Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
103 (2008) 40–51www.elsevier.com/locate/schres
Schizophrenia Research
Neurological basis of poor insight in psychosis:A voxel-based MRI study
Michael A. Cooke a, Dominic Fannon b, Elizabeth Kuipers a,c, Emmanuelle Peters a,c,Steven C. Williams d, Veena Kumari a,⁎
a Department of Psychology, Institute of Psychiatry, King's College London, London, UKb Division of Psychological Medicine, Institute of Psychiatry, King's College London, London, UK
c NIHR Biomedical Research Centre for Mental Health, South London and Maudsley Foundation NHS Trust, London, United Kingdomd Centre for Neuroimaging Sciences, Institute of Psychiatry, King's College London, London, UK
Received 11 December 2007; received in revised form 2 April 2008; accepted 11 April 2008
Available online 9 June 2008
Abstract
Background: As a reflection of poor insight, people with schizophrenia often disagree with carers and clinicians about whether(a) their experiences are abnormal, (b) they are mentally ill, and (c) they need treatment.Methods: This study used voxel-based morphometry to identify the associations between total and regional grey matter volumesand self-reported and observer-rated insight in 52 patients with schizophrenia or schizoaffective disorder. Thirty healthyparticipants were also studied.Results: There were positive associations in patients between (i) the ability to recognise experiences as abnormal and the total andright superior temporal gyrus grey matter volumes, (ii), awareness of problems (‘something wrong’) and the left precuneus greymatter volume and (iii) awareness of symptoms and attributing them to illness and grey matter volumes in the left superior–middletemporal gyrus and the right inferior temporal and lateral parietal gyri. The ‘recognition of the need for medication’ dimension didnot correlate with total or any regional grey matter volumes. Relative to controls, patients had less total and regional grey mattervolumes in the thalamus and middle occipital and superior temporal gyri.Conclusions: Lower grey matter volumes in the temporal and parietal regions that have been implicated in self-monitoring,working memory and access to internal mental states are associated with poor insight on certain dimensions in psychosis.© 2008 Elsevier B.V.Open access under CC BY license.
Keywords: Insight; Psychosis; Temporal lobe; Parietal lobe; Precuneus
1. Introduction
People with schizophrenia often disagree with theircarers and clinicians about whether (a) their experiencesand behaviours are abnormal, (b), they are mentally ill
⁎ Corresponding author. Department of Psychology (PO78), Insti-tute of Psychiatry, De Crespigny Park, London SE5 8AF, UK. Tel.:+44 207 848 0233; fax: +44 207 848 0860.
E-mail address: [email protected] (V. Kumari).
0920-9964 © 2008 Elsevier B.V.doi:10.1016/j.schres.2008.04.022
Open access under CC BY license.
and (c) they are in need of psychiatric treatment (David,1990). Such disagreements are considered to reflect poorinsight on the part of the patient. Apparent similaritiesbetween awareness deficits in neurological disorders andpoor insight in schizophrenia have led to the suggestionthat they have a comparable neurological basis (Amadoret al., 1991;McGlynn and Schacter, 1997). Evidence forthis suggestion has come primarily from studies showingsignificant relationships between measures of insight

41M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
and performance on neuropsychological tests of generalas well as specific cognitive domains (review, Cookeet al., 2005) which in turn are associated with the volume(review, Antonova et al., 2004) and functional responseof specific brain regions (review, Shad et al., 2007).
The use of modern neuroimaging methods hasallowed the neurobiological basis of insight in schizo-phrenia to be investigated more directly. Early neuroi-maging studies of insight, which tended to use globalbrain measurements, found relationships between poorinsight and ventricular enlargement (Takai et al., 1992)and smaller total brain volume (Flashman et al., 2000),although other studies did not replicate these relation-ships (David et al., 1995; Rossell et al., 2003).
Using more sophisticated methodologies, region ofinterest (ROI) studies have found a number of associa-tions between frontal brain regions and insight. Onestudy (Laroi et al., 2000) involving 21 patients withschizophrenia linked frontal cortical atrophy to poorinsight assessed with the Scale to Assess Unawarenessof Mental Disorders (SUMD, Amador et al., 1993).Another study (Flashman et al., 2001) examined theassociations between insight, again assessed with theSUMD, and eight frontal lobe sub-regions [frontal pole,superior frontal gyrus, middle frontal gyrus, inferiorfrontal gyrus, orbital frontal gyrus, precentral gyrus,gyrus rectus and cingulate] in a group of 15 patients withschizophrenia; the findings revealed large negativeassociations between awareness of symptoms andbilateral middle frontal gyrus volumes, and betweenmisattribution of symptoms and bilateral superior frontalgyrus volumes. Shad et al. (2004) reported smaller dor-solateral prefrontal cortex (DLPFC) volumes as well aspoor performance on the Wisconsin Card Sorting Test infirst-episode psychosis patients with poor insight (n=18;assessed with a single question, derived from the insightitem of the Hamilton Depression Rating Scale; Hamil-ton, 1960) relative to those with good insight (n=17). Arecent study by the same group involving 14 anti-psychotic naïve first-episode schizophrenia patients, andusing the SUMD to measure insight, found associationsbetween smaller right DLPFC volumes and impairedawareness of symptoms but also between larger rightmedial orbitofrontal volumes and misattribution ofsymptoms (Shad et al., 2006). More recently, we (Saparaet al., 2007) observed associations between smaller totalprefrontal grey matter volumes and lower insight into thepresence of illness and symptoms assessed using theBirchwood Insight Scale (Birchwood et al., 1994), andthe Schedule for the Assessment of Insight— Expanded(Kemp and David, 1997), in a sample of 28 chronicpatients with schizophrenia.
A number of recent studies have employed voxel-based morphometry (VBM) (Ashburner and Friston,2000; Good et al., 2001). For example, Ha and colleaguesreported a negative association between insight and greymatter concentrations bilaterally in the (middle) cingulateand temporal regions in 35 paranoid schizophreniapatients (illness duration 0.1 to 15 years) (Ha et al.,2004). However, this study used a unidimensionalmeasure of insight (the G12 item of the Positive andNegative Symptoms Scale, Kay et al., 1987), so it is notclear which aspects of insight may be related to greymatter volume in the temporal lobe. Bassitt and colleaguesfailed to find any relationship between insight assessedwith the SUMD and regional brain volumes examinedwith VBM in a sample of 50 chronic patients withschizophrenia (Bassitt et al., 2007).
