Embed Size (px)
Citation preview
NeoiasKa Medical Center
Center for Clinical and
Translational Research
Standard Operating Procedure
W Nebraska. � ... Medicine
Section Clinical Research Center
Title: Lab Specimens
SOP Number: SOP-17
Date Created: November 1. 2010
Date Reviewed/Modified: April 1, 2019
Version Number:
PURPOSE: This standard operating procedure (SOP) outlines the basic steps required when handling laboratory specimens from collection through processing and shipping so that the integrity of the specimen is preserved for analysis, thus providing information leading to appropriate treatment decisions or safety assessment of the participant during a clinical trial.
SCOPE: This SOP applies to all Clinical Research Center (CRC) personnel who are involved ( or may be involved) laboratory specimen collection, transport, processing, and storage for a clinical research trial.
PERSONNEL RESPONSIBLE: Nurses may draw blood samples via venipuncture and vascular access devices per Nebraska Medicine (NM) Nursing Policy and Procedures.
Research Assistants may draw blood via venipuncture only.
PROCEDURES:
Specimen Collection Impeccable clinical practice must be utilized when obtaining specimens from research participants, as these specimens represent important data required by the investigator. Methods used by staff when obtaining specimens must be accurately performed per the study protocol.
A training module is available through Nebraska Medicine manager of Clinical Laboratory Support Services. Phlebotomy and Specimen processing competency checklists and exam are to be completed by all appropriate staff (see attachments).
All patients are identified with at least two patient identifiers (patient's name and date of birth -room number cannot be used) whenever taking blood samples or other lab samples per NM policy Rll O Patient Identification.
1. Venipuncture Blood collection
Attention must be given to the accuracy of collecting the specimens at the proper time, using the correct collection tubes, drawing in the correct order, and handling and transporting in the proper manner. All CRC personnel will follow NM Nursing Policy and procedures related to venipuncture blood collection.
2. Vascular Access collection
Attention must be given to the accuracy of collecting the specimens at the proper time,
using the correct collection tubes, drawing in the correct order, and handling and
Page 1 of 4
NeBiasKa Medical Center
Center for Clinical and
Translational Research
Standard Operating Procedure
W Nebra.ska� .. Medicine
Section Clinical Research Center
Title: Lab Specimens
Date Created: November 1, 2010
Date Reviewed/Modified: April 1, 2019
Version Number: SOP Number: SOP-17
transporting in the proper manner. All CRC nursing personnel will follow NM Nursing
Policy and Procedures related to vascular access device.
3. Urine Specimens• Random urine specimens can be collected at any time; they are usually obtained without
prior participant preparation.
• One-time composite urine specimens are collected over a period that may range from 2 to24 hours. To collect a timed specimen, instruct the participant to void and discard the firstspecimen. This is annotated as the start time of the test. All subsequent urine is saved in aspecial container for the designated period of time. A preservative may be used tomaintain stability during the collection period or the container can be kept on ice orrefrigerated. Instruct participants not to void directly into the container as somepreservatives are acids, which should not be splashed on the skin. At the end of thespecified time period, the participant should void and add this urine to the container;thereby completing the collection process. The collection container should be labeledwith the participant's name or study identification number, the starting date/time, theending date/time, the name of the test, and the preservative (if any). Indicate on thelaboratory request any medications that may affect test results.
• All urine specimens must be placed in a sealed container, labeled and delivered to theappropriate laboratory.
4. Other Specimens
Specimen handling and processing • Protocols often require special handling of specimens from the time of collection until
they are processed. Protocols that specify special handling will be accurately followed.• Specimens for ammonia, blood gas determinations, acid phosphatase, lactate, pyruvate
and certain hormone tests must be kept at 4°C from the time the blood is drawn until thespecimens are analyzed or until the serum or plasma is separated from the cells.
• Specimens for bilirubin, carotene or Vitamin D must be protected from light to avoidphoto degradation.
• Since improper handling and specimen processing can result in unusable specimens, greatcare must be taken to ensure that blood or urine specimens are handled and processedproperly until analysis. Review thoroughly the Clinical Trial protocol and lab manualprocedures for a study prior to handling specimens for the study. This information willbe communicated to ·an staff involved with the protocol.
Page 2 of 4
Ne15ffisKa Medical Center
Center for Clinical and
Translational Research
Standard Operating Procedure
W Nebraska �,.. Medicine
Section Clinical Research Center
Title: Lab Specimens
SOP Number: SOP-17
Date Created: November 1. 2010
Date Reviewed/Modified: April 1, 2019
Version Number:
• Frozen specimens- CRC has available -20° and-80°C freezer for freezing and storingspecimens.
