Embed Size (px)
Citation preview

New Frontiers and Combination Pharmacotherapy for Obesity Management
Donna H. Ryan, MDPennington Biomedical Research Center
Baton Rouge, [email protected]

OUTLINE
• Pharmacotherapy: What is available?• What is anticipated?
– “Druggable targets” and new agents– Combination approaches (combinations of drugs
already on market for other indications)

What is available now?PHENTERMINE
DIETHYLPROPION
FDA approved 1959 Stimulant / promotes loss of appetite Once daily with or without food Some abuse potential
SIBUTRAMINE
FDA approved 1997 Induces feeling of satiety
– satisfied with less food– greater control of intake
Once daily with or without food
ORLISTAT FDA approved 1999
Blocks absorption of ~30% dietary fat
– GI side effects
3 times daily with meals vitamin supplement

Comparison of available drugs
Mechanism CentralNoradrenergic
Central SNRI
PeripheralPancreatic lipase
inhibitor
Approval Short term useClass II-IV
Long term useClass IV
Long term useNot scheduled
Cost $ $$$ $$$$
Efficacy – drug only/ drug + LS
5%/? 5%/15% 5%/8%
Pros Patient satisfaction &
cost
Demonstrated efficacy
Safety cost
Cons Prescribing time limit
? BP elevation
BP elevation
reimbursement
Tolerability
reimbursement
PHENTERMINE DIETHYLPROPION SIBUTRAMINE ORLISTAT

OUTLINE
• Pharmacotherapy: What is available?• What is anticipated?
– “Druggable targets” and new agents– Combination approaches (combinations of drugs
already on market for other indications)

Brain
Central signalsStimulate
NPYAGRPgalanin
Orexin-Adynorphin
Inhibita-MSH
CRH/UCNGLP-ICART
NE5-HT
External factors
EmotionsFood characteristicsLifestyle behaviorsEnvironmental cues
Peripheral signals Peripheral organs
Food intake
Glucose
CCK, GLP-1, Apo A-IVVagal afferents
Insulin
Leptin
Cortisol
–
–
+
Gastrointestinal tract
Adipose tissue
Adrenal glands
Ghrelin+
Regulation of Food Intake
Energyout

The first new obesity drug developed based on new biology of obesity
Patients Before Treatment

After 3 Months of Treatment

A Family AffairHormone Leads to Dramatic Weight Loss for Three Cousins
Aug. 7 – How can three family members slim down to half their body weight without even trying? With the help of an appetite control hormone called leptin, new research suggests.
Only 10 months later, the cousins have lost nearly half their body weight.
After Ten Months of Treatment
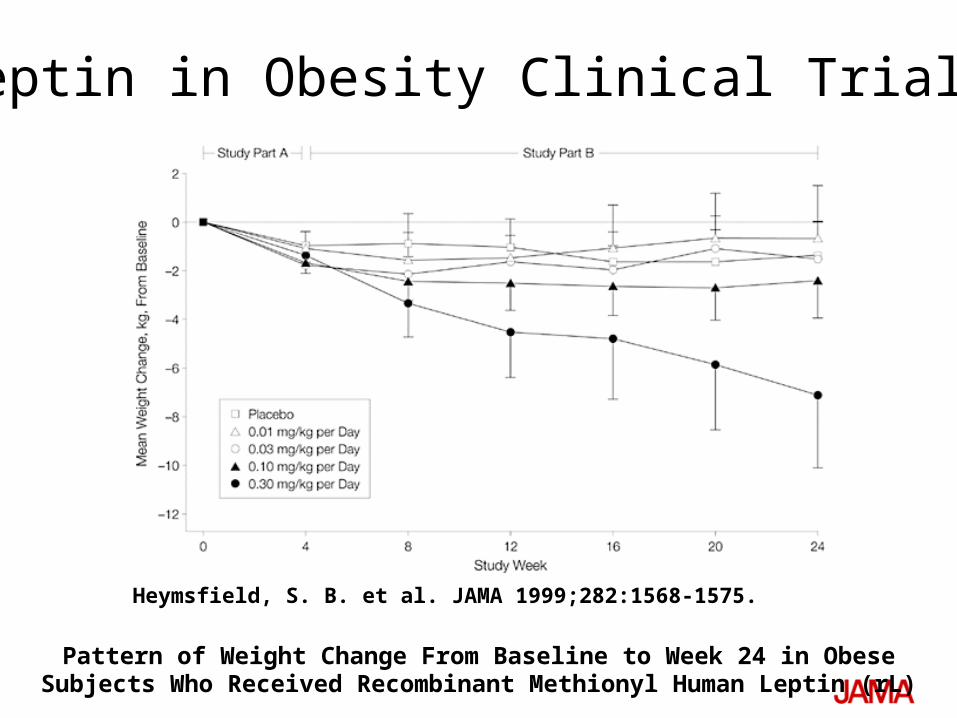
Heymsfield, S. B. et al. JAMA 1999;282:1568-1575.
Pattern of Weight Change From Baseline to Week 24 in Obese Subjects Who Received Recombinant Methionyl Human Leptin (rL)
Leptin in Obesity Clinical Trials

