Embed Size (px)
Citation preview

Neu
rolo
gy In
dia
• Volu
me 6
4 • Issu
e 6
• No
vem
ber-D
ecem
ber 2
016 • P
age
s ***-***
Neurology India Neurology India Official Publication of the Neurological Society of IndiaNovember-December 2016 / Vol 64 / Issue 6
ISSN 0028-3886www.neurologyindia.com

1347Neurology India / November 2016 / Volume 64 / Issue 6
Letters to Editor
with a successful outcome.They had no postoperative complications and the patients did not require lumbar CSF drainage during their postoperative course. Although most surgeons would prefer a posterior or far lateral extended posterolateral approach for ventral lesions, it is also fraught with risks of excessive cord manipulation and damage. It requires a special expertise for execution. Pure ventral intradural lesions, as depicted in the manuscript, would be possibly better tackled by an anterior approach. Instability and epidural bleeding are worrisome but can be avoided by experience gathered from the anterior surgery for degenerative cervical disc disease. The advantages and limitations of the approach have been well described.
Dattatraya MuzumdarDepartment of Neurosurgery, King Edward VII Memorial
Hospital and Seth Gordhandas Sunderdas Medical College, Mumbai, Maharashtra, India
E‑mail: [email protected]
References
1. Aboul-Enein HA, Khidr WM, Abdeen KM, Madawi AA. Surgical management of ventrally based lower cervical (subaxial) meningiomas through the lateral approach: Report on 16 cases. Clin Neurol Neurosurg 2015;139:152-8.
2. Mahore A, Muzumdar D, Chagla A, Goel A. Pure ventral midline long segment schwannoma of the cervicodorsal spine: A case report. Turk Neurosurg 2009;19:302-5.
3. Markert JM, Chandler WF, Deveikis JP, Ross DA. Use of the extreme lateral approach in the surgical treatment of an intradural ventral cervical spinal cord vascular malformation: Technical case report. Neurosurgery1996;38:412-5.
4. Mirzai H. Tuberculoma of the cervical spinal canal mimicking en plaque meningioma. J Spinal Disord Tech 2005;18:197-9.
5. Kim SD, Nakagawa H, Mizuno J, Inoue T. Thoracic subpial intramedullary schwannoma involving a ventral nerve root: A case report and review of the literature. Surg Neurol 2005;63:389-93.
6. Angevine PD, Kellner C, Haque RM, McCormick PC. Surgical management of ventral intradural spinal lesions. J Neurosurg Spine 2011;15:28-37.
7. Barami K, Dagnew E. Endoscope-assisted posterior approach for the resection of ventral intradural spinal cord tumors: Report of two cases. Minim Invasive Neurosurg 2007;50:370-3.
8. O’Toole JE, McCormick PC. Midline ventral intradural schwannoma of the cervical spinal cord resected via anterior corpectomy with reconstruction: Technical case report and review of the literature. Neurosurgery 2003;52:1485-6.
9. Banczerowski P, Lipóth L, Vajda J, Veres R. Surgery of ventral intradural midline cervical spinal pathologies via anterior cervical approach: Our experience. Ideggyogy Sz 2003;56:115-8.
10. Ogden AT, Feldstein NA, McCormick PC. Anterior approach to cervical intramedullary pilocytic astrocytoma. Case report. J Neurosurg Spine 2008;9:253-7.
11. Martin NA, Khanna RK, Batzdorf U. Posterolateral cervical or thoracic approach with spinal cord rotation for vascular malformations or tumors of the ventrolateral spinal cord. J Neurosurg1995;83:254-61.
12. Gambardella G, Gervasio O, Zaccone C. Approaches and surgical
results in the treatment of ventral thoracic meningiomas. Review of our experience with a postero-lateral combined transpedicular–transarticular approach. ActaNeurochir (Wien) 2003;145:385-92.
13. Rajagandhi S, Hari A, Krishna M, Rajakumar V. Deshpande RV. Transcorporeal excision of cervical intradural lesions: Two cases and a literature review. Neurol India 2016: 64:1341-5.
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
How to cite this article: Muzumdar D. Commentary: Surgery for pure midline ventral spinal intradural lesions. Neurol India 2016;64:1345‑7.
