Embed Size (px)
Citation preview

New Developments in OsteoporosisNew Developments in Osteoporosis
Douglas C. Bauer, MDDouglas C. Bauer, MD
University of California, San FranciscoUniversity of California, San Francisco
Research funding from NIH, Amgen, SKB, P and G, and MerckResearch funding from NIH, Amgen, SKB, P and G, and Merck

What’s New in OsteoporosisWhat’s New in Osteoporosis
• Absolute riskAbsolute risk
• Under recognition Under recognition
• Poor compliancePoor compliance
• When to stop bisphosphonatesWhen to stop bisphosphonates
• New treatmentsNew treatments

What Would You Do? Mrs. P…What Would You Do? Mrs. P…
• 66 grandmother and prominent politician 66 grandmother and prominent politician without previous fracture or other risk without previous fracture or other risk factors. Sister with breast cancer, factors. Sister with breast cancer, otherwise healthy. No medsotherwise healthy. No meds
• Hip BMD T-score –2.2Hip BMD T-score –2.2
• No contraindication to treatmentNo contraindication to treatment
• Will follow your advice…Will follow your advice…

What Would You Do?What Would You Do?
1)1) Start calcium 1000 mg + vitamin D 800 iu per Start calcium 1000 mg + vitamin D 800 iu per dayday
2)2) Start alendronate 70 mg or risedronate 35 Start alendronate 70 mg or risedronate 35 mg per weekmg per week
3)3) Start raloxifene 60 mg/dStart raloxifene 60 mg/d
4)4) Both 1) and 2)Both 1) and 2)
5)5) Both 1) and 3)Both 1) and 3)

Key Risk FactorsKey Risk Factors
• In addition to age, gender and race:In addition to age, gender and race:- Previous fracture (especially spine) - Previous fracture (especially spine)
- Family history of fracture- Family history of fracture- Low body weight - Low body weight - Current cigarette smoking- Current cigarette smoking
• Independent of BMD (additive) Independent of BMD (additive)

The W.H.O. Guidelines 1994The W.H.O. Guidelines 1994The measurement defines a diseaseThe measurement defines a disease
• Densitometry became widespreadDensitometry became widespread
• How to apply the BMD numbers to the concept of How to apply the BMD numbers to the concept of “diagnosis” of osteoporosis?“diagnosis” of osteoporosis?
• T < -2.5 = “osteoporosis”T < -2.5 = “osteoporosis”
• T between -1.0 and -2.5 = “osteopenia”T between -1.0 and -2.5 = “osteopenia”

Hip BMD and Fracture Risk at Age 70Hip BMD and Fracture Risk at Age 70
Hip fracture riskHip fracture risk
T-scoreT-score 5 year5 year LifetimeLifetime
> -1> -1 1% 1% 4% 4%
-1 to -2-1 to -2 1% 1% 8% 8%
-2-2 to -3to -3 4% 4% 16% 16%
< -3< -3 9% 9% 29% 29%

0
10
20
30
40
-3 -2.5 -2 -1.5 -1 -0.5 0 0.5 1
BMD T-score
Treatment Threshold ConceptTreatment Threshold Concept
8080
AGEAGE
7070
6060
5050
10-Year Fracture Probability (%)
Current treatment threshold based on T-score
Treatment threshold concept based on WHO Absolute Fracture Risk
Adapted from JA Kanis et al, Osteoporos Int. 2001;12:989-995

http://www.shef.ac.uk/FRAX/tool.jspCalculating Absolute Fracture Risk: FRAXCalculating Absolute Fracture Risk: FRAX

Who Should Be Tested and Treated*?Who Should Be Tested and Treated*?
• Preventive measures for everyone: calcium, vitamin D, Preventive measures for everyone: calcium, vitamin D, exercise, clean livingexercise, clean living
• Hip BMD: women >65, men >70, and after fractureHip BMD: women >65, men >70, and after fracture
• Treatment thresholds:Treatment thresholds:
– Anyone with hip or spine fractureAnyone with hip or spine fracture
– T-score < -2.5T-score < -2.5
– ““Osteopenia” and 10 year hip fracture risk >3% or Osteopenia” and 10 year hip fracture risk >3% or OP-related fracture risk >20%OP-related fracture risk >20%
*Revised 2008 NOF Guidelines*Revised 2008 NOF Guidelines

