetrainingneeds
• Identifiedrealisticstrategiesforaddressinghighprioritytrainingneeds
SEETABLE01
01 Clarifyobjectivesandcontextfortheanalysisby:
•Conductingaliteraturereviewonrelevantpracticestandardsandtrainingstrategies
•Interviewingkeystakeholders
02 Confirmtherequiredpracticestandardsasthebenchmarkforassessinggapsbetweencurrentperformanceandrequiredperformance
03 Surveysupportworkersandmanagerstoobtain:
•Aself-ratingoftheircurrentlevelsofskillandknowledgeagainstthepracticestandards,and
•Preferencesfortrainingdeliverystrategiesandrelevantdemographicinformation
04 Analysisofcollatedsurveydata
05 ValidationofinitialfindingsandrecommendationsthroughconsultationwithseniorPDRSsectorstakeholders
06 Documentationandreportingoffindingsandrecommendations
TABLE01
ANALYSIS PROCESS
METHODOLOGY
TRAININGNEEDSWEREIDENTIFIEDWhENSIGNIFICANTDEFICITEXISTEDBETWEENThESKILLSANDKNOWLEDGEREqUIREDTOPERFORMAjOBTOThEBENChMARKSTANDARD,ANDThEjOBhOLDERS’ACTUALLEVELSOFSKILLANDKNOWLEDGE.
Step 1
TheliteraturereviewandconsultationinStep1oftheprocessresultedintheuseoftheDepartmentofHumanServices’publicationStandards for Psychiatric Disability Rehabilitation and Support Services,2004,asthekeyinputtothetrainingneedsself-assessmentsurvey.AsynopsisoftheliteraturereviewisincludedasAppendix1ofthisreport.
Step 2
FocusgroupsofkeyPDRSserviceproviderswereconductedtorefinethestandardsintoappropriatesurveyitems,andtocontributetothedesignofthesurvey.Thesurveywasdevelopedforonlinecompletionusingbrowser-basedinterface.
SurveyitemswerebasedonperformancestandardsorjobfunctionsforthePDRSworkforce.
TheStandardsofPDRSserviceswerederivedfromtheNational Standards for Mental Health Services,19971.TheycontainelevenStandardsthatprovideguidanceforPDRSservicestomaintainafocusonservicequalitymeasurementandimprovement.
FromtheelevenStandards,38jobfunctionswerederivedforPDRSsupportworkers,andafurther38differentjobfunctionswerederivedforPDRSmanagers.Thesejobfunctionswereusedasthebenchmarksagainstwhichsupportworkersandmanagersratedthemselves.
ThejobfunctionsalsoalignwiththerelevantcompetencystandardsandassociatedqualificationsintheNationalCommunityServicesTrainingPackage.
Step 3
Atotalof231respondents(165supportworkersand66managers)fromallDHSregionsinVictoriaparticipatedinthesurvey.Thesurveygathereddataonrespondents:
•Demographicsandcareerinformation
•Trainingundertaken
•Perceivedadequacyoftrainingundertaken
• PerceptionsofthecriticalityofeachPDRSStandard
• PerceptionsoftheircompetenceforeachPDRSStandard
• Preferencesforarangeoftrainingmediaandrelatedmatters.
Step 4
Trainingneedswereidentifiedwhensignificantdeficitexistedbetweentheskillsandknowledgerequiredtoperformajobtothebenchmarkstandard,andthejobholders’actuallevelsofskillandknowledge.(ThebenchmarkjobstandardswerethejobfunctionsderivedinStep1.)
Forthepurposesofthisreport,developmentneedswereidentifiedwhen:
1 Asignificantnumber2ofthePDRSworkforcerespondentsratedthemselvesashavingskillandknowledgedeficits3inparticularbenchmarkstandards,and
2 Thejobfunctionswereconsideredessentialbyasignificantnumberofrespondents4.
TheresultswerevalidatedagainstthestrategicneedsofthesectorbyreviewsanddiscussionswithVICSERVandmemberorganisationmanagement.Additionaldevelopmentneeds,relatedtostrategicdirections,wereidentifiedduringthesediscussions.
Itbecameapparentthattrainingalonewouldnotbethemostappropriatesolutiontoaddressallskillandknowledgedeficits,sotheterm‘developmentneeds’wasadoptedforthepurposesofthisreport.
Thereportingofthedevelopmentneedswasseparatedintoneedsofsupportworkers,andneedsofmanagers.
Step 5
Thisstepinvolvedthevalidationofdraftfindingsandrecommendationsandfurtheranalysisoccurredthroughreviewsofthedraftreport,workshopsandfurtherinterviewswithseniorPDRSstakeholders.
Step 6
Thefindingsandrecommendationsweredocumentedandthereportwasfinalised.
Notesontheprocess
15

SECTION3•VICSERVTRAININGNEEDSANALYSISREPORT2010
FINDINGS–
Overview
The findings of this report are presented in the following structure:
3.1 CriticaldevelopmentneedsforPDRSsupportworkers:
•Summariseddevelopmentneeds
•Priorities
•Developmentpreferences
3.2 Criticaldevelopmentneeds
forPDRSmanagers:
•Summariseddevelopmentneeds
•Priorities
•Developmentpreferences
3.3Trainingcurrentlyavailabletomeetdevelopmentneeds
•Gapsincoverage
•Structuralissues
•Potentialopportunitiesforaddressingissues
3.4 Workforcesustainabilityissuesrelatedtodevelopmentneeds
16
SEETABLE02
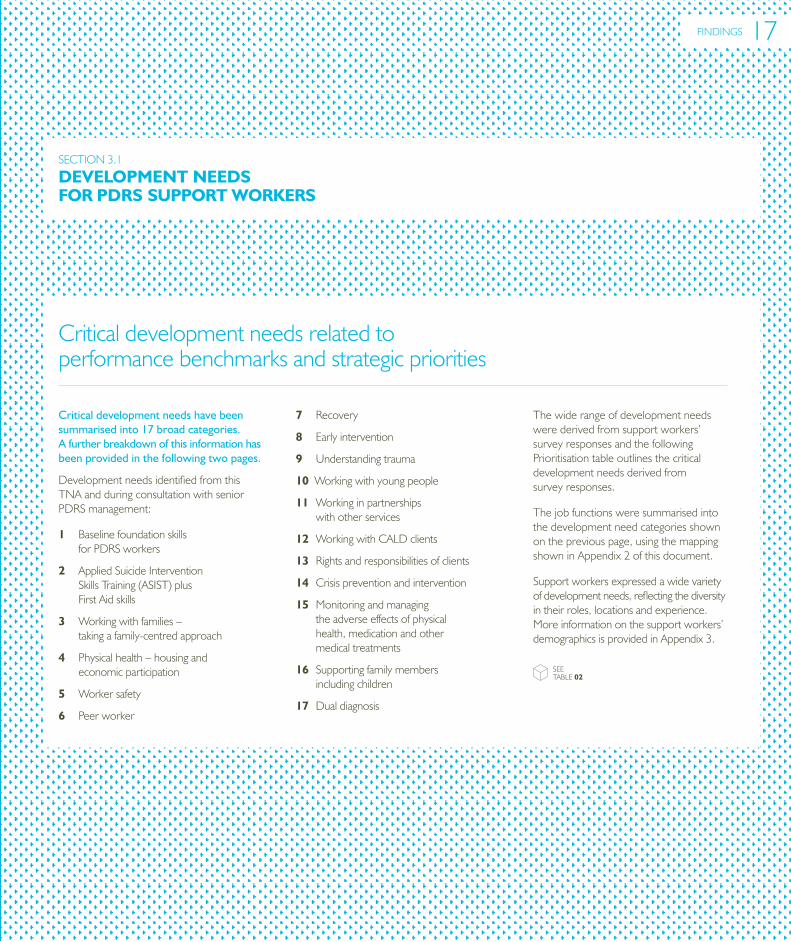
Critical development needs have been summarised into 17 broad categories. A further breakdown of this information has been provided in the following two pages.
DevelopmentneedsidentifiedfromthisTNAandduringconsultationwithseniorPDRSmanagement:
1 BaselinefoundationskillsforPDRSworkers
2 AppliedSuicideInterventionSkillsTraining(ASIST)plusFirstAidskills
3 Workingwithfamilies–takingafamily-centredapproach
4 Physicalhealth–housingandeconomicparticipation
5 Workersafety
6 Peerworker
7 Recovery
8 Earlyintervention
9 Understandingtrauma
10Workingwithyoungpeople
11Workinginpartnershipswithotherservices
12WorkingwithCALDclients
13Rightsandresponsibilitiesofclients
14Crisispreventionandintervention
15Monitoringandmanagingtheadverseeffectsofphysicalhealth,medicationandothermedicaltreatments
16Supportingfamilymembersincludingchildren
17Dualdiagnosis
Thewiderangeofdevelopmentneedswerederivedfromsupportworkers’surveyresponsesandthefollowingPrioritisationtableoutlinesthecriticaldevelopmentneedsderivedfromsurveyresponses.
Thejobfunctionsweresummarisedintothedevelopmentneedcategoriesshownonthepreviouspage,usingthemappingshowninAppendix2ofthisdocument.
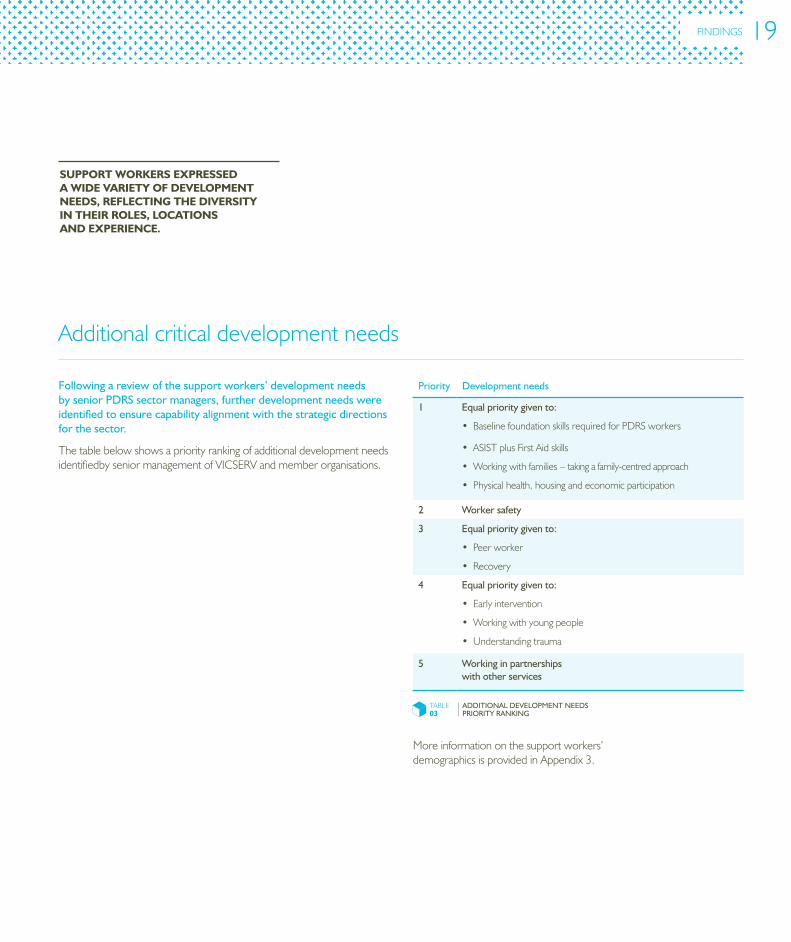
Supportworkersexpressedawidevarietyofdevelopmentneeds,reflectingthediversityintheirroles,locationsandexperience.Moreinformationonthesupportworkers’demographicsisprovidedinAppendix3.