The present study was designed to examine the asso-ciations between regional grey matter volumes and di-mensions of insight in schizophrenia assessed with a self-rated (Birchwood Insight Scale, Birchwood et al., 1994)and an observer-rated insight measure (the Schedulefor the Assessment of Insight — Expanded, Kemp andDavid, 1997). A factor analysis was undertaken to com-bine these measures, and is described in detail elsewhere(Cooke et al., 2007). The four factors derived from thisanalysis were: Awareness of and Attribution to Illness,Recognition of the Need for Medication, Awareness ofProblems, and Symptom Re-labelling (see Methods andmaterials for greater details). The focus of our study wason investigating associations between total and regionalgrey matter volumes and insight factors in a stable sampleof outpatients as it may be important to distinguish be-tween those individuals who lack insight in the presenceof acute psychopathology versus those who have stab-ilized or remitted and are still lacking in insight.
Based on previous data, we hypothesised that (i) greymatter volume in the frontal, anterior cingulate and tem-poral lobe regions would be positively associated withone or more insight factor scores, and (ii) grey mattervolume in the orbital/medial frontal region would beassociated with the Awareness of and Attribution toIllness insight factor. As the specific dimensions of insightunder investigation in our study were derived from afactor analysis, we expected them to associate primarilywith grey matter volumes in different brain regions.
2. Methods and materials
2.1. Participants
This was a cross-sectional study and involved 52 out-patients with schizophrenia or schizoaffective disorder

Table 1Demographic characteristics of study groups
Patients (n=52) Controls (n=30) Statistics
Mean (SD) Mean (SD)
[Range] [Range]
Gender (Male/Female) 40/12 24/6 χ21=0.105p=0.746
Age (Years) 38.35 (9.89) 32.13 (12.38) T80=2.495[19–61] [20–65] p=0.015
Handedness Edinburgh handedness 8.76 (2.27) 8.55 (1.31) T77=0.472Inventory a 0.5–10.0 5.5–10.0 p=0.638
Parental socioeconomic status (N=50) b (N=30) Some cells toosmall for χ2Professional 7 8
Intermediate 25 10Skilled: non-manual 3 7Skilled: manual 12 3Semi-skilled manual 1 1Unskilled manual 2 1Professional/intermediate 32 18 χ21=0.13Other 18 12 p=0.721
a Edinburgh handedness inventory (Oldfield, 1971).b Reliable information not available for two patients.
Table 2Clinical characteristics of patients (n=52)
Patient characteristic n
Diagnosis Schizophrenia 47Schizoaffective disorder 5
Medication Atypical antipsychotic 42Typical antipsychotic 10
Mean (SD) Range
Duration of illness Years 13.9 (9.6) 1–43PANSS scores Positive symptoms 16.5 (4.9) 7–28
Negative symptoms 18.0 (4.9) 7–32General psychopathology 31.8 (6.3) 18–48Total 66.2 (13.7) 39–108
42 M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
(diagnosed using the Structured Clinical Interview forDSM-IV Research Version; SCID-P, Spitzer et al., 1994).The patients included in this investigation were drawnfrom the larger sample of patients (n=65) described indetail in a recent paper (Cooke et al., 2007). Thirtyhealthy participants recruited from the local communitywere also studied for comparison purposes. Exclusioncriteria for healthy participants included a history ofmental illness, drug and alcohol abuse or a regularmedical prescription.
All patients were on stable doses of antipsychoticmedication for at least 3 months prior to taking part inthis study, and were in a stable (chronic) phase of theillness, living in the local community. The reasons fornon-inclusion of 13/65 patients (reported in Cookeet al., 2007) were: unsuitable for magnetic resonanceimaging (MRI; previous metalwork, claustrophobicor over-weight) (n=7), consent withdrawal prior toMRI (n=1), and movement artefacts /incomplete scan(n=5). Excluded patients did not differ significantlyfrom those included in the study in terms of age, pre-dicted IQ, symptoms, or any of the insight variables(all pN0.1).
Table 1 shows demographic characteristics of bothstudy groups and Table 2 shows clinical characteristicsof the patient sample.
The study procedures had the approval of the ethicscommittee of the Institute of Psychiatry and SouthLondon and Maudsley Foundation NHS Trust, London.All participants provided written informed consent.
2.2. Measures of insight
Insight was assessed using a self-rated instrument,the Birchwood Insight Scale (Birchwood et al., 1994),and an observer-rated instrument, the Schedule for theAssessment of Insight — Expanded (Kemp and David,1997). The SAI-E measures the dimensions of re-labelling of unusual mental events as abnormal, aware-ness of illness, and recognition of the need for treatmentincluded in the original SAI (David et al., 1992). TheSAI-E adds items regarding awareness of psychological/emotional changes, awareness that there is somethingwrong, awareness of the negative effects of mentalillness, and attribution of symptoms to a mental illness.Like the SAI-E, the BIS is based on David's (1990)

43M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
model of insight and measures the same three coredimensions of insight as the original SAI (David et al.,1992).
These two measures were combined, via a factoranalytic approach, to generate four factors of insight,namely, Awareness of and Attribution to Illness, Re-cognition of the Need for Medication, Awareness ofProblems and Symptom Re-labelling as described indetail by Cooke et al. (2007). Briefly stated, the Aware-ness of and Attribution to Illness factor includes itemsrelating to awareness of illness, together with the attri-bution of problems in general as well as symptomsspecifically to a mental illness. The Recognition of theNeed for Medication factor includes items relating toawareness of the need for treatment, specifically med-ication. The Awareness of Problems factor includesitems related to awareness of problems and the need toseek help. More specifically, the items which refer tobeing aware that one needs to take medication load onRecognition of the Need for Medication, whereas theitems which refer to the awareness of the need to seekhelp more generally, and being aware that there was‘something wrong’ load on Awareness of Problemsfactor. The Symptom Re-labelling factor comprisesitems referring to the ability to recognise that experi-ences are abnormal and label them as such but notperceive them as a problem or an illness. An individualmay be aware that his/her symptomatic experiences areunusual or internally generated, but not attribute them toa mental illness and therefore score highly on theSymptom Re-labelling factor but not on Awareness ofand Attribution to Illness.
2.3. MRI data acquisition
Structural MRI brain scans were acquired using a 1.5Tesla GE N/Vi Signa system (General Electric, Mil-waukee WI, USA) at the Maudsley Hospital, London. Aquadrature birdcage head coil was used for RF trans-mission and reception. Head movement was limited byfoam padding within the head coil and a restraining bandacross the forehead. Initially, a series of sagittal and axialfast gradient echo scout images were acquired in order tocorrect for head tilt and to orient subsequent imagesrelative to the anterior-commissure/posterior-commissureline and the interhemispheric fissure (TR=200 ms,TE=4.2 ms, theta=90°, field of view=24 cm, slicethickness=5 mm, slice gap=2.5 mm, 256×192 acquisi-tion matrix, one data average). The whole brain was thenscanned with a 3-D inversion recovery prepared fastspoiled GRASS T1-weighted dataset. These T1-weightedimages were obtained in the axial plane with 1.5 mm
contiguous sections. TR was 18 ms, TI was 450 ms, TEwas 5.1 ms and the flip angle was 20° with one dataaverage, a 256 × 256 × 128 pixel matrix and a0.937mm×0.937mm in-plane resolution. Image contrastfor all datasets was chosen with the aid of a software toolfor optimizing image contrast (Simmons et al., 1996).
