Embed Size (px)
Citation preview
fhg – Zentrum für Gesundheitsberufe Tirol GmbH / University of Applied Sciences Tyrol
Lehrgang zur Weiterbildung §14a FHStG Osteopathie Neurovegetative Reactions of Spinal
Manipulations and Mobilizations in
Manual Therapy, Chiropractic and
Osteopathic Medicine
A literature review Master Thesis
Author: Koen Groot Zwaaftink, D.O.
Supervisor: Johan Schelpe, D.O. - MSc.Ost.Med
Gent, July 2016
Preface and Acknowledgements
This thesis is made as a completion of the Master of Science in
Osteopathy education. The thesis is original, unpublished work by the
author, K.H.Groot Zwaaftink.
The first time I heard about neurovegetative reactions and segmental
processes following a spinal manipulation or mobilization was during my
physiotherapy education. I wondered how it was possible that a local
technique changes general physiologic parameters so widely spread in
our body. Because of the distant physiologic effects I started searching
in literature for treatment options and possibilities how to use this
phenomenon to my therapeutic advantage. During the osteopathic
education some of my questions were answered, but my interest in the
real effects of spinal manipulation and mobilization and the best
technique to choose was awakened.
I would like to thank my family for all the love, understanding and time
they gave me to complete this thesis. Especially my girlfriend Inge and
the kids who missed their father in the evenings and weekends the last
months. I thank my promotor Johan Schelpe for his excellent guidance
and support during the process. I ‘am grateful to Ronald van Oers for
finding some full-text articles and always responding quickly. Also my
parents and parents-in-law deserve a special thanks for their wise
counsel and kind words which kept me motivated.
Koen Groot Zwaaftink
June 22, 2016
Enschede
Dedication
This thesis is dedicated to:
My girlfriend Inge
She has given me love and inner peace to complete th is thesis
Gwen & Kai
Their presence and smiles kept me focussed
My parents
Who give me confidence and all the possibilities
Table of contents
1. Introduction 9
2. Spinal manipulation and mobilization techniques 13
2.1 Spinal Manipulation 13
2.2 Spinal Mobilization 13
2.3 Neurophysiological Mechanisms 14
3. Neurovegetative Nervous System 17
3.1 Definition and homeostasis 17
3.2 Neurovegetative Nervous System and SMT 18
3.2.1 Vasomotor System 18
3.2.2 Sudomotor System 19
3.2.3 Visceral System 20
4. Method 22
4.1 Literature search 22
4.2 Eligibility criteria 22
4.2.1. Inclusion criteria 22
4.2.2. Exclusion criteria 23
4.3 Types of manual intervention 23
4.4 Types of outcome measures 23
4.5 Data extraction 24
4.6 PEDro Quality Rating 24
5. Results 25
5.1 Study Characteristics 28
- Table 1. Results from data extraction 30
- Table 2. Quality Assessment PEDro Scale 35
5.2 Peripheral Reactions Neurovegatative Nervous System 36
5.3 Reactions on SNS in relation to Pain Perception 38
5.4 Visceral Reactions of Neurovegatative Nervous System 40
5.5 Types of manipulation/mobilization techniques 41
- Table 3. Spinal manipulation versus mobilization 42
5.6 Synthesis of results 44
6. Discussion 45
7. Conclusion 56
- Funding 56
- Competing interests 56
- Author contributions 56
- Author details 56
8. Bibliography 57
9. List of abbreviations 69
10. Appendices 70
10.1 Table Literature search strategy 70
10.2 Table first selection of literature search 73
10.3 PEDro Quality Assessment Scale 78
Curriculum Vitae 81
Affidavit 82
Abstract Neurovegetative Reactions of Spinal Manipulations and Mobilizations in Manual Therapy, Chiropractic and Osteopathic Medicine
A literature review Author: Koen Groot Zwaaftink D.O. Supervisor: Johan Schelpe D.O.-MSc.Ost.Med.
Master of Science in Osteopathy, University of Applied Sciences Tyrol
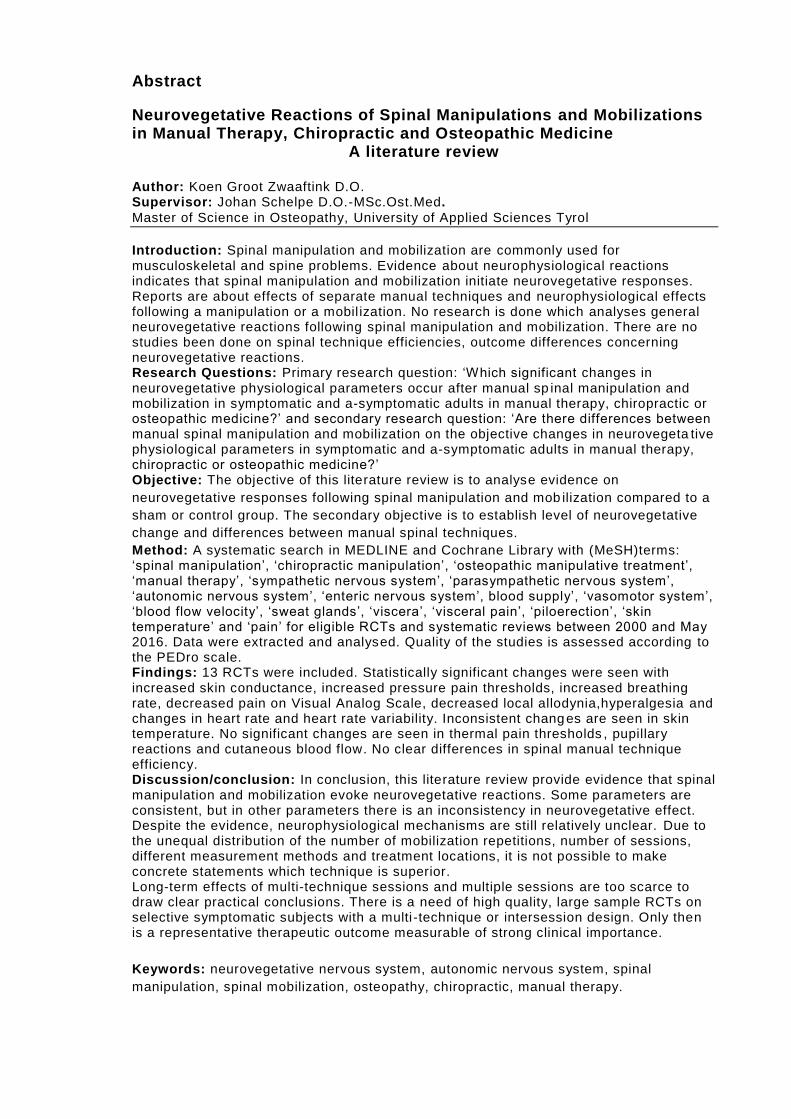
Introduction: Spinal manipulation and mobilization are commonly used for musculoskeletal and spine problems. Evidence about neurophysiological reactions indicates that spinal manipulation and mobilization initiate neurovegetative responses. Reports are about effects of separate manual techniques and neurophysiological effects following a manipulation or a mobil ization. No research is done which analyses general neurovegetative reactions following spinal manipulation and mobilization. There are no studies been done on spinal technique efficiencies, outcome differences concerning neurovegetative reactions. Research Questions: Primary research question: ‘Which significant changes in neurovegetative physiological parameters occur after manual sp inal manipulation and mobilization in symptomatic and a-symptomatic adults in manual therapy, chiropractic or osteopathic medicine?’ and secondary research question: ‘Are there differences between manual spinal manipulation and mobilization on the objective changes in neurovegeta tive physiological parameters in symptomatic and a-symptomatic adults in manual therapy, chiropractic or osteopathic medicine?’ Objective: The objective of this literature review is to analyse evidence on
neurovegetative responses following spinal manipulation and mob ilization compared to a
sham or control group. The secondary objective is to establish level of neurovegetative
change and differences between manual spinal techniques.
Method: A systematic search in MEDLINE and Cochrane Library with (MeSH)terms: ‘spinal manipulation’, ‘chiropractic manipulation’, ‘osteopathic manipulative treatment’, ‘manual therapy’, ‘sympathetic nervous system’, ‘parasympathetic nervous system’, ‘autonomic nervous system’, ‘enteric nervous system’, blood supply’, ‘vasomotor system’, ‘blood flow velocity’, ‘sweat glands’, ‘viscera’, ‘visceral pain’, ‘piloerection’, ‘skin temperature’ and ‘pain’ for eligible RCTs and systematic reviews between 2000 and May 2016. Data were extracted and analysed. Quality of the studies is assessed according to the PEDro scale. Findings: 13 RCTs were included. Statistically significant changes were seen with increased skin conductance, increased pressure pain thresholds, increased breathing rate, decreased pain on Visual Analog Scale, decreased local allodynia,hyperalgesia and changes in heart rate and heart rate variability. Inconsistent changes are seen in skin temperature. No significant changes are seen in thermal pain thresholds , pupillary reactions and cutaneous blood flow. No clear differences in spinal manual technique efficiency. Discussion/conclusion: In conclusion, this literature review provide evidence that spinal manipulation and mobilization evoke neurovegetative reactions. Some parameters are consistent, but in other parameters there is an inconsistency in neurovegetative effect. Despite the evidence, neurophysiological mechanisms are still relatively unclear. Due to the unequal distribution of the number of mobilization repetitions, number of sessions, different measurement methods and treatment locations, it is not possible to make concrete statements which technique is superior. Long-term effects of multi-technique sessions and multiple sessions are too scarce to draw clear practical conclusions. There is a need of high quality, large sample RCTs on selective symptomatic subjects with a multi -technique or intersession design. Only then is a representative therapeutic outcome measurable of strong clinical importance. Keywords: neurovegetative nervous system, autonomic nervous system, spinal
manipulation, spinal mobilization, osteopathy, chiropractic, manual therapy.
Abstract in German
Neurovegetative Reaktionen auf Manipulationen und Mobilisationen
der Wirbelsäule in der manuellen Therapie, Chiropraktik und
Osteopathie
Eine Literaturstudie
Autor: Koen Groot Zwaaftink D.O. Supervisor: Johan Schelpe D.O.-MSc.Ost.Med.
Master of Science in Osteopathy, University of Applied Sciences Tyrol
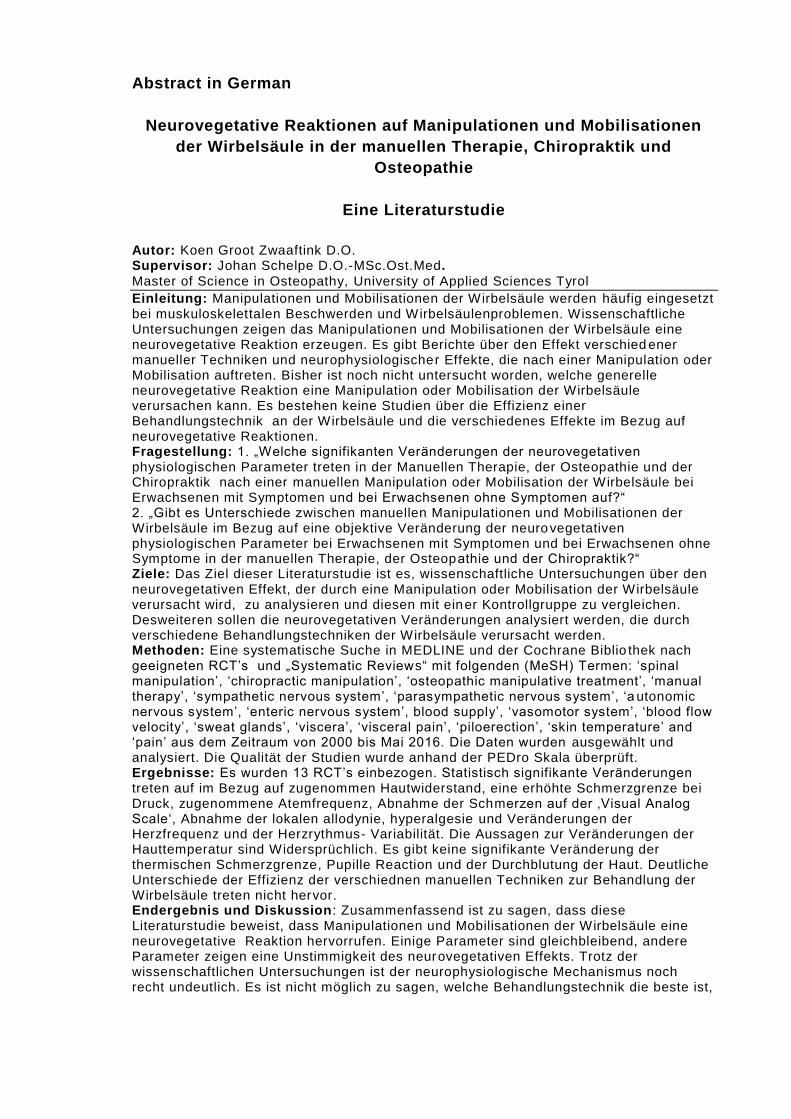
Einleitung: Manipulationen und Mobilisationen der Wirbelsäule werden häufig eingesetzt bei muskuloskelettalen Beschwerden und Wirbelsäulenproblemen. Wissenschaftliche Untersuchungen zeigen das Manipulationen und Mobilisationen der Wirbelsäule eine neurovegetative Reaktion erzeugen. Es gibt Berichte über den Effekt verschied ener manueller Techniken und neurophysiologischer Effekte, die nach einer Manipulation oder Mobilisation auftreten. Bisher ist noch nicht untersucht worden, welche generelle neurovegetative Reaktion eine Manipulation oder Mobilisation der Wirbelsäule verursachen kann. Es bestehen keine Studien über die Effizienz einer Behandlungstechnik an der Wirbelsäule und die verschiedenes Effekte im Bezug auf neurovegetative Reaktionen. Fragestellung: 1. „Welche signifikanten Veränderungen der neurovegetativen physiologischen Parameter treten in der Manuellen Therapie, der Osteopathie und der Chiropraktik nach einer manuellen Manipulation oder Mobilisation der Wirbelsäule bei Erwachsenen mit Symptomen und bei Erwachsenen ohne Symptomen auf?“ 2. „Gibt es Unterschiede zwischen manuellen Manipulationen und Mobilisationen der Wirbelsäule im Bezug auf eine objektive Veränderung der neurovegetativen physiologischen Parameter bei Erwachsenen mit Symptomen und bei Erwachsenen ohne Symptome in der manuellen Therapie, der Osteopathie und der Chiropraktik?“ Ziele: Das Ziel dieser Literaturstudie ist es, wissenschaftliche Untersuchungen über den neurovegetativen Effekt, der durch eine Manipulation oder Mobilisation der Wirbelsäule verursacht wird, zu analysieren und diesen mit einer Kontrollgruppe zu vergleichen. Desweiteren sollen die neurovegetativen Veränderungen analysiert werden, die durch verschiedene Behandlungstechniken der Wirbelsäule verursacht werden. Methoden: Eine systematische Suche in MEDLINE und der Cochrane Biblio thek nach geeigneten RCT’s und „Systematic Reviews“ mit folgenden (MeSH) Termen: ‘spinal manipulation’, ‘chiropractic manipulation’, ‘osteopathic manipulative treatment’, ‘manual therapy’, ‘sympathetic nervous system’, ‘parasympathetic nervous system’, ‘a utonomic nervous system’, ‘enteric nervous system’, blood supply’, ‘vasomotor system’, ‘blood flow velocity’, ‘sweat glands’, ‘viscera’, ‘visceral pain’, ‘piloerection’, ‘skin temperature’ and ‘pain’ aus dem Zeitraum von 2000 bis Mai 2016. Die Daten wurden ausgewählt und analysiert. Die Qualität der Studien wurde anhand der PEDro Skala überprüft. Ergebnisse: Es wurden 13 RCT’s einbezogen. Statistisch signifikante Veränderungen treten auf im Bezug auf zugenommen Hautwiderstand, eine erhöhte Schmerzgrenze bei Druck, zugenommene Atemfrequenz, Abnahme der Schmerzen auf der ‚Visual Analog Scale‘, Abnahme der lokalen allodynie, hyperalgesie und Veränderungen der Herzfrequenz und der Herzrythmus- Variabilität. Die Aussagen zur Veränderungen der Hauttemperatur sind Widersprüchlich. Es gibt keine signifikante Veränderung der thermischen Schmerzgrenze, Pupille Reaction und der Durchblutung der Haut. Deutliche Unterschiede der Effizienz der verschiednen manuellen Techniken zur Behandlung der Wirbelsäule treten nicht hervor. Endergebnis und Diskussion: Zusammenfassend ist zu sagen, dass diese Literaturstudie beweist, dass Manipulationen und Mobilisationen der Wirbelsäule eine neurovegetative Reaktion hervorrufen. Einige Parameter sind gleichbleibend, andere Parameter zeigen eine Unstimmigkeit des neurovegetativen Effekts. Trotz der wissenschaftlichen Untersuchungen ist der neurophysiologische Mechanismus noch recht undeutlich. Es ist nicht möglich zu sagen, welche Behandlungstechnik die beste ist,
da die Angaben zur Anzahl der Wiederholungen der Mobili sationen, sowie die Anzahl der Behandlungen, die Behandlungsorte und auch die Testmethoden unterschiedlich sind. Der Langzeiteffekt einer Behandlung mit verschiedenen Behandlungsmethoden und mehreren Behandlungen ist noch nicht ausreichend untersucht, um h ierzu eine Aussage für die Praxis machen zu können. Es werden mehr RCT’s mit guter Qualität und großen Untersuchungsgruppen benötigt, die sich auf selektive Zielgruppen beziehen, die mit verschiedenen Techniken behandelt werden oder mehrere Behandlungen be kommen, um ein repräsentatives therapeutisches Ergebnis mit wichtiger klinischer Bedeutung zu erzielen. Schlüsselwörter: neurovegetatives Nervensystem, autonomes Nervensystem, Manipulation der Wirbelsäule, Mobilisation der Wirbelsäule, Osteopathie, Chiro praktik, Manuelle Therapie
9
1. Introduction
Spinal manipulation is generally accepted as a treatment option in
management of musculoskeletal disorders. The effectiveness of spinal
manipulative therapy to treat musculoskeletal disorders and spinal pain has
been confirmed in several studies [46,136,4]. Evidence report that spinal
manipulative therapy provides greater improvement for pain and function
than a placebo or no treatment [4,46]. A systematic review of Michaleff et al.
found that SMT is a cost-effective treatment to manage spinal pain when
used alone or in combination with general practice care, like mobilization
[106]. Spinal manipulative therapy (spinal manipulation and mobilization) is
usually provided by manual therapists, osteopaths and chiropractic doctors
or therapists. Approximately 26% of the people worldwide visit a doctor or
therapist for spinal manipulative therapie [38].
Despite studies supporting the effectiveness of SMT, neurophysiological
mechanisms of SMT are not fully understood. As result that the National
Institutes of Health specially addresses the lack of a clear
neurophysiological explanation as a scientific problem [56].
Manipulation and mobilization effects cannot be solely biomechanically
explained. First, scientists believe that biomechanical changes following
SMT are only transient on range of motion, but no lasting structural
changes occur [165,54]. Second, improvement and effects following SMT are
reported not only locally, but also remote of the treated area [24,169]. Several
studies have shown that effects of spinal manipulation and mobilization are
beyond biomechanical changes only [10,15,37,126,159,121,118,91]. In the current
literature there is no clear explanation for some spinal manipulation and
mobilization effects [9]. Researchers proposed hypotheses on mechanical,
neurophysiological and psychological grounds. They think that extra-
biomechanical changes are supra-spinal modulated and partly caused by
the neurovegetative nervous system [9,10,37,50,126,138,147,178,168,184]. There is
evidence that manipulation and mobilization causes a sympathoexcitatory
effect and that the reaction is not only local but also segmentally and
supra-segmentally reactions are possible [18,20,80,86,91,121,150,154,159,171].
1 0
Bialosky et al. and Vicenzino et al. demonstrated a sympathoexcitatory and
hypoalgesic effect following manipulation and mobilization in areas that are
segmentally related [10,169,171]. Other studies provide evidence that the
hypoalgesic effect is not only segmentally coordinated, but also supra-
segmental [168,159,111].
Within the nervous system the somatic and neurovegetative nervous
system work together, with an interaction between both systems. By
treating or stimulating the somatic nervous system the neurovegetative
nervous system can be influenced [7,6,19,125,139,140,141,142,143]. Scientists have
found that in several regions nervous system there is an interaction
between the somatic and neurovegetative nervous system. Areas are
identified in the periphery, dorsal horn of spinal cord, brainstem and the
brain [7,150, 187]. After spinal manipulation and mobilization there are
changes in the neurovegetative nervous system reported. Significant
changes in peripheral skin temperature (ST), skin conductance (SC),
cutaneous blood flow (CBF) and pain perception is seen in several
studies.[159,91,122,123,134,111,113,80,170,171,172] Most of the performed studies
demonstrate significant neurovegetative changes in sympathetic nervous
system (SNS) [159,91,122,123,134,111,113,80].
Results of the studies are not always consistent and the outcome values
differ between the studies. Studies often used different manual techniques
and performed treatments on not the same spine region, making it difficult
to draw conclusions about efficacy for the practice. Studies on spinal
techniques and neurovegetative effects are focussed on a single region of
the spine (cervical, thoracic or lumbar spine) and effects are locally
measured (face, upper or lower extremity). There are a few systematic
reviews that combined the neurovegetative outcomes of the upper and
lower extremity, but analysed solely manipulation or mobilization effects.
Most of the studies investigate peripheral neurovegetative reactions
following spinal manipulation or mobilization and only a few examined
visceral reactions. Most researchers measure a single manual intervention
(mobilization or manipulation) and hardly any analyses outcomes and
1 1
differences of the various spinal techniques. A literature review on
neurovegetative reactions following a spinal manipulation or mobilization of
the total body, peripheral and visceral has not been done. No literature
review has been published that investigates the differences in
neurovegetative outcomes between various spinal manipulation and
mobilization techniques. Because of this the following research questions
have been drawn up.
The primary research question of the literature review is:
- Which significant changes in neurovegetative physiological
parameters occur after manual spinal manipulation and mobilization
of symptomatic and a-symptomatic adults in manual therapy,
chiropractic or osteopathic medicine?
Secondary research question:
- Is there a difference between manual spinal manipulation and
mobilization on neurovegetative physiological parameters of
symptomatic and a-symptomatic adults in manual therapy,
chiropractic or osteopathic medicine?
In order to answer the research questions a literature review between 2000
and May 2016 is done in MEDLINE and Cochrane Library with the following
MeSH-terms: ‘spinal manipulation’, ‘chiropractic manipulation’, ‘osteopathic
manipulative treatment’, ‘manual therapy’, ‘sympathetic nervous system’,
‘parasympathetic nervous system’, ‘autonomic nervous system’, ‘enteric
nervous system’, blood supply’, ‘vasomotor system’, ‘blood flow velocity’,
‘sweat glands’, ‘viscera’, ‘visceral pain’, ‘piloerection’, ‘skin temperature’
and ‘pain’. Afterwards the data is extracted and analysed. The quality of the
studies is assessed according to the PEDro scale.
The thesis shows general information and explanatory models on spinal
manipulation or mobilization and the neurovegetative nervous system. It
describes outcomes in the neurovegetative nervous system (sympathetic,
parasympathetic and enteric nervous system) of skin conductance (SC),
skin temperature (ST), cutaneous blood flow (CBF), pain perception (VAS
1 2
and pressure pain thresholds) and visceral changes. In the discussion
section the results following spinal manipulation or mobilization are
discussed as well as the used study methods and clinical relevance.
The thesis is orginized in 4 sections. The thesis starts with a short
theoretical section, spinal manipulation and mobilization are described and
current neurophysiological explanatory models are presented. Then
methodology and search strategy are described, followed by results and
discussion. Abbreviations, appendices, curriculum vitae of the author and
affidavit are listed at the end of the thesis.
This literature review should provide valuable information for manual
therapists, osteopaths and chiropractic practitioners about neurovegetative
reactions following spinal manipulation and mobilization. Information which
has an direct effect on the practice for all therapists and physicians who
uses spinal manipulative treatments. More understanding leads to better
desision-making and quality in health care.
1 3
2. Spinal manipulation and mobilization techniques
2.1 Spinal manipulation
Spinal manipulation can be described as: A therapeutic intervention
performed on spinal articulations which are synovial jo ints. These
articulations in the spine that are amenable to spinal manipulative therapy
include the zygapophyseal joints, the atlanto-occipital, atlanto-axial, lumbo-
sacral, sacroiliac, costotransverse and costovertebral joints [87]. Gross et
al. defined a spinal manipulation as “a localized force of high velocity and
low amplitude directed at the spinal joints” [46]. Manipulation is known by
several other names. Chiropractors usually refer to manipulation of a spinal
joint as an ‘adjustment’ and following the labeling system by Maitland a
manipulation is synonymous with a grade V mobilization [98,99]. Manipulation
has distinct biomechanics and can be distinguished from other spinal
manual techniques such as mobilizations [50,37,51]. Because of this
biomechanics the term high velocity low amplitude thrust (HVLAT) is
normally used.
2.2 Spinal mobilization
The definition of a spinal mobilization is; a type of passive movement of a
spinal segment or region and can be described as a gentle, often
oscillatory, passive movement applied to a spinal region or segment to
increase the passive range of motion of that segment or region ” [17,107].
Mobilizations use a low grade-velocity, small or large amplitude, passive
movement within the patient ’s range of spinal motion and control [46]. Some
researchers refer to spinal manipulative therapy (SMT), including both
manipulation and mobilization techniques. Also the term osteopathic
manipulative treatment (OMT) is used in several studies. This is a core set
of spinal (HVLAT and mobilization) and non-spinal (myofascial, muscle
energy, strain-counterstrain, vascular) techniques. In this literature review
with a spinal manipulation is meant a HVLAT technique and with a spinal
mobilization a low grade-velocity, small or large amplitude, passive
movement within the patient’s range of spinal motion and control . With SMT
in this literature review is meant spinal manipulation and/or mobilization.
1 4
2.3 Neurophysiological mechanisms
Evidence indicates that SMT techniques work through biomechanical and
neurophysiological mechanisms. Despite the evidence supporting the
effectiveness of SMT [46,136,4], neurophysiological mechanisms of SMT are
not fully understood. Studies suggest that in addition to the biomechanical
effects other neurophysiological mechanisms are present [126,9,37,184]. They
suggest that a mechanical force (manipulation or mobilization) is necessary
to initiate a chain of neurophysiological responses which are responsible
for the local and central effects following SMT [9,184]. Theories on
neurophysiological processes likely find the origin from a peripheral
mechanism, spinal cord mechanism and supra-spinal mechanisms.
Evidence for a peripheral mechanism is reported by studies that measure a
local change, like hypoalgesia and reflex changes, following SMT [9,109,184].
Peripheral lesions induce a local inflammatory response which stimulate
healing processes and produces local hyperalgesia. Inflammatory
mediators and peripheral nociceptors react due to the inflammatory
response and spinal manipulation and mobilization directly can affect this
process. Studies report a significant reduction of cytokines level in blood or
serum, changes in blood level of beta-endorphin, anandamide, N-
palmitoylethanolamide, serotonin and endogenous cannabinoids in subjects
that received SMT [162,29,104]. Studies have found anatomical vascular
connections between peripheral nociceptors and sympathetic neurons at
the terminal axons and within the spinal ganglion [157]. Local lesions
stimulate interconnection and makes primary afferent neurons more
sympathetic sensitive due to increase of adrenergic receptors [157].
Evidence report an increase sympathetic activity following SMT
[10,159,91,121,171], or the sympathoexcitation has an influence on the micro-
vascularization between primary afferents and sympathetic fibers is not
known.
