Embed Size (px)
Citation preview
Mehmet Ali Akalın V.ENG
Neuromuscular diseases (I)
Muscle and neuromuscular junction
Neuromuscular Diseases
• Group of miscellaneous diseases • Many are hereditary, some are not • Some are chronic, others progress very
rapidly
• Many share similar symptoms
Disorders of the Motor Unit (Classification of Neuromuscular Diseases)
• Motor neuron disease • Neuromuscular junction disease • Muscle disease • Peripheral nerve disorders
Motor Neuron Disease Diseases that can involve
1) Betz cells of the motor cortex, 2) the lower CN motor nuclei, 3) the CST, 4) and/or the anterior horn cells
– Amyotrophic Lateral Sclerosis (ALS) – Progressive bulbar palsy – Progressive muscular atrophy, spinal muscular
atrophy – Primary lateral sclerosis
ALS • Loss of motor neurons in the cortex,
brainstem and spinal cord • Mix of upper motor neuron and lower
motor neuron findings – Weakness, atrophy, fasciculations – Slurred speech, difficulty swallowing,
shortness of breath • Can start in any extremity or the bulbar
musculature • Relentlessly progressive
ALS
• 50 % dead in 3 years, 80% dead in 5 years, 5-10% live more than 10 years
• Death usually from respiratory failure • Etiology still only theoretical
– Excess glutamate – Oxidative stress – Free radicals – Mitochondrial dysfunction
• There is no therapy to date

Myopathies MUSCLE DISEASE
Largest group of neuromuscular diseases • Most diverse group • All show a loss of muscle fibers – Proximal
more than distal • No involvement of the anterior horn cell,
nerve axon, or neuromuscular junction
Subcategories
1. Muscular dystrophy 2. Endocrine disorders 3. Metabolic disorders 4. Myotonias 5. Periodic paralysis 6. Polymyositis
Endocrine Myopathies • Caused by some malfunction of the
endocrine system • Chronic • Respond to drug therapy (primarily
hormonal therapy) • Examples: –Addison’s Disease
–Cushing’s Syndrome (Steroid myopathy) – Thyrotoxic Myopathy
Metabolic Myopathies Myopathies characterized by a deficiency of a specific
enzyme resulting in muscle weakness Examples: • McArdle’s Disease
– Deficiency of the muscle enzyme myophosphorylase – Glycogen is thus stored in the muscles rather than being
