Embed Size (px)
Citation preview

1
Neurocardiogenic
Neurocardiogenic
Syncope
Syncope
Christopher Bonnet, M.D.
Christopher Bonnet, M.D.
Director, Clinical
Director, Clinical
Electrophysiology
Electrophysiology
Definition of Syncope
Definition of Syncope
Abrupt and transient loss of
Abrupt and transient loss of
consciousness
consciousness
Loss of postural tone
Loss of postural tone
Spontaneous and rapid recovery
Spontaneous and rapid recovery
Transient loss of
Transient loss of
consciousness with
consciousness with
prompt spontaneous
prompt spontaneous
recovery
recovery
2
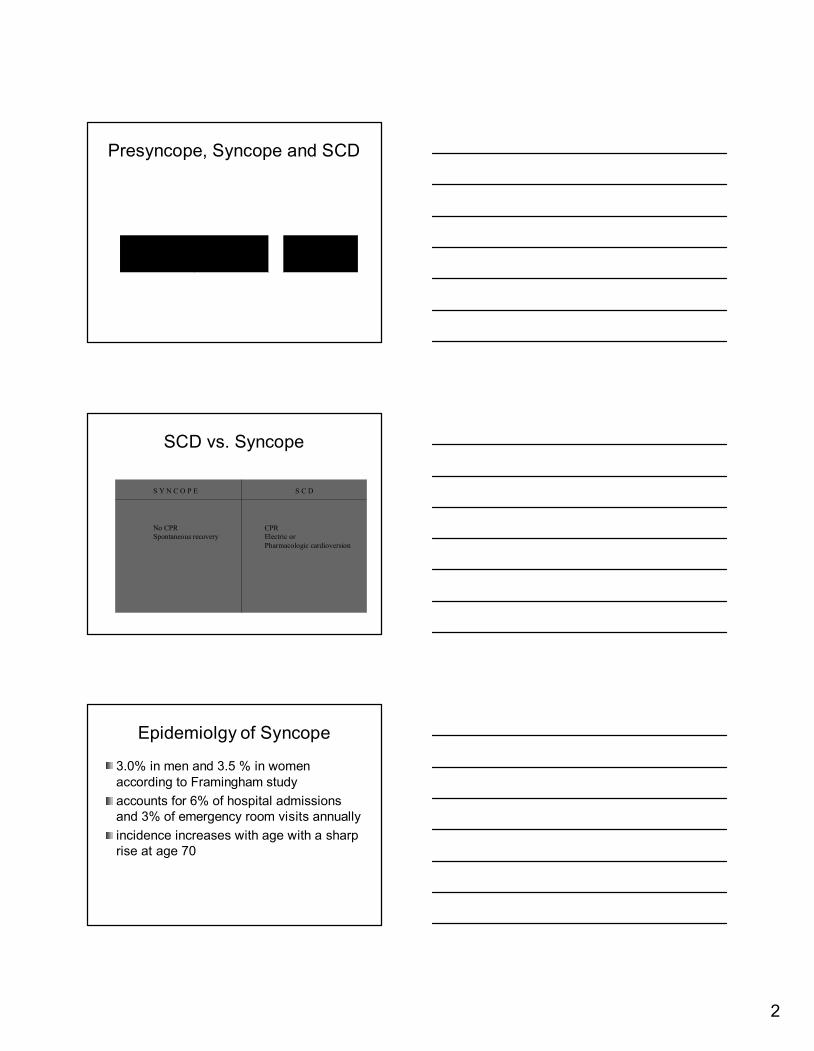
Presyncope
Presyncope
, Syncope and SCD
, Syncope and SCD
Presyncope Syncope Sudden Cardiac Death
SCD vs. Syncope
SCD vs. Syncope
S Y N C O P E S C D
CPR
Electric or
Pharmacologic cardioversion
No CPR
Spontaneous recovery
Epidemiolgy
Epidemiolgy
of Syncope
of Syncope
3.0% in men and 3.5 % in women
3.0% in men and 3.5 % in women
according to Framingham study
according to Framingham study
accounts for 6% of hospital admissions
accounts for 6% of hospital admissions
and 3% of emergency room visits annually
and 3% of emergency room visits annually
incidence increases with age with a sharp
incidence increases with age with a sharp
rise at age 70
rise at age 70

3
Recurrence rate
Recurrence rate
Review of 433 patients, the cumulative
Review of 433 patients, the cumulative
incidence of syncope at three years was:
incidence of syncope at three years was:
31% for patients with cardiovascular
31% for patients with cardiovascular
etiology
etiology
36% for those with
36% for those with
noncardiovascular
noncardiovascular
causes
causes
43% for those with syncope of unknown
