Embed Size (px)
Citation preview

EXPERIENCE SHARING AND
LEARNING WORKSHOP STOP DIARRHOEA INITIATIVE
May 30, 2017
India Habitat Center, New Delhi

Experience Sharing and Learning Workshop Page 2
Table of Contents
S. No. Session Topic Page
Number
1 Acronyms 3
2 Executive Summary 4-5
3 Welcome Address and Context Setting 7
4 Stop Diarrhoea Initiative - Mid Term Progress 7-8
5 National Perspective on Diarrhoea Management 9-10
6 Special Address 10
7 Closing Remarks 10-11
8 Panel Discussion - I
Low coverage to Zinc- Key challenges and possible solutions 13-16
9 Panel Discussion –II
Current challenges in achieving ODF and possible solutions 17-20
10 Taking the SDI forward and Vote of Thanks 20
11 Key Recommendations 21
12 ANNEXURE A: Mid Term Progress in Key Performance Indicators 22-23
13 ANNEXURE B: Agenda – Experience Sharing and Learning Workshop 24

Experience Sharing and Learning Workshop Page 3
Acronyms ANM Auxiliary Nurse Midwife
ASHA Accredited Social Health Activist
AWW Anganwadi Worker
BCC Behaviour Change Communication
CHAI Clinton Health Access Initiatives
CLTS Community Led Total Sanitation
CMO Chief Medical Officer
CSO Civil Society Organization
DUSIB Delhi Urban Shelter Institutional Board
FLW Field Level Worker
GoI Government of India
GP Gram Panchayat
IDCF Intensive Diarrhoea Control Fortnight
IEC Information Education Communication
IMR Infant Mortality Rate
M&E Monitoring and Evaluation
MCD Municipal Corporation of Delhi
MGNREGA Mahatma Gandhi National Rural Employment Guarantee Act
MO Medical Officer
MoHFW Ministry of Health and Family Welfare
MoWCD Ministry of Women and Child Development
NFHS National Family Health Survey
NGO Non-Government Organization
NHM National Health Mission
ODF Open Defecation Free
ORS Oral Rehydration Salt
ORT Oral Rehydration Therapy
PRI Panchayati Raj Institution
RB Reckitt Benckiser
SBA Swachh Bharat Abhiyan (Clean India Mission)
STC Save the Children
TAG Technical Advisory Group
U5 Under 5 children
UP Uttar Pradesh
VHNSC Village Health Nutrition and Sanitation Committee
VWSC Village Water and Sanitation Committee
WASH Water, Sanitation and Health

Experience Sharing and Learning Workshop Page 4
Executive Summary
Context
The experience sharing and learning workshop was organized by Save the Children with the objective to
share the mid-term progress and learning under its Stop Diarrhoea Initiative project with key
government departments, various civil society organizations, NGO partners etc.
Save the Children partnership with Reckitt and Benckiser (RB) was highlighted for a program especially
focused on Water, Sanitation and Hygiene in 2012, which further provided the genesis of Stop
Diarrhoea Initiative project in 2015, focused on WHO-UNICEF 7 Point Plan to prevent and control
diarrhoea.
A brief introduction about Stop Diarrhoea Initiative and the progress made by the programme by mid-
year of the period was shared with the participants. Various facts related to childhood mortality due to
diarrhoea globally as well as in India were highlighted with the participants. States with high prevalence
of diarrhoea as per National Family Health Survey (2015-16) were also focused.
Midterm progress against targets of key performance indicators (KPIs) were shared with the participants
and key priorities and challenges were discussed like i) Zinc and ORS coverage; ii) Roll out of Rotavirus
vaccine in SDI project locations; iii) Behavior change methods for community to attain ODF; iv)
Integration and synergy between major departments for combating diarrhoea effectively.
Key speakers of the inaugural session, Dr. Ajay Khera from MoHFW and Dr. Dinesh Chand from
MDWS shared the perspective of ministries on diarrhoea prevention and control. Dr. Khera shared
about Intensified Diarrhoea Control Fortnight (IDCF), a specific campaign on diarrhoea prevention and
control through which GoI was able to reach 56 million children last year. GoI efforts for availability of
Zinc tablets for every child and the new specific guidelines to strengthen the hospital for hospitalization
of children with dehydration and pneumonia were discussed. GoI perspective on expansion of Rotavirus
vaccine in the country in phased manner was also explained.
Dr. Chand emphasized that diarrhoea prevention and control is not just the task for Health department,
but all the related departments should get together with a common objective. He shared that MDWS is
planning to have solid waste management system in place especially in rural areas. However, for
behavior change of the community, which is a key task, NGOs and other agencies efforts are required.
Key Discussion
Two panel discussions with the themes i) Low coverage to Zinc- Key challenges and possible solutions and ii)
Current challenges in achieving ODF and possible solutions were organised during the workshop. Key issues
and concerns raised by the panel members of the following panel discussions were:
Low coverage to Zinc- Key challenges and possible solutions
a) Full compliance of zinc is a problem. It doesn’t prevent dehydration as ORS does; hence the
condition of the child does not significantly affected by zinc. Neither does zinc effectively help the
child to regain energy nor does it stop diarrhoea immediately. On the other hand, perceptions
about antibacterial and anti-diarrhoeal drugs helps to stop diarrhoea immediately is high and is
readily available over the counter and prescribed by local/ private practitioners.
b) Supply of zinc all year round in the state and compliance of zinc for 14 days by mothers were
identified as the key problems in zinc usage.