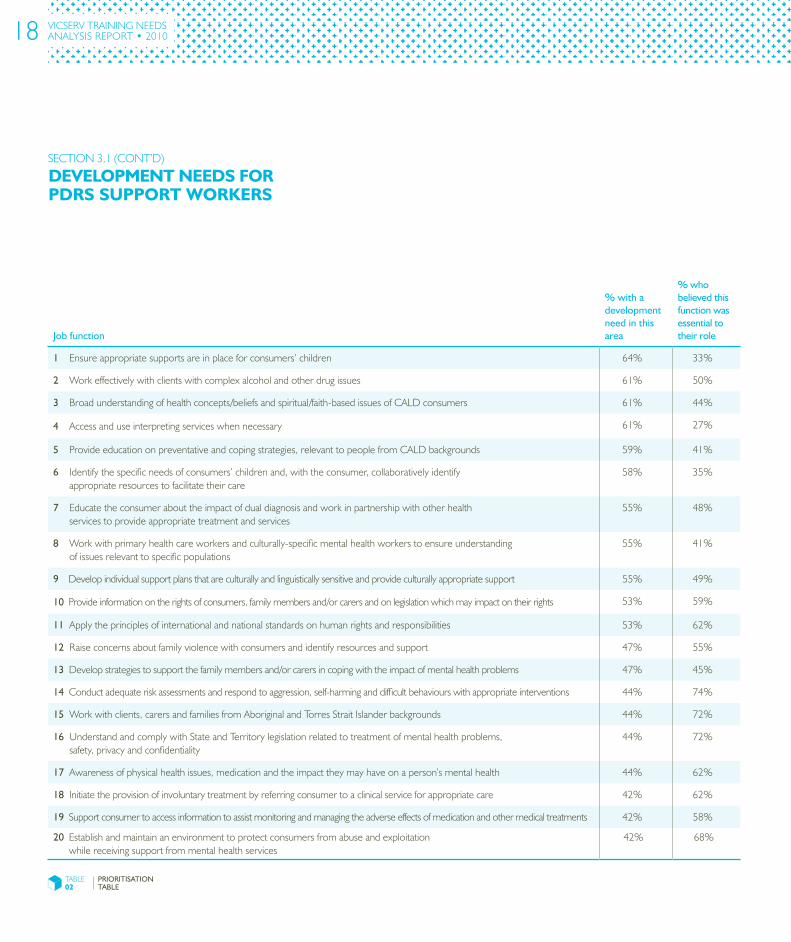
Criticaldevelopmentneedsrelatedtoperformancebenchmarksandstrategicpriorities
DEVELOPMENTNEEDSFORPDRSSUPPORTWORKERS
SECTION3.1
FINDINGS 17
Job function
% with a development need in this area
% who believed this function was essential to their role
1Ensureappropriatesupportsareinplaceforconsumers’children 64% 33%
2Workeffectivelywithclientswithcomplexalcoholandotherdrugissues 61% 50%
3Broadunderstandingofhealthconcepts/beliefsandspiritual/faith-basedissuesofCALDconsumers 61% 44%
4Accessanduseinterpretingserviceswhennecessary 61% 27%
5Provideeducationonpreventativeandcopingstrategies,relevanttopeoplefromCALDbackgrounds 59% 41%
6Identifythespecificneedsofconsumers’childrenand,withtheconsumer,collaborativelyidentifyappropriateresourcestofacilitatetheircare
58% 35%
7Educatetheconsumerabouttheimpactofdualdiagnosisandworkinpartnershipwithotherhealthservicestoprovideappropriatetreatmentandservices
55% 48%
8Workwithprimaryhealthcareworkersandculturally-specificmentalhealthworkerstoensureunderstandingofissuesrelevanttospecificpopulations
55% 41%
9 Developindividualsupportplansthatareculturallyandlinguisticallysensitiveandprovideculturallyappropriatesupport 55% 49%
10Provideinformationontherightsofconsumers,familymembersand/orcarersandonlegislationwhichmayimpactontheirrights 53% 59%
11Applytheprinciplesofinternationalandnationalstandardsonhumanrightsandresponsibilities 53% 62%
12Raiseconcernsaboutfamilyviolencewithconsumersandidentifyresourcesandsupport 47% 55%
13Developstrategiestosupportthefamilymembersand/orcarersincopingwiththeimpactofmentalhealthproblems 47% 45%
14Conductadequateriskassessmentsandrespondtoaggression,self-harminganddifficultbehaviourswithappropriateinterventions 44% 74%
15Workwithclients,carersandfamiliesfromAboriginalandTorresStraitIslanderbackgrounds 44% 72%
16UnderstandandcomplywithStateandTerritorylegislationrelatedtotreatmentofmentalhealthproblems,safety,privacyandconfidentiality
44% 72%
17Awarenessofphysicalhealthissues,medicationandtheimpacttheymayhaveonaperson’smentalhealth 44% 62%
18Initiatetheprovisionofinvoluntarytreatmentbyreferringconsumertoaclinicalserviceforappropriatecare 42% 62%
19Supportconsumertoaccessinformationtoassistmonitoringandmanagingtheadverseeffectsofmedicationandothermedicaltreatments 42% 58%
20Establishandmaintainanenvironmenttoprotectconsumersfromabuseandexploitationwhilereceivingsupportfrommentalhealthservices
42% 68%
DEVELOPMENTNEEDSFORPDRSSUPPORTWORKERS
TABLE02
PRIORITISATION TAbLE
VICSERV TRAININGNEEDSANALYSISREPORT•2010
SECTION3.1(CONT’D)
18
Additionalcriticaldevelopmentneeds
Following a review of the support workers’ development needs by senior PDRS sector managers, further development needs were identified to ensure capability alignment with the strategic directions for the sector.
ThetablebelowshowsapriorityrankingofadditionaldevelopmentneedsidentifiedbyseniormanagementofVICSERVandmemberorganisations.
Priority Development needs
1 Equal priority given to:
•BaselinefoundationskillsrequiredforPDRSworkers
•ASISTplusFirstAidskills
•Workingwithfamilies–takingafamily-centredapproach
•Physicalhealth,housingandeconomicparticipation
2 Worker safety
3 Equal priority given to:
•Peerworker
•Recovery
4 Equal priority given to:
•Earlyintervention
•Workingwithyoungpeople
•Understandingtrauma
5 Working in partnerships with other services
Moreinformationonthesupportworkers’demographicsisprovidedinAppendix3.
SUPPORTWORKERSEXPRESSEDAWIDEVARIETYOFDEVELOPMENTNEEDS,REFLECTINGThEDIVERSITYINThEIRROLES,LOCATIONSANDEXPERIENCE.
TABLE03
ADDITIONAL DEVELOPMENT NEEDS PRIORITY RANKING
FINDINGS 19
Trainingpriorities
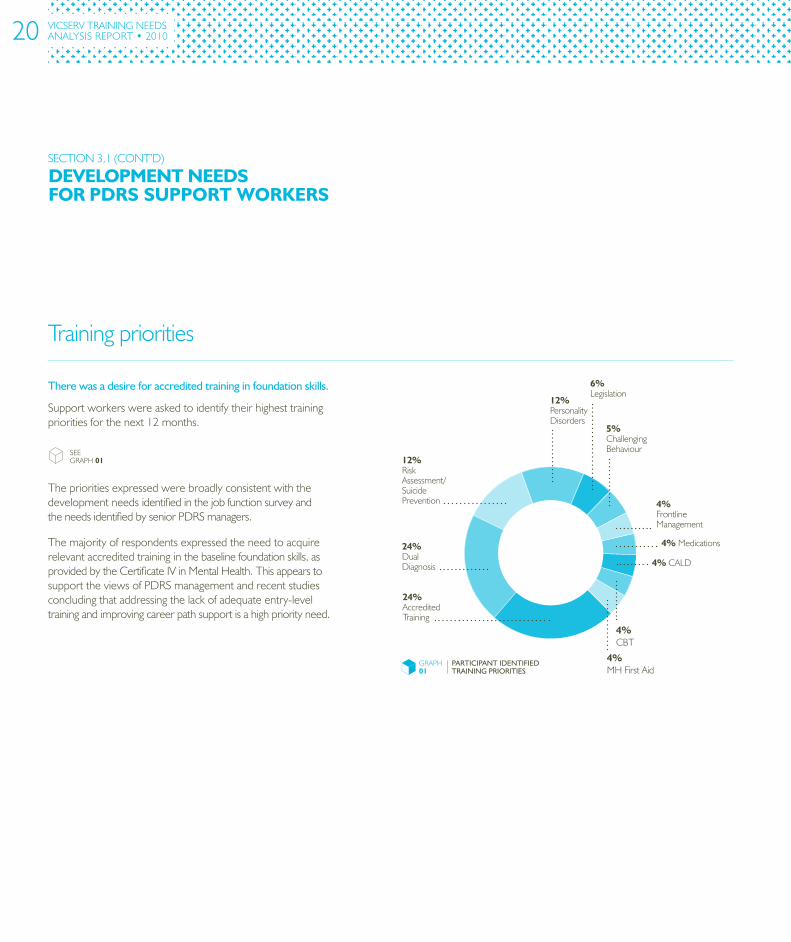
There was a desire for accredited training in foundation skills.
Supportworkerswereaskedtoidentifytheirhighesttrainingprioritiesforthenext12months.
TheprioritiesexpressedwerebroadlyconsistentwiththedevelopmentneedsidentifiedinthejobfunctionsurveyandtheneedsidentifiedbyseniorPDRSmanagers.
Themajorityofrespondentsexpressedtheneedtoacquirerelevantaccreditedtraininginthebaselinefoundationskills,asprovidedbytheCertificateIVinMentalHealth.ThisappearstosupporttheviewsofPDRSmanagementandrecentstudiesconcludingthataddressingthelackofadequateentry-leveltrainingandimprovingcareerpathsupportisahighpriorityneed.
SEEGRAPH01
DEVELOPMENTNEEDSFORPDRSSUPPORTWORKERS
VICSERV TRAININGNEEDSANALYSISREPORT•2010
GRAPH01
PARTICIPANT IDENTIFIED TRAINING PRIORITIES
24%DualDiagnosis
4%CBT
24%AccreditedTraining
12%PersonalityDisorders
6%Legislation
12%RiskAssessment/SuicidePrevention
4%MHFirstAid
4%FrontlineManagement
4%Medications
4%CALD
5%ChallengingBehaviour
SECTION3.1(CONT’D)
20

The results show a clear preference for face-to-face development.
Whileparticipantsshowedamarkedpreferenceforface-to-facedevelopment,theydidnotlimittheirpreferencestoconventionaltrainingprograms.
Thepreferredmodesofdevelopmentwereidentifiedas:
1 Workshops(preferredby59%ofrespondents)
2 ProfessionalSupervision(58%)
3 ShortCourses(58%)
4 ReflectivePractice(53%).
Thesepreferencesindicatethatsupportworkersarelikelytobesupportiveofalternativestoconventionaltrainingprograms,suchasworkplacecoaching,mentoring,developmentassignmentsandreflectivepracticeopportunities.
Several of the most frequently identified development needs were also reflected in the Mental Health Coordinating Council’s TNA of mental health workers in the NGO sector in December 2006, which found high priority needs relating to:
•Workingwithdualdiagnosis
•WorkingwithCALDcommunities,
•Workingwithchildrenandyoungpeople.
Thestudyalsoreflectedthesector’sneedfortrainingpathwaystoenablenewstafftobuildskillsandqualifications.
Supportingevidenceofdevelopmentneedsfromotherrecentstudies
Preferencesformeetingdevelopmentneeds
WhILEPARTICIPANTSShOWEDAMARKEDPREFERENCEFORFACE-TO-FACEDEVELOPMENT,ThEYDIDNOTLIMITThEIRPREFERENCESTOCONVENTIONALTRAININGPROGRAMS.
FINDINGS 21
Critical development needs for PDRS managers have been summarised into the following categories:
1 Managingchange
2 Applyingreflectivepractice
3 Applyingqualityprinciples
4 Applyingdataandoutcomemeasurementstoimproveservicedelivery
5 Ensuringlegislativecompliance
6 Managingcomplexstakeholderissuesthatareintegraltothechangeprocess
7 Writingtendersandsubmissions
8 Developingandmanagingcomplexbudgets
9 Interpretingstateandfederalpoliciesandplans
10 Managingcomplexstakeholderissuesthatareintegraltothechangeprocess
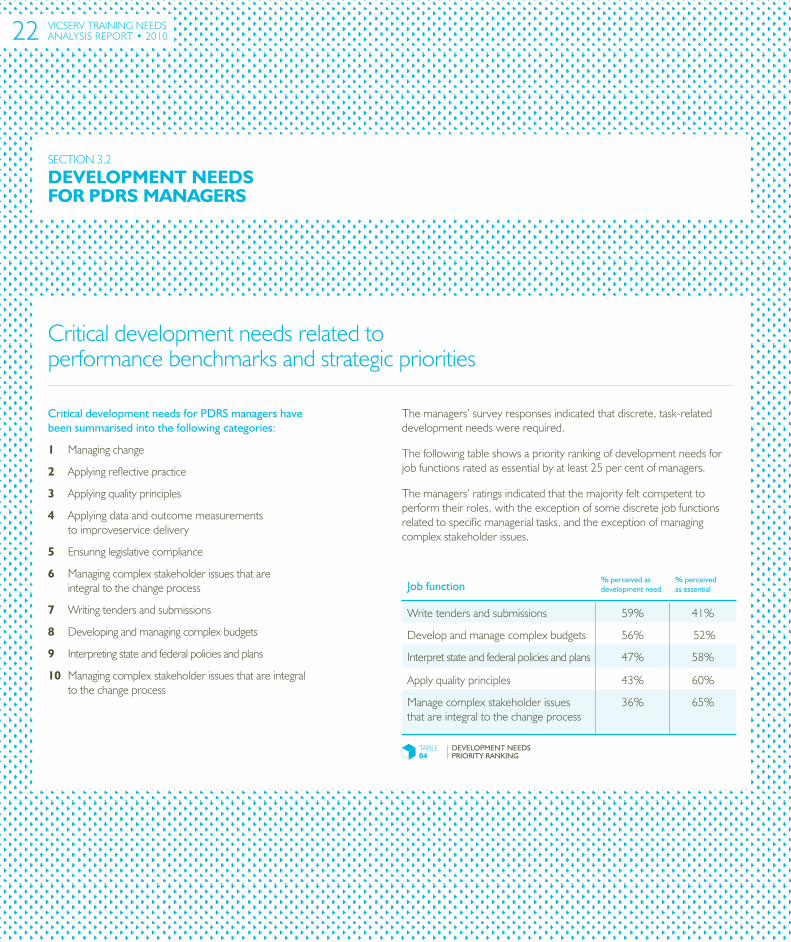
Criticaldevelopmentneedsrelatedtoperformancebenchmarksandstrategicpriorities
Job function
% perceived as development need
% perceived as essential
Writetendersandsubmissions 59% 41%
Developandmanagecomplexbudgets 56% 52%
Interpretstateandfederalpoliciesandplans 47% 58%
Applyqualityprinciples 43% 60%
Managecomplexstakeholderissuesthatareintegraltothechangeprocess
36% 65%
TABLE04
DEVELOPMENT NEEDS PRIORITY RANKING
DEVELOPMENTNEEDSFORPDRSMANAGERS
SECTION3.2
VICSERV TRAININGNEEDSANALYSISREPORT•2010
Themanagers’surveyresponsesindicatedthatdiscrete,task-relateddevelopmentneedswererequired.
Thefollowingtableshowsapriorityrankingofdevelopmentneedsforjobfunctionsratedasessentialbyatleast25percentofmanagers.
Themanagers’ratingsindicatedthatthemajorityfeltcompetenttoperformtheirroles,withtheexceptionofsomediscretejobfunctionsrelatedtospecificmanagerialtasks,andtheexceptionofmanagingcomplexstakeholderissues.
22
ThEMANAGERS’SURVEYRESPONSESINDICATEDThATDISCRETE,TASK-RELATEDDEVELOPMENTNEEDSWEREREqUIRED.
