Embed Size (px)
Citation preview

ORIGINAL ARTICLES
New Blindness in Diabetes Reduced byMore Than One-Third in StockholmCountyL.B. Backlund*1, P.V. Algvere1, U. Rosenqvist2
1Department of Ophthalmology, Karolinska Institutet, St Erik’s EyeHospital, Stockholm, Sweden2Department of Social Medicine, University of Uppsala, Uppsala,Sweden
To monitor changes over time in the incidence of blindness among people with diabetes,referrals (mentioning diabetes) to all vision rehabilitation centres in Stockholm County(1995 population 1 725 756) during 1981–1995 were registered. A mass mailing to peoplewith diabetes in 1989 urged them to have their eyes examined. Mobile fundus photographyteams initiated early diagnosis of diabetic retinopathy in primary health care in 1990.Referrals with diabetes and blindness, defined (WHO, ICD 10) as best-corrected visualacuity (VA) of the better eye less than 3/60 (0.05), occurred for 172 persons (7.6 % ofthose referred with diabetes). During 1981–1985, 93 were referred (95 % confidenceinterval 75 to 114); 1986–1990, 51 (38 to 67); 1991–1995, 28 (19 to 41). Five-yearaverage annual incidence rate of referrals with blindness was reduced by 47 % from 1.2to 0.63 to 0.33 per 100 000 population. Mean yearly reduction during 1981–1995 was11 % (8 to 15 %), 11.5 % (8 to 15 %) if blindness was defined as in the UK (VA 3/60or less), and 7 % (4 to 9 %) for legal blindness (VA 6/60 or less); test for trend p , 0.001(Poisson regression analysis). This is the first report of reduction in a geographical regionof a proxy measure for new blindness in diabetes by one-third or more, attaining one ofthe main targets of the St Vincent Declaration. 1997 by John Wiley & Sons, Ltd.
Diabet. Med. 14: 732–740 (1997)
No of Figures: 4. No of Tables: 4. No of Refs: 33
KEY WORDS Vision, subnormal Blindness Amaurosis Visual acuity RegistriesRehabilitation centres Diabetes mellitus Sweden
Received 7 February 1997; accepted 2 May 1997
reduces the risk for blindness.9,10 For eyes with proliferat-Introductionive retinopathy with high-risk characteristics, pan-retinalphotocoagulation reduced the 5-year risk of severe lossDiabetic eye complications are regarded as a major
cause of visual loss in several industrialized regions, of vision (defined as visual acuity , 5/200) by morethan 50 %.9 In eyes with clinically significant macularparticularly in the working age population,1–3 and as the
most important preventable cause of blindness in Europe. oedema, photocoagulation of the macular area reducedby at least 50 % the cumulative risk of doubling of theDevelopments in health care over the past 20 years have
raised hopes that the incidence of diabetes-associated visual angle, e.g., going from 6/9 to 6/18 or worse.10
The long-term incidence of visual impairment inblindness could be reduced.4–10 Reductions in theincidences of diabetic complications are among the main diabetes in large, geographically defined populations is
not known. The aim of this study was to investigate the5-year targets of the St Vincent Declaration, adopted in1989; new blindness due to diabetes should be reduced incidence of blindness in such a population.by one-third or more.4
Onset and progression of diabetic retinopathy can be Subjects and Methodsdelayed if glycaemic control is good.5–8 A 10 % reductionin HbA1c (e.g. 8 vs 7.2 %) is associated with a 43 % risk The study population was Stockholm County residents
(1995 end-of-year population 1 725 726). Mid-year popu-reduction of retinopathy progression.6 Other controlledtrials have shown that timely photocoagulation therapy lation data (broken down by age group and sex) for
Stockholm County 1981–95 were obtained from theRSDB regional population database (Inregia AB,* Correspondence to: Dr Lars Backlund, Fundus Photography Unit,
Sabbatsberg Hospital, Box 6401, S-113 82 Stockholm, Sweden Stockholm). Events under study were defined as referralletters from ophthalmologists, stating diabetes and blind-
Grant no. 06615 ness, sent to vision rehabilitation centres11 in StockholmSponsors: Stockholm County Council: The Elsa and Sigurd GoljeFoundation; The Swedish Medical Research Council County. Blindness was defined according to the World
732 CCC 0742–3071/97/090732–09$17.50 1997 by John Wiley & Sons, Ltd. DIABETIC MEDICINE, 1997; 14: 732–740

