Upload
others
View
1
Download
0
Embed Size (px)
Citation preview
Neural Regulation of Bone and Bone Marrow
Maria Maryanovich,1,2 Shoichiro Takeishi,1,2 and Paul S. Frenette1,2,3
1Ruth L. and David S. Gottesman Institute for Stem Cell and Regenerative Medicine Research, Albert EinsteinCollege of Medicine, Bronx, New York 10461
2Department of Cell Biology, Albert Einstein College of Medicine, Bronx, New York 104613Department of Medicine, Albert Einstein College of Medicine, Bronx, New York 10461
Correspondence: [email protected]
Bones provide both skeletal scaffolding and space for hematopoiesis in its marrow. Previouswork has shown that these functionswere tightly regulated by the nervous system. The centraland peripheral nervous systems tightly regulate compact bone remodeling, its metabolism,and hematopoietic homeostasis in the bone marrow (BM). Accumulating evidence indicatesthat the nervous system, which fine-tunes inflammatory responses and alterations in neuralfunctions, may regulate autoimmune diseases. Neural signals also influence the progressionof hematological malignancies such as acute and chronic myeloid leukemias. Here, wereview the interplay of the nervous system with bone, BM, and immunity, and discussfuture challenges to target hematological diseases through modulation of activity of thenervous system.
Bones constitute a part of the vertebrate skel-eton, and this organ is formed during thefetal stage of development from either connec-tive tissue (called intramembranous ossifica-tion) or cartilage (referred to as endochondralossification) (Berendsen and Olsen 2015). Afterthese processes, bones are consistently beingcreated and replaced, known as remodeling,which is accomplished through bone resorptionby osteoclasts and bone formation by osteoblasts(Manolagas 2000). Bones not only play a varietyof mechanical roles, but also have synthetic as-pects, one of which is production of blood cellsfrom hematopoietic stem cells (HSCs) in thebone marrow (BM) (Frenette et al. 2013; Men-delson and Frenette 2014). Like most organs invertebrates, these bone functions are regulated
by its constituents and also by long-rangesignals such as leptin from the adipose tissue(Thomas et al. 1999; Cornish et al. 2002; Yueet al. 2016), glucocorticoids from the adrenalglands (Canalis and Delany 2002; Pierce et al.2017), and parathyroid hormone from the para-thyroid glands (Calvi et al. 2003). In addition tothese factors, the nervous system has been sug-gested to regulate bone and BM since the dis-covery of innervation of the skeleton (Calvo1968; Hanoun et al. 2015).
Genetic mutations and epigenetic alter-ations in hematopoietic cells in the BM lead tohematological malignancies, and recent studiessuggested that neuropathy is involved in theprogression of these diseases (Arranz et al.2014; Hanoun et al. 2014). Moreover, previous
Editors: Gerard Karsenty and David T. ScaddenAdditional Perspectives on Bone: A Regulator of Physiology available at www.perspectivesinmedicine.org
Copyright © 2018 Cold Spring Harbor Laboratory Press; all rights reserved; doi: 10.1101/cshperspect.a031344Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
mailto:[email protected]:[email protected]:[email protected]:[email protected]://www.perspectivesinmedicine.orghttp://www.perspectivesinmedicine.orghttp://www.perspectivesinmedicine.orghttp://www.perspectivesinmedicine.org/site/misc/terms.xhtmlhttp://perspectivesinmedicine.cshlp.org/
studies have shown that the nervous system alsomodifies immune functions with deteriorationof this mechanism being associated with auto-immune diseases (Sternberg 2006). In this re-view, we summarize such neuronal regulationof bone, hematopoiesis, and immune functionsas well as provide perspectives to target hema-tological diseases by modulating the nervoussystem.
NEURAL REGULATION OF BONE
The skeleton, in addition to being a structuralorgan and a major site of mineral storage in thebody, also serves as an endocrine organ, secret-ing factors that control the function of othertissues. In parallel bone-derived regulators ofbone homeostasis, skeletal functions are alsoregulated by long-range signals originatingfrom the nervous system.
The central nervous system (CNS) coordi-nates voluntary and involuntary input transmit-ted to tissues by peripheral nerves. The involun-tary responses are regulated by the autonomicnervous system (ANS) comprised of two distinctbranches (Hanoun et al. 2015). The first is thesympathetic nervous system (SNS) that emergesfrom the thoracolumbar spinal cord, and pre-pares the body for alert situations by increasingheart rates and the contractility of myocytes,while diverting blood flow away from the gastro-intestinal (GI) tract. The second is the parasym-pathetic nervous system (PNS) emerging fromthe cranial nerves and the sacral spinal cord (Fig.1). In contrast to the SNS, the PNS decreasesheart rates and muscle contractility, while in-creasing the blood flow to the GI tract, therebypromoting restive and digestive responses.These ANS branches differ in the neurotrans-mitters used at the effector organs. The SNSreleases norepinephrine ([NE] also referred toas noradrenaline) to send signals, whereas ace-tylcholine (ACh) is used as a transmitter in thePNS. NE binds to two forms of the adrenergicreceptor (AR), α and β, which are further divid-ed into subtypes α1 and α2, and β1, β2, and β3,respectively. All of these are G-protein-coupledreceptors: α1 is Gq-coupled, α2 is Gi-coupled,and β1–β3 are Gs-coupled. On the other hand,
ACh from the PNS binds to two receptor sub-types, nicotinic and muscarinic cholinergic re-ceptors, which are classified into N1–N2 andM1–M5, respectively. Besides the ANS, the crosstalk between the CNS and periphery is also ex-erted by the hypothalamic–pituitary–adrenal(HPA) axis, in which glucocorticoids eventuallyreleased from the adrenal cortex into the circu-lation exert functions by binding to their intra-cellular receptors in tissues and regulating tran-scription of various genes (Revollo and Cid-lowski 2009).
Integration of skeletal functions with otherorgans, to maintain total body homeostasis, iscoordinated by the CNS and peripheral nervesoriginating from the ANS. The first histologicalevidence of skeletal innervation came from thepioneering studies of Calvo (1968), providingevidence of bone innervation by nerve fibers,through bone nutrient foramina, with a distri-bution pattern recapitulating the nutrient artery.Many studies since then have confirmed andextended Calvo’s observations and describeboth autonomic and sensory nerve innervationof the skeleton, reaching deep into the BM space(Calvo 1968).
Central Regulation of Skeletal Homeostasis
The initial indication that the CNS can controlbone turnover came from the studies of leptin, apolypeptide hormone exclusively produced bythe adipose tissue (Zhang et al. 1994). Leptinwas originally identified to control body weightand gonadal function through its action on thearcuate nucleus of the hypothalamus (Zhanget al. 1994; Halaas et al. 1995; Friedman andHalaas 1998). Studies focusing on peripheralaction of leptin and its receptor on bone cellssuggested that leptin acted as an osteogenic fac-tor by activating its receptor on bone osteoline-age cells (Thomas et al. 1999; Cornish et al.2002). Other studies, however, suggest thatthe signaling of leptin in the CNS regulatesbone mass, wherein intracerebroventricular(ICV) infusion of leptin corrected the highbone mass observed in ob/ob mice or reducedbone mass when infused into wild-type mice,highlighting the central function of leptin in
M. Maryanovich et al.
2 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
controlling skeletal homeostasis (Fig. 2) (Ducyet al. 2000).
Another centrally acting neurotransmitterlinked to bone homeostasis is serotonin (5-hy-droxytryptamine [5-HT]), which was found todifferentially regulate bone mass depending onits site of action (Walther et al. 2003). Serotoninis primarily produced in the CNS by tryptophanhydroxylase 2 (Tph2), or in the GI tract by tryp-tophan hydroxylase 1 (Tph1) that contributes toblood serotonin levels, which does not cross theblood–brain barrier and does not contribute toits role as a neurotransmitter in the brain (Dimi-tri andRosen2017). In theCNS, serotoninmain-ly functions as a mood stabilizer supporting
cognitive function, emotional well-being, andhappiness (Schmitt et al. 2006; Alenina andKlempin 2015). One of the initial links of sero-tonin and bone homeostasis came from clinicalstudies of depression patients with reduced sero-tonergic tone or patients taking selective seroto-nin reuptake inhibitors (SSRIs) as treatment ofdepression. These studies revealed that seroto-nergic deficiency or chronic use of SSRIs in-creased the risk of osteoporotic bone fractures(Feuer et al. 2015; Sheu et al. 2015; Rauma et al.2016). Further validation of these findings camefrom studies in mice in which pharmacologicalinhibition or genetic deletion of the 5-HT trans-porter, responsible for cellular serotonin reup-
T1
T2
T3
T4
T5
T6
T7
T8
T9
T10
T11
T12
L1
L2
L3
L4
L5
Lumbarspinal cord
Thoracicspinal cord
Cervicalspinal cord
Sacralspinal cord
Sympathetic ganglion chain
Brain stem PNSnerves
Sympathetic nerves
Parasympathetic nervesSensory nerves
C1
Para-sympathetic
ganglia
?
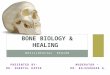
Figure 1. Schematic illustration depicting the anatomic origin of sympathetic, parasympathetic, and sensoryinnervation of bone. PNS, Parasympathetic nervous system.
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
take, resulted in a reduced bonemass phenotype(Warden and Haney 2008; Warden et al. 2010).Neurotransmitter profiling in the brain of ob/obmice revealed that leptin deficiency induced ac-cumulation of brain stem serotonin levels andthat deletion of Tph2 in mice (Tph2−/−) resultsin loss of bone mass attributable to increasedbone resorption and decreased bone formation(Yadav et al. 2009). Specific deletion of leptinreceptor (Lepr orObRb) in serotonergic neuronsby crossing Obrb-floxed mice with serotonintransporter promoter (Sert-Cre) or Tph2-Crelines resulted in morbid obesity associated withdramatic increase in bone mass, reminiscent ofthe Lepr deficiency (db/db), confirming that themechanism of leptin skeletal metabolism is byinhibition of serotonin synthesis in the brainstem. Moreover, loss of central Tph2 reducedadiposity owing to reduced appetite and in-creased energy expenditure, similar to the ob/ob leptin-deficient mouse model (Yadav et al.2009). These findings, thus, suggest a centralrole for serotonin in the CNS, downstreamfrom leptin, in regulating appetite, energy ex-penditure, and bone metabolism (Fig. 2).
