Embed Size (px)
DESCRIPTION
kjbjk
Citation preview

snaig
Clinical Opinion www.AJOG.org
OBSTETRICS
New directions in the diagnosis and treatmentof pulmonary embolism in pregnancy
Briony A. Cutts, B Med MD; Dhruba Dasgupta, MBBS, BSc, FRCR, MSc; Beverley J. Hunt, FRCP FRCPath, MDa
fimsrdts
tbi
ataocfl
rcmOnmlni9HdrchWtcfii
Venous thromboembolism (VTE)remains a major cause of maternal
death. Despite widespread thrombopro-phylaxis use, it was the third highestcause of direct maternal death in the re-cent UK Confidential Enquiries into Ma-ternal Deaths (17% of direct maternaldeaths).1 The diagnosis of pulmonaryembolism (PE) in pregnancy is difficult;a balance of maternal and fetal radiationexposure against potentially fatal misdi-agnosis is required.2 In pregnancy, pro-pective clinical predictive models haveot been validated, and D-dimer assaysre said not to be useful because of phys-ologically increasing levels throughoutestation with a resultant increased reli-
From the Thrombosis and Haemophilia Centre(Drs Cutts and Hunt) and the Department ofNuclear Medicine (Dr Dasgupta), Guy’s and StThomas’ Trust, London, UK.
Received January 27, 2012; revised June 11,2012; accepted June 15, 2012.
Supported in part by a Young Investigatorgrant from the Haemotology Society ofAustralia and New Zealand (B.A.C.).
The authors report no conflict of interest.
Reprints: Beverley J. Hunt, MD, Thrombosisand Haemophilia Centre, Guy’s and StThomas’ NHS Foundation Trust, WestminsterBridge Rd., London SE1 7EH, [email protected].
0002-9378/$36.00Crown Copyright © 2013 Published by Mosby, Inc. Allrights reserved.
The diagnosis and management of pulmonadiagnostic procedures and the use of anticfetus to adverse effects. This article reviewsing novel techniques for the diagnosis of puclinical prediction models, biomarkers, andment in the diagnosis and investigation of pThe usefulness of new anticoagulant agentin managing pulmonary embolism in future
Key words: pregnancy, pulmonary embolis
http://dx.doi.org/10.1016/j.ajog.2012.06.035
102 American Journal of Obstetrics & Gynecology
nce on imaging to exclude PE.3-6 Vali-dated clinical prediction models com-bined with biomarkers that are specificfor pregnancy may (1) enable risk strati-fication, (2) reduce the number of pa-tients whose condition requires imaging,and (3) reduce percentages of fetomater-nal radiation exposure.2,5,6 If risk strati-
cation is not possible, then imagingodalities with higher sensitivity and
pecificity and lower radiation risk areequired. We will discuss the use of 3-imensional nuclear medicine ventila-ion and perfusion single photon emis-ion computed tomography (V/QSPECT),
an exciting new imaging modality.7,8 Inhe past decade, new anticoagulants haveeen developed, and their potential role
n pregnancy will be explored.
New directions in diagnosisClinical prediction modelsIn the nonpregnant population, vali-dated clinical predictive models such asthe modified Well’s score stratify “likelyPE” from “unlikely PE” to exclude pa-tients from potentially harmful diagnos-tic imaging (Table 1).9,10 Combined with
negative D-dimer, the negative predic-ive value is 99.5%.11 Pregnancy confers
5-fold increased risk of VTE becausef venous stasis, a prothrombotic stateaused by increased levels of coagulationactors, reduced protein S, and fibrino-ytic activity.12 When pregnant women
mbolism in pregnancy is difficult, becauseulants potentially can expose mother and
dence for current best practice and emerg-nary embolism in pregnancy and includes
agnostic imaging that may offer improve-onary embolism in pregnancy in the future.ondaparinux, rivaroxaban, and dabigatran)gnancies is also explored.
thrombosis
have chest symptoms such as pain and
FEBRUARY 2013
shortness of breath, determination of“normal pregnant” from PE symptomsmay be difficult. The number of motherswho are imaged to exclude PE as a resultof those symptoms is high, which reflectsclinicians’ fear of fatal misdiagnosis. Thelow incidence of high-probability V/Qscans in the pregnant, compared withnonpregnant, population (�5% vs 15-20%) illustrates this.2,6,13
Rodger et al14 showed that interobservereliability was improved with the use oflinical prediction models vs clinical judg-ent alone. A retrospective assessment by’Connor et al15 that studied the useful-ess of the modified Well’s score of 125others with suspected PE who had a he-
ical computed axial tomographic pulmo-ary angiography (CTPA) found sensitiv-
ty and specificity levels of 100% and0%, respectively, using a score of �6.owever, this does not address how to
ifferentiate low- from intermediate-isk pregnant women and who can be ex-luded from diagnostic imaging, per-aps because of the criterion within theell’s score of an alternative diagnosis
hat is at least as likely as that of PE. Thisriterion contributes substantially to thenal score, is open to interpretation, and
s dependent on clinical expertise.16
There have been no prospective trialsthat have validated clinical predictionmodels to exclude PE in pregnancy.
