Embed Size (px)
Citation preview
Neonatal Jaundice &
Prolonged Jaundice Dr Lee Phaik Ngan
Paediatrician Sibu Hospital 8 April 2017
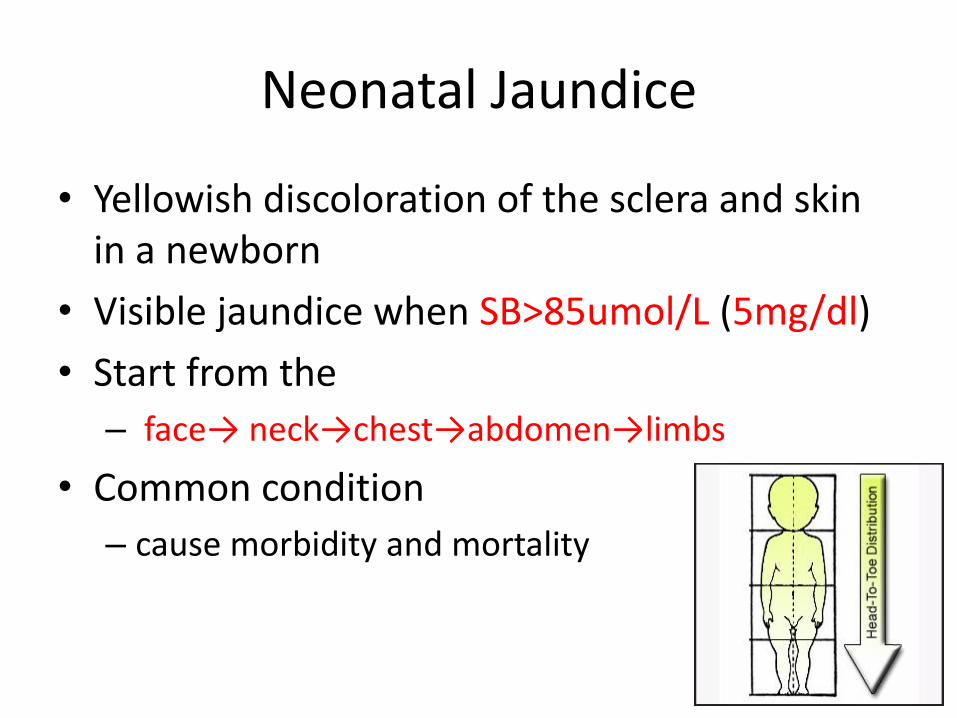
Neonatal Jaundice
• Yellowish discoloration of the sclera and skin in a newborn
• Visible jaundice when SB>85umol/L (5mg/dl)
• Start from the
– face→ neck→chest→abdomen→limbs
• Common condition
– cause morbidity and mortality
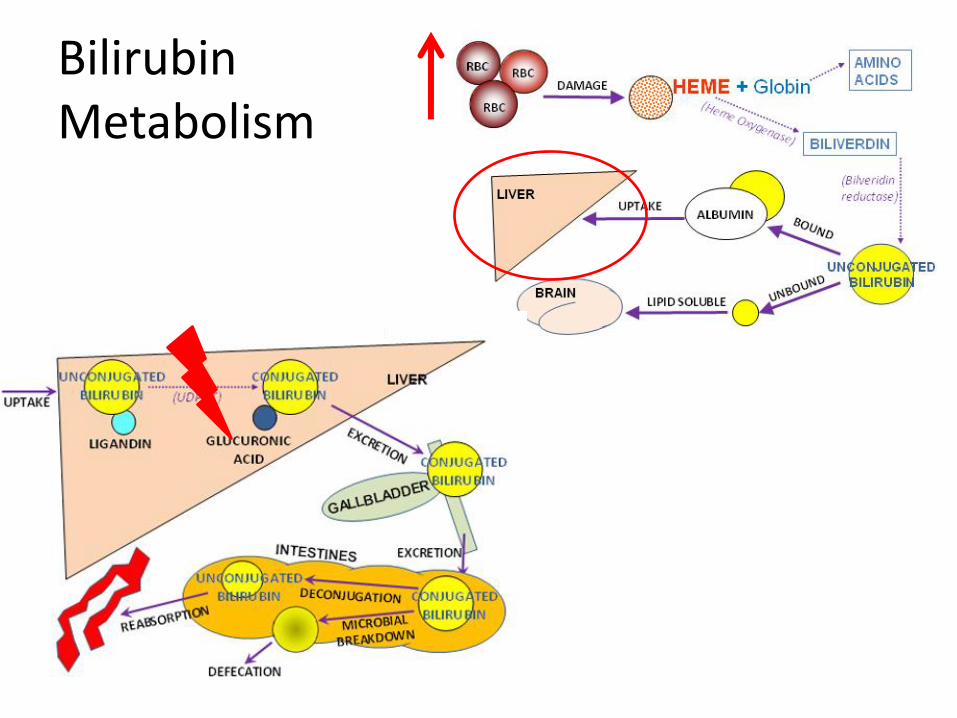
Bilirubin Metabolism
Newborn more prone to jaundice?