Along its role in the CNS, peripheral sero-tonin synthesized in the GI tract by enterochro-maffin cells in the duodenum has also beenshown to regulate bone homeostasis. The roleof peripheral serotonin on bone homeostasis
has emerged from studies of LRP5, an LDL-re-ceptor-related protein 5, a coreceptor for Wntligands and one of themost studied regulators ofbone homeostasis (Baron and Rawadi 2007).Mutations in LRP5 are associated with dramaticderegulation of bone formation, in which loss-of-function mutations cause severe bone lossand osteoporosis pseudoglioma, and gain-of-function mutations increase bone mass (Gonget al. 2001; Boyden et al. 2002; Little et al. 2002).Interestingly, deletion of Lrp5 gene in mice(Lrp5−/−) increased expression of Tph1 in bothbones and the gut and significantly elevatedserotonin serum levels (Yadav et al. 2008).Gut-specific deletion of Lrp5 recapitulated thephenotypes of low bone mass in Lrp5−/− mice,revealing a novel gut-to-bone exocrine axis in-volving serotonin (Kode et al. 2014). Once re-leased into the bloodstream, serotonin regulatesbone remodeling by direct signaling to its recep-tor 5-hydroxytryptamine receptor 1B (HTR1B)expressed by osteoblasts, inhibiting activation ofthe cyclic adenosine monophosphate (cAMP)response element-binding (CREB) transcrip-tion factor, whose activity is necessary for nor-mal osteoblast proliferation (Yadav et al. 2008).
Similar to leptin, neuropeptide Y (NPY) ishighly expressed in the hypothalamic arcuatenucleus where it regulates appetite downstreamfrom leptin (Stanley et al. 1986; Erickson et al.1996). NPY signals are mediated via five majorNPY receptors (Y1–5), of which both Y1 and Y2receptors, abundant in the CNS, have beenshown to regulate bone mass (Horsnell and Bal-dock 2016). Peripheral expression of NPY re-ceptors in adipocytes, osteoblasts, and osteo-cytes have also been reported (Kuo et al. 2007;Lundberg et al. 2007; Lee et al. 2010). Initialstudies showed that ICV infusion of NPY tothe cerebrospinal fluid, in contrast to leptin, in-duced loss of bone mass, indicating that NPYand leptin do not antagonize each other’s func-tion in the CNS (Ducy et al. 2000). Mice defi-cient in NPY (NPY−/−) or Y receptor 2 (Y2−/−)showed significantly increased bone mass asso-ciated with increased osteoblast activity and in-creased expression of osteogenic transcriptionfactors, Runx2 and Osterix (Osx), comparedwith wild-type controls (Baldock et al. 2002,
Adipose cells
Leptin
Hypothalamic serotonin
Sym
path
etic
Bone remodeling
Central Chrm3
Parasym
pathetic
Central IL-1
Bone remodeling
Figure 2. Schematic illustration summarizing centralnervous system (CNS) regulators of bone remodeling.
M. Maryanovich et al.
4 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
2005, 2009). The bone phenotype observed inY2−/− mice was independent of leptin signalingor expression of Y2 receptors in the osteolineagecells, highlighting the critical role of central Y2in regulating bone remodeling. The Y1 receptorhas also been implicated in bone remodeling inthat Y1−/− mice showed increased bone mass(Baldock et al. 2007). This function, however,was attributed to peripherally expressed Y1, be-cause hypothalamic deletion of Y1 resulted inno apparent bone phenotype. In addition to theaforementioned central regulators of bone re-modeling, the number of central neuropeptidesand hormones involved in skeletal homeostasisis expanding. Centrally acting cocaine- and am-phetamine-regulated transcript (CART), neuro-medin U, melatonin, adiponectin, and the en-docannabinoid system have all been implicatedto play diverse roles in bone remodeling. Owingto the limited focus of this review on these neu-ropeptides, a thorough review of thesemoleculesand pathways can be found elsewhere (Wee et al.2016; Dimitri and Rosen 2017).
Autonomic Control of the Bone Remodeling
The SNS represents the major arm of the CNS,controlling skeletal homeostasis, mainly by ac-tion of ARs expressed on target bone cells. Pre-ganglionic neurons from the thoracolumbar spi-nal cord form sympathetic ganglia from whichpostganglionic neurons innervate target organs(Fig. 1). Immunofluorescence imaging studieshave detected the presence of postganglionicneurons in bone by detection of the neuromod-ulators that they express. Peripheral sympa-thetic innervation of bone can be visualized bystaining for tyrosine hydroxylase (TH), a rate-limiting enzyme involved in catecholamine syn-thesis or NPY that is commonly expressed bysympathetic neurons (Bjurholm et al. 1988b).TH-expressing nerve fibers closely associateand ensheathe blood vessels and can be detectedin the periosteum,mineralized bone, and furtherinnervating the BM hematopoietic cavity (Bel-linger et al. 1992). The pattern of nerve distribu-tion in the bone microenvironment—wherelarge nerves accompany arteries that feed thebone at multiple locations—suggests that most
bone-associated cells do not come in direct con-tact with nerve fibers and that nerve signal trans-duction is nonsynaptic. In this scenario, over-flow of NE from vascular nerves may signal toARs expressed on bone cells. Evidence for therole of ARs in skeletal metabolism has emergedfrom studies in rodents, in which pharmacologicperturbation of β-adrenergic signals has impact-ed bonemass. Significant bone loss was detectedin mice treated with the β-adrenergic agonistisoproterenol, whereas treatment with propran-olol (nonselective β-adrenergic antagonist) hadbeneficial effects on bone homeostasis (Takedaet al. 2002).
Bone remodeling comprises two phases:bone resorption, which is facilitated by osteo-clasts, and bone formation mediated by osteo-blasts. β-ARs are the major transducers ofadrenergic signals in peripheral tissues. In thebone, β2-ARs are primarily expressed by osteo-blasts, and expression has also been detected inbone-forming osteocytes, osteoclasts, and chon-drocytes, suggesting neural control ofmost boneand cartilage cell types (Elefteriou et al. 2014). Itstill remains unclear which particular bone celltype is most responsive to SNS signals. Evidencesupporting the cross talk between leptin, SNS,and β2-AR signaling in bone remodeling camefrom studies of mice deficient in dopamine hy-droxylase (DBH) in which the inability to syn-thesize catecholamines led to bone mass accrual(Takeda et al. 2002). Moreover, clinical studiesof patients with reflex sympathetic dystrophy,associated with increased sympathetic tone,were found to produce osteoporosis, which insome cases can be rectified by antagonizing β-adrenergic signaling (Schwartzman 2000). A di-rect link between the SNS signaling and boneremodeling emerged from studies of β2-AR-de-ficient mice (Adrb2−/−). Similar to deletion ofleptin or Lepr, β2-AR deletion resulted in in-creased bone mass phenotype; however, ICV in-fusion of leptin in these mice failed to rescuethe increased bone mass (Elefteriou et al. 2005;Bonnet et al. 2008). Further analysis ofAdrb2−/−
mice revealed that the SNS favored bone resorp-tion by inducing production of osteoblast-de-rived osteoclast differentiation factor Rankl(Elefteriou et al. 2005). Interestingly, unlike in
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
ob/ob mice, Adrb2−/− did not induce weightgain or gonadal dysfunction, suggesting thatβ2-AR signaling specifically controlled skeletalturnover. Finally, osteoblast-specific deletionof β2-ARs, by crossing mice that express theβ2-AR-floxed allele with mice carrying theα1Col1-Cre, recapitulated the high bone massphenotype of Adrb2−/− mice, confirming thatβ2-ARs are major mediators of SNS signals byosteoblasts (Kajimura et al. 2011). Along withβ2-ARs, other ARs have been implicated toplay a role in both central and peripheral controlof skeletal homeostasis. A thorough review ofthese molecules and their functions is reviewedelsewhere (Dimitri and Rosen 2017).
Similar to the SNS, the PNS has also beensuggested to innervate the skeleton. Emergingfrom cranial nerves and the sacral spinal cord(Fig. 1), PNS nerves can be detected to penetratethe bone distal femoral metaphysis by im-munostaining for choline acetyltransferase(ChAT) (Artico et al. 2002; Bajayo et al. 2012),an enzyme responsible for synthesis of acetyl-choline. Peripheral cholinergic signaling can in-crease bone mass via activation of nicotinic re-ceptors (α2nAChR) expressed by osteoclasts,inhibiting bone resorption by induction of oste-oclast apoptosis (Bajayo et al. 2012). Moreover,activation of nAChRs by specific agonists caninduce osteoblast proliferation, further contrib-uting to bonemass accrual. However, deletion ofα2nAChR in mice leads to osteoclast-driven lossof bone mass (Bajayo et al. 2012). In addition tonAChRs, muscarinic receptors (mAChRs) havealso been implicated in skeletal homeostasis andshown to be expressed by bone cells (Liu et al.2011; Kauschke et al. 2015). There are fivemAChRs (Chrm1–5) of which type 3 muscarin-ic receptor (Chrm3) was shown to be crucial forbone remodeling. Deletion of Chrm3 in mice(Chrm3−/−) is associated with low bone massphenotype; however, unlike ARs or nAChRs ex-pressed by bone cells, Chrm3 expression andactivity in the brain stem affected bone remod-eling by suppressing the sympathetic tone (Shiet al. 2010). Interestingly, central expression ofinterleukin 1 (IL-1) cytokine was shown to be akey positive regulator of parasympathetic tone(Bajayo et al. 2012), illustrating the antagonistic
relationship between the SNS and PNS in con-trolling skeletal homeostasis (Fig. 2).
Sensory Innervation of the Bone
The presence of sensory nerves in the bone wasdocumented by detection of either substance P(SP) or calcitonin gene-related peptide (CGRP)-positive nerve fibers (Bjurholm et al. 1988).Femoral sensory nerves originate from the dor-sal root ganglia of the lumbar spinal cord andinnervate mineralized bone, periosteum, andfurther penetrate the BM (Fig. 1) (Bjurholmet al. 1988a; Yoshino et al. 2014). The role ofsensory innervation on skeletal homeostasisemerged fromdenervation studies in which cap-saicin was used to destroy sensory nerves. Thesestudies showed that denervation of sensorynerves induced reduction in bone mineral den-sity attributable to increased osteoclast activity(Offley et al. 2005; Ding et al. 2010). Interesting-ly, in vitro studies showed that CGRPmay act onosteoclasts, osteoblasts, and other stromal cellsto regulate bone formation. Treatments of oste-oclast or BM cultures with CGRP inhibited os-teoclast formation and activity, inhibiting boneresorption and promoting proliferation and os-teogenic differentiations of BM mesenchymalstem cell (MSC) cultures, leading to increasedmineralization (Zaidi et al. 1987; Cornish et al.2001; Ishizuka et al. 2005; Wang et al. 2010;Liang et al. 2015).