43% for those with syncope of unknown
etiology
etiology
Clinical Significance of Syncope
Clinical Significance of Syncope
• Injuries - occur in 35% of syncopal attacks
•Psychological impact
•Prognosis dependent on underlying disease
General Classification of Syncope
General Classification of Syncope
NONCARDIAC CARDIAC
UNDETERMINED
CAUSE
4
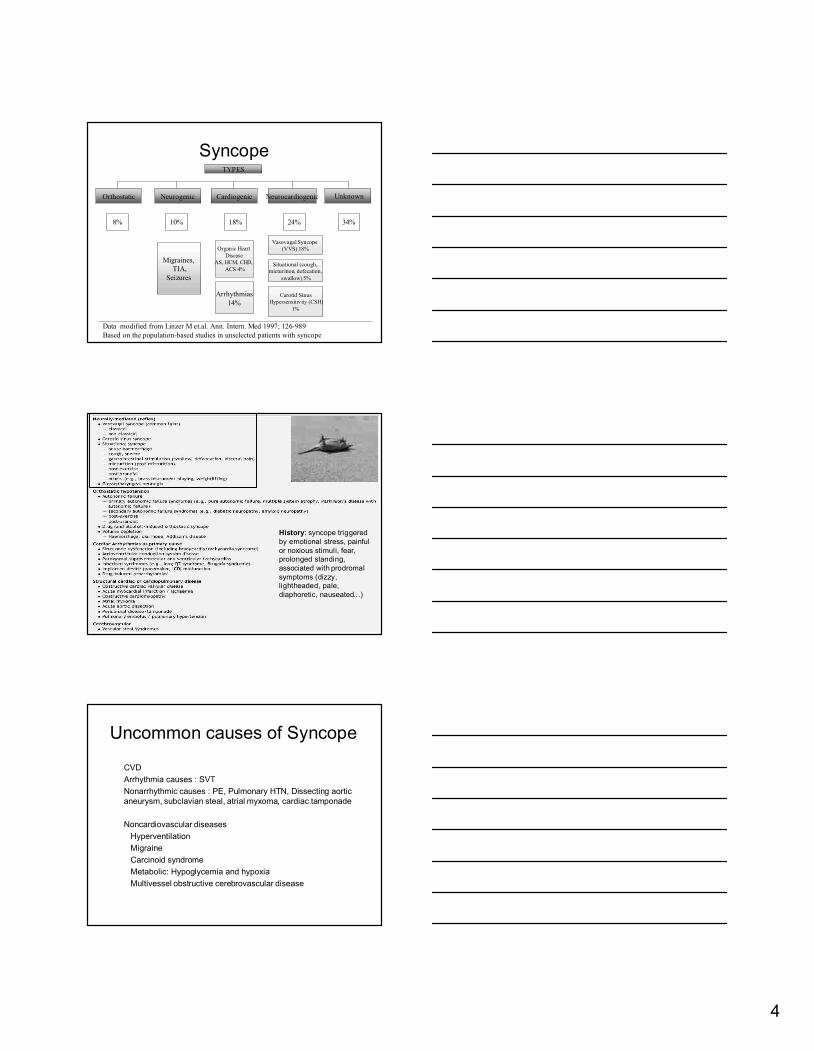
Syncope
Syncope
Orthostatic Neurogenic Cardiogenic Neurocardiogenic
Unknown
Data modified from Linzer M et.al. Ann. Intern. Med 1997; 126-989
Based on the population-based studies in unselected patients with syncope
34%8% 10% 18% 24%
Migraines,
TIA,
Seizures
Organic Heart
Disease
AS, HCM, CHD,
ACS 4%
Arrhythmias
14%
Vasovagal Syncope
(VVS) 18%
Situational (cough,
micturition, defecation,
swallow) 5%
Carotid Sinus
Hypersensitivity (CSH)
1%
TYPES
History: syncope triggered
by emotional stress, painful
or noxious stimuli, fear,
prolonged standing,
associated with prodromal
symptoms (dizzy,
lightheaded, pale,
diaphoretic, nauseated…)
Uncommon causes of Syncope
Uncommon causes of Syncope
CVD
CVD
Arrhythmia causes : SVT
Arrhythmia causes : SVT
Nonarrhythmic
Nonarrhythmic
causes : PE, Pulmonary HTN, Dissecting aortic
causes : PE, Pulmonary HTN, Dissecting aortic
aneurysm,
aneurysm,
subclavian
subclavian
steal,
steal,
atrial
atrial
myxoma
myxoma
, cardiac
, cardiac
tamponade
tamponade
Noncardiovascular
Noncardiovascular
diseases
diseases
Hyperventilation
Hyperventilation
Migraine
Migraine
Carcinoid
Carcinoid
syndrome
syndrome
Metabolic: Hypoglycemia and hypoxia
Metabolic: Hypoglycemia and hypoxia
Multivessel
Multivessel
obstructive
obstructive
cerebrovascular
cerebrovascular
disease
disease
5
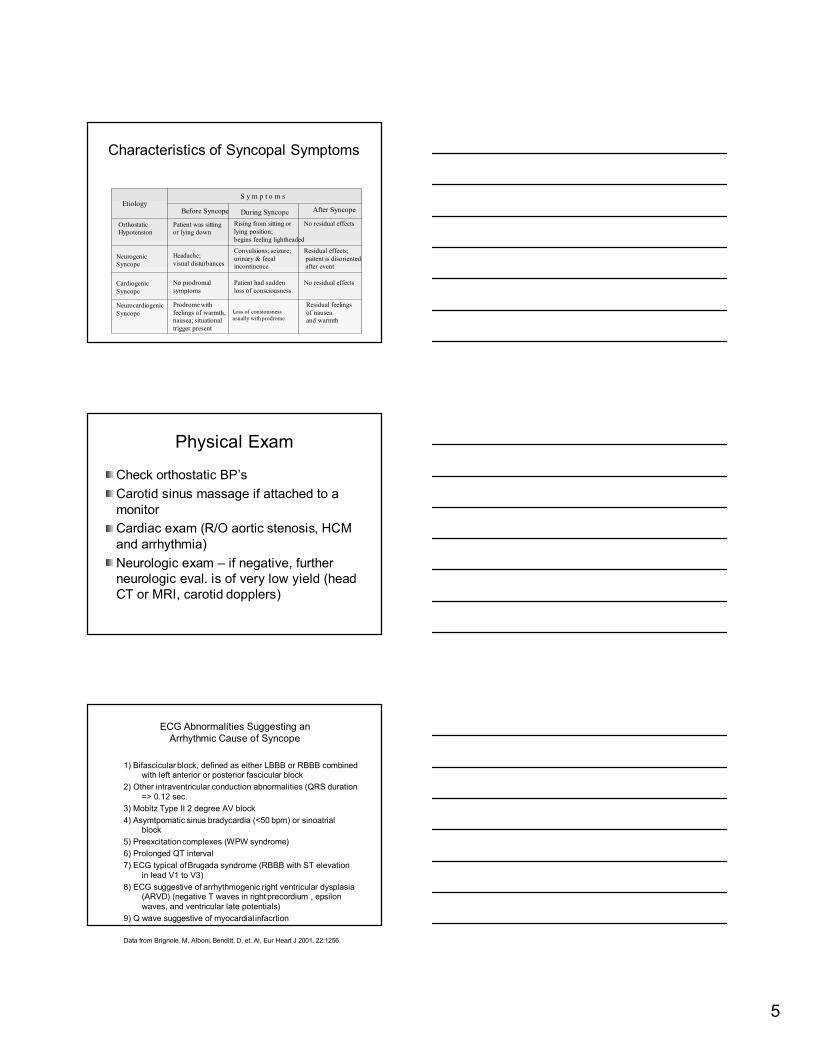
