Embed Size (px)
Citation preview

Neo-adjuvant therapies for RCC
Dr. Camillo PortaS.C. di Oncologia MedicaI.R.C.C.S. Policlinico San Matteo, Pavia
Back to the basics:terminology
• Neo-adjuvant therapy:– Treatment given as a first step to shrink a
tumor before the main treatment, which is usually surgery, is given
NCI Dictionary of Cancer Terms

Neo-adjuvant Tx:pros and cons
Pro Cons
Litmus test for patients who will do well Therapy may impact wound healing and recoveryPotential for higher incidence of wound complications
Incorporates cytoreductive surgery to examine tissue before and after therapy for endpoint targets
Local tumor progression in non-responders increases complexity of the surgeryMore “ectomies”= Worse outcome
May see responses in the primary tumor not seen before
Timing is everythingWhy interrupt a therapeutic response?Who wants to operate on therapy refractory disease?
Eliminates unnecessary and morbid surgery in patients who don’t respond

Are we able to achievetumor shrinkage?
Escudier B, et al. ECCO 13 – the European Cancer Conference, Paris, October 30-November 3, 2005; abs.794.
Sorafenib treatment
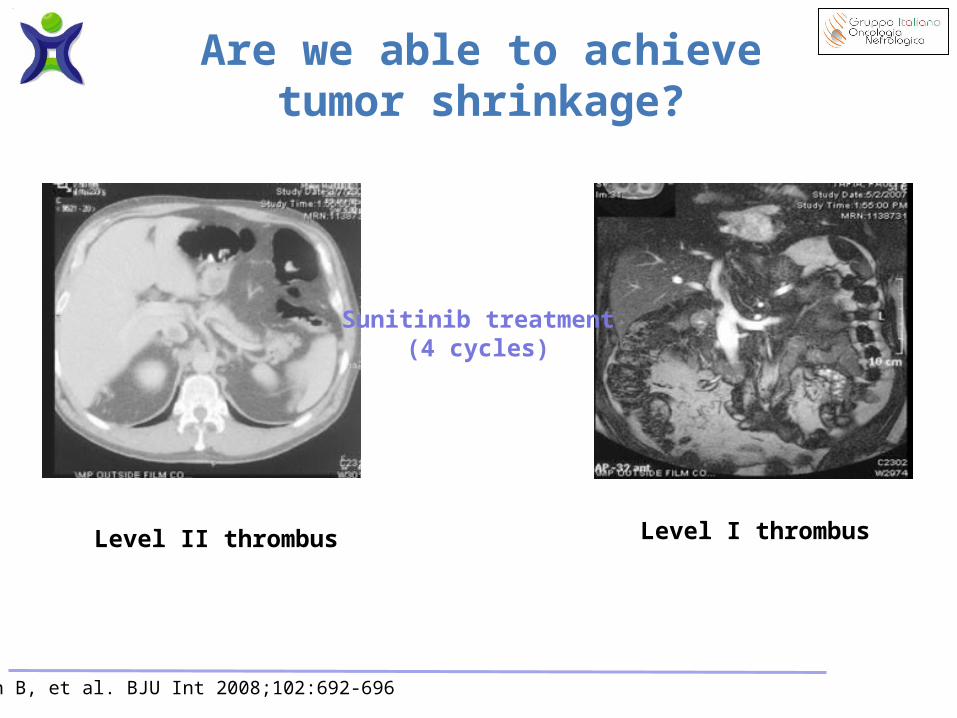
Shuch B, et al. BJU Int 2008;102:692-696
Level II thrombus Level I thrombus
Sunitinib treatment(4 cycles)
Are we able to achievetumor shrinkage?

Jonasch E, et al. J Clin Oncol 2009;27:4076-81
Baseline 8 Weeks of therapy
Bevacizumab treatment
Are we able to achievetumor shrinkage?

The issue is: how much tumorshrinkage are we really able to achieve?
Van der Veldt AAM, et al. Clin Cancer Res 2008;14:2431-6; Thomas AA, et al. J Urol 2009;181:518-23;Jonasch E, et al. J Clin Oncol 2009;27:4076-81
Primary Tumor Regressionn=45 (%)
>20% growth 1 (2)
10-20% growth 2 (4)
0-10% growth 19 (42)
1-10% shrinkage 13 (29)
11-20% shrinkage 7 (16)
20-30% shrinkage 3 (7)

CG Wood, personal communication
Are there risks with suchan approach?

Are there risks with suchan approach?
CG Wood, personal communication
Pre-Surgical Therapy
Immediate Surgery Total p
Overall 25 (43.1) 28 (28.7) 54 (33.5) 0.048
Peri-operative Death 1 (1.7) 2 (2.0) 3 (1.9) 0.91
Readmission to Hospital 6 (10.3) 11 (11.0) 17 (10.8) 0.90
Bleeding 1 (1.7) 2 (2.0) 3 (1.9) 0.91
Thromboembolic 5 (8.6) 5 (5.0) 10 (6.3) 0.36
Cardiac 1 (1.7) 3 (3.0) 4 (2.5) 0.63
Gastrointestinal 5 (8.6) 9 (8.9) 14 (8.8) 0.95
Infection 4 (6.9) 6 (5.9) 10 (6.3) 0.81
Superficial Wound Healing 12 (20.7) 2 (2.0) 14 (8.8) <0.001
Fascial dehiscence 2 (3.5) 0 (0.0) 2 (1.3) 0.06
Chylous Ascites 2 (3.5) 6 (5.9) 8 (5.0) 0.49

CG Wood, personal communication
Univariate analysis Odds Ratio 95 % CI P
Overall Complications 1.98 1.00, 3.89 0.049*
Peri-operative Death 0.87 0.08, 9.79 0.91
Readmission to Hospital0.93 0.33, 2.67 0.90
Bleeding 0.87 0.08, 9.79 0.91
Thromboembolic 1.81 0.50, 6.54 0.37
Cardiac 0.57 0.06, 5.64 0.63
Gastrointestinal 0.96 0.31, 3.03 0.95
Infection 1.17 0.32, 4.34 0.81
Superficial Wound Healing 12.91 2.78, 60.06 0.001*
Chylous Ascites 0.57 0.11, 2.90 0.49
Are there risks with suchan approach?

CG Wood, personal communication
• *Adjusted for:
– Pre-operative albumin
– Smoking status (never, current, former)
– Pre-operative hemoglobin
– Laparoscopic vs open surgery
– ECOG performance status
– Body mass index
– Age
Odds Ratio* 95% CI p-value
Superficial Wound Healing 19.7 2.13, 181.88 <0.01
Are there risks with suchan approach?

How to deal with these issues?
Withheld treatment for at least 2 or 3 half-lives before and after surgery
Max
imum
resp
onse
Days after wounding (log scale)
I. inflammation
II. cell proliferationand matrix deposition
III. matrix remodelling
Bleeding
Coagulation
Platelet activation
Complement activation
Granulocytes
Phagocytosis
Fibroplasia
Angiogenesis
Re-epithelization
Extracelluar matrix sythesis
Collagens
Fibronectin
Proteoglicans Macrophages
Cytokines
Stages of wound healing
Extracellular matrixsynthesis, degradationand remodelling
Tensile strength
Cellularity
Vascularity
Consider drug half-life
Temsirolimus: 17 hrs
Sorafenib: 24-48 hrs
Sunitinib: 60-110 hrs
Bevacizumab: 14-21 days
Pazopanib: 30.9 hrs

Conclusions
CG Wood, personal communication
• Present, initial, body of evidencewould suggest that
significant primary tumor downstagingwill not be realized with the current generation
of targeted therapy agents