Embed Size (px)
Citation preview

Ann. rheum. Dis. (1957), 16, 471.
NEUROPATHY IN RHEUMATOID DISEASE
BY
F. DUDLEY HART, J. R. GOLDING, AND D. H. MACKENZIE
Westminster Hospital, London
Our attention was focused sharply on the pre-valence of neuropathic disorder as part of rheuma-toid arthritic disease, when some 12 months agofour out of eight patients in the ward at one timewith rheumatoid arthritis complained of sensory or
motor changes; on examination signs of a peripheralneuropathy were present in all four. This factoraltered the symptomatology, treatment, and prog-nosis quite considerably. Since this time we haveseen further cases, and it now appears to be worthreporting them in some detail and discussing theirsignificance. The eleven *cases are listed in theTable.
The literature on the subject is very scanty. Inthe current textbooks of neurology we see occasionalreferences to "rheumatism" as a cause of peripheralneuritis, but there is no adequate description togive us greater details. Brain (1951) considers theso-called "rheumatic" polyneuritis following ex-
posure to wet and cold to be in all probability thesame as, or closely related to, acute infective poly-neuritis, very likely of virus origin. The currenttextbooks of rheumatology are silent on the subject,but an apparently recent increase in polyarteriticfeatures in rheumatoid subjects has been noted byseveral workers. Since steroid therapy has become
TABLE
PARTICULARS OF ELEVEN CASES
C Duration of Differential Relationship Course Motor and/or OtherNo. Sex Age Rheumatoid Nodules Agglutination to of Sensory Polyarteritic
No. (yIs) Arthritis (yrs) Test Steroid Neuropathy Involvement Features
1 M 59 6 + 1/512 14 days after Improved M + S +withdrawal
2 M 44 11 + 1/128 Nil Improved then M + Srelapsed
3 F 59 13 _ 1/16 Within a month Cured Sof gradual with-drawal
4 M 61 8 + 1/128 Nil Cured S +
5 F 51 19 - 1/128 Nil Progressive for M + S -
6/12 then un-changed
6 F 57 6 - - Nil Improved S -
7 M 80 20 - 1/64 Nil Unchanged M + S -
after 3 years
8 F 63 2j - 1/512 Nil Unchanged S -
9 M 70 6 + 1/2,048 Nil Improving S -
10 M 63 10 + - 7 days after Rapid recovery M - S -
withdrawal in 3 days11 F 38 1 - 1/4 7 days after Slow improve- M + S +
(Disseminated withdrawal mentlupus
erythematosus)
471
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASES
more widely used such cases appear to have in-creased, though "polyarteritis nodosa' has beenknown for some time to occur in rheumatoid arth-ritis, usually in the later stages, without steroidtherapy ever having been given. Neuropathy maybe a manifestation of either systemic (disseminated)lupus erythematosus or of polyarteritis nodosa;the question to be answered is whether all such casesmay be so explained or whether a true "rheumatoidneuritis" exists.
Case ReportsCase 1. a lorry driver aged 55, developed pain and stiffnessin many joints in 1951, beginning with the left shoulder.When first seen at the Westminster Hospital in 1952,he was diagnosed as having rheumatoid arthritis; ulnarnodules and olecranon bursae were present, and all hismetacarpophalangeal and proximal interphalangealjoints were swollen and stiff. Advanced radiologicalrheumatoid changes were present in most of the peri-pheral joints.
Treatment was by large doses of salicylates, whichcontrolled his symptoms, and he was able to work untilSeptember, 1955, when his fingers became increasinglypainful and blue, and several developed gangrenous tips.He was admitted to hospital for 6 weeks rest in bed in
October, 1955; salicylates were continued and he showedspontaneous improvement. It was noted at that timethat sensation in his fingers and toes was preserved.Polyarteritis nodosa was considered as a diagnosis,especially in view of an episode of left-sided pneumonitisin the following month, but there was no definite clinicalevidence to support this. On discharge the tips of hisfingers were no longer gangrenous.
His joints became worse during the next few monthsso that he was hardly able to get about, and prednisolone5 mg. twice daily was begun in April, 1956. There wasa week's initial improvement, but after that he thoughtthat the tablets were making him worse and giving himindigestion, and he stopped them himself abruptly onJune 18, 1956. Almost immediately his joints becamepainful, and a fortnight later he suddenly developedburning pains in both arms and legs of a type he hadnever experienced before. His legs became weak so thathe was unable to walk and in July he was again admittedto hospital.
There he was found to have a peripheral neuropathy.His hands showed only impaired sensation and weak grip,but there was complete anaesthesia of the feet withreduced sensation up to the knees. Bilateral foot dropwas complete and all movements at knee and anklejoints were weak; the ankle reflexes were absent.
There was uncertainty at this stage whether the neuro-pathy was a complication of the rheumatoid arthritis,whether he had developed polyarteritis nodosa, orwhether the cause was quite unrelated. A skin biopsyand two muscle biopsies were quite normal, neithershowing the least evidence of polyarteritis nodosa, andthe Congo red test was negative for amyloid disease.In October, 1956, a section of nerve taken from the cleftbetween the first and second toes had shown demyelina-
tion; an artery removed at the same time was completelynormal.