Experience Sharing and Learning Workshop Page 5
c) Mothers who have children suffering from diarrhoea want the diarrhoea to stop immediately, hence
medical officers encourage the usage of antibiotics and anti-diarrhoeal drugs.
d) Requirement of regular training of the frontline workers on diarrhoea management and usage of
ORS and zinc.
e) Usage of mass media on specific messaging over zinc.
f) Concern raised on remuneration of ASHAs by GoI on diarrhoea case identification and ORS and
zinc compliance
Current challenges in achieving ODF and possible solutions
a) Both hardware and software were focused for effective sanitation. b) Significance of solid waste management was discussed to keep the drains in slums free flowing which
are generally blocked by solid waste from households
c) Requirement of certain processes was explained to change the social acceptability of OD which is
being practiced since long period.
d) Challenges due to which OD is happening i.e. 1) Availability of enough infrastructure 2) Community
mindset to accept OD were discussed.
e) Various success stories on ODF in Uttar Pradesh, Rajasthan, and Uttarakhand were shared with the
participants. Uttarakhand is going to be declared 4th ODF state in the country.
Key Recommendations
Following key recommendations were provided by the panel members as well as the audience.
Correct communication and usage of mass media to increase the acceptability and compliance of
zinc.
Looking into available evidence of zinc inducing vomiting in children older and six months,
communication around the same may help in increasing compliance.
Problems of procurement and supply as well as promotion around zinc needs to be addressed.
Medical officers to prescribe zinc for children in cases of diarrhoea.
Counseling of mothers on zinc by FLWs.
Making zinc available in the rural areas all-round the year.
Remuneration of ASHA for ORS and zinc compliance can be looked.
Compliance of zinc syrups better than zinc tablets. GoI may look into the same for a change in
strategy, if feasible.
Innovative technologies around mobile toilet settings can be used in urban slums where setting up
permanent structured toilets are not possible
Structures provided to households should be of improved quality as per the family needs for better
usage. Counseling on usage is very important
Engagement with children as change agents as they are the best advocates for their parents and
community

Experience Sharing and Learning Workshop Page 6
Inaugural Session

Experience Sharing and Learning Workshop Page 7
Welcome Address and Context Setting:
All the dignitaries and participants of the workshop especially from Government departments, Civil
Society Organizations, Implementing partners etc. were welcomed by Ms. Bidisha Pillai, Director Policy,
Programme Impact, Save the Children India. She first focused about the strategy, adopted by Save the
Children in 2016, to achieve following 3 breakthroughs, aligned with SDGs, for children by 2030.
a. To ensure that no child dies of preventable causes under the age of 5 years;
b. To ensure all children have access to and learn quality basic education;
c. To ensure violence against children is no longer tolerated.
She shared the following key points
1) Emphasized on the severity of diarrhoea
making it the 2nd major cause of under-
five child hood mortality in India as well
as globally.
2) Highlighted on partnership of Save the
Children with Reckitt and Benckiser
(RB) in 2012 with a program especially
focused on Water, Sanitation and
Hygiene which was very much focused
on access to clean drinking water,
access to sanitation and promotion of
good hygiene practices. However, Save
the Children realized that WASH could not be sufficient to control diarrhoea related deaths
thus this provided the genesis of Stop Diarrhoea Initiative project in 2015 which was focused on
WHO-UNICEF 7 Point Plan to prevent and control diarrhoea.
3) Pointed out the need to focus on Zinc which has a major concern of availability and supply.
4) Expressed gratitude to Government for being very supportive and collaborative to Save the
Children especially ministries of Health and Family Welfare, Education, Panchayati Raj etc.
5) Assured that SDI would not be just an intervention but would be ensured that it becomes the
part for the next generation and adults and spreads much wider.
Mid Term Progress – Stop Diarrhoea Initiative
A brief introduction about Stop Diarrhoea Initiative and the progress made by the programme by mid-
year of the period was shared by Dr. O.P. Singh, Team Leader, Stop Diarrhoea Initiative, Save the
Children India.
Dr. Singh highlighted the following key facts and issues:
1. Almost 64 children die per hour globally while it is 13 in India.
2. Eighty percent of these children die before 2 years of life.
3. Focused on States with high prevalence of diarrhoea as per National Family Health Survey
(2015-16)