• Specimens will always be labeled with two identifiers when processed for a central lab.
5. Shipping Specimens
Ship lab specimens according to study-specific lab manuals and/or protocols
ASSOCIATED FORMS: Quality collections: the phlebotomist's role in pre-analytical errors
SOP-17 Attachment B MLO article_2019.1
Phlebotomy and Specimen Competency:
SOP-17 Phlebotomy Skills Checklist.docx
D SOP-17 Specimen
Processing Compete
D SOP-17 Specimen
Processing Compete
RESOURCES: Nebraska Medicine: Rll0 Patient Identification Nebraska Medicine Nursing Policy and Procedures:
• Lab-7, Venipuncture Blood Collection by Evacuated Tube, S ringe Method, orButterfl Device
• Lab-1 Laboratory Testing, Ancillary: Blood Glucose• Lab-2 - Laboratory Testing, Ancillary: Fecal Occult Blood - Fecal Application
only• Lab-9 Laboratory Testing, Ancillary: Fecal Occult Blood-Application and Test
Development
Page 3 of 4
Nel5ra5Ka Medical Center
Center for Clinical and
Translational Research
Standard Operating Procedure
W Nebraska�
"'If
Medicine
Section Clinical Research Center
Title: Lab Specimens
SOP Number: SOP-17
Date Created: November 1. 2010
Date Reviewed/Modified: April 1, 2019
Version Number:
• V AD-2 Intravenous Catheter Flushing: Push Pause Technique• V AD-4 Blood Draws via Central Lines
Staff Accountability:
Developed By: Director of Clinical Research Operations, Clinical Research Center Associate Vice Chancellor for Clinical Research
Reviewed By: Director of Clinical Research Operations, Clinical Research Center
Department Approval
Signed��J\L)..,lb, ) Directoc �ihicales�ch Operations
Page 4 of 4
Signed Medical Director of Clinical Research Center

SOP 17 Attachment
LAB MANAGEMENT
Quality collection: the phlebotornist's role in pre-analytical errors By Dennis J. Ernst, MT(ASCP), end Lisa 0. Ballance, MT(ASCP)
Medical error has been defined as a "failure to process.'' 1 The ultimate consequences of pre-analyticalerrors introduced during the specimen-collection
process span a bmad spectrum of negative outcomes. For the patient, these outcomes range from no detected harm to death. When patient blood specimens are required for examination, the collection process demands the knowledge nnd skills of a competent phlebotontlst. From receipt of the physician ·s order until examination of the specimen begins, the phlebotomist is often the primary guardian of specimen quality.
Studies have shown that a dedicated blood-culture team and/or phlebotomists are less likely than other healthcare
workers to contaminate b/ood�culture specimens.
Unfortunately, in today"s various healthcare settings. the role competent phlcbotomists piny in assuring specimen quality has been umlervalued. Evidem;e that their role is underestimateu includes:
■ disregard among other heallhcare professions for the complexily and invasive nature of phlebotomy procedures;
■ decentralization of phlebotomy services:■ lack of nationally i:Slablished minimum training and/or
certification requirements for U105e assigned blood collection rcsponsibilitie.�: and
■ lack of emphasis on. or a1.:cuss to. phlebotomy continuingeducation.
Here, we t>xplore some or the critical eoncepts all specimencollection pemmnel must master in order that physidun!I are not misled by laborntory results which constitute 70t;; of the objective infomrntion they receive on their patients' status. Strict adher�nce
30 September 2006 • MLO
to blood-collection procedures is the most effective meuns to ensure specimen quality during the collection and processing phaRes of laboratory te.<iting. Studies show up to 56% oflaboratory errors occur during the pre-analytic phase of testing.2 The expertise ofthe collector, therefore, is n pivotal link in the laboratory's chain of total quality-management activities.
Patient identification
Themosl potentially fatal pre-analytical error is improper patient identification. This is- basic but bears mentioning. Failure lo properly identify patients can lead them to be treated, diagnosed. medicated. and managed according to another patient's health status.
According to the Clinical and Laboratory Standa.rds Institute (CLSI, fonncrly NCCLS) an inpatient should be asked to st:ne her ft.ill name, address. birth date, and/or unique identification number. The infomllltion provjded must be compared with the information on the identincution bracelet. wbich must be attached to tl1e patient, and the test requisition or computer-genetute<l lubels brought to the bedside. All discrepancies must be reported to the appropriate caregiver according to facility policy and resolvetl before collection.