Treatment was begun with corticotropin 40 unitsdaily which gradually had to be reduced because of amoon face and indigestion, and a haematemesis inNovember, 1956. For 6 months there was no clinicalchange in the neuropathy, though the patient said thatthe hands and feet lost the burning pains. Large ulcersdeveloped on the heels and the legs had to be suspendedfrom a Balkan beam. At this time he had severalepisodes of chest infection, and an attack of paroxysmalauricular fibrillation lasting for 3 hours.
Early in 1957 he was at last beginning to make steadyprogress, the dose of corticotropin being 10 mg. daily.The signs of neuropathy gradually improved: sensationwas normal in his hands and his grip improved. Weakdorsiflexion at the ankle was regained, but there was stillreduced sensation over the feet of sock distribution.In March, 1957, he was able to walk a few steps.He died suddenly on June 7, 1957, with acute left
ventricular failure and pulmonary oedema.
Autopsy Findings.-The body was that of a well-nourished elderly man, showing generalized rheumatoidarthritis which was particularly marked in the jointsof the wrists, hands, and ankles. There were two trophiculcers on the right heel and one on the lateral side of theright foot.
Head and Neck.-The skull and contents, tongue,thyroid, pharynx, larynx, and oesophagus showednothing of note. The trachea contained frothy mucopus.
ThoraxHeart. The pericardial sac was almost totally
obliterated by a fibrinous pericarditis. When the peri-cardium was peeled off the whole surface of the heartappeared red and inflamed and a number of tiny noduleswere seen along the anterior descending branch of theleft coronary artery. The myocardium showed patchyfibrosis consistent with ischaemia and the whole coronarytree showed gross atheroma. There was a tiny noduleon the mitral valve but the valves and endocardiumappeared otherwise normal.
Lungs.-There were small bilateral loculated pleuraleffusions and there were multiple fine adhesions mostmarked over the left lower lobe. Both lungs appearedrather oedematous and showed chronic bronchitis.
Abdomen.-The peritoneal cavity was dry. The liverweighed 84 oz. and appeared congested and a little fatty.The spleen was also congested and weighed 81 oz.The kidneys appeared normal macroscopically andweighed I I oz. The remainder of the abdominalviscera showed nothing significant.
Histology-.All sections were stained with haemato-xylin and eosin and in addition the nerves were stainedwith Lillie's variant of the Weil-Weigert method formyelin. Selected sections were also stained withMallory's phosphotungstic acid haematoxylin andSheridan's elastic stain.
472
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

NEUROPATHY IN RHEUMATOID DISEASE
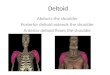
The most important findings concerned changes in thesmall blood vessels. These were observed in the heartand pericardium, in the lungs particularly the left lowerlobe, and in relation to nerve bundles in the peripheralnerves of the right foot. Though the severity of thedisease process varied considerably, the essential lesionwas an arteritis and periarteritis of the small vessels.The changes were most marked in the pericardium. Themilder lesions consisted of little more than perivascularcuffing with lymphocytes, the arterial walls being pre-served. In many instances, however, the vessels showedfibrinoid necrosis, an intense periarteritis made up oflymphocytes, plasma cells, and histiocytes (Fig. 1), andaneurysmal dilatation of the vessel walls typical of poly-arteritis nodosa. Aschoff bodies were observed in themyocardium of the left ventricle, but the nodule on themitral valve comprised only a fragment of granulationtissue.
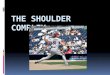
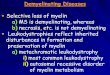
Sections from the right lateral and medial poplitealnerves and from the right posterior tibial nerve showedgross demyelination. The right median nerve appearednormal and acted as a control. The small vesselsadjacent to the nerves of the right lower limb showedwell-marked arteritis and the demyelinatioin may wellhave been the result of ischaemia (Fig. 2).The liver showed gross fatty change and the kidneys
a mild degree of chronic pyelonephritis with no evidence
--,~~~~~~~-!¢Po *;' *_~Ls-Xi :.
.-*1' I
Fig. I.-Case 1. Fibrinoid necrosis in pulmonary arteriole.Haematoxylin and eosin x 80.
of any arterial lesions suggestive of polyarteritis nodosaor of disseminated lupus erythematosus.
Comment.-While on aspirin therapy alone thispatient developed the typical necrotic finger lesionsdescribed and illustrated by Bywaters (1957, Fig. 22).These left puckered scars but no other disability.There was no sign of a neuropathy then, but pre-sumably an obliterative arteritis must have beenpresent at that time. Later, 14 days after abruptlystopping prednisolone therapy, signs of a neuro-pathy appeared suddenly in hands and feet. It islikely that the simple "rheumatoid" arteritis hadnow flared up and become a necrotizing arteritis orpolyarteritis nodosa, on which corticotropin had noreal effect. It is of interest that, as often happens,biopsies of skin, muscle, and artery were completelynegative, though autopsy revealed intensive arterialchanges, including those of polyarteritis nodosa(necrotizing arteritis).
Fig. 2.-Case 1. Demyelination of medial popliteal nerve andperiarteritis. Weil-Weigert Myelin Stain x56.