ORIGINAL ARTICLESHealth Organization (WHO) as best-corrected visual reduce the time lag between referral and rehabilitation,
thus further encouraging referral.acuity of the better eye less than 3/60.12,13
Eligibility for Low Vision Rehabilitation Searching for Events
After having obtained permission under Sweden’s DataIn Sweden, people experiencing visual impairment affect-ing activities in daily life, such as difficulty in reading a Protection Act and from the Regional Ethics Committee
of the Karolinska Institute to gather ophthalmic andnewspaper, may be referred by an ophthalmologist to alow vision rehabilitation centre, where teaching is other medical information on people with diabetes, we
approached the heads of low vision rehabilitation centresfree of charge and equipment is lent (e.g., magnifierstelescopes, special lighting, closed circuit television in Stockholm County. We were allowed to go through
records mentioning diabetes (but not to collect data onsystems, tape recorders, and specially adapted computerswith associated hardware and software). Referral to vision persons without diabetes). At the inception of this study,
there were no up-to-date master lists of all records andrehabilitation is widely perceived as a right, neither asa stigma nor as charity.11 referrals; in a capture-recapture study, we could retrieve
records of 94 % of diabetes patients known (from ourThere is no predefined cut-off level of age or visualacuity that might disqualify the patient from getting help retinopathy screening register) to have been referred to
vision rehabilitation. Persistent efforts were then madeat centres in Stockholm County. The ophthalmologiststates the best-corrected visual acuity of both eyes and to ascertain the total number of records existing at
centres in 1991 and to identify referrals with diabetes.conditions or diagnoses contributing to visual impairment(but is not required to select a main cause and does not All archives (and all records of patients currently being
helped at the centres) were repeatedly searched andhave to rank any co-existing causes). Awareness amongpatients of the free teaching and aids available increased duplicated records were identified; thus, 99.3 % retrieval
(of records of referrals with diabetes) was achieved.greatly towards the end of the 1970s; the total numberof referrals reached its present level 15 years ago. Data were collected from referrals during the period
1981–95. Total numbers of referrals with diabetes,In Stockholm County, low vision rehabilitation wasinitiated at the Karolinska Hospital 30 years ago; centres expected11 to be $ 200 per year, were 2272 for the
whole period (including all levels of visual acuity fromwere established by the County Council from 1975onwards; capacity was increased from 1983 (cf. Figure 1). no perception of light to 6/12), falling from a maximum
of 212 per year in 1985 to a minimum of 135 in 1994.Annual incidence of referral for all causes increasedsteadily until 1985. Rehabilitation resources have As recently recommended,14 referrals were categorized
by age and sex.increased since then, and efforts have been made to
Figure 1. Annual incidence rate of referrals with diabetes and WHO-defined blindness (visual acuity , 3/60) by year of referral;mean yearly change during 1981–1995 was −11.3 % with 95 % confidence interval (CI) from −8.0 to −14.6 %; test for trend:p , 0.001 (Poisson regression analysis)
733NEW BLINDNESS IN DIABETES REDUCED
1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 732–740 (1997)

ORIGINAL ARTICLESSince we were not given access to visual acuity, age tions noted below. Every referral letter arriving during
1981–95 contained data on visual acuity. There wereor sex data for patients without diabetes, yearly data onthe proportion with diabetes among blind people referred incomplete or inconsistent data on visual acuity in
referral letters for 14 patients referred in 1981–85, 6in each group by year cannot be presented here.However, we were allowed to ascertain the total number during 1986–90 and 7 in 1991–95, mostly for persons
initially mistakenly referred by non-ophthalmologists (butof referrals from April 1983 to March 1991 of personsliving in the southern half (population 800 000) of later examined by ophthalmologists and/or optometrists).