What if the patient is unable to speak her name due to language barriers or the patient's state of consciousness? The standard� require a caregiver or family member provide the information on the patient's behalf before drawing the specimen. 3 This requirementis justified in part by studies that show up to 16% ofidentification bracelet� contain erroneous infonnarion.4 Documenting the name or Lhe verifier is good risk management.
Emergency-room patients should he tagged with some sort of identification even if it is only a temporary number. The following items are not acceptable suhstitutcs for nn identification brncelel:
■ charts on the wall:■ water pitchers:• bed tags; and• identification bracelets 1wl attm:hcd to the patient.
There is no substitute for either having a hard identifier ,1uached to the patient, having the patil�nt speak her name. or having a caregiver vedfy the patient's ic.lentity.
For outpatients, CLSI recommendi. having the path-mt st.ite her name address, birth date. and/or unique identification n!Jmber and comparing that infonnntilln with the requisition or forms the patient brings to the draw station. Neither inpatients nor outpatients should be uskcd to aflinn their name as in .. Are you June Doc?'' Patients who muy Ix hard of hearing might misumkn;tanu and respond •·yes" just to he polite. A wiser solution i� to ask the puticnt to Ldl you her nume.
Co111ir111t•s all Jmg1· .U www.rnlo-onlir1e.con1

SOP 17 Attachment
L A B M A N A G E M E N T
Special-collection requirements
Special testing requirements must be met prior to collection. Fasting specimens must be collet.-ted after a lO- to 12-hour completedietary restriction of everything except water and medications.Although fasting for glucose must be ovemight, studies showthe difference between an overnight fast and a six- co nine-hourdaytime fast for lipids is not clinically significant.5
Because of the threat over- or under-medication can have onthe patient. strict adherence to the timine. of therapeutic dru"collections is imperative. Likewise. requir;m:nts that the patie,�be recumbent must be met in order for the physician 10 properlymanage the patient's health. Regular reviews of the laboratory'stest requirements help specimen-collection personnel remainmindful of 1ime- and posture-dependent tests.Collection restrictions
Few therapies threaten accurate b lood-test results more than theinfusion of intmvenous tluids. CLSI and most textbooks recommend avoiding draws from the same arm as nn active IV unlessabsolutely necessary. If unavoidable. CLSI recommends havingthe nurse or appropriate caregiver shut off 1he [V for two minutes, apply the tourniquet below the infusion site, and withdrawthe specimen below the tourniquet. Some authors rccommcriddiscarding the first Sec (cubic centimeters) ofbloml if possible.2,6Document the am1 from which the specimen was collected as wellas the race that it was drawn below an infusion site.. Dmwing above an rv 1ha1 has been temporarily shut off is
discouraged <lue to the potential for analyte contamination.3
Drawing blood at the same time thal dyes for radiological procedures are being or have been recently infused should be avoidedif possi bk:,
Neither venipuncturcs not skin punctures should be performedon the affected side of patients who have had a prior ma.�tectomy.3·7 Not only is there a risk of fluid imbalance in lhe affectedlimb, which can lead to erroneous results. the procedure puts thepatient at risk of painful short• or long�term lymphedema.Site preparation
Specimen collection personnel should also avoid sites that appearinfiltrated, infected, edematous, or burned - not only to protectthe patient from fmther complications but also to safeguard againstcollecting specimens that could be altered hy the condition. CLSladvises agaim,t drawing arterial specimens as a substitute forvenous blood when veins are clifficult to locate.
The best way to ensure a successful capillary collection is topre-warm the intended puncture site for three to five minutes.Applying a commercial infont heel wanner or warm compressnot exceeding 42"C to lhe skin increases blood flow to the areaup to sevenfold.7 Taking the time 10 perfonn this step promoteshigher quality �pecimens because the blood is obtained morequkkly and with less th.sue compression.
For routine venipuncture and capillary collections, cleansingthe si tc with 70% bopropyl alcohol is sufficient.Allowing the siteto air dry improves the alcohol's anti�cptic effect, as well as prevents hemolysis and contamination of the specimen that residualalcohol can causc.7 for capillary lead levels. a thorough scrubwith soap unt! water of the finger and nail area may be requireu.