7X %* o~p
i
473
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASES
Case 2, a man aged 44, had an 11-year history of rheuma-toid arthritis which caused gross deformities of the handsand feet, but he had been able to get about and con-tinue work as a machine operator. Phenylbutazone(300 mg. daily) was begun in 1953 and continued withgood analgesic effect.
In August, 1956, he complained for the first time ofa burning pain in the soles of his feet, spreading up thelegs to the knees and disturbing him at night. Similarbut less troublesome pains appeared at the same timein the hands.On examination at that time he had advanced and
deforming rheumatoid arthritis with ulnar nodules andolecranon bursae. He was hypertensive (Blood Pressure200/110), but his exercise tolerance was good. Thepower of his feet was normal but the right ankle reflexwas greatly reduced compared with the left. All formsof sensation below the knees were diminished, becomingmore severe peripherally. The only sensory change inthe hands was to pin prick.
There was a trace of albumen in the urine, but nothingabnormal in the deposit. The sheep cell agglutinationtest was positive 1: 128. No evidence of porphyrinuriawas found and the Congo red test was negative foramyloidosis. A skin and muscle biopsy from thedeltoid region showed no arteritis, but a nerve biopsyfrom the foot demonstrated demyelination.The symptoms of neuropathy persisted, making the
patient miserable, and walking became difficult. Heoften stated that the neuropathy was far more unpleasantand more disabling than the arthritis. Prednisolone10 mg. daily which was begun in April, 1957, had noeffect, good or bad, and was discontinued in May.
In July, 1957, the symptoms spontaneously improvedand clinical examination a month later could demon-strate no sensory abnormality at all, though the rightankle reflex was still reduced; 6 weeks later, with nochange in therapy, foot drop developed abruptly, andthis, though improved, has now persisted for severalmonths.
Comment.-In this case signs and symptoms of aperipheral neuropathy developed after 3 years on aregular daily dose of phenylbutazone, without anychange in therapy or preceding infection. Pred-nisolone in moderate dosage had no effect, andspontaneous improvement followed by relapseoccurred after its discontinuance.
Case 3, a housewife aged 59, gave a history of severe andprogressive rheumatoid arthritis which began in 1944.She was treated with salicylates and physiotherapy, anda short course of corticotropin in 1951 gave temporarybenefit. In that year she had an unexplained pyrexialillness with severe pain at both lung bases, more leftthan right. An x-ray film showed bilateral basalmottling and fibrosis. While corticotropin had aprofound effect on the arthritic features of the disease,the intractable basal (? pleural) pain was untouched butsubsided slowly and spontaneously.
Later in 1952 phenylbutazone was tried, but had to be
stopped because of purpura and indigestion. She wasadmitted to hospital in August, 1955, and long-termprednisolone was started (15 mg. daily). At first sheimproved, but in a month or two was as bad as ever.Accordingly prednisolone was gradually discontinuedbetween March and July, 1956.
In March, 1956, she had noted that her hands seemednumb and useless, and she was unable to pick up smallobjects. At night she would be awakened by intenseburning pains in both hands and these symptoms per-sisted. She was, therefore, admitted for further inves-tigation in October, 1956. Sensory and motor signs ofperipheral neuropathy were found in both hands, andthere was reduced sensation over the toes and distalparts of the feet. She said on direct questioning thatshe had numbness of the toes but had not mentioned itas her hands were so much worse. Her rheumatoidarthritis was severe, but unchanged from the previousyear.
Treatment was by graded rest and salicylates. In thenext 6 months symptoms and signs of the neuropathycompletely disappeared, astereognosis being the lastabnormal feature to disappear. A Congo red test foramyloid disease was negative and skin and musclebiopsies were normal.
Comment. Symptoms and signs of a peripheralneuropathy affecting hands and feet appeared onreduction of dosage of prednisolone. No form oftreatment appeared to have any effect, but improve-ment took place naturally over a period of some6 months. An unexplained pain in the lowerthorax possibly pleural in origin had been an out-standing feature of this case 5 years previously, andunlike the arthritic features of the disease had notresponded to corticotropin given at that time.
Case 4, a porter aged 61, had developed rheumatoidarthritis in 1949. with involvement of many of theperipheral joints. In 1954 a period of rest in hospitalhelped him; phenylbutazone 400 mg. daily was startedand continued with sustained analgesic effect.He remained reasonably well and at work until
August, 1956, when he became disturbed at night bynumbness, paraesthesia, and burning pains in the handsand feet, which began to spread proximally up the limbs.His hands became useless because he was unable to feelwith his fingers and did not know where they were;he would drop objects and was unable to feed himselfor undo buttons. He was emphatic that these symp-toms were unlike anything connected with the arthritisthat he had previously experienced. Later, in October,1956, a generalized relapse of the arthritis set in and hewas admitted to hospital for treatment.
Clinically, he presented the picture of active rheumatoidarthritis with large axillary and epitrochlear glands, ulnarnodules, and extensor sheath swellings of both wrists.There was reduction of all types of sensation belowboth wrists and knees, and the distal halves of all fingerswere anaesthetic; the deep reflexes were still preserved.
474
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

NEUROPATHY IN RHEUMATOID DISEASEThe erythrocyte sedimentation rate varied from
35-52 mm./hr (Westergren). The sheep cell agglutina-tion test was positive, 1 : 138. All other possiblecauses of peripheral neuropathy were excluded as in theother patients. At no time was there albuminuria.
