Embed Size (px)
Citation preview
Network Adequacy and Midwifery Care
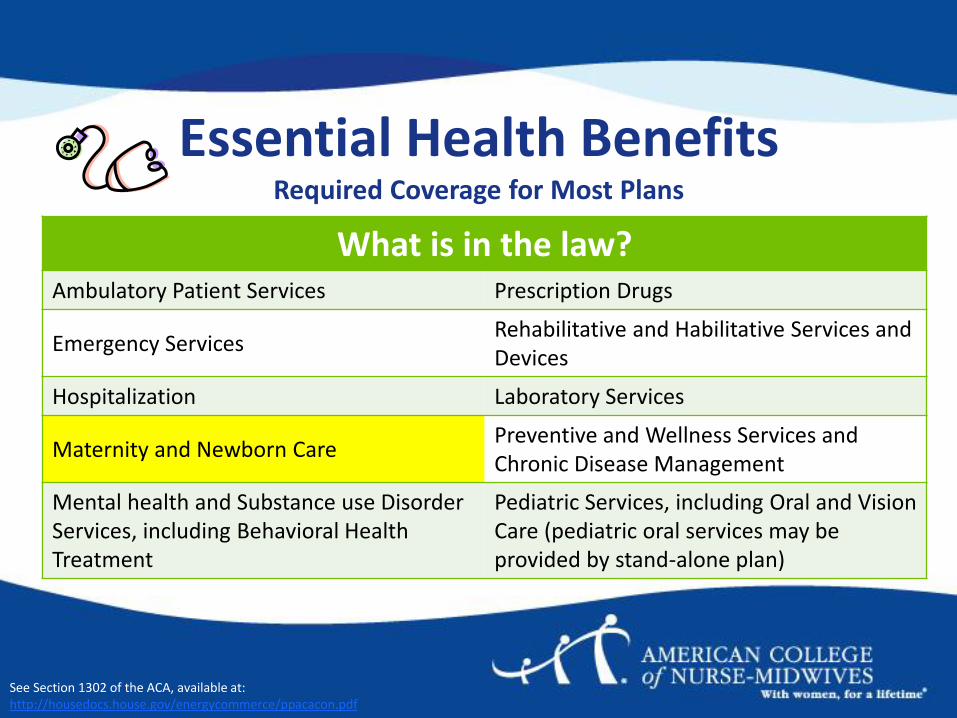
Essential Health Benefits Required Coverage for Most Plans
What is in the law? Ambulatory Patient Services Prescription Drugs
Emergency Services Rehabilitative and Habilitative Services and Devices
Hospitalization Laboratory Services
Maternity and Newborn Care Preventive and Wellness Services and Chronic Disease Management
Mental health and Substance use Disorder Services, including Behavioral Health Treatment
Pediatric Services, including Oral and Vision Care (pediatric oral services may be provided by stand-alone plan)
See Section 1302 of the ACA, available at: http://housedocs.house.gov/energycommerce/ppacacon.pdf
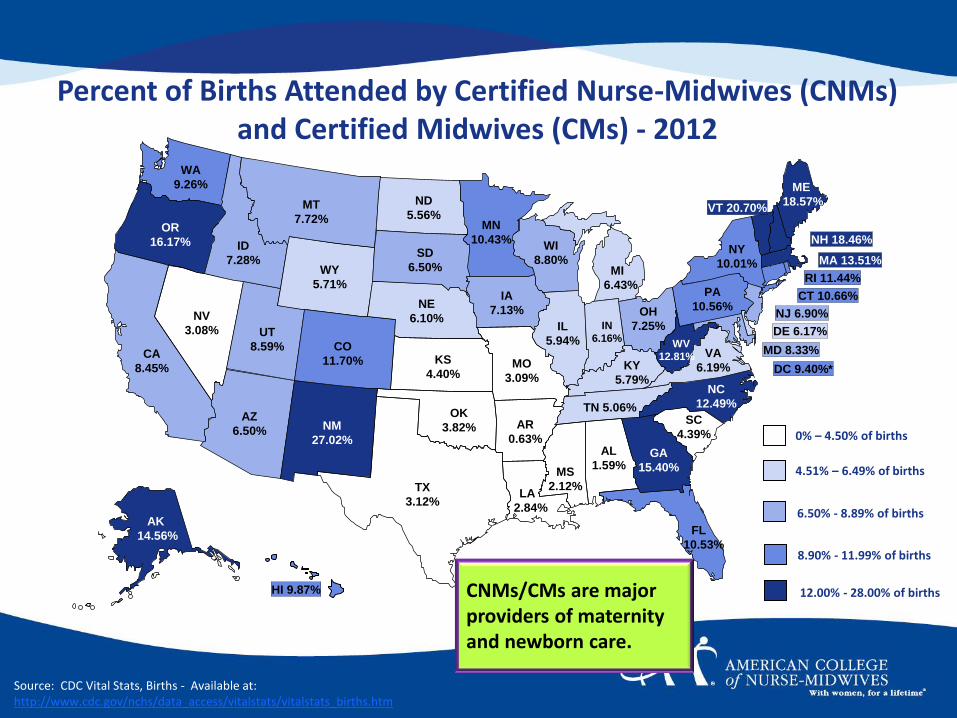
Percent of Births Attended by Certified Nurse-Midwives (CNMs) and Certified Midwives (CMs) - 2012
MT
7.72%
WY
5.71%
ID
7.28%
WA
9.26%
OR
16.17%
NV
3.08% UT
8.59% CA
8.45%
AZ
6.50%
ND
5.56%
SD
6.50%
NE
6.10%
CO
11.70%
NM
27.02%
TX
3.12%
OK
3.82%
KS
4.40%
AR
0.63%
LA
2.84%
MO
3.09%
IA
7.13%
MN
10.43% WI
8.80%
IL
5.94%
IN
6.16%
KY
5.79%
TN 5.06%
MS
2.12%
AL
1.59% GA
15.40%
FL
10.53%
SC
4.39%
NC
12.49%
VA