SMT has an effect on spinal processes and decreases activation of the
dorsal horn [14,126,184]. The result of SMT is an increased activation of
muscle spindles, capsule receptors and Golgi tendon organs which
1 5
influences pain transmission in the dorsal horn [14,126]. Direct evidence
comes from a study of Malisza et al. were decreased dorsal horn
excitability was seen by functional MRI following SMT [100]. Indirect
evidence for spinal mechanisms is reported in several studies. SMT is
associated with hypoalgesia [109,171,172,91], afferent discharge [27], motoric
function [21,31] and changes in muscle activity [52,161]. In addition to the
mentioned somatic changes, there are also changes described in visceral
and humeral function following SMT [15,137,43,138,18,19,91]. Also evidence
indicates that SMT has a postulated effect in visceral disorders, such as
asthma [5] and hypertension [128].
Spinal changes have been shown to occur in caudal dermatomes to the
treated area [12]. The presence or absence of cavitation during thrust
manipulation was not associated with differences in outcome [10].
Supra-spinal reactions after SMT are reported due to changes in insular
cortex oxygenation, dorsal periaqueductal grey matter (dPAG) and
participant’s expectation (placebo). Oxygenation changes in insular cortex
are seen by functional magnetic resonance imaging (fMRI) after SMT [156]. It
shows a significant relationship between reduced oxygenation and reduced
pain ratings immediately after thrust manipulation in a-symptomatic
subjects. These findings are consistent with the results of Malisza et al.
who also found supra-spinal changes with fMRI following SMT [100]. Other
studies demonstrate that these supra-spinal changes are associated with
neurovegetative changes [170,171,111,159,186].
Ogura et al. demonstrated that SMT elicits sympathetic inhibition in part of
the brain [118]. A study using positron emission tomography (PET) found a
reduced activation in the cerebellar vermis and increased activation in parts
of the limbic system. Several studies have showed that spinal mobilization
produced a hypoalgesic effect [152,91,109,159,121,171,172]. This effect could be
due to descending serotoninergic or noradrenergic inhibitory mechanisms
via corticospinal projects of the dPAG. Scientists relate to noradrenaline, a
dPAG neurotransmitter more effective in inhibiting mechanical nociception
than thermal nociception which is serotoninergic regulated [89,90].
Researchers think that SMT produces the right stimulus for dPAG regulated
1 6
nonopioid analgesia, hypoalgesia and sympathoexcitatory effects
[159,121,171].
Additionally psychological factors and placebo may be inseparable with
SMT effects [36,82,8,12]. Expectation for the effectiveness of SMT can
significantly influence the result [12]. This may support the hypothesis that
the psychological and emotional factors from the cortex influence the
descending anti-nociceptive pathways from the dPAG [12,8].
Some scientists claim that the biomechanical effects associated with spinal
techniques are non-specific and not related to the type of manual technique
[51,133,105]. Another claim is that the biomechanical effects are transitory and
without structural changes [165,49]. Bialosky et al. described that the
biomechanical input applied during manipulations and mobilizations is the
provocative factor for a cascade of neurophysiological reactions and that
the spinal techniques are imprecise [9]. Through this neurophysiological
cascade changes on peripheral, spinal and supra-spinal level are possible.
This indicates that we probably have to change our vision about
manipulations and mobilizations of the spine. Maybe we have to approach it
from a less technical, biomechanical point of view and have to shift more to
a neurophysiological explanation.
1 7
3. Neurovegetative Nervous System
3.1 Definition and homeostasis
Langley described the neurovegetative nervous system as “a system of
nerves that regulate the function of all innervated tissues and organs
throughout the vertebrate body except striated muscle fibers; that is, the
innervation of the viscera, vasculature, glands and some other tissues” [59].
The neurovegetative nervous system consists out of three parts: the
parasympathetic nervous system, the sympathetic nervous system and the
enteric nervous system” [59]. Spinal manipulation and mobilization can
affect the neurovegetative nervous system on a local, spinal and supra-
spinal level. A part of the interconnection of the somatic (spine) and
neurovegetatve system is formed by neurological spinal reflexes. According
to Pickar et al. the spinal reflexes are “a type of neurological circuit that
functionally connects the biomechanical and chemical environment of the
musculoskeletal tissues with the non-musculoskeletal tissues” [126]. This
circuit consists of primary afferents which carry mechanical, chemical and
thermal stimuli to the central nervous system. An interaction in the central
nervous system (spinal or supra-spinal) and an efferent neurovegetative
reaction [126]. An important function of these reflexes is body protection and
spinal regulation of maintaining the homeostasis and allostasis of the body
[78]. The concept of homeostasis is formulated by Walter B. Cannon in 1929
and it means the maintenance of physiological parameters such as
concentration of ions, blood glucose, arterial blood gases, core-
temperature in a narrow range. Allostasis is described as stabilizing the
internal milieu during changes of the body and during activity [78].
Homeostatic and allostatic regulation involves the neurovegetative nervous
system, the endocrine system, the central nervous system and the
respiratory system [59].
1 8
3.2 Neurovegetative Nervous System and SMT
Studies demonstrated that SMT can alter physiological processes and
affect the neurovegetative nervous system
[159,91,122,123,134,111,113,80,170,171,172,83,109,122,123] . Effects after spinal
manipulation and mobilization are reported in physiological changes of skin
temperature (ST), skin conductance (SC), cutaneous blood flow (CBF),
visceral activity, pressure pain threshold (PPT) and pain intensity
[159,91,122,123,134,111,113,80,170,171,172]. There are different types of spinal reflex
pathways between the somatic (spine) and neurovegetative nervous system
[65,91,126,139,140,141,142,143,67]. Spinal reflex pathways are modulated and
controlled by supra-spinal structures, like lower brain stem, telencephalon,
limbic system and hypothalamus [67,61]. For measuring the peripheral activity
of the SNS, the SC and ST are commonly used. SC and ST are
measurements values of the sudomotor and skin vasomotor function and
are dependent on the sympathetic activity.
3.2.1 Vasomotor system
Stimulation of the SNS results in vasoconstriction of the artero-venous
anastomoses in the skin, which results in a decreased cutaneous blood
flow, leading to a decrease of ST [23]. Animal experimental studies report
that low-threshold mechanoreceptive afferents out of the skin leads to
excitation of the skin vasoconstrictor neurons [65]. The opposite reaction
happens by stimulation skin nociceptors [69]. In the human skin the majority
of the vasomotor neurons are sympathetic vasoconstrictor neurons, but in
some parts there are also sympathetic vasodilator neurons [64]. Experiments
report that active sympathetic vasodilatation occur in the proximal skin of
the extremities due to vasodilator neurons [75,79]. It is unclear of distinct
populations of skin vasodilator neurons are active stimulated or are
generated in association of sudomotor neurons [70]. Evidence of existence
of skin vasodilator neurons is indirect and is still debated [75,79]. Animal
studies reported that the skin vasoconstrictor neurons differ according the
section of the vascular bed they innervated and according to the
localisation and type of skin (glabrous or hairy skin) [64]. It is expected that
the activity pattern of the skin vasomotor neurons is not uniform and
1 9
dependent on the above mentioned differences [66]. Skin vasoconstrictor
neurons are thermo-sensitive and react on arterial chemo- and
baroreceptors [66,68]. Activity of the supra-spinal level and cardiovascular
and respiratory reflexes also play an important role in regulation skin
vasoconstrictor neurons [66,67]. The baroreceptive spinal reflexes are
respiratory and cardiovascular controlled and skin vasomotor changes are
seen by deep breaths, body position changes and altered heart frequencies
[66,67]. The hairy skin vasoconstrictor neurons are more sensitive for
baroreceptor reflexes than the glabrous skin vasoconstrictor neurons (palm
of the hands) [68]. Thermal stimuli are the most specific stimuli and result in
increased or decreased activity in the distal skin vasoconstrictor neurons.
All or most distal extremity skin vasoconstrictor neurons are involved in
thermoregulation [66,45]. Vasoconstrictor neuron activity is also dependent
on the mental state, arousal because they are supra-spinal mediated by
cerebral cortex and limbic system [67]. Arousal, emotional stimuli and
hyperventilation has an excitatory effect on the skin vasoconstrictor
neurons [67].
3.2.2 Sudomotor system
Increased activity of the SNS also results in an increased sudomotor
function, via the cholinergic neurons, which results in increased sweat
gland activity. The increased sudomotor function leads to a subsequent
decrease of skin resistance potential and an increase skin conductance
(SC) [2]. This reaction is a result of a primitive ‘fight or flight’ mechanism
whereby blood flow is sent to the muscles and heart and is redirected away
from the cutaneous surface. This reaction is combined with increased
sweating of the palmar area of the hands and feet in order to strengthen
the grasp or grip for escape and to play a role in thermoregulation by
physical activity [2]. Sudomotor neurons are active in high ambient
temperatures and silent at low ambient temperatures [73].
Observed single sudomotor neuron action potentials are followed by fast
transient skin potential changes. This indicates that sudomotor neurons
discharge synchronously [71]. Sudomotor neuron and skin vasoconstrictor
neuron recordings in animal studies reveal that the both neurons not react
2 0
simultaneously in the glabrous skin [71]. Studies on cats reported that
sudomotor neurons are reciprocally organized to the vasoconstrictor
neurons. When afferent stimulation sudomotor neurons inhibits, skin
vasoconstrictor neurons are excited [73]. Sudomotor neurons react on
nociception, arterial chemoreceptors, arousal states and emotional stimuli
[61]. At high temperatures sudomotor neurons are rhythmic activated with
the arterial pressure wave [73]. Changes in arousal, emotional stimuli and
deep breathing alters sudomotor activity in the glabrous skin of hands, feet,
armpits and some parts of the face [61]. Activation of the sympathetic
pathway to the sudomotor neurons of the extremities is initiated from the
frontal cortex and demonstrates that spinal level is regulated by supra-
spinal processes [61]. Stimulation of arterial baroreceptors has no effect on
sudomotor neurons [72]. In cats a vibration stimulus and cutaneous
mechanoreceptors stimulus did not lead to a change in activity in
sudomotor neurons [72]. Sudomotor neurons thresholds are location and
skin type dependent [73]. Proximal hairy skin sudomotor neurons have other
thermal thresholds than in the glabrous skin [61].
Animal studies have reported that regulation of the neurovegetative
nervous system is regulated by segmentally organized reflexes in response
to stimulation of skin, muscles and various paraspinal tissues [139,140,141,142].
Depending on the type of stimulus or which visceral organ responses can
be dominant sympathetic or parasympathetic. Some responses have
propiospinal and segmental characteristics, while others have supra-spinal
characteristics [139]. Animal studies have reported that muscle spindle
activation can elicit responses of the neurovegetative nervous system [141].
Stimulation of muscle spindles due to spinal manipulation and mobilization
can trigger these responses. Especially the cervical region is of importance
because it histologically contains a high density of muscles spindles and
Golgi tendon organs [102].
3.2.3 Visceral system
There is evidence that SMT has a positive effect on certain visceral
disorders [15,5,115,128]. Studies report positive effects on the cardiovascular
2 1
system, gynecological problems and asthma [15,5,115,128]. Primary afferents
for skin, deep somatic tissues and viscera form spinal reflex circuits with
neurovegetative preganglionic neurons [76]. Spinal neurovegetative circuits
regulate the efferent activity to target organs. Spinal neurovegetative
outflow is dependent on the spinal neurovegetative circuits which are the
result of peripheral (visceral and somatic) afference and supra-spinal
descending control [77]. McLachlan and Deuchars demonstrate that
preganglionic neurovegetative neurons have synaptic connections with
peripheral somatic afferents [77]. Sato et al. have seen that the cutaneous
group II afferents did not change the heart rate and blood pressure in
animal experiments [141,142]. The cutaneous group III and IV led to an
increased cardiovascular system [141,142]. Volleys in the group I and II
muscle afferents were not effective. Stimulation of the muscle group III
afferents elicited a not consistent response, in some cases a bradycardiac
(40%) and in other cases a tachycardiac (30%) response. Triggering the
muscle IV afferents always led to an increase in heart rate [141,142]. Sato et
al. reported in another animal study that stimulation of the thoracic and
lumbar spine with forces of 0.5-3.0 kg lateral glide on the segment blood
pressure decreases 29.8(±3.1)mmHg and a decrease of 6.1(±1.6) beats per
minute (BPM) [140]. Also an increased adrenal nerve activity was seen,
which was attributed to baroreceptor effects, since bilateral dissection of
the vagus nerve and carotid sinus nerve (glossopharyngeal nerve)
abolished the reaction [140]. In a study of Camelleri et al. on the gastric
motility is reported that the location of the stimulus is not primary important
and that a non-dermatomal skin stimulation with transcutaneous electrical
nerve stimulation (TENS) can also elicit visceral responses [22]. Because of
the similarity of the gastric responses on different locations of the skin it is
suggested that the induced somatovisceral reaction relays predominantly at
the supra-spinal level [22]. The spinal cord has an integrative function and
controls different spinal neurovegetative reflex pathways. Peripheral
neurovegetative reactions are spinally mediated and receive synaptic input
from supra-spinal structures and primary afferents (somatic and visceral).
Supra-spinal structures can regulate and change the sensitivity of the
spinal reflex mechanisms [63].
2 2
4. Methodology
4.1 Literature search
The following electronic databases were searched for eligible articles.
MEDLINE and Cochrane Library were searched for articles between 2000
and May 2016. The search was conducted from October 2015 to May 2016.
The following search terms and Medical Subject Headings (MeSH) were
used:
Spinal Manipulation Sympathetic nervous system
Chiropractic Manipulation
Osteopathic Manipulative
Treatment
Manual Therapy
Blood Supply
Vasomotor System
Blood Flow Velocity
Sweat Glands
Parasympathetic nervous system
Autonomic nervous system
Enteric nervous system
Viscera
Visceral pain
Piloerection
Skin Temperature
Pain
For search strategy and the exact combinations of MeSH-terms see 10.1: Appendix 1
Citations and reference lists were also examined to identify any relevant
articles not captured in the electronic databases search. The search was
restricted to randomized controlled trials (RCTs) and systematic reviews
that were reported in English language.
4.2 Eligibility criteria
4.2.1 Inclusion criteria
- Articles in the English language
- Publication date 2000 – May 2016
- Randomized Controlled Trials and Systematic Reviews
- Adult (>18 years) and human (male and female)
- A-Symptomatic and Symptomatic subjects
2 3
- Manual spinal technique intervention (manipulation or mobilization)
- Objective measurement of at least one neurovegetative outcome
(autonomic, sympathetic, parasympathetic or enteric nervous system)
4.2.2 Exclusion criteria
- Articles in another language than English
- Studies other than RCTs and systematic reviews
- Studies on medicinal uses, chirurgical studies and molecular studies
- Neurologic diseases or neurologic pathologies
- Studies with no objective measurable neurovegetative outcome
(autonomic, sympathetic, parasympathetic or enteric nervous system)
- Neuro-adrenal/humeral reactions or reactions caused by the
hypothalamic-pituitary-adrenal axis
- Studies with no reproducible treatment, no studies with patients need
based treatment (Black Box)
- Studies which use a spinal correction device (Activator) as intervention
- Studies where the intervention do not consists only of manipulation or
mobilization techniques (spinal techniques combined with non-spinal
techniques)
4.3 Types of manual intervention
Studies that are included in this literature review use manual spinal
manipulation and/or mobilization techniques as an intervention. All general
or specific manual spinal manipulation and mobilization techniques used in
manual therapy, chiropractic and osteopathic medicine are included.
4.4 Types of outcome measures
This review will focus on the neurovegetative outcomes in three systems:
the peripheral system, the visceral system and the specific sympathetic
pain system. This includes outcomes for the peripheral system: skin
conductance, skin temperature, skin/local blood flow, blood supply, blood
flow velocity, piloerection, pupillary diameter.
2 4
For the visceral system: heart rate variability, heart rate, systolic and
diastolic blood pressure, respiratory rate, visceral motility/contractions,
filtration rate.
For the sympathetic nervous system in relation to pain: pressure pain
threshold, thermal pain threshold, pain intensity on Visual Analog Scale
(VAS).
4.5 Data extraction
The data are extracted from the studies and characteristics are summarized
and presented in table 1. The included studies were examined and
classified using the PEDro Quality Assessment Scale to identify
methodological quality (table 2). Citavi5 was used to create a bibliographic
database to manage the search results.
4.6 Quality Rating
To assess the risk of bias all included studies are examined and classified
using the PEDro Quality Assessment Scale (table 2). The PEDro Scale is
based on the Delphi list developed by Verhagen et al. [167]. It is an 11-item
scale designed for rating methodological quality of RCTs (appendix 10.3).
The PEDro Scale contains the 3-point Jadad Scale and the 9-item Delphi
list and is according to Maher et al. reliable for reviewing RCTs [97].
2 5
5. Results
The search strategies were first developed in MEDLINE and subsequently
adapted to the Cochrane Library database. The search in MEDLINE and
Cochrane Library yielded 259 articles (appendix 10.1). The first search with
MeSH-terms in MEDLINE resulted in 101 articles with 35 duplicate articles.
The second search with MeSH-terms in Cochrane Library resulted in 158
articles with 60 duplicates (duplicate articles within search MEDLINE and
Cochrane Library together). After the first selection the combined database
search in MEDLINE (n=19) and Cochrane Library (n=6) yielded 25 results
(for first selection strategy, see appendix 10.2). Searching the reference
lists of keys articles between 2000 and 2016 yielded a further article from
Win et al. [117] that was not captured in the electronic search.
22 Randomized Controlled Trials (RCTs) and 4 systematic reviews were
analysed in full-text. 12 RCTs and 2 systematic reviews were excluded
because they did not meet the eligibility criteria, leaving 12 primary studies
in this literature review. 10 RCTs and 2 systematic reviews. Because the
systematic reviews selected other inclusion criteria the results cannot be
extrapolated. Described studies in the systematic reviews were separate
analysed on the author’s criteria. From the studies that were examined in
the systematic review 3 studies met the inclusion criteria [154,134,20].
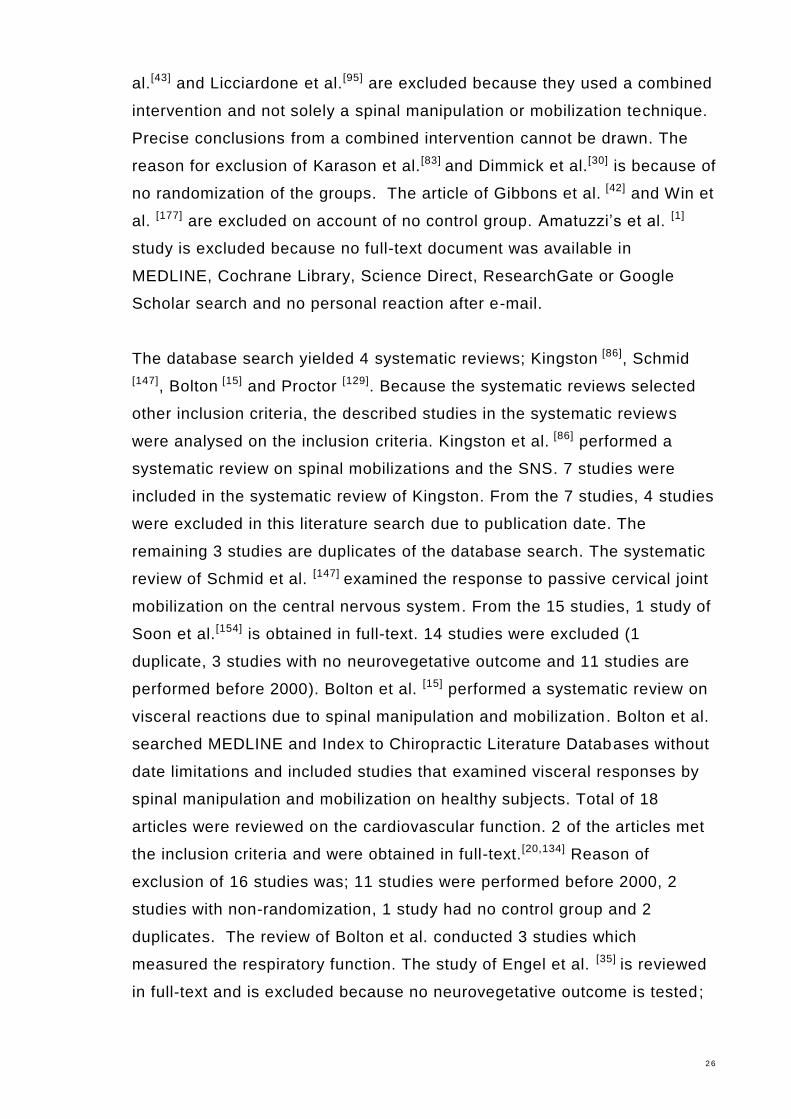
Finally there were 13 RCTs included in the qualitative syntheses. The
process of the study selection is shown in figure 1.
During full-text screening on eligibility criteria the following articles are
excluded; The record from Maclean et al.[103] is screened on eligibility
criteria and is excluded because of a non-spinal mobilization. The reason
for exclusion from Ogura et al.[118], Roy et al. [135] and Zhang et al.[186] was
that they didn’t use a manual technique. They tested the effect of a cervical
manipulation by correction of an Activator or pressure device. The study of
Ruffini et al.[137] is excluded because the osteopathic manipulative
treatment consisted of a patient’s need based treatment, no pre-determined
protocol was applied and thus the treatment is not reproducible. Giles et
2 6
al.[43] and Licciardone et al.[95] are excluded because they used a combined
intervention and not solely a spinal manipulation or mobilization technique.
Precise conclusions from a combined intervention cannot be drawn. The
reason for exclusion of Karason et al.[83] and Dimmick et al.[30] is because of
no randomization of the groups. The article of Gibbons et al. [42] and Win et
al. [177] are excluded on account of no control group. Amatuzzi’s et al. [1]
study is excluded because no full-text document was available in
MEDLINE, Cochrane Library, Science Direct, ResearchGate or Google
Scholar search and no personal reaction after e-mail.
The database search yielded 4 systematic reviews; Kingston [86], Schmid
[147], Bolton [15] and Proctor [129]. Because the systematic reviews selected
other inclusion criteria, the described studies in the systematic reviews
were analysed on the inclusion criteria. Kingston et al. [86] performed a
systematic review on spinal mobilizations and the SNS. 7 studies were
included in the systematic review of Kingston. From the 7 studies, 4 studies
were excluded in this literature search due to publication date. The
remaining 3 studies are duplicates of the database search. The systematic
review of Schmid et al. [147] examined the response to passive cervical joint
mobilization on the central nervous system. From the 15 studies, 1 study of
Soon et al.[154] is obtained in full-text. 14 studies were excluded (1
duplicate, 3 studies with no neurovegetative outcome and 11 studies are
performed before 2000). Bolton et al. [15] performed a systematic review on
visceral reactions due to spinal manipulation and mobilization. Bolton et al.
searched MEDLINE and Index to Chiropractic Literature Databases without
date limitations and included studies that examined visceral responses by
spinal manipulation and mobilization on healthy subjects. Total of 18
articles were reviewed on the cardiovascular function. 2 of the articles met
the inclusion criteria and were obtained in full-text.[20,134] Reason of
exclusion of 16 studies was; 11 studies were performed before 2000, 2
studies with non-randomization, 1 study had no control group and 2
duplicates. The review of Bolton et al. conducted 3 studies which
measured the respiratory function. The study of Engel et al. [35] is reviewed
in full-text and is excluded because no neurovegetative outcome is tested;
2 7
the other 2 studies were excluded because of publication date. On
gastrointestinal function 2 studies were described and both were excluded
because of date and non-control design. The studies selected by Bolton et
al. on somato-autonomic function (n=5) yielded no new studies. There is 1
study excluded on publication date; the remaining 4 are duplicates. The
systematic review of Proctor et al. [129] is excluded because of date
intervention; all 3 studies are performed before 2000.