All 27 have been included in the study because visualStockholm County; of their referral notes (with all visualacuity levels), 9.2 % stated a diagnosis of diabetes. acuity, measured within 1 year of referral, according to
rehabilitation centre records was , 3/60. Subjects (n = 38)whose visual acuity of the better eye was described asVisual Acuity Coding‘counting fingers’ (no distance given) were regarded asblind (13 women and 8 men referred during 1981–85,Visual acuity data were coded for the purpose of
computer-aided analysis as ISO 8596 numbers ranging 11 women and 2 men in 1986–1990, 1 woman in 1991and 3 women in 1992).from 0 (here: denoting no perception of light) to 1.0 (=
6/6) for full visual acuity (corresponding to 1 minute of For one patient referred in 1991, age and visual acuity(6/60) was known but identity unknown. Two patientsarc visual angle) and grouped according to ICD 9
category.12 Standardized (fixed-distance, adequately were excluded because their loss of light perception wasdue to bilateral optic nerve damage clearly unrelatedilluminated) visual acuity charts in use by ophthalmolo-
gists in Stockholm County during the study period to diabetes (one boy died blind after surgery forcraniopharyngeoma at the age of 3 years; methanolincluded Monoyer 0.1 or Snellen 6/60 (20/200) as the
lowest visual acuity level. poisoning was the cause of blindness for one managed 27).If the records show that patients had been uncertain
when reading a given line on the chart, or if non-standard numbers were recorded, the next worse level Ageing Population, Fewer with Amaurosisof visual acuity on the ISO scale was entered into thedatabase. According to the WHO, finger counting at 1 During the study period, population age structuremetre can be coded as 0.016 (1/60).13 Visual acuity data changed. When data from mid-1981 and mid-1995 werefrom the time of last examination at the centres were compared, the number of women aged 65–84 yearsrecorded for future publication. increased by 9 % (from 123 514 to 134 559) and of
those aged 85+ years by 83 % (from 12 386 to 22 600);Statistical Analysis the number of men aged 65–84 years increased by 17 %
(from 80 746 to 94 676) and of those aged 85+ years byConfidence intervals (CIs) for annual incidence (and 86 % (from 4084 to 7597).incidence rate) of referral and for standardized incidence The number of referrals with blindness defined asratios (SIRs) were calculated assuming a Poisson distri- WHO Category 5, i.e. no perception of light, was eightbution.15 Incidence was fitted by the model log ui = a + bi in 1981–85 and six in 1986–90; there were none inwhere ui is the incidence rate in calendar year i and a 1991–95. Light perception though with a visual acuityis an unknown constant. Trend tests were performed of the better eye of only 1/60 or less (WHO Categoryusing Poisson regression analysis and GLIM.16 The per 4) was noted for 129 subjects.cent total change in incidence rate was calculated as100 (exp ((n − 1) bi) − 1), where n is the number of years
Incidence of Blindness as Defined byduring the period.17 The Wilcoxon signed rank sum testWHO Decreased by More Than 45 %statistic was employed to obtain confidence intervals for
median ages of patients.18 Confidence intervals have95 % confidence levels. All tests are two-sided and their The number of patients referred per year with a best-
corrected visual acuity of the better eye less than 3/60results have been considered significant when p , 0.05.(WHO blindness categories 3, 4, and 5) reached amaximum of 28 in 1984, decreasing thereafter (with theResultsexception of a peak in 1990–91) to 2 in 1993 and 1994,4 in 1995 (Table 1).The number of people with diabetes referred between 1
January 1981 and 31 December 1995 with a visual The number of referrals with blindness for the period1981–85 was 93 (CI 75 to 114) and the count for 1986–acuity , 3/60 was 172 (7.6 % of all referred with diabetes
during the study period) with a CI from 147 to 200. 90 was 51 (CI 38 to 67), a 45 % reduction. The countfor 1991–95 was 28 (CI 19 to 41), still lower, a reductionOne-quarter of the 172 subjects were referred before
November 1983, half before June 1985, and three- by another 45 % (Table 2).Standardized incidence ratio (SIR, observed incidencequarters before February 1989.
Data quality was generally adequate, with the excep- in 1991–95 divided by indirectly standardized incidence
734 L.B. BACKLUND ET AL.
Diabet. Med. 14: 732–740 (1997) 1997 by John Wiley & Sons, Ltd.

ORIGINAL ARTICLESTable 1. Yearly number of events (patients referred with visual Table 2. Incidence, n (events), 95% CI, and incidence rate, R
(events per 105 same-sex population), of referrals with WHO-acuity ,3/60 and diabetes), size of the Stockholm County mid-year population, and incidence rate with 95 % confidence defined blindness (visual acuity ,3/60) and diabetes by sex
for each 5-year periodinterval (CI)
Year Population Events Incidence CI Period Women Men10−5 yr−1
n CI R n CI R1981 1 530 015 17 1.1 0.65–1.81982 1 538 142 14 0.91 0.50–1.5 1981–85 56 42.3–72.7 7 37 26.1–51 4.951983 1 547 810 19 1.2 0.74–1.9 1986–90 35 24.4–48.7 4.2 16 9.2–26 2.051984 1 556 828 28 1.8 1.20–2.6 1991–95 14 7.7–23.5 1.6 14 7.7–23.5 1.71985 1 570 395 15 0.96 0.53–1.61986 1 585 816 11 0.69 0.35–1.21987 1 599 745 13 0.81 0.43–1.41988 1 611 598 10 0.62 0.30–1.11989 1 623 335 5 0.31 0.10–0.7 pathy (PDR) fell from 39 to 15 and 13 per five-year1990 1 635 650 12 0.73 0.38–1.3
period. The frequency of referrals with non-proliferative1991 1 648 090 14 0.85 0.46–1.4diabetic retinopathy (NPDR) was reduced in recent years,1992 1 662 176 6 0.36 0.13–0.8
1993 1 678 035 2 0.12 0.01–0.4 from 27 to 24 to 10 per five-year period, respectively;1994 1 697 366 2 0.12 0.01–0.4 there were none in the past three years. Regarding1995 1 717 129 4 0.23 0.06–0.6 patients with other diagnoses (and no statement of
diabetic retinopathy in the referral forms), numbers fellfrom 18 to 7 to 5; the number with cataract among theirdiagnoses fell from 10 to 6 to 2, the number withduring 1986–90, 28/54.28) was 0.51, CI for the populationmacular degeneration among their diagnoses fell from 9value 0.34 to 0.75.to 7 to 2 per five-year period. Of four referred in 1996,Five-year average annual incidence of referrals due tonone had any retinopathy.blindness according to the WHO definition12,13 was
reduced from 1.2 (CI 0.97 to 1.5) to 0.63 (CI 0.47 to0.83) to 0.33 (CI 0.22 to 0.48) per 105 population, a Blindness Incidence Greatly Reduced forreduction by 47.3 % and 47.4 %, respectively (Figure 1). Women, Now Same as for MenAge and sex profiles changed (Figures 2–3).
