Embed Size (px)
Citation preview

Part 1: clinical and pathophysiologic considera-tions. Obstet. Gynecol. Surv. 57:598–618.
3. Podjarny, E., Baylis, C., and Losonczy, G. 1999. Ani-mal models of preeclampsia. Semin. Perinatol.23:2–13.
4. Maynard, S.E., et al. 2003. Excess placental solublefms-like tyrosine kinase 1 (sFlt1) may contribute toendothelial dysfunction, hypertension, and pro-teinuria in preeclampsia. J. Clin. Invest. 111:649–658.doi:10.1172/JCI200317189.
5. Eremina, V., et al. 2003. Glomerular-specific alter-ations of VEGF-A expression lead to distinct con-genital and acquired renal diseases. J. Clin. Invest.111:707–716. doi:10.1172/JCI200317423.
6. King, B.F. 1987. Ultrastructural differentiation ofstromal and vascular components in earlymacaque placental villi. Am. J. Anat. 178:30–44.
7. Goldman-Wohl, D., and Yagel, S. 2002. Regulationof trophoblast invasion: from normal implantationto pre-eclampsia. Mol. Cell. Endocrinol. 187:233–238.
8. Zhou, Y., et al. 2002. Vascular endothelial growthfactor ligands and receptors that regulate humancytotrophoblast survival are dysregulated insevere preeclampsia and hemolysis, elevated liverenzymes, and low platelets syndrome. Am. J.Pathol. 160:1405–1423.
9. Mattot, V., et al. 2002. Loss of the VEGF(164) andVEGF(188) isoforms impairs postnatal glomeru-lar angiogenesis and renal arteriogenesis in mice.J. Am. Soc. Nephrol. 13:1548–1560.
602 The Journal of Clinical Investigation | March 2003 | Volume 111 | Number 5
See the related article beginning on page 607.
Nephrolithiasis: site of the initial solid phase
David A. Bushinsky
University of Rochester School of Medicine and Dentistry and the Nephrology Unit, Strong Memorial Hospital, Rochester, New York, USA
J. Clin. Invest. 111:602–605 (2003). doi:10.1172/JCI200318016.
Most cases of nephrolithiasis are asso-ciated with the relatively commonmetabolic abnormality of idiopathichypercalciuria (1). These patients gen-erally absorb an excess amount ofdietary calcium leading to increasedurine calcium excretion and supersatu-ration with respect to calcium oxalateand calcium phosphate; they subse-quently form stones. Other patientswith nephrolithiasis, who have had anintestinal bypass procedure, absorboxalate in excess leading to increasedurine oxalate excretion and supersatu-ration with respect to calcium oxalate;they also subsequently form stones. Inthese and other causes of nephrolithi-asis, the site of the initial solid phasehas long been the subject of debate.Over 65 years ago, A. Randall demon-strated that interstitial crystals locatedat, or adjacent to, the papillary tip,Randall’s plaques, were common in
stone formers (2). He found that thesecrystals were composed not of calciumoxalate, the most common solid phasefound in patients with nephrolithiasis,but of calcium phosphate (3). Hebelieved that the calcium phosphatecrystals formed in the papillary inter-stitium and then eroded into the uri-nary space, serving as a heterogeneousnucleation surface for calcium oxalate.B. Finlayson later argued that, due torapid flow of the renal ultrafiltratethrough the tubule, there was insuffi-cient time for formation of a lumen-obstructing solid phase (4), which alsosuggested that an intratubular site ofstone formation was unlikely. Howev-er, other investigators found that calci-um oxalate crystals adhered to cul-tured tubular cells (5), where theycould either be endocytosed or remainon the cell surface, serving as a nidusfor growth into larger, clinically signif-icant, calculi.