Access this article onlineWebsite:
www.neurologyindia.com
Quick Response Code
DOI:
10.4103/0028-3886.193815
PMID:
xxxxx
Extracranial temporal cavernous hemangioma: Differential diagnosis, and a review of literature
Sir,A small swelling in the temporal region is often benign and managed conservatively unless it causes local pain, shows an increase in size or becomes cosmetically disfiguring. The differential diagnosis of pathology in this region is quite varied and includes soft tissue tumors such as lipoma, schwannoma, dermoid, mesenchymal angiolipoma, and spindle cell hemangioendothelioma; vascular malformations such as cavernous hemangiomas and arterio‑venous malformations (AVMs); and malignant lesions such as liposarcomas and angiosarcomas. Occasionally, extracranial extensions of intracranial meningiomas/hemangiopericytomas or osteoma of the calvarium can present in a similar fashion. Enlarged lymph nodes, myositis ossificans, and temporal arteritis complete the list.
We discuss the case of a 61‑year‑old female patient with an intramuscular cavernous hemangioma of the temporalis muscle and review varying presentations and the differential

1348 Neurology India / November 2016 / Volume 64 / Issue 6
Letters to Editor
Postoperatively, the patient developed a left frontalis paresis that had significantly improved at 4 weeks. The postoperative computed tomography (CT) scan done showed no residual lesion [Figure 4].
Histopathology showed a proliferation of large, thick‑walled vascular channels with foci of lymphoid inflammation and pieces of striated muscle. This was consistent with a cavernous hemangioma [Figure 5].
Less than 1% of hemangiomas are intramuscular and only 14% occur in the head and neck.[1‑4] The masseter and trapezius muscles are the most frequently affected sites.[2,4] Involvement of the orbicularis oris, mentalis, digastric and mylohyoid muscles has also been reported.[5] Intramuscular hemangiomas within the temporalis muscle are extremely rare. Histologically they are classified as capillary (small vessel), cavernous (large vessel), and mixed, depending on the predominant vascular channels that they are composed of.[6] Minor trauma, hormonal status, or excessive muscle contraction is believed to play a role in their growth by inducing changes in the blood flow. They have been reported to grow to a giant size, cross tissue planes, and can rarely have an intracranial extension, producing a mass effect on the brain.[7] Table 1 discusses the clinical, radiological, and pathological differential diagnosis of these lesions within the temporalis muscle.
While in most patients they present as a painless, progressive swelling within the temporalis muscle causing facial asymmetry, there are reports of cases presenting with significant pain and temporo‑mandibular joint dysfunction.[8] They can change in size with a Valsalva maneuver due to large venous channels within. They are also known to occasionally develop several years after blunt trauma to the head. The diagnosis is more straightforward when there is an associated cutaneous change, but this is uncommon.