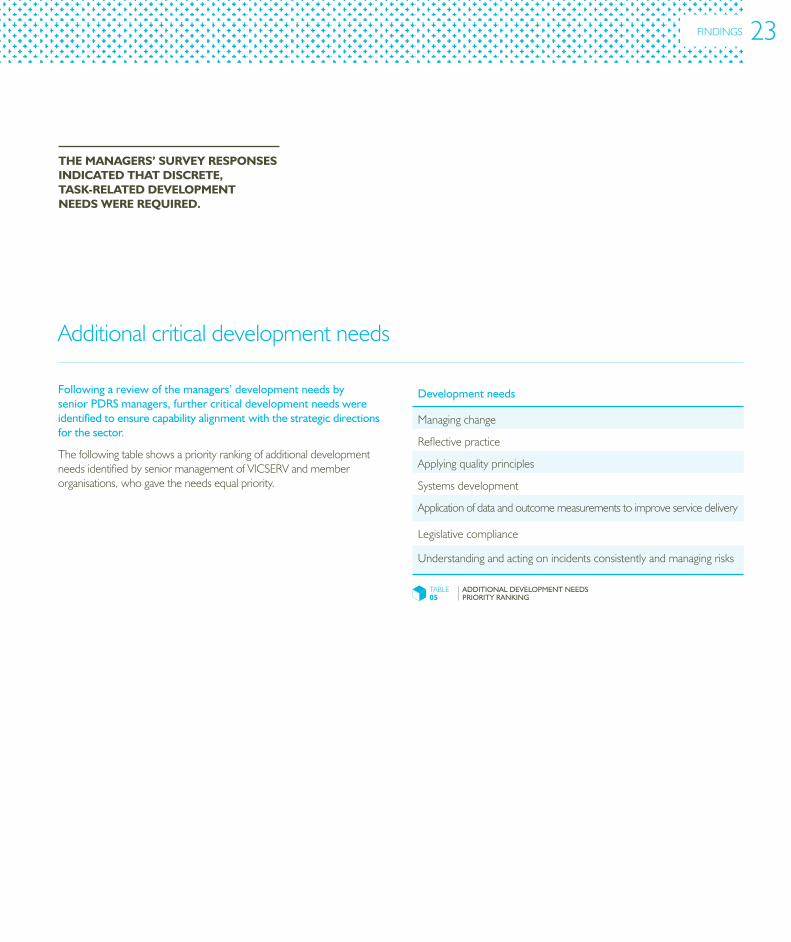
Following a review of the managers’ development needs by senior PDRS managers, further critical development needs were identified to ensure capability alignment with the strategic directions for the sector.
ThefollowingtableshowsapriorityrankingofadditionaldevelopmentneedsidentifiedbyseniormanagementofVICSERVandmemberorganisations,whogavetheneedsequalpriority.
Additionalcriticaldevelopmentneeds
Development needs
Managingchange
Reflectivepractice
Applyingqualityprinciples
Systemsdevelopment
Applicationofdataandoutcomemeasurementstoimproveservicedelivery
Legislativecompliance
Understandingandactingonincidentsconsistentlyandmanagingrisks
TABLE05
ADDITIONAL DEVELOPMENT NEEDS PRIORITY RANKING
FINDINGS 23
SECTION3.2(CONT’D)
DEVELOPMENTNEEDSFORPDRSMANAGERS
VICSERV TRAININGNEEDSANALYSISREPORT•2010
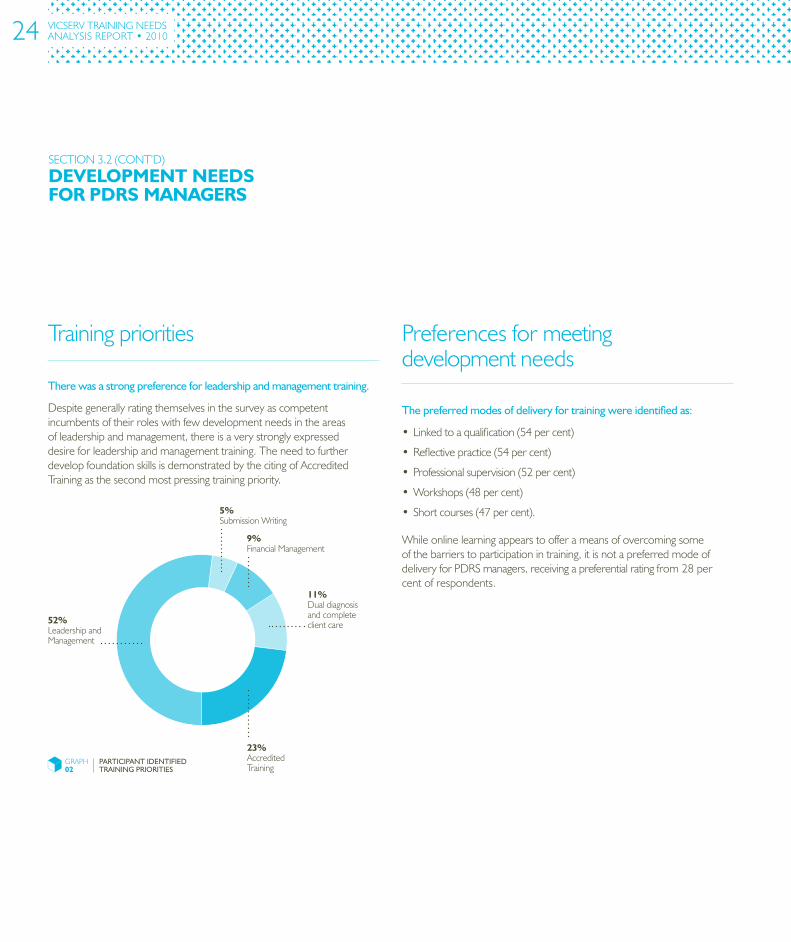
The preferred modes of delivery for training were identified as:
•Linkedtoaqualification(54percent)
•Reflectivepractice(54percent)
•Professionalsupervision(52percent)
•Workshops(48percent)
• Shortcourses(47percent).
Whileonlinelearningappearstoofferameansofovercomingsomeofthebarrierstoparticipationintraining,itisnotapreferredmodeofdeliveryforPDRSmanagers,receivingapreferentialratingfrom28percentofrespondents.
Preferencesformeetingdevelopmentneeds
Trainingpriorities
There was a strong preference for leadership and management training.
Despitegenerallyratingthemselvesinthesurveyascompetentincumbentsoftheirroleswithfewdevelopmentneedsintheareasofleadershipandmanagement,thereisaverystronglyexpresseddesireforleadershipandmanagementtraining.TheneedtofurtherdevelopfoundationskillsisdemonstratedbythecitingofAccreditedTrainingasthesecondmostpressingtrainingpriority.
GRAPH02
PARTICIPANT IDENTIFIED TRAINING PRIORITIES
5%SubmissionWriting
9%FinancialManagement
11%Dualdiagnosisandcompleteclientcare
23%AccreditedTraining
52%LeadershipandManagement
24
TRAININGCURRENTLYAVAILABLETOMEETDEVELOPMENTNEEDS
SECTION3.3
While many of the critical development needs, identified in this report, are ostensibly addressed by existing training, there are some needs that are yet to be adequately catered to. There are also some strategic and structural issues in training delivery that impede the provision of training and development to Victorian PDRS workers.
Thissectionofthefindingsreportsongapsthatexistbetweentrainingthatiscurrentlyavailableandissuesrelatedtotrainingdeliveryandconsumption.
Gapsinexistingtrainingcoverage
Available development does not meet all needs.
SignificantgapsbetweendevelopmentneedsandavailabledevelopmentopportunitiesforPDRSworkersinclude:
Support workers
•Workingwithfamilies
•Earlyintervention
•Workingwithyoungpeople
•Peerworker
Managers
•Riskmanagement
Note:InformationondevelopmentcurrentlyavailabletotheVictorianPDRSsectorisincludedinAppendix4.
There is insufficient coverage of PDRS philosophy and approaches in undergraduate training.
DiscussionswithPDRSmanagementindicatedthatthereisinadequateunderstandingoftheVictorianPDRSphilosophyandapproachestoprovidingservicesamongnewentrantstoPDRSroles.ThisappearstoreflectalackofadequatecoverageofPDRSphilosophyandapproachesinundergraduatetraining.Thismaycontributetoafurtherbarriertothesupplyofsuitably-skillednewentrants.
FINDINGS 25
Structuralissues Designissueswithfoundationskillstraining
Opportunitiesforaddressingissues
DisincentivesforPDRSworkerswithhigherqualifications
PDRS services cannot make the most of available development opportunities.
Inadditiontocoveragedeficits,therearealsodeliverycapacityissuesanddemandconstraints.PDRStrainingsuppliersareunablemeetthestate-widedemandforsomecriticaldevelopmentneedswiththeircurrentresourcing.
Atthesametime,itisnotuncommontofindPDRSserviceswishingtoaddressthedevelopmentneedsoftheirworkers,butlackingtheresourcesintermsofavailabletime,fundingandbackfillingpositionstodoso.
VICSERVoffersconsiderableresourcesfrombothitsaccreditedandnon-accreditedtraining,butmanymemberorganisationsareunabletoutilisetheseduetoresourcingconstraints.
ThisfindingisreinforcedinVICSERV’sBuilding Capacity in Community Mental Health Family Support and Carer Respite Project–Workforce Development Report,2009,whichhighlightedthebarrierstoparticipationintrainingforthePDRSworkforce,including:
• Alackofadequateinformationonavailabletraining
• Lackoftrainingaccessibility,particularlyinruralandremoteareas1
Thedevelopmentoffurthertrainingandrelateddevelopmentopportunitiesmayexacerbatethissituation.
The key source of foundation skills training for the PDRS sector— the Certificate IV in Mental Health —can take up to two years to complete, and is not readily available throughout Victoria.
Thiscreatesentrybarriersforprospectiveworkers,andpreventsarapidincreaseinthenumbersofappropriatelyqualifiedstaff.
Similarly,theapparentcomplexityofskillrecognitionprocedurescreatesafurtherbarrier,reducingthewillingnessofworkerstoattainthequalifications.
Discussions with members of the VICSERV Training Advisory Group provided the following suggestions for potential resources that may help to mitigate some coverage and structural issues:
• ExplorerelevanceofextensiveMentalHealthProfessionalOnlineDevelopment(MHPOD)e-LearningCurriculum,whichisbasedontheNationalStandardsforMentalHealthServices,1997.MHPODisprimarilyintendedforaclinicalaudience,buthasmanymodulesthatcovertopicsrelevanttothePDRSsector.
• VICSERVcouldadvocateonbehalfofthesectortoensurethatthedevelopedMHPODcurriculumremainsrelevanttoPDRS.
• Provisionofdevelopmentwithinthesectortodelivertrainingand/orworkshopsonbestpractice.
PDRS workers with higher qualifications who require Certificates IV to Advanced Diploma qualifications in Mental Health are currently unable to acquire funding.
Thissituationfurtherhamperstheacquisitionofcriticalfoundationskillsinthesector.
SECTION3.3(CONT’D)
TRAININGCURRENTLYAVAILABLETOMEETDEVELOPMENTNEEDS
Reference
1 VICSERV,(2009),Building Capacity in Community Mental Health Family Support and Carer Respite Project – Workforce Development Report,VICSERV,Melbourne
VICSERV TRAININGNEEDSANALYSISREPORT•2010 26
Overview
WORKFORCESUSTAINABILITYISSUESRELATEDTODEVELOPMENTNEEDS
SECTION3.4
Investment in training is wasted unless related workforce sustainability issues are addressed.
AccordingtoBecause mental health matters: Victorian mental health reform strategy 2009-2019,workforcesustainabilityisdependentonorganisationalcapacitybuildingpromotedby:
•Reducedturnover
•Highstaffmotivation
•Satisfyingworkroles
•Diverseandrewardingcareeropportunities.
Numerousstudiesacrossawidevarietyofindustriesdemonstrateahighdegreeofinterdependencebetweenthesefactors.InvestmentindevelopingPDRSworkerswillbeoflittlevalueunlessthesefactorsarealsoaddressed.
Nearly half of the workforce is considering or planning to leave the sector.
Forty-sevenpercentofsupportworkersandmanagerssurveyedindicatedthattheyareconsideringand/orplanningtoleavethesectorinthenextthreeyears.Whileturnover,motivationandjobsatisfactiondataarenotavailableforthePDRSworkforce,theresponsesofthe231respondentstothesurveysuggestthatthesustainabilityfactorscitedaboveareatanunacceptablelevel.
Thefindingsappeartoalignwithturnoverdataonthedirectmentalhealthworkforce,whichshowsthatofthestaffwhomovedfromorwithinthepublicmentalhealthsystemin2001to2002,around35percentleftafterlessthan12monthswiththeircurrentemployerand63.4percentleftwithinthreeyearsofcommencing.1
There are major factors influencing the desire to leave the PDRS sector.
ThefactorsinfluencingthedesiretoleavethePDRSsectorappeartobelinkedtosymptomsofinadequatelevelsofworkforcesustainability.
Factors
Support workers
Managers
Burnout 27% 21%
Remuneration 21% 25%
Exploreotheropportunities
14% 32%
Reference
1 DepartmentofHumanServices(2005),Victoria’s Direct Care Mental Health Workers: The Public Mental Health Workforce Study 2003–04 to 2001–12,StateGovernmentofVictoria,Melbourne,p1
TABLE06
MAJOR FACTORS INFLUENCING THE DESIRE TO LEAVE THE PDRS SECTOR
FINDINGS 27
SECTION4•VICSERVTRAININGNEEDSANALYSISREPORT2010
RECOMMENDATIONS–
The following recommendations have been developed through a consideration of the findings.
TherecommendationsarealignedwiththeappropriatestrategicdirectionsfortheVictorianPDRSsectorforthecomingdecade.