6.19%
WV
12.81%
OH
7.25%
MI
6.43%
NY
10.01%
PA
10.56%
MD 8.33%
DE 6.17%
NJ 6.90%
CT 10.66%
RI 11.44%
MA 13.51%
ME
18.57% VT 20.70%
NH 18.46%
AK
14.56%
HI 9.87%
4.51% – 6.49% of births
6.50% - 8.89% of births
12.00% - 28.00% of births
Source: CDC Vital Stats, Births - Available at: http://www.cdc.gov/nchs/data_access/vitalstats/vitalstats_births.htm
8.90% - 11.99% of births
0% – 4.50% of births
DC 9.40%*
CNMs/CMs are major providers of maternity and newborn care.
What do Midwives Do Differently? Normal Physiologic Birth
What is Normal Physiologic Birth?
Source: Supporting Healthy and Normal Physiologic Childbirth: A Consensus Statement by ACNM, MANA and NACPM. Available on-line at: http://www.midwife.org/ACNM/files/ccLibraryFiles/Filename/000000002179/Physioloigical%20Birth%20Consensus%20Statement-%20FINAL%20May%2018%202012%20FINAL.pdf
Spontaneous onset and progression of
labor
Biological and psychological conditions that promote
effective labor
Vaginal birth of the infant and placenta
Results in physiologic blood loss
Skin-to-skin contact between mother and
infant post partum
Supports early initiation of breastfeeding

Disruptions of Normal Physiologic Birth
• .