Site of the initial solid phaseWhere is the site of initial crystalliza-tion — the interstitium, the tubularlumen, or perhaps the renal calyx,where supersaturated fluid awaitsexcretion into the ureter? Knowing thesite of initial crystallization wouldimprove understanding of the patho-
genesis of stone formation and allowinvestigators to propose and test morefocused hypotheses. This would helpthem to devise effective therapy aimedat preventing recurrent nephrolithia-sis, which afflicts approximately 50%of stone formers within five years ofthe initial stone (6). Yet until the ele-gant study by A.P. Evan et al. reportedin this issue of the JCI (7), we did nothave an answer to this rather elemen-tary question. These investigators per-formed kidney biopsies on stone-forming patients to determine theanatomical site and composition ofthe initial solid phase. They sampledareas adjacent to Randall’s plaques inpatients undergoing percutaneousnephrolithotomy. In hypercalciuriccalcium oxalate stone formers, theyfound initial calcium phosphate(apatite) crystallization in the base-ment membrane of the thin limbs ofthe loop of Henle (Figure 1) with sub-sequent extension to the vasa recta,then to the interstitial tissue sur-rounding the terminal collectingducts, and finally, in the most severecases, to the papillae. Erosion of thissolid phase into the urinary space,which is supersaturated with respectto calcium oxalate, may have promot-ed heterogeneous nucleation and for-mation of kidney stones. In patientswith hyperoxaluria resulting fromintestinal bypass, the initial crystalswere again a calcium phosphate com-plex, but these arose within the tubulelumens of terminal collecting ducts(Figure 2). Contact of these crystalswith urine, supersaturated withrespect to calcium oxalate, may havepromoted heterogeneous nucleationand formation of kidney stones. Non-stone formers, subjected to nephrecto-my, had neither plaque nor crystals.Thus there are different sites of initial
Address correspondence to: David A.Bushinsky, University of Rochester School ofMedicine and Dentistry, Nephrology Unit,Strong Memorial Hospital, 601 ElmwoodAvenue, Box 675, Rochester, New York 14642,USA. Phone: (585) 275-3660; Fax: (585) 442-9201; E-mail:[email protected] of interest: The author has declaredthat no conflict of interest exists.

crystallization depending upon themetabolic abnormality leading tostone formation.
Potential mechanisms for stone formationWhy does the initial solid phase formin these distinct locations, and whyare the initial crystals apparently onlycalcium phosphate? The basementmembrane of the thin limb appears anunlikely site for initial crystallizationin patients with idiopathic hypercalci-uria. It is not the site of either vectori-al calcium or phosphorus transport(8) and, since even the transtubularpermeabilities of these ions are verylow (8), it is difficult to link supersat-uration within the thin limbs (9) tothe surrounding interstitium. Howev-er, anatomically, the thin limbs are invery close proximity to the vasa recta
and the collecting ducts, and all aresituated in a highly concentrated,hypertonic environment. One couldpropose a sequence of events whichmight lead to increased supersatura-tion and subsequent crystal forma-tion. Following ingestion and absorp-tion of dietary calcium, the renal-filtered load of calcium would increase,resulting in increased tubular calciumconcentration (10). The medullarycountercurrent mechanism wouldconcentrate the calcium extractedfrom the thick ascending limb intothe hypertonic papilla. The vasa recta,also with an increased calcium con-centration, would fail to readilyremove calcium from the interstitium.The increased serum calcium wouldstimulate the calcium receptor anddecrease reabsorption of water in thecollecting duct (11), further concen-
trating the interstitium. Vectorial pro-ton transport into the collecting ductwould alkalinize the interstitium. ThepH of the vasa recta would alsoincrease following gastric protonsecretion, the so-called alkaline tide,resulting in less bicarbonate removalfrom the medullary interstitium. Theincreased pH would decrease the solu-bility of calcium phosphate complex-es. Perhaps an extracellular matrixprotein, specific to the papillary inter-stitium, could provide a site promot-ing heterogeneous nucleation (12),which occurs with a lower degree ofsupersaturation than homogeneousnucleation. Future studies will be nec-essary to test these hypotheses.
Intraluminal crystal formation inthe collecting duct appears a morelikely site for initial crystallization inpatients following intestinal bypasssurgery. The collecting duct fluid canbe hypertonic with elevated concen-trations of calcium leading to super-saturation. Yet the urine from thepatients in Evan’s study was undersat-urated with respect to calcium phos-phate, indicating that, thermodynam-ically, a stone should not form.However, the lack of demonstrablesupersaturation may be a function ofthe 24-hour urine collection; the max-imal supersaturation, and thus thepropensity for stone formation, isnever detected. While a 24-hour urinecollection is an important predictor ofthe likelihood of forming stones, it isnot the sole predictor. It seems proba-ble that supersaturation initiates crys-tal formation, but we still do notunderstand the relationship betweenthe degree of urinary supersaturationand stone disease.
