Embed Size (px)
Citation preview

New CETP inhibitors and modulators
Jean-Claude Tardif MD, FRCPC, FACC, FCAHS Director, MHI Research Center
Professor of Medicine UdeM Endowed Research Chair in Atherosclerosis
Montreal Heart Institute Université de Montréal

Biological plausibility for benefit of raising HDL-C in CAD patients
♦ Cholesterol efflux, reverse cholesterol transport
♦ “Pleiotropic” effects of HDL
♦ Improves endothelial function and repair
♦ Anti-oxidant properties
♦ Anti-inflammatory properties
♦ Anti-thrombotic properties

Comparison of CETP inhibitors
Dalcetrapib Torcetrapib Anacetrapib
CETP binding site Cys 13 residue1 Helices at the end
ofthe C and N
barrels2
? (Similar to torcetrapib)3
IC50 9 µM1 0.05 µM2 0.057 µM3
CETP inhibition 37.2%4 ≥80%5 90%3
HDL-C increase 33.9%4 91%5 129%6
Blood pressure increase No7 Yes8 No3
Increases aldosteroneproduction (in vitro)
No7 Yes7 No9
1Okamoto et al. Nature 2000;406:203–7; 2Clark et al. J Lipid Res 2006;47:537–52; 3Masson D. Curr Opin Invest Drugs 2009;10:980-7; 4de Grooth et al. Circulation 2002;105:2159–65; 5Clark et al. Arterioscler Thromb Vasc Biol 2004;24:490–7; 6Krishna et al. Lancet 2007;370: 1907–14; 7Stein et al. Am J Cardiol 2009;104:82–91; 8Barter et al. N Engl J Med 2007;357:2109–22; 9Forrest et al. Br J Pharmacol 2008; 154:1465–73
NOTE: The clinical relevance of these differences is not known; these compounds have not been studied in head to head clinical trials, therefore no conclusion should be drawn based on these comparisons. Clinical development of torcetrapib was halted due to off-target adverse effects

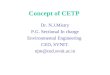
Dalcetrapib and torcetrapib differ in mechanism by which they decrease CETP
activity
dalcetrapib
HDL
CETP
HDL
● Dalcetrapib binds to CETP, inducing a conformational change to CETP that inhibitslipid transfer from HDL to LDL and VLDL1
● Dalcetrapib does not inhibit lipid transfer between HDL sub-particles in vitro2
● Torcetrapib binding to CETP results in a highaffinity complex of torcetrapib, HDL, and CETP that blocks lipid transfer3,4
1Okamoto et al. Nature. 2000;406:203-207; 2Dernick et al. Poster presented at 6th IAS-Sponsored Workshop on HDL. May 17-20, 2010; Whistler, BC, Canada; 3Niesor et al. Atheroslerosis. 2008;199:231; 4Clark et al. J. Lipid Res. 2006;47:537–552
torcetrapib

The dal-HEART Program tests a novel hypothesis: enhancing HDL efficacy through CETP modulation treats the underlying disease of atherosclerosis and will attenuate CV risk
dal-OUTCOMES1
15,600 patients recently hospitalized for ACS To evaluate the effect of dalcetrapib on CVoutcomes RECRUITMENT COMPLETE
dal-VESSEL2
450 patients withCHD or CHD risk equivalent To evaluate the effect of dalcetrapib onendothelial function and blood pressure, measured by FMD and ABPM RECRUITMENT COMPLETE
dal-PLAQUE3
130 patients withCHD To evaluate the effect of dalcetrapib oninflammation, plaque size and burden, measured by PET/CT and MRI RECRUITMENT COMPLETE
The dal-HEART Programdalcetrapib HDL Evaluation, Atherosclerosis & Reverse cholesterol Transport
1Schwartz et al. Am Heart J 2009;158:896-901; 2http://clinicaltrials.gov/ct2/show/NCT00655538 Accessed April 1st 2010; 3http://clinicaltrials.gov/ct2/show/NCT00655473 Accessed April 1st 2010; 4http://clinicaltrials.gov/ct2/show/NCT01059682 Accessed April 1st 2010 .
dal-PLAQUE-24
900 patients withCAD To evaluate the effect of dalcetrapib onatherosclerotic disease progression, assessed by IVUS and carotid B-mode ultrasound RECRUITING