Over time, the diagnostic panorama changed (Fig. 4). Counts of referred women with WHO-defined blindnessdeclined by 37.5 % and 60 %, respectively, when five-Numbers of referrals with proliferative diabetic retino-
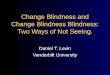
Figure 2. Scattergram showing age at referral with diabetes and blindness (visual acuity , 3/60) of 105 women (open circles) and67 men (filled circles) by date of referral; fewer persons under the age of 60 years were referred during the last 5 years
735NEW BLINDNESS IN DIABETES REDUCED
1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 732–740 (1997)

ORIGINAL ARTICLESstandardized incidence ratio (SIR) was 0.38 (CI 0.21to 0.63).
Less Blindness at All Ages
During the study period, there was a gradual shift towardshigher age at referral. The number of patients youngerthan 65 years fell. Mean age at referral (SD) for the three5-year periods was 59 (18), 64 (18), and 66 (16) years,respectively. Median age (CI) was 59 (55 to 64), 64 (59to 71) and 68 (60 to 73) years, respectively. The youngestreferred during 1981–95 was 22, the oldest 89 yearsold; for the whole period, median age was 68 years;25th and 75th centiles were 44 and 76 years of age,respectively (Figure 2).
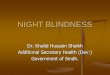
Comparing 5-year periods, numbers of those aged 65Figure 3. Men and women referred with diabetes and blindness(visual acuity , 3/60). Within-group annual incidence rate by or more years decreased from 48 to 31 to 18 (and theage group (, 65 years vs 65+ years) and 5-year period, showing corresponding proportions increased from 52 % to 60 %remarkable reduction of new blindness among the elderly to 64 %). The counts of subjects aged 45–64 years were(upper, dashed line)
reduced from 17 to 9 to 6; those subjects aged less than45 years fell from 28 to 11 to 4 (cf. Table 3).
For women, median age at referral increased from65.6 to 71.4 and 71.2 years; interquartile range (IQR)was 37, 17, and 17 years, respectively. For men, medianage at referral was 65, 47, and 70 years; IQR 37, 32,and 14 years, respectively (Figure 2). Three blind women(but no men) aged less than 25 years were referred, one(aged 22) in 1982, one (24) in 1987, and one (23) in1992. Remarkable reductions in the incidence of referralswere observed for women aged 25–44 years and forboth sexes in the 65–84 age groups (Table 3).
Among those aged 65 or more years, average annualincidence of blindness in 1991–95 was 1.4 per 105, 1.2per 105 women, and 1.8 per 105 men. On average, 1.8women and 1.8 men aged 65+ years were referred peryear. During the study period, mean mid-year populationsFigure 4. Annual incidence rate of referrals with diabetesfor this age group were 156 416 women and 101 407and WHO-defined blindness (visual acuity , 3/60) per 105
population by year of referral with proliferative diabetic men aged 65+ years, respectively (Figure 3).retinopathy (PDR) or non-proliferative diabetic retinopathy(NPDR). Other diagnoses (with no mention of retinopathy)comprised cataract and/or complications of cataract surgeryand/or age-related macular degeneration and/or glaucomasand/or retinal detachment and/or optic nerve atrophy
Table 3. Incidence, n (events), and annual incidence rate, R(events per 105 same-sex population), of referrals with WHO-defined blindness (visual acuity ,3/60) and diabetes by sex
year periods were compared. Referrals of blind men (F = female, M = male) and age group for each 5-year perioddecreased by 57 % and 13 %, respectively (Table 2).