NEURONAL REGULATION OF BONEMARROW
Autonomic nerves reaching the bones also pen-etrate the BM, reaching deep into regions ofhematopoietic activity. Out of all the autonomicnerves that reach the bone, it was shown thatonly close to 5% of SNS nerves actually penetratethe BM (Jung et al. 2017). However, taking intoaccount the relative volume of the bone cavitycompared with the periosteal bone region, theBM contains the highest density of autonomicnerves (Mach et al. 2002).
The BM microenvironment contains spe-cialized niches responsible for maintenance ofHSCs, which generate all blood cell lineages
M. Maryanovich et al.
6 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
throughout life. HSC niches are composed ofspecialized cell types derived from mesenchy-mal, endothelial, stromal, and neural originthat integrate membrane-bound and secretedsignals controlling quiescence, proliferation,and retention of HSCs (Fig. 3) (Asada et al.2017b). At steady state, most HSCs are main-tained in a quiescent state within their niche.In response to stress (such as radiation injury,chemotherapy, or infection), HSCs become ac-tivated to restore homeostasis (Wilson et al.2009). The SNS represents a critical regulatorycomponent of the BM microenvironment,where sympathetic nerve fibers and other neuralcrest derivatives form a niche, essential formaintaining HSC behavior during both homeo-stasis and stress situations (Hanoun et al. 2015).To date, the role of the PNS has largely been
attributed to bone remodeling and very little isknown about cholinergic signaling affectingHSCs or their microenvironment. A recentstudy revealed that Chrm1 promotes HSC mo-bilization from the BM but it did not act fromthe BM microenvironment but rather from theCNS where it activates the HPA axis, releasingglucocorticoids that prime HSCs to migrate(Pierce et al. 2017).
As previously mentioned, sensory nervesthat reach the bone are also detected in theBM (Bjurholm et al. 1988; Hill and Elde 1991;Mach et al. 2002). Ablation of sensory nerveswith capsaicin was reported to reduce BM cel-lularity and blood counts, suggesting a regula-tory role for sensory nerves in hematopoiesis(Broome and Miyan 2000). In vitro cultures ofhematopoietic progenitors with sensory neuro-
NE
CXCL12SCF
HSC
HSC retention
Sinusoid
Arteriole
SNS nerve fiberwith nonmyelinating
Schwann cells
Osteoblast β2-AR
β3-AR
Osteocyte
Osteoclast
HSC mobilization
NG2+/Nestinhigh MSC Sinusoidal
endothelium
CXCL12
CAR cell
LepR+ cell
Bone marrow
Bone
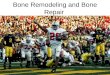
Figure 3. Autonomic signals modulate hematopoietic stem cell (HSC) niche homeostasis at steady state. Periph-eral sympathetic neurons are one of the main components of a healthy HSC niche. Circadian noradrenalinesecretion from sympathetic nerve terminals leads to circadian expression of C-X-C chemokine ligand 12(CXCL12) by Nestinhigh/NG2+ perivascular mesenchymal stem cells (MSCs), resulting in rhythmic release ofHSCs to the periphery. The adrenergic signals in this case aremediated through the β3-adrenergic receptor (AR).Secretion of HSC maintenance factors such as stem cell factor (SCF) and CXCL12 by Nestinhigh/NG2+ MSCskeeps a subset of HSCs quiescent and in close association with arteriolar blood vessels, ensheathed with sym-pathetic nervous system (SNS) nerve fibers. When activated, HSCs relocate near the Nestinlow leptin receptor(LepR)-expressing perisinusoidal area. SNS signals also regulate bone formation via β2-AR signaling in osteo-blasts. In addition to SNS nerves, nonmyelinating Schwann cells also maintain HSC dormancy through activa-tion of the transforming growth factor β (TGF-β)/SMAD signaling.
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
peptides SP and CGRP stimulated progenitoractivity (Rameshwar and Gascon 1995; BroomeandMiyan 2000), partly explaining the impairedblood production following capsaicin adminis-tration. Although these studies suggest a directinvolvement of sensory neuropeptides in regu-lating HSC and progenitor activity in the BM,further studies are required to determine theextent of sensory nerves cross talk with the au-tonomic control of hematopoiesis.
Neuronal Components of the HSC Niche
Aniche responsible formaintainingHSCs in theBM was initially proposed to be composed ofosteolineage-derived cells (Calvi et al. 2003;Zhang et al. 2003). Bone-lining osteoblasts andother osteolineage cell types were proposed tomaintain HSCs through secretion of angiopoie-tin-1 (Arai et al. 2004) and osteopontin (Opn)(Nilsson et al. 2005; Stier et al. 2005). More re-cent studies, however, have found that deletionof key HSC maintenance factors (C-X-C che-mokine ligand 12 [CXCL12] and stem cell factor[SCF] cytokines) inmature osteoblasts (express-ing osteocalcin [Bglap]-Cre or Col2.3-Cre) had anegligible effect on HSC maintenance (Dinget al. 2012; Ding and Morrison 2013). Thesedata support the notion that osteoblasts do notdirectly support HSCs, but rather osteolineagecells were suggested to create a niche for earlylymphoid progenitors, implying that HSCs andrestricted progenitors occupy distinct niches inthe BM microenvironment. Evidence for thiscame from immunofluorescence studies of BMsections, which revealed that lineage Il7Rα+ lym-phoid progenitors were predominantly localizedto the endosteal region of the BM, close to oste-oblasts and that genetic ablation of CXCL12 inosteoblasts (using the Col2.3-Cremodel) deplet-ed common lymphoid progenitors (CLPs) andIl7Rα+ lymphoid-primed multipotent progeni-tors (LMPPs) without affecting HSC homeosta-sis (Zhu et al. 2007; Ding and Morrison 2013).However, a more recent study showed that alarge percentage of CLPs were localized furtherthan 30 µm away from the endosteal region andno IL-7 production by osteoblasts could be de-tected. Furthermore, conditional deletion of Il7
in osteoblasts using the Col2.3-Cre model didnot affect B lymphopoiesis. In contrast, IL-7was predominantly produced by a subset ofCXCL12-abundant reticular (CAR) cells, whichare located in perivascular regions of the BM(Cordeiro Gomes et al. 2016).
Recent advances in imaging technologieshave revealed that HSCs were primarily locatedin perivascular areas of the BM in close prox-imity to endothelial cells and perivascular stro-mal cells (Entschladen et al. 2004; Kiel et al.2005; Mendez-Ferrer et al. 2010b; Ding et al.2012; Kunisaki et al. 2013; Acar et al. 2015; Itkinet al. 2016; Kusumbe et al. 2016). The BM vas-cular architecture is composed of two types ofblood vessels: (1) sinusoidal blood vessels, fen-estrated structures evenly distributed in the BMspace, and (2) arteriolar blood vessels, primarilylocated near the endosteal bone region and high-ly innervated by the SNS (Fig. 3) (Kunisaki et al.2013; Sivaraj and Adams 2016). The endothelialcell network contributes to niche activity andsupports HSCs by secreting essential factorssuch as CXCL12 and SCF (also known as Kitl)(Kiel et al. 2005; Ding et al. 2012; Ding andMor-rison 2013). Interestingly, a recent study of vas-cular niche aging failed to show that rejuvena-tion of vasculature could rescue age-relatedHSCattrition (Kusumbe et al. 2016), highlightingthat other niche regulators may be required tomaintain HSCs throughout life. SNS nerves andperivascular stromal cells, expressing a type VIintermediate filament protein Nestin, ensheathearterioles forming structural networks termedthe neuroreticular complex (Yamazaki and Al-len 1990; Mendez-Ferrer et al. 2010b; Kunisakiet al. 2013). Interestingly, a subset of quiescentHSCs is found to be closely associated withthese arteriolar structures (Mendez-Ferrer etal. 2010b; Kunisaki et al. 2013; Itkin et al. 2016;Kusumbe et al. 2016), placing sympatheticnerves as central components of the HSC niche.Nestin-expressing perivascular cells, which arehighly enriched for HSC maintenance andretention factors, including Vcam1, Cxcl12,Angpt1, Scf, and Opn, were shown to containBM MSC activity, giving rise to osteogenic, adi-pogenic, and chondrogenic lineages (Mendez-Ferrer et al. 2010b; Pinho et al. 2013). These
M. Maryanovich et al.
8 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
Nestin+ cells can also be labeled with the NG2pericyte marker-specific Ng2-Cre line (Kunisakiet al. 2013; Asada et al. 2017a) and represent amajor HSC regulatory component within theniche. Depletion of these cells (using the Ng2-CreERTM/iDTR model) significantly impairedHSC quiescence, leading to exhaustion of HSCs(Kunisaki et al. 2013), and Scf depletion inNG2-targeted cells (using the Ng2-Cre/Scfflox/− mod-el) reduced HSC numbers in the BM and com-promised their long-term reconstitution activity(Asada et al. 2017a). Several other candidateperivascular stromal cells have alsobeen suggest-ed to regulate healthyHSCs, including CARcells(Sugiyama et al. 2006), Lepr-expressing cells(Ding et al. 2012), and stromal cells targeted byeither Osx-Cre or paired related homeobox-1(Prx-1)-Cre (Ding and Morrison 2013; Green-baum et al. 2013); however, these cell types wereshown to largely overlap with Nestin-green fluo-rescent protein-positive (GFP+) MSCs (Kunisakiet al. 2013; Pinho et al. 2013; Asada et al. 2017a).
Like more mature osteolineage cells, Nestin-GFP+ MSCs express β-ARs. However, in con-trast to osteoblasts in which stimulation of β2-ARs controls bone remodeling (Takeda et al.2002), signaling via the β3-ARs on MSCs wasshown to be critical for their homeostasis (Men-dez-Ferrer et al. 2008, 2010a). Denervation stud-ies showed that ablation of SNS signals leads toproliferation and expansion of normally quies-cent MSCs, whereas adrenergic stimulation,mediated through β3-ARs, leads to decreasedosteogenic differentiation and expression ofHSC-regulating genes (Mendez-Ferrer et al.2010b; Lucas et al. 2013). Thus, similar to oste-oblasts and osteocytes abundant in the compactbone (Takeda et al. 2002; Elefteriou et al. 2005;Asada et al. 2013), BM-derived MSCs are a ma-jor target of the SNS.