Source: Supporting Healthy and Normal Physiologic Childbirth: A Consensus Statement by ACNM, MANA and NACPM. Available on-line at: http://www.midwife.org/ACNM/files/ccLibraryFiles/Filename/000000002179/Physioloigical%20Birth%20Consensus%20Statement-%20FINAL%20May%2018%202012%20FINAL.pdf
Induction or augmentation
of labor
An unsupportive environment (bright
lights, cold room, lack of privacy, multiple providers, lack of
supportive companions)
Time constraints, including those driven by institutional policy
and/or staffing
Nutritional
deprivation,
e.g., food and drink
Opiates, regional analgesia, or general
anesthesia
Episiotomy
Operative vaginal (vacuum, forceps) or abdominal (cesarean)
birth
Immediate cord clamping
Separation of
mother and infant
Any situation in
which the mother
feels threatened or unsupported
Practices that Support Normal Physiologic Birth
Source: Supporting Healthy and Normal Physiologic Childbirth: A Consensus Statement by ACNM, MANA and NACPM. Available on-line at: http://www.midwife.org/ACNM/files/ccLibraryFiles/Filename/000000002179/Physioloigical%20Birth%20Consensus%20Statement-%20FINAL%20May%2018%202012%20FINAL.pdf
Access to midwifery care
Time for shared decision making, freedom from
coercion
No inductions or augmentations without
an evidence-based indication
Encouragement of food and drink during labor as the
woman desires
Freedom of movement in labor and choice of birth
position
Intermittent auscultation of heart tones unless
electronic monitoring is indicated
Providers skilled in non-pharmacologic methods of
coping with pain
Care that supports woman’s comfort, dignity,
and privacy
Respect for woman’s
cultural needs

Midwifery Results - ACNM’s 2013 Benchmarking Data
Metric Reported Average
Performance
Total Rate of Vaginal Birth 87.2%
Rate of Spontaneous Vaginal Birth 83.3%
Primary Cesarean Rate 9.2%
Repeat Cesarean Rate 3.6%
Intact Perineum Rate 49.4%
Episiotomy Rate 3.1%
Preterm Birth Rate (<37 weeks) 3.2%
Rate of Low Birthweight Infant (<2500 grams) 4.4%
Rate of NICU Admissions 4.1%
Breastfeeding Initiation Rate (exclusive breastmilk for first 48 hours of life) 85.3%
Breastfeeding Continuation Rate (any breastmilk at 6 weeks postpartum) 87.3%
Data drawn from 232 practices, representing the work of 979 midwives on a total of 97,158 births occurring in 44 states.
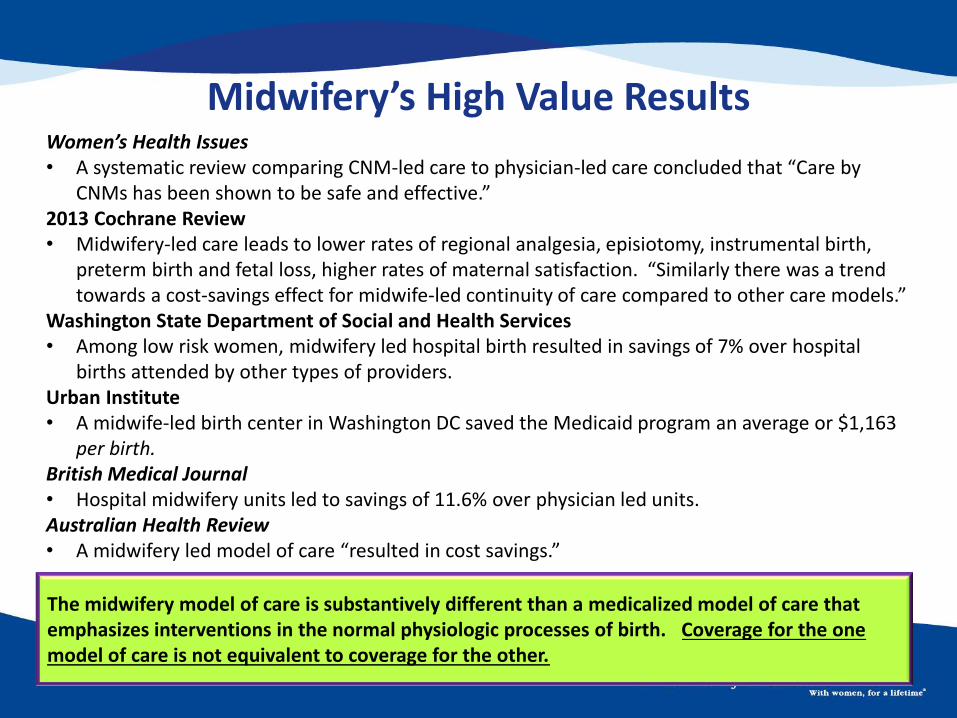
Midwifery’s High Value Results Women’s Health Issues • A systematic review comparing CNM-led care to physician-led care concluded that “Care by
CNMs has been shown to be safe and effective.” 2013 Cochrane Review • Midwifery-led care leads to lower rates of regional analgesia, episiotomy, instrumental birth,
preterm birth and fetal loss, higher rates of maternal satisfaction. “Similarly there was a trend towards a cost-savings effect for midwife-led continuity of care compared to other care models.”