Mean annual incidence of referral with blindness Age 1981–85 1986–90 1991–95among women was reduced from 1.4 to 0.84 to 0.32
n R n R n R n R n R n Rper 105 women, by 40 % and 62 %, respectively. Annualincidence among men fell from 0.99 to 0.41 to 0.34 per
F M F M F M105 men, by 59 % and 16 %, respectively, from a lowerinitial level to a within-group incidence similar to that
0–24 1 0.1 0 0 1 0.1 0 0 1 0.1 0 0of women (Table 2).25–44 17 1.4 10 0.8 3 0.2 7 0.5 1 0.08 2 0.2
During 1981–85, 56/93 (60 %) referred with blindness 45–64 9 1.4 8 1 5 0.6 4 0.5 3 0.3 3 0.3and diabetes were women; in 1986–90, 35/51 (69 %) 65–84 29 4.6 19 4.5 19 2.8 4 0.9 8 1.2 8 1.7
85–89 0 0 0 0 7 9 1 4 1 1 1 3and in 1991–95 14/28 (50 %). Comparing incidenceof blindness for women in 1986–90 and 1991–95,
736 L.B. BACKLUND ET AL.
Diabet. Med. 14: 732–740 (1997) 1997 by John Wiley & Sons, Ltd.

ORIGINAL ARTICLESguidelines,1 corresponding 5-year rates were reduced byIncidence of Blindness as Defined in the45 % and 49 %, respectively, with similar mean annualUK Halvedreduction (11.5 %). Legal blindness (US definition) 5-year rates were reduced by 27 % and 33 %, respectively,During the past 10 years, the 5-year number of patientsand mean annual legal blindness incidence rate by 7 %.referred with blindness defined according to UK rec-Thus, it appears that one of the St Vincent Declarationommendations1 or Italian rules,2 i.e. a best-corrected5-year main targets has been achieved for Stockholmvisual acuity for the better eye of # 3/60 (not includingCounty, that of reducing new blindness by one-thirdcases with a combination of higher visual acuity andor more.4visual field defects), decreased from 99 (CI 80 to 120)
in 1981–85 to 56 (CI 42.3 to 72.7) in 1986–90 to 30(CI 20.2 to 42.8) in 1991–95; SIR 0.50 (CI 0.34 to 0.71) Incidence of Blindness ‘Due to’ Diabetesusing data from 1986–90 and 1991–95. Five-year average Difficult to Assessannual incidence rate was reduced by 45 % from 1.28(CI 1.0 to 1.55) and then by 49 % from 0.70 (CI 0.51 Accurate whole-country data on ‘new blindness due toto 0.88) to 0.36 (CI 0.23 to 0.49) per 105 population diabetes’, as required for follow-up of the St Vincent(Table 4). Mean yearly reduction during 1981–1995 was Declaration, are not easily come by.1–4,19–23 Data11.5 % (8.3 to 14.6 %), p , 0.001. presented in this report indicate the incidence of referral
‘in’ diabetes but not necessarily ‘due to’ diabetes. Theincidence of retinal vascular occlusions, cataract, andIncidence of ‘Legal Blindness’ Reduced bysome other conditions increases with exposure to hyper-One-thirdglycaemia, contributing to the burden of blindness andvisual impairment in diabetes;8,24 therefore, it could beComparing the three 5-year periods, numbers referred
with a best-corrected visual acuity for the better eye of misleading to disregard blindness not presumed due todiabetic retinopathy. Thus, as did the Wisconsin study,246/60 (20/200) or less (termed3 ‘legal blindness’ in the
USA), not including persons with a combination of we report an estimate of new blindness in diabetes fromall causes.higher visual acuity and visual field defects, fell from
254 (CI 224 to 287) to 192 (CI 166 to 221) to 134 (CI This is, to the best of our knowledge, the first papershowing a reduction in the incidence of blindness in112 to 159), respectively. Average annual incidence
decreased from 3.3 (CI 2.9 to 3.7) to 2.4 (CI 2.1 to 2.7) diabetes, monitored over more than 10 years in ageographical region with more than one million inhabi-to 1.6 (CI 1.3 to 1.9) per 105 inhabitants per year, i.e.
