Embed Size (px)
Citation preview
CASE REPORT
Neonatal intrahepatic cholestasis associated with citrindeficiency (NICCD): a case series of 11 Malaysian patients
Hui Bein Chew & Lock Hock Ngu & Md Yunus Zabedah & Wee Teik Keng &
Shanti Balasubramaniam & Mohd Jamil M. Hanifah & Keiko Kobayashi
Received: 8 August 2009 /Revised: 7 September 2010 /Accepted: 8 November 2010# SSIEM and Springer 2010
Abstract Citrin deficiency, aetiologically linked to mutationsof SLC25A13 gene, has two clinical phenotypes, namelyadult-onset type II citrullinaemia (CTLN2) and neonatal/infantile intrahepatic cholestasis, caused by citrin deficiency(NICCD). Malaysian patients with NICCD, especially ofMalay and East Malaysian indigenous descent, have neverbeen reported in the literature.We present the clinical features,biochemical findings and results of molecular analysis in 11
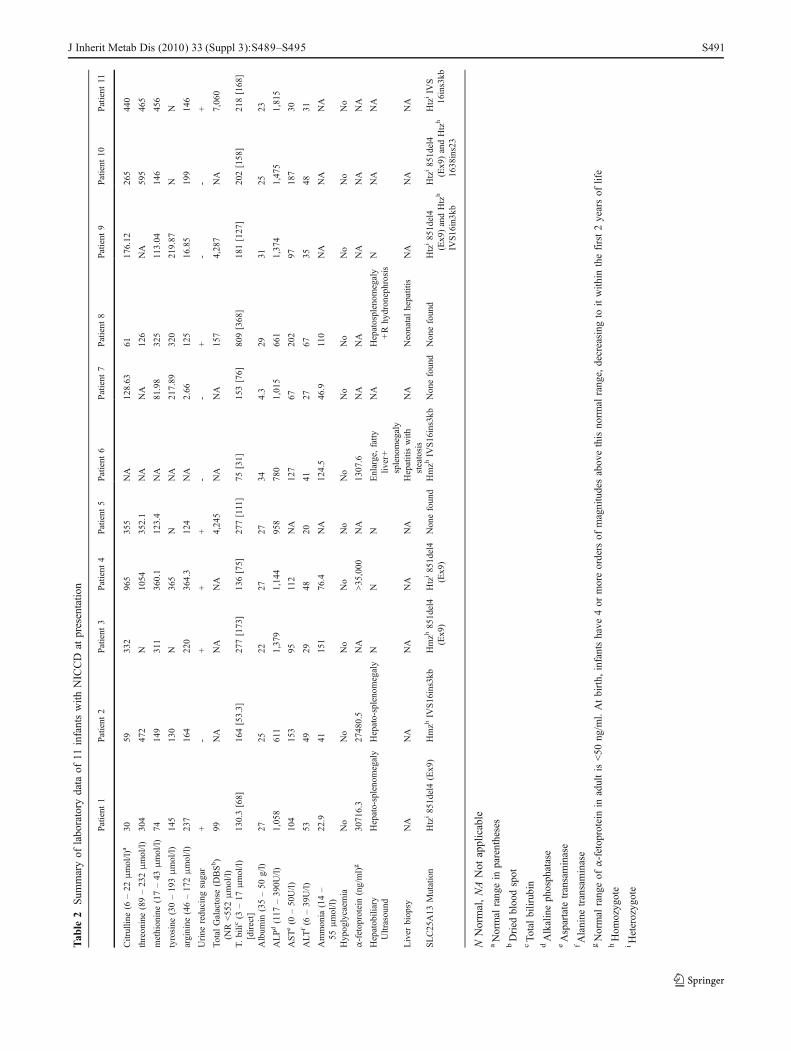
Malaysian children with NICCD. In this case series, allpatients manifested prolonged cholestatic jaundice and ele-vated citrulline levels. The other more variable featuresincluded failure to thrive, bleeding diathesis, hypoproteinae-mia, abnormal liver enzymes, prolonged coagulation profile,hyperammonaemia, hypergalactosaemia, multiple aminoaci-daemia, elevatedα-feto protein and urinary orotic acid as wellas liver biopsies showing hepatitis and steatosis. DNAanalysis of SLC25A13 revealed combinations of 851del4(Ex9), IVS16ins3kb and 1638ins23. Most of our patientsrecovered completely by the age of 22 months. However, onepatient had ongoing symptoms at the time of reporting andone had died of liver failure. Since a small percentage ofchildren with NICCD will develop CTLN2 and the mecha-nisms leading to this is yet to be defined, ongoing healthsurveillance into adulthood is essential.