BiomarkersD-dimers are plasma break-down prod-ucts of cross-linked fibrin and thereforeare used as markers of recent thrombusformation. Unfortunately, D-dimers arealso elevated in malignancy or acute in-flammatory states; therefore, they areused for their negative predictive value(ie, a normal value excludes VTE).17
They can be measured by a number ofmethods that enable rapid clinical turn-around. Highly sensitive D-dimer assays
ry eoagevilmodi
ulms (fpre
m,
with a cutoff value of 0.5 �g/mL will ex-

tnpsi
ifatstslsaimbpsrtnn
aVsCn
bs
www.AJOG.org Obstetrics Clinical Opinion
clude acute PE in nonpregnant patientswhen combined with “unlikely PE”stratification with the use of modifiedWell’s score criteria.9-11 In pregnancy,D-dimers rise throughout gestation,drop rapidly after delivery, and return tonormal 4-6 weeks after delivery. Thestandard cutoff value of 0.5 �g/mL forD-dimers shows their limited usefulnessin pregnancy. Kline et al18 found that,of 50 pregnant women, none had a D-dimer concentration of �0.50 �g/mL byhe third trimester. A case report of aegative D-dimer concentration in aregnant woman with PE who was sub-equently diagnosed on imaging also ex-sts.19 Chan et al20 hypothesized that
higher cut-off points for the diagnosis ofdeep venous thrombosis (DVT) maycompensate for the higher baselineD-dimer values that are seen in preg-nancy. Five D-dimer assays that diag-nose DVT in symptomatic mothers weretested and, with the use of receiver op-erating curves, showed improved spec-ificity (range, 61–79%) and a small re-duction in sensitivity in 4 of the 5assays (range, 93–100%). This ap-proach has not been assessed to ex-clude PE in pregnancy.
Brain natriuretic peptide (BNP) is anatriuretic hormone that is releasedfrom cardiac ventricles. Pro-hormonecleavage produces N-terminal pro-BNP(NT-pro-BNP). Cardiac troponin I andT are cardiac-specific proteins. All be-come elevated in cardiac damage andfailure.21,22 Recent metaanalyses showthat death in nonpregnant patients withPE is predicted by raised serum troponinand NT-pro-BNP levels; predicted deathfrom acute PE is 33% if both are ele-vated.23 BNP levels double during preg-nancy but remain stable irrespective ofgestation.24 Tanous et al25 showed thatwomen with preexisting cardiac diseasehad further elevation of BNP levels inpregnancy and that rising BNP levelspredated events or decompensation in88% of mothers. A level of �100 pg/mLhad a negative predictive value of 100%for gestational cardiac events. The use oftroponin I levels as a marker of rightheart strain in pregnancy have not beenstudied and require validation. Serum
BNP or NT-pro-BNP levels are an attrac-tive option for clinical trials of risk-stratifi-cation models for PE in pregnancy.
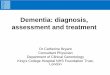
ImagingVarious diagnostic algorithms to ex-clude PE in pregnancy exist (Figure 1);however, most mothers will require ra-diologic imaging.2,6 A correct diagnosiss essential because missing a PE can beatal; a false-negative result has short-nd long-term management implica-ions for anticoagulation in current andubsequent pregnancies. The modalitieshat are used most frequently are V/Qcans and/or CTPA in conjunction withower limb compression Doppler ultra-onography. V/Q scans take planar im-ges of patient lungs after inhalation andnjection with a radioactive isotope. Pul-
onary arterial thrombus is identifiedy areas of mismatched perfusion com-ared with ventilation. Low-dose perfu-ion scans have comparable detectionates for PE in pregnancy, with no statis-ically significant difference between theumber of positive, nondiagnostic, orormal scans compared with CTPA.26,27
Unfortunately, approximately 20% ofwomen who undergo imaging withCTPA require further imaging becauseof initial nondiagnostic scans; however,most centers have 24-hour accessibility,unlike nuclear medicine imaging, whichdepends on isotope supply.26 CTPA canalso visualize emboli directly, diagnosealternative disease, and deliver a lowerdose of fetal radiation. Its main draw-backs are poor vessel opacification be-cause of physiologic higher cardiac out-puts in pregnancy and high doses ofradiation to maternal breast tissue.27
Compression Doppler ultrasonographyis a safe and accessible modality, but im-aging of pelvic DVT in pregnancy can bedifficult because the uterus obscures im-aging. If compression Doppler ultra-sonography shows a DVT, then chestsymptoms are assumed to be due to PE,and no further imaging is required.28
The fear that is associated with fetal radi-ation exposure has been over-stated.29
Low-dose radiation, defined as exposureof �50 mSv, does not increase fetal orinfant death or cause mental defects orgrowth retardation at 8-15 weeks’ gesta-
tion; however, a small increase of child-FEBRUARY 2013 Am
hood malignancy (1:5000), increasedheterochromia, and a mild preponder-ance of male sex have been seen.29 Radi-tion exposure to the fetus with both/Q scans and CTPA is 1-2 mSv. V/Q
canning has comparable exposure toTPA, although perfusion-only scan-ing decreases this further (Table 2).29
During the consent procedure in thepast, radiologists focused on fetal radia-tion exposure and neglected to informmothers of radiation exposure to mater-nal breast tissue. Perfusion-only scan-ning delivers a dose of 0.28 mSv to ma-ternal breast tissue, but CTPA gives adose 35 times higher at 10-70 mSv. In thelong-term, CTPA confers a 14% in-creased risk against the background forbreast cancer in pregnant women whoare �40 years old.30,31 This exposure can
e halved with the use of bismuthhielding.32
Disadvantages of current imaging mo-dalities means other diagnostic proce-dures such as magnetic resonance imag-ing (MRI; which is noninvasive and doesnot require radiation exposure) are ap-pealing in pregnancy.33 MRI direct
TABLE 1Well’s criteria for pretestprobability for pulmonaryembolism and diagnosticalgorithm for MWS
Criteria Score
Clinical symptoms of deepvenous thrombosis (legswelling, pain with palpation)
3
...........................................................................................................