a reduction by 27 % from 1981–85 to 1986–90 and a tants. Similar or higher incidences of blindness (definedas in the UK) have been reported elsewhere (Table 4).33 % reduction from 1986–90 to 1991–95. Mean yearly
change during 1981–95 was −7 % with CI from −4 to Recent papers report stable25 or even increasing2 inci-dence of blindness ‘due to’ diabetic retinopathy from−9 %. Test for trend: p , 0.001 (Poisson regression
analysis). registers of certificates from ophthalmologists collectedin Denmark25 and the province of Turin,2 respectively.Reported incidence rate of blindness ‘due to’ diabeticDiscussionretinopathy (based on BD8 forms from ophthalmologists)in England and Wales in the period from April 1990 toAnnual incidence rates of referrals to low vision rehabili-
tation centres in Stockholm County of patients with March 1991 (Table 4) was lower than reported earlier,26
but data collection methods were different prior todiabetes and WHO-defined blindness (Table 1) fell over15 years, on average by 11 % per year (Figure 1), and 1990.1,20,21
There is one landmark study of blindness ‘in’ diabetes.decreased by 47 % when consecutive five-year rateswere compared (for 1981–85, 1986–90 and 1991–95, Two eye examinations of a cohort diagnosed with
diabetes in a part of southern Wisconsin, USA withrespectively). When blindness was defined as in the UK
Table 4. Annual incidence rate of blindness (here defined as visual acuity # 3/60) with diabetic retinopathy fromregister-based studies, compared with concurrent annual incidence rate of referrals with blindness (visual acuity# 3/60) in diabetes from all causes in the present study
Site Period Source of data Incidence 10−5 yr−1 Events 10−5 yr−1, presentstudy
England and Wales1 4/90–3/91 BD8 forms 0.95 0.85N. Italy2 1982–86 Certificates 1.1 1.2N. Italy2 1987–91 Certificates 1.9 0.7Stockholm 1991–95 Referrals 0.36
Source: Evans1 Source: Porta et al2
737NEW BLINDNESS IN DIABETES REDUCED
1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 732–740 (1997)

ORIGINAL ARTICLESestimated 1983 population 851 400 were performed act extraction were substantially reduced during the
1991–95 period and increasing numbers of such pro-during 1980–82 and 1984–86, respectively. Not countingthose who had died or left the area during the intervening cedures were performed.4 years, annual incidence of legal blindness—defined asbest corrected visual acuity of the better eye 6/60 or Increasing Prevalence of Diabetesless—in diabetes (from all causes) in their study areawas estimated as 3.3 per 105 total population.24 This Geographical incidence data are influenced by variations
in levels of ascertainment, variations in diagnostic criteriaincidence rate was identical to the level found in thepresent investigation for Stockholm County during 1981– and variations in population structure.30 There are no
published data on diabetes incidence or prevalence,85, and twice the mean annual incidence (1.6 per 105
population) we found for 1991–95. diabetes care, or ophthalmic care in Stockholm Countythat could explain a decline of the number of referralswith blindness and diabetes.Changes Over Time in Health Care
Diabetes prevalence appears to be increasing31 andthe population is ageing; the numbers of persons agedIn Stockholm County, referrals of people with diabetes
increased until 1984 (Figure 1). Earlier, resources for more than 65 years (an age group with a high diabetesprevalence31 to which the majority of cases of newvision rehabilitation had not kept up with demand;
waiting lists increased and unmet needs accumulated. blindness in diabetes belongs)24,32,33 have been increasingduring the past 15 years. While it is not always knownReferrals before the age of 45, when blindness in diabetes
is mostly due to complications of insulin-dependent to patients that they have diabetes, thus not to theirophthalmologists, awareness of the diagnosis appears todiabetes mellitus (IDDM),24 are now rare, numbers falling
from 28 to 11 to 4 per 5-year period (Table 3). However, be increasing.31
visual impairment due to diabetic maculopathy amongelderly people with non-insulin-dependent diabetes Increasing Numbers of Eye Examinations(NIDDM) remains an important health problem.24–28
Since 1990 we have implemented a programme for If more people with diabetes have their eyes examined,chances for ascertainment of blindness will be improved,early diagnosis of diabetic retinopathy. Four-field 45°
Kodachrome 64 photography through tropicamide- resulting in higher recorded blindness incidence andprevalence, i.e. a form of surveillance bias.30 The annualdilated pupils has been performed28 in compliance with
the London Protocol27 by mobile fundus photography number of regularly recurring eye examinations indiabetes increased in Stockholm County during the pastteams in more than 100 primary health care centres and
five hospitals in Stockholm County, reaching more than 5 years; contributing factors could be a mailing todiabetes patients and the mobile fundus photography13 000 people with diabetes and providing visual acuity
and other follow-up data. Of persons with diabetes teams.28 The number of ophthalmologists in StockholmCounty (now 146) has increased during the study period,reached by this programme, 50 % were more than 67
years old.28 Accordingly, in 1991–95, 16 of 26 patients and access to ophthalmic care has improved. It istherefore unlikely that the tendency to refer a patient to(64 %) referred to vision rehabilitation with blindness
and diabetes were aged more than 65 years (Table 3). vision rehabilitation would be lower now than 5 or 15years ago.How was the reduction of new blindness in diabetes
achieved in Stockholm County? Certain changes in health Increased public awareness of the benefits of cataractsurgery, photocoagulation, and other ophthalmic treat-care were implemented during the past 15 years. A
diabetes control programme and training of doctors and ment modalities might increase the frequency of eyeexaminations, transiently increasing (and then possiblynurses from primary health care was started in 1980.29
During the past 15 years, diabetes education for patients decreasing) incidence of referral; that might explain theincrease in referrals up to 1984. The temporary increasehas been improved and use of self-monitoring of blood
glucose and glycated haemoglobin measurements of referrals of blind people with diabetes in 1990 and1991 (Figure 1) occurred after a direct mail campaign inincreased, allowing improvements in glycaemic control.
