Embed Size (px)
Citation preview
Bull Vet Inst Pulawy 53, 285-290, 2009
NEUROENDOCRINE PULMONARY SMALL CELL CARCINOMA IN A DOG. A CASE REPORT
RENATA NOWACZYK, MARCIN NOWAK, AND KAMILA GLIŃSKA-SUCHOCKA1
Department of Pathological Anatomy, Pathophysiology, Microbiology, and Forensic Veterinary Medicine, Faculty of Veterinary Medicine,
Wroclaw University of Environmental and Life Sciences, 50-375 Wroclaw, Poland 1Department of Internal and Parasitic Diseases with Clinic for Horses, Dogs, and Cats,
Faculty of Veterinary Medicine, Wroclaw University of Environmental and Life Sciences, 50-366 Wroclaw, Poland
Received for publication January 23, 2009
Abstract
The described case involves a German shepherd dog, 11-year-old, with a pulmonary tumour. Morphological and biochemical tests were performed on various blood parameters, and USG examinations of abdominal cavity and chest were carried out, as well as an X-ray examination of the chest. The fluid from pleural cavities was subjected to tests of physical, morphological, and biochemical properties, and to microbiological and cytological examinations. Due to the advanced age of the animal, increasingly severe morbid signs and unfavourable prognosis, the owner of the dog decided to ask for its euthanasia. Macroscopic examination of the pulmonary tissue disclosed neoplastic hyperplasia, involving the left adcephalic lobe and infiltrating the region of the pulmonary hilus. A small-cell carcinoma was diagnosed histopathologically and the diagnosis was confirmed by immunohistochemical examination. As a rule, it rapidly metastasises and bound to a poor-prognosis cancer, but in this case, the carcinoma manifested the rarely-observed limited form, and failed to produce metastases despite histological exponents of its malignant character.
Key words: dog, pulmonary tumour.
Primary pulmonary tumours are frequently
diagnosed in humans but they are very rare in household animals such as dogs and cats. According to Nowak et al. (20), tumours of the respiratory system comprised only 0.7% of the total number of neoplastic lesions demonstrated in dogs. Similarly to many other tumours they were encountered more frequently in older animals, usually above the age of 10 years (9, 17, 22, 27). Much more frequently than primary tumours, pulmonary tissue contains tumour metastases, which reflects the anatomic position of lungs in the blood circulation. Neoplastic transformation may involve any element of pulmonary tissues, including dispersed endocrine cells in the lungs, termed the Kulczycki’s cells. Their excessive and uncontrolled proliferation leads to the development of so-called neuroendocrine tumours (NET). NET represent a large group of neoplastic lesions, which may stem from endocrine glands and groups of endocrine cells within glandular structures as well as from dispersed endocrine cells of alimentary and respiratory systems (22, 28). The tumours comprise a heterogenous group and differ between each other in their histological pattern, secreted mediators, clinical symptoms and prognosis (18, 28, 31, 34). Their precursor cells or the so-called APUD (amine precursor uptake and
decarboxylation) cells trait in the discussed group. Both in physiological conditions and following neoplastic transformation the cells manifest the ability to incorporate amine precursors and to transform themselves by decarboxylation into peptide compounds, secreted to the extracellular space (26). In the lungs they may secrete serotonin, calcitonin, calcitonin gene-related peptide (CGRP), gastrin-releasing peptide (GRP), bombesin, enkephalin, and somatostatin (25, 26, 32).
Despite the enormous development of diagnostic techniques, histopathological diagnosis and appropriate classification of neuroendocrine tumours both in humans and in animals pose several difficulties (6). Immunohistochemical studies are thought to represent one of the most effective techniques in the diagnosis of the tumours (25). It should be noted that the presence of proteins in the cells, reflecting their neuroendocrine origin, represents a diagnostically very significant element. At the ultrastructural level, neuroendocrine differentiation is defined by the presence of so called cytoplasmatic neurosecretory granules. Applied immunohistochemical tests allow us to detect the presence and to evaluate the expression level of both neuroendocrine markers like synaptophysin and neuron-specific enolase (NSE), and also products of

286
secretory activity (calcitonin, bombesin) (4, 13, 32). Antibodies to synaptophysin, representing a homo-oligomeric membrane glycoprotein, label endocrine tumours of the nervous system and epithelial type endocrine tumours. Due to this property, synaptophysin is regarded as a highly-sensitive specific marker of neuroendocrine differentiation (13). Another important marker used in the diagnosis of neuroendocrine tumours involves neuron-specific enolase. This compound represents a glycolytic isoenzyme, detectable in central and peripheral neurons as well as in normal and neoplastically-transformed neuroendocrine cells (13, 21). Numerous studies confirm that synaptophysin and neuron-specific enolase are very sensitive indices of neuroendocrine differentiation, indispensable in the diagnosis of pulmonary neuroendocrine tumours (4, 13, 15, 21, 25, 29, 32).