Experience Sharing and Learning Workshop Page 8
4. Current trend of usage of Zinc and ORS is
not much encouraging, thus require more
efforts on it.
5. Explained each approach of 7 point plan i.e.
Treatment with ORS and Zinc, breastfeeding,
immunisation, hand washing with soap,
community wide sanitation, access to safe
drinking water attributing to reduction in the
prevalence of diarrhoea.
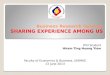
6. Shared the results of midterm progress against targets of key performance indicators.
Access of households to improved source of drinking water has increased from 42.1% in year I to 55.1%
in year II
Access of households to improved latrine/ flush toilets has increased to 57.9 % in year II from 39.4% of
year I.
Knowledge and practice of community workers on WASH according to national guidelines has shown an
increase from 42.9 % to 47.1 % from year I to II.
Percentage of front line health workers managing diarrhoea according to Government of India guidelines
has shown an increase from 72% in year I to 77.2% in year.
Percentage of fully immunized children as per the EPI schedule has gone up from 21% in year I to 62%
in year II.
Treatment of children under five suffering from diarrhoea with both ORS and Zinc has also shown a
slight increase from 7.1% in year 1 to 7.8%.
Percentage of households who could identify diarrhoea and its associated risk factors is 69.1% in year II
as against 48.7 % in year I.
Percentage of schools with effective participation of children has increased from 23 per cent in year I to
47.3 per cent.
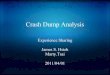
Percentage of health plans & programme documents developed with active participation and
consultation from community Ward Health Committee/WASH committee and CSOs increased from
28.9% in last to 52.5%.
7. Highlighted the key priorities and challenges:
a. Zinc and ORS coverage:
b. Roll out of Rotavirus vaccine in SDI project locations
c. Open Defecation Free: Need to work on longer behavior change methods for
community for changing their behavior and practices.
d. Integration and synergy between major departments like Health, Education. Women and
Child Development, Drinking Water and Sanitation and Panchayati Raj which would really be effective in combating diarrhoea.

Experience Sharing and Learning Workshop Page 9
National Perspective on Diarrhoea Management
Government of India perspective on diarrhoea management was shared by Dr. Ajay Khera, Deputy
Commissioner, In-charge Child Health, Ministry of Health and Family Welfare.
Dr. Khera first congratulated Save the Children to take up an initiative to address the issues of
diarrhoea. He focused on the following key points:
1) Despite number of efforts in direction to
reduce the prevalence of diarrhoea, which brought
substantial changes in child mortality, still around
lakh of children attribute to diarrhoeal deaths.
2) Availability and usage of ORS and Zinc
during diarrhoeal episodes is a challenge. If this
can be achieved for every child, than elimination of
deaths due to diarrhoea can be easily achieved.
3) To address diarrhoea, comprehensive and
holistic approaches are required. It has very close
association with malnutrition. It impacts overall cognition and child development. Thus, in
addition to survival of children, Government of India is now focusing on quality survival of
children.
4) Issues of diarrhoea cannot be dealt only by the health department, thus engagement of other
departments like drinking water and sanitation, Panchayati Raj, engagement of community and
school children would be more effective and would have multiplier effects.
Government of India perspective on Diarrhoea Management
a) GOI has been able to introduce specific campaign on diarrhoea named as Intensified Diarrhoea
Control Fortnight (IDCF). Under this campaign, ASHA visits all the under-five children in her
areas, delivers ORS and provides desired information and counseling. Through this campaign,
GoI was able to reach 56 million children last year, which is 55-56 percent coverage of all under
five children.
b) ORS and Zinc corners were established to demonstrate mothers, the correct process of
preparing ORS as many of them don’t know the correct way of its usage.
c) GoI is making efforts for availability of Zinc tablets for every child once he/she gets an episode
of diarrhoea. This would prevent future episodes of diarrhoea and reduce overall episodes of
illness.
d) Major issues around zinc are related to logistics and supply. GoI would be interested in knowing
whether the issues are related to availability or acceptability of zinc as many of the private
practitioners do not prescribe Zinc. For this awareness and dedicated counseling for health
professionals will be critical to increase zinc usage rate.
e) GoI has come up with specific guidelines to strengthen the hospital for hospitalization of
children with dehydration and pneumonia.
f) Rotavirus vaccine has been introduced in the country and will be expanded in the country in
phased manner. However, campaigns on measles and rubella vaccine (MR vaccine) are going on,
which would have impact on diarrhoea control.