For blo<Jd cultures. thepmbahility that a positive blood culturerepresent., infection rather than contamination is a function of32 September 2006 • MLO
the effectiveness of skin 1.mtisepsis ut the 1ime of the venipuncture. Growth of skin contaminanL-; muy not only be confusing toclinicians but also can be expensive for both the patient und the institution. 8 The traditional recommendation for skin preparation�as be:n the application of70% alcohol followed by or in conjunctmn with a 30- to 60-sccond friction scrub. Apply chlorhexidinc.povidone-iodine or 2% jodine tincture, and allow to air dry. Forinfants above two months of age, and for patients with iodinesensitivity, chlorhexidine gluconatc is rccommended.3 Regardlessof the type of skin prep:1ration used, meticulous care anl useptictechnique are essential 10 reduce contamination. S111dies haveshown that a dedicated blood-culture team and/or phlebotomistsare less likely than other healthcare workers co contuminate b loodculture specimens.8
Collection technique
The phlcbotomist's ability to select the appropriate supplies andequipment for each draw, based on an assessment of the patientand specimen test requirements, is crucial to assuring a successful collection. Equipment and supplies should be checked foracceptable expiration date$ and sterility. as appropriate.
When collecting capil lary specimens, proper positioning ofthe finger or heel will enhan\!e blood llow. To minimize the risksof tissue fluid contamination and hemolysis, the collector shouldwipe away the first formed drop of blood and avoid exertingexcessive pressure to the sUJrounding tbsue. When more thanone microcollcetion tube is required, the order of draw for eapil�lary collections as established by CLSJ should be followed.7 To preven1 the formalion of platelet clumps. microcollection tubescontaining EDTA should be collected first, followed by other-additive tubes and then non-additive tubes. Additive tubes shouldbe mixed periodically during collection. according to the tubemanufacturer's in�tructions. Once the appropriate volume ofbloodhas been obtained, tubes should be immediately capped and theblood mixed well by genlle inversion.
The appropriate number of test circles on newborn screeningcards should each be filled with one wel l-formed drop of bloodthn1 saturates the filter paper front to back. Care should be takennol to press the filter paper against the infant's hcd. Any technique that might scratch. compress, or indent the paper's fibersshould not be used.
Hcmolysis ii; the most common reason laboratories rejectspecimens.2 During venipuncture, rupture of red blood cells mayoccur for several reasons. including use of small bore needles ( i.e.,25-gauge), excessive pulling pressure on the syringe plunger,poor needle placement within the vein resulting in a slow draw.and aggressive mixing of the sample. To minimize the effects ofhemoconcentrarion during collection, the tourniquet should be released as i;oon a� possible after blood flow is Ci>tablished. Becausevigorous hand-pumping may also alter the concenrrntion of ce11ainunalyces in the blood, this practice should be discouraged.
For venipunctures. unless otherwise established b) facilityprotocol. tubes should be collected following the order of drawestablished by CLSI i n 2003 to prevent udditive carryover . .1 Additive carryover canMl be detected by the laboratory and. ns aresult. may lead to disastrnus consequences for the patient whenmedical decisions are based on altered result�. IL b imperative alladditive tube� be filled in the pmper order and adequately mixed�1ccording to the tube manufacturer·� instructions. Cotlection
CNrtinu,•� rm paflt' 34www.mlo-o11l ine.com

SOP 17 Attachment
LAB MANAGEMENT
tubes should be available in a variety of sizes to erumre minimum fill requirement� are met when presented with difficult or pediatric draws. According to CLSI, the order of draw is as follows:
I. Blood-culture tubes:2. Sodium-citrate tubes (e.g., blue stopper);3. Serum tubes with or without clot activator. wirh or without
gel separator (e.g., red, gold, speckled stopper);4. Heparin tubes with or withouL gel (e.g., green stopper):5. EDTA tubes {e.g .. lavender stopper); and6. Glycolytic inhibitor tubes (e.g., gray stopper).3
Underfilling of additive tubes alters the desired blood-l<Hmticoagulant ratio and, in the case of EDTA tubes. causes red-bloodcell shrinkage. An underfilled sodium-citrate tube will produce a falsely lengthened aPIT result.2 Manual filling of additive tubesshould also be avoided.
When using a winged blood-collection sec, a discard tube must be used to prime the tubing when a coagulation tube is the first or only tube drawn. For blood cultures, if both anaerobic and aerobic bottles -are included in the set, the nerobic bottle should be filled first. to remove air from the tubing. Underfilling of blood- culture bottles may result in failed recovery of organisms present in small quantities. whereas overfilling of blood- culture bottles may elicit a false-positive result during incubation.2 Inany case. improperly filled additive tubes and culture bottles may result in specimen rejection or, if tested, yield inaccurate results that jeopardize patient care.
In an age of technological advancement phlebotomy remains a manual procedure.