used as a source of energy • Pompe’s Disease
– deficiency in acid maltase – Excess storage of glycogen in many different organs
Case • A 23-year-old man… • was found to have difficulty relaxing after
grasping since teenage.. • he has boldness and a thin neck.. • his school performance was poor.. • routine check-up showed cataract and diabetes.. • currently he also has problems with opening
eyes and swallowing.. • his mother shares the same disease.. • we heard dive-bomber sound on EMG
Myotonias • Characterized by: – Inability to relax a previously contracted muscle • Elicited by either voluntary contractions or some
external stimuli such as percussion • Worsened by cold • Lessened by light exercise • Examples: – Myotonic Congenita (Thomsen’s Disease) – Myotonia Atrophica (Myotonic dystrophy)
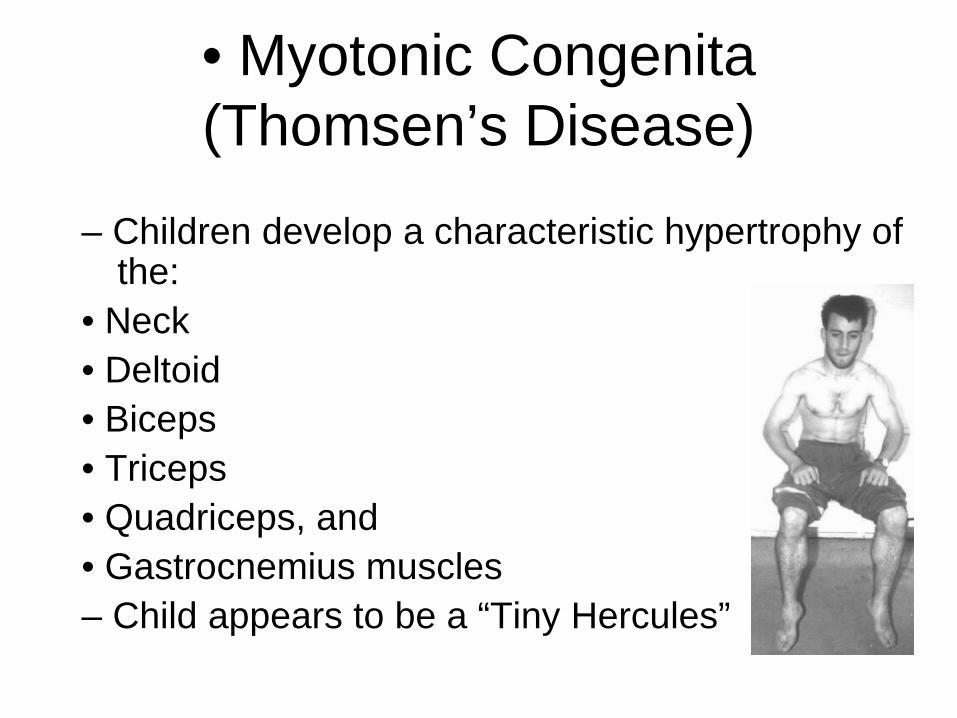
• Myotonic Congenita (Thomsen’s Disease)
– Children develop a characteristic hypertrophy of the:
• Neck • Deltoid • Biceps • Triceps • Quadriceps, and • Gastrocnemius muscles – Child appears to be a “Tiny Hercules”
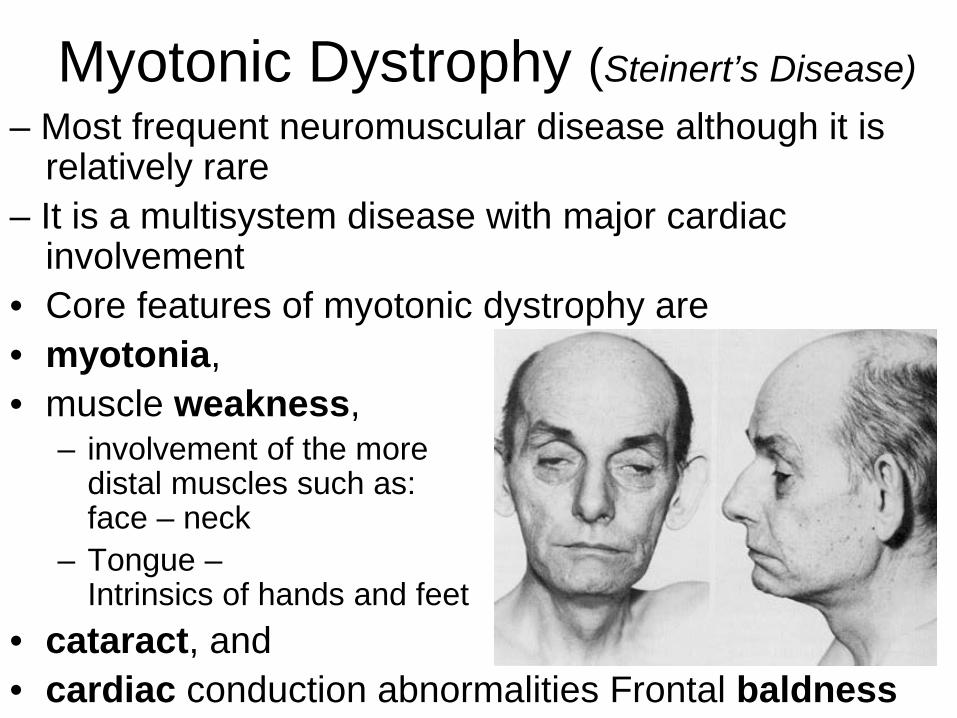
Myotonic Dystrophy (Steinert’s Disease) – Most frequent neuromuscular disease although it is
relatively rare – It is a multisystem disease with major cardiac
involvement • Core features of myotonic dystrophy are • myotonia, • muscle weakness,
– involvement of the more distal muscles such as: – face – neck
– Tongue – Intrinsics of hands and feet
• cataract, and • cardiac conduction abnormalities Frontal baldness
Myotonic dystrophy (dystrophia myotonica, DM )
• The most frequently inherited neuromuscular disease of adult life
• It is a multisystem disease with major cardiac involvement
• Core features of myotonic dystrophy are myotonia, muscle weakness, cataract, and cardiac conduction abnormalities
Periodic Paralysis
• Relatively rare myopathy • Hereditary – Autosomal dominant • Characterized by: – Transient flaccid paralysis or paresis affecting
primarily the muscle of the proximal limbs – Attacks of weakness may last from a few
seconds to several weeks
Primary Periodic Paralyses
Sodium channel
Hyperkalemic PP Paramyotonia congenita Potassium-aggravated myotonias