Under Recognition of OsteoporosisUnder Recognition of Osteoporosis
• Among women with fracture or BMD<-Among women with fracture or BMD<-2.5 , only 20-30% are evaluated and 2.5 , only 20-30% are evaluated and treated!treated!
• Ask about fracture history, note Ask about fracture history, note vertebral fractures, use chart reminders.vertebral fractures, use chart reminders.
• Be aggressive about screening and, Be aggressive about screening and, when indicated, appropriate treatmentwhen indicated, appropriate treatment
Soloman, Mayo Clin Proc, 2005

Medical Work-upMedical Work-up
• Very little data, lots of opinionsVery little data, lots of opinions
• A reasonable start:A reasonable start:
– Vitamin D (25-OH, not 1,25-OH) Vitamin D (25-OH, not 1,25-OH)
– serum calcium, Cr, TSHserum calcium, Cr, TSH
• Additional tests that may be helpful:Additional tests that may be helpful:
– Sprue serology, SPEP, UEPSprue serology, SPEP, UEP
• Unlikely to be helpful:Unlikely to be helpful:
– PTH, urine calciumPTH, urine calciumJamal et al, Osteo Inter, 2005

What Else Can Be Done To Prevent What Else Can Be Done To Prevent Osteoporosis?Osteoporosis?

Non-pharmacologic InterventionsNon-pharmacologic Interventions
• Little new data Little new data
• Smoking cessation, avoid alcohol abuseSmoking cessation, avoid alcohol abuse
• Physical activity: modest transient effect Physical activity: modest transient effect on BMD; may reduce fracture riskon BMD; may reduce fracture risk
• Conflicting data on hip protector pads Conflicting data on hip protector pads (compliance is big issue)(compliance is big issue)

Calcium and Vitamin DCalcium and Vitamin D
• Chapuy, 1992Chapuy, 1992
– Elderly women in long-Elderly women in long-term careterm care
– 30% decrease in hip 30% decrease in hip fracturefracture
181260
0
3
6
9
Placebo
Calcium + D
Months
Incidence (%)
• Porthouse, 2005: Porthouse, 2005:
– Women >70 with 1+ risk Women >70 with 1+ risk factorfactor
– No benefit on hip, nonspine No benefit on hip, nonspine (RR=1.01, CI: 0.71, 1,43)(RR=1.01, CI: 0.71, 1,43)
Chapuy, NEJM, 1992

BisphosphonatesBisphosphonates
• Four approved agents: alendronate, risedronate, Four approved agents: alendronate, risedronate, ibandronate, and zolendronic acid (recently)ibandronate, and zolendronic acid (recently)– No head-to-head fracture studiesNo head-to-head fracture studies
• What we know: fracture risk reduced 30-50% if What we know: fracture risk reduced 30-50% if – Existing vertebral fracture ORExisting vertebral fracture OR– Low BMD (T-score < -2.5)Low BMD (T-score < -2.5)
• What about those with higher BMD (“osteopenia”)? What about those with higher BMD (“osteopenia”)? Multiple risk factors?Multiple risk factors?

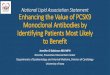
Effect of Alendronate on Non-spine Effect of Alendronate on Non-spine Fracture Depends on Baseline BMDFracture Depends on Baseline BMD
Baseline hip BMDBaseline hip BMD
OverallOverall
T < -2.5T < -2.5
T -2.0 – -2.5T -2.0 – -2.5
T -1.5 – -2.0T -1.5 – -2.0
0.10.1 11 1010Relative Hazard (± 95% CI)Relative Hazard (± 95% CI)
0.86 (0.73, 1.01)0.86 (0.73, 1.01)
0.69 (0.53, 0.88)0.69 (0.53, 0.88)
0.97 (0.72, 1.290.97 (0.72, 1.29))
1.06 (0.77, 1.46)1.06 (0.77, 1.46)
Cummings, Jama, 1998Cummings, Jama, 1998

Risedronate HIP Study: Two GroupsRisedronate HIP Study: Two Groups
Group 1Group 1
• 5445 age <80; hip BMD T-score < -3.05445 age <80; hip BMD T-score < -3.0
• 39% decreased hip fracture risk39% decreased hip fracture risk
Group 2Group 2
• 3886 age >80; risk factors for hip fx3886 age >80; risk factors for hip fx
• No significant effect on hip fracture riskNo significant effect on hip fracture risk
McClung, NEJM, 2001McClung, NEJM, 2001