Characteristics of
Characteristics of
Syncopal
Syncopal
Symptoms
Symptoms
Before Syncope
During Syncope
After Syncope
S y m p t o m s
Etiology
Orthostatic
Hypotension
Neurogenic
Syncope
Cardiogenic
Syncope
Neurocardiogenic
Syncope
Patient was sitting
or lying down
Headache;
visual disturbances
No prodromal
symptoms
Prodrome with
feelings of warmth,
nausea; situational
trigger present
Loss of consiousness
usually with prodrome
Patient had sudden
loss of consciousness
Convulsions; seizure;
urinary & fecal
incontinence
Rising from sitting or
lying position;
begins feeling lightheaded
No residual effects
Residual effects;
paitent is disoriented
after event
No residual effects
Residual feelings
of nausea
and warmth
Physical Exam
Physical Exam
Check orthostatic BP
Check orthostatic BP
’
’
s
s
Carotid sinus massage if attached to a
Carotid sinus massage if attached to a
monitor
monitor
Cardiac exam (R/O aortic
Cardiac exam (R/O aortic
stenosis
stenosis
, HCM
, HCM
and arrhythmia)
and arrhythmia)
Neurologic exam
Neurologic exam
–
–
if negative, further
if negative, further
neurologic
neurologic
eval
eval
. is of very low yield (head
. is of very low yield (head
CT or MRI, carotid
CT or MRI, carotid
dopplers
dopplers
)
)
ECG Abnormalities Suggesting an
ECG Abnormalities Suggesting an
Arrhythmic Cause of Syncope
Arrhythmic Cause of Syncope
1)
1)
Bifascicular
Bifascicular
block, defined as either LBBB or RBBB combined
block, defined as either LBBB or RBBB combined
with left anterior or posterior fascicular block
with left anterior or posterior fascicular block
2) Other
2) Other
intraventricular
intraventricular
conduction abnormalities (QRS duration
conduction abnormalities (QRS duration
=> 0.12 sec.