Calcium channel Hypokalemic PP Potassium channel Andersen-Tawil syndrome
Hyperkalemic PP or hypokalemic PP*
* Hypokalemic periodic paralysis • where potassium leaks into the muscle
cells from the bloodstream.
* Hyperkalemic periodic paralysis • where potassium leaks out of the cells into
the bloodstream.
Hyperkalemic Form – Has increased serum K+ – Triggered by: • Stress • Fasting • Cold • Rest following intensive or prolonged muscular
exercise – Attacks minimized by: • Light exercise • Ingestion of carbohydrates
Hypokalemic Form – Has decreased serum K+ – Affects men more than women – Triggered by: • Stress • Fasting • Cold • Rest following intensive or prolonged muscular
exercise • Alcohol consumption • High carbohydrate diets
Polymyositis • Second most common myopathy in adults • Chronic inflammatory condition of muscle • If skin is involved >>>>>(Dermatomyositis) • Insidious onset, Moderately progressive • Clinical signs:
– Muscle weakness Flexors more than extensors
– Fatigue – – Difficulty swallowing – Joint pain – Mild fever – Weight loss – Very diffuse erythema of face and neck
Polymyositis • Presents with proximal muscle weakness
in 92% • Myalgias in 25% • Slightly increased risk of cancer
– Bladder, lung, lymphoma • Biopsy of muscle confirms diagnosis • Treatment with immunosuppression
– Prednisone – Methotrexate
Muscular Dystrophy
• Largest group of the myopathies • Group of inherited diseases • Characterized by: – Progressive muscle weakness • Examples: – Pseudohypertrophic Muscular Dystrophy
(Duchenne’s) – Becker-type Muscular Dystrophy – Facioscapulohumeral Muscular Dystrophy – Limb-girdle Muscular Dystrophy
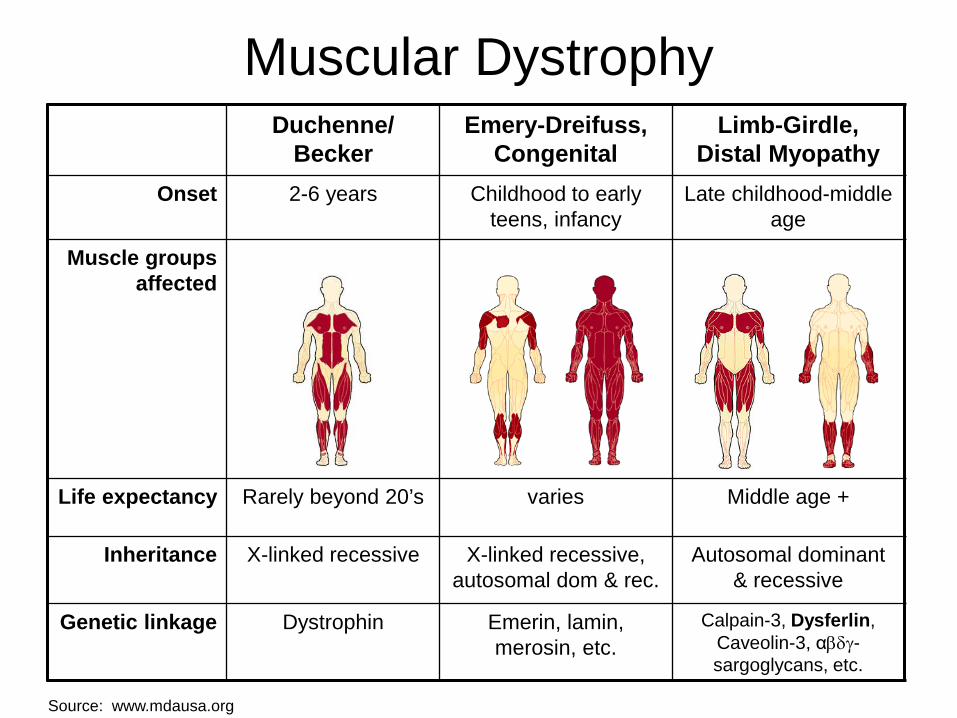
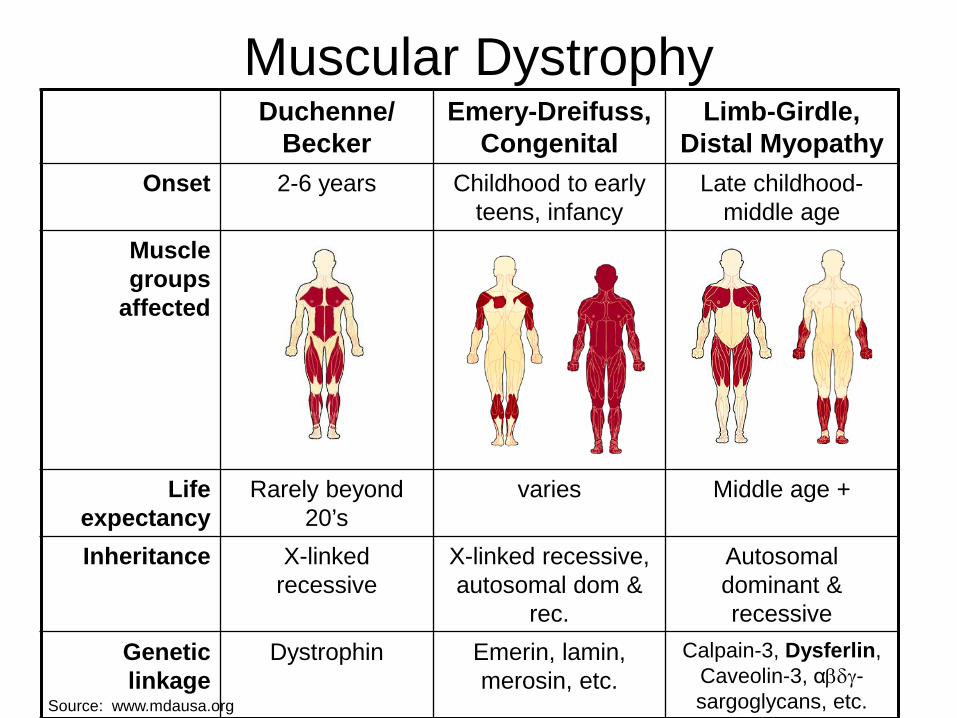
Muscular Dystrophy Duchenne/
Becker Emery-Dreifuss,
Congenital Limb-Girdle,
Distal Myopathy Onset 2-6 years Childhood to early
teens, infancy Late childhood-middle
age
Muscle groups affected
Life expectancy Rarely beyond 20’s varies Middle age +
Inheritance X-linked recessive X-linked recessive, autosomal dom & rec.
Autosomal dominant & recessive
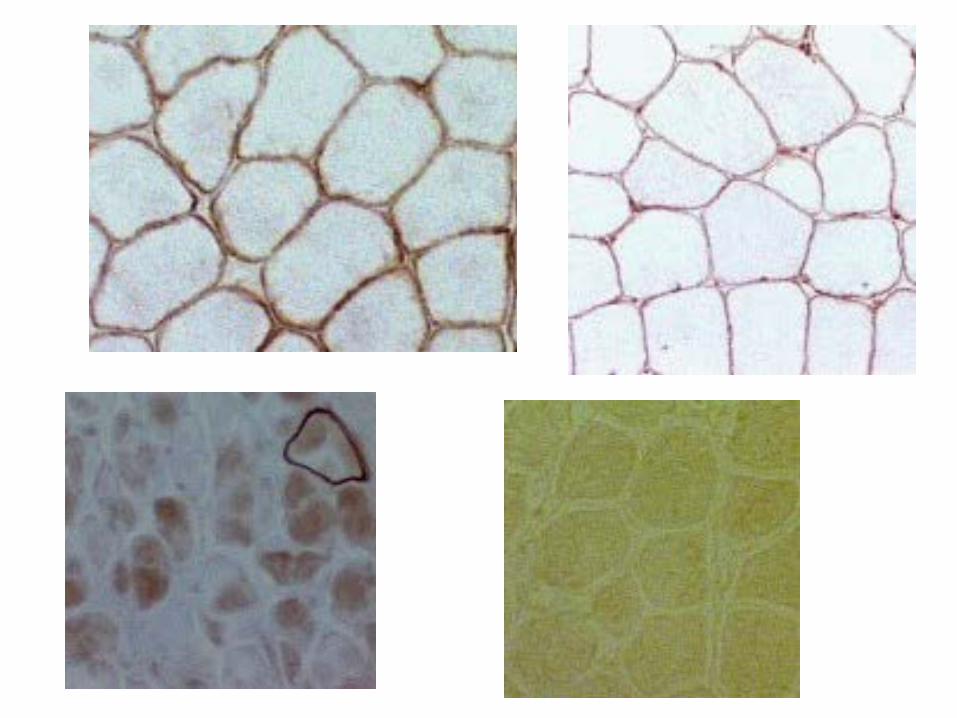
Genetic linkage Dystrophin Emerin, lamin, merosin, etc.
Calpain-3, Dysferlin, Caveolin-3, αβδγ-sargoglycans, etc.