Compliance with Bisphosphonates is PoorCompliance with Bisphosphonates is Poor
• Burdensome oral administration (fasting, Burdensome oral administration (fasting, remain upright for 30 minutes). Weekly dosingremain upright for 30 minutes). Weekly dosing
• 50-60% persistence after one year (ask!)50-60% persistence after one year (ask!)–Similar to other preventative txSimilar to other preventative tx–Multiple practice settingsMultiple practice settings
• Less frequent administration improves Less frequent administration improves compliance…compliance…

Zolendronate Once-a-year: Horizon Zolendronate Once-a-year: Horizon
• Extremely potent bisphosphonateExtremely potent bisphosphonate
• 3 year, multicenter controlled trial3 year, multicenter controlled trial
• 7741 women 55-89, T-score < -2.5 or < -1 7741 women 55-89, T-score < -2.5 or < -1 + vertebral fracture+ vertebral fracture
• IV zolendronate (5mg IV once/yr) vs. IV zolendronate (5mg IV once/yr) vs. placeboplacebo
• Outcome: BMD, turnover, fractureOutcome: BMD, turnover, fracture
Black et al, NEJM, 2007Black et al, NEJM, 2007

Bracketed values are least square mean difference*P < .0001
Horizon: Percentage Change in Total Hip BMDHorizon: Percentage Change in Total Hip BMD%
Ch
an
ge F
rom
Baselin
e
0 6 12 18 24 30 36
–2.0
–1.0
0.0
1.0
2.0
3.0
4.0
–3.0
5.0
Months
[2.83*]
[1.93*]
[4.70*][6.00*]
ZOL 5 mg
Placebo
35163516 35163516 32243224 23502350
35443544 35433543 32413241 24082408
ZOL n =
PBO n =
Black et al, NEJM, 2007Black et al, NEJM, 2007

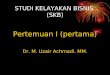
Horizon: Risk of Clinical Fractures Horizon: Risk of Clinical Fractures (Hip, Vert, Non-Vert) (Hip, Vert, Non-Vert)
RRR = relative risk reduction; 95% confidence interval
RRR 40%(CI: 15, 57)
RRR 75%(CI: 60, 85)
RRR 25%(CI: 13, 36)
Clinical Vertebral Fracture
HipFracture
Clinical Non- vertebral Fracture
1.5%0.6%
2.5% 2.6%
7.9%
10.6%
ZOL 5 mg (n = 3875) Placebo (n = 3861)
% P
ati
en
ts W
ith
New
Fra
ctu
re
0
10
5
15
Black et al, NEJM, 2007Black et al, NEJM, 2007

A New Side Effect of Potent A New Side Effect of Potent Bisphosphonates?Bisphosphonates?

Osteonecrosis of the JawOsteonecrosis of the Jaw
• Associated with potent bisphos use:Associated with potent bisphos use:
– 94% treated with IV bisphosphonates94% treated with IV bisphosphonates
– 4% of cases have OP, most have cancer4% of cases have OP, most have cancer
– 60% caused by tooth extraction60% caused by tooth extraction
• Risk factors unknown. Duration of tx? Over Risk factors unknown. Duration of tx? Over suppression of turnover?suppression of turnover?
• Key: early identification, conservative txKey: early identification, conservative tx
Woo et al; Ann Intern Med, April 2006

ONJ and OsteoporosisONJ and Osteoporosis
• How big a concern with oral treatments?How big a concern with oral treatments?– 30,000-40,000 subjects in RCTs30,000-40,000 subjects in RCTs– Duration of treatment 3-10 yearsDuration of treatment 3-10 years– No confirmed cases of ONJNo confirmed cases of ONJ
• Dental exam before initiating bisphosphonates Dental exam before initiating bisphosphonates recommended but unlikely to helprecommended but unlikely to help
• Utility of stopping bisphosphonates before Utility of stopping bisphosphonates before dental procedures unknown (not advised)dental procedures unknown (not advised)

Another Worry with Bisphosphonates?Another Worry with Bisphosphonates?

What Would You Do?What Would You Do?
• Mrs. P has now been on an oral Mrs. P has now been on an oral bisphosphonate for 5 yearsbisphosphonate for 5 years
• No new fracturesNo new fractures
• Repeat hip BMD: T-score –2.3Repeat hip BMD: T-score –2.3
• How would you advise her?How would you advise her?