Collections from 1,•ascular access devices (VADs) should be avoided since lhey pose an increased risk of contamination by intravenous fluids antl exhibit a higher rate of hemolysis compared to vcnipuncturc,2 It has also been :.hown that bloud culturescollected from VADi. arc more .likely to be contaminated than those obtained by venipuncture.8 \Vhen warranLed, a hei1lthcan: professional trnincd in IV management should perform the draw and include a 5-cc discurd.
34 September 2006 • MLO
Specimen labeling
To prevent specimen mix-up or rejection. specimens should be properly and permanently labeled at the patient's side, bearing al least the following:
■ the patient's first and last names;■ an identification number:■ the date;■ the time (as required); and• the collector's idcntification.3
If a bar-coding system i8 used. facility protocol should be followed.
Figure 1.
Analytes that are affected by prolonged exposure to red blood cells:
• APTT■ Bicarbonate■ Calcium■ Chloride■ Glucose■ HDL cholesterol■ Iron■ Lactate dehydrogen11se ILDH)■ Magnesium (Ionized)• Phosphorouio■ Potassium
Specimen handling and processing
Because improper handling and delays in specimen processing can compromise specimen integrity and result in erroneous Lest results, the phlcbotomist must transport specimens in an appropriate and timely manner, according to the facility's established protocol. A working knowledge of analyte stabmty is necessary for specimen processing and in evaluating requests for additional testing of u previously collected specimen.
To prevent excess agitaLion of tube contents that could induce hemolysis, filled collection tubes i;hould be transported in an up• right position whenever possible. Pneumatic transport sysLcms should be evaluated to dctenninc which analytes are affected during transport. The temperature at which specimens arc: mrns• ported may also compromise analyte stability. Unless collection protocol requires chilling of the specimen (e.g., rcnin. ammonia. and so on), specimens should be transported at room temperature (22 °C to 25°C). Bccnuse of the deteriorating effects of light on photosensitive analytes. such as bilirubin, steps must be taken to protect such specimens from light exposure.
Newborn-screening specimen!-. should be protected from potential sources of contamination (i.e., direct cont.i.ct with other blood tipot specimens, sprays, lotions, glove powder, and so on) while allowed to air dry on a Rut �urfuce for a minimum of three bnun;. Exposure to direct sunlight and environmental extremes, such .is ln!at and humidity. should a)s() be avoided.'1
Serum specimens should be allowed to fully dot p1ior to ccn-11ifogation. For l,ptimal specimen qua.lit). senim or pllL�llla !lhnuld be separated from i-pedmens as soon as pnssiblc unles� there is evidence that the unalyte(sl requested will be not b� affocteLl by prolonged exposure to cells. Calcium, glucose. LtlH. und potussium :ire some analytes thm ch:.111gl! significantly when serum 01·
Collliltll<'S t)JI /W/W 311
www.n11o-online.com
SOP 17 Attachment
Draw Quality Into
�f:: �-a,!t -;�� \�} ·
-;/
The SAFE-T-FILL III Capillary Blood Collection System Improves the quality of your capillary blood samples
Tissue contamination and clotting are the most common reasons for redraws. Our system uses caplllary action to reduce these as the tendency to "scoop· Is eliminated. With antlcoagulant also In the capillary tube, the sample mixes Immediately to prevent clotting.
Receive a complimentaiy sample pack by calling 1 .800.535.6734 or visiting www.ramscl.com.
R?lM •��-�$t;tc,nK.SAl'f-l'fU SCIENTIFIC ••--d-- SC�I
Visit www.rsleads.com/609ml-029
WHEN YOU NEED TO GET IT RIGHT:
labSoft, Inc. Laboratory Information Systems
Since 1992, we have provided our customers with powerful, fenlure-rich lab information systems
!hat get lob results quickly and otcurotelyto the people rho! need them.
Let us connect your lob with the future.
ContoCI LobSoft, Inc. today:
1 -800-767-3279 [email protected] www.labsoftweb.com
Vi$it www.r$l8i1ds,comf609ml-021
L A B M A N A G E M E N T
plasma b kept in contact with cells beyond two hours (see Figure lJ.10 Generally. chemistry specimens should be centrifuged and separated within two hours of collection. to Tubes should remain dosed until time of testing ro prevent evaporation.
Coagulation specimens to be tested for aPTI can remain at room temperature after collection. but should be tested within four hours i n order to be reliable. ti \',-'hen le.sting patients on unfrnctionated heparin, specimen processing personnel should centrifugethe s�cimen .• remove the pl.lsma from the cells within one hour and perform the test within four hours or collection.