diagnosis. Due their rarity and vague presentations, this entity presents significant diagnostic challenges.[1]
This 61‑year‑old female patient presented with a small swelling in the left temporal region of her head 4 years previously. She was initially asymptomatic and her family physician, who suspected that this was a lipoma, recommended a conservative approach. More recently, she noticed a significant growth in the size of the lesion over 1 year, which prompted a referral. Apart from the increasing size of the lesion, she was otherwise asymptomatic. Examination revealed a smooth, nonpulsatile, nontender, immobile globular swelling in the left temporal region. It was firm and noncompressible. There was no audible bruit. On examination, she had no neurological deficit.
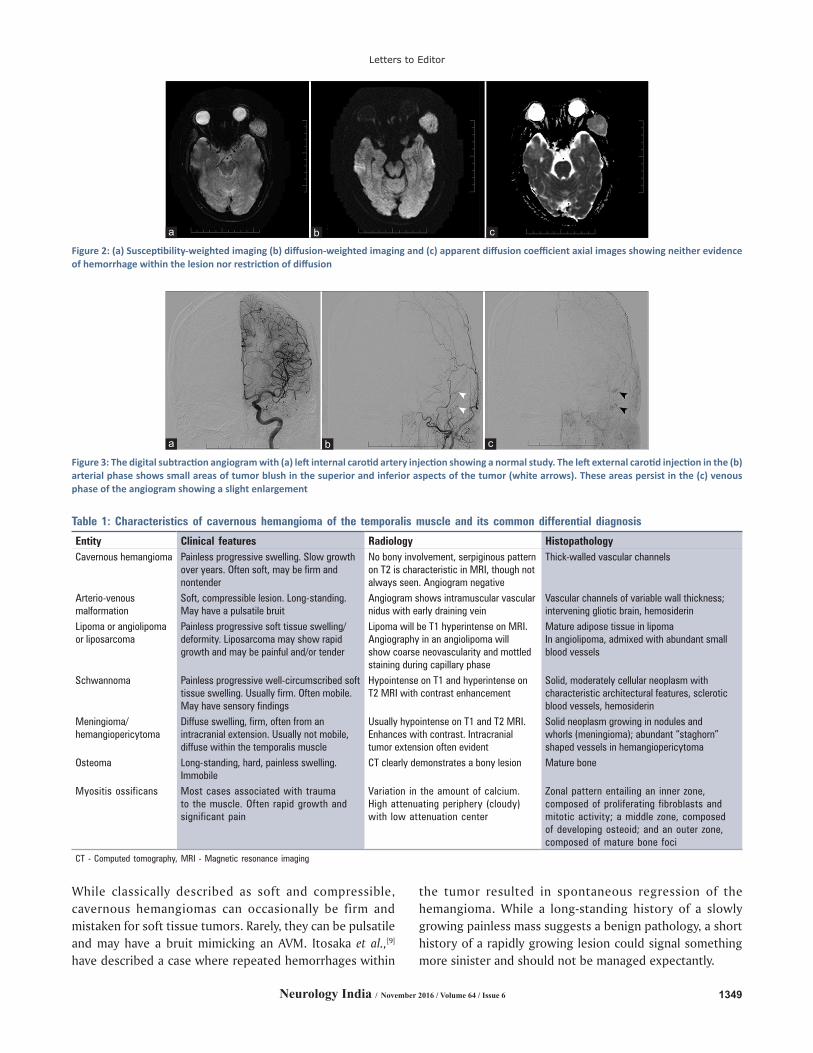
Magnet ic resonance imaging (MRI ) revea led a 3.5 cm × 2.5 cm × 4.5 cm lesion within the left temporalis muscle. There was no involvement of the underlying bone or scalp. The lesion was hypointense on T1‑weighted images and hyperintense on T2‑weighted images and showed heterogeneous enhancement with administration of gadolinium [Figure 1]. There was neither restriction of diffusion on the diffusion‑weighted imaging nor was there evidence of hemorrhage on susceptibility‑weighted imaging [Figure 2]. An angiogram ruled out an AVM, but showed evidence of minimal neovascularity of the mass. There were two small areas of contrast blush in the superior and inferior aspect of the lesion that appeared in the arterial phase and persisted, slightly enlarging into the venous phase. However, the bulk of the lesion did not demonstrate a vascular blush [Figure 3]. The preoperative diagnosis was that of a cavernous hemangioma. Surgery was recommended both for the confirmation of diagnosis as well as cosmesis. A frontal‑temporal skin flap was turned forward to the orbital rim. The tumor was then seen and felt within the temporalis muscle, from which it was dissected en bloc, excising it radically. There was no infratemporal or orbital extension.
Figure 1: (a) T2‑weighted axial, (b) T1‑weighted coronal with gadolinium, and (c) T1‑weighted plain sagittal magnetic resonance imaging of the head showing a 4.5 cm T1‑weighted hypointense, T2‑weighted hyperintense, and heterogeneously enhancing well‑defined intramuscular lesion in the left temporalis muscle
cba
1349Neurology India / November 2016 / Volume 64 / Issue 6
Letters to Editor
While classically described as soft and compressible, cavernous hemangiomas can occasionally be firm and mistaken for soft tissue tumors. Rarely, they can be pulsatile and may have a bruit mimicking an AVM. Itosaka et al.,[9] have described a case where repeated hemorrhages within
the tumor resulted in spontaneous regression of the hemangioma. While a long‑standing history of a slowly growing painless mass suggests a benign pathology, a short history of a rapidly growing lesion could signal something more sinister and should not be managed expectantly.