Washington State Department of Social and Health Services • Among low risk women, midwifery led hospital birth resulted in savings of 7% over hospital
births attended by other types of providers. Urban Institute • A midwife-led birth center in Washington DC saved the Medicaid program an average or $1,163
per birth. British Medical Journal • Hospital midwifery units led to savings of 11.6% over physician led units. Australian Health Review • A midwifery led model of care “resulted in cost savings.”
The midwifery model of care is substantively different than a medicalized model of care that emphasizes interventions in the normal physiologic processes of birth. Coverage for the one model of care is not equivalent to coverage for the other.
ACNM Survey of Health Plans • ACNM contacted 232 of the 277 insurance plans
offering coverage through the marketplace. • We were able to survey 85, from 33 different
states. • We inquired regarding inclusion of CNMs/CMs in
provider networks and coverage of their services. • Full survey results are available at:
http://www.midwife.org/ACNM/files/ccLibraryFiles/Filename/000000004394/EnsuringAccesstoHighValueProviders.pdf

ACNM Survey Results Do you contract with certified nurse-midwives as network providers for your plans? (N=87)
75%
19%
6%
Yes
No
Sometimes
Nearly one-fifth of insurers surveyed refuse to include CNMs in their provider networks.
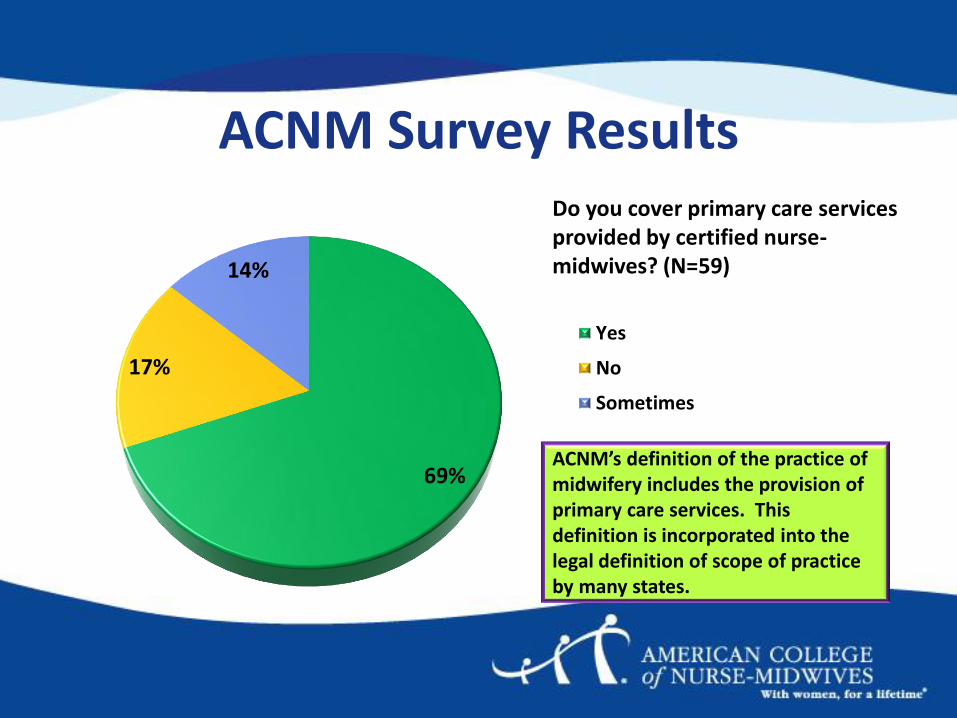
ACNM Survey Results Do you cover primary care services provided by certified nurse-midwives? (N=59)
ACNM’s definition of the practice of midwifery includes the provision of primary care services. This definition is incorporated into the legal definition of scope of practice by many states.
69%
17%
14%
Yes
No
Sometimes

ACNM Survey Results Do you impose any restrictions on what certified nurse-midwives can do, beyond those imposed by state scope of practice laws and regulations? (N=56)
The Public Health Service Act prohibits insurers from discriminating against providers acting within the scope of their license as defined by state laws and regulations.