Introduction
Citrin, a bipartite protein located in the mitochondrial innermembrane, functions as a calcium-binding/stimulatedaspartate-glutamate carrier that is a component of the malate-aspartate NADH (nicotinamide adenine dinucleotide) shuttle.It is mainly expressed in the liver and plays an important role inthe metabolic pathways of aerobic glycolysis, gluconeogene-sis, urea cycle, and synthesis of proteins and nucleotides(Kobayashi et al. 1999; Saheki and Kobayashi 2002; Sahekiet al. 2002, 2004; Tamamori et al. 2004). The deficiency ofcitrin results in two main clinical phenotypes: the adult-onsettype II citrullinaemia (CTLN2) that mainly presents withneuropsychiatric symptoms of confusion, seizure, coma anddeath associated with hyperammonaemia, and the neonatal/infantile form of transient intrahepatic cholestatic hepatitis(NICCD: OMIM #605814) Table 1 and Table 2.
Communicated by: Shamima Rahman
Competing interests: None declared.
References to electronic databases: NICCD: OMIM #605814Citrin: Solute Carrier Family 25,Member 13; SLC25A13OMIM*603859
H. B. Chew (*)Genetic and Metabolic Unit, Department of Paediatrics,University Malaya Medical Centre,50603 Kuala Lumpur, Malaysiae-mail: [email protected]
H. B. Chew : L. H. Ngu :W. T. Keng : S. BalasubramaniamDepartment of Medical Genetics, Institute of Paediatrics,Kuala Lumpur Hospital,Jalan Pahang,50586 Kuala Lumpur, Malaysia
M. Y. ZabedahBiochemistry Unit, Specialised Diagnostic Centre,Institute for Medical Research,50586 Kuala Lumpur, Malaysia
M. J. M. HanifahDepartment of Paediatrics, Hospital Raja Perempuan Zainab II,15590 Kota Bahru, Malaysia
K. KobayashiDepartment of Molecular Metabolism and Biochemical Genetics,Kagoshima University Graduate School of Medicine and DentalSciences,Kagoshima 890-8544, Japan
DOI 10.1007/s10545-010-9248-6J Inherit Metab Dis (201 ) 3 (Suppl 3):S489–S4950 3
/ Published online: 16 December 2010
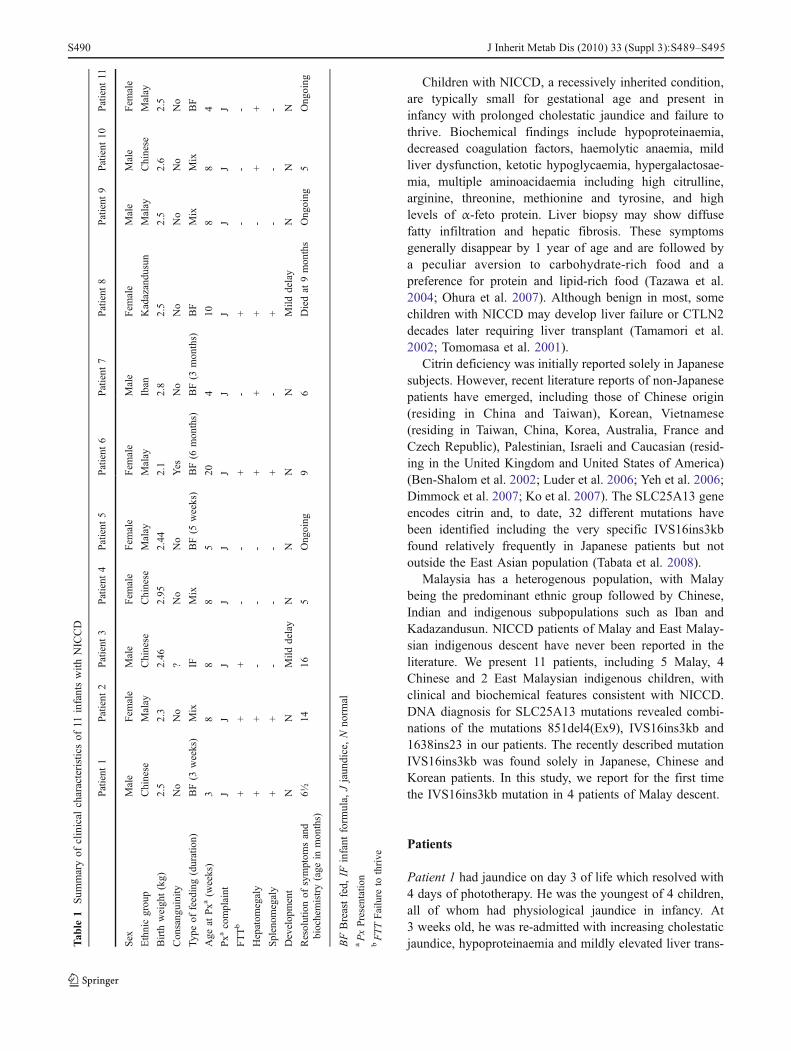
Children with NICCD, a recessively inherited condition,are typically small for gestational age and present ininfancy with prolonged cholestatic jaundice and failure tothrive. Biochemical findings include hypoproteinaemia,decreased coagulation factors, haemolytic anaemia, mildliver dysfunction, ketotic hypoglycaemia, hypergalactosae-mia, multiple aminoacidaemia including high citrulline,arginine, threonine, methionine and tyrosine, and highlevels of α-feto protein. Liver biopsy may show diffusefatty infiltration and hepatic fibrosis. These symptomsgenerally disappear by 1 year of age and are followed bya peculiar aversion to carbohydrate-rich food and apreference for protein and lipid-rich food (Tazawa et al.2004; Ohura et al. 2007). Although benign in most, somechildren with NICCD may develop liver failure or CTLN2decades later requiring liver transplant (Tamamori et al.2002; Tomomasa et al. 2001).
