Embed Size (px)
Citation preview

NEVADA STRATEGIC HEALTH PLAN
Burns & Associates, Inc.
Under Contract with EP&P Consulting, Inc.
May 5, 2006
EXHIBIT C-1 Health Care Document consists of 146 pages Entire document provided. Due to size limitations, pages _________ provided.
A copy of the complete document is available through the Research Library (775/684-6827 or e-mail [email protected]). Meeting Date: June 12, 2006

Burns & Associates, Inc. May 5, 2006
TABLE OF CONTENTS I. Executive Summary II. Policy Brief on Focus Group Recommendation: Medicaid and SCHIP
Coverage III. Policy Brief on Focus Group Recommendation: Behavioral Health IV. Policy Brief on Focus Group Recommendation: Health Care Professional
Education V. Policy Brief on Focus Group Recommendation: Small Employer Health
Insurance and the Safety Net VI. Policy Brief on Focus Group Recommendation: Planning VII. Policy Brief on Focus Group Recommendation: Prevention and Wellness Technical Appendix Appendix 1: 2006 Federal Poverty Levels
Appendix 2: Summary of Nevada’s Uninsured Appendix 3: Summary of Stakeholder Focus Groups Appendix 4: Environmental Scan
Selected Cost Estimates Appendix Appendix 1: Medicaid Expansion Model
Appendix 2: Cost of Adding the “210” Coverage Group Appendix 3: Direct Subsidy Model Appendix 4: Detail of Cost Estimates Across All Policy Briefs

Burns & Associates, Inc. I-1 May 5, 2006
Chapter I 1
Executive Summary 2
Materials for Participants 3
Summit on a Nevada State Health Plan 4 5 6 This document is prepared as an Executive Summary of the six Policy Briefs and two 7 Appendices prepared for participants of the Legislative Committee on Health Care’s 8 Summit on a Nevada State Health Plan. 9 10 The Legislative Committee on Health Care was charged with the development of such a 11 Plan by A. B. 342 (Chapter 418, Statutes of Nevada 2005). The Committee adopted a 12 work plan for the development of the Plan tha t has the participation of three separate 13 groups: stakeholders, consultants and the Committee itself. The roles and responsibilities 14 of the three groups in the Plan development are: 15 16
§ The Stakeholders. Approximately 120 individual stakeholders were invited to 17 participate in six focus groups that were held in February and March of 2006. 18 Each focus group addressed one of six areas of the health care system in 19 Nevada, i.e., health care facilities, health care professionals, medical coverage, 20 pharmaceutical coverage, health professional education and the public health 21 system. During the focus group, the participants engaged in a Strengths, 22 Weaknesses, Opportunity and Threats (SWOT) analysis and developed a list 23 of recommendations. The stakeholders will participate in the Summit and 24 seek to achieve consensus on a number of strategies developed from their 25 recommendations. 26
27 § The Consultants. Burns & Associates, Inc. (B&A) was retained through a 28
subcontract with EP&P Consulting, Inc. to assist the Committee in developing 29 the Plan. B&A has assisted the Committee in structuring requested testimony 30 before the Committee, facilitated the focus group process, prepared the six 31 Policy Briefs for the Summit, will conduct the Summit, and assist the 32 Committee in preparing the final Plan 33
34 § The Committee. The Committee is providing overall guidance for the 35
development of the Plan, assisted in identifying stakeholders to participate in 36 the process, received testimony on the six areas of the Nevada health care 37 system that the focus groups were organized around, participated in the focus 38 group sessions, and will ultimately compile the Plan. 39
40 With respect to the documents prepared for the Summit, the Technical Appendix contains 41 an Environmental Scan, a summary of the focus groups’ SWOT analysis and 42 recommendations, a summary of the uninsured in Nevada, and a listing of the Federal 43 Poverty Levels. 44 45

Burns & Associates, Inc. I-2 May 5, 2006
The conclusions that can be drawn from the Environmental Scan document are: 1 2
§ Nevada’s population has been and will continue to grow rapidly and that over 3 time, the 65+ age category will comprise a larger percentage of a larger 4 population. 5
6 § The health status of Nevada is ranked 37th in a ranking performed by the 7
UnintedHealth Foundation, below average but not in an extreme way. Poor 8 indicators are noted in child immunizations, prenatal care and the size of the 9 uninsured population in the state. 10
11 § There is an overall shortage of health care professionals in the state. 12
13 § There is a large percentage of the population without health insurance, ranking 14
the state 4th among the states with a high level of uninsurance. 15 16
§ A low percentage of the state’s population is covered by Medicaid compared 17 to the rest of the nation. 18
19 A summary of the SWOT analysis and recommendations from the focus groups is also 20 contained in the Technical Appendix. There were approximately 30 “high scoring” 21 strategies from the groups. These “high scoring” strategies served as the basis for 22 developing the recommendations outlined in the six Policy Briefs prepared for the 23 Summit. 24 25 The Summary of Nevada’s Uninsured presents a profile of the state’s uninsured 26 population as derived from the Current Population Survey. The analysis examines the 27 uninsured by age group, working status and citizenship among other factors. In short, 28 Nevada’s 426,000 uninsured can be divided into: 29 30
§ 110,000 children and 314,000 adults less than 65 31 § 72,000 children and 160,000 adults below 200% of the federal poverty level 32 § Of the adults below 200% of the poverty level, approximately 94,000 are 33
working 34 35 After completion of the focus group phase of the project, the recommendations from the 36 six groups were aggregated into six different topic areas. The six areas (and the six 37 Policy Briefs) are: 38 39
1. Medicaid and SCHIP Coverage 40 2. Behavioral Health 41 3. Health Care Professional Education 42 4. Small Employer Health Insurance and the Safety Net 43 5. Planning 44 6. Prevention and Wellness 45
46

Burns & Associates, Inc. I-3 May 5, 2006
For each of the six areas, a Recommendation Statement was developed. The 1 recommendation statements contained in the Policy Briefs are presented below. 2 3
Nevada will: 4 5
Expand program eligibility, enrollment and service coverage under the State’s 6 Medicaid and SCHIP programs. 7
8 Increase access to and funding for an appropriately designed mental health and 9 substance abuse program for Nevadans requiring these services. 10
11 Improve and expand its capacity to provide a health care professional education 12 continuum to increase the number of licensed health care professionals in the 13 state. 14
15 Develop mechanisms to provide coverage for the small employer market and for 16 individuals who are uninsurable. In addition, the State will improve access to 17 services for both the insured and uninsured by supporting and expanding the 18 safety net provider network. 19
20 Develop positive proactive plans for addressing its health care system challenges 21 with formalized planning bodies that coordinate and disseminate information on 22 health care policy, quality, community needs, workforce issues, and health 23 information technology and information exchange. 24
25 Expand and initiate programs that will improve the overall health status of its 26 citizens by focusing on prevention and wellness. 27
28 Each Policy Brief presents an overview of the topic area and then presents the strategies 29 that were developed for consideration of the Summit participants. The proposed 30 strategies are then linked to the recommendations of the focus groups. 31 32 For each strategy, background material is presented, the strategy summarized, and in 33 most instances, a high level or “placeholder” estimate of cost is provided. For three 34 strategies – expanding coverage groups in Medicaid, providing for an optional eligibility 35 category and small employer insurance subsidies – the Selected Cost Estimates Appendix 36 contains additional detail on the assumptions and calculations of costs. Additionally, a 37 fourth appendix in this section details the cost estimates of all of the strategies across all 38 of the policy briefs. 39 40 A summarized list of the strategies proposed for consideration of the Summit participants 41 is presented below. 42 43 In order to achieve improved coverage under Nevada’s Medicaid and Check Up 44 programs, the following strategies were developed: 45 46

Burns & Associates, Inc. I-4 May 5, 2006
1. Raise the income qualification level for parents in increments based on the 1 federal poverty level (FPL) to the following: a) from +/- 26% to 50% of the 2 FPL, b) 50% to 75% of the FPL, and c) 75% to 100% of the FPL. 3
4 2. Expand and/or expedite the process by which individuals who qualify for 5
Supplemental Security Income (SSI) are determined eligible for Medicaid. 6 7 3. Increase enrollment in Medicaid and Check Up through a) eliminating 8
requirement to pay premiums b) continuing and expanding outreach efforts, 9 and c) streamlining the Medicaid and Check Up eligibility processes. 10
11 4. Increase reimbursement to providers by increasing those specific rates that 12
have been identified by DHCFP. 13 14 5. Enhance coverage under the Medicaid home and community-based waivers 15
by: a) addressing workforce shortages in the area of case management, b) 16 adding additional covered services to waivers and c) reducing waitlists 17 through increasing the number of waiver slots. 18
19 6. Evaluate opportunities under the new Deficit Reduction Act for Nevada’s 20
Medicaid program as it relates to the delivery of long-term care services. 21 22 7. Explore the benefits of a long-term care system redesign, with a goal of a 23
coordinated and integrated service delivery model with a focus on consumer-24 directed, home and community-based care. 25
26 In order to increase access to and funding for an appropriately designed mental health and 27 substance abuse (i.e., behavioral health) program for Nevadans, the following strategies 28 were developed: 29 30
1. Decrease number of persons with behavioral health conditions who 31 inappropriately utilize the Emergency Departments by a) increasing number 32 of available psychiatric beds, b) expanding the crisis support system, or c) 33 expanding on-going services. 34
35 2. Conduct a review of the current low level of Medicaid reimbursement in the 36
DMHDS mental health program. 37 38 3. Enhance home and community-based services for Medicaid eligible persons 39
with SMI by utilizing a) the new Medicaid State Plan option made available 40 through the Deficit Reduction Act of 2006 or b) the 1915(c) home and 41 community-based waiver option. 42
43 4. Enhance home and community-based services for Medicaid eligible children 44
and adolescents with SED with a new Medicaid demonstration grant 45

Burns & Associates, Inc. I-5 May 5, 2006
established under the Deficit Reduction Act or the 1915(c) home and 1 community-based waiver option. 2
3 5. Establish a long term target funding level for behavioral health services in 4
Nevada. 5 6 6. Restructure and unify the behavioral health system in Nevada. 7 8
To increase the number of licensed health care professionals in the state through an 9 expansion of professional health care education, the following strategies were 10 developed: 11 12
1. Expand UNSOM and the Graduate Medical Education (GME) program by: 13 a. Increasing core faculty 14 b. Expanding the GME program 15 c. Increasing the enrollment in the School of Medicine 16
17 2. Expand public nursing school programs by: 18
a. Increasing faculty salaries 19 b. Doubling the enrollment at the public nursing schools 20 c. Funding necessary capital expenditures 21 d. Funding preceptor and clinical support 22
23 3. Start a School of Pharmacy and Pharmaceutical Services 24
25 4. Maximize Medicaid funding for GME 26
27 5. Expand scholarship opportunities to fund students seeking graduate and 28
undergraduate degrees in the health care professions 29 30 6. Expand state funding for the Area Health Education Centers (AHECs) to 31
support the education of health care professionals 32 33 In order to improve affordability and availability of health insurance in the small group 34 market, provide access to coverage for the uninsurable, and to increase access to 35 health care services by enhancing the safety net, the following strategies were developed: 36 37
1. Provide employers information on small group rating practices to allow them 38 to make informed decisions regarding health care coverage. 39
40 2. Create a standardized product that insurance companies will offer to small 41
employers that: 42 43
a) standardizes the benefit package offered in the small group market, or 44 b) both standardizes the benefit package and makes the package more 45
affordable, or 46

Burns & Associates, Inc. I-6 May 5, 2006
c) both standardizes the benefit package and limits premiums that can be 1 charged. 2 3
3. Provide subsidies for insurance either to the population at large or to small 4 employers. The subsidies can be through either: 5
6 a) direct premium subsidies or 7 b) reinsurance for a standardized product. 8
9 4. Allow small employers to buy into the state employee insurance program. 10 11 5. Establish a high-risk pool for the uninsurable. 12 13 6. Establish a universal coverage program for Nevada. 14 15 7. Improve access to health care services for the both the uninsured and the 16
insured through expansion of safety net provider networks. 17 18 8. Foster local community efforts to offer services to the uninsured through 19
leadership and planning grants. 20 21 9. Increase funding for Senior Rx and Disability Rx programs. 22
In order to plan for the current and future health care needs of Nevadans, and to improve 23 effectiveness of the health care system, the following strategies for health care planning 24 were developed: 25
1. An Office of Health Planning will be created to oversee health care planning 26 and policy development within Nevada. The Office of Health Planning will 27 be comprised of four divisions: 28
29 § Division of Analysis and Policy 30 § Division of Quality 31 § Division of Community Assessment 32 § Division of Facilities Planning 33
34 2. An Office of Healthcare Workforce Development will be created to oversee 35
professional workforce planning and policy development in Nevada. The 36 Office will be composed of three divisions: 37
38 § Division of Analysis and Planning 39 § Division of Special Projects on Regulatory Affairs 40 § Division of Incentive Administration 41
42

Burns & Associates, Inc. I-7 May 5, 2006
3. To ensure that Nevada develops health information technology and 1 coordinates the development of health information exchange, the following 2 strategies were developed: 3
4 § A time- limited statewide Steering Committee will be convened and 5 supported by the State for the purpose of developing a high level plan for 6 e-Health 7 8 § A statewide governance committee will be created and funded to 9 implement the steering committee’s high level plan 10 11 § Subsidies will be provided for the adoption and use of HIT and HIE 12 13 § Legislation will be enacted to clarify and protect consumer privacy 14
15 In order to improve the overall health of Nevadans, the following strategies related to 16 prevention and wellness were developed: 17
18 1. Improve Early Childhood Immunization 19 20 2. Expand Prenatal Care Services 21 22 3. Expand the Oral Health Care Program 23 24 4. Reduce Exposure to Second-hand Smoke 25 26 5. Invest in Wellness Programs to Prevent Chronic Disease 27
28 As noted above, the Policy Brief for each topic area further develops the potential 29 strategies outlined above. The following Table presents a summary of the high level and 30 “placeholder estimates” that were prepared for the potential strategies. While not all 31 strategies had cost estimates developed, the Summary below indicates that the strategies 32 developed for consideration of the Summit participants can have a substantial impact on 33 state finances. 34 35 All costs in the Summary are expressed in state funds. 36

Burns & Associates, Inc. I-8 May 5, 2006
1 Summary
Estimated Costs to Implement the Recommendations in the Strategic Health Plan (in millions) (All costs are reflected in State-share dollars.)
POLICY BRIEF SFY 08 SFY 09 SFY 10 SFY 11 SFY 12
Medicaid and SCHIP Coverage $56.4 $71.0 $92.4 $97.0 $101.8
Behavioral Health $29.4 $32.5 $50.3 $68.1 $86.0
Professional Education $53.6 $41.4 $69.9 $34.1 $46.9 Operating $4.4 $23.1 $32.4 $34.1 $46.9 Capital $49.3 $18.4 $37.4 $0.0 $0.0
Small Employer and Safety Net $11.1 $29.3 $30.2 $31.1 $32.1
Planning $5.1 $9.1 $9.3 $9.5 $9.7
Prevention and Wellness $7.3 $6.1 $6.1 $6.1 $6.1
TOTAL $162.9 $189.4 $258.1 $245.9 $282.6
Percent of Total Estimated Costs
POLICY BRIEF SFY 08 SFY 09 SFY 10 SFY 11 SFY 12
Medicaid and SCHIP Coverage 35% 37% 36% 39% 36%
Behavioral Health 18% 17% 19% 28% 30%
Professional Education 33% 22% 27% 14% 17% Operating 3% 12% 13% 14% 17% Capital 30% 10% 15% 0% 0%
Small Employer and Safety Net 7% 15% 12% 13% 11%
Planning 3% 5% 4% 4% 3%
Prevention and Wellness 4% 3% 2% 2% 2%
TOTAL 100% 100% 100% 100% 100% Note: The sum of the individual percentages may not equal 100% due to differences in rounding. 2 3 A more detailed summary is contained in the Selected Cost Estimates Appendix. 4

Burns & Associates, Inc. II-1 May 5, 2006
Chapter II 1
Policy Brief on Focus Group Recommendations 2
Medicaid and SCHIP Coverage 3 4 5
I. RECOMMENDATION STATEMENT 6 7
Nevada will expand program eligibility, enrollment and service coverage under 8 the State’s Medicaid and SCHIP programs. 9 10
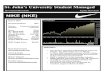
II. OVERVIEW 11 12 The Department of Health and Human Services (DHHS), Division of Health Care 13 Financing and Policy (DHCFP) is responsible for administering the State’s two federal 14 health coverage programs for low-income Nevadans: Medicaid, covering low-income 15 families and aged, blind and disabled individuals; and SCHIP (known as Nevada Check 16 Up), covering low-income uninsured children who are not eligible for Medicaid. 17 18 Expenditures in the Medicaid program more than doubled from SFY 00 – SFY 05 while 19 average enrollment has increased 77% to an enrollment of 176,418. Enrollment in 20 Nevada Check Up (referred to as Check Up in the rest of the document) averaged just 21 over 25,000 children in SFY 04, and the most recent enrollment in the program is 27,564. 22 23
Nevada Medicaid
Nevada Check Up
Enrollment
Average Enrollment SFY 05 176,418 26,750Average Enrollment SFY 04 172,779 25,025Percent Growth SFY 04-05 2.1% 6.9%Average Enrollment SFY 00 99,411 8,079Percent Growth SFY 00-05 77% 231%Expenditures
SFY 2005 Total $1,177,397,578 $38,441,266SFY 2004 Total $971,230,000 $30,157,920Percent Growth SFY 04-05 21% 27%SFY 2000 Total $489,379,242 $13,774,909Percent Growth SFY 00-05 140% 179% Total SFY 05 Per Member Per Month Costs $556.16 $119.75
24 Eligibility for Nevada’s Medicaid program is relatively restrictive compared to other 25 states. Nevada has among the lowest qualifying income levels and only a limited number 26 of optional eligibility categories. Check Up, which covers children up to 200% of the 27 Federal Poverty Level (FPL), is also restrictive in that to be eligible, children must not 28

Burns & Associates, Inc. II-2 May 5, 2006
have had health insurance within the last six months (Nevada is one of 15 states with the 1 longest allowable “going bare” period) and premiums are charged, though at nominal 2 levels. 3 4 These limitations have contributed to low public sector coverage and a high proportion of 5 uninsured. For example, 7.1% of Nevadans were covered by Medicaid in 2003-04, with 6 Nevada being ranked 50th nationally (out of 51) in terms of percent of population covered 7 under Medicaid. Further, 18.7% of Nevadans were uninsured, with Nevada being ranked 8 7th highest among states in terms of percentage of the population uninsured. 9 10 For both Medicaid and Check Up, the State delivers services through both a fee-for-11 service and managed care models. Services are delivered primarily on a fee-for-service 12 basis for enrollees who are blind, aged or disabled and/or reside in a rural/frontier area. 13 In Clark and Washoe counties, enrollment in one of the two managed care plans (Nevada 14 Care, Inc. or Health Plan of Nevada) is mandatory for Temporary Assistance for Needy 15 Families (TANF), Children Health Insurance Program (CHAP) and Check Up 16 populations. 17 18 The managed care plans are required to provide medical and dental care (dental care is 19 not yet implemented in Washoe County) as well as limited behavioral health and short-20 term nursing home services. Other services for these recipients, such as long-term care 21 services and more intensive behavioral health services, are not the responsibility of the 22 managed care plans and are provided on a fee-for-service basis. 23 24 In addition to the focus groups strongly recommending enhancements to the current 25 Nevada Medicaid and SCHIP programs, similar recommendations have been included in 26 strategic plans developed by other Nevada stakeholder groups: 27 28
Washoe County Access to Health Care Network – Five-Year Strategic Plan 29 (2003-2008) included recommendations related to expanding eligibility 30 criteria, improving reimbursement structures, and conducting outreach and a 31 resource awareness campaign. 32
33 State of Nevada Department of Human Resources - Strategic Plan for Rural 34
Health Care included recommendations related to expanding Check Up to 35 parents of eligible children, streamlining the Medicaid and Check Up 36 eligibility criteria, establishing an on-line application, considering Medicaid 37 reimbursement enhancements for rural providers, and providing payment for 38 services delivered via telemedicine. 39
40 State of Nevada Department of Human Resources - Strategic Plan for People 41
with Disabilities included numerous recommendations related to Medicaid 42 and delivery of services to people with disabilities (e.g., additional home and 43 community-based waiver services). 44
45

Burns & Associates, Inc. II-3 May 5, 2006
State of Nevada Department of Human Resources - Strategic Plan for Senior 1 Services included recommendations related to funding and implementing a 2 single point of entry system for information, referral, assistance, care planning 3 and management. 4
5 III. STRATEGIES 6 7 In order to achieve improved coverage under Nevada’s Medicaid and Check Up 8 programs, the following strategies were developed from recommendations identified by 9 stakeholders in the focus group process: 10 11
1. Raise the income qualification level for parents in increments based on the 12 federal poverty level (FPL) to the following: a) from +/- 26% to 50% of the 13 FPL, b) 50% to 75% of the FPL, and c) 75% to 100% of the FPL. 14
15 2. Expand and/or expedite the process by which individuals who qualify for 16
Supplemental Security Income (SSI) are determined eligible for Medicaid. 17 18
3. Increase enrollment in Medicaid and Check Up through a) eliminating 19 requirement to pay premiums b) continuing and expanding outreach efforts, 20 and c) streamlining the Medicaid and Check Up eligibility processes. 21
22 4. Increase reimbursement to providers by increasing those specific rates that 23
have been identified by DHCFP. 24 25
5. Enhance coverage under the Medicaid home and community-based waivers 26 by: a) addressing workforce shortages in the area of case management, b) 27 adding additional covered services to waivers and c) reducing waitlists 28 through increasing the number of waiver slots. 29
30 6. Evaluate opportunities under the new Deficit Reduction Act for Nevada’s 31
Medicaid program as it relates to the delivery of long-term care services. 32 33
7. Explore the benefits of a long-term care system redesign, with a goal of a 34 coordinated and integrated service delivery model with a focus on consumer-35 directed, home and community-based care. 36
37 These strategies were developed from the following “high scoring” recommendations 38 from the focus groups that addressed Medicaid and Check Up: 39 40
1. Implement presumptive eligibility under Nevada’s Medicaid program 41 including individuals applying for coverage under Supplemental Security 42 Income. (Health Facilities) 43
44 2. Expand eligibility and service coverage under Nevada’s Medicaid program. 45
(Health Facilities) (Public Health) 46

Burns & Associates, Inc. II-4 May 5, 2006
3. Through a collaborative effort increase outreach to Nevadans who are eligible 1 for Medicaid or SCHIP but not enrolled, as well as improve the eligibility 2 process itself. (Medical Coverage) 3
4 4. Adequately fund Medicaid (including mental health) to ensure that provider 5
compensation that will result in an adequate number of health care 6 professionals who are willing to accept Medicaid. (Health Care Professionals) 7
8 The last three strategies included in this policy brief (relating to long term care) were not 9 specifically recommended by the focus groups, but do reflect a broad spectrum of 10 comments made in several of the groups. 11 12 The balance of this Policy Brief presents and discusses each of the recommendations 13 listed above. 14 15 16 1. Raise the Income Qualification Levels for Medicaid 17 18 Income qualification levels for Nevada’s Medicaid program are low for both children and 19 adult populations as exemplified by: 20 21
For parents, income eligibility is set at approximately 26% of the FPL for a 22 family of three (i.e., $4,316 annual income), ranking Nevada 41st among the 23 states in terms of its Medicaid income eligibility level for parents. 24
25 Coverage under Medicaid is set at the lowest levels allowed under Medicaid – 26
at 133% of the FPL for children 0 to 5 years and at 100% of the FPL for 27 children 6 to 19 years. While children can be covered up to 200% of the FPL 28 under Check Up, they have to pay a premium. 29
30 Nevada is one of nine states that has adopted the lowest allowable income 31
eligibility level for pregnant woman (i.e., 133% of the FPL), contributing to 32 Nevada having one of the lowest percentage of births financed by Medicaid 33 (i.e., 21%, ranking Nevada 47th nationally). 34
35 Nevada has recently taken some steps to increase coverage under Medicaid. In 2005, 36 Nevada eliminated its asset test for pregnant women and children and implemented a 37 Medicaid buy-in/Ticket to Work Program (current caseload is 19 individuals). More 38 recently, the State submitted a Health Insurance Flexibility and Assurance (HIFA) waiver 39 which proposes to expand Medicaid eligibility in three ways: 40 41
Expanding coverage up to 185% of the FPL for pregnant women, although the 42 expansion is capped at 1,350 women 43
44 Providing for premium subsidies for employer sponsored insurance for a 45
limited number of parents (5,500) up to 200% of the FPL 46

Burns & Associates, Inc. II-5 May 5, 2006
Providing a limited amount of funding to expand coverage for parents with 1 catastrophic health care incidents up to 150% of the FPL 2
3 The proposed strategy for consideration of the Summit participants is to expand 4 eligibility for parents of Medicaid children below 100% of the FPL. Parents were 5 selected for this expansion because under federal Medicaid rules, parents can be added as 6 a coverage groups through a State Plan Amendment. With a State Plan Amendment, the 7 State does not have to demonstrate budget neutrality, but it does have to offer the 8 expansion statewide as an entitlement. 9 10 Because of the entitlement nature of such an expansion, the Summit participants may 11 want to consider expanding eligibility in three steps: 12 13
An expansion from current levels of approximately 26% of the FPL ($5,200 in 14 annual income for a family of four) to 50% of the FPL ($10,000 in annual 15 income for a family of four), followed by 16
17 An expansion from 50% of the FPL to 75% of the FPL ($15,000 in annual 18
income for a family of four), followed by 19 20
An expansion from 75% of the FPL to 100% of the FPL ($20,000 in annual 21 income for a family of four). 22
23 By utilizing this “stair step” approach to eligibility expansion, the State can validate the 24 cost estimates associated with the expansion. 25 26 Cost Estimate 27 28 The estimated annual cost of medical benefits for the eligibility expansion to parents with 29 incomes up to 100% of the FPL is $64.8 million (total funds). The state funds 30 requirement is $29.8 million annually. This expansion is estimated to bring an additional 31 22,000 individuals into the State’s Medicaid program. 32 33 This estimate is based on Current Population Survey (CPS) data, a national database that 34 estimates the population and its health insurance status. Assuming that the CPS 35 population estimates are correct, the $64 million estimate is considered a maximum 36 amount because it allows for all adults with dependent children with incomes up to 100% 37 of the FPL to be covered by Medicaid, regardless of current insurance status. This cost 38 estimate also assumes that every eligible adult will enroll immediately into the program 39 once it is offered to them. 40 41 If the eligibility expansion were to be implemented in the stair step fashion discussed 42 above, assuming a 100% take-up rate the medical costs are estimated to be: 43 44
Cost to implement up to 50% of the FPL: $21.8 million total, $10.0 million 45 state 46

Burns & Associates, Inc. II-6 May 5, 2006
Cumulative cost to implement up to 75% of the FPL: $37.5 million total, 1 $17.3 million state 2
3 Cumulative cost to implement up to 100% of the FPL: $64.8 million total, 4
$29.8 million state 5 6 The above estimates assume 100% participation in the program by eligible parents. It is 7 much more likely that only a fraction of those eligible would actually enroll. A Kaiser 8 Commission study that explored eligibility and enrollment among low-income uninsured 9 adults eligible for Medicaid found that 57% percent of all eligible parents actually 10 enrolled. This assumption was used to develop a more realistic cost estimate than the 11 maximum cost estimate presented above. 12 13 An assumption was also made for the individuals in this income range that are already 14 insured. The estimate assumes that only 30% of these insured individuals would drop 15 private insurance and switch to Medicaid. 16 17 If these assumptions are used, the total cost of the expansion would drop to $31.4 million 18 annually ($14.5 million in state funds). An eligibility expansion using the reduced take 19 up rate assumption is estimated to bring only an additional 10,800 individuals into the 20 State’s Medicaid program. 21 22 When these lower take up rates are assumed, a modified stair step cost estimate is: 23 24
Cost to implement up to 50% of the FPL: $11.4 million total, $5.2 million 25 state 26
27 Cumulative cost to implement up to 75% of the FPL: $18.8 million total, $8.7 28
million state 29 30 Cumulative cost to implement up to 100% of the FPL: $31.4 million total, 31
$14.5 million state 32 33 It should be noted that the cost estimates presented above do not include any 34 administrative costs associated with an expansion. Such costs will likely include systems 35 changes, eligibility workers, and other administrative personnel. 36 37 A more detailed explanation of the Medicaid eligibility expansion cost estimate is 38 contained in the “Selected Cost Estimates Appendix”. The explanation contains 39 additional tables that will allow the reader to find cost estimates under different 40 assumptions than are provided here. The Selected Cost Estimates Appendix is available 41 at the following web site: www.burnshealthpolicy.com. 42 43 A more detailed explanation of the number of uninsured in Nevada is contained in the 44 “Technical Appendix”. The explanation and tables in the Appendix present information 45

Burns & Associates, Inc. II-7 May 5, 2006
about who the uninsured are in Nevada. The Technical Appendix is also available at 1 www.burnshealthpolicy.com. 2 3 4 2. Expanding/Expediting Medicaid Eligibility for SSI Eligible Individuals 5 6 Low-income individuals who receive Supplemental Security Income (SSI) benefits 7 because of age, disability or blindness are eligible for Nevada’s Medicaid program under 8 a mandatory eligibility category. The Nevada Department of Employment, Training & 9 Rehabilitation is responsible for determining if individuals with permanent disabilities are 10 eligible for SSI. Most initial SSI decisions are made within 90 days, but on average with 11 appeals, it takes an average of 10 months for a final decision. 12 13 Many of these special need individuals who would meet SSI disability criteria (and either 14 have not applied or are waiting for a decision) need and seek health services through 15 emergency departments or through state-only or safety-net programs. For example, 16 DHCFP indicates that, as of 2004, there are approximately 2,000 such individuals who 17 are seriously mentally ill and who are being treated with State-only dollars. 18 19 Both the focus groups and Nevada’s 2004 Strategic Plan for People with Disabilities 20 recommended that the State adopt mechanisms to expedite Medicaid eligibility for low-21 income disabled individuals in order to allow these individuals to receive necessary 22 services in timely manner. Several possible strategies for accomplishing this have been 23 identified and are briefly discussed below. 24 25 The necessity of implementing any of these strategies should be evaluated in the context 26 of the new federal disability determination process that was announced on March 31, 27 2006. 28 29 This new rule provides a quick disability determination process for those who are 30 obviously disabled. It is reported that favorable decisions will be made in such cases 31 within 20 days after the claim is received by the state disability determination agency. 32 Although the new rule takes effect in August of 2006, the federal government is phasing 33 in its implementation. The new process will not be implemented in Nevada for at least a 34 year. 35 36 In lieu of –or perhaps in addition to—pursuing eligibility determinations according to the 37 newly-announced rule, Nevada could explore several alternatives for expediting 38 eligibility. Those options include: 39 40
210 Optional Medicaid Coverage Group. One optional eligibility category 41 under Medicaid (known as the 210 group because of the section of the Federal 42 Register section authorizing it is 42 CFR 435.210) allows individuals to 43 qualify for Medicaid if they would be eligible for, but are not receiving, cash 44 assistance under SSI. DHCFP believes that disability determination under the 45

Burns & Associates, Inc. II-8 May 5, 2006
210 group could be made within two months, thus making the applicant 1 eligible for Medicaid benefits before being finally determined eligible for SSI. 2
3 State Assessment for Serious Mentally Ill. With a few exceptions, federal 4
regulations require that the State use the same definition of disability as used 5 under SSI. In order to further streamline the process, some states have sought 6 approval by SSA for alternative, but comparable disability assessments. In 7 the case of Arizona, for example, SSA has agreed to accept the assessment for 8 serious mental illness (SMI) conducted by the State’s behavioral health 9 division in lieu of a determination by the disability determination bureau. 10 Nevada currently uses the LOCUS assessment tool to determine eligibility for 11 individuals with SMI. 12
13 Single Application for SSI and Medicaid. Most states, including Nevada, 14
automatically enroll all SSI recipients in Medicaid. Nevada, however, is one 15 of seven “SSI-Criteria states” that requires SSI beneficiaries to file a separate 16 Medicaid application with the state, which allows the State itself to determine 17 eligibility for Medicaid. Thirty-three states rely on SSA to determine 18 Medicaid eligibility for the SSI beneficiaries. The latter may afford a more 19 streamlined process for both the applicant as well as the State. 20
21 The strategy recommended for consideration by the Summit participants is the adoption 22 of the 210 option. This option should be adopted initially while implementation of the 23 new SSA rule “rolls out” across the country. Pending the outcome of these two 24 initiatives, the State then may want to consider approaching SSA to use the LOCUS 25 assessment tool for the SMI population. Separately, the State should consider unifying 26 the SSI and Medicaid application. 27 28 Cost Estimate 29 30 For the 210 option, the cost estimate involves two distinct pieces: 31 32
Administrative costs to reduce the eligibility determination wait time from 10 33 months to two months 34
35 The medical costs that will be incurred because the individuals will be eligible 36
for an additional eight months 37 38 The administrative costs are composed of systems modifications, an outside vendor to 39 perform medical reviews, and additional state staff. With the assumption that SFY 2008 40 is a “start up” year and SFY 2009 is the first full year of operations, the estimated state 41 costs for administration are $700,000 in SFY 08 and $3.5 million in SFY 09. 42 43 The cost of medical services for the 210 population reflects the 8 month period that this 44 population will be receiving medical services because of the accelerated eligibility 45

Burns & Associates, Inc. II-9 May 5, 2006
determination. Using assumptions provided by DHCFP, it is estimated that the cost to 1 the state of medical services provided to the 210 population will be: 2 3
For SFY 08 (start up year) $0 4 For SFY 09 $ 6.1 million 5 For SFY 10 $28.3 million 6
7 The estimates do not reflect potential savings from bringing these high-cost individuals 8 onto Medicaid earlier. The savings may accrue because they will be receiving health care 9 for an additional 8 months and their medical conditions may not be as severe as the 10 population that is currently entering the program, and because their care will be managed 11 more closely from an earlier time period. 12 13 There are a significant number of assumptions and calculations associated with this cost 14 estimate. A more detailed explanation of the estimate is contained in the “Selected Cost 15 Estimates Appendix”. The explanation contains tables that depict the current costs faced 16 by the state as well as costs under the proposed strategy. The Selected Cost Estimates 17 Appendix is available at the following web site: www.burnshealthpolicy.com. 18 19 20 3. Expanding Outreach Efforts and Streamlining Eligibility 21 22 Health care researchers have estimated that a large percentage of the uninsured would be 23 eligible for Medicaid and SCHIP if they applied. For example, one national study found 24 that for uninsured children, 52% would be eligible for Medicaid and 25% would be 25 eligible for SCHIP. Another study looking at adults estimated that 46% of low-income 26 adults (parents and adults without children) could be covered by public coverage. Given 27 these findings, numerous states have employed strategies to decrease the number of 28 uninsured in their states that involve: 1) simplifying their Medicaid and SCHIP 29 enrollment processes and 2) increasing their outreach efforts for these programs. 30 31 The situation appears to be similar for Nevada, especially with respect to children. Based 32 on an analysis of 2003 to 2005 CPS data, there are 72,000 uninsured children in families 33 with incomes up to 200% of the FPL. A substantial number of these children should be 34 eligible for either Medicaid or Check Up1. 35 36 For the past seven years, Nevada has had a Robert Wood Johnson Covering Kids & 37 Families grant (that totaled $1.6 million) to develop activities to increase enrollment and 38 retention in Nevada’s SCHIP and Medicaid programs. Monies from this grant were 39 matched with federal Medicaid and SCHIP dollars. With the Great Basin Primary Care 40 Association serving as the lead organization, the grant funds supported two local projects: 41 1) Clark County Health District, covering the southern part of the state and 2) United 42
1 A depiction of the uninsured in Nevada is contained in the “Technical Appendix”. The explanation and tables in the Appendix present information about who the uninsured are in Nevada. The Technical Appendix is available at www.burnshealthpolicy.com.