=> 0.12 sec.
3)
3)
Mobitz
Mobitz
Type II 2 degree AV block
Type II 2 degree AV block
4)
4)
Asymtpomatic
Asymtpomatic
sinus
sinus
bradycardia
bradycardia
(<50
(<50
bpm
bpm
) or
) or
sinoatrial
sinoatrial
block
block
5)
5)
Preexcitation
Preexcitation
complexes (WPW syndrome)
complexes (WPW syndrome)
6) Prolonged QT interval
6) Prolonged QT interval
7) ECG typical of
7) ECG typical of
Brugada
Brugada
syndrome (RBBB with ST elevation
syndrome (RBBB with ST elevation
in lead V1 to V3)
in lead V1 to V3)
8) ECG suggestive of
8) ECG suggestive of
arrhythmogenic
arrhythmogenic
right ventricular dysplasia
right ventricular dysplasia
(ARVD) (negative T waves in right
(ARVD) (negative T waves in right
precordium
precordium
, epsilon
, epsilon
waves, and ventricular late potentials)
waves, and ventricular late potentials)
9) Q wave suggestive of myocardial
9) Q wave suggestive of myocardial
infacrtion
infacrtion
Data from Data from BrignoleBrignole, M, , M, AlboniAlboni, , BendittBenditt, D, et. Al, , D, et. Al, EurEur Heart J 2001, 22:1256Heart J 2001, 22:1256

6
Indications for Ambulatory ECG Monitoring to Assess
Indications for Ambulatory ECG Monitoring to Assess
Symptoms Possibly Related to Rhythm Disturbances
Symptoms Possibly Related to Rhythm Disturbances
Class I
Class I
1) Patients with unexplained syncope, near syncope, or
1) Patients with unexplained syncope, near syncope, or
episodesic
episodesic
dizziness in whom the cause is not obvious
dizziness in whom the cause is not obvious
2) Patients with unexplained recurrent palpitation
2) Patients with unexplained recurrent palpitation
Class
Class
IIb
IIb
1) Patients with episodic shortness of breath, chest pain t
1) Patients with episodic shortness of breath, chest pain t
hat is
hat is
not otherwise explained
not otherwise explained
2) Patient with neurological events when transient
2) Patient with neurological events when transient
atrial
atrial
fibrillation or flutter is suspected
fibrillation or flutter is suspected
3) Patients with symptoms such as syncope, near syncope,
3) Patients with symptoms such as syncope, near syncope,
episodic dizziness, or palpitation in whom a probable cause
episodic dizziness, or palpitation in whom a probable cause
other than an
other than an
arrhyhmia
arrhyhmia
has been identified but in whom
has been identified but in whom
symptoms persists despite treatment of this other cause
symptoms persists despite treatment of this other cause
SYNCOPE
SYNCOPE
Inpatient versus outpatient evaluation
Inpatient versus outpatient evaluation
Usually dependent on severity (i.e. injury
Usually dependent on severity (i.e. injury
or MVA)
or MVA)
Structural heart disease suggests a more
Structural heart disease suggests a more
malignant etiology and usually requires
malignant etiology and usually requires
hospitalization
hospitalization
Neurocardiogenic
Neurocardiogenic
Syncope
Syncope

7
Neurocardiogenic
Neurocardiogenic
Syncope
Syncope
Also known as the common faint
Also known as the common faint
Neurally
Neurally
mediated syndrome (NMS),
mediated syndrome (NMS),
vasovagal
vasovagal
syncope (VVS) or
syncope (VVS) or
vasodepressor syncope
vasodepressor syncope
Often a diagnosis by exclusion
Often a diagnosis by exclusion
Rule out
Rule out
cardiogenic
cardiogenic
and
and
neurogenic
neurogenic
causes first
causes first
Review of 641 patients with recurrent
Review of 641 patients with recurrent
syncope in whom a cardiac, neurologic
syncope in whom a cardiac, neurologic
and metabolic etiology of syncope had
and metabolic etiology of syncope had
been excluded,
been excluded,
neurocardiogenic
neurocardiogenic
syncope
syncope
was considered the cause in
was considered the cause in
35%
35%
of
of
patients.
patients.
In a prospective study of 341 patients with
In a prospective study of 341 patients with
syncope,
syncope,
33 percent
33 percent
had
had
neurocardiogenic
neurocardiogenic
syncope.
syncope.