Phenylbutazone was continued and corticotropin20 mg. daily was begun. A week before his dischargefrom hospital the corticotropin was replaced in stages byprednisolone 15 mg. daily. The joints improved andover a month he lost his neuropathic symptoms, thoughsensation in all fingers was still reduced when he wasdischarged.When examined a month later in the out-patient
clinic, he was well and at work and there was no evidenceof neuropathy whatsoever.
Comment.-This patient, who was in his 3rd year oftreatment with phenylbutazone, developed a peri-pheral neuropathy with sensory but no motorfeatures affecting hands and feet. Treatment withphenylbutazone was continued, and the addition ofsteroid therapy had no immediate apparent effectthough features of the neuropathy gradually dis-appeared completely.
Case 5, a housewife aged 51, had had rheumatoid arthritisfor 19 years, beginning in the wrists and thereafterspreading to the hands and feet. The disease ran afluctuating but slowly progressive course, and there wasno improvement with courses of gold. 6 years ago(in 1951) cortisone therapy was started and has beencontinued until the present.
In May, 1956, the patient noted that her feet werebecoming numb up to the ankles. There was at firstassociated pain and paraesthesia, but these later passedoff. Numbness gradually spread proximally and herfeet became weak so that she could walk only with theaid of crutches. In September, 1956, her hands wereinvolved with burning pains and by the time of heradmission to hospital (November, 1956) she could nothold a pen or undo buttons.On examination she was moon-faced, and had
advanced but not very active rheumatoid arthritis.Sensation was reduced in the finger ends up to the proxi-mal interphalangeal joints. It was interesting how com-paratively slight these physical signs were compared withthe striking disability caused by the symptoms.
There was loss of all modes of sensation in the feetas far as the ankles, particularly over the lateral parts ofthe feet, and vibration sense was much diminished upto the knees. Ankle reflexes were absent and all move-ments of the feet were weak.The erythrocyte sedimentation rate was 58 mm. in
2 hours (Westergren), and haemoglobin was 94 per cent.with a normal total and differential white count. Therewas no albuminuria and no abnormality in the urinarydeposit. The Congo red test gave no evidence ofamyloiddisease. Examinations of the blood were negative forL.E. cells.
In hospital the patient was given corticotropin for a
time instead of cortisone, and afterwards cortisone wasstopped and then started again. None of these changesmade any difference to the neuropathy which was alsounaffected by vitamin B and vitamin B12.
Comment.-This mixed sensory and motor peri-pheral neuropathy of hands and feet came on after5 years of steroid therapy without any previouschange of dosage. The symptoms were extremelyincapacitating, though the physical signs wererelatively slight. Subsequent changes in steroidtherapy make no difference to the clinical picture.
Case 6, a spinster aged 57, gave a 6-year history ofrheumatoid arthritis, affecting knees, ankles, hands, andshoulders. When first seen in July, 1957, she statedthat for 2 months she had had "hot pins and needles in thefeet" and that more recently the feet had become numb;her hands were unaffected. She was taking an averageof 6 aspirins daily, together with 400 mg. phenylbutazone;steroids had never been given.On examination there were classical signs of rheuma-
toid arthritis in the joints, with enlarged epitrochlear andaxillary lymph nodes. Sensation to cotton wool andvibration was absent in the feet in a short sock distribu-tion, and sensation to pin prick was reduced. Powerwas well preserved in the feet, and the ankle reflexeswere present.
Case 7, a man aged 80, who was admitted to hospitalfor prostatectomy, later had a coronary thrombosis.When seen in the medical ward he gave a history ofhaving had rheumatoid arthritis for many years; he hadnever had cortisone. He said that for 2 to 3 years hehad noticed numbness and loss of control of his handsand feet.On examination, in addition to advanced changes of
rheumatoid arthritis, all modes of sensation were absentin the feet and grossly reduced in both hands.
Case 8, a housewife aged 63, had had progressive rheuma-toid arthritis for 2J years, which had been treated bysalicylates and physiotherapy. On admission to hos-pital she complained that she had lost sensation in the3rd, 4th, and 5th toes of both feet, and in the dorsum ofthe first joint proximally.On examination, she had active rheumatoid arthritis,
with swelling and tenderness of the metacarpophalangealjoints and proximal interphalangeal joints, the moreproximal joints being stiff and tender. Sensation wasabsent in the feet in the areas which she had noted werenumb.
Case 9, managing director aged 70, gave a 6-year historyof rheumatoid arthritis. When first examined in theWestminster Hospital in September, 1956, he was foundto have advanced and florid disease with large rheumatoidnodules. There were then no signs of neuropathy.Treatment was begun with 10 mg. prednisolone daily individed doses.During a subsequent admission (March, 1957) it was
6
475
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASESnoted that the arthritis had progressed despite steroidtherapy; he began to complain at that time of numbnessand paraesthesia of the feet, and sensation was absent onexamination, particularly on the lateral aspects of thefeet. These symptoms and signs had developed whilehe was taking prednisolone and without any reductionof the dose.The neuropathy is now improving, and there are no
objective signs though he still has minor subjectivecomplaints.