Description of the case and Discussion
The case described below involves a German shepherd male dog, of 11 years of age. For a week, the dog suffered from coughs, dyspnoea, lack of appetite, vomiting, and exertional insufficiency. Clinical examination disclosed inner body temperature of 38.5ºC, pronounced mixed dyspnoea, and general weakness. Morphological and biochemical tests were performed on various blood parameters. An USG examination of the
abdominal cavity and chest was performed as well as X-ray examination of the chest in the lateral and dorsal/abdominal projection. In addition, pleural puncture yielded 420 cm3 of fluid content. The fluid was subjected to tests of physical, morphological, and biochemical properties, and for microbiological and cytological examination. Blood morphology disclosed a marked granulocytosis. The remaining morphological parameters of blood proved to be within normal ranges. Biochemical examination detected an augmented level of blood urea with normal concentration of creatinine (Table 1).
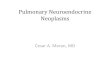
In the USG examination of the abdominal cavity, the urinary bladder was filled with a high volume of urine, the prostate was slightly enlarged and heteroechogenous. The liver was also enlarged but manifested the normal structure. No lesions were detected in the remaining abdominal organs. Chest USG examination demonstrated the presence of significant amounts of a fluid in pleural cavities and an uneven surface of pleura. X-ray examination in the lateral projection (Fig. 1) documented an intensified shadow of anterior pulmonary fields while the abdominal edge of ad-cranial pre-cardiac mediastinum was poorly visible.
In a sagittal projection (Fig. 2) a shadow was noted, which involved the ad-cranial left part of the chest with an even, oblique line separating the airless region from normal lungs.
Table 1
Haematologic and chemistry values
*Winnicka A.: Reference values in basic laboratory tests in veterinary medicine (in Polish). SGGW, Warszawa, 1997.
Haematologic variables Erythrocytes
T/L Haematocrit l/L
Haemoglobin mmol/L
MCV Fl
MCH pg
MCHC g/dl
Reference value*
5.5-8.5 0.37-0.55 12-18 60-77 19-24 32-36
Measured value
6.23 0.424 9.70 68 1.56 32
Leukocytes G/l
Lymphocytes %
Monocytes %
Granulocytes %
Platelets G/l
Reference value*
6-17 12-37 3-10 60-90 175-500
Measured value
24.3 3.7 2.7 93.6 273
Chemistry values BUN
mmol/L Creatininemmol/L
Ammo-nia µmol/L
AL U/L
AST U/L
ALP U/L
GGT U/L
Reference value*