2.4. Optimised voxel-based morphometry procedure
All structural brain data were analysed using Stat-istical Parametric Mapping — version 2 (SPM2, Well-come Department of Imaging Neuroscience, London;http://www.fil.ion.ucl.ac.uk/spm).
A series of study-specific, customised templates werecreated in preference to the standard SPM2 templates inorder to minimise any scanner-specific biases and toprovide templates appropriate to characteristics of thesample (Good et al., 2001). For the creation of thecustomised whole brain (T1) template, each structuralMRI image was registered to the standard SPM2 T1template using a 12 parameter affine transformation.These normalised images were then smoothed with an8 mm full width at half maximum (FWHM) isotropicGaussian kernel, and averaged to create the customisedT1 template with a resolution of 1 mm×1 mm×1 mm.
The (unsmoothed) normalised T1 images were thensegmented into their grey matter, white matter and ce-rebrospinal fluid components using the standard SPM2grey matter, white matter and cerebrospinal fluid pro-bability maps. Each individual segmented image wasthen automatically cleaned to remove non-brain tissueand smoothed with an 8 mm FWHM isotropic Gaussiankernel. The smoothed images were then averaged tocreate customised grey matter, white matter and ce-rebrospinal fluid templates in standard stereotactic space(Good et al., 2001).
The original T1 brain images were normalised to thecustomised T1 template using a 12 parameter affinetransformation and then segmented into grey matter,white matter and cerebrospinal fluid components usingthe customised grey matter, white matter and cerebrosp-inal fluid templates. After automatically cleaning thesesegmented images to remove non-brain tissue, each greymatter image was re-normalised to the study-specificgrey matter template using (i) a 12 parameter affinetransformation and (ii) a non-linear transformation com-prising a combination of smooth spatial basis functions(Ashburner and Friston, 1999) to account for globalnon-linear shape differences (16 iterations, 25 mm cut-off, medium regularisation). The parameters used tonormalise each segmented grey matter image are thenapplied to the corresponding native T1 image, to derive

44 M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
a whole brain image which is normalised to standardisedstereotactic space. Using the parameters from thenormalisation of the cleaned segmented grey matterimage to the grey matter template prevents non-brainvoxels (such as the skull, which is present in T1 images)from contributing to errors in spatial normalisation,‘optimising’ the process. These normalised whole brainT1 images, ‘optimised’ through using the parametersderived from the normalisation of grey matter images toa customised template, were used in the next step. Ineffect, the preceding stages of the process were con-catenated into the normalisation of the native T1 imagesto maximise registration accuracy.
The initial normalisation of the T1 images to the T1template prior to segmentation can be influenced bynon-brain voxels (as the cleaning of these voxels frombrain images can only be done once the images havebeen segmented, which must itself be preceded by aninitial normalisation). The optimally normalised T1images were therefore re-segmented into grey matter,white matter and cerebrospinal fluid using the custo-mised grey matter, white matter and cerebrospinal fluidtemplates. These images are then cleaned to removenon-brain tissue to derive the optimally normalisedsegmented images for each subject.
In order to account for the volumetric changesintroduced by non-linear transformations, images weremodulated by multiplying the ‘relative volume’ (theextent of distortion generated by non-linear transfor-mations) by the intensity value at each voxel in the(unsmoothed) optimally normalised, cleaned and seg-mented grey matter image. Differences between imagesin modulated intensities therefore reflect regionaldifferences in the absolute amount (volume) of greymatter (Good et al., 2001). The images were thensmoothed with a 12 mm FWHM isotropic Gaussiankernel, as recommended by Ashburner and Friston(2000) to ensure that the data are valid for the use ofparametric statistical tests. The voxel size in theseimages was 1 mm×1 mm×1 mm.
2.5. Data analysis
The total grey matter volume for each individual wascalculated from the unsmoothed modulated segmentedimages (which have the same grey matter volume as thesegmented images in native space) and examined for (a)difference between patients and controls in total greymatter volume using analysis of variance with andwithout controlling for age and gender, and (b) thecorrelations between total grey matter volumes andinsight measures (Pearson's r used for insight variables
distributed normally, Spearman rank order correlationsused when insight measures not normally distributed).Following the observation of positive associationsbetween the total grey matter volume and the Awarenessof Problems and Symptom Re-labelling factors of in-sight, we examined the relationships between (a) pre-dicted IQ (assessed with National Adult Reading Test,NART; Nelson andWillison, 1991) and total grey mattervolume, and (b) predicted IQ and insight factors. Sub-sequent to the observations of significant positiveassociations between predicted IQ and the total greyvolume, and between predicted IQ and the Awareness ofProblems and Symptom Re-labelling factors of insight,we re-evaluated the relationships between the total greymatter volume and relevant insight factors (Awarenessof Problems and Symptom Re-labelling) after control-ling for predicted IQ.
Regional differences between patients and controls ingrey matter volume were examined by analysing groupdifferences in modulated grey matter images. Both ageand gender were controlled for in these analyses due totheir known influence on brain structure (Coffey et al.,1998). To examine insight-regional grey matter associa-tions in patients, a separate regression analysis wascarried out for each insight factor. The effect of globalgrey matter volume was controlled for in the regression,and insight factor score was entered as an independentvariable. Each within-group analysis of modulated greymatter images comprised two contrasts: one to test forpositive associations between regional absolute greymatter volumes and insight measures, and another to testfor negative associations. In order to exclude voxelswhich are unlikely to be grey matter from the analysesand reduce the number of comparisons being made, onlyvoxels which had an absolute intensity of at least 0.05(5%) in all grey matter images being analysed (i.e.smoothed, modulated normalised images) were includedin each analysis.
The threshold for statistical parametric maps in thisstudy was set at pb0.001, uncorrected (using the Tstatistic in voxel-wise analyses). The threshold for localmaxima to be considered significant was set at pb0.05,family-wise error (FWE) corrected. The procedure forcorrection for multiple comparisons in SPM2, however,was originally designed for the analysis of functionaldata, and is overly strict when applied to structural data(Sowell et al., 1999). Relationships between insight andbrain regional volumes where clusters were larger than100 voxels with a local maxima reaching TN4.50(pb0.0001) were therefore treated as being of interest.If these clusters were in a region which was hypothe-sised in advance to be related to insight, small volume

Table 3Descriptive statistics of insight factors
Insight factors
AAI a RNM AP SRa
n 45 51 52 45Mean 9.86 4.78 4.31 3.39SD 4.98 1.78 2.02 1.93Minimum 0 0 0 0Maximum 16 6 6 6
Higher scores in each measure reflect greater insight. The maximumscores are the maximum scores possible for each factor.AAI — Awareness of and Attribution to Illness.RNM — Recognition of the Need for Medication.AP — Awareness of Problems.SR — Symptom Re-labelling.a 7 patients did not possess any marked symptoms for which insight
could be rated.