Case 10, a man aged 63, developed rheumatoid arthritis10 years ago, which progressed to involve most of hisjoints. After 2 years on steroid therapy, prednisolonewas gradually and very slowly reduced over a periodof4 months from 15 to 5 mg. daily. For the past 3 weekshe had had paraesthesia over the feet and heels, but oneweek after discontinuing steroid therapy completely helost the power of dorsiflexion in one foot, and paraesthe-sia became more marked, and sensation was diminishedover the anterior position of both feet, the lateral aspectmore than the medial. After 3 days power returned andthe sensory symptoms abated.
Comment.-This appears to be a steroid withdrawalsyndrome in miniature, followed by rapid improve-ment.
Case 11, a married woman aged 38, began to have painsin most peripheral joints in October, 1955, with earlymorning stiffness. Her symptoms were well controlledby soluble aspirin and she was able to continue all hernormal domestic activities. In April, 1956, she wasfirst referred to the Rheumatism Clinic at the West-minster Hospital; the sensitized sheep cell agglutinationtest was negative, and the erythrocyte sedimentationrate (Wintrobe) was 38 mm./hr. A diagnosis of rheu-matoid arthritis was made.Her condition began to deteriorate, and cortisone
100 mg. daily was begun by her general practitioner.Left lower chest pains occurred at this time with slighttenderness of the chest wall, but no L.E. cells werefound in the blood in June, 1956. There was apparentlya good response to cortisone for a few weeks.During August she had a relapse and had to remain
in bed with very painful joints, a fever of 100° F., head-ache and vomiting. Because of these symptoms corti-sone was suddenly stopped by her general practitioner,and a week later, her condition deteriorating, she wasadmitted to hospital as an emergency.She was ill and in great pain with tachycardia and
tenderness, but no swelling of the peripheral joints.Rales were present at both bases and it was noted thatboth ankle reflexes were absent and that sensation topin prick over her feet was impaired, although at thistime she made no complaint to suggest neurologicalinvolvement.On the day after admission L.E. cells were found in
the blood. Intense burning pains of both feet and legswere then present, necessitating large doses of pethidine.Signs of a peripheral neuropathy rapidly progressed sothat a week after admission there was complete anaes-
thesia of both feet with bilateral foot drop. By thattime a facial butterfly rash was obvious.
Despite treatment with antibiotics and large doses ofsteroid, up to 60 mg. prednisolone daily, she remainedextremely ill with an irregular fever of up to 1040 F., andsevere joint, chest, and limb pains; improvement wasvery slow and she was in hospital for over 5 months.On October 4, 1956, while she was on a maintenance
dose of 60 mg. prednisolone daily routine examinationfollowing a complaint of abdominal pain demonstrateda large cystic mass in the abdomen. A fortnight latershe passed per rectum a 30-cm. length of completethickness of colon, with disappearance of the "cyst" andrelief of her pain; this was thought to be due to anintussusception.
It was possible to let her leave hospital in February,1957, by which time she was quite well apart from acomplete bilateral foot drop; she was then taking 30 mg.prednisolone daily. Sensory signs had improved com-pared with those present on admission, but power inboth legs showed little sign of improvement.Her general condition has remained satisfactory and
the dose of prednisolone has been gradually reduced to15 mg. daily. Now, for the first time for a year, thereis slight dorsiflexion at the ankle and coarse sensationis present over both feet.
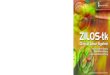
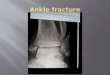
Comment.-This patient, probably a case of systemiclupus erythematosus from the commencement of hersymptoms, did not show the L.E. cell in the blooduntil prednisolone had been abruptly terminated byher general practitioner. This biological shock tothe system caused a flare-up, and apparently pro-duced the L.E. cell and precipitated a neuropathy.A high dosage of prednisolone was necessary to con-trol her symptoms; while she was on 60 mg. daily,a silent intussusception occurred and she passed30 cm. of her colon (Figs 3 and 4, opposite). Thisrelieved the abdominal symptoms, and now over ayear later, treated conservatively on a continued butlower dosage of prednisolone, she is in better generalcondition than since the onset of symptoms, thoughsome signs of the neuropathy persist. She has noresidual abdominal symptoms.
DiscussionA point to emphasize in all these cases was the
obvious clinical significance of the neuropathy; inmost cases this new group of symptoms was aprominent complaint. These, far from beingelicited by direct questioning, were often from thepatients' point of view the major disability. Ad-justed and used to some degree to their chronicrheumatoid complaints, they found these new super-imposed symptoms doubly distressing and demoral-izing. All these cases of peripheral neuropathyoccurred in long-standing advanced rheumatoidarthritis, but they did not occur in periods of
476
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

NEUROPATHY IN RHEUMATOID DISEASE
C)3 , o
'co
V~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Figs 3 and 4.-Case 11. Intuasuscepted colon from case of disseminated lupus erythematosus. The patient was on 60 ug. prednisolonedaily at the time. No operation was performed and the patient remains well I year later.