4.15-7.47 79.6-160.9 <32 3-50 1-37 20-155 5-25
Measured value
11.87 105 1 64 45 129 4
Total protein g/L
Albumin g/L
Amylase U/L
Lipase U/L
Na mmol/L
K mmol/L
Cl mmol/L
Ca mmol/L
Reference value*
50-70 33-56
388-1800
268-1769
139-156 4.1-5.4 98.7-115 2.25-3.0
Measured value
51 35 1547 879 4.3 102 2.56

287
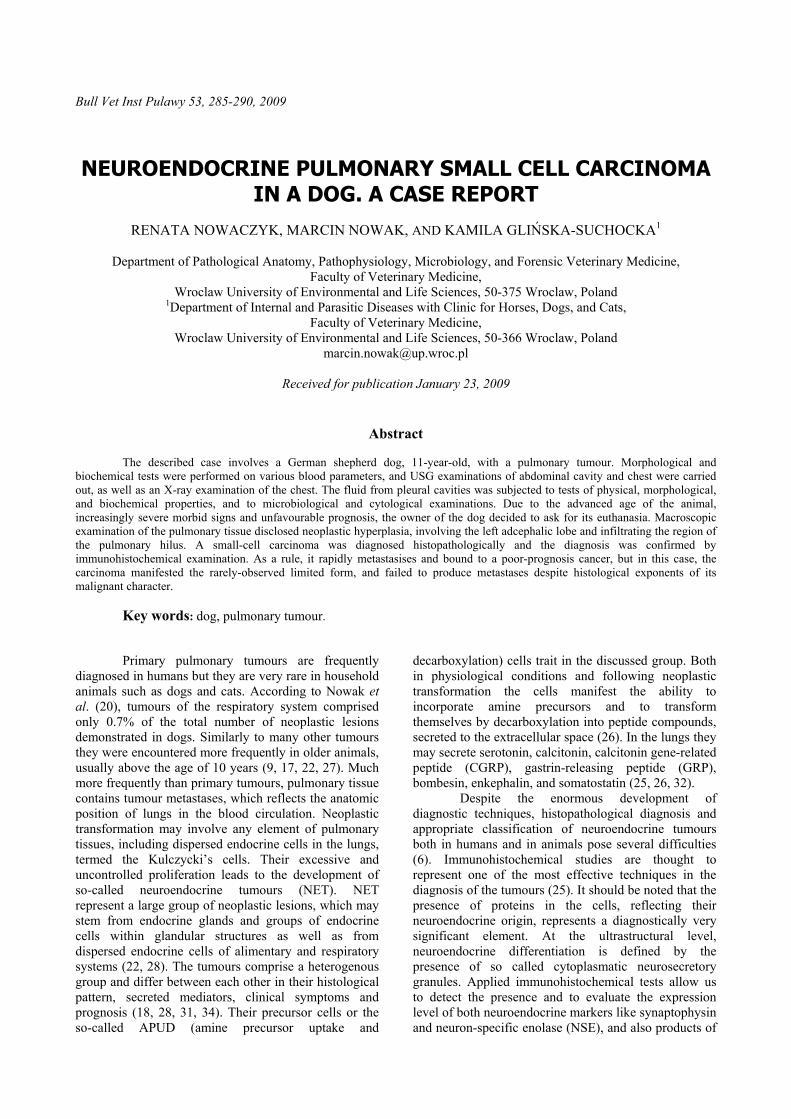
The character of the lesion suggested a complete airlessness of the pulmonary tissue in the ad-cranial part of the left lung, which, upon tapping the left pleural cavity, proved to be of red colour and manifested traits of an exudate. Sediment of the fluid contained numerous erythrocytes, lymphocytes, neutrophilic granulocytes, and individual desquamated mesothelial cells. Its microbiological tests failed to detect bacteria and cytological examination demonstrated no neoplastic cells. Due to the advanced age of the animal, increasingly severe morbid signs, and unfavourable prognosis, the owner of the dog decided to ask for its euthanasia. Autopsy disclosed good maintenance and nutrition condition in the animal. Available for the examination mucous membranes were cyanosed. The lungs demonstrated blood congestion. The left ad-cranial pulmonary lobe showed an uneven surface and showed scattered nodules of various size. The pleural cavity contained around 150 cm³ of blood-stained fluid. Both ventricles of the heart contained blood clots. The liver was enlarged and of a brown-red colour. The urinary bladder contained 100 cm³ of turbid urine. The prostate was slightly enlarged. Macroscopic examination of the pulmonary tissue disclosed neoplastic hyperplasia, involving the left adcephalic lobe and infiltrating the region of the pulmonary hilus (Fig. 3).
The altered lobe manifested solid consistency, its surface on a cross-section showed a lobular structure and a pink-red colour. Occasionally, small haemorrhagic foci and gray foci of necrosis were noted. Samples of the tumour were fixed for 24 h in a buffered 7% formalin, routinely processed to obtain paraffin blocks and cut to 4 µm thick sections. Histopathological appraisal of haematoxylin-eosin stained preparations took advantage of the currently-binding classification of tumours in the respiratory system (17). Under a microscope, the tumour of pulmonary tissue was qualified as small cell carcinoma in its limited form (LD). It was found to contain numerous small cells with scanty cytoplasm, hyperchromatic cell nuclei with a delicate, fine granular chromatin and small, poorly visible nucleoli (Fig. 4).