Experience Sharing and Learning Workshop Page 10
Dr. Khera further shared that GoI is keen to minimize deaths due to diarrhoea and learning from Save
the Children India would be very helpful in strategizing while PIPs are sanctioned.
Special Address by Dr. Dinesh Chand, Additional advisor to Ministry of
Drinking Water and Sanitation
Dr. Chand focused on following key points:
1) Diarrhoea prevention and control is not just the task for Health department, but all the related
departments should get together with a common objective.
2) People residing in many states especially
Uttar Pradesh, Bihar, Madhya Pradesh,
Rajasthan are mostly dependent on hand
pumps and thus disease burden in such
states is high due to mishandling of water.
Even storage of water is a big problem, thus
MDWS has introduced the scheme “Har
Ghar Nal ka Jal” to improve the piped water
supply in households.
3) Save the Children could be an intermediary
organization between MDWS and
Panchayats and community.
4) MDWS has been engaging with other departments like MoHFW and Education department for
these issues.
5) MDWS is also planning in a big way to have solid waste management system in place especially
in rural areas. Government can address the issue of processing the waste and constructing
infrastructures but for behavior change, NGOs and agencies efforts are required.
Closing Remarks
Closing remarks were given by Dr. Rajib Dasgupta, Professor, Center of Social Medicine and
Community Health, JLN University, Delhi.
Dr. Dasgupta raised the following key issues:
1) Access to treatment for acute
diarrhoeal disease is still a problem.
Diarrhoeal deaths still remain a
problem.
2) Lack of access to health services is a
very crucial factor in diarrhoea deaths.
3) Despite the large number of services
being provided under National health
Mission, pockets of exclusion remains,

Experience Sharing and Learning Workshop Page 11
towards which all the government departments, civil society organizations need to collectively
address the problem. Existence of such pockets means the weak or inadequate accountability
mechanism, which is required to be strengthened.
4) By the end of project, we will be able to document learning from the project and able to come
up with somewhat differently tailored strategy to address the problem in rural and urban areas
differently as similar approaches do not work.
5) It is envisaged that after project period, a system is left with inbuilt strengths and capabilities.
Dr. Dasgupta concluded by focusing on demonstration of some workable multi-sectoral model in SDI
intervention areas and leave the system strong over and above achieving, what has been sought to
achieve.
Play performed by School Children and Key material displayed in workshop
A very creative play was performed by school children. It was based on strengthening the
communication and messaging with the community for prevention and control of diarrhoea.
An exhibition stall was also set- up displaying various key materials about the project and IEC materials.
School Children performing play
IEC material displayed in the workshop

Experience Sharing and Learning Workshop Page 12
Panel Discussions

Experience Sharing and Learning Workshop Page 13
Panel Discussion – I: Low coverage to Zinc- Key challenges and possible
solutions
Chair:
1. Dr. Sila Deb, Deputy Commissioner, Child Health, Ministry of Health and Family Welfare,
Govt. of India
Panelists:
2. Dr. Samiran Panda, Scientist- F and Senior Deputy Director, Indian Council Of Medical
Research (ICMR)- National Institute of Cholera and Enteric Diseases (NICED)
3. Dr. Anil K. Verma, General Manager Child Health, National Health Mission, Uttar Pradesh
4. Dr. Vinod Anand, Technical Advisor, Health, Save the Children, India
5. Dr. Naresh Trikha, Clinton Health Access Initiative (CHAI), India
6. Dr. Praful, MO I/C, Laksar, Haridwar, UTK
Dr. Sila Deb first introduced the panelists and moderated the panel discussion.
Key points highlighted by the panelists are as follows:
1. Key points highlighted by Dr. Samiran Panda :
a) Defining of target audiences i.e. children and mothers.
b) Three things that matters most to the mothers whose child is suffering from Diarrhoea
a. Condition of the child should not deteriorate
b. Child should regain energy
c. Diarrhoea should stop