Citrin deficiency was initially reported solely in Japanesesubjects. However, recent literature reports of non-Japanesepatients have emerged, including those of Chinese origin(residing in China and Taiwan), Korean, Vietnamese(residing in Taiwan, China, Korea, Australia, France andCzech Republic), Palestinian, Israeli and Caucasian (resid-ing in the United Kingdom and United States of America)(Ben-Shalom et al. 2002; Luder et al. 2006; Yeh et al. 2006;Dimmock et al. 2007; Ko et al. 2007). The SLC25A13 geneencodes citrin and, to date, 32 different mutations havebeen identified including the very specific IVS16ins3kbfound relatively frequently in Japanese patients but notoutside the East Asian population (Tabata et al. 2008).
Malaysia has a heterogenous population, with Malaybeing the predominant ethnic group followed by Chinese,Indian and indigenous subpopulations such as Iban andKadazandusun. NICCD patients of Malay and East Malay-sian indigenous descent have never been reported in theliterature. We present 11 patients, including 5 Malay, 4Chinese and 2 East Malaysian indigenous children, withclinical and biochemical features consistent with NICCD.DNA diagnosis for SLC25A13 mutations revealed combi-nations of the mutations 851del4(Ex9), IVS16ins3kb and1638ins23 in our patients. The recently described mutationIVS16ins3kb was found solely in Japanese, Chinese andKorean patients. In this study, we report for the first timethe IVS16ins3kb mutation in 4 patients of Malay descent.
Patients
Patient 1 had jaundice on day 3 of life which resolved with4 days of phototherapy. He was the youngest of 4 children,all of whom had physiological jaundice in infancy. At3 weeks old, he was re-admitted with increasing cholestaticjaundice, hypoproteinaemia and mildly elevated liver trans-T
able
1Sum
maryof
clinical
characteristicsof
11infantswith
NICCD
Patient
1Patient
2Patient
3Patient
4Patient
5Patient
6Patient
7Patient
8Patient
9Patient
10Patient
11
Sex
Male
Fem
ale
Male
Fem
ale
Fem
ale
Fem
ale
Male
Fem
ale
Male
Male
Fem
ale
Ethnicgrou
pChinese
Malay
Chinese
Chinese
Malay
Malay
Iban
Kadazandu
sun
Malay
Chinese
Malay
Birth
weight(kg)
2.5
2.3
2.46
2.95
2.44
2.1
2.8
2.5
2.5
2.6
2.5
Consang
uinity
No
No
?No
No
Yes
No
No
No
No
No
Type
offeeding(duration)
BF(3
weeks)
Mix
IFMix
BF(5
weeks)
BF(6
months)
BF(3
months)
BF
Mix
Mix
BF
Age
atPxa
(weeks)
38
88
520
410
88
4
Pxa
complaint
JJ
JJ
JJ
JJ
JJ
J
FTTb
++
+-
-+
-+
--
-
Hepatom
egaly
++
--
-+
++
-+
+
Splenom
egaly
++
--
-+
-+
--
-
Develop
ment
NN
Mild
delay
NN
NN
Mild
delay
NN
N
Resolutionof
symptom
sand
biochemistry(age
inmon
ths)
6½14
165
Ong
oing
96
Diedat
9mon
ths
Ong
oing
5Ong
oing
BFBreastfed,
IFinfant
form
ula,
Jjaun
dice,Nno
rmal
aPxPresentation
bFTTFailure
tothrive
J Inherit Metab Dis (201 ) 3 (Suppl 3):S489–S4950 3 S490
Tab
le2
Sum
maryof
labo
ratory
data
of11
infantswith
NICCD
atpresentatio
n
Patient
1Patient
2Patient
3Patient
4Patient
5Patient
6Patient
7Patient
8Patient
9Patient
10Patient
11
Citrullin
e(6
–22
μmol/l)
a30
59332
965
355
NA
128.63
61176.12
265
440
threonine(89–232μmol/l)
304
472
N1054
352.1
NA
NA
126
NA
595
465
methionine(17–43
μmol/l)
74149
311
360.1
123.4
NA
81.98
325
113.04
146
456
tyrosine
(30–193μmol/l)
145
130
N365
NNA
217.89
320
219.87
NN
arginine
(46–172μmol/l)
237
164
220
364.3
124
NA
2.66
125
16.85
199
146
Urine
reducing
sugar
+-
++
+-
-+
--
+
Total
Galactose
(DBSb)
(NR
<552μmol/l)
99NA
NA
NA
4,245
NA
NA
157
4,287
NA
7,060
T.bilic
(3–17
μmol/l)
[direct]
130.3[68]
164[53.3]
277[173]
136[75]
277[111]
75[31]
153[76]
809[368]
181[127]
202[158]
218[168]
Album
in(35–50
g/l)
2725
2227
2734
4.3
2931
2523