In some places the cells manifested a pronounced atypia and intensified mitotic activity, expressed by the presence of mitotic figures, which frequently were abnormal (Fig. 5).
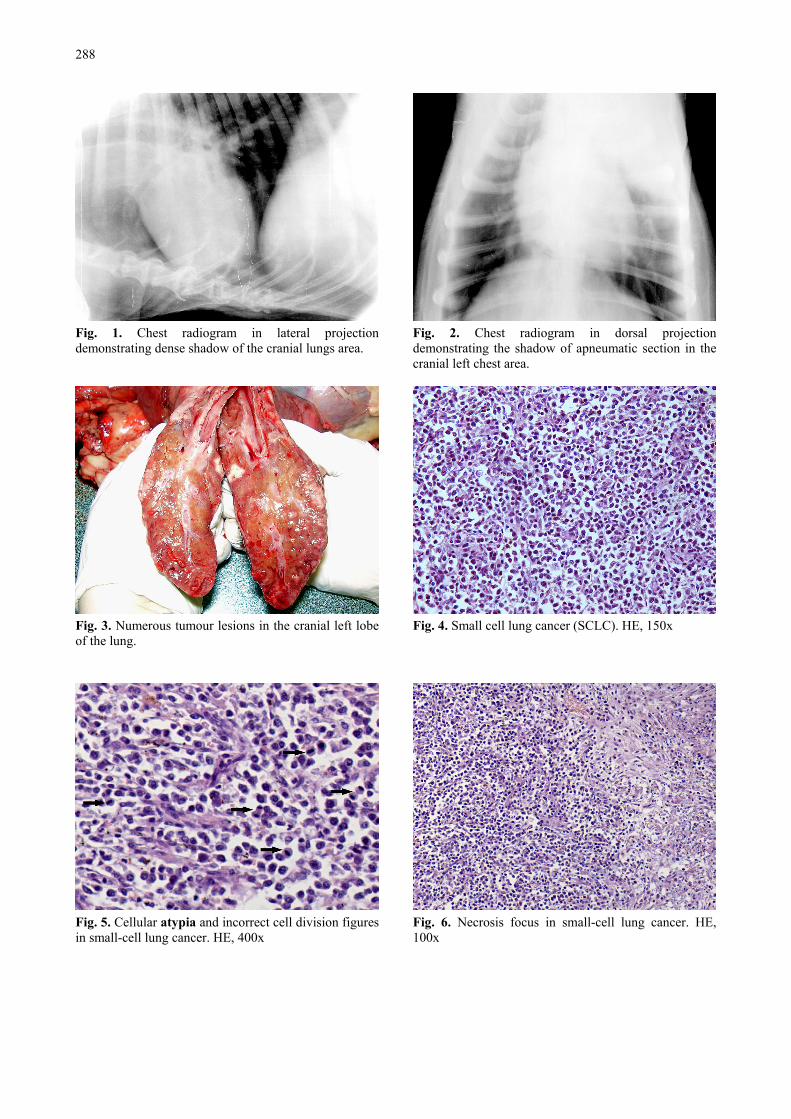
Frequently, small necrotic foci and haemorrhagic foci were seen (Figs 6, 7).