Other diagnosis less likelythan pulmonary embolism
3
...........................................................................................................
Heart rate, �100 mm Hg 1.5...........................................................................................................
Immobilization (�3 days) orsurgery in the previous 4 days
1.5
...........................................................................................................
Previous deep venousthrombosis/pulmonaryembolism
1.5
...........................................................................................................
Haemoptysis 1...........................................................................................................
Malignancy 1...........................................................................................................
MWS �4 ¡ pulmonary embolism unlikely ¡ no di-agnostic imaging required.MWS �4 ¡ pulmonary embolism likely ¡ diagnosticimaging required.MWS, modified Wells score.
Cutts. PE in pregnancy. Am J Obstet Gynecol 2013.
thrombus imaging requires no contrast
erican Journal of Obstetrics & Gynecology 103

aetrnn
nwgddf
2V
Clinical Opinion Obstetrics www.AJOG.org
agent but depends on inherent throm-bus qualities. Red cells that are trappedin venous clot become hypoxic and pro-duce methemoglobin with resultant re-duced T1 signaling. It has shown value inthe detection of DVT but has not beenvalidated for PE and requires an experi-enced interpreter.34 Magnetic resonancengiogram detects central and segmentalmboli accurately but is less able to de-ect smaller subsegmental emboli. It alsoequires gadolinium contrast, which hasot been verified as safe in human preg-
FIGURE 1Diagnostic algorithm used for the m
Thrombo
T
Thrombosis present
Yes
Treat
Nor
PE Ex
CTPA, computed axial tomographic pulmonary angiography; CXR
Cutts. PE in pregnancy. Am J Obstet Gynecol 2013.
ancy, although it has been used to diag-
104 American Journal of Obstetrics & Gynecology
ose placenta accreta and leiomyomaith no fetal side-effects.35 High-doseadolinium produced fetal growth retar-ation in mice, but clinically relevantoses showed no fetal teratogenic ef-
ects.35 Maternofetal pharmacokineticsof high-dose gadolinium in mice foundthe maximal gadolinium fetal concen-tration at 30 minutes after injection withundetectable level within 24 hours in thefetus and within 48 hours in amnioticfluid.36 Unfortunately, such studies inhumans are unethical. Real-time MRI
nagement of possible PE in pregnanc
Symptoms of PE
CXR
Normal
N
Doppler US
s present
Normal
at
Perfusion only Scan
l Non-Diagnostic
ded
PE Exst x-ray; PE, pulmonary embolism; US, ultrasound scanning.
with fast imaging steady-state precession i
FEBRUARY 2013
reduces artifact caused by motion by de-livering rapid radiofrequency excitationpulses that minimize the usual signal de-cay time for T1 or T2 signals that causesmagnetization to obtain a steady state. Itdoes not require the use of gadolinium,and initial trials show promise but re-quire further validation.37
The European Association of NuclearMedicine recently has published data onV/QSPECT imaging. In contrast to the
-dimensional image from standard/Q scanning, multiple 3-dimensional
at our institution
Abnormal
CTPA
Yes
Treat
Thrombosis present
ded
a y
o
si
re
ma
clu
clu, che
mages are acquired because the scanner

sspwc
d4Cddm
ctsftprsVtnu
www.AJOG.org Obstetrics Clinical Opinion
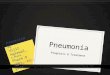
rotates around the patient. This results inbetter image quality and fewer nondiag-nostic scans and is faster than regularplanar V/Q imaging (Figure 2).7,8 Twotudies found V/QSPECT to have a higherensitivity and specificity compared withlanar V/Q: 97% and 91%, comparedith 76% and 85%, respectively.8,38 Ex-
itingly, V/QSPECT has higher rates ofsensitivity (97% vs 68-86%) and com-parative rates of specificity when com-pared with CTPA.39,40 The radiation
ose with V/QSPECT is approximately 35-0% of the dose that is required forTPA with a slightly lower radiationose to the fetus and a significantly lowerose to maternal breast tissue (approxi-ately 4% of CTPA).41 CTPA can be in-
conclusive in approximately 25% ofwomen, whereas V/QSPECT was incon-lusive in �1% of cases.27,41 Efficacy inhe determination of differential diagno-es, which include pneumonia and heartailure, was also seen. Its main disadvan-age is a limitation to the access of appro-riate radioactive isotopes. The currentecommendation by the European As-ociation of Nuclear Medicine is that/QSPECT become the gold standard for
he diagnosis of PE in all patients (preg-ant and nonpregnant) and should be
TABLE 2Maternofetal radiation exposure w
Procedure
Chest x-ray...................................................................................................................