Figure 1: Study Selection
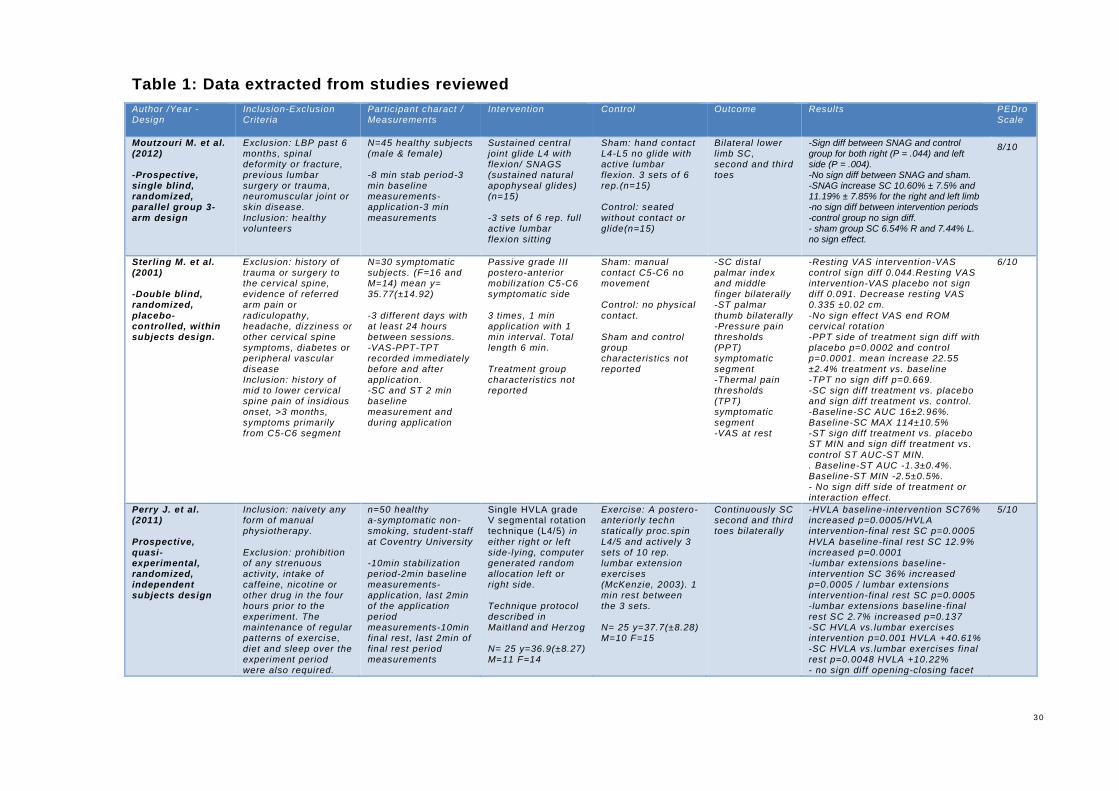
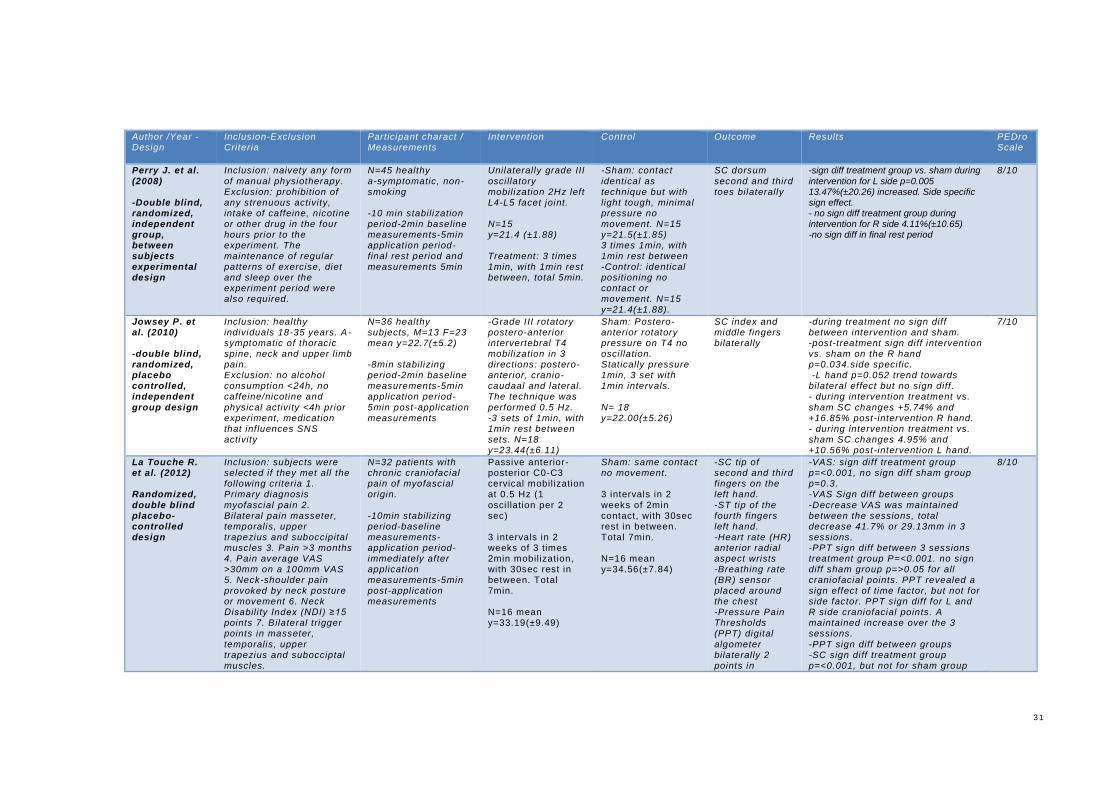
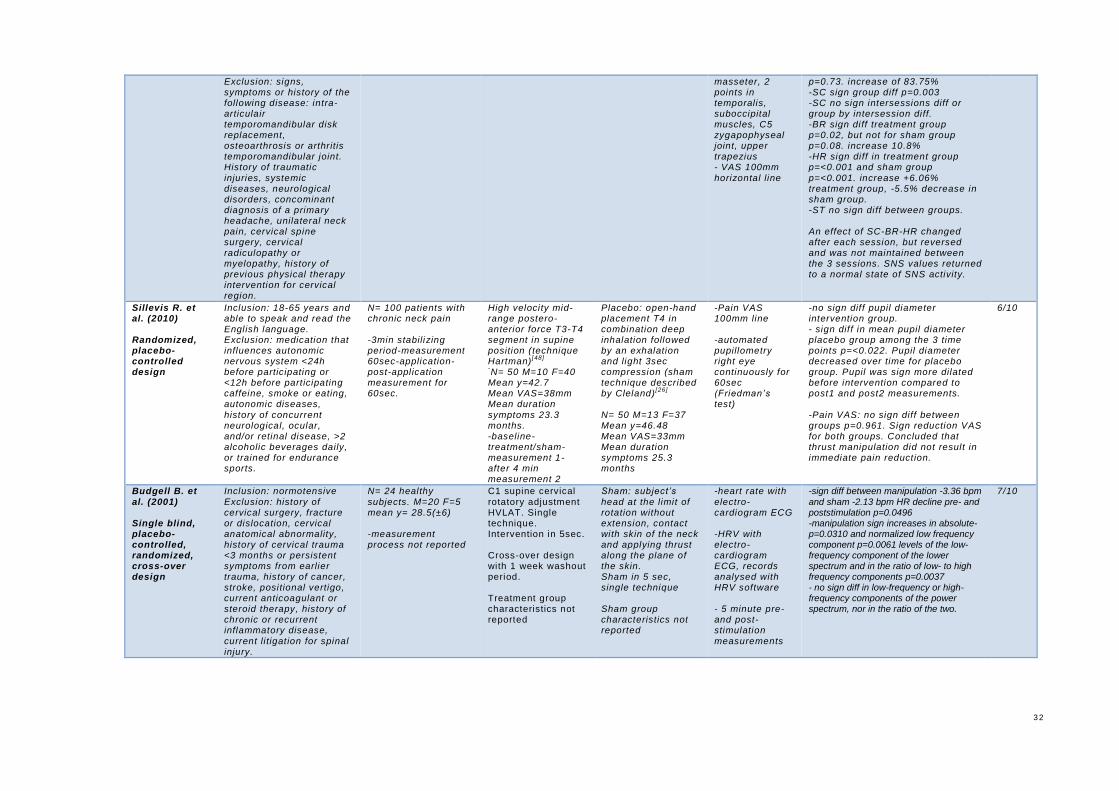
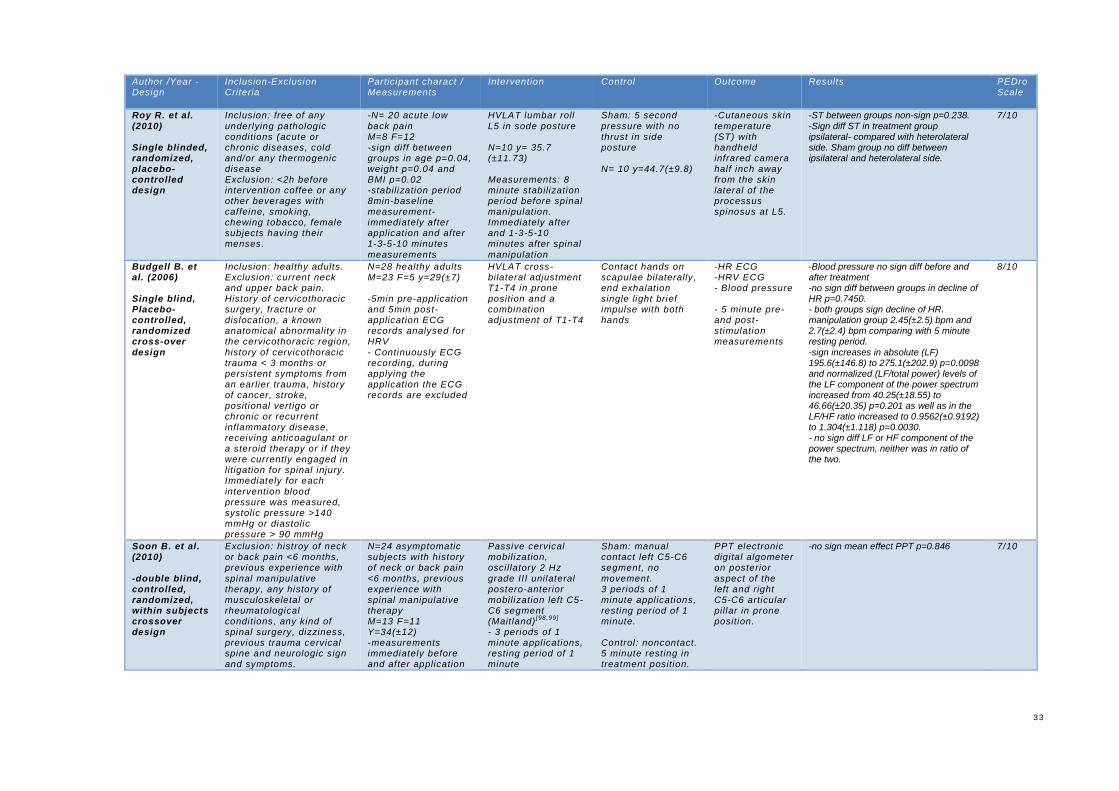
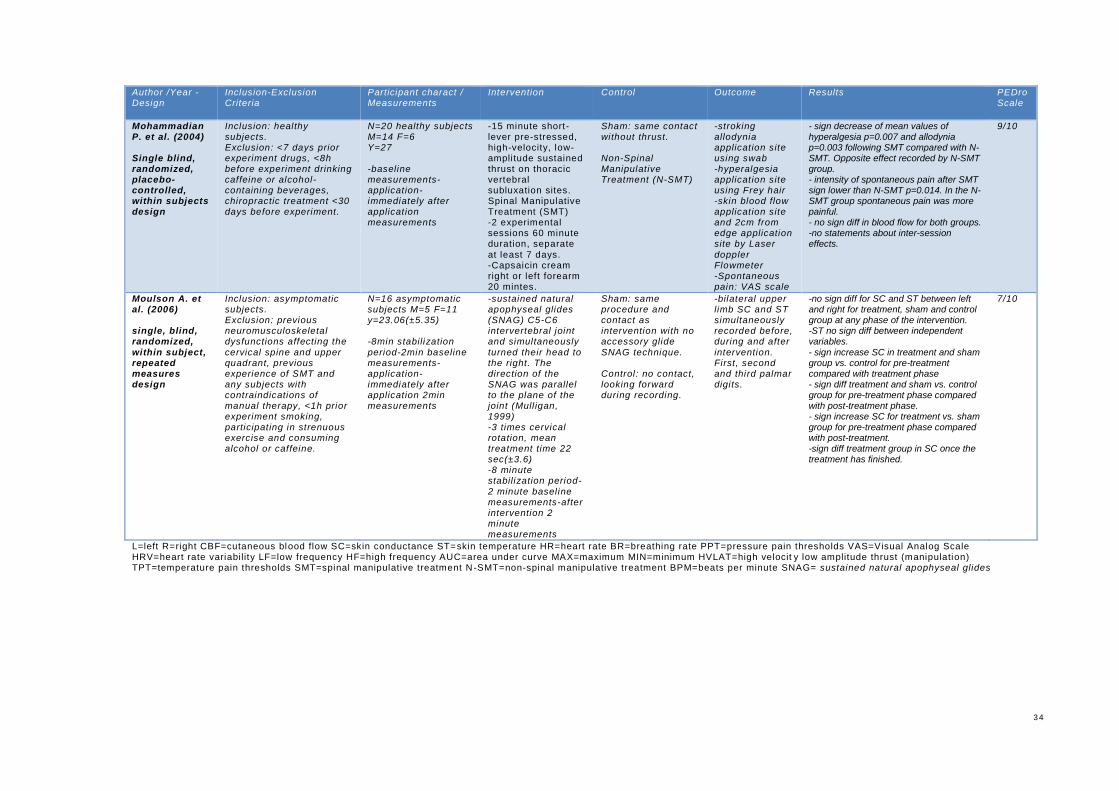
Table 1 summarises the studies, including author and publication year,
inclusion and exclusion criteria, participant characteristics, measurements,
type of intervention, type of sham and/or control group, type of outcome
measures, results and PEDro Quality Assessment Scale.
Search
•Records identified througt database search on keywords and date (n=259)
•Additional records identified through other sources (n=1)
•Total records identified (n=260)
Screening
• Records after duplicates removed (n=166)1
•Records after screened for eligibility criteria on title and abstract (n=26)1
Eligibility
•Full-text RCTs (n=22) and systematic reviews (n=4) assessed
•Full-text RCTs excluded (n=12)
•Full-text systematic reviews excluded (n=4) systematic review RCTs included (n=3)
Included •Randomized Controled Trials included in qualitative synthesis (n=13)
2 8
5.1 Study Characteristics The electronic search yielded 13 RCTs
[113,159,123,122,80,91,150,18,134,20,154,109,111]. From the 13 RCTs 7 studies
[113,123,122,80,91,150,134] performed a parallel group design and 6 studies
[159,18,20,154,109,111] performed a cross-over or within subjects design. All 13
studies examined neurovegetative reactions of spinal manipulation and
mobilization in adults. 4 studies included symptomatic adults [159,91,134,150]
and 9 studies investigated a-symptomatic adults [11,123,122,80,18,20,154,109,111].
Sterling et al. [159] and Sillevis et al. [150] examined subjects with chronic
cervical pain and La Touche et al. [91] included subjects with chronic
craniofacial pain. Roy et al. performed a study on patients with acute low
back pain [134].The total sample sizes from the examined studies ranged
from 16 to 100 subjects per study and for the different groups from 15 to 50
subjects. The search resulted in 7 RCTs which examined the effect of a
spinal mobilization [113,159,122,80,91,154,111] and 6 RCTs of a spinal
manipulation [123,150,134,18,20,109] 4 of the 13 studies included in this review
applied spinal techniques to lumbosacral spine [122,123,134,113], 4 to the upper
thoracic spine [80,150,20,109], 3 to the lower cervical spine [159,154,111] and 2 to
the upper cervical spine [91,18].
5 studies performed as a sham procedure manual contact that is identical
as the treatment technique, but with no movement and as control procedure
no physical contact. [113,159,122,154,111] La Touche et al. [91] uses the same
sham procedure (identical contact on the technique site) but with no control
measurements. In 3 spinal manipulation studies the sham procedure
contains the same starting position as the manipulation technique, but
without thrust [134,150,109]. In 2 of the 4 studies pressure without thrust is
added in the manipulation position [134,150]. Budgell et al. [20] conducted in 1
of his 2 studies single, light brief impulse on the treatment site as a sham
procedure and in the other study a sham manipulation with thrust [18].
Jowsey et al. mimics the treatment position and physical contact and uses
manual pressure as sham procedure [80]. In 2 studies treatment and sham
procedure involve active movements in the same direction [113,111]. Perry et
al. (2011) is the only study which analyses the outcomes between 2
common treatment techniques [123]. A spinal manipulation technique is
2 9
compared to a statically postero-anteriorly technique with active lumbar
extension exercises. 1 study used a multi-session design [91]. La Touche et
al. performed 3 sessions within 2 weeks. Other studies measured a single
application and immediate or short-term results
[113,159,123,122,80,150,18,134,20,154,109,111].
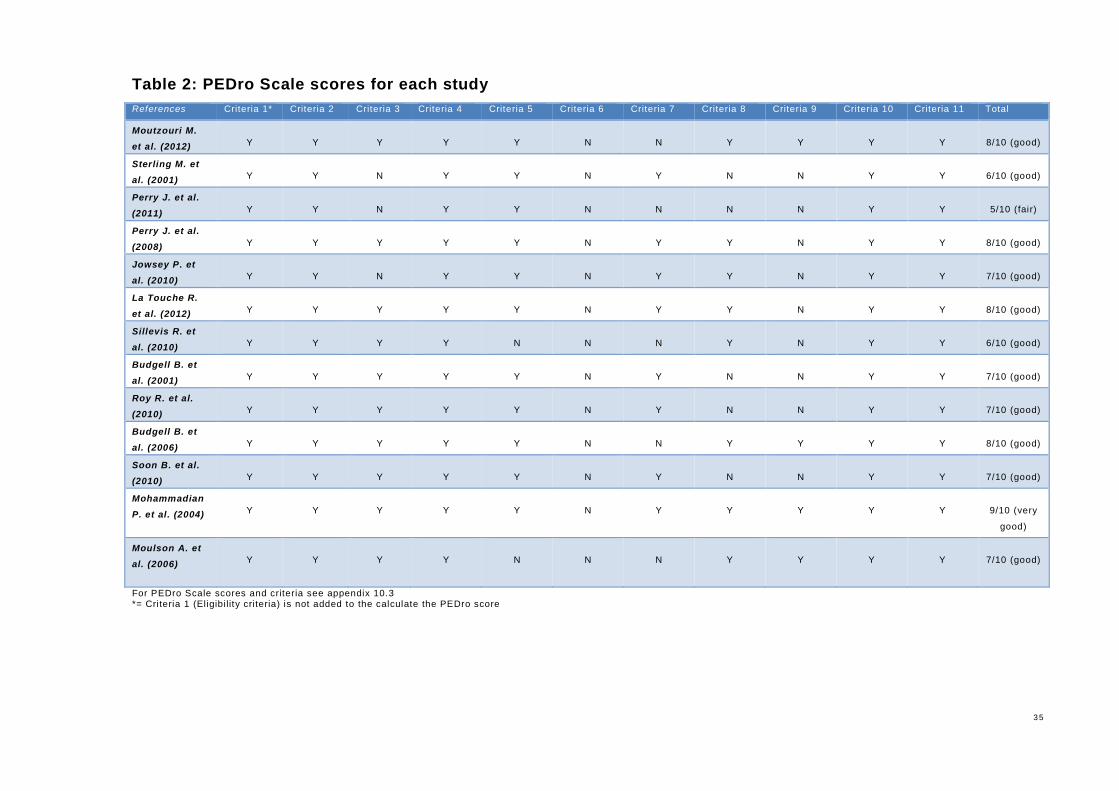
Assessment of the quality of the RCTs is performed with the PEDro Scale.
Table 2 summarizes the PEDro ratings for the different studies. The overall
quality of the 13 RCTs was good. 11 of the 13 RCTs received 6-8 points out
of 10 points and are classified as good [113,159,123,80,91,150,18,134,20,154,111],
Perry et al. (2009) [122] received 5 out of 10 points and is classified as fair
quality and Mohammadian et al. [109] is classified with 9 out of 10 points as
very good quality. The quality of the studies was mostly downgraded due to
the lack of therapist blinding, assessor blinding and because of insufficient
reports about the number of subjects that completed the study or subject
dropouts.
3 0
Table 1: Data extracted from studies reviewed
Author /Year - Design
Inclusion-Exclusion Criteria
Participant charact / Measurements
Intervention Control Outcome Results PEDro Scale
Moutzouri M. et al. (2012) -Prospective, single blind, randomized, parallel group 3-arm design
Exclusion: LBP past 6 months, spinal deformity or fracture, previous lumbar surgery or trauma, neuromuscular joint or skin disease.
Inclusion: healthy volunteers
N=45 healthy subjects (male & female) -8 min stab period-3 min baseline measurements-application-3 min
measurements
Sustained central joint glide L4 with flexion/ SNAGS (sustained natural apophyseal glides) (n=15)
-3 sets of 6 rep. full active lumbar flexion sitt ing
Sham: hand contact L4-L5 no glide with active lumbar flexion. 3 sets of 6 rep.(n=15) Control : seated
without contact or glide(n=15)
Bilateral lower limb SC, second and third toes
-Sign diff between SNAG and control group for both right (P = .044) and left side (P = .004). -No sign diff between SNAG and sham. -SNAG increase SC 10.60% ± 7.5% and 11.19% ± 7.85% for the right and left limb -no sign diff between intervention periods
-control group no sign diff. - sham group SC 6.54% R and 7.44% L. no sign effect.
8/10
Sterling M. et al. (2001) -Double blind, randomized, placebo-controlled, within subjects design.
Exclusion: history of trauma or surgery to the cervical spine, evidence of referred arm pain or
radiculopathy, headache, dizziness or other cervical spine symptoms, diabetes or peripheral vascular disease Inclusion: history of mid to lower cervical spine pain of insidious onset, >3 months, symptoms primarily from C5-C6 segment
N=30 symptomatic subjects. (F=16 and M=14) mean y= 35.77(±14.92)
-3 different days with at least 24 hours between sessions. -VAS-PPT-TPT recorded immediately before and after application. -SC and ST 2 min baseline measurement and during application
Passive grade III postero-anterior mobilization C5-C6 symptomatic side
3 times, 1 min application with 1 min interval. Total length 6 min. Treatment group characteristics not reported
Sham: manual contact C5-C6 no movement Control: no physical
contact. Sham and control group characteristics not reported
-SC distal palmar index and middle finger bilaterally -ST palmar
thumb bilaterally -Pressure pain thresholds (PPT) symptomatic segment -Thermal pain thresholds (TPT) symptomatic segment -VAS at rest
-Resting VAS intervention-VAS control sign diff 0.044.Resting VAS intervention-VAS placebo not sign diff 0.091. Decrease resting VAS 0.335 ±0.02 cm.
-No sign effect VAS end ROM cervical rotation -PPT side of treatment sign diff with placebo p=0.0002 and control p=0.0001. mean increase 22.55 ±2.4% treatment vs. baseline -TPT no sign diff p=0.669. -SC sign diff treatment vs. placebo and sign diff treatment vs. control. -Baseline-SC AUC 16±2.96%. Baseline-SC MAX 114±10.5% -ST sign diff treatment vs. placebo ST MIN and sign diff treatment vs.
control ST AUC-ST MIN. . Baseline-ST AUC -1.3±0.4%. Baseline-ST MIN -2.5±0.5%. - No sign diff side of treatment or interaction effect.
6/10
Perry J. et al. (2011) Prospective, quasi-experimental, randomized, independent subjects design
Inclusion: naivety any form of manual physiotherapy.
Exclusion: prohibition of any strenuous activity, intake of caffeine, nicotine or other drug in the four hours prior to the experiment. The maintenance of regular patterns of exercise, diet and sleep over the experiment period were also required.
n=50 healthy a-symptomatic non-smoking, student-staff
at Coventry University -10min stabilization period-2min baseline measurements-application, last 2min of the application period measurements-10min final rest, last 2min of final rest period measurements
Single HVLA grade V segmental rotation technique (L4/5) in
either right or left side-lying, computer generated random allocation left or right side. Technique protocol described in Maitland
and Herzog
N= 25 y=36.9(±8.27) M=11 F=14
Exercise: A postero-anteriorly techn statically proc.spin
L4/5 and actively 3 sets of 10 rep. lumbar extension exercises (McKenzie, 2003). 1 min rest between the 3 sets. N= 25 y=37.7(±8.28) M=10 F=15
Continuously SC second and third toes bilaterally
-HVLA baseline-intervention SC76% increased p=0.0005/HVLA intervention-final rest SC p=0.0005
HVLA baseline-final rest SC 12.9% increased p=0.0001 -lumbar extensions baseline-intervention SC 36% increased p=0.0005 / lumbar extensions intervention-final rest SC p=0.0005 -lumbar extensions baseline-final rest SC 2.7% increased p=0.137 -SC HVLA vs.lumbar exercises intervention p=0.001 HVLA +40.61% -SC HVLA vs.lumbar exercises final rest p=0.0048 HVLA +10.22% - no sign diff opening-closing facet
5/10
3 1
Author /Year - Design
Inclusion-Exclusion Criteria
Participant charact / Measurements
Intervention Control Outcome Results PEDro Scale
Perry J. et al. (2008) -Double blind, randomized, independent group, between subjects experimental design
Inclusion: naivety any form
of manual physiotherapy. Exclusion: prohibition of any strenuous activity, intake of caffeine, nicotine or other drug in the four hours prior to the experiment. The maintenance of regular patterns of exercise, diet and sleep over the experiment period were also required.
N=45 healthy
a-symptomatic, non-smoking -10 min stabilization period-2min baseline measurements-5min application period-final rest period and measurements 5min
Unilaterally grade III
osci llatory mobilization 2Hz left L4-L5 facet joint. N=15 y=21.4 (±1.88) Treatment: 3 t imes 1min, with 1min rest between, total 5min.
-Sham: contact
identical as technique but with light tough, minimal pressure no movement. N=15 y=21.5(±1.85) 3 times 1min, with 1min rest between -Control: identical positioning no contact or movement. N=15 y=21.4(±1.88).
SC dorsum
second and third toes bilaterally
-sign diff treatment group vs. sham during
intervention for L side p=0.005 13.47%(±20.26) increased. Side specific sign effect. - no sign diff treatment group during intervention for R side 4.11%(±10.65) -no sign diff in final rest period
8/10
Jowsey P. et al. (2010) -double blind, randomized, placebo controlled, independent group design
Inclusion: healthy individuals 18-35 years. A-symptomatic of thoracic spine, neck and upper limb pain. Exclusion: no alcohol consumption <24h, no caffeine/nicotine and
physical activity <4h prior experiment, medication that influences SNS activity
N=36 healthy subjects, M=13 F=23 mean y=22.7(±5.2) -8min stabilizing period-2min baseline measurements-5min application period-
5min post-application measurements
-Grade III rotatory postero-anterior intervertebral T4 mobilization in 3 directions: postero-anterior, cranio-caudaal and lateral. The technique was
performed 0.5 Hz. -3 sets of 1min, with 1min rest between sets. N=18 y=23.44(±6.11)
Sham: Postero-anterior rotatory pressure on T4 no oscillation. Statically pressure 1min, 3 set with 1min intervals. N= 18 y=22.00(±5.26)
SC index and middle fingers bilaterally
-during treatment no sign diff between intervention and sham. -post-treatment sign diff intervention vs. sham on the R hand p=0.034.side specific. -L hand p=0.052 trend towards bilateral effect but no sign diff. - during intervention treatment vs.
sham SC changes +5.74% and +16.85% post-intervention R hand. - during intervention treatment vs. sham SC changes 4.95% and +10.56% post-intervention L hand.
7/10
La Touche R. et al. (2012) Randomized, double blind placebo-controlled design
Inclusion: subjects were selected if they met all the following criteria 1. Primary diagnosis
myofascial pain 2. Bilateral pain masseter, temporalis, upper trapezius and suboccipital muscles 3. Pain >3 months 4. Pain average VAS >30mm on a 100mm VAS 5. Neck-shoulder pain provoked by neck posture or movement 6. Neck Disabili ty Index (NDI) ≥15 points 7. Bilateral trigger points in masseter,
temporalis, upper trapezius and subocciptal muscles.
N=32 patients with chronic craniofacial pain of myofascial origin.
-10min stabilizing period-baseline measurements-application period-immediately after application measurements-5min post-application measurements
Passive anterior-posterior C0-C3 cervical mobilization at 0.5 Hz (1 osci llation per 2 sec) 3 intervals in 2 weeks of 3 times 2min mobilization, with 30sec rest in between. Total 7min. N=16 mean y=33.19(±9.49)
Sham: same contact no movement. 3 intervals in 2 weeks of 2min contact, with 30sec rest in between. Total 7min. N=16 mean y=34.56(±7.84)
-SC tip of second and third fingers on the left hand.
-ST tip of the fourth fingers left hand. -Heart rate (HR) anterior radial aspect wrists -Breathing rate (BR) sensor placed around the chest -Pressure Pain Thresholds (PPT) digital
algometer bilaterally 2 points in
-VAS: sign diff treatment group p=<0.001, no sign diff sham group p=0.3. -VAS Sign diff between groups
-Decrease VAS was maintained between the sessions, total decrease 41.7% or 29.13mm in 3 sessions. -PPT sign diff between 3 sessions treatment group P=<0.001. no sign diff sham group p=>0.05 for all craniofacial points. PPT revealed a sign effect of time factor, but not for side factor. PPT sign diff for L and R side craniofacial points. A maintained increase over the 3 sessions.
-PPT sign diff between groups -SC sign diff treatment group p=<0.001, but not for sham group
8/10
3 2
Exclusion: signs, symptoms or history of the following disease: intra-articulair temporomandibular disk replacement, osteoarthrosis or arthritis temporomandibular joint. History of traumatic
injuries, systemic diseases, neurological disorders, concominant diagnosis of a primary headache, unilateral neck pain, cervical spine surgery, cervical radiculopathy or myelopathy, history of previous physical therapy intervention for cervical region.
masseter, 2 points in temporalis, suboccipital muscles, C5 zygapophyseal joint, upper trapezius - VAS 100mm
horizontal line
p=0.73. increase of 83.75% -SC sign group diff p=0.003 -SC no sign intersessions diff or group by intersession diff. -BR sign diff treatment group p=0.02, but not for sham group p=0.08. increase 10.8% -HR sign diff in treatment group p=<0.001 and sham group
p=<0.001. increase +6.06% treatment group, -5.5% decrease in sham group. -ST no sign diff between groups. An effect of SC-BR-HR changed after each session, but reversed and was not maintained between the 3 sessions. SNS values returned to a normal state of SNS activity.
Sillevis R. et al. (2010) Randomized, placebo-controlled design
Inclusion: 18-65 years and able to speak and read the English language. Exclusion: medication that influences autonomic nervous system <24h before participating or <12h before participating caffeine, smoke or eating, autonomic diseases,
history of concurrent neurological, ocular, and/or retinal disease, >2 alcoholic beverages daily, or trained for endurance sports.