Figure 3: The digital subtraction angiogram with (a) left internal carotid artery injection showing a normal study. The left external carotid injection in the (b) arterial phase shows small areas of tumor blush in the superior and inferior aspects of the tumor (white arrows). These areas persist in the (c) venous phase of the angiogram showing a slight enlargement
cba
Figure 2: (a) Susceptibility‑weighted imaging (b) diffusion‑weighted imaging and (c) apparent diffusion coefficient axial images showing neither evidence of hemorrhage within the lesion nor restriction of diffusion
cba
Table 1: Characteristics of cavernous hemangioma of the temporalis muscle and its common differential diagnosis
Entity Clinical features Radiology HistopathologyCavernous hemangioma Painless progressive swelling. Slow growth
over years. Often soft, may be firm and nontender
No bony involvement, serpiginous pattern on T2 is characteristic in MRI, though not always seen. Angiogram negative
Thick-walled vascular channels
Arterio-venous malformation
Soft, compressible lesion. Long-standing. May have a pulsatile bruit
Angiogram shows intramuscular vascular nidus with early draining vein
Vascular channels of variable wall thickness; intervening gliotic brain, hemosiderin
Lipoma or angiolipoma or liposarcoma
Painless progressive soft tissue swelling/deformity. Liposarcoma may show rapid growth and may be painful and/or tender
Lipoma will be T1 hyperintense on MRI. Angiography in an angiolipoma will show coarse neovascularity and mottled staining during capillary phase
Mature adipose tissue in lipomaIn angiolipoma, admixed with abundant small blood vessels
Schwannoma Painless progressive well-circumscribed soft tissue swelling. Usually firm. Often mobile. May have sensory findings
Hypointense on T1 and hyperintense on T2 MRI with contrast enhancement
Solid, moderately cellular neoplasm with characteristic architectural features, sclerotic blood vessels, hemosiderin
Meningioma/hemangiopericytoma
Diffuse swelling, firm, often from an intracranial extension. Usually not mobile, diffuse within the temporalis muscle
Usually hypointense on T1 and T2 MRI. Enhances with contrast. Intracranial tumor extension often evident
Solid neoplasm growing in nodules and whorls (meningioma); abundant “staghorn” shaped vessels in hemangiopericytoma
Osteoma Long-standing, hard, painless swelling. Immobile
CT clearly demonstrates a bony lesion Mature bone
Myositis ossificans Most cases associated with trauma to the muscle. Often rapid growth and significant pain
Variation in the amount of calcium. High attenuating periphery (cloudy) with low attenuation center
Zonal pattern entailing an inner zone, composed of proliferating fibroblasts and mitotic activity; a middle zone, composed of developing osteoid; and an outer zone, composed of mature bone foci
CT - Computed tomography, MRI - Magnetic resonance imaging

1350 Neurology India / November 2016 / Volume 64 / Issue 6
Letters to Editor
MRI is the investigation of choice in defining the nature of the tumor and in differentiating its vascular nature from soft tissue elements. These lesions are most often well‑circumscribed within the muscle, isointense on T1‑weighted images, and hyperintense on T2‑weighted images. Occasionally, a hypointense rim similar to what is seen in cavernous malformations of the brain is also visible on the T2‑weighted images. Some authors suggest that a serpiginous pattern on T2‑weighted images is characteristic.[10] The heterogeneity on enhancement is due to thrombosis, hemosiderin deposition, and calcification. Phleboliths can sometimes be seen inside the lesion as low‑intensity areas. Lipomas, angiolipomas, and dermoids are usually hyperintense on T1W images, whereas schwannomas and meningiomas have a more uniform enhancement. A CT scan may show remodeling of the underlying skull in long‑standing cases.[10]
Angiography is helpful to differentiate cavernous hemangiomas from an AVM.[11] AVMs will have either a compact or a diffuse intramuscular nidus and the presence of early draining veins. The main arterial feeders are branches of the superficial temporal and internal maxillary artery, and the draining veins are commonly the facial and external jugular. Cavernous malformations may be angiographically occult (involuting type) or they may show uniform hypervascularity (proliferating type). There may be separate visible areas of blush due to pooling of stagnant blood, as seen in our case. Angiolipomas, on the other hand, show coarse neovascularity and mottled staining during the capillary phase.[12] These findings should guide in the diagnosis, avoiding the need for an open biopsy, which could lead to unwarranted hemorrhage.
Hemangiomas are benign and not known to metastasize, but can have local recurrence due to infiltration of muscle and soft tissue. Capillary hemangiomas are more aggressive than the cavernous and mixed types. The objective of surgery should be total removal, preferably in an en bloc fashion. Care should be taken to prevent injury to the temporal and auricular branches of the facial nerve because if permanent,
this complication could be more disfiguring than the swelling itself. Ohyama et al.,[13] used an electric nerve stimulator where the facial nerve ran over the skin as well as subfacially to avoid this complication. Steroids, sclerosing agents, and radiation are other proposed treatment modalities but are not consistently effective.[14]
Due to the wide spectrum of diagnostic possibilities, a soft tissue swelling in the temporal region requires careful evaluation with an MRI as well as angiography, as the diagnosis has a significant impact on the management of these lesions. The definitive diagnosis is usually made by histopathological evaluation. Careful surgical planning and total removal usually result in a good result.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
Mazda K. Turel, Tim‑Rasmus Kiehl1, Fred GentiliDivision of Neurosurgery, Toronto Western Hospital,
1Department of Laboratory Medicine and Pathobiology, University of Toronto, Toronto, Ontario, Canada
E‑mail: [email protected]
References
1. Bucci T, De Giulio F, Romano A, Insabato L, Califano L. Cavernous haemangioma of the temporalis muscle: Case report and review of the literature. Acta Otorhinolaryngol Ital 2008;28:83-6.
