Embed Size (px)
Citation preview

REVIEW ARTICLE
Neuro-ophthalmologic manifestations of systemic lupuserythematosus: a systematic review
Bik Ling MAN, Chi Chiu MOK and Yat Pang FU
Department of Medicine, Tuen Mun Hospital, Hong Kong, China
AbstractHerein we summarize the clinical presentation, treatment and outcome of neuro-ophthalmologic manifesta-
tions in patients with systemic lupus erythematosus (SLE). We performed a systematic review of the neuro-oph-
thalmologic manifestations of SLE reported in the English literature from 1970 to 2010 by a Medline search.
The prevalence of neuro-ophthalmologic manifestations is 3.6% in adult and 1.6% in childhood SLE patients.
Neuro-ophthalmologic manifestations of SLE are highly variable, with the commonest presentation being optic
neuritis, followed by myasthenia gravis, visual field defects and pseudotumor cerebri. The underlying pathology
was thought to be either SLE activity or its vascular complications. Most neuro-ophthalmologic manifestations
of SLE are responsive to high-dose glucocorticoids. Anticoagulation is indicated when there is concomitant anti-
phospholipid syndrome. SLE-related neuromyelitis optica is often refractory to treatment and 92% of patients
require multiple immunosuppressive protocols. Neuro-ophthalmologic manifestations of SLE are uncommon
but heterogeneous. The prognosis of neuro-ophthalmologic manifestations in SLE is generally good because of
their rapid response to glucocorticoids. Relapses of these manifestations may be reduced by the use of mainte-
nance immunosuppression. Cyclophosphamide, azathioprine, plasmapheresis, intravenous immunoglobulin
and rituximab can be considered in glucocorticoid-dependent or refractory cases. Anticoagulation is indicated
when there is concomitant antiphospholipid syndrome.
Key words: lupus,myasthenia, neuromyelitis optica, neuro-ophthalmologic, optic neuritis, pseudotumor cerebri.
INTRODUCTION
Systemic lupus erythematosus (SLE) is a chronic multi-
systemic autoimmune disease that may affect any organ
of the body. Neurological manifestations are fairly com-
mon and the American College of Rheumatology
(ACR) has defined 19 neuropsychiatric syndromes that
may occur in patients with SLE.1 Neuro-ophthalmo-
logic manifestations refer to those that arise from pri-
mary lesions in the ocular muscles, neuromuscular
junction, optic nerves and visual pathways, and the cen-
tral nervous system, resulting in ptosis, visual
symptoms or visual field defects. Neuro-ophthalmo-
logic manifestations in SLE are heterogeneous and up
to the present, there are still no consensus criteria for
their classification. Neuro-ophthalmologic manifesta-
tions of SLE are related to either SLE activity or its vas-
cular complications. The underlying pathogenetic
mechanisms include vasculitis or vascular thrombosis,
autoantibodies directing against neural tissues such as
the neuromuscular junction, inflammation or ischemia
of the optic nerve, vasogenic edema of the brain in the
territory of the posterior cerebral circulation and intra-
cranial hypertension.
Only a small number of SLE patients with neuro-oph-
thalmologic manifestations have been reported in the
literature. Although these manifestations are uncom-
monly encountered in SLE, they are important causes of
disability and impairment of quality of life. In this arti-
cle, we summarize the prevalence, clinical presentation,
Correspondence: Dr Chi Chiu Mok, Department of Medicine,Tuen Mun Hospital, Tsing Chung Koon Road, New Territories,Hong Kong, China.Email: [email protected]
© 2014 Asia Pacific League of Associations for Rheumatology and Wiley Publishing Asia Pty Ltd
International Journal of Rheumatic Diseases 2014; 17: 494–501

treatment and outcome of SLE patients with neuro-oph-
thalmologic manifestations by performing a Medline
search.
METHODS
We performed a systematic review of neuro-ophthalmo-
logic manifestations in SLE by performing a Medline
search for publications from January 1970 to March
2010 using the keywords ‘lupus’, ‘neuro-ophthalmol-
ogy’, ‘neuro-psychiatric’, ‘optic neuritis’, ‘optic neuropa-
thy’, ‘neuromyelitis optica’, ‘ischemic optic neuropathy’,
‘eye movement disorders’, ‘orbital pseudotumor’,
‘pseudotumor cerebri’, ‘myasthenia’, ‘intracranial
hypertension’ and ‘visual field defect’. Searches were
limited to human trials and articles written in English.