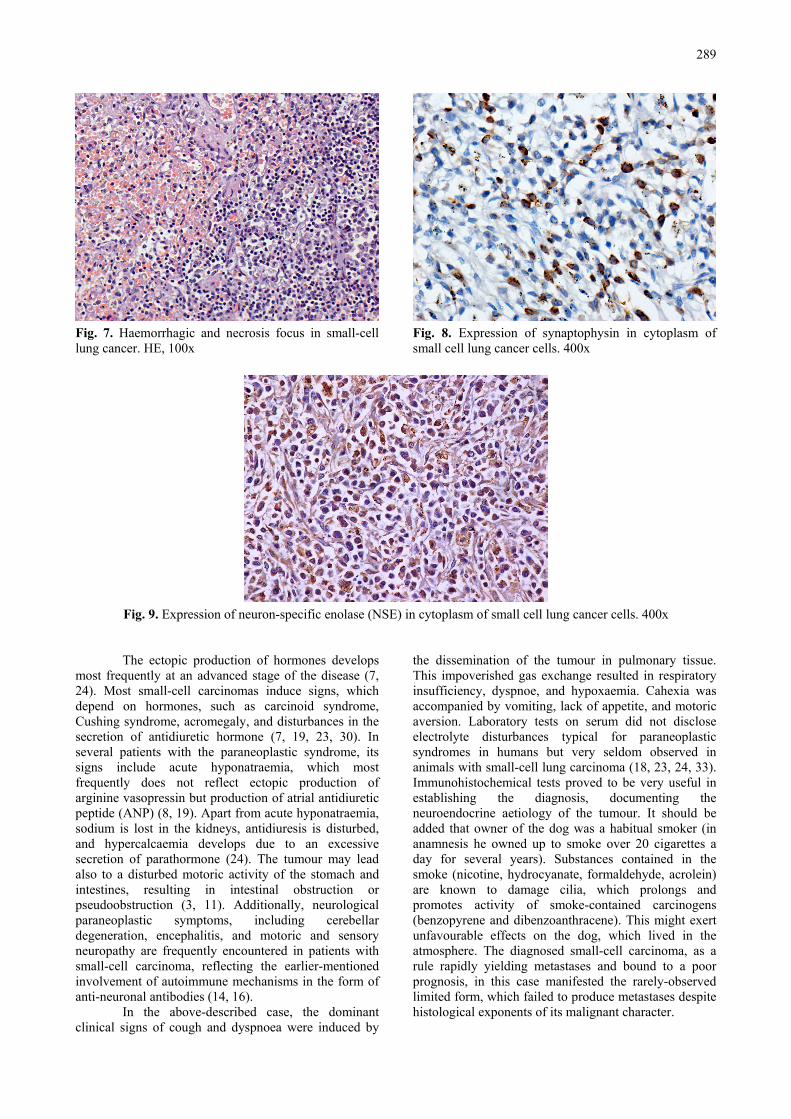
In the majority of tumour lesions, the cells formed solid areas, although regions were also encountered, which showed patterns of fascicles, separated by a fine stroma of connective tissue. In order to verify the results of the standard (haematoxylin-eosin) histopathological examination, an immunohistochemical technique was employed using a panel of antibodies identifying tumour cells of a neuronal and neuroendocrine origin (25, 32). The panel consisted of two monoclonal antibodies, directed to synaptophysin (clone SY38, dilution of 1:20, DakoCytomation) and NSE (clone BBS/NC/VI-H14, dilution of 1:150, DakoCytomation), respectively. All the reactions yielded positive results in the form of a delicate, fine-granular brownish reaction product, located mainly in
the cytoplasm of the tumour cells (Figs. 8, 9). This finding confirmed the preliminary diagnosis.
Neuroendocrine pulmonary tumours originate from neuroendocrine cells dispersed in bronchopulmonary epithelia. In humans, they account for around 20% of lung cancers. The tumours develop in four forms, as a typical carcinoid (TC), atypical carcinoid (AC), large-cell neuroendocrine carcinoma (LCNEC), or small-cell lung carcinoma (SCLC) (1, 6, 10, 34). The small cell lung carcinoma represents the neuroendocrine tumour most frequently diagnosed in the lungs. According to various authors, it accounts for 10% or even 25% of lung cancer cases (12, 33). Both small-cell and large-cell neuroendocrine lung carcinoma are characterised by a rapid growth, high metastatic potential, and a poor prognosis (1, 29, 31). The small-cell lung carcinoma is regarded to represent the most aggressive form of lung cancer with five-year survival rates below 5% (1, 5). The expansion of the carcinoma is expressed by massive infiltration of the surrounding tissues as well as by proximate and distant metastases (1, 12). The metastases develop most frequently in bones, bone marrow, liver, spleen, and the central nervous system (12, 22, 33). In humans, most small-cell lung carcinomas develop in elderly male smokers and tobacco smoking represents the most important risk factor (29, 33). Both in humans and animals most of patients are diagnosed at an advanced stage of the disease (29, 33).