Prothrombin times arc more forgiving and remain stable for up to 48 hours at room temperature, eve11 uncentrifuged, as long as the stopper has noc been removed. 11 If the tube is refrigerated,however, the PT results have been shown to increase after seven hours, 12 Freezing citrated plasma has been shown to effectivelypreserve PT and PTT results up to 21 days at • 70''C.
The phlebotomist's role in the workplace
In an age of technological advancement. phlebotomy remains n manual procedure. requiring critical decisions and human skills that will never be automated. The competent phlebr_itomisl recognizes and prevent� pre-analytic variableh that may introduce error, fol filling a vital role in the labmatory's quality-management system. Because diverse interactions nnd specialized knowledge are required. the phlebotomist profoundly impacts patient care. patient relations, and the accuracy and efficiency of the laboratory's path of work now. Facilities strh•ing for exeellcnec in these areas should begin by examining the value they place on the phlebotomist's role i n the workplace. After all. thut is where qual.ity collections begin. D
Dennis J. Emst MT(ASCP) is the Oiroctor of the Center ro, Phlebolomy Education and 1,as participated in the revision of several CLSI sp11cimcn collecUan standards Lisa 0. Ballance, a regional laboratory improvement consuhant with tho North Carortno Slate Laboratory of Public Health in Raleigh, NC.served on CLSl's Skin Puncture Subcommittee /or the NCCLS H4-A5 standard approved In June 2004, was the event organizer lorthe inaugural North Carolina Clinical Lab Tech Oayeducatiooal conforeoco in 2005, and is tho course director for the North Cerolina Public Health Phlebotomy lnirialive.
Roferences l, Clinical and laboratory Suindard$ lnslilute. Appk'cehon of a OuatityMan,,gementModel
far Labor11tory S11Nices, Wayne, PA: NCC LS� 2004. Approved Guideline, GP26-AJ. 2. Erns� D. Applied Phlebotomy, Philadelphia, PA. Lippincott Wiliams & Wilkins, 2005.3. Clinic el and Laboratory Standards Institute. Procedvtes for the Co/loccion o/ Oi•
agnostic Blood Specimens by Ven/puncturl/. Wayne, PA. NCCLS 2003. ApprovodStandard, H3-A5.
4. Pa�to.n, A. Stamping out Specimen Collection Errors. CAP Today. May 1999,5. Baer D, ed Tips from the Clinical Exports. MLO 2005;37(81:36.
6. McCall R, Tankersley C. Phlebotomy Essenriels. 3rd Ed Baltimore, MO: L1ppinconWilliams & Wilkins; 2003.
7 Clinical and laboratory Slandards lnstituto. Procedu;es and Devices for rhe Co/lac• lion of Oiagnosric Capillary Blood Specimens. Wayne, PA: NCCLS 2004. Approved Sraodard, tl4•A5.
8. Murray, Pf!, ed. Manual of Clinical Microbiology, 81h ed. Washington, DC. ASM Pross,2003;185•205,
9. Clinical and Laboralory Standards Institute. Blood Col/oction on filter Paper tor Newborn Screening Programs. Wayne, PA: NCClS, 2003. Approved Standard, lA4,A4
10. Clinical and Laboralory Standards Institute. Proceduros for 1h11 Handlirig and Processing of Blood Specimens. Wayne, PA, NCC! S, 2004. Approved Guideline, GPIO-A3.
1 1. Clinical and labororory Standards lnstiwte Colleclion Transport 11nd Proct>ssmo of Blood Specimuns for Tijsfing P/asmd·Based Congu/ation Asssys. Wayne, PA: NCCLS.2003, Approved Standard, H21-A4.