Burns & Associates, Inc. II-10 May 5, 2006
Way of Northern Nevada, covering northern urban cities and surrounding areas as well as 1 rural and frontier communities in the state. As a result of these projects, a number of 2 different outreach strategies have been implemented, including: 3 4
Direct one-to-one outreach in the community 5 Partnering with human service agencies who assist families in applying for 6
Check Up and Medicaid 7 Holding application assistance sessions at the local schools 8 Conducting trainings on the eligibility application process 9 Attending health fairs to distribute eligibility applications 10 Using Vista and AmeriCorps volunteers to assist families with application 11
processes 12 13 While this grant ends in August 2006, grant applications for additional outreach dollars 14 have been submitted to various funding organizations, including the Trust Fund for 15 Healthy Nevada. 16 17 DHHS, Division of Welfare and Supportive Services is responsible for determining 18 Medicaid eligibility and DHCFP is responsible for determining Check Up eligibility. 19 20 While there was no specific data available about the reasons for Medicaid denials, 21 disenrollments, and churning in the system (i.e., individuals falling off and coming back 22 on the program), Check Up data shows that about 20% of initial denials were due to 23 procedural reasons (e.g., lack of information, lack of cooperation) and about 37% of the 24 reasons for disenrollments were due to procedural reasons (e.g., not responding to 25 redetermination process, lack of information, loss of contact). 26 27 Nevada’s current eligibility process includes a number of “best practices” that have been 28 recommended by health care experts as effective means for streamlining eligibility and 29 reducing procedural barriers: 30 31
12 month redetermination periods 32 No asset test for pregnant women and children 33 No face-to-face requirement for Check Up and for Medicaid (if not also 34
applying for TANF/Food Stamp) 35 On-line Check Up application (can be submitted electronically but one still 36
needs to sign and submit with documentation) 37 38
Other recommended best practices that could be used to further enhanced Nevada’s 39 eligibility process would be: 40 41
12 month continuous eligibility for Medicaid and Check Up, in which a 42 person maintains eligibility regardless of certain changes in family income or 43 circumstances 44
Use of community agencies in both taking and submitting applications 45 Adoption of on-line interactive electronic applications as is used in California 46

Burns & Associates, Inc. II-11 May 5, 2006
Joint Medicaid and Check Up application 1 Reduction in Medicaid documentation requirements 2 Simplification of Medicaid notices, including issuing notices in Spanish as 3
well as English 4 Consolidation or alignment of the Medicaid and Check Up eligibility 5
processes so that it is performed by the same government unit or has similar 6 requirements 7
8 Additionally, the Check Up program charges quarterly premiums (that vary by income 9 level, ranging from quarterly premiums of $15 to $70)) for coverage under the program. 10 Researchers and experts generally agree that premiums—even nominal premiums—11 discourage enrollment of low-income populations. 12 13 The Summit participants may wish to consider a recommendation for the State to 14 eliminate premiums on this population. 15 16 Additional strategies related to expanding outreach and streamlining eligibility for the 17 Summit participants to consider include: 18 19
Provide new funds (either from the State General Fund or from the Trust Fund 20 for Healthy Nevada) to continue and expand the outreach efforts that 21 previously had been supported through the RWJ grant (e.g., fund the 22 approximately $500,000 two-year grant application for outreach activities that 23 was submitted to the Trust Fund for Healthy Nevada). 24
25 Have DHHS or a Task Force conduct a review of current eligibility processes 26
in the context of recommended best practices. In particular the review should 27 look at the best practices that have been proven to be effective in other states 28 with particular emphasis on streamlining eligibility and facilitating the ability 29 of individuals to apply for Medicaid and SCHIP. 30
31 Cost Estimate 32 33 The cost estimate for this recommendation only specifically includes the $500,000 for 34 continuing outreach programs. 35 36 With respect to the eliminating of the premiums in Check Up, such an action would yield 37 two fiscal changes —the loss of premium revenue and the increased medical costs for the 38 children that may enroll because there is no longer a premium charged. 39 40 The recommendation for a review of the current eligibility process also does not include a 41 cost estimate. This effort could be staffed with state resources, or Summit participants 42 may consider recommending monies to supplement existing staff resources with funds 43 for either expanding staff or using the services of outside consultants. 44 45

Burns & Associates, Inc. II-12 May 5, 2006
4. Increase Medicaid and SCHIP Reimbursement Rates 1 2 Nationally, adequacy of Medicaid reimbursement rates has been a longstanding concern 3 among policymakers and providers. Low reimbursement is often cited as one of the 4 causes for limited provider participation in Medicaid and SCHIP programs, leading 5 ultimately to reduced client access to care. These same concerns have been expressed by 6 Nevada stakeholders. 7 8 Recently, the State has taken a number of steps to increase provider reimbursement rates: 9 10
As the result of 2001 legislation, a Provider Rates Task Force was established 11 and was assigned to review provider rates related to home and community 12 based services provided to persons with developmental disabilities and 13 seniors, as well as for mental health services and therapies. The Task Force 14 recommendations have been implemented in stages, with the full 15 recommended provider rate increases implemented by FY 2005. 16
17 In the summer of 2004, the DHCFP held public workshops regarding 18
Medicaid and Check Up reimbursement rates, specifically focusing on rates 19 for services which are billed by physicians and other health care practitioners. 20
21 The Division proposed ten provider rate enhancements, of which three were 22
included in the Governor’s recommended budget and subsequently funded by 23 the legislature (air ambulance, mental health rehabilitative treatment services, 24 and home infusion therapy). 25
26 In 2006, DHCFP began considering other areas for rate increases in the Medicaid 27 program. Increasing the rates to providers will create incentives for providers to continue 28 to participate in the Medicaid program. 29 30 In the area of professional fee schedules, potential areas include: 31
32 1. Adopting the Medicare 2007 fee schedule to pay professionals beginning in 33
SFY 08 and updated annually thereafter. In following the Medicare schedule, 34 this would also incorporate the use of modifiers for services that are more 35 complex instead of an across-the-board upward adjustment for a certain type 36 of procedure or for a targeted population (e.g., pediatrics) which is done now 37 in Nevada. Further, the payment rates would be based on place of service 38 (facility vs. non-facility settings), rather than the current “either or” approach. 39 40
2. Paying the same rate to all providers delivering the same service regardless of 41 their licensing 42 43
3. Increasing payments for providers in rural settings by 20% above the rates set 44 for urban providers 45
46

Burns & Associates, Inc. II-13 May 5, 2006
4. Provide a rate increase to home health agencies 1 2
5. Allowing for reimbursement of telehealth for a peer to peer process 3 4
In the area of facility reimbursement, potential areas include: 5 6
1. Increasing hospital inpatient rates to cover costs and updated based on CMS 7 Health Care Indicators. Currently, hospitals are not reimbursed the full costs 8 to cover the care they provide to Medicaid recipients. The DHCFP reports 9 that as of SFY 05, hospitals on average received payment for 90% of their 10 Medicaid-allocated costs. This varies significantly by type of hospital as well. 11 For example, psychiatric hospitals received payment for almost all of their 12 costs (98.2%) whereas rehabilitation hospitals received payment for only 59% 13 of their costs. The specific changes outlined not only account for full cost 14 coverage but also build a long-term foundation for rate adjustments on a 15 regular basis by applying a medical inflation factor. 16
17 2. Reimburse critical access hospitals the full cost of outpatient hospital services 18
as is already done for inpatient hospital services. Medicare also pays the full 19 cost for these services to critical access hospitals. 20
21 3. Paying enhanced rates to free-standing in-state nursing facilities to care for 22
behaviorally-challenged Medicaid recipients to avoid out-of-state placement 23 24 Summit participants may want to consider recommending all or none of the provider rate 25 increases identified as priority areas by the DHCFP. 26 27 Cost Estimate 28 29 The cost estimates for the rate increases discussed above are shown in the tables below: 30 31
Professional Fee Schedule Increases 32 33
Total Funds Needed Federal Share State Share
SFY 2008 $ 32,494,287 $ 17,793,871 $ 14,700,415
SFY 2009 $ 33,221,796 $ 18,192,256 $ 15,029,541
Total for Biennium $ 65,716,083 $ 35,986,127 $ 29,729,956
Change Rates Paid for Professional Services to the 2007 Medicare Fee Scheduleand to Appropriately Pay Based on Place of Service
34 35 36

Burns & Associates, Inc. II-14 May 5, 2006
Total Funds Needed Federal Share State Share
SFY 2008 $ 860,465 $ 471,191 $ 389,274
SFY 2009 $ 879,730 $ 481,740 $ 397,990
Total for Biennium $ 1,740,194 $ 952,930 $ 787,264
Change Payments so that Providers are Paidthe Same Rate for Delivering the Same Service
1 2 3
Total Funds Needed Federal Share State Share
SFY 2008 $ 1,488,276 $ 814,980 $ 673,296
SFY 2009 $ 1,710,159 $ 936,483 $ 773,676
Total for Biennium $ 3,198,436 $ 1,751,463 $ 1,446,972
Change Rates so that Rural ProvidersReceive a 10% Increase in Rates Paid for Professional Services
4 5 6
Total Funds Needed Federal Share State Share
SFY 2008 $ 683,757 $ 360,408 $ 323,349
SFY 2009 $ 790,761 $ 416,810 $ 373,951
Total for Biennium $ 1,474,518 $ 777,218 $ 697,300
Increase Rates Paid to Home Health Agency Providers
7 8 9
Total Funds Needed Federal Share State Share
SFY 2008 $ 350,178 $ 184,579 $ 165,599
SFY 2009 $ 364,185 $ 191,962 $ 172,223
Total for Biennium $ 714,363 $ 376,541 $ 337,822
Funds to Support Telehealth InitiativesRelated to Consultation and Radiology Services in Rural Counties
10

Burns & Associates, Inc. II-15 May 5, 2006
1 2
Facility Fee Schedule Increases 3 4
Total Funds Needed Federal Share State Share
SFY 2008 $ 34,709,655 $ 18,295,459 $ 16,414,196
SFY 2009 $ 41,591,083 $ 21,922,660 $ 19,668,423
Total for Biennium $ 76,300,738 $ 40,218,119 $ 36,082,619
Additional Payments to Ensure all Medicaid Costs are CoveredFor General Acute Care, Psychiatric, and Rehab Hospitals Combined
5 6 7
Total Funds Needed Federal Share State Share
SFY 2008 $ 1,299,273 $ 684,847 $ 614,426
SFY 2009 $ 1,385,058 $ 730,064 $ 654,994
Total for Biennium $ 2,684,331 $ 1,414,911 $ 1,269,420
Change Methodology so that Critical Access HospitalsReceive Full Cost Reimbursement for Outpatient Hospital Services
8 9 10
Total Funds Needed Federal Share State Share
SFY 2008 $ 1,609,189 $ 848,203 $ 760,985
SFY 2009 $ 1,673,556 $ 882,131 $ 791,425
Total for Biennium $ 3,282,745 $ 1,730,335 $ 1,552,410
Funds to Support New Behaviorally-Challenged Medicaid Recipients(15 per year) Remain in Nevada Instead of Placement Out-of-State
11 12

Burns & Associates, Inc. II-16 May 5, 2006
5. Enhancing Coverage under the Home and Community-Based Waivers 1 2 Nevadans (both in the focus groups and in the recent strategic plans for seniors and the 3 disabled) have consistently stressed as a priority the need for Nevada to shift away from 4 institutional to home and community-based care. The overall goal being to develop 5 systems of care that provide a flexible array of community services and supports to frail 6 elderly or persons with developmental disabilities or physical disabilities who wish to 7 remain in the community. (See discussion under Policy Brief on Behavioral Health as it 8 relates to home and community-based services for persons with behavioral health 9 conditions.) 10 11 Historically, under Medicaid there have been three key avenues through which states 12 provide home and community-based services to persons at risk of institutionalization.2 13 14 Nevada’s Medicaid program is currently taking advantage of all three options: 15 16
Provision of home health services, a mandatory Medicaid service. In SFY 04, 17 891 clients received this service at a cost of $6.3 million. 18
19 Provision of personal care services, an optional Medicaid service. In SFY 04, 20
3,642 clients received this service at a cost of $33.8 million. 21 22
Provision of home and community-based services through 1915(c) waivers. 23 In waiver year3, a total of 3,045 clients were served through one of four 24 waivers at a cost of $35.7 million. (See the Table that follows this discussion 25 for specific information about individual waivers.) 26
27 The dollars expended on home and community-based waiver services increased 27% 28 from waiver year 2004 to waiver year 2005 to $45.4 million. It should be noted that 29 clients in the waiver programs also receive non-waiver services (also referred to as state 30 plan services) which other Medicaid clients receive. The total cost of services (waiver 31 and non-waiver) provided to clients enrolled in the waiver programs in waiver year 2005 32 was $91.7 million. 33 34 The State must prove to the federal government that the waiver programs are “cost 35 neutral”, meaning that the costs per person with the waiver are the same or less than what 36 they would have been without the waiver. In waiver year 2005, the annual costs for 37 waiver clients (including both waiver services and state plan services) were much below 38 the anticipated costs for these clients if the waivers were not in existence. These 39 differences, by waiver, are shown in the following table: 40 41 42
2 New options have recently been made available to states under the Deficit Reduction Act (see discussion under DRA issue following). 3 Each of Nevada’s four 1915(c) waivers have different reporting periods. The “waiver year” represents the reporting year for each specific waiver.

Burns & Associates, Inc. II-17 May 5, 2006
Waiver Costs with Waiver
Estimated Costs without
Waiver
Pct Lower with Waiver
WIN (persons with physical disabilities)
$31,861 $53,833 -41%
CHIP (frail elderly) $14,245 $36,939 -61% WEARC (elderly in adult residential care)
$19,832 $32,230 -38%
MRRC (persons with mental retardation and related conditions)
$32,858 $125,707 -74%
1 In comparing Nevada’s home and community-based waiver programs to other states’ 2 programs in 2002, the Kaiser Commission on Medicaid and the Uninsured (2005) found 3 that: 4 5
Nevada had a low number of clients participating in their waivers (47th 6 nationally) 7
8 Nevada’s total expenditures for the waiver programs was the lowest of all the 9
states 10 11
Nevada’s average expenditure per waiver participant (waiver services only) 12 was below the national average: 13
Nevada National 14 MR/DD $23,132 $34,581 15 Aged $ 4,450 $ 6,181 16 Physically Disabled $ 3,522 $13,433 17
18 Twenty-two states had separate home and community-based waivers for 19
persons with traumatic brain injury and spinal cord injury, 20 states had 20 waivers for children with special needs and 15 states had waivers for persons 21 with HIV/AIDS, and Nevada had none of these waivers 22
23 While consideration should be given to undertaking a redesign of the overall long-term 24 system (see next strategy), there are a number of short-term strategies related to 25 enhancing coverage under the current home and community-based waiver programs that 26 the Summit participants may wish to consider. These strategies include: 27 28
Increase in Number of Case Managers. Available waiver slots in the 29 Community Home-Based Initiative Program (CHIP), Waiver for Independent 30 Nevadans (WIN) and Waiver for Elderly and Adult Residence Care 31 (WEARC) programs are not being filled due to a lack of state case managers. 32 In order to fill these available slots, DHHS needs to implement interventions 33 to remove the barrier being created by the shortage of case managers. 34 35

Burns & Associates, Inc. II-18 May 5, 2006
There are two strategies that could be considered: 1 2
a) loosening the qualifications requirements for case managers (currently 3 limited to Nevada licensed social workers for CHIP and WEARC and to 4 licensed health professionals for WIN) and allowing other qualified (and 5 not necessarily licensed) health care professionals to serve as case 6 managers; and 7 8 b) contracting with an outside medical management firm to provide case 9 management services. 10 11
Other states, as well as Nevada’s Waiver for Persons with Mental Retardation 12 and Related Conditions (MRRC) waiver, do not have as restrictive 13 qualification requirements for case managers as do these three waivers. 14 15
Additional Services under WIN. In order to address the needs of individuals 16 with traumatic brain injuries who qualify for the WIN waiver, the Strategic 17 Plan for People with Disabilities recommended adding residential habilitation 18 and behavioral adult day care. DHCFP has estimated that 30 recipients per 19 year would be appropriate for residential habilitation and 15 recipients would 20 be appropriate for behavioral adult day care and other waiver services. 21
22 Elimination of the Waiting List for the MRRC Waiver through Increased Slots 23
and Funding. Currently, further expansion of the MRRC is limited due to lack 24 of state Medicaid matching funds and the lack of available slots. The number 25 of individuals on this waiting list continues to increase, along with the wait 26 time of ten months. 27
28 Cost Estimate 29 30 Increase in Number of Case Managers: No additional costs are required here if the State 31 opts to lower the qualification requirements of case managers to increase the available 32 pool of resources.( And to fill already “funded” positions.) 33 34 Additional Services under WIN: The estimated cost to add services under this waiver 35 targeted for persons with traumatic brain injury is estimated for SFY 09 to be $2.1 36 million in total funds and $1 million in state funds. 37 38 Elimination of Waiting Lists for the MRRC Waiver through Increased Funding: 39 Estimated annual costs are based upon estimated expenditures per person in the MRRC 40 waiver in FFY 2005 (including both waiver and state plan services). With a current 41 waiting list of 386 (as of February 2006) and annual costs per person of $32,858, the total 42 anticipated annual costs to eliminate the waiting list are $12,683,411 in total funds and 43 $5,997,985 in state funds. 44

Burns & Associates, Inc. II-19 May 5, 2006
Community Home-Based Initiative Program (CHIP)
Waiver for Elderly and Adult Residence Care (WEARC)
Waiver for Independent Nevadans (WIN)
Waiver for Persons with Mental Retardation and
Related Conditions (MRRC) Responsible State Agency
DHHS, Division of Aging DHHS, Division of Aging DHHS, Division of Health Care Financing and Policy
DHHS, Division of Mental Health and Developmental Services
Eligible Population 65 years of age or older At risk for institutionalization
(nursing facility) Income set at 300% SSI Need assistance with one or
more of the following: bathing, dressing, eating, toileting, ambulating, transferring
65 years of age or older Currently residing in nursing
home, hospital or receiving CHIP waiver*
Income set at 300% SSI Functioning at an
intermediate level of care Ambulatory (walk with or
w/o cane/walker) or transfer from wheelchair
Able to protect self in an emergency
*The renewal application that is at CMS for approval eliminates this criteria, allowing anyone who meets the other waiver criteria to qualify.
At risk for institutionalization (nursing facility)
Income set at 300% SSI Certified as physically
disabled by Central Office Disability Determination Team: disabilities must result from anatomical/physiological abnormalities with persons with psychological, behavioral or cognitive abnormities excluded unless have qualifying physical disability
At risk for institutionalization (ICF/MR)
Income set at 300% SSI Person with mental
retardation or related condition (cerebral palsy, epilepsy or other condition other than mental illness that is closely related to mental retardation – including autism due to a court decision)

Burns & Associates, Inc. II-20 May 5, 2006
Community Home-Based Initiative Program (CHIP)
Waiver for Elderly and Adult Residence Care (WEARC)
Waiver for Independent Nevadans (WIN)
Waiver for Persons with Mental Retardation and
Related Conditions (MRRC) Covered Services Case Management
Attendant Services Homemaker Services Adult Day Care Adult Companion Personal Emergency Response
System Chore Services Respite Nutrition Therapy
Case Management Personal Care
Case Management Homemaker Chore services Respite care Environmental Accessibility
Adaptations Extended Transportation Specialized Medical
Equipment Personal Emergency Response
System Assisted Living Independent Living Services Home Delivered Meals Extended Dental Service Attendant Care
Service Coordination (Targeted Case Management)
Community Day Habilitation: day habilitation, prevocational services, educational services and supported employment services
Habilitative Residential Supports: family support arrangement and supported living services/arrangement
Number of Slots Allotted under Waiver (represents unduplicated counts for the entire year)
2,030 (FY06) increasing to 2,483 (FY10)
505 (FY06) 1,092 (FY06) 1,392 (FY06)
Number of Current Waiver Clients (open cases at end of month- March 2006)
1,167
300
514 1,356
Number of Clients on Waiting List (snapshot at end of month)
217 (3/06) 41 (3/06) 138 (3/06) 386 (2/06)
Average Wait Time (6/05)
3.5 months <1 month 7.0 months 10.0 months

Burns & Associates, Inc. II-21 May 5, 2006
6. Evaluating Options Under the Deficit Reduction Act Related to Long-Term Care 1 2 The federal Deficit Reduction Act (DRA) which became law on February 1, 2006 3 provides states with a number of new Medicaid program options related to the delivery of 4 services to persons with disabilities and long term care needs. These provisions include: 5 6
Beginning 1/1/07, allowing families with incomes up to 300% of the FPL to 7 buy Medicaid coverage for their disabled children. 8
9 Continuing grants programs to the states to: 10
11 1. Allow working individuals with a disability to buy into Medicaid and 12
receive access to personal assistance and other health and employment 13 services 14
2. Provide benefits to workers who have physical or mental impairments 15 (grant applications will only be accepted through 6/30/06) 16
17 Beginning 1/1/07, allowing states to offer home and community-based 18
services as a Medicaid State Plan option (as opposed to needing to apply for a 19 waiver). Under this option, a state can establish the number of individuals to 20 be covered, services are limited to persons with income up to 150% of the 21 FPL, and individuals are not required to meet an institutional needs test in 22 order to receive home and community-based services. 23
24 Establishing or continuing the following community-based demonstration 25
grants: 26 27
1. “Money Follows the Person Rebalancing Demonstration” which is aimed 28 at shoring up community-based infrastructure so that individuals have a 29 choice of where they live and receive services (will begin to award grants 30 1/1/07). This competitive two-year grant provides incentives for states to 31 reallocate long-term care services to community options by providing an 32 enhanced match rate for one year for each person that the state transitions 33 from an institution to the community. This enhanced federal matching 34 funding is intended to free up state Medicaid match that could be used to 35 pay for one-time transition expenses (e.g. rental security deposits). 36
37 2. “Real Choice System Change Grants for Community Living” which is the 38
continuation of a current grant program used to design and construct 39 systems infrastructure that will result in improvements in community 40 long-term support systems (e.g., improved access to support services, 41 information technology, affordable housing). 42
43 3. “Demonstration to Offer Home and Community-Based Alternatives to 44
Psychiatric Residential Treatment Facilities for Children” which is aimed 45 at testing the effectiveness of improving and maintaining the functional 46

Burns & Associates, Inc. II-22 May 5, 2006
level of children with psychiatric disabilities as well as the cost-1 effectiveness of Medicaid-funded home and community-based services as 2 alternatives to residential psychiatric treatment centers (see more detailed 3 discussion in the Behavioral Health Policy Brief). 4
5 Beginning 1/1/07, allowing states to offer self-directed personal care services 6
(cash and counseling), including self-directed personal care services provided 7 by family members as a Medicaid State Plan option (as opposed to needing to 8 apply for a waiver.) This provision allows states to restrict the geographic 9 areas of the state where services are available and to limit the populations 10 eligible to receive such services. 11
12 Allowing an individual who purchases a qualified private long-term care 13
policy, but who eventually uses all its benefits, to apply for Medicaid without 14 having to spend most of his/her assets first. 15
16 Although states are currently awaiting guidance from the Centers for Medicare & 17 Medicaid Services as to how the DRA provisions will be implemented, the Summit 18 participants may wish to consider a strategy that recommends DHHS immediately 19 assemble an internal workgroup to analyze the pros and cons of the different provisions 20 for Nevada. This would also include cost-avoidance and cost-savings opportunities 21 afforded by the DRA. The strategy recommendation may (or may not) indicate which 22 provisions DHHS should focus on first. 23 24 The DRA contains opportunities that are consistent with several of the goals expressed by 25 the focus groups and advocacy groups for long term care services. A DHHS task force 26 could prioritize those items in the DRA that are time sensitive. 27 28 A second strategy that the Summit may wish to consider is the process to be followed 29 once the DHHS task force reports. Options here could include consideration by the 30 Legislative Committee on Health Care or by a commission composed of providers, 31 advocates and members of the public. The consideration of which options to pursue in 32 the short and long term would be determined once an assessment of the DRA provisions 33 have been performed. 34 35 Cost Estimate 36 37 No specific cost estimate is included as the strategies offered are for the work of a task 38 force. Summit participants may want to consider supplementing existing DHHS 39 resources with additional funds for either expanding DHHS staff resources or the services 40 of outside consultants. 41 42

Burns & Associates, Inc. II-23 May 5, 2006
7. Explore a Redesign of the Long-Term Care Service Delivery Model 1 2 Long-term care services nationally, as well as in Nevada, are a main driver of overall 3 costs for the Medicaid program. The Nevada DHCFP reports that in SFY 05, services to 4 the elderly comprised 14.5% of the total Medicaid budget but this population represented 5 only 5.8% of all Medicaid eligibles. Likewise, services to the blind and disabled 6 comprised 43.8% of the total SFY 05 budget, but these eligibles represented 14.7% of the 7 population. Combined, 58% of the Medicaid budget was used for 20% of the population, 8 a common occurrence for Medicaid programs across the country. 9 10 It is expected that the demands for long-term care services among Medicaid recipients 11 will grow as Nevada’s population grows and ages (i.e., 11.0% of the state’s population 12 was 65+ in 2000; by 2030, 18.6% of a much larger population will be in that age 13 category). 14 15 Additionally, long-term care functions and operations are dispersed in different Divisions 16 and are delivered through separate systems of care. Developing a more effective and 17 efficient system of care for the elderly and people with disabilities will likely improve 18 financial performance and definitely minimize access barriers and provide real choices to 19 recipients. 20 21 To support the overall goal of more Nevada seniors getting the benefits, services and 22 supports they need, Nevada’s Task Force on Senior Services identified the need to 23 design, fund and implement a single point of entry system for information, referral, 24 assistance, care planning and care management. More recently, the Accountability 25 Committee for the Nevada Strategic Plan for Senior Services added a recommendation 26 that the Governor support consolidating the Medicaid waivers. 27 28 Numerous state Medicaid programs are analyzing or undergoing structural reforms of 29 their long term care service delivery systems (e.g., Colorado, Maine, New Hampshire, 30 Arizona, Wisconsin and Kentucky). These reform efforts include: 31 32
Single point of entry systems, which serve multiple populations, combine or 33 coordinate financial and function eligibility determinations and coordinate 34 multiple funding streams. 35
36 Global budgeting in which all of the components of long-term care spending 37
(e.g., nursing facility, home and community-based, state-funded personal care 38 programs) are consolidated into a single state agency budget such that funding 39 can follow the person as they move between services. 40
41 Individual budget models (e.g. Independence Plus Medicaid initiative, 42
consumer self-directed programs), in which beneficiaries are given a budget to 43 purchase services and participate in the planning, hiring and managing of 44 workers, and a fiscal intermediary is used to issue checks and perform tax 45 withholding for workers. 46

Burns & Associates, Inc. II-24 May 5, 2006
Contracting with administrative services organizations or managed care 1 organizations to manage long term care services either on a performance basis 2 or on a risk basis. Responsibilities of these organizations range from the 3 provision of enhanced care coordination to the provision of the full array of 4 administrative related services including case management. 5
6 Building upon the recommendations of the Accountability Committee and the 7 opportunities afforded under the Deficit Reduction Act previously discussed, the Summit 8 participants may wish to consider a strategy that specifically recommends — either 9 within the context of the DRA task force or as a separate task force — an examination of 10 the strengths and weaknesses of the current system. The task force should then develop 11 optional service delivery models that can increase efficiencies, lead to better outcomes, 12 allow more individuals to receive services, and reduce the cost of care. 13 14 The charge of this task force would be broader than the DRA task forces and would 15 examine the long term care system with a “redesign” perspective. 16 17 Cost Estimate 18 19 There is no specific cost estimate included for this strategy as the recommendation 20 offered for consideration is a redesign task force. Summit participants may want to 21 consider supplementing existing resources with additional funds for either expanding 22 available state resources or using the services of outside consultants. 23

Burns & Associates, Inc. II-25 May 5, 2006
Resources 1 2 AARP Public Policy Institute (February 2006). Pulling Together: Administrative and 3 Budget Consolidation of State Long-Term Care Services. Retrieved April 6, 2006 from 4 http://www.aarp.org/ppi 5 6 Armour-Garb, Allison (April 30, 2004). Point of Entry Systems for Long-Term Care: 7 State Case Studies (Draft). Retrieved April 7, 2006 from 8 www.nyc.gov/html/dfta/pdf/ltc.pdf 9 10 Association of University Centers on Disabilities (February 17, 2006). Summary of the 11 Deficit Reduction Act of 1005 (PL 109-171) Excerpt from the Jan-Feb. Issue of the 12 ARC/UCP Disability Collaboration Washington Watch. Retrieved on April 6, 2006 from 13 http://www.aucd.org/Mediciad/DRA_Summary.htm 14 15 Bruen, Brian K., et al. (August 1999). State Usage of Medicaid coverage Options for 16 Aged, Blind, and Disabled People. Assessing the New Federalism: An Urban Institute 17 Program to Assess changing Social Policies. 18 19 Center for Medicare & Medicaid Services (August 2001). Enrolling and Retaining Low-20 Income Families and Children in Health care Coverage. 21 22 Center for Medicare & Medicaid Services (March 31, 2006). State Medicaid Director 23 Letters on Roadmap for Medicaid Reform – New Options to Support Individuals with 24 Disabilities and Long-Term Care Needs, New Options to Improve and expand Insurance 25 Coverage for Acute Care Needs, and Section 6044, State Flexibility in Benefit Packages. 26 Retrieved April 6, 2006 from http://new.cms.hhs.gov/SMDL/SMD/list.asp? 27 28 Covering Kids & Families. Nevada Covering Kids & Families Initiative. Retrieved 29 March 26, 2006 from http://coveringkidsandfamilies.org/projects/index.php?StateID=NV 30 31 Crowley, Jeffrey S. et al. (April 2006). Medicaid Long-Term Services Reforms in the 32 Deficit Reduction Act. The Kaiser Commission on Medicaid and the Uninsured: Issue 33 Paper. 34 35 Davidoff, Amy, et al. (April 2004). Medicaid and State-Funded Coverage for Adults: 36 Estimates of Eligibility and Enrollment. The Kaiser Commission on Medicaid and the 37 Uninsured. 38 39 Dubay, Lisa, et al., (March 2002). Children’s Eligibility for Medicaid and SCHIP. A 40 View from 2000. New Federalism: National Survey of America’s Families. The Urban 41 Institute. 42 43 Ellis, Eileen R., et al. (September 2005). Medicaid Enrollment in 50 States. The Kaiser 44 Commission on Medicaid and the Uninsured. 45

Burns & Associates, Inc. II-26 May 5, 2006
Federal Register (March 31, 2006). Social Security Administration: Administrative 1 Review Process for Adjudicating Initial Disability Claims. (20 CFR Parts 404, 405, 416 2 and 422). Vol 71 (No. 62) 3 4 Gibson, Mary Jo, et al. (2004). Across the States: Profiles of Long-Term Care: Nevada. 5 AARP Public Policy Institute. 6 7 Kasper, Judy and Molly O’Malley (April 2006). Nursing Home Transition Programs: 8 Perspectives of Medicaid Care Planners. The Kaiser Commission on Medicaid and the 9 Uninsured. 10 11 Ku, Leighton and Donna Cohen Ross (December 2002). Staying Covered: The 12 Importance of Retaining Health Insurance for Low-Income Families. The 13 Commonwealth Fund. 14 15 National Association of State Directors of Developmental Disabilities Services (February 16 3, 2006). House Ratifies Budget Reconciliation Bill; Measure Awaits President’s 17 Signature. Directors’ Alert Bulletin: No. 01-2006. 18 19 National Association of State Medicaid Directors. Aged, Blind, and Disabled Medicaid 20 Eligibility Survey. Retrieved April 3, 2006 from 21 http://www.nasmd.org/eligiblity/mandatory.asp 22 23 National Conference of State Legislatures (February 3, 2006). Deficit Reduction Act of 24 2005 – Summary of Medicaid/Medicare/Health Provisions. 25 26 National Law Center on Homelessness & Poverty (September 2003). Presumptive 27 Eligibility for SSI – An Overview. Retrieved March 24, 2006 from 28 www.nlchp.org/FA_Income/preseumptiveeligibility.pdf 29 30 Ross, Donna and Laura Cox (October 2005). In a Time of Growing Need: State Choices 31 Influence Health Coverage Access for Children and Families. The Kaiser Commission 32 on Medicaid and the Uninsured. 33 34 Shirk, Cynthia (March 3, 2005). Rebalancing Long-Term Care: The Role of the 35 Medicaid HCBS Waiver Program. National Health Policy Forum. 36 37 Smith, Vernon, et al. (October 2005). Medicaid Budgets, Spending and Policy Initiatives 38 in State Fiscal Years 2005 and 2006: Results from a 50-State Survey 39 40 Southern Institute on Children and Families (October 2003). The Burden of Proof: How 41 Much is Too Much for Health Care Coverage? Southern Institute on Children and 42 Families. 43 44

Burns & Associates, Inc. II-27 May 5, 2006
Spillman, Brenda C. et al. (April 2006). An Inventory of Individual budget-based 1 Community Long Term Care Programs for the Elderly. The Kaiser Commission on 2 Medicaid and the Uninsured: Issue Paper. 3 4 The Commonwealth Fund (March 2006). Federal Activity Affecting Performance of 5 State Health Care Systems. States in Action: A Quarterly Look at Innovations in Health 6 Policy: Volume 4. 7 8 The Kaiser Commission on Medicaid and the Uninsured (May 2002). Enrolling 9 Uninsured Low-Income Children in Medicaid and CHIP. 10 11 The Kaiser Commission on Medicaid and the Uninsured. State Medicaid Fact Sheet: 12 Nevada & United States. Retrieved April 5, 2005 from www.kff.orf/MFS/ 13 14 The Kaiser Commission on Medicaid and the Uninsured (July 2005). Medicaid 1915(c) 15 Home and Community-Based Service Programs: Data Update. 16 17 The Kaiser Commission on Medicaid and the Uninsured (February 2006). Deficit 18 Reduction Act of 2005: Implications for Medicaid. 19 20 United States, Social Security Administration. Supplemental Security Income: Expedited 21 Payments. Retrieved March 24, 2006 from http://www.ssa.gov/notices/supplemental-22 secuirty-income/text-expedite-ussi.htm 23 24 25 Nevada Specific Documents: 26 27 Division of Health Care Financing and Policy (January 2005). Medicaid and Nevada 28 Check Up Factbook. www.dhcfp.state.nv.us 29 30 Great Basin Primary Care Association. Nevada Covering Kids. Retrieved March 30, 31 2006 from http://www.gbpca.org/coveringkids/about_us.htm 32 33 State of Nevada Department of Health and Human Services, Strategic Plan 34 Accountability Committees 2004-2006: Nevada’s strategic Plan for People with 35 Disabilities Annual Report – July 2005, Strategic Plan for Rural Health Care – Positions 36 and Recommendations – 2004 Annual Report and State of Nevada Strategic Plan for 37 Senior Services Annual Report – July 200. Retrieved April 7, 2006 from 38 http://hr.state.nv.us/directors/SP-AccComm04/ 39 40 State of Nevada Department of Health and Human Services, Division of Aging Services. 41 State Plan: Services for Nevada’s Elders: October 1, 2004 to September 30, 2007. 42 Retrieved April 15, 2006 from http://www.nvaging.net/sp/04-07StatePlan.pdf 43 44

Burns & Associates, Inc. II-28 May 5, 2006
State of Nevada Department of Health and Human Services, Office of Disability 1 Services. Developmental Disability Strategic Five Year Plan. Retrieved April 7, 2006 2 from http://www.hr.state.nv.us/directors/disabilitysvcs/DDStrategicFiveYrPlan.pdf 3 4 State of Nevada Department of Health and Human Services, Division of Welfare and 5 Supportive Services. Eligibility & Payments: Medical Programs. Retrieved April 5, 6 2005 from http://welfare.state.nv.us/elig_pay/medical_home.htm 7 8 State of Nevada. Perspectives: A Biennial Report of State Agencies 2004. Retrieved 9 April 5, 2005 from http://budget.state.nv.us/BR04/ 10 11 State of Nevada, Department of Health and Human Services, Division of Health Care 12 Financing & Policy (August 18, 2005). Waiver Caseload Information. Retrieved April 13 7, 2006 from http://dhcfp.state.nv.us/MSM%20Table%20of%20Contenets.htm 14 15 State of Nevada, Department of Health and Human Services, Division of Health Care 16 Financing & Policy Medicaid Services Manual: Chapter 2100 – Home and Community 17 Based Waiver (MR), Chapter 2200 – Aging Waiver, Chapter 2300 – Physical Disability 18 Waiver and Chapter – Waiver for the Elderly in Adult Residential Car. Retrieved April 19 7, 2006 from http://dhcfp.state.nv.us/wcaseloads.htm 20 21 State of Nevada Department of Human Resources (October 2002). Strategic Plan for 22 People with Disabilities. 23 24 State of Nevada Department of Human Resources (October 2002). Strategic Plan for 25 Provider Rates. 26 27 State of Nevada Department of Human Resources (October 2002). Strategic Plan for 28 Rural Health Care. 29 30 State of Nevada Department of Human Resources (October 2002). Strategic Plan for 31 Senior Services. 32 33 Washoe County Access to Health Care Network (draft 11/12/03). Five-Year Strategic 34 Plan: 2003-2008. Retrieved April 5, 2005 from www.wcahcn.org/strategic 35 36 37 38

Burns & Associates, Inc. III-1 May 5, 2006
Chapter III 1
Policy Brief on Focus Group Recommendation 2
Behavioral Health 3 4 5
I. RECOMMENDATION STATEMENT 6 7
Nevada will increase access to and funding for an appropriately designed mental 8 health and substance abuse program for Nevadans requiring these services. 9 10
II. OVERVIEW 11 12 Responsibility for the delivery of publicly-funded mental health and substance abuse (i.e., 13 behavioral health) services is shared among a number of different units within the 14 Department of Health and Human Services (DHHS), including: 15 16
Division of Mental Health and Developmental Services (DMHDS) 17 This Division is responsible for the overall administration of the behavioral 18 health system in Nevada and has the specific responsibility for the delivery of 19 mental health services to adults (18 years of age and older) with serious 20 mental illnesses (SMI). The Division also has specific responsibility to serve 21 children and adolescents with serious emotional disturbances (SED) in the 22 state’s 15 rural counties. The Division oversees the operation of two inpatient 23 psychiatric hospitals for adults as well as outpatient community-based 24 programs. It operates 21 community mental health centers of which 17 are 25 clinics in rural areas. 26
27 Division of Child and Family Services (DCFS) 28
This Division is responsible for the delivery of all services to children and 29 adolescents in the two urban counties and, as such, provides community-based 30 outpatient behavioral health and residential treatment services to children and 31 adolescents (under 18 years of age) with SED, most of who are in the child 32 welfare and juvenile justice systems. DCFS operates one inpatient psychiatric 33 facility, a residential treatment facility, and two community-based mental 34 health programs for children and adolescents – one in the north and one in the 35 south. The one in the south includes five neighborhood family service 36 centers. 37 38
Division of Health Care Financing and Policy (DHCFP) 39 This Division is responsible for overseeing the State’s Medicaid and SCHIP 40 programs, including the coverage and funding of behavioral health services 41 for eligible recipients. In addition to funding Medicaid covered services 42 provided by DMHDS and DCFS, the Division also contracts with two 43

Burns & Associates, Inc. III-2 May 5, 2006
managed care plans that are responsible for delivering some behavioral health 1 services to plan enrollees.1 2 3
Division of Health Services, Bureau of Alcohol and Drug Abuse2 (BADA) 4 This Division is responsible for the oversight and funding of community-5 based prevention, treatment and recovery support related to alcohol and drug 6 addiction. BADA provides no direct services, but contracts with community 7 providers. 8 9
There is a great need for behavioral health services in Nevada. Nevada has the highest 10 prevalence of mental illness in the Western United States with 5.4% of the population 11 living with a serious mental illness. In terms of substance abuse, Nevada has the nation’s 12 highest percentage of population reporting dependence on illicit drugs and the 8th highest 13 rate of past month binge alcohol use. 14 15 Yet despite the “need” for behavioral health services, Nevada’s service delivery system 16 has not been able to successfully meet the demand. Along with service infrastructure 17 issues (e.g., lack of providers), behavioral health funding has historically been low in 18 comparison to other states’ programs. 19 20 For example, on a national comparison based on FY 2003 expenditures, Nevada ranked: 21 22
37th in overall mental health spending and 36th in per capita expenditure ($63) 23 41st in state hospital spending and 42nd in per capita expenditure ($18) 24 33rd in community-based program spending and 29th in per capita expenditure 25
($44) 26 34th in the percentage of total mental health revenues from Medicaid (23%). 27
The national average was 39% with the highest percentage found in the State 28 of Washington at 87%. 29
30 Another example of the unmet need is contained in the prevalence study published by the 31 DMHDS in 2004. The study estimated that there were 55,700 residents with either SMI 32 or SED conditions in the Division’s service area. The study reported that only 23,800 33 (43%) of these individuals received services from the Division. 34 35 The Clark County Mental Health Consortium reports similar figures for Clark County 36 elementary school children in its 2004 report. Of the estimated 7,800 children with SED 37 that need services, only 37% received services, and of them, 83% were underserved. 38 39 Recognizing the need to enhance Nevada’s behavioral health delivery system, the State 40 has recently provided significant resources to the system. Examples of recent funding 41 initiatives include: 42
1 Enrollees who are SED or SMI may choose to opt out of managed care and receive traditional fee-for-service benefits. 2 This Bureau will be moving under the Division of Mental Health and Developmental Services in 2006.