• High hemoglobin mass at birth
• Shorter fetal hemoglobin life span
• Low enzyme Glucuronyltransferase activity (reach adult level by 14 days regardless of gestation)
• Low concentration of ligandin Y protein (carries unconjugated bilirubin to the smooth endoplasmic reticulum) – increase to adult level by 5-10 days of age
Conditions causes severe neonatal jaundice
• Haemolysis
– ABO or Rh-isoimmunisation, G6PD deficiency
• Cephalhaemotama, subaponeurotic haemorrhage
• Polycythemia
• Sepsis
– Septicaemia, meningitis, Urinary tract infection
• Gastrointestinal tract obstruction
Danger of acute severe neonatal jaundice
• Risk of bilirubin neurotoxicity (Kernicterus) – Unconjugated bilirubin cross blood brain barrier
toxic to deep grey matter (esp globus pallidus) athetoid cerebral palsy &SNHL
• Higher risk of Kernicterus – sepsis, prematurity, small for gestational age,
acidosis, asphyxia, hypoalbuminemia and jaundice < 24 hrs of life
• The risk decreases as the baby
grows older
Assessment
History
• Age of onset
• Previous infant with NNJ, kernicterus, neonatal death, G6PD deficiency
• Mother’s blood group
• Gestational
• Presence of symptoms suggestive of sepsis
Physical examination
• General condition, weight, hydration status, sign of sepsis
• Sign of kernicterus: lethargy, hypotonia, seizure, opisthotonus, high pitch cry
• Pallor, plethora, SAH, cephalhaematoma
• Sign of intra-uterine infection: petechiea, hepatospelnomegaly
• Severity of jaundice
Assessment 2
Baby looks more jaundice than the SB level?
• Watch out for sepsis
• Repeat SB if needed
• Sometimes occurs in anaemic or fair baby
Baby looks less jaundice than the SB?
• Polycythaemic baby
• Dark baby
• If the baby is under photo, look at the area which is not exposed to the light
Management
Investigations
• Total serum bilirubin
• G6PD status
• If hemolysis is suspected, in severe/ within 24 hours – Blood group, Direct Coomb’s test
– FBC, reticulocyte count, PBF
• If infection is suspected – Blood culture, urine culture
Refer to hospital if …