Source: www.mdausa.org
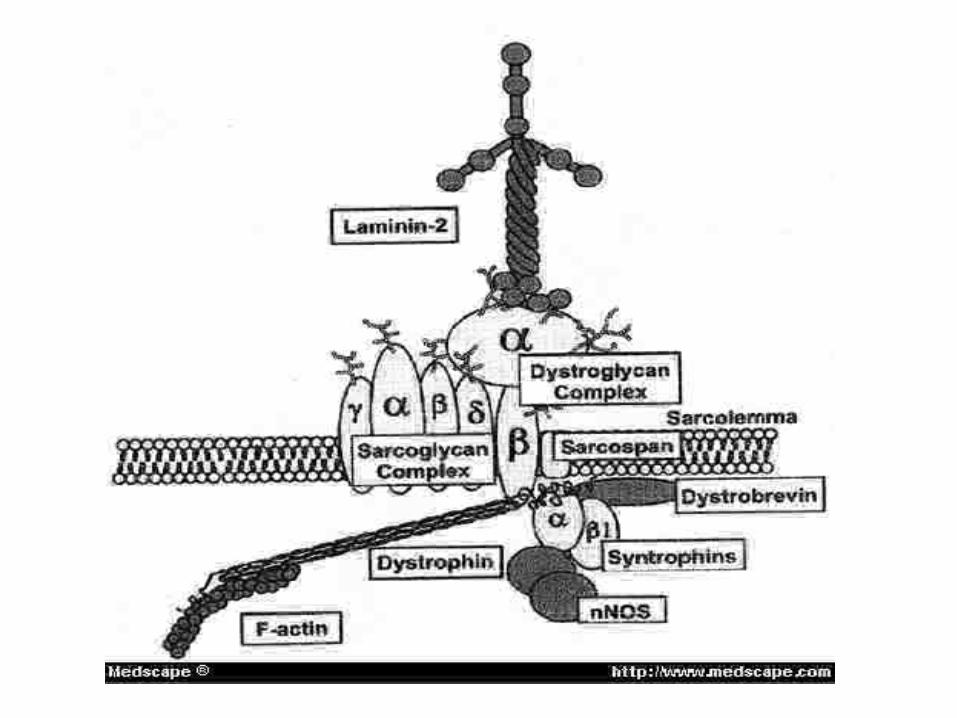
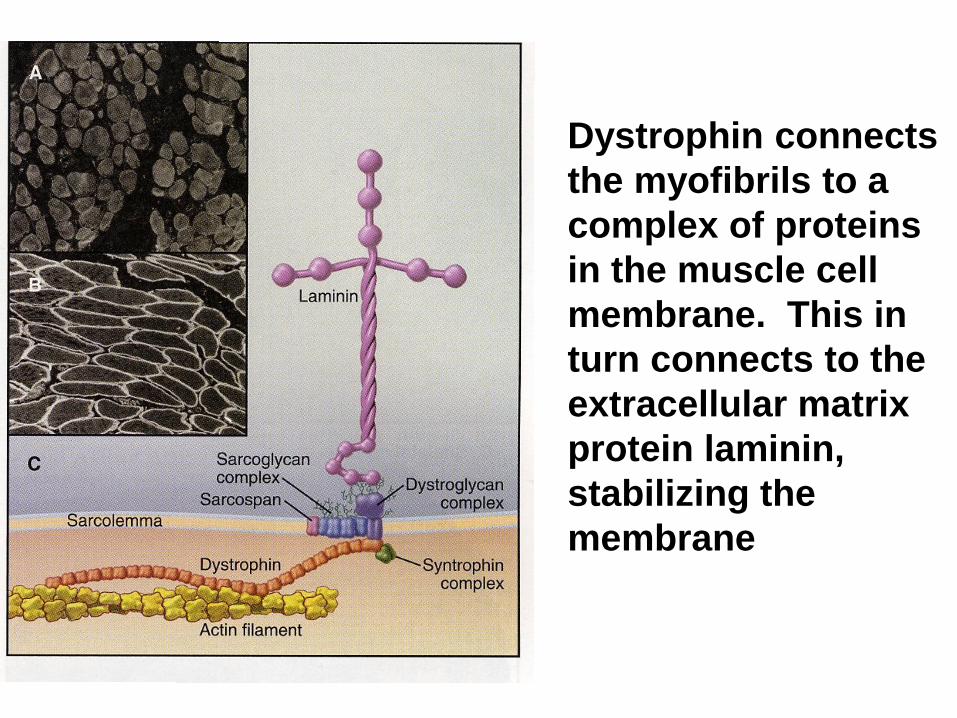
Dystrophin connects the myofibrils to a complex of proteins in the muscle cell membrane. This in turn connects to the extracellular matrix protein laminin, stabilizing the membrane
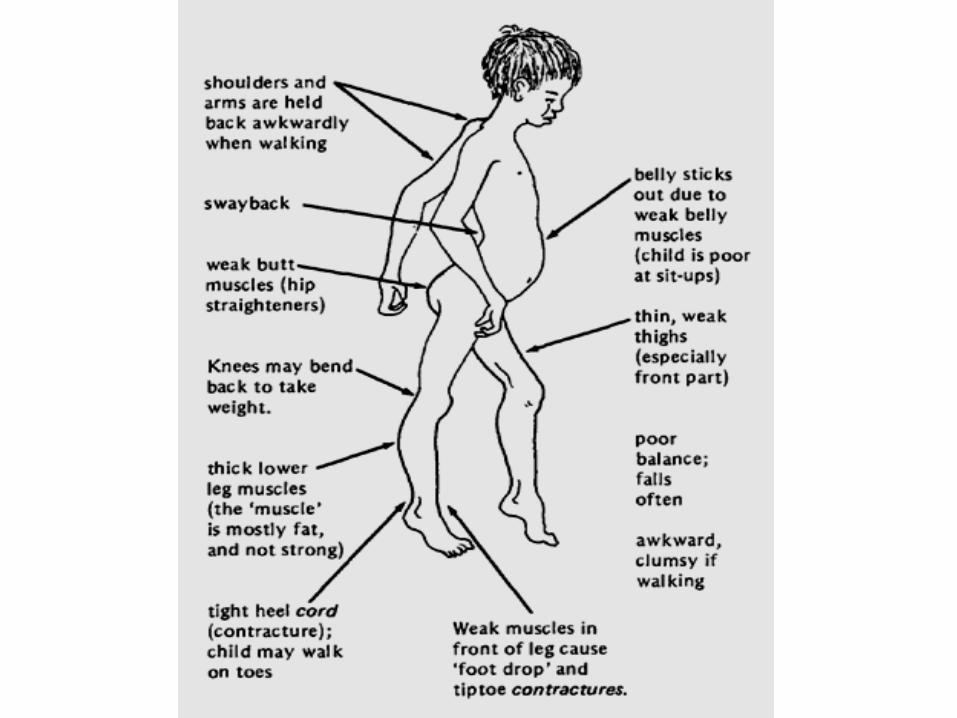
Case
• A school boy , aged 10 yr…with • delayed development of walking since
childhood.. • and frequent falls.. • NE showed..
– proximal muscle weakness, waddling gait..toe walking..
– Gower’s sign..lordosis.. – enlarged and stiff calves..
• mental retardation seems obvious.
Duchenne's dystrophy (DMD) History and epidemiology
• Described in 1852.
• The most common X-linked, lethal disease.
• Occurs in 1: 3,500 male newborns.