12. Narayanan S, The preanalytic phJso an important cooipuneot af lohorarorytnstingAm J Clin Pathol 2000; 1 13:429-452.
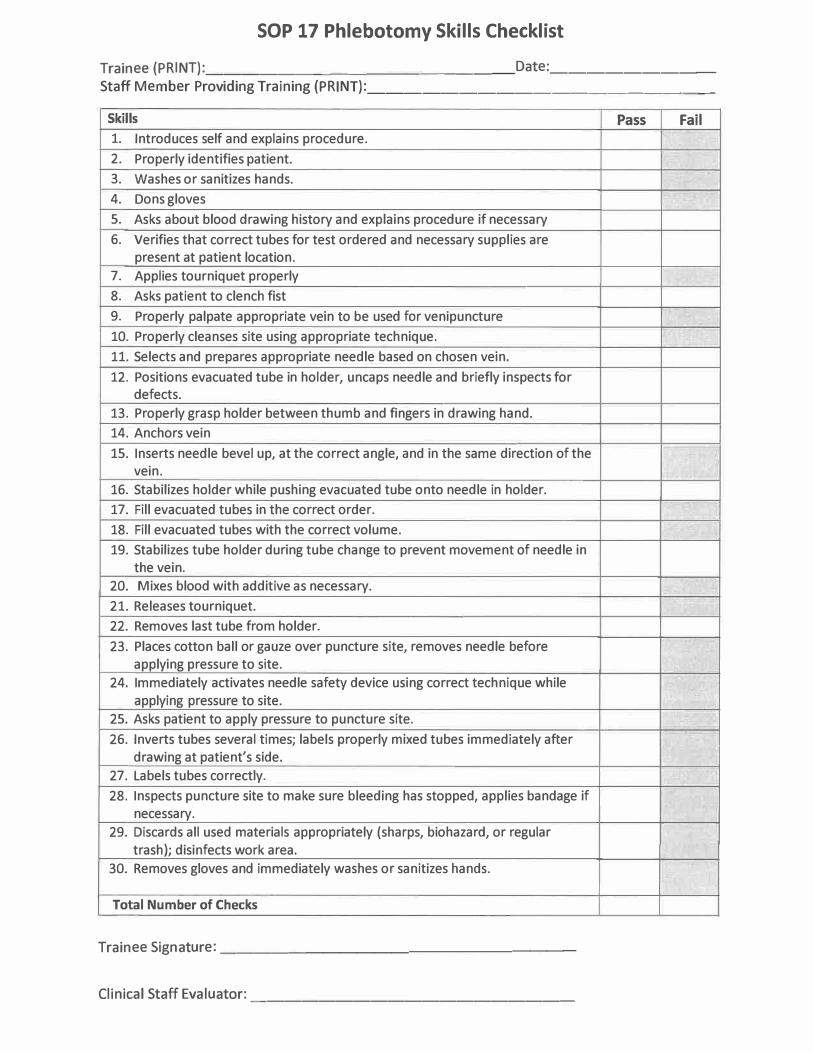
SOP 17 Phlebotomy Skills Checklist
Trainee (PRINT): __________ _ ______ Date: ________ _ Staff Member Providing Training (PRINT): __________________ _
Skills Pass Fail
1. Introduces self and explains procedure.
2. Properly identifies patient.
3. Washes or sanitizes hands.
4. Dons gloves
5. Asks about blood drawing history and explains procedure if necessary
6. Verifies that correct tubes for test ordered and necessary supplies are
present at patient location.
7. Applies tourniquet properly
8. Asks patient to clench fist
9. Properly palpate appropriate vein to be used for venipuncture
10. Properly cleanses site using appropriate technique.
11. Selects and prepares appropriate needle based on chosen vein.
12. Positions evacuated tube in holder, uncaps needle and briefly inspects for
defects.
13. Properly grasp holder between thumb and fingers in drawing hand.
14. Anchors vein
15. Inserts needle bevel up, at the correct angle, and in the same direction of the
vein.
16. Stabilizes holder while pushing evacuated tube onto needle in holder.
17. Fill evacuated tubes in the correct order.
18. Fill evacuated tubes with the correct volume.
19. Stabilizes tube holder during tube change to prevent movement of needle in
the vein.
20. Mixes blood with additive as necessary.
21. Releases tourniquet.
22. Removes last tube from holder.
23. Places cotton ball or gauze over puncture site, removes needle before
applying pressure to site.
24. Immediately activates needle safety device using correct technique while
applying pressure to site.
25. Asks patient to apply pressure to puncture site.
26. Inverts tubes several times; labels properly mixed tubes immediately after
drawing at patient's side.
27. Labels tubes correctly.
28. Inspects puncture site to make sure bleeding has stopped, applies bandage if
necessary.
29. Discards all used materials appropriately (sharps, biohazard, or regular
trash); disinfects work area.
30. Removes gloves and immediately washes or sanitizes hands.
Total Number of Checks
Trainee Signature: ____________________ _
Clinical Staff Evaluator: -------------------
Instructions:
1. The mentor/ staff member should complete the Skills Checklist page by placing a check
mark in the appropriate column for each listed skill.
2. Competency skills are either "Pass" or "Fail".
a. The trainee should have a total of 23 out of 30 checks
with no checks in the shaded "fail" boxes to be deemed
entry level competent.
b. A check in the shaded "fail" box indicates a failure of a critical
competency skill.
3. Tally the number of checkmarks in both the "Pass" and "Fail" columns at the bottom of
the page.
4. Based upon the information obtained, check either the "Pass" of "Fail" competency box
at the bottom of the page.