Incidence of NeurocardiogenicSyncope
Neurocardiogenic
Neurocardiogenic
Syncope
Syncope
Reflex response causing
Reflex response causing
vasodilation
vasodilation
and
and
bradycardia
bradycardia
resulting in
resulting in
systemic hypotension and
systemic hypotension and
cerebral
cerebral
hypoperfusion
hypoperfusion
8
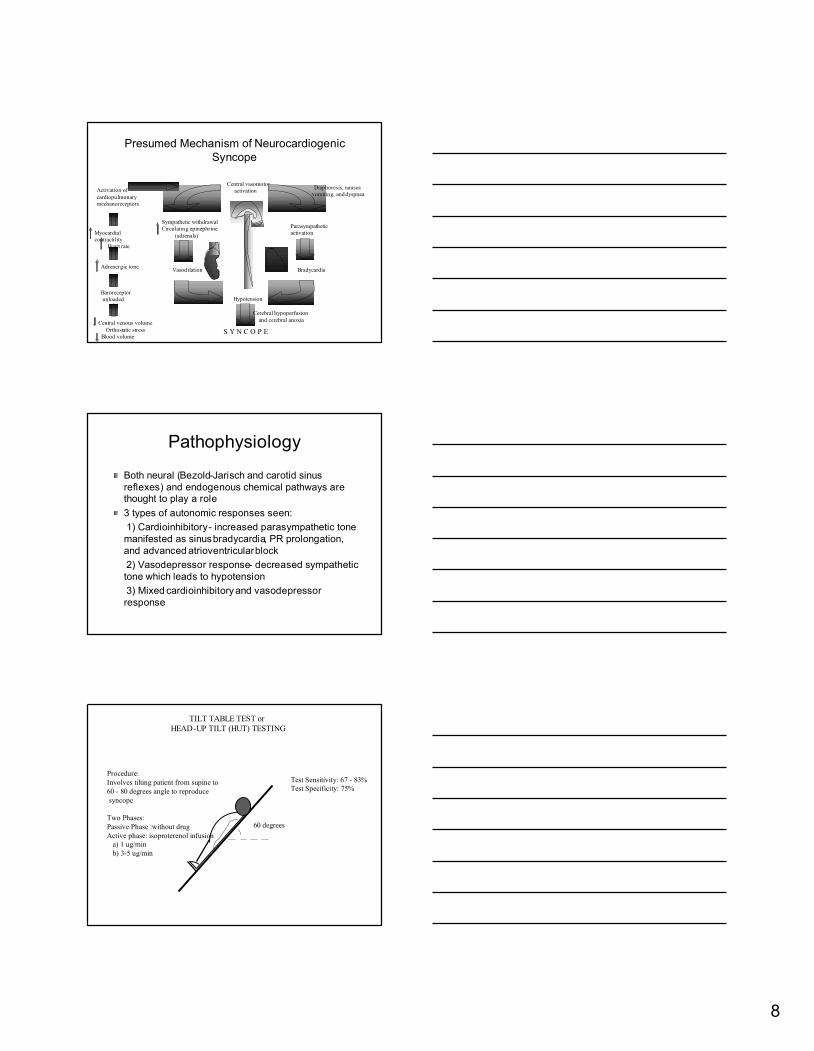
Presumed Mechanism of
Presumed Mechanism of
Neurocardiogenic
Neurocardiogenic
Syncope
Syncope
Central venous volume
Orthostatic stress
Blood volume
Baroreceptor
unloaded
Adrenergic tone
Myocardial
contractility
Heart rate
Activation of
cardiopulmonary
mechanoreceptors
Parasympathetic
activation
Bradycardia
Hypotension
Vasodilation
Central vasomotor
activation
Sympathetic withdrawal
Circulating epinephrine
(adrenals)
S Y N C O P E
Diaphoresis, nausea
vomiting, and dyspnea
Cerebral hypoperfusion
and cerebral anoxia
Pathophysiology
Pathophysiology
Both neural (
Both neural (
Bezold
Bezold
-
-
Jarisch
Jarisch
and carotid sinus
and carotid sinus
reflexes) and endogenous chemical pathways are
reflexes) and endogenous chemical pathways are
thought to play a role
thought to play a role
3 types of autonomic responses seen:
3 types of autonomic responses seen:
1)
1)
Cardioinhibitory
Cardioinhibitory
-
-
increased parasympathetic tone
increased parasympathetic tone
manifested as sinus
manifested as sinus
bradycardia
bradycardia
, PR prolongation,
, PR prolongation,
and advanced
and advanced
atrioventricular
atrioventricular
block
block
2) Vasodepressor response
2) Vasodepressor response
-
-
decreased sympathetic
decreased sympathetic
tone
tone
which leads to hypotension
which leads to hypotension
3) Mixed
3) Mixed
cardioinhibitory
cardioinhibitory
and vasodepressor
and vasodepressor
response
response
60 degrees
TILT TABLE TEST or
HEAD-UP TILT (HUT) TESTING
Test Sensitivity: 67 - 83%
Test Specificity: 75%
Procedure:
Involves tilting patient from supine to
60 - 80 degrees angle to reproduce
syncope
Two Phases:
Passive Phase :without drug
Active phase: isoproterenol infusion
a) 1 ug/min
b) 3-5 ug/min
9
Tilt Table Test
Tilt Table Test
Indications:
Indications:
1) Work
1) Work
-
-
up of syncope in patients
up of syncope in patients
with structurally normal heart
with structurally normal heart
(normal ECG, ECHO, stress
(normal ECG, ECHO, stress
test or a non
test or a non
-
-
diagnostic
diagnostic
Holter
Holter
)
)
2) Men > 45 y.o. and women
2) Men > 45 y.o. and women
> 55 y.o. should undergo
> 55 y.o. should undergo
stress testing before the test
stress testing before the test
3) Women of child bearing age
3) Women of child bearing age