N= 100 patients with chronic neck pain -3min stabilizing period-measurement 60sec-application-post-application measurement for 60sec.
High velocity mid-range postero-anterior force T3-T4 segment in supine position (technique Hartman)
[48]
-N= 50 M=10 F=40
Mean y=42.7 Mean VAS=38mm Mean duration
symptoms 23.3 months. -baseline-treatment/sham-measurement 1- after 4 min measurement 2
Placebo: open-hand placement T4 in combination deep inhalation followed by an exhalation and light 3sec compression (sham technique described by Cleland)
[26]
N= 50 M=13 F=37 Mean y=46.48 Mean VAS=33mm Mean duration symptoms 25.3 months
-Pain VAS 100mm line -automated pupillometry right eye continuously for 60sec (Friedman’s test)
-no sign diff pupil diameter intervention group. - sign diff in mean pupil diameter placebo group among the 3 time points p=<0.022. Pupil diameter decreased over time for placebo group. Pupil was sign more dilated before intervention compared to post1 and post2 measurements.
-Pain VAS: no sign diff between groups p=0.961. Sign reduction VAS for both groups. Concluded that thrust manipulation did not result in immediate pain reduction.
6/10
Budgell B. et al. (2001) Single blind, placebo-controlled, randomized, cross-over design
Inclusion: normotensive
Exclusion: history of cervical surgery, fracture or dislocation, cervical anatomical abnormality, history of cervical trauma <3 months or persistent symptoms from earlier trauma, history of cancer, stroke, positional vertigo, current anticoagulant or steroid therapy, history of chronic or recurrent inflammatory disease,
current li tigation for spinal injury.
N= 24 healthy
subjects. M=20 F=5 mean y= 28.5(±6) -measurement process not reported
C1 supine cervical rotatory adjustment HVLAT. Single technique. Intervention in 5sec. Cross-over design with 1 week washout period. Treatment group characteristics not reported
Sham: subject’s
head at the limit of rotation without extension, contact with skin of the neck and applying thrust along the plane of the skin. Sham in 5 sec, single technique Sham group characteristics not reported
-heart rate with
electro-cardiogram ECG -HRV with electro-cardiogram ECG, records analysed with HRV software - 5 minute pre- and post-stimulation
measurements
-sign diff between manipulation -3.36 bpm
and sham -2.13 bpm HR decline pre- and poststimulation p=0.0496 -manipulation sign increases in absolute- p=0.0310 and normalized low frequency component p=0.0061 levels of the low-frequency component of the lower spectrum and in the ratio of low- to high frequency components p=0.0037 - no sign diff in low-frequency or high-frequency components of the power spectrum, nor in the ratio of the two.
7/10
3 3
Author /Year - Design
Inclusion-Exclusion Criteria
Participant charact / Measurements
Intervention Control Outcome Results PEDro Scale
Roy R. et al. (2010) Single blinded, randomized, placebo-controlled design
Inclusion: free of any
underlying pathologic conditions (acute or chronic diseases, cold and/or any thermogenic disease Exclusion: <2h before intervention coffee or any other beverages with caffeine, smoking, chewing tobacco, female subjects having their menses.
-N= 20 acute low
back pain M=8 F=12 -sign diff between groups in age p=0.04, weight p=0.04 and BMI p=0.02 -stabilization period 8min-baseline measurement- immediately after application and after 1-3-5-10 minutes
measurements
HVLAT lumbar roll
L5 in sode posture N=10 y= 35.7 (±11.73) Measurements: 8 minute stabilization period before spinal manipulation. Immediately after and 1-3-5-10 minutes after spinal
manipulation
Sham: 5 second
pressure with no thrust in side posture N= 10 y=44.7(±9.8)
-Cutaneous skin
temperature (ST) with handheld infrared camera half inch away from the skin lateral of the processus spinosus at L5.
-ST between groups non-sign p=0.238.
-Sign diff ST in treatment group ipsilateral- compared with heterolateral side. Sham group no diff between ipsilateral and heterolateral side.
7/10
Budgell B. et al. (2006) Single blind, Placebo-controlled, randomized cross-over design
Inclusion: healthy adults. Exclusion: current neck and upper back pain. History of cervicothoracic surgery, fracture or dislocation, a known anatomical abnormality in the cervicothoracic region,
history of cervicothoracic trauma < 3 months or persistent symptoms from an earlier trauma, history of cancer, stroke, positional vertigo or chronic or recurrent inflammatory disease, receiving anticoagulant or a steroid therapy or i f they were currently engaged in litigation for spinal injury. Immediately for each
intervention blood pressure was measured, systolic pressure >140 mmHg or diastolic pressure > 90 mmHg
N=28 healthy adults M=23 F=5 y=29(±7) -5min pre-application and 5min post-application ECG records analysed for HRV
- Continuously ECG recording, during applying the application the ECG records are excluded
HVLAT cross-bilateral adjustment T1-T4 in prone position and a combination adjustment of T1-T4
Contact hands on scapulae bilaterally, end exhalation single light brief impulse with both hands
-HR ECG -HRV ECG - Blood pressure - 5 minute pre- and post-stimulation measurements
-Blood pressure no sign diff before and after treatment -no sign diff between groups in decline of HR p=0.7450. - both groups sign decline of HR. manipulation group 2.45(±2.5) bpm and 2.7(±2.4) bpm comparing with 5 minute resting period.
-sign increases in absolute (LF) 195.6(±146.8) to 275.1(±202.9) p=0.0098 and normalized (LF/total power) levels of the LF component of the power spectrum increased from 40.25(±18.55) to 46.66(±20.35) p=0.201 as well as in the LF/HF ratio increased to 0.9562(±0.9192) to 1.304(±1.118) p=0.0030. - no sign diff LF or HF component of the power spectrum, neither was in ratio of the two.
8/10
Soon B. et al. (2010) -double blind, controlled, randomized, within subjects crossover design
Exclusion: histroy of neck or back pain <6 months, previous experience with
spinal manipulative therapy, any history of musculoskeletal or rheumatological conditions, any kind of spinal surgery, dizziness, previous trauma cervical spine and neurologic sign and symptoms.
N=24 asymptomatic subjects with history of neck or back pain
<6 months, previous experience with spinal manipulative therapy M=13 F=11 Y=34(±12) -measurements immediately before and after application
Passive cervical mobilization, osci llatory 2 Hz
grade III unilateral postero-anterior mobilization left C5-C6 segment (Maitland)
[98,99]
- 3 periods of 1 minute applications, resting period of 1 minute
Sham: manual contact left C5-C6 segment, no
movement. 3 periods of 1 minute applications, resting period of 1 minute. Control: noncontact. 5 minute resting in treatment position.
PPT electronic digital algometer on posterior
aspect of the left and right C5-C6 articular pillar in prone position.
-no sign mean effect PPT p=0.846
7/10
3 4
Author /Year - Design
Inclusion-Exclusion Criteria
Participant charact / Measurements
Intervention Control Outcome Results PEDro Scale
Mohammadian P. et al. (2004) Single blind, randomized, placebo-controlled, within subjects design
Inclusion: healthy subjects. Exclusion: <7 days prior experiment drugs, <8h before experiment drinking caffeine or alcohol-containing beverages, chiropractic treatment <30 days before experiment.
N=20 healthy subjects M=14 F=6 Y=27 -baseline measurements-application-immediately after application measurements
-15 minute short-lever pre-stressed, high-velocity, low-amplitude sustained thrust on thoracic vertebral subluxation sites. Spinal Manipulative Treatment (SMT) -2 experimental sessions 60 minute duration, separate
at least 7 days. -Capsaicin cream right or left forearm 20 mintes.
Sham: same contact without thrust. Non-Spinal Manipulative Treatment (N-SMT)
-stroking allodynia application site using swab -hyperalgesia application site using Frey hair -skin blood flow application site and 2cm from edge application site by Laser
doppler Flowmeter -Spontaneous pain: VAS scale
- sign decrease of mean values of hyperalgesia p=0.007 and allodynia p=0.003 following SMT compared with N-SMT. Opposite effect recorded by N-SMT group. - intensity of spontaneous pain after SMT sign lower than N-SMT p=0.014. In the N-SMT group spontaneous pain was more painful. - no sign diff in blood flow for both groups. -no statements about inter-session effects.
9/10
Moulson A. et al. (2006) single, blind, randomized, within subject, repeated measures design
Inclusion: asymptomatic subjects. Exclusion: previous neuromusculoskeletal dysfunctions affecting the
cervical spine and upper quadrant, previous experience of SMT and any subjects with contraindications of manual therapy, <1h prior experiment smoking, participating in strenuous exercise and consuming alcohol or caffeine.
N=16 asymptomatic subjects M=5 F=11 y=23.06(±5.35) -8min stabilization
period-2min baseline measurements-application-immediately after application 2min measurements
-sustained natural apophyseal glides (SNAG) C5-C6 intervertebral joint and simultaneously
turned their head to the right. The direction of the SNAG was parallel to the plane of the joint (Mull igan, 1999) -3 times cervical rotation, mean treatment time 22 sec(±3.6) -8 minute stabilization period-
2 minute baseline measurements-after intervention 2 minute measurements
Sham: same procedure and contact as intervention with no accessory glide
SNAG technique. Control: no contact, looking forward during recording.
-bilateral upper limb SC and ST simultaneously recorded before, during and after
intervention. First, second and third palmar digits.
-no sign diff for SC and ST between left and right for treatment, sham and control group at any phase of the intervention. -ST no sign diff between independent variables.
- sign increase SC in treatment and sham group vs. control for pre-treatment compared with treatment phase - sign diff treatment and sham vs. control group for pre-treatment phase compared with post-treatment phase. - sign increase SC for treatment vs. sham group for pre-treatment phase compared with post-treatment. -sign diff treatment group in SC once the treatment has finished.
7/10
L=left R=right CBF=cutaneous blood flow SC=skin conductance ST=skin temperature HR=heart rate BR=breathing rate PPT=pressure pain thresholds VAS=Visual Analog Scale HRV=heart rate variability LF=low frequency HF=high frequency AUC=area under curve MAX=maximum MIN=minimum HVLAT=high velocit y low amplitude thrust (manipulation) TPT=temperature pain thresholds SMT=spinal manipulative treatment N -SMT=non-spinal manipulative treatment BPM=beats per minute SNAG= sustained natural apophyseal glides
3 5
Table 2: PEDro Scale scores for each study
References Criteria 1* Criteria 2 Criteria 3 Criteria 4 Criteria 5 Criteria 6 Criteria 7 Criteria 8 Criteria 9 Criteria 10 Criteria 11 Total
Moutzouri M.
et al. (2012)
Y
Y
Y
Y
Y
N
N
Y
Y
Y
Y
8/10 (good)
Sterling M. et
al. (2001)
Y
Y
N
Y
Y
N
Y
N
N
Y
Y
6/10 (good)
Perry J. et al.
(2011)
Y
Y
N
Y
Y
N
N
N
N
Y
Y
5/10 (fair)
Perry J. et al.
(2008)
Y
Y
Y
Y
Y
N
Y
Y
N
Y
Y
8/10 (good)
Jowsey P. et
al. (2010)
Y
Y
N
Y
Y
N
Y
Y
N
Y
Y
7/10 (good)
La Touche R.
et al. (2012)
Y
Y
Y
Y
Y
N
Y
Y
N
Y
Y
8/10 (good)
Sillevis R. et
al. (2010)
Y
Y
Y
Y
N
N
N
Y
N
Y
Y
6/10 (good)
Budgell B. et
al. (2001)
Y
Y
Y
Y
Y
N
Y
N
N
Y
Y
7/10 (good)
Roy R. et al.
(2010)
Y
Y
Y
Y
Y
N
Y
N
N
Y
Y
7/10 (good)
Budgell B. et
al. (2006)
Y
Y
Y
Y
Y
N
N
Y
Y
Y
Y
8/10 (good)
Soon B. et al.
(2010)
Y
Y
Y
Y
Y
N
Y
N
N
Y
Y
7/10 (good)
Mohammadian
P. et al. (2004)
Y
Y
Y
Y
Y
N
Y
Y
Y
Y
Y
9/10 (very
good)
Moulson A. et
al. (2006)
Y
Y
Y
Y
N
N
N
Y
Y
Y
Y
7/10 (good)
For PEDro Scale scores and criteria see appendix 10.3 *= Criteria 1 (Eligibility criteria) is not added to the calculate the PEDro score
3 6
5.2 Peripheral reactions of the neurovegetative nervous system
Skin Conductance
7 included studies measure skin conductance (SC) as reaction of the
neurovegetative nervous system on a manipulation or mobilization
[159,123,113,122,80,91,111]. All the studies measures significant differences in SC
between intervention and sham or control group. In the study of Perry et
al.(2008)[122] there was only a significant difference during treatment and
Jowsey et al.[80] found only significant differences post-intervention period.
Moulson et al. found a significant difference intervention versus control group,
but no significant difference between intervention versus sham group [111]. The
other studies found a significant difference between intervention and sham or
control group.
SC increases in all studies and rates vary between 10.6% and 83.75%. Sterling
et al.[159] used a different measurement technique for SC and in the study of
Moulson et al. [111] no SC percentages are reported.
Results of side-specific changes are not consistent. 6 out of 7 studies did side
specific measurements [159,123,113,122,80,111]. Bilateral changes are found in the
majority of the studies. In 2 studies side specific changes are reported [122,80].
Perry et al.(2008)[122] found during a unilateral grade III oscillatory 2 Hz
mobilization at the left L4-L5 facet joint a significant difference during treatment
only at the left side and Jowsey et al. [80] performed a grade III rotatory postero-
anterior intervertebral T4 mobilization and reported post-treatment a significant
effect only at the right side. 6 out of 7 studies examined SC changes during and
after spinal mobilization [159,113,122,80,91,111] and 1 study reported SC changes after
spinal manipulation [123]. 5 studies included a-symptomatic subjects
[123,113,122,80,111] and 2 studies symptomatic subjects. Sterling et al. [159] examined
chronic cervical pain patients and La Touche et al. [91] examined patients with
chronic craniofacial pain of myofascial origin. No consistent differences are
reported in results between a-symptomatic and symptomatic subjects. All studies
except the study of La Touche et al. [91] analysed a single-intervention and short-
term results. La Touche et al. performed 3 intervals of 2 minute upper cervical
mobilizations in 2 weeks. SC reversed after each session and is not maintained
between the 3 sessions. This effect is also seen in the study of Perry et al.(2011)
3 7
[123], SC increases 76% during treatment and 10 minutes post-treatment SC is
descreased to 12.9%. Effect measurements in other studies are till 2-5 minutes
post-intervention. No statements are done about long-term effects.
Skin temperature
4 of the 13 RCTs measured skin temperature (ST) [159,91,134,111] and 1 RCT
measured cutaneous blood flow (CBF) [109]. Reports on ST effects are not
consistent. 3 of the 4 studies report no significant differences in ST between
groups [91,134,111]. Only the study of Sterling et al. [159] found significant differences
after a passive grade III postero-anterior mobilization from C5-C6 between
intervention versus sham group for ST minimum (MIN) and between intervention
versus control group for ST area under curve (AUC) -1.3% and ST MIN -2.5%. 3
of the 4 studies examined reactions by symptomatic subjects. Sterling et al. [159]
included patients with chronic cervical spine pain, La Touche et al. [91] patients
with chronic craniofacial pain of myofascial origin and Roy et al. [134] acute low
back pain patients requiring chiropractic care. ST is measured in 3 of the 4
studies at the palmar surface of the hands [159,91,111]. Sterling et al.[159] and
Moulson et al. [111] measures at the thumb or digits and La Touche et al. [91]
measures at the left fourth digit. The study of Roy et al. measures the ST
paravertebral, lateral of the processus spinosus at L5 [134]. The studies of
Sterling et al.[159], Moulson et al. [111] and Roy et al. [134] measures bilaterally and
La Touche et al. [91] measures unilateral on the left side. Only Roy et al. reported
side specific differences paravertebral L5 after a lumbar HVLAT manipulation
[134]. No significant differences were found between groups. Significant
differences within treatment group were reported between ipsilateral and
heterolateral side, these differences were not side significant between groups.
Immediately after adjustment the ST at the ipsilateral side cooled down -0.46ºF
and 10 minutes after adjustment the ST was 0.49 ºF warmer compared to
baseline measures. The heterolateral side cooled down the entire period and 10
minutes after adjustment the ST was -0.17 ºF cooler than baseline values. All the
studies except La Touche et al. analysed a single-intervention and short-term (2-
5 minutes post-intervention) results [91].
3 8
Cutaneous blood flow
Mohammadian et al. examined cutaneous blood flow (CBF) after experimental
induced inflammatory reaction with capsaicin cream on the forearm [109]. 20
healthy, a-symptomatic subjects were treated with a short lever pre-stressed
HVLAT manipulation of the thoracic spine or with sham treatment. Outcomes
were measured with Laser Doppler Flowmeter on the site of the forearm. No
significant changes in CBF in the groups after 15 minutes adjustments, high
velocity low amplitude sustained thrust manipulation at the thoracic spine were
found.
Pupillary reactions
1 included study examined pupillary reactions after a high velocity mid-range
postero-anterior T3-T4 manipulation [150]. Right eye is continuously measured
with fully automated pupillometry. There was a significant difference in the mean
pupil diameter within the sham group, no significant difference in the treatment
group. The pupil diameter constricted over time for the sham group. The pupil
was significantly more dilated before sham compared to both post-intervention
measures. Immediate post-intervention measurement reported 4.28mm pupillary
constriction and 4 minutes later post-intervention 2 measurement reported
3.89mm pupillary constriction, compared with 1.68mm pupillary dilatation and
1.23mm pupillary dilatation for the treatment group. Between the 2 post-
intervention measures there was no significant difference. No statements are
reported about significance between groups. No conclusions can be done
regarding long-term effects.
5.3 Reactions of sympathetic nervous system in relation to pain perception
Sympathetic pain related outcomes that are measured in the included studies
are; pressure pain thresholds (PPT), thermal pain thresholds (TPT), allodynia,
hyperalgesia and pain intensity on the Visual Analog Scale (VAS). Pain threshold
is defined as “the least stimulus intensity at which a subject perceives pain” as
stated by the International Association for The Study of Pain [57]. 3 studies
measured PPT after a spinal technique [159,91,154]. Changes of the PPT in the 3
studies are not consistent. Sterling et al.[159] did a passive grade III postero-
anterior mobilization of C5-C6 at the symptomatic side by chronic cervical pain
3 9
patients and found significant ipsilateral differences between mobilization and
sham or control group. The PPT at the symptomatic cervical segment increased
22.55%. La Touche et al. performed 3 passive antero-posterior C0-C3 cervical
mobilization at 0.5Hz over 2 weeks by chronic craniofacial pain patients and
reported a significant bilateral effect on all craniofacial PPT and all cerv ical PPT
[91]. Namely a PPT increase of 64-77% for masseter, 38-59% for temporalis and
47-79% for all cervical points. Post hoc testing revealed significant differences
between the 3 sessions for the treatment group, which is indicative of a
maintained increase over the sessions. Soon et al. examined a-symptomatic
subjects with a passive grade III unilateral postero-anterior C5-C6 mobilization at
the left zygapophyseal joint at 2 Hz [154]. PPT at the posterior aspect of the left
and right C5-C6 articular pillar did not change significantly.
TPT is only measured in the study of Sterling et al. at the symptomatic cervical
segment [159]. After a passive grade III postero-anterior mobilization of C5-C6
there were no significant differences in TPT.
A not consistent change in VAS-scores is seen in 4 studies [159,91,150,109]. Sterling
et al. found a significant difference between VAS intervention and VAS control
group and no significant difference between VAS intervention and VAS sham
group [159]. In the study VAS-scores decreased 3.35mm [159]. The study of La
Touche et al. described a significant decrease in VAS between groups [91]. Post
hoc analysis revealed significant differences in the treatment group and no
significant differences in the sham group. The decrease of VAS in the treatment
group was maintained between the 3 sessions over the 2 weeks, with a total
decrease of 41.71% or 29.11mm on the VAS-scale. Sillevis et al. reported no
significant differences between intervention and sham group for VAS-scores [150].
Mohammadian et al. found that spontaneous pain (experimental induced
inflammatory reaction and pain with capsaicin cream) measured with the VAS-
scale, decreases significant after 15 minutes of multiple short lever pre-stressed
HVLAT of thoracic vertebral subluxation sites compared with sham group [109].
Spontaneous VAS rate in the sham group increases after sham treatment. In the
same study researchers also found significant decreases of hyperalgesia and
allodynia on the capsaicin site following HVLAT compared with the sham group.
In the sham group the intensity of the hyperalgesia and allodynia increases
following sham application.
4 0
La Touche et al. performed multiple sessions, 3 sessions in 2 weeks [91].
Significant changes in PPT and VAS-scores are maintained during the 2 weeks
experimental period. Other studies performed short-term measurements and no
statements are reported about long-term or maintained pain-reducing or
hypoalgesic effect.
5.4 Visceral reactions of the neurovegetative nervous system
3 studies examine visceral reactions after a spinal mobilization or manipulation
[91,18,20]. 2 studies [18,20] are included that measures heart rate (HR) and heart
rate variability (HRV) and 1 study [91] that examined HR and breathing rate (BR)
after a spinal technique. 1 study reports next to HR and HRV also effects on
blood pressure (BP) [20]. Bugell et al. performed 2 studies which analysed HR
and HRV with electrocardiogram (ECG) [18,20]. Both studies included a-
symptomatic subjects and tested cardiovascular reactions after a spinal
manipulation. In the first study in 2001 Budgell et al. performed a C1 cervical
rotatory HVLAT adjustment and reported a significant difference between HVLAT
and sham treatment on HR and some HRV frequencies [18]. HR declined -3.36
BPM after HVLAT and -2.13 BPM after sham treatment pre- and post-stimulation.
HRV changes after HVLAT of C1 significant with increase of the absolute (+67.9)
and normalized low frequency (+6.7) component levels of low frequency
component of the lower spectrum and in the ratio of low and high frequency
components (+0.43). In the second study in 2006 Budgell et al. found no
significant changes in HR and blood pressure after a cross-bilateral HVLAT
adjustment of T1-T4 compared to a sham treatment [20]. In both groups the HR
declined significantly. HRV changed significant at some levels following a HVLAT
at T1-T4. Significant increase of HRV levels are reported for absolute (195.6 to
275.1) and normalized levels (40.25 to 46.7) of the low frequency component of
the power spectrum and low frequency versus high frequency ratio increased
from 0.9562 to 1.304. No significant differences are described for the low
frequency of high frequency component of the power spectrum, neither for the
ratio of the two. This indicates as an increase in sympathetic output to the heart
and a shift in the balance of sympathetic and parasympathetic cardiac output in
favor of the sympathetic component. La Touche et al. measured the breathing
rate and heart rate after 3 sessions of passive anterior -posterior mobilization at

4 1
0.5Hz of C0-C3 [91]. Breathing rate increased significant with 10.8% in the
intervention group compared to the sham group. Also the HR changed significant
following mobilization compared with the sham group. HR increase 6.06% and in
the sham group HR declined -5.05%. No significant maintained or intersession
differences for both variables are seen.
5.5 Types of manipulation and mobilization techniques and outcomes
The different types of spinal techniques, intervention process and specific results
are listed in table 3. The study included 6 different types of mobilization
techniques [113,159,122,80,91,154,111] and 6 different types of manipulation techniques
[123,150,18,134,20,109]. Perry et al.(2011) [123] and Soon et al. [154] analysed the same
mobilization technique, namely a unilateral grade III oscillatory mobilization at 2
Hz. Side specific changes are seen in 3 studies [122,80,134] , other studies found
bilateral effects [113,159,91,154,111,123,150,18,20,109]. Perry et al.(2011) [123] used a
unilateral grade III oscillatory 2Hz technique, Jowsey et al. [80] a rotatory postero-
anterior 0.5Hz technique and Roy et al. a HVLAT lumbar roll. No side specific
effects are reported by similar rotatory, HVLAT and oscillatory techniques. No
superior effects are seen by oscillatory techniques, results of 2Hz or 0.5Hz
oscillatory techniques are similar as non-oscillatory techniques.
SC increased following a manipulation with 76% [122], due to mobilization SC
increases in range of 10.56% to 16.85% and an outlying value of 83.75% in the
study of La Touche et al [113,159,80,91,111,123]. Sterling et al. [159] reported a VAS
score reduction of 3.35mm after 3 times, 1 minute passive grade III postero -
anterior mobilization C5-C6 and La Touche et al. [91] described a VAS score
reduction of 29.13mm after 3 sessions of 3 times, 2 minutes passive anterior-
posterior C0-C3 mobilization 0.5Hz. Sterling et al. [159] reported after 1 session
an increase of 22.5% for PPT and La Touche et al. [91] described after 3 sessions
a maintained intersession main increase for the craniofacial and cervical PPT of
60%. Contradictory HR reactions are measured between 2 studies following an
upper cervical technique [91,18]. After a passive posterior-anterior C0-C3
mobilization of 0.5Hz HR increased with 6.06% BPM and following a C1 rotatory
HVLAT HR declined with -3.36 BPM [91]. Budgell et al. reported after 2 different
types of manipulation techniques at the thoracic and cervical spine similar
changes in HRV. A T1-T4 cross-bilateral HVLAT manipulation and a C1 rotatory
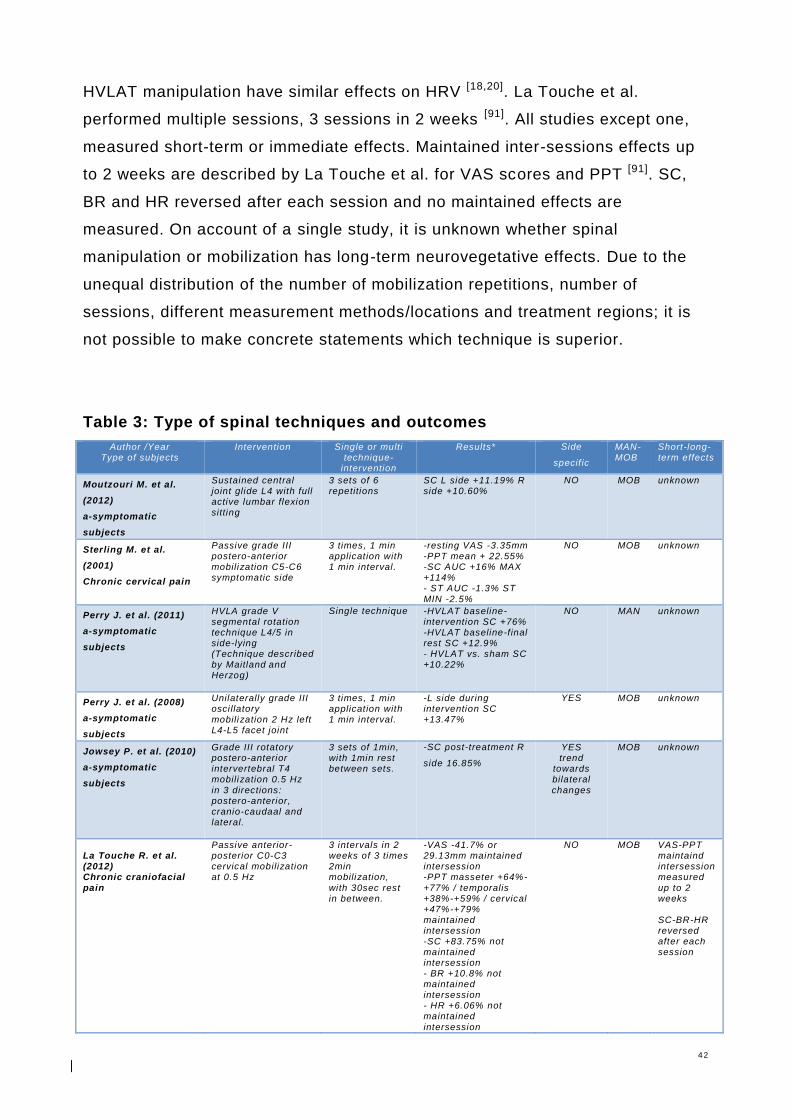
4 2
HVLAT manipulation have similar effects on HRV [18,20]. La Touche et al.
performed multiple sessions, 3 sessions in 2 weeks [91]. All studies except one,
measured short-term or immediate effects. Maintained inter-sessions effects up
to 2 weeks are described by La Touche et al. for VAS scores and PPT [91]. SC,
BR and HR reversed after each session and no maintained effects are
measured. On account of a single study, it is unknown whether spinal
manipulation or mobilization has long-term neurovegetative effects. Due to the
unequal distribution of the number of mobilization repetitions, number of
sessions, different measurement methods/locations and treatment regions; it is
not possible to make concrete statements which technique is superior.