Experience Sharing and Learning Workshop Page 14
In line with the above perceptions, Zinc
doesn’t prevent dehydration as ORS does;
hence the condition of the child does not
significantly affected by zinc. Neither does
zinc effectively help the child to regain energy
nor does it stop diarrhoea immediately.
Hence the full compliance of zinc is a
problem.
On the other hand the perceptions about
antibacterial and anti-diarrhoeal drugs helps
to stop diarrhoea immediately is high and is
readily available over the counter and
prescribed by local/ private practitioners
c) Zinc being a new entrant in the market its availability in public and private facilities is a
challenge.
d) Treatment modality in case of diarrhoea need to be reemphasized and male participation
needs to be encouraged.
e) Cochrane review in December 2016 cites, although zinc supplementation probably shortens
the average duration of diarrhoea by around 16 hours it increases the risk of vomiting
(moderate certainty evidence) in children older than six months
f) Hence communications around zinc needs to be relooked to avoid the mothers not giving
zinc to their children in spite of having access to it.
II. Key points highlighted by Dr. Anil K. Verma
a) Emphasized on the utility of zinc in diarrhoea
and challenging problems of procurement and
promotion of zinc.
b) Management of acute and moderate to severe
diarrhoea.
c) Acknowledged the challenge of Medical
officers on counselling and prescribing zinc.
d) Emphasized on the importance of counselling
of mothers through frontline health workers.
e) Supply of zinc all year round is an issue in the
state, and compliance of zinc for 14 days by mothers
are also identified problems.
f) Acceptability of zinc tablets at the field is low, zinc being dispersible tablet hence may
breakdown easily if not properly handled.
g) Taste masking of zinc was also proposed to ensure better compliance.
h) Suggested AYUSH medical practitioners to be inducted in IDCF to attain larger coverage and
acceptability.

Experience Sharing and Learning Workshop Page 15
III. Key Points highlighted by Dr. Praful
a) Mothers not willing to comply with zinc especially for 14 days;
b) Counselling of mothers is key for compliance on ORS and zinc;
c) Availability of zinc is still a challenge in the rural areas all year round.
IV. Key points highlighted by Dr. Naresh Trikha
a) Shared his experience of the diarrhoea
management programme, implemented by
CHAI
b) Cognitive understanding of diarrhoea
low among mothers and caregivers
c) Zinc tablets should be dispersed
within 60 seconds in water which is generally
not the case with from the Govt. supplies.
d) Care seeking pattern of the mothers
and care givers with the local RMPs
e) Zinc is not seen or perceived as
treatment by the mothers and caregivers
f) He emphasized on usage of mass media on specific messaging over zinc
g) ASHAs not currently remunerated by GoI on Diarrhoea case identification and ORS and zinc
compliance
h) Zinc syrup compliance is better than zinc tablets where mothers complain about its taste and
tendency of the children to vomit
i) He also share an internal survey result where about 47% mothers who had their children
suffering from diarrhoea could not identify zinc tablets
V. Key Points shared by Dr. Vinod Anand
a) Mothers who have children suffering from
diarrhoea want the diarrhoea to stop,
which ORS and zinc are not capable of;
hence medical officers encourage the usage
of antibiotics and anti-diarrhoeal drugs.
b) He emphasized on the messaging and
communication with mothers that clearly
state the purpose of ORS and zinc not as
medicines that will stop diarrhoea but will
not deteriorate the child’s condition. It will also help the child recover faster and avoid future
relapses. However, supply issue needs to be addressed by the government.
c) Regular training of the frontline workers required on diarrhoea management and usage of ORS
and zinc.

Experience Sharing and Learning Workshop Page 16
Dr. Sila Deb summarized the discussion points
and concluded the discussion
a) She acknowledged the fact of noncompliance
of zinc due to long treatment schedule;
b) She emphasized on the correct
communication strategies on zinc, importance
of correct messaging.
c) Acknowledged the role of the informal sector
in promotion of ORS and zinc
Dr. Deb thanked all the panelists for their rich inputs regarding issues around diarrhoea and concluded
the session with a vote of thanks.
Panel Discussion – II: Current challenges in achieving ODF and possible
solutions
Chair:
1. Prof. Vijayaraghavan M Chariar, Professor, IIT Delhi
Panelists:
2. Mr. Sanjay Singh Chauhan, Consultant- Panchayati Raj Dept, Uttar Pradesh
3. Mr. S.K. Mahajan, Chief Engineer, DUSIB
4. Dr. Nabaneeta Rudra, Technical Advisor, Plan India
5. Mr. Shailendra Singh Bisht, Programme coordinator, Swajal, Uttarakhand
6. Col. Prabhat Chaturvedi , Retd. Chief Engineer, DUSIB