RESULTSPrevalence of neuro-ophthalmologicmanifestations in SLETable 1 summarizes the prevalence of neuro-ophthal-
mologic manifestations in SLE patients reported in 12
studies.2–13 There are eight adult3,5,6,8,9,11–13 and four
childhood SLE2,4,7,10 series, with a total number of
1433 patients (1067 adult and 366 pediatric patients).
The mean age at the onset of neuro-ophthalmologic
manifestations was 34.6 � 6.8 years in adult patients
and 12.6 � 1.0 years in childhood patients. The
reported prevalence of neuro-ophthalmologic manifes-
tations in childhood SLE2,4,7,10 was between 0.5% and
4%, whereas in adult-onset SLE patients,3,5,6,8,9,11–13
the prevalence figures ranged from 1% to 23%. A pool-
Table 1 Prevalence of neuro-ophthalmologic manifestations in SLE
Author, year Patient
Characteristics
No. of
patients
Ethnicity
(%)
Mean age
(years)
Prevalence
(%)
Manifestations
(no. of patients)
Petri M, 20088 Adult 111 C (55)
B (15)
H (21)
A (5)
33 3 (3) CN (2), MG (1)
Hershko AY, 20089 Adult 651 A 24 10 (2) PTC (10)
Hanly JG, 200811 Adult 572 C (52)
B (13)
H (16)
A (16)
35 5 (1) CN (5)
Yu HH, 20064 Childhood 185 A 13.5 1 (0.5) CN (1)
Harel L, 200610 Childhood 106 C (20)
B (8.5)
H (26)
A (37)
M (8.5)
12.3 4 (4) CN (1), PTC (3)
Al-mayouf SM, 20037 Childhood 52 A 11.3 14 (27) ON (3), VFD (11)
Brey RL, 200213(13) Adult 128 C (30)
B (8)
H (56)
43 2 (2) CN (2)
Sibbitt WL, 20022 Childhood 75 C (27)
B (8)
H (61)
A (4)
13.3 1 (1) CN (1)
Ainiala H, 20016 Adult 46 C 45 4 (9) CN (3), MG (1)
Yap EY, 19985 Adult 70 A 32.9 2 (3) ON (2)
Keane JR, 19953 Adult 113 NS 33.5 26 (23) Ptosis (8), PTC (2)
CN(4), spontaneous
eye movements (12)
Feinglass EJ, 197612 Adult 140 C (52)
B (48)
30 22 (16) CN (16)
Scotoma (4), PTC (2)
A, Asian; C, Caucasian; B, Black; H, Hispanic; M, mixed; NS, not specified; MG, myasthenia gravis; CN, cranial neuropathy; ON, optic neuropathy;PTC, pseudotumor cerebri; VFD, visual field defects.
International Journal of Rheumatic Diseases 2014; 17: 494–501 495
SLE neuro-ophthalmologic manifestations

ing of these figures reveals that the prevalence of neuro-
ophthalmologic manifestations is 3.6% and 1.6% in
adult and childhood SLE patients, respectively.
Clinical presentation and treatment outcomeof neuro-opthalmologic disease in SLEOptic neuropathy
The commonest and most well-known neuro-ophthal-
mologic manifestation of SLE is optic neuropathy. This
may present as isolated optic neuritis, neuromyelitis op-
tica (NMO) (optic neuritis together with myelitis) or
ischemic optic neuropathy.
Isolated optic neuritis occurs in about 1% of SLE
patients. It is typically unilateral and may present as ret-
robulbar ischemic optic neuritis or papillitis. The most
common presentations are decreased visual acuity, orbi-
tal pain and central scotoma.14 SLE-optic neuritis is not
due to a primary inflammatory demyelinating process
but rather an ischemic process that can cause subse-
quent demyelination and axonal necrosis. The degree
of axonal loss correlates to visual outcome. The optic
neuritis responds dramatically to corticosteroid treat-
ment.15 Early diagnosis and prompt treatment with
high-dose corticosteroids is associated with better visual
outcomes.