should have a pregnancy
should have a pregnancy
test
test
Upright Tilt Table Test
Upright Tilt Table Test
Measure HR and BP
Measure HR and BP
while tilting them
while tilting them
upright
upright
Attempt to elicit
Attempt to elicit
symptoms
symptoms
Cannot be used to
Cannot be used to
test efficacy of
test efficacy of
pharmacologic
pharmacologic
therapy
therapy
Carotid Sinus Massage
Carotid Sinus Massage
Indication:
Indication:
a) patients > 40 years old with unknown etiology
a) patients > 40 years old with unknown etiology
of syncope after initial evaluation
of syncope after initial evaluation
Procedure:
Procedure:
b) Continuous ECG and BP monitoring mandatory
b) Continuous ECG and BP monitoring mandatory
c) Carotid massage done for 5
c) Carotid massage done for 5
-
-
10 sec. in both supine and erect
10 sec. in both supine and erect
positions
positions
Positive Result:
Positive Result:
a) symptoms are reproduced during or immediately after the
a) symptoms are reproduced during or immediately after the
massage
massage
b)
b)
asystole
asystole
longer than 3 sec. and or
longer than 3 sec. and or
c) a fall in SBP of =>50 mmHg
c) a fall in SBP of =>50 mmHg
Data from Brignole, M, Albani, O Benditt, D, et. Al., Eur Heart J 2001; 22:1256
10
Preventive Measures
Preventive Measures
Avoid dehydration and severe dieting
Avoid dehydration and severe dieting
Liberal salt intake if not contraindicated
Liberal salt intake if not contraindicated
Counterpressure
Counterpressure
support garments from
support garments from
ankles to waist
ankles to waist
Avoid prolonged periods of motionless
Avoid prolonged periods of motionless
standing
standing
Once with
Once with
prodromal
prodromal
or trigger
or trigger
-
-
assume
assume
a recumbent position and cough
a recumbent position and cough
Avoid triggers like heat exposure,
Avoid triggers like heat exposure,
painful stimuli
painful stimuli
Treatment
Treatment
Reassurance, education, avoidance
Reassurance, education, avoidance
Support stockings, salt liberalization
Support stockings, salt liberalization
Beta blockers
Beta blockers
Midodrine
Midodrine
Selective Serotonin Reuptake Inhibitors
Selective Serotonin Reuptake Inhibitors
Fludrocortisone
Fludrocortisone
(
(
Florinef
Florinef
)
)
Drug therapy is often not very effective
Drug therapy is often not very effective

11
Non
Non
-
-
random, observational
random, observational
RCTs
RCTs
comparing
comparing
vs
vs
RCTs
RCTs
comparing
comparing
vs
vs
What are the indications for pacemaker
What are the indications for pacemaker
therapy in
therapy in
neurocardiogenic
neurocardiogenic
syncope?
syncope?