“Druggable Targets” – Record to Date
• Serotonin, Norepinephrine, Dopamine– amphetamines, fenfluramine, dexfenfluramine, bupropion, phentermine,
diethylpropion, sibutramine, ecopipam • Cannabinoid receptor
– rimonabant, taranabant, at least 3 others• NPY
– Merck MK 0557 and Shionogi S2367• Uncertain neural mechanisms
– topiramate, CNTF• Leptin• Amylin
– pramlintide• GLP-1 ,GIP, PYY, oxyntomodulin
– exenatide, liraglutide, DPP IV inhibitors (sitagliptin), PYY 3-36, oxyntomodulin

“Druggable Targets” – Record to Date
• Serotonin, Norepinephrine, Dopamine– amphetamines, fenfluramine, dexfenfluramine, bupropion, phentermine,
diethylpropion, sibutramine, ecopipam • Cannabinoid receptor
– rimonabant, taranabant, at least 3 others• NPY
– Merck MK 0557 and Shionogi S2367• Uncertain neural mechanisms
– topiramate, CNTF• Leptin• Amylin
– pramlintide• GLP-1 ,GIP, PYY, oxyntomodulin
– exenatide, liraglutide, DPP IV inhibitors (sitagliptin), PYY 3-36, oxyntomodulin
On market with
weight loss indication
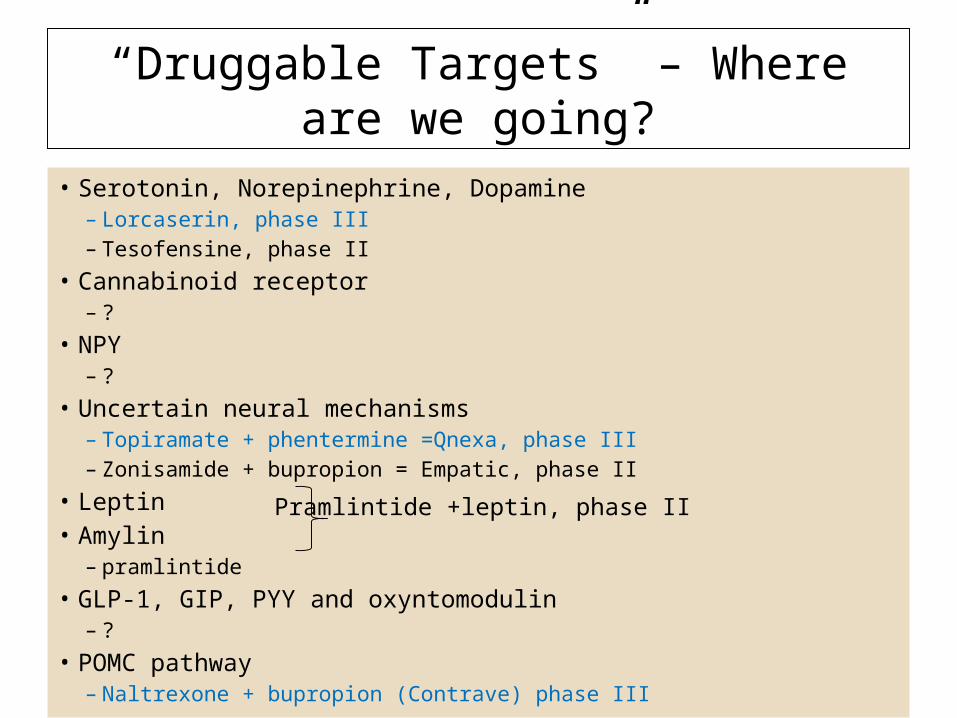
“Druggable Targets” – Where are we going?
• Serotonin, Norepinephrine, Dopamine– Lorcaserin, phase III– Tesofensine, phase II
• Cannabinoid receptor– ?
• NPY– ?
• Uncertain neural mechanisms– Topiramate + phentermine =Qnexa, phase III– Zonisamide + bupropion = Empatic, phase II
• Leptin• Amylin
– pramlintide• GLP-1, GIP, PYY and oxyntomodulin
– ?• POMC pathway
– Naltrexone + bupropion (Contrave) phase III
Pramlintide +leptin, phase II