45M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
correction (SVC) was applied to determine whether acluster is significant correcting for multiple comparisonswithin a locally defined volume rather than the wholebrain. A 10 mm radius sphere centred on the maximavoxel was used in SVC analyses.
The values representing the percentage of total greyvolume under a smoothing kernel for each patient atpeak voxels of the regions that showed an associationwith insight factors (see Results) were extracted andexamined first using Pearsons' correlations and then re-examined using partial correlations after partialling outthe effect of duration of illness in the observed asso-ciations (within SPSS). All significant associations re-mained significant with very similar p values after wepartialled out the effect of duration of illness (resultsnot presented further) most likely because neither theInsight factors nor the percentages of total grey volumein relevant regions were correlated with the duration ofillness in this sample (all pN0.10).
Finally, we explored possible associations betweeninsight factors and white matter and CSF volumes(using the same methods and thresholds for significancetesting as described above for the grey matter volume).The global volumes of white matter and CSF did notcorrelate significantly with any of the insight factors.The analyses to explore associations between regionalwhite matter and each of the insight factor scores alsodid not reveal any significant relationships (all Tb4.5;results not presented further).
3. Results
3.1. Patients versus controls
3.1.1. Global grey matter volumePatients had significantly smaller global grey matter
volume (in litres) than healthy controls (patients'mean=0.716, SD=0.066; controls' mean= 0.762,SD=0.070; F=9.299, df=1,80, p=0.003). This differ-ence remained significant after controlling for age andgender (F=6.607, df=1,78, p=0.012).
3.1.2. Regional grey matter volumePatients had significantly less grey matter volume in
two regions: the first had its local maximum voxel in theright brainstem [(x=9, y=−28, z=,−8), T(78)=5.54,number of contiguous voxels=8540, p=0.004 FWEcorrected] and extended into the dorsal thalamus, andthe second was located in the left middle occipital gyrus[BA 19, centred at −53,−82,−1, T(78)=4.80, numberof contiguous voxels=24468, p=0.012 FWE cor-rected]. There was a trend towards less grey matter
volume in the right superior temporal gyrus [STG, BA38, centred at 55,16,−8, T(78)=4.34, number of con-tiguous voxels=17,680, p=0.079 FWE corrected].
There were no regions showing more grey mattervolume in patients relative to controls (no voxels reachedsignificance at the pb0.001 uncorrected level).
3.2. Relationships between insight and GM volume
The mean scores for the four insight factors aredescribed in Table 3. The associations reported betweeninsight factors and MRI values are all positive — i.e.between greater grey matter volume and higher insightscores (see Table 4).
3.2.1. Global grey matter volumeGreater global grey matter volume was significant-
ly associated with higher Awareness of Problems(rho=0.275, pb0.05) and higher Symptom Re-labellingscores (r=0.315, pb0.05). The Awareness of andAttribution to Illness and Recognition of the Need forMedication factors also showed positive associationswith grey matter volume, but were not significant(r=0.151 and r=0.186 respectively, all pN0.1).
Predicted IQ correlated positively with total greymatter volume (r=0.385, p=0.006, n=50) and also withthe Symptom Re-labelling (r=0.328, p=0.030) andAwareness of Problems scores (rho=0.330, p=0.019)but did not correlate significantly (pN0.1) with theAwareness of and Attribution to Illness, and Recognitionof the Need for Medication scores. The associationbetween the total grey matter volume and relevant in-sight factors (Awareness of Problems and Symptom Re-labelling) became non-significant (pN0.1) after control-ling for predicted IQ.

Table 4Relationships between grey matter volume and insight factors
Brain region BA Clustersize⁎ (voxels)
Maxima voxels T value p valueuncorrected
p value FWEcorrected
p value SVC^corrected
x y z
Awareness of and Attribution to IllnessLeft STG 21 2214 −67 1 6 4.83 b0.001 0.115 b0.001Left MTG 21 1487 −73 −42 −4 4.52 b0.001 0.242 0.001Right ITG 21 709 71 −5 −23 4.68 b0.001 0.166 0.001Right inferior parietal lobule 40 6445 72 −38 32 4.63 b0.001 0.187 0.001Right supramarginal gyrus 63 −58 34 4.50 b0.001 0.251 0.001
Awareness of ProblemsLeft precuneus 7 1581 −2 −65 66 5.01 b0.001 0.049
Symptom Re-labellingRight STG 21 3775 66 −7 −8 4.56 b0.001 0.224 0.001
BA — Brodmann area.FWE — Family-Wise Error.⁎Cluster size at the uncorrected threshold of p=0.001.^Small Volume Correction — FWE corrected for 10 mm radius sphere search volume.STG — Superior temporal gyrus.MTG — Middle temporal gyrus.ITG — Inferior temporal gyrus.
46 M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
3.2.2. Regional grey matter volume
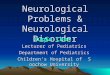
3.2.2.1. Awareness of and Attribution to Illness. Therewas an association between higher score on Awarenessof and Attribution to Illness and greater grey mattervolume in the left STG, as well as amore posterior regionin the left middle temporal gyrus. In the right hemi-sphere, this factor was associated with the volume of theright inferior temporal gyrus and a large lateral parietalcluster with two local maxima: one in the right inferiorparietal lobule and another in the right supramarginalgyrus (see Table 1 and Fig. 1).
3.2.2.2. Recognition of the Need for Medication.There were no significant correlations between thisfactor score and regional grey matter volumes (allvoxels Tb4.5 and pN0.3, FWE corrected).
Fig. 1. Association between Awareness of and Attribution to Illness score atemporal gyrus, and right inferior parietal lobule/supramarginal gyrus.
3.2.2.3. Awareness of Problems. There was a sig-nificant association between higher score and greatergrey matter volume in the left precuneus (see Table 3and Fig. 2).
3.2.2.4. Symptom Re-labelling. There was an associa-tion between higher score and greater absolute greymatter volume in the right STG (see Table 3 and Fig. 3).
4. Discussion
A number of studies have suggested that insight inschizophrenia has a structural brain basis. Frontal brainregions have been particularly implicated, although ROIstudies have rarely examined regions outside of thefrontal lobes. This investigation aimed to extend theliterature by using VBM, an automated approach which
nd absolute volume of the left superior temporal gyrus, right inferior

Fig. 2. Association between greater absolute grey matter volume in the left precuneus and the Awareness of Problems insight factor.