In patients with NMO, aquaporin-4 antibody could
be detected in 60% of cases, and higher titers of anti-
aquaporin-4 were associated with poorer prognosis,
such as complete blindness and more extensive cerebral
and spinal cord lesions on magnetic resonance imaging
(MRI). Florid antibody-mediated inflammatory
response could be demonstrated in NMO lesions.16
Neuromyelitis optica is well known for its resistance
to treatment. Table 2 summarizes the outcomes of
NMO in 12 patients with SLE.17–28 All except one
patient were treated with a combination of immuno-
suppressive agents. One patient had poor response after
multiple immunosuppressants and was relapse-free
after use of immunoablative cyclophosphamide proto-
col without stem cell rescue.20
The coexistence of SLE and multiple sclerosis (MS)
has rarely been described29 and the activity of lupus
remained quiescent in all patients while on standard
immunomodulatory MS therapy.29
Ischemic optic neuropathy is rare in SLE. The cause is
thought to be due to vasculitis of the short posterior cil-
iary artery with resultant hypoperfusion and infarction
of the anterior optic nerve.30 Ischemic optic neuropathy
usually responds to glucocorticoid treatment. Patients
with concomitant antiphospholipid syndrome should
be treated with anticoagulation.
Myasthenia gravis
Myasthenia gravis (MG) has long been reported in asso-
ciation with SLE. Most patients presented as generalized
MG with ptosis, ophthalmoplegia and proximal muscle
weakness. In some patients, SLE developed after thy-
mectomy for MG.31 The thymus is important in main-
taining tolerance to self-antigens by clonal depletion of
self-reactive T cells32 or rendering the self-reactive T cells
anergic.33 It was postulated that thymectomy leads to
loss of central tolerance and over-production of autoan-
tibodies, which triggers the onset of SLE in susceptible
individuals.31
Most SLE patients with concomitant MG responded
well to pyridostigmine, glucocorticoid and thymectomy
treatment. Some patients required additional immuno-
suppressive agents for disease control such as cyclo-
phosphamide, azathioprine, plasmapheresis,
immunoglobulin, mycophenolate mofetil, tacrolimus
and cyclosporin A.
Visual field defects
Optic chiasmal and retro-chiasmal lesions may cause
visual field defects. Symptoms included homonymous
hemianopia due to occipital infarcts and posterior
reversible encephalopathy syndrome (PRES). SLE
patients are prone to arterial thromboembolism that
includes cerebrovascular accidents. This is due to the
increased prevalence of traditional vascular risk factors
and lupus-specific factors such as the antiphospholipid
antibodies.34
Posterior reversible encephalopathy syndrome is a
reversible neurological condition characterized by
headache, nausea, vomiting, altered mental status,
visual disturbances, and seizures. MRI shows the typi-
cal features of vasogenic edema at the parieto-occipital
areas in the ‘watershed’ areas of the posterior circula-
tion of the brain which reduces after subsidence of the
underlying causes.35 PRES has been associated with a
variety of clinical conditions such as malignant hyper-
tension in SLE patients due to active renal disease. The
pathophysiology of PRES is elevation of arterial pres-
sure that exceeds the limit of cerebral auto-regulation
which leads to hydrostatic brain edema or brain ische-
mia.36 In SLE patients with concomitant active disease,
increase in inflammatory cytokine production may fur-
ther up-regulate cell adhesion molecules, leading to
chemotaxis of leukocytes and cerebral microcirculatory
dysfunction.36 These further aggravate the leakage of
cerebral circulation and cause PRES. The posterior cir-
culation is more involved in PRES because of a relative
lack of sympathetic innervation of the arterioles.37
496 International Journal of Rheumatic Diseases 2014; 17: 494–501
B. L. Man et al.

Posterior reversible encephalopathy syndrome is a
reversible condition and management mainly focuses
on the control of the underlying conditions, such as
treatment of hypertension. Supportive care for other
complications such as control of seizures is also
needed.35 PRES is also related to medications used for
the treatment of SLE. A possible link between PRES and
a number of offending drugs, such as cyclosporine,
mycophenolate mofetil, tacrolimus, intravenous immu-
noglobulin and rituximab have been suggested.
Pseudotumor cerebri (PTC) is a complex syndrome
consisting of: (i) elevated intracranial pressure over
200 mmH2O; (ii) normal cerbrospinal fluid (CSF)
compositions; (iii) papilloedema with occasional sixth
nerve paresis; and (iv) absence of a space-occupying
lesion in the brain or ventricular enlargement.38
Headache and papillodema (Fig. 1) are the most
common presentations. PTC is associated with anti-
phospholipid antibodies and dural sinus thrombosis.