3 Drugs will go before FDA Panels in 2010
• lorcaserin• bupropion + naltrexone (Contrave)• topiramate + phentermine (Qnexa)
• safety• safety• safety
3 most important factors in successful review

Zero tolerance for neuropsychiatric adverse profile: RIO-North America: Adverse Events
Leading to Drug Discontinuation in Year 1
Placebo(n = 607)
(%)
Rimonabant 5 mg(n = 1214)
(%)
Rimonabant 20 mg
(n = 1219)(%)
Psychiatric disorder 2.3 3.6 6.2
Depressed mood 1.3 2.1 2.2
Anxiety 0.3 0.6 1.0
Irritability 0 0.2 0.5
Insomnia 0.2 <0.1 0.5
Nervous system 1.0 1.2 2.2
Headache 0.3 0.3 0.5
Dizziness 0.2 0 0.7
Gastrointestinal tract 0.7 0.7 1.6
Nausea 0.2 0.2 0.9Adapted with permission from Pi-Sunyer FX, et al. JAMA. 2006;295:761-775.

FDA Guidelines for Obesity Products
Efficacy Benchmark Categorical response: > 35% of patients on drug lose at least 5% of their body weight and
that the proportion is double placebo- OR -
Mean weight loss: >5% difference between active product and placebo group
Additional Endpoints: Study markers of CV and metabolic risk
Experience in Diabetes Study measures of glycemic control
Trial Size & Duration >3,000 subjects randomized to active doses of the product and >1,500 subjects randomized
to placebo for 1 year of treatment

Lorcaserin – selective approach to the serotonin receptor
• 5-HT2C receptor is a validated target
– Located in the hypothalamus
– Regulates satiety
– May affect metabolic rate
• NME* that selectively targets the 5-HT2C receptor
– ~100-fold selectivity over 5-HT2B receptor
– ~15-fold selectivity over 5-HT2A receptor
• Fenfluramine is a non-specific serotonin receptor agonist
– Potential to activate all 14 known serotonin receptors
* New molecular entity