Pulmonary neuroendocrine tumours are very rarely diagnosed in domestic animals. Cases of the tumours are reported more frequently in the naso-pharyngeal cavity, which reflects their location, providing much earlier symptoms as compared to pulmonary tumours (22, 28). Clinical signs of neuroendocrine tumours show low specificity (22, 26). Their intensity depends on the location of the tumour, its size and type of growth, the degree of infiltration in surrounding tissues and lymph nodes, and the presence of distant metastases (1, 12, 18). Symptoms of pulmonary cancer used to develop at a well-advanced stage of the disease and reflect most frequently infiltration of bronchi, pulmonary tissue, and surrounding structures in the chest (12, 33). The principal clinical symptoms include cough, haematoptysis, loss of body weight, dyspnoe, syndrome of the main ad-cranial vein (oedema of head, neck, and thoracic extremities), and terminally obturatory pneumonia (2, 27, 33). Due to neuroendocrine differentiation of small-cell lung carcinoma, it used to be accompanied by various symptoms forming the so called paraneoplastic syndrome (4, 7). In the course of small-cell carcinoma, the paraneoplastic syndrome develops, on one hand, due to ectopic production of hormones and, on the other hand, due to immunologically-conditioned destruction of tissues reflecting expression by the cancer cells of a neuronal antigen, which induces production of antibodies cross-reacting with nervous tissues.
288
Fig. 1. Chest radiogram in lateral projection demonstrating dense shadow of the cranial lungs area.
Fig. 3. Numerous tumour lesions in the cranial left lobe of the lung.
Fig. 5. Cellular atypia and incorrect cell division figures in small-cell lung cancer. HE, 400x
Fig. 2. Chest radiogram in dorsal projection demonstrating the shadow of apneumatic section in the cranial left chest area.
Fig. 4. Small cell lung cancer (SCLC). HE, 150x
Fig. 6. Necrosis focus in small-cell lung cancer. HE, 100x
289
Fig. 7. Haemorrhagic and necrosis focus in small-cell lung cancer. HE, 100x
Fig. 8. Expression of synaptophysin in cytoplasm of small cell lung cancer cells. 400x
Fig. 9. Expression of neuron-specific enolase (NSE) in cytoplasm of small cell lung cancer cells. 400x
The ectopic production of hormones develops most frequently at an advanced stage of the disease (7, 24). Most small-cell carcinomas induce signs, which depend on hormones, such as carcinoid syndrome, Cushing syndrome, acromegaly, and disturbances in the secretion of antidiuretic hormone (7, 19, 23, 30). In several patients with the paraneoplastic syndrome, its signs include acute hyponatraemia, which most frequently does not reflect ectopic production of arginine vasopressin but production of atrial antidiuretic peptide (ANP) (8, 19). Apart from acute hyponatraemia, sodium is lost in the kidneys, antidiuresis is disturbed, and hypercalcaemia develops due to an excessive secretion of parathormone (24). The tumour may lead also to a disturbed motoric activity of the stomach and intestines, resulting in intestinal obstruction or pseudoobstruction (3, 11). Additionally, neurological paraneoplastic symptoms, including cerebellar degeneration, encephalitis, and motoric and sensory neuropathy are frequently encountered in patients with small-cell carcinoma, reflecting the earlier-mentioned involvement of autoimmune mechanisms in the form of anti-neuronal antibodies (14, 16).
In the above-described case, the dominant clinical signs of cough and dyspnoea were induced by
the dissemination of the tumour in pulmonary tissue. This impoverished gas exchange resulted in respiratory insufficiency, dyspnoe, and hypoxaemia. Cahexia was accompanied by vomiting, lack of appetite, and motoric aversion. Laboratory tests on serum did not disclose electrolyte disturbances typical for paraneoplastic syndromes in humans but very seldom observed in animals with small-cell lung carcinoma (18, 23, 24, 33). Immunohistochemical tests proved to be very useful in establishing the diagnosis, documenting the neuroendocrine aetiology of the tumour. It should be added that owner of the dog was a habitual smoker (in anamnesis he owned up to smoke over 20 cigarettes a day for several years). Substances contained in the smoke (nicotine, hydrocyanate, formaldehyde, acrolein) are known to damage cilia, which prolongs and promotes activity of smoke-contained carcinogens (benzopyrene and dibenzoanthracene). This might exert unfavourable effects on the dog, which lived in the atmosphere. The diagnosed small-cell carcinoma, as a rule rapidly yielding metastases and bound to a poor prognosis, in this case manifested the rarely-observed limited form, which failed to produce metastases despite histological exponents of its malignant character.