Clinical features Skeletal muscle involvement • Onset usually between ages 3 and 5 years. • Proximal muscles and neck flexor muscles
(severely) are affected early. • Difficulty doing a sit-up. • Calf hypertrophy (pseudohypertrophy). • Contractures of heel cords and iliotibial bands. • Scoliosis • Cardiomyopathy (can be asymptomatic)
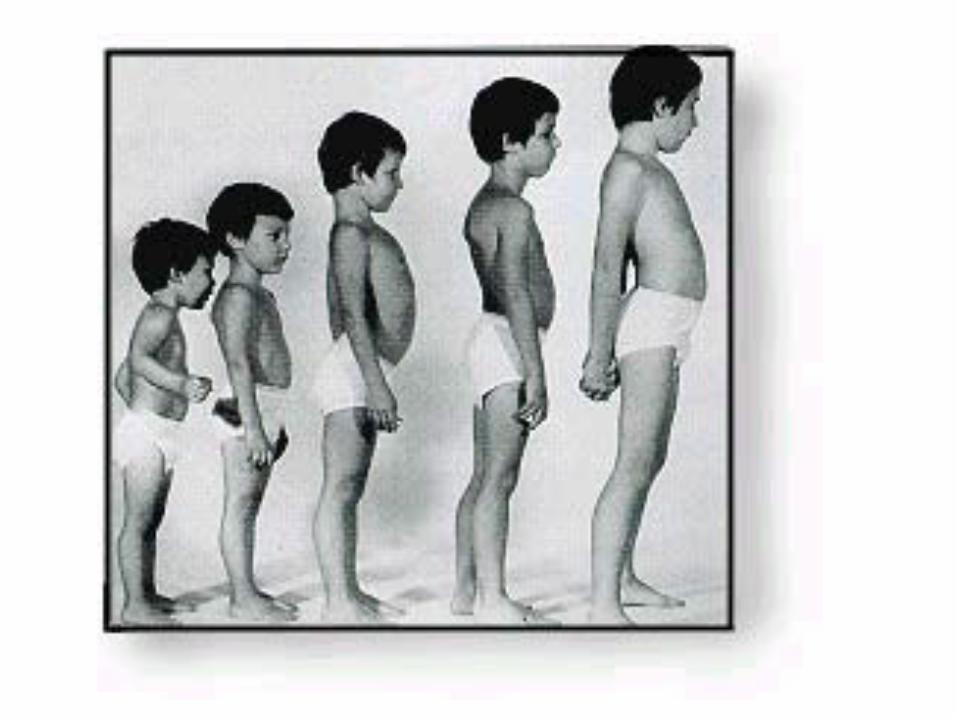
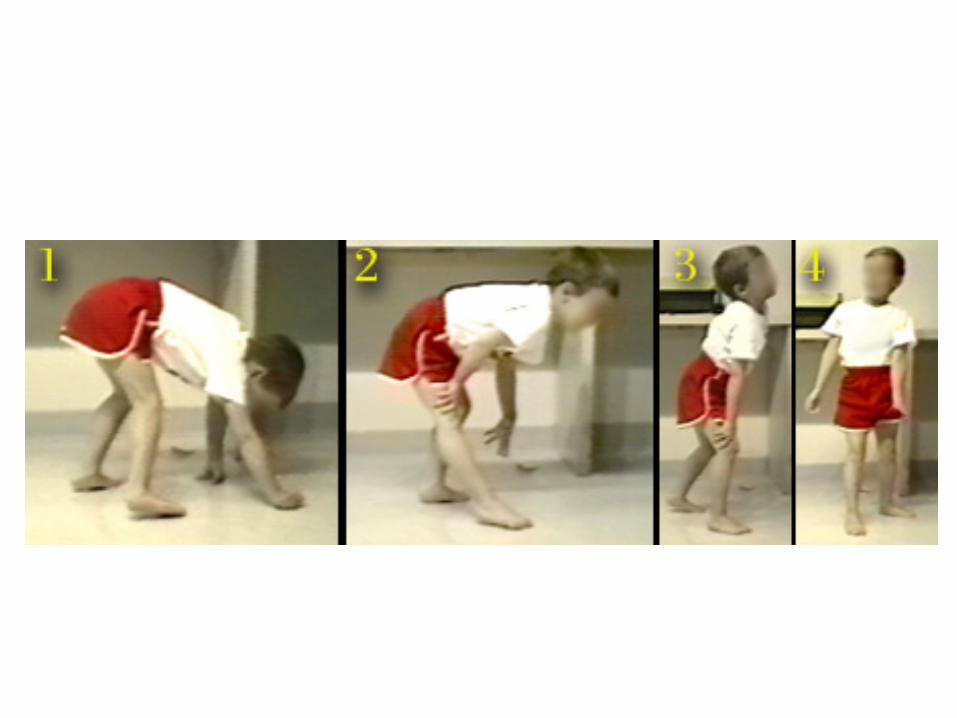
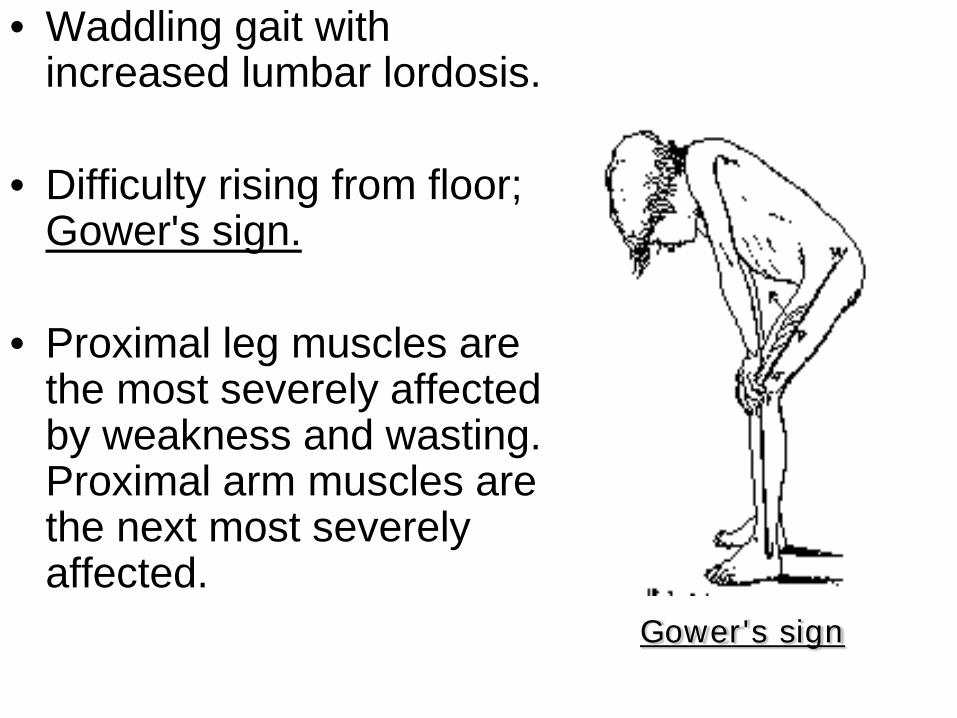
• Waddling gait with increased lumbar lordosis.