Lorcaserin: 1 Year Results
18
% Categoricalor
% Mean Weight Loss
BLOOMN=3182
BLOSSOMN=4008
10 mg BID
Placebo 10 mg BID
10 mg QD
Placebo
5% Per Protocol 66.4 32.1 63.2 53.1 34.9
5% ITT-LOCF 47.5 20.3 47.2 40.2 25.0
10% Per Protocol 36.2 13.6 35.1 26.3 16.1
10% ITT-LOCF 22.6 7.7 22.6 17.4 9.7
Mean Per Protocol (%) 8.2 3.4 7.9 6.5 3.9
Mean ITT-LOCF (%) 5.8 2.2 5.9 4.8 2.8
Data courtesy Arena
19
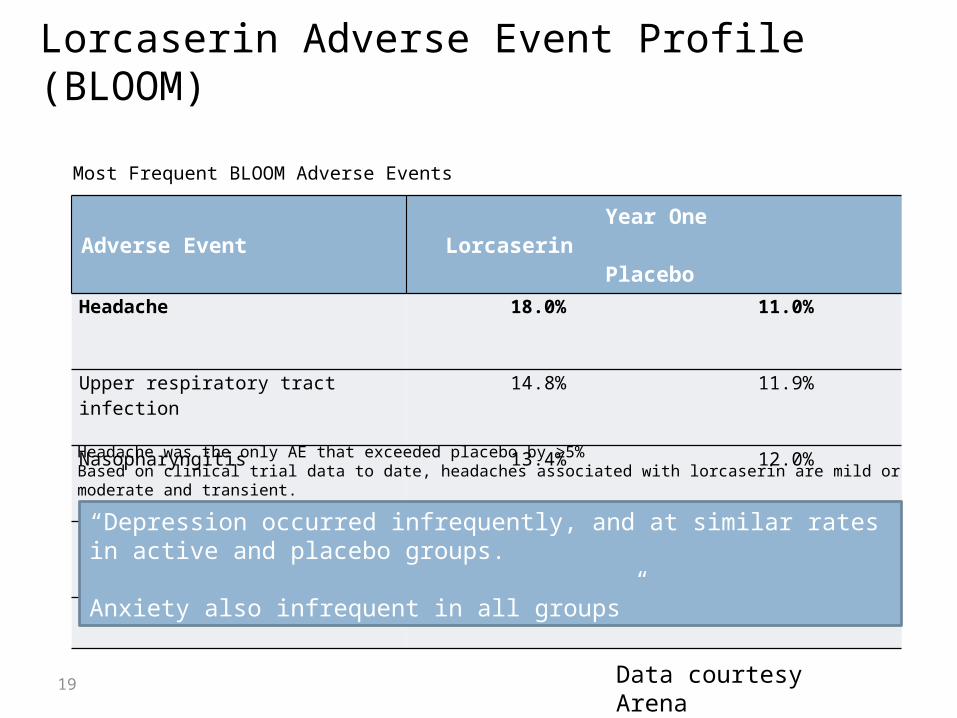
Adverse Event Year OneLorcaserin Placebo
Headache
18.0% 11.0%
Upper respiratory tract infection
14.8% 11.9%
Nasopharyngitis
13.4% 12.0%
Dizziness
8.2% 3.8%
Nausea
7.5% 5.4%
Most Frequent BLOOM Adverse Events
Headache was the only AE that exceeded placebo by ≥5%Based on clinical trial data to date, headaches associated with lorcaserin are mild or moderate and transient.
Lorcaserin Adverse Event Profile (BLOOM)LOOM Tolerability: Adverse Events
“Depression occurred infrequently, and at similar rates in active and placebo groups.
Anxiety also infrequent in all groups”
Data courtesy Arena

Lorcaserin Weight Loss Over Time(BLOSSOM)
20
17.0 lbs, 7.9% at wk 52
14.3 lbs, 6.5% at wk 52
8.7 lbs, 3.9% at wk 52
Data courtesy Arena

BLOSSOM: Secondary Endpoints
21
Risk Factor Improved ITT p-valuePer Protocol
p-value
HDL cholesterol Yes 0.0001 0.0004
Triglycerides Yes 0.0172 0.0011
LDL cholesterol Yes 0.0676 0.0727
Systolic BP Yes 0.0689 0.0003
Diastolic BP Yes 0.0804 0.0006
Top-line Results
• Data on glycemic parameters is pending but were positive in BLOOM• Inflammatory markers were not measured but were significantly reduced
in BLOOM
Data courtesy Arena