290
References 1. Asamura H., Kameya T., Matsuno Y., Noguchi M., Tada
H., Ishikawa Y., Yokose T., Jiang S.X., Inoue T., Nakagawa K., Tajima K., Nagai K.: Neuroendocrine neoplasms of the lung: a prognostic spectrum. J Clin Oncol 2006, 24, 70-76.
2. Chan R.H., Dar A.R., Yu E., Stitt L.W., Whiston F., Truong P., Vincent M.D., Kocha W.I.: Superior vena cava obstruction in small-cell lung cancer. Int J Radiat Oncol Biol Phys 1997, 38, 513-520.
3. Cuillerier E., Coffin B., Potet F., Dapoigny M., Flourie B., Coffin J.C., Benyahia B., Bitoun A., Messing B., Rambaud J.C.: Paraneoplastic intestinal pseudo-obstruction revealing small cell lung carcinoma: "the anti-Hu syndrome". Gastroenterol Clin Biol 1998, 22, 346-348.
4. Dragan A.M., Simu G., Vaida T.: The histopathological and immunohistochemical diagnosis in small cell lung carcinoma. Rom J Morphol Embryol 1999-2004, 45, 91-95.
5. Fischer B., Arcaro A.: Current status of clinical trials for small cell lung cancer. Rev Recent Clin Trials 2008, 3, 40-61.
6. Flieder D.B.: Neuroendocrine tumors of the lung: recent developments in histopathology. Curr Opin Pulm Med 2002, 8, 275-280.
7. Gandhi L., Johnson B.E.: Paraneoplastic syndromes associated with small cell lung cancer. J Natl Comp Canc Netw 2006, 4, 631-638.
8. Gross A.J., Steinberg S.M., Reilly J.G., Bliss D.P. Jr., Brennan J., Le P.T., Simmons A., Phelps R., Mulshine J.L., Ihde D.C., Johnson B. E.: Atrial natriuretic factor and arginine vasopressin production in tumor cell lines from patients with lung cancer and their relationship to serum sodium. Cancer Res 1993, 53, 67-74.
9. Harkema J.R., Jones S.E., Naydan D.K., Wilson D.W.: An atypical neuroendocrine tumor in the lung of a Beagle dog. Vet Pathol 1992, 29, 175-179.
10. Hasleton P.S., Bostanci G.: Pulmonary carcinoid and related tumours. Rocz Akad Med Bialymst 1997, 42, 28-42.
11. Jun S., Dimyan M., Jones K.D., Ladabaum U.: Obstipation as a paraneoplastic presentation of small cell lung cancer: case report and literature review. Neurogastroenterol Motil 2005, 17, 16-22.
12. Junker K., Wiethege T., Muller K.M.: Pathology of small-cell lung cancer. J Cancer Res Clin Oncol 2000, 7, 361-368.
13. Kasprzak A., Zabel M., Biczysko W.: Selected markers (chromogranin A, neuron-specific enolase, synaptophysin, protein gene product 9.5) in diagnosis and prognosis of neuroendocrine pulmonary tumours. Pol J Pathol 2007, 58, 23-33.
14. Kawakami M., Bando M., Mato N., Nakaya T., Ohno S., Sugiyama Y.: A case of paraneoplastic cerebellar degeneration associated with small cell lung cancer showing marked response to intravenous immunoglobulin. Nihon Kokyuki Gakkai Zasshi 2008, 46, 325-330.
15. Krueger P., Nitz C., Foster R., MacDonald C., Gelber O., Lalehzadeh G., Goodson R., Winter J., Gelber C.: A new small cell lung cancer (SCLC)-specific marker discovered through antigenic subtraction of neuroblastoma cells. Cancer Immunol Immunother 2003, 52, 367-377.
16. Mason W.P., Graus F., Lang B., Honnorat J., Delattre J.Y., Valldeoriola F., Antoine J.C., Rosenblum M.K., Rosenfeld M.R., Newsom-Davis J., Posner J.B., Dalmau J.: Small-cell lung cancer, paraneoplastic cerebellar degeneration and the Lambert-Eaton myasthenic syndrome. Brain 1997, 120, 1279-1300.