Additional neural crest derivatives have alsobeen identified in the HSC niche. Nonmyelinat-ing Schwann cells that wrap around sympatheticnerve fibers were suggested to preserve HSCquiescence through activation of transforminggrowth factor β (TGF-β) and SMAD signaling(Yamazaki et al. 2011). In this study, denerva-tion of sympathetic nerves resulted in significantdecrease in Schwann cell numbers, which com-
promisedHSC dormancy and induced HSC lossas early as 3 days after denervation surgery.However, in another study, acute surgical andchemical sympathectomy did not alter HSCand progenitor numbers in the BM (Mendez-Ferrer et al. 2008). Thus, it remains unclearhow sympathetic nerves can signal to Schwanncells and to what extent BM denervation, inde-pendent from off-target effects such as inflam-mation following surgery, contributed to theeffects observed on HSCs. Other neurotrophicfactors and neuropeptides may also regulateHSC homeostasis (Liu et al. 2007). For instance,release from NPY by SNS nerves was shown toenhance the activity of matrix metalloprotein-ase-9 in the BM microenvironment, leading todegradation of HSC and progenitor retentionfactors, resulting in HSC mobilization (Parket al. 2015, 2016). Moreover, SP and neuroki-nin-A,members of the tachykinin family of neu-ropeptides, have been suggested to stimulateproduction of hematopoietic cytokines by BMstromal cells, in addition to serving as essentialmodulators of both normal and malignant he-matopoiesis (Nowicki et al. 2007).
Sympathetic Control of HealthyHematopoiesis
Initial evidence that SNS nerves might regulatehematopoiesis emerged from studies describinga positive correlation between BM circadian os-cillations of NE and proliferation of hematopoi-etic cells (Maestroni et al. 1998). The findingthat fucoidan, a selectin glycomimetic inhibitor,induced rapid HSC mobilization, independentof selectin inhibition (Frenette 2000; Sweeneyet al. 2000), raised the possibility that sulfatedglycans in the BM microenvironment modulateHSC retention. Indeed, mice deficient in theuridine diphosphate (UDP)-galactose ceramidegalactosyltransferase (Cgt−/−), an enzyme thatcatalyzes the final step of galactocerebroside(GalC) synthesis, the major component of my-elin sheaths and responsible for adequate nerveconduction (Norton and Cammer 1984),showed poor mobilization of HSCs when stim-ulated with granulocyte colony-stimulating fac-tor (G-CSF) (Katayama et al. 2006).
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
HSC and progenitor mobilization from theBM to peripheral organs depends on an intactgradient of the CXCL12 chemokine, which canbe disrupted following administration of G-CSF,leading to rapidHSC and progenitor egress fromthe BM (Hattori et al. 2001; Petit et al. 2002).Local sympathetic nerves deliver, in a circadianmanner, SNS signals to the BM, which are trans-duced by β-ARs, leading to down-regulation ofCXCL12 expression and rhythmic release ofHSCs (Mendez-Ferrer et al. 2008). Sympatheticdenervation in genetic and pharmacologicalmodels blunts the CXCL12 down-regulation af-ter G-CSF treatment, resulting in impaired he-matopoietic stem and progenitor cell (HSPC)mobilization (Katayama et al. 2006; Mendez-Ferrer et al. 2008, 2010a). Nevertheless, the de-fective HSPC mobilization in Cgt−/− mice wasnot caused by the lack of GalC production butrather impaired adrenergic regulation of nichecells involved in the mobilization of HSCs (Ka-tayama et al. 2006). Additional studies of leuko-cyte and stem cell recruitment to the BM showedthat circadian oscillations in endothelial adhe-sion molecules depended on expression ofβ-ARs and require local delivery of NE (Schei-ermann et al. 2012). These seminal studiespropose a model in which core genes of the mo-lecular clock in the CNS act through local circa-dian NE secretion to regulate HSC retention,mobilization, and homing.
CXCL12 is largely secreted by perivascularMSCs, and to lesser extent by endothelial cellsand osteoblasts (Ding and Morrison 2013;Greenbaum et al. 2013; Asada et al. 2017a).The circadian release of HSCs is mediated byβ3-ARs that are predominantly expressed byNestin-GFP+ MSCs (Mendez-Ferrer et al.2010b). However, G-CSF-enforcedmobilizationof HSPCs depends on adrenergic signals medi-ated through both β2 and β3-ARs (Mendez-Fer-rer et al. 2010a), associated with suppression ofMSC and osteolineage cell function (Semeradet al. 2005; Katayama et al. 2006; Christopherand Link 2008; Mendez-Ferrer et al. 2008,2010a; Asada et al. 2013). It is important tonote that G-CSF-mediated mobilization notonly down-regulates CXCL12 production byNestin-GFP+ MSCs but also suppresses the
function of macrophages, which was shown toaffect HSC mobilization (Semerad et al. 2005;Chowet al. 2011). Therefore, enforcedmobiliza-tion is a complex process involving cross talkbetween several different cell types in the BMmicroenvironment.
Besides HSC mobilization, SNS signals areessential for regeneration of hematopoiesis fol-lowing genotoxic stress (Lucas et al. 2013). Ex-posure to neurotoxic drugs (e.g., chemotherapyor exposure to irradiation) damages the BMmi-croenvironment leading to sympathetic neurop-athy and induction of MSC and endothelial cellproliferation. Excess proliferation further sensi-tizes these cells to genotoxic insults, leading toreduced niche size and failure to support hema-topoietic recovery. Administering of the neuro-protective agents 4-methylcatechol (4-MC) orthe glial-derived neurotrophic factor (GDNF)together with the neurotoxic agents rescuedsympathetic nerve fibers (Lucas et al. 2013).This combined treatment protected BM nichecells from genotoxic insults and allowed normalhematopoietic recovery. These studies thus sug-gest that diseases or therapies accompanied withperipheral neuropathy have an underappreciat-ed long-term damaging effect on hematopoiesis,which is preventable.
Despite the essential role of the SNS in reg-ulating the HSC niche, one must also consider adirect effect on hematopoietic cells. Expressionof ARs on HSCs and progenitors was docu-mented in both human and rodent, with HSCsmainly expressing the α1, α2, and β2-ARs butnot β3-ARs (Muthu et al. 2007). Interestingly,however, the function of AR stimulation onHSCs still remains poorly understood. Humanhematopoietic progenitors were shown to beregulated directly by SNS signals, as immatureclusters of differentiation 34-positive (CD34+)progenitors express dopamine receptors, whichcan be induced following G-CSF mobilization(Spiegel et al. 2007). Furthermore, catechol-amines support both motility and proliferationof CD34+ progenitors, which suggests that theSNS has both HSC autonomous and nonauton-omous (niche-mediated) effects. Similar to ro-dents, mobilized human stem and progenitorcells also fluctuate in a circadian manner, al-
M. Maryanovich et al.
10 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
though the circadian rhythm in humans is in-verted with significantly higher yields of stemcells toward the evening (Lucas et al. 2008).This might be clinically relevant for mobiliza-tion and BM transplantation when treating ma-lignant blood disorders (Gratwohl et al. 2013).
Role of SNS Nerves in the Progressionof Hematological Malignancies
In line with the findings of neuronal regulationof normal hematopoiesis as described earlier,recent studies show that neuropathy in theSNS is involved in the development of hemato-logical malignancies. It is becoming increasinglyclear that at least in some malignancies includ-ing leukemia, cancer progression displays fea-tures similar to normal tissue organization.That is, there may be a developmental hierarchyin cells that constitute cancer in which cancerstem cells (CSCs) have a potential to self-renewand give rise to transient-amplifying cancer cellsthat are driving tumor growth (Clevers 2011;Kreso and Dick 2014). The origin of CSCs is stillcontroversial, and one of the proposed hypoth-eses is that CSCs emerge as a result of accumu-lation of mutations in stem cells (or other long-lived cells) in the tissue (Passegue et al. 2003;Bjerkvig et al. 2005). Consistent with this no-tion, CSCs are known to share many biologicalcharacteristics with their healthy counterparts,including maintenance of quiescence in the cellcycle (Pece et al. 2010; Roesch et al. 2010; Saitoet al. 2010). Given that it is considered that suchproperties render CSCs resistant to currentlyavailable anticancer drugs that preferentiallytarget dividing cells and that residual CSCs aftertherapies are a potential cause of relapse (Cle-vers 2011; Kreso and Dick 2014), research aim-ing to comprehend CSC behavior has drawnmore attention in the field of cancer biology,and therapies that are able to eradicate CSCsare now being intensely developed.
Leukemia stem cells (LSCs), the CSCs of leu-kemia, have contributed to our knowledge just asHSCs have long served as an important experi-mental subject to dissect mechanisms by whichhealthy stem cell function is regulated. Previousstudies with the use of the xenograft model of
LSCs in human primary acute myelogenous leu-kemia (AML) showed that leukemic cells residein the endosteal region of the BM after treatmentwith the antileukemic agent cytosine arabino-side (Ara-C) (Ishikawa et al. 2007), and theseresidual cells were found to be quiescent (Saitoet al. 2010). Although the detailed localization ofLSCs in the BM still remains to be solved, giventhe clinical finding that patients with hemato-logical malignancies are likely to show pancyto-penia (a reduction in the number of red andwhite blood cells as well as platelets), it hasbeen postulated that HSCs are expelled fromtheir niche in these diseases and LSCs use theresultant vacant area for leukemogenesis. An-other evidence that leukemia patients who havereceived allogeneic stem cell transplantation candevelop donor-derived leukemia (Wiseman2011) further suggests that LSCs might notonly occupy the HSC niche but also remodel itinto a malignant microenvironment. Indeed,there are several studies showing morphologi-cal and functional alterations of BMstromal cellsin patients with various hematological diseases,including AML, myelodysplastic syndrome(Duhrsen and Hossfeld 1996), and primary my-elofibrosis (Pereira et al. 1990).
Owing to recent advances in generationof murine models of hematological diseases,mechanistic insights into the formation andfunction of malignant niches have been provid-ed. For instance, a mouse model of chronic my-elogenous leukemia (CML), which is caused by achromosomal translocation that joins the BCRand ABL genes (Rowley 1973; de Klein et al.1982), was established by generation of induc-ible BCR-ABL transgenic mice (Reynaud et al.2011). In this model, leukemia cells inducedMSCs to expand their osteolineage cells, andsuch MSC stimulation required direct contactof leukemic cells (Fig. 4A) (Schepers et al.2013). These interactions led to the overproduc-tion of C-C motif ligand 3 (CCL3) and throm-bopoietin (TPO) and alteration of several signal-ing pathways, including TGF-β, Notch, andWnt. The remodeled osteolineage cells showedimpaired capacity to support HSCs while LSCswere maintained in such an environment, indi-cating that leukemic cells indeed remodel the
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
CML
Cortex
BM
BCR-ABL+leukemic cell
Cytokines(CCL3, TPO, etc.)