2727 dualdual--chamber pacemakerschamber pacemakers
with ratewith rate--drop responsedrop response
54 pts
54 pts
2727 No pacemakerNo pacemaker
Included
Included
>6 lifetime episodes
>6 lifetime episodes
+ tilt
+ tilt
-
-
table test
table test
–
–
(relative
(relative
bradycardia
bradycardia
)
)
Primary outcome: first recurrence of syncope
54 days54 days112 days112 daysTime to Time to
recurrencerecurrence
19/27 (70%)19/27 (70%)6/27 (22%)6/27 (22%)Recurrence of Recurrence of
SyncopeSyncope
No pacemakerNo pacemakerPacemakerPacemaker
Excluded
Excluded
Vascular, coronary, myocardial
Vascular, coronary, myocardial
or conduction system disease
or conduction system disease
The North American
The North American
Vasovagal
Vasovagal
Pacemaker Study (VPS)
Pacemaker Study (VPS)
J. Am. Coll Cardiol. 1999;33:16-20
VPS
VPS
Limitations:
Limitations:
Unblinded
Unblinded
Small study size
Small study size
Time to first
Time to first
occurrence
occurrence
vs
vs
total
total
disease burden
disease burden
J. Am. Coll Cardiol. 1999;33:16-20

12
Vasovagal
Vasovagal
Syncope International
Syncope International
Study (VASIS)
Study (VASIS)
Repeat tilt testing: no differenceRepeat tilt testing: no difference
Pacer arm 10/17 + testsPacer arm 10/17 + tests
–– 5 had no 5 had no bradycardiabradycardia, 5 pacer did , 5 pacer did
not prevent syncopenot prevent syncope
–– 1/7 pacer activated in 1/7 pacer activated in negneg testtest
>
>
3 episodes in last 2 yrs
3 episodes in last 2 yrs
Tilt test
Tilt test
cardioinhibition
cardioinhibition
–– VentricVentric. Rate <40 for 10 sec. Rate <40 for 10 sec
–– AsystoleAsystole >3sec>3sec
Circulation 2000;102:294-299
Permanent cardiac pacing versus medical treatment for the
Permanent cardiac pacing versus medical treatment for the
prevention of recurrent
prevention of recurrent
vasovagal
vasovagal
syncope
syncope
93 pts
93 pts
46 47
46 47
DDD pacemaker
DDD pacemaker
atenolol
atenolol
+ rate drop 100mg daily
+ rate drop 100mg daily
Unblinded
Unblinded
older, highly symptomatic
older, highly symptomatic
patients with an
patients with an
asystolic
asystolic
response to tilt testing in pacer
response to tilt testing in pacer
group
group
Circulation 2001;104;52-57
VPS II
VPS II
>3 episodes in 2 years
>3 episodes in 2 years
+tilt test
+tilt test
–
–
HR x BP< 6000/min
HR x BP< 6000/min
-
-
mmHg
mmHg
Risk of syncope at 6
Risk of syncope at 6
months: 40% ODO,
months: 40% ODO,
31% DDD
31% DDD
–
–
RRR 30% (P = 0.14)
RRR 30% (P = 0.14)
Compared to VPS I
Compared to VPS I
Fewer events in non
Fewer events in non
-
-
paced group in VPS II
paced group in VPS II
(40%
(40%
vs
vs
70%)
70%)
JAMA 2003;289:2224-2229

13
SYNPACE
SYNPACE
6 events lifetime
6 events lifetime
+tilt test
+tilt test
–
–
Asystolic
Asystolic
: >3
: >3
secs
secs
–
–
Mixed:
Mixed:
bradycardic
bradycardic
<60bpm
<60bpm
but no
but no
asystole
asystole
–
–
Vasodepressor: hypotension
Vasodepressor: hypotension
only, were excluded
only, were excluded
29 pts randomized to pacemaker
29 pts randomized to pacemaker
ON (16) or OFF (13)
ON (16) or OFF (13)
Syncope recurred 8 (50%) in ON
Syncope recurred 8 (50%) in ON
group, 5 (38%) in OFF group
group, 5 (38%) in OFF group
No significant difference
No significant difference
Syncopal
Syncopal
rates lower
rates lower
postimplantation
postimplantation
for both
for both
groups
groups
Non
Non
-
-
significant trend of pacing
significant trend of pacing
prolonging time to first
prolonging time to first
occurrence
occurrence
Euro Heart J 2004;25:1741-1748
Conclusions
Conclusions
ACC/AHA/HRS 2008 Guidelines for Device
ACC/AHA/HRS 2008 Guidelines for Device
-
-
based Therapy
based Therapy
Class Class IIaIIa
Permanent pacing is reasonable for syncope without clear Permanent pacing is reasonable for syncope without clear
provocative events and with a hypersensitive provocative events and with a hypersensitive cardioinhibitorycardioinhibitory
response of 3 seconds or longer.response of 3 seconds or longer.
Class Class IIbIIb
Permanent pacing may be considered for Permanent pacing may be considered for
significantly symptomatic significantly symptomatic neurocardiogenicneurocardiogenic syncope syncope
associated with associated with bradycardiabradycardia documented spontaneously or at documented spontaneously or at
the time of tiltthe time of tilt--table testing.table testing.
Class IIIClass III
Permanent pacing is not indicated for situational Permanent pacing is not indicated for situational vasovagalvasovagal
syncope in which avoidance behavior is effective and syncope in which avoidance behavior is effective and
preferred.preferred.