natural exacerbation or relapse. In the two worst(Case I and Case 11), severe motor and sensorychanges occurred within 2 weeks of abruptlystopping steroid therapy; as in all such cases sensorychanges preceded motor changes, the former beingthe more common. Two further cases occurredwithin 4 weeks of discontinuing steroid therapy;four out of eleven cases thus appear to have beenprecipitated by steroid withdrawal. Once theneuropathy had occurred, therapy appeared to beof no help; vitamins, steroids, and physiotherapycaused no improvement in the condition which,if it was going to improve, did so without regard tothe clinician's therapeutic endeavours. Naturalrecovery occurred in 4 days (Case 10) and after
10 months (Case 2); the latter case relapsed soonafterwards. It is of interest to compare these caseswith the acute infective polyneuritis described byGraveson (1957) which responded very satisfactorilyto steroid therapy within 1 to 2 weeks in seven out ofeight cases.The sensory changes occurring in rheumatoid
arthritis were symmetrical as compared with thefrequent asymmetry of the neuropathy seen inpolyarteritis nodosa unrelated to rheumatoid arth-ritis (Talbott and Ferrandis, 1956). As stated above,sensory always preceded motor changes; if the feetonly were affected the outer part of the foot showedmore marked changes than the inner. Three ofthese ten rheumatoid cases had fibrotic changes in
477
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASES
the lungs not explicable in terms of any otherpathological process. Blue, cold, moist hands,common in early rheumatoid arthritis, were notparticularly apparent in these cases; there seemedto be no correlation between a poor peripheralcirculation and the development of a neuropathy.In Case 1 small black areas, of the type describedand well illustrated by Bywaters (1957), occurredwhen there were no signs of peripheral neuropathy,sensory and motor changes taking place many
months later when the discoloured necrotic areas
had healed. It would seem that the milder arterialchanges present earlier were responsible for theselesions which flared into a florid polyarteritis on
steroid withdrawal.Unlike disseminated lupus erythematosus, rheu-
matoid arthritis rarely involves the kidneys, exceptby amyloid disease (Muehrcke, Kark, Pirani, andPollak, 1957). In these ten cases no renal abnor-malities were noted, nor did hypertension appear inany case. Other causes for a neuropathy, such as
porphyria, amyloidosis, avitaminosis, diabetes mel-litus, and subacute combined degeneration of thecord were looked for, but no signs of these disorderswere present. No cases occurred during or aftergold therapy. None of the rheumatoid cases was
highly febrile, though fever was present in the case
of disseminated lupus erythematosus (Case 11).The development of the neuropathy was not heraldedor accompanied by fever or systemic upset, or byany particular elevation of sedimentation rate or
sudden alteration in the pattern of plasma proteins.Skin and muscle biopsies in four cases were unhelpfuland a nerve biopsy showed only a non-specificdemyelination. An arterial biopsy showed no
abnormality in Case 1, who later at autopsy hadwidespread changes of polyarteritis nodosa. Eosino-philia was not present in any case.
How common are these lesions? We have no
exact figure to answer this question. After thefirst four cases were found, 100 consecutive cases ofrheumatoid arthritis attending the Unit as out-patients were carefully examined for this complica-tion, but none was found. Nevertheless, thoughrare, it is certainly not excessively rare, and it is ourimpression that the incidence is greater since steroidtherapy was introduced.
Freund, Steiner, Leichtentritt, and Price (1942)reported characteristic pathological lesions locatedin the perineurium in three out of five cases ofrheumatoid arthritis. They commented that thesharply nodular and peculiar granulomatous mor-
phology were features of a disease-specific appear-ance, but made no particular point of any vascularchanges; no such changes were seen in our cases.
Radnai (1953), however, emphasized the importanceof vascular changes in the development of a neuro-pathy in rheumatoid arthritis:
" . . . we have arrived at the conclusion that inthe muscles and nerves of patients suffering fromrheumatoid arthritis the continuous influence ofsome injury of unknown nature gives rise to con-stantly relapsing acute vascular changes of smallintensity for years or even for decades. Healing ofsuch lesions brings about complete or partialobstruction in more and more arterioles, thusleading to a permanent or transitory functionaldisturbance."
Slocumb (1953) drew attention 4 years ago to the"panangiitic and panmesenchymal" reactions whichoccurred on reduction of steroid dosage in rheuma-toid arthritis. Four of our eleven cases of peri-pheral neuropathy were seen within 4 weeks ofstopping such treatment.Kemper, Baggenstoss, and Slocumb (1957) also
reported that, of 52 rheumatoid patients studied atautopsy, 38 had received no cortisone. None ofthese developed generalized lesions of polyarteritisnodosa, whereas of the fourteen cortisone-treatedpatients four developed these lesions. In reviewingthe literature on the subject they consider that thevascular changes observed in rheumatoid arthritisfall into three groups:
(1) Perivascular or adventitial accumulation ofleucocytes, plasma, and other cells withoutnoticeable necrosis.
(2) Subacute arteritis with histiocytic and lympho-cytic infiltration through all layers of the vesselwall, without necrosis, but possibly with someexudation of fibrin and swelling of collagen.
(3) Lesions of acute arteritis with cellular infiltrationand necrosis of the vessel wall, a necrotizingangiitis.
These workers consider that their findings suggestthat in certain susceptible patients with rheumatoidarthritis the administration of cortisone mayprecipitate changes of the third group.