SEETABLE07
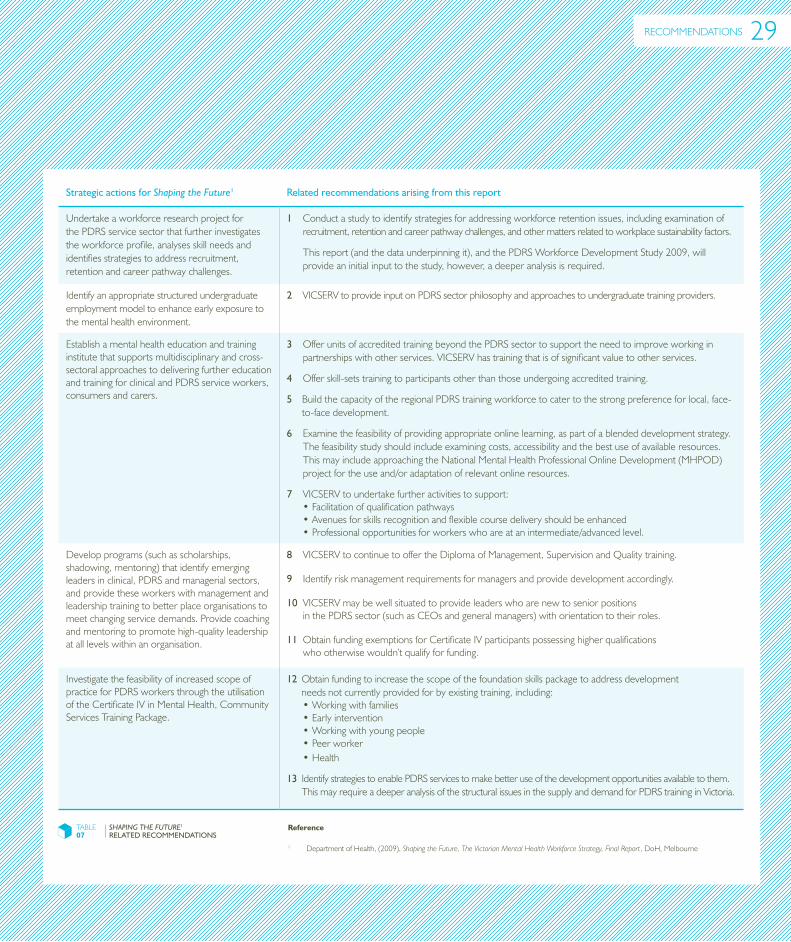
Strategic actions for Shaping the Future1 Related recommendations arising from this report
UndertakeaworkforceresearchprojectforthePDRSservicesectorthatfurtherinvestigatestheworkforceprofile,analysesskillneedsandidentifiesstrategiestoaddressrecruitment,retentionandcareerpathwaychallenges.
1 Conductastudytoidentifystrategiesforaddressingworkforceretentionissues,includingexaminationofrecruitment,retentionandcareerpathwaychallenges,andothermattersrelatedtoworkplacesustainabilityfactors.
Thisreport(andthedataunderpinningit),andthePDRSWorkforceDevelopmentStudy2009,willprovideaninitialinputtothestudy,however,adeeperanalysisisrequired.
Identifyanappropriatestructuredundergraduateemploymentmodeltoenhanceearlyexposuretothementalhealthenvironment.
2 VICSERVtoprovideinputonPDRSsectorphilosophyandapproachestoundergraduatetrainingproviders.
Establishamentalhealtheducationandtraininginstitutethatsupportsmultidisciplinaryandcross-sectoralapproachestodeliveringfurthereducationandtrainingforclinicalandPDRSserviceworkers,consumersandcarers.
3OfferunitsofaccreditedtrainingbeyondthePDRSsectortosupporttheneedtoimproveworkinginpartnershipswithotherservices.VICSERVhastrainingthatisofsignificantvaluetootherservices.
4Offerskill-setstrainingtoparticipantsotherthanthoseundergoingaccreditedtraining.
5BuildthecapacityoftheregionalPDRStrainingworkforcetocatertothestrongpreferenceforlocal,face-to-facedevelopment.
6Examinethefeasibilityofprovidingappropriateonlinelearning,aspartofablendeddevelopmentstrategy.Thefeasibilitystudyshouldincludeexaminingcosts,accessibilityandthebestuseofavailableresources.ThismayincludeapproachingtheNationalMentalHealthProfessionalOnlineDevelopment(MHPOD)projectfortheuseand/oradaptationofrelevantonlineresources.
7 VICSERVtoundertakefurtheractivitiestosupport:•Facilitationofqualificationpathways•Avenuesforskillsrecognitionandflexiblecoursedeliveryshouldbeenhanced•Professionalopportunitiesforworkerswhoareatanintermediate/advancedlevel.
Developprograms(suchasscholarships,shadowing,mentoring)thatidentifyemergingleadersinclinical,PDRSandmanagerialsectors,andprovidetheseworkerswithmanagementandleadershiptrainingtobetterplaceorganisationstomeetchangingservicedemands.Providecoachingandmentoringtopromotehigh-qualityleadershipatalllevelswithinanorganisation.
8VICSERVtocontinuetooffertheDiplomaofManagement,SupervisionandQualitytraining.
9Identifyriskmanagementrequirementsformanagersandprovidedevelopmentaccordingly.
10VICSERVmaybewellsituatedtoprovideleaderswhoarenewtoseniorpositionsinthePDRSsector(suchasCEOsandgeneralmanagers)withorientationtotheirroles.
11ObtainfundingexemptionsforCertificateIVparticipantspossessinghigherqualificationswhootherwisewouldn’tqualifyforfunding.
InvestigatethefeasibilityofincreasedscopeofpracticeforPDRSworkersthroughtheutilisationoftheCertificateIVinMentalHealth,CommunityServicesTrainingPackage.
12Obtainfundingtoincreasethescopeofthefoundationskillspackagetoaddressdevelopmentneedsnotcurrentlyprovidedforbyexistingtraining,including:•Workingwithfamilies•Earlyintervention•Workingwithyoungpeople•Peerworker•Health
13IdentifystrategiestoenablePDRSservicestomakebetteruseofthedevelopmentopportunitiesavailabletothem.ThismayrequireadeeperanalysisofthestructuralissuesinthesupplyanddemandforPDRStraininginVictoria.
TABLE07
SHaping THe FuTure1
RELATED RECOMMENDATIONSReference
1 DepartmentofHealth,(2009),Shaping the Future, The Victorian Mental Health Workforce Strategy, Final Report,DoH,Melbourne
RECOMMENDATIONS 29
SECTION5•VICSERVTRAININGNEEDSANALYSISREPORT2010
BIBLIOGRAPhY–
ACTDepartmentofHealthandCommunityCare,(1999),Dual Diagnosis: Stopping the merry-go-round,ACTDepartmentofHealthandCommunityCare,Canberra
AustralianGovernmentDepartmentofHealthandAgeing,(1997),National Standards for Mental Health Services,AustralianGovernmentDepartmentofHealthandAgeing,Canberra
DepartmentofEducation,EmploymentandWorkplaceRelations,(2008),CHC08CommunityServicesTrainingPackage,DEEWR,Canberra
DepartmentofHealth,(2009),Shaping the Future, The Victorian Mental Health Workforce Strategy, Final Report,DoH,Melbourne
DepartmentofHumanServices,(2004),Standards for psychiatric disability rehabilitation and support services,DHS,Melbourne
DepartmentofHumanServices,(2009), Because mental health matters: Victorian mental health reform strategy 2009 – 2011,MentalHealthandDrugsDivision,DHS,Melbourne
DepartmentofHumanServices,(2005),Victoria’s direct care mental health workers: The public mental health workforce study2003–04to2001–12,StateGovernmentofVictoria,DHS,Melbourne
LondonRefugeeEconomicAction(LORECA),(2007),Report of the Training Needs Analysis exercise carried with London Refugee Community Organisations in 2005-06,LORECA,London
MentalHealthCoordinatingCouncil,(2006),Mental Health Training Needs Assessment for the NGO Sector in NSW- Final Report,MHCC,Lilyfield
TheNationalCentreofMentalHealthResearch,InformationandWorkforceDevelopment,(2007)Pacific Mental Health Workforce, Training Needs Analysis, Research Report,TheNationalCentreofMentalHealthResearch,InformationandWorkforceDevelopment,Auckland
VICSERV,(2008),Sector Snapshot,ReportonMemberCensusandWorkerSurvey,VICSERV,Melbourne
VICSERV,(2009),Building Capacity in Community Mental Health Family Support and Carer Respite Project Workforce Development Report,VICSERV,Melbourne
VolunteeringGeelong,(2009),Praise Volunteers: Training for Volunteers and Volunteer-involving Organisations Report,Geelong
SECTION6•VICSERVTRAININGNEEDSANALYSISREPORT2010
APPENDICES–
Appendix1:LiteratureReview
Appendix2:Summariseddevelopmentneedsmappedtojobfunctionsforsupportworkers
Appendix3:Profileofthesupportworker
Appendix4:Profileofthemanager
Appendix5:DevelopmentcurrentlyavailabletothePDRSsector
32
36
37
45
53
The literature review examined:
Service and support standardsrelevanttothePDRSsectorinVictoria,toprovidebenchmarksfortheTNA.
PDRS sector workforce challengesinthepresentandfuture.ThisinvolvedreviewingstrategicdirectionsinmentalhealththatwillaffectthePDRSsector,andrecentstudiesintoPDRSworkforceissues.
Current training packages relevant to the PDRS sector,tocontributetoassessingtheextenttowhichtrainingneedsmaybeaddressedbyexistingresources.
APPENDIX1
Serviceandsupportstandards
Itisunderstoodthatservicestandardsandqualityassuranceprogramswithinhealthservicesareanessentialpartofachievinghighqualityhealthcare.On3rdDecember1996,theAustralianHealthMinisters’AdvisoryCouncil’sNationalMentalHealthWorkingGroupendorsedtheNational Standards for Mental Health Services.
TheNationalStandardsprovideaguideforthedevelopmentofnewservices,andtosteerserviceenhancementandcontinuousimprovementofexistingservices.TheirscopeincludesstandardsforPDRSservices.
ThedevelopmentoftheNationalStandardswasguidedbytheprinciplescontainedintheAustralianHealthMinisters’MentalHealthStatementofRightsandResponsibilities,andtheUnitedNationsPrinciplesontheprotectionofpeoplewithamentalillness.
AreviewoftheStandardsoccurredin2008.Todate,therehasnotbeenacceptanceoftherevisedstandardsbytheMentalHealthStandingCommittee,onbehalfoftheAustralianHealthMinisters’AdvisoryCouncil.
The publication Standards for psychiatric disability rehabilitation and support services,2004,wasadaptedfromtheNationalStandardsandcontainselevenStandardsthatprovideaguidancefor:
‘…PDRSservicestomaintainafocusonservicequalitymeasurementandimprovement.TheStandardsassistservicestoachieveandmaintainthehigheststandardofsupportandrehabilitationforpeoplewithapsychiatricdisability’,p2.
VICSERV TRAININGNEEDSANALYSISREPORT•2010
LITERATUREREVIEW
32
NEWPARTNERShIPSWILLNEEDTOBEMADEACROSSTRADITIONALBOUNDARIESANDNEWWAYSOFWORKINGTOGEThERWILLNEEDTOBEESTABLIShED.
PDRSsectorworkforcechallenges
Recent studies addressing PDRS workforce issues
PDRSservicesareoperatinginatimeofsignificantchangeinthementalhealthsector.
ThedirectionsoftheStateGovernment’sten-yearplanBecause mental health matters: Victorian mental health reform strategy 2009 – 2019,suggestthatoverthenextfewyearsthePDRSsectorwillbegoingthroughsignificantreforms.Partnershipswillbecentraltothefuturegrowthanddevelopmentofthesector.Existingpartnershipswillneedtobestrengthenedandrefocused.Newpartnershipswillneedtobemadeacrosstraditionalboundariesandnewwaysofworkingtogetherwillneedtobeestablished.
ThechallengesfacingthePDRSsectorworkforcehavealsobeenrecognisedinanumberofstudies,including:
an analysis of the Victorian rehabilitation and recovery Care Service System for people With Severe Mental illness and associated Disability project report, DHS, 2007. The report states that in relation to workforce issues:
‘Thefollowingtwokeyissuesareimpactingonthelong-termsustainabilityofVictoria’spublicmentalhealthservicesystem:
• Existingandprojectedshortagesintheskilledmentalhealthworkforce
• Workforcequalitybothintermsofvariablepracticestandardsandtheneedtostrengthenmentalhealthleadershipacrossthespectrumofservices’,p2.
a report on the Training needs assessment of Mental Health Workers in the ngO sector, Mental Health Coordinating Council, 2006, based on data from 59 survey respondents (a 42 per cent response rate), states that:
‘Anumberofrespondentsexpressedaneedforallmentalhealthtrainingtoinclude:
• Moreemphasisonethicsandprofessionalboundariesissues
• Anincreaseinthecommunicationandinterpersonalskillsinvolvedinengagingwithconsumers
• Informationrelatedtolocalservicenetworksorreferralprocedures
• Opportunitiesfortrainingpathwaystoenablenewstaff,aswellasconsumersandcarers,tobuildskillsandqualifications
• Opportunitiesforhigherleveltrainingforskilledstaff,particularlyincomplexareassuchasdualdiagnosis,andforspecialistgroupssuchasthoseworkingwithCALDcommunities,olderpeoplewithdementia,orinfants,childrenandyoungpeoplewithmentalhealthproblems’,p32.
APPENDICES 33
PreviousstudiesintoPDRSworkforceissues
Significantly, previous VICSERV studies have been undertaken including Sector Snapshots in 2000 and 2007 (reported as Sector Snapshot, report on Member Census and Worker Survey in 2009).
Thesereportshadaresponserateof52and43respectivelyandprovidedinsightintotrainingneedsidentifiedbytheworkforceincluding:
•Substanceuseandpsychiatricdisability
•Peoplewithborderlinepersonalitydisorder
In addition, the following documents provided insights on PDRS workforce issues:
• NationalCentreofMentalHealthResearch,InformationandWorkforceDevelopment,(2007),PacificMentalHealthWorkforce,TrainingNeedsAnalysis,ResearchReport,NationalCentreofMentalHealthResearch,InformationandWorkforceDevelopment,Auckland
• ACTDepartmentofHealthandCommunityCare,(1999),DualDiagnosis:Stoppingthemerry-go-round,ACTDepartmentofHealthandCommunityCare,Canberra
• VolunteeringGeelong,(2009),PraiseVolunteers:TrainingforVolunteersandVolunteer–involvingOrganisationsReport,Geelong
• LondonRefugeeEconomicAction(LORECA),(2007),ReportoftheTrainingNeedsAnalysisexercisecarriedwithLondonRefugeeCommunityOrganisationsin2005–06,LORECA,London
LITERATUREREVIEW
APPENDIX1(CON’D)
VICSERV TRAININGNEEDSANALYSISREPORT•2010 34
APPENDICES
The most recent national community services training package endorsed in December 2008 includes qualifications and skill sets that encompass most competencies required by the mental health workforce.
Somegapsremain,includingworkingwithfamiliesandcoordinatingservices.
Thefollowingqualificationshavebeenreviewedandmodifiedtoreflecttheneedsofmentalhealthservices:
•CertificateIVinMentalHealth[CHC40508]
• DiplomaofCommunityServices(AlcoholandOtherDrugs)[CHC50208]
• DiplomaofCommunityServices(MentalHealth)[CHC50308]
• DiplomaofCommunityServices(AlcoholandOtherDrugsandMentalHealth)[CHC50408]
Noticeably, the inclusion of skill sets provides an opportunity to augment a worker’s foundation qualification with more specialised knowledge and skill, according to work requirements.