Perfusion lung scanning 99-m Technetium mto human albumin
..........................................................................................................
Low dose: 40 MBq..........................................................................................................
High dose: 200 MBq...................................................................................................................
Ventilation 99-m Technetium aerosol...................................................................................................................
Computed tomography pulmonary angiograph...................................................................................................................
Ventilation and perfusion single photon emisstomography (V/QSPECT)...................................................................................................................
Background radiation from living 1 year in Lo...................................................................................................................
Radiation from long-haul international air fligh...................................................................................................................
N/A, not applicable.Data reproduced, with permission, from Chunilal29 and Bajc ea Fifty millisievert is equivalent to 5 rads or 50 mGy.
Cutts. PE in pregnancy. Am J Obstet Gynecol 2013.
sed in preference to CTPA.8
New directions in treatmentNew anticoagulant agentsClinical trials to establish best practicefor treatment of VTE in pregnancy arelacking; thus, treatment with current
FIGURE 2V/QSPECT for the detection of pulmon
Perfusion
Ventilation
/QSPECT thermal imaging coronal posterior sectiary-ventilatory areas of mismatch that indicate
obes of the right lung (white arrows)./QSPECT, ventilation and perfusion single photon emission comput
utts. PE in pregnancy. Am J Obstet Gynecol 2013.
different imaging modalities for pulm
Estimated fetal radiationexposure (millisievert)a
�0.01.........................................................................................................................
aggregates
.........................................................................................................................
0.11-0.20.........................................................................................................................
0.20-0.60.........................................................................................................................
0.10-0.30.........................................................................................................................
ultidetector 0.24-0.66.........................................................................................................................
computed 1.90
.........................................................................................................................
n, UK N/A.........................................................................................................................
N/A.........................................................................................................................
FEBRUARY 2013 Am
anticoagulants has been extrapolatedfrom trials in nonpregnant populations.Treating VTE with vitamin K antago-nists in pregnancy is avoided preferablybecause warfarin embryopathy causes
embolism
in a female patient show multiple large pulmo-onary emboli that involve the upper and lower
mography.
nary embolism in pregnancy
Estimated maternal radiation exposureto breast tissue (millisievert)
�1.00..................................................................................................................
..................................................................................................................
0.28-0.50..................................................................................................................
1.20..................................................................................................................
�0.01..................................................................................................................
10-70..................................................................................................................
2.50
..................................................................................................................
2.50..................................................................................................................
0.05..................................................................................................................
ary
V onsn pulmlV ed to
C
ith o
......... .........
acro
......... .........
......... .........
......... .........
......... .........
y m......... .........
ion
......... .........
ndo......... .........
t......... .........
t al.8
erican Journal of Obstetrics & Gynecology 105

ahcwptfrogVtela
ntrbaplgnadsbcai
twcr
ifntbast12
oLntfbn
p(ctiD
srwcKo
TsP8Giyd
Clinical Opinion Obstetrics www.AJOG.org
nasal hypoplasia and epiphysis stipplingduring the first trimester.42 In the secondand third trimester, there is increasedrisk of fetal intracranial hemorrhage,spontaneous abortion, stillbirth, ven-tricular septal defects, and growth retar-dation, especially with maternal warfarindoses of �5 mg.43 Warfarin’s transpla-cental passage results in a higher interna-tional normalized ratio in the fetus thanin the mother because the fetal liver failsto metabolize vitamin K and warfarin aseffectively as an adult liver.42
Low molecular weight heparins(LMWHs) are the anticoagulants of choicein pregnancy because they do not cross theplacenta.44 LMWHs act by potentiatingantithrombin 10,000-fold; their main ef-fect is through anti-Xa activity. Unlikeunfractionated heparin, they have reli-able pharmacokinetics (ie, dose has a linearrelationship anti-Xa activity).45 LMWHsre cleared renally and so, in pregnancy,ave a shorter half-life with improvedreatinine clearance.46 This combinedith the increased plasma volumes ofregnancy reduce peak drug concentra-ions and shorten the half-life.45,46 Un-ortunately, existing twice daily dosingecommendations in the Royal Collegef Obstetricians and Gynaecologistsuidelines (no. 37b) for treatment ofTE in pregnancy are extrapolated from
hromboprophylactic data only.47 Knightt al44 reviewed the UK obstetric surveil-ance data and found that a variety of once-nd twice-daily dosing regimens existed.