47M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
covers the whole brain, to examine the structural braincorrelates of clinical insight and its specific dimensions.
4.1. Patients versus controls
The patient group had a significantly smaller totalgrey matter volume compared to controls, a differencewhich survived controlling for age and sex. This result isconsistent with the global reduction in grey mattervolume in individuals with schizophrenia found in ameta-analysis (Wright et al., 2000). Regionally, therewere significant grey matter reductions in patients in a
Fig. 3. Association between greater absolute grey matter volume in the rigassociated) and the Symptom Re-labelling insight factor.
right brainstem/dorsal thalamus cluster and the leftmiddle occipital gyrus (BA 19), as well as a trendtowards a reduction in the right STG (BA 38). Thesefindings are consistent with those of a number ofprevious VBM studies. Four studies have found re-ductions in grey matter in the right thalamus in patientswith schizophrenia compared to controls (Hulshoff Polet al., 2001; Marcelis et al., 2003; Salgado-Pineda et al.,2003, 2004), while left middle occipital gyrus reduc-tions have been found in one previous study (Moorheadet al., 2004). Reductions in the right STG are one of themost replicated VBM findings (Sigmundsson et al.,
ht temporal gyrus (the two other clusters seen were not significantly

48 M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
2000; Hulshoff Pol et al., 2001; Job et al., 2002; Kubickiet al., 2002, Spalletta et al., 2003; Moorhead et al.,2004). The STG finding is also in accord with findingsof ROI studies (Shenton et al., 2001). Reductions in theright STG in schizophrenia are thought to be particularlyimportant in the aetiology of auditory hallucinations, asSTG volume has been found to correlate with theseverity of such experiences (Barta et al., 1990). How-ever, it should be noted that, although no healthyparticipant or patient was abusing drugs or alcohol at thetime of their participation, there was a past history ofdrug abuse in a proportion of patients and this may haveled or contributed to some of the observed grey matterdifferences between patients and controls.
4.2. Insight and grey matter volume
It was hypothesised that insight factors would becorrelated with total grey matter volume. This hypoth-esis was supported by the significant correlations be-tween total grey matter volume and both the Awarenessof Problems and Symptom Re-labelling factors. How-ever, predicted IQ was also correlated with the total greymatter volume and the Awareness of Problems andSymptom Re-labelling factors and the associationsbetween total grey matter volume and the Awarenessof Problems and Symptom Re-labelling factors becamenon-significant after controlling for predicted IQ. Gen-erally, our findings are consistent with previous datashowing (a) a relationship between IQ and total greymatter volume (review, Antonova et al., 2004) and (b) arelationship between insight and general cognitive abi-lity in psychosis (reviews, Cooke et al., 2005; Alemanet al., 2006). Our findings, however, also suggest thatthe total brain volume has a noticeable association onlywith Symptom Re-labelling and Awareness of Problemsdimensions of insight and this effect is mediated via itsassociation with general cognitive ability.
A number of previous (mainly ROI) studies havefound relationships between dimensions of insight andthe volume of specific frontal lobe regions. However, nosignificant relationships were found between the insightfactors and frontal lobe regions in this study. Instead, wefound associations between insight factors and a numberof temporal and parietal lobe areas. Previous ROIstudies have not measured parietal or temporal loberegions, making it impossible for them to identifycorrelations between the volume of these regions andinsight. Furthermore, anosognosia, which is held bysome to be the neurological analogue of poor insight(Amador et al., 1994), is associated with lesions tosubcortical, parietal lobe and temporal lobe structures,
as well as with frontal lesions (meta-analytic review, Piaet al., 2004), suggesting that it is not a purely frontalphenomenon.
The strongest relationship found in this investigationwas between the Awareness of Problems score and thevolume of the left precuneus, located in the medialparietal lobe. This relationship survived FWE correctionfor multiple comparisons without the need for smallvolume correction. A number of studies have demon-strated that grey matter volumes of specific brain re-gions are closely associated with behavioural measuresof their function both in healthy people and in patientswith schizophrenia (review, Antonova et al., 2004).Although the precuneus has not been investigated inprevious structural imaging (ROI) studies within thecontext of schizophrenia (as discussed by Antonovaet al., 2004), functional imaging studies in healthypeople have revealed a number of observations con-cerning its functions that allow us to postulate how itmight play a role in this particular dimension of insightin psychosis. Specifically, a network involving the pre-cuneus and medial prefrontal regions has been proposedas the mechanism through which personal identity andpast personal experiences are interlinked, allowing aperson to move between representation and awarenessof the self (Andreasen et al., 1995). Functional magneticresonance imaging studies have shown precuneusactivation in comparing self to non-self representations,including judging whether psychological/personalitytrait adjectives were self-referential (Kircher et al.,2000, 2002). Positron emission tomography studies toohave shown precuneus activation when participants re-flect about their own personality traits and physicalappearance (Kjaer et al., 2002), and a linear relationshipbetween precuneus activation and the degree to whichthe retrieval of previous retrieval of psychological traitswas self-referential (Lou et al., 2004). These observa-tions indicate that the precuneus is either involved inassigning first-person perspective (e.g. awareness ofone's own mental states) (Vogeley and Fink, 2003), ormore generally in internal representation through mentalimagery and episodic/autobiographical memory retrie-val (Cavanna and Trimble, 2006; Cavanna, 2007) andcould explain why the volume of the left precuneus wasassociated with the Awareness of Problems. If an in-dividual with schizophrenia has a deficit in an area of thebrain which mediates the ability to access representa-tions of his/her own mental states, he/she may not beable to identify that these mental states are problematic,and may therefore be unaware that there is ‘somethingwrong’. We (Cooke et al., 2007) had previously foundan association between lower awareness of problems

49M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
and ‘preference for mental disengagement’ coping style.This raises an interesting possibility that precuneus de-ficit causes mental disengagement via reducing aware-ess of one's own mental states.
A large cluster in a different parietal lobe region wascorrelated with Awareness of and Attribution to Illnessfactor score. This cluster had maxima voxels in the rightinferior parietal lobule and right supramarginal gyrus,and was significant after small volume correction hadbeen applied. This area of the parietal cortex has a well-established role in visual attention (review, Culham andKanwisher, 2001) and working memory/executive func-tioning tasks that also activate the DLFPC (Bor andOwen, 2007). It is plausible that as well as being in-volved in awareness of sensory information, the rightinferior parietal cortex is involved in awareness ofillness via the same cognitive dysfunctions, namelydeficits in executive working memory and cognitive setshifting, that link the DLPFC deficit to poor insight inpatients with schizophrenia (review, Shad et al., 2007).In our recent study (Cooke et al., 2007), we had found‘Awareness of and Attribution to Illness’ factor score tobe correlated with ‘planning’ and ‘use of instrumentalsocial support’ styles of coping which may also rely onthe same set of cognitive functions. It is also interestingto note that damage to the right parietal cortex hasfrequently been linked to anosognosia in neurologicaldisorders (Pia et al., 2004; Vuilleumier, 2004).