What Would You Do?What Would You Do?
1)1) Assess compliance and continue Assess compliance and continue current an oral bisphosphonatecurrent an oral bisphosphonate
2)2) Switch to IV bisphosphonateSwitch to IV bisphosphonate
3)3) Switch to raloxifene 60 mg/daySwitch to raloxifene 60 mg/day
4)4) Stop bisphosphonate, continue Stop bisphosphonate, continue calcium/D, repeat BMD in 3-5 yearscalcium/D, repeat BMD in 3-5 years

How Long to Use Bisphosphonates?How Long to Use Bisphosphonates?
• Long half-life also suggests that life-Long half-life also suggests that life-long treatment may not be necessarylong treatment may not be necessary
• Concerns about excessive suppression Concerns about excessive suppression of bone resorptionof bone resorption
• FIT Long-term Extension (FLEX) studyFIT Long-term Extension (FLEX) study– 1099 ALN-treated FIT subjects1099 ALN-treated FIT subjects– Randomized to ALN or PBO for 5 yr.Randomized to ALN or PBO for 5 yr.
Black Jama, 2006

FLEX Change in Femoral Neck BMD: FLEX Change in Femoral Neck BMD: % Change from FIT Baseline% Change from FIT Baseline
= Placebo= Placebo= ALN (Pooled 5 mg and 10 mg groups)= ALN (Pooled 5 mg and 10 mg groups)
0
1
2
3
4
5
6
F 0 F 1 F 2 F 3 F 4 FL 0 FL 1 FL 2 FL 3 FL 4 FL 5
Me
an
Pe
rce
nt
Ch
an
ge
Me
an
Pe
rce
nt
Ch
an
ge
YearYear
2%
Start of FLEXStart of FLEX
PP<0.001 ALN vs PBO<0.001 ALN vs PBO
FITFIT FLEXFLEX

Cumulative Incidence of Fractures Cumulative Incidence of Fractures During FLEXDuring FLEX
ALN ALN (N = 662)(N = 662) RR (95% CI)RR (95% CI)
3%3%
19%19%
2%2%
1.1 (0.5, 2.3)1.1 (0.5, 2.3)
1.0 (0.8, 1.4)1.0 (0.8, 1.4)
0.5 (0.2, 0.8)0.5 (0.2, 0.8)
3%3%HipHip
20%20%Non-vertebralNon-vertebral
5%5%
PBO PBO (N = 437)(N = 437)
10%10% 0.9 (0.6, 1.2)0.9 (0.6, 1.2)11%11%MorphometricMorphometric
VertebralVertebral
Other fracturesOther fractures
Clinical Clinical

Implications of Bisphosphonate TrialsImplications of Bisphosphonate Trials
• Bisphosphonates reduce risk of spine, hip and non-spine Bisphosphonates reduce risk of spine, hip and non-spine fracture in women with spine fracture or low BMD (T-score < fracture in women with spine fracture or low BMD (T-score < -2.5)-2.5)
• May not reduce risk of hip or non-spine fracture in women May not reduce risk of hip or non-spine fracture in women withoutwithout osteoporosis osteoporosis
• Intermittent dosing, even yearly, effectiveIntermittent dosing, even yearly, effective
• After 5 years of treatment, some may stop. After 5 years of treatment, some may stop. – Who? For how long? How to monitor?Who? For how long? How to monitor?
• Best data of any approved treatmentBest data of any approved treatment

The NOF Guidelines Revisited in 2008: The NOF Guidelines Revisited in 2008: Who Should Be Treated?Who Should Be Treated?
• Treatment thresholds:Treatment thresholds:
–Existing hip or vertebral fracture. Existing hip or vertebral fracture. YesYes
–T-score < -2.5. T-score < -2.5. YesYes
–““Osteopenia” with risk factorsOsteopenia” with risk factors. . Probably notProbably not

Other Anti-resorptive AgentsOther Anti-resorptive Agents
• Less effective than bisphosphonatesLess effective than bisphosphonates
–Calcitonin Calcitonin
–RaloxifeneRaloxifene
• Hormone replacementHormone replacement