64yo F
HPI: walks in
the door, finds
her friends
down, runs to
call 911, steps
on a banana
peel, falls, no LOC
66yo F
HPI: Attending
to her friends
when she falls
to floor, +LOC,
+loss bladder,
+jerking
movements of her arms and legs
59yo F
HPI: vomiting +
diarrhea x3 days,
stands up rapidly
from supine, falls
back onto couch,
+LOC
case
case
85yo F
HPI: LOC while sitting
on toilet, no head
trauma
PMH: Afib, HTN, HL,
recurrent syncope
-previous syncope: sitting in church, at
restaurant, bowel movement
-hx + tilt table test, ILR: bradycardic to 40s

14
Recommendations for Driving
Recommendations for Driving
in Patients with Syncope
in Patients with Syncope
Diagnosis
Diagnosis
Disqualifying
Disqualifying
Criteria
Criteria
NMS (
NMS (
Neurally
Neurally
mediated syncope)
mediated syncope)
VVS and CSH
VVS and CSH
-
-
Single episodes, mild symptoms No restric
Single episodes, mild symptoms No restric
tions
tions
-
-
Severe symptoms Un
Severe symptoms Un
til symptoms
til symptoms
controlled
controlled
-
-
Situational forms
Situational forms
No restrictions
No restrictions
Syncope of uncertain cause In case of severe sync
Syncope of uncertain cause In case of severe sync
ope
ope
until cause identified,
until cause identified,
especially in patients with
especially in patients with
hea
hea
rt disease or at least 6
rt disease or at least 6
mon
mon
ths without symptoms
ths without symptoms
before (re)
before (re)
-
-
licensing
licensing
Recommendations for Driving
Recommendations for Driving
in Patients with Syncope
in Patients with Syncope
Diagnosis Disqualifying cri
Diagnosis Disqualifying cri
teria
teria
Cardiac
Cardiac
Arrhytmias
Arrhytmias
Any disturbance of cardiac
Any disturbance of cardiac
rhythm which is likely to cause
rhythm which is likely to cause
which is likely to cause syncope
which is likely to cause syncope
Pacemaker implant Within one week
Pacemaker implant Within one week
Successful catheter ablation
Successful catheter ablation
ICD Within 6 mont
ICD Within 6 mont
hs if no
hs if no
arrhythmia recurrence
arrhythmia recurrence
and no dis
and no dis
abling symptoms at
abling symptoms at
time of ICD discharge.
time of ICD discharge.
If prophylactic ICD placement
If prophylactic ICD placement
-
-
one week then no restrictions
one week then no restrictions
15
ESC Recommendations for
ESC Recommendations for
Treatment of
Treatment of
Neurocardiogenic
Neurocardiogenic
Syncope
Syncope
Class I
Class I
1) Explanation of the risk
1) Explanation of the risk
Conclusions
Conclusions
ACC/AHA/HRS 2008 Guidelines for ACC/AHA/HRS 2008 Guidelines for
DeviceDevice--based Therapybased Therapy
Class Class IIaIIa
Permanent pacing is reasonable for Permanent pacing is reasonable for
syncope without clear provocative syncope without clear provocative
events and with a hypersensitive events and with a hypersensitive
cardioinhibitorycardioinhibitory response of 3 seconds response of 3 seconds
or longer.or longer.
Class Class IIbIIb
Permanent pacing may be considered Permanent pacing may be considered
for significantly symptomatic for significantly symptomatic
neurocardiogenicneurocardiogenic syncope associated syncope associated
with with bradycardiabradycardia documented documented
spontaneously or at the time of tiltspontaneously or at the time of tilt--
table testing.table testing.
Class IIIClass III
Permanent pacing is not indicated for Permanent pacing is not indicated for
situational situational vasovagalvasovagal syncope in which syncope in which
avoidance behavior is effective and avoidance behavior is effective and
preferred.preferred.
European Society of Cardiology European Society of Cardiology
Guidelines on Management of Guidelines on Management of
Syncope 2004Syncope 2004
Class IIIClass III
Cardiac pacing in patients with Cardiac pacing in patients with
cardioinhibitorycardioinhibitory vasovagalvasovagal syncope syncope
with a frequency >5 attacks per year or with a frequency >5 attacks per year or
severe physical injury or accident and severe physical injury or accident and
age>40age>40
TTT/HUT (8/30/99)
TTT/HUT (8/30/99)
* Nausea, diaphoresis, & altered gaze
*
16
Pacing
Pacing
DDD type of pacemaker
DDD type of pacemaker
Case to case basis
Case to case basis
Rx
Rx
Neurocardiogenic
Neurocardiogenic
syncope
syncope
Beta
Beta
-
-
blockers
blockers
-
-
most commonly effective
most commonly effective
therapy
therapy
SSRI :
SSRI :
sertraline
sertraline
,
,
flouxetine
flouxetine
or
or
paroxetine
paroxetine
Midodrine
Midodrine
(alpha 1 adrenergic agonist)
(alpha 1 adrenergic agonist)
Florinef
Florinef
Theophylline
Theophylline














![Syncope AHD[1]](https://img.pdfslide.net/doc/110x75/577d36611a28ab3a6b92ec10/syncope-ahd1.jpg)