ALPd(117
–390U
/l)1,058
611
1,379
1,144
958
780
1,015
661
1,374
1,475
1,815
ASTe(0
–50U/l)
104
153
95112
NA
127
67202
97187
30
ALT
f(6
–39U/l)
5349
2948
2041
2767
3548
31
Ammonia
(14–
55μmol/l)
22.9
41151
76.4
NA
124.5
46.9
110
NA
NA
NA
Hypoglycaem
iaNo
No
No
No
No
No
No
No
No
No
No
α-fetoprotein
(ng/ml)g
30716.3
27480.5
NA
>35,000
NA
1307.6
NA
NA
NA
NA
NA
Hepatobiliary
Ultrasound
Hepato-splenomegaly
Hepato-splenomegaly
NN
NEnlarge,fatty
liver+
splenomegaly
NA
Hepatosplenom
egaly
+Rhydronephrosis
NNA
NA
Liver
biopsy
NA
NA
NA
NA
NA
Hepatitiswith
steatosis
NA
Neonatalhepatitis
NA
NA
NA
SLC25A13
Mutation
Htzi851del4(Ex9)
Hmzh
IVS16ins3kb
Hmzh
851del4
(Ex9)
Htzi851del4
(Ex9)
Nonefound
Hmzh
IVS16ins3kb
Nonefound
Nonefound
Htzi851del4
(Ex9)andHtzh
IVS16in3kb
Htzi851del4
(Ex9)andHtzh
1638ins23
HtziIV
S16ins3kb
NNormal,NANot
applicable
aNormal
rangein
parentheses
bDried
bloo
dspot
cTo
talbilirubin
dAlkalinephosphatase
eAspartate
transaminase
fAlanine
transaminase
gNormal
rang
eof
α-fetoprotein
inadultis<50
ng/m
l.Atbirth,
infantshave
4or
moreorders
ofmagnitudesabovethisnorm
alrange,
decreasing
toitwith
inthefirst2yearsof
life
hHom
ozygote
iHeterozygote
J Inherit Metab Dis (201 ) 3 (Suppl 3):S489–S4950 3 S491

aminases. A diagnosis of breast milk jaundice was made inlight of normal G6PD, thyroid function, full blood count,negative Coomb’s test and normal infective hepatitisscreen. However, an increasing trend of conjugated hyper-bilirubinaemia, unsatisfactory weight gain and hepatosple-nomegaly prompted further investigations at 10 weeks old.Radio-imaging excluded biliary atresia. α-feto protein wasmarkedly elevated and plasma amino acid profile wasconsistent with citrin deficiency. He was commenced onlactose free milk, vitamin K and multivitamins. Over thecourse of the next 4 months, he sustained good weight gainwith normal developmental milestones and resolution ofjaundice, hepatosplenomegaly and α-feto protein. Plasmaamino acid normalised at 15 months old. At 17 months ofage, he suffered 4 episodes of generalised tonic clonicconvulsions, 2 of them associated with fever and 2 episodesunexplained. Electroencephalogram was normal. Growth,physical examination and biochemical data remainednormal at 7 years old.
Patient 2 was first noticed to be jaundiced at 2 monthsold. Her older sister reportedly suffered physiologicaljaundice in infancy. Jaundice persisted at 4½ months oldassociated with 3-cm hepatomegaly and 2-cm splenomeg-aly below the costal margin. Abdominal ultrasonographyexcluded biliary atresia. Abnormal investigations were liverfunction tests, coagulation profile, lactate and α-fetoprotein. Urine orotic acid was mildly elevated at5.2 Mmol/mol creat (NR 1.0–3.2). Extensive investigationsruled out infective hepatitis, storage diseases and neonatalhaemachromatosis. She was empirically treated as having amitochondrial respiratory chain disorder, and receivedmultivitamins, folic acid, vitamin B complex and adviceon avoidance of fasting. Serum amino acid subsequentlyrevealed a profile consistent with NICCD and the diagnosiswas supported by DNA analysis of SLC25A13. Mitochon-drial cocktail was discontinued. Growth was slow in thefirst year of life with an average increase of 400 g permonth; however, this eventually normalised. Citrullinaemiaresolved at 8 months of age with normalisation of liverfunction and urine orotic acid at 14 months of age. In hersecond year of life, she was noticed to have a peculiarfondness for protein-rich food like peanuts and seafood andan aversion to carbohydrate-rich food. She is currently6 years old and enjoys excellent health.