2. Eryilmaz MA, Varsak YK, Gül Z, Ugur A. Intramuscular cavernous hemangioma of the temporalis muscle. J Craniofac Surg 2014;25:1400-1.
3. Calisaneller T, Ozdemir O, Yildirim E, Kiyici H, Altinörs N. Cavernous hemangioma of temporalis muscle: Report of a case and review of the literature. Turk Neurosurg 2007;17:33-6.
4. Heckl S, Aschoff A, Kunze S. Cavernous hemangioma of the temporal muscle. Neurosurg Rev 2002;25:63-5.
5. Sherman JA, Davies HT. Intramuscular hemangioma of the temporalis muscle. J Oral Maxillofac Surg 2001;59:207-9.
6. Allen PW, Enzinger FM. Hemangioma of skeletal muscle. An analysis of 89 cases. Cancer 1972;29:8-22.
7. Voelker JL, Stewart DH, Schochet SS Jr. Giant intracranial and extracranial cavernous malformation. Case report. J Neurosurg
Figure 5: (a) Low power and (b) high power images showing proliferation of large, thick‑walled vascular channels with foci of lymphoid inflammation and pieces of striated muscle, consistent with a cavernous hemangioma
ba
Figure 4: The postoperative (a) coronal and (b) axial images do not show any residual tumor
ba
1351Neurology India / November 2016 / Volume 64 / Issue 6
Letters to Editor
1998;89:465-9.8. Hughes C, Hutchison I. Temporalis haemangioma presenting as
temporomandibular joint pain dysfunction syndrome. Br J Oral Maxillofac Surg 1993;31:21-2.
9. Itosaka H, Tada M, Sawamura Y, Abe H, Saito H. Vanishing tumor of the temporalis muscle: Repeated hemorrhage in an intramuscular venous hemangioma. AJNR Am J Neuroradiol 1997;18:983-5.
10. Tada M, Sawamura Y, Abe H, Itoh F, Saito H, Nagashima K. Venous hemangioma of the temporalis muscle. Neurol Med Chir (Tokyo) 1996;36:23-5.
11. Geibprasert S, Fanning NF, Pedroza A, Terbrugge KG. Imaging characteristics of arteriovenous malformations simulating vascular tumors of the temporalis muscle: A report of two cases. Int J Oral Maxillofac Surg 2010;39:402-6.
12. Hoeft S,Luettges J,Werner JA. Infiltrating angiolipomaof theM.temporalis. Auris Nasus Larynx 2000;27:265-9.
13. Ohyama A, Kamo R, Yanagihara S, Kimura Y, Kusutani N, Ozawa T, et al. Subfascial lipoma in the temporal muscle that extended to under the zygomatic arch. J Dermatol 2015;42:1011-2.
14. Stofman GM, Reiter D, Feldman MD. Invasive intramuscular hemangiomas of the head and neck. Ear Nose Throat J 1989;68:612-6.
This is an open access article distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as the author is credited and the new creations are licensed under the identical terms.
How to cite this article: Turel MK, Kiehl TR, Gentili F. Extracranial temporal cavernous hemangioma: Differential diagnosis, and a review of literature. Neurol India 2016;64:1347‑51.
Access this article onlineWebsite:
www.neurologyindia.com
Quick Response Code
DOI:
10.4103/0028-3886.193800
PMID:
xxxxx
Pediatric intraparenchymal meningioma: A review of literature
Sir,Meningiomas are rare tumors in the pediatric population accounting for approximately 1 to 2% of all intracranial neoplasms in this age group.[1] An intraparenchymal meningioma, which consists of a meningioma without a dural tail and is surrounded by the normal brain parenchyma is very rare, with very few case reports available in the literature.[2] We report one such case and present a pertinent literature review.
A 16‑year‑old male child presented with a history of multiple seizures. The last seizure occurred 4 months back, and the
patient was seizure free after starting oral phenytoin tablets. Patient had no neurological deficits on examination.