The present investigation found relationships be-tween the volume of a number of temporal lobe regionsand the Awareness of and Attribution to Illness insightfactor. Ha et al. (2004) had previously reported anassociation between insight, as measured by the PANSSG12 item, and a temporal lobe grey matter cluster. Ourfindings suggest a role for grey matter in the temporallobe specifically in the awareness of symptoms andattributing them to an illness rather than in insight acrossall dimensions. In the present investigation, two clustersin the left temporal lobe were significant after smallvolume correction had been applied: one with a maximavoxel in the left STG, and another more posterior clusterwith a maxima voxel in the left middle temporal gyrus.A further cluster in the right inferior temporal gyrus wasalso significant after applying small volume correction.A cluster with its maxima voxel in the right middletemporal gyrus which extended into the right STG wasalso associated with the Symptom Re-labelling factorand was significant after small volume correction hadbeen applied. Functional neuroimaging studies havedemonstrated the role of the STG in the cortical networksubserving the interpretation, production and self-mon-itoring of speech and language in healthy people
(review, Pearlson, 1997). Activation of this region hasbeen found to correlate with severity of auditoryhallucinations in people with schizophrenia (Bartaet al., 1990; review, Raveendran and Kumari, 2007),supporting the view that auditory hallucinations reflectimpaired self-monitoring of internal speech (Frith,1992). The correlations found in this study suggestthat the self-monitoring deficits in schizophrenia, whichassociated with the STG, may extend beyond an inabi-lity to monitor internal speech, to an inability to monitorwhether mental experiences are abnormal, and whetherone is experiencing a psychiatric illness.
Shad et al. (2007) have very recently proposed thatreduced volumes of the right DLPFC and/or the rightparietal regions underlie unawareness of symptoms(anosognosia), while relatively increased volumes of theorbitofrontal cortex underlies misattribution of symp-toms (dysnosgnoia). Our data provide support for thetheorised parietal cortex–insight relationship. The lackof any inverse relationship between any dimensions ofinsight and brain volumes especially of the orbitofrontalregion may be due to the fact that all our patients weremedicated and chronic outpatients. Very recently,Lacerda et al. (2007) using the same ROI proceduresas used in studies by Shad and colleagues have reportedlarger orbitofrontal volume in first-episode schizophre-nia patients. Patients diagnosed with schizophrenia whohave long term difficulties on the other hand are re-ported to show reduced grey matter volume in thisregion (Kuperberg et al., 2003). It is thus possible that amisattribution of symptoms–larger orbitofrontal vol-umes relationship is specific to first-episode patients.However, unlike the findings of ROI studies, greymatter volume in no frontal region associated positivelyor negatively with insight dimensions in this study. This,at least in part, may be related to the methodologicaldifferences between voxel-averaged, landmark-basedROI analyses and the single, voxel-by-voxel wholebrain VBM measurements (Gilulani et al., 2005).
We did not find any association between the ‘Re-cognition of the Need for Medication’ factor and total orregional grey matter volumes. Although we earlier sug-gested that this insight dimension may be less biologicalin nature and better correlated with psychological mech-anisms, such as denial, poor self-esteem or a copingstyle (Sapara et al., 2007), our recent study did not showan association between this dimension and denial, poorself-esteem or a particular coping style (Cooke et al.,2007). The biological, psychological and/or socialvariables that influence, or may be associated with,this particular dimension of insight remain unclear atpresent.

50 M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
5. Conclusions
The findings of this study demonstrate positive re-lationships between total grey matter volume and greymatter volumes in a number of regions and specificdimensions of insight in psychosis. Specifically, greaterleft precuneus grey matter volume, perhaps via facil-itating increased access to own mental states, has apositive association with awareness of problems and theneed to seek help. Greater grey matter volumes in theSTG, a region implicated in self-monitoring and perhapsin an extended capacity in the ability to monitor whethermental experiences are abnormal and whether one isexperiencing a psychiatric illness, and the lateral parietalcortex, which has a role in working memory/executivefunctioning, are associated with higher awareness ofsymptoms and attributing them to an illness.
Role of the funding sourceThe sponsor (the Wellcome Trust) had no role in the study design;
in the collection, analysis and interpretation of data; in the writing ofthe report; or in the decision to submit the paper for publication.
ContributorsVeena Kumari, Elizabeth Kuipers, Emmanuelle Peters, Steven C
Williams and Michael Cooke designed the study and obtained thefunding.Michael Cooke collected the data. Dominic Fannon performedthe clinical diagnostic interviews. Michael Cooke undertook thestatistical analysis. Veena Kumari andMichael Cooke prepared the firstdraft. All authors contributed to and approved the final manuscript.
Conflict of interestThe authors declare no conflict of interest.
AcknowledgementsThis research was funded by the Wellcome Trust (067427/z/02/z &
072298/z/03/z).
References
Aleman, A., Agrawal, N., Morgan, K.D., David, A.S., 2006. Insight inpsychosis and neuropsychological function: meta-analysis. Br. J.Psychiatry 189, 204–212.
Amador, X.F., Strauss, D.H., Yale, S.A., Gorman, J.M., 1991.Awareness of illness in schizophrenia. Schizophr. Bull. 17,113–132.
Amador, X.F., Strauss, D.H., Yale, S.A., Flaum, M.M., Endicott, J.,Gorman, J.M., 1993. Assessment of insight in psychosis. Am. J.Psychiatry 150, 873–879.
Amador, X.F., Flaum, M., Andreasen, N.C., Strauss, D.H., Yale, S.A.,Clark, S.C., Gorman, J.M., 1994. Awareness of illness inschizophrenia and schizoaffective and mood disorders. Arch.Gen. Psychiatry 51, 826–836.
Andreasen, N.C., O'Leary, D.S., Cizadlo, T., Arndt, S., Rezai, K.,Watkins, G.L., Ponto, L.L., Hichwa, R.D., 1995. Remembering thepast: two facets of episodic memory explored with positronemission tomography. Am. J. Psychiatry 152, 1576–1585.
Antonova, E., Sharma, T., Morris, R., Kumari, V., 2004. Therelationship between brain structure and neurocognition inschizophrenia: a selective review. Schizophr. Res. 70, 117–145.
Ashburner, J., Friston, K.J., 1999. Nonlinear spatial normalizationusing basis functions. Hum. Brain. Mapp. 7, 254–266.