Bywaters (1957) has described arteritis in tenpatients with rheumatoid arthritis and states thata bland intimal proliferation of fibroblasts andmucoid material, sometimes with secondary fibrinclots on it, not unlike changes noted previously inscleroderma, is typical, Cruickshank (1953) foundevidence of an arteritis, past or present, in eighteenof 72 fatal cases of rheumatoid arthritis. He statesthat this arteritis of rheumatoid arthritis wasencountered most often in heart, muscles, andnerves, and that the incidence is probably consider-ably higher than these figures suggest. Arterialchanges in the lung in this condition have been
478
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

NEUROPATHY IN RHEUMATOID DISEASE
mentioned by Ellman and Ball (1948) and havebeen well illustrated by Price and Skelton (1956).
Ball (1953) and Sokoloff and Bunim (1957) havedrawn attention to the wide spectrum of changesthat may be seen in blood vessels in rheumatoidarthritis. It is noteworthy that in many articles onthis subject the illustrations show changes varyingfrom early inflammatory involvement of vessels toa fully-developed necrotizing arteritis histologicallyindistinguishable from polyarteritis nodosa.As has been remarked before, the majority of
such lesions in life are probably in silent areas andgive no outward sign or symptom of their presence;should they occur in the nervous system, however,and in particular in the peripheral nerves of handsor feet, the picture of a neuropathy rapidly becomesevident. That they did occur before the advent ofsteroid therapy is certain, but it seems likely thatthey are occurring more commonly and dramaticallynow that a large number of patients are receivingthis form of treatment. It may be that a milddiffuse arteritis is suppressed by such treatment,on withdrawal of which the condition flares intomore florid form, as seen in two of our cases wheretherapy was abruptly terminated.
Is the neuropathy entirely a feature of an arteritisor is there a rheumatoid neuropathy apart fromthis ? Against the latter are the following considera-tions:
(a) The absence of such a neuropathy in the activeflorid early case of rheumatoid arthritis. Patientswith neuropathy are mostly relatively advancedrheumatoids of long standing, and the diseaseis not particularly active at the time of develop-ment of the condition; a withdrawal of steroidsuppressive treatment seems more likely to befollowed by a peripheral neuropathy than doesa natural relapse.
(b) High-dosage suppressive steroid therapy doesnot improve the neuropathy as it does otherfeatures of the arthritis. Of interest here is thefinding that in Case 3 the acute lower chestpain from which she suffered and which appearedto be associated with a lower zone pulmonaryfibrosis was also completely untouched bysteroid therapy, which removed at the time allother symptoms and signs of the disease.
However, as the neuropathy appears to be dueto an arteritis which is part of the rheumatoiddisease process, one is in fact dealing with a realcomplication of rheumatoid arthritis. The con-dition is in fact a "rheumatoid neuropathy", unlessconsidered entirely a polyarteritic complication ofsteroid therapy. Against this is the fact that fiveof our patients had never had steroid therapy. Thedemyelination seen is merely a feature of ischaemicchange and is a non-specific finding.
Summary(1) Ten cases of peripheral neuropathy in rheu-
matoid arthritis are described and for comparisonone case of systemic lupus erythematosus. Of theseeleven cases, five had never received steroids, butin four the neuropathy developed within one monthof discontinuing such therapy. The two worstcases occurred within 7 and 14 days of abruptlystopping treatment with prednisolone.
(2) Sensory changes preceded motor in all casesin which both occurred. In six cases sensorychanges only were present.
(3) The development of a neuropathy led allthese patients to make fresh complaints. Theweakness and discomfort superadded to their usualarticular symptoms often proved particularly dis-tressing and demoralizing.
(4) Therapy had no effect on the nervous lesion:high steroid dosage, vitamins, and physiotherapymade no difference to the nervous signs and symp-toms. A major spontaneous improvement or com-plete recovery occurred in all cases in periods varyingfrom 3 days to one year, but signs persist to somedegree in all but two cases, and one case has relapsedafter partial recovery.
(5) There was no connexion in these cases withgold or phenylbutazone therapy. None hadreceived the former and the latter apparently playedno part in the three cases in which it was given.
(6) The unusual complication of intussusceptionand sloughing of 30 cm. of colon is reported in apatient with severe systemic lupus erythematosuswho was receiving 60 mg. prednisolone daily. Shemade a good recovery without operation and stillremains well 12 months later.
(7) The concept of a diffuse arteritis as part ofthe rheumatoid disease best explains these cases ofperipheral neuropathy; withdrawal of steroidtherapy, particularly if abrupt, may precipitate moreflorid changes.
Our thanks are due to Dr. William S. Tegner for per-mission to report the case histories of two of his patients,to Dr. Peter Hansell and the Department of MedicalPhotography, Westminster Medical School, for theirhelp with the illustrations, and to Professor D. H. Collinsand Dr. Bruce Cruickshank for their helpful commentsin Case 1.
REFERENCESBall, J. (1954). Annals of the Rheumatic Diseases, 13, 277.Brain, W. R. (1951). "Diseases of the Nervous System", 4th ed,
p. 814. Oxford University Press.Bywaters, E. G. L. (1957). Annals of the Rheumatic Diseases, 16, 84.Cruickshank, B. (1954). Ibid., 13, 136.Ellman, P., and Ball, R. E. (1948). Brit. med J., 2, 816.Freund, H. A., Steiner, G., Leichtentritt, B., and Price, A. E. (1942)
Amer. J. Path., 18, 865.Graveson, G. S. (1957). Lancet, 1, 340.Kemper, J. W., Baggenstoss, A. H., and Slocumb, C. H. (1957)
Ann. intern. Med., 46, 831.