Future directionsNow that we know where the initialsolid phase forms, what are the nextquestions? Investigators studying thekidney generally concentrate on theeffects of transport on tubular fluidion concentration; the current studywill force us to look more carefully atthe effects of basolateral membranetransport on interstitial ion concen-trations. We know little about super-saturation in this critical region of thekidney, yet this is where the majority ofstones originate.
Unneeded calcium and oxalate mustbe excreted in a minimal amount ofurine to rid the body of these potential
The Journal of Clinical Investigation | March 2003 | Volume 111 | Number 5 603
Figure 1Stone formation in patients with idiopathic hypercalciuria. Initial calcium phosphate (apatite) crys-tallization was found in the basement membrane of the thin limbs of the loop of Henle (A) withsubsequent extension to the vasa recta (B), then to the interstitial tissue surrounding the terminal(inner medullary) collecting ducts (C), and finally, in the most severe cases, extension to the papil-lae (D). Erosion of this solid phase into the urinary space (E), which is supersaturated with respectto calcium oxalate (CaOx), may have promoted heterogeneous nucleation and formation of cal-cium oxalate kidney stones (F).

toxins while conserving extracellularfluid volume. Human urine and bloodare supersaturated with respect to cal-cium oxalate (1) and calcium hydro-gen phosphate (13), respectively, yetsolid phases rarely form because weproduce inhibitors to initial nucle-ation and subsequent aggregation(12). In rats, stone formation occurswhen the magnitude of the supersatu-ration overcomes this potent inhibi-tion (14). The current study shouldpoint us in the direction of investigat-ing the relationship between supersat-uration and inhibitor proteins notonly in the urine but in the intersti-tium as well.
Crystals may stimulate productionof proteins, such as osteopontin,which appear to regulate growth of thesolid phase (15). In patients with idio-pathic hypercalciuria, there was evi-dence for crystal-induced cell injury inareas of dense crystal deposition, whilein the bypass patients there was not
only cell injury but also cell death (7).Were levels of osteopontin increased inthe medullary interstitium in either ofthese types of stone formers?
An animal model of stone formationThe genetic hypercalciuric stone–forming rat exhibits metabolic abnor-malities similar to patients with idio-pathic hypercalciuria in that these ratsabsorb excessive amounts of intestin-al calcium, they fail to adequatelyreabsorb filtered calcium, and theirbone resorption is uniquely sensitiveto 1,25(OH)2D3. All of these charac-teristics are apparently due to anincrease in the number of receptorsfor vitamin D (16, 17). The genetichypercalciuric stone-forming ratsspontaneously form calcium phos-phate stones (18) similar to thosefound in this study unless their diet isaugmented with an oxalate precursor(19). Both hypercalciuric rats and
humans appear to be predisposed toinitially form calcium phosphatestones and not the commonly ob-served calcium oxalate stones. In bothrats (20) and humans (21) the upperlimit of metastability, that level ofsupersaturation at which a solid phaseforms, increases with increasing calci-um oxalate, but not calcium phos-phate, supersaturation. Thus rats andhumans appear protected against cal-cium oxalate stone formation unless anucleation site, such as the more easi-ly formed calcium phosphate crystal,is present.
This study highlights the role ofphysician scientists working with basicscientists in medical research to joint-ly address important problems usingsophisticated clinical and laboratorytechniques and then applying theseresults to refine hypotheses for furthertesting. Agile movement between thebedside and the bench, as exemplifiedin this study, will provide insight into,and ultimately prevention of, disor-ders such as nephrolithiasis.
AcknowledgmentsThis work was supported in part byNIH Grants AR 46289, DK 57716, andDK 56788.
1. Monk, R.D., and Bushinsky, D.A. 2003. Kidneystones. In Williams textbook of endocrinology. P.R.Larsen, H.M. Kronenberg, S. Melmed, and K.S.Polonsky, editors. W.B.Saunders. Philadelphia,Pennsylvania, USA. 1411–1425.