More NIDDM patients are taking insulin and many May 1989 to 13 400 patients (whose names were foundin the Stockholm County hospital discharge register ofIDDM patients have increased the number of daily doses.
A campaign intended to ensure regular eye examin- in-patients with diabetes among the diagnoses); thiscould be an indicator of prior under-ascertainment ofations for all persons with diabetes has been going on in
the county since 1989, including professional education visual impairment in diabetes. Conceivably, some personswith diabetes and visual impairment have not beenefforts, a direct mail campaign addressed to diabetic
patients (intended to increase their awareness and activity examined by an ophthalmologist and referred to arehabilitation centre; the magnitude of this source oflevel, urging them to have their eyes examined), and the
mobile fundus photography teams mentioned above. bias is not easy to assess. However, opticians findingvisual loss are instructed to refer the patient to an ophthal-Waiting lists for eye examinations, fluorescein angiogra-
phy, laser photocoagulation, vitreous surgery, and catar- mologist.
738 L.B. BACKLUND ET AL.
Diabet. Med. 14: 732–740 (1997) 1997 by John Wiley & Sons, Ltd.

ORIGINAL ARTICLESBlindness in Diabetes Now Less Frequent References
1. Evans JR. OPCS. Causes of Blindness and Partial Sight inThe absence of visual acuity limits allows vision rehabili-England and Wales 1990–91. London: HMSO, 1995.tation to start early, apparently increasing chances of
2. Porta M, Tomalino MG Santoro F, Ghigo LD, Cairo M,success in learning to use visual and other aids.11 AgeAimone M, et al. Diabeteic retinopathy as a cause of
at referral is now higher and visual acuity is better than blindness in the province of Turin, North-west Italy, inwas the case 15 years ago (data not shown). Apparently, 1967–1991. Diabetic Med 1995; 12: 355–361.
3. National Society to Prevent Blindness. Vision Problemspatients are now being referred earlier, before visualin the U.S. Data analysis, definitions, data sources,disability is severe; this may result in under-recording ofdetailed data tables, analyses, interpretation. New York:new blindness that occurs after referral. It is difficult toNational Society to Prevent Blindness, 1980.
assess the influence of this source of bias, particularly for 4. WHO/IDF Europe. Diabetes care and research in Europe:recent referrals. Some observations could be considered the Saint Vincent Declaration. Diabetic Med 1990; 7: 360.
5. Reichard P, Nilsson B-Y, Rosenqvist U. The effect of long-incomplete. If, for instance, more than 5 years elapsedterm intensified insulin treatment on the development offor a patient to go from a visual acuity of 20/60 to 2/60,microvascular complications of diabetes mellitus. N Englsuch events could not be identified for patients referred J Med 1993; 329: 304–309.
during the past 5 years. When available, the latest visual 6. Anonymous. The relationship of glycemic exposureacuity data recorded at vision rehabilitation centres were (HbA1c) to the risk of development and progression of
retinopathy in the Diabetes Control and Complicationscompared to visual acuity according to referral notes.Trial. Diabetes 1995; 44: 968–983.Detailed analysis of these data will be the subject of a
7. Wang PH, Lau J, Chalmers TC. Meta-analysis of effectsfuture paper, but it can be stated here that for manyof intensive blood glucose control on late complications
patients visual acuity improved after referral to vision of type I diabetes. Lancet 1993; 341: 1306–1309.rehabilitation, e.g., after surgical or other procedures, and 8. Klein R, Klein BEK, Moss SE, Cruickshanks KJ. The
relationship of hyperglycemia to the long-term incidencein a preliminary analysis such improvements appeared toand progression of diabetic retinopathy. Arch Int Medequal or exceed the 5-year incidence of visual loss after1994; 154: 2169–2178.referral 1981–90. The long-term vision prognosis for
9. Diabetic Retinopathy Study Group. Photocoagulationmore recent referrals merits investigation. treatment of proliferative diabetic retinopathy: Clinical
Are the visual acuity data reliable? Since low visual application of Diabetic Retinopathy Study (DRS) findings.DRS Report No. 8. Ophthalmology 1981; 88: 583–600.acuity is not a prerequisite for vision rehabilitation or
10. ETDRS Research Group. Photocoagulation for diabeticother benefits in Stockholm County, one possible sourcemacular edema. Arch Ophthalmol 1985; 193: 1796–1806.of misclassification bias20,21 is reduced; during the past
11. Guidelines for Rehabilitation of Visually Disabled. [In15 years, there has been no reason for ophthalmologists Swedish]. Stockholm: Socialstyrelsen (National Board ofto over- or under-record any level of visual acuity when Health and Welfare), 1990.