HSC(impaired hematopoiesis)
HSC maintenancefactors
(SCF, CXCL12, etc.)
RemodeledMSC Partial recovery of
HSC maintenancefactors
Skeweddifferentiation
HSC(rescued hematopoiesis)
Imatinibtreatment
Osteocyte
Osteoblast
AML
Degeneratedcatecholaminergic fiber
Osteoblasticcell
HSC(impaired hematopoiesis)
MLL-AF9+
leukemic cell
HSC maintenancefactors
(SCF, CXCL12, etc.)
RemodeledMSC
Skeweddifferentiation
NE
2-AR
MPN
A
B
C
Damage inSNS and Schwann cell
IL-1 HSC(impaired
hematopoiesis)
JAK2(V617F)+
HSPC
Apoptosis ofMSCNE
3-AR
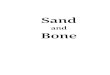
Figure 4.Altered hematopoietic stem cell (HSC) niche, including sympathetic neuropathy, promotes progressionof hematological malignancies. (A) In a mouse model of chronic myelogenous leukemia (CML), BCR-ABL+
leukemic cells produce cytokines, including C-C motif ligand 3 (CCL3) and thrombopoietin (TPO), and mes-enchymal stem cells (MSCs) show skewed differentiation toward osteolineage cells. HSC maintenance factorssuch as SCF and CXCL12 are down-regulated in these remodeled MSCs, leading to impaired hematopoiesis.Imatinib treatment partially corrects the alteration of HSC maintenance factor expression in MSCs. (B) In anacute myelogenous leukemia (AML) mouse model transduced with mixed lineage leukemia AF9 (MLL-AF9)retrovirus, catecholaminergic fibers around arterioles are degenerated. Neuropathy is accompanied by expandedβ2-adrenergic receptor (AR)-expressingMSCs that are directed toward the osteoblastic cells. Similar to the CMLmouse model, the expression of HSC maintenance factors is decreased in MSCs and normal hematopoiesis iscompromised. (C) In a myeloproliferative neoplasm (MPN) mouse model harboring human Janus kinase 2(JAK2[V617F]) transgene, mutant hematopoietic stem and progenitor cells (HSPCs) secrete interleukin 1β (IL-1β) that damages sympathetic nervous system (SNS) fibers and Schwann cells. In contrast to AML mice,neuropathy results in apoptosis of β3-AR-expressing MSCs and a reduction of these cells.
M. Maryanovich et al.
12 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
HSC niche into a self-reinforcing malignantmicroenvironment at the expense of normalhematopoiesis. Another study showed that ex-pressions of cytokines, including CXCL12 andIL-1α, were also altered in the BM of CML pa-tients, some of which were partially correctedafter the complete cytogenetic remission (no de-tection of BCR-ABL+ cells by fluorescence insitu hybridization) was obtained by the treat-ment of BCR-ABL inhibitor imatinib mesylate(IM) (Fig. 4A) (Zhang et al. 2012).
In the case of AML, it has been recently re-ported that this disease disrupted catecholamin-ergic fibers around arterioles in a murine modelgenerated by retroviral infection of HSPCs withMLL-AF9 (Hanoun et al. 2014). In line with thisfinding, the treatment of these mice with 6-hydroxydopamine, which specifically damagescatecholaminergic neurons (Katayama et al.2006;Mendez-Ferrer et al. 2008), increased phe-notypic LSCs. Neuropathy was accompanied byactivation of the cell cycle in phenotypic MSCsand endothelial cells, leading to expansion ofthese cells. Similar to the finding in the CMLmouse model, these expanded MSCs were di-rected toward the osteoblastic lineage (Fig. 4B).In addition, the frequency of NG2+ periarterio-lar cells was reduced and the expression of HSCmaintenance factors such as CXCL12 and SCFwas decreased in MSCs, which underlies thecompromised hematopoiesis in AML. Consis-tent with previous studies showing that signal-ing through β2-AR and β3-AR plays a role inbone formation (Takeda et al. 2002; Elefteriouet al. 2005) and HSC niche maintenance (Men-dez-Ferrer et al. 2008), respectively, the expres-sion of β3-ARs was reduced in MSCs of AMLmice compared with healthy animals, whereasβ2-AR levels were equivalent between thesegroups. Furthermore, the β2-AR antagonist,but not the β3-AR antagonist, increased thenumber of LSCs in the BM and augmented col-ony-forming capacity of leukemic cells, leadingto shorten survival of AML mice. Although β2-ARs were also expressed in leukemic cells, trans-plantation experiments of wild-type leukemiccells into β2-AR-deficient or -sufficient mice re-vealed a higher BM infiltration of leukemic cellsin the former mice, suggesting a critical role for
β2-ARs expressed in the microenvironment.Conversely, the administration of β2-AR agonistresulted in a decrease of LSCs in the BM, pro-viding further evidence that neuropathy in theSNS is essential for LSC maintenance and dis-ease progression in AML through down-regula-tion of β2-AR signaling in the malignant niche.It is notable that β2-AR agonist was also shownto have a potential to enhance proliferation ofleukemic cells in a cell-autonomous manner,suggesting that the SNS neuropathy affectsLSCs and their niche differently. In the samemouse model, another study showed thatBmal1-deficient LSCs showed the compromisedpotential to evoke the disease in the wild-typemicroenvironment, indicating that the circadianrhythm in leukemic cells is essential for AMLdevelopment (Puram et al. 2016). Althoughthe precise mechanism underlying this pheno-type remains elusive, this study again raises thepossibility of the differential role of the SNS inthe maintenance of LSCs and their microenvi-ronment. In addition to involvement of the SNS,it was recently reported that vascular permeabil-ity in the BM is increased inAML and inhibitionof endothelial cell–derived nitric oxide is able tonormalize the vasculature and improve responseto Ara-C (Passaro et al. 2017).
Most patients with myeloproliferative neo-plasm (MPN) who do not carry the BCR-ABLfusion gene have an acquired mutation in Januskinase 2 (JAK2[V617F]) in HSCs, conferringconstitutive kinase activity to this molecule(Baxter et al. 2005; Kralovics et al. 2005), andmice harboring such mutated human JAK2transgenes show phenotypes that resembleMPN (Tiedt et al. 2008). With the use of thismodel, it was shown that the density of Schwanncells and SNS fibers in the BM were reduced inMPN, which was triggered by mutant HSPC-producing IL-1β (Fig. 4C) (Arranz et al. 2014).In contrast to the finding in AMLmice, neurop-athy in MPN led to apoptosis of MSCs and areduction of these cells. Neuroprotectivemanip-ulation with 4-MC treatment rescued Schwanncells and prevented neutrophilia (an increase ofneutrophils in the peripheral blood, which is oneof the hematological abnormalities in MPN).Similarly, the treatment with β3-AR agonist
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
led to recovery of the number of MSCs and adecrease of mutant HSCs that prevented MPNprogression, indicating that alteration of signal-ing through β3-ARs plays a role in the patho-genesis of MPN unlike AML. Collectively, he-matological malignancies induce alterations inHSC microenvironment in the BM, includingneuropathy, which are essential for disease pro-gression.
NEURONAL REGULATION OF IMMUNEFUNCTION
It was during the ancient Roman period thatdolor (pain) was originally depicted as a cardinalsign of inflammation, and this long-known factimplies the interaction of the immune systemwith the nervous system. Such interplay appearsto be ideal for immediate pathogen clearance,considering that the nervous system is able toreact rapidly to stimuli. Several immune celltypes express receptors for neurotransmitters,and these transmitters and immune mediatorsuse the same secondary signaling pathways suchas cAMP. Indeed, it was shown that inflamma-tory signals can activate sensory nerves duringan immune response, leading to the secretion ofseveral neuropeptides (Fig. 5A) (Deutschmanand Tracey 2014). For instance, some cytokinescan induce production of SP and CGRP, whichare released from sensory nerve endings andtransmits pain information to the CNS (De Fe-lipe et al. 1998; Schafers et al. 2003). These neu-ropeptides also act as a vasodilator (Brain et al.1985; Bossaller et al. 1992) and facilitate inflam-mation by enhancing blood flow, vascular leak-iness, and leukocyte trafficking to sites of infec-tion, which evokes calor (heat), rubor (redness),and tumor (swelling), the other classical signs ofinflammation. In line with these findings, theadministration of antagonists to these neuro-peptides and the severance of peripheral nerveswere shown to attenuate inflammation (Greenet al. 1993). On the contrary, a recent study hasreported that activation of the sensory sciaticnerve by electroacupuncture led to dampenedinflammation in an experimental sepsis modelthrough dopamine production in the adrenalglands (Torres-Rosas et al. 2014), suggesting
that sensory nerves can also function as ananti-inflammatory mechanism.
The facts that infection causes fever and thebody temperature is regulated primarily by thehypothalamus point to a link between CNS areaand the immune system. Previous studies haveshown that signals through afferent nerves andinflammatory mediators activate the HPA axis,leading to the secretion of glucocorticoids fromthe adrenal cortex (Sternberg 2006). Glucocor-ticoids act to suppress proliferation and differ-entiation ofmany types of immune cells, includ-ing macrophages and dendritic cells (Matyszaket al. 2000; Woltman et al. 2002). Furthermore,glucocorticoids tend to prevent trafficking ofthese cells from immune organs to sites of in-flammation through suppression of the expres-sion of cell-adhesionmolecules and chemokines(Fig. 5B) (Cronstein et al. 1992; Miyamasu et al.1998). Consistent with these findings that theHPA axis provides a negative feedback loop ofinflammation, deregulation of this axis is ob-served in patients with a wide range of autoim-mune diseases such as rheumatoid arthritis(RA) and systemic lupus erythematosus (Stern-berg 2006). In addition, glucocorticoid resis-tance attributable tomutations of glucocorticoidreceptors is also seen in these diseases (Derijket al. 2001; Lee et al. 2004). Conversely, an ele-vation of circulating glucocorticoids, which canresult from chronic stress, was found to be as-sociated with increased susceptibility to viral in-fections and decreased antibody production af-ter vaccination (Vedhara et al. 1999; Glaser andKiecolt-Glaser 2005). Collectively, the HPA axisfine-tunes immune homeostasis to avoid bothprolonged proinflammatory responses and ex-cessive immunosuppression.
Although the SNS innervates primary andsecondary lymphoid organs and provides sig-nals in inflammation, the description in the lit-erature is complex and it appears that this sys-tem has varying effects over the time course ofan immune response; the SNS is proinflamma-tory in the early stage of a mouse model ofarthritis, whereas adrenergic signals have ananti-inflammatory impact at the later stage(Fig. 5C) (Harle et al. 2005). Such observationsmight be attributable in part to the fact that NE
M. Maryanovich et al.
14 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
Pro-inflammatory
Neuropeptides(SP, CGRP, etc.)