• Jaundice level requires phototherapy
• Any unwell infant with jaundice
• G6PD deficient – observe for 5 days
Management2
• Depends on the SB level and the underlying condition
• Antibiotic coverage for unwell baby
• Phototherapy (single/double)
• Hydration if baby is dehydrated
• Exchange transfusion (ET)
• Human albumin
• AntiD immunoglobulin or pooled immunoglobulin
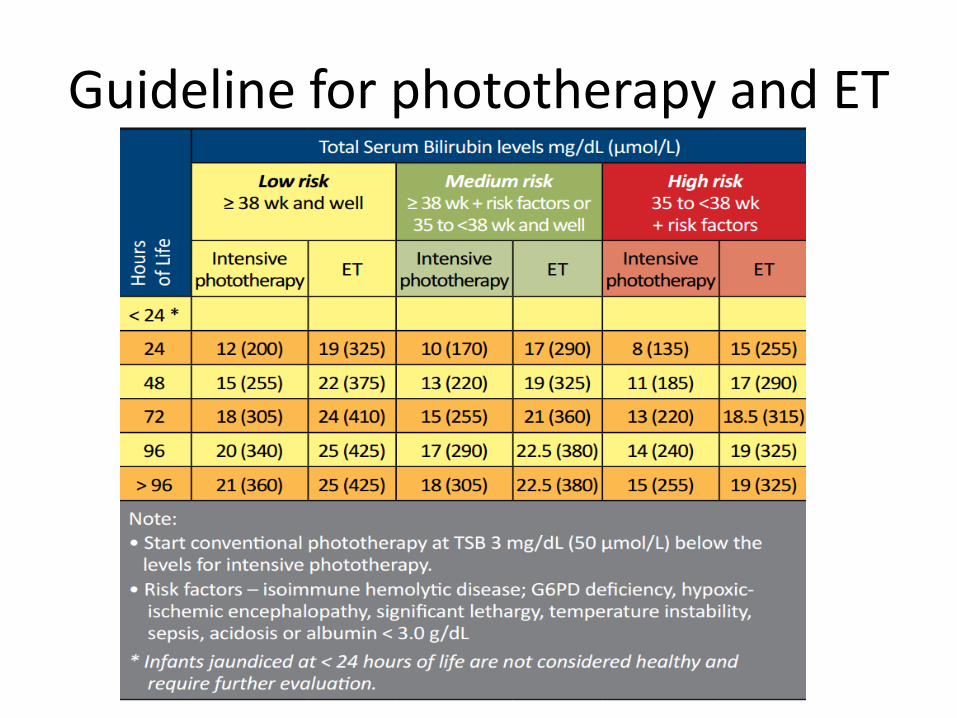
Guideline for phototherapy and ET
Phototherapy
• Phototherapy lights with minimum irradiance of 15µW/cm2/nm
• Intensive photo >30µW/cm2/nm • Photo light source 35-50cm above the top surface
of the baby • Proper exposure • Cover the eyes • Turn baby 2 hourly • Monitor temperature and hydration • Off photo light when taking blood
Breastfeeding Jaundice
• Failure to successfully initiate breastfeeding
• occurs within the first week of life
• Lactation failure inadequate intake – Significant weight and fluid loss hypovolemia
hyperbilirubinemia & hypernatremia
– Slower bilirubin elimination & increased enterohepatic circulation
• Maternal breastfeeding issues (engorgement, cracked nipples, and fatigue)
• Neonatal factors (ineffective suck)
• Not be properly addressed prior to hospital discharge
Safe to discharge?
• SB is below photo level – The trend of the SB is important
• Can discharge the baby – if the baby is more than 7 days old even though
the SB level is still at the photo level but is not rising
• Remember, the role of the phototherapy is to prevent the SB level reaches the ET level
• All babies discharge from the ward need to be followed up at the polyclinic (1-3 days later)

Prolonged jaundice
• Prolonged jaundice
– Visible jaundice that persisted beyond 14 days of life in a term baby
• 21 days in a preterm baby
• Conjugated or Unconjugated Hyperbilirubinemia?
– Conjugated hyperbilirubinemia if conjugated bilirubin ≥ 25 µgmol/L or >15% of total bilirubin
Prolonged Jaundice 2
Unconjugated hyperbilirubinemia
• Breast milk jaundice
• Hemolytic anaemia
• Increased enterohepatic circulation