Table 3: Type of spinal techniques and outcomes
Author /Year Type of subjects
Intervention Single or multi technique-
intervention
Results*
Side
specif ic
MAN-MOB
Short-long-term effects
Moutzouri M. et al.
(2012)
a-symptomatic
subjects
Sustained central joint glide L4 with full active lumbar flexion sitting
3 sets of 6 repetitions
SC L side +11.19% R side +10.60%
NO MOB unknown
Sterling M. et al.
(2001)
Chronic cervical pain
Passive grade III postero-anterior mobilization C5-C6 symptomatic side
3 times, 1 min application with 1 min interval.
-resting VAS -3.35mm -PPT mean + 22.55% -SC AUC +16% MAX +114% - ST AUC -1.3% ST
MIN -2.5%
NO MOB unknown
Perry J. et al. (2011)
a-symptomatic
subjects
HVLA grade V segmental rotation technique L4/5 in side-lying (Technique described by Maitland
and
Herzog)
Single technique -HVLAT baseline-intervention SC +76% -HVLAT baseline-final rest SC +12.9% - HVLAT vs. sham SC +10.22%
NO MAN unknown
Perry J. et al. (2008)
a-symptomatic
subjects
Unilaterally grade III osci llatory mobilization 2 Hz left L4-L5 facet joint
3 times, 1 min application with 1 min interval.
-L side during intervention SC +13.47%
YES MOB unknown
Jowsey P. et al. (2010)
a-symptomatic
subjects
Grade III rotatory postero-anterior intervertebral T4 mobilization 0.5 Hz
in 3 directions: postero-anterior, cranio-caudaal and lateral.
3 sets of 1min, with 1min rest between sets.
-SC post-treatment R
side 16.85%
YES trend
towards bilateral
changes
MOB unknown
La Touche R. et al. (2012) Chronic craniofacial pain
Passive anterior-posterior C0-C3 cervical mobilization at 0.5 Hz
3 intervals in 2 weeks of 3 times 2min mobilization,
with 30sec rest in between.
-VAS -41.7% or 29.13mm maintained intersession -PPT masseter +64%-
+77% / temporalis +38%-+59% / cervical +47%-+79% maintained intersession -SC +83.75% not maintained intersession - BR +10.8% not maintained intersession - HR +6.06% not maintained
intersession
NO MOB VAS-PPT maintaind intersession measured
up to 2 weeks SC-BR-HR reversed after each session
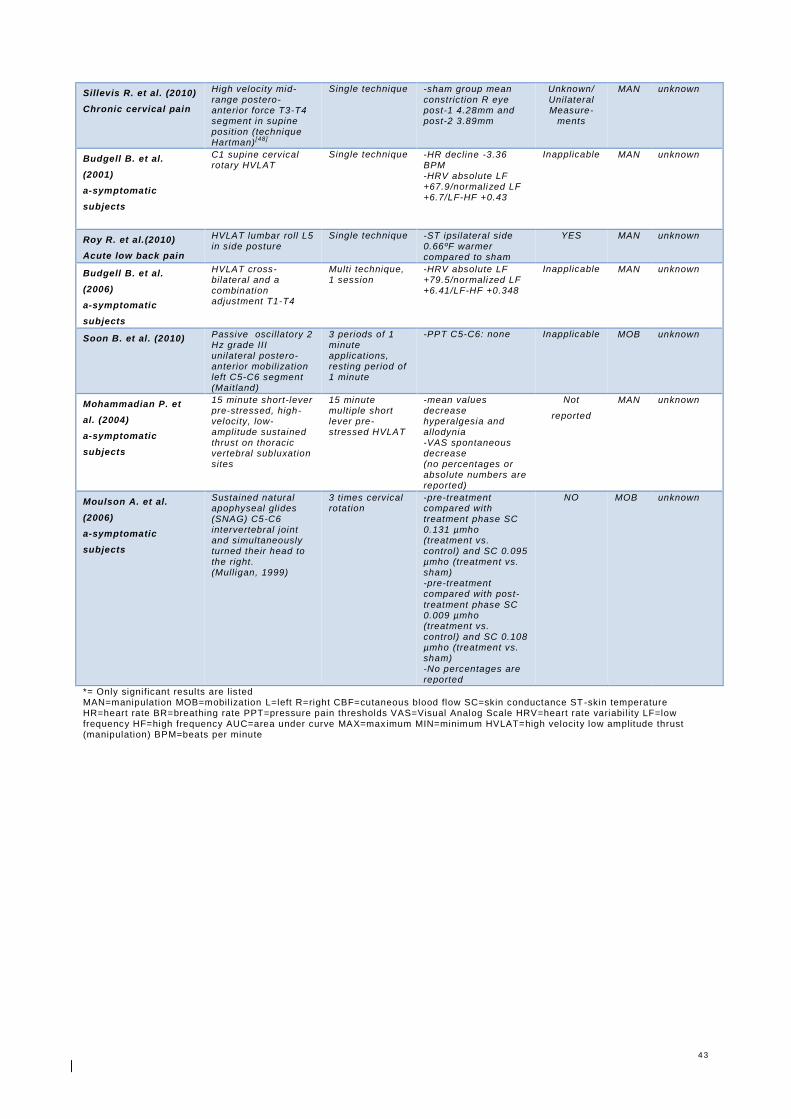
4 3
Sillevis R. et al. (2010)
Chronic cervical pain
High velocity mid-range postero-anterior force T3-T4 segment in supine position (technique Hartman)
[48]
Single technique -sham group mean constriction R eye post-1 4.28mm and post-2 3.89mm
Unknown/ Unilateral Measure-
ments
MAN unknown
Budgell B. et al.
(2001)
a-symptomatic
subjects
C1 supine cervical rotary HVLAT
Single technique -HR decline -3.36 BPM -HRV absolute LF +67.9/normalized LF +6.7/LF-HF +0.43
Inapplicable MAN unknown
Roy R. et al.(2010)
Acute low back pain
HVLAT lumbar roll L5 in side posture
Single technique -ST ipsilateral side 0.66ºF warmer compared to sham
YES MAN unknown
Budgell B. et al.
(2006)
a-symptomatic
subjects
HVLAT cross-bilateral and a combination adjustment T1-T4
Multi technique, 1 session
-HRV absolute LF +79.5/normalized LF +6.41/LF-HF +0.348
Inapplicable MAN unknown
Soon B. et al. (2010) Passive oscillatory 2 Hz grade III unilateral postero-anterior mobilization left C5-C6 segment (Maitland)
3 periods of 1 minute applications, resting period of 1 minute
-PPT C5-C6: none
Inapplicable MOB unknown
Mohammadian P. et
al. (2004)
a-symptomatic
subjects
15 minute short-lever pre-stressed, high-velocity, low-amplitude sustained thrust on thoracic vertebral subluxation sites
15 minute multiple short lever pre-stressed HVLAT
-mean values decrease hyperalgesia and allodynia -VAS spontaneous decrease (no percentages or absolute numbers are reported)
Not
reported
MAN unknown
Moulson A. et al.
(2006)
a-symptomatic
subjects
Sustained natural apophyseal glides (SNAG) C5-C6 intervertebral joint and simultaneously turned their head to the right. (Mulligan, 1999)
3 times cervical rotation
-pre-treatment compared with treatment phase SC 0.131 µmho (treatment vs. control) and SC 0.095 µmho (treatment vs. sham) -pre-treatment compared with post-
treatment phase SC 0.009 µmho (treatment vs. control) and SC 0.108 µmho (treatment vs. sham) -No percentages are reported
NO MOB unknown
*= Only significant results are listed MAN=manipulation MOB=mobil ization L=left R=right CBF=cutaneous blood flow SC=skin conductance ST -skin temperature HR=heart rate BR=breathing rate PPT=pressure pain thresholds VAS=Visual Analog Scale HRV=heart rate variabil ity LF=low frequency HF=high frequency AUC=area under curve MAX=max imum MIN=minimum HVLAT=high velocity low amplitude thrust (manipulation) BPM=beats per minute
4 4
5.6 Synthesis of results
The overall quality of the included studies is fair till good; the majority received
6-8/10 points on the PEDro scale and is categorized as good quality. SC
[113,159,123,122,80,91,111] and BR [91] increased significantly following spinal
manipulation or mobilization. 2 of the 3 studies confirmed a significant increase
in PPT [159,91]. Not consistent results are found for ST. Studies found no
significant effects in ST between intervention and sham group [91,134,111]. One
study reported significant ST effects between intervention and control group [159].
Except one study [150] VAS scores decreased significantly when intervention is
compared to control group [159,91,109] and 2 of the 4 studies found a significant
decrease of VAS scores between intervention versus sham group [91,109]. No
significant effects are reported on TPT [159], cutaneous blood flow [109] and
pupillary reactions [150]. For HR are inconsistent and contradictory effects
reported [18,20,91]. Almost all significant effects were excitatory for SNS in nature.
An increase of SC, PPT, BR, HR, changes in HRV and a decrease of ST and
VAS scores. Only Budgell et al.(2006) reported following a C1 HVLAT a
decrease in HR [20]. For VAS scores and PPT are maintained (up to 2 weeks)
results described [91]. Reversed, not maintained inter-session changes in SC, BR
and HR are reported [91]. Except one study [91] short-term or immediate effects
are measured. There is no solid evidence that neurovegetative effects persist
following spinal manipulation or mobilization. No concrete differences in the
magnitude of effects are found between symptomatic versus a-symptomatic
subjects. Reports on side specific reactions are inconsistent. Due to the unequal
distribution of the number of mobilization repetitions, number of sessions,
different measurement methods and treatment locations, it is not possible to
make concrete statements which technique is superior.
4 5
6. Discussion
To answer the primary research question; Which significant changes in
neurovegetative physiological parameters occur after manual spinal manipulation
and mobilization of symptomatic and a-symptomatic adults in manual therapy,
chiropractic or osteopathic medicine? the literature review included 13 fair to
high quality RCTs [113,159,123,122,80,91,150,18,134,20,154,109,111]. 11 of the 13 included
studies established a significant change in neurovegetative outcome following a
spinal manipulation or mobilization compared to control or sham treatment
[113,159,123,122,80,91,18,134,20,109,111]. SNS responses are demonstrated by measures
of different physiological parameters, but mostly SC, ST and pain associated
SNS reactions (VAS scores and PPT). The included studies measured
neurovegetative modulated physiological parameters. Outcome measures are
SC, ST, PPT, TPT, VAS scores, CBF, BR, HR, HRV and pupillary reactions. All
except one study [20] report effects due to sympathetic excitation
[113,159,123,122,80,91,150,18,134,154,109,111].
Inconsistent side specific changes are reported by SC. Perry et al. [122] describe
a significant side specific, unilateral effect during intervention and Jowsey et al.
[80] describe a significant side specific, unilateral effect post-intervention.
According to the authors the side specific effects are due to the oscillatory
nature of the technique. This is in contradiction with the findings of La Touche et
al. [91] and Soon et al. [154] who found no side specific effects by oscillatory
techniques. A study in 2011 Perry et al. reported that further group analysis
revealed that side specific changes are not dependent on closing or opening of
the joint [123]. There were no significant differences p=0.76 between the opening
and closing facet joint and sympathetic effects. Analysis has shown that side
specific changes are not dependent on the unilateral nature of the technique,
because similar unilateral techniques are used in other studies with no side
specific results. Findings of Lovick [96], Wright [178], Zusman [187] and Bialosky [10]
support a more general bilateral central response to a local spinal applied
technique. Findings suggest that sympathetic excitation is mediated via the
dPAG in the midbrain, through neural descending pathways. Manipulation and
mobilization of the spine stimulates capsule, muscle, tendon and connective
4 6
tissue receptors which are capable of directly or indirectly activate dPAG
mechanisms [159,37,126,147]. Some authors believe that side specific effects are
possible by specific mediation within the dPAG reactions [159,151]. They report that
dPAG has a somatotopic distribution and can centrally generate side specific
responses. Mouton et al. examined dPAG in cats and saw that dPAG regions are
modulated in medullary control nuclei with either unilateral or bilateral
anatomical projections [112]. Other researchers report local biomechanical
explanatory models for side specific changes [159,88,37]. Activation of local
sympathetic fibers is possible due to the unilateral vertebral movement caused
by spinal manipulation and mobilization. This local biomechanical theory is
inconsistent with bilateral findings in studies which uses similar unilateral spinal
manipulation and mobilization techniques and reports bilateral findings. The
unilateral nature of a spinal technique is questionable. Anterior-posterior,
posterior-anterior and rotatory techniques stress the ipsilateral facet joint and
indirectly also the heterolateral facet joint. Side specific effects are not
consistent and cannot be explained by type of technique or oscillatory nature.
About the exact neurophysiological processes and pathway is debated.
SC has been proposed as a valid method to investigate SNS responses for
outcome greater than 4.6% change from baseline [123]. Besides Moulson et al.
[111] (no percentages reported), all studies measure a greater effect than 4.6%
compared to baseline. All the studies measure SC at the hands (palmar index
and middle finger) and the feet (second and third toes). Because sudomotor
neurons distribution is skin type and localisation dependent, it is not possible the
compare hand SC outcomes with feet SC outcomes [74]. In the under extremity
the mobilization techniques increased SC 10.6-13.47% [113,122]. The manipulation
technique increased SC 76% [123]. This seems to be in favour of the manipulation
technique. In the upper extremity SC varies between a 10.56% and 83.75%
increase [80,91]. This consistent with previous studies performed on SC [23,124,153].
Sterling et al. used a different measurement technique for SC; this makes it
impossible to compare the values [159]. Previous studies used data analysis using
AUC-MAX and MIN SC values to illustrate results [23,171,172]. However this
process has been statistically questioned [173]. In the study of Moulson et al. no
SC percentages are reported, so according to Perry et al. (2011) no conclusions
4 7
can be drawn about the validity of the measurement [111]. All spinal techniques of
the upper extremity are mobilizations, so no comparison can be made between
manipulation and mobilization techniques. The high percentages after
mobilization (83.75%) in the study of La Touche et al. are a outlier and probably
explained by a longer treatment session [91]. 3 times, 2 minutes mobilization
compared to 3 times, 1 minute mobilization in most studies. Several studies
examined the relationship between duration, dose of SMT and the SNS activity
[23,155]. Results of studies demonstrated that frequency and duration of treatment
time has a significant effect on the response of SC and ST [23,155]. Some
researchers cautioned the uses of SC measurements on the palm of the hands
[144,34,53]. They say that the SC on the palm of the hands is solely controlled by
psychological and emotional centres and may measure only a psycho-emotional
reaction. The SC on the palm of the hands is regulated by numerous control
centres in the central nervous system [144,34,53]. This psycho-emotional reaction
causes an outcome inaccuracy and may be the reason why some sham
treatments have significant effects on SC. Significant changes in sham group in
the study of Perry et al.(2008) following McKenzie exercises can be explained by
active nature of the exercises [122]. The exercises cause a vertical movement of
the heart and as reaction altered SNS activity, cardio-vascular and orthostatic
changes [153].
The majority of the included studies describe no significant difference for ST
[91,134,111]. This is consistent with previous studies of Chiu and Wright [23] and
Peterson et al. [124]. They have identified that ST is often smaller and more
inconsistent compared to SC. Thermometric measures of ST is a reliable and
valid manner for measuring the vascularization in the cutaneous skin [114,120].
Owens et al. reported that, for an accurate and reproducible measurement, an 8-
16 minute stabilization period and a stable room temperature 22ºC (±1.0ºC) is
needed [120]. A guideline from Chui and Wright describe that the room
temperature and humidity needed to be constant for all experiments varied by a
maximum of 2% [23]. All 4 studies controlled temperature [91,134,111,159], only 2 of
the 4 studies controlled humidity [159,111]. In 2 studies temperature is reported,
21.95ºC and 25ºC [91,134]. The room temperature in the study of La Touche et al.
(25ºC) does not match the guideline which requires 22ºC [91]. Jänig et al.

4 8
describe that activity of skin vasoconstrictor neurons are dependent on
temperature [68]. Because of the room temperature differs in the studies, it is
possible that the sudomotor neurons react physiological differently. Evidence
indicates that ST reactions are dependent on body mass index and age. Dufour
et al. demonstrated that older subjects and middle-aged subjects have a higher
ST than younger subjects [33]. This is in contrast to a study of Wilson et al. who
describe an inability to prevent heat loss via the skin by cutaneous
vasoconstrictor dysfunction by older subjects [176]. In the study of Roy et al.
participant characteristics significant differ between groups in age, weight and
BMI [134]. This makes it hard to draw statistically correct conclusions. La Touche
et al. described group characteristics in age and gender, no group data abou t
weight or BMI is reported [91]. The other 2 studies performed a within subjects
design [159,111]. Roy et al. used measurements in the local ST direct after a spinal
technique can be through heat transfer of the hand of the researcher [134]. It is
also possible that direct ST reactions after a spinal technique are a result of a
reactive hyperemia that is caused by compression of local tissues. 2 of the 4
studies uses mobilization movements of the head compared to a no movement
sham application [159,91]. Skin vasoconstrictor neurons are centrally mediated and
are responsive for baroreceptor reflexes, cardiovascular reflexes, respiratory
reflexes and changes of body position [66]. Evidence demonstrated that vestibular
stimulation (movement of head) can elicit cardiovascular reflexes [179,180,181,182].
These cardiovascular reflexes can influence skin vasoconstrictor neurons by
head movements. Yates et al. described an inhibitory vestibule-sympathetic
reflex mediated by neurons in the ventrolateral medulla [179,180,181,182]. The
neurons in the ventrolateral medulla respond to vestibular stimuli, but also on
carotid sinus stimulation. Suggesting a role in cardiovascular regulation. Low-
amplitude accelerations of the head can produce responses in heart rate, with
the latency of the response prolonged in subjects with vestibular dysfunction
[130]. Additionally, there is evidence from animals studies with cats that cervical
mechanoreceptors stimuli interacts in an antagonistic manner with input from the
vestibulum to modify the activity of the SNS [16]. Because skin vasoconstrictor
neurons differ according type, localization of skin and the section of the vascular
bed they innervate, studies results on different body locations cannot be
compared [64,185]. Roy et al. [134] measured paravertebral and in other studies the
4 9
hands [159,91,111]. On the exact physiological reaction of blood vessels is debated.
Perry et al. (2008) [122] suspect a supra-spinal mediation from the ventral
periaqueductal grey matter (vasoconstriction) and the dorsal periaqueductal grey
matter (vasodilatation) [185,122]. Other possible theories are, release of cytokines
and pro- and anti-inflammatory mediators, immunologic reactions and neurologic
neurovegetative effects. From the included studies we cannot draw conclusions
regarding long-term results.
There is limited evidence concerns visceral reactions following spinal
manipulation or mobilization. 3 of the 13 studies measured and reported
significant visceral changes [18,20,91]. Differences are seen in HR, BR and HRV.
Surprisingly there are contradictory results following upper cervical treatment. La
Touche et al. [91] report a significant increase of HR (+6.06%) and Budgell et al.
(2001) [18] demonstrated a significant decline of HR (-3.36). This could be
explained by the nature and duration of the technique. La Touche et al. [91]
performed a 3 times, 2 minutes C0-C3 mobilization and Budgell et al.(2001) [18]
did a single C1 HVLAT in 5 seconds. 6 minutes of repetitive C0-C3 mobilizations
evokes more cervical proprioception and vestibular-sympathetic reflex stimuli,
than a single HVLAT. About the exact neurophysiological pathway is debated. Or
the manipulation and mobilization technique stimulate local sympathetic fibers
from superior cervical ganglion or does it influences the cervico-trigeminal
complex, vestibular-sympathetic reflexes and supra-spinal structures is not
known. Both studies of Budgell et al. saw significant changes in HRV [18,20]. With
an increase of sympathetic outflow in direction of the heart and a shift in balance
between parasympathetic and sympathetic cardiac output in favour of the
sympathetic component. The same outcome in HRV is surprisingly, because in
the first study C1 is manipulated and in the second study T1-T4. Neuro-
anatomical is suspected that a C1 region influences the PSNS and the T1-T4
region affects the SNS. Possible explanations of results may be supra-spinal
mediating, vestibule-sympathetic reflexes (C0-C3) and hemodynamic
alternations due to the thoracic thrust (thoracic thrust compression has direct
mechanical effect on the heart and great blood vessels, influence on blood
pressure and cardiovascular mechanoreceptors).
5 0
The majority of the studies reported significant differences in PPT and VAS
between intervention and sham or control group [159,91,109]. These positive
foundings are similar as previous studies [171,44,121,152]. Nociceptic mechanisms of
pain are known to be complex, involving bi-directional interactions between
peripheral nociceptors, spinal cord and supra-spinal centers [10,12,116].
Nociception is centrally regulated by, dorsal horn neurons and dPAG activity
[92,93,164]. Also local nociceptors threshold and local mediators play an important
role in processing from nociception. The SNS has the possibility to influence
nociception on a peripheral, local or central level. Evidence has shown that
spinal manipulation and mobilization has an effect on the descending pain
inhibitory systems upon short-term hypoalgesic effect [159,91,109,147,178,171].
Vincenzino et al. reported a hypoalgesic affect following a cervical manipulation
[169]. The hypoalgesia was significantly correlated with sympathoexcitation
[169,171]. Skyba et al. supported this theory in an animal study; mobilization of a
hyperalgesic knee joint in rats had a hypoalgesic effect [152]. This effect could be
possible due to descending serotoninergic or noradrenergic inhibitory
mechanisms via corticospinal pathways from the dPAG [96, 9,178,187]. A
noradrenergic effect is most likely because, this dPAG neurotransmitter is more
effective in inhibiting mechanical nociception than thermal nociception, which is
serotoninergically mediated [89,90]. This explains the significant difference in PPT
and the non-significant difference in TPT in the study of Sterling et al. [159]. These
reports are consistent with previous studies which found significant changes in
PPT and no significant changes in TPT following manipulation or mobilization
[171,172,121]. Studies have shown that manipulation or mobilization might be the
perfect stimulus for dPAG regulated nonopioid hypoalgesia and
sympathoexcitatory effects [171,172,10,159,91]. Or these effects segmental or extra-
segmental occur is still debated. Some included studies measured bilateral
effects in the related segment [159,123,113,122,111] however other studies have
shown to changes values distal to the treated segment; that is, manipulation of
the thoracic spine has positive effects on arm or cervical pain [80,109] and cervical
application influences cardiac outcomes and face [18,91,20]. Unfortunately the
studies which found segmental differences only measured in the related
segmental [159,123,113,122,111], hereby no conclusions can be drawn about extra-
segmental effects. Most of the segmental related effects are bilaterally, which

5 1
assumes that these are probably extra-segmentally coordinated. Also is the
somatic segmental distribution more accurate segmented than the
neurovegetative or SNS segmental distribution. Because of the difference in the
segmental distribution it is difficult to draw conclusions.
Immediately hypoalgesia effects can also be described to dorsal horn modulat ion
[9,10,14]. Researchers suggest that manipulation inhibit pain at the dorsal horn
through alternations of the neuroplastic changes [14]. They think that a
manipulation and mobilization stimulus closes the ‘gate’ for C-fiber mediated
nociception [159,126,171,169,178].
Statistically significant changes are dependent of the minimal clinically important
difference (MCID). The MCID is the smallest change in outcome perceived as
important and beneficial for the patients management [175]. Todd et al. reported
that a minimal VAS change of -13mm is clinically significant [163]. Bird et al. say
that the minimal clinically significant change in VAS depends on the baseline
VAS of the participant [11,32]. They have calculated that a change of -13mm in
VAS would be clinically significant for a baseline VAS <34mm, a change of -
17mm VAS for a baseline VAS between 34mm and 67mm and a change of -
28mm VAS for a baseline VAS >67mm [11,32]. According to Todd and Bird et al.
the VAS changes in the study of Sterling et al. [159] (3.35mm) has no clinical
value. La Touche et al. [91] found a change of 29.13mm and is clinically
important. Mohammadian et al. reported no mean or absolute VAS values, only a
bar graph [109]. According to the bar graph the VAS decreases +/-15mm (45mm-
30mm) following spinal manipulation. According the opinion of Todd et al. it is a
significant decrease (>13mm) and in opinion of Bird et al. it is not (<17mm).
3 included studies examined PPT. 2 studies found significant differences.
Sterling et al. [159] found a 22.55% increase of PPT and La Touche et al. [91]
found an increase of 64-77% for masseter, 38-59% for temporalis and 47-79%
for all cervical PPT point. Significant results are consistent with previous studies.
Vicenzino et al. [171] reported an increase of 25%, Yeo and Wright [183] an
increase of 23% following an accessory ankle dorsiflexion mobilization, Moss et
al. [110] an increase of 27.3% following an anterior-posterior mobilization of
osteoarthritic knee joints and Paungmali et al. [121] an 15.4% increase after a
mobilization with movement of the elbow. The increase found by La Touche et al.
5 2
clearly exceeds the other studies [91]. La Touche et al. performed 3 treatment
sessions in 2 weeks of 3 times 2 minutes C0-C3 mobilization [91]. The duration
and number of treatment sessions is similar as in the studies of Paungmali et al.
[121] and Moss et al. [110]. La Touche et al. [91] found a maintained carry-over
effect of PPT and VAS between the sessions; this is not found in the study of
Moss et al. [110]. A explanation could be that Paungmali et al. [121] and Moss et al.
[110] treated peripheral joints and La Touche et al. [91] performed a mobilization
technique on a cervical vertebrae, which has a higher density of proprioceptors
[102,132] and a greater central neurological connection (cervico-trigeminale
interaction and different specialist tracts) [91,85,13]. Previous research has
demonstrated the reliability and validity of PPT measures in pain-free individuals
[117]. Also a study of Ohrbach et al. suggest PPT-validity between groups data of
pain vs. no-pain subjects [119]. Findings in a study of Bird et al. and Gallagher et
al. suggest that a change of at least 15% in PPT is needed for a clinically
significant difference [11,40]. Both studies, Sterling et al. and La Touche et al.
exceed 15% and have a clinically significant effect [159,91]. Prior to the study of
Sterling et al. the reliability of the PPT measurement was determined on 10
subjects (5 male and 5 female) [159]. The intra-examiner reliability was excellent
with intraclass correlation coefficients of 0.923 for the right and 0.912 for the left
articular pillars of C5-C6 vertebral segment. Standard error of measurements
(SEM) was 1.41 kPa for the right and 1.62 kPa for the left side. Indicating small
variability in mean PPT values.
Regarding to SC, ST and CBF, no minimal clinically important difference or
clinically significant values are published. As result it is not clear if the found
differences in SC, ST and CBF are clinically important for our practice.
It is unknown whether neurovegetative changes provoke a significant reaction in
the body or produce lasting results. There is limited evidence on long-term
effects. 1 included study measured inter-session carry-over effects over 2 weeks
[91]. Only PPT and VAS scores had a maintained intersession effect and changes
in SC, BR and HR reversed after each session. Vincenzino et al. reported a
22mm pain reduction on the VAS score 24 hours after cervical manipulation on
lateral epicondylalgia [169].