It was suggested that absorptive failure of the CSF,
and thrombosis of the venous sinuses, may be
involved in the pathogenesis of PTC in SLE.39 The
anti-phospholipid antibodies are associated with cere-
bral venous thrombosis or stenosis which causes dis-
ruption of the blood–brain barrier and thus decreases
CSF adsorption.
Table 2 Treatment and outcome of neuromyelitis optica in SLE
Author, year No. of
patients
Treatment Outcome
Karim S, 200918 1 Steroid
Plasmapheresis
Partial reponse
Mottaghi P, 200921 1 Steroid
Plasmapheresis
Cyclophosphamide
Full response
Nasir S, 200923 1 Steroid
Cyclophosphamide
Rituximab
Full response with relapses
Mok CC, 200820 1 Steroid
Immunoglobulin
Mycophenolate Mofetil
Tacrolimus
Cyclophosphamide
No response to multiple
immunosuppressants and
finally responded to
immunoablative cyclophosphamide
Birubaum J, 200828 1 Steroid
Cyclophosphamide
Rituximab
Partial response with relapses
Jacobi C, 200624 1 Steroid
Immunoglobulin
Cyclophosphamide
Partial response with relapses
Hagiwara N, 200525 1 Steroid Full response
Ferrerira S, 200526 1 Steroid
Cyclophosphamide
Plasmapheresis
Immunoglobulin
Partial response with relapses
Gibbs AN, 200217 1 Steroid
Cyclophosphamide
No response
Margaux J, 199922 1 Steroid
Anticoagulation
Azathioprine
Full response
Bonnet F, 199927 1 Steroid
Plasmapheresis
Cyclophosphamide
Partial response with relapses
Cordeiro MF, 199419 1 Steroid
Cyclophosphamide
Warfarin
Partial response
International Journal of Rheumatic Diseases 2014; 17: 494–501 497
SLE neuro-ophthalmologic manifestations

Most patients need glucocorticoid treatment as con-
comitant active SLE was almost universally present. This
contrasts with acetazolamide as the first-line treatment
of PTC not related to SLE. Ventriculoperitoneal shunt-
ing may be indicated for sight-threatening papilloedem-
a. Relapse of PTC and persistent papilloedema were
reported in some patients.9
DISCUSSION
Neuro-ophthalmologic manifestations of SLE are
uncommon but heterogeneous and the diagnostic para-
digm is shown in Figure 2. Optic neuropathy is the
most common neuro-ophthalmologic presentation in
SLE. Most patients respond completely to glucocorti-
coid treatment. Optic atrophy may be found in patients
with severe or recurrent optic neuritis (Fig. 1). The MRI
orbit in optic neuritis may show contrast enhancement
and swelling of optic nerves. New sequences such as dif-
fusion tensor imaging (DTI) can quantitatively assess
lesions to reveal alterations in tissue structure which
may predict visual outcomes in patients with optic neu-
ritis.40 Another modality is optical coherence tomogra-
phy, which can be used to measure the thickness of the
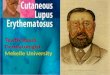
(a) (b)
Figure 1 Fundi photos. (a) Optic atro-phy in neuromyelitis optica. (b) Papille-dema in pseudotumor cerebri (Courtesyof Dr. Andy Cheng, the Hong Kong EyeHospital, Hong Kong).
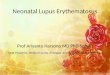
Neuro-ophthalmologic manifestations in SLE
Afferent pathwaySymptoms: blurring of vision, visual field defects
Efferent PathwaySymptoms: diplopia, ptosis
Optic neuropathy
Papilledema Hemianopia
Isolated optic neuritis
NMO
INO
MS
Cranial neuropathy
Fatigability
MG
PRES
StrokePTC Vasculitis
Findings
Etiology
Investigations: fundi examination, OCT, MRI brain and orbit, lumbar puncture,VEP, NMO antibody
Investigations: autoimmune markers, anti-AchR, Tensilon test, MRI brain, LP, SFEMG
Figure 2 Diagnostic paradigm of neuro-ophthalmologic manifestations in SLE.OCT, Optical Coherence Tomography;Anti-AchR, anti-acetylcholine receptorantibody; VEP, visual evoked potential;NMO, Neuromyelitis Optica; INO,Ischemic optic neuropathy; MS, multiplesclerosis; PTC, pseudotumor cerebri;PRES, Posterior reversible leukoencepha-lopathy; MG, Myasthenia Gravis;SFEMG, single fiber electromyography.