Sensory nerve
A
C D
BHPA axis
SNS PNS
Pain
Activa
tion
Leukocytetrafficking
Vasodilation
Dopamine
Anti-inflammatory
Immune cellrecruitmentGlucocorticoids
Early stage of inflammation
Immuneorgan
Late stage of inflammation
Sensorynerve
-AR NE SNS
-AR
Afferent branchof PNS
Cytokines(IL-1, etc.)
Efferentbranch
Hypothalamus
Pituitary
Adrenalgland
Anti-inflammatory
Pro-inflammatory
Anti-inflammatory
Anti-inflammatory
nAChR7
Inflammation
Immune cells
Inflammation
Inflammation
Inflammation
Sympatheticganglion
Inflammation
NE
Activation
Nucleustractus solitarius
Proinflammatorycytokines
(TNF, etc.)Inflammatory
reflex
Immune cells(CD4+ T cell, macrophage)
ACh
Macrophage
NE
SNS
ACh
Figure 5.The nervous systemfine-tunes the inflammatory responses andmaintains the immune homeostasis. (A)Sensory nerves are activated by inflammatory signals, leading to the secretion of neuropeptides such as substanceP (SP) and calcitonin gene-related peptide (CGRP) from nerve endings. These substances induce proinflamma-tory responses through several processes, including enhancing blood flow and trafficking leukocytes to inflam-mation sites. Activated sensory nerves also transmit pain information to the central nervous system (CNS). Onthe other hand, sensory nerves can evoke anti-inflammatory responses through dopamine production in theadrenal glands. (B) Activation of hypothalamic–pituitary–adrenal (HPA) axis by inflammatory mediators leadsto the glucocorticoid secretion from the adrenal cortex. This hormone prevents trafficking of immune cells fromimmune organs to inflammation sites, acting as an anti-inflammatorymechanism. (C) The sympathetic nervoussystem (SNS) is proinflammatory in the early stage of inflammation, which might be attributable in part to thefact that norepinephrine (NE) promotes inflammation through α-adrenergic receptors (ARs) at low concentra-tions. In contrast, high concentrations of NE suppress inflammation through β-ARs, which could underlie theobservation that adrenergic signals have an anti-inflammatory impact at the later stage of inflammation. (D)Afferent branches of the parasympathetic nervous system (PNS) are activated by cytokines, including interleukin(IL)-1β from inflammation sites and signals are sent to the nucleus tractus solitarius (the parasympathetic brainregion). This, in turn, activates efferent branches of the PNS, referred to as “inflammatory reflex.” Signals throughthe nAChRα7 subunit of macrophages inhibit the production of proinflammatory cytokines such as tumornecrosis factor (TNF) in these cells, rendering the PNS an anti-inflammatory mechanism. The origin of acetyl-choline (ACh) that acts on macrophages is controversial and among the candidates are the efferent branches ofthe PNS and immune cells, including CD4+ T cells and macrophages that are triggered by NE from the SNS.
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 15
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
has proinflammatory effects through α-ARs atlow concentrations, whereas it has predomi-nantly anti-inflammatory effects through β-ARs at high concentrations (Pongratz andStraub 2013). These studies indicate that theSNS acts initially to amplify immune responsesto clear pathogens and, subsequently, it maycounterbalance to terminate inflammation. Inline with these findings, a clinical study suggest-ed that the level of β2-AR expression in mono-nuclear cells is lower in RA patients than inhealthy donors (Baerwald et al. 1992). In addi-tion, in active juvenile RA, leukocytes have alower cAMP response to β2-AR agonist (Kuiset al. 1996), indicating that AR expression pat-tern in immune cells as well as neuroimmuneresponse are altered in autoimmune diseases.Such SNS-mediated modulation of the immunesystem is influenced by the circadian rhythm(Scheiermann et al. 2012). This study showedthat leukocytes were recruited to tissues, includ-ing the BM, in a circadian rhythm-dependentmanner peaking at night, and conversely thenumber of leukocytes in the peripheral bloodincreased during the day as was observed forHSCs (Mendez-Ferrer et al. 2008). Surgical ab-lation of the SNS abolished such oscillation, em-phasizing the role of the SNS in the circadianrhythm-dependent leukocyte trafficking. Fur-thermore, mouse survival deteriorated whensepsis was induced in the night compared withthemorning, suggesting that a circadian rhythmin leukocyte recruitment can affect the outcomeof inflammation. Consistent with the fact thatrodents and humans display opposite circadianrhythms, the number of leukocytes in the circu-lation decreases during the night in humans(Haus and Smolensky 1999). It is possible thatthe leukocyte recruitment in tissues peaks dur-ing the day in humans, and this might explain inpart the mechanism underlying symptoms ofseveral chronic diseases that show circadian ex-acerbations (Scheiermann et al. 2013), such asjoint stiffness in RA patients, which is typicallyexperienced in the earlymorning (Cutolo 2012).
The PNS also senses inflammation andmodulates immune responses. Previous studieshave shown that IL-1β released from activatedimmune cells binds to its receptor on parasym-
pathetic ganglia and sends signals to afferentfibers of the vagus nerve and subsequently para-sympathetic brain regions (Fig. 5D) (Goehleret al. 2000). This leads to activation of efferentvagus nerve fibers, which induces release of AChfrom this branch. Although both nAChRs andmAChRs are found in immune cells, nAChRsspecifically mediate cholinergic signals. Activa-tion of the nAChRα7 subunit was shown to ex-hibit anti-inflammatory effects by inhibitingproinflammatory cytokine production (Borovi-kova et al. 2000; Wang et al. 2003) and by sup-pressing the expression of endothelial cell-adhe-sion molecules (Saeed et al. 2005), and thus thePNS counteracts the systemic inflammatory re-sponses. However, unlike the SNS, there is nodefinite evidence for parasympathetic innerva-tion of the immune system (Schafer et al. 1998;Nance and Sanders 2007). It is notable that theanti-inflammatory effect of vagus nerve stimu-lation requires a β2-AR on CD4+CD25− lym-phocytes (Vida et al. 2011), indicating that thisstimulation uses sympathetic nerve relay.
In summary, the interplay between the neu-ral system and the immune system allows thehost to enhance inflammatory responses topromptly clear pathogens as well as to terminateinflammation and return the host to a restingstate after elimination of pathogens. This fine-tuned mechanism plays a pivotal role in themaintenance of immune homeostasis with de-regulation of such a system being associatedwith autoimmune diseases.
CONCLUDING REMARKS
Although enormous progress has been made inelucidating neuronal regulation of bone andBM,there are several important unanswered ques-tions.For instance, it remainsunexploredwheth-er and how such regulation alters with aging. It isknown that bone remodeling and hematopoiesisundergo functional changes with aging, and theelderlyaremore likely to experience osteoporosisand hematological abnormalities. In the case ofhematopoiesis, previous studies have shown thatthe number of phenotypic HSCs increases ac-companied by disrupted cell cycle and biaseddifferentiation toward the myeloid lineage and
M. Maryanovich et al.
16 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
compromised BM reconstitution potential(Mendelson and Frenette 2014; Oh et al. 2014).In addition, it was reported that the HSCmicro-environment was also altered in old mice,including the decrease in the number of mesen-chymal progenitor cells located near the endos-teal surface (Siclari et al. 2013) and the decline ofvasculature (Kusumbe et al. 2016). However, it iscurrently unknown whether deregulation of thenervous system is involved in these phenotypes.
Another important point is whether target-ing the nervous system indeed becomes a newtherapy for hematological malignancies. As in-troduced in this review, there are two strategiesadopted so far to alter the neuronal regulation:(1) targeting ARs, and (2) modulating the circa-dian rhythm. Regarding the former approach,although β2-AR agonist is broadly used for thetreatment of bronchial asthma, its application toAML patients warrants careful consideration,given the potential of this drug to promote pro-liferation of leukemic cells in a cell-autonomousmanner (Hanoun et al. 2014). β3-AR agonistappears promising for the MPN treatment, butthe direct effect of this drug on leukemic cellswas not investigated. Fortunately, β3-AR agonistBRL37344 did not affect blood counts in wild-type mice (Arranz et al. 2014), and the effect ofthis agent on human HSCs also needs to becarefully monitored in a clinical trial. Regardingthe latter approach, there are currently no FDA-approved drugs that are able to directly targetBmal1. Ramelteon, which modulates circadianrhythm by binding to melatonin receptors onthe suprachiasmatic nucleus (a brain regioncontrolling circadian rhythm), is now used forthe treatment of insomnia (Brasure et al. 2015),and it will be intriguing to test the effect of suchdrugs on leukemia progression.
The finding that characteristics of BM stro-mal cells in the CML mouse model were notcompletely reverted by imatinib administration(Zhang et al. 2012) points out one critical issueabout currently performed therapies. Anti-leu-kemic agents, including molecular-targeteddrugs, have been developed to damage leukemiccells, and it is known that patients experiencerelapse after discontinuation of therapies inmost cases. There are many proposed explana-
tions for such unfavorable outcomes, and thefinding in the IM-treated CML mice impliesthe possibility that alterations in the microenvi-ronment that persist after therapies potentiallyinitiate and/or sustain leukemia. Together withevidence that stromal cell populations isolatedfrom individuals withmyeloidmalignancies canharbor genetic abnormalities that are differentfrom mutations in leukemic clones (Blau et al.2007), agents that target leukemic cells should becombined with approaches to modulate malig-nantmicroenvironments. Indeed, it was recentlyreported that a combination of IL-1 receptorantagonist with another BCR-ABL inhibitor ni-lotinib ameliorated the survival of CML micecompared with nilotinib treatment alone(Zhang et al. 2016). Combination with anti-leu-kemic cell drugs is also expected to mitigate theeffect of β2-AR agonist on proliferation ofleukemic cells. Another important question iswhether the strategy to target the nervous systemis expandable to other types of cancer. Giventhat growth of prostate cancer cells was inhibitedwhen these cells were orthotopically transplant-ed into β2-AR and β3-AR-deficient mice (Mag-non et al. 2013), modulation of activity of thenervous system may be a promising approachagainst a broad spectrum of cancers.
ACKNOWLEDGMENTS
Work in the Frenette laboratory is supportedby the National Institutes of Health (NIH)(DK056638, HL116340, HL097819) and theLeukemia and Lymphoma Society (LLS) Trans-lational Research Program. M.M. is a New YorkStem Cell Foundation (NYSCF) DruckenmillerFellow and was previously supported by theEMBO European Commission FP7 (Marie Cu-rie Actions; EMBOCOFUND2012, GA-2012-600394, ALTF 447-2014). S.T. is supported bythe Japan Society for the Promotion of Science(JSPS) Postdoctoral Fellowships for ResearchAbroad.