Burns & Associates, Inc. III-3 May 5, 2006
Increasing funding for DMHDS mental health services. During the 2005 1 legislative session, DMHDS received a 47% funding increase ($91.4 million) 2 that provided: 3
4 – For Southern Nevada Adult Mental Health Services: medication clinic 5
services, residential support, psychiatric ambulatory services, the 6 opening of the new hospital and the addition of beds to two other state 7 facilities. Additionally, funding was provided for community 8 residential placements, overflow beds, a Mental Health Court in Clark 9 County and support for a community triage center. 10
11 – For Northern Nevada Adult Mental Health Services: medication clinic 12
services, community residential services, and psychiatric ambulatory 13 services. Additional funding was also provided to expand and support 14 the Washoe and Carson City Mental Health Courts and a triage center 15 for Washoe County. 16
17 – For Rural Clinics: medication clinic services and an increase in 18
outpatient services 19 20
Expansion of the Wraparound In Nevada (WIN) program to provide case 21 management and wraparound support to child welfare custody children with 22 SED 23
24 The implementation of the behavioral health redesign by DHCFP to change 25
the revenue flows and payment rules for behavioral health services. The 26 redesign increased the availability of community-based services. Included in 27 the redesign is the development of specialty clinics for the delivery of lower 28 level services and the expansion of the number of providers available. 29
30 The significance of the recent funding increase for DMHDS’s mental health services is 31 depicted below. Also revealed is the dependency of the Division’s mental health budget 32 on general fund monies. 33 34
DMHDS Mental Health Agencies Budget Sources - Selected Years
SFY 2005
SFY 2006
General Fund $ 69,237,137 78% $ 106,977,744 85% Federal Funds 10,033,870 11% 10,850,540 9% Fees 236,364 0% 940,942 1% Other 9,160,733 10% 7,780,093 6% Total $ 88,668,104 100% $ 126,549,319 100%
35 A similar depiction of funding sources for the DCFS mental health budget was not 36 available for this Policy Brief. 37 38

Burns & Associates, Inc. III-4 May 5, 2006
III. STRATEGIES 1 2 In order to increase access to and funding for an appropriately designed mental health and 3 substance abuse (i.e., behavioral health) program for Nevadans, the following strategies 4 were developed for the consideration of Summit participants: 5 6
1. Decrease number of persons with behavioral health conditions who 7 inappropriately utilize the Emergency Departments by a) increasing number 8 of available psychiatric beds, b) expanding the crisis support system, or c) 9 expanding on-going services. 10
11 2. Conduct a review of the current low level of Medicaid reimbursement in the 12
DMHDS mental health program. 13 14 3. Enhance home and community-based services for Medicaid eligible persons 15
with SMI by utilizing a) the new Medicaid State Plan option made available 16 through the Deficit Reduction Act of 2006 or b) the 1915(c) home and 17 community-based waiver option. 18
19 4. Enhance home and community-based services for Medicaid eligible children 20
and adolescents with SED with a new Medicaid demonstration grant 21 established under the Deficit Reduction Act or the 1915(c) home and 22 community-based waiver option. 23
24 5. Establish a long term target funding level for behavioral health services in 25
Nevada. 26 27
6. Restructure and unify the behavioral health system in Nevada. 28 29
These strategies were developed from the following “high scoring” recommendations 30 from the focus groups that addressed the behavioral health system: 31 32
1. Change current requirements related to mental health screening and medical 33 clearance for mental health patients presenting at the emergency room in order 34 to facilitate triage of these individuals to appropriate settings and services and 35 to reduce unnecessary utilization of emergency rooms. [Health Facilities] 36
37 2. Increase funding and access to appropriate placements and services for 38
individuals with mental health conditions. [Health Facilities] 39 40
3. Improve timeliness and appropriate utilization of emergency room services. 41 [Health Facilities] 42
43 The balance of this Policy Brief presents and discusses each of the strategies listed above. 44

Burns & Associates, Inc. III-5 May 5, 2006
1. Decreasing Inappropriate Emergency Department Usage 1 2 Hospital emergency departments (ED) across the country are facing increased pressure as 3 the number of ED visits continues to grow. In the past decade, ED visits have increased 4 by 26%. National health experts have attributed this growth to an increase in the 5 unwillingness of physicians to provide on-call coverage, an increase number of patients 6 using the ED as their source of primary care, and an increased number of patients with 7 serious mental illness (SMI) going to EDs. While the privately insured are still the 8 largest proportion of ED users, ED visits by Medicaid increased by 23%. 9 10 Overcrowded hospital EDs continue to be a serious health care challenge in Nevada, 11 especially with the State’s unprecedented population growth. Nevada hospital utilization 12 data shows an increase in the average number of ED visits per day from 1,959 in CY 13 2004 to 2,259 in the first quarter of CY 2005. 14 15 In January 2006 in Clark County, there were an average of 67 acutely suicidal or 16 homicidal psychiatric patients per day that were waiting on legal hold either in the ED or 17 in a hospital bed before being transferred to an inpatient psychiatric bed. These patients 18 waited an average of 4.6 days. 19 20 These long waits are attributed to both a shortage of psychiatric inpatient beds (Nevada 21 ranked 43rd nationally in number of state psychiatric beds per 100,000 in 2002) and 22 Nevada’s medical clearance law. This law (NRS 433A.165) requires persons with mental 23 health needs to be examined by a medical health care professional to determine if the 24 person has a medical problem prior to transferring the person to a mental health facility. 25 26 To date, Nevada has taken the following steps to address this “crisis”: 27 28
Relieving ambulance wait times in the EDs through the passage of SB 458 in 29 2005 which required hospitals to provide emergency services and care to 30 persons not later than 30 minutes after arrival at the hospital ED. 31
32 Increasing the number of psychiatric inpatient beds with the opening in 2006 33
of a new inpatient psychiatric hospital, the funding of beds in the Old 34 Hospital, in Building 1300, and providing for 50 “overflow” psychiatric beds 35 in Clark County. 36
37 Increasing the funding for crisis and emergency behavioral health services 38
including psychiatric ambulatory services which provide 24-hour emergency 39 walk-in services and psychiatric observation units. The increased level of 40 funding for the FY 06-07 biennium should provide services to approximately 41 6,000 clients. 42
43 Implementing a new service (mobile crisis) which in Clark County provides 44
evaluation services 10 hours a day, 7 days a week to persons who are on legal 45 holds. The teams evaluate between 300 and 400 clients a month with between 46

Burns & Associates, Inc. III-6 May 5, 2006
30% to 40% of those evaluated being diverted from inpatient care and 1 provided community services and supports. In the rural counties, the service 2 provides immediate mental health response to jails, hospitals and other 3 settings 24 hours a day, 7 days a week. 4
5 Despite these efforts, the Nevada Health Plan Project stakeholders continued to identify 6 this is an ongoing issue that needed to be addressed. Several possible strategies for 7 continuing the effort to decrease inappropriate use of EDs include: 8 9
Increasing the number of available psychiatric beds. This could involve: 10 11
– In the short term, paying for placement patients in vacant private 12 psychiatric beds 13
– Funding additional state-operated beds 14 – Incentivizing the private sector to add psychiatric beds to hospitals 15
through establishment of appropriate reimbursement rates 16 17 Expanding the crisis support system to relieve EDs of patients waiting for 18
inpatient psychiatric placements 19 20 Expanding ongoing services that have been shown to reduce readmissions to 21
inpatient psychiatric services 22 23
Reviewing and implementing as appropriate the Legislative Committee on 24 Health Care recommendations to the 74th Session (2007). Chapter 450B of 25 NRS requires DHHS, Health Division to conduct a study to identify the 26 causes of excessive wait times in EDs and submit a quarterly report to the 27 Legislative Committee on Health Care who in turn is to develop a final report. 28
29 Increasing the number of psychiatric beds. 30 31
There are three options under this possible strategy: 32 33
Paying for placement in vacant private beds. Two private psychiatric 34 inpatient facilities in the Las Vegas Valley have beds that are available for 35 overflow placements. For the purposes of this estimate, it is assumed that the 36 cost per day for each bed (with attending doctors) would be approximately 37 $615 per day (compared to approximately $425 per day at state-owned 38 facilities). The facilities report having a combined availability of between 24 39 and 27 beds that could be used to relieve the pressure on EDs. Therefore, the 40 cost estimate metrics under this option would be: 41
42 o Cost per day per bed: $615 43 o Cost per month per bed: $18,450 44 o Cost per year per bed: $224,475 45 o Cost per month for 25 beds: $461,250 46

Burns & Associates, Inc. III-7 May 5, 2006
o Cost per year for 25 beds: $5,611,875 1 2
Funding additional state-operated beds. Based on the capital and operating 3 appropriations for the Psychiatric Hospital at SNAMHS, it is assumed that the 4 capital costs per bed are approximately $290,000 with a daily per bed 5 operating cost of approximately $425 ($155,000 annually). Therefore, to add 6 an additional 100 beds, the costs are estimated to be: 7
8 o Capital costs (100 beds) $29,000,000 9 o Annual operating costs (100 beds) $15,512,500 10
11 Incentivizing the private sector to add psychiatric beds to hospitals through 12
the establishment of appropriate reimbursement rates. No specific cost 13 estimate is provided for this option. However, it should be noted that in the 14 above two options, if Medicaid eligible adults between the ages of 21 and 65 15 are placed, no Medicaid funding is available. The above two options use 16 facilities that are Institutes for Mental Disease (IMD). Under Medicaid rules, 17 no reimbursement is available for adults in IMDs. However, Medicaid 18 reimbursement is available for psychiatric beds in a general acute hospital, 19 even for adults. Such a situation presents the opportunity for the State to 20 increase its reimbursement rate to a level where no more state funds are 21 expended than at a state facility (say $425 per day), but with federal funds, the 22 hospital could receive a reimbursement level that may prove attractive. 23
24 Expanding Crisis Support System 25 26 Two crisis support services may relieve the EDs of patients that are potentially acutely 27 suicidal or homicidal and awaiting placement: Psychiatric Emergency Service and 28 Mobile Crisis Teams. 29 30 Psychiatric Emergency Services provides 24 hour emergency walk in services for people 31 in crises through the service’s Psychiatric Ambulatory Unit (PAS) and emergency 32 treatment in a 72-hour observation unit for persons in need of short-term observation, 33 stabilization and treatment in a secure environment through the Psychiatric Observation 34 Unit (POU). Together, these components deflect approximately 45% of the persons 35 receiving the services from inpatient admission. 36 37 Based on the appropriation for the FY 06-07 biennium, the PAS component costs 38 approximately $665 per client seen. To add an additional 6,000 clients to the service 39 would cost approximately $4 million. Again, using the FY 06-07 biennium 40 appropriation, the annual cost for a POU bed is approximately $325,000. This is a more 41 expensive per bed cost than either a state- or privately-operated inpatient bed. The cost to 42 add an additional 50 beds would be approximately $16.3 million. 43 The Mobile Crisis Team travels to the Las Vegas area EDs to evaluate psychiatric 44 patients that are waiting placement. If appropriate, the team can develop a discharge plan 45 and, if approved by the attending physician, have the patient discharged. It is uncertain 46

Burns & Associates, Inc. III-8 May 5, 2006
how many waiting patients this service has discharged from EDs, but the service operates 1 7 days a week from 7:00 AM to 10:00 PM. Based on discussions with DMHDS 2 personnel, the annual cost of a team is approximately $450,000. 3 4 Expanding On-Going Services 5 6 Based on a review of the DMHDS Performance Indicators, there are three services that 7 have a positive record of reducing the percentage of time that SMI clients spend in an 8 inpatient setting. These three services are Group Housing, the Program for Assertive 9 Community Treatment (PACT) and Intensive Supported Living Arrangements (SLA). 10 11 The Performance Indicators depict: 12 13
For Group Housing, the percentage of time that a client spends in an inpatient 14 setting falls from approximately 10% to approximately 2% after initiating 15 services. There are currently 382 clients in the program in the Las Vegas area. 16
17 For PACT, the percentage of time that a client spends in an inpatient setting 18
falls from approximately 15% to approximately 5% after initiating services. 19 There are currently 132 clients in the program in the Las Vegas area. 20
21 For Intensive SLA, the percentage of time that a client spends in an inpatient 22
setting falls from approximately 35% to approximately 5% after initiating 23 services. There are currently 25 clients in the program in the Las Vegas area. 24
25 At the present time it is not known if any of these three programs can absorb additional 26 caseload, or the cost to add additional clients. However, the Summit may wish to 27 consider the strategy of recommending programs that produce results such as these to 28 keep SMI clients stable and avoid situations where they appear in the ED at all. 29 30 31 2. Conduct a Review of the Low Level of Medicaid Reimbursement in the DMHDS 32
Mental Health Program 33 34 Based on a nationwide comparison of states’ revenue sources for behavioral health, the 35 Nevada percentage of FY 2003 revenue from Medicaid is much lower than the national 36 average (23% vs. 39%). According to that comparison, some of the highest percentages 37 of revenues from Medicaid are found in several nearby western states (e.g., Washington 38 at 87%, and Arizona at 69%). These states also have higher mental health per capita 39 expenditures (e.g., $91.01 and $126.33, respectively) than Nevada ($62.78). 40 41 In examining the budget by funding source for DMHDS for SFY 2005 and 2006, it is 42 difficult to see how the percentage of Medicaid funding reported in the above cited 43 national comparison can be achieved. The earlier presentation of the DMHDS budget 44 indicated that the percentage of federal funds was 11% in SFY 2005 and is 9% in SFY 45 2006. It is suspected that a considerable portion of these monies are made up of 46

Burns & Associates, Inc. III-9 May 5, 2006
Medicare and federal grant receipts. A detailed breakdown of the SFY 2005 DMHDS 1 expenditures by funding source is not available, but there is considerable evidence that 2 the amount of Medicaid funding is low, somewhere around $5.0 million. If that is true, it 3 would be difficult for total Medicaid expenditures for mental health services to be 23%. 4 5 If indeed the Medicaid reimbursement is low, the suspected cause would be a low 6 Medicaid enrollment rate for the SMI population. The insurance eligibility report for the 7 Division indicates that only 23% of the SMI and SED caseload has Medicaid eligibility. 8 9 The advantage that Medicaid offers from a state fiscal standpoint is that the State receives 10 federal match dollars for every dollar the State spends on covered services, delivered to 11 eligible individuals, by registered providers. For FY 2006, the federal match rate for 12 Nevada is 54.76% for Medicaid. 13 14 In order to maximize federal Medicaid funds, the State needs to ensure that all persons 15 who are potentially eligible for Medicaid apply and enroll. Ideally, enrollment should 16 occur (or final denials should be received) prior to the delivery of state-funded services. 17 18 However, since most SMI clients will likely qualify for Medicaid because they are SSI 19 eligible – and SSI determinations on average take 10 months (see the Medicaid and 20 SCHIP Policy Brief strategies) – this requirement may not be practical. In this instance, 21 it may be necessary to have an aggressive program to both qualify the SMI for eligibility 22 and to file retro-active Medicaid claims. 23 24 In addition to ensuring that the clients are Medicaid eligible, to claim Medicaid funds the 25 State must ensure that: 26
27 All behavioral health providers are registered Medicaid providers. Provider 28
registration and qualification with DHCFP is a federal requirement for 29 Medicaid reimbursement. It is unknown to what extent all providers of 30 services to the SMI are currently registered providers. 31
32 The services provided are Medicaid covered services. This means that the 33
array of behavioral health services covered by Medicaid should be broadly 34 defined. Many of the community services delivered to SMI appear to qualify 35 as Medicaid covered services3. Additionally, through the behavioral health 36 redesign, DHCFP has further increased Medicaid’s ability to fund support 37 services needed by individuals with behavioral health conditions. Medicaid 38 now covers the following behavioral health services for adults who are SMI: 39
40 – Targeted case management 41 – Mental health outpatient services including assessments, nuero-42
cognitive, psychological and mental status testing, mental health 43
3 An “Institute for Mental Disease” is not a covered service for an individual aged 21 to 65.

Burns & Associates, Inc. III-10 May 5, 2006
therapeutic interventions (e.g., partial hospitalization, intensive 1 outpatient, medication management, crisis intervention) 2
– Mental health rehabilitation services including basic skills training, 3 program for assertive community treatment, day treatment program, 4 family-to-family support services, peer-to-peer support services, 5 psychosocial rehabilitation, and treatment homes 6
– Outpatient alcohol and substance abuse services including therapies 7 and evaluations 8
9 The redesign has also expanded the types of providers who are allowed to bill 10 for services. 11
12 Provider always bill Medicaid for any covered service provided to a Medicaid 13
eligible person. 14 15 SMI are moved out of psychiatric hospitals (IMDs) as soon as possible 16
because, while residents, they are not eligible for Medicaid-financed 17 behavioral health services. 18
19 It is reasonable to assume that an additional number of the SMI could qualify for 20 Medicaid, especially given their disabling condition. Data published by DMHDS 21 indicates that 92% of the SMI caseload has an income below $16,000 per year. This is 22 approximately 160% of the FPL. 23 24 The Summit should consider adopting a strategy to develop a program to increase the 25 Medicaid coverage of the SMI population so that the Division can maximize as much of 26 its general fund expenditures with federal funds as possible. 27
If it is determined that it is not possible to enroll additional SMI under current eligibility 28 rules, the Division should consider pursuing other avenues to federalize SMI 29 expenditures (see next strategy). 30 31 Cost Estimate 32 33 If 80% of the SMI caseload would be eligible for Medicaid (up from an assumed level of 34 23%), and 75% of the community service dollars are used for Medicaid eligible services 35 by Medicaid registered providers, the Division could realize an approximate $8 million 36 increase in Medicaid funds. Since these funds would be a repayment of previously 37 expended state funds, these funds could in turn be used as Medicaid match. In the end, 38 the Division could increase expenditures by approximately $17 million without any 39 additional state appropriations. 40 41 In order to determine the extent to which the existing SMI caseload’s enrollment could be 42 increased, a preliminary study should be undertaken. This study could be performed by 43 existing state staff or the Summit may wish to recommend additional resources for the 44 study. If the outcome of the study is favorable, additional resources would be required to 45

Burns & Associates, Inc. III-11 May 5, 2006
perform the eligibility function. The amount required for this activity has not been 1 estimated. 2 3 4 3. Enhance Home and Community-Based Services for Medicaid Eligible Persons 5
With Serious Mental Illness 6 7 In FY 2005, DMHDS provided mental health services to approximately 27,400 8 Nevadans, the majority of which were clients with SMI. It did not provide services to an 9 estimated 27,000 additional residents that have an SMI condition. In addition to 10 expanding services to cover these individuals, increasing the use of home and 11 community-based services is a high priority for both consumers and the Division. 12 13 The Division has implemented programs that support a model of community care such as 14 an assertive community treatment program, mobile crisis teams, medication clinics, 15 supported employment programs and supported living arrangements. 16 17 As previously discussed (in Strategy 2 above) Nevada’s Medicaid program can serve as 18 an important funding source for clients enrolled in DMHDS programs. 19
20 Historically, many states (including Nevada) have been able to fund support services for 21 Medicaid recipients through the Medicaid State Plan. In order to do this, a state needs to 22 invoke the “rehabilitation service option”. However, given recent pronouncements by the 23 Centers for Medicare & Medicaid Services (CMS), there is a nationwide fear in state 24 Medicaid programs that coverage under the rehabilitation option will be limited in the 25 future. 26 27 There are, however, two other options that Nevada could pursue that would allow it to 28 enhance its community-based program for adults with SMI. These options would allow 29 the State to increase eligibility for adults with SMI and to expand the service array of 30 home and community-based services, for example to provide respite, prevocational and 31 supported employment. 32 33 The first of these two options has just recently become available under the Deficit 34 Reduction Act (DRA). The other option is to pursue a home and community-based 35 waiver for the SMI. A discussion of each of these options follows. 36 37 Home and Community-Based State Plan Option 38 39 Under the DRA of 2006, states are now allowed to offer home and community-based 40 services as a Medicaid State Plan option as opposed to needing to apply for a waiver. 41 42 Under this option: 43 44
Services are limited to persons with incomes up to 150% of the FPL 45 46

Burns & Associates, Inc. III-12 May 5, 2006
Individuals are not required to meet an institutional needs test in order to 1 receive home and community-based services 2
3 The scope of services may include any services permitted under the 1915(c) 4
waiver 5 6
A state can limit the number of individuals to be covered and the geographical 7 area in which services are provided 8
9 There must be a needs-based criteria and an independent evaluation to 10
determine an individual’s eligibility for the services. 11 12 The CMS has not yet issued guidance to the states as to how this new state plan option 13 will be implemented. 14 15 1915(c) Home and Community-Based Waiver 16 17 Under a 1915(c) wavier option, states can provide home and community-based services 18 to targeted populations at risk of institutionalization with incomes up to 300% of SSI 19 (221.5% of the FPL). The program can also be limited to a specific geographic region 20 and the number of waiver participants can be limited. 21 22 Approval of a waiver is contingent on a state being able to document the cost-neutrality 23 of the waiver. That is, costs under the waiver cannot be higher than the cost of the person 24 residing in an institutional setting. This requirement has created problems for many 25 states in their attempt to cover SMIs through a waiver. 26 27 The Medicaid statute specifically excludes coverage of individuals aged 21 to 64 in 28 institutions for mental diseases (IMD), and thus only SMI individuals under age 21 and 29 over 65 may receive waiver services. 30 31 However, Colorado was successful in obtaining a 1915(c) waiver for adults with a major 32 mental illness. Their waiver uses the nursing facility level of care as the institutional 33 standard. Through this waiver, they cover adult day care, alternative care facilities, 34 electronic monitoring, home modifications, non-medical transportation, respite care, 35 personal care and homemaker services. 36 37 Although pursuing a waiver is an option, it is unclear as to whether CMS would grant 38 such a waiver, particularly since a state plan option has been introduced under the DRA. 39 40 The Summit should consider one or both of the potential strategies outlined to increase 41 eligibility and to expand services under Medicaid for the SMI. 42 43 44 45 46

Burns & Associates, Inc. III-13 May 5, 2006
Cost Estimate 1 2 There are two items to consider in developing a cost estimate for this recommendation. 3 4 The first relates to investigating the option and performing cost and caseload estimates to 5 determine the fiscal impact of implementing the selected option. In the case of the DRA 6 state plan option, this will also entail closely monitoring the guidance from CMS with 7 respect to implementing the option. To execute this phase of the strategy, either existing 8 state staff, expanded state staff, or outside consultants could be used. At this time a 9 “placeholder estimate” of $200,000 is suggested. 10 11 The second item is the net costs to serve the SMI clients under the strategy. It is 12 presumed that utilizing one of the two strategies will result in savings to the State at a 13 constant caseload, no expansion of the service package, and the injection of additional 14 Medicaid funds. If that is indeed the case, it would be a policy decision whether to 15 increase enrollment, services, or both, as well as whether or not to add additional state 16 funds to significantly increase services. Summit participants may consider making a 17 recommendation with respect to the policy issues associated with the net state fiscal 18 impact. 19 20 4. Enhance Home and Community-Based Services For Medicaid Eligible Children and 21
Adolescents With SED 22 23 The provision of behavioral health services for children and adolescents with SED is a 24 shared responsibility between DCFS (who cares for children in the northern and southern 25 regions of the State) and DMHDS (who cares for children in the rural counties). 26 27 Nevada’s Medicaid and SCHIP programs play a more significant role in the funding of 28 behavioral health services for children than for adults. This is due to the fact that 29 children are eligible for Medicaid at higher family income levels than adults and foster 30 care children are covered under Medicaid. Additionally, behavioral health service 31 coverage for children and adolescents is broader since there is no IMD exclusion like 32 there is for adults, and children and adolescents have access to expanded services under 33 Early Periodic Screening, Diagnosis, and Treatment (EPSDT). 34 35 Through the behavioral health redesign, DHCFP has increased Medicaid’s ability to fund 36 support services needed by individuals with behavioral health conditions. Medicaid now 37 covers the following behavioral health services for children and adolescents who are 38 SED: 39 40
Inpatient mental health services and alcohol/substance abuse detoxification 41 and treatment for adults under 21 years of age 42
43 Targeted case management 44 Mental health outpatient services including assessments, nuero-cognitive, 45
psychological and mental status testing, mental health therapeutic 46

Burns & Associates, Inc. III-14 May 5, 2006
interventions (e.g., partial hospitalization, intensive outpatient, medication 1 management, crisis intervention) 2
3 Mental health rehabilitation services including basic skills training, day 4
treatment program, family-to-family support services, peer-to-peer support 5 services, psychosocial rehabilitation, treatment home 6
7 Outpatient alcohol and substance abuse services including therapies and 8
evaluations 9 10 The legislature and DCFS have expanded the Wraparound In Nevada Program (WIN), 11 which serves up to 500 children (and families) in the child welfare foster care system. 12 Based on a wraparound process model, WIN uses intensive case management, focuses on 13 individual case planning that is family-driven, and uses informal supports to reduce the 14 need for out-of-home placement. 15 16 An initial analysis of WIN youth compared to “traditional youth” (i.e., children that are 17 not in the waiver) showed: costs were lower for WIN youth, more WIN youth moved to 18 lower levels of care, and a greater percentage of WIN youth had improved functioning 19 levels (decrease in mental health symptoms). 20 21 While there is a strong commitment by the State to develop an effective home and 22 community-based program, there is still an “institutional component” to the behavioral 23 health delivery system for children with SED. Currently, DCFS maintains an inpatient 24 psychiatric facility with 58 beds, a state-operated residential treatment center with 16 25 beds, and places approximately 25 children and adolescents in out-of-state facilities. The 26 average length of stay for the children placed out of state is 18 months. 27 28 While there are some 500 children in WIN, many more children receive services through 29 the rehabilitation option under the State Plan. As noted in the previous strategy, there is a 30 fear that CMS may restrict coverage under the rehabilitation option. There are, however, 31 two other options that Nevada could pursue that would allow it to enhance its 32 community-based program for children and adolescents with SED. 33 34 As in the previous strategy discussion for the SMI, the first of the two options for SED 35 children and adolescents has just recently become available under the Deficit Reduction 36 Act. The other option, also paralleling the SMI strategy, is to pursue a home and 37 community based waiver for the SED. A discussion of each of these options follows. 38 39 Medicaid Grant to Move Children from Residential Treatment Centers into the 40 Community. 41 42 Under the Deficit Reduction Act, demonstration projects will be funded for up to 10 43 states to test the effectiveness of improving or maintaining a child’s functional level and 44 the cost-effectiveness of providing home and community-based alternatives to psychiatric 45 residential treatment services for children enrolled in Medicaid. This provision differs 46

Burns & Associates, Inc. III-15 May 5, 2006
from regular 1915(c) waivers in that, under those waivers, the standard of institutional 1 care that must be met is care in a hospital, nursing facility or ICF/MR. 2 3 Other than the institutional level of care standard, demonstration projects must apparently 4 follow the other requirements of the 1915(c) waiver program, including a demonstration 5 that the average costs of home and community-based services do not exceed the average 6 cost of residential child psychiatric treatment facilities. Participants in the demonstration 7 program will be eligible to continue to receive Medicaid reimbursable home and 8 community-based services following the termination of the demonstration, but no new 9 recipients can be enrolled. The demonstration will last for five years. States will be 10 selected through a competitive bidding process, with $218 million available for the 11 projects during FY 2007 - 2011. 12 13 Here again, CMS has not yet issued guidance to the states as to how this program will be 14 implemented. 15 16 1915(c) Home and Community-Based Waiver. 17 18 Under the 1915(c) waiver option, states can provide home and community-based services 19 to targeted populations at risk of institutionalization (e.g., inpatient psychiatric hospital) 20 with incomes up to 300% of SSI (221.5% FPL). Under the waiver, a state may exempt 21 parental income and look only at a child’s income, which means that children could 22 qualify who are not found in regular Medicaid and SCHIP (Kansas has done this.) 23 24 The program can be limited to a specific geographic region and the number of waiver 25 participants can be limited. Approval of a waiver is contingent on a state being able to 26 document the cost-neutrality of the waiver (that is, the cost of the waiver services cannot 27 be higher than the cost of the child residing in an institutional setting). For purposes of 28 this waiver, an institutional setting must be a hospital, intermediate care facility for the 29 mentally retarded, or a nursing home. For a 1915(c) waiver, institutional care does not 30 refer to a residential treatment center. 31 32 Four states (Indiana, Kansas, New York and Vermont) have been able to offer home and 33 community-based waiver services for children with SED by documenting the cost 34 neutrality of the waiver compared to the state’s hospital expenditures. 35 36 Cost Estimate 37 38 Similar to the cost estimate described in the strategy for SMIs, it is anticipated that if 39 SED children were placed in home and community services rather than an institutional 40 setting, the relative program costs would either be the same or be reduced. 41 42 The policy question that is presented is whether or not to expand the population that 43 would receive services. The Clark County Mental Health Coalition reported in 2004 that: 44 45

Burns & Associates, Inc. III-16 May 5, 2006
2% of the SED elementary school children in Clark County, that are in foster 1 care, did not receive any service 2
36% of the SED children and youth in the juvenile justice system received no 3 services 4
43% of the SED children and youth in the Clark County child welfare system 5 received no services 6
62% of the SED children in the Clark County schools did not receive any 7 service 8
9 As with the cost estimate for the SMI strategy, it left to the Summit participants to 10 recommend a policy strategy. If the grant or 1915(c) options are to be pursued, 11 additional resources to supplement state staff should also be considered by the Summit 12 participants. A “placeholder estimate” of $200,000 is offered. However, if this strategy 13 were pursued in conjunction with the SMI “exploration” strategy, some economies of 14 scale could be achieved. If a grant or waiver is received, additional funds would have to 15 be available for service. 16 17 18 5. Establish a Long Term Target Funding Level for Behavioral Health Services in 19
Nevada 20 21 Throughout this Policy Brief, there has been discussion of the number of residents with 22 SMI and children with SED who are not being served by the current system. There has 23 also been discussion regarding the low level of historical spending by Nevada relative to 24 the other states. While spending has increased in recent years, it may be useful for policy 25 makers and stakeholders to establish a target level of either service (say 75% of all SED 26 children) or expenditures (say 90% of the national per capita average) that can be used 27 for planning purposes. It would be equally useful to establish a timeline when the State 28 would hope to achieve the goal. 29 30 For example, if one half the SMI residents that are not receiving services were to be 31 provided services at the calculated SFY 2007 per individual served rate, the total cost 32 would be approximately $71 million. Similarly, if the State chose to reach the national 33 average per capita expenditure for mental health, the total increased cost would be 34 approximately $67 million. 35 36 Summit participants may want to consider recommending such a goal and timeline. 37 38 Cost Estimate 39 40 A “placeholder estimate” of $17 million in additional funds in SFY 09 and an additional 41 $17 million in each year through SFY 12 is proposed to achieve the $68 million needed 42 to meet the national average per capital expenditure on behavioral health. 43 44 45 46

Burns & Associates, Inc. III-17 May 5, 2006
6. Restructure and Unify the Behavioral Health System in Nevada 1 2 In 2002, President George W. Bush’s New Freedom Commission on Mental Health 3 identified fragmented delivery of mental health services as a major obstacle and 4 encouraged states to 1) facilitate new partnerships among governmental entities to better 5 use existing resources for persons with mental illness and 2) develop comprehensive 6 strategies to respond to needs and preferences of consumers or families. 7 Nevada’s current behavioral health system is extremely fragmented with a quilt work of 8 services, funding, and entry points and with multiple service delivery systems and 9 multiple agencies responsible for delivering the care. For example, a child who is 10 Medicaid eligible and residing in Clark County could receive behavioral health services 11 through a Medicaid health plan, through a DCFS clinic or through BADA for substance 12 abuse services. Once the child turns 18, a DMHDS clinic may provide services as 13 oppose to DCFS. 14 15 This type of fragmentation has serious consequences both for the client and their families 16 as well as for the funders of the system (e.g., lack of coordination and continuity of care, 17 lack of access to needed care, financial inefficiencies in terms of inability to maximize 18 federal Medicaid money, and purchase cost effective services, inability to effectively 19 monitor overall system performance and ensure accountability in terms of expenditures). 20 21 Additionally, recent studies have found that Nevada has a large numbers of individuals 22 with behavioral health conditions who are not currently being served in the system. 23 Developing a more effective and efficient system of care for persons with behavioral 24 health conditions would eliminate barriers to service and improve financial performance. 25 These efficiencies could allow the State to serve more of the individuals who are not 26 being served now. 27 28 With tighter resources, a growing demand for services and poor performing program 29 outcomes, numerous states (e.g., New Mexico, Arizona) have focused on system 30 redesigns in order to unify the delivery of behavioral health services in a more effective 31 whole. For example, the unifying of Philadelphia’s behavioral health system has 32 produced 1) significant savings that are being reinvested in a wide range of programs for 33 homeless persons, children in schools and other supports services, 2) increased access to 34 treatment, 3) better coordination of services across all jurisdictions and funding streams 35 and 4) greater accountability to consumers of services and their families and more 36 involvement in planning and monitoring services. 37 38 Similarly, in Nevada there has been a growing concern among behavioral health 39 stakeholders with regard to the fragmentation and lack of integration of Nevada’s 40 behavioral health service delivery model. This is exemplified by the findings and 41 recommendations set forth by: 42 43
The Nevada Mental Health Plan Implementation Commission. The 44 Commission recommended that the Governor provide for the development of 45 a comprehensive State Mental Health Plan that is designed to overcome the 46

Burns & Associates, Inc. III-18 May 5, 2006
problems of fragmentation in the mental health delivery system. Further, it 1 recommended that the Plan identify opportunities to leverage resources across 2 multiple agencies that administer both state and federal funds. The 3 Commission goes on to state that they envision s single entity coordinating the 4 plan. 5
6 The Clark County Mental Health Consortium. After completing an 7
assessment of the children’s behavioral health system in Clark County, the 8 Consortium identified the need for an integrated infrastructure to support 9 effective and accessible behavioral health service delivery. It recommended 10 that this infrastructure should include: public engagement and outreach, 11 system management, integrated access, collaborative service processes, 12 utilization management, workforce development, integrated financing and 13 ongoing utilization focused evaluation. 14
15 Building upon the recommendations of the focus group, the Summit participants may 16 wish to consider a strategy for a task force to develop a service delivery model that can 17 increase efficiencies, lead to better outcomes, allow more individual to receive services 18 and reduce the cost of care. Consideration should be given to developing a system in 19 which: 20 21
There is consolidated management responsible for overseeing the delivery of 22 behavioral health services to all individuals with behavioral health conditions 23 regardless of age, condition or geographical location (e.g., a single state entity, 24 behavioral health purchasing collaborative). 25
26 Services are driven by consumer choice, utilizing disease management 27
principles and evidence based practice models with an emphasis on 28 community care and the recovery focus of services. 29
30 Funding streams are integrated and follow the client, not the agency (e.g. as in 31
consumer directed or capitated service delivery models). 32 33 34 Cost Estimate 35 36 There is no specific cost estimate included for this strategy as the recommendation 37 offered for consideration is a redesign task force. Summit participants may want to 38 consider supplementing existing resources with additional funds for either expanding 39 available state resources or using the services of outside consultants. 40 41