498 International Journal of Rheumatic Diseases 2014; 17: 494–501
B. L. Man et al.

retinal peripapillary nerve fiber layer which may be
reduced in optic neuritis, and this reduction correlates
well with findings from testing visual acuity and visual
field and with the disability scores.41 Visual evoked
potentials are prolonged in optic neuritis.42
Neuromyelitis optica is a less common but more seri-
ous neuro-ophthalmologic manifestations of SLE.
NMO presents as optic neuritis and myelitis. MRI in
NMO typically shows longitudinal and confluent spinal
cord lesions across more than three vertebral segments.
MRI brain abnormalities are present in with 60% of
NMO cases and are quite distinct from MS lesions.43
The cerebral lesions are usually linear, as opposed to
oval lesions with Dawson finger configuration in MS
(Fig. 3). Special techniques such as diffusion tensor and
magnetization transfer imaging may show abnormal
findings due to axonal degeneration secondary to
lesions in the spinal cord and optic nerves.40 Oligoclo-
nal bands in CSF are negative in most NMO patients.
NMO is associated with the aquaporin-4 antibody
(NMO-IgG). NMO carries a poor prognosis because it
is often refractory to treatment. Our analysis shows
most patients required a combination of multiple
immunosuppressive agents for treatment but despite
this, relapse was usual. Prevention of relapse with long-
term immunosuppressive drugs that include low-dose
glucocorticoids, azathioprine, cyclophosphamide and
rituximab, remains the cornerstone of therapy in NMO.
Systemic lupus erythematosus and MG are part of the
same autoimmune spectrum of diseases and coexistence
of the two diseases is commonly encountered. Some
MG patients developed SLE after thymectomy. When
thymectomy is considered for patients with MG, one
should be alerted to the possibility of onset of SLE. SLE
patients with ocular or generalized muscular weakness
and worsening symptoms during the day should be
referred to the neurologist for work-up of MG.
The prognosis of neuro-ophthalmologic manifesta-
tions in SLE appears to be good because of their rapid
response to glucocorticoid treatment. Relapses may be
reduced by the use of maintenance immunosuppres-
sion. Alkylating agents, azathioprine, plamapheresis,
immunoglobulin and rituximab can be considered in
glucocorticoid-dependent or refractory cases. Patients
with antiphospholipid antibody syndrome should be
treated with anticoagulation.
CONCLUSIONS
Neuro-ophthalmologic manifestations of SLE are unu-
sual but heterogeneous. The pathophysiology is prob-
ably multifactorial, including occlusive vasculitis,
direct autoantibody cytotoxicity, antiphospholipid
antibodies and non-inflammatory vasculopathy. The
prognosis of neuro-ophthalmologic manifestations in
SLE seems to be good because of its rapid response to
glucocorticoids. Relapses may be reduced by the use
of maintenance immunosuppression. Patients with
concomitant antiphospholipid syndrome should be
anti-coagulated.
(a) (b)
(c) (d)
Figure 3 Magnetic resonance imagingin neuromyelitis optica. (a) AbnormalT2-weighted signal at bilateral thalamiand midbrain. (b) Long segment abnor-mal T2 hyperintense cord signal from T1to T8. C and D. Decreased T2-weightedabnormal signal in brain and spinalcord after plasma exchange.
International Journal of Rheumatic Diseases 2014; 17: 494–501 499
SLE neuro-ophthalmologic manifestations

DISCLOSURE
None.
FUNDING
The authors did not receive any external funding.
CONFLICTS OF INTERESTS
None.
REFERENCES
1 Tan EM, Cohen AS, Fries JF et al. (1982) The 1982 revised
criteria for the classification of systemic lupus erythemato-
sus. Arthritis Rheum 25, 1271–7.2 Sibbitt WL Jr, Brandt JR, Johnson CR et al. (2002) The
incidence and prevalence of neuropsychiatric syndromes
in pediatric onset systemic lupus erythematosus. J Rheuma-
tol 29, 1536–42.3 Keane JR (1995) Eye movement abnormalities in systemic
lupus erythematosus. Arch Neurol 52, 1145–9.4 Yu HH, Lee JH, Wang LC, Yang YH, Chiang BL (2006)
Neuropsychiatric manifestations in pediatric systemic
lupus erythematosus: a 20-year study. Lupus 15, 651–7.5 Yap EY, Au Eong KG, Fong KY et al. (1998) Ophthalmic
manifestations in Asian patients with systemic lupus ery-
thematosus. Singapore Med J 39, 557–9.6 Ainiala H, Loukkola J, Peltola J, Korpela M, Hietaharju
A (2001) The prevalence of neuropsychiatric syndromes
in systemic lupus erythematosus. Neurology 57, 496–500.
