Embed Size (px)
DESCRIPTION
neurologia
Citation preview

Radiology Case Presentation
David R. Beckert, MS-4
11/8/05

Case Background
• Clinical History: 22 y.o. female presented to Neuro angio for imaging of AVM, which was discovered at OSH, in order to proceed to interventional radiology for gamma knife ablation procedure.
• (Note: Unclear as to her original complaint that lead to the discovery of the AVM at the OSH)

Radiographic Images

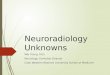
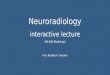
Medium-sized AVM

• Blood flow to AVM from internal carotid and vertebral
• Distal venous stricture also noted

Arteriovenous malformations
• Intracranial AVMs = 0.1% prevalence (aneurysms =1.0%).
• Supratentorial lesions = 90%
• Posterior fossa = 10%
• AVMs account for:– 1 to 2 % of all strokes– 3 % of strokes in young adults– 9 % of subarachnoid hemorrhages

AVM Clinical Summary
• AVMs usually present in the second to the fourth decade of life.
• Presentation: – Intracranial hemorrhage = 41-79 %– Seizures = 11-33 %– Headaches or progressive deficit– Younger patients (<30 yo) most often present
with seizures, while older patients more commonly present with hemorrhage

AVM Imaging
• Angiography is the gold standard for the diagnosis, treatment planning, and follow-up after treatment
• Anatomical and physiological information such as the nidus configuration, its relationship to surrounding vessels, and localization of the draining or efferent portion of the AVM are readily obtained
• Contrast transit times provide additional useful information regarding the flow state of the lesion; this is critical for endovascular treatment planning
• AVMs typically first discovered via MRI/CT• MRI- very sensitive for location purposes and following
pts after treatment



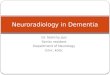
AVM Grading Scale

AVM Treatment• Pt. Age is most important factor• Options include surgery, stereotactic radiosurgery, and
endovascular embolization• Stereotactic radiosurgery — Stereotactically focused high energy
beams of photons or protons to a defined volume containing the AVM nidus induces progressive thrombosis.
• Time course usually one to three years, and the time between treatment and obliteration is referred to as the latency period.
• Once the lesion is completely obliterated, the hemorrhage risk from the AVM is very low
• Successful AVM obliteration with radiosurgery depends upon lesion size and dose of radiation (complications also depend on location/size of AVM and volume treated)

References
• Singer, RJ, Ogilvy, CS, Rordorf, G. Cerebral arteriovenous malformations. UpToDate Online 13.3. February 25, 2005.
• Spetzler, RF, Martin, NA. A proposed grading system for arteriovenous malformations. J Neurosurg 1986; 65:476.