Burns & Associates, Inc. III-19 May 5, 2006
Resources 1 2 Association of University Centers on Disabilities (February 17, 2006). Summary of the 3 Deficit Reduction Act of 1005 (PL 109-171) Excerpt from the Jan-Feb. Issue of the 4 ARC/UCP Disability Collaboration Washington Watch. Retrieved on April 6, 2006 from 5 http://www.aucd.org/Mediciad/DRA_Summary.htm 6 7 Bazelon Center for Mental Health Law (September 1999). Making Sense of Medicaid for 8 Children with Serious Emotional Disturbance. 9 10 Bazelon Center for Mental Health Law (July 1994). Making Medicaid Work to Fund 11 Intensive Community Services for Children with Serious Emotional Disturbance. 12 13 Center for Medicare & Medicaid Services (March 31, 2006). State Medicaid Director 14 Letters on Roadmap for Medicaid Reform – New Options to Support Individuals with 15 Disabilities and Long-Term Care Needs, New Options to Improve and expand Insurance 16 Coverage for Acute Care Needs, and Section 6044, State Flexibility in Benefit Packages. 17 Retrieved April 6, 2006 from http://new.cms.hhs.gov/SMDL/SMD/list.asp? 18 19 Community Behavioral Health. November 2003. City of Philadelphia Behavioral 20 Health System: A Brief History. Retrieved May 3, 2006 from http://www.phila-21 bhs.org/history.html. 22 23 Kenny, Holly, et al. (June 2002). Mental Health Services for Children: An Overview. 24 National Conference of State Legislatures: Children’s Policy Initiative 25 26 Medical Expenditure Panel Survey (January 2006). Expenses for a Hospital Emergency 27 Room Visit, 2003. Statistical Brief #111. 28 29 NASMHPD Research Institute. FY’03 Funding Sources and Expenditures of SMHAs: 30 Data Table. Retrieved April 9, 2006 from 31 http://www.nri-inc.org/RevExp/RE03/re03main.htm 32 33 NASMHPD Research Institute. State Mental Health Agency Profiling System: 2004 - 34 Nevada. Retrieved March 26, 2006 from 35 http://www.nri-inc.org/Profiles/StateProfileReportA.cfm 36 37 National Conference of State Legislatures (February 3, 2006). Deficit Reduction Act of 38 2005 – Summary of Medicaid/Medicare/Health Provisions. 39 40 National Governor’s Association (January 26, 2005). Funding for Children’s Mental 41 Health Services: Making the Most of Medicaid. NGA Center for Best Practices: Issue 42 Brief. 43 44

Burns & Associates, Inc. III-20 May 5, 2006
O’Malley, Ann S., et al. (November 2005). Rising Pressure: Hospital Emergency 1 Departments as Barometers of the Health Care System. Center for Studying Health 2 System Change Issue Brief: No 101. 3 4 Shirk, Cynthia (March 3, 2005). Rebalancing Long-Term Care: The Role of the 5 Medicaid HCBS Waiver Program. National Health Policy Forum. 6 Substance Abuse and Mental Health Services Administration. Mental Health and 7 Substance Abuse Services in Medicaid and SHCIP in Nevada. Retrieved March 26, 2006 8 from http://www.mentalhealth.samhsa.gov/Publications/allpubs/State_Med/Nevada.pdf 9 10 The Kaiser Daily Health Policy Report (March 29, 2006). Most People Seeking 11 Treatment in Emergency Departments Have Health Insurance, Study Says. Retrieved 12 March 29, 2006 from http://www.kaisernetwork.org/daily_reports/ 13 14 15 Nevada Specific Documents 16 17 Allen, Tina (June 2005). Healthcare Checkup: Managing Nevada’s Medical 18 Challenges. Nevada Business Journal. Retrieved January 1, 2006 from 19 http://www.nbj.com/articles/templates/default.aspx?a=81&z=7 20 21 Clark County Mental Health Consortium. July 2004. Third Annual Plan 22 23 Department of Health and Human Services, Division of Child & Family Services (April 24 7, 2005). White Paper: Transforming Children’s Mental Health Treatment Services in 25 Nevada. Retrieved March 29, 2006 from 26 http://www.dcfs.state.nv.us/Reports/TransformingChildrensMHWhitePaper040705.pdf 27 28 Department of Health and Human Services, Division of Health Care Financing and 29 Policy (2006). Behavioral Health Redesign. Retrieved March 24, 2006 from 30 http://dhcfp.state.nv.us/pdf%20forms/misc/Behavioral%20Health%20Redesign%202006.31 pdf 32 33 Department of Health and Human Services, Division of Mental Health and 34 Developmental Services. 2004 Mental Health Prevalence Report. 35 36 Department of Health and Human Services, Division of Mental Health and 37 Developmental Services (2002). Community Mental Health Services Block Grant Core 38 Monitoring Report. 39 40 Department of Health and Human Services, Division of Mental Health and 41 Developmental Services (2004). Facts About the New State Psychiatric Hospital in Las 42 Vegas Valley. 43 44 Department of Health and Human Services, Division of Mental Health and 45 Developmental Services (February 9, 2006). Presentation by Carlos Brandenburg, PhD, 46

Burns & Associates, Inc. III-21 May 5, 2006
Division Administrator to Nevada Legislative Committee on Health Care. Agenda Item 1 VIIa. 2 3 Department of Health and Human Services, Division of Mental Health and 4 Developmental Services (December 13, 2005). Status of Mental Health Services in the 5 Clark County Area. Presentation by Carlos Brandenburg, PhD, Division Administrator to 6 Nevada Legislative Committee on Health Care. 7 8 Department of Health and Human Services, Division of Mental Health and 9 Developmental Services. 2006 Needs Assessment. 10 11 Department of Health and Human Services, Division of Mental Health and 12 Developmental Services. 2006 Monthly Caseload Reports. 13 14 Department of Health and Human Services, Division of Mental Health and 15 Developmental Services. 2004 Monthly Caseload Reports. 16 17 Department of Health and Human Services, Division of Mental Health and 18 Developmental Services. MHDS General Financial Overview for Fiscal Year 2003. 19 20 Department of Health and Human Services, Division of Mental Health and 21 Developmental Services. MHDS FY 2004 Biennial Report. 22 23 Department of Human Resources, Health Division (2003 Edition). Healthy People 24 Nevada 2010. 25 26 Department of Human Resources, Division of Child & Family Services (December 31, 27 2004). Wraparound in Nevada for Children and Families: Program Accomplishments. 28 http://www.dcfs.state.nv.us/Reports/WIN%20Outcome%20Report%2012-31-04.pdf 29 30 Department of Human Resources, Division of Health Care Financing and Policy. 31 Summary Utilization Report for Nevada Medical Providers – Calendar 1Q2005 (interim 32 and Calendar Year 2004. Retrieved March 26, 2006 from 33 http://www.unlv.edu/Research_Centers/chia/utilizationandfinancial.htm 34 35 Fund for a Healthy Nevada (June 2003). Health and Wellness in Nevada: An Assessment 36 of Selected Aspects of Health Status and Health Service Capacity. 37 38 Karr, Donald, et al. (July 2005). How Nevada Stacks Up: National and Regional 39 Comparisons of Nevada’s Public Mental Health System. 40 41 Landreth, K et al (March 2006). 2006 Nevada Mental Health Problems and Needs. 42 Retrieved April 7, 2006 from http://mhds.state.nv.us/pdfs/MentalHealthProbs2006.pdf 43 44 Legislative Counsel Bureau (January 2005). Legislative Committee on Children, Youth 45 and Families. Bulletin No. 05-17 46

Burns & Associates, Inc. III-22 May 5, 2006
Legislative Counsel Bureau (January 2005). Nevada Mental Health Plan Implementation 1 Commission. Bulletin No. 05-8. 2 3 Legislative Counsel Bureau (March 7, 2005). Memorandum: Subcommittee Report on 4 Mental Health Issues. Retrieved March 24, 2006 from 5 http://leg.state.nv.us/lcb/research/publications.cfm 6 7 State of Nevada Senate Committee on Human Resources and Education (March 7, 2005). 8 Committee Minutes. 9 10 State of Nevada, Division of Mental Health and Developmental Services, Division of 11 Child and Family Services and Mental Health Planning Advisory Council (September 1, 12 2005). CMHS Block Grant Application for Federal Fiscal Year 2006. 13 14 State of Nevada, Department of Human Resources (June 2005). Division of Mental 15 Health and Developmental Services: 2nd Quarter FY2006 Performance Indicators. 16 Retrieved March 24, 2006 from 17 http://mhds.state.nv.us/pdfs/PerformanceIndicators2006.pdf 18 19 20

Burns & Associates, Inc. IV-1 May 5, 2006
Chapter IV 1
Policy Brief on Focus Group Recommendation 2
Health Care Professional Education 3 4 5
I. RECOMMENDATION STATEMENT 6 7
Nevada will improve and expand its capacity to provide a health care 8 professional education continuum to increase the number of licensed health care 9 professionals in the state. 10 11
II. OVERVIEW 12 13 When compared to other states, Nevada ranks near the bottom for the number of health 14 care professionals per 100,000 population in nearly every category. Moreover, there is a 15 significant disparity between Nevada’s ratio and the national averages. Examples 16 include: 17 18
Nevada ranks 48th with 196 physicians per 100,000 population compared to 19 the national rate of 262. 20
21 Nevada ranks 43rd among 46 states with medical schools in the number of 22
graduates in 2000, and graduated fewer new physicians per 100,000 23 population (2.8) than did the nation as a whole (6.4). 24
25 Nevada ranks 49th among the states with 604 nurses per 100,000 population 26
compared to the national rate of 825. 27 28
Nevada has one of the lowest per capita rates of nurse practitioners in the 29 nation at 15.2 per 100,000 population, well below the national rate of 33.7, 30 and ranks near the bottom of the states in the ratios of certified nurse 31 midwives and registered nurse anesthetists. 32
33 Nevada ranks 48th in the number of dentists per capita. 34
35 Nevada ranks 31st in the number of pharmacists and 42nd in the number of 36
pharmacy techs per capita. 37 38
Nevada ranks 44th in psychologists per capita and 48th in the number of social 39 workers per capita. 40
41 Historically, Nevada has depended in large part on attracting health care professionals 42 from other states. Efforts to develop capacity for educating the health care workforce 43 have not kept up with the State’s explosive population growth. A current inventory of the 44 health care professional education system includes: 45 46

Burns & Associates, Inc. IV-2 May 5, 2006
The University of Nevada School of Medicine (UNSOM) with an entering 1 class size of 52 students and 194 residents and fellows enrolled in 14 2 approved programs 3
4 Touro University College of Osteopathic Medicine with an entering class size 5
of 78 (and a capacity for 165) and 75 physician assistant students (with a 6 potential enrollment capacity of 120) 7
8 Eight approved Schools of Nursing with a total enrollment of 1,570 RN 9
students 10 11
Two community colleges offering LPN programs 12 13 Masters Degree in Nursing programs at UNR and UNLV and a PhD program 14
at UNLV with a combined total enrollment of 40 15 16 A Masters Degree in Nursing program at Touro with class size of 17 (and a 17
capacity for 90) 18 19 A School of Dental Medicine at UNLV with 300 doctoral students and 16 post 20
doctoral students 21 22 A School of Pharmacy at the University of Southern Nevada School with a 23
2005 entering class of 142 students 24 25
Schools of Public Health at both UNR and UNLV with combined enrollments 26 of 367 undergraduates and 172 graduate students 27
28 UNLV School of Health and Human Sciences programs in physical therapy, 29
health physics, kinesiology, nutrition sciences, clinical laboratory sciences and 30 radiology with a combined enrollment of 1,152 undergraduate and 120 31 graduate students 32
33 Other Social and Behavioral Sciences Programs at UNLV and UNR with 34
combined enrollments of 150 undergraduates and 40 graduate students 35
On March 17, 2006 a Strategic Vision and Plan for the University of Nevada Health 36 Sciences Center (UNHSC Plan) was presented for consideration to the Nevada Board of 37 Regents. The proposal was prepared by LarsonAllen, a consulting company retained by 38 UNSOM and Nevada System of Higher Education (NSHE). 39
The Strategic Vision and Plan defines the Health Sciences Center as “a University-based, 40 integrated set of health professional education and biomedical research programs, aligned 41 with supportive patient care programs.” The overview of the UNHSC Plan calls for the 42 following actions: 43

Burns & Associates, Inc. IV-3 May 5, 2006
Build a more complete School of Medicine by increasing class size, increasing 1 Graduate Medical Education (GME) program scope, strengthening 2 community relationships and partnerships, and increasing faculty depth and 3 breadth 4
5 Expand programs for nursing and other areas of the health professional 6
workforce by increasing the class size and scope of programs, establishing a 7 School of Pharmacy, increasing faculty and expanding community 8 relationships 9
10 Improve state health outcomes and community health by enhancing 11
community health education, research and service initiatives; focusing efforts 12 across UNHSC on distinct education, research and service initiatives and the 13 needs of Nevada; and collaborating with other agencies 14
15 Increase research and economic development by focusing research 16
investments, increasing faculty depth and breadth, building community 17 partnerships, and using UNHSC as an integrating vehicle 18
19 While the proposal to create a Health Sciences Center has the potential to expand and 20 advance health care professional education in Nevada, at this point it is still in the 21 conceptual stage. The collaborators who put forth the proposal are working on better 22 defining the initiative with more detail. The next iteration of the plan will be available in 23 the coming months. 24 25 III. STRATEGIES FOR HEALTH CARE PROFESSIONAL EDUCATION 26 27 There was considerable support for the Health Sciences Center in the focus groups. 28 Many participants saw the UNHSC as at least part of the solution to the shortage of 29 licensed health care professionals in the state. However, support of the UNHSC is not an 30 explicit strategy that is recommended for the Summit to consider, though if the 31 participants desire, it may emerge as a recommendation. 32 33 For the Summit, individual strategies were developed for consideration to expand 34 UNSOM, expand nursing programs, and to establish a pharmacy school. These strategies 35 are in concert with the initial UNHSC concept and can be adopted by the Summit without 36 adopting the as yet to be determined details of the UNHSC plan. 37 38 Therefore, to increase the number of licensed health care professionals in the state 39 through an expansion of the professional health care education, the following strategies 40 were developed for consideration of the Summit participants: 41 42
1. Expand UNSOM and the Graduate Medical Education (GME) program by: 43 a. Increasing core faculty 44 b. Expanding the GME program 45 c. Increasing the enrollment in the School of Medicine 46 47

Burns & Associates, Inc. IV-4 May 5, 2006
2. Expand public nursing school programs by: 1 a. Increasing faculty salaries 2 b. Doubling the enrollment at the public nursing schools 3 c. Funding necessary capital expenditures 4 d. Funding preceptor and clinical support 5 6
3. Start a School of Pharmacy and Pharmaceutical Services 7 8 4. Maximize Medicaid funding for GME 9 10 5. Expand scholarship opportunities to fund students seeking graduate and 11
undergraduate degrees in the health care professions 12 13 6. Expand state funding for the Area Health Education Centers (AHECs) to 14
support the education of health care professionals 15 16 These strategies were developed from the following “high scoring” recommendations 17 from the focus groups that addressed education of health care professionals: 18 19
Expand state funding for educational infrastructure – both operational and 20 capital. [Health Care Professional Education] 21
22 Create, endorse and fund an integrated health sciences center for statewide 23
research and training, including post-graduate education. [Health Care 24 Professional Education] 25
26 Develop and enhance the educational continuum to increase number of all 27
licensed professionals that are educated in the state. This includes increasing 28 class sizes for students/residents, improving infrastructure needed to support 29 the program (e.g., clinical sites, faculty, mentoring), developing rural training 30 tracks and post-graduate training. [Health Care Professional Education] 31
32 Tie funding for health care education to a systematically designed plan that is 33
based on the identified state health care workforce needs. [Health Care 34 Professionals] 35
36 Increase the number of instructors in health professional schools. This 37
includes looking at criteria needed to teach and providing funding for health 38 care instructors. (Also noted the need to increase recruitment of physicians 39 and other health care professionals as well as ensuring high retention rates). 40 [Facilities] 41
42 Refocus Millennium scholarships on health care professionals and educators. 43
[Health Care Professional Education] 44 45 The balance of this brief presents and discusses each of the strategies listed above. 46

Burns & Associates, Inc. IV-5 May 5, 2006
1. Expand the UNSOM and the Graduate Education Program 1 2 Based on data from the Nevada Office of Rural Health, it is estimated that 1,358 3 additional patient care physicians will be needed by 2015 to maintain Nevada’s current 4 172 physicians to 100,000 population ratio. In order to increase the ratio to the national 5 average of 222 by 2015, Nevada will need an additional 2,917 patient care physicians. 6 7 Nevada’s current educational system cannot produce this number of physicians. With a 8 class size of 52, UNSOM has one of the smallest medical school class sizes in the nation, 9 and the smallest compared with neighboring states of Arizona (107), Utah (104), and 10 New Mexico (76 increasing to 101 in 2011). 11 12 Additionally, the American Association of Medical Colleges places Nevada 46th in a 13 national ranking of the number of residents trained in each of the 50 states. Nevada 14 substantially lags behind its neighboring states in number of residency and fellowship 15 programs, total number of residents and fellows, and total number of faculty. 16 17 Moreover, UNSOM is heavily dependent on community-based physicians who act as 18 faculty. While this approach to providing faculty is appropriate for a small medical 19 school and has served Nevada well, it will not support a significant expansion of either 20 the School of Medicine or the GME programs. 21 22 The UNHSC Plan calls for substantial growth at UNSOM in three dimensions – class 23 size, GME and faculty. Building on this outline, strategies for the Summit were 24 developed in the same three components, but in a different configuration. 25 26 The strategies that have been developed for the Summit should be considered “place 27 holder” strategies until the UNHSC plan is further refined. Considerably more resources, 28 time and detail are being devoted to refining the UNHSC Plan than are available for the 29 professional education aspect of the Nevada Health Plan. However, the proposed 30 Summit strategies and the initial plans of the UNHSC are similar in terms of final results. 31 32 The table below illustrates the numbers of faculty, students and residents currently at 33 UNSOM compared to the strategies proposed for the Summit and those contained in the 34 initial UNHSC Plan. 35 36
Number of: Faculty Students Residents Current UNSOM Situation 189 208 194 Summit Strategy 445 384 329 Initial UNHSC Plan 500 384 444
Change from Current to Summit 256 176 135 Change from Current to UNHSC 311 176 250
37 38

Burns & Associates, Inc. IV-6 May 5, 2006
As more detailed information becomes available through the UNHSC planning process, 1 the increased numbers of faculty and residents contained in the proposed Summit strategy 2 will likely need to be adjusted. 3 4 The discussion below presents the three aspects of the strategy offered for consideration 5 by the Summit. 6 7 Increase Core Faculty 8 9 The UNHSC planning process examined the faculty to student and the faculty to resident 10 ratios of a number of UNSOM’s geographical peer medical schools. Those metrics 11 reveal that UNSOM’s ratios of 1.1 faculty to student and 1.03 faculty to resident were 12 significantly higher than the ratios of peer institutions. The peer institutions averaged .74 13 and .87, respectively. 14 15 As the UNHSC presentation materials point out, the development of a more robust 16 faculty should be the number one priority of any expansion of the medical school. The 17 proposed Summit strategy for core faculty expansion will bring the UNSOM ratios of 18 faculty to students and faculty to residents in line with UNSOM’s peer institutions. 19 20 The strategy proposes adding faculty until the ratios of .77 (students) and .89 (residents) 21 can be achieved with the existing levels of students and residents. The strategy 22 supplements the existing faculty at UNSOM (which is reliant on community-based 23 physicians) with a larger contingent of full time faculty. The new faculty will 24 supplement the research, teaching, and resident training programs at the school. 25 26 This component of the overall UNSOM strategy will increase the faculty by 81, bringing 27 total faculty to 270. 28 29 Cost Estimate 30 31 High level assumptions were used in compiling the cost estimate for this component. 32 These assumptions included the level of state support for each faculty member ($100,000 33 per year) and the amount and cost of space for research, clinical and support activities for 34 each faculty member. The results of these calculations can only be regarded as “place 35 holder” estimates. 36 37 The estimates indicate that the amount of state funding required to add 81 faculty 38 members to the UNSOM would be: 39 40
Annual faculty support: $ 8,100,000 41 One time capital, with 40% state support: $22,752,000 42
43 44 45 46

Burns & Associates, Inc. IV-7 May 5, 2006
Expand the GME Program 1 2 The UNHSC Plan calls for an expansion of the GME program as “the best way” to meet 3 the state’s workforce shortage. The importance of having a robust GME program is 4 supported by a National Conference of State Legislators study that shows that a majority 5 of generalist physicians and physicians in metropolitan areas practice in the same state 6 they complete their most recent GME training. 7 8 The UNHSC Plan recommends expanding or adding 15 new residencies and 20 9 fellowships over the next 12 years. The Nevada Hospital Association has proposed 10 expanding or adding 15 GME programs for residents and fellows. Consensus will have 11 to be achieved between UNSOM and the sponsoring hospitals on the specific GME 12 programs to be expanded or added, as well as the timetable for implementation. 13 14 In formulating a recommendation for expanding the GME program at UNSOM for 15 Summit consideration, the amount of support offered by the Nevada Hospital Association 16 (NHA) was examined. NHA has indicated its willingness to fund an additional $22 17 million in GME costs through its participating hospitals. Using this funding level and a 18 metric of $163,000 in annual hospital costs to support a resident in a hospital, the strategy 19 presented for consideration adds 135 residents to the UNSOM program. This will bring 20 the total number of residents to 329 (from 195) but is considerably short of the 444 21 contained in the UNHSC Plan. 22 23 It has been pointed out that it can take anywhere from four to eight years to fully 24 implement a GME expansion. One aspect that must be factored in is the length of time it 25 takes to receive accreditation from the Accreditation Council for Graduate Medical 26 Education (ACGME) which requires site visits and extensive reviews. During this 27 development time, a more precise estimate of the need and capacity for residents can be 28 developed. 29 30 When adding residents, it is necessary to add additional faculty as well. When adding 31 faculty, it is also necessary to add space. The proposed strategy, in addition to adding 32 135 resident positions, contains an additional 65 faculty positions. 33 34 Cost Estimate 35 36 As with the cost estimate for adding faculty, high level assumptions were used to 37 determine the level of state support necessary for adding residents and faculty to expand 38 GME. The same assumptions were used for both estimates, with the added assumption 39 that all operating costs of GME beyond faculty would be borne by the teaching hospitals. 40 As with the estimates for expanding faculty, the results of these calculations can only be 41 regarded as “place holder” estimates. 42 43 The estimates indicate that the amount of state funding required to add 135 residents and 44 65 faculty members to the UNSOM would be: 45 46

Burns & Associates, Inc. IV-8 May 5, 2006
Annual faculty support: $ 6,500,000 1 One time capital, with 40% state support: $18,355,000 2
3 Increase the Enrollment at UNSOM 4 5 As pointed out earlier in this brief, the existing class size at UNSOM will not provide the 6 number of physicians needed in Nevada. Neither will doubling the class size of the 7 School of Medicine. That is why other strategies are proposed for the Summit to 8 consider in attracting physicians to the state (see the Policy Brief on Planning). However, 9 doubling the class size of UNSOM will help to defray the physician shortage and is a 10 strategy that is included in the UNHSC plan. It is a strategy that Summit participants 11 should consider. 12 13 This doubling, as with the faculty expansion and the residency expansion, will necessitate 14 an increase in both faculty and space. 15 16 Cost Estimate 17 18 The “place holder” estimates that were derived for the doubling of the UNSOM class size 19 anticipate the addition of another 110 faculty as well as some 232,000 square feet of 20 space. This space addition includes classroom, research, clinical, administrative and 21 support space. As with the initial UNHSC estimate, the proposed strategy does not 22 include space for ancillary activities such as parking and student housing. The same 23 assumptions were used for this estimate as for the previous two estimates. 24 25 The estimates indicate that the amount of state funding required to add 176 students and 26 110 faculty members to the UNSOM would be: 27 28
Annual faculty support: $11,000,000 29 One time capital, with 40% state support: $37,438,000 30 31
Summary of UNSOM Initiatives 32 33 In summary, the strategy recommended for consideration by the Summit contains three 34 aspects: expand the core faculty, expand GME, and double the class size of UNSOM. 35 The “place holder” cost estimates for state support for the overall UNSOM strategy is: 36 37
Type of Cost Increase Faculty
Increase Residents Increase Students
State Appropriations
Expenditure Frequency
Salary & Related $ 8,100,000 $ 6,500,000 $ 11,000,000 $ 25,600,000 On Going Capital Requirements $ 22,752,000 $ 18,355,000 $ 37,438,000 $ 78,545,000 One Time
Increase Required $ 30,852,000 $ 24,855,000 $ 48,438,000 $ 104,145,000 38 39 40 41

Burns & Associates, Inc. IV-9 May 5, 2006
2. Expand Public Nursing School Programs 1 2 In 2003, the Legislature provided funding to double the enrollment in the Nevada public 3 Schools of Nursing. By 2005, most of the Schools had successfully reached that goal. 4 Enrollment increased from 623 in 2001 to 1,323 in 2004-05. 5 6 While the doubling of enrollment may have contributed to the movement of Nevada from 7 51st to 49th in the state ranking of RNs to population ratio, additional steps must be taken 8 for Nevada to have an adequate supply of nurses. 9 10 The UNHSC Plan contains estimates that illustrate the public Schools of Nursing will 11 have to double again in order to meet the nursing demand over the next 15 years. The 12 Nevada Hospital Association projects that Nevada will need 662 additional nurses each 13 year for the next 5 years to meet the demand. In testimony to the Interim Legislative 14 Committee, the Nevada Nurses Association stated that for the 2005-06 academic year, 15 nursing schools were able to accept only 546 out of 1,442 qualified applicants. 16 17 If nursing school enrollment is to be doubled, there are infrastructure improvements that 18 must be made before such a doubling can be undertaken. These infrastructure 19 improvements include nursing faculty salaries, rehabilitating existing facilities at some of 20 the nursing programs, and with the doubling of nursing enrollment, funding will have to 21 be available for preceptor and clinical support activities. 22 23 The following discussion examines these various aspects of the proposed Summit 24 strategy for nursing education expansion. 25 26 Increasing Faculty Salaries 27 28 First among the infrastructure elements required to double the public nursing school 29 programs in Nevada is the question of nursing faculty salaries. It has been reported that 30 there is substantial inequity in faculty salaries between the various nursing programs in 31 the state. The Board of Regents is reportedly studying this problem and expects to make 32 recommendations before the start of the legislative session. 33 34 However, Nevada should take a broader view of nursing faculty salaries. Nursing 35 programs must be taught by nurses and other professionals with at least a masters level of 36 education. Currently, there is a shortage of qualified faculty in the nation. The faculty 37 shortage is attributable to the scarcity of masters and higher level nurses as well as 38 competition from the private sector. If teaching positions are not competitive with 39 compensation in the private sector, attracting adequate faculty will be an ongoing 40 problem. 41 42 Compounding the difficulty of attracting faculty is the fact that 44 other states are 43 reportedly facing nursing shortages. While there are a variety of options available to the 44 states to alleviate these shortages, education and training are preeminent. Therefore, 45 there is likely to be an increased demand throughout the country for nursing faculty. 46

Burns & Associates, Inc. IV-10 May 5, 2006
Summit participants may want to consider a strategy that not only removes the current 1 inequity in nursing faculty salaries within Nevada, but expanding the salary question to 2 ensure that faculty salaries are competitive with both the private sector and with other 3 nursing programs throughout the country. 4 5 Doubling Public Nursing Program Enrollment 6 7 In the recent doubling of the nursing programs, the State provided for an increase of 8 approximately 681 nursing students. This required the addition of approximately 19 9 faculty to bring total faculty in the various programs to 108. 10 11 The strategy element for Summit participants to consider with respect to the doubling of 12 the public nursing enrollment program is estimated to provide for an additional 1,300 13 students and 108 additional faculty positions. 14 15 Providing Sufficient and Adequate Space 16 17 During the focus group process it was reported that some of the existing facilities used by 18 the nursing programs are old and in need of renovation. The strategy for consideration of 19 the Summit participants encompasses a renovation of existing space as well as providing 20 the space required to double the nursing enrollment. 21 22 Increasing Preceptor and Clinical Support 23 24 A key aspect of the nursing program is adequate clinical experience both while in school 25 and after graduation. The strategy for consideration for Summit participants anticipates 26 increasing the support necessary for these functions. 27 28 Cost Estimate 29 30 Detailed cost estimates for an expansion of the public nursing program are not available. 31 As mentioned above, the Regents are currently studying the question of equitable faculty 32 salaries between the nursing programs in the state. As also discussed above, the UNHSC 33 is in the process of refining the initial plan offered in March of 2006. It is anticipated that 34 the refinement will include estimates for expanding the nursing programs in the state. 35 36 In order to provide the Summit participants with a “placeholder estimate”, the budget 37 request for the original nursing program expansion was examined. Based on the metrics 38 used in that request, together with some assumptions, the following estimate has been 39 compiled: 40 41
Annual operating costs for the expansion: $10,000,000 42 One time equipment costs for the expansion: $ 1,500,000 43 One time capital costs for the expansion: $25,000,000 44 45

Burns & Associates, Inc. IV-11 May 5, 2006
At this time, it is anticipated that the amounts presented will cover the costs of all four 1 aspects of the nursing expansion strategy (increasing faculty salaries, doubling 2 enrollment, funding capital expenditures and providing for preceptor and clinical 3 support). More detail on these items should be available as the UNHSC planning process 4 proceeds. 5 6 3. School of Pharmacy and Pharmaceutical Services 7 8 Nevada currently has one private school of pharmacy at the University of Southern 9 Nevada (USN). With 1,500 applications a year (150 from Nevada residents), the 10 program currently accepts 140 students per year, with 40 to 45 coming from Nevada. In 11 addition Nevada, through the Western Interstate Compact on Higher Education 12 (WICHE), sends five students to attend out-of-state, publicly-supported colleges. 13 14 In 2000 and again in 2004, the Nevada Board of Regents approved plans to establish a 15 School of Pharmacy to be shared by UNR and UNLV. When fully developed, the 16 program would graduate 60 new pharmacists (Pharm.D.) a year. The plans for a 17 pharmacy school were not funded by the Legislature. 18 19 The UNHSC Plan released in March mentioned, but did not develop, the role that a 20 pharmacy school would play in the HSC. A pharmacy school may figure more 21 prominently in the next iteration of the UNHSC plan. 22 23 The current plans for a pharmacy school anticipate a program to be phased in over six 24 years, with an ultimate class size of 220 professional students and 60 Pharm.D. graduates 25 a year. It is anticipated that the first class will be graduating in 2012. 26 27 Summit participants may want to consider a strategy to establish and fund the School of 28 Pharmacy and Pharmaceutical Services. 29 30 Cost Estimate 31 32 The current plan for the pharmacy school presents a six year funding requirement. The 33 annual amounts of state support required to establish and operate the school are presented 34 below. 35 36
Year 1 $3.5 million 37 Year 2 $3.6 million 38 Year 3 $5.4 million 39 Year 4 $5.6 million 40 Year 5 $5.2 million 41 Year 6 $5.3 million 42
43 44 45 46

Burns & Associates, Inc. IV-12 May 5, 2006
4. Maximize Medicaid Funding of GME 1 2 Medicare has long been a primary source of funding for Graduate Medical Education. 3 However, in 1996 Medicare instituted a cap on the number of residents that it would 4 support and allocated the number of slots to the various states. The total number of 5 available resident slots has essentially been frozen at the 1996 counts. 6 7 This is a serious problem for states like Nevada that are experiencing rapid growth. 8 According to the Nevada Hospital Association, in 2004-05 there were 155.68 residents in 9 non-VA hospitals in Nevada while only 133.55 of those slots were Medicare approved. 10 This means that the teaching hospitals in the state had to absorb the full cost of over 22 11 residents during that year. 12 13 While Medicare is the largest payer nationally for the expenses of GME, Medicaid is the 14 second largest payer. In fact, it has been reported that the average state Medicaid GME 15 payments are about 8 to 9 percent of total Medicaid inpatient hospital expenditures while 16 Medicare’s GME payments represent only about 7 percent of its total inpatient hospital 17 expenditures. State Medicaid GME contributions range from less than 1 percent to a high 18 of 32 percent of inpatient costs. 19 20 In SFY 2004 Nevada’s Medicaid program provided approximately $820,000 in targeted 21 GME payments to the three teaching hospitals in the state: UMC, WMC and Sunrise. 22 23 There are three potential opportunities for Nevada Medicaid to expand its support for 24 GME. Nevada Medicaid can reconstitute the methodology it uses to pay hospital based 25 residency costs; it can potentially include nursing program educational costs in the GME 26 payment formula; and Nevada Medicaid can explore expanding its support for graduate 27 medical education that is delivered outside of the hospital setting. 28 29 Payments for Medicaid GME are permitted both under federal law and regulation. 30 However, the Centers for Medicare and Medicaid Services (CMS) has issued no 31 regulations concerning how Medicaid GME payments are to be made. As a result, states 32 are free to design their own reimbursement systems for GME, though these systems must 33 receive approval from CMS. 34 35 It should be noted that the increased GME funding contemplated for this option would 36 not benefit UMC. UMC currently receives Upper Payment Level (UPL) payments. 37 These payments implicitly include payment for the full share of Medicaid GME costs. 38 39 For basic GME payments to hospitals, Nevada uses a fixed amount of state funding and a 40 modified Medicare methodology. If the amount of state funding were increased, the 41 amount of Medicaid funding that could be provided to teaching hospitals could be 42 increased by as much as $680,000 through a methodology change that CMS has approved 43 for a number of states. To implement this change, DHHS would have to file and receive 44 approval for a State Plan Amendment. 45 46

Burns & Associates, Inc. IV-13 May 5, 2006
Another potential opportunity to increase GME payments concerns nursing program 1 costs. In a review of Medicare cost reports for the three teaching hospitals, it was noted 2 that none of the hospitals segregate the costs associated with the training of nursing 3 graduates. If these costs were separately reported, it may be possible to receive approval 4 from CMS for nursing GME payments. Such payments, as with the basic GME 5 payments, are limited to Medicaid’s share of the costs – most often derived by allocating 6 costs based on the number of bed days in a facility that are paid for by Medicaid. 7 8 The third opportunity for increasing GME payments concerns non-hospital facilities or 9 programs. Some states have reportedly been successful in getting approval from CMS 10 for these types of GME payments. Non-hospital facilities or programs may include 11 mental health programs and community health clinics. In order to seek CMS approval 12 for such a strategy, Nevada would have to determine the appropriate method of isolating 13 and identifying the GME costs and prepare an amendment to the State Plan for Medicaid. 14 15 To pursue these opportunities, Summit participants may want to consider the use of the 16 Nevada Medical Education Council. In 2003, the Legislature established the Medical 17 Education Council, modeled after a similar effort in Utah which obtained a substantial 18 amount of additional GME funding for that state. 19 20 The Nevada Medical Education Council is charged by the Legislature with: 21 22
Determining the workforce needs for the provision of health care in the state 23 and making recommendations to UNSOM and the Legislature regarding those 24 needs 25
26 Applying to CMS for GME monies and permission to distribute those monies 27
28 Applying for other grants, gifts and donations 29
30 Initiating a cooperative agreement with Department of Human Resources to 31
promote intergovernmental transfers 32 33
Distributing financial resources received by the Council 34 35 The Council would seem to be the appropriate body to manage efforts to increase 36 Medicaid GME payments. The Council could also pursue either a CMS waiver or seek a 37 federal statutory change to increase Nevada’s Medicare GME cap based on the state’s 38 rapid population growth. 39 40 Cost Estimate 41 42 The cost estimate for increasing Medicaid support of GME has been limited to the sub-43 strategy of changing the current formula used to pay basic GME. 44 45