Combined Echocardiographic Data Set FDA Valvulopathy : grade I Aortic Regurgitation, grade II Mitral
Regurgitation
Valvulopathy Rates
BLOOM BLOSSOM
10 mg BID
Placebo 10 mg BID
10 mg QD
Placebo
Week 52 2.7% 2.3% 2.0% 1.4% 2.0%
Week 104 2.6% 2.7%
22
Pulmonary Artery Systolic Pressure did not increase in any group
Data courtesy Arena

Orexigen strategy: POMC Pathway Targets• POMC pathways are common
pathways of signals of energy balance – Represent a “node of influence;” can
alter how the brain perceives body weight
– Resistance to leptin in obesity– Agonist of the melanocortin system
• STEP 1: accelerate POMC neuron firing by the by-pass of leptin resistance
– reduces appetite– increases energy expenditure
• STEP 2: inhibit compensatory mechanisms thought to mitigate drug benefits over time
– Beta endorphin– AgRP
POMC*
Source: Orexigen
Contrave = Bupropion +
naltrexone
Empatic = Bupropion +
zonisimide

% ofPatientsLosing>5% ofBody
Weight
Bupropion + Naltrexone in Large Phase III Trials
NB-301 Results5% Categorical Analysis (ITT-LOCF)
NB-303 Results^ 5% Categorical Analysis (ITT-LOCF)
% ofPatientsLosing>5% ofBody
Weight
Placebo Contrave16 Contrave32
n= 456
n=825 n=511
n=471
n=471
n=511
n=471
n=471
n= 456
n=702
Note: All differences between drug and placebo highly statistically significant at p<0.001^ Results of re-randomized NB48 group not shown; no statistical difference from re-randomized NB32 group‡ Primary Endpoint* Weighted LOCF Data courtesy
Orexigen

Bupropion + Naltrexone 1 Year Weight Loss Trajectory
NB-301 Observed Case Weight Loss
NB-303 Observed Case Weight Loss *
% Weight Loss vs.
Baseline
Week 0 Week 14
Week 28
Week 42
Week 56
Week 0 Week 14
Week 28
Week 42
Week 56
Placebo Contrave32
8.2%8.2%
1.9% 1.4%
* Contrave32 weighted analysis
% Weight Loss vs.
Baseline
Data courtesy Orexigen

Bupropion + Naltrexone Most Common Treatment-Emergent Adverse Events
NB-301 & NB-303 NB-304 (Diabetes)
Placebo Contrave 16 Contrave32 Contrave32
Overall Treatment-Emergent Adverse Events
68-85% 80% 83-86% 90%
Nausea 5% – 7% 27% 29% – 30% 42%‡
Constipation 6% – 7% 16% 16% – 19% 18%
Headache 9% 16% 14 % – 18% 14%
Vomiting 2 % – 4% 6% 9% – 10% 18%
Upper respiratory infection 10% – 11% 9% 9% – 10% 8%
Insomnia 5% – 7% 6% 8% – 10% 11%
Dizziness 3% – 5% 8% 7% – 9% 12%
Dry mouth 2% – 3% 7% 8% – 9% 6%
Nasopharyngitis 5% - 14% 6% 5% – 8% 8%
Diarrhea 4% - 10% 5% 5% – 6% 16%
Note: Represents adverse event experience in trials NB-301, NB-303, NB-304. ‡ Nausea rate for patients not taking Metformin = 27% Data courtesy
Orexigen