Patient 3 is a 4-year-old Chinese boy from the east ofMalaysia. Antenatal and family history was unobtainable ashe was an adopted child. He was admitted at 1 month oldwith cholestatic jaundice and elevated liver transaminasesthat were attributed to an overdose of Dothiepin andDiazepam, antidepressants taken by his biological mother.His urine reducing sugars were recorded as 4+. He wasdischarged well after this event but re-presented at 2 monthsold with increasing cholestatic liver dysfunction. NICCD
was diagnosed based on serum amino acid and DNAanalysis of SLC25A13. He was commenced on lactose freemilk with supplementation of fat-soluble vitamins andMCT oil. Cholestasis resolved at 16 months old andCitrulline level normalised at 22 months of age. Thispatient also demonstrated a preference for protein-richfoods with an aversion to sugary foods. Currently, hisgrowth is normal, but development is delayed especially inthe area of speech.
Patient 4 is a 3½-year-old Chinese girl who had transientneonatal physiological jaundice on day 3 of life. Thisresolved with natural sunlight but subsequent intermittentjaundice led to further investigations at 2 months of age.NICCD was diagnosed based on clinical phenotype,conjugated hyperbilirubinaemia, plasma amino acid profileand markedly elevated α-feto protein. She received lactosefree formula milk, supplementation of fat soluble vitaminsand MCT oil. All investigations normalised at 5 monthsold. Her physical examination, growth and development arenormal at the time of reporting.
Patient 5 had jaundice on day 4 of life which persisted at5 weeks old. She was otherwise clinically well and thriving.Investigations including plasma amino acid profile andelevated total galactose level were consistent with NICCD.Breast feeding was continued supplemented by lactose freemilk. At her current age of 11 months old, development andphysical examination are normal. Plasma citrulline levelremained high at 328.2 μmol/l.
Patient 6 is a 6-year-old Malay girl born via emergencycaesarean section to parents who are second cousins. Ofher 4 siblings, one older brother (current age 19 years)had a history of prolonged neonatal jaundice thatresolved without sequelae. She had jaundice on day 3of life which resolved with 2 days of phototherapy. Shere-presented at 5 months old with cholestatic jaundice,poor weight gain, 3-cm hepatomegaly and 1-cm spleno-megaly below the costal margins. Ultrasonography of thehepatobiliary system showed hepatosplenomegaly withfeatures of fatty change. A liver biopsy showed gener-alised macrovesicular steatosis with bile stasis, portaltract expansion by lymphocytic infiltrate with associatedinterface hepatitis. Unfortunately, plasma amino acid wasnot performed at the acute stage, but elevated ammoniaand α-feto protein accompanied by homozygocity forIVS16ins3kb mutation in SLC25A13 gene led to thediagnosis of NICCD. Urine orotic acid was elevated at8 Mmol/mol creat. In addition, she had hypokalaemiaand hypophosphataemia with normal anion gap metabol-ic acidosis that was attributed to renal tubulopathy. Thisresolved spontaneously without intervention. Jaundiceresolved at the age of 9 months with normalisation ofliver transaminases at the age of 1 year and 3 months.Plasma amino acid is now normal.
J Inherit Metab Dis (201 ) 3 (Suppl 3):S489–S4950 3 S492

Patient 7, the 3rd child of Ibanese (Malaysian aborigi-nes) parents, presented at 1 month old with jaundice whichpersisted to 6 months of age. Examination revealed 5-cmhepatomegaly below the costal margin. NICCD wasdiagnosed based on clinical phenotype and amino acidprofile. He was commenced on lactose-free diet withsupplementation of multivitamins. At his current age of3 years, he remains clinically well.