5 3
By far the majority of the included interventions provoked sympathoexcitatory
responses. This reaction was irrespective of the region of the spine. This finding
is consistent with the findings of the majority of the high-quality RCTs. This
review revealed convincing evidence that sympathetic reactions can be evoked
by spinal manipulation and mobilization techniques and is excitatory of nature.
Andreassi et al. describe that there might be a difference in sympathetic
response between a-symptomatic and symptomatic subjects. They describe a
sympathetic ‘rebound effect’ by symptomatic subjects [2]. Pain changes the
activity of the SNS and an increased SNS due to pain returns to levels below
their pre-stimulus values following spinal manipulation and mobilization [2]. Other
studies report no differences in SNS changes following spinal manipulation and
mobilization between a-symptomatic and symptomatic subjects [10,9]. Probably it
is dependent on the type of lesion and how the SNS is involved. Also a-
symptomatic participants may have spine dysfunctions that could affect
neurophysiological processes [9,126]. Future studies on a large scale in various
types of symptomatic participants are necessary in order to draw concrete
conclusions.
It is not possible to answer the secondary research question; Is there a
difference between manual spinal manipulation and mobilizat ion on
neurovegetative physiological parameters of symptomatic and a-symptomatic
adults in manual therapy, chiropractic or osteopathic medicine? This because of
the differences in duration, number of sessions, location of application on the
spine and measurement methods. Also not every physiological parameter is
examined following spinal manipulation and mobilization. As result, a comparison
between spinal manipulation and mobilization for these parameters is not
possible. Results in BR and PPT are solely reported following spinal mobilization
[91,159,154] and pupillary [150] and HRV changes [18,20] are solely measured after
spinal manipulation. Regarding to SC changes it appears that manipulation [123]
have better results than mobilization [113,159,122,111,91], but on account of a single
study it is not advisable to draw conclusions. Given the overall good results in
the study of La Touche et al. it seems like multiple sessions for some
physiological parameters (PPT-VAS) have beneficial effects [91]. Also the
duration of the application seems to be of interest. Studies demonstrated a
5 4
relationship between SNS results and duration and dose [23,155]. They reported
that frequency and duration of application time has a significant effect on the
response of SNS. Also here the results should be handled with caution because
there is limited evidence on multiple- or inter-session neurovegetative effects.
General, due to the unequal distribution of the number of mobilization
repetitions, number of sessions, different measurement methods/locations and
treatment regions, it is not possible to make concrete statements which
technique is superior.
Despite the evidence, neurophysiological mechanisms are still relatively unclear.
Future research should consider investigating multi -technique, inter-session
effects on different populations. Multi-techniques settings are more therapeutic
representative and results have practical relevance. Inter-session or long-term
measurements give valuable information about time related effects. Evidence
showed that some effects are maintained and other are only short -term [91].
Knowledge about time related effects has practical importance and provides
information about the therapeutic possibilities. The majority of the studies
included have a sample size less than 25 and primary a-symptomatic subjects.
Due to the low number of subjects the significant ‘power’ of the results is
questionable. There is a need for studies with a high ‘power’, sufficient number
of a-symptomatic and selective symptomatic subjects. All except one study
measure neurophysiological, short-term or immediate effects of a single
technique which makes the long-term effects and clinical importance hard to
predict. Effects of multi-technique sessions and multiple sessions are to scare to
drawn concrete conclusions. Multi-technique and multi-session, high-quality
study designs need to be done to measure real clinical importance and
applicability. During the last years there is a paradigm shift in spinal
manipulative therapy and therapists search for scientific answers to
neurophysiological effects due to spinal manipulation. Answers to these
questions are important since spinal manipulations and mobilizations are a
multidisciplinary non-invasive technique, worldwide used and economically
interesting. There is a need of high quality, large sample RCTs on selective
symptomatic subjects with a multi-technique or intersession design. Only than is
a representative therapeutic outcome measurable of strong clinical importance.

5 5
Results will provide important information for all therapists which lead to more
understanding about neurophysiological effects following spinal manipulation or
mobilization what will in the end benefit patients.
Limitations
The results of this literature review should be interpreted with some limitations.
First, the goal of the database search is inclusion current studies. No studies
before 2000 are included in this review. The review may have missed potentially
relevant studies published prior to 2000. Second, this review searched solely in
MEDLINE and Cochrane Library to find selective, high quality studies. A search
in other databases like Google Scholar, EMBASE and CINAHL will result in more
studies. Third, this review may miss some relevant studies despite the broad
search with multiple MeSH-term, adding more MeSH-term probably provide new
studies. Also this study selected only studies in the English language, which may
have excluded some relevant studies. However this is not likely, because the
majority of the RCTs are published in English. Finally, this review is conducted
by a single researcher, search and study analyses performed by 2 or more
researchers provide probably a more accurate and broad vision on this topic.
5 6
7. Conclusion
In conclusion; this review provides evidence that spinal manipulation and
mobilization evoke significant neurovegetative reactions in SC [159,123,122,80,91,111],
PPT [159,91], VAS [91,109], local allodynia and hyperalgesia [109], BR [91], HR [91,18]
and HRV [18,20]. Inconsistent results are found for ST [134,111,109,159,91] and no
significant differences are found for TPT [159], cutaneous blood flow [109], blood
pressure [20] and pupillary reactions [150]. There is no concrete difference in
outcome and efficiency between different types of manual spinal techniques and
between a-symptomatic and symptomatic subjects. Some parameters are
consistent, but in other parameters there is an inconsistency in neurovegetative
effects between studies following spinal manipulation or mobilization. Due to the
unequal distribution of the number of mobilization repetitions, number of
sessions, different measurement methods and treatment locations, it is not
possible to make clear statements which technique is superior. Despite the
evidence, neurophysiological mechanisms are still relatively unclear.
Funding sources and potential conflicts of interest The author declares to have received no funding sources or conflicts of interest for
this review.
Author contributions
All process elements; literature search, analyses and writing are performed by the
author.
Author Details
Koen Groot Zwaaftink is Osteopath at an Osteopathic clinic in Albergen (The
Netherlands). He was awarded with a Bachelor degree in Physiotherapy in 2004
from the University of Applied Sciences of Enschede (The Netherlands). He earned
his Diploma in Osteopathy (D.O.) in 2009 from the International Academy of
Osteopathy (Gent, Belgium). From 2010 he is a teacher in Clinical Neurology and
Cranial Nerves at the International Academy of Osteopathy.
5 7
8. Bibliography
1. Amatuzzi, Fellipe, et al. "Acute effects of osteopathic manipulative treatment in heart rate variability of patients with heart failure: a cross-over study." EUROPEAN JOURNAL OF HEART FAILURE. Vol. 16. 111 RIVER ST, HOBOKEN 07030-5774, NJ USA: WILEY-BLACKWELL, 2014.
2. Andreassi John L. Psychophysiology: human behaviour and physiological response. 3rd ed. London: Erlbaum; 1995. p. 166-370. [Chapters 9-16].
3. Arendt-Nielsen, Lars, et al. "Sensitization in patients with painful knee osteoarthritis." Pain 149.3 (2010): 573-581.
4. Assendelft, Willem JJ, et al. "Spinal manipulative therapy for low back pain: a meta-
analysis of effectiveness relative to other therapies." Annals of internal medicine 138.11 (2003): 871-881.
5. Balon, Jeffrey W., and Silvano A. Mior. "Chiropractic care in asthma and allergy."
Annals of Allergy, Asthma & Immunology 93.2 (2004): S55-S60.
6. Barman, SUSAN M., and ROBERT D. Wurster. "Interaction of descending spinal
sympathetic pathways and afferent nerves." American Journal of Physiology-Heart and Circulatory Physiology 234.3 (1978): H223-H229.
7. Benarroch, E. E. "Pain-autonomic interactions." Neurological Sciences 27.2 (2006):
s130-s133.
8. Bialosky, Joel E., et al. "Placebo response to manual therapy: something out of
nothing?." Journal of Manual & Manipulative Therapy 19.1 (2011): 11-19.
9. Bialosky, Joel E., et al. "The mechanisms of manual therapy in the treatment of
musculoskeletal pain: a comprehensive model." Manual therapy 14.5 (2009): 531-538.
10. Bialosky, Joel E., et al. "The relationship of the audible pop to hypoalgesia associated
with high-velocity, low-amplitude thrust manipulation: a secondary analysis of an experimental study in pain-free participants." Journal of manipulative and physiological therapeutics 33.2 (2010): 117-124.
11. Bird, Steven B., and Eric W. Dickson. "Clinically significant changes in pain along the
visual analog scale." Annals of emergency medicine 38.6 (2001): 639-643.
12. Bishop, Mark D., Jason M. Beneciuk, and Steven Z. George. "Immediate reduction in
temporal sensory summation after thoracic spinal manipulation." The Spine Journal 11.5 (2011): 440-446.
13. Blaschek, Astrid, et al. "Self-reported neck pain is associated with migraine but not with
tension-type headache in adolescents." Cephalalgia 34.11 (2014): 895-903.
14. Boal, Robert W., and Richard G. Gillette. "Central neuronal plasticity, low back pain and
spinal manipulative therapy." Journal of manipulative and physiological therapeutics 27.5 (2004): 314-326.
15. Bolton, Philip S., and Brian Budgell. "Visceral responses to spinal manipulation."
Journal of Electromyography and Kinesiology 22.5 (2012): 777-784.
16. Bolton, Philip S., and Chester A. Ray. "Neck afferent involvement i n cardiovascular
control during movement." Brain research bulletin 53.1 (2000): 45-49.
17. Bronfort, Gert, et al. "Efficacy of spinal manipulation and mobilization for low back pain
and neck pain: a systematic review and best evidence synthesis." The spine journal 4.3 (2004): 335-356.
5 8
18. Budgell, Brian, and Fumie Hirano. "Innocuous mechanical stimulation of the neck and
alterations in heart-rate variability in healthy young adults." Autonomic Neuroscience 91.1 (2001): 96-99.
19. Budgell, Brian, et al. "Responses of adrenal function to stimulation of lumbar and
thoracic interspinous tissues in the rat." Neuroscience research 28.1 (1997): 33-40.
20. Budgell, Brian, & Polus, B. (2006). The effects of thoracic manipulation on heart rate
variability: a controlled crossover trial. Journal of manipulative and physiological therapeutics, 29(8), 603-610.
21. Bulbulian, Ronald, Jeanmarie Burke, and J. Donald Dishman. "Spinal ref lex excitability
changes after lumbar spine passive flexion mobilization." Journal of manipulative and physiological therapeutics 25.8 (2002): 526-532.
22. Camilleri, Michael, et al. "Effect of somatovisceral reflexes and selective dermatomal
stimulation on postcibal antral pressure activity." American Journal of Physiology-Gastrointestinal and Liver Physiology 247.6 (1984): G703-G708.
23. Chiu, T. W., and A. Wright. "To compare the effects of different rates of application of a
cervical mobilisation technique on sympathetic outflow to the upper limb in normal subjects." Manual Therapy 1.4 (1996): 198-203.
24. Cleland, J. A., Childs, M. J. D., McRae, M., Palmer, J. A., & Stowell, T. (2005).
Immediate effects of thoracic manipulation in patients with neck pain: a rand omized clinical trial. Manual therapy, 10(2), 127-135.
25. Cleland, Joshua A., et al. "Short-term effects of thrust versus nonthrust
mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial." Physical therapy 87.4 (2007): 431-440.
26. Cleland, Joshua, et al. "Short-term effects of thoracic manipulation on lower trapezius
muscle strength." Journal of Manual & Manipulative Therapy (2013).
27. Colloca, Christopher J., Tony S. Keller, and Robert Gunzburg. "Neuromec hanical
characterization of in vivo lumbar spinal manipulation. Part II. Neurophysiological response." Journal of manipulative and physiological therapeutics 26.9 (2003): 579-591.
28. Cutler, Michael J., et al. "Cranial manipulation can alter sleep latency and sympathetic
nerve activity in humans: a pilot study." Journal of Alternative & Complementary Medicine 11.1 (2005): 103-108.
29. Degenhardt, Brian F., et al. "Role of osteopathic manipulative treatment in altering pain
biomarkers: a pilot study." The Journal of the American Osteopathic Association 107.9 (2007): 387-400.
30. Dimmick, Karen R., Martin F. Young, and David Newell. "Chiropractic manipulation
affects the difference between arterial systolic blood pressures on the left and right in normotensive subjects." Journal of manipulative and physiological therapeutics 29.1 (2006): 46-50.
31. Dishman, J. Donald, and Jeanmarie Burke. "Spinal reflex excitability changes after
cervical and lumbar spinal manipulation: a comparative study." The spine journal 3.3 (2003): 204-212.
32. Dixon, J. S., and H. A. Bird. "Reproducibility along a 10 cm vertical visual analogue
scale." Annals of the Rheumatic Diseases 40.1 (1981): 87-89.
5 9
33. Dufour, Andre, and Victor Candas. "Ageing and thermal responses during passive heat exposure: sweating and sensory aspects." European journal of applied physiology 100.1 (2007): 19-26.
34. Edelberg, Robert. "Relation of electrical properties of skin to struct ure and physiologic
state." Journal of Investigative Dermatology 69.3 (1977): 324-327.
35. Engel, Roger M., and Subramanyam Vemulpad. "The effect of combining manual
therapy with exercise on the respiratory function of normal individuals: a randomized control trial." Journal of manipulative and physiological therapeutics 30.7 (2007): 509-513.
36. Ernst, E. "Does spinal manipulation have specific treatment effects?." Family Practice
17.6 (2000): 554-556.
37. Evans, David W. "Mechanisms and effects of spinal high-velocity, low-amplitude thrust
manipulation: previous theories." Journal of manipulative and physiological therapeutics 25.4 (2002): 251-262.
38. Fisher, Peter, and Adam Ward. "Complementary medicine in Europe." BMJ: British
Medical Journal 309.6947 (1994): 107.
39. Fujimoto, Takahiro, et al. "Arterial tonometry in the measurement of the effects of
innocuous mechanical stimulation of the neck on heart rate and blood pressure." Journal of the autonomic nervous system 75.2 (1999): 109-115.
40. Gallagher, E. John, Michele Liebman, and Polly E. Bijur. "Prospective validation of
clinically important changes in pain severity measured on a visual analog scale." Annals of emergency medicine 38.6 (2001): 633-638.
41. George, Steven Z., et al. "Immediate effects of spinal manipulation on thermal pain
sensitivity: an experimental study." BMC Musculoskeletal disorders 7.1 (2006): 1.
42. Gibbons, Peter F., and Cameron M. Gosling. "Short -term effects of cervical manipulation
on edge light pupil cycle time: a pilot study." Journal of manipulative and physiological therapeutics 23.7 (2000): 465-469.
43. Giles, Paul D., et al. "Suboccipital decompression enhances heart rate variability indices
of cardiac control in healthy subjects." The Journal of Alternative and Complementary Medicine 19.2 (2013): 92-96.
44. Goodsell, Michalene, Michael Lee, and Jane Latimer. "Short -term effects of lumbar
posteroanterior mobilization in individuals with low-back pain." Journal of Manipulative and Physiological Therapeutics 23.5 (2000): 332-342.
45. Grewe, W., W. Jänig, and H. Kümmel. "Effects of hypothalamic thermal stimuli on
sympathetic neurones innervating skin and skeletal muscle of the cat hindlimb." The Journal of physiology 488.1 (1995): 139-152.
46. Gross, Anita R., et al. "A Cochrane review of manipulation and mobi lization for
mechanical neck disorders." Spine 29.14 (2004): 1541-1548.
47. Harris, W., and R. J. Wagnon. "The effects of chiropractic adjustments on distal skin
temperature." Journal of manipulative and physiological therapeutics 10.2 (1987): 57-60.
48. Hartman, Laurie S. Handbook of osteopathic technique. Springer, 2013.
49. Hegedus, Eric J., et al. "The neurophysiological effects of a single session of spinal joint
mobilization: does the effect last?." Journal of Manual & Manipulative Therapy 19.3 (2011): 143-151.
6 0
50. Herzog, Walter. "The biomechanics of spinal manipulation." Journal of bodywork and movement therapies 14.3 (2010): 280-286.
51. Herzog, Walter. "The biomechanics of spinal manipulation." Critical Reviews™ in
Physical and Rehabilitation Medicine 13.2-3 (2001).
52. Herzog, Walter, David Scheele, and Philip J. Conway. "Electromyographic responses of
back and limb muscles associated with spinal manipulative therapy." Spine 24.2 (1999): 146-152.
53. Holstege, Gert. "Descending pathways from the periaqueductal g ray and adjacent
areas." The midbrain periaqueductal gray matter . Springer US, 1991. 239-265.
54. Hsieh, C-Y., et al. "Mulligan's mobilization with movement for the thumb: a single case
report using magnetic resonance imaging to evaluate the positional fault hypothesis." Manual therapy 7.1 (2002): 44-49.
55. Ianuzzi, Allyson, and Partap S. Khalsa. "Comparison of human lumbar facet joint
capsule strains during simulated high-velocity, low-amplitude spinal manipulation versus physiological motions." The Spine Journal 5.3 (2005): 277-290.
56. Ianuzzi, Allyson, and Partap S. Khalsa. "High loading rate during spinal manipulation
produces unique facet joint capsule strain patterns compared with axial rotations." Journal of manipulative and physiological therapeutics 28.9 (2005): 673-687.
57. International Association for the Study of Pain. IASP Pain Terminology; 2006. Available at
http://www.iasp-pain.org/AM/Template.cfm?Section=Home&Template=/CM/HTMLDisplay.cfm&ContentID=3058. Accessed September 29, 2010.
58. Jäkel, Anne, and Phillip von Hauenschild. "Therapeutic effects of cranial osteopathic manipulative medicine: a systematic review." J Am Osteopath Assoc 111.12 (2011): 685-93.
59. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis.
Cambridge University Press, 2008. Chapter: 1, pp.13.
60. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 2, pp.49.
61. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.128.
62. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 10, pp.376.
63. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 10, pp.386.
64. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.113.
65. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.115.
66. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.116.
67. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.122.
68. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.120.
69. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.121.
6 1
70. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.131.
71. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.125.
72. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.126.
73. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.127.
74. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.129.
75. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 4, pp.130.
76. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 9, pp.332.
77. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: 9, pp.367.
78. Jänig, Wilfrid. Integrative action of the autonomic nervous system: Neurobiology of homeostasis. Cambridge University Press, 2008. Chapter: Introduction, pp.2.
79. Joyner, Michael Joseph, and J. R. Halliwill. "Sympathetic vasodilatation in human limbs." The Journal of physiology 526 (2000): 471-480.
80. Jowsey, Pete, and Jo Perry. "Sympathetic nervous system effects in the hands following
a grade III postero-anterior rotatory mobilisation technique applied to T4: a randomised, placebo-controlled trial." Manual therapy 15.3 (2010): 248-253.
81. Kang, Yu-Ming, et al. "Somatosympathetic reflexes from the low back in the
anesthetized cat." Journal of neurophysiology 90.4 (2003): 2548-2559.
82. Kaptchuk, Ted J. "The placebo effect in alternative medicine: can the performance of a
healing ritual have clinical significance?." Annals of internal medicine 136.11 (2002): 817-825.
83. Karason, Agust B., and Ian P. Drysdale. "Somatovisceral response following osteopathic
HVLAT: a pilot study on the effect of unilateral lumbosacral high -velocity low-amplitude thrust technique on the cutaneous blood flow in the lower limb." Journal of manipulative and physiological therapeutics 26.4 (2003): 220-225.
84. Keller, Tony S., and Christopher J. Colloca. "Mechanical force spinal manipulation
increases trunk muscle strength assessed by electromyography: a comparative clinical trial." Journal of Manipulative and Physiological Therapeutics 23.9 (2000): 585-595.
85. Kerr, Frederick WL. "The potential of cervical primary afferents to sprout in the spinal
nucleus of V following long term trigeminal denervation." Brain research 43.2 (1972): 547-560.
86. Kingston, L., Claydon, L., & Tumilty, S. (2014). The effects of spinal mobilizations on the
sympathetic nervous system: a systematic review. Manual therapy, 19(4), 281-287.
87. Koes, Bart W., et al. "An updated overview of clinical guidelines for the management of non-specific low back pain in primary care." European Spine Journal 19.12 (2010): 2075-2094.
88. Kuchera, William A., and Michael L. Kuchera. Osteopathic principles in practice.
Greyden Press LLC, 1994.
6 2
89. Kuraishi, Y., et al. "Separate involvement of the spinal noradrenergic and serotonergic systems in morphine analgesia: the differences in mechanical and thermal algesic tests." Brain research 273.2 (1983): 245-252.
90. Kuraishi, Y., et al. "Intrathecal injections of galanin and its antiserum affect nociceptive
response of rat to mechanical, but not thermal, stimuli." Pain 44.3 (1991): 321-324.
91. La Touche, Roy, et al. "Does mobilization of the upper cervical spine affect p ain
sensitivity and autonomic nervous system function in patients with cervico -craniofacial pain?: A randomized-controlled trial." The Clinical journal of pain 29.3 (2013): 205-215.
92. LaMotte, Robert H., L. E. Lundberg, and H. E. Torebjörk. "Pain, hyperalge sia and
activity in nociceptive C units in humans after intradermal injection of capsaicin." The Journal of Physiology 448.1 (1992): 749-764.
93. LaMotte, Robert H., et al. "Neurogenic hyperalgesia: psychophysical studies of
underlying mechanisms." Journal of neurophysiology 66.1 (1991): 190-211.
94. Li, To Shan, and Kristie Grove Bridges. "Effects of rib raising on the autonomic nervous
system: a pilot study using noninvasive biomarkers." J Am Osteopath Assoc 110.6 (2010): 324-330.
95. Licciardone, John C., et al. "Osteopathic manipulative treatment of back pain and
related symptoms during pregnancy: a randomized controlled trial." American journal of obstetrics and gynecology 202.1 (2010): 43-e1.
96. Lovick, T. A. "Interactions between descending pathways from the dorsal and
ventrolateral periaqueductal gray matter in the rat." The midbrain periaqueductal gray matter. Springer US, 1991. 101-120.
97. Maher, Christopher G., et al. "Reliability of the PEDro scale for rating quality of
randomized controlled trials." Physical therapy 83.8 (2003): 713-721.
98. Maitland, Geoffrey Douglas. Vertebral manipulation. Butterworth-Heinemann, 2013.
99. Maitland, Geoffrey Douglas. Maitland's vertebral manipulation. Eds. Elly Hengeveld,
Kevin Banks, and Kay English. Vol. 1. Butterworth-Heinemann, 2005.
100. Malisza, Krisztina L., et al. "Functional MRI of the rat lumbar spinal cord
involving painful stimulation and the effect of peripheral joint mobilization." Journal of magnetic resonance imaging 18.2 (2003): 152-159.
101. McGuiness, J., B. Vicenzino, and A. Wright. "Influence of a cervical mobilization
technique on respiratory and cardiovascular function." Manual Therapy 2.4 (1997): 216-220.
102. McLain, Robert F. "Mechanoreceptor endings in human cervical facet joints."
Spine 19.5 (1994): 495-501.
103. McLean, Sionnadh, et al. "A pilot study of the manual force levels required to
produce manipulation induced hypoalgesia." Clinical Biomechanics 17.4 (2002): 304-308.
104. McPartland, John M., et al. "Cannabimimetic effects of osteopathic manipulative
treatment." JOURNAL-AMERICAN OSTEOPATHIC ASSOCIATION 105.6 (2005): 283.
105. McSweeney, Terence P., Oliver P. Thomson, and Ross Johnston. "The
immediate effects of sigmoid colon manipulation on pressure pain thresholds in the lumbar spine." Journal of bodywork and movement therapies 16.4 (2012): 416-423.
6 3
106. Michaleff, Z. A., et al. "Spinal manipulation epidemiology: systematic review of cost effectiveness studies." Journal of Electromyography and Kinesiology 22.5 (2012): 655-662.
107. Mierau, D., et al. "Manipulation and mobilization of the third
metacarpophalangeal joint: a quantitative radiographic and range of motion study." Manual Medicine 3 (1988): 135-140.
108. Miller, Stephen D., and H. Stanley Thompson. "Edge-light pupil cycle time."
British Journal of Ophthalmology 62.7 (1978): 495-500.
109. Mohammadian, Parvaneh, et al. "Areas of capsaicin-induced secondary
hyperalgesia and allodynia are reduced by a single chiropractic adjustment: a preliminary study." Journal of manipulative and physiological therapeutics 27.6 (2004): 381-387.
110. Moss, Penny, Kathleen Sluka, and Anthony Wright. "The initial effects of knee
joint mobilization on osteoarthritic hyperalgesia." Manual therapy 12.2 (2007): 109-118.
111. Moulson, Andrea, and Tim Watson. "A prelim inary investigation into the
relationship between cervical snags and sympathetic nervous system activity in the upper limbs of an asymptomatic population." Manual Therapy 11.3 (2006): 214-224.
112. Mouton, Leonora J., Veronique GJM VanderHorst, and Gert Holste ge. "Large
segmental differences in the spinal projections to the periaqueductal gray in the cat." Neuroscience letters 238.1 (1997): 1-4.
113. Moutzouri, Maria, et al. "The effects of the Mulligan Sustained Natural
Apophyseal Glide (SNAG) mobilisation in the lumbar flexion range of asymptomatic subjects as measured by the Zebris CMS20 3-D motion analysis system." BMC Musculoskeletal disorders 9.1 (2008): 1.
114. Nance, P. W., and C. S. G. Hoy. "Assessment of the autonomic nervous system."
Physical Medicine and Rehabilitation 10 (1996): 15-36.
115. Nansel, Dale, and Mark Szlazak. "Somatic dysfunction and the phenomenon of
visceral disease simulation: a probable explanation for the apparent effectiveness of somatic therapy in patients presumed to be suffering from true v isceral disease." Journal of manipulative and physiological therapeutics 18.6 (1994): 379-397.
116. Nijs, Jo, and Boudewijn Van Houdenhove. "From acute musculoskeletal pain to
chronic widespread pain and fibromyalgia: application of pain neurophysiology in manual therapy practice." Manual therapy 14.1 (2009): 3-12.
117. Nussbaum, Ethne L., and Laurie Downes. "Reliability of clinical pressure -pain
algometric measurements obtained on consecutive days." Physical therapy 78.2 (1998): 160-169.
118. Ogura, T., et al. "Regional cerebral metabolic changes in patients with neck pain
following chiropractic spinal manipulation:[18F] FDG PET Analysis." Alternative Therapies in Health and Medicine (2007).
119. Ohrbach, Richard, and Elliot N. Gale. "Pressure pain thresholds, clinical
assessment, and differential diagnosis: reliability and validity in patients with myogenic pain." Pain 39.2 (1989): 157-169.
120. Owens, Edward F., et al. "Paraspinal skin temperature patterns: an interexaminer
and intraexaminer reliability study." Journal of manipulative and physiological therapeutics 27.3 (2004): 155-159.
6 4
121. Paungmali, Aatit, et al. "Hypoalgesic and sympathoexcitatory effects of mobilization with movement for lateral epicondylalgia." Physical Therapy 83.4 (2003): 374-383.
122. Perry, Jo, and Ann Green. "An investigation into the effects of a unilaterally
applied lumbar mobilisation technique on peripheral sympathetic nervous system activity in the lower limbs." Manual therapy 13.6 (2008): 492-499.
123. Perry, Jo, et al. "A preliminary investigation into the magnitude of effect of
lumbar extension exercises and a segmental rotatory manipulation on sympathetic nervous system activity." Manual therapy 16.2 (2011): 190-195.