Burns & Associates, Inc. IV-14 May 5, 2006
Based on a calculation of potential GME payments for the two teaching hospitals that 1 could benefit from the new formula (WMC and Sunrise), it is estimated that total GME 2 payments could increase by approximately $677,000. This would necessitate an increase 3 in state funding of approximately $300,000. 4 5 A cost estimate for the other sub-strategies discussed above cannot be performed because 6 there is insufficient data available at the present time. This data could be developed by 7 state staff resources or the Summit may wish to recommend additional resources to either 8 supplement state staff or retain the services of an outside consultant. 9 10 5. Expand Scholarship Opportunities 11 12 The focus groups recommended refocusing the Millennium Scholarships to health care 13 professionals and educators. The Scholarships are currently available to every Nevada 14 high-school senior with a B average or better to continue their education at a Nevada 15 University or College. 16 17 Funding for the Millennium Scholarship Program comes primarily from the tobacco 18 Master Settlement Agreement. In addition to the Tobacco Settlement monies, the Nevada 19 Legislature in 2005 provided a general fund appropriation of $35 million to the trust fund 20 and designated $7.6 million from Unclaimed Property revenue each year starting in SFY 21 2007. 22 23 In 2002, UNR’s Center for Applied Research studied the program. The study looked at 24 the first two years of the program and found that: 25 26
10,077 (66%) of high school graduates eligible for the program utilized the 27 scholarship 28
High school students and parents felt the scholarship had a positive impact of 29 student efforts 30
73% of the recipients said the scholarship effected their choice of colleges 31 58% stated they would not have been able to attend college without the 32
scholarship 33 34
The most recent data from the State Treasurer’s Office shows that 18,108 students 35 utilized Millennium Scholarship funding in the fall of 2005. Total scholarship payments 36 were over $15 million. 37 38 With the popularity and rate of utilization of this program as it is currently configured, it 39 would not appear to be prudent to restructure it. Moreover, undergraduate students 40 preparing for careers in health care are eligible to receive assistance if they meet the 41 qualifications. As an alternative, the Summit participants may want to consider the 42 creation of new loan repayment programs for those health care professionals that are 43 willing to practice in medically underserved areas. A discussion of this option is 44 contained in the Policy Brief on Planning. 45 46

Burns & Associates, Inc. IV-15 May 5, 2006
6. Expand State Funding for AHECs 1 2 Area Health Education Centers (AHECs) are academic-community partnerships serve a 3 number of functions including: 4 5
Training health care providers in sites and programs that are responsive to 6 state and local needs 7
8 Providing health career education and recruitment programs targeted to K-12 9
students 10 11
Linking the resources of university health science centers with local planning, 12 educational and clinical resources to provide multidisciplinary educational 13 services to improve health care delivery in underserved areas 14
15 Nevada has three AHECs: 16 17
AHEC of Southern Nevada serving Clark, Esmeralda, Lincoln and Nye 18 Counties 19
20 High Sierra AHEC serving Carson City, Douglas, Lyon, Storey and Washoe 21
Counties 22 23
Northeastern Nevada AHEC 24 25 Southern Nevada and High Sierra each receive approximately $80,000 in federal funding. 26 Northeastern Nevada is not a federally recognized AHEC and therefore operates under 27 the auspices of the UNSOM Office of Rural Health. The State currently appropriates 28 $300,000 to $400,000 annually that is used by the AHECs to leverage federal grant 29 money. 30 31 The Nevada AHECs participated in the effort to double nursing school enrollment by 32 contributing funding for the nursing programs in the two rural colleges. The 33 Northeastern Nevada AHEC also built the new medical and dental clinic in Elko that is 34 used for medical and dental student rotations. 35 36 Initiatives that could be implemented by AHECs with expanded state funding include: 37 38
1. Expanding the high school health career awareness and recruitment program 39 2. Enhancing salaries for preceptors and clinical supervisors 40 3. Upgrading telemedicine equipment 41 4. Covering continuing education costs for faculty 42
43 Summit participants may wish to consider including increased state support for the state’s 44 three AHECs. 45
46

Burns & Associates, Inc. IV-16 May 5, 2006
Cost Estimate 1 2 A “placeholder estimate” of the increased cost to the state for support of the AHECs is 3 $500,000. 4
5

Burns & Associates, Inc. IV-17 May 5, 2006
Resources 1 2 Accreditation Council for Graduate Medical Education (ACGME). List of accredited 3 programs by states. Retrieved April 1, 2006 from 4 http://www.acgme.org/adspublic/report/program_sponsor_list.asp 5 6 Amednews.com (January 2006). Innovative Funding Opens New Residency Slots. 7 Retrieved April 4, 2006 from http://www.ama-assn.org/amednews/site/free/prl20130.htm 8 9 Bruccoleri, Rebecca E. (2005). Graduate Medical Education Funding. Retrieved March 10 21, 2006 from www.amsa.org/pdf/Medicare_GME.pdf 11 12 Council on Graduate Medical Education (July 2004). State Managed Care Support for 13 Graduate Medical Education: Innovations and Implications for Federal Policy. 14 Retrieved March 20, 2006 from http://www.cogme.gov/ManagedCareReport.pdf 15 16 HRSA Bureau of Health Professionals (2005). The Nevada Health Workforce: Highlights 17 from the Health Workforce Profile. Retrieved April 2, 2006 from 18 http://bhpr.hrsa.gov/healthworkforce/reports/statesummaries/nevada.htm 19 20 HRSA Bureau of Health Professionals (2004). State Health Workforce Profiles 21 Highlights from the 2000 Profiles. Retrieved April2, 2006 from 22 http://bhpr.hrsa.gov/healthworkforce/reports/profiles 23 24 Henderson, Tim (December 2003). Medicaid Direct and Indirect Graduate Medical 25 Education Payments: A 50-State Survey. 26 27 National Governors’ Association Center for Best Practices (September 1999). State 28 Graduate Education Financing Reform Efforts. Issue Brief. Retrieved March 23, 2006 29 from 30 http://www.nga.org/portal/site/nga/menuitem.50aeae5ff70b817ae8ebb856a11010a0/ 31 32 National Rural Health Association (February 1998). Funding Graduate Medical 33 Education. Retrieved April 2, 2006 from 34 http://www.nrharural.org/advocacy/sub/issuepapers/ipaper1.html 35 36 Needleman, Jack et al. (January/February 2006). Market Watch Nurse Staffing in 37 Hospitals: Is There a Business Case for Quality? 38 39 40 Nevada Specific Documents: 41 42 Black, Lisa (January 10, 2006). The State of the Nursing Profession in Nevada. Exhibit 43 CC, Nevada Legislative Committee on Health Care. 44 45

Burns & Associates, Inc. IV-18 May 5, 2006
Bowles, Cheryl and Candela, Lori (Journal of Nursing Administration 2005). First Job 1 Experiences of Recent RN Graduates. 2 3 Board of Examiners for Alcohol, Drug, and Gambling Counselors (February 2006). 4 Information on Alcohol and Drug Abuse Counselors. Agenda Item X A, Nevada 5 Legislative Committee on Health Care. 6 7 Board of Examiners for Social Workers (February 2006). Nevada Social Workers 2005. 8 Agenda Item X D, Nevada Legislative Committee on Health Care. 9 10 Board of Medical Examiners (January 2006). “2005 Licensure Numbers.” Exhibit V, 11 Nevada Legislative Committee on Health Care. 12 13 Center for Education and Health Services Outreach, Area Health Education Centers. 14 Retrieved April 19, 2006 from http://www.unr.edu/med/dept/CEHSO/ahecs.html 15 16 Center for Education and Health Services Outreach (April 2006). Outline and Budget 17 Enhancement Request Form. 18 19 Las Vegas Review Journal (July 2005). Coming Up Short: Nevada Struggles to Meet 20 Patients’ Needs. Retrieved March 26, 2006 from 21 http://reviewjournal.printthis.clickability.com 22 23 LarsonAllen (March 2006). University of Nevada Health Sciences Center, Strategic 24 Vision and Plan. 25 26 LarsonAllen (April 2006). University of Nevada Health Sciences Center, Initial Draft: 27 Subject to Revision, HSC Visioning Model (SOM), Key Model Assumptions. 28 29 McDonald, John A. (September 2006). Strategic Planning for the University of Nevada 30 Schools of Medicine and the Nevada Health Sciences Center. 31 32 Nevada Hospital Association (March 2006). Nevada Hospital Industry Report, 33 Governor’s Commission on Medical Education, Research and Training. 34 35 Nevada State Board of Dental Examiners (January 2006). Exhibit Q, Nevada Legislative 36 Committee on Health Care. 37 38 Nevada State Board of Osteopathic Medicine (January 2006). Amended Testimony-Active 39 Instate License Distribution. Exhibit F, Nevada Legislative Committee on Health Care. 40 41 Office of the State Treasurer (March 2003). Millennium Scholarship Baseline Study. 42 43 Packham, John and Griswold, Mary Tabor (April 2005). Health Care and Health Care 44 Education Opportunities in Nevada, 2005 Edition. 45 46

Burns & Associates, Inc. IV-19 May 5, 2006
Regulatory Economics, Inc. (June 2004). A Win-Win Solution Focusing on Nurse 1 Retention to Improve Hospital Profits and Quality Patient Care in Nevada. 2 3 Ruchala, Patsy L. (January 2006). Testimony before the Nevada State Legislative 4 Committee on Health. Exhibit L, Nevada Legislative Committee on Health Care. 5 6 State Board of Nursing (January 2006). Nevada State Board of Nursing Annual Report 7 2004-2005. Exhibit X, Nevada Legislative Committee on Health Care. 8 9 Touro University (January 2006). Touro University Nevada College of Medicine, College 10 of Health & Human Services. Retrieved March15, 2006 from 11 www.leg.state.nv.us/73rd/Interim 12 13 University and Community College System of Nevada, Office of Academic and Student 14 Affairs (December 2004). Status Report on The Revised Nursing Plan. 15 16 University of Nevada School of Medicine (January 2006). The University of Nevada 17 School Of Medicine’s Report to Governor Guinn’s Commission on Health Care. 18 19 University of Nevada School of Pharmacy and Pharmaceutical Sciences (April 10, 2006). 20 Planning Document School of Pharmacy Managed and Taught Jointly by UNR and 21 UNLV. 22 23 University of Utah, Health Sciences Center (June 2005). Clinical Faculty Associates 24 Model. Retrieved March 26, 2006 from http://www.nurs.utah.edu/cfa/index.htm 25 26 Welch, Bill (February 2006). Hospital Industry Report to the Legislative Committee on 27 Health. 28 29

Burns & Associates, Inc. V-1 May 5, 2006
Chapter V 1 Policy Brief on Focus Group Recommendation 2
Small Employer Health Insurance and the Safety Net 3 4 5
I. RECOMMENDATION STATEMENT 6 7 Nevada will develop mechanisms to provide coverage for the small employer 8 market and for individuals who are uninsurable. In addition, the State will 9 improve access to services for both the insured and uninsured by supporting and 10 expanding the safety net provider network. 11
12 II. OVERVIEW 13 14 This policy brief presents a discussion of the issues relating to the small employers’ 15 access to and affordability of health insurance, the individual insurance market, and the 16 care provided through safety net programs. Safety net providers are those providers who 17 deliver health care services regardless of the patient’s ability to pay. Individual strategies 18 identified through the focus group process are analyzed, along with examples of 19 strategies implemented in other states. 20 21 Nevada’s explosive population growth continues to fuel a thriving economy. The State’s 22 unemployment rate of 3.8% is one of the lowest in the nation. The Nevada Workforce 23 Informer estimates that statewide job growth will exceed 40% between 2002 and 2012. 24 Job growth in Nevada’s two largest employment sectors, services and construction, will 25 increase at even faster rates. 26 27 As in other states, there is a mix in the size and types of employers. The largest 28 employers, those with over 100 employees, are predominantly in the gaming industry. 29 But 73% of all Nevada employers are small, with fewer than 50 employees. 30 Approximately 25% of the State’s workers are employed in companies with less than 50 31 employees. 32 33 The vast majority of Americans receive health insurance through their employers. The 34 size of the employer is a key factor in determining the cost of insurance, both to the 35 employers and their employees. Large groups have lower premiums because they can 36 divide the cost of claims for the group among a large number of people. In a small 37 group, one employee with high medical claims can have a significant impact on the 38 employer’s cost of insurance. Small employers also incur higher administrative costs 39 both because they are small, and because they typically work through a broker. Broker 40 commissions, which range from 2 – 8%, are usually added to premiums. As such, cost is 41 the largest barrier to small employers offering insurance to their employees. 42 43

Burns & Associates, Inc. V-2 May 5, 2006
Over the past five years, the cost of employer-sponsored coverage has increased 59%1. 1 Between 2002 and 2003, health care premiums rose 13.9%, and again by 11.2% in 2004, 2 while the rate of inflation increased only 2.5%2. In contrast, wages increased only 3 increased 2.2%. Increases in premium rates are pricing an increasing number of small 4 businesses out of the insurance market. Firms do have the option of requiring employees 5 to bear more of the cost of health care coverage, but in doing so may make the cost of 6 insurance beyond the reach of the employee. 7 8 More than a decade ago, Nevada attempted to address the cost of small group insurance 9 by allowing insurance companies and health plans to offer small employers a basic 10 benefit plan. The premiums on this product were thought to be lower, largely because it 11 was exempt from the state-mandated benefits laws. It was also exempt from premium 12 taxes. Unfortunately, due to a very low take-up rate, the legislation was repealed shortly 13 after it was enacted. At least two factors have been cited for the very poor take-up rate. 14 The law limited the broker commission to 2% on these policies and, as a result, brokers 15 had little incentive to “push” the product. Also, the rollout of the product was not 16 accompanied by any sort of marketing campaign. 17 18 Federal efforts to reform the small group market resulted in enactment of the Health 19 Insurance Portability and Accountability Act (HIPAA) in 1996. The key provisions of 20 HIPAA required states to adopt a series of insurance reforms designed to improve the 21 availability and affordability of insurance products for small employers. HIPAA set a 22 floor for rating restrictions, required guaranteed availability, and guaranteed renewal of 23 policies in the small group market. As a result of HIPAA, small employers can access 24 health insurance coverage. The cost of that coverage remains the primary barrier. 25 26 In January 2005, the Legislative Committee on Health Care, Subcommittee to Study 27 Health Insurance Expansion Options issued a report identifying the Health Insurance 28 Flexibility and Accountability (HIFA) waiver as a means to expand insurance to small 29 employers. The original intent of this initiative was to target small employers (2-50 30 employees) by offering a subsidy paid with state and federal funds. The subsidy would 31 be available for the working uninsured with incomes below 200% of the federal poverty 32 level (FPL). 33 34 Unfortunately, the recently enacted Deficit Reduction Act placed restrictions on the use 35 of the federal funds Nevada was to use for the subsidy. The legislation prohibits the use 36 of SCHIP funds for childless adults. This effectively negated the State’s effort to target 37 small employers with the use of leveraged federal funds. 38 39 The State has redirected its HIFA waiver to target the population of working uninsured 40 that are parents, and whose children are currently covered by Medicaid or Nevada Check 41 Up (200% of the FPL). 42 43
1 Employer Health Benefits Annual Survey 2004 (September 9, 2004). 2 Kaiser Family Foundation and Health Research and Educational Trust (HRET)

Burns & Associates, Inc. V-3 May 5, 2006
As small employers are forced to drop or not offer insurance because of the cost, their 1 employees join the ranks of the uninsured. There are approximately 426,000 uninsured 2 in Nevada. Of this number, it is estimated that 83% are in households that have a full or 3 part-time worker. As this population grows, it is more and more likely to turn to the 4 safety net system for access to health care services. Because of the state’s provider 5 shortage, the safety net system fills gaps for both the insured and uninsured. In Nevada, 6 the safety net system is largely comprised of: 7 8
Community Health Centers 9 University Medical Center and Rural Public Hospitals 10 County Indigent Fund Programs 11
12 The safety net strategies discussed in this brief focus on the Community Health Centers 13 (CHCs). There are two CHC systems in the state-- the Nevada Health Centers Inc. and 14 Health Access Washoe County (HAWC). These CHC systems provide services through 15 28 facilities across the State offering a range of medical, behavioral health and dental 16 services. 17 18 The CHCs provide services in every age, income, and ethnic demographic range. Their 19 clients are both uninsured and insured, with the insured being covered by group, private 20 and public programs such as Medicare and Medicaid. In 2004, the CHCs served 55,588 21 Nevadans. By 2005, the CHCs served 67,904 Nevadans, an increase of 22%. These 22 clients utilized 170,903 total visits of care, reflecting the increased pressure on the safety 23 net system. Of the total visits, 53% were utilized by the uninsured, 23% were utilized by 24 people enrolled in Medicaid, and the remaining 24% were utilized by people who had 25 either Medicare coverage or private insurance. The total annual operating cost of the 26 two systems is approximately $20.6 million. 27 28 Within the uninsured population is another segment which must be considered separately 29 in developing strategies for coverage. This group is the uninsurable, or those who cannot 30 access health insurance coverage due to the severity of their medical condition. A 31 portion of this group has jobs, potentially in small firms which do not offer coverage. 32 Their incomes usually exceed the thresholds for public programs. 33 34 Only four states require insurers to issue policies in the individual market (known as 35 guaranteed issue) making coverage available to the uninsurable. Medical underwriting, 36 in most instances, would set premiums far above an individual’s ability to pay. 37 38 Expanding the affordability of insurance for small employers, finding innovative ways to 39 enhance or expand the safety net provider network, and providing for a high risk pool 40 offer significant opportunities to ensure Nevadans are able to receive health care services. 41 42 43

Burns & Associates, Inc. V-4 May 5, 2006
III. STRATEGIES 1 2 In order to improve affordability and availability of health insurance in the small group 3 market, provide access to coverage for the uninsurable, and to increase access to health 4 care services by enhancing the safety net, the following strategies were developed for 5 consideration of Summit participants: 6 7
1. Provide employers information on small group rating practices to allow them 8 to make informed decisions regarding health care coverage. 9 10
2. Create a standardized product that insurance companies will offer to small 11 employers that: 12
13 a) standardizes the benefit package offered in the small group market, or 14 b) both standardizes the benefit package and makes the package more 15
affordable, or 16 c) both standardizes the benefit package and limits premiums that can be 17
charged. 18 19
3. Provide subsidies for insurance either to the population at large or to small 20 employers. The subsidies can be through either: 21
22 a) direct premium subsidies or 23 b) reinsurance for a standardized product. 24
25 4. Allow small employers to buy into the state employee insurance program. 26
27 5. Establish a high-risk pool for the uninsurable. 28
29 6. Establish a universal coverage program for Nevada. 30
31 7. Improve access to health care services for the both the uninsured and the 32
insured through expansion of safety net provider networks. 33 34
8. Foster local community efforts to offer services to the uninsured through 35 leadership and planning grants. 36
37 9. Increase funding for Senior Rx and Disability Rx programs. 38
39 The first four strategies are directly or indirectly focused on increasing insurance 40 coverage in the small employer sector, the fifth strategy addresses the uninsurable and the 41 sixth strategy addresses all of the uninsured. The last three strategies address the 42 improvement of access to health services rather than coverage. 43 44 These strategies were developed from the following “high scoring” recommendations 45 from the focus groups that addressed these topics: 46

Burns & Associates, Inc. V-5 May 5, 2006
1. Improve opportunities for small employers to offer employee health care 1 coverage (e.g., greater product flexibility). [Medical Coverage] 2
3 2. Develop strategies to ensure access to coverage for the uninsurable. [Medical 4
Coverage] 5 6
3. Preserve county safety-net programs. [Public Health] 7 8 4. Develop primary care and prevention services in order to ease the burden on 9
tertiary care facilities, especially in underserved areas and to ensure a 10 culturally sensitive, holistic approach to caring for patients. (Health 11 Professionals) 12
13 5. Increase funding for the Senior Rx and Disability Rx programs. 14
[Pharmaceutical Coverage] 15 16 The balance of this policy brief presents and discusses each of the strategies outlined 17 above. 18 19 1. Provide Employers Additional Information on Rating Practices 20 21 Small employers are at a disadvantage when shopping for health insurance: they often 22 lack full-time human resources staff to do research and comparisons on the choice of 23 policies. Providing information to enable them (and their brokers) to be more prudent 24 purchasers may have the effect of lowering premiums. 25 26 The types of information which would benefit small employers when evaluating 27 insurance options include: 28 29
Medical Loss Ratio - the percentage of total premiums that are used to pay 30 medical claims; 31
Base Rate - the best rate possible for a healthy group of employees and 32 dependents; and 33
Index Rate – the average of the base (best) rate and the highest possible rate 34 after medical conditions are underwritten. 35
36 In Nevada, insurers are currently required to file with the Division of Insurance their loss 37 ratio history when seeking rate increases. Requiring the disclosing of this information 38 will add some degree of transparency to the purchasing process and can assist the 39 employer in evaluating whether or not a carrier is operating efficiently. Low loss ratios 40 should raise significant concern for the small employer. A number of states mandate loss 41 ratios of 75% or higher. If small employers know that their insurance carrier has a loss 42 ratio of less than 60%, they may find cheaper policies elsewhere. 43 44 Additionally, Nevada has a statute for base rates and index rates for small employer 45 health care coverage, and the Nevada administrative code requires carriers to disclose to 46

Burns & Associates, Inc. V-6 May 5, 2006
small employers and producers how much a quoted premium rate may vary from the 1 index rate because of the health status of persons to be covered. The statute provides: 2 3
NRS 689C.230 Determination and application of index rate. 4 1. The index rate for a rating period for any class of business may not exceed the 5 index rate for any other class of business by more than 20 percent. 6 2. For a class of business, the premium rates charged during a rating period to small 7 employers with similar characteristics for the same or similar coverage, or the rates that 8 could be charged to such employers under the rating system for that class of business, 9 may not vary, because of health status-related factors, from the index rate by more than 10 30 percent. 11 3. As used in this section: 12 (a) “Base premium rate” means, for each class of business as to a rating period, the 13 lowest premium rate charged or that could have been charged under a rating system for 14 that class of business by the carrier to small employers with similar characteristics for 15 health benefit plans subject to regulation by the Commissioner. 16 (b) “Index rate” means, for each class of business as to a rating period for small 17 employers with similar characteristics, the arithmetic average of the applicable base 18 premium rate and the corresponding highest premium rate. 19 (Added to NRS by 1995, 984; A 1997, 2947) 20 21
Restated, the statute limits the index rate a carrier may have on a class of business to no 22 more than 20% above the index rate for any other class of business. Further, a carrier can 23 charge no more than 30% above the index rate within a class of business. 24 25 The National Association of Insurance Commissioners reports the national average 26 percentage that states permit carriers to charge the small employer market above the 27 index rate is 25%. Therefore, Nevada’s statute is somewhat more lenient on carriers 28 than the average of the rest of the states. 29 30 Summit participants may wish to consider providing employers information on small 31 group rating practices to allow them to make informed decisions regarding health care 32 coverage. This strategy of disclosure presumes that by making the base and index rates 33 routinely available to small employers and their producers, compliance with the statutory 34 requirement can be evaluated and the small employer can determine if a rate increase is 35 legitimate3. 36 37 Cost Estimate 38 39 Requiring the reporting of the three key indices will not add additional paperwork for 40 insurance carriers. There may, however, be administrative costs incurred by the 41 Department of Insurance for compiling and distributing the recommended information. 42 43 44
3 The strategy also presumes that small employers will understand what they have been told. If the referenced statute and the subsequent explanation do not convince the reader of the density of insurance law and the disadvantaged position of small employers, nothing will. The readability of this brief increases from this point forward.

Burns & Associates, Inc. V-7 May 5, 2006
2. Create Standardized Products that Insurance Companies can Offer to Small Employers 1 2 As mentioned above, small employers do not have the administrative staff to comparison 3 shop for insurance. Standardizing a benefit package for small employers levels the 4 playing field for the employer. The employer’s purchasing decisions can be focused not 5 on benefit design, but on price and delivery system (e.g., Preferred Provider 6 Organization, Point of Service, or HMO). Standardizing the benefit package works hand-7 in-hand with adding transparency in the reporting of rate information to enable the 8 employer to evaluate proposed premiums for health care coverage. 9 10 Standardized Plan 11 12 One example of a standardized group benefit package exists in Oregon. Oregon first 13 implemented a standardized benefit package as a component of its Small Employer 14 Health Insurance Reform (SEHI) initiative in 1993. It was originally targeted at 15 employers with 3 to 25 employees but now is targeted to groups of 2 to 50 employees. 16 The Basic Health Benefit Plan implemented in 1993 was modeled on the Oregon Health 17 Plan’s (the state’s Medicaid program) priority list. The SEHI reform initiative also 18 included a number of additional provisions including rate bands, underwriting standards, 19 renewability provisions and guaranteed issue. 20 21 Oregon recently supplemented the SEHI product by adding a more affordable package 22 with limited benefits. Beginning in 2005, Oregon began offering two low-cost 23 guaranteed issue plans for small employers: 24 25
The Alternative Group Plan for adults designed to provide a low-cost 26 alternative to the basic plans already on the market. The plan covers 27 physician and hospital services, and prescription drugs 28
The Children’s Group Plan which adds to the adult package coverage of 29 preventive, mental health and vision benefits for children 30
31 Oregon issued a request for proposal to determine which health insurance companies 32 would offer the plans. Small employers can choose between an HMO and a Preferred 33 Provider Organization. In order to participate, employees must work 17.5 hours per week 34 and employers who existed at that time must not have offered health insurance on or after 35 July 1, 2003. Employers must also pay a minimum of $50 per employee. 36 37 Standardized Plan with Premium Cap 38 39 Another strategy that has been deployed by states for the small group market is to 40 combine a standardized product with a limit on the premiums that may be charged for 41 that product. Maryland has implemented this strategy. The state created a guaranteed 42 issue product that all carriers participating in the small group market must sell. The 43 comprehensive standard health benefit plan (CSHBP) was designed by the Maryland 44 Health Care Cost Commission (MHCCC) with input from stakeholders. The plan has a 45 floor equal to the actuarial equivalent of the minimum benefits required to be offered by a 46

Burns & Associates, Inc. V-8 May 5, 2006
federally qualified HMO. Benefits may be added through the purchase of riders but 1 cannot be reduced. The cost of the plan is not permitted to exceed 10 percent of 2 Maryland’s average annual wage. If the cost of the package does exceed this cap, then 3 the MHCCC adjusts the cost sharing that is permitted under the policy. 4 Unlike many other states, Maryland has also permitted self-employed individuals to 5 participate in the program. Maryland provides a great number of options under their 6 plan for delivery systems – indemnity, preferred provider, point of service, HMO, or 7 health savings account-compatible preferred provider. 8 9 Other states have combined the standard benefit package with a subsidy component for 10 the individuals purchasing the coverage. Pennsylvania, Maine and New York have each 11 addressed this in different ways. Each is discussed in depth under Strategy #3 that 12 follows. 13 14 Summit participants may wish to consider a particular standardized small employer 15 insurance product as a strategy for expanding coverage, or may wish to consider the 16 appointment of a task force to further consider the question. If a task force is 17 recommended, it should likely be composed of insurers, small business owners, State 18 Insurance Department staff, and brokers. 19 20 Cost Estimate 21 22 No specific cost estimate is included as the standardized small group coverage strategies 23 will not involve significant expenditures by the State. If a task force is recommended, 24 this can be staffed by existing state resources. Summit participants may want to consider 25 a strategy that supplements existing staff resources with funds for either expanding state 26 staff or using the services of outside consultants. 27 28 29 3. Provide Subsidies for Either the General Population or Only to Small Employers 30 31 There are two types of subsidies that could be offered. 32 33 One is a direct premium subsidy that would be used to reduce either (or both) the 34 employer’s or the employee’s costs, and is tied to the specific enrollment of a particular 35 employee. For example, this may be a subsidy payment of $100 per month to an 36 employee. 37 38 The other form of subsidy is a reinsurance device. This approach limits the dollar 39 amount of claims that an insurance company will have to pay for any enrollee. Costs 40 above this limit are paid (either in whole or in part) by the state. By limiting the amount 41 of claims that an insurance company will have to pay for any enrollee, the insurance 42 company will have reduced risk and will in turn reduce premiums. For example, the state 43 may pay (in whole or in part) all of the claims above $50,000 in a year submitted to an 44 insurance company for a particular individual that has coverage. 45 46

Burns & Associates, Inc. V-9 May 5, 2006
The balance of the discussion for this strategy discusses each of these subsidy options in 1 turn. 2 3 Direct Premium Subsidies 4 5 In designing a direct subsidy program, there are a number of overall policy decisions that 6 need to be considered: 7 8
Benefit package. Is the benefit package standardized or are different packages 9 offered by different commercial carriers eligible for subsidy? Is the benefit 10 package limited or comprehensive? What deductibles and copays are 11 allowable? 12
13 Target population. Is the target population small employers or the uninsured 14
in general? Are both adults with children and those who are childless eligible 15 for the subsidy? Is the subsidy limited to those whose income is below a 16 certain threshold? Are dependents of employees eligible for the subsidy? Are 17 part time workers eligible for the program? 18
19 Contribution. If the subsidy is directed to small businesses, is there a 20
minimum contribution required by the employer? What contribution is 21 expected of employees? How much is the subsidy of the total premium? 22 Does the amount of the subsidy vary based on the enrollee’s income? 23
24 Limited liability. Does the state limit its liability under the direct subsidy 25
program to a fixed amount of appropriated dollars on a first come, first served 26 basis? Or, will the State provide a subsidy for everyone that wants to take 27 advantage of the program, regardless of the cost to the state? 28
29 Adverse selection. Will there be a “going bare” period required? This means 30
that in order to be eligible for the product, the business could not have offered 31 creditable insurance for a set period of time? Is there a minimum level of 32 employee participation? 33
34 There are a number of variations of direct subsidy programs that Summit participants can 35 consider. One would be a standardized, subsidized product offered to a broad subset of 36 the population (e.g., low-income). Another would be a standardized, subsidized product 37 focused on small employers. A third would be to offer a subsidy for any health insurance 38 package that a small business may want to buy, as long as it meets certain state 39 requirements. 40 41 Standardized Benefit with Subsidy 42 43 An example of a standard benefit plan coupled with direct premium subsidy that is 44 offered to a broad population is the Commonwealth of Pennsylvania’s adultBasic 45 product. The benefits include preventive care, physician services, inpatient 46

Burns & Associates, Inc. V-10 May 5, 2006
hospitalization, outpatient services, and emergency care. Coverage for prescription drugs 1 is not available. 2 3 At present, the individual premium varies across the Commonwealth, but on average is 4 about $312 per month. The target population for the product is working individuals ages 5 19-64 with annual incomes up to 200% of the FPL. The individual contracts directly 6 with a health plan authorized to offer the product. The employer does not participate in 7 the process. This means that sole proprietors who meet the income eligibility 8 requirement may participate. 9 10 Enrollees in adultBasic pay $32 per month to the health plan and the Commonwealth 11 pays the difference. Due to limited funds, the total enrollment in the program in the last 12 few years has been approximately 40,000, with a waiting list of between 80,000 and 13 110,000. Those individuals on the waiting list may pay the full premium amount and 14 receive coverage. The total amount of the subsidy is approximately $110 million per 15 year. The Commonwealth uses a portion of its tobacco settlement money to fund the 16 program. 17 18 Small Employer with Subsidy 19 20 Rather than offering a subsidized product to the broad population, many states are 21 looking to target small businesses. There are at least three rationales for states to target 22 subsidy programs to this group of uninsured. 23 24 One rationale for including a subsidy component for employees of a small employer is 25 that by reducing the costs to the employees, more employees will participate in the 26 program. With more employees participating, the risk is spread across more people and 27 premium rates are lowered. 28 29 Another rationale for the small business subsidy is that when premiums are lowered, 30 employers may be encouraged to offer insurance. 31 32 The third, and perhaps most important rationale that states have for subsidizing employer 33 sponsored insurance, is that with multiple payers, the costs for every payer is reduced. 34 The HIFA waivers available from Medicaid are motivated by this notion and require that 35 there be an employer-sponsored insurance component in any waiver request submitted. 36 With state-funded programs and HIFA waivers, employers, employees, the state and, in 37 the case of a HIFA waiver, the federal government, all share the cost of coverage. 38 39 This approach, often referred to as 3-share (employer, employee, state), has been 40 modestly successful in a number of states. 41 42 The first 3-share initiative began in Muskegon County, Michigan in 1994 under a grant 43 from the W.K. Kellogg Foundation. The cost of the program is divided among 44 employers, employees, and the state or a private foundation, although the shares may or 45 may not be equal. 46

Burns & Associates, Inc. V-11 May 5, 2006
Parameters for employee participation differ among the 3-share programs, but are 1 generally consistent in requiring that the employee and his/her dependents must be 2 uninsured and not eligible for public programs. The programs are sometimes available to 3 part-time (> 15 hours) as well as full-time workers. The specifics of the benefit plans 4 vary. Some are standardized and some are not, but most include primary care, 5 hospitalization, x-ray and labs, surgery, and prescription drugs. Discounted dental and 6 vision services may also be available. 7 8 Some programs also limit the provider network. For example, in Galveston County, 9 Texas, a program is being developed for a HIFA waiver where services will only be 10 offered within the county and through physicians within the University of Texas Medical 11 Branch. If approved by the federal government, the county anticipates serving between 12 3,000 and 5,000 residents a year. 13 14 With Standard Plans 15 16 Both Maine’s Dirigo Choice program and New Mexico’s State Coverage Initiative are 17 examples of standardized benefits coupled with a subsidy targeted to individuals working 18 for small employers. Maine’s Dirigo program negotiates directly with commercial 19 carriers to underwrite two Dirigo Choice products for groups of 1 to 50 individuals. The 20 products are identical except for deductibles. The subsidy, which is available to 21 employees and individuals with incomes below 300% of the FPL, buys down both the 22 deductible and the premium on a sliding scale basis. Under Maine’s plan, the employee 23 pays the entire premium through a wage deduction. However, Dirigo provides qualified 24 employees an electronic debit card with the subsidy amount so the result is that the 25 employee is reimbursed immediately. The ongoing costs of Maine’s plan are financed by 26 an assessment on insurers not to exceed 4%. 27 28 The New Mexico plan also has a standardized benefit package that may be offered to 29 small employers with 1 to 50 employees. A subsidy is available for employees with 30 incomes below 200% of the FPL. The amount of the subsidy is scaled to family income. 31 The subsidy is not available for dependents. Employers must not otherwise offer health 32 care coverage in order to participate. New Mexico’s initiative is funded using SCHIP 33 dollars to support both childless adults and parents. The State’s waiver was granted prior 34 to the Deficit Reduction Act (DRA) prohibition on the use of SCHIP funds for childless 35 adults. 36 37 With Non-Standard Plans 38 39 Nevada’s original HIFA waiver proposal in 2005 contained an employer-sponsored 40 insurance component with a subsidy component. The original (and the current) HIFA 41 waiver concept included a non-standardized benefit package. Insurers and health plans 42 can offer small employers any benefit plan so long as that plan meets the minimum 43 benefit plan allowed by the Department of Insurance. Small employers must not have 44 offered insurance coverage within the last six months to participate in the program. 45 Under the original plan, the State, with matching federal funds, would have provided 46

Burns & Associates, Inc. V-12 May 5, 2006
subsidies for all employees below 200% of the FPL. With the subsidy being allowed for 1 all employees, the marketing target for the program was small businesses. 2 Because of the prohibition in the DRA with respect to using SCHIP funds for childless 3 adults, this has now been changed. The HIFA waiver is now proposed to target 4 employees who are parents of children enrolled in the Medicaid or Nevada Check Up, 5 which should make the remaining premium more affordable for the employee. 6 7 The Oregon Family Health Insurance Assistance Program (FHIAP) is a second example 8 of a subsidy coupled with a non-standardized benefit package targeted to small 9 employers. Under the program, employees and individuals with incomes below 185% of 10 the FPL pay the entire premium and are reimbursed based on a sliding scale. 11 12 Reinsurance 13 14 There are a few states that offer state-funded reinsurance programs for targeted 15 populations enrolled in private health insurance. New York currently has a reinsurance 16 program built into its Healthy NY program, whereby private health insurers who offer 17 Healthy NY are reinsured for individuals who have higher annual medical costs. 18 19 Healthy NY is not part of the Medicaid program or another government-sponsored 20 program. The program is targeted to low-wage workers, small employers and the self-21 employed. It is administered by New York’s Department of Insurance, but the 22 Department funnels all eligibility determinations and enrollment functions down to the 23 private sector health plans. 24 25 There are only two products offered under Healthy NY—one that includes and one that 26 excludes a pharmacy benefit. As such, the product is the same across all health plans, so 27 individuals choosing to enroll in the program only have to make decisions on health plan 28 preference and price. 29 30 Health plans are able to charge what they wish for the Healthy NY product under the 31 state’s “file and use” provision for rate regulation. Up until recently, the premiums 32 charged for Healthy NY were significantly lower than the regular commercial market, in 33 part because of a slimmer benefit package but primarily due to the reinsurance 34 component. For example, when the Insurance Department changed the reinsurance level 35 in July 2003 from covering 90% of annual costs per person in the $30,000-$100,000 36 range to the lower range of $5,000-$75,000, all health plans lowered their Healthy NY 37 premiums by 17%. 38 39 To be eligible to participate in Healthy NY, a small employer must have fewer than 50 40 employees, 30% of whom must earn less than $33,000 a year (adjusted for inflation). 41 The employer must contribute half of the premium, and at least 30% of employees must 42 participate in the program. Part-time workers and an employee’s dependents are allowed 43 to participate, but the employer does not have a mandatory contribution toward the 44 premiums for these enrollees. Self-employed individuals and working individuals not 45