2. Randall, A. 1937. The origin and growth of renalcalculi. Ann. Surg. 105:1009–1027.
3. Randall, A. 1940. Papillary pathology as a precur-sor of primary renal calculus. J. Urol. 44:580–589.
4. Finlayson, B., and Reid, F. 1978. The expectationof free and fixed particles in urinary stone disease.Invest. Urol. 15:442–448.
5. Lieske, J.C., and Toback, F.G. 2000. Renal cell-uri-nary crystal interactions. Curr. Opin. Nephrol.Hypertens. 9:349–355.
6. Asplin, J.R., Favus, M.J., and Coe, F.L. 2000.Nephrolithiasis. In The kidney. B.M. Brenner, edi-tor. W.B. Saunders Company. Philadelphia, Penn-sylvania, USA. 1774–1819.
7. Evan, A.P., et al. 2003. Randall’s plaque ofpatients with nephrolithiasis begins in basementmembranes of thin loops of Henle. J. Clin. Invest.111:607–616. doi:10.1172/JCI200317038.
8. Rocha, A.S., Magaldi, J.B., and Kokko, J.P. 1977.Calcium and phosphate transport in isolated seg-ments of rabbit Henle’s loop. J. Clin. Invest.59:975–983.
9. Asplin, J.R., Mandel, N.S., and Coe, F.L. 1996. Evi-dence for calcium phosphate supersaturation inthe loop of Henle. Am. J. Physiol. 270:F604–F613.
10. Bushinsky, D.A., and Monk, R.D. 1998. Calcium.Lancet. 352:306–311.
11. Hebert, S.C., Brown, E.M., and Harris, H.W. 1997.Role of the Ca2+-sensing receptor in divalent min-eral ion homeostasis. J. Exp. Biol. 200:295–302.
12. Coe, F.L., and Parks, J.H. 1997. New insights intothe pathophysiology and treatment ofnephrolithiasis: new research venues. J. Bone.
604 The Journal of Clinical Investigation | March 2003 | Volume 111 | Number 5
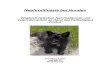
Figure 2Stone formation in patients following intestinal bypass. Initial calcium phosphate (apatite) crys-tallization was found within the tubule lumens of the terminal collecting ducts (A and B). Contactwith the urine, supersaturated with respect to calcium oxalate, may have promoted heterogeneousnucleation and formation of calcium oxalate kidney stones (C).

Miner. Res. 12:522–533.13. Neuman, W.F., and Neuman, M.W. 1958. The
chemical dynamics of bone mineral. University ofChicago Press. Chicago, Illinois, USA. 209 pp.
14. Bushinsky, D.A., Parker, W.R., and Asplin, J.R.2000. Calcium phosphate supersaturation regu-lates stone formation in genetic hypercalciuricstone-forming rats. Kidney Int. 57:550–560.
15. Xie, Y., et al. 2001. Expression, roles, receptors,and regulation of osteopontin in the kidney. Kid-ney Int. 60:1645–1657.
16. Bushinsky, D.A. 1999. Genetic hypercalciuricstone-forming rats. Curr. Opin. Nephrol. Hypertens.8:479–488.
17. Li, X.-Q., Tembe, V., Horwitz, G.M., Bushinsky,D.A., and Favus, M.J. 1993. Increased intestinalvitamin D receptor in genetic hypercalciuric rats:a cause of intestinal calcium hyperabsorption. J. Clin. Invest. 91:661–667.
18. Bushinsky, D.A., Grynpas, M.D., Nilsson, E.L.,Nakagawa, Y., and Coe, F.L. 1995. Stone forma-tion in genetic hypercalciuric rats. Kidney Int.
48:1705–1713.19. Bushinsky, D.A., et al. 2002. Calcium oxalate
stone formation in genetic hypercalciuric stone-forming rats. Kidney Int. 61:975–987.
20. Asplin, J.R., et al. 1997. Relationship betweensupersaturation and crystal inhibition in hyper-calciuric rats. Kidney Int. 51:640–645.
21. Asplin, J.R., Parks, J.H., and Coe, F.L. 1997.Dependence of upper limit of metastablility onsupersaturation in nephrolithiasis. Kidney Int.52:1602–1608.
The Journal of Clinical Investigation | March 2003 | Volume 111 | Number 5 605