REFERENCES
AcarM, Kocherlakota KS,MurphyMM, Peyer JG, Oguro H,Inra CN, Jaiyeola C, Zhao Z, Luby-Phelps K,Morrison SJ.
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 17
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
2015. Deep imaging of bone marrow shows non-dividingstem cells are mainly perisinusoidal. Nature 526: 126–130.
Alenina N, Klempin F. 2015. The role of serotonin in adulthippocampal neurogenesis. Behav Brain Res 277: 49–57.
Arai F, Hirao A, OhmuraM, Sato H, Matsuoka S, Takubo K,Ito K, Koh GY, Suda T. 2004. Tie2/angiopoietin-1 signal-ing regulates hematopoietic stem cell quiescence in thebone marrow niche. Cell 118: 149–161.
Arranz L, Sanchez-Aguilera A, Martin-Perez D, Isern J,Langa X, Tzankov A, Lundberg P, Muntion S, TzengYS, Lai DM, et al. 2014. Neuropathy of haematopoieticstem cell niche is essential for myeloproliferative neo-plasms. Nature 512: 78–81.
Artico M, Bosco S, Cavallotti C, Agostinelli E, Giuliani-Pic-cari G, Sciorio S, Cocco L, Vitale M. 2002. Noradrenergicand cholinergic innervation of the bone marrow. Inter-national J Mol Med 10: 77–80.
Asada N, Katayama Y, Sato M, Minagawa K, Wakahashi K,Kawano H, Kawano Y, Sada A, Ikeda K, Matsui T, et al.2013. Matrix-embedded osteocytes regulate mobilizationof hematopoietic stem/progenitor cells. Cell Stem Cell 12:737–747.
Asada N, Kunisaki Y, Pierce H, Wang Z, Fernandez NF,Birbrair A, Maayan A, Frenette PS. 2017a. Differentialcytokine contributions of perivascular haematopoieticstem cell niches. Nat Cell Biol 19: 214–223.
AsadaN, Takeishi S, Frenette PS. 2017b. Complexity of bonemarrow hematopoietic stem cell niche. Int J Hematol 106:45–54.
Baerwald C, Graefe C, Muhl C, Von Wichert P, Krause A.1992. β2-adrenergic receptors on peripheral bloodmono-nuclear cells in patients with rheumatic diseases. Eur JClin Invest 22: 42–46.
BajayoA, BarA,DenesA, BacharM,KramV,Attar-NamdarM, Zallone A, Kovács KJ, Yirmiya R, Bab I. 2012. Skeletalparasympathetic innervation communicates central IL-1signals regulating bone mass accrual. Proc Natl Acad Sci109: 15455–15460.
Baldock PA, Sainsbury A, CouzensM, Enriquez RF, ThomasGP, Gardiner EM, Herzog H. 2002. Hypothalamic Y2receptors regulate bone formation. J Clin Invest 109:915–921.
Baldock PA, Sainsbury A, Allison S, Lin EJD, Couzens M,Boey D, Enriquez R, During M, Herzog H, Gardiner EM.2005. Hypothalamic control of bone formation: Distinctactions of leptin and Y2 receptor pathways. J Bone MinerRes 20: 1851–1857.
Baldock PA, Allison SJ, Lundberg P, Lee NJ, Slack K, LinEJD, Enriquez RF, McDonald MM, Zhang L, During MJ,et al. 2007. Novel role of Y1 receptors in the coordinatedregulation of bone and energy homeostasis. J Biol Chem282: 19092–19102.
Baldock PA, Lee NJ, Driessler F, Lin S, Allison S, Stehrer B,Lin EJD, Zhang L, Enriquez RF, Wong IPL, et al. 2009.Neuropeptide Y knockout mice reveal a central role ofNPY in the coordination of bone mass to body weight.PLos ONE 4: e8415.
Baron R, Rawadi G. 2007. Targeting the Wnt/β-cateninpathway to regulate bone formation in the adult skeleton.Endocrinology 148: 2635–2643.
Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N,Swanton S, Vassiliou GS, Bench AJ, Boyd EM, CurtinN, et al. 2005. Acquired mutation of the tyrosine kinaseJAK2 in humanmyeloproliferative disorders. Lancet 365:1054–1061.
Bellinger DL, Lorton D, Felten SY, Felten DL. 1992. Inner-vation of lymphoid organs and implications in develop-ment, aging, and autoimmunity. Int J Immunopharmacol14: 329–344.
BerendsenAD,OlsenBR. 2015. Bone development.Bone 80:14–18.
Bjerkvig R, Tysnes BB, Aboody KS, Najbauer J, Terzis AJ.2005. Opinion: The origin of the cancer stem cell: Currentcontroversies and new insights. Nat Rev Cancer 5: 899–904.
Bjurholm A, Kreicbergs A, Brodin E, Schultzberg M. 1988a.Substance P- and CGRP-immunoreactive nerves in bone.Peptides 9: 165–171.
BjurholmA, KreicbergsA, Terenius L, GoldsteinM, Schultz-berg M. 1988b. Neuropeptide Y-, tyrosine hydroxylase-and vasoactive intestinal polypeptide-immunoreactivenerves in bone and surrounding tissues. J Auton NervSyst 25: 119–125.
Blau O, Hofmann WK, Baldus CD, Thiel G, Serbent V,Schumann E, Thiel E, Blau IW. 2007. Chromosomal ab-errations in bonemarrowmesenchymal stroma cells frompatients with myelodysplastic syndrome and acute mye-loblastic leukemia. Exp Hematol 35: 221–229.
Bonnet N, Benhamou CL, Malaval L, Goncalves C, Vico L,Eder V, Pichon C, Courteix D. 2008. Low dose β-blockerprevents ovariectomy-induced bone loss in rats withoutaffecting heart functions. J Cell Physiol 217: 819–827.
Borovikova LV, Ivanova S, Zhang M, Yang H, Botchkina GI,Watkins LR, Wang H, Abumrad N, Eaton JW, Tracey KJ.2000. Vagus nerve stimulation attenuates the systemicinflammatory response to endotoxin. Nature 405: 458–462.
Bossaller C, Reither K, Hehlert-Friedrich C, Auch-SchwelkW, Graf K, Grafe M, Fleck E. 1992. In vivo measurementof endothelium-dependent vasodilation with substance Pin man. Herz 17: 284–290.
Boyden LM, Mao J, Belsky J, Mitzner L, Farhi A, MitnickMA, Wu D, Insogna K, Lifton RP. 2002. High bone den-sity due to a mutation in LDL-receptor–related protein 5.N Engl J Med 346: 1513–1521.
Brain SD, Williams TJ, Tippins JR, Morris HR, MacIntyre I.1985. Calcitonin gene-related peptide is a potent vasodi-lator. Nature 313: 54–56.
Brasure M, MacDonald R, Fuchs E, Olson CM, Carlyle M,Diem S, Koffel E, Khawaja IS, Ouellette J, Butler M, et al.2015. Management of insomnia disorder. Agency forHealthcare Research and Quality, Rockville, MD.
Broome CS, Miyan JA. 2000. Neuropeptide control of bonemarrow neutrophil production: A key axis for neuroim-munomodulation. Ann NY Acad Sci 917: 424–434.
Calvi LM, Adams GB,Weibrecht KW,Weber JM, OlsonDP,Knight MC, Martin RP, Schipani E, Divieti P, BringhurstFR, et al. 2003. Osteoblastic cells regulate the haemato-poietic stem cell niche. Nature 425: 841–846.
Calvo W. 1968. The innervation of the bone marrow inlaboratory animals. Am J Anat 123: 315–328.
M. Maryanovich et al.
18 Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
Canalis E, Delany AM. 2002. Mechanisms of glucocorticoidaction in bone. Ann NY Acad Sci 966: 73–81.
Chow A, Lucas D, Hidalgo A, Mendez-Ferrer S, HashimotoD, Scheiermann C, Battista M, Leboeuf M, Prophete C,van Rooijen N, et al. 2011. Bone marrow CD169+ macro-phages promote the retention of hematopoietic stem andprogenitor cells in themesenchymal stem cell niche. J ExpMed 208: 261–271.
Christopher MJ, Link DC. 2008. Granulocyte colony-stim-ulating factor induces osteoblast apoptosis and inhibitsosteoblast differentiation. J Bone Miner Res 23: 1765–1774.
Clevers H. 2011. The cancer stem cell: Premises, promisesand challenges. Nat Med 17: 313–319.
Cordeiro Gomes A, Hara T, Lim VY, Herndler-BrandstetterD, Nevius E, Sugiyama T, Tani-ichi S, Schlenner S, RichieE, Rodewald HR, et al. 2016. Hematopoietic stem cellniches produce lineage-instructive signals to control mul-tipotent progenitor differentiation. Immunity 45: 1219–1231.
Cornish J, CallonKE, BavaU, Kamona SA, CooperGJS, ReidIR. 2001. Effects of calcitonin, amylin, and calcitoningene-related peptide on osteoclast development. Bone29: 162–168.
Cornish J, Callon K, Bava U, Lin C, Naot D, Hill B, Grey A,Broom N, Myers D, Nicholson G, et al. 2002. Leptin di-rectly regulates bone cell function in vitro and reducesbone fragility in vivo. J Endocrinol 175: 405–415.
Cronstein BN, Kimmel SC, Levin RI, Martiniuk F, Weiss-mann G. 1992. A mechanism for the antiinflammatoryeffects of corticosteroids: The glucocorticoid receptor reg-ulates leukocyte adhesion to endothelial cells and expres-sion of endothelial-leukocyte adhesion molecule 1 andintercellular adhesion molecule 1. Proc Natl Acad Sci89: 9991–9995.
Cutolo M. 2012. Chronobiology and the treatment of rheu-matoid arthritis. Curr Opin Rheumatol 24: 312–318.
De Felipe C, Herrero JF, O’Brien JA, Palmer JA, Doyle CA,Smith AJ, Laird JM, Belmonte C, Cervero F, Hunt SP.1998. Altered nociception, analgesia and aggression inmice lacking the receptor for substance P. Nature 392:394–397.
de Klein A, van Kessel AG, Grosveld G, Bartram CR, Hage-meijer A, Bootsma D, Spurr NK, HeisterkampN, GroffenJ, Stephenson JR. 1982. A cellular oncogene is translocat-ed to the Philadelphia chromosome in chronicmyelocyticleukaemia. Nature 300: 765–767.