ThefollowingskillsetsaremostrelevanttothePDRSsector:
• Mentalhealthskillset–includingrespondtoriskofsuicide
• Mentalhealthskillset–includingrecogniseindividualsatrisk
•Alcoholandotherdrugsskillset.
CurrenttrainingpackagesrelevanttothePDRSsector
ThEINCLUSIONOFSKILLSETSPROVIDESANOPPORTUNITYTOAUGMENTAWORKER’SFOUNDATIONqUALIFICATIONWIThMORESPECIALISEDKNOWLEDGEANDSKILLS,ACCORDINGTOWORKREqUIREMENTS.
35

The table below shows the relationship between the summarised development needs identified in this report, and the job functions identified by support workers were essential for the workers’ role and development needs that existed.
SUMMARISEDDEVELOPMENTNEEDSMAPPEDTOjOBFUNCTIONSFORSUPPORTWORKERS
APPENDIX2
Summarised development need
Job functions with development needs (NumberingrelatestoPrioritisationtableonpage18)
WorkingwithCulturallyandLinguisticallyDiverse(CALD)clients
3 Broadunderstandingofhealthconcepts/beliefsandspiritual/faith-basedissuesofCALDconsumers
4Accessanduseinterpretingserviceswhennecessary
5Provideeducationonpreventativeandcopingstrategies,relevanttopeoplefromCALDbackgrounds
8Workwithprimaryhealthcareworkersandculturallyspecificmentalhealthworkerstoensureunderstandingofissuesrelevanttospecificpopulations
9Developindividualsupportplansthatareculturallyandlinguisticallysensitiveandprovideculturallyappropriatesupport
15Workwithclients,carersandtheirfamilieswhoarefromAboriginalandTorresStraitIslanderbackgrounds
Rightsandresponsibilitiesofclients
10Provideinformationontherightsofconsumers,familymembersand/orcarersandonlegislation,whichmayimpactontheirrights
11Applytheprinciplesofinternationalandnationalstandardsonhumanrightsandresponsibilities
16UnderstandandcomplywithStateandTerritorylegislationrelatedtotreatmentofmentalhealthproblems,safety,privacyandconfidentiality
Crisispreventionandintervention
12Raiseconcernsaboutfamilyviolencewithconsumersandidentifyresourcesandsupport
18Initiatetheprovisionofinvoluntarytreatmentbyreferringconsumertoaclinicalserviceforappropriatecare
20Establishandmaintainanenvironmenttoprotectconsumersfromabuseandexploitationwhilereceivingsupportfrommentalhealthservices
Monitoringandmanagingtheadverseeffectsofphysicalhealth,medicationandothermedicaltreatments
14Conductadequateriskassessmentsandrespondtoaggression,self-harminganddifficultbehaviourswithappropriateinterventions
17Awarenessofphysicalhealthissues,medicationandtheimpacttheymayhaveonaperson’smentalhealth
19Supportconsumerstoaccessinformationtoassistmonitoringandmanagingtheadverseeffectsofmedicationandothermedicaltreatments
Supportingfamilymembersincludingchildren
1 Ensureappropriatesupportsareinplaceforconsumers’children
6 Identifythespecificneedsofconsumers’childrenand,withtheconsumer,collaborativelyidentifyappropriateresourcestofacilitatetheircare
13 Developstrategiestosupportthefamilymembersand/orcarersincopingwiththeimpactofmentalhealthproblems
Dualdiagnosis 7Educatetheconsumerabouttheimpactofdualdiagnosisandworkinpartnershipwithotherhealthservicestoprovideappropriatetreatmentandsupport
Workwithclientswithcomplexalcoholandotherdrugissues
2Workeffectivelywithclientswithcomplexand/oralcoholandotherdrugissues
TABLE08
SUMMARISED DEVELOPMENT NEEDS AND JOb FUNCTION
VICSERV TRAININGNEEDSANALYSISREPORT•2010 36
PROFILEOFThESUPPORTWORKER
APPENDIX3
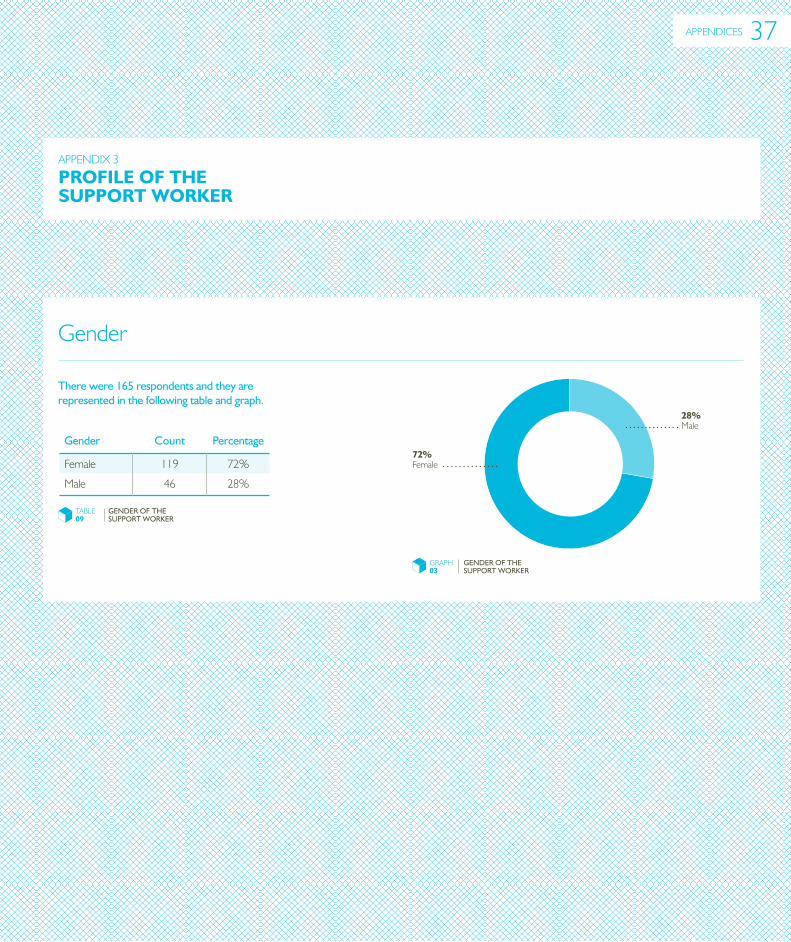
Gender
There were 165 respondents and they are represented in the following table and graph.
Gender
Count
Percentage
Female 119 72%
Male 46 28%
TABLE09
GENDER OF THE SUPPORT WORKER
GRAPH03
GENDER OF THE SUPPORT WORKER
72%Female
28%Male
APPENDICES 37
VICSERV TRAININGNEEDSANALYSISREPORT•2010
APPENDIX3(CONT’D)
Employmentstatus Agedistribution
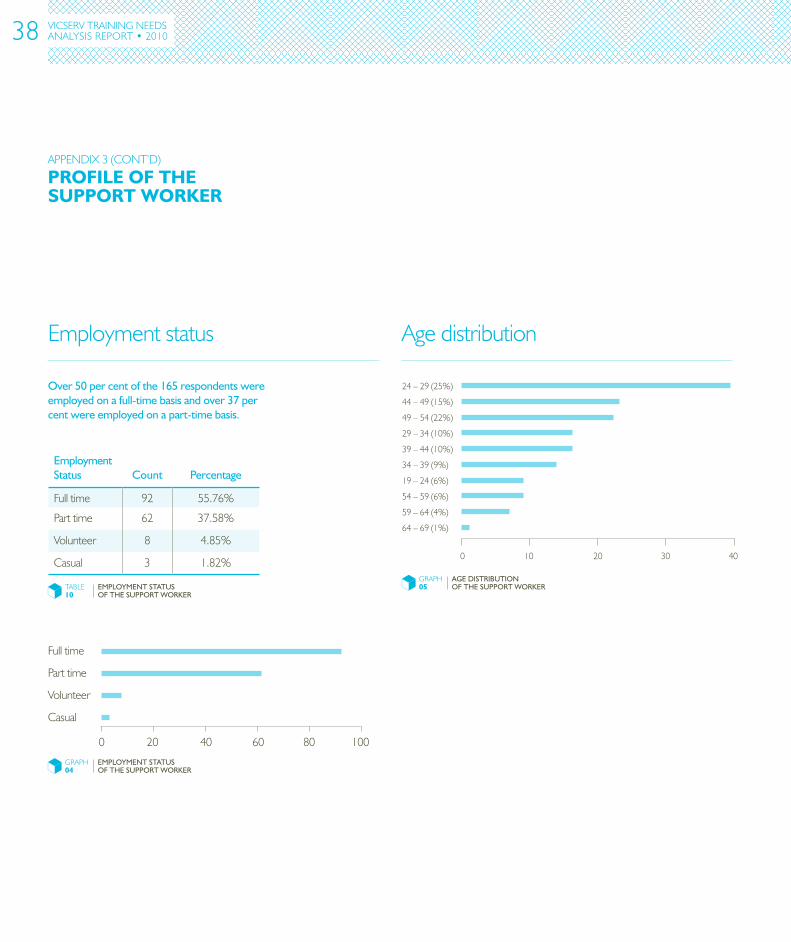
24–29(25%)
44–49(15%)
49–54(22%)
29–34(10%)
39–44(10%)
34–39(9%)
19–24(6%)
54–59(6%)
59–64(4%)
64–69(1%)
0 2010 30 40
GRAPH05
AGE DISTRIbUTION OF THE SUPPORT WORKER
Over 50 per cent of the 165 respondents were employed on a full-time basis and over 37 per cent were employed on a part-time basis.
Employment Status
Count
Percentage
Fulltime 92 55.76%
Parttime 62 37.58%
Volunteer 8 4.85%
Casual 3 1.82%
TABLE10
EMPLOYMENT STATUS OF THE SUPPORT WORKER
GRAPH04
EMPLOYMENT STATUS OF THE SUPPORT WORKER
Fulltime
Parttime
Volunteer
Casual
0 20 40 60 80 100
PROFILEOFThESUPPORTWORKER
38
ThERANGEOFMENTALhEALThSERVICESDELIVEREDBYCOMMUNITY-BASEDORGANISATIONSVARIESENORMOUSLY,FROMINTENSIVEPERSONALSUPPORTTOMUTUALSUPPORTANDSELF-hELP.
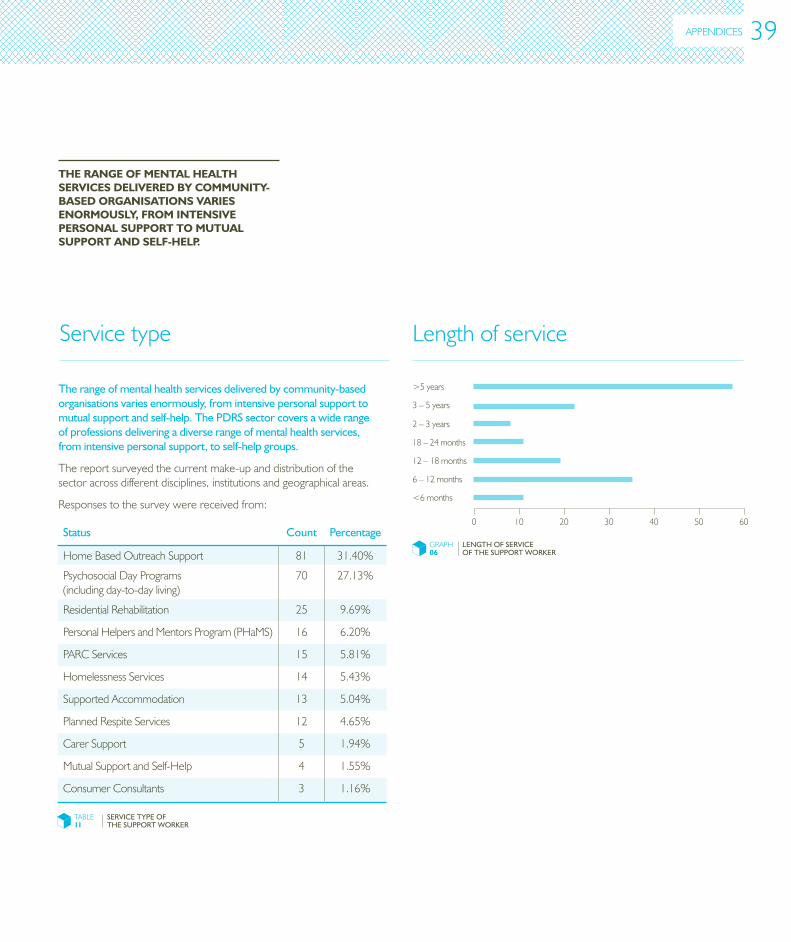
The range of mental health services delivered by community-based organisations varies enormously, from intensive personal support to mutual support and self-help. The PDRS sector covers a wide range of professions delivering a diverse range of mental health services, from intensive personal support, to self-help groups.
Thereportsurveyedthecurrentmake-upanddistributionofthesectoracrossdifferentdisciplines,institutionsandgeographicalareas.