Experience Sharing and Learning Workshop Page 17
Dr. Chariar welcomed all the panel members on the dais. He briefly introduced all the members to the
audience.
Key discussion points highlighted by the panel members are as follows:
I. Mr. Sanjay Singh Chauhan highlighted the following key points:
a) Stressed upon two important things in
sanitation: hardware and software.
b) Mentioned that from last one year, SBM in UP is
gearing up and focusing on CLTS. Many families
in districts like Bijnor and Sahranpur have left
the incentives to construct toilet. They are
constructing the toilets on their own and are
also using them.
c) Shared that around 7000 GPs in Uttar Pradesh
have become ODF till now. From last one year, people are coming forward and behavior change
is actually seen happening on ground. Shamli is the first district in UP which has become Open
Defecation free. In a recent meeting at Varanasi, Hon’ble Chief Minister declared about making
30 districts ODF in this year. However State Government and Central Government do not
have enough funds for it, so it will be done through community incentives.
II. Key Points highlighted by Dr. S.K. Mahajan
a) Shared about the DUSIB’s work in JJ Basti. Last year, a research study was conducted to know
the actual number of open defecation spots in JJ Basti. Study results revealed that there are as
such 253 OD spots in the area. On the basis of this study, gap analysis was done. On an average
there is a ratio of 1:25 toilet for women and 1: 35 toilet for men, so on an average of 1: 30 ratio
was taken and thus the gap of 17000 seats in that area was identified.
b) Slums have been provided with almost
all basic amenities by different departments.
They have been allotted individual water
connections at their doorsteps. After gap
analysis DUSIB started constructing community
toilet complexes (CTC) and rehabilitating
insanitary CTCs. But the big issue in front of
DUSIB was about the usage of these facilities.
DUSIB has created an app and online
monitoring system to strengthen the
monitoring mechanism.
c) Discussed about importance of solid waste management to keep the drains in slums free flowing
which are generally blocked by solid waste from households.

Experience Sharing and Learning Workshop Page 18
d) Out of total 675 slums, DUSIB has decided to make 52 slums as model slums. Karotiya camp is
the first model slum where people have come forward to make it clean. He concluded by
stressing upon community involvement in making any movement successful.
III. Key points shared Dr. Nabaneeta Rudra
a) Shared that OD is socially acceptable and
being practiced since long period hence
certain processes are required to change it
which needs time and monitoring.
However, open defecation is also happening
at places which have been declared ODF.
b) Mentioned two challenges due to which OD
is happening. 1) Availability of enough
infrastructure 2) Community mindset to
accept OD.
c) OD is ultimately leading to diarrhoea hence it is important to control factors which are
responsible for diarrhoea.
d) Shared about Plan India’s initiatives in Udaipur and Bikaner and their engagement with
community to reach to the root cause of problem.
She concluded by mentioning that behavior change is important in sanitation and retaining behavior
change is further more important.
IV. Key points shared by Mr. Shailendra Singh Bisht
a) Highlighted that India is the largest open defecation country in the world. Around 60% of
population in India is defecating in open. Nigeria is on second position.
b) Shared the problem of non-usage
starts with the kind of facility provided to
them. If people have been provided with
good toilet facility they tend to use it. He
mentioned that two years back, sanitation
coverage in Uttarakhand was 70%. Now,
after Sikkim, Kerala and Himachal,
Uttarakhand will be the fourth state going
to be ODF.
c) Uttarakhand has constructed 5 lakh
80 thousand toilets in last two years. IEC,
IPC and BCC are the key aspects of sanitation and sustainability is equally important. He
stressed upon, to see the socioeconomic and educational profile of any state before launching
IEC for any state. The biggest challenge in ODF is convergence of different departments. To
make Uttarakhand ODF, they adopted multi-pronged strategy.

Experience Sharing and Learning Workshop Page 19
d) Mentioned four issues which came up during the process were 1) As per baseline, the toilet
construction figure was 5, 90,000; 2) Left out HHs in population growth 3) Defunct toilets
4) who have taken the subsidy under other programme but not constructed toilet.
e) Tapping CSR fund to construct toilets for left outs was also a good strategy according to him.
He mentioned that Save the Children is also constructing toilets, though in small amount, which
helped the Government to reach the goal of ODF.
f) Shared the process of Government’s success in making Uttarakhand ODF. The government
designed a strategy divided into three parts. Statistics were shared with PRIs about their
position in OD at district, block and village level which made them to think to improve their
position. Literate representatives of PRIs were Uttarakhand’s advantage. After 3 months of
continuous rigorous work Uttarakhand is about to be ODF. Uttarakhand prepared a local logo
for SBM, SWACHATA KI UDAAN to bring impact on local people.
g) The strategy of sending post cards to all five lakh families which were addressed by Chief
Minister created wonders. Bulk SMS, documentaries were supplemented in their communication
strategy. Motivation was given to Pradhan and they played an important role in this journey.
Uttarakhand is in state of ODF + now.
h) Providing proper infrastructure is a key to usage as because defunct infrastructure leads to non-
usage.
V. Key points highlighted by Col. Prabhat Chaturvedi
1) Shared about his engagement with Save the
Children since last 5 years. He stressed upon
preventive factors for diarrhoea like
breastfeeding and hand washing.
2) Mentioned 3 suggestions to improve on
WASH:
Engagement with children as they are the
best advocates for their parents and
community.
Engagement with school children to bring
water efficiency. Tell children to prepare
projects to save water
Construction of Sewage treatment plants to treat the sewage coming out from slums
Prof. Vijayaraghavan M Chariar summarized the points shared by the panel members.
a) He focused on identifying the triggering factor for community to make Swacch Bharat Mission
successful. Understanding the context is important before planning any intervention for any
area.
b) Shared that lot of work is required to be done on software side so that hardware can be
utilized.