Derijk RH, SchaafMJ, Turner G,DatsonNA,Vreugdenhil E,Cidlowski J, de Kloet ER, Emery P, Sternberg EM,Detera-Wadleigh SD. 2001. A human glucocorticoid receptorgene variant that increases the stability of the glucocorti-coid receptor β-isoform mRNA is associated with rheu-matoid arthritis. J Rheumatol 28: 2383–2388.
Deutschman CS, Tracey KJ. 2014. Sepsis: Current dogmaand new perspectives. Immunity 40: 463–475.
Dimitri P, Rosen C. 2017. The central nervous system andbone metabolism: An evolving story. Calcif Tissue Int100: 476–485.
Ding L, Morrison SJ. 2013. Haematopoietic stem cells andearly lymphoid progenitors occupy distinct bone marrowniches. Nature 495: 231–235.
Ding Y, Arai M, Kondo H, Togari A. 2010. Effects of capsa-icin-induced sensory denervation on bone metabolism inadult rats. Bone 46: 1591–1596.
Ding L, Saunders TL, Enikolopov G, Morrison SJ. 2012.Endothelial and perivascular cells maintain haemato-poietic stem cells. Nature 481: 457–462.
Ducy P, Amling M, Takeda S, Priemel M, Schilling AF, BeilFT, Shen J, Vinson C, Rueger JM, Karsenty G. 2000. Lep-tin inhibits bone formation through a hypothalamic relay:A central control of bone mass. Cell 100: 197–207.
Duhrsen U, Hossfeld DK. 1996. Stromal abnormalities inneoplastic bone marrow diseases. Ann Hematol 73: 53–70.
Elefteriou F, Ahn JD, Takeda S, Starbuck M, Yang X, Liu X,Kondo H, Richards WG, Bannon TW, Noda M, et al.2005. Leptin regulation of bone resorption by the sympa-thetic nervous system and CART. Nature 434: 514–520.
Elefteriou F, Campbell P, Ma Y. 2014. Control of bone re-modeling by the peripheral sympathetic nervous system.Calcif Tissue Int 94: 140–151.
Entschladen F, Drell TL 4th, Lang K, Joseph J, Zaenker KS.2004. Tumour-cell migration, invasion, and metastasis:Navigation by neurotransmitters. Lancet Oncol 5: 254–258.
Erickson JC, Hollopeter G, Palmiter RD. 1996. Attenuationof the obesity syndrome of ob/ob mice by the loss ofneuropeptide Y. Science 274: 1704.
Feuer AJ, Demmer RT, Thai A, Vogiatzi MG. 2015. Use ofselective serotonin reuptake inhibitors and bone mass inadolescents: An NHANES study. Bone 78: 28–33.
Frenette PSWL. 2000. Sulfated glycans induce rapid hema-topoietic progenitor cell mobilization: Evidence for selec-tin-dependent and independent mechanisms. Blood 96:2460–2468.
Frenette PS, Pinho S, Lucas D, Scheiermann C. 2013. Mes-enchymal stem cell: Keystone of the hematopoietic stemcell niche and a stepping-stone for regenerative medicine.Ann Rev Immunol 31: 285–316.
Friedman JM, Halaas JL. 1998. Leptin and the regulation ofbody weight in mammals. Nature 395: 763–770.
Glaser R, Kiecolt-Glaser JK. 2005. Stress-induced immunedysfunction: Implications for health.Nat Rev Immunol 5:243–251.
Goehler LE, Gaykema RP, Hansen MK, Anderson K, MaierSF, Watkins LR. 2000. Vagal immune-to-brain commu-nication: Avisceral chemosensory pathway.AutonNeuro-sci 85: 49–59.
Gong Y, Slee RB, Fukai N, Rawadi G, Roman-Roman S,Reginato AM, Wang H, Cundy T, Glorieux FH, Lev D,et al. 2001. LDL receptor-related protein 5 (LRP5) affectsbone accrual and eye development. Cell 107: 513–523.
Gratwohl A, Baldomero H, Passweg J. 2013. Hematopoieticstem cell transplantation activity in Europe. Curr OpinHematol 20: 485–493.
Green PG, Luo J, Heller PH, Levine JD. 1993. Further sub-stantiation of a significant role for the sympathetic ner-vous system in inflammation. Neuroscience 55: 1037–1043.
Greenbaum A, Hsu YM, Day RB, Schuettpelz LG, Christo-pher MJ, Borgerding JN, Nagasawa T, Link DC. 2013.CXCL12 in early mesenchymal progenitors is required
Neural Regulation of Bone and Bone Marrow
Cite this article as Cold Spring Harb Perspect Med 2018;8:a031344 19
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 28, 2021 - Published by Cold Spring Harbor Laboratory Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
for haematopoietic stem-cell maintenance. Nature 495:227–230.
Halaas JL, Gajiwala KS, Maffei M, Cohen SL, Chait BT,Rabinowitz D, Lallone RL, Burley SK, Friedman JM.1995. Weight-reducing effects of the plasma protein en-coded by the obese gene. Science 269: 543.
Hanoun M, Zhang D, Mizoguchi T, Pinho S, Pierce H, Ku-nisaki Y, Lacombe J, Armstrong SA, Duhrsen U, FrenettePS. 2014. Acute myelogenous leukemia-induced sympa-thetic neuropathy promotes malignancy in an altered he-matopoietic stem cell niche. Cell Stem Cell 15: 365–375.
Hanoun M, Maryanovich M, Arnal-Estapé A, Frenette PS.2015. Neural regulation of hematopoiesis, inflammation,and cancer. Neuron 86: 360–373.
Harle P,MobiusD, Carr DJ, Scholmerich J, Straub RH. 2005.An opposing time-dependent immune-modulating effectof the sympathetic nervous system conferred by alteringthe cytokine profile in the local lymphnodes and spleen ofmice with type II collagen-induced arthritis. ArthritisRheum 52: 1305–1313.
Hattori K, Heissig B, Tashiro K, Honjo T, Tateno M, ShiehJH, Hackett NR, QuitorianoMS, Crystal RG, Rafii S, et al.2001. Plasma elevation of stromal cell-derived factor-1induces mobilization of mature and immature hemato-poietic progenitor and stem cells. Blood 97: 3354–3360.
Haus E, Smolensky MH. 1999. Biologic rhythms in the im-mune system. Chronobiol Int 16: 581–622.
Hill EL, Elde R. 1991. Distribution of CGRP-, VIP-, DβH-,SP-, and NPY-immunoreactive nerves in the periosteumof the rat. Cell Tissue Res 264: 469–480.
Horsnell H, Baldock PA. 2016. Osteoblastic actions of theneuropeptide Y system to regulate bone and energy ho-meostasis. Current Osteoporosis Rep 14: 26–31.
Ishikawa F, Yoshida S, Saito Y, Hijikata A, Kitamura H,Tanaka S, Nakamura R, Tanaka T, Tomiyama H, SaitoN, et al. 2007. Chemotherapy-resistant humanAML stemcells home to and engraft within the bone-marrow en-dosteal region. Nat Biotech 25: 1315–1321.
Ishizuka K, Hirukawa K, Nakamura H, Togari A. 2005. In-hibitory effect of CGRPon osteoclast formation bymousebone marrow cells treated with isoproterenol. NeurosciLett 379: 47–51.
Itkin T, Gur-Cohen S, Spencer JA, Schajnovitz A, RamasamySK, Kusumbe AP, Ledergor G, Jung Y,Milo I, PoulosMG,et al. 2016. Distinct bone marrow blood vessels differen-tially regulate haematopoiesis. Nature 532: 323–328.
JungWC, Levesque JP, RuitenbergMJ. 2017. It takes nerve tofight back: The significance of neural innervation of thebonemarrowand spleen for immune function. SeminCellDev Biol 61: 60–70.
Kajimura D, Hinoi E, Ferron M, Kode A, Riley KJ, Zhou B,Guo XE, Karsenty G. 2011. Genetic determination of thecellular basis of the sympathetic regulation of bone massaccrual. J Exp Med 208: 841.
Katayama Y, Battista M, Kao WM, Hidalgo A, Peired AJ,Thomas SA, Frenette PS. 2006. Signals from the sympa-thetic nervous system regulate hematopoietic stem cellegress from bone marrow. Cell 124: 407–421.
Kauschke V, Kneffel M, Floel W, Hartmann S, KampschulteM, Dürselen L, Ignatius A, Schnettler R, Heiss C, Lips KS.
2015. Bone status of acetylcholinesterase-knockout mice.Int Immunopharmacol 29: 222–230.
Kiel MJ, Yilmaz ÖH, Iwashita T, Yilmaz OH, Terhorst C,Morrison SJ. 2005. SLAM family receptors distinguishhematopoietic stem and progenitor cells and reveal endo-thelial niches for stem cells. Cell 121: 1109–1121.
Kode A, Obri A, Paone R, Kousteni S, Ducy P, Karsenty G.2014. Lrp5 regulation of bone mass and serotonin syn-thesis in the gut. Nat Med 20: 1228–1229.
Kralovics R, Passamonti F, Buser AS, Teo SS, Tiedt R, Pass-weg JR, Tichelli A, CazzolaM, Skoda RC. 2005. A gain-of-function mutation of JAK2 in myeloproliferative disor-ders. N Engl J Med 352: 1779–1790.
Kreso A, Dick JE. 2014. Evolution of the cancer stem cellmodel. Cell Stem Cell 14: 275–291.
Kuis W, de Jong-de Vos van Steenwijk C, Sinnema G, Ka-velaars A, Prakken B, Helders PJ, Heijnen CJ. 1996. Theautonomic nervous system and the immune system injuvenile rheumatoid arthritis. Brain Behav Immun 10:387–398.
Kunisaki Y, Bruns I, Scheiermann C, Ahmed J, Pinho S,Zhang D, Mizoguchi T, Wei Q, Lucas D, Ito K, et al.2013. Arteriolar niches maintain haematopoietic stemcell quiescence. Nature 502: 637–643.
Kuo LE, Kitlinska JB, Tilan JU, Li L, Baker SB, JohnsonMD,Lee EW, Burnett MS, Fricke ST, Kvetnansky R, et al. 2007.Neuropeptide Y acts directly in the periphery on fat tissueand mediates stress-induced obesity and metabolic syn-drome. Nat Med 13: 803–811.
Kusumbe AP, Ramasamy SK, Itkin T, MäeMA, Langen UH,Betsholtz C, Lapidot T, Adams RH. 2016. Age-dependentmodulation of vascular niches for haematopoietic stemcells. Nature 532: 380–384.
Lee Y