Responsestothesurveywerereceivedfrom:
Servicetype
Status
Count
Percentage
HomeBasedOutreachSupport 81 31.40%
PsychosocialDayPrograms(includingday-to-dayliving)
70 27.13%
ResidentialRehabilitation 25 9.69%
PersonalHelpersandMentorsProgram(PHaMS) 16 6.20%
PARCServices 15 5.81%
HomelessnessServices 14 5.43%
SupportedAccommodation 13 5.04%
PlannedRespiteServices 12 4.65%
CarerSupport 5 1.94%
MutualSupportandSelf-Help 4 1.55%
ConsumerConsultants 3 1.16%
TABLE11
SERVICE TYPE OF THE SUPPORT WORKER
Lengthofservice
GRAPH06
LENGTH OF SERVICE OF THE SUPPORT WORKER
0 10 20 30 40 50 60
<6months
6–12months
12–18months
18–24months
2–3years
3–5years
>5years
APPENDICES 39
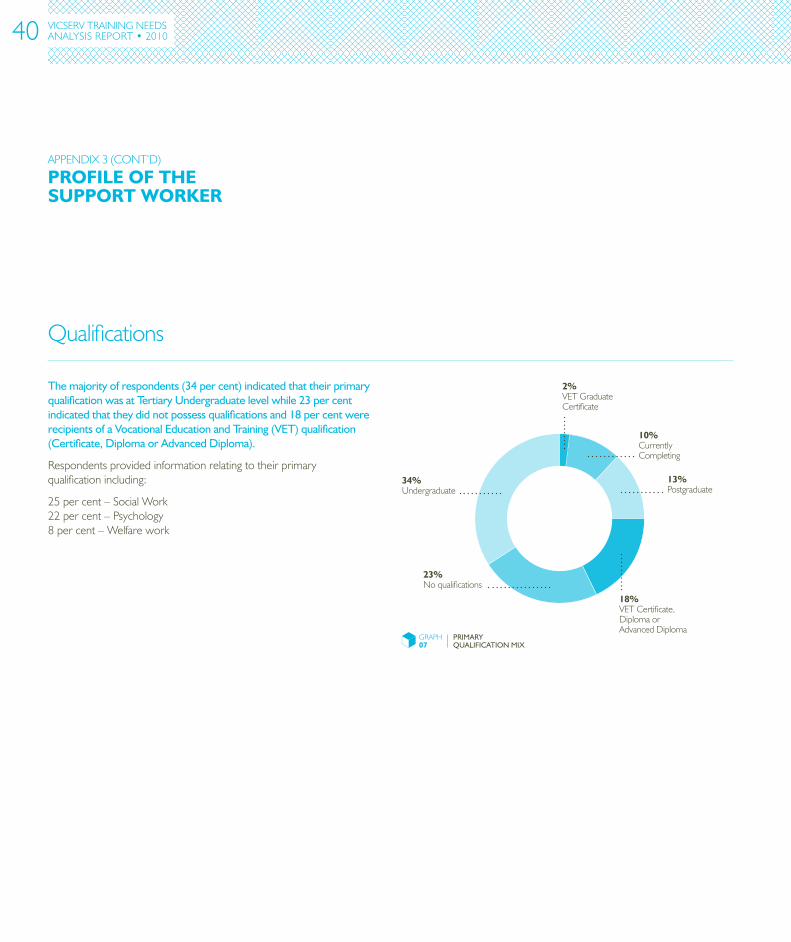
Qualifications
VICSERV TRAININGNEEDSANALYSISREPORT•2010
GRAPH07
PRIMARY QUALIFICATION MIX
34%Undergraduate
18%VETCertificate,DiplomaorAdvancedDiploma
23%Noqualifications
2%VETGraduateCertificate
10%CurrentlyCompleting
13%Postgraduate
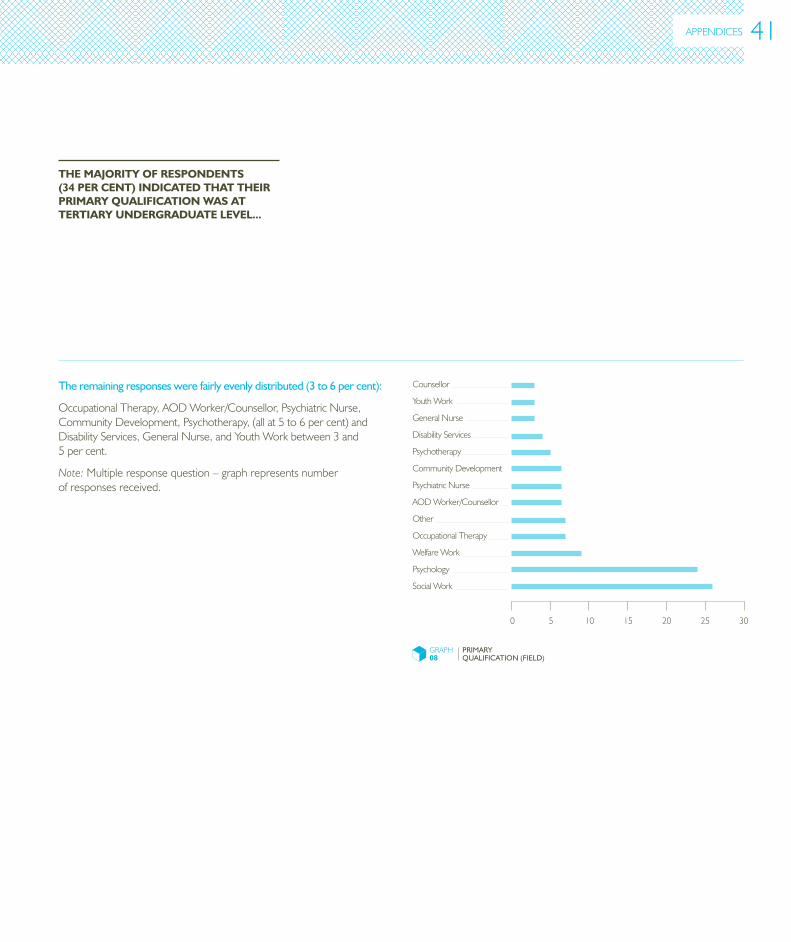
The majority of respondents (34 per cent) indicated that their primary qualification was at Tertiary Undergraduate level while 23 per cent indicated that they did not possess qualifications and 18 per cent were recipients of a Vocational Education and Training (VET) qualification (Certificate, Diploma or Advanced Diploma).
Respondentsprovidedinformationrelatingtotheirprimaryqualificationincluding:
25percent–SocialWork22percent–Psychology8percent–Welfarework
APPENDIX3(CONT’D)
PROFILEOFThESUPPORTWORKER
40
APPENDICES
ThEMAjORITYOFRESPONDENTS(34PERCENT)INDICATEDThATThEIRPRIMARYqUALIFICATIONWASATTERTIARYUNDERGRADUATELEVEL...
The remaining responses were fairly evenly distributed (3 to 6 per cent):
OccupationalTherapy,AODWorker/Counsellor,PsychiatricNurse,CommunityDevelopment,Psychotherapy,(allat5to6percent)andDisabilityServices,GeneralNurse,andYouthWorkbetween3and5percent.
Note: Multipleresponsequestion–graphrepresentsnumberofresponsesreceived.
GRAPH08
PRIMARY QUALIFICATION (FIELD)
0 5 10 15 20 25 30
Counsellor
YouthWork
GeneralNurse
DisabilityServices
Psychotherapy
CommunityDevelopment
AODWorker/Counsellor
Other
OccupationalTherapy
WelfareWork
Psychology
SocialWork
PsychiatricNurse
41
Current/futureVETparticipation
VICSERV TRAININGNEEDSANALYSISREPORT•2010
PROFILEOFThESUPPORTWORKER
GRAPH09
CURRENT VET COURSE ENROLMENT
14%Other
32%DiplomaofCommunityServices(AOD)
4%CertificateIVinAlcoholandOtherDrugs
50%CertificateIVinMentalHealth
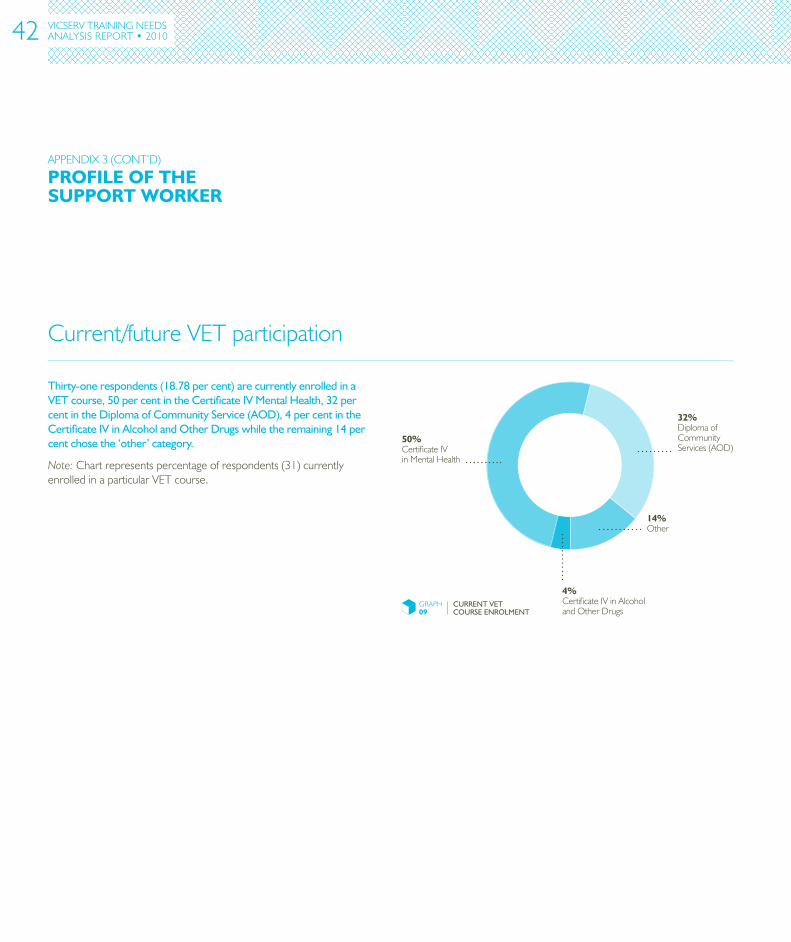
Thirty-one respondents (18.78 per cent) are currently enrolled in a VET course, 50 per cent in the Certificate IV Mental Health, 32 per cent in the Diploma of Community Service (AOD), 4 per cent in the Certificate IV in Alcohol and Other Drugs while the remaining 14 per cent chose the ‘other’ category.
Note:Chartrepresentspercentageofrespondents(31)currentlyenrolledinaparticularVETcourse.
APPENDIX3(CONT’D)
42

APPENDICES
ThIRTY-ONERESPONDENTS(18.78PERCENT)ARECURRENTLYENROLLEDINAVETCOURSE...
GRAPH10
INTEREST IN VET COURSE (COUNT) 0 10 20 30 40 50 60
DiplomaofCommunityServices(AOD)
DiplomaofCommunityServices(AOD&MentalHealth)
DiplomaofCommunityServices(MentalHealth)
CertificateIVMentalHealth
CertificateIVinAlcoholandOtherDrugs
Respondents were asked to indicate their interest in completing the following courses:
• CertificateIVinMentalHealth[CHC40508]
• CertificateIVinAlcoholandOtherDrugs[CHC40408]
• DiplomaofCommunityServices(AlcoholandOtherDrugs[CHC50208]
• DiplomaofCommunityServices(MentalHealth)[CHC50308]
• DiplomaofCommunityServices(AlcoholandOtherDrugsandMentalHealth)[CHC50408]
Note:Multipleresponsequestion–graphrepresentsnumberofresponsesreceived.
43
VICSERV TRAININGNEEDSANALYSISREPORT•2010
Professionaldevelopmentinfluences
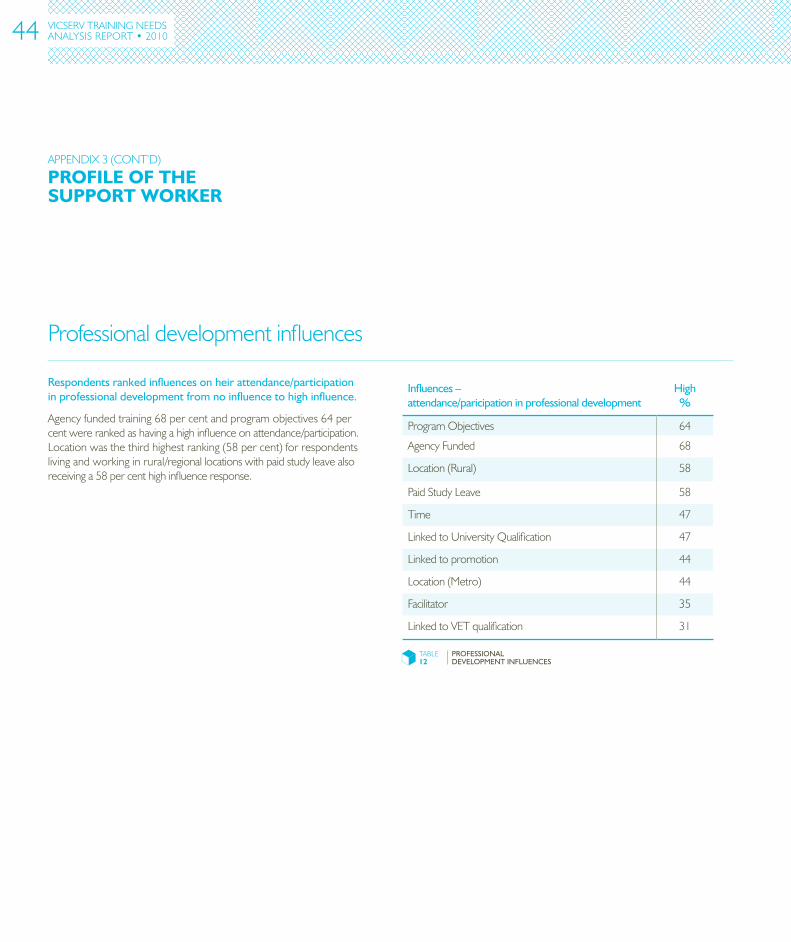
Respondents ranked influences on heir attendance/participation in professional development from no influence to high influence.
Agencyfundedtraining68percentandprogramobjectives64percentwererankedashavingahighinfluenceonattendance/participation.Locationwasthethirdhighestranking(58percent)forrespondentslivingandworkinginrural/regionallocationswithpaidstudyleavealsoreceivinga58percenthighinfluenceresponse.