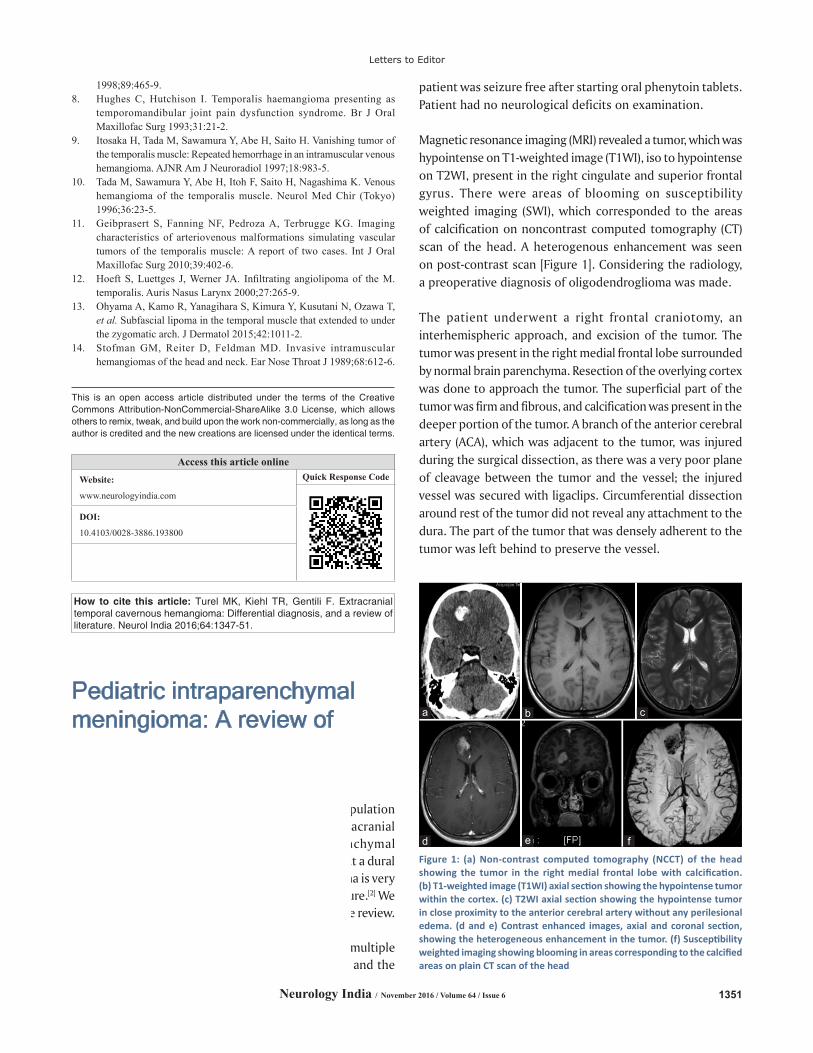
Magnetic resonance imaging (MRI) revealed a tumor, which was hypointense on T1‑weighted image (T1WI), iso to hypointense on T2WI, present in the right cingulate and superior frontal gyrus. There were areas of blooming on susceptibility weighted imaging (SWI), which corresponded to the areas of calcification on noncontrast computed tomography (CT) scan of the head. A heterogenous enhancement was seen on post‑contrast scan [Figure 1]. Considering the radiology, a preoperative diagnosis of oligodendroglioma was made.
The patient underwent a right frontal craniotomy, an interhemispheric approach, and excision of the tumor. The tumor was present in the right medial frontal lobe surrounded by normal brain parenchyma. Resection of the overlying cortex was done to approach the tumor. The superficial part of the tumor was firm and fibrous, and calcification was present in the deeper portion of the tumor. A branch of the anterior cerebral artery (ACA), which was adjacent to the tumor, was injured during the surgical dissection, as there was a very poor plane of cleavage between the tumor and the vessel; the injured vessel was secured with ligaclips. Circumferential dissection around rest of the tumor did not reveal any attachment to the dura. The part of the tumor that was densely adherent to the tumor was left behind to preserve the vessel.
Figure 1: (a) Non‑contrast computed tomography (NCCT) of the head showing the tumor in the right medial frontal lobe with calcification. (b) T1‑weighted image (T1WI) axial section showing the hypointense tumor within the cortex. (c) T2WI axial section showing the hypointense tumor in close proximity to the anterior cerebral artery without any perilesional edema. (d and e) Contrast enhanced images, axial and coronal section, showing the heterogeneous enhancement in the tumor. (f) Susceptibility weighted imaging showing blooming in areas corresponding to the calcified areas on plain CT scan of the head
d
cb
f
a
e