• Decreased conjugation eg UTI/hypothyroidism/Gilbert syndrome
Conjugated hyperbilirubinemia
• Cholestasis or impaired bile flow
• Always pathological
• Time sensitive
Extrahepatic Biliary atresia Choledochol cyst
Intrahepatic Infections Drugs/toxins Endocrine Genetic Idiopathic hepatitis
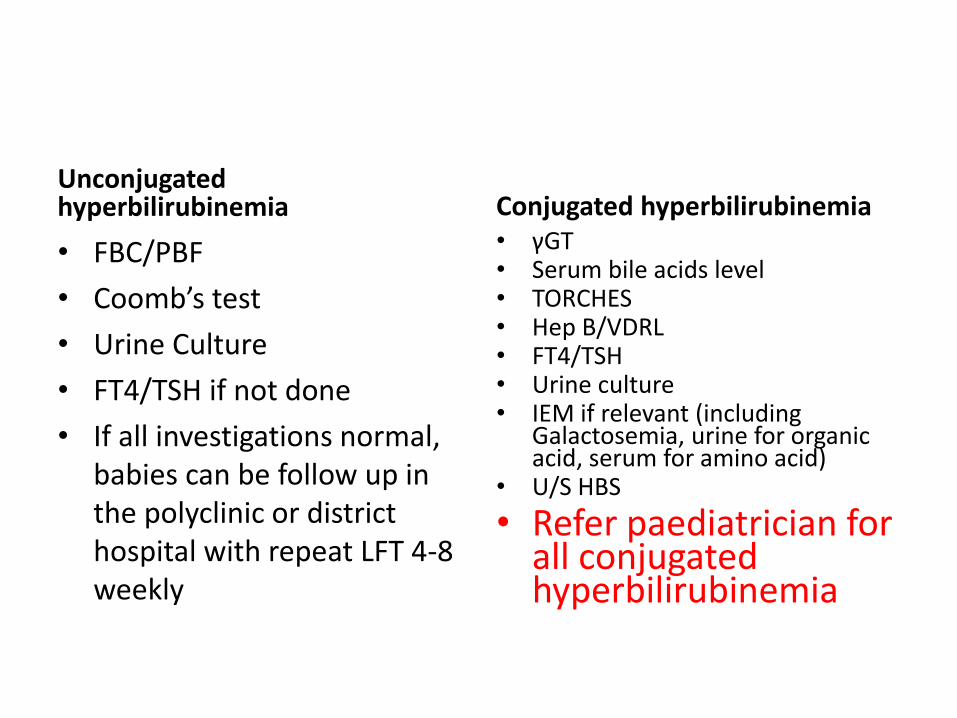
Unconjugated hyperbilirubinemia
• FBC/PBF
• Coomb’s test
• Urine Culture
• FT4/TSH if not done
• If all investigations normal, babies can be follow up in the polyclinic or district hospital with repeat LFT 4-8 weekly
Conjugated hyperbilirubinemia • γGT • Serum bile acids level • TORCHES • Hep B/VDRL • FT4/TSH • Urine culture • IEM if relevant (including
Galactosemia, urine for organic acid, serum for amino acid)
• U/S HBS
• Refer paediatrician for all conjugated hyperbilirubinemia
Conjugated hyperbilirubinemia –Extrahepatic cholestasis
• Biliary atresia
– Need early diagnosis
– Prognosis is better if surgery (Kasai operation) done within 60 days of age
– Diagnosis
• Ultrasound
• HIDA
• OTC/liver biopsy
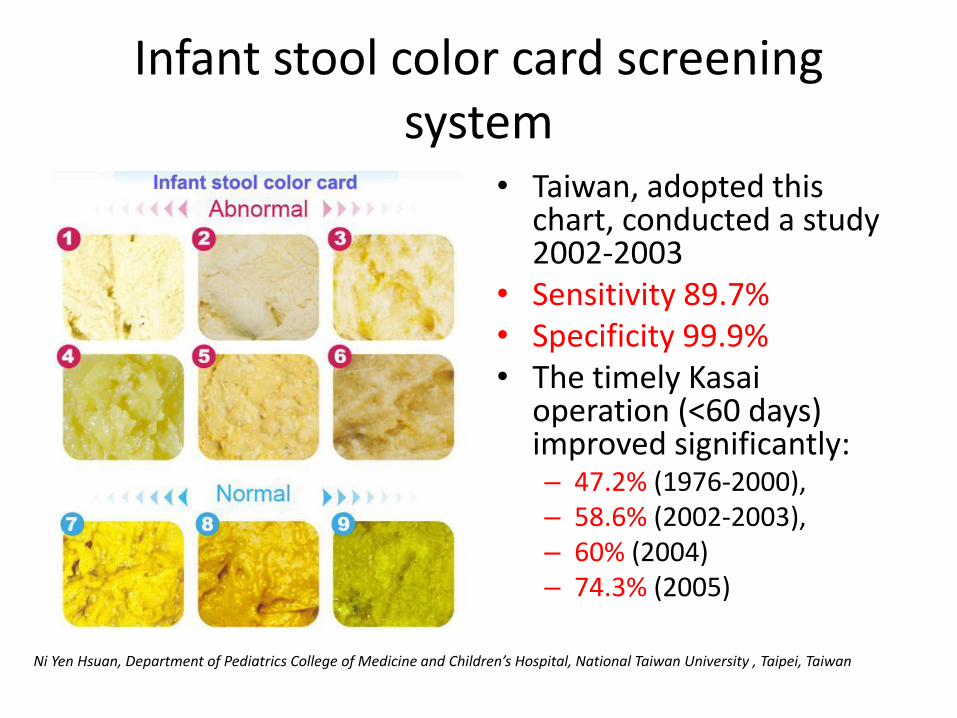
Infant stool color card screening system
• Taiwan, adopted this chart, conducted a study 2002-2003
• Sensitivity 89.7% • Specificity 99.9% • The timely Kasai
operation (<60 days) improved significantly: – 47.2% (1976-2000), – 58.6% (2002-2003), – 60% (2004) – 74.3% (2005)
Ni Yen Hsuan, Department of Pediatrics College of Medicine and Children’s Hospital, National Taiwan University , Taipei, Taiwan
Breast milk jaundice
• Babies are well and thriving
– Seen in up to 1/3 of breastfed babies
– More severe in the presence of G6PD deficiency
– Can persist up to 4 months of age
How to follow up prolonged jaundice?
• Treat any treatable conditions
– Biliary atresia
– Hypothyroidism
– UTI
– Syphilis
– IEM
How to follow up prolonged jaundice?
• Follow up the baby 4-8 weekly with LFT
• Watch out for worsening LFT/liver cirrhosis/liver failure
• Once investigations for prolonged jaundice done and the SB is not increasing trend, no need to check regular SB