Because of the reliable pharmacoki-etics of LMWH in nonpregnant pa-
ients, the monitoring of anti-Xa levels iseserved for the elderly, extremes ofodyweight, and impaired renal clear-nce.47 No published data exists to sup-ort recommendations in the Royal Col-
ege of Obstetricians and Gynaecologistsuidelines to test anti-Xa levels in preg-ant women at extremes of bodyweightnd renal impairment.45 A 3-hour post-ose peak level of 0.4-1.2 unit/mL is con-idered within the “therapeutic range”y 1 expert, but this is not supported bylinical trials because few studies of dos-ge and the monitoring of anti-Xa levelsn the pregnant population exist.42
Those investigators who have studied
thromboprophylactic doses show con-106 American Journal of Obstetrics & Gynecology
flicting data about whether doses corre-late with anti-Xa levels.48,49 Moreover,the UK quality program showed enor-mous variation between hospital labora-tories when a sample spiked withLMWH was sent out for evaluation ofanti-Xa activity.50 Whether the altera-ion of doses to maintain anti-Xa levelsithin a theoretic target window impacts
linical outcomes, which include recur-ent VTE and hemorrhage, is unknown.
LMWH has a lower incidence of heparin-nduced thrombosis compared with un-ractionated heparin. Indeed in preg-ancy, no cases of heparin-induced
hrombosis because of LMWH haveeen published.46 The bleeding risk islso low; in a systematic review of 64tudies that involved 2777 pregnancies,he overall frequency of bleeding was.98% (95% confidence interval, 1.50-.57%).51 Osteoporosis is a known com-
plication of unfractionated heparin, butonly a handful of cases have been de-scribed with the use of LMWH through-out pregnancy.52 Thus, despite the lack
f clinical trials studying the efficacy ofMWH in thromboprophylaxis in preg-ancy, it is used widely and perceived as
o be safe. However, the use of LMWHor treatment of VTE in pregnancy haseen studied inadequately and shouldot be considered so benevolently.46,47
In the last 5 years, new anticoagulantshave been developed; their usefulness oftreating PE in pregnancy is discussedlater.
FondaparinuxFondaparinux is a synthesized derivativeof the natural pentasaccharide withinheparin. It shows high-affinity reversiblebinding to antithrombin that causesconformational change with enhancedfactor Xa inactivation. It has a longerhalf-life of 17 hours when comparedwith the half-life of approximately 12hours for LMWH.53 There is limited ex-
erience with its use in pregnancymainly animal studies and a few humanase reports), so it is used as an alterna-ive anticoagulant. There is a lack of clar-ty of its ability to cross the placenta.
empfle54 reported drug cord blood lev-els one-tenth of maternal levels using anti-
Xa and activated partial thromboplastinFEBRUARY 2013
time assays that indicated minor trans-placental passage of the drug. However,Knol et al55 documented no fetal hemor-rhages or anomalies in 12 pregnantwomen who received treatment doses of7.5-mg fondaparinux daily; median de-livery blood loss was 450 mL with 3 sig-nificant (�1000 mL) postpartum hem-orrhages occurring, 2 within 12 hours ofthe last injection. From limited datafondaparinux appears efficacious inpregnancy, but bleeding risk is not ab-sent, and care is required when used assecond-line therapy.
The new oral anticoagulantsThere are a number of new, exciting oralanticoagulants coming that have pre-dictable pharmacokinetics so that, un-like vitamin K antagonists, they do notrequire monitoring. At the vanguard arerivaroxaban and dabigatran followed byapixiban and endoxaban, among others.Rivaroxaban is a direct factor Xa inhibi-tor, and dabigatran is a direct thrombininhibitor. Worldwide both have been li-censed for VTE prophylaxis after hip andknee replacement and are licensed orawaiting license for stroke prevention inatrial fibrillation and for secondary VTEprevention.56-60 However, there are nodata for the use of either agent in humanpregnancy. Animal studies with bothdrugs have found teratogenic effects, re-duced fetal viability, hemorrhagic changes,and placental abnormalities. Rivaroxabanis secreted in breast milk, but no such dataexists for dabigatran.61,62 For these rea-ons, dabigatran or rivaroxaban cannot beecommended for use in pregnancy, andomen who take these drugs and wish to
onceive are advised to change to a vitaminantagonist and then LMWH, depending
n their underlying problem.
hrombolysis, graduated compressiontockings, and inferior venacaval filtersostthrombotic syndrome develops in0% of pregnant women after DVT.rade II graduated compression stock-
ngs (ankle pressure, 30-40 mm Hg) for 2ears after diagnosis reduces the inci-ence of postthrombotic syndrome.63
There is minimal experience of throm-
bolysis of PE in pregnancy. Case reports
ttrnntrtiamo
pAB22em13Dri13p33Ttwo3K
www.AJOG.org Obstetrics Clinical Opinion
show its use in women who are compro-mised hemodynamically from PE. Hem-orrhagic complication rates are similar tononpregnant patients with pregnancy-re-lated complications that include placen-tal abruption and documented pretermlabor.64
A fresh DVT (ie, after 37 weeks’ gesta-tion), especially in the pelvis or proximalveins, has a likelihood of embolizationduring labor, possibly made more so byanticoagulation withdrawal in labor.Temporary retrievable inferior venaca-val filters are used most appropriately inthis setting.2,65
Future directionsClinical trials are needed to improve themanagement of PE in pregnancy. Exist-ing clinical prediction models requireprospective validation in pregnancy.Do biomarkers such as high cutoffD-dimers and BNP in conjunction withclinical prediction models exclude low-risk women and thus reduce the risk ofmaternofetal radiation exposure? Cer-tainly V/QSPECT is a major advance, andhe latest magnetic resonance imagingechnology requires trials to investigateates of sensitivity and specificity in preg-ancy. Given the altered pharmacoki-etics of LMWH in pregnancy, future
rials that will identify optimal dosingegimens for the treatment of VTE andhe study of maternal and fetal outcomesn women are needed. Finally, new oralnticoagulant agents cannot be recom-ended for use in pregnancy; any data
btained will be based on case reports.