Experience Sharing and Learning Workshop Page 20
c) Stressed upon more networking between
CSOs to improve the sanitation status of country and
also significant role of academia.
He concluded the session with Jack smith quote who
heads World Toilet Organization “Toilet is the
cheapest medicine”. Hence everyone should move
towards toilets and more sustainable use of toilets.
Taking the SDI Forward and Vote of Thanks
Dr. Rajesh Khanna, Sr. Technical Advisor, Health and Nutrition, closed the session with his vote of
thanks to all the participants for their participation and involvement in the workshop and making it
successful.
He expressed his gratitude to all the panel members
for presenting their views on burden of diarrhoea in
India and its prevention and control through
engaging and provoking panel discussions.
He shared the vision of Save the Children and
rationale behind implementation of Stop Diarrhoea
Initiative.
He also emphasized on the following key points of
the programme and takeaways from the day
discussions:
a) Comprehensive and integrated approach for diarrhoea prevention and control;
b) Involvement of children as agents of change;
c) Evidence based sustainable, context specific behavior change;
d) Supply side innovations;
e) Involving private sectors;
f) Scale up learning from the project;
He extended a Vote of thanks, for the participants who have travelled from the states and project
locations. He extended his heartiest thanks for representatives from the ministries: Dr. Ajay Khera,
Dr. Sila Deb and Dr. Dinesh Chand. He also extended his gratitude towards Government officials from
the States, Dr. Anil Verma, Mr. Sanjay Singh and participants from Uttarakhand, Delhi and West Bengal.
He thanked all the NGO partners who are directly or indirectly working with Save the Children to
combat diarrhoea and lastly the Stop diarrhoea Initiative project team for their efforts to reach where
they are now. In last, Dr. Khanna promised the gathering to get back to them after the completion of
the project to share project updates and key learnings.

Experience Sharing and Learning Workshop Page 21
Key recommendations from the panel discussions:
Key issues discussed Key recommendations from the Panelists
1. Low coverage to
Zinc
a. Correct communication and usage of mass media to increase the
acceptability and compliance of zinc.
b. Looking into available evidence of zinc inducing vomiting in children older
and six months, communication around the same may help in increasing
compliance.
c. Male participation needs to be encouraged.
d. Problems of procurement & supply, promotion and phobia around zinc
needs to be addressed.
e. Medical officers to prescribe zinc for children in cases of diarrhoea.
f. Counseling of mothers on zinc by FLWs.
g. Taste masking of zinc tablets to ensure better compliance.
h. Making zinc available in the rural areas all-round the year.
i. Remuneration of ASHA for ORS and zinc compliance can be looked.
j. Compliance of zinc syrups better than zinc tablets. GoI may look into the
same for a change in strategy, if feasible.
2. Achieving ODF and
possible solutions
a. Innovative technologies around mobile toilet settings can be used in
urban slums where setting up permanent structured toilets are not
possible
b. Key focus on personal hygiene behaviors can work wonders if
interventions are planned keeping in minds, local customs, behaviors,
beliefs and practices.
c. Structures provided to households should be of improved quality as per
the family needs for better usage. Counselling on usage is very important
d. Multi-pronged strategy for achieving ODF should be very specific,
considering socio economic, cultural and educational profile of the
community
e. Engagement with children as change agents as they are the best
advocates for their parents and community

Experience Sharing and Learning Workshop Page 22
ANNEXURE A
Mid Term Progress in Key Performance Indicators
Outcome 1: Access to quality diarrhoea prevention and control services for at least
80% of households in target areas of nine districts by the end of the programme
Outcome 2: Community Awareness and Practices for Prevention and Control of
Diarrhoea in target areas improved
42.1 39.4 42.9
72
21
7.1
60 55 55
75
55
45
55.1 57.9
47.1
77.2
62
7.8
% of householdswith access to
improved source ofdrinking water
% of householdswith access to
improved latrine/flush toilets
% of communityworkers with
Knowledge andpractice on WASH
% of front linehealth workers
managingdiarrhoea
according to GoIguideline
% of children underfive children fullyimmunised as perthe EPI schedule
% of children underfive with diarrhoeatreated with both
ORS and Zinc
Year 1 achievement Year II Target Year II achievement
48.7
23
55
30
69.1
47.3
% o f h o u s e h o l d s w h o c o u l d i d e n t i f y d i a r r h o e a a n d i t s a s s o c i a t e d r i s k f a c t o r s
% o f s c h o o l s w i t h e f f e c t i v e p a r t i c i p a t i o n o f c h i l d r e n i n s c h o o l h e a l t h c l u b s a n d
c o m m i t t e e s
Year 1 achievement Year II SDI Target Year II SDI Achievement