Burns & Associates, Inc. V-13 May 5, 2006
eligible through an employer’s plan may also participate in Healthy NY if their 1 household income is below 250% of the FPL. 2 One important consideration associated with a reinsurance program is the notion of 3 adverse selection – that is, that only (or at least a disproportional number of) people with 4 high medical needs will sign up for the program. If adverse selection occurs in a 5 reinsurance program, the claims of these individuals would typically exceed the 6 reinsurance threshold. If a reinsurance program is in place and has adverse selection, the 7 cost to the state increases. With increasing costs, either more funding must be put into 8 the program or a fewer number of individuals can participate. 9 10 New York may be one of the few states in the nation that can successfully “pull off” a 11 reinsurance program because the state has community rating of the small market. With 12 community rating (and an exclusion of pre-existing conditions in the Healthy NY 13 program), New York has not seen a great deal of adverse selection in their program. 14 15 Nevada does have a Program of Reinsurance for small employers in statute. For those 16 policies written under the program, losses for any individual above a threshold are 17 covered at 90%. The program is funded through an assessment on reinsuring carriers. At 18 this point in time, there is no enrollment in this Program because the carriers that would 19 be participating in contributing to the reinsurance fund would in essence be reinsuring 20 themselves. 21 22 Summit participants may consider a specific subsidy program for small employer 23 insurance as a strategy for expanding coverage, or may wish to consider the appointment 24 of a task force to further consider the question. If a task force is recommended, it should 25 likely be composed of insurers, small business owners, State Insurance Department staff, 26 and brokers. 27 28 Cost Estimate – Direct Premium Subsidy 29 30 The cost to the State of any direct premium subsidy (other than for administrative 31 expenses) is a direct function of the number of people to receive the subsidy and the 32 amount of subsidy. For example, if 1,000 individuals are to be covered at $100 per 33 month, the cost for the program for a year would be $1.2 million a year. 34 35 The cost estimate below was prepared with the following major assumptions: 36 37
$100 monthly insurance subsidy 38 Eligible group is: 39
– Uninsured 40 – Working at small firms 41 – Under 200% of the FPL 42 – Not already enrolled in a government-sponsored health insurance program 43
(e.g. Medicaid, Medicare or Tricare). 44 45

Burns & Associates, Inc. V-14 May 5, 2006
Additional assumptions were used in performing the estimates, most notably that 1 Medicaid will participate in the program and offset some of the costs. If Medicaid does 2 not participate in the program, the figures reported for “State Responsibility” would be 3 replaced by the figures contained under “Total Costs”. 4 5 The two estimates in the Table below vary because of the “Take-up” rate. This refers to 6 the percentage of the individuals eligible for the program that will actually enroll in the 7 program. A take-up rate of 100% is unrealistic, but presents one estimate of the outside 8 limit of the State’s exposure under the program. 9 10 Take-up rate Number of
Uninsured CoveredTotal Costs State Responsibility
58% 17,734 $21.3 million $17.3 million 100% 30,576 $36.7 million $29.8 million
11 Based on the estimates provided above, approximately 18,000 of the 426,000 uninsured 12 in Nevada would qualify and enroll in the direct subsidy program for small employers. 13 14 A more detailed explanation of the Direct Subsidy Cost estimate is contained in the 15 “Selected Cost Estimates Appendix”. The explanation contains additional tables that will 16 allow the reader to find cost estimates under different assumptions than are provided 17 here. The Selected Cost Estimates Appendix is available at the following web site: 18 www.burnshealthpolicy.com. 19 20 A more detailed explanation of the number of uninsured in Nevada is contained in the 21 “Technical Appendix”. The explanation and tables in the Appendix present information 22 about who the uninsured are in Nevada. The Technical Appendix is also available at 23 www.burnshealthpolicy.com. 24 25 26 4. Allow Small Employers to Buy Into the State Employee Health Program 27 28 Because they lack sufficient size, small employers are disadvantaged when purchasing 29 insurance. Larger pools such as state employees exert more “clout” in the marketplace 30 and are able to negotiate better pricing with providers. If small employers can access 31 better provider pricing, premiums should decline. 32 33 West Virginia has created a public-private partnership between the state’s Public 34 Employee Insurance Agency (PEIA) and insurance carriers which choose to offer the 35 Small Business Plan. Small employers capitalize on the purchasing power of the PEIA, 36 while carriers get access to the PEIA reimbursement rates. The PEIA is self-funded and 37 has statutory authority to set fee schedules for participating providers. 38 39 The program is available to small employers who have not provided coverage to the 40 employees in the 12 months preceding enrollment. Employers are also responsible for 41 50% of the premium. Access to the State’s self-insured pool, negotiated provider 42

Burns & Associates, Inc. V-15 May 5, 2006
payment, and reduced administrative costs (through decreased carrier margins) were 1 factors in reducing costs for small employers. The product includes the benefits 2 mandated by the State. The plan is underwritten for the small employer, and renewal 3 rates are based on the individual employer group’s experience. The State is currently 4 preparing a similar initiative for uninsured persons in the individual market. 5 It is unknown is whether Nevada’s state employees’ insurance has more purchasing 6 power than insurance carriers and health plans. 7 8 Summit participants may wish to consider having the proposed task force previously 9 discussed as an option under Strategy 3 also assess the state employee plan and its 10 potential benefit for small employers. 11 12 Cost Estimate 13 14 No specific cost estimate is included to implement this option. However, if it is decided 15 to pursue this option, considerable effort will likely be required in formulating the details. 16 This effort could be staffed with state resources, or Summit participants may want to 17 consider recommending monies to supplement existing staff resources with funds for 18 either expanding staff or using the services of outside consultants. 19 20 21 5. Establish a High Risk Pool for the Uninsurable 22 23 Nevada is one of 15 states that do not have a high risk pool. These state-sponsored 24 programs offer insurance to residents who are considered “uninsurable” and are unable to 25 buy coverage in the individual market. The features of high risk pools typically include: 26 27
The individual must prove denial of coverage by at least one, and occasionally 28 as many as three insurance plans in order to participate 29
The pools offer a range of deductibles (e.g. $2500, $5000, $7500, and 30 $10,000) to reduce the cost of the premium 31
The pools limit premiums that may be charged for the high risk plan to a 32 percentage of the highest or average premiums charged by the largest carriers 33 in the state (e.g. 150% of the highest premium) 34
35 Waiting periods may also be imposed or exclusions from coverage for conditions that 36 manifested or medical advice or treatment received during a period prior to the effective 37 date of coverage. The pools may also include lifetime benefit of $1,000,000. In 2004, 38 there were 181,441 individuals in state high risk pools nationwide. 39 40 A major criticism of high risk pools is that they lose money. Because pools are not self-41 sustaining through premium revenue (the premiums charged do not cover the costs of 42 claims paid), subsidization is required. States have looked to a variety of funding 43 mechanisms to maintain the pools’ stability. These have included assessments on 44 insurance carriers and HMOs operating in the state based on the amount of business they 45 conduct, surcharging hospital bills, or general revenue or special dedicated state funds. A 46

Burns & Associates, Inc. V-16 May 5, 2006
few states subsidize high risk pool premiums with state and federal matching funds under 1 HIFA waivers for low-income participants. To reduce exposure, states may limit 2 enrollment in the high risk pool to available dollars. 3 4 Congress has provided funding to establish state high risk pools through the Trade 5 Adjustment Assistance Act of 2002 (TAA) but the assistance is time limited to two years. 6 The Deficit Reduction Act of 2006 appropriated $75 million in FY 2006 for grants to 7 help fund existing qualified state high risk pools and $15 million for grants to assist states 8 to create and initially fund qualified high risk pools. The legislation also authorizes 9 appropriations of $75 million for each year FY 2007 through FY 2010. 10 11 The advantage of a high risk pool is that it increases access for individuals who would not 12 otherwise be able to obtain coverage. The disadvantage, as noted above, is that pools are 13 expensive for the state to fund. 14 15 An example of one state’s high risk pool is discussed below. This state has a similar-16 sized population and an uninsured rate that is very close to Nevada’s. The high-risk pool 17 covered about 400 people throughout 2003, with an overall per member per month 18 (PMPM) cost of about $1,000. This resulted in an annual medical expense of $5 million. 19 To fund this program, the state generated revenue from three main sources with a fourth 20 used for reserve funding. 21 22 Premium revenue covered nearly half of the medical expenses at $450 per member per 23 month (PMPM), while another $400 PMPM was covered by appropriations from the 24 legislature (set at $2 million per year). As another source of income, the state enacted a 25 tax on hospital admissions for people insured by private plans that generated $140 26 PMPM for the high-risk pool program. To cover any remaining costs from year to year 27 and to generate some extra income from interest, the state also set up an investment trust 28 ($10-$15 million in the fund). This trust serves as another source of income and as a pool 29 of money to cover any shortfalls from year to year. 30 31 The number of people this program can cover changes from year to year. Since the 32 maximum amount the state can set the premiums is set in statute (a fixed percentage 33 above the premiums of private insurers), the number of available slots becomes an 34 artifact of: how much revenue the hospital admissions tax generates, the annual 35 appropriation, and the amortization of the trust reserve. 36 37 Summit participants may wish to consider the establishment of a high risk pool. 38 39 Cost Estimate 40 41 No specific cost estimate is included to implement this option. The above-mentioned 42 federal grants from the Deficit Reduction Act could be used in implementing this option, 43 but the federal monies are time-limited. Enrollment in the program is a function of how 44 much subsidy (at approximately $500 PMPM) the state is willing to provide. If the 45

Burns & Associates, Inc. V-17 May 5, 2006
Summit participants decide to pursue this option, some estimate of enrollment should be 1 included in the recommendation. 2 3 It should also be noted that considerable effort will be required in formulating the details 4 of start up and implementation. This effort could be staffed with state resources, or 5 Summit participants may want to consider recommending monies to supplement staff 6 resources with funds for either expanding staff or using the services of outside 7 consultants. 8 9 10 6. Establish a Universal Coverage Program 11 12 Three states have passed universal coverage laws (Hawaii in the 1970s, Maine in 2003, 13 and Massachusetts earlier this year). The states differ in their approach to providing 14 coverage. 15 16 Hawaii’s law is an employer mandate – coverage must be offered to employees but not 17 dependents. Hawaii is unique in that it is exempt from Employment Retirement Income 18 Security Act (ERISA) so the mandate applies to these firms as well. The Census Bureau 19 reports a current uninsured rate of 9.9% for Hawaii, but the rate of uninsurance had been 20 as low as 2%. 21 22 Maine’s program was implemented in 2003 and uses a basic structure of a state-operated 23 health purchasing coalition for small employers, sole proprietors, and individuals. Dirigo 24 Choice offers subsidies to enrollees with family income below 300% of the FPL to meet 25 their cost for premiums and the plan’s deductible. The program has statutory authority to 26 request an assessment on insurers not to exceed four percent of gross premiums per year 27 to fund the program. 28 29 Massachusetts has built upon the concept of employer and personal responsibility with a 30 “play or pay” approach. Massachusetts likened this approach to car insurance, i.e., you 31 have to have it or face fines. Employers not currently offering coverage are provided 32 incentives to pay for employee coverage through the use of pre-tax dollars. Those 33 choosing not to offer coverage will face penalties of $295 per full-time equivalent 34 employee beginning in 2007. Individuals face penalties (eliminating the personal 35 exemption on state taxes) if they fail to obtain coverage. 36 37 In their program, Massachusetts recognized that very small employers (less than 10 38 workers) find it difficult to find affordable plans. Therefore, the State is allowing the 39 merger of individual markets and small group markets. This merger will provide a larger 40 risk pool, and hopefully, lower overall premiums for a significant number of employees. 41 The conference report on the legislation estimates a 24% reduction in non-group 42 premium costs. The Governor signed the bill into law on April 12 and the provisions will 43 become effective in July 2007. 44 45

Burns & Associates, Inc. V-18 May 5, 2006
Summit participants may wish to consider the establishment of a universal coverage 1 program for Nevada. 2 3 Cost Estimate 4 5 No specific cost estimate is included to implement this option. However, if it is decided 6 to pursue this option, considerable effort will be required in formulating the details. This 7 effort could be staffed with state resources, or Summit participants may want to consider 8 recommending monies to supplement staff with funds for either expanding staff or using 9 the services of outside consultants. 10 11 12 7. Expand the Safety Net Provider System 13 14 With a shortage of providers for the insured, and the number of people who are 15 uninsured, safety net providers in Nevada are seeing increased demand for their services. 16 With state support for the enhancement and expansion of Community Health Centers 17 (CHCs), Nevada will increase access to health care for a broad spectrum of people and 18 likely restrain the cost increases in the health care system. 19 20 National studies have found that community health centers which serve as a key provider 21 of primary care and prevention services, save the Medicaid program at least 30% 22 annually. This savings accrues from Medicaid beneficiaries that use health centers, and 23 then have reduced need for specialty care referrals and hospital admissions. It is also 24 estimated that if patients utilizing the emergency rooms for non-emergency services were 25 redirected to a CHC, up to $8 billion could be saved nationally. 26 27 Since 2001, there has been a federal focus to increase the number of health centers and to 28 expand funding for the overall program. Appropriations have increased 53% from $1.16 29 billion to $1.78 billion over the past five years, and the FY 2007 President’s budget 30 request is at $2 billion. 31 32 A number of states provide direct funding to CHCs. The most common sources of 33 funding are general revenue, tobacco settlement or tobacco tax dollars, and provider 34 taxes. Among the neighboring states, Arizona provides $10 million, New Mexico $16.7, 35 and Utah $700,000 to CHCs. Oregon and Idaho do not provide direct support. In 2006, 36 Nevada provided $817,000 in support to CHCs for oral health, specialty care for the 37 uninsured, public health preparedness and other health services. 38 39 In the past five years, Nevada’s CHCs (including Tribal Health Clinics) saw their annual 40 client visits climb from 50,000 to 170,000. Patient payment for those visits is based on a 41 sliding scale, with low-income individuals paying nothing and higher-income individuals 42 paying per visit fees. Over half of the visits were provided to uninsured residents. The 43 cost per medical visit averages approximately $90 with the cost per dental visit being 44 higher. 45 46

Burns & Associates, Inc. V-19 May 5, 2006
With state support, the existing centers can provide more or expanded services, and new 1 centers can be developed. If Nevada was to significantly increase support for community 2 health centers (or more generally for safety net providers), some criteria for that support 3 should be adopted. Among the questions that should be considered are: 4 5
Whether support should go to only federally-qualified health centers (FQHCs) 6 or whether other potential sponsors (such as hospitals) could receive support. 7
8 Whether support should be offered for any service or should a minimum 9
service package should be required. One state requires safety net providers to 10 provide the following services in order to receive support: 11
12 1. outreach services 13 2. primary and preventive health services 14 3. diagnostic laboratory and diagnostic imaging services 15 4. pharmacy services, health education and health promotion 16 5. referral and follow-up (tracking services) 17 6. well-woman services 18 7. prenatal care 19 8. family planning 20 9. preventive dental care 21 10. transportation 22 11. same day services 23 12. onsite emergencies 24 13. 24-hour coverage 25 14. behavioral health services 26
27 Whether support should be for “incubation” of new clinics and expansion for 28
existing clinics, or should support on be for ongoing operations of existing 29 clinics. 30
31 Summit participants may consider as an option the implementation of the following 32 program which has been designed to expand and support services through community 33 health centers and other eligible safety net providers (such as sponsoring hospitals). The 34 program contemplates $10 million per year in state support. For the first five years, the 35 funds would be distributed in two ways: 36 37
$5 million for support of new facilities or expansion of existing clinics 38 $5 million for support of services provided to the uninsured on a per visit 39
basis 40 41
Modeled after an Arizona program, Nevada would issue a request for proposals to 42 determine the recipients and distribution of funds. For the $5 million in new and 43 expansion funds, the State would offer grants of up to $500,000 per location with no 44 individual site receiving more than two grants during the five-year period. Unused funds 45 from one year would roll over to subsequent years until all funds are exhausted. 46

Burns & Associates, Inc. V-20 May 5, 2006
For the $5 million for ongoing operations, at an average per visit cost of $90, the funds 1 would support an approximate 35% increase in visits per year. 2 3 After the first five years of operation, the $10 million annual amount would be used 4 exclusively to support on a per visit basis clinic services to uninsured clients. 5 6 The Summit participants may want to consider the above outlined program or any 7 variation of the option. The annual amounts can be scaled and the program design 8 modified. 9 10 Cost Estimate 11 12 The above program does not specifically include administrative costs. The Arizona 13 program referenced above permits the Department operating the program to use 4% of 14 the monies for administration and operation. 15 16 However, if it is decided to pursue this option, effort will be required to formulate the 17 details. This effort could be staffed with state resources, or Summit participants may 18 want to consider recommending monies to supplement existing resources with funds for 19 additional state staff or using the services of outside consultants. 20 21 22 8. Foster Local Community Efforts to Offer Services to the Uninsured 23 24 In Nevada and throughout the country local communities have implemented initiatives 25 designed to provide access to health services for the uninsured. These initiatives are 26 based on local relationships within the health care delivery system. The State can foster 27 these local initiatives through planning grants. 28 29 Growing out of the Clark County Health Access Consortium, AccessHealth is a 30 community initiative managed by Great Basin Primary Care Association. AccessHealth 31 is designed to coordinate enrollment, assignment to a medical home, and referrals that 32 make a range of discounted health services available to the uninsured. AccessHealth is 33 not a health insurance program but instead provides access to a coordinated range of 34 health services at discounted rates. 35 36 To be eligible for the program, individuals must be Nevada residents and have income 37 above the Medicaid standard but below a designated threshold (for a family of four, 38 annual income must be between $20,000 and $50,000). The individual or family must 39 also not have coverage through Medicaid, Medicare or their employer. Once enrolled, 40 each individual is assigned a primary care physician who coordinates referrals to 41 specialists and hospitals. 42 43 There is no enrollment fee for AccessHealth. However, members are expected to pay for 44 services at the time the service is rendered but at the negotiated discounted rate. The 45 network of providers that has agreed to discounted rates includes CHCs, multi-specialty 46

Burns & Associates, Inc. V-21 May 5, 2006
groups, sole practitioners, hospitals, radiology and lab services, outpatient surgery centers 1 as well as other providers. To discourage utilization, the network does not include 2 emergency rooms. 3 4 Similarly, the Pima County Access Program (PCAP) is a membership-based, health care 5 referral program in southern Arizona. Unlike AccessHealth, there is an enrollment fee in 6 PCAP. Once enrolled in PCAP, an individual has access to deeply discounted primary 7 and specialty care, and hospital services. Primary care, provided through a CHC, is based 8 on a sliding fee scale. Specialist consults are $25, hospitalization is $400/day; ICU is 9 $600/day. Specialty care services are set at 30% of the Medicare rate. Prescriptions are 10 offered through pharmacy discount programs. All fees are payable at the time of service. 11 Emergency room services are not covered unless the member is admitted. If not 12 admitted, the patient is responsible for 100% of the charges. 13 14 The PCAP program is open to individuals ineligible for public programs, and with 15 income levels up to 250% of FPL. If an employer subsidizes any portion of an 16 employee’s health insurance costs, that individual is not eligible to participate. However, 17 if the individual is in a probationary or waiting period, enrollment would be permitted. 18 Employers who have never offered health insurance are permitted to pay the enrollment 19 fee on behalf of the employee. 20 21 These types of community-based initiatives fills gaps for the uninsured but their 22 development depends on local initiative and local relationships. 23 24 Summit participants may wish to consider fostering local community efforts to offer 25 services to the uninsured through leadership and planning grants. 26 27 Cost Estimate 28 29 If ten planning grants of $50,000 each were to be offered the total cost of the local 30 support program would be $500,000. Additional monies would have to be made 31 available for state staff to set up and administer the program. 32 33 34 9. Increase Funding for the Senior Rx and Disability Rx Programs 35 36 Nevada has statutorily mandated that a portion of the tobacco settlement monies be used 37 to support two state-sponsored drug assistance programs, Senior Rx and Disability Rx. 38 39 With the enactment of Medicare Part D, Senior Rx provides assistance with out of pocket 40 expenses for seniors that are eligible for Medicare Part D and cost-sharing for members 41 not eligible. Eligibility for the Senior Rx is set at annual income levels of $23,175 for a 42 single individuals and $30,168 for couples. The program has no asset test, but eligibles 43 must be 62 years of age or older and have continuously lived in Nevada for the preceding 44 12 months. 45 46

Burns & Associates, Inc. V-22 May 5, 2006
For SFY 2006 Senior Rx will receive approximately $8 million in funding and serve 1 approximately 8,600 seniors. While there is a great deal of uncertainty surrounding the 2 implementation of Part D, program administrators are reasonably confident that Senior 3 Rx has sufficient funding to support the seniors that have applied for the program. There 4 is no waiting list for services. 5 6 It may take another year before the impact of Part D on Senior Rx is fully understood, at 7 which time the question of whether or not the program will require additional state 8 support can be revisited. 9 10 In January of 2006 Nevada began the Disability Rx program. This program assists 11 disabled individuals with the cost of prescription medicines. The income, asset and 12 residency requirements of Senior Rx apply to the Disability Rx program, with the 13 additional requirement of some proof of disability. Funding for Disability Rx is the 14 residual amount not expected to be required for Senior Rx. For SFY 2006 approximately 15 $470,000 is available for the program, which is estimated to support 147 individuals. 16 17 With the uncertainty of the impact of Part D, and the lack of experience in supporting the 18 disabled community (no claims experience), Disability Rx has stopped admitting 19 individuals into the program. There were approximately 87 individuals on the waiting 20 list as of mid April 2006. 21 22 Summit participants may wish to consider increasing the amount of support for Disability 23 Rx to the $1 million level. Such a recommendation should be time limited until the 24 program reaches a better understanding of both the Part D program under Medicare and 25 the cost to serve Disability Rx participants. 26 27 Cost Estimate 28 29 The cost of funding the option for Disability Rx is approximately $600,000. 30

Burns & Associates, Inc. V-23 May 5, 2006
Resources 1 2 Blumberg, L. J., et.al. (December 2005). Lowering Financial Burdens and Increasing 3 Health Insurance Coverage for Those With High Medical Costs. The Urban Institute. 4 Retrieved on April 6, 2006 from 5 http://www.urban.org/UploadedPDF/311261_financial_burdens.pdf 6 7 Communicating for Agriculture and the Self-Employed (2006). Overview – State High 8 Risk Health Insurance Pools Today. Retrieved March 16, 2006 from 9 http://www.selfemployedcountry.org/riskpools/overview.html 10 11 Council for Affordable Health Care (March 2006). Health Insurance Mandates in the 12 States 2006. Retrieved on April 6, 2006 from 13 http://www.cahi.org/cahi_contents/resources/pdf/MandatePub2006.pdf 14 15 Employee Benefits Research Institute (June 2005). The Muskegon Access Health 16 “Three-Share” Plan: A Case History. Issue Brief No. 282. Retrieved April 5, 2006 from 17 http://www.ebri.org/publications/ib/index.cfm?fa=ibDisp&content_id=3509 18 19 Fronstin, P. (March 2006) Workers’ Health Insurance: Trends, Issues, and Options to 20 Expand Coverage. The Commonwealth Fund. Retrieved on April 6, 2006 from 21 http://www.cmwf.org/usr_doc/908_Fronstin_workers_health_insurance.pdf 22 23 Gencarelli, Dawn (April 19, 2005 ). Health Insurance Coverage for Small Employers. 24 National Health Policy Forum. Retrieved April 6, 2006 from 25 http://www.nhpf.org/pdfs_bp/BP_SmallBusiness_04-19-05.pdf 26 27 Georgetown University Health Policy Institute (April 2004). Summary of Key Consumer 28 Protections in Individual Health Insurance Markets. Retrieved April 6, 2006 from 29 http://www.healthinsuranceinfo.net/newsyoucanuse/discrimination_limits.pdf 30 31 Gitterman, D. (July 25, 2003) Applying the Brakes on Mandated Benefits? FTC/DOJ 32 Hearings on Health Care and Competition Law and Policy. Retrieved April 6, 2006 from 33 http://www.ftc.gov/ogc/healthcarehearings/docs/030625gitterman.pdf 34 35 Government Accountability Office (May 20, 1998). Implementaion of HIPAA: State-36 Designed Mechanisms for Group-to-Individual Portability. GAO/HEHS-98-161R 37 “Alternative Mechanisms” Under HIPAA. Retrieved April 5, 2006 from 38 http://archive.gao.gov/paprpdf2/160522.pdf 39 40 Government Accountability Office (September 2003). PRIVATE HEALTH INSURANCE 41 Federal and State Requirements Affecting Coverage Offered by Small Businesses. GAO-42 03-1133. Retrieved April 5, 2006 from http://www.gao.gov/new.items/d031133.pdf 43 44 Health Insurance Portability and Accountability Act (August 21, 1996). Public Law 104-45 191. 46

Burns & Associates, Inc. V-24 May 5, 2006
Interview with Michal Goforth, Director, Pima County Health Communities Access 1 Program (PCAP). (April 14, 2006) 2 3 Kaiser Family Foundation and Health Research and Educational Trust (September 9, 4 2004). Employer Health Benefits Annual Survey 2004. Retrieved April 6, 2006 from 5 http://www.kff.org/insurance/7148/upload/2004-Employer-Health-Benefits-Survey-Full-6 Report.pdf 7 8 Maine Office of Health Policy and Finance (2006). Dirigo Choice Program. Retrieved 9 April 25, 2006 from http://www.dirigohealth.maine.gov/dhlp02.html 10 11 Maryland Health Care Commission. Maryland’s Comprehensive Standard Benefit Plan 12 for Small Business, A guide to Purchasing Health Insurance for Small Employers. 13 Retrieved March 21, 2006 from 14 http://mhcc.maryland.gov/smgrpmkt/cshbp_brochure.htm 15 16 Massachusetts State Legislature (April 10, 2006). Health Care Access and Affordability 17 Conference Committee Report. Retrieved April 10, 2006 from 18 http://www.mass.gov/legis/summary.pdf 19 20 Massachusetts Legislature (April 3, 2006). Health Care Reform Conference Committee 21 Bill, Joint Caucus for House Members. Retrieved April 10, 2006 from 22 http://www.mass.gov/legis/presentation.pdf 23 24 National Association of Community Health Centers (March 2004). A Nation’s Health at 25 Risk: A National and State Report on America’s 36 Million People Without a Regular 26 Health Care Provider. Retrieved April 5, 2006 from 27 http://www.nachc.com/press/files/UnservedReportSTIB5.pdf 28 29 National Association of Community Health Centers (August 2005). Shifting Sands: 30 State Funding, Medicaid Cuts, and Health Centers. Retrieved April 10, 2006 from 31 http://www.nachc.com/advocacy/Files/state-policy/statepolicyreport8.pdf 32 33 New Mexico Human Services Department, Medical Assistance Division (June 2004). 34 New Mexico State Coverage Initiative. Retrieved April 25, 2006 from 35 http://www.statecoverage.net/0604/ingram.ppt 36 37 Pennsylvania Insurance Department. Facts About adultBasic. Retrieved March 17, 2006 38 from http://www.ins.state.pa.us/ins/cwp/view.asp?a=1278&q=527068 39 40 Pollitz, K., and Bangit, E. (November 2005). Federal Aid to State High-Risk Pools: 41 Promoting Health Insurance Coverage or Providing Fiscal Relief? Retrieved April 5, 42 2006 from http://www.cmwf.org/usr_doc/Pollitz_highriskpools_875.pdf 43 44

Burns & Associates, Inc. V-25 May 5, 2006
Schwartz, Katherine (July 2005). Reinsurance: How States Can Make Health Coverage 1 More Affordable for Employers and Workers. The Commonwealth Fund. Retrieved 2 April 5, 2006 from http://www.cmwf.org/usr_doc/820_swartz_reinsurance.pdf 3 4 Silow-Carroll, S. and Alteras, T., (October 2004). Stretching State Health care Dollars 5 During Difficult Times. Retrieved April 5, 2006 from 6 http://www.cmwf.org/publications/publications_show.htm?doc_id=243623 7 8 State Coverage Initiatives (November 2005). State Coverage Matrix. Retrieved April 9 13, 2006 from http://www.statevcoverage.net/matrix/index.htm 10 11 State Coverage Initiatives (Fall 2005) Profiles in Coverage: West Virginia Small 12 Business Plan. Retrieved April 14, 2006 from 13 http://www.statecoverage.net/westvirginiaprofile2.htm 14 15 State Coverage Initiatives (July 2004). Limited-Benefit Policies: Public and Private-16 Sector Experiences. Retrieved April 6, 2006 from 17 http://www.statecoverage.net/pdf/issuebrief704.pdf 18 19 State Coverage Initiatives (January 2006). State of the States Finding Their Own Way. 20 Retrieved April 6, 2006 from http://www.statecoverage.net/stateofthestates/index.html 21 22 State Coverage Initiatives (January 2005). Profiles in Coverage: Healthy New York. 23 Retrieved April 14, 2006 from http://www.statecoverage.net/newyorkprofile2.htm 24 25 State of Oregon, Office of Private Health Partnerships, Insurance Pool Governing Board 26 (2006). Small Employer Health Plans. Retrieved April 18, 2006 from 27 http://www.oregon.gov/OPHP/docs/cover_with_insert.pdf 28 29 State of Oregon, Office of Private Health Partnerships, Family Health Insurance 30 Assistance Program (2006). Program Summary. 31 http://www.oregon.gov/OPHP/docs/fhiap_sum_employr.pdf 32 33 Taylor, Jessamy (August 31, 2004.) The Fundamentals of Community Health Centers. 34 National Health Policy Forum. Retrieved April 5, 2006, 2006 from 35 http://www.nhpf.org/pdfs_bp/BP_CHC_08-31-04.pdf 36 37 The Commonwealth Fund (May 2005). The Illinois “3-Share” Model: County-Level 38 Partnerships to Cover the Uninsured. Retrieved April 6, 2006 from 39 http://www.cmwf.org/tools/tools_show.htm?doc_id=278331 40 41 The New York Times (April 5, 2006). Massachusetts Sets Health Plan for Nearly All. 42 Section A, Page 1. 43 44

Burns & Associates, Inc. V-26 May 5, 2006
U.S. Census Bureau (September 30, 2005). Nevada, Arizona Lead Growth. Retrieved 1 April 17, 2006 from http://www.census.gov/Press-2 Release/www/releases/archives/business_ownership/005784.html 3 4 5 Nevada Specific Resources: 6 7 Interviews with Steve Hansen, CEO, Nevada Health Centers, Inc.; Dr. Michael Rodolico, 8 Executive Director, Health Access Washoe County; Sherri Rice, AccessHealth; Jack 9 Kim, Sierra Health Service; Jim Wadhams, Nevada Association of Health Underwriters; 10 and Christine Dugan, Las Vegas Chamber of Commerce. (April 6, 2006) 11 12 Legislative Counsel Bureau (January 2005). Study of Health Insurance Expansion 13 Options. Bulletin No. 05-24. 14 15 Nevada JobConnect. Nevada Economy in Brief February 2006. Retrieved April 5, 16 2006 from 17 http://www.nevadaworkforce.com/admin/uploadedPublications/1697_EIB_2006_Q1.pdf 18 19 Nevada Senior RX. Retrieved April 5, 2006 from http://nevadaseniorrx.nv.gov/ 20 21 Whitman, Nancy (March 15, 2006). Testimony on AccessHealth. Presented before the 22 Legislative Committee on Health Care. 23 24

Burns & Associates, Inc. VI-1 May 5, 2006
Chapter VI 1
Policy Brief on Focus Group Recommendation 2
Planning 3 4 5
I. RECOMMENDATION STATEMENT 6 7
Nevada will develop positive proactive plans for addressing its health care system 8 challenges with formalized planning bodies that coordinate and disseminate 9 information on health care policy, quality, community needs, workforce issues, 10 and health information technology and information exchange. 11
12 II. OVERVIEW 13
14 All states have at least nominal health planning functions, and Nevada is no exception. 15 However, the focus groups collectively expressed their perception that there is no 16 centralized responsibility for health care planning in Nevada. There were 17 recommendations and observations that Nevada needs a planning function that will have 18 the attention of policy makers, perform analysis on the volumes of data that are collected, 19 and promote policies to address the challenges facing the Nevada health care system. 20 21 The focus groups pointed to the stress that population growth is placing on the health care 22 delivery system, the shortage of health care professionals, the lack of access to primary 23 and specialty care – including mental health and long term care– as evidence of 24 inadequate planning in the State. Additionally, the focus groups commented that more 25 could be done to encourage evidence-based practices, promote the evaluation of the 26 system on the basis of outcomes and quality, and to address the disparity in access, 27 coverage and outcomes between population groups. It was also observed that there was 28 no regular, standardized assessment of community needs, no detailed analysis of the 29 uninsured population, and inadequate or no planning for health care manpower needs. 30 31 Collectively, the focus groups saw an opportunity for a centralized health care systems 32 planning function, possibly with regulatory powers, that could create a vision for the 33 health care system, promote quality and technology, analyze data that is collected, define 34 best practices, and inform consumers through the benchmarking health care indicators. 35 36 The strategies outlined for consideration of the Summit participants are divided into three 37 broad sections: 38 39
Establishing a state-sponsored planning function with separate divisions that 40 address analysis and policy, quality, community assessment, and regulation 41
Establishing an office of health care professional workforce development 42 Initiating the coordinated development of health information technology and 43
health information exchange in Nevada 44 45
Each of these broad strategies is addressed in turn in this policy brief. 46

Burns & Associates, Inc. VI-2 May 5, 2006
III. OVERVIEW OF HEALTH SYSTEMS PLANNING 1 2 The need for a centralized planning component charged with comprehensive health 3 planning was identified in almost every focus group. The ideal planning function would 4 have a systematic process for collecting and disseminating quality and performance data, 5 assessing and evaluating community and statewide health care system needs, compiling 6 and analyzing data, and developing policy options. It is also possible for regulatory 7 functions to be included in the planning body’s portfolio of activities. 8 9 Several states have state-level health systems planning functions. These programs vary 10 in their scope and in their size. 11
For example, California has the Office of Statewide Health Planning and Development in 12 the Department of Health Services. This Office is responsible for analyzing health care 13 quality and costs, making policy recommendations for future health-related needs, 14 conducting research activities in the development of statewide health policy, and 15 disseminating data to various audiences. The Office produces risk-adjusted reports on 16 hospital and physician outcomes; produces reports on current health care policy issues; 17 analyzes and makes recommendations on specific issues affecting the quality or cost of 18 health care. It also has programs that address health care workforce, facilities 19 development and an insurance program for health facility construction. The budget for 20 this Office is approximately $70 million per year and it has 388 positions, with close to 21 200 of the positions (and $34 million) in facilities development. 22
Another example is the Office for Oregon Health Policy and Research. This Office has a 23 more narrow focus to provide analysis, technical, and policy support to assist the 24 Governor and the Legislature in setting health policy. It conducts analyses relating to 25 health care costs, utilization, quality, and access as well as providing staff support to a 26 number of commissions and advisory bodies. The budget for this office is $5 million of 27 which $1.4 million is general fund. The Office has 17 positions. 28 29 A final example is Maryland’s Health Care Commission. This body was established as 30 both a health care regulatory office and an entity that articulates, coordinates, and 31 implements health policy. The Commission is charged to: 32 33
Direct and administer state health planning functions to produce the State 34 Health Plan 35
Monitor the fiscal impact of state mandated benefits 36 Develop a database on all non-hospital health care services 37 Develop quality and performance measures for hospitals, ambulatory care 38
facilities, nursing homes and health maintenance organizations 39 Develop the comprehensive standard health benefit plan for small employers 40 Oversee electronic claims clearinghouses 41 Conduct the Certificate of Need program for regulated entities 42
43 The Maryland Health Care Commission operates with a budget of approximately $8.9 44 million. 45

Burns & Associates, Inc. VI-3 May 5, 2006
IV. STRATEGIES FOR A NEVADA HEALTH CARE PLANNING 1 FUNCTION 2
In order to plan for the current and future health care needs of Nevadans, and to improve 3 effectiveness of the health care system, the following strategy for a health care planning 4 function was developed for consideration of Summit participants: 5
An Office of Health Planning will be created to oversee health care planning and 6 policy development within Nevada. The Office of Health Planning will be 7 comprised of four divisions: 8
9 Division of Analysis and Policy 10 Division of Quality 11 Division of Community Assessment 12 Division of Facilities Planning 13
14 This strategy was developed from the following “high scoring” recommendations from 15 the focus groups that addressed the need for planning: 16 17
1. Develop a comprehensive and systematic process to identify community costs, 18 access issues, service gaps, duplication of services/programs, impact of aging 19 population, etc. (community needs assessment). [Medical Coverage focus 20 group] 21
22 2. Create a new model for the delivery of health care services that includes use 23
of technology and independent practice models. [Public Health focus group] 24 25 The functions of each division will be briefly discussed below. 26 27 Division of Analysis and Policy 28 29 This division will integrate available data, perform analysis, plan for the health system 30 needs, promote informed decision-making, and provide accurate information about cost 31 of health care and health care related issues to the public and Nevada’s policymakers. 32 33 The Division will be a major focal point for state health policy development. It will be 34 responsible for identifying current health issues and emerging trends that will affect the 35 State. It will conduct policy analysis on issues relating to health care and the delivery of 36 health care services. The Division will partner with health care experts and stakeholders 37 from across Nevada to develop projects focused on improving the health status and 38 access to health care services in the most efficient and effective manner. 39 40 The Division will also prepare and update a biennial State Health Plan. 41 42 43 44