Treatment Discontinuations due to Adverse Events
NB-301 & NB-303 NB-304 (Diabetes)
Placebo Contrave16 Contrave32 Contrave32
Overall Discontinuation Rate 41% - 50% 51% 46 – 49% 48%
Discontinuation Rate Due to AEs 10% – 15% 22% 20% – 24% 29%
Nausea + 5% 6% 10%
Headache + 2% 1% – 3% 2%
Dizziness + 2% + +
Vomiting + + + 3%
Depression 0% – 2% + + +
Insomnia + + + +
Anxiety + + + +
Diabetes mellitus (worsened) + + + +
Note: Represents adverse event experience in trials NB-301, NB-303, NB-304. (> 1% in any arm)+ Incidence < 1%
Data courtesy Orexigen
28
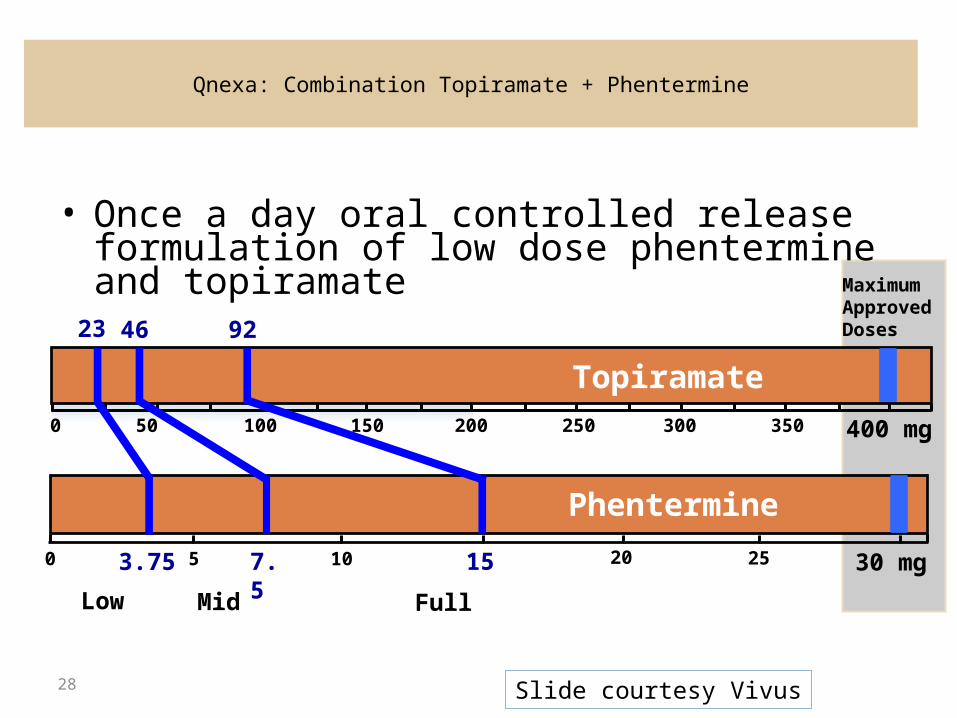
Qnexa: Combination Topiramate + Phentermine
• Once a day oral controlled release formulation of low dose phentermine and topiramate
0 400 mg200100 30050 150 250 350
Topiramate
0 30 mg
155 10 253.75 7.5
Phentermine
Maximum Approved Doses
20
23 46 92
Low Mid Full
Slide courtesy Vivus

Baseline characteristicsCONQUER n=2487 EQUIP n=1267
Age 51 43
Female 70% 83%
Baseline BMI 36.6 42.1
Weight (lbs) 227 256
Waist Circumference (in) 44.5 48
History of Hypertension 69% 25%
Blood Pressure (mmHg) 128/81 122/77
History of Dyslipidemia 57% 19%
Total Cholesterol (mg/dL) 205 194
History of Psychiatric Disorders 30% 26%
History of Diabetes 16%
Data courtesy Vivus
Topiramate + Phentermine

Results at 56 weeks
EQUIP CONQUER
Low dose Full dose placebo Mid dose
Full dose placebo
Retention 57% 59% 47% 57% 64% 69%
Wt loss LOCF 5.1% 11% 1.6% 8.4% 10.4% 1.8%
Wt loss observed 7.0% 14.7% 2.5% 10.5% 13.2% 2.4%
>5% weight loss 45% 67% 17% 62% 70% 21%
Data courtesy Vivus
Topiramate + Phentermine