Ashburner, J., Friston, K.J., 2000. Voxel-based morphometry — themethods. Neuroimage 11, 805–821.
Barta, P.E., Pearlson, G.D., Powers, R.E., Richards, S.S., Tune, L.E.,1990. Auditory hallucinations and smaller superior temporal gyralvolume in schizophrenia. Am. J.Psychiatry 147, 1457–1462.
Bassitt, D.P., Neto, M.R.L., de Castro, C.C., Busatto, G.F., 2007.Insight and regional brain volumes in schizophrenia. Eur. Arch.Psychiat. Clin. Neurosci. 257, 58–62.
Birchwood, M., Smith, J., Drury, V., Healy, J., Macmillan, F., Slade, M.,1994. A self-report insight scale for psychosis: reliability, validityand sensitivity to change. Acta Psychiatr. Scand. 89, 62–67.
Bor, D., Owen, A.M., 2007. A common prefrontal-parietal network formnemonic and mathematical recoding strategies within workingmemory. Cereb. Cortex 17, 778–786.
Cavanna, A.E., 2007. The precuneuos and consciousness. CNSSpectrums 12, 545–552.
Cavanna, A.E., Trimble, M.R., 2006. The precuneus: a review of itsfunctional anatomy and behavioural correlates. Brain 129, 564–583.
Coffey, C.E., Lucke, J.F., Saxton, J.A., Ratcliff, G., Unitas, L.J., Billig,B., Bryan, R.N., 1998. Sex differences in brain aging: a quantitativemagnetic resonance imaging study. Arch. Neurol. 55, 169–179.
Cooke, M.A., Peters, E.R., Anilkumar, A.P., Aasen, I., Kuipers, E.,Kumari, V., 2007. Insight, distress and coping styles in schizo-phrenia. Schizophr. Res. 94, 12–22.
Cooke, M.A., Peters, E.R., Kuipers, E., Kumari, V., 2005. Disease,deficit or denial? Models of poor insight in psychosis. ActaPsychiatr. Scand. 112, 4–17.
Culham, J.C., Kanwisher, N.G., 2001. Neuroimaging of cognitive func-tions in human parietal cortex. Curr. Opin. Neurobiol. 11, 157–163.
David, A.S., 1990. Insight and psychosis. Br. J. Psychiatry 156,798–808.
David, A., Buchanan, A., Reed, A., Almeida, O., 1992. Theassessment of insight in psychosis. Br. J. Psychiatry 161, 599–602.
David, A., van Os, J., Jones, P., Harvey, I., Foerster, A., Fahy, T., 1995.Insight and psychotic illness. Cross-sectional and longitudinalassociations. Br. J. Psychiatry 167, 621–628.
Flashman, L.A., McAllister, T.W., Andreasen, N.C., Saykin, A.J.,2000. Smaller brain size associated with unawareness of illness inpatients with schizophrenia. Am. J. Psychiatry 157, 1167–1169.
Flashman, L.A., McAllister, T.W., Johnson, S.C., Rick, J.H., Green,R.L., Saykin, A.J., 2001. Specific frontal lobe subregions correlatedwith unawareness of illness in schizophrenia: a preliminary study. J.Neuropsychiatry Clin. Neurosci. 13, 255–257.
Frith, C.D., 1992. The Cognitive Neuropsychology of Schizophrenia.Erlbaum (UK) Taylor and Francis.
Gilulani, N.R., Calhoun, V.D., Pearlson, G.D., Francis, A., Buchanan,R.W., 2005. Voxel-based morphometry versus region of interest: acomparison of two methods for analyzing gray matter differencesin schizophrenia. Schizophr. Res. 74, 135–147.
Good, C.D., Johnsrude, I.S., Ashburner, J., Henson, R.N., Friston, K.J.,Frackowiak, R.S., 2001. A voxel-based morphometric study ofageing in 465 normal adult human brains. Neuroimage 14, 21–36.
Ha, T.H., Youn, T., Ha, K.S., Rho, K.S., Lee, J.M., Kim, I.Y., Kim, S.I.,Kwon, J.S., 2004. Gray matter abnormalities in paranoid schizo-phrenia and their clinical correlations. PsychiatryRes. 132, 251–260.
Hamilton, M., 1960. A rating scale for depression. J. Neurol.Neurosurg. Psychiatry 25, 55–62.

51M.A. Cooke et al. / Schizophrenia Research 103 (2008) 40–51
Hulshoff Pol, H.E., Schnack, H.G., Mandl, R.C., van Haren, N.E.,Koning, H., Collins, D.L., Evans, A.C., Kahn, R.S., 2001. Focal graymatter density changes in schizophrenia. Arch. Gen. Psychiatry 58,1118–1125.
Job, D.E., Whalley, H.C., McConnell, S., Glabus, M., Johnstone, E.C.,Lawrie, S.M., 2002. Structural gray matter differences betweenfirst-episode schizophrenics and normal controls using voxel-based morphometry. Neuroimage 17, 880–889.
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The positive and negativesyndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13,261–276.
Kemp, R. and David, A., 1997. Insight and compliance. Chronicmental illness, Vol. 5, Blackwell, B. (Ed.), Treatment complianceand the therapeutic alliance. Chronic mental illness, Vol. 5. xvii,325pp., pp. 61–84.
Kircher, T.T.J., Brammer, M., Bullmore, E., Simmons, A., Bartels, M.,David, A.S., 2002. The neural correlates of intentional andincidental self processing. Neuropsychologia 40, 683–692.
Kircher, T.T.J., Senior, C., Phillips, M.L., Benson, P.J., Bullmore, E.T.,Brammer, M., Simmons, A., Williams, S.C.R., Bartels, M., David,A.S., 2000. Towards a functional neuroanatomy of self processing:effects of faces and words. Cognitive Brain Research 10, 133–144.
Kjaer, T.W., Nowak, M., Lou, H.C., 2002. Reflective self-awarenessand conscious states: PET evidence for a common midlineparietofrontal core. Neuroimage 17, 1080–1086.
Kubicki, M., Shenton, M.E., Salisbury, D.F., Hirayasu, Y., Kasai, K.,Kikinis, R., Jolesz, F.A., McCarley, R.W., 2002. Voxel-basedmorphometric analysis of gray matter in first episode schizo-phrenia. Neuroimage 17, 1711–1719.
Kuperberg, G.R., Broome, M.R., McGuire, P.K., David, A.S., Eddy,M., Ozawa, F., Goff, D., West, W.C., Williams, S.C., van derKouwe, A.J., Salat, D.H., Dale, A.M., Fischl, B., 2003. Regionallylocalized thinning of the cerebral cortex in schizophrenia. Arch.Gen. Psychiatry 60, 878–888.