REFERENCES1. Confidential enquiry into maternal and childhealth: saving mothers’ lives: reviewing mater-nal deaths to make motherhood safer; 2003-2005: the seventh report of the confidential en-quiries into maternal deaths in the UnitedKingdom. London: CEMACH; 2007.2. Bourjeily G, Paidas M, Khalil H, Rosene-Mon-tella K, Rodger M. Pulmonary embolism in preg-nancy. Lancet 2010;375:500-12.3. Morse M. Establishing a normal range for D-dimer levels through pregnancy to aid in thediagnosis of pulmonary embolism and deepvein thrombosis. J Thromb Haemost 2004;2:1202-4.4. Chabloz P, Reber G, Boehlen F, Hohlfeld P,de Moerlooseo P. TAFI antigen and D-dimerlevels during normal pregnancy and at delivery.
Br J Haematol 2001;115:150-2.5. Chan WS, Ray JG, Murray S, Coady GE,Coates G, Ginsberg JS. Suspected pulmonaryembolism in pregnancy: clinical presentation,results of lung scanning, and subsequent ma-ternal and pediatric outcomes. Arch Intern Med2002;162:1170-5.6. Fatima N, uz Zaman M, Sajjad Z, Hashmi I.Pulmonary embolism in pregnancy: a diagnos-tic dilemma. Ann Nucl Med 2011;25:603-8.7. Bajc M. Value of ventilation/perfusion SPECTdetecting extensive pulmonary embolism in apatient with pneumonia. Thromb Haemost2005;93:993-4.8. Bajc M, Neilly JB, Miniati M, Schuemichen C,Meignan M, Jonson B. EANM guidelines forventilation/perfusion scintigraphy: part 1, pul-monary imaging with ventilation/perfusion sin-gle photon emission tomography. Eur J NuclMed Mol Imaging 2009;36:1356-70.9. Perrier A, Desmarais S, Miron MJ, et al. Non-invasive diagnosis of venous thromboembolismin outpatients. Lancet 1999;353:190-5.10. Wells PS, Anderson DR, Rodger MA, et al.Excluding pulmonary embolism at the bedsidewithout diagnostic imaging: management ofpatients with suspected pulmonary embolismpresenting to the emergency department by us-ing a simple clinical model and D-dimer. AnnIntern Med 2001;135:98-107.11. Wells PS, Anderson DR, Rodger M, et al.Excluding pulmonary embolism at the bedsidewithout diagnostic imaging: management ofpatients with suspected pulmonary embolismpresenting to the emergency department by us-ing a simple clinical model and D-dimer. Ann IntMed 2001;135:98-107.12. Pabinger I, Grafenhofer H. Thrombosis dur-ing pregnancy: risk factors, diagnosis and treat-ment. Pathophysiol Haemost Thromb 2002;32:322-4.13. PIOPED Investigators. Value of the ventila-tion/perfusion scan in acute pulmonary embo-lism: results of the prospective investigation ofpulmonary embolism diagnosis (PIOPED).JAMA 1990;263:2753-9.14. Rodger MA, Maser E, Stiell I, Howley HE,Wells PS. The interobserver reliability of pretestprobability assessment in patients with sus-pected pulmonary embolism. Thromb Res2005;116:101-7.15. O’Connor C, Moriarty J, Walsh J, Murray J,Coulter-Smith S, Boyd W. The application of aclinical risk stratification score may reduce unnec-essary investigations for pulmonary embolism inpregnancy. J Matern Fetal Neonatal Med2011;24:1461-4.16. Bounameaux H, Perrier A, Righini M. Diag-nosis of venous thromboembolism: an update.Vasc Med 2010;15:399-406.17. Crippa L, D’Angelo SV, Tomassini L, RizziB, D’Alessandro G, D’Angelo A. The utility andcost-effectiveness of D-dimer measurements inthe diagnosis of deep vein thrombosis. Haema-tologica 1997;82:446-51.18. Kline JA, Williams GW, Hernandez-Nino J.