31
Patients Placebo
QnexaLow
QnexaFull
Randomized 514 241 512
ITT Population1
(% of randomized)498
97%234
97%498
97%
Completers2
(% of randomized)241
47%138
57%*301
59%*
1 ITT Population = randomized patients with at least one dose of therapy and one post randomization assessment
2 Completers = randomized patients completing 56-week study on drug therapy
Completion Rates with Topiramate + Phentermine
32
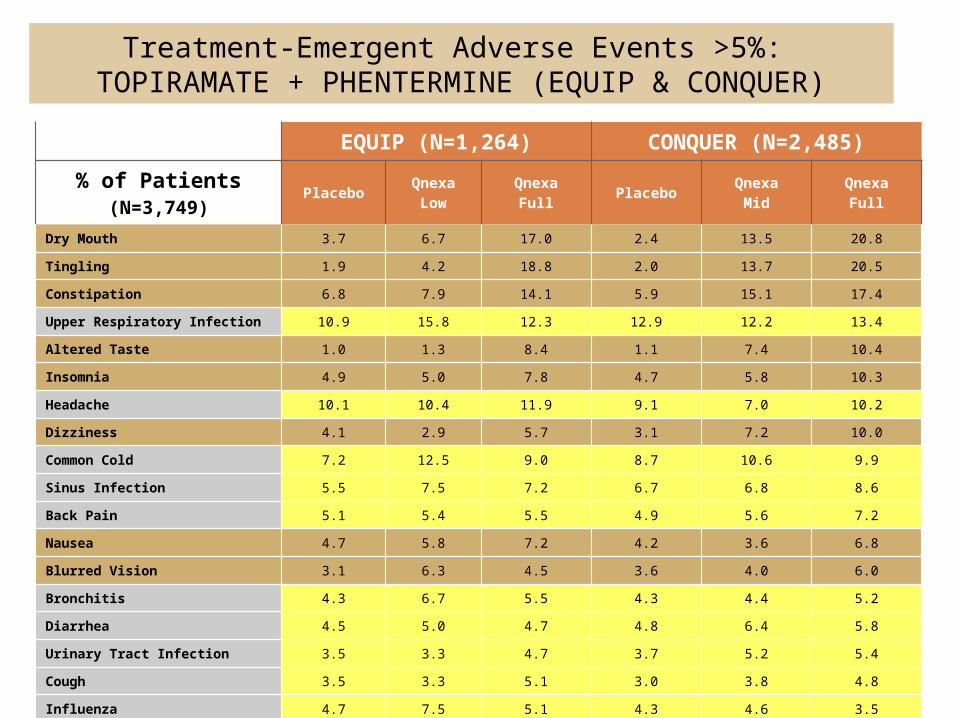
Treatment-Emergent Adverse Events >5%: TOPIRAMATE + PHENTERMINE (EQUIP & CONQUER)
EQUIP (N=1,264) CONQUER (N=2,485)
% of Patients(N=3,749)
Placebo QnexaLow
QnexaFull Placebo Qnexa
MidQnexa
Full
Dry Mouth 3.7 6.7 17.0 2.4 13.5 20.8
Tingling 1.9 4.2 18.8 2.0 13.7 20.5
Constipation 6.8 7.9 14.1 5.9 15.1 17.4
Upper Respiratory Infection 10.9 15.8 12.3 12.9 12.2 13.4
Altered Taste 1.0 1.3 8.4 1.1 7.4 10.4
Insomnia 4.9 5.0 7.8 4.7 5.8 10.3
Headache 10.1 10.4 11.9 9.1 7.0 10.2
Dizziness 4.1 2.9 5.7 3.1 7.2 10.0
Common Cold 7.2 12.5 9.0 8.7 10.6 9.9
Sinus Infection 5.5 7.5 7.2 6.7 6.8 8.6
Back Pain 5.1 5.4 5.5 4.9 5.6 7.2
Nausea 4.7 5.8 7.2 4.2 3.6 6.8