• Difficulty rising from floor; Gower's sign.
• Proximal leg muscles are the most severely affected by weakness and wasting. Proximal arm muscles are the next most severely affected.
Gower's sign
• Cranial nerve supplied muscles are relatively spared.
• Between ages 3 and 6 the child's function may improve due to growth and the normal increase in strength, which more than offset the loss of function.
• Usually unable to walk by age 10 to 12. • Scoliosis develops following wheelchair-
dependency. • Death by age 20 in most without a ventilator • Steroids may delay time until wheelchair
bound
Cardiac involvement
• The heart develops fibrosis, mainly in the posterobasal part of the left ventricular wall.
• Congestive heart failure and cardiac arrhythmias occur in later stages.
• Congestive heart failure may develop in some patients who have adequate respiratory muscle function.
Smooth muscle of GI tract
• Acute gastric dilatation can cause episodic vomiting, abdominal pain, and gastric distension.
• May be mistaken for intestinal obstruction.
CNS involvement
• The average IQ of DMD patients is one standard deviation below the normal mean.
• The intellectual impairment is not progressive.
• Verbal IQ is affected more than performance IQ.
Case A young man,aged 20 years … was found to have problems with walking since age 12 years.. right now …he has waddling gait.. CK level was as high as 20 times normal..
EMG.. myopathic patterns.. Dystrophin stain showed a defective pattern
Becker's dystrophy Clinical features • Onset is usually between age 5 and 15
years. Sometimes, onset is much later. • • By definition, Becker patients walk past
the age of 15.
• Life expectancy is generally reduced.
Other phenotypes • Exertional cramps and myalgia. • Myoglobinuria. • Quadriceps myopathy.
Intermediate forms (outliers) • Recognized clinically as early as 3
years. • Preservation of anti-gravity strength in
neck flexor muscles. • Stair-climbing and walking to age 12 to
15.
• A 21-year-old young man …with.. • marked contractures of arms and • legs..his spine was rigid..he had • weakness of biceps and peroneal • muscles..he underwent pacemaker • implantation because of heart block
Emery-Dreifuss Muscular Dystrophy
• Genetics ... • X-linked recessive ( X q 28 ) • emerin defect • Features … • humeroperoneal weakness plus .. • early contractures , rigid spine • and heart block
Case
• A 19-year-old male … complaining of • progressive worsening of left arm for • a couple of years..his left arm shows • a Popeye appearance..in addition.. • he has difficulty blowing..slight ptosis.. • otherwise..he remains quite healthy
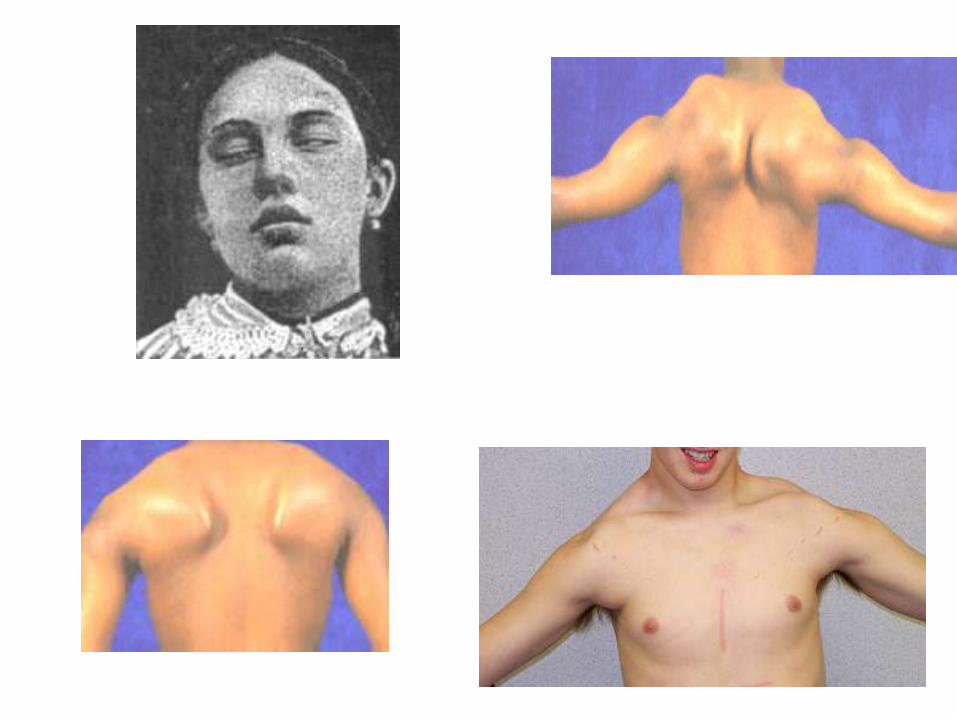
Facioscapulohumeral Muscular Dystrophy (FSH)
• Genetics AD , chromosome 4 • Features … • onset since adolescence • slowly progressive , life span unaffected • assymmetric weakness and wasting • of face,serratus anterior muscle ,biceps
muscles,etc. with deltoid spared … Popeye appearance
• CK : slightly elevated • EMG : myopathic patterns • Biopsy : myopathic patterns
Case
• A 52-year-old female …complaining • of progressive worsening of weakness • and wasting of both legs during the • past 6 years..recently she noticed • slight weakness in both arms too.. • N.E. showed weakness and atrophy • of leg and shoulder girdles...
Limb Girdle Muscular Dystrophy
• Genetics … • heterogenous pathogenesis • Features … • proximal weakness • legs early than arms • face and eye spared • knee jerk diminished early than • ankle jerk
Muscular Dystrophy Duchenne/
Becker Emery-Dreifuss,
Congenital Limb-Girdle,
Distal Myopathy Onset 2-6 years Childhood to early
teens, infancy Late childhood-
middle age Muscle groups
affected
Life expectancy
Rarely beyond 20’s
varies Middle age +
Inheritance X-linked recessive
X-linked recessive, autosomal dom &
rec.
Autosomal dominant & recessive
Genetic linkage
Dystrophin Emerin, lamin, merosin, etc.