Experience Sharing and Learning Workshop Page 23
Outcome 3: Provincial, district and community commitment, accountability and
ownership for increased access to diarrhoea prevention and control and scale up at
all levels enhanced by the end of the programme
28.9
22.2
50 50 52.5
55.6
P e r c e n t a g e o f h e a l t h p l a n s & p r o g r a m m e d o c u m e n t s d e v e l o p e d w i t h a c t i v e
p a r t i c i p a t i o n a n d c o n s u l t a t i o n f r o m c o m m u n i t y W a r d H e a l t h C o m m i t t e e / W A S H
c o m m i t t e e a n d C S O s
P e r c e n t a g e o f w a r d s / b l o c k s m a i n t a i n i n g m i n i m u m s t a n d a r d s M I S d a t a q u a l i t y
a c c o r d i n g t o n a t i o n a l g u i d e l i n e
SDI Year I achievement SDI Year II Target SDI Year II Achievement

Experience Sharing and Learning Workshop Page 24
ANNEXURE B
Stop Diarrhoea Initiative – Experience Sharing and Learning Workshop
Indian Habitat Center, New Delhi
May 30, 2017
Agenda
Particulars Time Speakers
Registration 09:00 AM – 10:00
AM
Inaugural Session
Welcome Address and Context Setting 10:00 AM - 10:10 AM Bidisha Pillai, Director, Policy, Programme and Impact Save the Children,
India
Stop Diarrhoea Initiative - Mid Term Progress 10:10 AM – 10:30 AM Dr. O.P. Singh, Team Leader, Stop Diarrhoea Initiative, Save the
Children, India
National Perspective on Diarrhoea Management 10:30 AM - 10:45 AM Dr. Ajay Khera, Deputy Commissioner, I/C Child Health, Ministry of
Health and Family Welfare, GoI
Special Address 10:45 AM – 11:00 AM Dr. Dinesh Chand, Additional Advisor, Ministry of Drinking Water and Sanitation, GoI
Closing Remarks 11:00 AM - 11:15 AM Dr. Rajib Dasgupta, Professor, Centre of Social Medicine and
Community Health, Jawaharlal Nehru University, Delhi
High Tea and showcasing state wise project interventions – Exhibition display 11:15 AM- 11:45 AM
Discussion Session
Panel Discussion - I
Low coverage to Zinc- Key challenges and
possible solutions
11:45 AM – 12:30 PM
Chair – Dr. Sila Deb, Deputy Commissioner, Child Health, Ministry
of Health and Family Welfare, GoI
Panelists
1. Dr. Samiran Panda, Scientist-F & Senior Deputy Director, ICMR-
NICED
2. Dr. Anil K. Verma, General Manager, Child Health, National
Health Mission, Uttar Pradesh
3. Dr. Praful, , Medical Officer, Laksar, Haridwar, Uttarakhand
4. Dr. Vinod Anand, Technical Advisor, Health, Save the Children,
India
5. Dr. Naresh Trikha, Clinton Health Access Initiative(CHAI), India
Panel Discussion –II
Current challenges in achieving ODF and
possible solutions
12:30 PM – 01:15 PM
Chair – Prof. Vijayaraghavan M Chariar, Professor, IIT
Delhi
Panelists
1. Mr. Shailendra Singh Bisht, State Coordinator SBM,
Dept. of Drinking Water and Sanitation, Uttarakhand
2. Dr. Nabaneeta Rudra, Technical Advisor, WASH,
Plan India
3. Mr. Sanjay Singh Chauhan, State Consultant, SBM,
Department of Panchayati Raj, Govt. of Uttar Pradesh
4. Mr. S.K. Mahajan, Chief Engineer, DUSIB
5. Col. Prabhat Chaturvedi , Retd. Chief Engineer,
DUSIB
Way Forward
Taking the SDI forward 01:15 PM – 01:25 PM Dr. Rajesh Khanna, Sr. Technical Advisor, Health and Nutrition
Vote of Thanks 01:25 PM – 01:30 PM Dr. O.P. Singh, Team Leader, Stop Diarrhoea Initiative
Lunch 01:30 PM – 02:30 PM

Experience Sharing and Learning Workshop Page 25