Burns & Associates, Inc. VI-4 May 5, 2006
Division of Quality 1 2 This Division will promote more informed decision making through the dissemination of 3 information about the quality and price of health care services provided in Nevada. The 4 public and health care providers will be the target audience of this Division. 5 6 In the short term, the Division will produce reports on current issues affecting quality of 7 health care. This activity may begin by focusing on the publicly reported health care 8 quality information currently available. In the future, it is anticipated to produce risk-9 adjusted reports on health care facility and provider outcomes and provider pricing 10 information to the public. 11 12 Division of Community Needs Assessment 13 14 This Division will perform community needs assessments throughout Nevada that will 15 serve as the basis for responding to gaps in services, disparities among populations and 16 better health outcomes for all Nevadans. 17 18 A community health assessment is a tool used to assess the overall health status of a 19 given population. Through extensive information gathering, the assessment identifies the 20 availability of resources, such as the number of physicians or hospitals, as well as 21 financial sources, such as state or federal funding or grants. It also provides a snapshot of 22 the health status of the population, including factors which may have specific effects on 23 health, such as smoking. The information from the assessment is then used to propose 24 solutions and to make informed policy decisions on how best to meet the needs of the 25 population. 26 27 It will also be the responsibility of this Division to recommend benchmarks for the health 28 care system so improvements to the system can be measured. 29 30 Division of Facilities Planning 31 32 If the Summit participants support the expansion of the certificate of need (CON) process 33 in Nevada, this Division will operate the CON program. CON programs regulate the 34 placement of new health care facilities and/or services. Nevada has an existing CON 35 program that has been in place since 1972. Washoe and Clark Counties were exempted 36 from the CON in 1991. The law currently covers only construction of new health 37 facilities requiring capital expenditures in excess of $2 million. 38 39 If a broader CON were to be adopted, the specific scope of the new CON will have to be 40 developed, but could extend to all hospitals and selected acute care services intending to 41 develop or improve capacity, services, or facilities. The CON process would be intended 42 to maximize cost effectiveness, quality, and access to health care services by eliminating 43 redundancy and inefficiency in the provision of health care services. 44

Burns & Associates, Inc. VI-5 May 5, 2006
The literature does not contain convincing data demonstrating that CON programs have 1 achieved the goal of containing health costs, but evidence does exist that CON has been 2 successful in redirecting funds from investments in capital to the subsidization of indigent 3 care. 4
The Federal Trade Commission and the Department of Justice issued a report in 2004 5 which recommended that states reconsider their CON process on the basis that it does not 6 control health care costs and is used by market incumbents to create barriers to 7 competition. 8 9 Cost Estimate 10 11 The estimate for this strategy was developed after examining the operating budgets fro 12 the California and Oregon models. The estimate should be considered a “placeholder 13 estimate” and subject to revision. The estimate reflects an average budget per person of 14 $150,000, which is all-inclusive of wages, benefits, capital and operating costs. The 15 estimate for each division, reflected by the number of staff and budgeted cost per person, 16 are shown in the table below. 17 18
Division Number of FTEs Total Budget Administrative Umbrella over all Divisions 2 $300,000
Division of Analysis and Policy 5 $750,000 Division of Quality 2 $300,000 Division of Community Assessment 6 $900,000 Division of Facilities Planning 3 $450,000 TOTAL 18 $2,700,000
19 20

Burns & Associates, Inc. VI-6 May 5, 2006
V. OVERVIEW OF HEALTH CARE WORKFORCE PLANNING 1 2 The second major strategy in this planning policy brief is the establishment of an Office 3 of Healthcare Workforce Development. 4 5 Nearly all states have a shortage of some type of health care professional. According to a 6 2002 survey of the states, 90% of the states had a shortage of Registered Nurses and a 7 majority had shortages in five other professional categories. 8 9
Percent of States Experiencing Shortages in Selected Health Professions, 2002
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Registered Nurses Pharmacists Certified NursingAssistants
Home Health Aides RadiologicTechnicians
Dentists
10 Source: The Center for Health Workforce Studies, School of Public Health, University at Albany, SUNY. “State Responses to 11 Health Worker Shortages: Results of 2002 Survey of States,” November 2002. 12
13 There is concern that with an aging population across the country, the supply of health 14 care professionals will not adequately respond to increasing demand. This concern has 15 spurred 44 states to create commissions charged with finding ways to encourage more 16 people into these fields (see Appendix to this document). Examples of initiatives 17 undertaken by states include: 18 19
Creating task forces related to workforce development 20 Developing loan repayment programs for individuals entering health care 21
professions 22 Health career marketing 23 Career ladder development 24 Labor department or workforce investment boards 25 Collecting and tracking workforce data on health care professions 26

Burns & Associates, Inc. VI-7 May 5, 2006
If most states have a workforce shortage problem, Nevada has one of the worst. In 2000, 1 Nevada ranked among the bottom states in the number of health care professionals per 2 100,000 residents for almost all of the health care profession categories. Nevada’s 3 population grew at a rate approximately three times the national average in 2005, so 4 without substantial growth in the health care workforce, these rankings very well may 5 deteriorate. 6 7 The Health Care Professional Education policy brief outlines strategies that the Summit 8 participants may want to consider for educating health care professionals in Nevada. 9 This brief outlines several strategies that Nevada could use to attract and better utilize 10 health care professions that have completed their education. 11 12 13 VI. STRATEGIES FOR PROFESSIONAL WORKFORCE DEVELOPMENT 14 15 In order to ensure that planning for health care professionals in Nevada includes a 16 workforce component, the following strategy was developed for consideration by Summit 17 participants: 18 19
An Office of Healthcare Workforce Development will be created to oversee 20 professional workforce planning and policy development in Nevada. The Office will 21 be composed of three divisions: 22 23
Division of Analysis and Planning 24 Division of Special Projects on Regulatory Affairs 25 Division of Incentive Administration 26
27 These strategies were developed from the following “high scoring” recommendations 28 from the focus groups that addressed the need for workforce planning: 29 30
1. Establish an independent task force to determine how to better utilize licensed 31 health care health professionals in order to address workforce needs. [Health 32 Care Professionals focus group] 33 34
2. Create and fund independent commission to study and develop a 35 comprehensive plan that includes all the options (e.g., training, recruitment, 36 retention, Graduate Medical Education (GME), use of retirees) for addressing 37 health care professional workforce needs. [Health Care Professional 38 Education focus group] 39 40
3. Examine the interaction of health care disciplines and their scopes of practice 41 in order to develop strategies for improving utilization of health care 42 professionals in the State. [Health Care Professionals focus group] 43 44
4. Expand use of ancillary personnel (e.g., pharmacy technicians). 45 [Pharmaceutical Coverage focus group] 46

Burns & Associates, Inc. VI-8 May 5, 2006
Nevada needs to find effective and immediate ways to address their growing shortages of 1 health care professionals. While the expansion of health care professional education is an 2 important strategy, emphasis also needs to be placed on recruitment and retention in 3 terms of both new graduates and already trained professionals who are licensed in other 4 states. 5 6 The private sector has taken the lead in this endeavor with a variety of approaches 7 including providing both monetary (e.g. signing bonuses, compensation packages, 8 financial assistance to set up practice) and non-monetary incentives (e.g., redefined job 9 specifications). 10 11 The State can also play a significant role in shaping an attractive health care workforce 12 environment. This can include: 13 14
Documenting where shortages are most acute through data analysis and 15 reporting 16
Tracking and monitoring the strategies used throughout the State to attract 17 health care professionals 18
Monitoring the State’s regulatory activities 19 Developing and administering provider incentives, and 20 Providing attractive compensation for health professionals working for public 21
programs 22 23
Any efforts the State undertakes must carefully balance the need to address workforce 24 shortages with the mandate to protect the public health and safety. 25 26 According to the 2002 survey conducted by the State University of New York (SUNY) 27 Center for Workforce Studies, 44 states have convened task forces or commissions to 28 study workforce shortages and develop recommendations to address workforce supply 29 and demand (see Appendix). In most cases, these bodies were temporary; however, in a 30 few cases, they evolved into more permanent structures. For example: 31 32
The Iowa Center for Health care Workforce Planning was established in 2002 33 and is housed in the Iowa Department of Public Health. This Center came 34 about as a result of a task force initiated by the Governor on Iowa’s nursing 35 shortage. The Center’s mission is to assess and forecast health workforce 36 supply and demand; address barriers to recruitment and retention; support 37 strategies developed at the local level that prevent shortages; and assure a 38 competent, diverse health workforce. There is an Advisory Committee that 39 meets quarterly with approximately 20 representatives, most of whom come 40 from the nursing profession. Funding has come from three grants from the 41 Health Resource and Services Administration (HRSA) through its Bureau of 42 Health Professions. The grants have amounted to almost $2.9 million, which 43 cover the period July 2002 to August 2005. 44
45

Burns & Associates, Inc. VI-9 May 5, 2006
The Indiana State Health Care Professional Development Commission was 1 established in 1995 and reports to the State Health Commissioner. There are 2 60 commissioners who represent all aspects of health care from both the 3 public and private sectors. The Commission is directed to study the 4 distribution of health care professionals, develop a strategic plan for 5 professional development, and make recommendations to the General 6 Assembly to achieve an even flow of health care professionals with 7 appropriate distribution by specialty and type. Indiana has received federal 8 grant money of $274,402 covering the years FY 2005-06 and FY 2006-07. 9 The State legislature has matched the funds in each year. 10
11 The California Office of State Health Planning and Development, Healthcare 12
Workforce Division provides training courses for individuals to grow health 13 care professionals in underserved areas, promotes public/private partnerships 14 to increase the number of health care professionals, administers loan 15 repayment programs and tuition assistance to economically disadvantaged 16 students and graduates pursuing careers in the health care profession. The 17 budget for the Healthcare Workforce Division is $16.3 million in FY 2007 18 and it has 26 positions. 19
20 By establishing an Office of Healthcare Workforce Development (OHWD), Nevada 21 would begin to centralize its response to shortages of health professionals. 22 23 The Nevada OHWD could include a Health Workforce Advisory Council with members 24 appointed by the Governor. The membership would represent government agencies, 25 education institutions, the health care industry and other interested parties (e.g., 26 consumers, advocates, unions). The council could help guide data collection and 27 analysis, shape recommendations regarding changes to regulatory processes and changes 28 to scopes of practice, and identify strategies to recruit and retain health professionals. 29 30 The OHWD could be housed either in a consolidated health planning entity that will be 31 formed, be a separate office, or be housed in the Department of Health and Human 32 Services. 33 34 The functions of each division of the office are briefly discussed below. 35 36 Division of Analysis and Planning 37 38 This Division will have overall responsibility for developing options to address Nevada’s 39 health care workforce needs. 40 41 In executing this mission, the Division will provide staff support to the Health Workforce 42 Advisory Council; collect, maintain and provide an analysis of data; issue reports; link 43 with universities, relevant state departments and other public and private entities; and 44 commission studies. In addition, the Division will monitor developments in other states, 45

Burns & Associates, Inc. VI-10 May 5, 2006
research and apply for grant opportunities, and issue a biennial report on the status of, 1 and issues confronting, the Nevada health care workforce. 2 3 To a limited degree, the Division could also operate as an information clearing house for 4 out of state health care professionals considering relocating to Nevada. 5 6 Division of Special Projects on Regulatory Affairs 7 8 This Division will be charged with a review of the State’s regulation of health care 9 professionals. It will fulfill this responsibility by undertaking three initial projects, and if 10 at the completion of these projects it is determined that the division has completed its 11 mission, it will expire. 12 13 The three initial projects that this Division will be assigned include 1) a review of the 14 advisability of maintaining separate health care professional licensing boards; 2) a review 15 of the operation of the boards with respect to inappropriate barriers to licensing, and; 3) a 16 review of the scopes of practice statutes for the various licensed professionals. 17 18 The balance of this discussion presents information on each of these three assignments. 19 20 Examining Consolidation of Licensing Boards 21 22 There are currently 19 separate health care professional licensing boards in Nevada. 23 Each of these boards is established in statute and has a set of accompanying regulations 24 that detail their responsibilities. 25 26 According to a paper prepared in 2005 by the North Dakota Legislative Council, there are 27 33 states with central regulatory agencies. The role of consolidated boards and 28 administrators varies considerably. In some states, the boards have maintained all of 29 their regulatory authority with the central agency merely performing administrative duties 30 such as payroll, purchasing, printing, etc. In other states, the boards serve as advisory 31 bodies to the director of the umbrella agency. 32 33 The pros and cons of consolidation have been debated for years. According to the 34 Council on Licensure, Enforcement and Regulation (CLEAR), perceived benefits of a 35 centralized agency include: 36 37
Administrative efficiency – Allows for consolidation of staff, space, time and 38 equipment 39
Coordination – Provides a single point of contact for consumer questions and 40 complaints as well as for legislative and executive interaction 41
Oversight – Increases equity through uniform application of criteria for board 42 decisions 43
Accountability – Provides greater accountability to public and legislature 44 45 Arguments that have been made to retain autonomous boards include: 46

Burns & Associates, Inc. VI-11 May 5, 2006
Need for professional expertise – Assures appropriate peer review of 1 professional practice standards, qualified personnel to investigate complaints, 2 and professional perspective of the public interest 3
Administrative efficiency – Provides for efficient decision-making, greater 4 visibility to the public, and serves as a deterrent to potential violators 5
Insulation from political interference – Provides for better understanding of 6 the licensees’ and public’s concerns 7
Accountability – Provides for greater controls over allocation of funds and 8 clearer levels of accountability 9
10 One model for consolidation of state licensing board that Summit participants may want 11 to consider is Virginia. Established 20 years ago, the Department of Health Professions 12 is made up of 13 health regulatory boards including the Boards of Audiology and Speech 13 Pathology, Counseling, Dentistry, Funeral Directors and Embalmers, Health Professions, 14 Long-Term Care Administrators, Medicine, Nursing, Optometry, Pharmacy, Physical 15 Therapy, Psychology, Social Work, and Veterinary Medicine. 16 17 Under the Virginia model individual case decisions regarding licensing are made by the 18 individual boards and can only be appealed through the courts. However, most other 19 administrative functions are carried out at the Department level including: 20 21
Complaint receipt and investigation (with results turned over to the individual 22 boards for action) 23
Legislative recommendations 24 Rule making 25 Information technology -- there is one computer system which tracks license 26
renewals and accounts for revenues. Approximately 80% of the renewals are 27 done online. 28
Finance 29 Human Resources 30
31 Virginia believes that this model enhances the efficiency of the various boards’ 32 operations. 33 34 Summit participants may wish to consider recommending a study to determine the 35 advantages and disadvantages of the current health professional licensing organizational 36 structure and the identification of options that would better serve the state. 37 38 Examining Potential Barriers in the Licensing Application and Renewal Process 39 40 Anecdotal evidence suggests that health care professional licensing can be a painfully 41 protracted process for both health care professionals and the licensing boards. 42 43 During the focus group process there were reports of long waiting times, inefficiencies 44 and a desire to be “regulatory friendly” to health care professionals seeking to locate in 45 Nevada. To ensure that health care professional licenses are being granted in the most 46

Burns & Associates, Inc. VI-12 May 5, 2006
“regulatory friendly” fashion consistent with the protection of the public, the Division of 1 Special Projects on Regulatory Affairs could undertake a project to evaluate: 2
The amount of time it takes from application to granting of license for each 3 board. The resulting data would be compared to comparable licensing 4 activities both within the State and in other states. Process improvements 5 should be identified and implemented for those boards where granting of 6 licenses falls outside of an acceptable time frame. 7
The licensing/certification requirements in Nevada compared to the rest of the 8 nation. This evaluation would assess such items as testing, educational and 9 internship requirements for licensure. This may reveal unnecessary barriers 10 these requirements pose to potential licensees. The result of this evaluation 11 could also lead to alternative levels of licensing. 12
The extension of endorsements and reciprocity to out of state health care 13 professionals. 14
The timing and accessibility for required tests, in terms of both administering 15 and scoring. This could include utilization of electronic and on-demand 16 testing (e.g. Certified Nurse Assistant testing through a contract between the 17 Board of Nursing and a private testing company). 18
The use of an online application and renewal process for licenses. 19
Examining the Scope of Practice Statutes and Rules 20
The 1995 Pew Health Professions Commission Report, which is still the seminal study on 21 workforce regulation, suggests that states should base their practice acts on health care 22 professionals being able to demonstrate competence based on knowledge, training, skills 23 and experience. Moreover, states must allow and expect different professionals to share 24 overlapping scopes of practice. Unnecessarily restricting practices can result in 25 diminished services to the consumers, particularly in medically underserved areas. 26
Since the release of the Pew Commission Report, the use of physician extenders (e.g., 27 advanced practice nurses and physician assistants) is playing an increasingly important 28 role in the delivery of effective health care services. The Council on Graduate Medical 29 Education reports (2004) that many of these non-physician clinicians are now operating 30 with a new degree of practice autonomy based on statutory and regulatory changes that 31 have been made in many of the states. 32
Nevada should review existing scopes of practices to see if there are ways to allow health 33 care professionals such as physicians’ assistants, advanced practice nurses, pharmacists 34 and pharmacy technicians, as well as dental hygienists to act as extenders beyond what 35 they are currently permitted to do. Any change would likely have to be accompanied by 36 a demonstration of the necessary skills to safely perform any expanded duties, or provide 37 that they be performed under appropriate supervision. 38
California has a program that provides for health care related organizations to 39 demonstrate, test and evaluate new or expanded roles for health care professionals or new 40

Burns & Associates, Inc. VI-13 May 5, 2006
health care delivery alternatives prior to amending regulations or laws. With this pilot 1 program, trainees in pilot projects are exempted from other provisions of the law. 2
Division of Incentive Administration 3 4 This Division will be charged with administering any incentive programs that the State 5 may adopt to attract or retain medical professionals in the State, or in a particular area of 6 the state. 7
Nevada needs to consider strategies to attract students who have completed their 8 education to stay in Nevada as well as to recruit out of state professionals. The Division 9 of Analysis and Planning could develop such incentive programs that would be 10 administered by the Division of Incentive Administration. The strategies developed 11 could be based on the best practices from other states. Some options for incentives that 12 the Summit may consider recommending include: 13 14
Loan Repayment Programs – The Nevada Health Services Corp is the state’s 15 only health education loan repayment program. With just over $100,000 in 16 state and federal matching funds, the NHSC is currently supporting 13 active 17 participants including MDs, dentists, clinical social workers and mental health 18 workers. The NHSC is relatively quite small in comparison with other states. 19 For example, Indiana contributes approximately $1 million annually to three 20 loan repayment programs for physician and nursing students and Arizona 21 contributes more than $500,000 to several loan repayment programs. 22
23 These programs allow loan forgiveness in exchange for providing a certain 24 number of years (usually two to five years) in a medically underserved area. 25 Loan programs can be targeted to primary care physicians – which can be 26 matched by HRSA grant funds – as well as a broad array of other health 27 professionals. While there is some concern that these loan repayment 28 programs do not provide long-term solutions, they can be an effective interim 29 solution as other longer-range options are put into place. 30
31 Health Professionals Employed by Public Programs – There are several health 32
care professionals working for public programs in the State. With state 33 personnel rules and the necessity for legislative appropriations, the State is 34 often not as nimble in responding to market forces as is the private sector. As 35 a result, it is not unusual for health professionals working in the public sector 36 to be compensated at lower than market levels, with the result being position 37 vacancies and difficulties in recruiting. 38
39 This is acutely true in the area of mental health services. With the large 40 number of mental health facilities and services operated by the State, it is 41 critical that the State address its own shortages of health care professionals. 42 To address this need, the Office of Workforce Development may undertake 43 salary surveys and review the needs for stipends and other payments to attract 44

Burns & Associates, Inc. VI-14 May 5, 2006
and retain health care professionals, particularly in rural and remote areas. A 1 fund could be made available to the Interim Finance Committee that could be 2 released during the biennium to address these requirements. 3
4 In addition to creating new incentive programs, the State should ensure that it is 5 maximizing the incentive programs that are available on a national level, and identify 6 potential private funding sources to supplement these programs. A possible strategy for 7 Summit participants to consider would be to transfer the administration of existing 8 federal programs to the new OHWD. The programs that could be transferred include: 9 10
The National Health Service Corps (NHSC) program. This program is 11 currently administered by the DHHS Primary Care Development Center. 12 There is no cap on the number of students who can receive this funding. 13
14 The J-1 Visa Waiver Program. This program allows foreign physicians who 15
have completed medical training in the United States to remain in this country 16 after their studies are completed if they satisfy certain requirements including 17 serving in a medically underserved area for at least three years. In 2004, the 18 J-1 Waiver Program was extended to 2006 by Congress and permitted up to 19 five of the 30 annual authorized slots per state to be placed in areas that are 20 not classified as medically underserved. In March 2006, a bill was introduced 21 to permanently extend J-1 Waiver Program. 22
23 The Nevada J-1 Waiver Program is also administered by the DHHS Primary 24 Care Development Center. There are currently 68 physicians (out of a 25 possible 90) in the program. 26
27 Cost Estimate 28 29 “Placeholder estimates” have been prepared for the three components of the Office of 30 Healthcare Workforce Development: 31 32
Establish the Office of Healthcare Workforce Development with an operating 33 budget of $1,200,000 per year. In addition, the OHWP would pursue federal 34 grant money either from HRSA or other federal agencies (e.g. the Department 35 of Labor, Employment and Training Administration’s Business Relations 36 Group). 37
38 Review and Revise Health Care Licensing, Operations, and Scopes of 39
Practice. A “placeholder estimate” of $300,000 for the SFY 08-09 biennium. 40 41
Establish and fund a loan repayment program. A “placeholder estimate” of 42 $500,000 per year is recommended. In addition, a one-time funding of 43 $50,000 is suggested to retain outside assistance to identify HRSA or other 44 federal grant opportunities to expand the loan repayment program in Nevada 45 and to write the grant application(s). 46

Burns & Associates, Inc. VI-15 May 5, 2006
VII. OVERVIEW OF HEALTH INFORMATION TECHNOLOGY AND 1 HEALTH INFORMATION EXCHANGE 2
3 The third major strategy area with respect to planning for the Summit participants to 4 consider is the area of health information technology and health information exchange. 5 Given the relatively scarce health care resources in the State, it is essential that existing 6 resources be used as efficiently and effectively as possible. Health Information 7 Technology (HIT) and Health Information Exchange (HIE) are strategies that promote 8 efficiency in the delivery of health care. 9 10 HIT refers to the information technology used by providers in their offices, clinics, 11 laboratories and hospitals. Examples include electronic prescribing, digital results 12 delivery, and electronic medical records. HIE is the exchange of that information with 13 other providers, with consumers, with health quality monitoring organizations, and with 14 payers and researchers. 15 16 The Rand Corporation recently estimated that HIT would save the nation $77 billion 17 annually if its adoption were widespread. Savings accrue primarily through: 18 19
Reductions of medical errors 20 Increased efficiency 21 Avoidance of duplicative health care procedures 22 Improved coordination 23 Increased participation of consumers 24
25 There is considerable momentum at the federal level both in Congress and within the 26 Administration in moving toward comprehensive HIT and HIE. The Office of the 27 National Coordinator for Health Information Technology (ONCHIT) was established “to 28 achieve 100 percent electronic health data exchange between payers, health care 29 providers, consumers of health care, researchers and government agencies as 30 appropriate.” 31 32 The Centers for Medicare and Medicaid (CMS) also has a number of initiatives to 33 support the adoption of health information technology, including the Doctor’s Office 34 Quality Information Technology (referred to as DOQ-IT), a pay for performance 35 demonstration, and a chronic disease demonstration program. Eleven legislative 36 initiatives have been proposed (with funding) in Congress to promote health information 37 technology and exchange. A number of states such as Arizona, Indiana, Kentucky, 38 Louisiana, Massachusetts, Michigan, New York, Oregon and Rhode Island have taken 39 steps to guide the development of HIT and HIE. 40 41 In 2005, eHealth Initiative conducted the Second Annual Survey of State, Regional, and 42 Community Based Organizations on Emerging Trends and Issues in Health Information 43 Exchange (supported by a Cooperative Agreement with the Health Resources and 44 Services Administration, Department of Health and Human Services). eHealth Initiative 45

Burns & Associates, Inc. VI-16 May 5, 2006
is a national organization that monitors HIT and HIE initiatives across the states and 1 provides assistance to states that want to move forward. In April 2006, the eHealth 2 Initiative released the rankings of states in the western region on their stage of progress 3 toward HIE: 4 5
Stage 1 Awareness 6 Stage 2 Regional Activity 7 Stage 3 State Leadership 8 Stage 4 Statewide Planning 9 Stage 5 Statewide Plan 10 Stage 6 Statewide Implementation 11
12 Nevada was ranked at Stage 1 behind all of the other states in the west including Arizona 13 (ranked at Stage 4) and California, Colorado, Utah and New Mexico (all ranked at Stage 14 2). 15 16 It is important to recognize that there are barriers in statewide implementation of HIT and 17 HIE. These barriers include: 18 19
The cost of implementation, which Rand estimates at $8 billion per year 20 nationally for HIT alone 21
Privacy and security concerns 22 Lack of a governance structure 23 Lack of interoperability standards for HIE 24 Consumer resistance 25 Provider resistance 26 Regional differences, e.g. rural areas face particular challenges in adoption of 27
HIT and HIE 28 Laws and regulations 29
30 There are health information technology initiatives going on in Nevada but there are few 31 initiatives in health information exchange. The following descriptions of the ongoing 32 HIT efforts are illustrative of what is occurring in Nevada. 33 34 Sierra Health Services is aggressively moving to statewide electronic prescribing and has 35 already adopted electronic health records. As a result, their clinics and facilities are 36 almost paperless. 37 38 For e-prescribing, Sierra implemented Allscripts initially in Southwest Medical 39 Associates, a unit of Sierra covering 250 physicians. Based on the success of this 40 initiative, Sierra is now working with the Clark County Medical Society (CCMS) to 41 provide e-prescribing for all physicians practicing in the State. Physicians who are 42 members of CCMS will receive the software license for ten years at no charge and up to 43 two years of monthly maintenance fees. Physicians outside of Clark County will receive 44 the software at no charge, but will be responsible for monthly maintenance fees. 45 46

Burns & Associates, Inc. VI-17 May 5, 2006
The benefits of e-prescribing include: 1 2
Reduction of medication errors 3 Improved patient safety 4 Allowing physicians to select appropriate doses 5 Alerting the physician if the drug is contraindicated or if there are other 6
safety concerns 7 Accessing current consumer medication histories 8
9 Sierra adopted an electronic medical record in its facilities and clinics in 2004. Using the 10 TouchWorks system, 700,000 patient records are available through a secure website to 11 the 250 physicians at Southwest Medical Associates. Sierra offers members of its health 12 plan access to a snapshot of their medical records, including online access to test results. 13 14 Washoe Medical Center had previously adopted an electronic medical record, but it is 15 now implementing the integrated EPIC system. The EPIC system allows a unified record 16 in facilities and ambulatory settings, e-prescribing, and a billing system. Washoe is 17 offering the ambulatory component of the EPIC system to physician offices outside its 18 integrated health system, which makes the Washoe initiative an example of Health 19 Information Exchange. 20 21 University Medical Center (UMC) is in the process of securing funding to replace their 22 current system with a system that: 23 24
Integrates clinical, patient financial and hospital administrative systems 25 Provides for a comprehensive electronic medical record 26 Allows electronic physician ordering 27 Provides a results delivery system 28
29 UMC already has in place the Picture Archiving Communication System which provides 30 online access to its 1,600 physicians of results from radiology and cardiovascular testing. 31 UMC also has in place a financial and clinical decision support system that examines 32 health outcomes and enables case management. 33 34 The Center for Health Data and Research housed within the Bureau of Health Planning 35 and Statistics of the DHHS is developing a data warehouse that will link 35 health and 36 related databases. The data warehouse will link the databases with common identifiers to 37 provide standardized information for research, statistical/analytical and programmatic 38 purposes. The data warehouse will be available on-line. The Center works with 39 University of Nevada – Las Vegas (UNLV) Center for Health Information and Analysis 40 (CHIA) which currently provides on-line access to hospital financial and utilization 41 information. 42 43 There is other activity in HIT in Nevada including Spring Valley Hospital, where 44 components of an electronic medical record have been implemented. The system 45 includes such features as vital signs, digital online test results and electronic ordering. 46

Burns & Associates, Inc. VI-18 May 5, 2006
As evidenced by eHealth Initiative’s ranking, Health Information Technology in Nevada 1 is developing in silos with little activity in Health Information Exchange. Summit 2 participants should consider a strategy to initiate a planning process with the goal of 3 implementing Health Information Technology and Health Information Exchange within 4 ten years. Implementation of such systems will help to restrain health care expenditures 5 as well as improving the quality of care. 6 7 The benefits of such systems for the citizens of the State are: 8 9
Reduction of medication errors that could lead to adverse consequences 10 Making available patient’s conditions, treatments, allergies and medication 11
history during an emergency 12 Reducing unnecessary and duplicative tests and procedures because there will 13
be sharing of the results among providers 14 Coordination of care across the health care delivery system through the 15
sharing of information, with resulting improved health outcomes 16 Consumers can access their own health record and test results 17 There is a restraint on increasing health care costs, resulting in an improved 18
business environment 19 20 The State can provide leadership in the execution of this strategy by sponsoring the 21 planning process, providing financial support for Health Information Technology and by 22 supporting Regional Health Information Organizations moving to Health Information 23 Exchange. Implementation of HIE is likely to occur regionally for a number of reasons, 24 most notably because there are existing relationships within the health care delivery 25 system in a region and, as a result, the trust necessary for data sharing agreements already 26 exists. 27 28
VIII. STRATEGIES FOR HEALTH INFORMATION TECHNOLOGY AND 29 HEALTH INFORMATION EXCHANGE INITIATIVES 30
31 In order to ensure that Nevada develops health information technology and coordinates 32 the development of health information exchange, the Summit participants may wish to 33 consider the following strategies: 34 35
A time-limited statewide Steering Committee will be convened and supported 36 by the State for the purpose of developing a high level plan for e-Health 37
A statewide governance committee will be created and funded to implement 38 the steering committee’s high level plan 39
Subsidies will be provided for the adoption and use of HIT and HIE 40 Legislation will be enacted to clarify and protect consumer privacy 41
42 These strategies were developed from the following “high scoring” recommendations 43 from the focus groups that addressed the need for health information technology and 44 health information exchange: 45

Burns & Associates, Inc. VI-19 May 5, 2006
1. Develop a plan to leverage technology related to electronic transfer of 1 information for both data base analysis and medical records. [Medical 2 Coverage focus group] 3 4
2. Create a new model for the delivery of health care services that includes use 5 of technology and independent practice models. [Public Health focus group] 6
7 3. Fund program(s) targeted at increasing use of e-prescribing. [Pharmaceutical 8
Coverage focus group] 9 10 Each of the strategies for Summit participants to consider is discussed below. 11 12 Statewide Steering Committee for e-Health 13 14 A Statewide Steering Committee for e-Health should be convened as soon as possible to 15 develop the direction and a high level plan for statewide implementation of HIT and HIE 16 within ten years. The Steering Committee activities should be supported with state and 17 private resources. 18 19 The primary responsibilities of the Steering Committee are to: 20 21
Create a vision for HIT and HIE in Nevada 22 Begin an inventory of HIT and HIE initiatives 23 Test the waters with Nevada leaders 24 Identify and propose solutions to barriers to implementation 25 Develop a high level plan that can guide implementation over a seven to ten 26
year period 27 28 The Steering Committee should include physicians, hospitals (including public, for profit, 29 urban and rural), health plans, insurers, consumers, medical trade associations, 30 pharmacies, employers, medical schools, unions, government agencies (including 31 Medicaid and the Department of Information Technology), and researchers. 32 33 The entity (e.g., the Governor’s office, Legislature or another entity) that would provide 34 sponsorship of the Steering Committee is an open question. 35 36 In order to expeditiously complete its charge, the Steering Committee will require a 37 subcommittee structure that involves many more stakeholders. At least five 38 subcommittees should be considered: 39 40
The Clinical Subcommittee should be charged with identifying key interim 41 products that will eventually lead to a statewide electronic medical record. 42
The Technical Subcommittee should be charged with developing a technical 43 architecture that leverages current available technology and identifies gaps in 44 the technical infrastructure. 45

Burns & Associates, Inc. VI-20 May 5, 2006
The Legal Subcommittee should be charged with identifying real and 1 perceived legal barriers, and recommending solutions including, but not 2 limited to, issues of privacy, confidentiality, and required statutory changes. 3
The Financial Subcommittee should be charged with making the business case 4 for HIE and recommending short and long term financing strategies for HIE 5 and HIT from all potential sources of funds – government, private sector, 6 grants, etc. 7
The Governance Subcommittee should be charged with developing a public-8 private collaborative structure that defines the responsibilities of the 9 collaborative. 10
11 It is assumed that subcommittees will look to successful initiatives in other states and 12 build on those initiatives. This planning process will take an enormous commitment by 13 the health care system to donate key players and to remain engaged over the several years 14 it will take for statewide health information exchange. 15 16 The resulting high level plan should define: 17 18
The ongoing governance structure for HIT and HIE 19 Identify achievable goals and the steps to get there 20 Establish HIT and HIE priorities 21 Begin to resolve financial barriers including how government can subsidize 22
HIT and HIE 23 Formulate a strategy to ensure that privacy and security is protected 24 Determine how to leverage current Nevada initiatives. 25
26 From the initial Steering Committee meeting, the plan should be completed in six to eight 27 months. At the outset, it is critical that the plan provide for flexibility while at the same 28 time defining (as best it can) at what point in time what needs to occur, why it needs to 29 occur, and who is responsible. 30 31 Governance and Implementation 32 33 Once the Steering Committee plan is formulated, the governance structure recommended 34 should be implemented and provided funds to operate and subsidize early 35 implementation. The governing entity, whether governmental or a nonprofit corporation, 36 will have responsibility for guiding implementation of the plan. The entity will: 37 38
Provide guidance and direction for HIT and HIE in Nevada 39 Guide policy and legislative changes 40 Collaborate with existing HIT efforts in Nevada 41 Develop standards for the interface of HIT and HIE, building on the national 42
efforts defining interoperability standards of ONCHIT and CMS 43 Develop and support Regional Health Information Organizations (RHIOs) and 44
promote health information exchange initiatives 45

Burns & Associates, Inc. VI-21 May 5, 2006
Develop the statewide technical infrastructure that is necessary for data access 1 and sharing, including a web portal for shared information such as a patient 2 health summary, results delivery service, immunization records and advance 3 directives 4
Develop a statewide patient health summary that is a first step toward 5 statewide electronic medical records 6
Receive and distribute funds 7 Create incentives to promote HIT and HIE such as grants and subsidies (see 8
next strategy) 9 10 In order to fulfill these responsibilities, the governing body should be supported with a 11 full time staff, have a governing board comprised of key players, and have an extensive 12 committee structure. The subcommittee structure of the planning process can be 13 maintained so long as the responsibilities of each are clearly articulated in the plan and 14 deliverables are defined. 15 16 Subsidize Adoption of HIT and HIE 17 18 The widespread adoption of health information technology products depends on getting 19 past financial barriers. HIT investment may not be within the financial realities of some 20 providers including: 21 22
Rural providers 23 Small physician offices 24 Safety net providers such as Community Health Centers 25 Public providers 26 The behavioral health system 27
28 HIT investment includes both purchase of the product and ongoing maintenance fees. 29 The state (as well as other sources of funds) should provide financial support to promote 30 the adoption of e-prescribing and electronic medical records statewide. 31 32 Health Information Exchange initiatives also require development and support. The 33 challenges faced by HIE include: 34 35
Initial and ongoing costs and financing 36 Complex interface challenges between HIT systems 37 Concerns about privacy and security including specially protected public 38
health, mental health and substance abuse information, as well as information 39 concerning minors 40
Trust and acceptance within the health care delivery system 41 42 As a result of these challenges, state leadership and financial support will be required. 43 44 45 46

Burns & Associates, Inc. VI-22 May 5, 2006
Enact Legislation Clarifying and Protecting Consumer Privacy 1 2 Based on the work of the Steering Committee and the Governance Body, the State should 3 enact legislation which allows for HIE initiatives that are in compliance with federal 4 HIPAA standards. Nuances in Nevada law may have to be modified to facilitate HIE and 5 encourage information sharing between providers. 6 7 Cost Estimates 8 9 To assist the Steering Committee, an e-Health consultant should be retained at a cost of 10 approximately $350,000. 11 12 The governance structure that succeeds the initial planning process should be fully 13 staffed. A “placeholder estimate” for the cost of staffing and supporting this phase of the 14 planning process is approximately $3 million per year. The State does not have to bear 15 this cost alone. Rather, grants, donations, in-kind contributions, transaction fees and state 16 support can be used. 17 18 A “placeholder estimate” for the costs of supporting rural providers, small physician 19 offices, public providers, as well as safety net providers is $1.5 million annually. This 20 funding should be continued until such time that e-prescribing and electronic medical 21 records have been implemented by providers statewide. 22 23 Health Information Exchange is estimated to cost $2.5 to $4.0 million per one million 24 population according to eHealth Initiate. Here again, other sources of funds including 25 federal grant programs can be tapped. In fact, some electronic information exchange may 26 eventually be self-funded, generating revenue through user fees. As a placeholder 27 estimate, Nevada should appropriate $1.5 million per year to support regional HIE 28 efforts. 29 30 The model statute can be implemented at no additional cost. 31 32