Patient 8, the 4th child of Kadazandusun (Malaysianaborigines) parents, presented at 10 weeks old withprolonged conjugated hyperbilirubinaemia. Investigationsruled out biliary atresia and liver biopsy showed neonatalhepatitis. She was followed up in the district hospital asliver disease progressively worsened. At 7 months old, shewas admitted in a decompensated state with liver failure,coagulopathy and gastrointestinal bleed precipitated bysepsis. Physical examination revealed growth parametersbelow the 3rd percentile, jaundice, ascites and hepatosple-nomegaly recorded at 4.5 cm and 5 cm below the costalmargins, respectively. Doppler ultrasound of the abdomensuggested cirrhotic changes in the liver, gross splenomegalyand mild right hydronephrosis. Liver enzymes and coagu-lation profile were abnormal with ongoing bleedingrequiring rescue with fresh frozen plasma. Full blood countshowed normocytic normochromic anaemia. Investigationsfor infective hepatitis, autoimmune hepatitis, hypothyroid-ism, Wilson’s disease, α-1-Anti-Trypsin deficiency yieldednegative results. Urine reducing sugars were positive buttotal galactose level was normal. Serum amino acid profilewas consistent with citrin deficiency. She was treated withlactose free diet, multivitamins, folate and vitamin D.Unfortunately, she passed away from liver failure shortlyafter.
Patient 9 is a 6-month-old Malay boy, who had transientphysiological jaundice at 2 days old, re-presented at2 months old with conjugated hyperbilirubinaemia. Phys-ical examination was unremarkable. Investigations ruledout biliary atresia, hypothyroidism and congenital infec-tions. Plasma amino acid profile, elevated galactose leveland DNA analysis of SLC25A13 led to the diagnosis ofNICCD. He was commenced on lactose-free milk as asupplement with continuation of breast feeding.
Patient 10 is a 5-month-old Chinese boy who presentedwith prolonged cholestatic jaundice at 2 months old.Physical examination revealed a well and thriving childwith jaundice and 3-cm hepatomegaly below the costalmargin. Plasma amino acid profile was consistent withNICCD and this was supported by DNA analysis ofSLC25A13.
Patient 11 is a 3-month-old Malay girl who presentedwith prolonged cholestatic jaundice at 1 month old.Clinically, she was jaundiced, has bilateral cataract and 3-cm hepatomegaly. Citrin deficiency was diagnosed based
on clinical and biochemical data. She was commenced onlactose-free diet and examination at 3 months of ageshowed resolving jaundice and cataracts.
Molecular analysis
Fifteen known common mutations among Asians werescreened according to the methods described previously byusing GeneScan/SNaPshot and/or PCR/gel running (Tabataet al. 2008). These mutations are: (1) [851del4 (Ex9)]; (2)(g.IVS11+1 G>A); (3) [1638ins23 (Ex16)]; (4) [S225X(Ex7)], (5) (g.IVS13+1 G>A); (6) [1800ins1 (Ex17)]; (7)[R605X (Ex17)]; (8) [E601X (Ex17)]; (9) [E601K (Ex17)];(10) (g.IVS6+5 G>A); (11) [R184X (Ex6)]; (14) (g.IVS6+1 G>C); (16) [G531D (Ex16)]; (19) (g.IVS16ins3kb); (20)(g.Ex16+74_IVS17-32del516).
Discussion
The diagnosis of NICCD can be reliably achieved bymolecular studies as mutations of the SLC25A13 gene hadbeen established as the cause of citrin deficiency. However,studies have estimated that mutations are not detected inabout 15% of cases (Tokuhara et al. 2007). So far, 32mutations have been described and novel mutations are stillbeing discovered. The phenotype of NICCD patients havebeen delineated in studies over the past decade (Ohura et al.2007; Saheki et al. 2002, 2004; Tazawa et al. 2004). Thediagnosis of NICCD in our series is confirmed bymolecular studies in 5 patients (patient 2, 3, 6, 9, 10); inthe other 6 patients, published clinical phenotype andbiochemical data form the basis of our diagnosis. Interest-ingly, all our patients who carry the mutation IVS16ins3kbare from the Malay ethnic group. This mutation wasthought to have occurred historically very early on in EastAsia and has never been reported outside the Japanese,Chinese and Korean populations. This may lend support tothe theories regarding the origin of Malaysians of Malaydescent. One theory postulates migration from Yunnan,China; another states that they are sea migrants originallyfrom Taiwan. Genetic heterogeneity exists among differentraces in the mutations of SLC25A13. This may be the otherreason that abnormal mutations were not found in patients 7and 8, children of Iban and Kadazandusun descent. TheIbans are the original inhabitants of Borneo Island andKadazandusun is an ethnic group indigenous to the state ofSabah in East Malaysia (North Borneo). With advancementin this field, these samples should be re-tested for novelmutations of SLC25A13.
The characteristic clinical feature of NICCD is neonatalhepatitis associated with cholestasis. Some patients are
J Inherit Metab Dis (201 ) 3 (Suppl 3):S489–S4950 3 S493

picked up on newborn screening with hypercitrullinaemia,hypermethioninaemia, and hypergalactosaemia prior toemergence of symptoms. All our patients presented withcholestatic jaundice. Three of these patients had citrullinae-mia detected on high risk dried blood spot screening usingtandem mass spectrophotometry (TMS) on presentation(patients 5, 7, 9). Asymptomatic infants with NICCD maybe picked up when nationwide newborn screening isestablished in Malaysia.