7 Al-Mayouf SM, Al-Hemidan AI (2003) Ocular manifesta-
tions of systemic lupus erythematosus in children. Saudi
Med J 24, 964–6.8 Petri M, Naqibuddin M, Carson KA et al. (2008) Cognitive
function in a systemic lupus erythematosus inception
cohort. J Rheumatol 35, 1776–81.9 Hershko AY, Berkun Y, Mevorach D, Rubinow A, Napars-
tek Y (2008) Increased intracranial pressure related to sys-
temic lupus erythematosus: a 26-year experience. Semin
Arthritis Rheum 38, 110–5.10 Harel L, Sandborg C, Lee T, von Scheven E (2006) Neuro-
psychiatric manifestations in pediatric systemic lupus
erythematosus and association with antiphospholipid
antibodies. J Rheumatol 33, 1873–7.11 Hanly JG, Urowitz MB, Su L et al. (2008) Short-term out-
come of neuropsychiatric events in systemic lupus erythe-
matosus upon enrollment into an international inception
cohort study. Arthritis Rheum 59, 721–9.12 Feinglass EJ, Arnett FC, Dorsch CA, Zizic TM, Stevens MB
(1976) Neuropsychiatric manifestations of systemic lupus
erythematosus: diagnosis, clinical spectrum, and relation-
ship to other features of the disease. Medicine (Baltimore)
55, 323–39.13 Brey RL, Holliday SL, Saklad AR et al. (2002) Neuropsy-
chiatric syndromes in lupus: prevalence using standard-
ized definitions. Neurology 58, 1214–20.14 Jabs DA, Miller NR, Newman SA, Johnson MA, Stevens
MB (1986) Optic neuropathy in systemic lupus erythemat-
osus. Arch Ophthalmol 104, 564–8.15 Siatkowski RM, Scott IU, Verm AM et al. (2001) Optic
neuropathy and chiasmopathy in the diagnosis of sys-
temic lupus erythematosus. J Neuroophthalmol 21, 193–8.16 Lucchinetti CF, Mandler RN, McGavern D et al. (2002) A
role for humoral mechanisms in the pathogenesis of
Devic’s neuromyelitis optica. Brain 125, 1450–61.17 Gibbs AN, Moroney J, Foley-Nolan D, O’Connell PG
(2002) Neuromyelitis optica (Devic’s syndrome) in sys-
temic lupus erythematosus: a case report. Rheumatology
(Oxford) 41, 470–1.18 Karim S, Majithia V (2009) Devic’s syndrome as initial
presentation of systemic lupus erythematosus. Am J Med
Sci 338, 245–7.19 Cordeiro MF, Lloyd ME, Spalton DJ, Hughes GR (1994)
Ischaemic optic neuropathy, transverse myelitis, and epi-
lepsy in an anti-phospholipid positive patient with sys-
temic lupus erythematosus. J Neurol Neurosurg Psychiatry
57, 1142–3.20 Mok CC, To CH, Mak A, Poon WL (2008) Immunoabla-
tive cyclophosphamide for refractory lupus-related neuro-
myelitis optica. J Rheumatol 35, 172–4.21 Mottaghi P, Ashtari F, Karimzadeh H, Seidbonakdar Z,
Karimifar M, Salesi M (2009) Devic’s syndrome concomi-
tant with nephritis in a young woman. Clin Rheumatol 28,1239–40.
22 Margaux J, Hayem G, Meyer O, Kahn MF (1999) Systemic
lupus erythematosus with optical neuromyelitis (Devic’s
syndrome). A case with a 35-year follow-up. Rev Rhum
Engl Ed 66, 102–5.23 Nasir S, Kerr DA, Birnbaum J (2009) Nineteen episodes of
recurrent myelitis in a woman with neuromyelitis optica
and systemic lupus erythematosus. Arch Neurol 66, 1160–3.