The Future: Anabolic AgentsThe Future: Anabolic Agents
• Most treatments for osteoporosis inhibit bone Most treatments for osteoporosis inhibit bone resorption (and formation)resorption (and formation)
• Anabolic agents stimulate formation > resorptionAnabolic agents stimulate formation > resorption
• Example: anabolic steroids, fluoride Example: anabolic steroids, fluoride
• Surprise finding: PTH is anabolic when administered Surprise finding: PTH is anabolic when administered intermittently in animals and humansintermittently in animals and humans
• RCT of PTH (20 or 40 mcg) among 1637 older women RCT of PTH (20 or 40 mcg) among 1637 older women with vertebral fracturewith vertebral fracture

Daily SQ PTH (1-34) for 18 months
• Big effects on BMDBig effects on BMD– Spine increased 9-13%Spine increased 9-13%– Hip increased 3-6%Hip increased 3-6%– Wrist Wrist decreaseddecreased 1-3% 1-3%
• Big effects on fractureBig effects on fracture– Vertebral decreased 65%Vertebral decreased 65%– Non-spine decreased 54%Non-spine decreased 54%
• Well toleratedWell tolerated
Neer, NEJM,Neer, NEJM, 20012001

• PTH and Alendronate (PaTH) StudyPTH and Alendronate (PaTH) Study
• 238 postmenopausal osteoporotic women238 postmenopausal osteoporotic women
• 11stst year randomize to: year randomize to:– PTH (1-84) alone, 100 ug/d (N=118)PTH (1-84) alone, 100 ug/d (N=118)– Alendronate alone, 10 mg/d (N=60) Alendronate alone, 10 mg/d (N=60) – PTH + Alendronate (N=59)PTH + Alendronate (N=59)
Change in spine BMD similar in all three groupsChange in spine BMD similar in all three groups
• 22ndnd year re-randomize the PTH groups to: year re-randomize the PTH groups to:– ALN (10mg/d) or PlaceboALN (10mg/d) or Placebo
Anabolic + Anti-resorptive? Anabolic + Anti-resorptive? Sequential Treatment?Sequential Treatment?
Black, NEJM 2005

Change in DXA Spine BMD Over 24 Change in DXA Spine BMD Over 24 Months of TreatmentMonths of Treatment
Me
an
ch
ang
e (%
)M
ea
n c
han
ge
(%)
00
55
1010
1515
2020
00 1212 2424MonthMonth
PLBPLB
ALNALN
PTH DiscontinuedPTH Discontinued
PTHPTH
24 month change24 month change
+12%+12%
+ 4%+ 4%
Black, NEJM, 2005

Summary: PTHSummary: PTH
• Substantial BMD increase. Reduction in spine and non-Substantial BMD increase. Reduction in spine and non-spine fractures. Hip fracture?spine fractures. Hip fracture?
• Use with antiresorptive agents? Not during, after.Use with antiresorptive agents? Not during, after.
• Lingering PTH safety issues:Lingering PTH safety issues:
– Cortical bone BMD decreases during therapy?Cortical bone BMD decreases during therapy?
– Carcinogenesis?Carcinogenesis?
• Very expensive, daily self-administered injections...Very expensive, daily self-administered injections...
– Use with severe OP, when other agents have failed? Use with severe OP, when other agents have failed?

Conclusions 1Conclusions 1
• Aggressive screening and treatment = fewer fracturesAggressive screening and treatment = fewer fractures
– Identify those who have already have the disease!Identify those who have already have the disease!
• Bisphosphonates: treatment of choiceBisphosphonates: treatment of choice
– Use for spine fracture or low BMD. Intermittent dosing.Use for spine fracture or low BMD. Intermittent dosing.
– Duration of therapy? 5 years then off?Duration of therapy? 5 years then off?
• Data for other anti-resorptive agents (SERMs, calcitonin) Data for other anti-resorptive agents (SERMs, calcitonin) less compelling less compelling

Conclusions 2Conclusions 2
• PTH: impressive effects on BMD and fracturePTH: impressive effects on BMD and fracture
– Indications not established: severe cases?Indications not established: severe cases?
– Long-term safety? Convenience?Long-term safety? Convenience?
– Sequential treatment?Sequential treatment?
• Many other potential treatments (tibolone, Many other potential treatments (tibolone, strontium, statins, RANKL AB). Stay tuned... strontium, statins, RANKL AB). Stay tuned...

Thanks For Listening. Questions Welcome!Thanks For Listening. Questions Welcome!