Calpain-3, Dysferlin, Caveolin-3, αβδγ-sargoglycans, etc. Source: www.mdausa.org
Evaluation of the Patient with Suspected Muscle Disease
• Lab – Muscle enzymes (CPK, aldolase) – Erythrocyte sedimentation rate (ESR or
sed rate) if suspect inflammatory disease – Genetic test
• Duchenne’s • Myotonic dystrophy
• EMG/NCS • Muscle biopsy
• May provide a definitive diagnosis
Case for quiz
• A 49-year-old mother was examined • on the visit…she was found to have • lid ptosis, difficulty swallowing and • slight weakness in finger flexors and foot
drop.. • she also has diabetes and cataract.. • one of her sons shares the same illness...
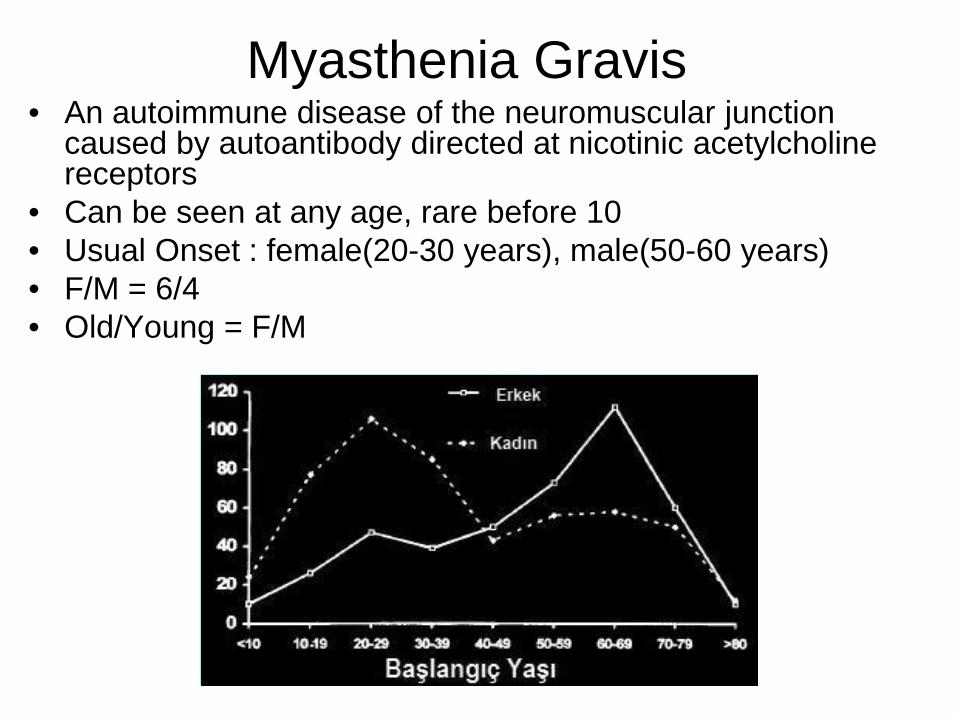
Myasthenia Gravis • An autoimmune disease of the neuromuscular junction
caused by autoantibody directed at nicotinic acetylcholine receptors
• Can be seen at any age, rare before 10 • Usual Onset : female(20-30 years), male(50-60 years) • F/M = 6/4 • Old/Young = F/M
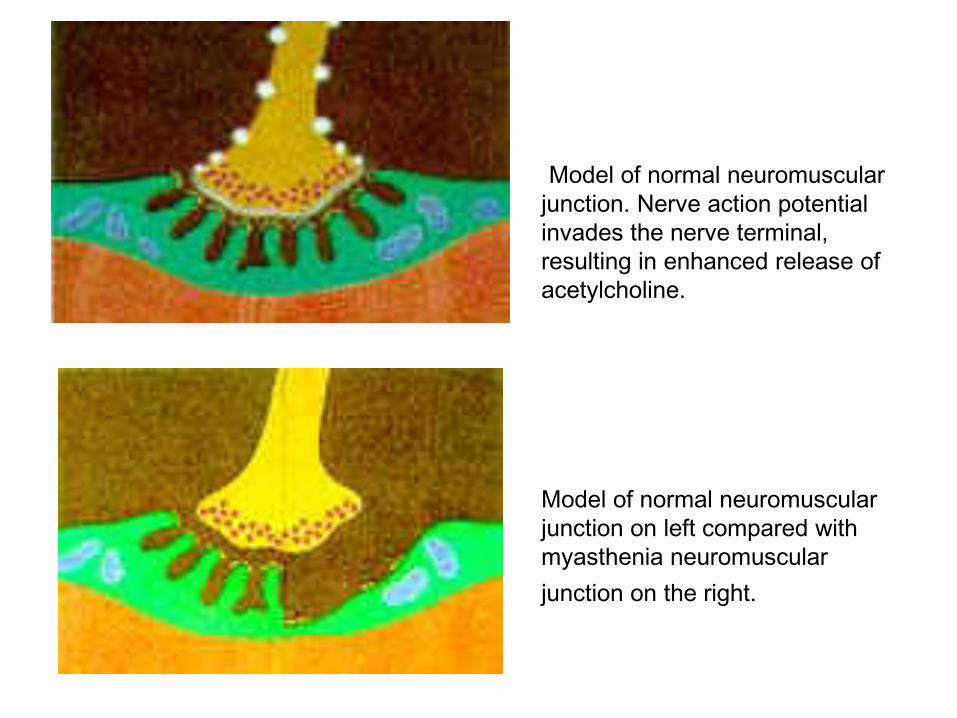
Model of normal neuromuscular junction. Nerve action potential invades the nerve terminal, resulting in enhanced release of acetylcholine.
Model of normal neuromuscular junction on left compared with myasthenia neuromuscular junction on the right.
Onset
Presenting symptoms – Ocular (50%): Ptosis; Diplopia – Weakness (35%): Bulbar; Legs; Arms – Fatigue (10%) – Respiratory failure: Rare
Progression: Generally insidious over weeks to months
Classification after Osserman & Genkins 1. Adult MG
– Group I: Ocular (20%) – Group IIA: Mild generalized (30%) – Group III: Acute fulminating (11%), rapid
onset, early respiratory involvement, high mortality.
– Group IV: Late Severe (9%), > 2 years after onset.