Influences – attendance/paricipation in professional development
High %
ProgramObjectives 64
AgencyFunded 68
Location(Rural) 58
PaidStudyLeave 58
Time 47
LinkedtoUniversityQualification 47
Linkedtopromotion 44
Location(Metro) 44
Facilitator 35
LinkedtoVETqualification 31
TABLE12
PROFESSIONAL DEVELOPMENT INFLUENCES
PROFILEOFThESUPPORTWORKER
APPENDIX3(CONT’D)
44
PROFILEOFThEMANAGER
APPENDIX4
Gender
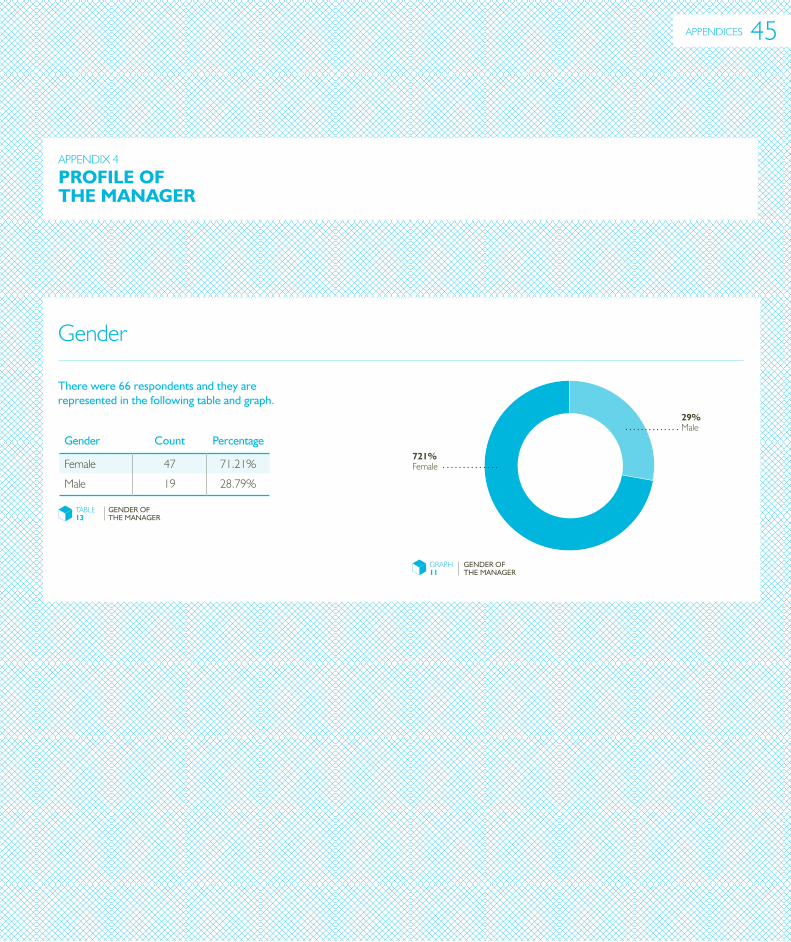
There were 66 respondents and they are represented in the following table and graph.
Gender
Count
Percentage
Female 47 71.21%
Male 19 28.79%
TABLE13
GENDER OF THE MANAGER
GRAPH11
GENDER OF THE MANAGER
721%Female
29%Male
APPENDICES 45
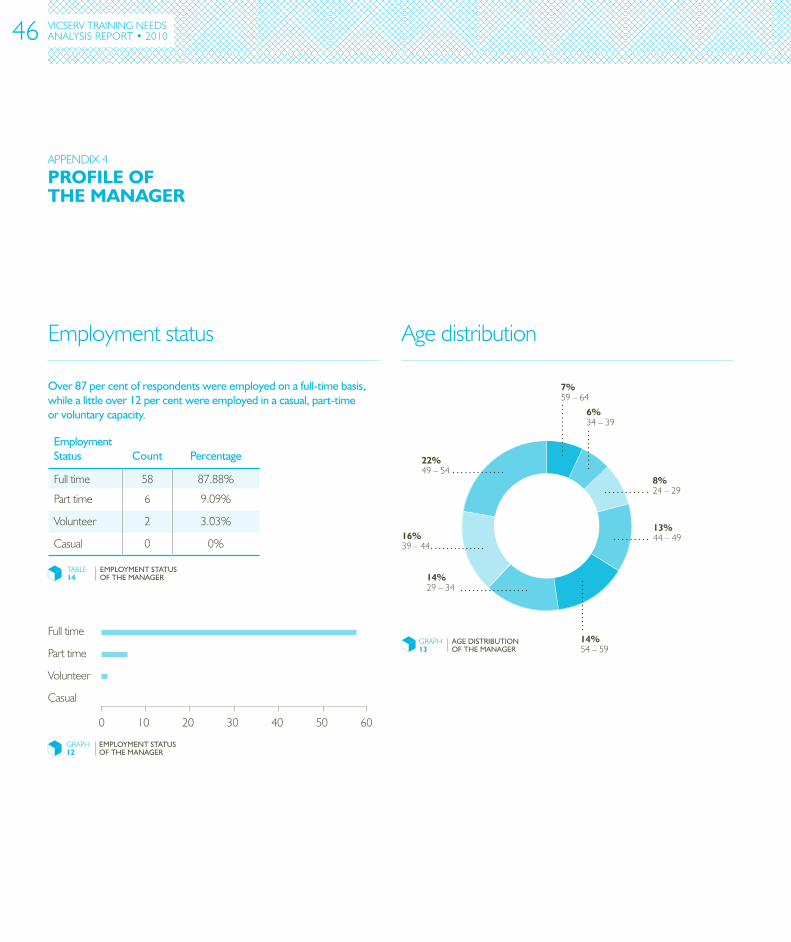
Employmentstatus Agedistribution
Over 87 per cent of respondents were employed on a full-time basis, while a little over 12 per cent were employed in a casual, part-time or voluntary capacity.
VICSERV TRAININGNEEDSANALYSISREPORT•2010
PROFILEOFThEMANAGER
APPENDIX4
Employment Status
Count
Percentage
Fulltime 58 87.88%
Parttime 6 9.09%
Volunteer 2 3.03%
Casual 0 0%
TABLE14
EMPLOYMENT STATUS OF THE MANAGER
GRAPH12
EMPLOYMENT STATUS OF THE MANAGER
Fulltime
Parttime
Volunteer
Casual
0 10 20 30 40 50 60
GRAPH13
AGE DISTRIbUTION OF THE MANAGER
22%49–54
14%54–59
14%29–34
16%39–44
7%59–64
6%34–39
8%24–29
13%44–49
46
APPENDICES
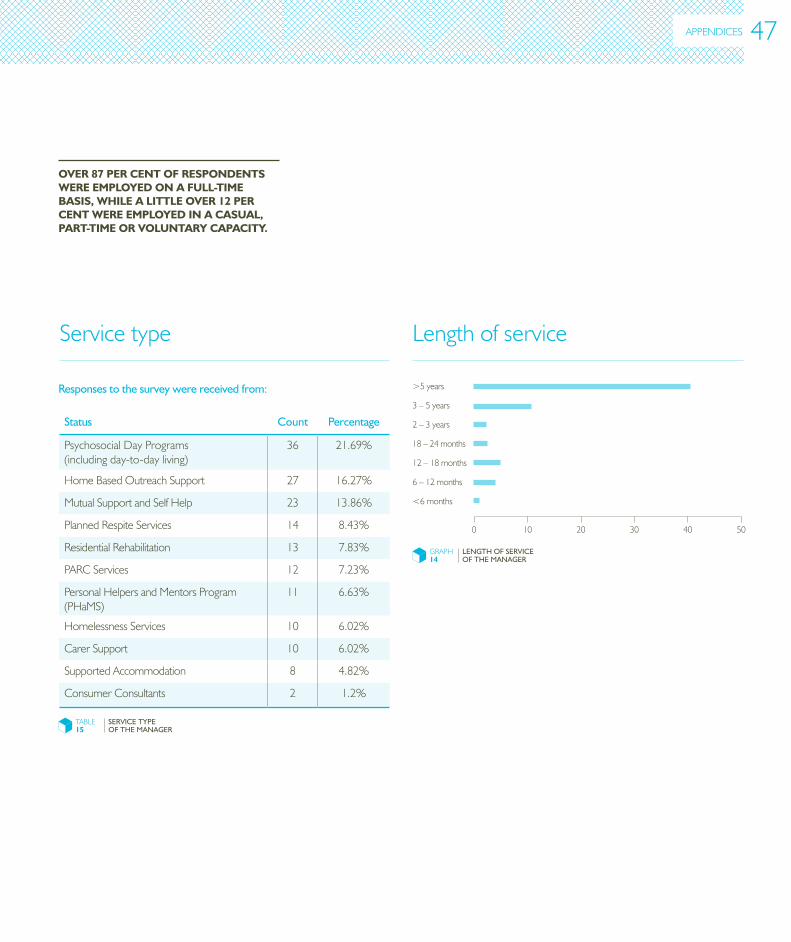
Responses to the survey were received from:
Servicetype Lengthofservice
OVER87PERCENTOFRESPONDENTSWEREEMPLOYEDONAFULL-TIMEBASIS,WhILEALITTLEOVER12PERCENTWEREEMPLOYEDINACASUAL,PART-TIMEORVOLUNTARYCAPACITY.
Status
Count
Percentage
PsychosocialDayPrograms(includingday-to-dayliving)
36 21.69%
HomeBasedOutreachSupport 27 16.27%
MutualSupportandSelfHelp 23 13.86%
PlannedRespiteServices 14 8.43%
ResidentialRehabilitation 13 7.83%
PARCServices 12 7.23%
PersonalHelpersandMentorsProgram(PHaMS)
11 6.63%
HomelessnessServices 10 6.02%
CarerSupport 10 6.02%
SupportedAccommodation 8 4.82%
ConsumerConsultants 2 1.2%
TABLE15
SERVICE TYPE OF THE MANAGER
GRAPH14
LENGTH OF SERVICE OF THE MANAGER
0 10 20 30 40 50
<6months
6–12months
12–18months
18–24months
2–3years
3–5years
>5years
47
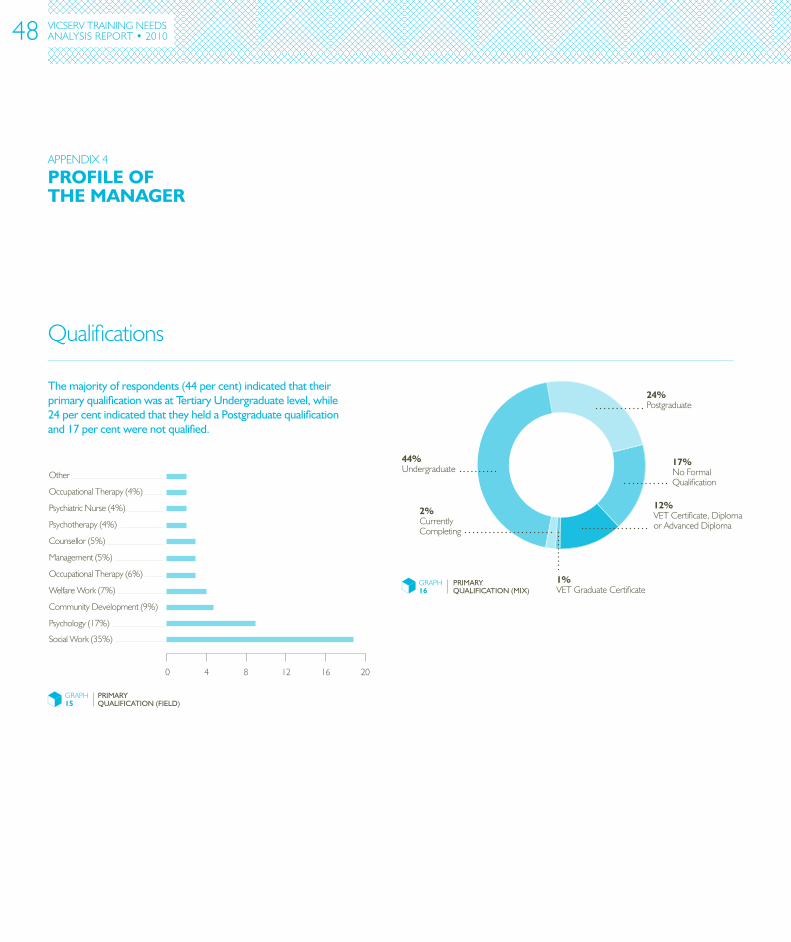
Qualifications
VICSERV TRAININGNEEDSANALYSISREPORT•2010
GRAPH16
PRIMARY QUALIFICATION (MIX)
44%Undergraduate
12%VETCertificate,DiplomaorAdvancedDiploma
17%NoFormalQualification
1%VETGraduateCertificate
2%CurrentlyCompleting
24%Postgraduate
The majority of respondents (44 per cent) indicated that their primary qualification was at Tertiary Undergraduate level, while 24 per cent indicated that they held a Postgraduate qualification and 17 per cent were not qualified.
PROFILEOFThEMANAGER
APPENDIX4
GRAPH15
PRIMARY QUALIFICATION (FIELD)
0 4 8 12 16 20
Other
OccupationalTherapy(4%)
PsychiatricNurse(4%)
Psychotherapy(4%)
Management(5%)
OccupationalTherapy(6%)
WelfareWork(7%)
CommunityDevelopment(9%)
Psychology(17%)
SocialWork(35%)
Counsellor(5%)
48
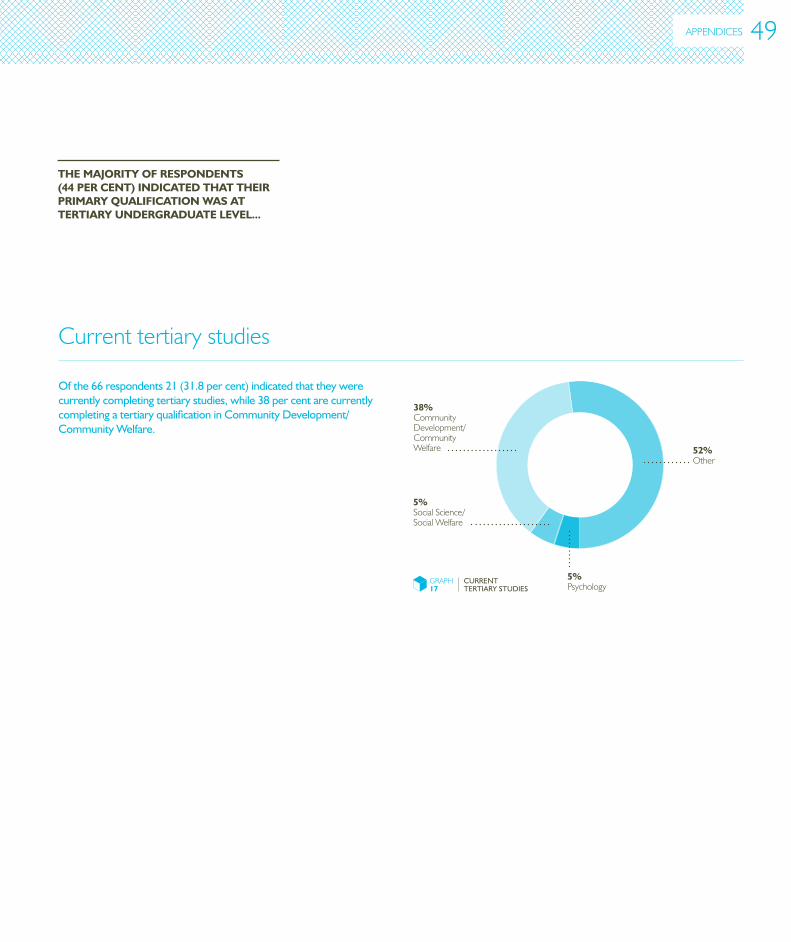
Of the 66 respondents 21 (31.8 per cent) indicated that they were currently completing tertiary studies, while 38 per cent are currently completing a tertiary qualification in Community Development/Community Welfare.