14%
86%
Yes
No
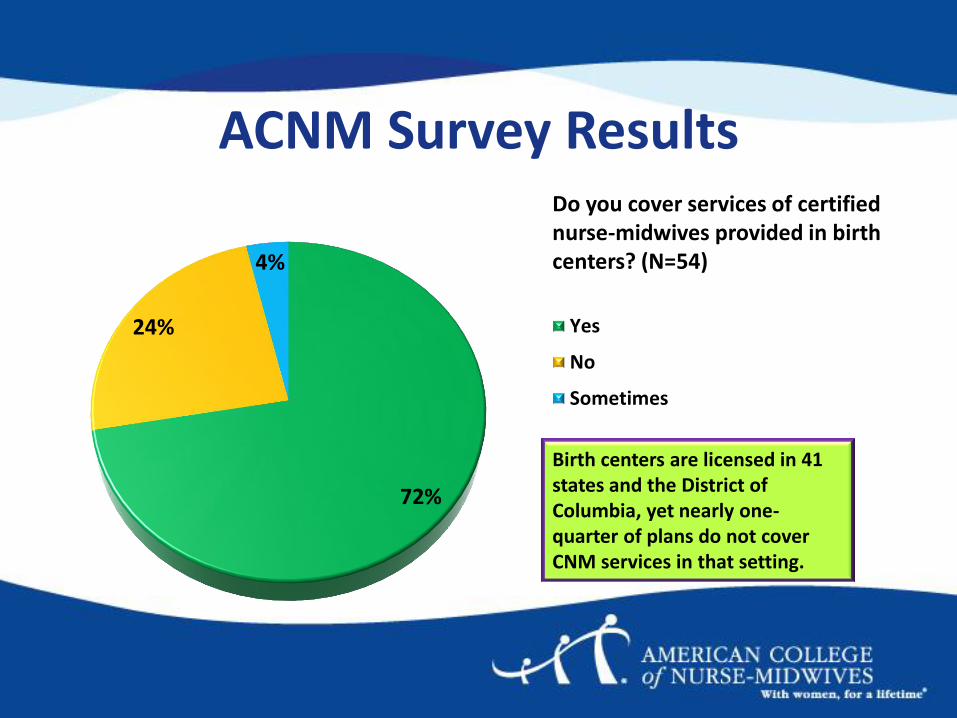
ACNM Survey Results Do you cover services of certified nurse-midwives provided in birth centers? (N=54)
Birth centers are licensed in 41 states and the District of Columbia, yet nearly one-quarter of plans do not cover CNM services in that setting.
72%
24%
4%
Yes
No
Sometimes
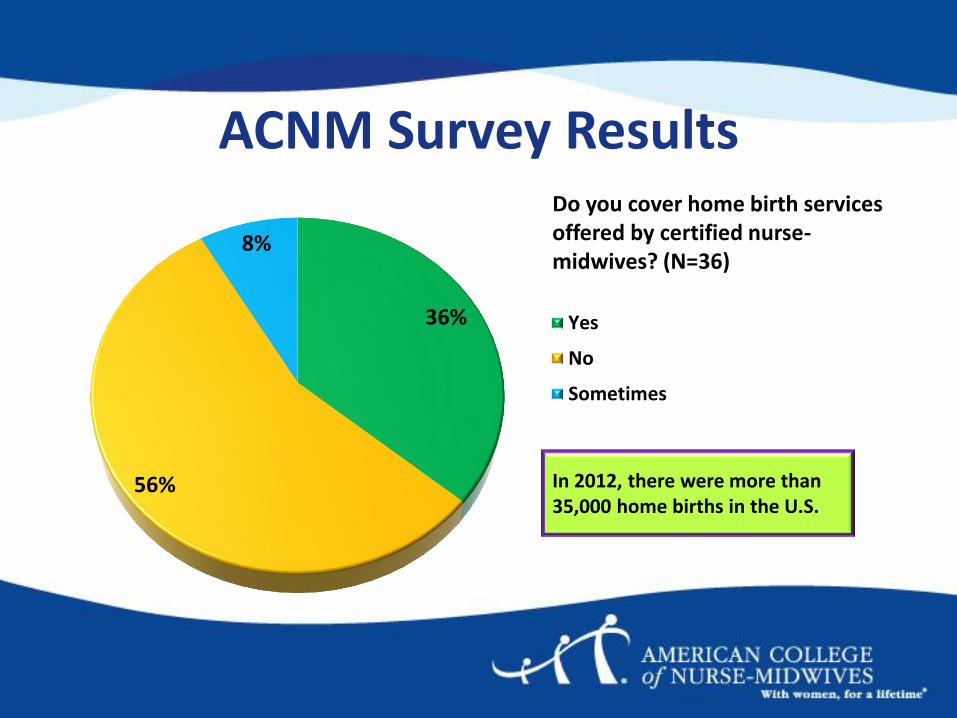
ACNM Survey Results Do you cover home birth services offered by certified nurse-midwives? (N=36)
In 2012, there were more than 35,000 home births in the U.S.