Burns & Associates, Inc. VI-23 May 5, 2006
Resources for Central Planning Overview 1 2 Department of Health and Human Services; Nevada State Health Division Website. 3 4 Hospital Quality Initiative Overview Centers for Medicare and Medicaid Services 5 December 2005 6 7 Rising Health Care Costs: State Health Cost Containment Approaches; Ellen Jane 8 Schneiter; Trish Riley; Jill Rosenthal. 9 10 National Academy for State Health Policy, June 2002 11 12 13 Resources for Workforce Planning 14 15 Arizona Health Cost Containment System Administration (October 2001). Inventory of 16 Arizona Strategies to Address Rural Health Care Infrastructure. 17 18 Arizona Health Cost Containment System Administration (October 2002). Rural Health 19 Care Providers Interviews: Developing a Strong Rural Health Care Infrastructure – 20 Challenges and Successes. 21 22 Center for Education and Health Services Outreach (2006). Medical Education Council 23 of Nevada. Retrieved March 27, 2006 from 24 http://www.unr.edu/med/dept/CEHSO/mecon.html 25 26 Center for Education and Health Services Outreach (2006). Nevada Health Service 27 Corps. Retrieved April 19, 2006 from http://www.unr.edu/med/dept/CEHSO/nhsc.html 28 29 Dower, Catherine (June 2005). Healthcare Workforce: The Role of Regulation. Retrieved 30 from http://www.futurehealth.ucsf.edu 31 32 HRSA Bureau of Health Professions (2004). The Health Care Workforce in Eight States: 33 Education, Practice & Policy. Retrieved April 11, 2006 from 34 http://bhpr.hrsa.gov/healthworkforce/reports/states04/INTERSTATE.htm 35 36 HRSA Bureau of Health Professions (2005). State Health Workforce Data Resource 37 Guide. Retrieved March 30, 2006 from http://bhpr.hrsa.gov 38 39 Indiana Health Care Professional Development Commission (1997). Annual Report. 40 Retrieved April 15, 2006 from http://www.state.in.us/isdh/publications 41 42 Indiana Professional Licensing Agency (2006). Indiana Online Licensing. Retrieved 43 April 12, 2006 from https://extranet.in.gov/mylicense/Login.aspx 44 45

Burns & Associates, Inc. VI-24 May 5, 2006
North Dakota Legislative Council (November 2005). Boards and Commissions – 1 Consolidation Efforts in Other States. Retrieved April 4, 2006 from 2 www.legis.nd.gov/assembly/59-2005/docs/pdf/79101.pdf 3 4 Pew Health Professions Commission (1995). Reforming Health Care Workforce 5 Regulation, Policy Considerations for the 21st Century. Retrieved April 2, 2006 from 6 http://www.futurehealth.ucsf.edu 7 8 Spetz, JoAnne and Dyer, Wendy (June 2005). Forecasts of the Registered Nurse 9 Workforce in California. Retrieved April 2, 2006 from 10 http://www.futurehealth.ucsf.edu 11 12 University of California San Francisco, Center for the Health Professions (2005). The 13 Pharmacy Safety Net. Retrieved April 2, 2006 from http://www.futurehealth.ucsf.edu 14 15 Virginia Department of Health Professions (2006). Health Regulatory Boards. Retrieved 16 April 12, 2006 from 17 http://dhp.state.va.us 18 19 20 Nevada Specific Documents: 21 22 Landreth, K et al. (2006). Nevada Mental Health Problems and Needs. Retrieved April 23 13, 2006 from http://[email protected] 24 25 Nevada State Board of Nursing (2006). Annual Report 2004-2005. Retrieved from 26 www.nursingboard.state.nv.us 27 28 University of Nevada School of Medicine (2006). Post-Graduate Residencies and 29 Fellowships. Retrieved April 9, 2006 from http://www.unr.edu/med/residency 30 31 32 Resources for HIT and HIE Overview 33 34 America’s Health Insurance Plans (2005). Innovations in Health Information 35 Technology. Retrieved April 5, 2006 from 36 http://www.ahip.org./content/default.aspx?bc=31 37 38 America’s Health Insurance Plans. Washington Update – July 1, 2005. Retrieved April 39 5, 2006 from http://www.ahip.org./content/default.aspx?bc=39. 40 41 Center for Health Data and Research (2005). Mission and Center Components. 42 Retrieved April 4, 2006 from http://health2k.state.nv.us/nihds/center.htm 43 44 45

Burns & Associates, Inc. VI-25 May 5, 2006
eHealth Initiative Foundation (2005). Arizona Steering Committee, April 4th, 2006 1 Presentation of the Roadmap. Retrieved April 6, 2006 from 2 http://workspace.ehealthinitiative.org/medigent/collaborate/category/default.aspx?CID=13 26. 4 5 eHealth Initiative Foundation (2005). Arizona Health-e Connection Roadmap. April 6 2006. 7 8 eHealth Initiative Foundation (2006). Arizona Health-e Connection Briefing Paper, 9 Retrieved April 1, 2006 from 10 http://workspace.ehealthinitiative.org/medigent/collaborate/category/default.aspx?CID=111 26. 12 13 eHealth Initiative Foundation (2005). Second Annual Survey of States, Regional and 14 Community-Based Health Information Exchange Initiatives and Organizations. 15 Retrieved April 9, 2006 from 16 http://www.toolkit.ehealthinitiative.org/assets/Documentss/eHI2005AnnualSurveyofHeal17 thInformationExchange2.0 18 19 Interviews on HIT initiatives with Chris Bosse and Chuck Scully, Washoe Medical 20 Center; Jack Kim, Sierra Health System; Terry Savage, Chief Information Officer, 21 Department of Information Technology; Bill Welch, Nevada Hospital Association, Karla 22 Perez, Spring Valley Hospital; Doug Northcutt, University Medical Center 23 24 Rand Corporation (2005). Health Information Technology. Can HIT Lower Costs and 25 Improve Quality? Retrieved April 6, 2006 from 26 http://www.rand.org/pubs/research_briefs/RB9052/index1.html 27 28 Rand Corporation. Electronic Prescribing Systems. Making It Safer to Take Your 29 Medicine? Retrieved April 6, 2006 from 30 http://www.rand.org/pubs/research_briefs/RB9136/index1.htnl 31 32

Burns & Associates, Inc. VI-26 May 5, 2006
Appendix 1
Task Force, Commission
or Panel
Scholarships, Loan
Repayment
Career Ladder
Development
Health Career
Marketing
Labor Department or
Workforce Investment
Board
Job DesignWorkforce
Data Collection
Alabama X X XAlaska X X XArizona X X Arkansas X X XCalifornia X X X X X X XColorado X X XConnecticut X XDelaware X XFlorida X X X X XGeorgia X X X X XHawaii X X XIdaho X X XIllinois X XIndiana X X XIowa X X X XKansas X X XKentucky X XLouisiana X X XMaine X X X XMaryland X X XMassachusetts X X XMichigan X XMinnesota X X X XMississippi X XMissouri X X X XMontana X Nebraska X X X X XNevada X New Hampshire X XNew Jersey X X X X XNew Mexico X X XNew York X X X X XNorth Carolina X X XNorth Dakota X X X X XOhio X X XOklahoma X Oregon X XPennsylvania X XRhode Island X XSouth Carolina X XSouth Dakota XTennessee X XTexas X X X XUtah X X XVermont X X X X X X XVirginia X Washington X X X X X XWest Virginia X X X XWisconsin X X X X XWyoming X X X X# of states 44 38 14 25 7 5 26
Source: SUNY Center for Workforce Studies, 2002 survey
State Initiatives Related to Health Care Workforce Development
2

Burns & Associates, Inc. May 5, 2006 VII-1
Chapter VII 1 Policy Brief on Focus Group Recommendation 2
Prevention and Wellness 3 4 5 I. RECOMMENDATION STATEMENT 6 7
Nevada will expand and initiate programs that will improve the overall health 8 status of its citizens by focusing on prevention and wellness. 9
10 II. OVERVIEW 11 12 Health indicators serve as a benchmark for assessing the health of a given population and 13 provide a baseline for measuring improvement. The Fund for a Healthy Nevada reported 14 statistics on the health status of Nevadans in September 2005. These statistics showed 15 the State ranking low when compared to other states on a number of key health 16 indicators: 17 18
The lowest rate of children vaccinated 19 A high rate of mothers receiving late or no prenatal care 20 The fewest dentists per capita 21 The second highest rate of adults who smoke 22 The highest rate of women smokers 23
24 While these statistics cause concern, there are some areas where the State is showing 25 improvement. The UnitedHealth Foundation report on state health rankings reveals that 26 Nevada has been making positive strides since 1990. Specifically, the State has reduced 27 infant mortality (from 9.4 per 1,000 live births in 1990 to 6.2 per 1,000 in 2005) and 28 reduced the incidence of infectious disease (from 50 cases per 100,000 population in 29 1990 to 23 cases per 100,000 in 2005). 30 31 In its 2005 report, the Foundation ranked Nevada as 37th among the states, citing the low 32 childhood immunization rate, a high violent crime rate, and a high uninsurance rate as 33 Nevada’s primary concerns. 34 35 Other studies also show Nevada with mixed results when compared to other states. For 36 example, the Kaiser Family Foundation’s StateHealthFacts.org website showed that 37 Nevada is generally either average or slightly below average when compared to other 38 states or national averages. 39 40 Kaiser indicates that Nevada compares favorably on its rate of obesity among its 41 population (NV: 19%; US: 21%) and has a very low rate of death related to diabetes (NV: 42 17.6 per 100,000; US: 25.4 per 100,000). The rankings indicate that Nevada is at or near 43 the national average for these measures: 44 45
Cancer deaths per 100,000 (NV: 203; US: 194) 46

Burns & Associates, Inc. May 5, 2006 VII-2
Stroke deaths per 100,000 (NV: 57; US: 56) 1 Heart disease deaths per 100,000 (NV: 246; US: 241) 2 Percent of persons with a disability (NV: 18%; US: 18%) 3
4 The Kaiser rankings also indicate that Nevada ranks below the national average for the 5 following measures: 6 7
Number of deaths per 100,000 (NV: 919; US: 845) 8 Motor vehicle deaths per 100 million miles driven (NV: 2.0; US: 1.6) 9 Percent of adults who are smokers (NV: 23%; US: 21%) 10 Percent of persons reporting poor mental health (NV: 41%; US: 34%) 11 Percent of persons with visits to a dentist or dental clinic in the past year (NV: 12
65%; US: 70%) 13 14 The implementation of prevention and wellness strategies can improve the overall health 15 status of Nevadans and help mitigate the rate of increase in health care expenditures. 16 17 18 II. STRATEGIES 19 20 In order to improve the overall health of Nevadans, the following strategies were 21 developed from recommendations identified by stakeholders in the focus group process: 22
23 1. Improve Early Childhood Immunization 24
25 2. Expand Prenatal Care Services 26 27 3. Expand the Oral Health Care Program 28 29 4. Reduce Exposure to Secondhand Smoke 30 31 5. Invest in Wellness Programs to Prevent Chronic Disease 32 33
These strategies were developed from the following “high scoring” recommendations 34 from the focus groups that addressed prevention and wellness: 35 36
1. Improve funding for chronic disease prevention and control. (Public Health) 37 38 2. Develop primary care and prevention services in order to ease the burden on 39
tertiary care facilities, especially in underserved areas and to ensure a 40 culturally sensitive, holistic approach to caring for patients. (Health 41 Professionals) 42
43 3. Initiate a campaign focused on importance of early detection of health care 44
issues and preventive services as a means to mitigate cost of expensive care 45 later on. (Medical Coverage) 46

Burns & Associates, Inc. May 5, 2006 VII-3
4. Strengthen the Public Health Foundation and expand private-public 1 partnerships. (Public Health) 2
3 The balance of this Policy Brief presents and discusses each of the strategies listed above. 4 5 6 1. Improve Early Childhood Immunization 7 8 Nevada’s rate of childhood immunizations is the lowest in the nation, with only 68% of 9 children ages 19 to 36 months receiving recommended vaccinations. The national 10 average for this age group is 81%. A number of factors have been identified as 11 contributing to the low Nevada rates including: the rapid growth in population, the loss of 12 medical records when citizens move into Nevada, the shortage of health care providers to 13 meet the demand for services, and the lack of utilization of the State’s immunization 14 registry. 15 16 An Institute of Medicine (IOM) report in 2002 called immunization programs a “national 17 treasure that is too often taken for granted”. The report emphasized the importance of 18 reminders and assessments as vital to successful immunization programs and noted that 19 these functions are facilitated by the use of immunization registries. Overall, the IOM 20 ranked immunization registries as one of the most useful instruments for assessing the 21 effectiveness of targeted health and medical care programs. 22 23 An immunization registry is used to consolidate immunization records into a centralized 24 repository. The benefits to having records located in one database and accessible via 25 computer are numerous: 26 27
For families, a registry means there is an official record of immunizations 28 available to meet requirements for day care or school enrollment, a source to 29 verify immunizations are up to date, and a check to prevent unnecessary 30 duplication of vaccinations. 31
32 For health care providers or health plans, a registry provides information on 33
current recommendations or new vaccine requirements, consolidates 34 immunization history from multiple providers into a single record, reduces 35 paperwork, and can provide information about when a patient’s 36 immunizations are overdue. 37
38 For public health officials, a registry provides information for targeting 39
interventions, can be used to generate immunization reminders, and helps in 40 the monitoring of adverse events. 41
42 The recent outbreak of mumps in the Midwest provides an example of a registry’s 43 usefulness. By reviewing records in the state’s immunization registry, Indiana public 44 health officials found almost 200 middle school and high school students in one county 45 had not received the second required measles-mumps-rubella (MMR) inoculation. 46

Burns & Associates, Inc. May 5, 2006 VII-4
1 Nevada has had efforts underway for several years to implement an immunization 2 registry. The Robert Wood Johnson Foundation’s All Kids Count project awarded a two-3 year grant to the State in 1998 to establish an online immunization information system. 4 That project encountered a number of difficulties due to bankruptcy of the software 5 vendor and contractor personnel issues. The goal of establishing a computerized-6 accessible registry was not immediately achieved. In 2003, the State revamped the 7 system and went online in 2004. The registry is now operational and staffed by one IT 8 person. 9 10 The majority of Nevada’s immunization program is federally funded. The State uses 11 funds provided through the Vaccines for Children program, the federal section 317 12 program, the Social Services Block Grant and the Nevada Check-Up program for both 13 the purchase of vaccines and operational expenses. The state support for the program is 14 limited to the state match required for the Nevada Check-Up program. The CDC has 15 indicated it will be cutting funding for the 317 grants (which are the only source of 16 funding for Nevada’s immunization program operations) by 5% in calendar year 2006 17 and by another 5% in 2007. 18 19 Other states provide supplemental support for their immunization program and have 20 enhanced the operation of their registries. For example, New Mexico, a state not too 21 dissimilar to Nevada, has an immunization registry that is staffed with a program 22 manager, help desk support, trainers, quality assurance, and IT personnel. The 23 maintenance cost of New Mexico’s program is $400,000 annually. Another state, 24 Wisconsin, has made the state’s registry accessible to individuals via the internet under a 25 program called ‘Public Immunization Record Access.’ By allowing public access, the 26 registry allows parents to determine whether or not their children’s shots are up-to-date. 27 28 In order to assure that Nevada’s children are appropriately immunized, Summit 29 participants may want to consider enhancing the state’s immunization registry and 30 making it more accessible to public health officials, providers, and families. A strategy 31 for improvement may include: 32 33
Provide additional staff to take advantage of the information captured in the 34 registry. Additional staffing would allow dissemination of information to 35 entities that provide and fund immunizations (e.g., Medicaid, health plans, 36 public health agencies, community health centers, physicians) as well as the 37 monitoring of immunization rates at the local and state level. 38
39 The staff would also train health care professionals in the use of the system, 40 develop tools for statewide and national assessments and reports, and respond 41 to questions. The New Mexico program could be used as a model for Nevada, 42 i.e., provide six additional staff including a program manager, four help desk 43 staff, and a quality assurance/training position. 44
45

Burns & Associates, Inc. May 5, 2006 VII-5
Initiate an outreach and follow-up program with parents. A few months prior 1 to each time a child’s immunization is due, notify the parent via postcard of 2 the need for the immunization. It may be necessary to link the immunization 3 registry with the birth registry to maximize the effectiveness of this strategy. 4
5 Cost Estimate 6 7 The “placeholder estimate” for the additional staff to support and expand the operation of 8 the State’s immunization registry, to initiate the postcard reminder system, and to offset 9 the funding reductions from the CDC is $550,000 a year. 10 11 2. Expand Prenatal Care Services 12 13 The National Center for Health Statistics defines adequate prenatal care as a prenatal visit 14 with a health professional within the first trimester of pregnancy, and additional visits 15 according to a defined periodicity schedule. Nevada ranks 41st in the nation for adequate 16 prenatal care, and 49th in early entry into prenatal care. 17 18 Research has shown a relationship between prenatal care and birth outcomes. It has also 19 correlated prenatal care with improved birth weights. Similarly, lack of such care has 20 been linked to increased risks of low-birth-weight births, premature births, neonatal 21 mortality, infant mortality, and maternal mortality. 22 23 The reasons why women fail to obtain prenatal care are varied and are influenced by age, 24 socioeconomic status, race, or related to the health care system. An Institute of Medicine 25 report conducted a review of studies of risk factors and the lack of prenatal care in 1988. 26 Some of the influences associated with low rates of prenatal care that the report identified 27 included: 28 29
Socio/demographic factors 30 o Poverty 31 o Inner-city or rural residence 32 o Less than 18 years of age 33 o Unmarried 34 o Lack of a high school diploma 35 36
System-related factors 37 o Lack of insurance coverage 38 o Shortage of providers 39 o Language and cultural barriers 40 o Lack of information regarding availability of care 41 42
Attitudinal factors 43 o Unplanned pregnancy 44 o Prenatal care not valued or understood 45 o Fear of doctors, hospitals or procedures 46

Burns & Associates, Inc. May 5, 2006 VII-6
o Lifestyle (drug abuse, smoking, homelessness) 1 o Denial, apathy or concealment of pregnancy 2
3 Other studies have identified race and ethnicity as factors in whether or not a woman 4 receives proper prenatal care. This appears to be true in Nevada as well. The Nevada 5 Vital Statistics Report indicates the percentage of Blacks and Hispanics receiving 6 prenatal care in the first trimester lags behind that for Whites and Asians: 7 8
Percentage of Mothers Receiving 9 Prenatal Care in the First Trimester 10
11 White 89% 12 Asian 85% 13 Native American 76% 14 Black 71% 15 Hispanic 65% 16
17 What is particularly alarming about the low percentages of mothers receiving prenatal 18 care among Blacks and Hispanics is that the Black infant mortality rate is over three 19 times the rate for Nevada as a whole and the Hispanic population has the highest birth 20 rate of any group in the state. Hispanics also tend to have children at a younger age than 21 the state as a whole. 22 23 As indicated above, lack of information about the need for prenatal care and where that 24 care can be accessed are significant factors in pregnant women failing to obtain proper 25 prenatal care. The Maternal and Child Bureau currently operates an information and 26 referral line called the ‘Maternal and Child HealthLine’ and also conducts a $100,000 27 media campaign to encourage mothers to access prenatal care. 28 29 The Nevada Maternal Child Health Advisory Board (MCHAB) has as its top priority 30 improving access to comprehensive preconceptual, prenatal and postpartum services for 31 all Nevada women of childbearing age. The MCHAB is also seeking ways to expand 32 prenatal services. 33 34 Strategies to improve the early entry and continued use of prenatal care in Nevada that 35 Summit participants may want to consider include: 36 37
Expanding the media campaign to inform women about the necessity of 38 prenatal care and to direct them to providers 39
40 Launch an expanded outreach campaign focused on the Hispanic and African 41
American populations 42 43 Cost Estimate 44 45 A “placeholder estimate” of $400,000 per year is proposed for this initiative. 46

Burns & Associates, Inc. May 5, 2006 VII-7
3. Expand the Oral Health Care Program 1 2 During his term as U.S. Surgeon General, Dr. C. Everett Koop noted, “You are not 3 healthy without good oral health.” In 2000, a Surgeon General report noted that research 4 had pointed to associations between oral infections – primarily gum infections – and 5 diabetes, heart disease, stroke, and preterm low-weight births. The report also noted that 6 for children, tooth decay is the most common chronic childhood disease. 7 8 Oral health is a real concern for the children in Nevada. According to the report The 9 Burden of Oral Disease in Nevada 2005 over 60 percent of five-year olds in Nevada’s 10 Head Start program have already developed one or more cavities. The report further 11 indicated that tooth decay was experienced in 47% of the children by age 3, 52% by age 12 4, and by the third grade, fully 67% of the children had experienced tooth decay. The 13 Burden report also indicated that 37% of third graders had not received treatment for the 14 decay. 15 16 Nevada established an Oral Health Initiative in 1999 with funding from the Maternal and 17 Child Health (MCH) Block Grant. The State has developed an Oral Health Plan, 18 implemented a broad-based Oral Health Program, and invested in the infrastructure 19 required to address the needs of its citizens statewide. The program is supported through 20 federal dollars, volunteer services, and donations from the private sector. 21 22 With these resources Nevada has developed the following state-wide activities: 23 24
Oral health surveillance – Information is collected and evaluated through 25 telephone surveys, oral health screenings, Medicaid data, and data collected 26 from safety-net providers throughout the state. An annual report of the 27 findings are published. 28
29 Dental Sealants (Nevada Seal) - Volunteer hygienists apply dental sealants to 30
2nd graders in schools where 50% of the students are enrolled in the free or 31 reduced lunch programs and in rural schools where access to dental care is 32 limited. 33
34 Healthy Smile Happy Child – An awareness and prevention effort targeted to 35
parents to reduce incidence of ‘baby bottle’ tooth decay. 36 37
Oral health education – A consumer awareness program of the importance of 38 oral health that utilizes radio and television advertising, brochures, and direct 39 consumer education in community-based settings such as Family Resource 40 Centers. 41
42 These programs are supplemented by community based initiatives that utilize donations 43 and safety net providers to operate the following services: 44
45 Miles for Smiles – a program operated by Nevada Health Centers, Inc. 46

Burns & Associates, Inc. May 5, 2006 VII-8
consisting of three mobile dental clinics. Two units, sponsored in part by 1 Anthem Blue Cross/Blue Shield Foundation, are open to all persons and 2 operate in Las Vegas. The third unit was donated by the Ronald McDonald 3 Charities and provides services to children under age 18 in and around Elko. 4 The program also received a $50,000 grant from the Fund for a Healthy 5 Nevada (FFHN). 6
7 Each Miles for Smiles van is staffed with a dentist, dental assistants and office 8 assistants. Eligibility workers are also available to assist with enrollment in 9 Nevada Check-Up or Medicaid. A sliding fee program is available for low-10 income, uninsured patients. From July 1, 2002 through March 26, 2003, 11 Miles for Smiles performed 3,824 procedures and provided $208,652 worth of 12 services. 13
14 Health Access Washoe County (HAWC) Dental Clinic – HAWC’s two dental 15
clinics have 4 full-time dentists, 8 full-time dental assistants, 2 full-time 16 hygienists and a full-time project coordinator. In 2003, the clinics had over 17 15,944 visits. The activities of the clinic were partially funded by a $69,500 18 grant from FFHN to purchase dental equipment to provide direct services to 19 children. 20
21 At least two other mobile dental programs are underway in the state. The Care-A-Van 22 operated by Saint Mary’s Medical Center is funded through donations and a grant from 23 the FFHN. The unit visits schools and applies sealants to second graders. Uninsured 24 patients, as well as Medicaid and Nevada Check Up clients, are seen based on a sliding 25 fee scale. 26 27 The other program focuses on reducing the incidence of oral cancer. The ‘Crackdown on 28 Cancer’ program, operated by the UNLV Dental School, travels to public high schools 29 throughout Nevada via a mobile RV health clinic to screen students for oral health 30 problems resulting from tobacco use. Once identified, students are provided treatment, 31 preventive education, and counseling. 32 33 As previously mentioned, the State provides no general fund support for the Oral Health 34 Program. In fact, the State has not had a state Dental Officer for over 12 years. 35
The state can supplement the community-based dental efforts through increased support 36 for safety net providers (see Policy Brief on Small Employer Health Insurance and the 37 Safety Net) as well as providing for a State Dental Officer and adding additional mobile 38 dental units. 39 40 Cost Estimate 41 42 The “place holder estimates” for these strategies are a one-time cost for two mobile 43 dental units of approximately $1.2 million and an annual appropriation of $150,000 to 44 support a State Dental Officer. 45 46

Burns & Associates, Inc. May 5, 2006 VII-9
4. Reduce Exposure to Secondhand Smoke 1 2 Nevada has the highest rate of women smokers in the country and second highest rate of 3 adults who smoke. 4 5 The potential risks associated with long-term smoking are well-documented and current 6 research on the effects of exposure to secondhand smoke finds that non-smokers are also 7 at increased risk for lung cancer and heart disease. 8 9 A 1992 EPA risk assessment found the link between secondary exposure to tobacco 10 smoke for infants and children was increased respiratory tract infections and middle ear 11 infections. 12 13 Public health officials have indicated that tobacco use and exposure to secondhand smoke 14 as having the single most significant impact on the overall health of Nevadans. These 15 officials report that reducing the exposure to secondhand smoke and requiring smoke-free 16 workplaces will have significant positive long-term health effects. 17 18 Restrictions on where smoking is allowed are also associated with decreased cigarette 19 consumption and increased cessation rates among workers and the general public. In 20 2000, the American Journal of Public Health reported that “laws with comprehensive 21 restrictions led to more worksites with smoking policies and increased the likelihood that 22 workers would quit smoking”. At the present time, twelve states have enacted 100% 23 smoke-free workplaces; they are Colorado, Delaware, Florida, Massachusetts, Montana, 24 New Jersey, New York, North Dakota, Rhode Island, South Dakota, Utah, and 25 Washington. 26 27 Recent surveys have noted a reduction in heart attacks in cities with newly-enacted no 28 smoking ordinances. In Pueblo, Colorado, health officials found that heart attack rates 29 dropped 27 percent in the 18 months after a smoking ban went into effect. Similarly, 30 Helena, Montana’s heart attack-related hospital admissions dropped by half six months 31 after its ordinance became effective. 32 33 Acknowledging the adverse impact on the public’s health, the Nevada Comprehensive 34 Tobacco Control Five-Year Strategic Goals and Objectives 2005-2010 has as its second 35 objective eliminating non-smoker’s exposure to secondhand smoke1. A similar objective 36 is reiterated in the Nevada Cancer Plan. Currently, Nevada allows smoking in designated 37 areas and in some state governmental buildings. It does not require the buildings to be 38 completely smoke-free. 39 40 A potential strategy for consideration by Summit participants is to require all 41 governmental buildings to be 100% smoke-free by 2008. Additionally, the Summit may 42 consider a recommendation that Nevada ban smoking in public places where children are 43 allowed (such as restaurants, grocery and convenience stores, licensed day care facilities, 44 schools, shopping malls and movie theaters) by 2009. 45 1 The first goal is to prevent initiation of tobacco use among young people.

Burns & Associates, Inc. May 5, 2006 VII-10
Cost Estimate 1 2 Legislation to require smoke-free workplaces in Nevada was introduced in the last 3 legislative session. The Legislative Counsel Bureau did not provide a fiscal note on the 4 measure, but it is anticipated that any one-time cost for this initiative would be nominal. 5 6 7 5. Invest in Wellness Programs to Prevent Chronic Disease 8 9 According to the U.S. National Center for Health Statistics, a chronic disease is a disease 10 lasting three months or longer. The disease generally cannot be prevented by vaccines or 11 cured by medications. Examples of chronic disease include arthritis, asthma, diabetes, 12 and obesity. 13 14 According to the CDC, chronic diseases are among the most preventable health problems 15 since many share the same known risk factors such as physical inactivity, poor nutrition, 16 and tobacco use or exposure to tobacco. 17 18 Based on current population statistics, almost half of all Nevadans will develop at least 19 one chronic disease, and one in five will have two or more. Investing in prevention 20 programs, or those aimed at delaying the onset of chronic disease, would have a 21 significant impact on the both the overall long-term health of Nevadans, and on health 22 care expenditures. 23 24 The financial burden of chronic disease is significant. According to an article in Obesity 25 Research, Nevada’s annual medical expenses attributable to obesity were estimated at 26 $337 million (2003), of which $56 million was paid for by Medicaid. Estimated costs to 27 the Nevada Medicaid program for smoking was $90 million in 1998. The Nevada Cancer 28 Plan notes that the direct impact for cancer on Nevada was $1.1 billion, or $585 per 29 person, in 2002. 30 31 Prevention and education are among the best strategies for reducing the costs associated 32 with chronic disease, and partnering with communities to support and develop prevention 33 and wellness programs have proven to be an effective tactic in this regard. 34 35 Earlier this year, the National Governor’s Association (NGA) embarked on a campaign to 36 create healthier states. Understanding that the cost to states for treating chronic diseases 37 is substantial, the NGA urged state leaders to initiate and support prevention and wellness 38 programs, to partner with local communities and the private sector, and to improve the 39 health status of their citizens. The foundation of the program is that wellness must be 40 promoted where we work, learn, and live. NGA recommended that states partner with 41 employers, local communities and the schools. 42 43 Schools in particular are an excellent place to initiate such wellness programs. In the past 44 thirty years, childhood obesity rates have doubled for children ages 2-5, and more than 45 tripled for those aged 6-11. Approximately 15% of school-age children are overweight or 46

Burns & Associates, Inc. May 5, 2006 VII-11
obese. Over 9 million children, or one in seven, are at increased risk of weight-related 1 chronic disease. These statistics led to the U.S. Surgeon General’s declaration, in 2004, 2 that obesity among American children had reached an epidemic level. 3 4 Preventing childhood obesity, or other chronic diseases, begins with education. Schools 5 are a natural setting to educate children about healthy diets, the importance of active play, 6 and healthy behaviors. It is also a setting where children can see such concepts 7 reinforced. 8 9 In this vein, the federal government has recently required all schools participating in the 10 National School Lunch Program to have local wellness policies in place by July 2006. 11 Though not dictating what those policies should be, the federal requirements specify that 12 at a minimum the programs should include goals for: 13 14
Nutrition education 15 Physical activity 16 A plan for measuring implementation of the local wellness policy 17 Involve parents, students, representatives of the school food authority, and the 18
public in the policy development. 19 20 While schools are required to develop these programs, no new federal or state dollars are 21 provided for implementation. A partnership between the state, county health district 22 officials and the schools should be considered for the development of school-based and 23 other wellness programs. 24 25 State support for public health programs at the local level has ranged from sporadic to 26 non-existent. It has been reported that in the 1990’s, the State supported public health by 27 providing a per capita amount of funding to support general public health activities. At 28 that time, the funding amount was $1.00 per capita. During a time of fiscal stress for the 29 State, it is understood that the funding was dropped to $.50 per capita, and then further 30 reduced to a total funding level of $1.00 (a technical move that was made to keep the 31 budget line open). 32 33 The Summit participants may want to consider restoring the state support for public 34 health. The funding would be used by public health authorities to engage in a variety of 35 activities including: 36 37
Providing technical assistance to community organizations, school districts, 38 coalitions, taskforces and employers 39
Assisting communities in establishing prevention programs 40 Conducting chronic disease screening and educational activities 41 Engaging in outreach at public events to promote awareness 42
43 44

Burns & Associates, Inc. May 5, 2006 VII-12
Cost Estimate 1 2 A “placeholder estimate” for reinstituting annual state support of public health initiatives 3 is $5 million using a $2.00 per capita rate. 4 5

Burns & Associates, Inc. May 5, 2006 VII-13
Resources 1 2 2006 Child Immunization Schedule, Advisory Committee on Immunization Practices 3 (ACIP). Retrieved on April 29, 2006, from http://www.cdc.gov/nip/default.htm 4 5 American Non-Smokers’ Rights Foundation (2006). States and Municipalities with 6 100% Smokefree Laws in Workplaces, Restaurants, or Bars. Retrieved on April 29, 2006 7 from http://www.no-smoke.org/pdf/100ordlist.pdf 8 9 Campaign for Tobacco-Free Kids. The Toll of Tobacco in Your State. Retrieved on 10 April 10, 2006 from 11 http://www.tobaccofreekids.org/reports/settlements/toll.php?StateID=NV 12 13 Centers for Disease Control and Prevention (February 2003). The Power of Prevention: 14 Reducing the Health and Economic Burden of Chronic Disease. Atlanta: Department of 15 Health and Human Services, Centers for Disease Control and Prevention. 16 17 Centers for Disease Control and Prevention (February 10, 2006). FY 2007 CDC/ATSDR 18 President’s Budget Request. 19 20 Centers for Disease Control and Prevention (October 17, 2005). From Data to Action 21 CDC’s Public Health Surveillance For Women, Infants, and Children. Division of Vital 22 Statistics, National Center for Health Statistics, Centers for Disease Control and 23 Prevention, Retrieved on April 28, 2006 from 24 http://www.cdc.gov/reproductivehealth/Products&Pubs/DatatoAction/pdf/rhow8.pdf 25 26 Finkelstein, Eric A., Fiebelkorn, Ian, and Wang, Guijing (January 2004). State Level 27 Estimates of Annual Medical Expenditures Attributable to Obesity. Obesity Research, 28 Vol. 12 No.1. 29 30 Institute of Medicine (IOM) report in 2002, "Calling the Shots: Immunization Finance 31 Policy and Practices.” Retrieved on April 28, 2006 from 32 http://www.iom.edu/CMS/3809/5508/4113.aspx 33 34 Moskowitz, J., et al (2000)."The Impact of Workplace Smoking Ordinances in California 35 on Smoking Cessation," American Journal of Public Health, 90(5). 36 37 Midwest Mumps Outbreak Prompts Concern (April 25, 2006). Tribune-Star, Terre 38 Haute, Indiana. Retrieved on April 26, 2006 from 39 http://www.tribstar.com/siteSearch/apstorysection/local_story_115221242.html 40 41 National Governors Association (2006). CREATING HEALTHY STATES: Actions for 42 Governors. Retrieved on April 3, 2006 from 43 http://www.nga.org/Files/pdf/0602CREATINGHEALTHYSTATESACTIONS.PDF 44 45 46

Burns & Associates, Inc. May 5, 2006 VII-14
Snider, Dixie E., Jr., M.D., M.PH.; Acting Chief of Science, Centers for Disease Control 1 and Prevention, U.S. Department of Health and Human Services, on Reducing Childhood 2 Obesity: HHS’ Public Health Response, before the Senate Committee on Health, 3 Education, Labor and Pensions, October 5, 2004. 4 5 Study: Heart Attacks Drop With Smoking Ban (November 14, 2005.) Associated Press. 6 7 U.S. Department of Health and Human Services (2000). Oral Health in America: A 8 Report of the Surgeon General—Executive Summary. U.S. Department of Health and 9 Human Services, National Institute of Dental and Craniofacial Research, National 10 Institutes of Health, 2000. 11 12 U.S. Environmental Protection Agency (1992). Respiratory Health Effects of Passive 13 Smoking (Also Known as Exposure to Secondhand Smoke or Environmental Tobacco 14 Smoke ETS). Retrieved on April 29, 2006, from 15 http://cfpub.epa.gov/ncea/cfm/recordisplay.cfm?deid=2835 16 17 Wisconsin Department of Health and Family Services (2006). Wisconsin Immunization 18 Registry website. http://www.dhfs.state.wi.us/immunization/WIR.htm 19 20 21 Nevada Specific Resources: 22 23 Board of Trustees for the Trust Fund for Public Health. Annual Report 2005. Retrieved 24 from on April 13, 2006, http://health2k.state.nv.us/administration/index.htm 25 26 Department of Health and Human Services, Health Division. Chronic Disease 27 Presentation by Dr. Bradford Lee, Nevada State Health Officer. Retrieved on April 26, 28 2006 from http://health2k.state.nv.us/pio/ChronicDisease.ppt 29 30 Department of Health and Human Services, Health Division, Oral Health Program. 31 Annual Report Program Year 2003-04, Executive Summary (August 2004). Retrieved on 32 April 24, 2006 from http://health2k.state.nv.us/oral/OraHealthProgramRpt2004.pdf 33 34 Department of Health and Human Services, Health Division, Bureau of Family Health 35 Services. Burden of Oral Disease in Nevada (December 2004). 36 37 Department of Health and Human Services, Health Division, Bureau of Family Health 38 Services. Burden of Oral Disease in Nevada (December 2005). 39 40 Department of Health and Human Services, Health Division, Bureau of Family Health 41 Services (May 2005). Nevada Five-Year Maternal and Child Health Report 2006-2010. 42 Retrieved on April 25, 2006 from 43 http://health2k.state.nv.us/BFHS/MCHneedsassessmentreport20062010.pdf 44 45

Burns & Associates, Inc. May 5, 2006 VII-15
Interviews with Judith Wright, Bureau Chief, Bureau of Family Health Services, 1 Department Health and Human Services; Dr. Donald Kwalick, Chief Medical Officer, 2 Southern Nevada Health District, Melissa Ely Moore, CDC Public Health Advisor, 3 Immunization Program, Nevada Department of Health and Human Services; Michelle 4 Kling, Washoe County Health District; Dave Anderson, St. Mary’s; Maury Astley, 5 Nevada Dental Association; Dr. Larry Sands, Southern Nevada Health District. 6 7 Nevada Cancer Plan (2006). Retrieved on April 17, 2006 from 8 http://health2k.state.nv.us/cccp/canplan.pdf 9 10 Nevada’s All Kids Count Project (February 25, 2000). Annual Progress Report, Grant 11 No. 033691, 2/01/99-1/31/00. 12 13 The Nevada Comprehensive Tobacco Control Five-Year Strategic Goals and Objectives 14 2005-2010, February 7, 2006 15 16 The Fund For A Healthy Nevada (June 2003). 2003-2008 Evaluation Plan. Retrieved on 17 April 10, 2006 from 18 http://www.healthynevada.state.nv.us/eval/pdf/Evaluation_Plan_Final.pdf 19 20 21