Currenttertiarystudies
ThEMAjORITYOFRESPONDENTS(44PERCENT)INDICATEDThATThEIRPRIMARYqUALIFICATIONWASATTERTIARYUNDERGRADUATELEVEL...
GRAPH17
CURRENT TERTIARY STUDIES
52%Other
5%Psychology
5%SocialScience/SocialWelfare
38%CommunityDevelopment/CommunityWelfare
APPENDICES 49
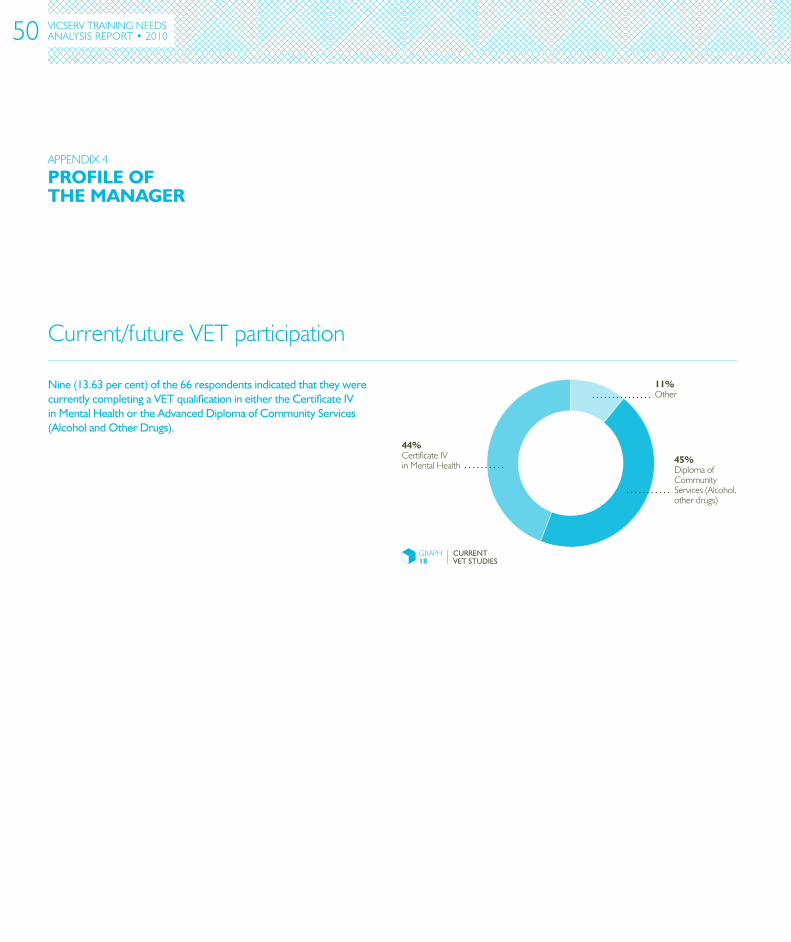
Current/futureVETparticipation
VICSERV TRAININGNEEDSANALYSISREPORT•2010
GRAPH18
CURRENT VET STUDIES
44%CertificateIVinMentalHealth
45%DiplomaofCommunityServices(Alcohol,otherdrugs)
11%Other
Nine (13.63 per cent) of the 66 respondents indicated that they were currently completing a VET qualification in either the Certificate IV in Mental Health or the Advanced Diploma of Community Services (Alcohol and Other Drugs).
PROFILEOFThEMANAGER
APPENDIX4
50
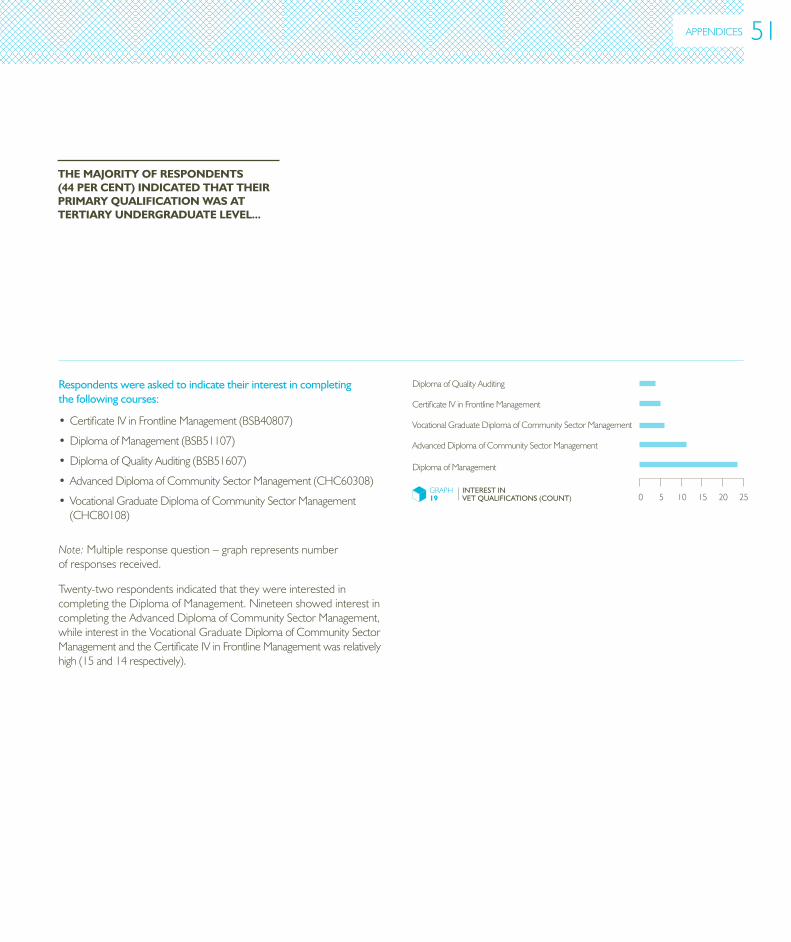
Respondents were asked to indicate their interest in completing the following courses:
• CertificateIVinFrontlineManagement(BSB40807)
•DiplomaofManagement(BSB51107)
•DiplomaofQualityAuditing(BSB51607)
• AdvancedDiplomaofCommunitySectorManagement(CHC60308)
• VocationalGraduateDiplomaofCommunitySectorManagement(CHC80108)
Note:Multipleresponsequestion–graphrepresentsnumberofresponsesreceived.
GRAPH19
INTEREST IN VET QUALIFICATIONS (COUNT)
DiplomaofQualityAuditing
CertificateIVinFrontlineManagement
VocationalGraduateDiplomaofCommunitySectorManagement
AdvancedDiplomaofCommunitySectorManagement
DiplomaofManagement
0 5 10 15 20 25
ThEMAjORITYOFRESPONDENTS(44PERCENT)INDICATEDThATThEIRPRIMARYqUALIFICATIONWASATTERTIARYUNDERGRADUATELEVEL...
Twenty-tworespondentsindicatedthattheywereinterestedincompletingtheDiplomaofManagement.NineteenshowedinterestincompletingtheAdvancedDiplomaofCommunitySectorManagement,whileinterestintheVocationalGraduateDiplomaofCommunitySectorManagementandtheCertificateIVinFrontlineManagementwasrelativelyhigh(15and14respectively).
APPENDICES 51
VICSERV TRAININGNEEDSANALYSISREPORT•2010
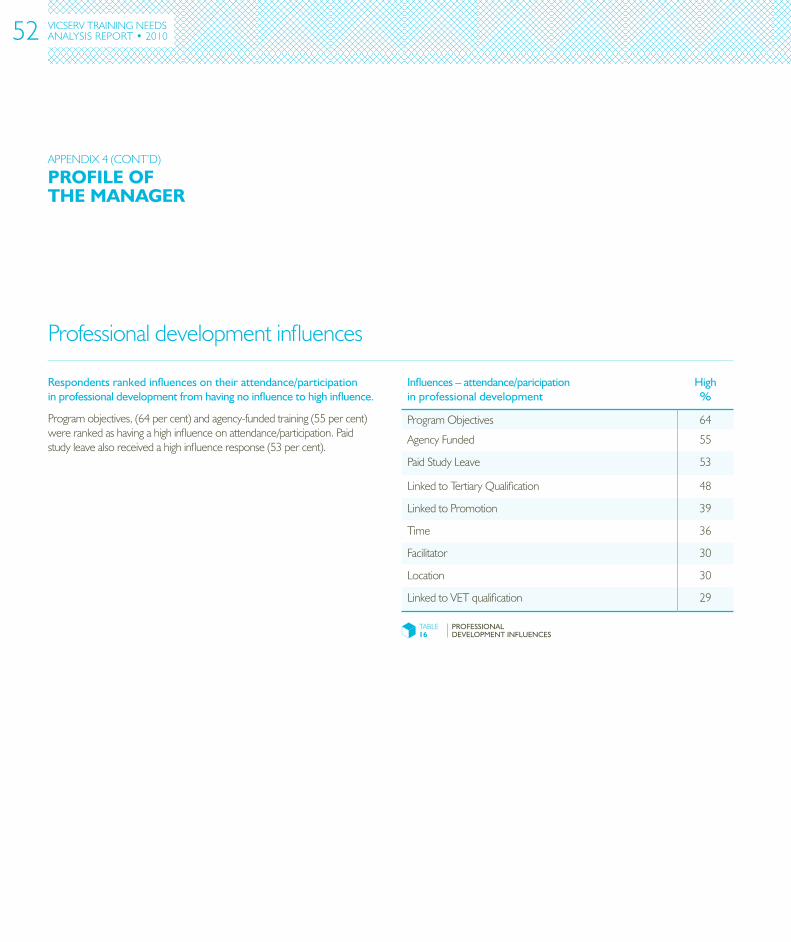
Professionaldevelopmentinfluences
Respondents ranked influences on their attendance/participation in professional development from having no influence to high influence.
Programobjectives,(64percent)andagency-fundedtraining(55percent)wererankedashavingahighinfluenceonattendance/participation.Paidstudyleavealsoreceivedahighinfluenceresponse(53percent).
Influences – attendance/paricipation in professional development
High %
ProgramObjectives 64
AgencyFunded 55
PaidStudyLeave 53
LinkedtoTertiaryQualification 48
LinkedtoPromotion 39
Time 36
Facilitator 30
Location 30
LinkedtoVETqualification 29
TABLE16
PROFESSIONAL DEVELOPMENT INFLUENCES
PROFILEOFThEMANAGER
APPENDIX4(CONT’D)
52
APPENDICES
Relevant accredited training
ThemostrecentNationalCommunityServicesTrainingPackageendorsedinDecember2008includesqualificationsandskillsetsthatencompasstheskillsareasrequiredbytheMetalHealthworkforce.Thequalificationsprovidesuitableentry-leveldevelopmentfornewentrantstomanyPDRSroles,aswellasspecificskillsetsformoreexperiencedworkers.
Relevant entry-level qualifications for PDRS workers
Thefollowingqualificationshavebeenreviewedandmodifiedtoreflecttheneedsoftheindustry:
•CertificateIVinMentalHealth
• DiplomaofCommunityServices(AlcoholandOtherDrugs)
• DiplomaofCommunityServices(MentalHealth)
• DiplomaofCommunityServices(AlcoholandOtherDrugsandMentalHealth)
Further development for skilled PDRS workers
TherevisedTrainingPackageprovidesspecificskillsetstoaugmentaworker’sbasequalificationwithmorespecialisedknowledgeandskill.ThefollowingskillsetsaddresshighprioritydevelopmentneedsexpressedbythePDRSsectorworkersandserviceorganisations:
•AlcoholandOtherDrugsskillset
• Mentalhealthskillset–includingrecogniseindividualsatrisk
• Mentalhealthskillset–includingrespondtoriskofsuicide.
DEVELOPMENTCURRENTLYAVAILABLETOThEPDRSSECTOR
APPENDIX5
53
RelevantVICSERVandotherPDRSsectordevelopmentavailable
VICSERV currently provides the following courses that are relevant to the development needs:
•CertificateIVinMentalHealth
• VICSERVtrainingonbaselinefoundationskills:
OrientationtoPDRS
PrinciplesandPracticeofPsychiatricDisabilityRehabilitationandSupport
BeingaKeyworker1–Establishingtherelationship
BeingaKeyworker2–Therehabilitationjourney
BeingaKeyworker3–Goalsetting
RecordingClientInformation
WorkingwithclientswithDualDiagnosis
• IntroductiontoMotivationalInterviewing
•MentalHealthFirstAid
•BorderlinePersonalityDisorder–Introduction
• IntroductiontoDualDiagnosis–MentalHealthandAlcoholandOtherDrugs
•AppliedSuicideInterventionSkills(ASIST)
•ProfessionalSupervision
•DiplomaofManagement
•DiplomaofQualityAuditing
DEVELOPMENTCURRENTLYAVAILABLETOThEPDRSSECTOR
APPENDIX5(CONT’D)
54

PsychiatricDisabilityServicesofVictoria(VICSERV)Level2,22HorneStreet,ElsternwickVictoria3185AustraliaT0395197000F0395197022training@vicserv.org.auwww.vicserv.org.au






