36%
56%
8%
Yes
No
Sometimes
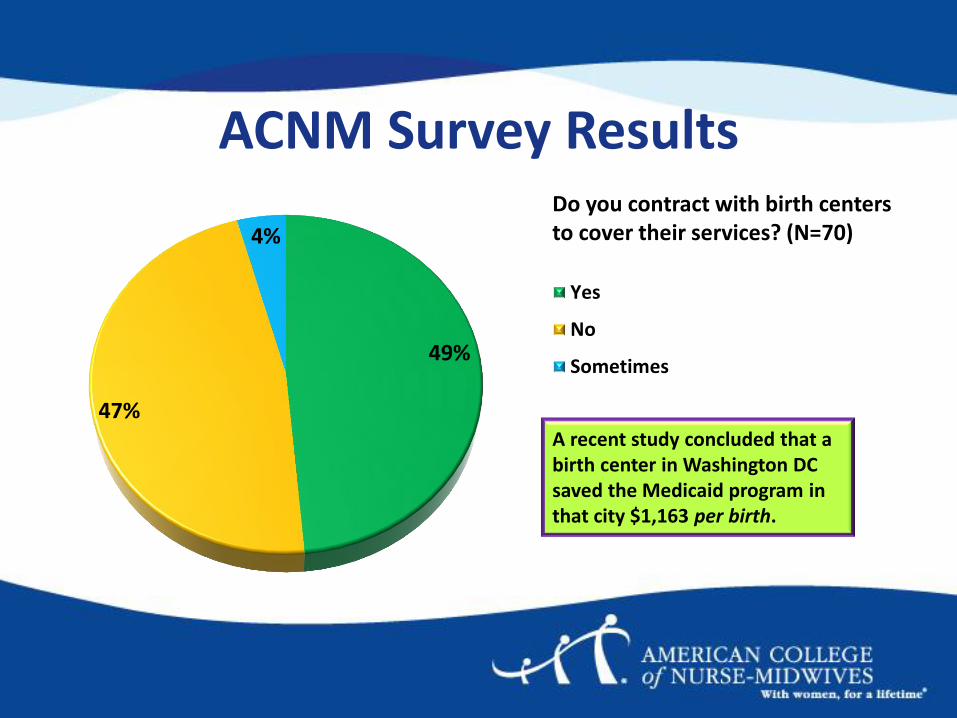
ACNM Survey Results Do you contract with birth centers to cover their services? (N=70)
A recent study concluded that a birth center in Washington DC saved the Medicaid program in that city $1,163 per birth.
49%
47%
4%
Yes
No
Sometimes
Provider Discrimination is Illegal “A group health plan and a health insurance issuer offering group or individual health insurance coverage shall not discriminate with respect to participation under the plan or coverage against any health care provider who is acting within the scope of that provider’s license or certification under applicable State law. This section shall not require that a group health plan or health insurance issuer contract with any health care provider willing to abide by the terms and conditions for participation established by the plan or issuer. Nothing in this section shall be construed as preventing a group health plan, a health insurance issuer, or the Secretary from establishing varying reimbursement rates based on quality or performance measures.” Section 2706(a), Public Health Service Act
Conclusions • ACNM’s survey demonstrates that many plans are systematically
discriminating against CNMs/CMs purely on the basis of licensure. • This behavior is explicitly prohibited by Section 2706(a) of the Public Health
Service Act. • State insurance commissioners have a duty to see that insurers comply with
the provisions of Section 2706(a) of the Public Health Service Act. • State insurance commissioners should closely examine plan networks to
determine whether they are including CNMs/CMs and should inquire as to whether plans are providing coverage for all services CNMs/CMs are allowed to render under applicable state scope of practice requirements.
• Plans that include CNMs/CMs in their networks will save money because the midwifery model of care involves the use of fewer interventions.





