124. Petersen, Neil, Bill Vicenzino, and Anthony Wright. "The effects of a cervical
mobilisation technique on sympathetic outflow to the upper limb in normal subjects." Physiotherapy Theory and Practice 9.3 (1993): 149-156.
125. Pickar Joel G., Kenny M.J., Henderson C.N.R., Gudavalli M.R. “Somatosympathic reflex
mechanisms.” In book: The Science and Clinical Application of Manual Therapy, (2011): Chapter: 3, Publisher: Churchill Livingstone, Editors: H.H. King, W. Janig, M.M. Patterson, pp.55-69 (Ed.).
126. Pickar, Joel G. "Neurophysiological effects of spinal manipulation." The Spine Journal 2.5 (2002): 357-371.
127. Pincus, Tamar, et al. "Cognitive-behavioral therapy and psychosocial factors in low back pain: directions for the future." Spine 27.5 (2002): E133-E138.
128. Plaugher, Gregory, and Trent R. Bachman. "Chiropractic management of a
hypertensive patient." Journal of manipulative and physiological therapeutics 16.8 (1993): 544-549.
129. Proctor, M. L., et al. "Spinal manipulation for primary and secondary
dysmenorrhoea." The Cochrane Library (2001).
130. Radtke, Andrea, et al. "Vestibulo-autonomic control in man: short-and long-
latency vestibular effects on cardiovascular function." Journal of Vestibular Research 13.1 (2003): 25-37.
131. Ren, Yong, et al. "Sympathetic modulation of activity in Aδ-and C-primary
nociceptive afferents after intradermal injection of capsaicin in rats." Journal of neurophysiology 93.1 (2005): 365-377.
132. Richmond, F. J., and D. A. Bakker. "Anatomical organization and sensory
receptor content of soft tissues surrounding upper cervical vertebrae in the cat." Journal of neurophysiology 48.1 (1982): 49-61.
133. Ross, J. Kim, David E. Bereznick, and Stuart M. McGill. "Determining cavitation
location during lumbar and thoracic spinal manipulation: is spinal manipulation accurate and specific?." Spine 29.13 (2004): 1452-1457.
134. Roy, Richard A., Jean P. Boucher, and Alain S. Comtois. "Paraspinal cutaneous temperature modification after spinal manipulation at L5." Journal of manipulative and physiological therapeutics 33.4 (2010): 308-314.
135. Roy, Richard A., Jean P. Boucher, and Alain S. Comtois. "Heart rate variability
modulation after manipulation in pain-free patients vs patients in pain." Journal of manipulative and physiological therapeutics 32.4 (2009): 277-286.
136. Rubinstein, Sidney M., et al. "Spinal manipulative therapy for chronic low-back
pain: an update of a Cochrane review." Spine 36.13 (2011): E825-E846.
6 5
137. Ruffini, Nuria, et al. "Variations of high frequency parameter of heart rate variability following osteopathic manipulative treatment in healthy subjects compared to control group and sham therapy: randomized controlled trial." Frontiers in neuroscience 9 (2015).
138. Sampath, Kesava Kovanur, et al. "Measureable changes in the neuro-endocrinal
mechanism following spinal manipulation." Medical hypotheses 85.6 (2015): 819-824.
139. Sato, Akio. "The reflex effects of spinal somatic nerve stimulation on visceral
function." Journal of manipulative and physiological therapeutics 15.1 (1992): 57-61.
140. Sato, Akio, and R. S. Swenson. "Sympathetic nervous system response to
mechanical stress of the spinal column in rats." Journal of manipulative and physiological therapeutics 7.3 (1984): 141-147.
141. Sato, Akio, Y. Sato, and R. F. Schmidt. "Heart rate changes reflecting
modifications of efferent cardiac sympathetic outflow by cutaneous and muscle afferent volleys." Journal of the autonomic nervous system 4.3 (1981): 231-247.
142. Sato, Akio, Y. Sato, and R. F. Schmidt. "Changes in heart rate and blood
pressure upon injection of algesic agents into skeletal muscle." Pflügers Archiv 393.1 (1982): 31-36.
143. Sato, Y., H-G. Schaible, and R. F. Schmidt. "Reactions of cardiac postganglionic
sympathetic neurons to movements of normal and inflamed knee joints." Journal of the autonomic nervous system 12.1 (1985): 1-13.
144. Scerbo, Angela Scarpa, et al. "A major effect of recording site on measurement
of electrodermal activity." Psychophysiology 29.2 (1992): 241-246.
145. Schattschneider, Jorn, et al. "Complex regional pain syndromes: the influence of
cutaneous and deep somatic sympathetic innervation on pain." The Clinical journal of pain 22.3 (2005): 240-244.
146. Schomacher, Jochen. "The effect of an analgesic mobilization technique when
applied at symptomatic or asymptomatic levels of the cervical spine in subjects with neck pain: a randomized controlled trial." Journal of Manual & Manipulative Therapy (2013).
147. Schmid, Annina, et al. "Paradigm shift in manual therapy? Evidence for a central nervous system component in the response to passive cervical joint mobilisation." Manual Therapy 13.5 (2008): 387-396.
148. Shi, X., Rehrer, S., Prajapati, P., Stoll, S. T., Gamber, R. G., & Fred Downey, H. (2011). Effect of
cranial osteopathic manipulative medicine on cerebral tissue oxygenation. Journal of the American Osteopathic Association, 111(12), 660.
149. Sillevis, Rob, and Joshua Cleland. "Immediate effects of the audible pop fr om a thoracic spine thrust manipulation on the autonomic nervous system and pain: a secondary analysis of a randomized clinical trial." Journal of manipulative and physiological therapeutics 34.1 (2011): 37-45.
150. Sillevis, Rob, et al. "Immediate effects of a thoracic spine thrust manipulation on
the autonomic nervous system: a randomized clinical trial." Journal of Manual & Manipulative Therapy 18.4 (2010): 181-190.
151. Simon, R., B. Vicenzino, and A. Wright. "The influence of an anteroposterior
accessory glide of the glenohumeral joint on measures of peripheral sympathetic nervous system function in the upper limb." Manual Therapy 2.1 (1997): 18-23.
6 6
152. Skyba, D. A., et al. "Joint manipulation reduces hyperalgesia by activation of monoamine receptors but not opioid or GABA receptors in the spinal cord." Pain 106.1 (2003): 159-168.
153. Slater, H., and A. Wright. "An investigation of the physiological effects of the sympathetic slump on peripheral sympathetic nervous system function in patients with frozen shoulder." Moving in on Pain (1995): 174-184.
154. Soon, Benjamin TC, et al. "A crossover study on the effect of cervical
mobilization on motor function and pressure pain threshold in pain -free individuals." Journal of manipulative and physiological therapeutics 33.9 (2010): 652-658.
155. Souvlis, T., B. G. T. Vicenzino, and A. Wright. "Dose of spinal manual therapy
influences changes in sympathetic nervous system function." More than Skin Deep . Musculoskeletal Physiotherapy Australia, 2001.
156. Sparks, Cheryl, et al. "Using functional magnetic resonance imaging to determine
if cerebral hemodynamic responses to pain change following thoracic spine thrust manipulation in healthy individuals." journal of orthopaedic & sports physical therapy 43.5 (2013): 340-348.
157. Stanton-Hicks, M., et al. "Reflex sympathetic dystrophy: changing concepts and
taxonomy." Pain 63.1 (1995): 127-133.
158. Staud, Roland, et al. "Abnormal sensitization and temporal summation of second
pain (wind-up) in patients with fibromyalgia syndrome." Pain 91.1 (2001): 165-175.
159. Sterling, Michele, G. Jull, and A. Wright. "Cervical mobilisation: concurrent
effects on pain, sympathetic nervous system activity and motor activity." Manual therapy 6.2 (2001): 72-81.
160. Sterling, Michele, et al. "Cervical lateral glide increases nociceptive flexion reflex
threshold but not pressure or thermal pain thresholds in chronic whiplash associated disorders: a pilot randomised controlled trial." Manual therapy 15.2 (2010): 149-153.
161. Symons, Bruce P., et al. "Reflex responses associated with activator treatment."
Journal of manipulative and physiological therapeutics 23.3 (2000): 155-159.
162. Teodorczyk-Injeyan, Julita A., H. Stephen Injeyan, and Richard Ruegg. "Spinal
manipulative therapy reduces inflammatory cytokines but not substance P production in normal subjects." Journal of manipulative and physiological therapeutics 29.1 (2006): 14-21.
163. Todd, Knox H., and Joseph P. Funk. "The minimum clinically important difference
in physician–assigned visual analog pain scores." Academic Emergency Medicine 3.2 (1996): 142-146.
164. Torebjörk, H. E., L. E. Lundberg, and R. H. LaMotte. "Central changes in
processing of mechanoreceptive input in capsaicin ‐induced secondary hyperalgesia in humans." The Journal of Physiology 448.1 (1992): 765-780.
165. Tullberg, Tycho, et al. "Manipulation does not alter the position of the sacroiliac
joint: a roentgen stereophotogrammetric analysis." Spine 23.10 (1998): 1124-1128.
166. Van Cranenburgh, B. "Inleiding in the toegepaste neurowetenschappen, Vol. 1."
Lochem: Uitgeversmaatchappij de Tijdstroom (1989).
167. Verhagen, Arianne P., et al. "The art of quality assessment of RCTs included in
systematic reviews." Journal of clinical epidemiology 54.7 (2001): 651-654.
168. Vicenzino, Bill, et al. "Cardiovascular and respiratory changes produced by
lateral glide mobilization of the cervical spine." Manual Therapy 3.2 (1998): 67-71.
6 7
169. Vicenzino, Bill, David Collins, and Anthony Wright. "The initial effects of a
cervical spine manipulative physiotherapy treatment on the pain and dysfunction of lateral epicondylalgia." Pain 68.1 (1996): 69-74.
170. Vicenzino, Bill, David Collins, and Tony Wright. "Sudomotor changes induced by
neural mobilisation techniques in asymptomatic subjects." Journal of Manual & Manipulative Therapy (2013).
171. Vicenzino, Bill, et al. "An investigation of the interrelationship between manipulative therapy-induced hypoalgesia and sympathoexcitation." Journal of manipulative and physiological therapeutics 21.7 (1998): 448-453.
172. Vicenzino, Bill, et al. "An investigation of the effects of spinal manual therapy on
forequarter pressure and thermal pain thresholds and sympathetic nervous system activity in asymptomatic subjects: a preliminary report." Moving in on pain. 1995.
173. Vickers, Andrew J. "The use of percentage change from baseline as an outcome
in a controlled trial is statistically inefficient: a simulation study." BMC Medical Research Methodology 1.1 (2001): 1.
174. Watanuki, Shoichi, and Katsuhiko Shibuya. "Cerebral metabolic changes in men
after chiropractic spinal manipulation for neck pain." Alternative therapies in health and medicine 17.6 (2011): 12.
175. Wells, George, et al. "Minimal clinically important differences: review of
methods." The Journal of Rheumatology 28.2 (2001): 406-412.
176. Wilson, Thad E., et al. "Effect of age on cutaneous vasoconstrictor responses to
norepinephrine in humans." American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 287.5 (2004): R1230-R1234.
177. Win, Ni Ni, et al. "Effects of Upper and Lower Cervical Spinal Manipulative
Therapy on Blood Pressure and Heart Rate Variability in Volunteers and Patients With Neck Pain: A Randomized Controlled, Cross-Over, Preliminary Study." Journal of chiropractic medicine 14.1 (2015): 1-9.
178. Wright, A. "Hypoalgesia post-manipulative therapy: a review of a potential
neurophysiological mechanism." Manual therapy 1.1 (1995): 11-16.
179. Yates, Bill J. "Vestibular influences on the sympathetic nervous system." Brain
research reviews 17.1 (1992): 51-59.
180. Yates, Bill J. "Vestibular Influences on the Autonomic Nervous Systema." Annals
of the New York Academy of Sciences 781.1 (1996): 458-473.
181. Yates, Bill J., and A. D. Miller. "Properties of sympathetic reflexes elicited by
natural vestibular stimulation: implications for cardiovascular control." Journal of neurophysiology 71.6 (1994): 2087-2092.
182. Yates, Bill J., and A. D. Miller. "Physiological evidence that the vestibular system
participates in autonomic and respiratory control." Journal of Vestibular Research 8.1 (1998): 17-25.
183. Yeo, Hwee Koon, and Anthony Wright. "Hypoalgesic effect of a passive
accessory mobilisation technique in patients with lateral ankle pain." Manual therapy 16.4 (2011): 373-377.
184. Zafereo, Jason A., and Beth K. Deschenes. "The Role of Spinal Manipulation in
Modifying Central Sensitization." Journal of Applied Biobehavioral Research 20.2 (2015): 84-99.

6 8
185. Zegarra-Parodi, Rafael, et al. "Assessment of skin blood flow following spinal
manual therapy: a systematic review." Manual therapy 20.2 (2015): 228-249.
186. Zhang, John, Brian J. Snyder, and Lori Vernor. "The effect of low force
chiropractic adjustments on body surface electromagnetic field." The Journal of the Canadian Chiropractic Association 48.1 (2004): 29.
187. Zusman, M. "Forebrain-mediated sensitization of central pain pathways:‘non -
specific’pain and a new image for MT." Manual therapy 7.2 (2002): 80-88.
6 9
9. List of Abbrevations BP – Blood Pressure
BPM – Beats Per Minute
BR – Breathing Rate
CBF – Cutaneous Blood Flow
CT- Cutaneous Skin Temperature
dPAG – dorsal Peri-Aquaductal Gray Matter
fMRI - functional Magnetic Resonance Imaging
HR – Heart Rate
HRV – Heart Rate Variability
HVLA – High Velocity Low Amplitude
HVLAT – High Velocity Low Amplitude Thrust (Manipulation)
MRI - Magnetic Resonance Imaging
OMT – Osteopathic Manipulative Treatment
PPT – Pressure Pain Threshold
PSNS – Parasympathetic Nervous System
RR – Blood Pressure
SC – Skin Conductance
SMT – Spinal Manipulative Treatment
SNAG – Sustained Natural Apophyseal Glides
SNS – Sympathetic Nervous System
ST – Skin Temperature
TENS - Transcutaneous Electrical Nerve Stimulation
TPT – Thermal Pain Threshold
VAS – Visual Analoge Scale
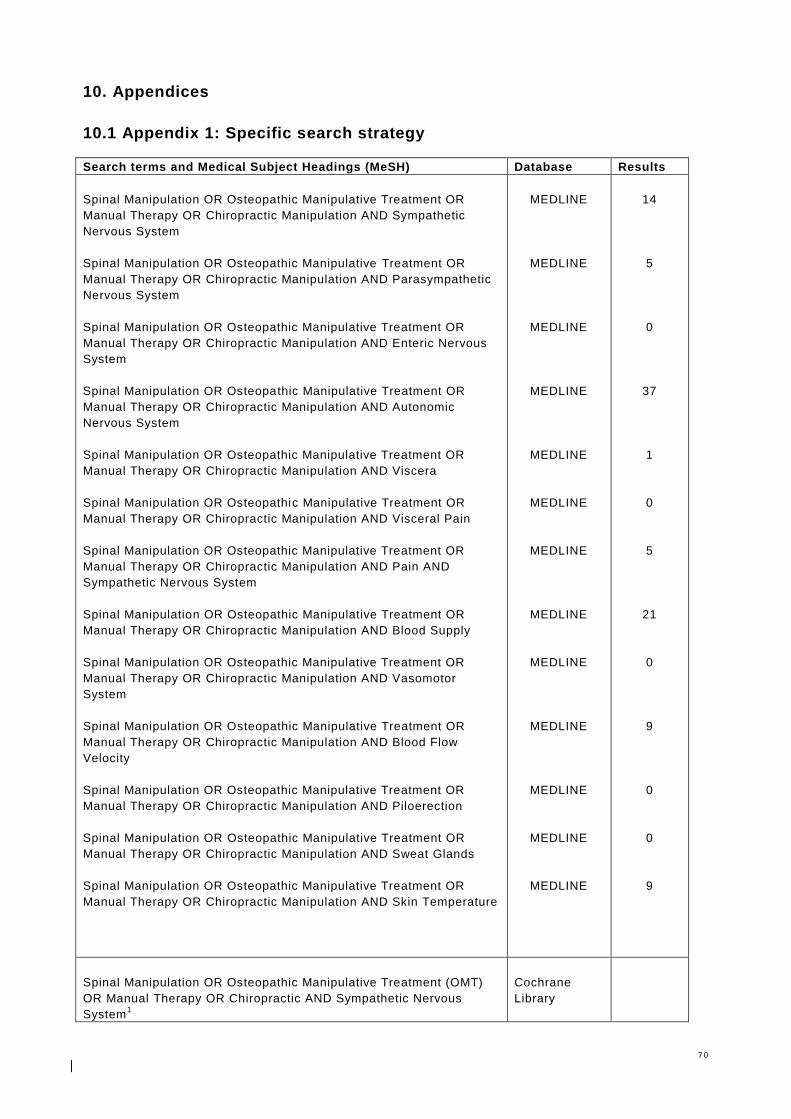
7 0
10. Appendices
10.1 Appendix 1: Specific search strategy Search terms and Medical Subject Headings (MeSH) Database Results
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Sympathetic
Nervous System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Parasympathetic
Nervous System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Enteric Nervous
System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Autonomic
Nervous System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Viscera
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Visceral Pain
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Pain AND
Sympathetic Nervous System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Blood Supply
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Vasomotor
System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Blood Flow
Velocity
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Piloerection
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Sweat Glands
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Skin Temperature
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
MEDLINE
14
5
0
37
1
0
5
21
0
9
0
0
9
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Sympathetic Nervous
System1
Cochrane
Library
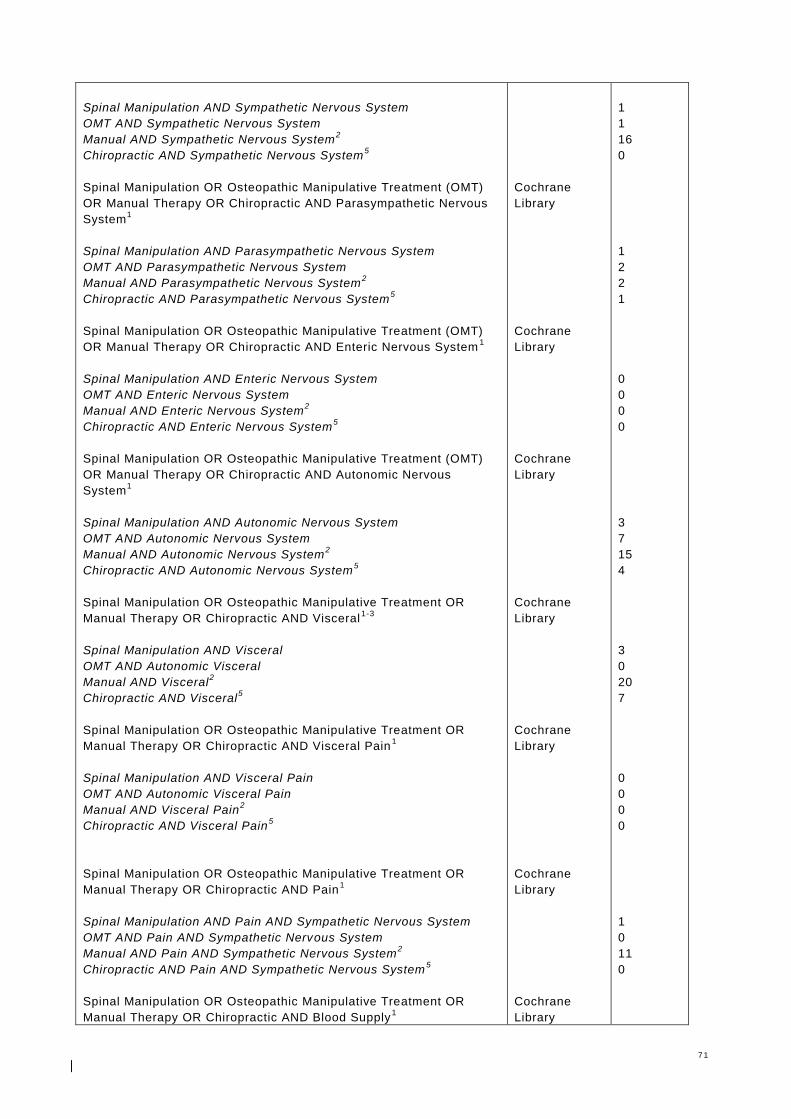
7 1
Spinal Manipulation AND Sympathetic Nervous System
OMT AND Sympathetic Nervous System
Manual AND Sympathetic Nervous System2
Chiropractic AND Sympathetic Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Parasympathetic Nervous
System1
Spinal Manipulation AND Parasympathetic Nervous System
OMT AND Parasympathetic Nervous System
Manual AND Parasympathetic Nervous System2
Chiropractic AND Parasympathetic Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Enteric Nervous System1
Spinal Manipulation AND Enteric Nervous System
OMT AND Enteric Nervous System
Manual AND Enteric Nervous System2
Chiropractic AND Enteric Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Autonomic Nervous
System1
Spinal Manipulation AND Autonomic Nervous System
OMT AND Autonomic Nervous System
Manual AND Autonomic Nervous System2
Chiropractic AND Autonomic Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Visceral1-3
Spinal Manipulation AND Visceral
OMT AND Autonomic Visceral
Manual AND Visceral2
Chiropractic AND Visceral5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Visceral Pain1
Spinal Manipulation AND Visceral Pain
OMT AND Autonomic Visceral Pain
Manual AND Visceral Pain2
Chiropractic AND Visceral Pain5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Pain1
Spinal Manipulation AND Pain AND Sympathetic Nervous System
OMT AND Pain AND Sympathetic Nervous System
Manual AND Pain AND Sympathetic Nervous System2
Chiropractic AND Pain AND Sympathetic Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Blood Supply1
Cochrane
Library
Cochrane
Library
Cochrane
Library
Cochrane
Library
Cochrane
Library
Cochrane
Library
Cochrane
Library
1
1
16
0
1
2
2
1
0
0
0
0
3
7
15
4
3
0
20
7
0
0
0
0
1
0
11
0
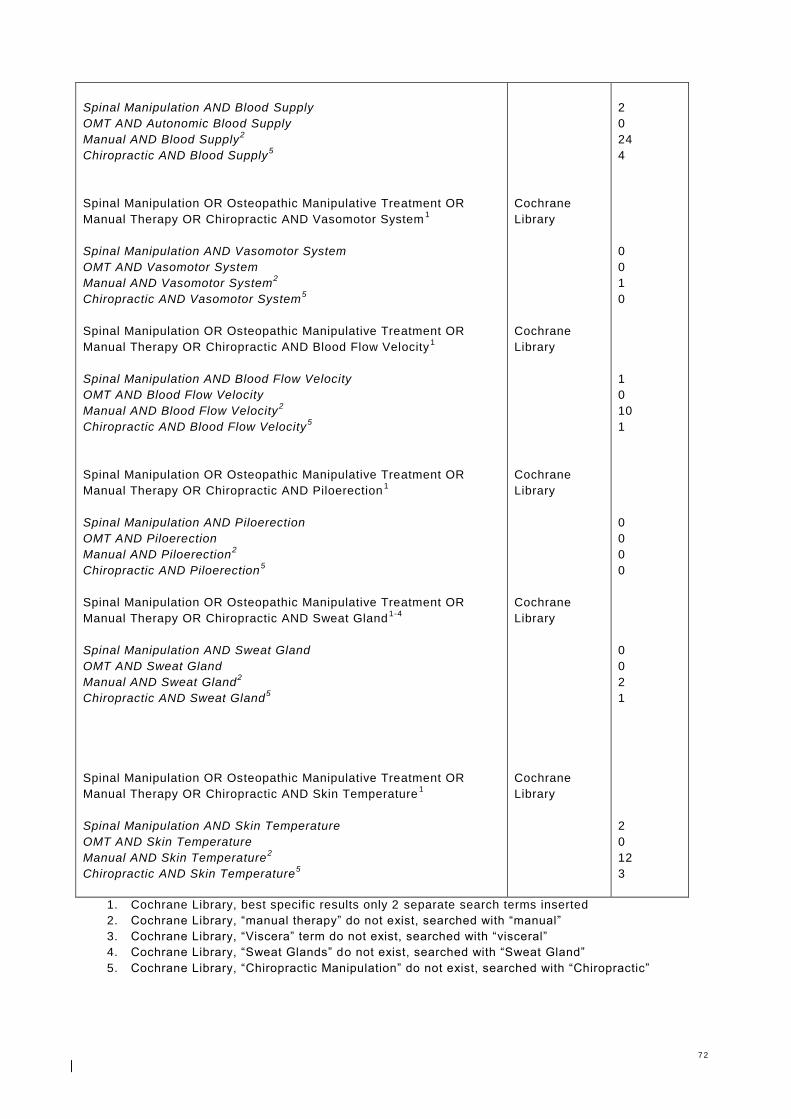
7 2
Spinal Manipulation AND Blood Supply
OMT AND Autonomic Blood Supply
Manual AND Blood Supply2
Chiropractic AND Blood Supply5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Vasomotor System1
Spinal Manipulation AND Vasomotor System
OMT AND Vasomotor System
Manual AND Vasomotor System2
Chiropractic AND Vasomotor System5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Blood Flow Velocity1
Spinal Manipulation AND Blood Flow Velocity
OMT AND Blood Flow Velocity
Manual AND Blood Flow Velocity2
Chiropractic AND Blood Flow Velocity5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Piloerection1
Spinal Manipulation AND Piloerection
OMT AND Piloerection
Manual AND Piloerection2
Chiropractic AND Piloerection5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Sweat Gland1-4
Spinal Manipulation AND Sweat Gland
OMT AND Sweat Gland
Manual AND Sweat Gland2
Chiropractic AND Sweat Gland5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Skin Temperature1
Spinal Manipulation AND Skin Temperature
OMT AND Skin Temperature
Manual AND Skin Temperature2
Chiropractic AND Skin Temperature5
Cochrane
Library
Cochrane
Library
Cochrane
Library
Cochrane
Library
Cochrane
Library
2
0
24
4
0
0
1
0
1
0
10
1
0
0
0
0
0
0
2
1
2
0
12
3
1. Cochrane Library, best specific results only 2 separate search terms inserted
2. Cochrane Library, “manual therapy” do not exist, searched with “manual”
3. Cochrane Library, “Viscera” term do not exist, searched with “visceral”
4. Cochrane Library, “Sweat Glands” do not exist, searched with “Sweat Gland”
5. Cochrane Library, “Chiropractic Manipulation” do not exist, searched with “Chiropractic”

7 3
10.2 Appendix 2: Specific search strategy / First study selection Search terms and Medical Subject Headings (MeSH) Database Results
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Sympathetic
Nervous System
[Excluded: 2 studies on preterm infants or children with cerebral palsy. 1
study because of medicinal uses, 2 study no spinal technique]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND
Parasympathetic Nervous System
[Excluded: 3 studies on preterm infants. 4 studies no spinal manipulation or
mobilization techniques]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Enteric
Nervous System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Autonomic