The age of presentation ranged from 3 weeks to5 months, occurring most commonly around 2 monthsold. Previous reports have suggested that symptoms andsigns in NICCD resolve completely by 1 year old ifuncomplicated by liver failure. In 2 of our patients,cholestasis resolved after the age of 1 year at 14 and16 months respectively (patients 2 and 3) and in patient 3,citrulline level normalised at the age of 22 months. 3 otherpatients had ongoing symptoms at the time of reporting(patients 5, 9, 11) and patient 8 died from liver failure at theage of 9 months.
Children with NICCD are generally small for theirgestational age; this is thought to be due to intrauterinecitrin deficiency (Tamamori et al. 2004). Our patients, allborn at term, had birth weights ranging from 2.1 to 2.95 kg.Mean birth weight was 2.5 kg (± 0.32 SD), at the lowerlimit of normal. However, since Asian children may besmaller than Caucasians, the birth weights in our case seriesmay be considered normal rather than small at birth. Fiveout of 11 of our patients failed to thrive. Four of these 5patients demonstrated catch up growth upon resolution ofliver dysfunction and citrullinaemia, while one had passedaway.
Patient 1 had 2 episodes of febrile convulsions and 2episodes of unexplained afebrile convulsions. Afebrileconvulsions have previously been reported in a patientwith NICCD by Tazawa et. al. (2004). It is uncertainwhether this is related to the disease or a separate entity. InTazawa’s case, the patient also suffered developmentaldelay which resolved with time. Development was normalin all our patients except for patient 3 who had concurrentpsychosocial factors which may have contributed to hisdelay and patient 8 who was very ill and spent much timein the hospital.
In our series, the amino acid profile showed an elevatedcitrulline level 1.3–43.8 times the upper limit of normal atpresentation. The concentration of threonine, methionine,tyrosine and arginine ranged from normal to 8.3 times theupper limit of normal. It has previously been suggested thata higher protein, proline and asparagine content in formulamilk may replenish the depleted intracellular stores ofamino acid and stimulate urea synthesis under citrindeficiency, thus conferring a beneficial effect compared tobreast milk (Saheki et al. 2002; Ben-Shalom et al. 2002).
The level of hyperamino acidaemia was not related to themode of feeding in our patients, suggesting that otherfactors may be responsible, for example endogenousproduction. Previous studies have recommended a highprotein/low carbohydrate diet because a high carbohydratediet may increase cytosolic NADH, overloading thedefective malate aspartate shuttle resulting in difficulty inconversion to NAD+ and the subsequent fatty liver (Sahekiet al. 2002). Patients with NICCD therefore naturallyexhibit a fondness for protein-rich food and a dislike forcarbohydrate-rich food. Dietary modifications have notbeen studied with structured protocols, and therefore havenot been applied in our patients. However, high levels ofgalactose may have adverse effects as shown in patient 11who had cataract at presentation. The galactosaemia presentis thought to be due to the high NADH/NAD+ ratio sincethere is no abnormality in the enzymes of galactosemetabolism (Saheki et al. 2004). Tazawa et. al. (2004)have proposed that lactose is a toxic substance in NICCDand may worsen cholestasis. As such, when infant formulawas introduced in our patients, we have used lactose-freeformula. In addition, dietary management is directed attreating the consequences of cholestasis with supplementa-tion of fat soluble vitamins and MCT oil.
Elevated levels of urinary orotic acid and involvement ofthe renal system have not previously been reported inNICCD. Orotic acid was elevated in patients 2 and 6.Elevated orotic acids would be expected since the deficien-cy of citrin directly affects the detoxification of ammonia tourea at the start of urea cycle. Two patients had renaldiseases; patient 6 had biochemical evidence of renaltubulopathy and patient 8 had an incidental radiologicalfinding of mild right hydronephrosis of which the aetiologyis unknown. Since there was no single unifying factor, it ispossible that these renal pathologies are unrelated to theirmetabolic problem.