D-dimer concentrations in normal pregnancy: pFEBRUARY 2013 Am
new diagnostic thresholds are needed. ClinChem 2005;51:825-9.19. To MS, Hunt BJ, Nelson-Piercy C. A nega-tive D-dimer does not exclude thromboembo-lism (VTE) in pregnancy. J Obstet Gynaecol2008;28:222-3.20. Chan WS, Lee A, Spencer FA, et al.D-dimer testing in pregnant patients: towardsdetermining the next ‘level’ in the diagnosis ofdeep vein thrombosis. J Thromb Haemost2010;8:1004-11.21. Hunt PJ, Richards AM, Nicholls MG, YandleTG, Doughty RN, Espiner EA. Immunoreactiveamino-terminal pro-brain natriuretic peptide(NT-PROBNP): a new marker of cardiac impair-ment. Clin Endocrinol 1997;47:287-96.22. Jaffe AS. The 10 commandments of tro-ponin, with special reference to high sensitivityassays. Heart 2011;97:940-6.23. Vuilleumier N, Le Gal G, Verschuren F, et al.Cardiac biomarkers for risk stratification in non-massive pulmonary embolism: a multicenterprospective study. J Thromb Haemost 2009;7:391-8.24. Hameed AB, Chan K, Ghamsary M, El-kayam U. Longitudinal changes in the B-typenatriuretic peptide levels in normal pregnancyand postpartum. Clin Cardiol 2009;32:E60.25. Tanous D, Siu SC, Mason J, et al. B-typenatriuretic peptide in pregnant women withheart disease. J Am Coll Cardiol 2010;56:1247-53.26. Revel MP, Cohen S, Sanchez O, et al. Pul-monary embolism during pregnancy: diagnosiswith lung scintigraphy or CT angiography? Ra-diology 2011;258:590-8.27. Cahill AG, Stout MJ, Macones GA, Bhalla S.Diagnosing pulmonary embolism in pregnancyusing computed-tomographic angiography orventilation-perfusion. Obstet Gynecol 2009;114:124-9.28. Bates SM, Greer IA, Pabinger I, Sofaer S,Hirsh J. Venous thromboembolism, thrombo-hilia, antithrombotic therapy, and pregnancy:merican College of Chest Physicians Evidence-ased Clinical Practice Guidelines, 8th ed. Chest008;133(suppl):844S-86S.9. Chunilal SD, Bates SM. Venous thrombo-mbolism in pregnancy: diagnosis, manage-ent and prevention. Thromb Haemost 2009;01:428-38.0. Nijkeuter M, Geleijns J, De Roos A, et al.iagnosing pulmonary embolism in pregnancy:
ationalizing fetal radiation exposure in radiolog-cal procedures. J Thromb Haemost 2004;2:857-8.1. Cook JV, Kyriou J. Radiation from CT anderfusion scanning in pregnancy. BMJ 2005;31:350.2. Hopper KD, King SH, Lobell ME, TenHaveR, Weaver JS. The breast: in-plane x-ray pro-ection during diagnostic thoracic CT-shieldingith bismuth radioprotective garments. Radiol-gy 1997;205:853-8.3. Hochhegger B, Marchiori E, Zanetti G, IrionL. MR imaging in pulmonary embolism during
regnancy. Radiology 2011;260:304-5.erican Journal of Obstetrics & Gynecology 107

53CvroM34ForP4NilpC4T4Tcw1
Clinical Opinion Obstetrics www.AJOG.org
34. Fraser DGW, Moody AR, Morgan PS, Mar-tel AL, Davidson I. Diagnosis of lower-limb deepvenous thrombosis: a prospective blindedstudy of magnetic resonance direct thrombusimaging. Ann Intern Med 2002;136:89-98.35. Katzberg RW, McGahan JP. Science topractice: will gadolinium-enhanced MR imagingbe useful in assessment of at-risk pregnancies?Radiology 2011;258:325-6.36. Mühler MR, Clément O, Salomon LJ, et al.Maternofetal pharmacokinetics of a gadoliniumchelate contrast agent in mice. Radiology2011;258:455-60.37. Kluge A, Muller C, Hansel J, Gerriets T,Bachmann G. Real-time MR with TrueFISP forthe detection of acute pulmonary embolism: ini-tial clinical experience. Eur Radiol 2004;14:709-18.38. Gutte H, Mortensen J, Jensen CV, et al.Detection of pulmonary embolism with com-bined ventilation-perfusion SPECT and low-dose CT: head-to-head comparison with multi-detector CT angiography. J Nucl Med 2009;0:1987-92.9. Bajc M, Neilly JB, Miniati M, Schuemichen, Meignan M, Jonson B. EANM guidelines forentilation/perfusion scintigraphy: part 2, algo-ithms and clinical considerations for diagnosisf pulmonary emboli with V/P(SPECT) andDCT. Eur J Nucl Med Mol Imaging 2009;6:1528-38.0. Sostman HD, Stein PD, Gottschalk A, Matta, Hull R, Goodman L. Sensitivity and specificityf perfusion scintigraphy combined with chestadiography for acute pulmonary embolism inIOPED II. J Nucl Med 2008;49:1741-8.1. Reinartz P, Wildberger JE, Schaefer W,owak B, Mahnken AH, Buell U. Tomographic