/__
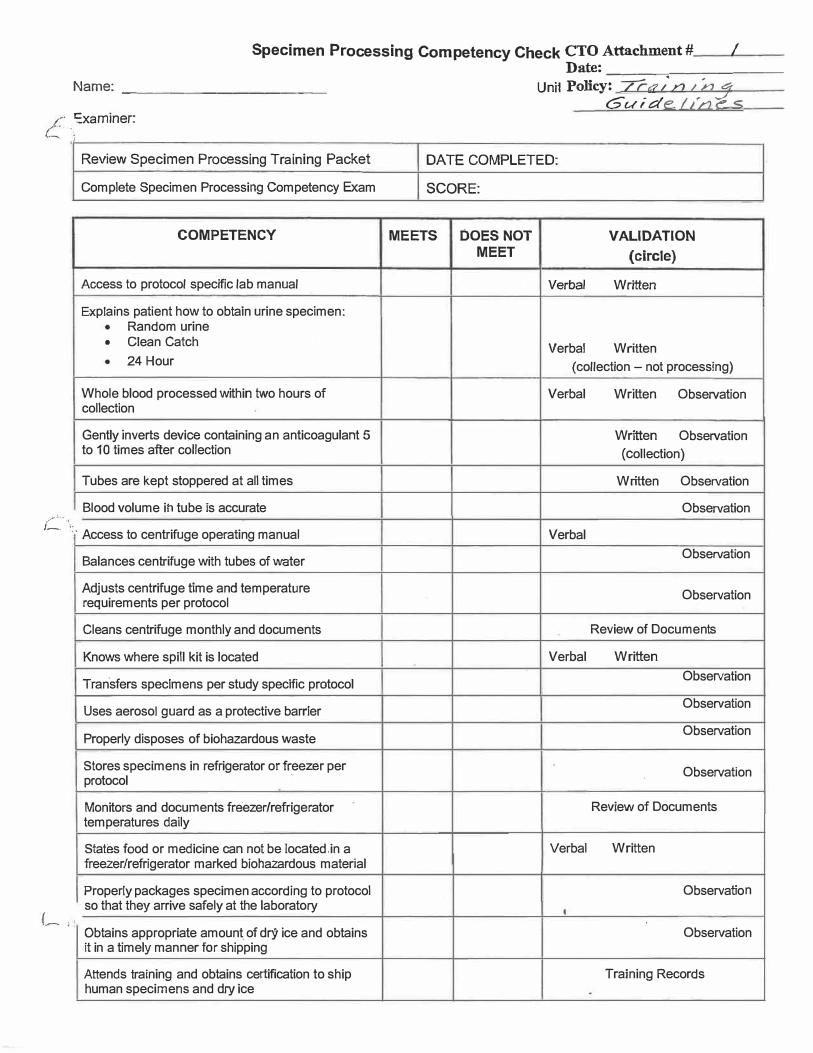
Specimen Processing Competency Check CTO Attachment# /
Name: ____________ _
C _xam,ner: ,.
Review Specimen Processing Training Packet
Complete Specimen Processing Competency Exam
COMPETENCY
Access to protocol specific lab manual
Explains patient how to obtain urine specimen: Random urine
• Clean Catch24 Hour
Whole blood processed within two hours of collection
Gently inverts device containing an anticoagulant 5 to 10 times after collection
Tubes are kept stoppered at all times
Blood volume ih tube is accurate
:: · Access to centrifuge operating manual
Balances centrifuge with tubes of water
Adjusts centrifuge time and temperature requirements per protocol
Cleans centrifuge monthly and documents
Knows where spill kit is located
Transfers specimens per study specific protocol
Uses aerosol guard as a protective barrier
Properly disposes of biohazardous waste
Stores specimens in refrigerator or fr_eezer per protocol
Monitors and documents freezer/refrigerator temperatures daily
States food or medicine can not be located.in a freezer/refrigerator marked biohazardous material
Properly packages specimen according to protocol so that they arrive safely at the laboratory
Obtains appropriate amount of dry ice and obtains it in a timely manner for shipping
Attends training and obtains certification to ship human specimens and dry ice
Date:-----=------Uni1 Policy: 7r,:u·n I ny
Guide. 1,�ne---=5
DATE COMPLETED:
SCORE:
MEETS DOES NOT VALIDATION MEET (circle)
Verbal Written
Verbal Written ( collection - not processing)
Verbal Written Observation
Written Observation (collection)
Written Observation
Observation
Verbal Observation
Observation
Review of Documents
Verbal Written Observation
Observation
Observation
Observation
Review of Documents
Verbal Written
Observation
Observation
Training Records