12. World Health Organization. International Classificationreferring patients to low vision centres in Stockholm Coun-of Diseases, Ninth Revision. Geneva: WHO, 1977.ty.
13. World Health Organization. The Prevention of Blindness.In conclusion, a proxy measure for blindness incidenceTechnical Report Series No 518. Geneva: WHO, 1973.
rate in diabetes was reduced by 11 % per year (confidence 14. Tooke J, Baker R, Burden M, Clark A, Dornan T, Gowerinterval from 8 to 15 %). Thus, one of the main targets J et al. Report of the research and development group.
Diabetic Med 1996; 13: S77–S89.of the St Vincent Declaration for diabetes care4 appears15. Liddell FDK. Simple exact analysis of the standardisedto have been achieved.
mortality ratio. J Epidemiol Commun Health 1984; 38:85–88.
16. Numerical Algorithms Group Ltd. The Generalised LinearInteractive Modelling System GLIM 3.77. Oxford, 1987.
17. Breslow NE, Day NE. Statistical Methods in CancerAcknowledgements Research, Vol II: The Design and Analysis of Cohort
Studies. Oxford: Oxford University Press/IARC, 198718. Gardner MJ, Altman D. Statistics with Confidence. London:
This study was supported by Stockholm County Council, BMJ, 1989.19. Cullinan TR. The Epidemiology of Visual Disability.The Elsa and Sigurd Golje Foundation, and the Swedish
Health Services Research Unit Report No. 28. London:Medical Research Council (grant no. 06615). A. Taube,HMSO, 1977.University of Uppsala, gave advice on study design. J. 20. Evans JR, Wormald RPL. Epidemiological function of BD8
Ranstam performed Poisson regression. U.-G. Neglen certification. Eye 1993; 7: 172–179.and H. Ericsson helped with database programming. 21. Wormald RPL, Evans JR. Registration of blind and partially
sighted people. Br J Ophthalmol 1994; 78: 733–734.Records were repeatedly searched and data collected by22. Martin J, Meltzer H, Elliot D. The Prevalence of DisabilityE. Bergavik Stromberg, Å. Fogelberg, L. Insulander, M.
Among Adults. OPCS Surveys of Disability in GreatSkoglund and, in particular, K. Jagsander. The manuscriptBritain, Report 1. London: HMSO 1988.
was read and commented on by G. Hoddle and J. 23. Cullinan TR, Gould ES, Silver JH, Irvine D. Visual disabilityRanstam. The authors are also grateful for friendly and home lighting. Lancet 1979; i: 642–644.
24. Moss SE, Klein R, Klein BEK. The incidence of vision losscooperation with staff at vision rehabilitation centres.
739NEW BLINDNESS IN DIABETES REDUCED
1997 by John Wiley & Sons, Ltd. Diabet. Med. 14: 732–740 (1997)

ORIGINAL ARTICLESin a diabetic population. Ophthalmology 1988; 95: 29. Rosenqvist U. Diabetes care management training and1340–1348. the need for a patient perspective: a 10-year evolution
25. Rosenberg T, Klie F. Current trends in newly registered of training strategies and goals. Patient Education andblindness in Denmark. Acta Ophthalmol Scand 1996; 74: Counseling 1995; 26: 209–213.395–398. 30. Barker DJP, Rose G. Epidemiology in Medical Practice,
26. Government Statistical Service. Causes of Blindness and 4th edn. Edinburgh: Churchill Livingstone, 1990: 53.Partial Sight among Adults in 1976/77 and 1980/81. 31. Andersson DK, Svardsudd K, Tibblin G. Prevalence andLondon: HMSO, 1988. incidence of diabetes in a Swedish county 1972–1987.
27. Retinopathy Working Party. A protocol for screening for Diabetic Med 1991; 8: 428–434.diabetic retinopathy in Europe. Diabetic Med 1991; 8: 32. Aclimandos WA, Galloway NR. Blindness in the City of263–267. Nottingham (1980–85). Eye 1988; 2: 431.
28. Backlund LB, Algvere PV, Rosenqvist U. Performing 33. Kohner E, Allwinkle J, Andrews J, Baker R, Brown F,diabetic retinopathy screening and measuring the inci- Cheng H, et al. Report of the visual handicap group.dence of blindness in an urban region. G Ital Diabetol Diabetic Med 1996; 13: S13–S26.1995; 15 (suppl): 44–46.
740 L.B. BACKLUND ET AL.
Diabet. Med. 14: 732–740 (1997) 1997 by John Wiley & Sons, Ltd.