maging in the diagnosis of pulmonary embo-ism: a comparison between V/Q lung scintigra-hy in SPECT technique and multislice spiralT. J Nucl Med 2004;45:1501-8.2. Greer IA. Anticoagulants in pregnancy. Jhromb Thrombolysis 2006;21:57-65.3. Vitale N, De Feo M, De Santo LS, Pollice A,edesco N, Cotrufo M. Dose-dependent fetalomplications of warfarin in pregnant womenith mechanical heart valves. J Am Coll Cardiol
999;33:1637-41.108 American Journal of Obstetrics & Gynecology
44. Knight M; UKOSS. Antenatal pulmonaryembolism: risk factors, management and out-comes. BJOG 2008;115:453-61.45. Laurent P, Dussarat G-V, Bonal J, et al. Lowmolecular weight heparins: a guide to their op-timum use in pregnancy. Drugs 2002;62:463-77.46. Patel JP, Hunt BJ. Where do we go nowwith low molecular weight heparin use in obstet-ric care? J Thromb Haemost 2008;6:1461-7.47. Royal College of Obstetricians and Gynae-cologists: Green-top guideline no. 37b. Theacute management of thrombosis and embo-lism during pregnancy and the puerperium.2007.48. Nelson-Piercy C, Letsky EA, de Swiet M.Low molecular weight heparin for obstetricthromboprophylaxis: experience of sixty-ninepregnancies in sixty-one women at high risk.Am J Obstet Gynecol 1997;176:1062-8.49. Hunt BJ, Doughty H, Majurndar G, et al.Thromboprophylaxis with low molecular weightheparin (dalteparin) in high risk pregnancies.Thromb Haemost 1997;77:39-43.50. Kitchen S, Lampietro R, Woolley AM, Pres-ton FE. Anti-Xa monitoring during treatment ofLMWH or danaparoid: inter-assay variability.Thromb Haemost 1999;82:1289-93.51. Greer IA, Nelson Piercy C. Low molecularweight heparins for thromboprophylaxis andtreatment of venous thromboembolism in preg-nancy: a systematic review of safety and effi-cacy. Blood 2005;106:401-7.52. Lefkou E, Khamashta M, Hampson G, HuntBJ. Review: low-molecular-weight heparin-in-duced osteoporosis and osteoporotic frac-tures: a myth or an existing entity? Lupus2010;19:3-12.53. Aauer KA, Hawkins DW, Peters PC, et al.Fondaparinux, a synthetic pentasaccharide; thefirst in a new class of antithrombotic agents: theselective factor Xa inhibitors. Cardiovasc DrugRev 2002;20:37-52.54. Dempfle CE. Minor transplacental passageof fondaparinux in vivo. N Engl J Med 2004;350:1914-5.55. Knol HM, Schultinge L, Erwich JJ, Meijer K.
Fondaparinux as an alternative anticoagulantFEBRUARY 2013
therapy during pregnancy. J Thromb Haemost2010;8:1876-9.56. Eriksson BI, Borris LC, Friedman RJ, et al.Rivaroxaban versus enoxaparin for throm-boprophylaxis after hip arthroplasty. N EnglJ Med 2008;358:2765-75.57. Bauersachs R, Berkowitz SD, Brenner B, etal. Oral rivaroxaban for symptomatic venousthromboembolism. N Engl J Med 2010;363:2499-510.58. Wolowacz SE, Roskell NS, Plumb JM,Caprini JA, Eriksson BI. Efficacy and safety ofdabigatran etexilate for the prevention of ve-nous thromboembolism following total hip orknee arthroplasty: a meta-analysis. ThrombHaemost 2009;101:77-85.59. Schulman S, Kearon C, Kakkar AK, et al.Dabigatran versus warfarin in the treatment ofacute venous thromboembolism. N Engl J Med2009;361:2342-52.60. Connolly SJ, Ezekowitz MD, Yusuf S, et al.Dabigatran versus warfarin in patients with atrialfibrillation. N Engl J Med 2009;361:1139-51.61. European Medicines Agency Product In-formation Leaflet: Dabigatran 2010. Avail-able at: http://www.ema.europa.eu/ema/index.jsp?curl�pages/medicines/human/medicines/000829/human_med_000981.jsp&jsenabled�true. Accessed July 20, 2012.62. European Medicines Agency Product In-formation Leaflet: Rivaroxaban 2010. Avail-able at: http://www.ema.europa.eu/ema/index.jsp?curl�pages/medicines/pips/EMEA-000430-PIP01-08-M02/pip_000339.jsp&mid�WC0b01ac058001d129. Accessed July 20, 2012.63. Brandjes DPM, Buller HR, Heijboer H, et al.Randomised trial of effect of compression stock-ings in patients with symptomatic proximal-veinthrombosis. Lancet 1997;349:759-62.64. Trukhacheva E, Scharff M, Gardner M, Lak-kis N. Massive pulmonary embolism in preg-nancy treated with tissue plasminogen activa-tor. Obstet Gynecol 2005;106:1156-8.65. Jamjute P, Reed N, Hinwood D. Use of in-ferior vena cava filters in thromboembolic dis-ease during labor: case report with a literaturereview. J Matern Fetal Neonatal Med 2006;19:
741-4.