In several of our patients, many other diagnoses wereconsidered before the final diagnosis of NICCD. Theseincluded biliary atresia, breast milk jaundice, drug toxicity,infective hepatitis, galactosaemia, mitochondrial cytopa-thies, glycogen storage diseases, urea cycle defects,tyrosinaemia, organic acidaemias and neonatal haemachro-matosis. This led to many expensive, unnecessary and onoccasion invasive investigations. NICCD should be con-sidered in all children who present with prolongedconjugated hyperbilirubinaemia, and all investigationsshould include a serum/plasma amino acid profile withgalactose level and urine organic acid. If citrulline level isnormal but suspicion of NICCD still high, repeat of aminoacid profile should be considered followed by molecularstudies. Achieving an accurate diagnosis rapidly translatesto prompt treatment, counselling and expectation ofprognosis. Although most patients with NICCD experience
J Inherit Metab Dis (201 ) 3 (Suppl 3):S489–S4950 3 S494

a benign course and recover completely, a small percentagemay develop the more severe CTLN2 in adulthood or liverfailure (Tamamori et al. 2002, 2004). One of our patients(patient 8) suffered liver failure and subsequently suc-cumbed at 9 months old. These patients should have long-term follow-up as the mechanisms that lead to thedevelopment of CTLN2 are yet to be elucidated. Theyshould also avoid alcohol, acetaminophen and certain anti-inflammatory drugs that are implicated as triggers ofCTLN2.
Conclusion
Our study has identified 11 cases of NICCD presenting to atertiary unit in Malaysia. These patients are made up of 4different ethnic groups: Malay, Iban, Kadazandusun andMalaysian Chinese. This has implications for the preva-lence of the condition, suggesting that it may be commonerin South East Asians than previously thought.
References
Ben-Shalom E, Kobayashi K, Shaag A et al (2002) Infantilecitrullinemia caused by citrin deficiency with increased dibasicamino acids. Mol Genet Metab 77:202–208
Dimmock DP, Kobayashi K, Iijima M et al (2007) Citrin deficiency: anovel cause of failure to thrive that responds to a high protein,low carbohydrate diet. Pediatrics 119:e773–777
Ko JM, Kim GH, Kim JH et al (2007) Six cases of citrin deficiency inKorea. Int J Mol Med 20:809–815
Kobayashi K, Sinasac DS, Iijima M et al (1999) The gene mutated inadult-onset type II citrullinaemia encodes a putative mitochon-drial carrier protein. Nat Genet 22:159–163
Luder AS, Tabata A, Iijima M, Kobayashi K, Mandel H (2006)Citrullinaemia type 2 outside East Asia: Israeli experience. JInherit Metab Dis 29(suppl):59
Ohura T, Kobayashi K, Tazawa Y et al (2007) Clinical pictures of 75patients with neonatal intrahepatic cholestasis caused by citrindeficiency (NICCD). J Inherit Metab Dis 30:139–144
Saheki T, Kobayashi K (2002) Mitochondrial aspartate glutamatecarrier (citrin) deficiency as the cause of adult-onset type IIcitrullinemia (CTLN2) and idiopathic neonatal hepatitis(NICCD). J Hum Genet 47:333–341
Saheki T, Kobayashi K, Iijima M et al (2002) Pathogenesis andpathophysiology of citrin (a mitochondrial aspartate glutamatecarrier) deficiency. Metab Brain Dis 17(4):335–346
Saheki T, Kobayashi K, Iijima M et al (2004) Adult-onset type IIcitrullinaemia and idiopathic neonatal hepatitis caused by citrindeficiency: involvement of the aspartate glutamate carrier forurea synthesis and maintenance of the urea cycle. Mol GenetMetab 81(suppl 1):20–26
Tabata A, Sheng J-S, Ushikai M et al (2008) Identification of 13 novelmutations including a retrotransposal insertion in SLC25A13gene and frequency of 30 mutations found in patients with citrindeficiency. J Hum Genet 53:534–545
Tamamori A, Okano Y, Ozaki H (2002) Neonatal intrahepatic cholestasiscaused by citrin deficiency: severe hepatic dysfunction in an infantrequiring liver transplantation. Eur J Pediatr 161:609–613
Tamamori A, Fujimoto A, Okano Y et al (2004) Effects of citrindeficiency in the perinatal period: feasibility of newborn massscreening for citrin deficiency. Pediatr Res 56(4):608–614
Tazawa Y, Kobayashi K, Abukawa D et al (2004) Clinical heterogeneityof neonatal intrahepatic cholestasis caused by citrin deficiency: casereports from 16 patients. Mol Genet Metab 83:213–219
Tokuhara D, Iijima M, Tamamori A et al (2007) Novel diagnosticapproach to citrin deficiency: Analysis of citrin protein inlymphocytes. Mol Genet Metab 90:30–36
Tomomasa T, Kobayashi K, Kaneko H et al (2001) Possible clinicaland histologic manifestations of adult-onset type II citrullinaemiain early infancy. J Pediatr 138:741–743
Yeh J-N, Jeng Y-M, Chen H-L, Ni Y-H, Hwu W-L, Chang M-H(2006) Hepatic steatosis and neonatal intrahepatic cholestasiscaused by citrin deficiency (NICCD) in Taiwanese infants. JPediatr 148:642–646
J Inherit Metab Dis (201 ) 3 (Suppl 3):S489–S4950 3 S495