DAL-OUTCOMES Study DesignA double-blind, randomized, placebo-controlled, parallel group, multi-centre study in 15,600 patients recently hospitalized for ACS
Visit 1 Visit 2
Visit 3 randomizatio
n1 : 1
Double-blind
Single-blind Placebo Run-in
4-12 Weeks
Until 1600 events
occur but at least a minimum
of2 years
Follow up 1st year: every 3 months
Following years: every 4 months
Dalcetrapib 600 mg
Placebo

dal-PLAQUE-2: Study Design • Objective: to assess the effect of dalcetrapib versus placebo
on atherosclerotic disease progression in patients with CAD
• A double-blind, randomized, placebo-controlled, parallel-group multicenter study in 900 patients with CAD
dalcetrapib 600 mg
placebo
Randomization 24 months
Primary endpoints: IVUS and CIMT at 24 months Other assessments: CIMT at 6+12 months; QCA at 24 months
Pre-rando phase Screening phase up to 8 weeksBaseline IVUS, QCA and CIMT
Double-blind
Background of contemporary evidence-basedtherapy for CAD and CV risk factors

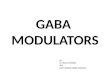
Effects on LDL-C and HDL-C
HDL-C
Study Week
Baseline Wk 6 Wk 12 Wk 18 Wk 24 Wk 30 Wk 46 Wk 62 Wk 76
HD
L-C
(mg/
dL) (
SE)
0
20
40
60
80
100
120
Anacetrapib Placebo
Anacetrapib n = 776 757 718 687 647 607 572 543 Placebo n = 766 761 741 744 736 711 691 666
LDL-C
Study Week
Baseline Wk 6 Wk 12 Wk 18 Wk 24 Wk 30 Wk 46 Wk 62 Wk 76
LDL-
C (m
g/dL
) (SE
)
0
20
40
60
80
100
Anacetrapib Placebo
Anacetrapib n = 804 771 716 687 646 604 568 540 Placebo n = 803 759 741 743 735 711 691 666
-39.8% (p<0.001) +138.1% (p<0.001)

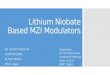
Anacetrapib had no effect on BP
SBP
DBP
Syst
olic
blo
od p
ress
ure
(mm
Hg)
Dia
stol
ic b
lood
pre
ssur
e (m
mH
g) Baseline 6 1 2 1 8 2 4 3 0 3 8 4 6 5 4 6 2 7 0 7 6 0 2 0 4 0 6 0 8 0 1 0 0 1 2 0 1 4 0 1 6 0 1 8 0 2 0 0 2 2 0
A = A n a c e t r a p i b B = P l a c e b o
0 2 0 4 0 6 0 8 0
1 0 0 1 2 0 1 4 0
A = A n a c e t r a p i b B = P l a c e b o
Week
Baseline 6 1 2 1 8 2 4 3 0 3 8 4 6 5 4 6 2 7 0 7 6 Week
L
L

10
Conclusions • Despite current optimal care, substantial residual CV risk remains • HDL-C is a promising target to reduce the burden of CV diseases
– Studies using coronary IVUS suggest that raising HDL-C can slow progression of atherosclerosis
• Clinical trials with dalcetrapib and anacetrapib have demonstrated
– Effective raising of HDL-C (> 30% after 12 weeks) – Excellent tolerability profile
• The dal-HEART program (dalcetrapib) and REVEAL trial (anacetrapib) will: – Evaluate the effects of the CETP modulator dalcetrapib on
atherosclerosis progression and clinical outcomes – Evaluate the effects of the CETPi anacetrapib on clinical
outcomes