Blurred Vision 3.1 6.3 4.5 3.6 4.0 6.0
Bronchitis 4.3 6.7 5.5 4.3 4.4 5.2
Diarrhea 4.5 5.0 4.7 4.8 6.4 5.8
Urinary Tract Infection 3.5 3.3 4.7 3.7 5.2 5.4
Cough 3.5 3.3 5.1 3.0 3.8 4.8
Influenza 4.7 7.5 5.1 4.3 4.6 3.5
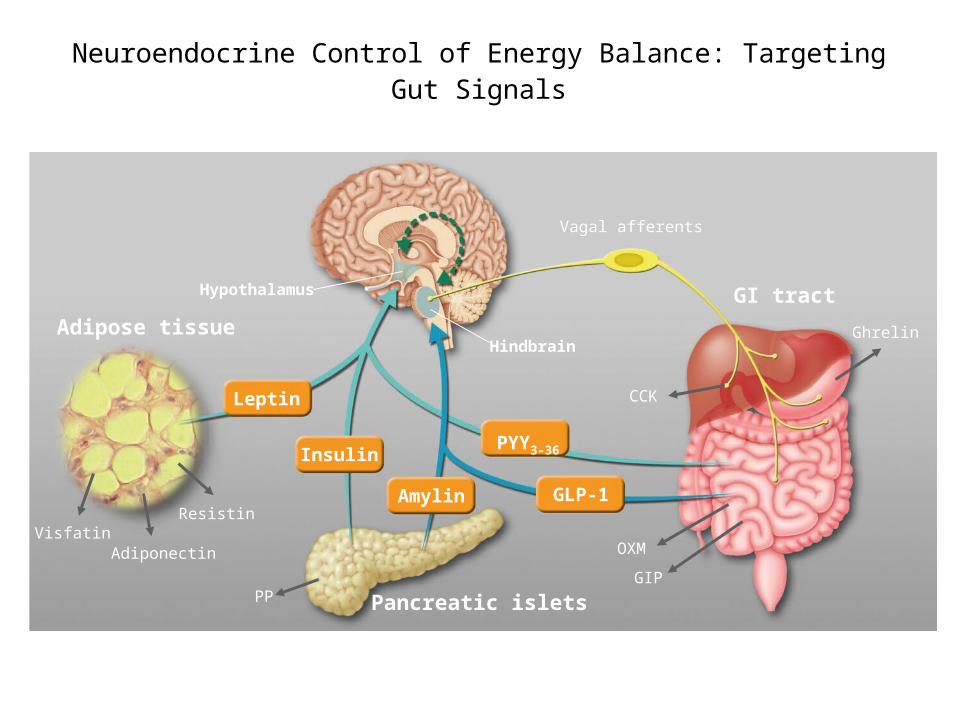
Neuroendocrine Control of Energy Balance: Targeting Gut Signals
GI tract
Adipose tissue
Pancreatic islets
Hypothalamus
Hindbrain
CCK
Adiponectin
Insulin
Amylin
Leptin
OXM
Ghrelin
GLP-1
PYY3-36
GIP PP
ResistinVisfatin
Vagal afferents
Adapted from Badman M.K. and Flier J.S. Science 2005; 307:1909-1914.

Weight loss effect of combined amylin and leptin agonism in DIO rats and overweight/obese humans
Roth J D et al. PNAS 2008;105:7257-7262
©2008 by National Academy of Sciences

Conclusion
• Imagine a world… – where there are nine classes of drugs for managing overweight and
obesity,– where there are minimally invasive devices and surgery for obesity, – where there are sophisticated risk engines to determine health risk
from obesity and comorbidities and directs treatment approach, – and where there is reimbursement for medical and surgical
management of obesity.