17. Moulton J. E., von Tscharner C., Schneider R.: Classification of lung carcinomas in the dog and cat. Veterinary Pathology 1981, 18, 513-528.
18. Murakami Y., Kanazawa K., Okuno K., Maekawa S., Matsuda Y., Miyamoto Y., Nishimura Y., Kanomata N., Ohbayashi C., Hashimoto M., Akita H.: High-grade neuroendocrine carcinoma of the lung presenting an unusual spread mimicking pleural mesothelioma associated with dermatomyositis. Am J Med Sci 2004, 327, 227-230.
19. Müssig K., Horger M., Häring H.U., Wehrmann M.: Syndrome of inappropriate antidiuretic hormone secretion and ectopic ACTH production in small cell lung carcinoma. Lung Cancer 2007, 57, 120-122.
20. Nowak M., Madej J. A.: Prevalence of neoplasms in domestic animals in Lower Silesia in 2000-2004. Medycyna Wet. 2006, 62, 900-904.
21. Pankiewicz W., Minarowski L., Niklińska W., Naumnik W., Nikliński J., Chyczewski L.: Immunohistochemical markers of cancerogenesis in the lung. Folia Histochem Cytobiol 2007, 45, 65-74.
22. Patnaik A.K., Ludwig L.L., Erlandson R.A.: Neuroendocrine carcinoma of the nasopharynx in a dog. Vet Pathol 2002, 39, 496-500.
23. Radulescu D., Bunea D., Pripon S., Duncea C., Radulescu L.: Severe paraneoplastic hyponatremia and hypoosmolality in a patient with small-cell lung carcinoma: syndrome of inappropriate antidiuretic hormone secretion versus atrial natriuretic peptide or both? Clin Lung Cancer 2007, 8, 392-395.
24. Radulescu D., Pripon S., Bunea D., Ciuleanu T.E., Radulescu L.I.: Endocrine paraneoplastic syndromes in small cell lung carcinoma. Two case reports. J BUON 2007, 12, 411-414.
25. Rusch V.W., Klimstra D.S., Venkatraman E.S.: Molecular markers help characterize neuroendocrine lung tumors. Ann Thorac Surg 1996, 62, 798-809.
26. Rydzewska-Rosołowska A.E., Kasacka I., Sulewska A., Rudy A., Chyczewski L.: Pulmonary neuroendocrine cells in physiology and pathology. Folia Histochem Cytobiol 2001, 39, 58-63.
27. Saegusa S., Yamamura H., Morita T., Hasegawa A.: Pulmonary neuroendocrine carcinoma in a four-month-old dog. J Comp Pathol 1994, 111, 439-443.
28. Sako T., Shimoyama Y., Akihara Y., Ohmachi T., Yamashita K., Kadosawa T., Nakade T., Uchida E., Okamoto M., Hirayama K., Taniyama H.: Neuroendocrine carcinoma in the nasal cavity of ten dogs. J Comp Pathol 2005, 133, 155-163.
29. Serke M., Schönfeld N.: Diagnosis and staging of lung cancer. Dtsch Med Wochenschr 2007, 132, 1165-1169.
30. Shepherd F.A., Laskey J., Evans W.K., Goss P.E., Johansen E., Khamsi F.: Cushing's syndrome associated with ectopic corticotropin production and small-cell lung cancer. J Clin Oncol 1992, 10, 21-27.
31. Takei H., Asamura H., Maeshima A., Suzuki K., Kondo H., Niki T., Yamada T., Tsuchiya R., Matsuno Y.: Large cell neuroendocrine carcinoma of the lung: a clinicopathologic study of eighty-seven cases. J Thorac Cardiovasc Surg 2002, 124, 285-292.
32. Taneja T.K., Sharma S.K.: Markers of small cell lung cancer. World J Surg Oncol 2004, 2, 1186-1198.
33. Thammakumpee K., Juthong S., Viriyachaiyo V., Rittirak W., Tanomkiat W.: Clinical manifestation and survival of patients with small-cell lung cancer. J Med Assoc Thai 2007, 90, 1303-1308.
34. Travis W.D., Gal A.A., Colby T.V., Klimstra D.S., Falk R., Koss M.N.: Reproducibility of neuroendocrine lung tumor classification. Hum Pathol 1998, 29, 272-279.