Lacerda, A.L.,Hardan, A.Y., Yorbik, O.,Vemulapallia,M., Prasad, K.M.,Keshavan, M.S., 2007. Morphology of the orbitofrontal cortex infirst-episode schizophrenia: relationship with negative symptomatol-ogy. Prog. Neuropsychopharmacol. Biol. Psychiatry 31, 510–516.
Laroi, F., Fannemel, M., Ronneberg, U., Flekkoy, K., Opjordsmoen, S.,Dullerud, R., Haakonsen, M., 2000. Unawareness of illness inchronic schizophrenia and its relationship to structural brainmeasures and neuropsychological tests. Psychiatry Res. 100, 49–58.
Lou, H.C., Luber, B., Crupain, M., Keenan, J.P., Nowak, M., Kjaer,T.W., Sackeim, H.A., Lisanby, S.H., 2004. Parietal cortex andrepresentation of the mental Self. Proc. Nat. Aca. Sci. U.S.A.101, 6827–6832.
Marcelis, M., Suckling, J., Woodruff, P., Hofman, P., Bullmore, E., vanOs, J., 2003. Searching for a structural endophenotype in psychosisusing computational morphometry. Psychiat. Res.: Neuroimag.122, 153–167.
McGlynn, S.M., Schacter, D.L., 1997. The neuropsychology of in-sight: impaired awareness of deficits in a psychiatric context.Psychiatr. Ann. 27, 806–811.
Moorhead, T.W., Job, D.E., Whalley, H.C., Sanderson, T.L.,Johnstone, E.C., Lawrie, S.M., 2004. Voxel-based morphometryof comorbid schizophrenia and learning disability: analyses innormalized and native spaces using parametric and nonparametricstatistical methods. Neuroimage 22, 188–202.
Nelson, H., Willison, J., 1991. National Adult Reading Test Manual.Nfer-Nelson, Windsor.
Oldfield, R.C., 1971. The assessment and analysis of handedness: theEdinburgh inventory. Neuropsychologia 9, 97–113.
Pearlson, G.D., 1997. Superior temporal gyrus and planum temporalein schizophrenia: a selective review. Prog. Neuro-Psychopharma-col. Biol. Psychiatry 21, 1203–1229.
Pia, L., Neppi-Modona, M., Ricci, R., Berti, A., 2004. The anatomy ofanosognosia for hemiplegia: a meta-analysis. Cortex 40, 367–377.
Raveendran, V., Kumari, V., 2007. Clinical, cognitive and neuralcorrelates of self-monitoring deficits in schizophrenia: an update.Acta Neuropsychiatrica 19, 27–37.
Rossell, S.L., Coakes, J., Shapleske, J., Woodruff, P.W., David, A.S.,2003. Insight: its relationship with cognitive function, brain volumeand symptoms in schizophrenia. Psychol. Med. 33, 111–119.
Salgado-Pineda, P., Baeza, I., Perez-Gomez, M., Vendrell, P., Junque, C.,Bargallo, N., Bernardo, M., 2003. Sustained attention impairmentcorrelates to gray matter decreases in first episode neuroleptic-naiveschizophrenic patients. NeuroImage 19, 365–375.
Salgado-Pineda, P., Junque, C., Vendrell, P., Baeza, I., Bargallo, N.,Falcon, C., Bernardo, M., 2004. Decreased cerebral activationduring CPT performance: structural and functional deficits inschizophrenic patients. Neuroimage 21, 840–847.
Sapara, A., Cooke, M.A., Fannon, D., Francis, A., Buchanan, R.W.,Anilkumar, A.P., Barkataki, I., Aasen, I., Kuipers, E., Kumari, V.,2007. Prefrontal cortex and insight in schizophrenia: a volumetricMRI study. Schizophr. Res. 89, 22–34.
Shad, M.U., Muddasani, S., Prasad, K., Sweeney, J.A., Keshavan,M.S., 2004. Insight and prefrontal cortex in first-episode Schizo-phrenia. Neuroimage 22, 1315–1320.
Shad, M.U., Muddasani, S., Keshavan, M.S., 2006. Prefrontalsubregions and dimensions of insight in first-episode schizophre-nia — a pilot study. Psychiat. Res.: Neuroimag. 146, 35–42.
Shad, M.U., Keshavan, M.S., Tamminga, C.A., Cullum, C.M., David,A., 2007. Neurobiological underpinnings of insight deficits inschizophrenia. Int. Rev. Psychiatry 19, 437–446.
Shenton, M.E., Dickey, C.C., Frumin, M., McCarley, R.W., 2001. Areview ofMRI findings in schizophrenia. Schizophr. Res. 49, 1–52.
Sigmundsson, T., Suckling, J.,Maier,M.,Williams, S.C.R., Bullmore, E.T.,Greenwood, K., Fukuda, R., Ron, M.A., Toone, B.K., 2000. Structuralabnormalities in frontal, temporal and limbic regions and interconnect-ing white matter tracts in schizophrenia. Schizophr. Res. 41, 5–6.
Simmons, A., Arridge, S.R., Barker, G.J., Williams, S.C.R., 1996.Simulation of MRI cluster plots and application to neurologicalsegmentation. Magn. Reson. Imaging 14, 73–92.
Sowell, E.R., Thompson, P.M., Holmes, C.J., Batth, R., Jernigan, T.L.,Toga, A.W., 1999. Localizing age-related changes in brainstructure between childhood and adolescence using statisticalparametric mapping. Neuroimage 9, 587–597.
Spalletta, G., Tomaiuolo, F., Marino, V., Bonaviri, G., Trequattrini, A.,Caltagirone, C., 2003. Chronic schizophrenia as a brain mis-connection syndrome: a white matter voxel-based morphometrystudy. Schizophr. Res. 64, 15–23.
Spitzer, R.L., Williams, J.B., Gibbon, M., 1994. Structured ClinicalInterview for DSM-IV-Patient Version (SCID-P). New York StatePsychiatric Institute, New York.
Takai, A., Uematsu, M., Ueki, H., Sone, K., 1992. Insight and itsrelated factors in chronic schizophrenic patients: a preliminarystudy. Eur. J. Psychiatry 6, 159–170.
Vogeley, K., Fink, G.R., 2003. Neural correlates of the first-person-perspective. Trends Cogn. Sci. 7, 38–42.
Vuilleumier, P., 2004. Anosognosia: the neurology of beliefs anduncertainties. Cortex 40, 9–17.
Wright, I.C., Rabe-Hesketh, S., Woodruff, P.W.R., David, A.S.,Murray, R.M., Bullmore, E.T., 2000. Meta-analysis of regionalbrain volumes in schizophrenia. Am. J. Psychiatry 157, 16–25.