Nervous System
[Excluded: Duplicates 22 studies. 8 studies no manipulation or mobilization
technique. 2 studies on preterm infants ]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Viscera
[Excluded: none]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Visceral Pain
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Pain AND
Sympathetic Nervous System
[Excluded: 5 duplicates]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Blood Supply
[Excluded: 2 duplicates. 3 diagnostic studies. 2 studies in Chinese
language. 12 studies no manipulat ion or mobilization technique]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Vasomotor
System
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Blood Flow
Velocity
[Excluded: 3 duplicates. 1 study on medicinal uses. 4 studies no
manipulation or mobilization technique, 2 studies in Chinese]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Piloerection
MEDLINE
Relevant
MEDLINE
Relevant
MEDLINE
MEDLINE
Relevant
MEDLINE
Relevant
MEDLINE
MEDLINE
Relevant
MEDLINE
Relevant
MEDLINE
MEDLINE
Relevant
MEDLINE
14
9
8
1
0
37
5
1
1
0
5
0
21
2
0
9
0
0
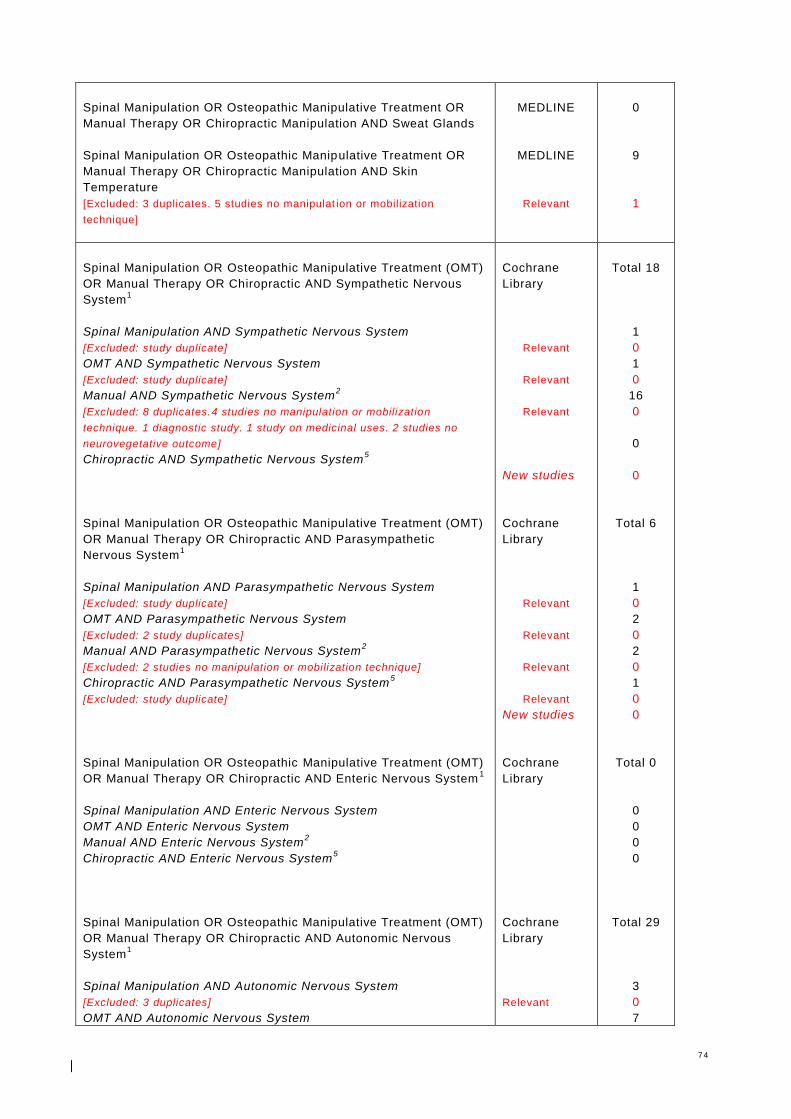
7 4
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Sweat Glands
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic Manipulation AND Skin
Temperature
[Excluded: 3 duplicates. 5 studies no manipulat ion or mobilization
technique]
MEDLINE
MEDLINE
Relevant
0
9
1
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Sympathetic Nervous
System1
Spinal Manipulation AND Sympathetic Nervous System
[Excluded: study duplicate]
OMT AND Sympathetic Nervous System
[Excluded: study duplicate]
Manual AND Sympathetic Nervous System2
[Excluded: 8 duplicates.4 studies no manipulation or mobilization
technique. 1 diagnostic study. 1 study on medicinal uses. 2 studies no
neurovegetative outcome]
Chiropractic AND Sympathetic Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Parasympathetic
Nervous System1
Spinal Manipulation AND Parasympathetic Nervous System
[Excluded: study duplicate]
OMT AND Parasympathetic Nervous System
[Excluded: 2 study duplicates]
Manual AND Parasympathetic Nervous System2
[Excluded: 2 studies no manipulation or mobilization technique]
Chiropractic AND Parasympathetic Nervous System5
[Excluded: study duplicate]
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Enteric Nervous System1
Spinal Manipulation AND Enteric Nervous System
OMT AND Enteric Nervous System
Manual AND Enteric Nervous System2
Chiropractic AND Enteric Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment (OMT)
OR Manual Therapy OR Chiropractic AND Autonomic Nervous
System1
Spinal Manipulation AND Autonomic Nervous System
[Excluded: 3 duplicates]
OMT AND Autonomic Nervous System
Cochrane
Library
Relevant
Relevant
Relevant
New studies
Cochrane
Library
Relevant
Relevant
Relevant
Relevant
New studies
Cochrane
Library
Cochrane
Library
Relevant
Total 18
1
0
1
0
16
0
0
0
Total 6
1
0
2
0
2
0
1
0
0
Total 0
0
0
0
0
Total 29
3
0
7
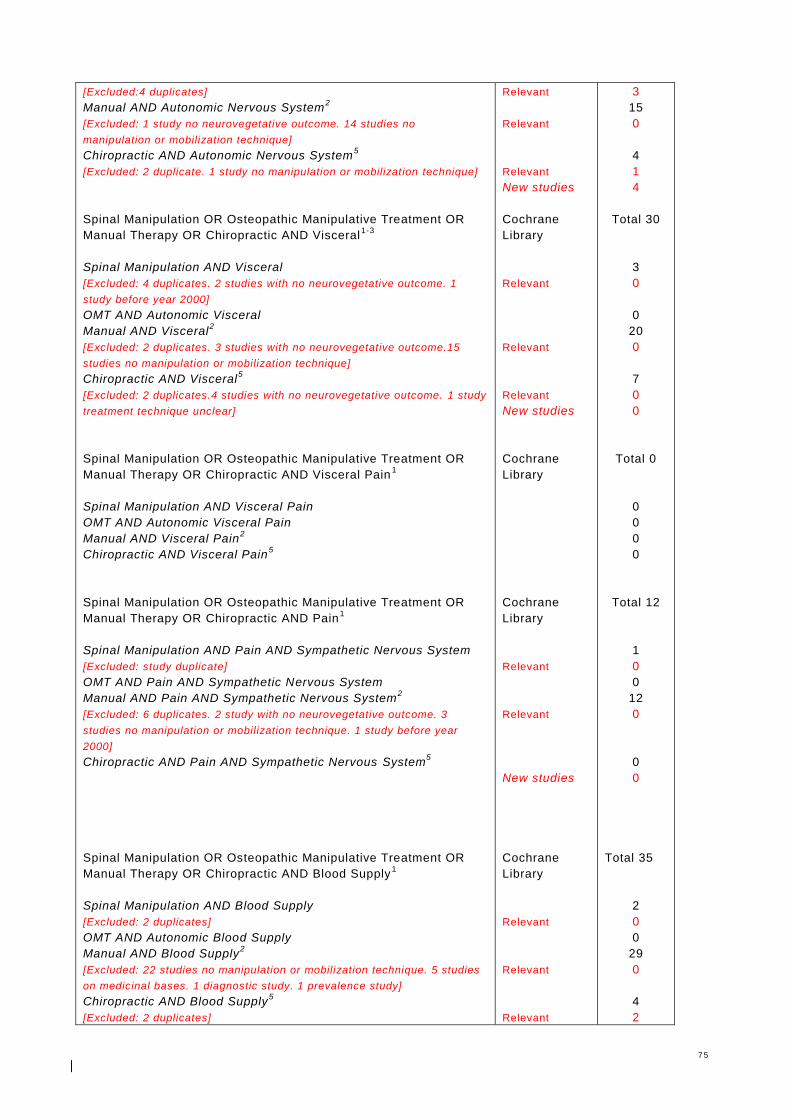
7 5
[Excluded:4 duplicates]
Manual AND Autonomic Nervous System2
[Excluded: 1 study no neurovegetative outcome. 14 studies no
manipulation or mobilization technique]
Chiropractic AND Autonomic Nervous System5
[Excluded: 2 duplicate. 1 study no manipulation or mobilization technique]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Visceral1-3
Spinal Manipulation AND Visceral
[Excluded: 4 duplicates. 2 studies with no neurovegetative outcome. 1
study before year 2000]
OMT AND Autonomic Visceral
Manual AND Visceral2
[Excluded: 2 duplicates. 3 studies with no neurovegetative outcome.15
studies no manipulation or mobilization technique]
Chiropractic AND Visceral5
[Excluded: 2 duplicates.4 studies with no neurovegetative outcome. 1 study
treatment technique unclear]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Visceral Pain1
Spinal Manipulation AND Visceral Pain
OMT AND Autonomic Visceral Pain
Manual AND Visceral Pain2
Chiropractic AND Visceral Pain5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Pain1
Spinal Manipulation AND Pain AND Sympathetic Nervous System
[Excluded: study duplicate]
OMT AND Pain AND Sympathetic Nervous System
Manual AND Pain AND Sympathetic Nervous System2
[Excluded: 6 duplicates. 2 study with no neurovegetative outcome. 3
studies no manipulation or mobilization technique. 1 study before year
2000]
Chiropractic AND Pain AND Sympathetic Nervous System5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Blood Supply1
Spinal Manipulation AND Blood Supply
[Excluded: 2 duplicates]
OMT AND Autonomic Blood Supply
Manual AND Blood Supply2
[Excluded: 22 studies no manipulation or mobilization technique. 5 studies
on medicinal bases. 1 diagnostic study. 1 prevalence study]
Chiropractic AND Blood Supply5
[Excluded: 2 duplicates]
Relevant
Relevant
Relevant
New studies
Cochrane
Library
Relevant
Relevant
Relevant
New studies
Cochrane
Library
Cochrane
Library
Relevant
Relevant
New studies
Cochrane
Library
Relevant
Relevant
Relevant
3
15
0
4
1
4
Total 30
3
0
0
20
0
7
0
0
Total 0
0
0
0
0
Total 12
1
0
0
12
0
0
0
Total 35
2
0
0
29
0
4
2

7 6
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Vasomotor System1
Spinal Manipulation AND Vasomotor System
OMT AND Vasomotor System
Manual AND Vasomotor System2
[Excluded: 1 duplicate. 1 study before year 2000]
Chiropractic AND Vasomotor System5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Blood Flow Velocity1
Spinal Manipulation AND Blood Flow Velocity
[Excluded: 2 duplicates. 1 study no manipulation or mobilization technique.
1 study no neurovegetative outcome]
OMT AND Blood Flow Velocity
Manual AND Blood Flow Velocity2
[Excluded: all studies no manipulation or mobilization technique]
Chiropractic AND Blood Flow Velocity5
[Excluded:3 duplicates]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Piloerection1
Spinal Manipulation AND Piloerection
OMT AND Piloerection
Manual AND Piloerection2
Chiropractic AND Piloerection5
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Sweat Gland1-4
Spinal Manipulation AND Sweat Gland
OMT AND Sweat Gland
Manual AND Sweat Gland2
[Excluded: 1 duplicate. 1 study no manipulation or mobilization technique]
Chiropractic AND Sweat Gland5
[Excluded no manipulation or mobilization technique]
Spinal Manipulation OR Osteopathic Manipulative Treatment OR
Manual Therapy OR Chiropractic AND Skin Temperature1
Spinal Manipulation AND Skin Temperature
[Excluded:3 duplicates. 1 study no manipulation or mobilization technique]
OMT AND Skin Temperature
Manual AND Skin Temperature2
[Excluded:2 duplicates. 12 studies no manipulation or mobilization
technique]
Chiropractic AND Skin Temperature5
[Excluded:4 duplicates]
New studies
Cochrane
Library
Relevant
New studies
Cochrane
Library
Relevant
Relevant
Relevant
New studies
Cochrane
Library
Cochrane
Library
Relevant
Relevant
New studies
Cochrane
Library
Relevant
Relevant
Relevant
New studies
2
Total 1
0
0
1
0
0
0
Total 19
4
0
0
12
0
3
0
0
Total 0
0
0
0
0
Total 3
0
0
2
0
1
0
0
Total 22
4
0
0
14
0
4
0
0
1. Cochrane Library, best specific results only 2 separate search terms inserted

7 7
2. Cochrane Library, “manual therapy” do not exist, searched with “manual”
3. Cochrane Library, “Viscera” term do not exist, searched with “visceral”
4. Cochrane Library, “Sweat Glands” do not exist, searched with “Sweat Gland”
5. Cochrane Library, “Chiropractic Manipulation” do not exist, searched with “Chiropractic”
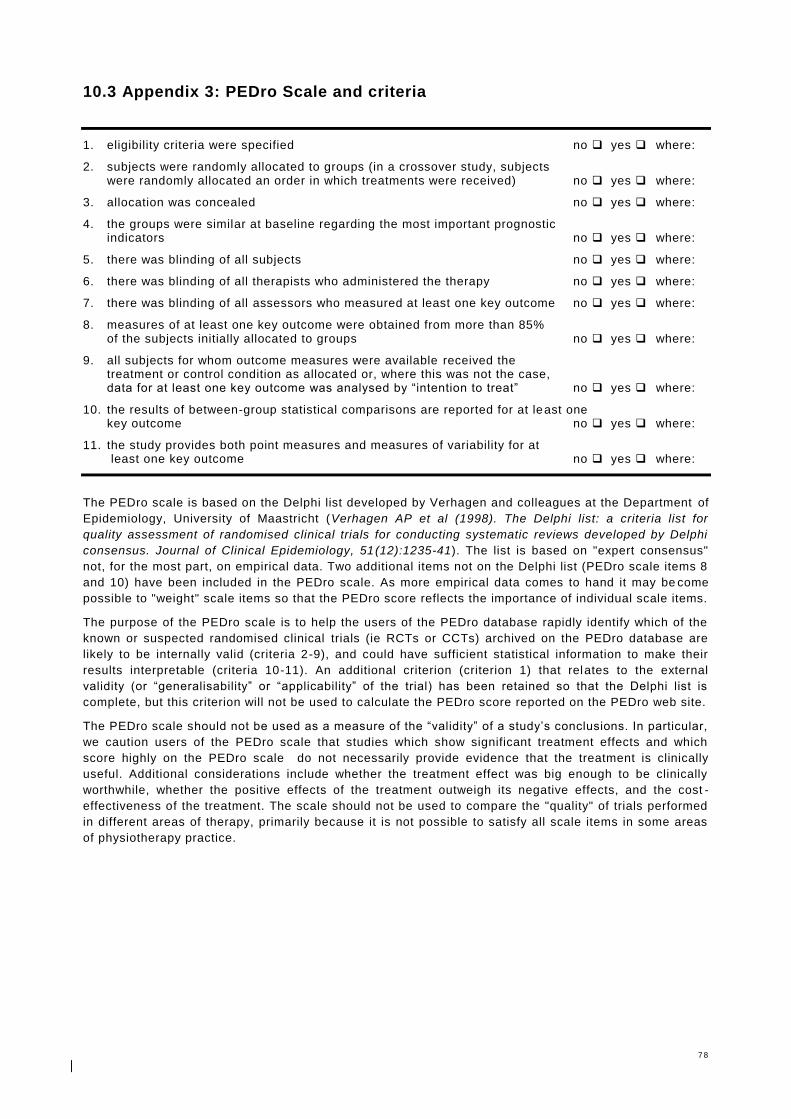
7 8
10.3 Appendix 3: PEDro Scale and criteria
1. eligibility criteria were specified no yes where:
2. subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received) no yes where:
3. allocation was concealed no yes where:
4. the groups were similar at baseline regarding the most important prognostic indicators no yes where:
5. there was blinding of all subjects no yes where:
6. there was blinding of all therapists who administered the therapy no yes where:
7. there was blinding of all assessors who measured at least one key outcome no yes where:
8. measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups no yes where:
9. all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat” no yes where:
10. the results of between-group statistical comparisons are reported for at least one key outcome no yes where:
11. the study provides both point measures and measures of variability for at least one key outcome no yes where:
The PEDro scale is based on the Delphi list developed by Verhagen and colleagues at the Department of
Epidemiology, University of Maastricht (Verhagen AP et al (1998). The Delphi list: a criteria list for
quality assessment of randomised clinical trials for conducting systematic reviews developed by Delphi
consensus. Journal of Clinical Epidemiology, 51(12):1235-41). The list is based on "expert consensus"
not, for the most part, on empirical data. Two additional items not on the Delphi list (PEDro scale items 8
and 10) have been included in the PEDro scale. As more empirical data comes to hand it may be come
possible to "weight" scale items so that the PEDro score reflects the importance of individual scale items.
The purpose of the PEDro scale is to help the users of the PEDro database rapidly identify which of the
known or suspected randomised clinical trials (ie RCTs or CCTs) archived on the PEDro database are
likely to be internally valid (criteria 2-9), and could have sufficient statistical information to make their
results interpretable (criteria 10-11). An additional criterion (criterion 1) that relates to the external
validity (or “generalisability” or “applicability” of the trial) has been retained so that the Delphi list is
complete, but this criterion will not be used to calculate the PEDro score reported on the PEDro web site.
The PEDro scale should not be used as a measure of the “validity” of a study’s conclusions. In particular,
we caution users of the PEDro scale that studies which show significant treatment effects and which
score highly on the PEDro scale do not necessarily provide evidence that the treatment is clinically
useful. Additional considerations include whether the treatment effect was big enough to be clinically
worthwhile, whether the positive effects of the treatment outweigh its negative effects, and the cost -
effectiveness of the treatment. The scale should not be used to compare the "quality" of trials performed
in different areas of therapy, primarily because it is not possible to satisfy all scale items in some areas
of physiotherapy practice.
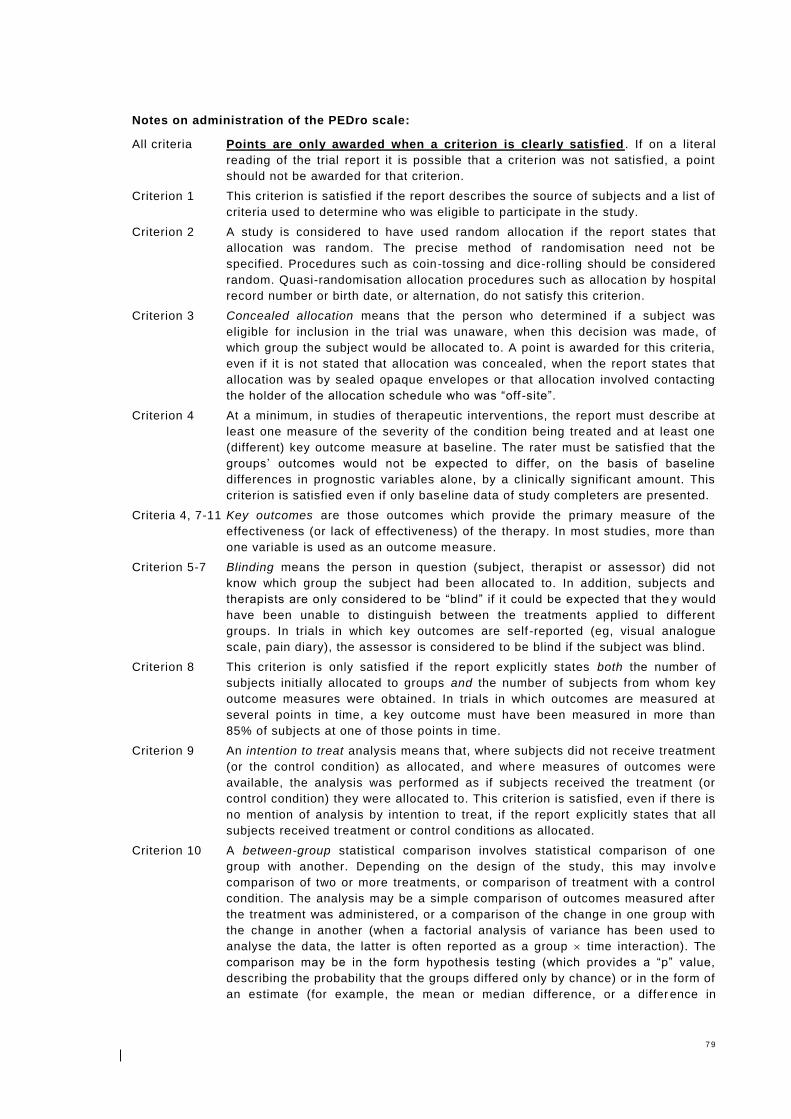
7 9
Notes on administration of the PEDro scale:
All criteria Points are only awarded when a criterion is clearly satisfied . If on a literal
reading of the trial report it is possible that a criterion was not satisfied, a point
should not be awarded for that criterion.
Criterion 1 This criterion is satisfied if the report describes the source of subjects and a list of
criteria used to determine who was eligible to participate in the study.
Criterion 2 A study is considered to have used random allocation if the report states that
allocation was random. The precise method of randomisation need not be
specified. Procedures such as coin-tossing and dice-rolling should be considered
random. Quasi-randomisation allocation procedures such as allocation by hospital
record number or birth date, or alternation, do not satisfy this criterion.
Criterion 3 Concealed allocation means that the person who determined if a subject was
eligible for inclusion in the trial was unaware, when this decision was made, of
which group the subject would be allocated to. A point is awarded for this criteria,
even if it is not stated that allocation was concealed, when the report states that
allocation was by sealed opaque envelopes or that allocation involved contacting
the holder of the allocation schedule who was “off -site”.
Criterion 4 At a minimum, in studies of therapeutic interventions, the report must describe at
least one measure of the severity of the condition being treated and at least one
(different) key outcome measure at baseline. The rater must be satisfied that the
groups’ outcomes would not be expected to differ, on the basis of baseline
differences in prognostic variables alone, by a clinically significant amount. This
criterion is satisfied even if only baseline data of study completers are presented.
Criteria 4, 7-11 Key outcomes are those outcomes which provide the primary measure of the
effectiveness (or lack of effectiveness) of the therapy. In most studies, more than
one variable is used as an outcome measure.
Criterion 5-7 Blinding means the person in question (subject, therapist or assessor) did not
know which group the subject had been allocated to. In addition, subjects and
therapists are only considered to be “blind” if it could be expected that the y would
have been unable to distinguish between the treatments applied to different
groups. In trials in which key outcomes are self -reported (eg, visual analogue
scale, pain diary), the assessor is considered to be blind if the subject was blind.
Criterion 8 This criterion is only satisfied if the report explicitly states both the number of
subjects initially allocated to groups and the number of subjects from whom key
outcome measures were obtained. In trials in which outcomes are measured at
several points in time, a key outcome must have been measured in more than
85% of subjects at one of those points in time.
Criterion 9 An intention to treat analysis means that, where subjects did not receive treatment
(or the control condition) as allocated, and where measures of outcomes were
available, the analysis was performed as if subjects received the treatment (or
control condition) they were allocated to. This criterion is satisfied, even if there is
no mention of analysis by intention to treat, if the report explicitly states that all
subjects received treatment or control conditions as allocated.
Criterion 10 A between-group statistical comparison involves statistical comparison of one
group with another. Depending on the design of the study, this may involv e
comparison of two or more treatments, or comparison of treatment with a control
condition. The analysis may be a simple comparison of outcomes measured after
the treatment was administered, or a comparison of the change in one group with
the change in another (when a factorial analysis of variance has been used to
analyse the data, the latter is often reported as a group time interaction). The
comparison may be in the form hypothesis testing (which provides a “p” value,
describing the probability that the groups differed only by chance) or in the form of
an estimate (for example, the mean or median difference, or a differ ence in

8 0
proportions, or number needed to treat, or a relative risk or hazard ratio) and its
confidence interval.
Criterion 11 A point measure is a measure of the size of the treatment effect. The treatment
effect may be described as a difference in group outcomes, or as the outcome in
(each of) all groups. Measures of variability include standard deviations, standard
errors, confidence intervals, interquartile ranges (or other quantile ranges), and
ranges. Point measures and/or measures of variability may be provided
graphically (for example, SDs may be given as error bars in a Figure) as long as it
is clear what is being graphed (for example, as long as it is clear whether error
bars represent SDs or SEs). Where outcomes are categorical, this criterion is
considered to have been met if the number of subjects in each category is given
for each group.
8 1
Curriculum Vitae
K.H. (Koen) Groot Zwaaftink D.O.-MRO
Personal Details
Address: Pathmossingel 49 7513 CB Enschede The Netherlands
Phone: +31641557330 Date of birth: 13 May 1983 Place of birth: Oldenzaal
Nationality: Dutch E-mail: [email protected]
Present Position
Osteopath in a privite practise, OsteoCura - Albergen
Teacher International Academy of Osteopathy - Clinical Neurology and Cranial Nerves
Education
2013-present Osteopathy MSc. - University of Applied Sciences, Innsbruck
2004-2009 Osteopathy D.O. - International Academy of Osteopathy, Gent
2005-2006 Ultrasound of the Musculoskeletal System - Fysus Communications, Delft
2000-2004 Physiotherapy Bac.- Saxion University of Applied Sciences, Enschede
Courses
2015 Das vegetative Nervensystem – Osteopathie Schule Deutschland, Hamburg
2013 Shoulder Plus – Saxion University of Applied Sciences, Enschede
2013 Shoulder Basic – Saxion University of Applied Sciences, Enschede
2012 Mobilisation of the Nervous System – Paramedic Institute, Papendal
2011 Manipulations-Functional Techniques of the Spine – Panta Rhei, Hoeven
2011 Visceral Manipulations – Panta Rhei, Hoeven
2011 Kneeproblems - Saxion University of Applied Sciences, Enschede
2010 Musculoskeletal Ultrasound – Specialists Course, Amersfoort
2008 Musculoskeletal Ultrasound – Specialists Course, Amersfoort
2007 Musculoskeletal Ultrasound – Specialists Course Shoulder, Amersfoort
2007 Medical Taping – Fysiotape Courses, Alphen aan de Rijn
2004 Functional Taping - Saxion University of Applied Sciences, Enschede
Professional Experience
2004-2009 Physical therapist in a private practice
2009-present Osteopath in a private practice
2009-present Teacher International Academy of Osteopathy
Membership of Professional Association
Dutch Association for Osteopathy (NVO)
Dutch Register of Osteopathy (NRO)
Language Skills
Dutch, English and German
8 2
Declaration of originality
o
Affidavit concerning
Master's thesis
I hereby deciare that the present paper is entirely my own work and that I have not used any
sourees and/or resources other than those specified in the bibliography. AII quotes taken literally or
analogously from any works either published or as yet unpublished or taken from the Internet are
indicated as such in accordance with the rules of academie writing.
The present work has never been submitted as part of another examination procedure, in either this or a similar form, and neither have any excerpts from it ever been used in such a procedur
Date St
fh gesundheit
wir bilden die zukunft
21-06-2016
fhg - Zentrum für Gesundheitsberufe Tirol GmbH. lnnrain 98. 6020 Innsbruck, Tel. +43(0)50/8648-4700. Fax -674700. [email protected]. www.fhg-tirol.ac.at
FN 224932 h, VAT Reg. No. ATU54638904. HYPO TIROL BANK AG. Account No. 54011035606. Sort Code 57000. IBAN AT 605700054011 035606. BIC HYPTAT22
Commercial Register Court. District and Commercial Court of Innsbruck







![Generelle EU droneregler - Databaseret Service ......Generelle EU droneregler. [1] Generelle EU droneregler. De nye EU-regler skal ikke forstås sådan, at der kommer ens regler i](https://img.pdfslide.net/doc/110x75/61117030bfcdf25ad9624ec4/generelle-eu-droneregler-databaseret-service-generelle-eu-droneregler.jpg)