479
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from

ANNALS OF THE RHEUMATIC DISEASESMuehrcke, R. D., Kark, R. M., Pirani, C. L., and Pollak, V. E. (1957).
Medicine (Baltimore), 36, 1.Price, T. M. L., and Skelton, M. 0. (1956). Thorax, 11, 234.Radnai, B. (1953). Acta morph. Acad. Sci. hung., 3, 87.Slocumb, C. H. (1953). Proc. Mayo Clin., 28, 655.Sokoloff, L., and Bunim, J. J. (1957). J. chron. Dis., 5, 668.Talbott, J. H., and Ferrandis, R. Moleres (1956). "Collagen
Diseases", p. 98. Grune and Stratton, New York and London.
Neuropathie dans l'arthrite rhumatismaleREsuME
(1) On decrit dix cas de neuropathie peripherique dansl'arthrite rhumatismale et, pour comparaison, un cas delupus erythemateux generalist. Parmi ces onze cas,cinq n'avaient jamais recu de steroides, mais chezquatre autres, la neuropathie survint dans le mois quisuivit l'interruption de cette therapie. Les deux cas lesplus graves se produisirent entre 7 et 14 jours apresl'arr& soudain du traitement a la prednisolone.
(2) Les phenomenes sensoriels prec&derent toujoursles moteurs; dans six cas ceux-ci furent absents.
(3) Le developpement de la neuropathie provoquades plaintes renouvellees des malades. La faiblesse etle malaise s'ajoutant a leurs habituels sympt6mesarticulaires se revle&ent deprimants et demoralisants.
(4) La therapie n'eut aucun effet sur la lesion nerveuse;administration de st6roides a haute dose, les vitamineset la physiotherapie n'amen&ent aucun changementdans les sympt6mes nerveux. Une amelioration impor-tante spontanee ou une complete guerison se produisirentdans tous les cas en des periodes variant de trois jours aun an, mais certains signes persisterent dans tous les cas,sauf deux, et un cas rechuta apres guerison partielle.
(5) Dans aucun cas n'y avait-il de lien avec la chryso-therapie ou la phenylbutazone. Aucun des maladesne recut de premise; la seconde, administree a troisd'entre eux apparemment ne joua aucun r6le.
(6) La complication rare d'invagination et de sphacelede 30 cm. de colon est signalee chez une malade atteintede lupus erythemateux generalise severe et recevant 60 mg.de prednisolone par jour. Elle guerit sans operation etse porte toujours bien, 12 mois plus tard.
(7) Le principe d'une arterite diffuse formant partiede la maladie rhumatismale offre la meilleure explicationde ces cas de neuropathie peripherique; l'interruption de
la therapie steroide, surtout si elle est faite brusquement,peut precipiter des alterations assez spectaculaires.
Neuropatia en la artritis reumatoideSUMARIO
(1) Se describen diez casos de neuropatia perifericaen la artritis reumatoide y, para comparar, un caso delupus eritematoso generalizado. De estos once casos,cinco nunca recibieron terapia esteroide, pero en cuatrootros la neuropatia ocurri6 dentro del mes que sigui6la interrupci6n de tal terapia. Los dos casos mas gravesse produjeron entre 7 y 14 dias despues de la interrupci6nrepentina del tratamiento con prednisolona.
(2) Los fen6menos motores, ausentes en seis casos,fueron siempre precedidos por las manifestacionessensorias.
(3) El desarrollo de la neuropatia trajo quejas repetidasde los enfermos. La debilidad y el malestar vinieron aanadirse a los sintomas articulates habituales con unefecto penoso y desmoralizador.
(4) Terapia fue sin efecto sobre la lesi6n nerviosaadministraci6n de esteroides en dosis altas, vitaminas yfisioterapia no produjeron cambio alguno en los sin-tomas nerviosos. Una mejoria importante espontaneao una cura completa se produjeron en todos los casos enperiodos de 3 dias a un ano, pero ciertas manifestacionespermanecieron en todos casos, salvo dos, y en un casohubo una recaida despues de una cura partial.
(5) En ningun caso se vi6 un lazo con sales de oroo la fenilbutazona. Ningun enfermo habia recibido losprimeros; la segunda, administrada en tres casos, nopareci6 haber desmpenado papel alguno.
(6) Se seniala la complicaci6n rara de invaginaci6n yesfacelo de 30 cm. del colon en una enferma con lupuseritematoso generalizado grave, recibiendo 60 mg. deprednisolona diaria. Recobr6 sin operaci6n y aun estabien, despues de doce meses.
(7) El concepto de una arteritis difusa formandoparte de la enfermedad reumatica ofrece la mejorexplicaci6n de estos casos de neuropatia periferica;la interrupci6n de la terapia esteroide, en particularrepentina, puede precipitar alteraciones algo asombrosas.
480
copyright. on January 29, 2021 by guest. P
rotected byhttp://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.16.4.471 on 1 Decem
ber 1957. Dow
nloaded from