2. Transient Neonatal MG: 1/6 born to MG mother. Last a few weeks.
3. Congenital Myasthenic Syndrome
Symptoms & Signs 1- Weakness • Variable:
• increses through the day or • with prolonged physical activity
• Onset: • Diplopia or ptosis 2° to extraocular muscle or levator
palpebrae weakness
• Most patients develop weakness in other muscles
• Weakness remains limited to ocular muscles during entire course of the illness >>>Ocular myasthenia
A- Ocular weakness • Ptosis & Ophthalmoplegia • Usually asymmetric & bilateral • Pupils: Normal • Rule out focal neural lesions
III or VI nerve lesion; Internuclear ophthalmoplegia Especially when unilateral signs
B - Facial vweakness : > 95%

C- Bulbar weakness Symptoms: Dysarthria, Dysphagia, Weak mastication Signs:
– Poor gag reflex & palate elevation; – Weak tongue – May result in aspiration pneumonia
Considered life-threatening – Usually an indication for rapidly-acting therapeutic
intervention – Plasma exchange most commonly used
D- Respiratory muscle weakness
Usually due to Diaphragmatic and Intercostal muscle weakness
•Strong indication for rapidly-acting therapeutic intervention •Pyridostigmine & Plasma exchange most commonly used
May be due to vocal cord paralysis1 •Vocal cords in adductor position: Produces stridor •May require intubation Considered life-threatening
E- Systemic muscle weakness
Typical: Proximal > Distal; Arms > Legs; Symmetric
• Weakness in selective areas • Posterior neck (head ptosis) • Triceps • Quadriceps • Occasionally: Distal musculature
• 3- Fatigue – Induced by repetitive muscle strength testing or
prolonged tonic contraction – Quantitation: Timed upward gaze; Forward arm
abduction • 4- Muscle wasting: Uncommon, except
when MG is chronic & untreated • 5- Deep tendon reflexes: Usually preserved;
May be somewhat brisk in clinically weak muscles
• 6- Sensory: Normal
Other Symptoms & Signs
Testing
• Anti-acetylcholine receptor Ab: – Present in 80% of patient
Tindall: – Ocular 55% positive – Mild Generalized 80% positive – Moderately severe or acute 100% positive – Chronic severe 89% – In remission 24%
Antibodies to striated muscle (StrAb)
• Positive in 30% of all adult onset MG. • Highly associated with thymoma
– Positive in 80% of MG patients with thymoma – Positive in 24% of patients with thymoma
without MG. – Seronegativity does not exclude thymoma. – Most useful as a marker of thymoma in
patients with MG onset before age 40. – A progressive rise in StrAbs titer after
resection of thymoma is a good indicator of tumor recurrence.
Thymoma
• 15% of patient has thymoma, 50% has thymic hyperplasia.
• Antiskeletal muscle Ab are detected in 90% of patients with thymoma.
• CT Chest detect over 85% of thymoma. • Removal of thymoma produces a delayed
improvement of MG 6 - 24 months later. Sustained improvement in > 50%, probably less in older patients. No known long-term side effects.
Tensilon test (Edrophonium) Given in incremental doses. Start with 2 mg, observe the
response for 45 to 60 seconds, followed by doses of 3 and 5 mg and observation for a clinical response for 1 to 2 minutes following each dose.
During the injection, patients often experience 1 to 3 minutes of increased salivation, mild sweating, perioral fasciculations and mild nausea.
Hypotension and bradycardia are extremely rare but
precautions should be taken. Atropine sulfate (0.6 mg intramuscular or intravenously) should be available in case of an emergency.
Tensilon test cont’d
• Positive means unequivocally improvement of weakness. • Slight to moderate improvement in muscle strength
must be interpreted with extreme caution. • Mild to moderate clinical improvement after tensilon
has been reported in: – brain stem lesions, – oculomotor palsy due to cerebral artey aneurysm, – diabetic abducens paresis and – even in normal control subjects.
Electrophysiology 1. Repetitive stimulation at 3 hertz.
>10% decrement of compound action potential.
2. Single fiber EMG: Increased jitter: jitter is the varying time interval between the triggered muscle action potential in 2 muscle fibers within the same motor unit.
• Positive in over 90%.
Principles of treatment
• Onset before age 60 – Thymectomy, pretreat with
plasmapheresis, cholinesterase inhibitors – If response unsatisfactory before or after
thymectomy, consider high dose daily prednisone and/or other immunosuppressive agents
Principles of treatment
• Onset after age 60 – Cholinesterase inhibitors with prednisone,
azathioprine or other immunosuppressant – Plasmapheresis for severe exacerbations – Consider thymectomy
Principles of treatment • Anticholinesterase useful in all forms • For patient with thymoma, thymectomy is
indicated in all ages. They may spread in the mediastinum.
• Plasmapharesis is effective, but practical only on a short term basis.
Pyridostigmine (Mestinon)
Tab: 60 mg, – half life 4 hrs, – take 1 q 4 while awake
– Side effect:
– diarrhea, – fasciculation, – hypersecretion
» treat with Lomotil or Motilium
Steroid treatment • Indications:
– Insufficient control with Mestinon – Diplopia rarely respond to Mestinon alone – Older male
• Start at 100 mg to avoid treatment failure.
After remission obtained, switch to alternate day dose, slow taper over 6 to 12 months. Patient may get weaker initially.
• Exacerbation is common.
Azathioprine (Imuran) – Initial dose 2-3 mg/kg/day.
• Complete remission 40%, • partial remission 51%, • minimal improvement 6.4%, • no effect in 2.6%.
• Improvement begins in 2-3 months, peaks in 6-15 months.
• Keep WBC above 3000/ml. • Monitor liver function weekly X 3 months,
then 2x/month. • Sometimes used in combination with
steroid.
If treatment fails, consider 1. Cyclosporine (Sandimmune)
– 5 mg/kg/day, in bid dose. Monitor BP, renal function, Cyclosporine level, Amylase, Cholesterol.
– May cause nephropathy, hypertension, hirsutism, liver function abnormality, opportunistic infection, may increase risk of malignancy.
2. Plasma Exchange: short term improvement
3. Human Immune Globulin: Effective but short term improvement
Drugs that may adversely affect MG 1. Antibiotics
– Aminoglycosides: Neomycin, Gentamycin – Peptide: Polymyxin B, Colistin – Other: tetracycline, Clindamycin,
Erythromycin, Ampicillin 2. Neuromuscular blockers:
– Botulinum Toxin 3. Cardiac drugs:
– Quinine, Quinidine, Procanamide, Lidocaine, Beta blockers, Calcium Channel Blockers
Drugs that may adversely affect MG cont’d
4. Miscellaneous: – Epdantion, Oxytocin, Lithium,
Magnesium, Diazapam, D penicillamine, Cloroquine, Interferon
5. Corticosteroids may initially produce worsening of MG.
Other causes of exacerbation
• Febrile illness • Thyroid disease • Heat • Pregnancy • Major Physical Stress