24 Jacobi C, Stingele K, Kretz R et al. (2006) Neuromyelitis
optica (Devic’s syndrome) as first manifestation of sys-
temic lupus erythematosus. Lupus 15, 107–9.25 Hagiwara N, Toyoda K, Uwatoko T, Yasumori K, Ibayashi
S, Okada Y (2005) Successful high dose glucocorticoid
treatment for subacute neuromyelitis optica with systemic
lupus erythematosus. Intern Med 44, 998–1001.26 Ferreira S, Marques P, Carneiro E, D’Cruz D, Gama G
(2005) Devic’s syndrome in systemic lupus erythematosus
and probable antiphospholipid syndrome. Rheumatology
(Oxford) 44, 693–5.27 Bonnet F, Mercie P, Morlat P et al. (1999) Devic’s neuro-
myelitis optica during pregnancy in a patient with sys-
temic lupus erythematosus. Lupus 8, 244–7.
500 International Journal of Rheumatic Diseases 2014; 17: 494–501
B. L. Man et al.

28 Birnbaum J, Kerr D (2008) Optic neuritis and recurrent
myelitis in a woman with systemic lupus erythematosus.
Nat Clin Pract Rheumatol 4, 381–6.29 Fanouriakis A, Mastorodemos V, Pamfil C et al. (2013)
Coexistence of systemic lupus erythematosus and multiple
sclerosis: Prevalence, clinical characteristics, and natural
history. Semin Arthritis Rheum (in press).
30 Luneau K, Newman NJ, Biousse V (2008) Ischemic optic
neuropathies. Neurologist 14, 341–54.31 Omar HA, Alzahrani MA, Al Bshabshe AA et al. (2010)
Systemic lupus erythematosus after thymectomy for myas-
thenia gravis: a case report and review of the literature.
Clin Exp Nephrol 14, 272–6.32 Kisielow P, Bluthmann H, Staerz UD, Steinmetz M, von
Boehmer H (1988) Tolerance in T-cell-receptor transgenic
mice involves deletion of nonmature CD4 + 8 + thymo-
cytes. Nature 333, 742–6.33 Ramsdell F, Fowlkes BJ (1990) Clonal deletion versus clo-
nal anergy: the role of the thymus in inducing self toler-
ance. Science 248, 1342–8.34 Mok CC, Ho LY, To CH (2009) Annual incidence and
standardized incidence ratio of cerebrovascular accidents
in patients with systemic lupus erythematosus. Scand J
Rheumatol 38, 362–8.35 Ozgencil E, Gulucu C, Yalcyn S et al. (2007) Seizures and
loss of vision in a patient with systemic lupus erythemato-
sus. Neth J Med 65, 274.
36 Bartynski WS (2008) Posterior reversible encephalopathy
syndrome, part 2: controversies surrounding pathophysi-
ology of vasogenic edema. AJNR Am J Neuroradiol 29,1043–9.
37 McKinney AM, Short J, Truwit CL et al. (2007) Posterior
reversible encephalopathy syndrome: incidence of atypical
regions of involvement and imaging findings. AJR Am J
Roentgenol 189, 904–12.38 Ahlskog JE, O’Neill BP (1982) Pseudotumor cerebri. Ann
Intern Med 97, 249–56.39 Ogawa M, Ishimaru K, Shiroto T, Baba M, Matsunaga M
(1994) A case of benign intracranial hypertension associ-
ated with systemic lupus erythematosus (SLE) showing
diffuse white matter lesions on MRI. Rinsho Shinkeigaku
34, 577–81.40 Yu C, Lin F, Li K et al. (2008) Pathogenesis of normal-
appearing white matter damage in neuromyelitis optica:
diffusion-tensor MR imaging. Radiology 246, 222–8.41 Merle H, Olindo S, Donnio A, Richer R, Smadja D, Cabre
P (2008) Retinal peripapillary nerve fiber layer thickness
in neuromyelitis optica. Invest Ophthalmol Vis Sci 49,4412–7.
42 Nandhagopal R, Al-Asmi A, Gujjar AR (2010) Neuromyeli-
tis optica: an overview. Postgrad Med J 86, 153–9.43 Li Y, Xie P, Lv F et al. (2008) Brain magnetic resonance
imaging abnormalities in neuromyelitis optica. Acta Neu-
rol Scand 118, 218–25.
International Journal of Rheumatic Diseases 2014; 17: 494–501 501
SLE neuro-ophthalmologic manifestations